The Corona Virus –What You Need to Know
The first episode on pandemic freedomwith Dr. JudyMikovits
Dr. Michael: Welcome to an hour of HealthMade Radio. HealthMade is a community for natural health seekers where we educate people about common health conditions, share extensive research on the most effective natural health treatments, and promote legislation that protects our health freedoms. A core concept belief is the innate intelligence and healing power of the body; and if properly supported spiritually, emotionally, and nutritionally, it can find its way back to health.
HealthMade radio will bring information from integrative health experts throughout the world. Check us out at HealthMade.co. Health is what you make it. I am Dr. Michael Karlfeldt; I will be your host. Today's guest is Dr. Judy Mikovits.
What You Should Know about

Dr. Judy Mikovits: Dr. Judy Mikovits has a Ph.D. in Molecular Biology and Biochemistry with over 30 years of experience. She has directed programs on HIV, cancer, epigenetics, and neuroimmune disease with a focus on the development of novel drug and diagnostic technologies.
In 2011 when she made a horrifying discovery that was contaminating all vaccinations, she presented her data to government officials and was threatened and told to destroyall her data. Whenshe did not, she was jailed, her career systematically destroyed, and a gag order put in place for four years threatening that if she spoke out, she would be thrown back in jail.
The gag order has been lifted and now she’s talking. In this interview, she takes an hour sharing insight into: the release of the coronavirus in China, the impact that this double-stranded RNA virus has on the body,whether US citizens should be concerned about exposure, the ONE THING YOU SHOULDN’T DO out of fear of the virus, and many resources to help you create a confident immune system.
Dr. Mikovits has written a revolutionary book called Plague: One Scientist's Intrepid Search for the Truth About Human Retrovirus and Chronic Fatigue Syndrome (ME/CFS), Autism, and Other Diseases. The book details the discovery and consequences of retroviruses in vaccines and their effects on current health issues. She also has a new book, PlagueofCorruption:RestoringFaithinthePromiseofScience
Dr. Judy Mikovits was instrumental in our fight against HIV. She earned a Ph.D. in Biochemistry and Molecular Biology from George Washington University in 1992.
At The National Cancer Institute she developed purification methods for interferon alpha used in the first immune therapy treatment for hairy cell leukemia in 1986. In 1986-7, she developed production methods to ensure biological materials manufactured using human blood products were free of
contamination from HIV-1 —Her Ph.D. thesis changed the paradigm for the therapeutic treatment of HIV.
Her pioneering work during a twenty-year career at the National Cancer Institute includes the discovery of the modulation of DNA methylation machinery by human retroviral infection and the development of the concept of inflammatory cytokines and chemokine signatures of infection and disease —therapies that are still standard of care twenty-five years later and credited with saving millions of deaths from HIV/AIDS.
In 2001, she moved back to the industry where she directed the Cancer Biology Program of EpiGenX Pharmaceuticals. In 2009, Drs. Ruscetti and Mikovits’ labs isolated, for the first time, a new family of human retroviruses then identified as XMRV. In 2012, it was learned XMRV was a contaminant of The Silverman Lab and the XMRVs isolated were a new human exogenous and transmissible retrovirus family which are strongly associated with neuroimmune disease and cancer.
Dr. Mikovits has co-authored more than 50 peer-reviewed publications, and the book chapter and the book The Plague. And also, there's a new book coming out which is a sequence of The Plague. Is that correct Dr. Mikovits?
Dr. Mikovits: Yes, it is. It's called The Plague of Corruption and everything in it fits the topic we're talking about today.
Dr. Michael: And that is what I was thinking. We are going to be talking about the coronavirus, I know there is a lot
of fear and I want to hear from you whether the fear is founded. But tell the listeners a little bit about this coronavirus. What is that and is that something similar to something that you've seen before?
Dr. Mikovits: Yes. This coronavirus, that's a family of viruses of RNA viruses, double-stranded RNA viruses, and the one everyone will remember is SARS. SARS stands for Severe Acute Respiratory Syndrome. So, this SARS virus was a coronavirus and there's another called MERS, which again, these viruses tend to cause respiratory dysregulation, you know, so deaths are due to the respiratory tract infections.
And interestingly enough, interferon-alpha type one interferons are anti-viral and they're healing in these coronavirus infections and when peoplehave competent immune systems and they're not compromised, they're just fine.
So, if you can if you can increase the antiviral response, which is the type one interferon, with type one interferon, or products like "Paximune" and available interferon modulators, like cannabinoids increase type one interferes and decrease the excessive inflammation.
So, death and severe disease caused by an over-response of inflammatory cytokines, that you just discussed in my background, as well as inhibition by the viruses themselves of the type one interferon pathway.
Dr. Michael: So at the end of the day, if you support your immune system properly, if you have a strong healthy immune system especially, you
know, the respiratory component is very important. The nasal passages and respiratory are very important, and also, then control the inflammatory aspect.
Like you're saying that these retroviruses or the coronavirus triggers an inflammatory response, a cytokine response, that can be what is pushing the body over and can't handle it anymore. So, there are ways that you're mentioning that you can control this?
Dr. Mikovits: Correct. There are natural ways to control it; the way we would control retroviruses or other RNA viruses like: Coronaviruses, Influenza viruses, Measles, Mumps, Rubella. RNA viruses, different classes of viruses, are controlled by these innate pathways: the frontline of your immune response. So yes, keeping healthy nasal passages, vitamin C, vitamin A products that keep your immune system strong. The product I like is Paximune, which is a protein that is an immune booster and is good against all of these conditions —and it's a spray.
So, it sprays right away and can give you that type one interferon response it derives it promotes a type one interferon response. So, it's a very effective immune booster. Hence, these natural immune boosters and vitamin C will block excessive inflammation and excessive proinflammatory cytokines through, you know, IL1, IL6, IL8 are things that we know in these excessive immune responses which are driven by vaccines.
So, one of the most important things, essentially, anyone can do to protect themselves from this coronavirus is not to get a vaccination of any kind. Especially not influenza because that's a different kind of RNA virus and you will drive that excessive inflammation. Well, a coronavirus infection
would then suppress that type one anti-viral immune response which is critical to prevent the over replication of the virus.
Dr. Michael: So, that's interesting because most people think, "well, I should get my vaccines so that my immune system is stronger." But what you're saying is that getting a vaccine that is not specific for this virus will then drive an inflammatory response that if you're then exposed to the coronavirus, will add to that inflammatory response and now, you're double hit. In addition to that, it then creates that the energy of the body is focused on something else and can't focus on the coronavirus.
Dr. Mikovits: Correct. And the coronavirus encodes its major proteins; what it does is stop that type one interferon response. And then, more replication of that virus itself drives further pro-inflammatory cytokines and I would say any vaccines as well. That is nice what you mentioned, the XMRV being lab-created in The Silverman Lab that wasn't the family of viruses we isolated that came from the mouth tissue and were contaminating vaccines in the blood supplies for at least the last 30 years; that's how they got into people. So, the vaccines not only has known theoretically antigens from RNA viruses, but they also carry other animal RNA viruses, including retroviruses, which severely cripple that type one interferon response and your ability to respond.
So really, with the toxic nature of 21st-century vaccines, you really don't want any vaccine: pneumonia, even to bacterial agents because those are loaded with metals like aluminum and mercury which cripple your immune system as well.
Dr. Michael: So, going back again to vaccines. Here first, we're talking about that it will trigger an inflammatory condition, which will make it even worse to deal with if we're exposed to the coronavirus. And then in addition to that, it confuses the immune system because it starts to hunt for something else rather than the coronavirus. But then we also have the impact of some of the adjuvants and preservatives that exist within the new vaccines like aluminum, mercury, and so forth.
And then, you're telling me also that the vaccines are tainted with other retroviruses or RNA material. You were talking about the XMRV that has tainted the supply of vaccines. So, we're dealing with all these different factors thinking that they're going to benefit us but in essence, it's completely the opposite.
Dr. Mikovits: Correct. And so, it's the idea that the evolution or the release of this particular coronavirus. This coronavirus is not a retrovirus. It's just a double-stranded RNA virus which makes it easier for the immune system of the immune-competent— for a healthy immune system to clear. It is simply because, theoretically, it cannot integrate into your genome and stay through your lifetime or your generation.
Therefore, if you have a competent immune system and you have your type one interferon responses, if you have your RNA cell gene thus, in all of your RNA there are some pathogen recognition receptors that recognizes this entire family Whether it be: RNA virus, simple RNA viruses, single strand, double-strand, or retroviruses, your immune system has multiple ways which we call pattern recognition receptors.
Therefore, natural products such as cannabinoids will block excessive if pro-inflammatory cytokines like the NF Kappa-b pathway and drive towards a type one interferon response which is critical for clearing this coronavirus. Thus, the idea is to keep a very healthy immune system vitamin C will do the same thing.
You can look at formulations and combinations of foods, of natural products, and in natural sprays that you can get to keep your immune system healthy. Because of the way this particular strain this new coronavirus appears to have been released through manipulation of bat and bat tissue is what people think. The bat is one of the hosts of coronavirus. Camels are hosts of coronaviruses that were related to an outbreak a few years ago which have something called MERS; and it's the one and SARS I think as well came from bats in 2011 or '12. So, the management of these RNA virus infections is important and simple by keeping your nasal passages intact.
Keep your respiratory system healthy and not having co-infections such as: respiratory syncytial viruses, pneumonia, influenza, those other things that affect it. It is the immune-compromised who are most likely to succumb to the disease or have the most severe forms of the disease.
Dr. Michael: So, here you're saying then that you shouldn't have the influenza or pneumonia and these things are immune compromising? I just want to highlight the point again, that people don't think of the vaccine as a protection against those, but what you're saying is that the real protection is things like your natural agents like: vitamin C, like vitamin A, and also then controlling the
inflammation with cannabinoids because when the inflammation is controlled, then these immune system components that are protecting us become more active and available.
Dr. Mikovits: Exactly.
Dr. Michael: And tell me a little bit about how cannabinoids —are we talking about hemp? Are we talking about THC, CBD? I mean, what are we talking about? Are there other herbs as well that have cannabinoids? Tell me where do we find these things?
Dr. Mikovits: Oh, absolutely. YesterdayI gave a talk at the Hemp Culture Expo in San Diego and we were talking obviously about this very topic and I'll provide you after, my slides to that talk. But yes the natural products are the cannabinoid receptors and we have an endogenous cannabinoid system and it's a key regulator of immune balance neuroimmune health immune homeostasis.
Every aspect of your physiological signaling comes through this receptor family and there are dozens, if not hundreds of these. So many plants and natural products not just hemp or other strains of cannabis, but things like beta-caryophyllene and natural products terpenes; all cannabinoids are terpenes, but not all terpenoids are cannabinoids, so you can take advantage of synergies.
For instance, lemons have terpenes, limonene, linalool alpha-pinene— they're a natural product in many, many foods that are very stimulatory and contain healing properties, calming the inflammation. I consider them a dimmer switch on the fire. So, they're not the on/off switch that the
immune cytokines and chemokines times we were just talking about are; but they are a dimmer switch.
So, there are many, many of these cannabinoids and terpenes in nature, and you can take advantage of synergies in these foods and in these natural plant products to keep your immune system strong. And of course, many companies now sell very high quality of adaptogenic herbs including cannabis full-spectrum products to calm that fire because the way that the coronavirus is going to produce the most severe diseases: number one, inhibiting the type one interferon pathway.
So if replication goes unchecked then that replication can turn the flames up as high as possible. If you can dim the flames, and calm the flames, and keep them from getting too high so they don't produce too much tissue damage from the host response to the unchecked pathogen —you win the game.
Dr. Michael: Oh, yeah, so here we have something that we've been fighting so hard to have access to talking about hemp products, and that ended up being the thing that saves the day when we're exposed to these kinds of things. And it is not the vaccines that seem to be the solution. It's these natural substance that have been around for eons of time.
Dr. Mikovits: Currently correct. And in fact, it's interesting because as you read my biography that my earliest work was as a natural products chemist, simply isolating. As I mentioned, I put the first isolated, the first interferon alphas, which we put in humans as antiviral agents for cancer, and of course we then developed similar products for AIDS. I developed natural
products for cancer, breast cancers, known as "Adriamycin". We call it "The Red Devil" , but it's from a red plant. I was a bucket chemist in the early 80's. And so, we're going right back and this product that I have talked about over the weekend called "Paximune"— youcan get it online at boostmyimmunesystem.com.
I had to go way back in the literature because we developed these products back in the early 70's and 80's. And they control all of the things we're thinking of, and that's really why we got a handle on treating HIV and other retroviruses, influenza, pneumonia, whooping cough flu.
Yes, it's natural products, immune boosting, homeopathic and just simple vitamin C immune health that is the staple of the health of our immune system; and they can be found in our diet. And yes, it's not the vaccines, it's the overuse of vaccines that are causing a crippling to the immune systems as we've been discussing.
Dr. Michael: So, regarding the coronavirus, I'm curious I mean, since all of these different viruses seem to be coming from some kind of animal, how do we get it? I mean, they are supposed to be living in the animals, not in us.
Dr. Mikovits: Well, unfortunately, this is the topic of our book,Plagueof Corruption. This was the unfortunate thing we found when we started isolating the mouse viruses from humans with these diseases that had been skyrocketing up. The problem is that as we manipulate viruses in animal tissues in our lab, we can't clean these animals tissues out of the vaccines.
So, what we're doing is attempting to attenuate, that is, weaken these viruses by passing them through other animal tissues in the process, which is called zoonosis.
What you'll be told by the government is that the zoonosis occurred naturally. Let's just say, "somebody forgot to cook the food, right?"
That's what we heard in China with this coronavirus. "Oh! it was a wet market and contaminated game from a vendor, and improperly cooked food from the wet market."
What it actually came from was a biosafety level four facility about ten miles away from that food market where the animals were being sold as food; where the viruses were being cultured in other animal tissues with the attempt to attenuate them and weaken them.
And what happens, because we're not God, is we make a stronger, more kept pathogenic virus that was released apparently from that laboratory and has acquired the ability to infect humans cells more easily and cause more disease because it has sequences of other viruses, including HIV sequences, that have been found in this that come from the labs.
So when we manipulate viruses in the laboratory in animal tissues, we grow these in fermenters; and the way we've done our work, and the reason I can speak with such knowledge is because: in 1992, I worked in Fort Detrick's biosafety level 4 lab, which is similar to the Wuhan facility. I was working with Ebola to teach it to infect human macrophages without killing them because we can't study the viruses unless we can grow them in cell lines.
In fact, that virus beat was released, and is the strain of virus that killed more than 21,000 people in Liberia in an outbreak in 2014. We were told by our government that this was the Zaire Strain. And again,
somebody forgot how to cook their food or coexist with a virus that coexisted with the animals, and eaten those animals for millions of years, and all of a sudden it jumps into the human species.
Well, you can look at the virus and sequence the virus and see that that there were more than 300 mutations in that Ebola strain from those Zaire strains that were the natural virus. So, zoonosis is when an animal virus jump species, whether it be from humans to animals, or from animals to humans. We were told that this coronavirus came from bats and meat, or a market near Wuhan and we have clear evidence, and I think it's been admitted now by the authorities and by the scientists involved that they've been manipulating these viruses for more than a decade in the laboratory the biosafety level 4 laboratory in Wuhan, China.
And this work was even funded by the NIH. So it's no different in the story in Plague of Corruption. We now know the cost. We've known the costs for at least a decade or 15 years since we've seen these huge outbreaks of diseases like: Autism, Myalgic Encephalomyelitis, Chronic Fatigue Syndrome, cancer, cancer, cancer; you're dealing with it every day. Cancers associated with these RNA viruses and retroviruses and yes they've come largely from our laboratories and this one's no different.
So, concerning Americans: Americans aren't at risk from this virus. It's almost certain that it has infected a lot of people here I do see it in the news; I try to keep it off. But I do see that they're going to start mandating that we get vaccinated for this virus. And isn't that convenient that they have already made a vaccine for this virus? And again, that'll make people sicker.
This is the same thing as H1N1, so everybody's scared; everybody with the H1N1 flu, I guess, it was back in 2010: we developed a vaccine and forced the vaccine on everybody through fear or mandates. And it's that vaccine from that H1N1 that was the most pathogenic; we've done dozens of cases in vaccine court for the damage done and the people killed by the vaccine.
So, we have essentially no risk of exposure to the coronavirus released from Wuhan, but we're at great risk from the things they will try to force upon us if we don't have the knowledge to say "no" to that or resist that and maintain our health freedoms.
Dr. Michael: Yeah, that is fascinating how conveniently we just happen to have a vaccine for the outbreak.
Dr. Mikovits: Correct.
Dr. Michael: That is pretty convenient. So, you're saying that we're at no risk here in the United States? I mean, can you just repeat why have we no risk here?
Dr. Mikovits: Well, the virus was released somehow from Wuhan China. So, they've quarantined people traveling from that area I don't see how we would because human to human transmission is essentially the only way, we're going to get it.
They've already stopped travel from China. They've got a detection how convenient they also have a way to make money and to detect this virus, which, I'm sorry, I don't trust anything they do.
So, I'm laughing because it's decidedly not funny but I mean, certainly, health care professionals but because there are many coronaviruses in nature, we were at little risk of exposure to SARS back a few years ago.
And the virus from India, called MERS, causing the upper respiratory infections; so the only risk is from the contaminated vaccines. Where did the vaccine come from and how did they make it?
You can't make a vaccine without having an antigen. So, where'd they get the Antigen? What tissues? What animal tissues are they growing it in? And why would you inject something like that into you?
Dr. Michael: I agree. I'm just curious and now we're concerned about the outbreak of the coronavirus and thinking that it's pointed towards contamination of these manipulated viruses and pathogens that then leave the lab, so to say, and how do they leave the lab? You're in a level 4 lab. I mean, how does something that you're experimenting on gets out?
Dr. Mikovits: Yeah, I mean, that's a really good question. Biosafety level 4 laboratories like you see there at Fort Detrick that I worked in, I mean, I was completely gowned up and had my air supply through a suit that looks much like a spacesuit.
I was perfectly prevented from any kind of exposure. But of course, what are we releasing into the air and the water? Only God knows. So how do they get them out? We're producing something in those labs, and we're adapting them to grow in mouse cell lines, cow cell lines; look at the list of cell lines used in our vaccines. And we cannot filter all of the cell material or all of the viruses out because they're all RNA viruses. Hence, whether it be retroviruses we don't filter on because we don't check for them now. So anytime you make a product in fluids, we know that these things are not the things we're doing in mice that we call "mouse biosafety level 2," which means: you don't have to have
specialairflow; you don't have to autoclave on the trash;the water's not kept; the air is not checked out of the buildings.
We know around Fort Detrick, Maryland many, many people who were infected with the XMRVs and the mouse viruses develop diseases like multiple sclerosis, cancer, and just so much worse. Thus, we know these things were released at Fort Detrick during 9/11; God only knows how that got there as well. But again, we're using cell lines and animal tissue, and we're growing that at very large scale: 200, 300 liter fermenters. These are aerosolized in viruses as well; it doesn't take much to release them.
And I have no idea how the virus was released from the Wuhan facility. But again, it doesn't take much since they're airborne and they can spread through the airwaves and the nasal passages.
Dr. Michael: And you're matching, so yeah, that's an interesting point. So how does this virus move from one person to another if you said it's from person to person, and then also you're saying that it's airborne? So how does one get infected?
Dr. Mikovits: Sneezing you know, coughing.
Dr. Michael: Yeah.

(Wuhan Lab)
Dr. Mikovits: Just like measles, just like influenza. You know that it's a cough. Its upper respiratory infection nasal passages are the easiest way. And so, this one's aerosolized much easier so contagious, you're just coughing, sneezing and you won't even know that you got exposed. I believe, it's like a five day incubation period of before you develop any of the symptoms, which are: fever, malaise, fatigue,
body aches, cough and sneezing, like any upper respiratory infection. It could even be masked as allergies.
And there's evidence in a few papers about mast cells, the other innate immune response primary response So mast cells, our allergic responses could even masquerade as an allergy. So, one might think one only had an allergy if they hadn't been in an endemic region. So the reason I said we have essentially no risk of being exposed is that the endemic region is thousands of miles from here.
And now it's pretty clear that it was released from that facility. So, lab workers and the doctors, are the ones at most risk of exposure. And it is easy enough to protect them with, vitamin C, cannabinoids, natural products, beta-caryophyllene that modulate that cannabinoid receptor, which is primarily modulating inflammatory responses.
Dr. Michael: And in your book, The Plague, you talked a lot about what we've been mentioning: the XMRV vaccine; and you were exposed to it and the lab that you were working in?
Dr. Mikovits: Correct.
Dr. Michael: What happened to your co-workers? I mean, what would we see because now you're all exposed to this. What kind of health impact did it have on the people that were exposed?
Dr. Mikovits: Well, many of us were infected. I was infected zero converted in 2010, meaning, I developed antibodies and had very high levels of viral proteins. I think you can hear it my voice now. It is somewhat raspy.
Thus, my colleagues, my co-workers: several people with multiple sclerosis, liver cancer, co-infections, in some cases with hepatitis when I
worked with HIV. We were all encouraged, if not required to get the HBV hepatitis B vaccine. The early Hepatitis B vaccines in the early 90's,
when they were made, they were made from human plasma. So, now we know we acquired infections from those as well, which could compromise our immune system. Therefore, I'm at increased risk for cancer; I've had quite a lot of problems with my lungs.
And you know, my friends and several of my colleagues are dead from their tumors from working with these viruses, retroviruses from the XMRV, which simplymeans the xenotropic murine leukemia related viruses. So, retroviruses and murine leukemia viruses obviously cause cancers.
So many of my colleagues are dead for cancers. The blessing that I had was that I work most of my life in biosafety level 3 or 4 facilities. So, the big fraud that the government has continued to play on lab workers, first responders, doctors, nurses, health care professionals is number one: forcing them to get vaccinated and spreading the infection through them even further by weakening that immune response as we discussed.
And number two: declaring without any reason that these biosafety level 2 reagents unintended spread of a biosafety level 2 reagent and yet our or infection.
And at the same time in the chapter of my first book of The Plague, the chapter with the invitation-only meeting that is a highly secret meeting that was held on July 22, 2009; The big "oh my god, wasn't that the animal caretakers and lab workers who are getting infected that is zero converting exposed?" Clearly, this was the first human retroviral virus family that was aerosolized and contagious, like this coronavirus.
The "Oh My God" is, we can't afford to retrofit our labs so that everybody working with mice can prevent themselves from being infected with mouse
cancer-causing viruses which are released in essentially every biological drug we've made since the 90's.
Dr. Michael: That is an "OH MY GOD" and...
Dr. Mikovits: It's an "OH MY GOD"
Dr. Michael: Yeah, and to me, because this just highlights when we have these different outbreaks that are impacting people on such a massive scale to understand what is the driver behind that because we've been exposed to all these different pathogens for eons of time and our immune system have figured out how to deal with them.
But now like you're saying when we're playing God, and we're we're mixing genetic material. We take a little bit of HIV and then put that into that, and all of a sudden, we have to deal with pathogens that your immune system is not equipped quite yet to figure out how to deal with.
Dr. Mikovits: And the sheer amount of these pathogens to which we're being exposed, and I would say unwittingly exposed because we're being lied to about being injected with them. And earlier this year, maybe 2019, the CDC, The Centers for Disease Control, changed the excipient list of vaccines to simply remove all the animal cell lines that were listed previously because we've been talking about them for a decade.
So, it's not that the cell lines that the vaccines are no longer being made that way, that there's not aborted fetal tissue. And remember: when we get tissue from another human being, they have their component of endogenous retroviruses, which had been previously crippled by the immune system or suppressed so they can't be expressed.
But when you inject them as a provirus or pieces of a provirus, and you've injected them in the quantities, the incomprehensible quantities, that these vaccines have, have been ingested into the population particularly in the immune-compromised; in infants that don't have the machinery already developed for a healthy microbiome, methylation machinery; all these pathways we're discussing and now we know to be antiviral and develop immunity and the very old whose immune systems are weakened.
So, what do we do? Oh, we inject four times as much in the very old, recognizing their immune system is weak, and that is a stupid. But we're being lied to. I mean, why would you inject four times as much?— and this is the influenza vaccine. And then, of course, The Corvelva Group showedrecently how many contaminants how many different? I think there were aquiline viruses, 11 different kinds ofhuman endogenous viruses, retroviruses, mouse, pig, cow, bovine, dog look at the excipient list.
And you'll have to go back and look from 2010 through about 2017. Because the CDC, when they got caught, they simply eliminated it from the list not that it was eliminated from the vaccine. Let's just confuse the people and the doctors who are trying to do the right thing for their patients and let them know.
But one thing I'd like to say maybe after the next break, but I want to discuss, you know, how we can stay healthy again. Because that was why I said our word changed the paradigm, and, you know, I'm not concerned with my XMRV infections because, of course, I've moved to the therapeutics with the cannabinoids; with the Paximune back to the products that stimulate type one interferon response back to natural health where we can heal from all of these diseases.
And that's what we want to make available and so that your patients are well aware that we don't have to live in fear that we're wonderfully and fearfully made by God and we have not only the resources, but the knowledge to fight this.
Dr. Michael: I actually would like to get to that aspect right now. What do you feel would be the best? We talked about cannabinoids; you talked about vitamin C. What do you see as being good protection against all the exposure that we're dealing with?
Dr. Mikovits: Well, I use everything. First of all: a healthy diet no GMOs in any of it as many natural products as you can. I do use this point product and, you know, because it is a point in time that we need more than just food.

So, first I use healthy foods and make sure my diet is clean as possible. Stay away from inflammatory foods, away from gluten. I eat very clean meat; vitamins A,D,K and E, and cod liver oils.
I know that you know vegan is an aspect but it's always, you know and vegan diets are thought to be healthier, but the amount of glyphosate, Roundup, and the contamination of our food makes it very difficult to get enough healing through our diets.
I use lots of berries to get vitamin C from. As I said, lemons and I just work very hard to keep a clean diet first and foremost for a healthy immune system.
And then I have some go-to products because not all cannabinoids in the products are healthy and well made. So, we work with many companies worldwide. I've worked the past
few years, closely with Chris Shade, who is brilliant in these formulations and has the laboratory.
So, Chris has the company, quicksilverscientific.com, and he's made a couple of new products which one is called "Microb-Manager", a fabulous detox called "PushCatch," where the "catch" has a patent-pending. I forgot what the name of what the compound is, but the "Ultra-Binder" is the only thing on the market, that I'm aware of, that can clear mercury.
So, from the flu vaccines, every multi-dose flu vaccine which is what most of America gets, has mercury in these, and it further cripples the immune system
Of course, I don't get any vaccines, but there are products in the formulation so, take advantage of adaptogens because the THC is the easiest way to modulate CB-2 from the cannabis plant. But according to our laws, in most states, you can't get and use THC. So, you need to think about other modulators of that cannabinoid two, that CB-2 receptor. And there are a number of them, you know, as I mentioned earlier: beta-caryophyllene, some of the hops, some of the lemon, limonene, linalool, alpha- and beta-pinene. So, these are things that can be used to take advantage of synergies, and there are some excellent products out there for doing that.
Therefore, to support your immune system, and I take very little, I get really good sources of vitamin C. I'm not a supplement promoter or taker; I do very few things. I use the product that Zack Bush, the endocrinologist, developed called, "Ion Biome." It comes in a nasal spray and in a gut product that you can take for the gut.
It restores the nasal passages, so again with coronavirus, I would go first to making sure I have "Ion Biome" on my shelf now because I have been, and I do spray it, in my nasal passages so that I don't have cracked open membranes and inflamed membranes. So, as you can keep the fire down, the inflammation down, so you can keep yourself well.
Dr. Michael: Yeah and I think they've changed the name ofthe product from"Restore" to "Ion Gut Health. "
Dr. Mikovits: Okay.
Dr. Michael: Yeah, but that is a fantastic product that I use day in and day out at my practice, and like you're mentioning your nasal passages —yeah, we think of the gut as we need to bring in healthy bacteria to heal the gut, but we have biome in all these different locations.
We have it on the skin; we have it in the ears and in the nasal passages, and on the eyes; and we have this kind of the culture different bacteria. So, to be able then to use this "Restore" spray to heal your nose bacteria is huge, and that creates that additional protection against these pathogens that are then spread through sneezing, coughing, etc.
Dr. Mikovits: Correct, and I should say, we don't smoke marijuana for medicinal purposes because with respiratory infections you do not want to smoke anything and we rarely do. We apply it as tinctures, oils, sub-linguals and sprays.
And again, some fabulous formulations are available. I know several companies I'm not intending to give commercials, and you know I don't have any vested interest in any these are just products that I've developed with scientists and worked with, basically
because of what we learned with in the last decade, in The Plague. In 2011, when our research was stopped on the XMRVs. All of the so-called negative studies show that between 10 and 25 million Americans had been infected either through contaminated blood supplies or contaminated vaccines with these leukemia causing retroviruses and other diseases, other autoimmune and inflammatory chronic diseases.
And so, that's 25 million Americans who are going to be at increased susceptibility of whatever the next Corona, Zika, Ebola is. I guess it's unfortunate that nobody knows that in December of 2019, the World Health Organization admitted at an international conference that the vaccines weren't safe. As we know from Bobby Kennedy and Dell Bigtree's work, they were never tested safe as required by federal law for 30 years.
So, for 30 years, we don't have any knowledge whatsoever. Other than that, our vaccines are decidedly not safe. Our WHO, our CDC, our FDA just admitted it and were caught on tape at that international conference and as my jaded colleagues and I now said, "wait for it, there will be an outbreak".
You know, two weeks later you've got Wuhan and the coronavirus and, now they're giving themselves license to mandate vaccines for this, which is, as we've discussed, the worst thing we could do; but we can't stop "the plague of corruption" until we're all educated and aware of it. But we can protect ourselves from the diseases that are emerging thanks to The PlagueofCorruption.
Dr. Michael: Yeah, and the protection is, at the end of the day, it's our innate immune system and using natural agents to support it so it can do its
jobratherthanbombarding it withforeignmaterial,andchemicals,and heavy metals.
Dr. Mikovits: Correct, absolutely.
Dr. Michael: Dr. Judy, thank you so much for bringing allthis information at a time where a lot of people are wandering and trying to figure out what to do and how scared they need to be, what kind of precautions they need to take. So, this information was hugely, hugely vital. Thank you so much for taking the time.
Dr. Mikovits: Thank you, Dr. Karlfeldt, I appreciate it.
Dr. Michael: Thank you. That is it for today. You're listening to HealthMade Radio. Remember check us out at HealthMade.co, Health is what you make it.
Welcome to the second episode with Dr. KnutWittkowski

Listen to the full episode to hear Dr. Karlfeldt and Dr. Wittkowski answer these questions:
What about the Italian death toll; does America compare? How do epidemic figures compare to the non-response of Sweden, and its neighboring countries Norway and Finland? Does our current knowledge in the US give us an advantage in dealing with the outbreak? A vaccine – an appropriate solution? What about viral mutations?
In this episode of HealthMade Radio, Dr. Michael Karlfeldt discusses the nationwide response to the current health crisis with Dr. Knut M. Wittkowski, who has been modeling epidemics for 35 years. He is the former Chief Biostatistician and Epidemiologist at Rockefeller University Hospital. Dr. Wittkowski believes that our response to the virus is not only wrong but will increase the length of the outbreak and put the elderly and susceptible at a greater risk.
“With all respiratory diseases, the only thing that stops the disease is (natural) herd immunity,” the epidemiologist said. “About 80% of the people need to have had contact with the virus, and the majority of them won’t even have recognized that they were infected, or they had very, very mild symptoms, especially if they are children.”
HERD IMMUNITY
This term is widely used but not widely understood. Herd Immunity: a form of indirect protection from infectious disease that occurs when a large percentage of a population has become immune to an infection through previous infections, thereby providing a measure of protection for individuals who are not immune.
“As witheveryrespiratorydisease, we should protect the elderlyand fragile because when they get pneumonia, they have a high risk of dying of
pneumonia. So that is one of the key issues that we should keep in mind.
On the other hand, children do very well with these diseases.
They’re evolutionarily designed to be exposed to all sorts of viruses during their lifetime, and so they should keep going to school and infecting each other. Then, that contributes to herd immunity, which means after about four weeks at the most, the elderly people could start joining their families because by then the virus would have been extinguished.”
OUR CURRENT REACTION TO THIS VIRUS WAS BASED ON GUESSWORK & IT IS WRONG
Epidemiologists, public health professionals who investigate patterns and causes of disease and injury in humans, were left out of the discussion when models were developed for the outbreak of this flu, which resulted in the knee-jerk reaction to shut down schools and implement "antisocial" distancing. “It was all based on guesswork without a clear understandingoftheepidemicspread.”
“We did not take appropriate action with the knowledge we had.”
For example, China and South Korea reached a max peak of infections before implementing "social distancing," when the number of cases was already at a decline.
Their epidemic peak was four weeks; in contrast, here in the United States, it is taking a lot more time. By not allowing the virus to run its course, especially among the children who are at little to no risk of complications, our country is unable to develop herd immunity increasing the risk to those most susceptible.
HUMAN AND VIRUSES MUST CO-EXIST
The idea that we can and should eradicate viruses to keep us safe is counterproductive and quite impossible. Dr. Widtkowski explains it this way:
“The best course of action is to rely on what nature has come up with in the last 100,000 years. The virus enters the human population and stays there for a week or two. Its infection in the population rises -reaches a peakthen the number of infections declines, and in the end, the virus is eradicated. Why? Because there are many more people in the population that are immune than those that are susceptible. So anybody that brings the virus into the population would not bring any further infection. Its the initial course of any disease. Humans don’t need to do much about it.”
OUR RESPONSE IS BASED ON UNREASONABLE FEAR
Dr. Michael Karlfeldt explains the current reaction of individuals in the United States: “It is scary. This invisible virus can’t be seen, and it’s everywhere. Some people can be asymptomatic and spread it.”
“What you are describing – we go through this every year during the flu season. The flu enters the population, starts spreading, then declines. We never see it (it is always invisible). We never know who will be infected. Why is this year different? I don’t know. Maybe it is because the internet, the media, and rumors are spreading faster than any virus is spread. The President and Mayor of New York from one day to the next went from a reasonable to the unreasonable response. “
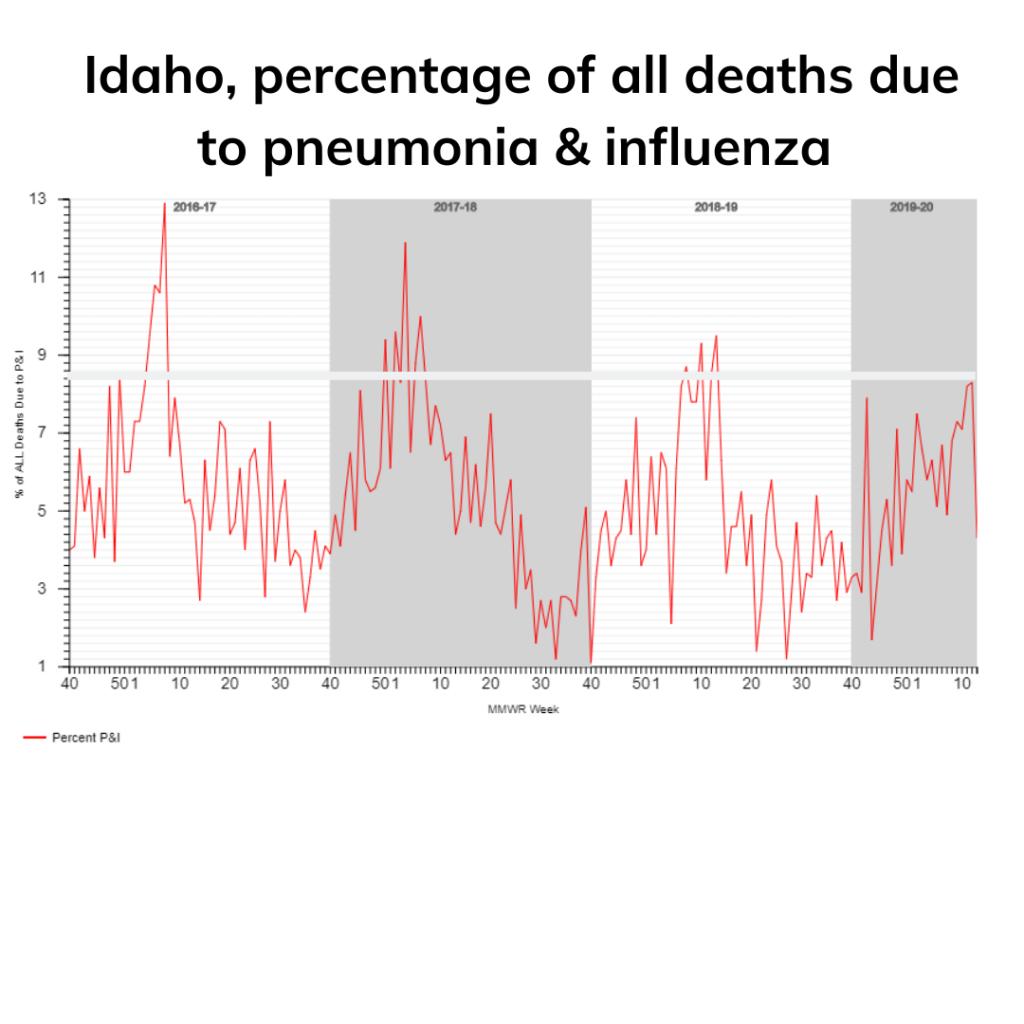
If we look at the data, what we are seeing is very typical for our annual flu virus. Every year, during the flu season, there are approximately 35,000 deaths. We have ten thousand who died from this COVID-19 flu, and even this number were doubled, it would still be of the lower end of what is regular for flu season.
Notice the RED LINE below from a CDC generate-graph reflecting FLU Hospitalizations.
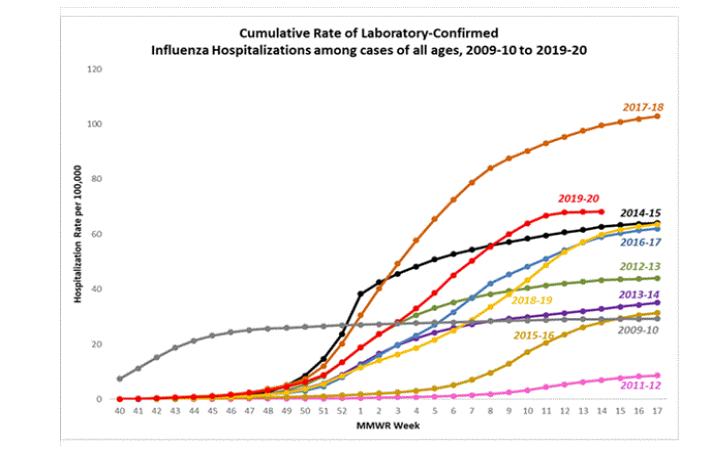
https://www.cdc.gov/flu/weekly/#S2
Let’s use Idaho as an example: Here are some statistics from April 4 from the CDC. It shows 299 flu deaths in Idaho. The Health Department is reporting 27 COVID-19 deaths. Combined these deaths are similar/less than previous years https://coronavirus.idaho.gov/ https://gis.cdc.gov/ grasp/fluview/mortality. html #stayhome
See Idaho Statistics from the CDC: https://gis.cdc.gov/grasp/fluview/fluportaldashboard.html
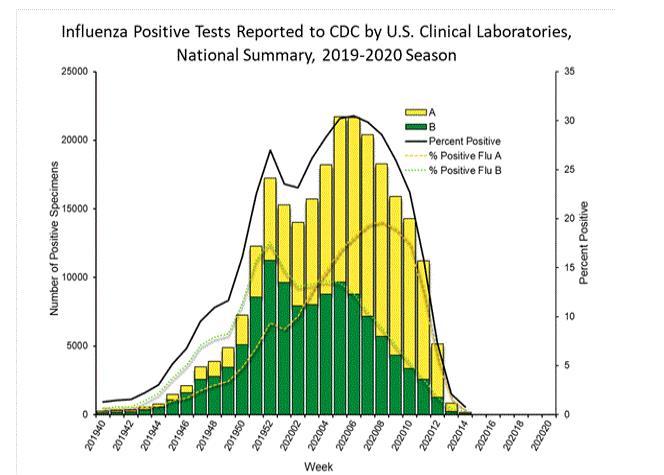
SHARP DECLINE IN FLU POSITIVE TESTS NATIONWIDE
Unfortunately, at the end of March, the CDC changed its parameters for reporting deaths from COVID-19. Now, anyone with the virus will be considered a death from the virus, even if it did not contribute to death.
A 61-year-old man dies from a head injury, but the virus was listed as a contributing factor to his death.
https://www.lehighvalleylive.com/coronavirus/2020/03/2nd-coronaviruspatient-dies-in-lehigh-valley-he-was-61-and-from-warren-county.html
DOES NOVEL MEAN MORE DANGEROUS?
No, "novel" means that a particular virus hasn’t been seen before. It doesn’t mean it’s more dangerous or kills more people. Every influenza virus that hasn’t been around for 15 years would also be considered a "novel" virus, otherwise, people would already have herd immunity, and the infections wouldn’t spread.
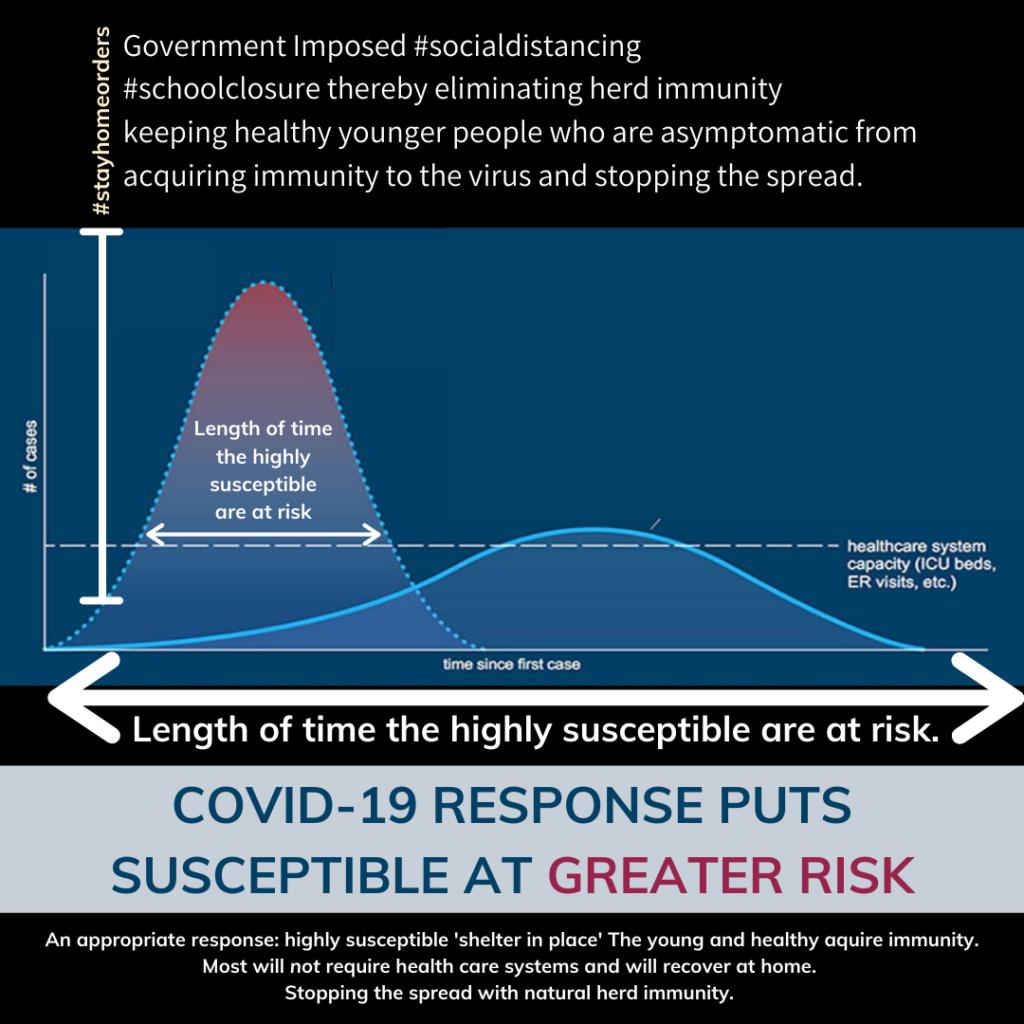
FLATTENING THE CURVE INCREASES THE RISK
There are several sources of data available worldwide, and if you analyze the data, it reveals that there is no major difference between these epidemic and other flu epidemics. The only major difference is: everywhere we see socialdistancing implemented, it takes more time for the virus to reach the levelof herd immunity; therefore, it stays in the population longer. This allows more time for exposure forthe elderlyand susceptible people at risk.
By flatting the curve, we are INCREASING the risk for the elderly and the number of deaths overall. It is better to let nature take the course.
CLOSING SCHOOLS, THE WRONG APPROACH
“Ifthere had been no intervention, the epidemic would have been over, like every other respiratory disease epidemic,” Wittkowski said. The virus should have been allowed to spread among healthy children and young people who generally don’t even experience symptoms. The entire population could have achieved herd immunity in two weeks. Wittkowski believes only elderly and at-risk individuals should have been isolated until herd immunity was reached.
What we have done has only prolonged this epidemic and prevent us from getting herd immunity, putting the susceptible at more risk for a more extended period of time. We have prevented the children from becoming infected and then immune, allowing the virus to spread among other parts of the population a portion of which is the elderly who are now at risk of becoming infected, seriously ill, and then might possibly die.
If schools had remained open, the virus would have been allowed to take its course naturally. Children would develop immunity, creating overall herd immunity. As the virus is actively circulating, the emphasis should have been on protecting the medically frail and those over age 60, and in particular, those over 70 and 80, from exposure.
IT’SNOTTHEVIRUSTHATISDANGEROUSITS OUR IMMUNE RESPONSE
We are not suffering from the virus being in our bodies. The danger comes with the immune response of killing all the cells that are infected, resulting in inflammation. The inflammatory response can create respiratory problems, bacteria on the inflamed skin, etc.; it is rarely the virus itself. The danger of relying on a vaccine is the potential for a vaccine that makes the immune response even more ridged. A more robust response could then cause the symptoms of the disease to get worse.
“Closing the schools probably one of the most destructive actions the governmenthasdone.”
THE CORRECT RESPONSE
The correct response will be to allow the virus to run its course, especially in our young people. Allow the children to go back to school.
Continuing this nationwide school shutdown this is the worst thing you can do, not only for the epidemic of the virus but also for the children. That will strengthen their immune system, build immunity, transfer immunity to their parents, and start to establish herd immunity and protect the elderly from this virus.
A correct course of action would be “preferentially protecting” the high risk and highly susceptible population. This course of action is something people have been doing for many years.
Welcome to an hour of HealthMade Radio. We bring information from integrative health experts throughout the world. Check us out at HealthMade.co. Health is what you make it.
I'm Dr. Michael Karlfeldt and I'll be your host. Today's guest is Dr. Knut Wittkowski. Dr. Wittkowski, it is such an honor to have you on the show. Can you please tell me a little bit about your background? Obviously, we're going to be talking about the pandemic that we're seeing currently and tell me a little bit about why you are the perfect person to talk about that?
Dr. Knut Wittkowski: I'm not sure if I'm the perfect person, but I think I have something to add to the discussion. I've been an epidemiologist for 35 years. I trained and worked with Klaus Dietz in Germany, one of the leading epidemiologists who actually coined the term "reproduction number."
I was one of the few early on that said that HIV would not spread into the heterosexual population and actually it was true. But it came out only after a couple of years and now I feel that I should raise my voice again because
I think that many of the interventions that are currently being tried and implemented are not well thought through.
Dr. Michael Karlfeldt: So, tell me a little bit about this virus; the coronavirus has everyone running scared thinking that all their elderly is going to die of any exposure. And now, it's impacting the younger population and thinking that we have to isolate ourselves in order to be able to protect ourselves and then just going to sit huddled down untilwe get the vaccine and then we will be safe finally. What are your thoughts in regards to how this has been taken care of so far?
Dr. Knut Wittkowski: As in every respiratory disease epidemic or flu, those who are elderly and fragile, and have co-morbidities should stay away and not try to expose them too much to the circulating virus. Other than that, it's probably the best to rely on what nature has come up with over the last hundred thousand years or so and that is a way for humans and viruses to coexist.
So, every virus comes and enters the human population stays there for a week or two and raises the number of people who are infected, rises and then reaches a peak, and in the next week or two the number of infections declines. In the end, the virus is eradicated because there are many more people in the population that are immune than those that are susceptible. So anybody who brings a virus into that population would not create any further infections and then the whole story is over. And it's a natural course of every disease and we don't really need to do much about it.
Dr. Michael Karlfeldt: So now, it sounds like you're talking about the term "herd immunity". Can you explain a little bit about what that is because that seems to be the solution in your eyes?
Dr. Knut Wittkowski: It's a term that is often used and often not well understood. So, as the disease spreads and people become infected after a week or so they become immune the vast majority of them. And as soon as there are more immune people than infected people in the population the spread of the disease stops; and about a week later it reaches a peak, and then declines again because then the majority of people are already immune and only a minority is susceptible.
Dr. Michael Karlfeldt: So the issue with this virus was it seemed like it was spreading; I mean, the estimations were that it was going to hit the population in such a massive wave that we had to take a massive precaution. What do you feel about those estimates that they were having? Were they based on good calculations? what were they based on?
Dr. Knut Wittkowski: Guesswork: Ihaven't heard any epidemiologists being asked and everything that was discussed was based on the opinion of people who didn't really understand how epidemics spread.
Dr. Michael Karlfeldt: Because the scary part is that it is a virus. You're looking at something you can't see and it's everywhere and you have no idea if you're exposed to it. And also, with this virus, people can be asymptomatic and can still be a carrier and then you can be exposed to it. Hence, there's a lot of fear because you don't know and you can't see.
Dr. Knut Wittkowski: What you are describing is what we go through every year during the flu season. The flu season is called flu season because there tend to be cases of flu. And so, every year we have the flu, and every year that flu enters the population it starts spreading; and then the spread declines and, eventually, it's gone. We can never see the flu: we never know
whether we are infected or not; and until this year, as The President said, "we have never shut down the economy for the flu."
Dr. Michael Karlfeldt: So, why are we taking such strong measures now versus if this is just the same as a flu season? Why are we taking such strong measures?
Dr. Knut Wittkowski: I have no clue. Maybe it is because the internet is now a medium where rumors are spreading faster than any virus could spread and then people get infected by these rumors and that's causing their fear.
It is also that, at least here in the US, I could observe that we had both the President and, in New York City, the Mayor saying on one day, "we're not doing anything because this is just the flu" and on the next day saying, "no, we are shutting down the country or the city." And I don't understand what is causing politicians, from one day to the next, to change from saying something reasonable to something that is unreasonable.
Dr. Michael Karlfeldt: So, I would assume that you as an epidemiologist would have access to the data that's available and also you would be the expert to read that data to see whether this is something that we need to react stronger to versus having just the same kind of precautions we would if there's a flu season.
Dr. Knut Wittkowski: The data, or a lot of data, is actually available. The New York Times makes data available, the European CDC is making data available, there are several sources for data available; and if you analyze it then you see that there's no major difference between this epidemic and other epidemics. The only difference that we see is that everywhere we're
social distancing, although I don't know how "social" that is, was implemented.
It takes more time for the virus to reach the level of, as you said "herd immunity," and therefore it stays longer in the population; and the longer it stays at the population the more the elderly and highly susceptible people are at risk. Therefore, whereby what people call "flattening the curve," they're increasing the risk for the elderly and the number of deaths. It is better to let nature take the course because nature has played with this for a very long time and we as humans are not always better than nature in predicting what is good to do.
Dr. Michael Karlfeldt: So, you're actually thinking that the social distancing was detrimental and that would then prolong this epidemic that we're dealing with, and then possibly prevent us and from getting herd immunity. Is that what you're saying?
Dr. Knut Wittkowski: That's what's happening. Now the argument is that people say they are afraid of their health system being overwhelmed, but if you don't shut schools then children will get infected most of them. And the vast majority of them will have no symptoms, or minor symptoms at most. And so, once the children are all immunized, we already have a high level of herd immunity and that will protect the elderly.
If we prevent the children from becoming infected and becoming immune then the virus is spreading among other parts of the population and that is the elderly who are at risk. So, by producing a new form of prohibition what we are doing is we're actually increasing the risk for the elderly to become infected, become seriously ill, and then die.
Dr. Michael Karlfeldt: You mentioned that the appropriate thing to do is to keep children in school so that the virus can pass around the part of the population that, evolutionary-wise, have a strong immune system; and they can handle this. They will then be able to pass this virus around without really getting sick, with the majority of them not having any symptoms. During that time it will then promote herd immunity; and that herd immunity will then protect the elderly later on. Am I hearing you right?
Dr. Knut Wittkowski: Yes, during that time the elderly should try not to get in contact with children. They should stay at home and reduce their exposure to the circulating virus as much as they can. That is something that makes a lot of sense, and that is something that people have been doing all the time.
If you know there's a virus spreading around then you don't take the subway, bus, or other things you stay at home and wait until the virus has spread and there's herd immunity. And then you can go back and their grandparents can play with their grandchildren and everybody is happy because the virus is gone. It has taken its course as nature has prescribed it and it's over and it doesn't need any further intervention.
Dr. Michael Karlfeldt: And so, if you do it that way then what would the need of vaccination be?
Dr. Knut Wittkowski: Wellthe vaccination speeds up the process because then you have already part of what otherwise would be needed to reach herd immunity; it's already there.
Dr. Michael Karlfeldt: And what I'm curious about though is that these viruses are known to mutate. They're known for how they affect one population; what they look like in Asia may be different than what they looked like in Germany, for instance, and probably here in the United States. So, if you develop a vaccine how are you able to be then specific to the strain that you're dealing with at the time?
Dr. Knut Wittkowski: Viruses don't mutatethat fast.So, avirus that enters the population stays more or less the same for the next couple of weeks or even months; therefore, the immunity protects. Is that the question you asked? Sorry if I didn't quite get what the question was.
Dr. Michael Karlfeldt: Yes, that's okay. I was thinking in regards to the vaccine because you need to obviously be fairly strain-specific; I would assume to trigger an immune response for the vaccine. So, if we're in the making of a vaccine, let's say they roll it out, like, six months from now or so —how are they going to be specific in regards to the virus we're dealing with right now to make sure that that vaccine is working?
Dr. Knut Wittkowski: The virus wouldn't mutate that fast, so there's always a cross-immunity, so even if the virus changes a bit a vaccine would still be effective. But the problem is, sometimes, vaccines are actually increasing the immune response in a way that is not foreseen, and we have had cases where vaccination actually made the disease worse.
So, it's very important that we first test the safety and the efficacy of a vaccine before we give it to the population, and that is going to cost time. Thus, I would not expect any vaccine to be available within 12 months. I think it will take more time.
Dr. Michael Karlfeldt: Okay, because it would need to go through the proper safety channel to make sure that what you're rolling out—
Dr. Knut Wittkowski: Definitely.
Dr. Michael Karlfeldt: Has a vaccine been tested in the past for the coronavirus?
Dr. Knut Wittkowski: To my knowledge, they tested the coronavirus in animals and that was one of the cases where they tested the vaccine that was one of the cases where the vaccines made it actually worse.
Dr. MichaelKarlfeldt: Okay, so it actuallywas detrimental. The onlytests we've done so far; it was detrimental at that time.
Dr. Knut Wittkowski: Yes. I mean we should keep in mind we are not really suffering from the virus being there. Most of the viruses don't cause any major symptoms by themselves. We are suffering from the reaction of the immune system killing all the cells that are infected, and that creates a lot of inflammation and all the problems that come with it.
Now, ifthe vaccine makes that immune response even more rigid, stronger, then it could be that the effects of the symptoms of the disease get worse and that is one of the fears that we have and why we have to be careful in the development of vaccines.
Dr. MichaelKarlfeldt: So, ifI amhearing you right, it's not reallythe virus that kills you. It's more of the impact of the immune system, the inflammatory response, or the immune cytokines storm that they sometimes refer to that really can impact you and have a negative effect it's not the virus itself.
Dr. Knut Wittkowski: Yes. And that can cause respiratory problems that can cause bacteria to settle down on the inflamed skin and then cause pneumonia, so there are all these consequences of what the immune system does it’s rarely the virus itself. If the cells have to fight some more viruses, they could shrug that off.
Dr. Michael Karlfeldt: So, we really don't need to be afraid of the virus in itself; we just need to make sure that the immune system behaves properly around the virus.
Dr. Knut Wittkowski: And that is what vaccines are for. So, the immune system is trained. The immune system knows already how the virus looks like, and so the immune system can react immediately if a virus enters the body. So, the number of cells that need to be killed is only minor, and there is no major immune problem.
Dr. Michael Karlfeldt: But then, as you mentioned, the key then, with the vaccine, is to make sure that you have it at an appropriate dose or strength so you don't overwhelm the immune system to have a hyper reaction.
Dr. Knut Wittkowski: Well I don't think, but I'm not a virologist, but I don't think it is well known why the SARS vaccine created this unexpected overreaction of the immune system. But things like this can happen, and this is why we need to test thoroughly before we can make something available to the public.
Dr. Michael Karlfeldt: Yes, wonderful. And going to the SARS, because the virus we're dealing with now is very similar to the SARS virus. I mean it's called, "COVID-SARS" and impact in the respiratory. We had that outbreak of SARS and then it disappeared so is that what you're thinking will happen again with the coronavirus?
Dr. Knut Wittkowski: Okay, we had the SARS virus in 2003, if I'm correct, we had the MERS virus in 2009, and now we have another SARS virus they're all coronaviruses; they all come and go. This is not traumatic; this is the normal thing that's happening during the flu season.
Dr. Michael Karlfeldt: Because there is so much, I mean, we're looking at the flu season, but we never see that this can be heightened. There are so many people dying; is it just because of the media, or is it that it was different in some way?
Dr. Knut Wittkowski: The only difference is that this flu may cause a bit more severe respiratory symptoms than other flu. So, flu is coming slightly different, but there is no fundamental difference and the politicians, as I said. Both the president and the New York Mayor originally had the correct approach. They would say, "this is the flu we never shut down the economy for the flu."
We don't shut down schools; it doesn't make any sense we just wait it out. And for some reasons that are unknown that changed; the economy was shut down. It was costing two trillion dollars, and one can only imagine how much good one could do with two trillion dollars, and it's not clear yet that it won't take more money than two trillion dollars. So, I think this was an overreaction in many ways and it was due to not having epidemiologists involved in the whole decision process, that's my view.
Dr. Michael Karlfeldt: So, I'm curious because one of the things is that in order to be able to react appropriately you need to have appropriate data to be able to have an appropriate action, and you feel that appropriate data was available with the action that we took.
Dr. KnutWittkowski:Thedatathatwasavailable did notaskfortheaction that was taken.
Dr. Michael Karlfeldt: And you feel also that in order to be able to get data you need to collect it in a very scientific fashion and in a consistent fashion. Do you feel that that has taken place?
Dr. Knut Wittkowski: Not to the extent that I would have wished. We had in different countries at different times, certainly with China, and situations were either the definition of the disease or the process of collecting data was changed in the midst of an epidemic. And that is the worst thing that could happen if you try to make sense of data. If you try to see what's changing over time in the epidemic you don't want to change the way the data is collected during the epidemic. And unfortunately, that happened.
Dr. Michael Karlfeldt: So, it means that actually by changing the way that you collect and report data you can actually then skew how the numbers look to make it look worse or better depending on what direction you would like to take.
Dr. Knut Wittkowski: Well, what you see is you suddenly have spikes in the data and you know that nature does not jump, as Darwin said a long time ago. So you know if there is a spike, the spike must be an artifact but you don't really know where the data comes from and then you have to wait for a couple of days until you can understand what actually happens, and these couple of days can be important and delay whatever decision you would want to make.
But there was actually enough knowledge available to tell you to which point you should wait and then what is the right window of opportunity to do an intervention if anything. And that opportunity was not used or taken advantage of.
Dr. Michael Karlfeldt: The opportunity to wait and Dr. Knut Wittkowski: To wait and to decide exactlywhat is the right point to do an intervention. So, once the number of people who are infected has reached the highest point you could actually start a short-term intervention and drive the epidemic down faster than it would normally go down.
That can make sense but if you start too early you will just protract the epidemic, make it last longer and longer and longer, and then if you stop you may even have a situation where the epidemic starts again simply because you haven't allowed the epidemic to create herd immunity.
Dr. Michael Karlfeldt: Obviously there are somewhat different interventions and different timings what happened in China than in Europe and here in The United States? Could you take us through the progress of the pandemic and how it impacted the different countries differently?
Dr. Knut Wittkowski: China and South Korea have the advantage that very little was known about the virus. So, they did not, as many other countries, start too early because they didn't have the information yet that one might want to start. So, they started only very late before the intervention had little of an impact, but at least it didn't do any damage. Otherwise, we have a very great example, and that is Sweden.
In Sweden, there was no social, as I call it, I would call it, "antisocial distancing" required or employed. And now we can compare the epidemic in Sweden to the epidemic in the neighboring countries Norway, Denmark, and Finland— all around Sweden. And we see that the course of the epidemic in Sweden was exactly the same as in the three neighboring countries. So,
the effect of what they call, "social distancing" the effect of prohibition was nil.
Dr. Michael Karlfeldt: Because in Sweden, all they did was suggest that the elderly, especially the immune-compromised with respiratory or heart conditions, to be cautious and to quarantine themselves. And then business went on as usual just with a little bit of awareness of the social distancing —correct?
Dr. Knut Wittkowski: The awareness of the social distance I don't think is very effective as we have seen in Sweden and the neighboring countries. And the thing that is effective is for those who are highly susceptible to make sure that they have as little contact with those who are infected or potentially infected as possible. So, to isolate themselves whatever you call it.
That makes sense and we would do that in each and every flu epidemic that is around. I mentioned that earlier: during a flu epidemic if you are scared of becoming infected you don't use the subway; you don't use buses; you don't go to places where a lot of people are around because that's where you can easily get infected so you stay away. But there is no reason whatsoever to stop businesses from doing business, and, in particular, to stop children from going to school.
Dr. Michael Karlfeldt: So, going back, you said that South Korea and China had an advantage meaning that they didn't implement social distancing until later on because they were kind of caught unaware.
Dr. Knut Wittkowski: They started implementation at the point where the number of cases had already reached the maximum or the peak. And that
means that the number of infections had a peak a week before and was already declining had already declined.
So, when they started the intervention, it didn't do that much and that was actually good. And that's why the epidemic in China and South Korea was over after about four weeks only while right now in Europe and in the US, it's taking a lot more time.
Dr. Michael Karlfeldt: And because we had the disadvantage of knowing ahead and with that, we initiated the social distancing before kind of in the course of action of this epidemic.
Dr. Knut Wittkowski: The advantage of having knowledge was not combined with the methodology to make use of it.
Dr. MichaelKarlfeldt: Okay, we did not dothe appropriate actionwiththe knowledge that we had?
Dr. Knut Wittkowski: Correct.
Dr. Michael Karlfeldt: Okay, and the appropriate action would have been that we would have looked at China and South Korea and seeing that it peaked on its own and then it was dropping even before social distancing so there was no reason to do social distancing here.
Dr. Knut Wittkowski: Yes. The problem with epidemics is: these are systems that are nonlinear, so, it's simple linear thinking. We do more of this and then it has more of an effect of that; it is not necessarily true, it really depends on what you do at what time in the epidemic and this basic knowledge of Epidemiology was not considered and taken advantage of.
Dr. MichaelKarlfeldt: I'mcurious. What are your thoughts why it went so badly in Italy?
Dr. Knut Wittkowski: Well Italy has, next to Japan, the oldest population in the world. So, there were many people who were old and had lots of co-morbidities. The average age of those who died was 81 years. The Italian government has created a very detailed report saying that of those who were young and had no co-morbidities virtually nobody died.
All deaths were among the elderly 75 years and older and those who had many co-morbidities. And so, you had that very fragile population there and it might even be that a slightly different virus strain came to Italy that was a bit more dangerous than other virus strains, although that is a hypothesis. The data could suggest that, but I wouldn't yet state this as knowledge.
Dr. Michael Karlfeldt: And I've heard also that the kind of urgent care system is not really as fully developed there, or they have kind of strong limitations, so if there's a flood of people that are needing help, they may not really be able to accommodate that.
Dr. Knut Wittkowski: I can't really comment on that. I don't have enough information to speculate about what that contribution might have been.
Dr. Michael Karlfeldt: No that's okay. So, with that, and going back to Wuhan, I mean if we would have seen a normal flu virus going through Wuhan, would that have behaved differently than this virus that we're seeing?
Dr. Knut Wittkowski: No.
Dr. Michael Karlfeldt: It wouldn't. So, we would have seen the same; it's just that this was hyped up?
Dr. Knut Wittkowski: Yes, it was just that for whatever reason this was treated as something dangerous and people were looking at it and investigating things that typically would not have been investigated.
Dr. Michael Karlfeldt: And do viruses spread this fast normally because it seemed like we had the first case back at the beginning of December then, all of a sudden, we had it in a hundred countries I mean, is that usually how things go?
Dr. Knut Wittkowski: Epidemics started exponentially. That is, initially, the growth is very, very, very little and then the curve increases and suddenly it becomes very steep but then it slows down again. And so, it is very typical that you, during the first month or two, don't really see anything and then you start seeing something.
Dr. Michael Karlfeldt: But then again, we were starting to see it in February here, I would assume that would have been the gap in December, January, then February. So, like two and a half months, is that the appropriate time for it to spread to so many countries?
Dr. Knut Wittkowski: Sorry to do what?
Dr. MichaelKarlfeldt: Is that the appropriate amount oftime for a virus to spread to so many countries so fast?
Dr. Knut Wittkowski: It took a month or even more to go from China to South Korea and then some time to go to Iran and then to Italy and then to other European countries.
So, there were several parallel paths. Thus, the more countries that have been affected, the more origins for a separate path to exist and the faster it goes
to the next. So, what we see is something that is very typical for a virus of this sort.
Dr. Michael Karlfeldt: So, the rate of how it is moving forward and also the impact on the population is, I've heard you say this many times before but I just want to reiterate, it is not very much different than any kind of flu season.
Dr. Knut Wittkowski: No not at all and I want to go back to the numbers in the United States. So, every year during flu season, we have around 35,000 death in The United States. So far, we have 10,000 deaths from this flu. Even if this should double, it should become 20,000 deaths; it would still be at the lower end of what is a typical flu season.
Dr. Michael Karlfeldt: I'm curious. Are they creating some kind of separation between normal flu deaths and coronavirus deaths or are theyall becoming coronavirus deaths now? Do we have statistics on both that they're running right now?
Dr. Knut Wittkowski: It is rare that we have two viruses entering a population at the same time. So, I wouldn't expect another virus to be circulating here right now. Would it be possible? It would be possible we don't know.
Dr. Michael Karlfeldt: So, the deaths that are currentlytaking place due to this flu season, are they all considered to be coronavirus related or they relate?
Dr. Knut Wittkowski: We don't know. We don't know because right now everybodywho dies with the virus or withsymptoms that are also seenwith
the virus;the coronavirus is consideredcaused bythe virus and that is simply not true, so, that is exaggerating the effects of that virus.
It maywell be that inItaly, for instance, some of the 90-year-olds who died; died for other reasons. They just happen to also have had been exposed to the virus but the virus didn't do anything or the immune system didn't do anything. So, they died of something entirely different and they are still considered cases of SARS or Covid.
Dr. Michael Karlfeldt: And then you have the question also that if an individual that maybe that, that individual wouldn't have lived that much longer anyway; that they were kind of on that cusp and then the flu or…
Dr. Knut Wittkowski: I mean people in their 90's: theytend to die at some point in time.
Dr. Michael Karlfeldt: That is correct
Dr. Knut Wittkowski: That is sad to know but on the other hand, this is just how life is. That is natural.
Dr. Michael Karlfeldt: I apologize for harping on this. So, the number of cases of flu or the number of flu deaths, right now, if you lump them all together with coronavirus and all the other things that would be considered influenza right now, it is not much different in any shape or formthat it has been the other years.
Dr. Knut Wittkowski: No, not at all.
Dr. Michael Karlfeldt: So, what is it? I mean they're calling this virus a "novel" coronavirus; what does that even mean?
Dr. Knut Wittkowski: It means that this particular coronavirus has never been seen before.
Dr. Michael Karlfeldt: It doesn't mean that it's more dangerous or doesn't mean that it kills more people; it just means that it hasn't been seen before?
Dr. Knut Wittkowski: Yes. And every influenza virus that's coming around is also one that's novel because it would at least have not been around for something like 15 years because otherwise, people would already have the herd immunity and the virus couldn't spread.
Dr. Michael Karlfeldt: So, the best thing right now, just to kind of summarize it is for children to go back to school; pass the virus around?
Dr. Knut Wittkowski: Definitely. Children should go back to school. This is the worst thing you can do, not only for the epidemic ofthe virus but also for the children.
Dr. MichaelKarlfeldt: And that willthenstrengthentheir immune system; they will develop immunity; they don't need vaccines if they are already immune, I would assume. And that would also then transfer immunity to their parents and we will then start to build herd immunity that will then protect the elderly from this virus.
Dr. Knut Wittkowski: Right.
Dr. MichaelKarlfeldt: Okay. So, with what we're doing right now, here in the United States, where do you feel we are at right now and where do you feel we're heading with the actions we're taking?
Dr. Knut Wittkowski: I think the action ofclosing schools is definitelythe worst that could have been done. The whole anti-social distancing or prohibition or whatever you call it is totally unnecessary and has cost at
leasttwotrilliondollarsand so sevenmillionpeoplebecomingunemployed and manyother social problems.
I think the cost of all that is immense and was totally unnecessary. I don't know why politicians resorted to doing something so drastic to deal with something the flu during the flu season.
Dr. Michael Karlfeldt: And I would assume that the impact of this economic depression that it looks like a recession that we're heading into. And that would have an impact on our health system as well with other diseases that are going to be more prominent that will outweigh…
Dr. Knut Wittkowski: Of course, it has because two trillion dollars were spent on damage control. Just imagine what you could have done with two trillion dollars spent intelligently on a tunnel between New York and New Jersey or other infrastructure projects or on health.
Improving health, improving hospitals,providing hospitals withmoreofthe stuffthattheyneed,and is now lacking.Ifthesetwotrilliondollars had been spent intelligently, the country would be in a much better position than it is right now where two trillion dollars have been spent increasing the deficit without any benefit.
Dr. Michael Karlfeldt: And another point there, another question I have and then we need to close. The mass testing, how important is that to prevent the outbreak and also to help us in the future?
Dr. Knut Wittkowski: Testing in this situation doesn't help a lot. As an epidemiologist, I would like to see eventually antibody tests to see how much herd immunitydo we have but that's aneasything to do and you don't even have to do this right now.
Dr. Michael Karlfeldt: Well thank you so much Dr. Wittkowski, I appreciate what you're doing and that you are a sane voice in all this craziness right now, so, I really appreciate that. Do you have any closing remarks that you'd like to say?
Dr. Knut Wittkowski: What I would like to say is read on a broader scale. Here is one of these examples where politics not listening to science is creating problems.
It would be better if politicians put the inside fighting aside and say well you are a scientist appointed bythis and you're scientist supported bythere. And politicians should interact with scientists, learn from them and I think that would make the world a better world.
Dr. Michael Karlfeldt: I agree instead of doing these knee-jerk reactions that have tremendous consequences it would be nicer to have.
Dr. Knut Wittkowski: One last point, I think we should also listen to nature. Nature has thought about all of this and when we are screwing up what nature has designed, it's not always beneficial.
Dr. Michael Karlfeldt: Thank you very much. That is it for today. You're listening to HealthMade radio. Remember to check us out at HealthMade.co. Health is what you make it.
Here is what you should know about Dr. Wittkowski: Dr. Wittkowski received his Ph.D. in Computer Science from the University of Stuttgart and his ScD (Habilitation) in Medical Biometry from the Eberhard-Karls-University Tuüingen, both Germany.
He worked for 15 years with Klaus Dietz, a leading epidemiologist who coined the term “reproduction number” on the epidemiology of HIV before
heading, for 20 years, the Department of Biostatistics, Epidemiology, and Research Design at The Rockefeller University, New York.
Dr. Wittkowski is currently the CEO of ASDERA LLC, a company discovering novel treatments for complex diseases from data of genomewide association studies.
Welcome to the third episode with Research Scientist Dr. James LyonWeiler-
In this episode of HealthMade Radio, Dr. Michael Karlfeldt is with Dr. James Lyons-Weiler, a research scientist and author to discuss the Covid19 virus; lack of accurate statistical data; the failed CDC tests that cause failure in disease tracking and allowed for the spread of COVID.
In addition, to address the problems with a fast-tracked vaccine that could potentially cause pathogenic priming making 100,000’s individuals more susceptible to a similar virus in the future. Dr. Lyons-Weiler offers a proposed plan for private COVID testing allowing individuals the freedom to know their own infection status to make better choices about health care, caring for others, and/or returning to the workforce.
Manipulated CDC Studies and Statistics
“I designed 100’s studies at the University of Pittsburg. If I had done to those studies, what the CDC did to their studies, I would have lost my job.” Dr. Lyons-Weiler says about his discovery of CDC data manipulation.
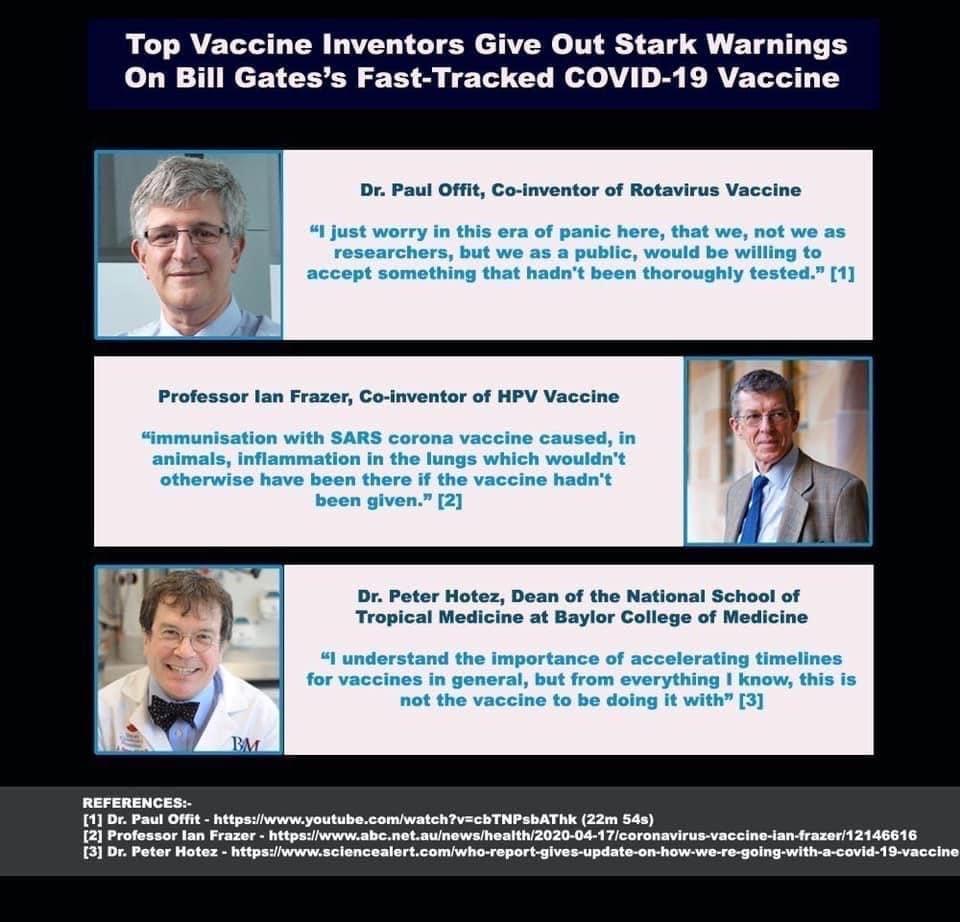
Is COVID-19 similar to the flu in mortality rate?
The struggle to answer that question will be in the CDC’s manipulation of the numbers. The data has been skewed from the beginning combining pneumonia with lab-tested influenza.
“Individuals comparing 'flu cases' to COVID-19 to flu don’t know the asymptomaticrate forinfluenza.It is verydifficult to estimateacase fatality rateduringanoutbreak – andit mayvaryfromcountrytocountrydepending on, obviously, the medical facilities’ ability to save lives during the critical phaseofadisease,whichforCOVID-19involves,Ibelieve,anautoimmune
attack leading to unresolvable pneumonia (symptomatic) but massive tissue damage to the lungs (lung immunopathology).”
Keep in mind that the World Health Organization’s numbers of influenza cases and deaths come from the CDC. “The fact that they represent 'flu-syndrome' cases are a failure of public health administration – a failure of EPIC… no, COSMIC proportions.
Bottomline: No one canestimate a solid deathratebetweenCOVID-19 and Influenza.” However, IPAC is tracking statistics specifically to have more accurate data.
World Health Organization Offered CDC An Accurate Test: CDC Refused
CDC is supposed to be the world leader in Infectious Disease Control. They refused to use an existing COVID-19 test and instead developed one that was flawed with false positives and false negatives. Allowing the further spread of the virus in a critical window of time.
“WHEN THE WORLD HEALTH ORGANIZATION offered the CDC a test – made by Germany – that had already been tested, one has to wonder who held the conversation within CDC leading to the disastrous conclusion that CDC should make ‘their own’ test.”
Whoever made those fateful decisions made them according to the status quo of the CDC – they prefer that which leads to massive amounts of positive revenue, regardless of the effect of that decision on safety. “
This allowed for the spread of the disease and made meaningful contract tracing difficult. CDC’s deadly mistake is directly responsible for the death and permanent lung damage to come across the US. It is also a major factor
in the economic downturn in which the stock market lost 20% of its value – a wallop that may be one of manyto come. ”
https://jameslyonsweiler.com/2020/03/
Governors Across the Country are Saying the Cure is a Vaccine. Could this be possible?
But given the current pressure to stave off the pandemic, a COVID-19 vaccine has been touted as the solution to the current crisis. The risk of the vaccine is "Pathogenic Priming". The vaccine has the potential to make people MORE susceptible to the virus in the future.
One way to get hundreds of thousands super sick from a coronavirus is to have sensitized the population with a vaccine containing a spike protein. Why? Because prior animal studies showed high mortality following rechallenge (virus exposure) in vaccinated animals.
Fuchi convinced the FDA to skip animal trials.
Even the most vocal vaccine proponents such as Paul Offit and Peter Hotez now say skipping the animal studies could result in unacceptable risks. And yet, here we are with numerous vaccines in development and human trials beginning.
https://news.yahoo.com/european-firms-step-covid-19-161057879.html
#IPAKBacktoWorkPlan Private, Non-CompulsoryIn-HomeAntibody Testing.
Many people believe that coronavirus testing will be an important tool for lifting restrictions.
https://www.cbsnews.com/news/coronavirus-second-wave-testingsurveillance-fda-stephen-hahn/
Dr. Lyons-Weiler proposes private testing for individuals to know their status of infection. The goal is the REDUCTION in the number of new transmissions. If individuals can test themselves with guidance, then they can participate in their self-governance.
The #IPAKBacktoWork Program defends your liberties and rights to #KnowYourStatus without ever having to report it – to anyone.
If you do nothing, mandatory testing and all the rest will surely come. For more details, check out the IPAK Back to Work Plan at the IPAK Website http://ipaknowledge.org
DR. LYONS-WEILER BACKGROUND
Dr. James Lyons-Weiler is the founder and CEO of the Institute for Pure and Applied Knowledge, also known as IPAK. He is the author on 57 peerreviewed publications, and has written and published three books, one on Ebola, another on Cures vs. Profits and a third on The Environmental and Genetic Causes of Autism. He, along with other scientists at IPAK, performs research in the public interest aimed at finding ways to reduce human suffering using funds donated from the public and that he raises at IPAK educational events. His latest research is focused around COVID-19 with proposed solutions to allow people to return to the workforce.
The Institute for Pure and Applied Knowledge is a not-forprofit organization that exists to perform scientific research in the public interest We use the principles and practices of scientific research to help individual researchers, research teams, consortia, and companies push their projects
through roadblocks, or map their way around them via evidence-based alternatives. We provide independent views and intellectual effort on scientific progress in three main areas:
Helping investigators in their efforts to reduce human pain & suffering through biomedical and related forms of scientific research.
Helping investigators increase their understanding of the universe using science as a way of knowing.
Educating the public in robust and reliable advances in medicine and science.
Our activities are varied, and include:
Conductingandpublishing independent andobjective nonpartisananalyses, studies, and research on legislative issues that impact public health and scientific progress in light of peer-reviewed and published scientific findings.
Providing support in many forms to endeavors that advance understanding via science (publications, consortia, conferences).
Providing support to progress in science in specific critical areas that are likelyto reduce humanpainand suffering – and we go the extra mile to help make those successes in translation happen.
Voicing informed opinions and issues on select government agency and court rulings, and actions and positions taken byother government agencies that influence healthcare practice and affect public health.
IPAK: Bringing knowledge & people together in the pursuit ofsuccesses in research via progressive science.
IPAK is a not-for-profit organization funded by private donations from the public.
Dr. Karlfeldt: I'mDr.MichaelKarlfeldt andI'llbe your host. Today'sguest is Dr. James Lyons-Weiler. Dr. James Lyons-Weiler is the founder and CEO of the Institute for Pure and Applied Knowledge. A not-for-profit research Institute, also known as IPAK. He's the author of three books, one on Ebola, another on Cures Versus Profit, and the third on the Environmental and Genetic Causes ofAutism, which is based onover 2000 peer-reviewed studies on autism.
He along with other scientists that IPAK performed research in the public interest aimed at finding ways to reduce human pain and suffering through knowledge. He lives in Weston, Pennsylvania with his fiancé Grace and his two sons. James, it’s such an honor to have you on the show. When I read a number of your articles and I loved them and I feel you're spot on all different areas. So, thank you so much for spending some time with me today.
Dr. Lyons-Weiler: Well, thank you. It's truly an honor to be on your show, you know with all the true health that you bring forward, actually addressing root causes and augmenting, health, cognitive neurological, the autonomic health— it's a pleasure to be speaking with you, so thank you.
Dr. Karlfeldt: Well, thank you so much. I'm curious what made you take the step to found the Institute for Pure and Applied Knowledge?
Dr. Lyons-Weiler: Right. So, life is a winding road on a journey. And while I was at the University of Pittsburgh as a faculty member in the Department of Pathology and the Department of Biomedical Informatics, I decided to step out of the tenure stream because I like helping people. I had
brought in in the first three years, two and a half years at the Cancer Institute under Ronald Herberman, $27.5 million dollars in collaborative funding to fight cancer. Mom died from breast cancer and people all around campus had found me a useful resource in their research studies.
At being an expert in molecular pathophysiology, genomics, proteomics, and bioinformatics. And I had established a bioinformatics core at the University of Pittsburgh. I had a staff of four people and an annual budget of $650,000. And we cranked through a hundred studies, and I think it was seven years that I ran that.
So, and then there was an administration change, the new chancellor of the university came in, he was the former director of the National Institutes of Standards and Technology. And he found my supercomputer. He found my shop basically in his kingdom and said that he wanted that for his people.
So, it was a sad day for me and my staff. Nevertheless, I was set loose and set free and decided, well, this is 2014 Ebola broke out. And so, I decided to look at that from a scientific perspective and track everything that was going on. And that's all covered in my book on Ebola.
But then I decided to write a book that celebrated all the great successes in biomedical research that can occur and have occurred despite the profit motive, the pressure for profit. And money is the bottom line, increasingly in allopathic medicine and biomedical practices as influencing research and the outcomes of the research.
So, having written that book called Cures Versus Profits, you know, there's a formula in there for how to be a good guy and a formula in there, how to be a bad guy. I probably shouldn't have published the latter.
Dr. Karlfeldt: Yeah got to look at both sides when you publish as a scientist.
Dr. Lyons-Weiler: It's a good example of what not to be. And then while writing that book, I came into an understanding of the sorry state of vaccine safety science because I was going to write a chapter on the successes of vaccines. I walked into the topic of vaccines expecting to find the kinds of studies that we would expect rigorous science to be founded upon. And they were nothing of the sort. I had to add an appendix to the book on four major controversies surrounding vaccines.
One of which was a whistleblower named William Thompson. That information came through Brian Hooker. I had found the transcripts and video of the phone calls of Dr. William Thompson and then when he was outlining for Brian Hooker how they routinely send their vaccine safety studies to a committee that sanitizes them for anything that might make vaccines look unsafe.
And that was horrifying, understanding that millions of people, millions of children, hundreds of millions of children are vaccinated every year. So, I just chronicled everything that I found, put it in the book, and that book,CuresVersusProfits, changed my life.
Thequestionremains for me, isthereanyplausible evidence inthescientific literature at the cellular molecular animal studies, tissue studies that might support the idea that vaccines might contribute to autism risk?
Hence, I decided to write a book starting from scratch on the genetics of autism. And by the end of the reading, 2000 studies, I concluded that the book should be titled,EnvironmentalandGeneticCausesofAutism. It is a
reference resource for what was known up until about I think 2015 or '16on everything that was known about autism. And why we think vaccines might not contribute to autism, but why in reality vaccines probably are a major contributor notonly to autism, but also to ADHD, and many, many autoimmune disorders. And naturally, that changed my life.
And so, Ithink it was 2015, in2015, right there inthe middle, I decided that if I'm going to accept reality and what I'm seeing and I'm going to be a research scientist, I have to create my own Institute. And so, I created the Institute for Pure and Applied Knowledge for a not-for-profit in western Pennsylvania, north of Pittsburgh. And we do science and the public interest without any profit motive. It's in the bylaws. I can't personally profit from any of the discoveries that we make. I can't patent any of my findings or any of the discoveries that I make.
It becomes public domain. So, the public donates and then we channel all of that hunger, desire for bonafide objective science into a bonafide and objective science. And we do peer-reviewed studies and it's been a blast. It's fantastic, the new development on the landscape of science and I'm very proud of it.
Dr. Karlfeldt: Yeah, I love what you're doing. I'm a big fan of that area. I'm curious, I had Del Bigtree on my show a while back ago, I'm curious what your thoughts are about the movie "Vaxxed" and how accurate it is and in regards to the science that you came about or that you were exposed to writing your book.
Dr. Lyons-Weiler: Yeah, so the book was written and in the publisher's hands. And I decided to interview BrianHookerrather than just go verbatim because there were some allegations that there was a conflict of interest in a research study where he re-analyzed the data from the CDC’s team.
The study in question in 2004 the study where they looked at kids around the Atlanta, Georgia urban area who had on-time versus delayed MMR vaccine.
And were there any increased risks of autism in those who had on time MMR? Under the theory that perhaps earlier developmental procedure processes hadn't yet occurred and that the vaccine somehow interrupted those developmental processes in the brain.
And what I found Brian saying and most of them, more importantly, what I found William Thompson saying that they excluded results from this study that Brian Hooker would naturally find when he re-analyzed the data.
And he realized the data by the same methodology as William Thompson. And he published it and the paper was retracted because Brian Hooker allegedly had a conflict of interest with one of the peer reviewers and that there were some complaints about the way he had statistically analyzed the data. For subgroups, the study had not included all of the results. When I looked at it, the study had excluded results.
The study authors did not tell the Institutes of Medicine that the African American boys who had received the vaccine on time had, I think it was a 4.3-fold increased risk of autism compared to those who had delayed vaccines. And the way that the study authors left that result out was to re-analyze the data many times until they could find a way to make the association go away.
They played around with age groups in defining the studydesign. They left out a bunch of kids from the study because they didn't have valid birth certificates. The vaccine doesn't check your birth certificate to see if it's a valid Georgia birth certificate if it's going to have an adverse event on you.
So, I don't understand that manipulation of the study design. And nevertheless, he found a way to make it go away. And the same thing happened with cases of isolated autism kids that had no other diagnosis other than autism.
They didn't have seizures, they didn't have other developmental disorders, no other, you know, what I call core risk factors, but no other potential confounding variables that they consider them. And so, that was enough for it to get my interest. for sure.
I didn't know about vaccine, then I called Brian, I emailed him and I said, "listen, I'd like to interview you because I'd like you in my book to be able to state whether you had a conflict of interest and what went on with the retraction of your study." And he graciously agreed to be interviewed and he said that he had dispensed with his association, with the organization that that other person was part of.
And he and I both agreed that since he analyzed the data the same way the CDC did then, therefore, the "Frank De Stefano et al." paper, the original paper, must also be similarly flawed and it too should be retracted. I sent in a statement of concern to Frank De Stefano, the journal editor of that paper. And of course, they didn't write back.
Nevertheless, I squared my conscience with an expression of my concern, I finished the chapter. But at the end of the interview, Brian said, "you know,
we're making a documentary about this. Did I say?" So that's when I knew it was going to be big. I knew it was going to affect my life. It wasn't going to be a book that was going to linger on the shelf somewhere. And that I had already accepted the task of remaining objective as a scientist and coming to this information.
Nevertheless, I made very fast friends with Del and Polly Tommey and everyone and we're all a big happy family. And we've been fighting shoulder to shoulder for truth and reality and objectivity in science and science-based public health policies ever since. You know, IPAK, is independent of Del's organization and Bobby Kennedy's organization.
We're kind of a third leg and, you know, I'm happy to continue working with these guys. But the most important thing that Brian Hooker was told by William Thompson wasn't about the Stefano study.
Ironically, from a scientific perspective, the most important thing that William Thompson said to Brian Hooker isn't even in the movie "Vaxxed". It is that, William Thompson said that they cook the books on all of their vaccine safety studies routinely by sending it to a sanitation committee.
When I saw that in the transcripts, and saw it or heard it on the video, that was on YouTube of the transcripts of the actual phone conversation, I should say. I immediately went to all the studies. I downloaded all the vaccine safety science studies that CDC had mounted to say that vaccines do not cause autism to see for myself in black and white on the page; the manipulations, because I could recognize it.
I designed studies for a living when I was at the University of Pittsburgh; that’s what I did for over a hundred studies I designed them and we analyzed the data. And if I had done to those studies at Pittsburgh, what
CDC had done, I would have lost my job and I should have lost my job. So, it was a life-changing event. My eyes were wide open. And then to watch the political shenanigans; to watch the deferments and; to watch the cover-up from a distance and see, you know I couldn't sit back.
So, Ihadto go intothe literatureand find out ifthere was anyother evidence that I could find in literature independent of anyone else and go and see if there were some plausible mechanisms. And I have a theory of autism. The paper that I wrote on it is "Autism is an Acquired Cellular Detoxification Deficiency Syndrome", which means that there's a genetic component where these kids just simply can't handle the same level of toxins as other kids.
None of the vaccine safety science none of it. Zero percent of the vaccine safety science considers that there might be a subgroup of genetic at-risk kids that are susceptible to developmental disorders from vaccines. They all assume a population-wide risk. It's terrible, absolutely horrible.
Dr. Karlfeldt: Dr. Weiler, so, I'm curious where right now we're in the midst of a crisis where we're dealing with the COVID-19, or coronavirus. I mean, what are your thoughts about this crisis? Do you feel all the measures are warranted? What, do you feel in regards to that?
Dr. Lyons-Weiler: Okay, so I want to take a look at that from the perspective of comparing coronavirus to influenza, which has been attempted several times. And the problem is trying to make a comparison of coronavirus to influenza. And concluding that coronavirus is just like influenza in terms of its scope.
There are several problems epidemiologically with that. The first is that we don't know the true extent to which coronavirus would have spread throughout the United States by now; the number of people that would have
died from coronavirus if we weren't in this; self-isolation/lockdown and shutdown of society.
And that's an obvious problem looking at raw numbers now, but before the lockdown if you look at the numbers before the lockdown, it's still difficult because, in an epidemic or pandemic of an infectious agent that does cause disease during the pandemic or epidemic, it's very difficult to even begin to model the population-wide rate while it's still spreading into a new population.
And so, while it's spreading, it's almost virtually impossible. You can look atthecurvesand youcanmake estimations, but wedon't knowat what point in time the virus is going to reach its carrying capacity. And it is extremely responsive to what people do in terms of: do we self-isolate? Do we socially distance? Do people stay home if they're sick?
And there are characteristics of the virus like: it's an asymptomatic period that isrealand itstransmissibilityis increasedover comparedtoSARS.And so, let's say that we could take the real-time numbers during the advancing stage of the epidemic before we reached the point of the curve. The comparison is flawed because there is a flu vaccine and there is no COVID vaccine.
So, wecan't say,welllook,this is just asbadasthe flu because ifthe vaccine does confer anyprotectionwhatsoever against influenza,thenwe're looking at a rate of spread and death rate in flu, in a vaccinated population. Some have vaccinated and coronavirus in an unvaccinated population. That's another problem.
And then finally, the biggest problem in that comparison I think is that the CDC has been cooking the books, as CDC so often does, on the actual
number of flu-related deaths. The common person at this point, if they've looked into it at all, has probably run to the statistic of anywhere between 38,000 to 66,000 is the typical number of deaths from flu every year.
But if you drill down into it and you go back into the books, and I've done this on an article on LinkedIn and everything I find I publish in articles. I do a deep dive into everything to make sure that we have a firm foundation in the reality of what we have to think of or say, but in 2014, yeah, there were 55,000 deaths reported, but they were reported separately for flu and influenza.
The laboratory-confirmed, flu, and then anything labeled in I'm sorry, influenza, I shouldn't say that flu and pneumonia, anything labeled flu from 2014 afterward was a combination. Okay. So, 2014 was the last time they separated flu and pneumonia. In 2015, they combined flu and pneumonia; they called it flu disease. Sometimes, you see CDC referring to it as PNI, pneumonia, and influenza.
Nevertheless, they are commonly referred to as the number of flu deaths. So, there are not 55,000 deaths from flu, excuse me, to begin with. There's only something like 5,000 deaths from flu every year. And the reason why they add flu and pneumonia to the flu, and these are noninfluenza pneumonia deaths, was because, then, influenza would not qualify as an epidemic in the United States if it did not explain more than 7.3% of deaths.
So, this kind of sham wizardry; this statistical sham wizard playing numbers with the games has put CDC in a bind because now, the coronavirus is here. coronavirus is taking its share of its deaths and IPAK is undertaking several studies in this. My institute is undertaking several studies to track the number of coronavirus lab-confirmed deaths,
flu laboratory-confirmed deaths and other respiratory virus laboratoryconfirmed deaths or no confirmed deaths, I should say, to make sure that we have a proper tally of what's going on so that when the CDC publishes their flu deaths month to month, that we have an independent assessment of that because my math tells me that coronavirus if you exclude pneumonia and you're only looking at flu, that coronavirus is 12.5 times more deadly than flu.
But flu is only causing, you know, 5,000 deaths per year. So, doing the math, right, it's like, okay, well yeah, it's definitely probably worse than the flu, but flu is a pussycat anyway. And you know, we've been lied to by the CDC on the statistics. It's going to be very interesting to see how they cook the books.
And I think the way that they're cooking the books is to call anything and everything that looks like coronavirus— so they have enough deaths so that they can retain their hide. Flu death rate, and they can try to retain their coronavirus death rate as well.
But I don't know howthey're going to do it because now, we're moving into a more thoroughlytested population as well. And so, I think this is going to be proved to be a big, big problem for the infectious diseases’ unit, the tracking units who have been cooking the books; they have a lot to answer on this question— on whether I think coronavirus is a problem. I'm sorry, go ahead.
Dr. Karlfeldt: Yeah, and I'm curious about that. I mean, going back, like you're saying, they're cooking the books. You're talking about pneumonia and influenza or the flu. How the flu isn't that big of a deal, but pneumonia truly is. So, it seems like you're saying that everyone that's dying from
anything that could be possibly related to corona all of a sudden becomes corona. So, how do you separate them, the true numbers, when these kinds of reporting are taking place?
Dr. Lyons-Weiler: Exactly. So, you have to start with about— of the past years, looking at past years, my estimate is 8.1% of flu and pneumonia and influenza deaths are actually due to flu and that gives me about 5,000. The rest is due to something else. And then, coronavirus deaths are being attributed to everything. And where it's a land it's a mess.
The United States internationally should have a very poor reputation in terms of infectious disease, and handling and managing public health because the other thing that's most disturbing about what CDC has done, January 16th, the Germans came out with an RT-PCR test that was already laboratory validated. That's very sensitive, very specific, meaning, very accurate. Uh, it also had high pathogen specificity, meaning that it didn't give positive reports due to other viruses and things like that.
And the World Health Organization put that out there as a good test. Offered it to countries, and 141 countries took it, and the United States turned their nose up at it so the CDC could develop their test. And in trying to develop their tests, they made some fatal errors that I say that literally; the CDC is deadly testing because they shipped out their test and their test was flawed.
And the CDC, this is the other huge black eye on CDC right now because CDC supposed to be the world's leader, not just the best in the United States, but the leader of the world in terms of infectious disease management and they've created a flawed test, shipped out a flawed test. People were testing positive who did not have coronavirus. People were testing negative who did.
Those people on the Princess cruise ship, who tested negative were going to be dropped off at a mall. The local city said, no, you can't drop them off at a mall. What if your test is inaccurate? We don't know how good your test is. So, they ended up going to a military base, but you know the types of decisions that have been made by the CDC in terms of testing.
Then now, the minute, two weeks later, they learned that it was flawed because local people, and local hospitals, and research institutions started making their tests because theycouldn't believe that the CDC test was right, given what they were seeing clinically with the patients. And so, the world came to know that the CDC’s test was flawed and the CDC was supposed to validate everybody else's test using their's as the gold standard.
And, you know, months went by, there's a whistleblower that came forward and said that the CDC leadership lied to President Trump by lying to Secretary Azar about the nature of the test and when it's going to be ready and whether it's going to be a persistent problem. And the FDA held off on giving emergency authorization to other people's tests for some time too long. So, this allowed coronavirus to spread throughout the United States.
This led to the shutdown of our society. This prevented real meaningful contact tracing. And the CDC owns this 100%. The CDC, in my view, should be shut down. It says it's bad, I've published this idea. It's a stupid idea for us to have our national bio-defense system located in one geographic location, having it all clustered in the CDC, where we know it's a corrupt culture is stupid.
Having it located in one geographical location where there's one culture that could lead to group-think anyway, it was really stupid. And I have proposed that we develop an 18 institute national bio-defense network. Where these
18 universities, private institutions, all work independently on the same problem.
We have 18 examples of teams working to solve the same problems, to detect bio-weapons, to be ready for bio-weapons, and focus on this readiness independent of each other so that the best ideas can come forward. They're not cross-contaminating each other's ideas.
And it's top-secret. It was what I would like to see funded by, the military. But the idea then, being that it's managed by someone who has no profit motive and the CDC is just chock full of conflicts of interest. You know, IPAK did deep-dive research for Bobby Kennedy.
He wanted to know which members of ACIP, the American Committee of Immunization Practices, have conflicts of interest with Pharma. And we looked at every member two years ago. We did this, I think 18 months ago. Every single member had direct conflicts of interest except for the military guy that was the representative of the US military.
This is unacceptable. What they do is they vote for each other's vaccines to approve each other's vaccines. That opens up a market for a new market, say for HPV or rotavirus or whatever. And then its quid pro-quality turnaround and then they okay the others. These companies have control of our regulatory agencies. They have captured the CDC; they've captured the FDA; they've captured EPA.
And we need to change. We need to. People call it, "draining the swamp." We need to end fascism. This is American style fascism where the corporations are running our government. And you know, I've come a long way on my learning curve, but man, I can't imagine a more, clear recipe for disaster
than for fake science on vaccines to be the norm. Science like activities; I don't even call it science.
There's just science like activities. They're going through the motions of a demonstration project, where they cook the books to make vaccines look safer than they are routine across the board. And then put the people into the decision-making capacity about which vaccines are recommended for the entire population.
They put a committee together and allow them to have conflicts of interest where they will profit personally— handsomely. If a vaccine comes to market, no one in its total group thinks, no one asks any tough questions about each other's vaccines.
They don't dare do it because next time around, you won't get the same kind of rub on your back. This needs to end. This is ridiculous. We don't have a viable bio-defense infrastructure in the United States at all. The CDC has sold its soul and American safety with it.
Dr. Karlfeldt:
And, um, with that, then we are making these financial decisions, that is, then paralyzing all of the United States-based upon this group-think and false information.
Dr. Lyons-Weiler: Absolutely.
Dr. Karlfeldt: So, we're talking about the testing then of the coronavirus. I mean, what kind of testing would you like to see take place?
Dr. Lyons-Weiler: That's a great question. Clinical testing for coronavirus is already in place. The FDA has approved emergency use authorization for a large number of different kinds of tests. There are RT-PCR tests which, you know, amplify copies of the messenger RNA, from the virus.
Andthen, thereareantibodytestswhichgive youtwo piecesofinformation. Do you have an active infection, or have you had a past infection? Do you have a mounted immune response? The RT-PCR tests don't tell you whether you have an active sorry, a past exposure, and an active immune response.
I think it's important to have both tools in our toolkit. But what I'd like to see instead of just clinical testing is I'd like to see private testing where individual citizens can go to the drug store without going to a physician and then pickup a test kit, bring it home, do a finger pick, blood prick, and put the blood on the assay and add some reagent to it.
And just like an EPT for pregnancy know their results privately in the privacy of their own home. They don't have to and under my model, which is called the "IPAK Back to Work" model this type of information is extremely valuable to some people who might need to know their status.
They might not want the government to know their status, but they might need to know their status. For instance, they might have at risk members of their family who are at higher risk of severe coronavirus, COVID-19 disease.
They might have people that are high risk of mortality that they could, if they have an active infection, obviously they probably should, you know, take care of that for a couple of weeks. This private testing, this model that I have, it's just more information for an individual to know. It's not for the doctors to know. It's not for the government to know and it's just like HIV testing. You can get yourself a private test for HIV no problem. You can make your personal decision on what you're going to do that day. That mass consumption, these antibody tests, not the RT-PCR test,
that's not going to ever be private. It's just not feasible, they have to send your sample away.
But the antibody tests can be done in 15 minutes and that could be private— and more information is always better. And so right now, the FDA has a restriction on private testing for a coronavirus. It doesn't make any sense whatsoever to me.
The United States lags behind every other country in the world on testing and it's just chaos raining and there's no plan going forward towards a sensible, rational way to open up society again.
And so, the "IPAK Back to Work" plan, which you can read about, and then #IPAKbacktowork, or you can see it on ipaknowledge.org, is a set of guidance that says, if you're positive for an active infection, wait this long and then retest, then go forward.
And if you're negative for an active infection, but you have evidence of what looks like immunity, do the following: —right. And if you do appear to have been exposed to the virus at all, you kind if need to know that.
And so, you should probably wait a period. And you know, the plan includes antivirals, which are both the natural therapeutics as well as allopathic therapeutics. So, the CDC and Anthony Fauci have fought against therapeutics.
And now I see in the science that's coming out on hydroxychloroquine, that they're doing the same cooking of the books that they did on vaccines to make it look like hydroxychloroquine might be harmful. Last I knew hydroxychloroquine doesn't check a person's co-variates to determine whether or not it's going to reduce viremia.
Right. And so, the epidemiological analysis is extremely manipulative. And John Unitas at Stanford University said it best, he said, "to you, if you get no more discovery studies, no more observational studies because if you give me an observational study, I can give you any result you want, depending on how I analyze the data." And he's exactly right.
So, in terms of testing, you know, imagine if I could snap my fingers right now and everyone knew their COVID-19 status, but the government didn't know wow, that would be a really big helpful thing to know. Right? It would be amazingly useful. And you know, people that were IGM positive, that means that they have an active infection, they might take their symptoms a little more seriously. They might seek medical care; they might go on a vitamin regimen. Interestingly, the small clinics are doing so much better. They have such a higher, a much better track record than the large medical centers in terms of more serious illness and death. And I've interviewed a large number of them on my show on "Breaking Science" .
The small clinics, they know what they're doing. This is not something that you can just wave away. It's not a trivial infection, but it is something that if you boost the immune system with the right strategies, you can seriously reduce the risk of serious and critical illness.
So, testing I think, is a tool and the fact that American citizens cannot know their status independently, I think that's not right. It should be a basic human right to know something about yourself, like your immune system status. Why not?
Dr. Karlfeldt: One issue also, I know that you have discussed quite a bit is, the issue obviously of the coronavirus vaccine that they are working on
creating. And then also, you talked about kind of the immune enhancement or pathogenic priming in regards to this vaccine and also exposure. Can you talk a little bit more about that?
Dr. Lyons-Weiler: Yeah, absolutely. So, past attempts at coronavirus, vaccines have not gone well. Specifically, I'm referencing the past outbreaks of SARS and MERS, the Middle Eastern Respiratory Syndrome. These are all related. So, SARS-Cov2 is a very closely related virus related to the SARS virus.
They're all beta coronaviruses. I looked at the past published studies and foundthat whenpast vaccineshad beenattempted,whethertheywerewhole virus vaccines or just use the spike protein, they tended to lead to increased incidents of severe and critical illness in animals. Those vaccines did if they were then exposed to the virus after being vaccinated and death as well. There was an increased risk of death in the animals after being vaccinated and then exposed to the virus compared to animals that had not been vaccinated and who were exposed to the virus.
Originally, it was called "disease enhancement", and I haven't determined who or where, but someone changed it to "immune enhancement". And immune enhancement is what you do immune enhancement is what you do when you go out into the sunshine and you get your 18,000 international units of vitamin D because you're out there for two hours.
The reality it's not immune enhancement at all it's disease enhancement. And then, looking at the studies and studying the proteins of SARS-Cov2, most of the proteins in the virus are capable of mounting an immune
response. That means that they have parts of the protein, which are what's called "immunogenic" . There, the protein can activate an immune response. But the problem is that every single protein that the virus has is capable of activating an immune response in humans, except one, I think, has a stretch that is very similar to human proteins. And I looked into it, I published this study on pathogenic priming in The Journal of Translational Auto-Immunity. It just came out last week.
And it's really clear that either if you take a virus and you make a vaccine, a coronavirus, and you’ve injected it into animals, they have increased risk of bad disease outcome, including death, once they're exposed to the virus. Now that there's a push to create vaccines for SARS-Cov2 for some unknown reason. Anthony Fauci at NAID and the company that he works with, Moderna, managed to convince the FDA that it was so important to get the vaccine that they could skip animal studies to check for what we now call "pathogenic priming" .

And this is a shortsighted. A decision that could have profoundly bad health impacts on our population. Let's say they're successful and they get a vaccine through regulatory approval. And then they unleashed the vaccine under the public. I'm not going to get into mandates and all that right now. But, just let's say that there's a vaccine and let's say a hundred million Americans take the vaccine. Then two years from now another coronavirus comes out of China, or Hong Kong, or anywhere that has coronaviruses similar to SARS and SARS-Cov2 and it infects 60% of the population cause there's no vaccine against that one. Then that means that 60% of a hundred million people are at risk of enhanced disease.
Anthony Fauci
This seems to me like a recipe for disaster an absolute recipe for disaster.
So, the pathogenic priming risk is not an immediate risk of a vaccine, but it isanattendant riskthat willlikelymanifest aftera year later,two years later, five years later. And there's some evidence to support that.
This is very likely what's happened with SARS-Cov2 in China. The reason why I've struggled since the outbreak in China first started, it was on my radar quite early, and I struggled to understand why the mortality in a Wuhan was so high, so very high from looking at the Chinese data.
And then the mortality outside of Wuhan was less. And I thought maybe the Chinese had conducted a large-scale phase two clinical trial on a SARS vaccine and maybe we're looking at pathogenic priming.
But then I also realized that these people may have been exposed many times to these kinds of coronaviruses and we just happened to have a nasty one now. And there's a huge percentage of people in that province that may have been exposed to SARS and SARS-Cov2-like viruses in the past.
So pathogenic priming, then it could happen either potentially from a vaccine or from an infection, which means back to your original question, is it worth a lockdown? I have a solution to get the country back on track and the solution involves three weeks of the lockdown of at least 60% of the population combined with natural or pharmacological, therapeutics that are antivirals for at least 60% of the population.
Not necessarily the same people. And it's better if it's if they overlap, but thought, you know, there's not 40% of the people that take neither lockdown nor antivirals. And if you do those two things and you do independent
privatetesting, so people make rationaldecisions about whento self-isolate, we can end this, I suspect we can end this in about three or four weeks.
We can go to the point where the number of cases that are occurring, the number of transmissions, and that's what we want to look at, the number of new transmissions, it goes down so low that the CDC can get back to the job of doing realistic contact tracing.
They're calling, like, yesterday or today for an army of contact tracers and that's not going to happen. You're simply going to spread the disease around by sending people out into the community doing contact tracing, and you're going to scare the heck out of everyone and you're going to get accusations of spreading of the disease by bringing CDC people into every neighborhood.
So why not let the American people be good independent Americans, test themselves, and make rational decisions with guidance. So, and then when it comes to the vaccine itself, who in the world would want to expose themselves to avaccine that could cause an increased risk ofsevere, serious, or critical illness? When you get exposed to the natural thing, we hear that many people have been exposed to this virus but they don't know it.
Okay, fine. So, there are some steps towards widespread immunity, we have every right to presume through natural infection, but the vaccines themselves are usually adjuvanted. If they're injected intramuscularly in this way, they can get away with using lower dose antigen.
So, in the paper that I wrote on the study that I conducted in The Journal of Translational Auto-Immunity, I published all of the unsafe epitopes and I put out a call to the vaccine manufacturers to please exclude these epitopes that match human proteins.
If they match human proteins they're likely to induce a problem through auto-immunity, which is how vaccines can cause autoimmunity issues— then shouldn't we exclude these unsafe epitopes and try for the safest possible vaccine that then might not be so susceptible to causing pathogen priming?
I did this with the Zika virus as well. IPAK sent a letter to Anthony Fauci when they were coming out with the Zika vaccine. That letter went to Anthony Fauci right after he had announced that he was going to have a vaccine within a month for Zika. And I included all the pathogenic epitopes, the dangerous epitopes, parts of the proteins that match human brain proteins.
And I said, you could induce auto-immune and encephalopathy if you've vaccinated mothers, well, expectant mothers. And he, like, three days later, announced that he needed eight more months before they could get to a Zika vaccine. He never wrote back to me and said, thank you. So, I don't have that.
Dr. Karlfeldt: You don’t have that?
Dr. Lyons-Weiler: Satisfaction and gratification.
Dr. Karlfeldt: Well, I appreciate what you did because there was a huge amount of harm that could have come out of that. And an interesting point, or I wouldn't say an interesting it's a very important point, in addition to being interesting, is that people always think that then the vaccines are going to save me and so that I develop immunity against this pathogen.
But what you're saying with pathogenic priming is that the vaccine enhances your reaction to a subsequent infection. Meaning that making that infection even more harmful than it would have been just by itself.
Dr. Lyons-Weiler: Yeah, absolutely that's what the studies showed for SARS vaccines. That's what the study shows for MERS vaccines. And these studies were done with rats, mice, and ferrets. So, the background knowledge going into SARS-Cov2 is that if you develop a vaccine, you should test it in animals.
And why they've have allowed them to skip over the animal testing, I have no idea. I don't think that these vaccines should proceed to phase two without appropriate and thorough animal testing.
And, you know,ideally, I'd like to see a reformofallvaccine safetyscience. Mybig idea onthe reformofallvaccine safetysciences thatthe government would fund independent investigators to study vaccines, without any direct connection with no contact with whoever invented the vaccine.
If we want vaccines, then we should try to make them as safe as possible. The palliation given to the public that they're safe in light of what the CDC has done to try to fool the public into making them think that they're safe is not holding water anymore. And vaccine risk awareness has spread like wildfire.
Now, through the efforts of Bobby Kennedy, Del Bigtree, many others Polly Tommey, where they brought forward the evidence, just part of the evidence that the institutes of medicine had in their hands you know, a directive from CDC not to find an association between vaccines and autism, from Walter Orenstein.
People understand that there's a lot of corruption going on. This is not just another day to say, "Oh, everything's corrupt." What are you going to do? No, look at what you've got. If you don't stand up and participate in your
governance, you're not able to think independently. You're not able to act independently.
You become subject to the whims and desires of other people who will manipulate you for their ends. And that's not what we as American citizens would like to think that we do, but we certainly are subjecting ourselves to a lot of manipulation.
Dr. Karlfeldt: Yeah. I couldn't agree more. Just another point on the vaccine, that the scary part is like you're saying, is that you can get the vaccine and be perfectly fine and then two years later down the road you're impacted. So, then it's hard to trace it back to the vaccine. Then you can just say, well, the vaccine was fine; it’s not the vaccine, it's something else.
Dr. Lyons-Weiler: Right, absolutely. And this is part of the reason why they would push for a mandate and the universal vaccination. If they can push for universal vaccination, then there's no control group. There's no one to say, "well, wait a minute. You know, this disease; this new novel coronavirus that just came out and says, '2024 is not impacting anyone any differently because they're all vaccinated.'" So, there's no way to know.
That's why we have translational research. You know, the clinical translational research, that I am an expert in, requires a systematic, almost algorithmic, you know, formulaic approach to checks and doublechecks on safety.
My jaw hit the floor when it was announced that they were going to skip animal testing. Now, we hear that they might do it in tandem, right? But I think that everyone concerned about this should call their federal
representatives and senators and say, "no phase two studies. Don't go to any larger studies." You have your small pilot studies or those variant studies where they're looking at the effect of ranges of doses on small numbers of people.
There's ethics are wrong within that as well from a study to pay people to take on this lifelong risk of increased risk of mortality from coronavirus infection in a world full of cold viruses and for $4,500, you're signing away your risk. But that seems unethical. But you know, everyone should contact their Congressman and Senator and say that there should be no phase two testing.
That the trials need to stop unless the animal studies are conducted and the animal studies need to be independently reviewed. The CDC is not the arbiter of all things real. I understand in New York, there's a study on hydroxychloroquine that was held up because it's allegedly supposed to go to CDC for checking. No, I don't think so. I think the CDC needs to sit this one out.
CDC scientists and all those, they just need to sit this out and let independent scientists do their job and bring the truth forward. And while you're talking to your Congressman and Senator, you probably should tell them that you also want a right to know your status privately if you want to.
That you think American citizens should be able to know their coronavirus status independent of any other person or entity on the earth just for the sake of knowing it. And it's not a clinical test. It doesn't lead to any change in your clinical care. It doesn't exclude clinical care, you know, clinical testing, critical testing.
The people that were IG positive, if they seek medical care, they will be retested. You know, women who use a pregnancy test, they can report to
their doctor that they're pregnant because of the pregnancy test. But guess what? They do their pregnancy test. There's a clinical version of the test.
So, it seems to me that the FDA has it completely wrong by regulating this such that I can't go to CVS or Rite Aid and buy my coronavirus test. We could get hundreds of millions of people tested quickly. The market pressure would cause production.
Thesetestsarecheapandeasyto make and it would beagreat thingtoknow and if they can set up a volunteer reporting, if you want to, if you'd care to share your results so that we can help out with terms of, your zip code, your age, and your gender maybe. And that's it. And that's all CDC gets when they get results reported anyway.
But it would have to be a hundred percent volunteer. Just a little note onthe package. If you want to share your results, here's the website to do it. Your results are anonymous, they're not going to be traced back. There won't be any knock on your door. And then we can, you know more information is always better. And the FDA needs to be changed and the way to do that is to go govern yourselves America. That's what we need to do.
Dr. Karlfeldt: Yeah. I appreciate that. And yeah, I mean we can go on forever but I appreciate you coming on the show cause this is such a time we need this information so that Americans can make appropriate decisions and also put pressure on the legislators to make sure that the appropriate actions are taken. So that we are not just being pushed around in fear, but we can feel that we have control of our destiny.
Dr. Lyons-Weiler: Yeah, absolutely. I've kind of a closing point that I would add is that, you know, you still have HIPAA rights. There's nothing
that has suspended your HIPAA rights over, you know, your medical care, your medical information. And so, you need to stand firm.
Don't assume that just because there's a pandemic and they've shut down society, that now you have to be good little boys and girls and you have excuse me. That you have to surrender any of your rights.
Now's the time that we have to stand firmest and defend our rights and it's very difficult to. I have been consistently 2 ½ to 3 weeks ahead on kind of the main thought stream on this. But the time is closing. The window of time is closing before mandatory testing comes.
And when mandatory testing comes, then optional private testing will be seen as redundant. And so, we need to invert that and we need to get, you know, people should have the ability to order a test online and get it mailed to their house and right now and take it if they want it.
Ifthey don't want it, theydon't have to do it. So please, pleading with every personthat hears this, to just write an email, go online, you know, find your representatives and get them activated to have private testing, you know, approved change the regulation. FDA has to change the regulation for coronavirus testing so it can be private.
Dr. Karlfeldt: Oh, thank you so much, Dr. James. I appreciate you taking the time. This is it for today. You're listening to HealthMade Radio. Remember, check us out at HealthMade.co, health is what you make it.
