Legal Notice & Disclaimer
This eBook and the information it contains is not, nor is it claimed to be, a program to treat or diagnose cancer or any other disease, and is not intended as a substitute for medical care. Neither the author nor the publisher is engaged in rendering professional advice or services to the individual reader. If you suffer from any disease, seek immediate medical attention, and always consult with your physician or other health care provider as appropriate before engaging in any new endeavor related to your health. The author and publisher specifically disclaim all responsibility for any liability, loss or risk, personal or otherwise, which is incurred as a consequence, directly or indirectly, of the use and application of any of the contents in this book. All matters pertaining to your personal health should be supervised by a healthcare professional.
Copyright(C) 2023 by William Pawluk, MD, MSc.. All rights reserved, including the right of reproduction in whole or in part in any form.

7 Introduction A Word About Me .................................................................................................................. 8 10 What Is Cancer? Healthy Cells Gone Rogue 11 The Most Common Types of Cancer 19 Genes and Cancer .......................................................................................................... 20 Other Causes of Cancer .............................................................................................22 34 Testing For Cancer Warning Signs For Cancer ........................................................................................ 34 The Importance of An Annual Comprehensive Physical Examination ..................................................................................................... 35 Conventional and Other Cancer Tests 39 43 Cancer and the Mind/Body Connection The Findings of Dr. Ryke Geerd Hamer 43 Emotional Characteristics Common to Cancer Patients 45 Are Your Emotions Making You Sick ................................................................ 46 Getting Help .............................................................................................................................47 Cancer Resistant Personality Traits................................................................. 48 Spontaneous Remissions 50 52 Conventional Cancer Treatments and Their Limitations Surgery 52 Chemotherapy .................................................................................................................... 54 Radiation Therapy ............................................................................................................ 55 Late Effects of Chemotherapy and Radiation Therapy ........................................................................................................................................ 58 59 Chapter References Table of Content
61 Pulse Electromagnetic Field (PEMF) Therapy and the Many Health Benefits It Provides Basic Cell Function and How Magnetic Fields Facilitate Them ...................................................................................................................... 61 PEMF Therapy’s Healing Benefits 62 The Top 10 Benefits of PEMF Therapy .............................................................. 63 Enhanced Healing, Repair, and Recovery Processes .................... 68 Other Health Benefits of PEMFs............................................................................. 69 76 How and Why PEMF Therapy Aids Cancer Prevention and Recovery How PEMF Therapy Enhances Existing Cancer Treatments ......................................................................................................... 76 Research Into PEMF Therapy As A Potential Cancer Treatment .............................................................................................................78 82 PEMF Therapy As An Aid To Conventional Cancer Care Cancer Bone/Metastases ......................................................................................... 84 Cancer, Brain Radiation Therapy 85 Cancer, Breast 88 Cancer, Chemotherapy Complications..................................................... 89 Cancer, Head, Neck, And Oropharyngeal ................................................... 91 Cancer, Liver 92 Cancer, Lung 92 Cancer, Pancreatic .......................................................................................................... 94 Cancer, Stage IV ................................................................................................................. 95 98 PEMF Therapy and Cancer: What The Research Shows A Sampling of In Vitro (Cell Line) Studies 98 Animal Studies 100 Human Studies .................................................................................................................... 102 105 Combining PEMFs With Other Complementary Cancer Treatment Methods Diet—The Vital Cornerstone of Your Health ........................................... 105 Complementary Therapies That Can be Used With PEMFs 108
Complementary Treatments That Can Be Enhanced By PEMF Therapies 109 116 Choosing PEMF Devices and Systems Whole-Body System Or Local PEMF System? .......................................... 117 Beware Of Scams And Outright Lies ............................................................... 119 Working With A Trained Professional Is The Best Way To Find The PEMF Device That’s Right For You ......................... 120 121 Appendix Summary ....................................................................................................................................121 Introduction 122 Breast cancer aspects and survival 123 Characteristics of cancer cells .......................................................................... 125 Normal versus cancer cell growth factors ............................................. 126 Breast cancer growth and development 127 Natural aromatase inhibitors 130 Limitations of conventional chemotherapy ........................................... 131 Survivorship ............................................................................................................................ 132 Complementary or alternative care (CAM) 133 Effective CAM therapies – research-based evaluations ............................................................................................................................. 134 Survival rates for cancer 136 Mind-Body Medicine .....................................................................................................136 Is there a “cancer personality”? ......................................................................... 137 Cancer treatment resistance ..............................................................................139 Cancer and bone metastases 140 Natural killer (NK) cells ................................................................................................. 143 Medications that lower NK levels in the body ......................................145 Psychological stress ......................................................................................................145 Narcotics lower natural killer cell levels 146 Sedatives, tranquilizers or SSRIs lower natural killer cell levels 146 PEMFs improve NK cells 146 Testing for Cancers ........................................................................................................ 147 Inflammation and cancer ...................................................................................... 149 Cytokines in Cancer-Related Inflammation 149
Interleukins ............................................................................................................................ 150 Inflammation and hypoxia ...................................................................................... 151 Hypoxia 153 Cancer Stem Cells (CSCs) 154 Cancer stem cells and hypoxia ........................................................................ 156 Mitochondria and Cancer ...................................................................................... 158 Mitophagy 161 Cell Death 162 Oxidative Stress ..................................................................................................................163 Metabolism ............................................................................................................................ 164 Microbiome and cancer 166 Obesity and cancer 168 Biological mechanisms linking overweight/obesity to cancer 170 Factors that contribute to the development of obesity and cancer ........................................................................................................ 174 Hyperbaric Oxygen Therapy (HBOT) and cancer 175 Combining HBOT and PEMF .................................................................................... 177 Spontaneous Remissions of Cancers .......................................................... 179 Dr. Dwight McKee holistic oncologist ............................................................183 Testing for Cancers 185 Combining cancer therapies.............................................................................. 186 How does cancer kill? ................................................................................................... 187 PEMF actions in the body .......................................................................................... 187 PEMF research in cancer 190 Effect of magnetic fields on implanted breast tumor growth and viability in mice 192 Human studies 196 General ..................................................................................................................................... 202 PEMFs and chemotherapy .................................................................................... 208 PEMFs and radiation therapy 211 PEMF therapy combined with radiation therapy for breast cancer – an in vivo study ...................................................................... 214 PEMFs and surgery 216 Recommended PEMF devices 216 References............................................................................................................................... 217 List of abbreviations ..................................................................................................... 223
Introduction
In this eBook, I provide you with the information you need to better understand cancer, including what cancer is and the various ways it can manifest, its primary and co-factor causes, how to most effectively screen for it, why early detection significantly increases the likelihood of successful treatment and long-term remission. I will also share with you the role that one’s beliefs and emotions can play in cancer, as well as the traits that long-term cancer survivors have in common which you can adopt for yourself to reduce your risk of developing cancer in the first place. I also explain the primary methods conventional oncologists employ to treat cancer, including their limitations and the side-effects that they can cause.
The main focus of this eBook, however, is on how and why the use of Pulsed Electromagnetic Field (PEMF) therapy can improve cancer care, with a particular emphasis on its role in modifying the cancer microenvironment in order to achieve better treatment outcomes. My goal is to educate both individuals with cancer and their healthcare providers about the potential benefits of this relatively unknown, yet impactful, treatment option.
PEMF therapy, which has been available for over 40 years, is a complex concept that is often misunderstood due to the influx of equipment and misleading claims in the market. This confusion is further compounded by a lack of understanding of the extensive research available on the subject.
The book underscores the importance of PEMF therapy in all stages of cancer care, from prevention to palliative care. It highlights how PEMF therapy can effectively address many physiological actions, the breakdown of which are common to all health conditions, including cancer.
In the pages that follow, you will learn what PEMF therapy is and the many health benefits is can provide when properly used. You will also discover how and why these benefits are important for both preventing and helping to reverse cancer. In addition, you will learn how PEMF therapy can improve the beneficial effects of conventional cancer treatments, as well as the scientific research that confirms PEMF therapy’s usefulness as a supportive cancer treatment. You will also learn about other complementary cancer treatments from the world of holistic and integrative medicine and how they can be combined with PEMF therapy to further improve treatment outcomes.
I will also provide you with the information you need to choose the most appropriate PEMF devices and systems for your specific healthcare needs. And for readers with a deeper interest in the scientific and technical aspects of PEMF therapy as a cancer treatment, I have included an Appendix supported by more than 120 scientific references.
7 Super Charge Your Health To Protect Yourself Against Cancer
A Word About Me
I began my medical career as a conventionally trained physician. In the 1980s, I was an academic family doctor, managing a multispecialty medical group of 30 other practitioners. We were the largest group of family physicians on the East Coast of the US at the time.
In 1985, within the same month, three of our group’s patients were admitted to the hospital for gastric bleeding from the stomach. One of them died, and the other two almost died, all because they had been regularly taking lots of ibuprofen, a nonsteroidal anti-inflammatory (NSAID) drug, to manage their pain.
I was devastated and asked myself how this could this happen to my patients. The answer became obvious after a good medical workup. The patients’ use of ibuprofen, aspirin, or both, had caused the gastric bleeding, along with kidney and liver damage. Why was I using these medications? Because that’s what all doctors did at the time. It was the main solution that we had for helping people with their chronic pain problems.
My colleagues accepted these side effects as a natural consequence of managing pain. I didn’t. I thought there had to be a different, better solution, and was determined to find it. I also realized that the solution I sought would probably have to come from outside the field of conventional medicine.
Stepping outside this “House of Medicine” was not a simple or easy decision for me. But I was committed to finding a better and safer method for treating pain. And so I began my journey in search of better alternatives. I stepped well outside of my comfort zone, which until that point remained firmly within the confines of traditionally accepted medicine. I looked into tools my peers and I would have previously looked down upon. I made a decision to study several non-conventional disciplines, including acupuncture, energy medicine, nutrition, hypnosis, homeopathy, and spiritual healing. I was also impressed by reports out of the Roswell Park Medical Center of spontaneous recoveries of cancer that were not a result of conventional medical therapies for cancer.
During this period of experimentation, a spider bit me on my leg, causing a huge welt to form. I placed a big magnet on the bite site. Within two hours, the welt was gone. Now I was really intrigued about what was happening with the magnets. Wanting to know more, I studied the available scientific literature on magnet therapy but found a great deal of it to be in foreign languages and inaccessible to me.
Then I met Dr. Jiri Jerabek from the Czech Republic, who had translated and summarized a large body of work done in Eastern Europe. He shared my goal of getting this important work published in English. He gave me a copy of his manuscript and we
8 Super Charge Your Health To Protect Yourself Against Cancer
agreed to edit it into an English-language book. The result was the publication of our book Magnetic Therapy in Eastern Europe: A Review of 30 Years of Research.
Most of the studies cited in that book were based on the use of PEMFs as opposed to static magnets. Around the time that it was published, nonmedical PEMF devices started becoming available in the US for the first time. Because of these studies, I had much more confidence in the huge range of benefits of PEMFs for helping all sorts of health conditions – a much greater variety of conditions than were possible with static magnets. So I decided to purchase some PEMF devices to further my research.
Since that time, I’ve purchased and evaluated a large number of different devices, spending hundreds of thousands of dollars. And I’ve used, treated, or supported the treatment of thousands of individuals—myself, family members, neighbors, patients and the curious, and even pets—using the PEMF systems my research and experimentation have shown me are most effective.
Keep in mind that I’m a practical, medically and holistically trained physician. My first priority is my patients and my interest is in treating the whole person. While I continue to explore all the theories and science around PEMF devices, the true test is whether or not they work. Based on my extensive exploration, I know that they do work. I have over 30,000 documents on the effects of magnetic fields in biology, and another 5,000 full-length articles of studies on different magnetic systems, that prove that fact. PEMF therapy is rooted in science, with thousands of university-level controlled studies with PEMFs having been conducted on a large variety of health conditions, including cancer. I wrote this eBook to inform you about that research as it applies to cancer, perhaps our most feared disease, so that you can discover the potential PEMF therapy has for supercharging your health and helping to keep cancer at bay.
9 Super Charge Your Health To Protect Yourself Against Cancer
What Is Cancer?
“You have cancer.”
For many Americans and other people these are the most frightening words in the English language. That’s because they believe that a diagnosis of cancer is akin to being handed a death sentence.
While this is certainly not always the case, the fact remains that the so-called “war on cancer” that began in 1971 when President Nixon first officially declared it continues to wage on with little evidence of victory being in sight, except for early stage cancers and the innovations that have been made in the arena of early detection.
Today, the incidence of cancer is greater than at any time in history. In fact, cancer is now the leading cause of death among all Americans age 85 or younger, and second only to heart disease overall. In 1971, cancer affected one in ten Americans. Today, despite annual expenditures of tens of billions of dollars in cancer research within the United States, cancer strikes an average of 2 million American each year and kills over 600,000. Research data shows that cancer will affect nearly 50 percent of all Americans at some point in their lives, striking more than one out of every three women and one of every two men. In addition, despite the enormous amounts of money that have been spent on cancer research in the US, as well as around the world, the overall long-term success rate for cancers that have metastasized (spread beyond localized tumors) has barely improved since the “war on cancer” began.
Compounding this tragedy is how survival rates for cancer patients are calculated. Patients who are still alive five years after their initial diagnosis of cancer are considered to be long-term cancer survivors by the National Cancer Institute (NCI) and other cancer organizations. No attention is paid to the quality of life of these patients, however, which is often poor, due not only to the ravages of cancer, but also the serious negative side effects that can be caused by conventional cancer treatments such as surgery, chemotherapy and radiation, as well as the various drugs cancer patients are prescribed to assist in their recovery. But even more troubling is the fact that many of these patients end up dying soon after the five-year benchmark as a direct result of cancer or side effects caused by its treatment, yet these deaths are ignored by the cancer establishment in terms of tabulating “successful outcomes.” This statistical sleight-of-hand is all too typical of the ways in which the cancer establishment promotes the “progress” it is making in the “war on cancer.”
Despite these grim facts, a diagnosis of cancer is not a death sentence if proper treatment is used and treatment begins in a timely fashion. But one of the biggest problems facing cancer patients is the “cookie-cutter” approach to treatment that is
10 Super Charge Your Health To Protect Yourself Against Cancer PART ONE - CANCER: AN OVERVIEW | CHAPTER 1
the hallmark of most oncologists in the United States and elsewhere. Therefore, in order to make the best possible choices about cancer should you or your loved ones be affected by it, it is absolutely vital that you arm yourself with the facts so that you can avoid the many pitfalls that otherwise lay in wait for cancer patients. To begin with, you need to understand exactly what a diagnosis of cancer means.
Healthy Cells Gone Rogue
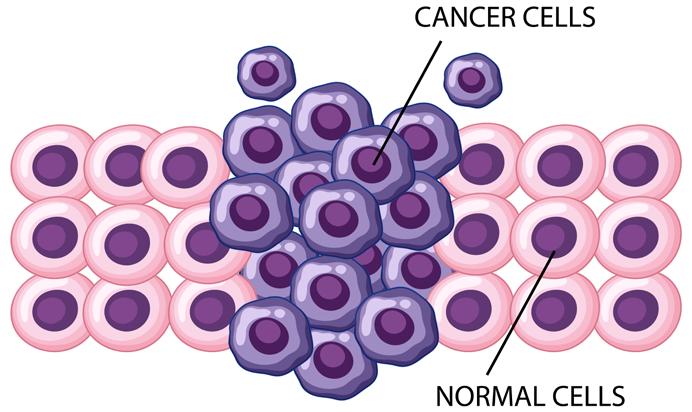
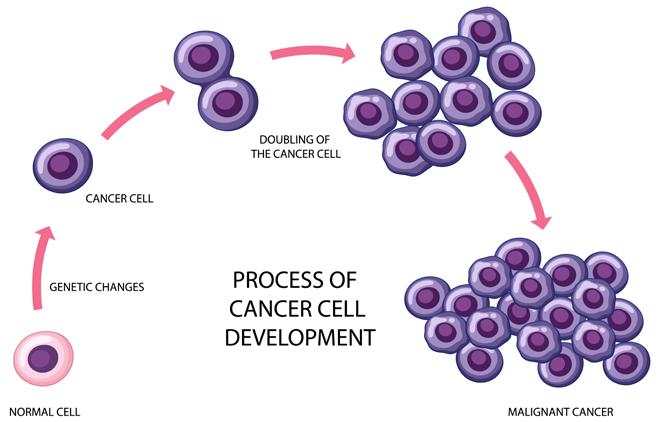
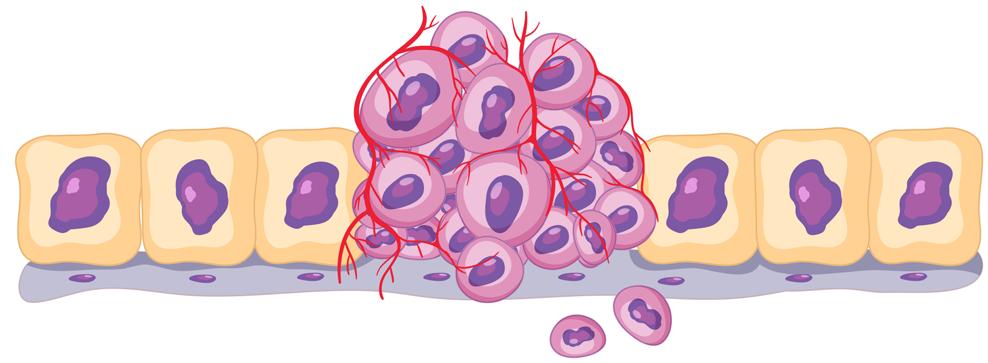
Cancer is a disease that is characterized by the unchecked spread of mutated cells in the body that occurs when normal, healthy cells stop maturing and functioning as nature intended. As these abnormal cells continue their uncontrolled proliferation, the various roles they were intended to play when healthy are interfered with, causing multiple disruptions in the body’s various biological processes. In addition, the mutated cancer cells, in order to further their growth, begin to divert necessary nutrients away from healthy cells, causing a weakening of overall health and impaired immune function. This diverting of nutrients away from healthy cells and tissues is accomplished by the formation of a network of blood vessels formed by the cancer cells. If this process is not reversed, eventually the cancer cells will start to clump together to form a tumor. The tumor will then continue to grow, fed by nutrients that are intended for healthy cells but are being diverted. Left untreated, cancer cells can eventually spread, migrating to other areas of the body.
11 Super Charge Your Health To Protect Yourself Against Cancer
This process is known as metastasis. As additional tumors form, they cause further damage to the body, including poisoning it with its buildup of toxic wastes. If this process is not reversed, death will eventually occur.
Ironically, the process described above occurs to some degree on a daily basis in the bodies of every person. This is because the initial aspects of cancer—the formation of abnormal cells—is part of a natural process that occurs as the body attempts to balance and regulate the literally millions, possibly billions of actions that occur within it every single second. When you are healthy, these abnormal cells are recognized and eliminated by the body before they can cause any harm. But when the body becomes overburdened, its ability to identify and eliminate abnormal cells becomes impaired, allowing for the growth and spread of abnormal cells to continue on unchecked. The development and continued spread of cancer cells is known as carcinogenesis, and the various elements that can trigger carcinogenesis are known as carcinogens.
12 Super Charge Your Health To Protect Yourself Against Cancer
One of the steps that leads to cancer is an unhealthy mutation in the DNA of normal, healthy cells. DNA is what provides each cell with its genetic purpose and function. When cellular DNA becomes damaged, cells no longer function properly. Moreover, since one of the functions programmed into each cell by DNA is to replicate, or reproduce itself, prior to the end of the cell’s natural life cycle, cells that have damaged DNA cause the cells that they replicate to possess damaged DNA as well. This, in turn, leads to further production of cancer cells, ultimately resulting in the formation of one or more cancerous tumors.
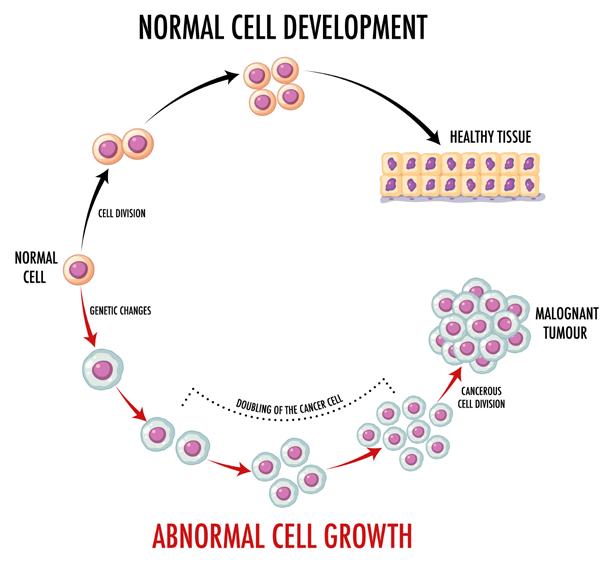
Adding to the problem of cancer is how cancer cells function, compared to normal, healthy cells. All of the healthy cells in your body have a natural life cycle that is programmed into them by their DNA. As a result, healthy cells, as they are created in the body, grow and differentiate, becoming specific cells with specific functions. For example, certain cells will differentiate and become kidney cells, while other cells will become heart cells, and so forth. Whatever form healthy cells differentiate into determines the role they will play in the body, with kidney cells helping to carry out kidney function, heart cells aiding in cardiovascular activity, and so on. When the human body forms in the womb, its trillions of cells differentiate into over 400 different types of cells. (Hatton IA, et al. The human cell count and size distribution. Proc Natl Acad Sci U S A. 2023 Sep 26;120(39):e2303077120.)
Each of these cells has a preprogrammed lifespan, as well. As these healthy cells mature, they will eventually replicate themselves and then die off, completing their life cycle. And then they are replaced by new healthy cells. The preprogrammed death of healthy, normal cells is known as apoptosis
Cancer cells, by contrast, do not follow the process of differentiation and apoptosis. Instead of fully differentiating, cancer cells usually bear little resemblance to the healthy cells they once were after the DNA of the healthy cells has become damaged. Instead of evolving into specialized cells, cancer cells can be said to be in a state of “devolution,” concerned only with their own survival, regardless of how achieving that goal negatively impacts the rest of the body. Finally, and most importantly, unlike normal cells, cancer cells tend to have a much longer lifespan, avoiding apoptosis as they tenaciously go about the business of survival by diverting vital nutrients from healthy cells, tissues, and organs. They become somewhat immortal. This is why the tumor microenvironment is so important, since it enables cancer cells to take over the metabolism of adjoining cells, which is a large part of the reason why and how the cancer tumor grows.
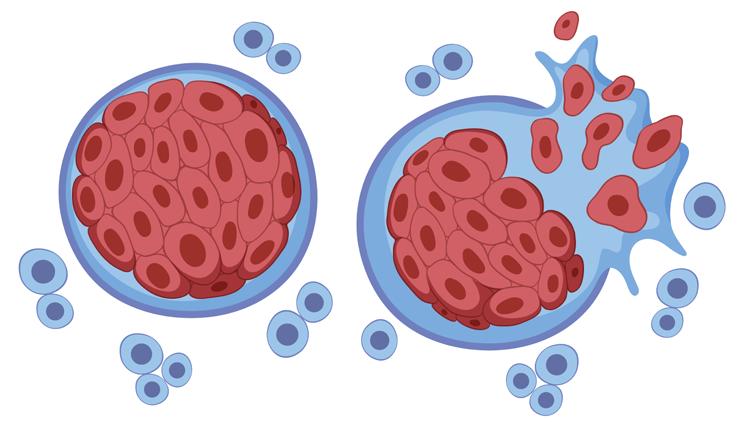
As a result of these factors, cancer cells are nearly immortal and act as parasites in the body, spreading wherever they are able through both the blood stream and the lymphatic system, and invading healthy tissues as they do so. This process, if unchecked, is what causes tumors to form, often leading to metastasis.
13 Super Charge Your Health To Protect Yourself Against Cancer
Once metastasis occurs, cancer poses a very serious health risk that can often be fatal if not properly treated. In addition to the creation of additional tumors in different areas of the body, metastasis results in the outpouring of toxins in the body, due to the significant increase in the amount of cancer cells, all of which eliminate waste products as they continue to grow. These toxins further sap the body of its energy supply, as well as interfering with the ability of the immune system to do its job. In addition, the spread of cancer cells and their toxins hampers what is known as the body’s biochemical defense system (BDS), which acts in parallel with the immune system. Unlike the immune system, which seeks to destroy and eliminate cancer cells, the biological defense system seeks to reprogram damaged cells so that they revert to healthy cells, thereby inhibiting cancer cell growth. Once the ability of the BDS to do its job becomes disrupted, cancer is able to spread more easily, putting a further burden on the immune system, eventually to the point where the immune system becomes overwhelmed.
14 Super Charge Your Health To Protect Yourself Against Cancer
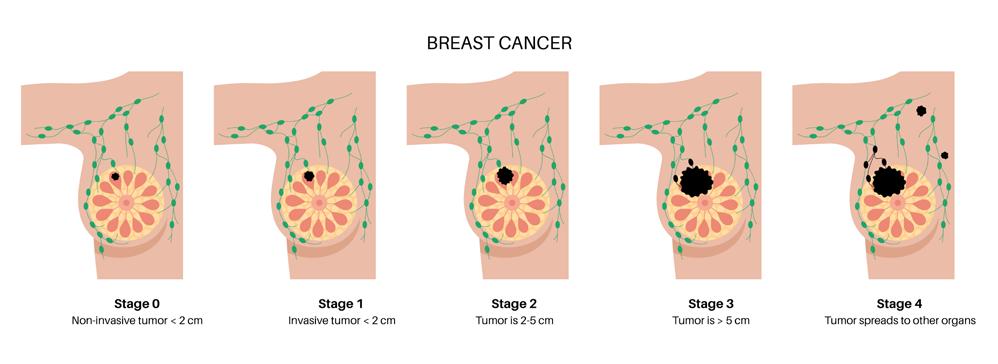
Oncologists and other physicians who treat cancer diagnose it according to four stages. Each stage is based on the amount of cancer that exists in the body at the time of diagnosis. The earliest stage of cancer (Stage 1) is also the stage in which cancer is most treatable.
Stage 1 cancers are cancers that comprise only a localized tumor, with no signs that the cancer has spread beyond the tumor itself.
Stage 2 cancers exhibit the spread of cancer beyond the tumor itself into surrounding healthy tissues and, in some cases, into the lymph nodes (part of the body’s lymphatic system, which helps to eliminate waste products and harmful microorganisms destroyed by the immune system).
Stage 3, cancer has metastasized beyond the tumor and spread into lymph nodes in other areas of the body, away from where the original tumor is situated. In Stage 4, metastasis has spread into other organs of the body.
Stage 4 cancers pose the greatest challenge in terms of their treatment, especially conventional “cookie-cutter” treatments, which have an extremely poor success rate with Stage 4 cancer.
As Stage 1 cancer progress into latter stages, the body’s internal milieu, or microenvironment, also changes, becoming increasingly unhealthy and anaerobic (oxygen deficient). This toxic microenvironment is what allows cancer to thrive and become resistant to treatment.
15 Super Charge Your Health To Protect Yourself Against Cancer
One of the primary reasons why pulsed electromagnetic field (PEMF) therapy offers significant benefit as a supportive treatment option for cancer is because of how it has been shown to help shift this microenvironment back to a healthier state. In addition, PEMF therapy also acts directly on cancer cells and tumors themselves by bolstering the ability of the body’s immune system to target and fight cancer. Moreover, PEMFs also help to reduce the toxins and damage caused by many of the therapies used in conventional cancer care today. How and why PEMF therapy is able to do all of this is explained in more detail in Part Two of this eBook.
Cancer is a complex disease. It can manifest in many different forms and has multiple causes. This explains why it can be so difficult to treat, especially in its later stages. Further compounding this problem is the fact that how well people respond to treatment can vary considerably from one patient to another, even when they have the same type of cancer at the same stage. This explains why there is no such thing as a single “ magic bullet” cure for cancer, and why there likely never will be. Recognizing that is important for anyone dealing with cancer, and their caregivers.
In the next chapter, I will explain about the different ways cancer can manifest, as well as the many factors that can cause cancer. Contrary to popular belief, cancer is far more than a disease caused by faulty genes.
16 Super Charge Your Health To Protect Yourself Against Cancer
The Many “Faces” and Multiple Causes of Cancer
The term “cancer” actually refers to a broad category of diseases that can take many forms. All told, there are over 100 different types of cancerous conditions. All of them are divided into one of five categories of classification.
The most common class of cancers are carcinomas. These are cancers that occur in epithelial cells, which are cells that line the surfaces of organs in the body and function as a protective barrier. Epithelial cells cover the surfaces of the skin, mouth and throat, the nose, the airways of the lungs, the breasts, thyroid gland, the gastrointestinal tract, and the genitourinary tract, as well as blood vessels and various other organs. Examples of carcinomas include breast, colorectal, lung, prostate, stomach, and skin cancers, such a melanoma.
Sarcomas are second category of cancers. These cancer can occur in the bones and in the body’s soft connective tissues that surround and connect blood vessels, cartilage, fat, joint linings, muscles and tendons. Sarcoma cancers are rare in adults, occurring in only about one percent of all adult cases of cancer, but more prevalent in childhood, where they account for approximately 15 percent of all cancers in children. Overall, soft tissue sarcomas occur more frequently in adults, while sarcomas of the bone more often strike children and teenagers, although they also occur more frequently in adults aged 65 and older, compared to younger adults. The most common bone cancer sarcoma is osteosarcoma. Other bone sarcomas include Ewing’s sarcoma, chondrosarcoma, and chordoma. Examples of soft tissue sarcomas include angiosarcoma, gastrointestinal stroma tumor (GIST), liposarcoma, and synovial sarcoma, among others.
17 Super Charge Your Health To Protect Yourself Against Cancer CHAPTER 2
A third class of cancers are lymphomas. These are cancers that occur in the lymph glands in the body’s lymphatic system. In most cases, lymphomas are caused by abnormalities in a class of white blood cells called lymphocytes. As these lymphocytes “go rogue” they can cause the onset and progression of tumors in the lymph glands. The most common types of lymphomas are Hodgkin’s disease and non-Hodgkin’s lymphoma. Outside of the US, especially in certain parts of Africa, a third type of lymphoma called Burkitt’s lymphoma is also common.
The above three categories of cancer are characterized by solid tumor formations. The remaining other two classes do not involve solid tumors. Rather, they are cancers in the blood.
The first of these classes of blood tumors is leukemia. Leukemia is caused by abnormalities in blood cells found in both the blood and in bone marrow, where most of the body’s blood supply is made. Leukemia occurs when developing blood cells begins to multiply uncontrollably. As they do so, they crowd out healthy developing red and white blood cells, as well as platelets inside the bone marrow. As they form, they can travel in the bloodstream to affect various body organs and tissues.
There are four main types of leukemia:
● Acute lymphocytic leukemia: which is the most common in children, teens and young adults up to age 39, although it can strike adults at any age;
● Acute myelogenous leukemia: the most common type of acute leukemia in adults, especially those 65 and older;
● Chronic lymphocytic leukemia: the most common chronic leukemia in adults;
● and Chronic myelogenous leukemia: which is also most common in older adults, and very rare in children.
The final category of cancer is a rare type of blood cancer called multiple myeloma
Myelomas are cancers of plasma cells, a type of white blood cells that aids immune function by producing antibodies to prevent and combat infections. When myeloma occurs, plasma cells also multiply uncontrollably within bone marrow, crowding out healthy blood cells. In addition, they switch from producing healthy antibodies to producing abnormal antibodies and unhealthy proteins.
Characteristics of Cancer Cells: Cancer cells differ from normal, healthy cells is a number of significant ways. A chief difference between cancer cells compared to normal cells is the fact that, while healthy cells have a normal life cycle, after which they die and are replaced by new healthy cells, cancer cells continue to grow and divide in an unchecked fashion. In addition, in order to grow, normal cells need to re-
18 Super Charge Your Health To Protect Yourself Against Cancer
ceive growth signals. By contrast, cancer cells continue growing in the absence of such growth signals. Cancer cells are also able to travel to various locations in the body to invade tissues and organs, whereas normal cells do not typically travel around the body. Moreover, when normal cells come into contact with other cells, they stop growing, whereas cancer cells do not.
Another important characteristic of cancer cells is their ability to evade detection by the body’s immune system. When normal cells are damaged or reach the end of their life cycle, the immune system detects and eliminates them.
Unlike normal cells, which function best is an oxygen-enriched microenvironment, cancer cells and tumors thrive in an oxygen-deficient (anaerobic) environment. They also are able to derive sustenance from different kinds of nutrients than those that normal cells feed upon.
Another major characteristic of cancer cells is their ability to create their own network of blood vessels via a process called angiogenesis. This cancer cell-created network diverts essential nutrients from normal cells, tissues, and organs, sapping the body of its energy via this nutrient loss. The end result is that, as the body weakens, its immune defenses are increasingly impaired, enabling cancer cells to continue growing and dividing.
In addition, as cancer cells continue to grow and spread, they emit waste byproducts that act as toxins on healthy cells, tissues, and organs, further weakening the body’s ability to fight cancer.
The Most Common Types of Cancer
As part of its overall mission, the US federal government’s National Cancer Institute (NCI) tracks the annual incidence of all types of cancer in the United States. According to the NCI, 14 types of cancer account for the vast amount of new cancer cases in the US each year. Leading this list is breast cancer (in both women and men), followed by prostate cancer, lung cancer, and colorectal cancer (cancers of the colon or rectum).
Rounding out this list in descending order of incidence are:
● Melanoma
● Bladder cancer
● Kidney cancer
● Non-Hodgkin’s lymphoma
● Endometrial cancer
● Pancreatic cancer
● Leukemia (all types)
● Thyroid cancer
● Liver and bile duct cancer.
(Source: www.cancer.gov/types/common-cancers and Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023 Jan;73(1):17-48.)
19 Super Charge Your Health To Protect Yourself Against Cancer
Genes and Cancer

In order to successfully prevent and treat cancer, it is vitally important to understand the various factors that can cause cancer.
As I mentioned in the previous chapter, cancer is far more than simply a disease caused by genes gone bad, even though a significant amount of funding in cancer research continues to go towards achieving a better understanding of the “gene theory” of cancer.
Still, there is no question that genes—both in terms of genetic defects and genetic predisposition—are involved in the onset and progression of cancer. The question is to what degree?
When the body’s cells turn cancerous, they lose the normal shape of healthy cells to become deformed, and also change in other ways, including abnormal alterations in their internal structures. Cancer research has established that these changes occur because of unhealthy mutations in cancer cells’ DNA. Research has also established that three classes of genes also determine whether or not a person will develop cancer. These gene classes are called proto-oncogenes, oncogenes, and tumor suppressor genes. Proto-oncogenes play an important role in normal cell division. But should they start to mutate, they can turn into oncogenes. Oncogenes trigger changes in healthy cells that cause then to transform into cancer cells, causing them to repeatedly divide in an unchecked process instead of dying out at the end of their life cycle as normal cells do via apoptosis.
The third class of genes involved in cancer are called tumor suppressor genes, which are responsible for producing proteins involved in the process of normal cell growth. Certain tumor suppressor genes help regulate normal cell division and trigger apoptosis as normal cells age or are damaged, while other of these genes help repair damaged cellular DNA. Damage to and mutations of tumor suppressor genes can cause them to be deactivated or malfunction, thus disrupting their ability to perform their functions.
Damage to and/or mutations in these classes of genes are significant causes of cancer, which is why many cancer researchers consider cancer to be a genetic disease.
20 Super Charge Your Health To Protect Yourself Against Cancer
According to the National Cancer Institute, “Genetic changes can lead to cancer if they alter the way your cells grow and spread. Most cancer-causing DNA changes occur in genes, which are sections of DNA that carry the instructions to make proteins or specialized RNA...For example, some DNA changes raise the levels of proteins that tell cells to keep growing. Other DNA changes lower the levels of proteins that tell cells when to stop growing. And some DNA changes stop proteins that tell cells to self-destruct when they are damaged.
For a healthy cell to turn cancerous, scientists think that more than one DNA change has to occur. People who have inherited a cancer-related genetic change need fewer additional changes to develop cancer. However, they may never develop these changes or get cancer.
As cancer cells divide, they acquire more DNA changes over time. Two cancer cells in the same tumor can have different DNA changes. In addition, every person with cancer has a unique combination of DNA changes in their cancer.
One genetic change, called a DNA mutation or genetic variant, is a change in the DNA code, like a typo in the sequence of DNA letters. Some variants affect just one DNA letter, called a nucleotide. A nucleotide may be missing, or it may be replaced by another nucleotide. These are called point mutations...Cancer-causing genetic changes can also occur when segments of DNA—sometimes very large ones—are rearranged, deleted, or copied. These are called chromosomal rearrangements. For example, most chronic myelogenous leukemias (a type of blood cancer) are caused by a chromosomal rearrangement that places part of the BCR gene next to the ABL gene. This rearrangement creates an abnormal protein, called BCR-ABL, that makes leukemia cells grow out of control.
Some cancer-causing DNA changes occur outside genes, in sections of DNA that act like ‘on’ or ‘off’ switches for nearby genes. For example, some brain cancer cells have multiple copies of ‘on’ switches next to genes that drive cell growth. Other DNA changes, known as epigenetic changes, can also cause cancer. Unlike genetic variants, epigenetic changes (sometimes called epimutations) may be reversible and they don’t affect the DNA code. Instead, epigenetic changes affect how DNA is packed into the nucleus. By changing how DNA is packaged, epigenetic changes can alter how much protein a gene makes. Some substances and chemicals in the environment that cause genetic changes can also cause epigenetic changes , such as tobacco smoke, heavy metals like cadmium, and viruses like Epstein-Barr virus.” (The Genetics of Cancer. National Cancer Institute. www.cancer.gov/about-cancer/causes-prevention/genetics)
However, ongoing research indicates that there is more to the development of cancer than defective genes alone.
Other Causes of Cancer
In recent years, in addition to ongoing research into the connection between genes and cancer, a growing number of researchers have come to theorize that cancer is more likely caused by various factors within three principle categories other than genetics. Based on their findings, they estimate that over 90 percent of all cases of cancer are primarily caused by poor diet and nutritional imbalances, unhealthy life-
21 Super Charge Your Health To Protect Yourself Against Cancer
style habits, and various environmental factors, not genetics. While this is sobering news, it also shows that we all have more control over what we can do to prevent, as well as help reverse cancer, than you may realize because the way we eat, our lifestyle choices are within our power to change for the better. Even many of the environmental factors that have been linked to cancer are things we can control in terms of our exposures to them, at least to some extent.
Diet: Both the National Cancer Institute (NCI) and the American Cancer Society (ACS), along with most integrative and holistic physicians, now recognize the role that a person’s diet plays in reducing or increasing the risk of developing cancer, depending on whether the diet is healthy or unhealthy. Yet most oncologists today still fail to educate their patients about the vital roles healthy diet and proper nutrition have when it comes to dealing with cancer.
Compounding this problem are the eating habits of the vast majority of Americans today. As a people, we are eating more than we ever did, yet are also suffering from the highest rates of malnutrition in our nation’s history. Simply put, the average meal consumed in America today is overly high in calories and dangerously low in essential nutrients.
Even more alarming is the fact that the segment of our population with the worst diets are typically people in their 30s or younger, setting the stage for an explosion in chronic diseases, including cancer, that once were very rare until late middle-to old-age.
In the first part of the 20th century, cancer was relatively rare, both in the United States and abroad. At the beginning of the last century approximately one of every 100 Americans developed cancer. Even in 1971, when President Nixon officially declared “war on cancer”, cancer struck only one out of every ten people in the U.S.
The spike in cancer rates only really started to become noticeable around the middle of the 20th century. Since then, the rate of increase has continued to rise at an increasingly alarming rate.
What happened by the mid-1900s to account for the rise in cancer rates?
One major occurrence was the shift in our nation’s food supply away from food production that primarily occurred at the local level to be overtaken by today’s near monopolistic commercial farming methods. Along with that shift came a much greater use of herbicides, pesticides, preservatives, food colorings and dyes, and various other substances that, despite subsequently being discovered to be potentially carcinogenic, are still widely used today in the production, harvesting, and packaging of most of the foods grown and consumed, not only in America, but in much of the rest of the industrialized world.
Today’s commercial farming methods rely heavily on a wide range of potentially harmful chemicals to ensure a profitable supply of food crops, along with poultry,
22 Super Charge Your Health To Protect Yourself Against Cancer
beef, etc. To this end, commercial farmers use an array of pesticides to grow their grains, fruits and vegetables, and now are also using genetically-modified (GM) seeds which have never been studied for their long-term safety. But that’s only the beginning. Once their crops are harvested many other unhealthy chemicals are added to them. In all, more than 3,000 chemicals are used each year to produce and preserve our nation’s food supply, while processed foods contain more than 10,000 chemical solvents, emulsifiers and preservatives.
It’s often said that “You are what you eat.” Based on the above facts, it’s clear that as a nation we are well on our way of becoming a nation of walking carcinogenic time bombs because of all the chemicals we daily ingest with the foods and beverages we consume. Poor diet and unhealthy eating habits lead to chronic nutritional imbalances (both deficiencies and excesses, such as too much iron, which has been linked to cancer and other diseases), and also increases susceptibility to pathogenic infections (bacterial, fungal, parasitic, and viral) that are known to increase cancer risk. In addition, such a diet and poor eating habits are the principal ways that the body’s internal environment, or microbiome, shifts into one in which cancer can thrive.
The good news is that, if you are willing to take responsibility for your dietary choices and commit to eating for optimal health, there is much you can do to significantly reduce your cancer risk. The key lies in knowing how to do so. In essence, this all comes down to knowing and following some important dietary “dos and don’ts. Let’s start with the some of the most important “don’ts”.

● 1. Avoid excess intake of animal protein.
While protein is essential for health and many people, due to their genetic makeup and metabolic profile, must regularly consume relatively high amounts animal pro-
23 Super Charge Your Health To Protect Yourself Against Cancer
tein to stay healthy, as a nation we consume far more animal foods than is necessary. This high intake of animal protein foods is associated with an increased risk of breast, colon, pancreatic, kidney, prostate, and endometrial cancer, as well as non-Hodgkin’s lymphoma.
In addition, excess animal protein consumption results in large amounts of nitrogenous wastes being produced in the intestine, some of which can be converted into highly carcinogenic compounds such as nitrosamines and ammonium salts. Heavy-protein diets can also cause metabolic acids to buildup in the body, forcing the body to call on its calcium reserves in the bones. As calcium is leached from bones it can cause not only osteoporosis, but also increase the risk of bone cancer.
The cancer risks associated with high animal protein consumption is also worsened by “factory farming” methods that result in animals being administered a plethora of toxic chemicals, including growth hormones and antibiotics, in order to accelerate growth rates and increase animal weight for higher yields. Other toxins are now also being included in animal feed lots. For example, food fed to the vast majority of factory-raised chickens in the U.S. contains arsenic, a known poison. Factory-raised animals are also fed foods that are not suited to them, such as corn and grains instead of grass, their natural preference. This further increases the unhealthy nature of the animal products derived from them.
How animal protein foods are prepared is another serious factor. Smoked, pickled and salt-cured animal foods, especially meats, also increase cancer rates, as do eating processed animal foods, which are high in a variety of potentially harmful substances. Animal protein foods that are cooked at high temperatures can produce a cancer-causing agent known as polycyclic aromatic hydrocarbon (PAH). which has been shown to increase the risk of breast, lung and gastrointestinal cancers.
● 2. Avoid farm-raised fish and fish higher up the food chain.
Because of how polluted our planet has become a variety of toxic chemicals and poisonous heavy metals such as oil, PCPs, hydrocyanic acid, mercury, and nickel have increasingly been deposited into our oceans and other waterways. In the oceans, these toxins are absorbed by ocean-borne plankton, where they then travel up the ocean food chain. As they do so, they become concentrated in the tissues of fish. Shellfish, tuna, swordfish, and other large fish are particularly high in such carcinogenic contaminants.
“Farm-raised” fish are also unsafe as they too are fed corn and other foods that nature did not intend them to eat, and are laced with antibiotics and food dyes to make them appear fresh in your grocery store.
24 Super Charge Your Health To Protect Yourself Against Cancer
● 3. Avoid consumption of unhealthy oils.
Unhealthy oils include most vegetable oils (organic, extra virgin olive oil is a notable exception), partially hydrogenated oils, margarine, commercial dressings, and trans-fatty acids, nearly all of which are high in omega-6 fatty acids. Before modern-day farming and food production methods took hold, human consumption of omega-6s was usually no more than two times as high as human consumption of omega-3 fatty acids. Today, however, the ratio of omega-6s to omega-3s in most people’s diets is a minimum of 6 to1 and often much greater than that, setting the stage for increased and chronic inflammation in the body, as well as an inner environment more conducive to the promotion of the growth of cancer cells and tumors.
● 4. Avoid excessive alcohol consumption.
Although moderate consumption of beer and wine has been touted for promoting good health, even these low-alcoholic contents drinks can increase cancer risk if consumed regularly. The risk is much higher with other alcoholic beverages. Alcohol can suppress your immune system’s natural killer (NK) cells. NK cells play an essential role in seeking out and eliminating cancer cells before they can spread, and are also very important for helping the body to fight off cancer when it takes hold. Regular alcohol intake is also associated with an increased risk of breast, mouth, throat, pancreatic, and liver cancer, as well as cancer of the head and neck.
● 5. Avoid “junk foods” (processed and preserved foods, and foods that contain artificial food additives).
Given the wide range of carcinogenic compounds these foods contain, it should go without saying that you should completely eliminate them from your diet.
What follow are some of the most important and easiest to implement “do’s” for healthy eating and cancer prevention.
1. Increase your vegetable intake.
Despite how powerfully effective this single dietary step can be, it remains one that many people have trouble abiding by. Don’t be one of them.
Vegetables are by far the richest source of nutrients than any other food group. In addition, vegetables are also nutrient-dense foods, meaning they contain an abundance of nutrients per mouthful. This is significant for many reasons. First, eating nutrient-dense foods typically results in less over-eating and caloric intake due to the rich supply of vitamins, minerals, and other nutrients they contain, all of which lead to feelings of satiety, unlike empty-nutrient foods. Second, because of the abundant supply of enzymes vegetables contain, the nutrients they supply to the body are able
25 Super Charge Your Health To Protect Yourself Against Cancer
to be digested and utilized far more quickly, sparing your body from having to expend energy to metabolize them. Third, vegetables are rich in antioxidants, nutrients that help protect cells, tissues, and organs from free-radical damage, as well as damage to cellular DNA that causes healthy, normal cells to turn cancerous. Vegetables are also the richest food source for fiber, which has a protective effect against certain types of cancer, including colon and rectal cancer.
Eating primarily vegetables at your meals will also greatly assist your body in ridding itself of harmful toxins, which also play a big role in the initiation of the cancer process. In addition, vegetables, due to the wealth of nutrients they contain, directly assist your body’s immune system in its anticancer defenses. This includes increasing the activity of your body’s natural killer (NK) cells. NK cells are one of your immune system’s prime tools for detecting and eliminating cancer cells and fighting tumors.
Another important health benefit that vegetables provide is reduction of inflammation inside of your body. Chronic, low-grade inflammation is a leading cause of most chronic degenerative diseases, including cancer. In addition, a diet high in vegetables will help to maintain your body’s acid-alkaline balance. In order to thrive, cancer cells need an acidic environment in which to develop and grown. Vegetables help to prevent such acidity by providing your body with buffering alkalis so that acid-alkaline balance is maintained.
To ensure you eat enough vegetables each day, I recommend eating raw or lightly steamed vegetables with every meal. Other cooking methods destroy vegetables’ enzyme content and greatly diminish their overall nutrient supply. Try to eat a “rainbow” medley of at least nine servings of vegetables each day. Consuming an assortment of different colored vegetables helps to ensure that you are receiving a wide variety of nutrients, since different vitamins and minerals are to be found in vegetables based on their color or pigment.
I also recommend choosing organic vegetables whenever possible. Not only are organically grown foods free of harmful pesticides, fertilizers, and chemicals, but they also have a higher density of nutrients.
2. Go “Low-Carb”.
To avoid and help reverse cancer, restricting your intake of carbohydrate foods can often enhance health. This means limiting your intake of breads, pastas, and especially “simple carbohydrates,” such as bagels, muffins, bleached flour, white rice, most cereals, and so forth. Although you require a certain amount of carbohydrates each day to help your body meet its energy needs, too much carbohydrate food intake can prove to be unhealthy for a number of reasons.
First, carbohydrates contain glucose and other sugars. Such sugars act as fuel for cancer cells. Therefore, the more carbohydrate foods you eat, the better able can-
26 Super Charge Your Health To Protect Yourself Against Cancer
cers are to “feed” and grow.
Many carbohydrate foods also tend rank high on the glycemic index, a scale used to determine how likely a food is to cause a spike in insulin levels. High- glycemic foods cause the most severe insulin spikes, leading to a greater likelihood of inflammation developing inside your body, as well as a lack of energy. Insulin spikes have also been shown to promote tumor growth. Low-glycemic foods, by contrast, do not result in either of these unhealthy effects.
In place of high-glycemic carbohydrate foods such as breads, pasta, etc, substitute whole grains, such as brown rice, quinoa, and bulgur, as well as legumes such as lentils, chickpeas, green beans, and peas.
3. Eat more berries.
Over the last few decades, berries have emerged as a class of “super food” due to the many health benefits they provide, including their anticancer benefits. Various foods in the berry family, especially organic blackberries, blueberries, raspberries, and strawberries, have been shown to be just as effective as new antiangioneic cancer drugs, without any of the drugs side effects.
As I explained above, angiogenesis describes the process cancer cells and tumors use to literally grow their own network of blood vessels from which they derive sustenance in the form of glucose and other sugars. Shutting down this network of blood vessels, or preventing them from forming in the first place, is essential to prevent and reverse cancer.
Research shows that various compounds in berries, such as ellagic acid, provide antiangiogenic benefits. In fact, ellagic acid from berries has been shown to inhibit two of the primary mechanisms that stimulate the growth of blood vessels. This points out another advantage that berries have over antiangiogenic drugs. Unlike the drugs, which typically only have one mechanism of action, ellagic acid and other anticancer compounds found in berries have multiple mechanisms of action. In addition, they have also been shown to increase cellular detoxification, compared to many cancer drugs, which can be highly toxic and immunosuppressive.
As with other foods, choose organic berries whenever possible.
4. Drink green tea.
In place of coffee, try to drink at least 2-3 cups of organic green tea each day. Research has shown that green tea is a powerful anticancer beverage because it is rich in a class of nutrients known as catechins. The catechins green tea contain help prevent the invasion of healthy tissues by cancer cells and other foreign cells, such as from bacteria or viruses. Catechins also have potent antiagiongenic properties.
27 Super Charge Your Health To Protect Yourself Against Cancer
Green tea also acts as a detoxifying agent in the body, especially with regard to its ability to activate mechanisms in the liver that eliminate cancerous toxins.
5. Include healthy fats in your meals.
Healthy fats assist the body’s production of energy, help reduce inflammation, and are essential for the manufacture and stability of cell membranes. They also help to transport oxygen throughout the body, and help maintain the health of nerves, mucous membranes, and the skin. Healthy fat food sources include avocado, organic butter, coconut, pastured eggs, fatty fish, and various nuts and seeds, including almonds, walnuts, and pumpkin and sunflower seeds. Coconut oil, flaxseed oil, ghee, and extra virgin olive oil are also rich in healthy fats.
Other healthy eating steps include eating wild caught fish and free-range meats and poultry food that are free of hormones and antibiotics, varying your meals in order to maximize you intake of the wide variety of nutrients foods contain, and eating fermented foods such as kimchi, sauerkraut, and miso, all of which contain hundreds of different strains of “friendly” bacteria that are essential for maintaining and improving the healthy functioning of the GI tract, thereby also aiding immune function.
Lifestyle Choices: In addition to poor diet and unhealthy eating habits, other common lifestyle factors that increase the risk of cancer are smoking and/or regular exposure to secondhand smoke, excessive alcohol consumption, a sedentary lifestyle of little to no regular exercise, unhealthy sleeping habits (going to bed too late, choosing to go without adequate sleep, etc.), unhealthy sexual habits and promiscuity, and the use of illegal drugs. In many cases, being unhealthily overweight or obese is also a lifestyle choice brought about by overeating and other poor eating habits and choosing to avoid regular exercise and other physical activities. It’s well-established that being overweight/obese significantly increases the risk of cancer, as well as heart disease, stroke, diabetes, and other chronic, degenerative diseases.
All of these unhealthy lifestyle choices and habits can be overcome and transformed into healthier choices by making a commitment to stop or change them.
Environmental Factors: In 2010, the President’s Cancer Panel, a bipartisan committee responsible for monitoring the development and execution of the activities of the federal government’s National Cancer Program, issued a report based on findings compiled during the course of a two-year investigation. The Panel’s findings revealed that environmental toxins from a variety of sources play a significant, yet still largely unrecognized, role in the development of cancer, causing “grievous harm” to a large segment of the American population each year.
The Panel’s report was a grim confirmation of what a growing number of cancer researchers have been warning about for years. It also further substantiated studies that found that children in America today are meaning born “pre-polluted” due to
28 Super Charge Your Health To Protect Yourself Against Cancer
environmental toxins that are passed on to them from their mothers’ bodies while they are still in the womb. One such study, commissioned by the Environmental Working Group, found the presence of over 200 environmental toxins in the umbilical cord blood of newborns, including industrial chemicals, pesticides, and other contaminants, all of which have been shown to be carcinogenic (cancer-causing) in previous studies. (232 Toxic Chemicals in 10 Minority Babies. Environmental Working Group, 2009. www.ewg.org/research/pollution-minority-newborns)
According to the Panel, the primary means of exposure to environmental toxins for the majority of Americans are:
● Contaminants from industrial and manufacturing sources
● Contaminants from agricultural sources (antibiotics, food additives, food colorings and dyes, pesticides, preservatives, etc)
● Contaminants related to our modern lifestyle (cell phones, computers, etc)
● Hazards from medical sources (x-rays, CT scans, nuclear medical tests, various pharmaceutical drugs, etc)
● Hazards from natural sources (toxins in our nations, air, land, and water supply).
Prefacing the main body of their report, the Panel wrote to then President Obama, “With nearly 80,000 chemicals on the market in the United States, many of which…are un- or understudied and largely unregulated, exposure to potential environmental carcinogens is widespread…All levels of government, from federal to local, must work to protect every American from needless disease through rigorous regulation of environmental pollutants…The Panel urges you most strongly to use the power of your office to remove the carcinogens and other toxins from our food, water, and air that needlessly increase health care costs, cripple our Nation’s productivity, and devastate American lives.” (2008-2009 Annual Report. President’s Cancer Panel. Reducing Environmental Cancer Risk. Available at: https://deainfo.nci.nih.gov/advisory/pcp/ annualReports/pcp08-09rpt/PCP_Report_08-09_508.pdf)
Laudable as these recommendations are, to this day neither the White House nor Congress has shown much willingness to tackle the serious problems that the Panel identified. Therefore, it is up to each of us to do what we can to minimize our exposure to environmental toxins in order to reduce our risk of developing cancer and other serious diseases. Fortunately, there is much that we can do on our own, staring with the following recommendations.
29 Super Charge Your Health To Protect Yourself Against Cancer
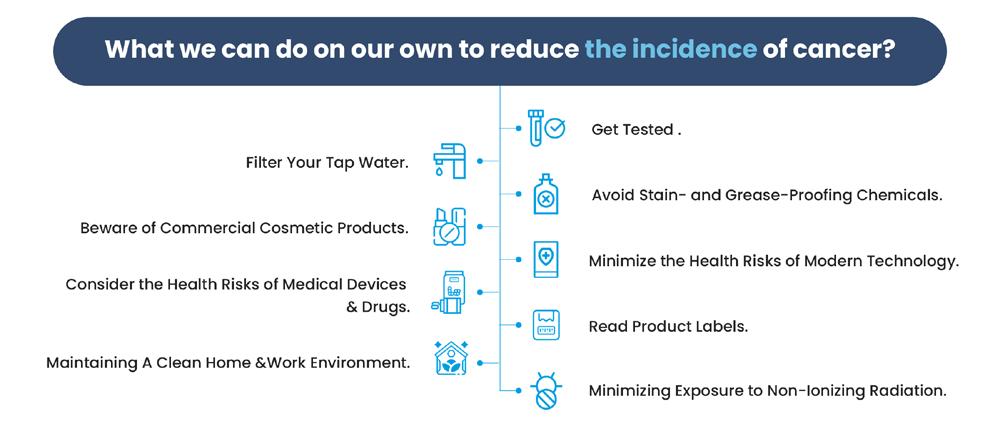
1. Get Tested.
Although the body has its own elegant system of detoxification, if it is continually exposed to toxins eventually it is overwhelmed. When this happens, toxins become stored in the body, especially in fat cells and tissues, and start to wreck havoc on the body’s immune and defense systems.
Despite this fact, many doctors still do not screen their patients for toxins as part of a regular checkup. For this reason, you may want to consider working with an MD who specializes in the prevention and treatment of environmental toxicity. Such doctors can screen you for the presence of toxins in your body and create a program of detoxification most suited to your needs. You can find a list of doctors who specialize in what is known as environmental medicine by contacting the American Academy of Environmental Medicine (AAEM) at www.aaemonline.org.
2. Filter Your Tap Water.
Most sources of tap water in the US contain common carcinogens such as arsenic, chromium, chlorine, fluoride, and various metals and other compounds, as well as chemical byproducts that form when water is disinfected. To avoid this problem, in the last decade or more, more and more people have chosen to drink bottled water. However, research has shown that most types of bottled water are no healthier than tap water, and in some cases are actually unhealthier. Moreover, the plastic used to manufacture drinking water bottles often contain toxins that leech into the water during storage, including bisphenol A (BPA), which has been linked to various types of cancer, as well as other diseases. Additionally, the proliferation of plastic water bottles has led to a serious environmental problem due to the fact that many bottles are never properly recycled. Instead, they wind up in landfills, and even in our water supplies, where the chemicals they contain leech into the soil and water to further pollute the earth.
30 Super Charge Your Health To Protect Yourself Against Cancer
A much better solution than drinking bottled water is to invest in a home water filter system. (To find out how your town or city’s tap water ranks in terms of cleanliness, visit http://www.ewg.org/tap-water/home.)
3. Avoid Stain- and Grease-Proofing Chemicals.
Such chemicals, known as fluorochemicals, are commonly used as optional stain repellants on carpets and couches, and as greaseproof coatings for packaged and fast foods. You can avoid them by simply not choosing stain treatments for carpets and furniture, and by not eating packaged foods. (Also consider replacing commercial home cleansing products with safer, more natural brands.)
4. Beware of Commercial Cosmetic Products.
Such products often contain chemicals that act as potential carcinogens, and which are easily absorbed into the skin and then into the body’s tissues.
5. Minimize the Health Risks of Modern Technology.
This includes minimizing cell phone use (when you use a cell phone, wear an earpiece, use the speaker option, or text), and sitting at least 18 inches away from computer monitors and TVs. Although such devices do not contain environmental toxins, per se, they do increase your exposure to EMF frequencies, which are known to cause cancer during over-exposure.
6. Consider the Health Risks of Medical Devices and Drugs.
Although there is no question that breakthroughs in medical imaging devices, as well as the development of a wide array of new pharmaceutical drugs, have contributed to improvements in our nation’s health care system, ironically, they have also led to increased health risks, as well. As the Panel’s report statesd “It is becoming increasingly clear that some of these same technologies and drugs that have contributed so greatly to health status and longevity also carry risks.” The report further pointed out that Americans today “receive nearly half of their total radiation exposure from medical imaging and other medical sources, compared with only 15 percent in the early 1980s…Computed tomography (CT) [scans] and nuclear medicine tests alone now contribute 36 percent of the total radiation exposure” that Americans receive each year. In addition, the list of potential side effects, include those that interfere with the body’s immune functions, continues to grow when it comes to today’s pharmaceutical drugs. Therefore, it is important that you discuss the “risk to benefit” ratio of such procedures and drugs with your doctor.
7. Read Product Labels.
A growing number of products sold in the US today list warnings of cancer risks. Be sure to read product labels and warnings of all products before you buy them.
31 Super Charge Your Health To Protect Yourself Against Cancer
8. Maintaining A Clean Home and Work Environment.
Maintaining a clean and healthy environment, both at home and at work, is also important. They key to doing so is eliminating sources of indoor pollution. Such sources include chemicals found in synthetic products, including home flooring, wall, and ceiling materials, and also synthetic rugs, carpets, and bedding, clothing, and furniture made from synthetic products. Common household cleaning products, as well as synthetic air fresheners, paint, glue, solvents, and varnishes also contain a variety of chemicals known to cause cancer. To improve the air quality of your home, you should also be sure to change dirty filters in your air and furnace systems. Also beware of harmful chemicals outside your house and workplace, such as those found in pesticides and other garden and lawn care products.
9. Minimizing Exposure to Non-Ionizing Radiation.
Exposure to non-ionizing radiation comes in the form of harmful electromagnetic fields, or EMFs, which are produced by electrical currents. Power lines near or into your home are a major source of EMF radiation, as are poorly insulated electrical wiring. Other common sources of EMF radiation include computers, dimmer switches, TV sets, electric blankets, and smart meters. Cell phones are another all too common source of EMF radiation. Becoming aware of such sources of EMF radiation in your home and doing all that you can to minimize exposures to them can make a big difference in the quality of your health.
In addition to these steps, by adopting a healthier diet and overall lifestyle, you will also assist your body’s detoxification systems to do their job more effectively.
While the above recommendations alone are not enough to clean up the toxins that pollute our planet, by following them, you can significantly reduce your risk of exposure.
In addition to the above categories of cancer risk factors, chronic stress, unresolved trauma (both physical and psychological), unresolved or repressed emotions, and unexpected life shocks, such as the death of a loved one, divorce, or job loss, can also increase the risk for cancer. These factors are discussed in more detail in Chapter 4.
All of the above factors also cause and perpetuate chronic inflammation and related factors, such as free radical damage, excessive and chronic production of reactive oxygen species ROS, cellular redox, and insulin resistance, all of which must be addressed in order to prevent and reverse cancer. As you will learn later in Part Two of this eBook, regular (ideally, daily) treatments with PEMF therapy can substantially reduce inflammation and its related factors, which is one of the reasons why it is effective for both helping to prevent and reverse cancer.
32 Super Charge Your Health To Protect Yourself Against Cancer
Testing For Cancer
Regularly getting screened for cancer is one of the most important steps each of us can take in the fight against cancer. Cancer screening tests can oftentimes enable physicians to detect cancer in its earliest stages, which greatly increases the likelihood of a complete and lasting recovery should cancer be found. Should tumors be found, early screening also means that they can be removed as early as possible. With every passing day that adequate removal of the primary tumor is delayed, more and more metastatic cells are able to spread further in the body. This is true of cancer surgery for most cancer, but especially true in cases of breast cancer. From that point forward, whole body PEMF therapy becomes critical for everybody found to have tumors, especially with high intensity PEMFs, to make sure the various depths of the body are all saturated with PEMFs to be able to keep dormant stem cells quiet.
Warning Signs For Cancer
In addition to regular checkups with the cancer screening test discussed later in this chapter, knowing the early warning signs for cancer is also important, and can potentially save your life. The most common early warning signs include:
● Unexplained, persistent fatigue.
● Unexplained weight loss.
● The appearance of a lump or thickening in the breasts or testicles.
● Changes in warts or moles, including growth and bleeding, and/or the appearance of dry, scaly, inflamed, or ulcerated patches of skin that does not heal. All of these can be signs of melanoma (skin cancer).
● Skin or throat sores that don’t heal, as well as persistent lumps or in the throat, and/or difficulty swallowing. Persistent mouth sores can also be an early warning sign.
● Changes in bladder or bowel habits, such as urinary pain or difficulty urinating, constipation, diarrhea, gas pains, rectal bleeding, or blood in the urine or stool.
● Persistent cough or hoarseness, or coughing up blood.
● Persistent digestive problems, including indigestion, heartburn, nausea, bloating, flatulence, and/or loss of appetite.
● Unusual bleeding or discharge from the vagina.
33 Super Charge Your Health To Protect Yourself Against Cancer CHAPTER 3
● Unexplained pain or weakness in muscles or bones.
● Persistent pains in the sides of the abdomen or lower back, or lumps or swelling in these areas, which can be signs of kidney cancer, as can a persistent and unexplained increase in blood pressure levels.
● Frequent infections, night sweats, swollen lymph nodes, unexplained fever and other flu-like symptoms, all of which can indicate leukemia.
If you experience any of the above symptoms, speak with your doctor and as to receive cancer screening tests.
The Importance of An Annual Comprehensive Physical Examination
I recommend that all adults, regardless of their age, schedule a comprehensive physical examination once a year. Such examination will provide you and your physician with a good picture of your current health status and alert you to any health issues, including cancer, that you might be developing.
A thorough physical checkup includes blood tests, urinalysis, and stool tests. Based on your doctor’s determination, it may also include X-rays, PET, CT and/or MRI scans, depending on any symptoms you present with. (You should always keep your doctor informed of any symptoms you experience, especially if they are sudden or persistent.) During the course of your exam, your doctor will take your blood pressure, and assess you resting heart rate and blood oxygen levels using a pulse oxygen monitor.
Typically, the blood and urinalysis tests you will receive include the following:
● CBC blood test: The CBC (complete blood count) test measures the amount of red and white blood cells, plus platelets in your blood.
● BUN blood test: BUN stands for “blood urea nitrogen”. This test helps physicians assess kidney function. Elevated BUN levels are an indicator of possible kidney damage or disease.
● Creatinine blood test: Creatinine is a waste product produced by your muscles and excreted by your kidneys. The creatinine test is usually ordered in conjunction with the BUN test to compare the ratio level of each substance.
● Glucose blood test: This test is used to determine your fasting blood sugar (glucose) level. For accurate results, you will need to fast for at least eight hours before the test is administered, and also refrain from drinking anything that contains sugar, including fruit juices.
34 Super Charge Your Health To Protect Yourself Against Cancer
● Hemoglobin A1C (A1C): The hemoglobin A1C test measures the average amount of glucose in the bloodstream over an 8 to 12 week time period. It is a more accurate marker for diabetes (both type I and type II) and prediabetes than a the blood glucose test and can be administered without the need for fasting.
● Lipid Panel: This test measures your HDL, LDL, total cholesterol, and triglyceride levels, all of which are markers for both cardiovascular health and disease.
● 25-hydroxy-vitamin D, or 1,25-dihydroxy vitamin D: These tests are used to determine vitamin D levels in your bloodstream.
● Liver blood tests (ALT/AST/ALP/GGT): These test assess liver function.
● Prothrombin Test: Also known as a PT/INR, this blood test is used to determine how well your body’s blood clotting factors are working. Usually, it is administered in conjunction with another test known as the partial thromboplastin time test (PTT) to provide a more complete picture of what happens when a person forms blood clots.
In addition to analyzing the body’s blood clotting performance and detecting bleeding or clotting disorders, these tests can be helpful in screening for liver problems, vitamin K deficiencies, immune diseases, certain types of cancer, such as leukemia.
Fibrinogen: Fibrinogen is a pivotal element of the coagulation system, which plays a major role in regulating blood clotting, inflammation, and neoplasia. Increased activity was associated with cancer cell growth and progression. Hyperfibrinogenemia is related to cancers, such as colorectal, gastric, and non‐small cell lung cancer (NSCLC). High levels can be caused by many factors and indicate an increased risk of clots forming. Low fibrinogen levels indicate a risk of bleeding.
Uric Acid Test: This blood test used to determine uric acid levels. Elevated uric acid levels can be an indication of gout, risk of kidney stones and other types of kidney disease, and cancer.
Comprehensive Metabolic Panel (CMP): This test is very useful for assessing the your body’s overall health metabolism, and chemical balance, and overall kidney and liver function. It can also be used to screen for various conditions.
Comprehensive Vitamin and Mineral Panel Tests: These tests measure vitamin and mineral levels in the bloodstream to determine both vitamin and mineral deficiencies and excesses. Both of these tests can be measured with urine as well as blood.
35 Super Charge Your Health To Protect Yourself Against Cancer
Thyroid Panel: The thyroid panel test measures three thyroid hormones—T3, T4, and TSH—to assess thyroid function and to screen for symptoms of hyperthyroidism, hypothyroidism, and Hashimoto’s disease, a thyroid-related autoimmune disease.
Homocysteine: Elevated blood levels of homocysteine (a non-protein-derived amino acid in the blood )are indications of systemic inflammation in the body, a primary cause of the mircoenvironment that cancer cells and tumors thrive within, and can also indicate an increased risk of coronary heart disease, atherosclerosis, blood clots, heart attack, and stroke. It is also useful for diagnosing malnutrition, folate and vitamin B12 deficiencies, and genetic defects in intracellular methylation enzymes.
hs-C-reactive Protein (CRP) and Fibrinogen: These tests measure the amount of the pro-inflammatory markers high sensitivity C-reactive protein, or hs-CRP, and fibrinogen in the bloodstream, and can be used to detect chronic inflammation and to monitor your progress as you work to reduce inflammation levels in your body.
Ferritin Test: This test screens for iron overload and excess free iron (unbound iron in the blood). While iron plays many important roles in the body, excess iron and iron overload has been linked to cancer and other diseases because of how it can cause oxidative stress.
Mg RBC: Magnesium is vitally important to overall health, yet most people are chronically deficient in magnesium. The Mg RBC test measures the amount of magnesium inside the red blood cells and is a far more accurate measurement of your body’s overall magnesium status than a standard serum (blood) test.
Comprehensive Female or Male Hormone Panel: These tests are available either as a single blood draw or a spit test in which saliva is collected multiple times over a 24hour period.
They typically measure the cycling and production of cortisol, DHEA, estradiol, pregnenolone, progesterone, and testosterone.
Serum Lactate Dehydrogenase (LDH) Test: One of the hallmarks of cancer cells is increased energy requirements associated with the higher rate of cellular proliferative activity. Metabolic changes in rapidly dividing cancer cells are closely associated with increased uptake of glucose and abnormal activity of lactate dehydrogenase (LDH), which regulates the processing of glucose to lactic acid. As serum LDH levels were found to be commonly increased in cancer patients and correlated with poor clinical outcome and resistance to therapy, the determination of LDH has become a standard supportive tool in diagnosing cancers or monitoring the effects of cancer treatment. (Forkasiewicz A, Dorociak M, Stach K, Szelachowski P, Tabola R, Augoff K. The usefulness of lactate dehydrogenase measurements in current oncological practice. Cell Mol Biol Lett. 2020 Jun 9;25:35 )
36 Super Charge Your Health To Protect Yourself Against Cancer
D-Dimer Test: D-Dimer is produced when a blood clot dissolves in the body. Under normal, healthy conditions, D-dimer in undetectable or only detectable at low levels, but its levels rise when the body forms and significantly breaks down blood clots, whether many small ones or even larger clots. For this reason, a D-dimer test is often used to detect blood clotting disorders.
Elevated D-dimer levels can also be an indication of certain cancers. As the authors of one medical study pointed out, “Research has established a direct link between the plasma level of D-dimer and underlying malignancy. D-dimer has a strong association with the detection and prognosis of several cancers. Pretreatment D-dimer levels can assist with cancer screening and prognosis assessment. Pretreatment plasma D-dimer levels can function as an effective cancer recurrence control. Elevated pre-treatment plasma D-dimer concentration is valuable in facilitating cancer screening, predicting an augmented risk of cancer recurrence, and anticipating a worse cancer prognosis.” (Siddiqui
NA, Malik M, Wijeratne Fernando R,
et al. D-Dimer: A Potential Solution to Problems of Cancer Screening, Surveillance, and Prognosis Assessment. Cureus. 2021 May 16;13(5):e15064.)
Tumor Markers
Should you or your doctor suspect you have cancer, tumor marker tests will also be ordered. These tests are primarily blood tests (in some cases, they are urine or bone marrow tests) used to both detect cancer and assess patients’ progress as they undergo treatment should cancer be detected. The tumor markers themselves are various proteins and other substances produced by cancer cells. The most common tumor markers, the cancers they screen for, and how they are used, can be found at the following section of the National Cancer Institute’s website: www.cancer.gov/ about-cancer/diagnosis-staging/diagnosis/tumor-markers-list.
Tumor marker tests used for detection purposes are not necessarily definitive. For a conclusive diagnosis should tumor marker testing indicate the presence of cancer, or changes in normal cells that can increase the risk of the probability for cancer. the cancer tests discussed below will often be required. In addition, sometimes tumor market tests can result in a “false positive” reading, showing that people have cancer when in actuality they do not. Such false positive readings can be due to other pre-existing health conditions, as well as other factors, that can potentially elevate tumor marker levels.
“False negative” results are common, as well, especially in the early stages of some cancers and when cancers are well encapsulated. Such false negative readings can leave physicians and patients alike thinking the patients are cancer-free, when in actuality they do have cancer, which can continue to grow and spread undetected. For this reason, tumor marker tests alone should never be the sole factor used by physicians to determine whether or not their patients have cancer.
37 Super Charge Your Health To Protect Yourself Against Cancer
Conventional and Other Cancer Tests
In addition to the testing methods covered above, commonly recommended cancer screening tests include colonoscopy, mammograms, prostate exam tests for me, and hemoccult stool tests.
Colonoscopy: Colonoscopy is a testing method that screens for signs of colon and rectal cancers. It involves inserting a tube known as a colonoscope, to which a video camera is attached, up through the rectum and the entire large intestine. Colonoscopy allows doctors to see inside this section of the gastrointestinal tract to screen for polyps, inflamed tissues and lesions, and other possible signs of cancer. Should polyps or suspect tissues be found, they can be removed during the procedure to be further examined via biopsy. It is recommended that all men and women age 50 and older have receive a colonoscopy every five to ten years. In people with a family history of cancer, the procedure may be recommended even earlier.
Various alternatives to colonoscopy might also be recommended by physicians, such as sigmoidoscopy and virtual colonoscopy, and well as hemoccult stool tests discussed below. While similar to a colonoscopy, the tube with an attached camera (sigmoidscope) that is used in sigmoidoscopy is not inserted beyond the lower part of the large intestine, but only through the rectum, sigmoid colon, and parts of the descending colon. It, too, can detect and remove polyps and suspect tissues and lesions, and can also screen for diverticulitis.
The advantages of sigmoidoscopy compared to colonoscopy are that it is less likely to cause perforation and internal bleeding, and can be performed more quickly and often without anesthesia.
Virtual colonoscopy employs CT scans or, in some cases, magnetic resonance imaging (MRI), of the entire large intestine. It also screens for polyps and other signs of colorectal cancers, but is incapable of removing them.
Hemoccult Tests: These tests can also screen for colorectal cancer. Hemoccult means “hidden blood,” and the tests screen for hidden blood in stool samples, in particular hemoglobin, a primary component of human blood. A positive finding of hemoglobin will usually result in further diagnostic tests being ordered, such as a colonoscopy or sigmoidoscopy, in order to screen for potentially cancerous polyps or tumors in the colon or rectum. One of the most commonly used hemoccult tests is the Cologuard test, which can also screen for DNA mutations that are common in cases of colorectal cancer.
A major advantage of the Cologuard and other hemoccult tests is that they can be performed at home, with the collected samples sent out to a lab for analysis. However, these tests aren’t always accurate, and can also result in false-positive readings.
38 Super Charge Your Health To Protect Yourself Against Cancer
Mammograms: Mammograms are among the most common cancer screening tests for women. They employ X-rays to screen dense structures of the breasts, which can be signs of tumors. Mammograms have been shown to detect up to 80 percent of all cases of breast cancers, although that percentage can fall depending on various factors, including a woman’s age, weight, breast size, breast density, and ethnicity. Mammograms are also less effective for finding tumors in the upper breast area and breast tumors located near the wall of the chest. Breast implants and fibrocystic breast disease can also interfere with the ability of mammograms to detect breast cancer.
An alternative to mammography is called thermography, which is discussed below.
Prostate Screening Tests: A variety of testing methods can be used to screen for prostate cancer in men. The most common is called the PSA (prostate-specific antigen) test. It is used to measure the level of PSA in the bloodstream. Elevated PSA levels can be an indication of prostate cancer, as well as an enlarged prostate gland (BPH). Should elevated PSA levels be found, usually physicians will follow up with a biopsy of prostate tissue.
Other prostate screening methods include a digital rectal exam, diagnostic ultrasound imaging of the prostate gland, a urine test called the Mi-prostate score (MiPS) which measures levels of various prostate cancer markers, and various blood tests that measure both bound and unbound (free) PSA levels, as well as the levels of certain proteins that PSA can bind to.
As with the standard PSA test, none of these other tests can definitively confirm if prostate cancer is present without a follow up biopsy.
Thermography: Thermography is the name given to a diagnostic technique that employs thermal (heat) imaging to enable physicians to get a clearer idea about what is taking place inside their patients’ bodies. It is an effective cancer screening method, and also very safe. It is can also be more effective than mammography for detecting breast cancer, including often detecting it earlier than mammograms are capable of doing. This is important because the earlier cancer is detected, the better the odds are for a full and lasting recovery.
Perhaps you are familiar with night vision goggles used by the military and police agencies. These goggles enable their wearers to spot people in the darkness by the heat signature emitted by their bodies. Thermography works in much the same way. It employs a special infrared sensitive camera to digitally record images of the surface temperature of the body. This enables thermography technicians to detect variations in surface body temperature throughout the entire body.
Abnormal variations in surface body temperature are biomarkers, or “fingerprints”, indicating the sign of tumors in the breasts or other potential health problems. These
39 Super Charge Your Health To Protect Yourself Against Cancer
temperature variations can be very subtle, but where they occur can be indications of cancer, since elevated metabolic activity and vascular circulation in both pre-cancerous and cancerous tissues and the surrounding areas are almost always higher, resulting in an increase in surface body temperature compared to that of normal, healthy tissue. This rise in surface body temperature is also due to the way that cancer cells nourish themselves via angiogenesis,which raises surface body temperature in the areas of the body wherever blood vessels have been taken over by tumors. Currently, only thermography is capable of detecting these temperature variations at their earliest stages.
Another major advantage of thermography is that it is noninvasive and quick, and free of the discomfort associated with mammograms. There is no compression, no direct contact with the body, and no harmful substances to be exposed to, let alone the cancer-causing radiation emitted by mammograms.
When receiving a thermogram, you will be positioned in front of the thermography camera so that all surfaces of the parts of your body being tested can be imaged. The images are captured in real time and then transmitted to a computer for analysis. The computer allows your doctor to isolate differences in surface body temperature and vascularity.
After the images are analyzed, they are graded using a standardized system based on five categories. Depending on the results of your exam, further tests may be ordered should there be any indication of tissue abnormalities. If your reading is normal, then your doctor has a baseline reading that she or he can compare to follow-up thermography readings as part of your annual health checkup.
Note: Many proponents of thermography, especially breast thermography, mistakenly make the claim that it can detect cancer up to ten years prior to the ability of mammography to do so. But this is not true. What thermography does is detect areas of inflammation in the body, including in the breasts.
Although chronic inflammation is certainly a major risk factor for cancer, its detection by thermography does not necessarily mean that cancer is present. Rather, it often only means that inflammation is present. This is still a useful finding, since it can lead patients and their physicians to address and reverse the inflammation and thus reduce the risk of cancer developing, but unless physicians and patients understand thermography’s limitations in this regard, findings of inflammation can lead to a “false positive” diagnosis of breast or other cancers, followed by unnecessary, inappropriate, and even harmful treatment.
Galleri® Test: The Galleri test is one I also recommend for cancer screening because of its effectiveness for detecting early signs of cancer signals. It works by screening for abnormalities in the specific patterns of cell-free DNA (cfDNA) in the blood. Should
40 Super Charge Your Health To Protect Yourself Against Cancer
they be detected, these abnormalities undergo analysis using the Galleri test’s unique sequencing and algorithm technology.
I discuss the Galleri test in more detail in the Appendix of this eBook. You can also find more information about it at www.galleri.com.
Now that you know about the importance of these cancer screening tests, let’s explore whether or not people’s personality traits can increase their likelihood of developing cancer. That is the topic of Chapter 4.
41 Super Charge Your Health To Protect Yourself Against Cancer
Cancer and the Mind/Body Connection
Ongoing research in the field of mind/body medicine (also known as psychoneuroimmunology, or PNI) continues to highlight the impact that our habitual thoughts, beliefs, and emotions have on our physical health and vice versa. So-called “negative” emotions, such as anger, anxiety, and depression have been shown to increase susceptibility to disease, whereas feelings of happiness, joy, and an optimistic nature can enhance the body’s resilience and resistance to disease by boosting immune function.
In the 1980s, based on his evaluations of cancer patients, O. Carl Simonton, MD, a radiation oncologist, found that patients who were habitually optimistic by nature typically achieved better outcomes from their cancer treatments, along with fewer side effects, compared to patients with the same type and degree of cancer who underwent similar treatments who were pessimistic. His study of the link between attitude and emotions among cancer patients led him to become a pioneer in the use of guided imagery as a supportive treatment for cancer. (See the Appendix for more about Dr. Simonton and his work.)
These findings by Dr. Simonton and other researchers parallel those of former Stanford University scientist Dr. Bruce Lipton and others, whose research shows that chronic stress is a primary cause of more than 95 percent of all types of disease conditions. (Lipton, Bruce. The Biology of Belief, 10 Anniversary Edition. 2016.)
What all of this research indicates is that effectively preventing and recovering from cancer, as well as other chronic condition, often requires healing long-standing unresolved emotional issues, negative beliefs and “faulty” thinking patterns.
The Findings of Dr. Ryke Geerd Hamer
Perhaps the most controversial research linking unresolved emotions to cancer (as well as all other forms of illness) was that of Dr. Ryke Geerd Hamer of Germany. Dr. Hamer’s work in this area not only resulted in him being banished from his position at a Munich hospital as an oncologist and specialist in internal medicine, but also led him to be arrested in Spain and extradited to France, where he was imprisoned after being sentenced in absentia (meaning he was never given the opportunity to defend himself) to three years in jail solely because of his groundbreaking research.
The pivotal moment in Dr. Hamer’s life that set him on his journey of discovery occurred in the 1980s when his 17-year-old son Dirk was accidentally shot while on va-
42 Super Charge Your Health To Protect Yourself Against Cancer CHAPTER 4
cation and died three months later. Soon thereafter, Dr. Hamer, who up until that time had always been healthy, was diagnosed with testicular cancer. Suspecting a link between his diagnosis and the death of his son, Dr. Hamer began researching the personal histories of cancer patients. Eventually, after extensively reviewing the cases of over 31,000 patients, Hamer found that, without exception, every one of them had suffered some type of shock, distress, or trauma prior to developing cancer. This led him to conclude that cancer, as well as all other diseases, occurs as a result of shock or trauma for which patients are totally unprepared.
According to Hamer, such shocks or traumas create a biological conflict in the body that causes visible changes in the brain. These changes in the brain, in turn, lead to functional disturbances in the organ or organs of the body that correspond to the areas of the brain that have been altered by shock or stress. The end result is the manifestation of cancer or some other type of disease.
All of the cancer patients whose cases Hamer researched underwent CT scans. In every case, the scans clearly showed anomalies in the area of the brain that corresponded to the organ of the body in which cancer occurred. Hamer was convinced that these findings confirmed his hypothesis. He also found that when the emotional issues that resulted from the shock or trauma that preceded cancer were resolved, follow-up CT scans revealed a normalization of the patients’ brains, which was then followed by a reversal of their cancer.
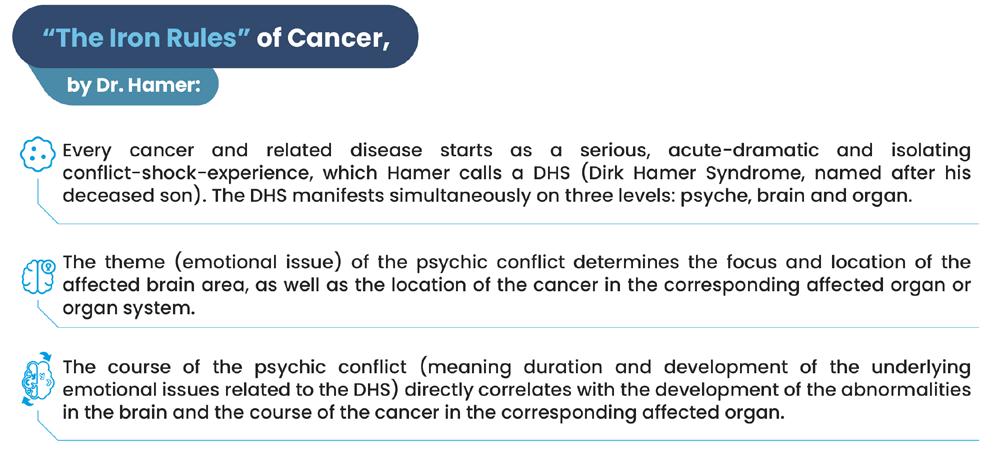
Based on his observations and research, Dr. Hamer developed what he calls “The Iron Rules of Cancer,” which are:
1. Every cancer and related disease starts as a serious, acute-dramatic and isolating conflict-shock-experience, which Hamer calls a DHS (Dirk Hamer Syndrome, named after his deceased son). The DHS manifests simultaneously on three levels: psyche, brain and organ.
43 Super Charge Your Health To Protect Yourself Against Cancer
2. The theme (emotional issue) of the psychic conflict determines the focus and location of the affected brain area, as well as the location of the cancer in the corresponding affected organ or organ system.
3. The course of the psychic conflict (meaning duration and development of the underlying emotional issues related to the DHS) directly correlates with the development of the abnormalities in the brain and the course of the cancer in the corresponding affected organ.
These so-called Iron Rules have been repeatedly verified using CT scans, not only by Dr. Hamer, but also by other physicians who have investigated his research.
Based on his findings, Hamer does not consider cancer and other diseases to be mistakes of nature that should be combated, but, rather, meaningful events that serve as indications of the need to restore equilibrium by the person affected with illness. Moreover, Hamer believed that if people can be prepared for any type of shocking event or trauma they will not become sick. And, if they can effectively undo the shock or trauma by healing their related emotional issues, recovery from cancer take place more easily.
Hamer also believed that most cases of cancer metastases or secondary tumors are caused by fears (of death or of cancer itself) that arise when cancer patients are given a cancer diagnosis or a negative prognosis, or by anger, resentment, or other emotions that can result from such a diagnosis and then remain unresolved.
Although Hamer’s research into the link between trauma, unresolved emotions, and cancer has been independently confirmed by other physicians, his view that shock and unresolved emotions are the sole causes of cancer, as well as other diseases, is not considered responsible by most health experts, even those who treat cancer from a holistic (body, mind, and spirit) perspective. I agree, especially in light of the extensive amount of research and documentation that exists linking cancer to many other causes and co-factors. Effective, long-term success when it comes to treating cancer can only be achieved by addressing all such causes.
Emotional Characteristics Common to Cancer Patients
In addition to depression and chronic stress, the most common emotional characteristics of cancer patients are anxiety, fear, grief, hopelessness, indecisiveness, loneliness, and low self-esteem and lack of self-worth. Many cancer patients also live isolated lives and lack meaningful personal relationships. Other emotional issues that can act as co-factors in the cancer process are bigotry, hostility, resentment, and selfishness.
Limited and erroneous beliefs can also play a significant role in how patients respond to their cancer treatments. For example, many people, upon being diagnosed with cancer, automatically assume the worst, even when there is no reason to do so. As a
44 Super Charge Your Health To Protect Yourself Against Cancer
result, they can unconsciously sabotage their ability to recover even when they receive the most appropriate and effective forms of cancer treatment.
Chronic, unresolved emotions have also been shown to significantly affect the immune system by lowering the immune response. This is of utmost importance when it comes to preventing and treating cancer since a healthy immune system is essential in both cases. Therefore, it is vitally important that all of us, whether or not we have cancer, take care to properly manage and express our emotions and to do all that is necessary to heal and recover from any unexpected shocks or traumas we may have sustained.
For a number of years, researchers speculated that people having the above traits had what was called a “Type C” personality that more readily predisposed them to developing cancer. While this theory of a specific type of cancer personality has subsequently been rejected by many researchers, the evidence remains clear that one’s habitual attitudes, emotions, thoughts and beliefs can and do influence both susceptibility and resistance to disease depending on the characteristic traits and attitudes one holds about life.
Are Your Emotions Making You Sick
The following checklist of questions can help you to determine if you at risk for developing cancer, as well as various other illnesses, due to unresolved and improperly expressed emotions, as well as your habitual attitude, beliefs, and behaviors. Answer each question truthfully. The more Yes answers you give, the more likely it is that you need to start addressing your emotions and beliefs in order to stop them from compromising your health.
1. Have you endured an unexpected shock or trauma within the last 3 years (examples: death of a loved one, divorce, break up of a relationship, loss of your job, etc)?
2. Do you regularly experience bouts of sadness or grief?
3. Do you regularly experience bouts of anxiety or depression?
4. Are you experiencing lingering feelings of anger or resentment towards anyone or anything?
5. Do you suffer from low self-esteem?
6. Do you lack meaningful relationships in your life?
7. Do you feel isolated and lonely due to spending much of your personal time by yourself?
8. Do you overburden yourself by taking on more than your fair share of responsibilities despite the stress that doing so causes you?
9. Are you pessimistic by nature?
10. Do you harbor lingering regrets over experiences from your past?
45 Super Charge Your Health To Protect Yourself Against Cancer
11. Do you feel as if you are cut off from support from others and have to do everything on your own?
12. Are you prone to compromise so as not to hurt others’ feelings even when doing so means giving up on your own desires and dreams?
13. Do you believe that life is a struggle filled with hardships that only a few, lucky or privileged people ever escape?
14. Are you pessimistic about the future and the way things are going in the world?
15. Are you an “all work and no play” type of person?
16. Are you a “people pleaser” who puts the needs of others before your own needs and desires?
17. Do you regularly crave the approval of others and do you become upset or depressed if you don’t receive it?
18. Do you fear or are you resistant to life changes and moving out of your “comfort zone”?
19. Do you habitually repress your emotions, both positive and negative?
20. Do you lack a sense of purpose in your life and/or do you excessively worry about the future.
Healing your mind and emotions requires a committed effort on your part, and may also require, at least initially, working with a trained counselor or health care practitioner trained in the field of mind/body medicine. If you feel that you require such assistance based on your responses to the above question, don’t hesitate to seek it out.
Getting Help
The following therapies are highly effective treatments for mental and emotional conditions:
● Bach flower remedies
● Biofeedback and neurofeedback therapy
● Breathwork
● Energy psychology
● Guided imagery and visualization,
● Hypnotherapy
● Journaling
● And meditation
Professional counseling can also be helpful, as can certain other forms of “talk therapy,” such as cognitive therapy. However, avoid counselors and psychiatrists who focus on treating emotional issues with drugs—not only does this approach fail to address the deeper underlying issues that are causing your emotional problems, it is also highly toxic and can cause a host of serious side effects, including liver and kidney damage, impaired brain functioning, and even violent acts, including suicide.
46 Super Charge Your Health To Protect Yourself Against Cancer
Note: In many cases of mental and emotional difficulty, physical factors such as food allergies, poor diet, and nutritional deficiencies can also play a significant role. These and other physical factors should always be screened for whenever emotional or mental difficulties become chronic, as well as for all cases of cancer.
Cancer Resistant Personality Traits
Just as research has established that there are habitual personality traits that can add to the risk of cancer and other illnesses, as well as reducing the likelihood of full and lasting recoveries, studies also show that more positive and life-affirming traits can improve one’s resistance to cancer and illness in general and aid in recovery.
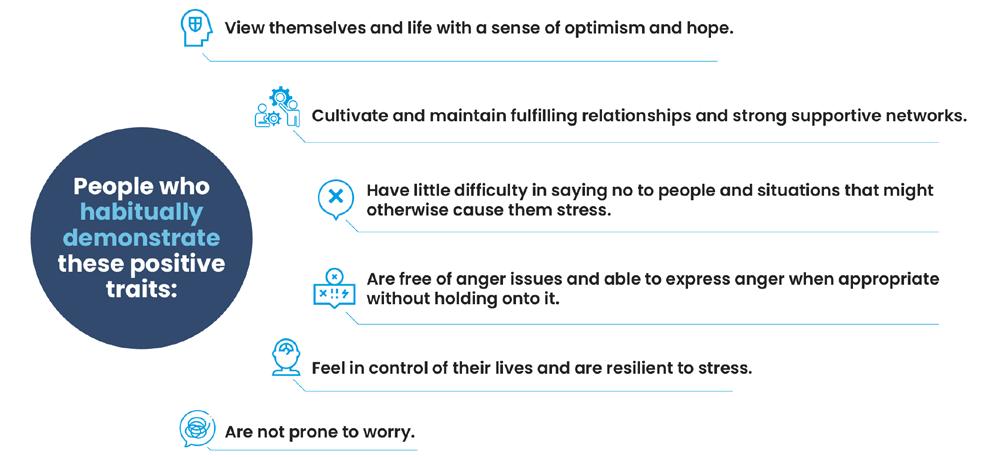
People who habitually demonstrate these positive traits typically:
● View themselves and life with a sense of optimism and hope.
● Cultivate and maintain fulfilling relationships and strong supportive networks.
● Have little difficulty in saying no to people and situations that might otherwise cause them stress. Are free of chronic depression and anxiety.
● Are free of anger issues and able to express anger when appropriate without holding onto it.
● Feel in control of their lives and are resilient to stress.
● Are not prone to worry.
In addition, although they enjoy pleasing others, they do not do so out of a need to seek approval from others.
(Golizek A, PhD. Is There A Cancer-Prone Personality? Psychology Today. Nov 13, 2014. Available at www.psychologytoday.com/us/blog/how-the-mind-heals-thebody/201411/is-there-cancer-prone-personality)
47 Super Charge Your Health To Protect Yourself Against Cancer
Traits and Life Choices of Cancer Survivors: People who undergo treatments for cancer and achieve remission also typically share characteristic traits and make similar life choices. This is especially true of people who have triumphed over advanced cases of cancer even after being told that their chances of recovery were very low. These same traits and life choices can be used to prevent cancer, as well.
Kelly A. Turner, PhD, identified nine factors that survivors of advanced cancer all have in common after spending over a decade reviewing more than 1,500 cases of patients who successfully recovered from late-stage cancers despite being given poor prognoses by their doctors. These factors are also common to people who have Spontaneous Remissions or Regressions of their cancers. She shared her discoveries in her book Radical Remission: Surviving Cancer Against All Odds
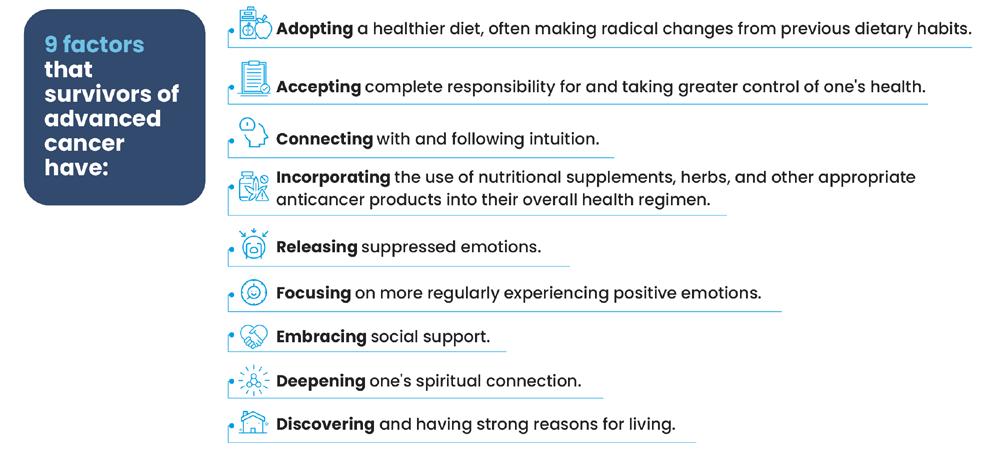
The nine factors are:
1. Adopting a healthier diet, often making radical changes from previous dietary habits.
2. Accepting complete responsibility for and taking greater control of one’s health.
3. Connecting with and following intuition.
4. Incorporating the use of nutritional supplements, herbs, and other appropriate anticancer products into their overall health regimen.
5. Releasing suppressed emotions.
6. Focusing on more regularly experiencing positive emotions.
7. Embracing social support.
8. Deepening one’s spiritual connection.
9. Discovering and having strong reasons for living.
48 Super Charge Your Health To Protect Yourself Against Cancer
These traits and life choices can be adopted and made by everyone to enhance health and prevent disease, and to improve recovery outcomes should cancer or other diseases strike.
Spontaneous Remissions
Perhaps the most remarkable indication of how inextricably physical health, as well as physical diseases, including cancer, are connected to our habitual thoughts, beliefs, and emotions are recoveries from cancer and other potentially fatal diseases that are termed “spontaneous remissions”. Such recoveries are seemingly miraculous in that they often occur despite poor prognoses by doctors and when treatments show little improvements. In such cases, recovery is often credited to shifts within the psyches of patients that include a new or renewed commitment on the part of the patients to live out the rest of their lives in ways that are radically different than how they were previously living prior to their diagnoses. Such shifts also typically bring about new perspectives and levels of awareness that appear to mobilize inner resources within the patients that enable their bodies to arrest and eliminate cancer.
Research into the phenomena of spontaneous remissions began decades ago. What studies have shown is that such remissions are not actually spontaneous. Rather, they are the result of internal changes patients made in terms of their thoughts and beliefs. As Dr. Jeffrey D. Rediger, a licensed physician, board-certified psychiatrist and theologian who has studied cases of spontaneous remissions and interviewed patients who have achieved them explains, “All of these individuals changed their perception of themselves and the world. Although many eliminated processed foods, changed their lifestyles, and dealt with repressed emotions or came to terms with difficult relationships, what they really want to talk about—what has caused them to eventually view the illness as a gift—is how the illness helped them change their relationship with themselves. Whether it took ten minutes or ten years, each individual I have spoken with has talked about how, at the core of their healing, they learned to let go of negative voices of criticism and self-criticism, and to see themselves in a more compassionate, unconditional light.” (Rediger J. Spontaneous Remission: Fact Or Fiction? Psychology Today. Feb 10, 2016. Available at www.psychologytoday.com/ intl/blog/stress-is-laughing-matter/201602/spontaneous-remission-fact-or-fiction)
Discovering or rediscovering what one perceives to be one’s life mission, and then committing to fulfilling it, is another important dynamic exhibited by patients who experience partial or complete spontaneous remissions. In a scientific paper published in 2004 in The Scienitific World Journal, the authors began by writing:
“The recovery of the human character and purpose of life with consciousness-based medicine seems to be able to induce spontaneous remissions in several diseases. On two different occasions, we observed breast tumors reduced to less than half
49 Super Charge Your Health To Protect Yourself Against Cancer
their original diameters (clinically judged) during a holistic session, when working with the patients in accordance with the holistic process theory of healing, the life mission theory, and the theory of human character...
“We find it extremely interesting that the size of a tumor can be reduced dramatically within a few hours of holistic treatment, when the patient is highly motivated for personal development. The reduction of tumor size is in accordance with the holistic view that many types of cancer are caused by emotional and existential disturbances. From a holistic perspective, cancer can be understood as a simple disturbance of the cells, arising from the tissue holding on to a trauma with strong emotional content. This is called ‘a blockage’, where the function of the cells is changed from their original function in the tissue to a function of holding emotions. “The reduction of the tumor in the two cases happened when old painful emotions were identified in the tissues, in and around the tumor, and processed into understanding; when the patients finally did let go of negative beliefs and attitudes that had kept the feeling(s) repressed to that part of the body, the tumor first softened and then disappeared, presumably by apoptosis... “An additional aspect for the patient who is able to cure her own cancer is that she is much less likely to get cancer again and much better prepared to deal with other diseases and challenges in life...To support the patient in learning the mastery of coherence of body and life, using the crisis of cancer to recover the human character and the purpose of life, seems turning a personal potential disaster into the greatest gift of all. When it comes down to it, life is not just about surviving; what is more important is to live fully, to learn from the great challenges of life, and to obtain the optimal quality of life while being here.” Ventegodt S, Morad M, Hyam E, Merrick J. The Clinical Holistic Medicine: Induction of Spontaneous Remission of Cancer by Recovery of the Human Character and the Purpose of Life (the Life Mission) The Scientific World Journal. 2004; 4:362–377.
Based on what researchers continue to discover about the traits and life choices of patients who achieve spontaneous and other long-lasting remissions of cancer and other illnesses, it seems apparent that adopting and making them are important steps we all should consider.
50 Super Charge Your Health To Protect Yourself Against Cancer
Conventional Cancer Treatments and Their Limitations
The main conventional treatment methods used to treat cancer patients today are the same as they were decades ago: surgery, chemotherapy, and radiation therapies, often in combination with each other. In recent years, immunotherapies have also been developed, although their use currently is limited. Each of these three primary classes of treatments have their benefits, and advances have continue to be made within each of them. However, their long-term success rates, especially for late-stage cancers, still leaves much room for improvement (see Survivorship in the Appendix). In this chapter, I discuss the benefits and limitations of each of them.
Surgery
Surgery is usually the first treatment recommended for cancers that present as localized tumors that have not yet spread (metastasized) to other parts of the body. It has little value as a treatment for metastatic (late-stage), and no value for cancers of the blood (leukemias). If localized cancerous tumors are detected early enough, surgery may be the only conventional treatment that is required. Usually, however, it will be followed with a course of chemotherapy or radiation treatments, and often both. In either case, surgery is an important, even essential, treatment for localized tumors because research shows that the longer tumors remain in the body and continue to grow, the more that cancer is able to spread beyond the primary tumor site to metastasize to other areas of the body, making successful eradication of cancer much more difficult to achieve. (For more information about the need for surgery to prevent tumor spread, see the Appendix.)
The purpose of surgery is to remove localized tumors, ideally entirely, but sometimes only partially. Partial removal of a tumor is known as debulking surgery. It is typically employed if removing the entire tumor carries a risk of damaging a nearby organ. During surgery, patients are anesthetized as surgeons cut through skin and muscle, and sometimes bone, to get at the tumor.
There are two types of traditional surgery: open and minimally invasive. Open surgery involves the surgeon opening up the body with a large cut to take out the tumor. In some cases, surrounding healthy tissue and nearby lymph nodes may also be removed.
Another name for minimally invasive surgery is laparoscopic surgery. In this procedure the surgeon makes small cuts in the area of the body in which the tumor is located. A tube with an attached camera, called a laparoscope, is then inserted into
51 Super Charge Your Health To Protect Yourself Against Cancer CHAPTER 5
one of the cuts, enabling the surgeon to view the inside of the body area. Using specialized surgical tools inserted into the other small cuts, the surgeon is able to remove the tumor. Typically, recovery from laparoscopic surgery requires less time than from open surgery.
Biopsy is another commonly used minimally invasive surgery.
Cryosurgery and laser surgery are two other types of surgical cancer treatments. Cryosurgery involves exposing tissues to extreme cold, typically by applying a probe containing liquid nitrogen, or sometimes argon gas, in order to destroy and eliminate abnormal cells and tissues. It is often used to treat precancerous growth on the skin and skin cancer in its earliest stages. It can also be used to address growths on the cervix.
As its name implies, laser surgery involves the use of lasers. The light emitted by laser surgical devices are powerful enough to cut through tissue. Since the beams of light can be tightly focused on small areas of the body, laser surgery is often used to perform precision surgeries. It is also sometimes effective for shrinking and potentially destroying tumors and precancerous growths. Among the cancers that laser surgery may be used to treat are basal cell carcinoma, cervical cancer, esophageal cancer, and non-small cell lung cancer.
Side Effects: In addition to the pain in the area of the body on which surgery was conducted, surgery can cause abnormal bleeding, infections, and tissue damage, all of which can suppress immune function, as does surgery itself. Some patients also experience side effects related to the anesthesia they receive during surgery.
Another serious and not uncommon risk factor of surgery to remove tumors is the unnecessary removal of other parts of the body. Two examples of this are radical mastectomy of the breast instead of a less invasive lumpectomy, and the removal of the prostate gland in cases of prostate cancer, causing multiple side effects, including urinary incontinence, erectile dysfunction, and impotence, in men.
But potentially the biggest risk of surgery as a cancer treatment, because it is so often ignored, has to do with what are called circulating tumors cells (CTCs). CTCs are microscopic cancer cells that break off from tumors as the tumors are being operated on. Once they do so, CTCs can then travel in the bloodstream to other areas of the body, where they can go undetected and act as seeds for the subsequent formation of additional tumors in other organs. This mechanism of action by CTCs is responsible for the vast majority of cancer recurrences and cancer-related deaths. Even biopsy procedures can cause CTCs to break away from tumor samples. A special class of CTCs are known as cancer stem cells (CSCs), which are what trigger other cells to become cancerous. (For more about CSCs, see the Appendix.)
52 Super Charge Your Health To Protect Yourself Against Cancer
Chemotherapy
Chemotherapy is the most commonly used treatment for most types of cancer. It typically follows surgery to remove tumors in an effort to destroy any remaining cancer cells and thus prevent a recurrence of cancer, and is often the first recommended course of action for cancers that have progressed to a point where surgery is not an option. In some cases, chemotherapy might be employed before surgery in an effort to shrink a tumor, making it easier to for surgeons to remove it. (Radiation therapy can also be used for this purpose.) Chemotherapy is also used to treat leukemias and lymphomas.
There a many different chemotherapy drugs and chemo treatment plans depend the type of cancer to be treated, its staging, and its location in the body. Whether or not patients are suffering from other health conditions and, if so, what medications they have been prescribed, are also determining factors.
As the National Cancer Institute (NCI) explains, “[T]he weapons used to fight cancer in chemotherapy are a host of anti-cancer drugs. How differently these drugs kill cancer cells, or prevent them from dividing, depends on their classification. Drugs in the same class kill cancer cells by the same mechanism: they all attack the same target within the cell
“Depending on the type of cancer and the kind of drug used, chemotherapy drugs may be administered differently. They can be administered orally (oral chemotherapy), or injected into a muscle (intramuscular injection), injected under the skin (subcutaneous injection), or into a vein (intravenous chemotherapy). In special cases, chemotherapy drugs may be injected into the fluid around the spine (intrathecal chemotherapy). Two or more methods of administration may be used at the same time under certain circumstances. No matter what method is used, chemotherapy drugs are absorbed into the blood and carried around the body.
“Of all the methods of chemotherapy drug administration mentioned above, intravenous injection is most commonly used. It is the most efficient way to get the medication into the bloodstream. Oral chemotherapy is more convenient and does not require any specialized equipment.
In chemotherapy, cancer patients may be given one or several drugs from the available anti-cancer drugs. Since different chemical agents damage cancer cells in different ways and at different phases in the cell cycle, a combination of drugs is often employed to increase the cancerous cell-killing effectiveness. This is called combination chemotherapy.”
Patients respond to chemotherapy in different ways, depending on the type and dosage of chemotherapy they receive, and the type and staging of the cancer they have, as well as their overall health status at the start of treatment. Because of this
53 Super Charge Your Health To Protect Yourself Against Cancer
variance in response rates, oncologists carefully monitor cancer patients to determine the effectiveness of their treatments and to mitigate side effects should they occur. During their course of treatment, patients typically will also undergo follow-up physical exams, receive tumor marker and other blood tests, and receive CT, MRI, or PET scans if necessary, to further assess how well they are responding to the chemotherapy they receive.
Side Effects: Chemotherapy drugs can be highly toxic. Although they are used in the hope that they will kill cancer cells and prevent further tumor growth, they can, and often do, cause harm to the body’s healthy cells and tissues. This can result in a wide range of side effects.
According to the NCI, “normal cells most likely to be affected by chemotherapy are blood cells forming in the bone marrow, and cells in the digestive tract, reproductive system, and hair follicles. Common side effects of chemotherapy include fatigue, nausea, diarrhea, mouth sores, hair loss, and anemia.”
Chemotherapy can also negatively affect the body’s ability to produce platelets and red and white blood cells in bone marrow. Platelets help blood to clot and prevent bleeding, while red blood cells transport oxygen throughout the body, and white blood cells fight infection. Reduction in the levels of these cells caused by chemotherapy also impairs their functions. In most cases, this is temporary, with recovery occurring after chemotherapy treatments are completed. Even so, the resulting impairment during treatment can often be severe, causing intense fatigue, as well as a greater risk for infection.
Healthy cells within the gastrointestinal tract can also be harmed by chemotherapy, causing a host of GI tract-related side effects ranging from loss of appetite to mouth sores, nausea, constipation and/or diarrhea, vomiting, and overall diminished digestive function.
Other common side effects of chemotherapy include pain, impaired memory and other cognitive function (“chemo brain”), neuropathy, and damage to the heart (cardiotoxicity), liver, and lungs. Finally, chemotherapy can also cause secondary cancers to occur, and in rare cancer can trigger leukemia when it is used as a prolonged treatment for solid-state cancerous tumors.
Radiation Therapy
More over 50 percent of all cancer patients in the U.S. are treated with radiation therapy. It can be used alone, and also as treatment used in combination with surgery and/or chemotherapy.
Radiation therapy as a treatment for cancer involves the use of x-rays, gamma rays and other sources of radiation to target and destroy cancer cells. In some cases,
54 Super Charge Your Health To Protect Yourself Against Cancer
the cells are eliminated immediately. In other cases, the radiation damages cellular DNA and various other cancer cell components, impeding the ability of cancer cells to continue dividing and spreading.
Radiation therapy is usually administered using specialized instruments that produce beams of high intensity x-rays directed at cancer sites. According to the NCI, “Due to the advancement of technologies, newly developed machines are able to produce radiation beams of much greater energy while maintaining pinpoint accuracy.” Since the emitted radiation affects both cancer and normal cells and tissues, radiation treatments must be carefully planned to minimize damage to health cells, tissues, and organs near the cancer sites exposed to radiation.
In general, radiation therapy is directed to the tumor and to the area of the body surrounding it The goal is to destroy the tumor and prevent any potential further spread of cancer cells. Higher total doses of radiation are used to destroy the main tumor, with lower doses administered to destroy the spread of the tumor cells. Patients receive multiple doses of radiation treatments, with time in between each treatment to allow healthy cells to repair any radiation damage.
According to the NCI, “The decision to treat a tumor with radiation is based on the location of the primary tumor and whether the tumor cells are radiosensitive. Although radiation therapy and surgery have similar cure rates, for some types of cancer, radiation therapy is preferred to surgery if the patient has a preexisting condition that makes surgery impossible or if surgery would require removing part or all of an organ. For example, radiation therapy may be chosen to treat cancer of the larynx in order to preserve the voice.
“Radiosensitive tumors respond by promptly showing regression after moderate doses of radiation. Two examples of highly radiosensitive cancers are leukemia (cancer of the blood cells) and lymphoma (cancer of the lymphatic system).
“Radiation therapy is most effective when a tumor is contained, easily accessible, and located away from major organs of the body. Testicular cancer, for example, is one of the best candidates for radiation therapy. During the process of radiation therapy for testicular cancer, the rest of the body can be easily protected from the radiation. Radiation can be directed from all angles to increase the effectiveness of the treatment.
“Radiocurability means that the normal tissue-tumor relationship is such that curative doses of radiation can be used without excessively damaging the normal tissue. Radiocurative tumors include carcinoma of the cervix, larynx, breast, and prostate. Radiation may be the only therapy necessary for radiocurative tumors.”
As with chemotherapy, the way that radiation therapy is used depends on various factors, starting with the type of cancer one has, its location and staging, and how
55 Super Charge Your Health To Protect Yourself Against Cancer
close tumors are to healthy organs that could potentially be harmed by radiation, as well as patient age, medical history, and any other types of medical care they may be receiving.
There are two main types of radiation treatments: external beam radiation and internal radiation therapy. External beam radiation, the most commonly used type, directs targeted radiation to cancer sites in the body. Typically, the radiation is emitted using devices called linear accelerators . With internal therapy, a radioactive substance is placed inside the body close to cancer cells or the tumor mass. The radiation source can be a capsule or a liquid. In the case of internal radiation therapy using capsules, the capsule is inserted inside of or near to a a tumor using a minimally invasive surgical procedure, so that the radiation the capsule contains can destroy the tumor. In some cases, the capsule is kept in place, in others, it is removed, as determined by the radiation oncologist.
Just as with chemotherapy, radiation therapy, regardless of whether it is external or internal, cannot be used indefinitely due to safety issues. Regardless of which type of radiation therapy is used, there is a limit to how much radiation treated areas of the body can safely receive, and patients must be carefully monitored to address any potential side effects.
Side Effects:
The most common side effect of radiation therapy is fatigue, both during and after treatments. At times, the fatigue can be quite severe. Another common side effect of radiation therapy include unhealthy changes in skin in the areas of the body that are irradiated. Hair loss can also occur, as can loss of appetite, nausea, and vomiting.
Side effects of radiation used to treat breast cancer include edema and tenderness in and around the breasts. Radiation directed at the breasts and chest can also cause chronic coughing, breathing difficulties.
Common side effects of radiation therapy that targets the head or neck include difficulty swallowing and other throat issues, blurred vision, headache, memory and cognition problems, impaired thyroid function, and damage to the thyroid gland.
Radiation therapy directed at the stomach, pelvic area, or rectum can cause bladder and other urinary tract issues, as well as diarrhea and other gastrointestinal problems. Infertility and other sexual issues can also occur in both men and women.
Damage to other healthy cells and tissues in the body can also be caused by radiation therapy. Usually, such damage is not permanent and will resolve within a few months after the therapy ends, but in some cases the damage can last indefinitely, impairing patients’ overall quality of life.
56 Super Charge Your Health To Protect Yourself Against Cancer
Late Effects of Chemotherapy and Radiation Therapy
In some cases, potential side effect of both chemotherapy and radiation therapy may not arise until months, and even years, have passed from the time patients complete their treatments. Such delayed side effects are known as “late effects”, and are well established and recognized by the National Cancer Institute and other cancer organizations, cancer researchers, and oncologists.
As with side effects in general, late effects vary from patient to patient, and also vary according to the specific treatments patients received, and at what dose.
Bone loss over time is one late effect that can occur. It can be caused by either chemotherapy or radiation therapy. The difference is that chemotherapy can cause delayed bone loss anywhere in the body, whereas delayed bone loss caused by radiation therapy typically only occur in the area of the body that received radiation.
Other late effects known to occur from both chemotherapy and radiation include cardiovascular issues; lung problems; include scar tissue formation in the joints, leading to impaired mobility; cataracts and other vision problems; hearing loss, tinnitus, and other hearing issues; issues in the mouth, including dry mouth, cavities, and bone loss in the jaw; impaired digestion and other gastrointestinal problems; unhealthy weight gain; and damage or unhealthy changes to various endocrine glands, particularly the thyroid gland, ovaries, and testes.
Delayed issues in the brain can also happen, especially in terms of memory loss and impaired cognition. In some cases, personality and other behavioral changes can also arise.
In addition, according to the NCI, both chemotherapy and radiation therapy can set the stage for new cancers to occur, even “many years after you have finished treatment. When a new primary cancer occurs in a person with a history of cancer, it is known as a second primary cancer. Second primary cancer is not the same thing as metastatic cancer, which is when cancer spreads from where it started.”
The risks for all of the above side effects associated with surgery, chemotherapy, and radiation therapy can be reduced when those therapies are supported by pulsed electromagnetic field (PEMF therapy) as well as other complementary and alternative (CAM) therapies. How and why this is so is explained in Part Two of this eBook.
57 Super Charge Your Health To Protect Yourself Against Cancer
Chapter References
● Abid SH, Malhotra V, Perry MC. Radiation-induced and chemotherapy-induced pulmonary injury.CurrOpinOncol. 2001 Jul;13(4):242-8.
● Broder H, Gottlieb RA, Lepor NE. Chemotherapy and cardiotoxicity. Rev Cardiovasc Med. 2008 Spring;9(2):75-83.
● Chatterjee K, Zhang J, Honbo N, Karliner JS. Doxorubicin cardiomyopathy. Cardiology. 2010;115(2):155-62.
● Curative Radiation Therapy. National Cancer Institute. https://training. seer.cancer.gov/treatment/radiation/therapy.html
● Introduction to Radiation Therapy. National Cancer Institute. https:// training.seer.cancer.gov/treatment/radiation
● Late Effects of Cancer Treatment. National Cancer Institute (NCI). www. cancer.gov/about-cancer/coping/survivorship/late-effects
● Lefrak EA, Pitha J, Rosenheim S, Gottlieb JA. A clinicopathologic analysis of adriamycin cardiotoxicity. Cancer. 1973 Aug;32(2):302-14.
● Miller KD, Nogueira L, et al. Cancer treatment and survivorship statistics, 2022.CA: A Cancer Journal for Clinicians Sept/Oct 2022;72(5):409-36.
● Possible Side Effects. National Cancer Institute. Available at training.seer. cancer.gov/treatment/chemotherapy/sideeffects.html
● Possible Side Effects. National Cancer Institute. https://training.seer. cancer.gov/treatment/radiation/sideeffects.html
● Radiation Therapy Side Effects. National Cancer Institute (NCI). www. cancer.gov/about-cancer/treatment/types/radiation-therapy/side-effects
● Ramadori G, Cameron S. Effects of systemic chemotherapy on the liver. Ann Hepatol. 2010 Apr-Jun;9(2):133-43.
● Sharma A, Houshyar R, Bhosale P, et al. Chemotherapy induced liver abnormalities: an imaging perspective. ClinMolHepatol. 2014 Sep;20(3):317-26.
● Singal PK, Deally CM, Weinberg LE. Subcellular effects of adriamycin in the heart: a concise review. J Mol Cell Cardiol. 1987 Aug;19(8):817-28.
● Surgery to Treat Cancer. National Cancer Institute (NCI). www.cancer. gov/about-cancer/treatment/types/surgery
● Swain SM, Whaley FS, Ewer MS. Congestive heart failure in patients treated with doxorubicin: a retrospective analysis of three trials. Cancer. 2003 Jun 1;97(11):2869-79.
● Takemura G, Fujiwara H. Doxorubicin-induced cardiomyopathy from the cardiotoxic mechanisms to management. ProgCardiovasc Dis. 2007 Mar-Apr;49(5):330-52.
58 Super Charge Your Health To Protect Yourself Against Cancer
● Types of Chemotherapy Drugs. National Cancer Institute. Available at training.seer.cancer.gov/treatment/chemotherapy/types.html
● Types of Radiation. National Cancer Institute. https://training.seer.cancer. gov/treatment/radiation/types.html
● Vander Els NJ, Stover D. Chemotherapy-Induced Lung Disease.Clin Pulmonary Med. 2004 Mar;11(2):84-91.
● Vento S, Cainelli F, Temesgan Z. Lung infections after cancer chemotherapy. The Lancet Oncology. 2008 Oct;9(10):982-992.
● Von Hoff DD, Layard MW, Basa P, et al. Risk factors for doxorubicin-induced congestive heart failure. Ann Intern Med. 1979 Nov;91(5):710-7.
59 Super Charge Your Health To Protect Yourself Against Cancer
Pulse Electromagnetic Field (PEMF) Therapy and the Many Health Benefits It Provides
If you have ever held two magnets in your hands, tried to force them together, and felt a resistance between them, then you have experienced a magnetic field. That type of magnetic field is produced by a static magnet and is called a static magnetic field.
A changing magnetic field (such as a magnetic field moving through a coil) generates an electric field (which would drive a current in the coil). This forms the basis for many electrical generators and motors. Similar to the way that a changing magnetic field generates an electric field, a changing electric field generates a magnetic field. Since the magnetic field is being generated by an electric current, it’s called an electromagnetic field—a physical field produced by moving, or pulsing, electrical charges. PEMF stands for Pulsed Electromagnetic Field.
Magnetic fields affect the behavior of any other charged objects in the vicinity of the field. This is the fundamental basis for their therapeutic use. Our bodies are electric— every heartbeat generates electromagnetic waves throughout the blood vessels of the body, stimulating tissues at a cellular level. External magnetic fields and the normal electric and electromagnetic fields produced by the body interact. So, a magnetic field passing through our whole body will have an electromagnetic effect on each of our trillions of cells. As a result, magnetic fields act in basic and fundamental ways on molecules and tissues. They affect the most basic functions of all cells, not only in humans, but also in animals and plants.
Basic Cell Function and How Magnetic Fields Facilitate Them
Some of the basic actions of a cell are to generate energy to eliminate waste, to repair and regenerate itself, and to perform its predetermined functions based on the cell’s type and location in the body. Magnetic fields cause or increase motion of ions and electrolytes in the tissues and fluids of the body. It’s both easy to quickly move an ion or electrolyte in a living organism using magnetic fields. This movement stimulates a vast array of chemical and electric actions in the tissues of the body, helping them to rebalance or heal themselves where necessary.
All cells need energy to function. Cellular energy requires ATP (adenosine triphosphate), which is fundamental to all cell and body functions, and necessary to sustain life itself. ATP regulates cell metabolism by transporting chemical energy within our
60 Super Charge Your Health To Protect Yourself Against Cancer PART TWO - PEMF THERAPY AND CANCER | CHAPTER 6
cells. Low ATP levels cause our cells to be sick, and decreases their ability to heal, regenerate, or function properly. Through the increased motion of ions and electrolytes, magnetic fields help cells increase their energy, or “charge”, by up to 500 percent.
Magnetic fields also affect the charge of the cell membrane, which allows membrane channels to open up. These channels are like the doors and windows of a house. By opening cell channels, nutrients are better able to enter the cell and cellular waste is more easily eliminated. This helps to rebalance and restore optimum cell function. If you restore enough cells, they will all work more efficiently.
Cells of the same type come together to make tissues, and those tissues come together to make organs. By restoring or maintaining cellular function, you will, in turn, restore or maintain organ function, allowing the entire body to function better. We all know that the body ages over time. Maintaining the function of every individual cell at an optimal level every day is an important part of slowing aging.
Magnetic fields are proven to help maintain cellular function. They also protect against cell injury, a primary cause of disease conditions. Among the ways that such fields can prevent cell injury is by improving circulation, repair processes, and energy production, and increasing special stress proteins in the cells. These proteins are used to prevent cell breakdown and wear and tear, as well as help speed recovery from injury. Magnetic fields, particularly pulsed electromagnetic fields, balance cells, tissues and bodily functions at very fundamental levels, even before damage and problems become obvious.
PEMF Therapy’s Healing Benefits
Ongoing research into PEMFs have identified more than 25 ways that PEMF therapy supports both physical and psychological health. My own investigations, as well as my work as a physician who treats patients with PEMF therapy, has confirmed these research findings. PEMF therapy is one of the most effective health treatments available to us today, as well as one of the most versatile. The fact that it also readily lends itself to home treatment as a significant self-care tool significantly adds to its overall value. This is of particular importance for cancer patients because of how PEMF therapy can support the treatments they receive from their doctors.
Most of the beneficial effects of PEMFs occur through the basic actions of magnetic fields and electrical charge on cellular biology. All cellular communications in our bodies require an electrical signal which triggers the release of chemicals. In turn, these chemical reactions cause a change in the neighboring cell. This chain of electrical signal actions continues rapidly until the cell’s function has been completed. PEMFs enhance and support this charge activity when it is out of balance, causing cells to function more efficiently, but only when they need extra help. Research studies have confirmed that the appropriate therapeutic use of PEMFs only
61 Super Charge Your Health To Protect Yourself Against Cancer
affects or improves body systems that are compromised, while not affecting normal or healthy systems or tissues, unlike even properly prescribed medications and other medical interventions.
The benefits of this type of electrical charge support are both big and small. From the tiniest molecule or enzyme up to the largest organ system (skin), you can find a process PEMFs either streamline, correct, improve, or don’t affect. Therefore, PEMFs have the potential to positively affect an extremely broad range of physiological and biological actions. Any negative or non-reaction effects PEMFs have on these processes are usually self-limited and do not result in any significant problems. In general, when used appropriately PEMF therapy is extraordinarily safe.

The Top 10 Benefits of PEMF Therapy
As is documented in my books, Supercharge Your Health With PEMF Therapy and Power Tools For Health, research shows that PEMF treatments are an effective treatment for preventing, managing, and helping to reverse over 80 serious health conditions, including cancer. What follows are ten of the most powerful benefits that explain why.
Pain Relief:
Pain management is one of the most common applications for PEMF therapy. Whether the pain is acute or chronic, inflammatory or vascular, musculoskeletal, or in the nervous system, PEMFs help address both pain perception (pain blocking) and the cause of the pain itself (pain reduction). I have fairly often seen people get miraculous, sudden, and complete relief of pain after only one treatment of even low intensity PEMFs.
Pain mechanisms are extremely complex, but on the most basic level they involve a signal being transferred to a receptor and causing a change in cellular behavior. My goal is always to help my patients prevent cellular injury in the first place, which is why, in many cases, daily treatment with PEMF therapy is essential. In cases of acute injuries, or for those people who have found PEMF therapy after an injury or disease
62 Super Charge Your Health To Protect Yourself Against Cancer
condition has already taken hold of the body, the goal changes from prevention to injury resolution and pain management.
The body normally does its own pain blocking in response to pain signals through an increase in levels of serotonin, dopamine, endorphin, and encephalins. along with a decrease in cortisol and noradrenaline.
The primary mechanisms for pain in response to cell injury are edema, apoptosis or necrosis, diminished circulation, decreased cellular metabolism, and impaired cellular repair processes. PEMF therapy addresses each of these mechanisms in very basic and measurable ways.
In addition, PEMF therapy helps to manage and relieve pain because of its positive effects on adenosine, a molecule that plays a vital role in controlling inflammation that triggers pain. Adenosine is a building block for RNA/DNA. It is also a part of the energy molecule ATP, and helps regulates the function of every cell, tissue, and organ in the body. Because of this regulatory role, adenosine has been called the “guardian angel” protecting against human disease.
Through various metabolic processes, adenosine is released by the breakdown of ATP to create energy and then is re-used to create more ATP in a perpetual cellular cycle. The concentrations of adenosine are naturally at low levels in body fluids between the cells of unstressed tissues. These concentrations increase rapidly in response to cell injury-causing stress conditions such as low oxygen (hypoxia), lack of blood supply (ischemia), inflammation, or trauma, all of which are factors involved in the initiation and progression of cancer. When adenosine production drops off or is low, inflammation persists and produces chronic inflammation.
Adenosine acts through four subtypes of adenosine receptors: A1, A2A, A2B and A3. PEMFs appear to primarily influence the A2A and A3 receptors, stimulating their activation, increasing their functionality, and augmenting chemical agents that also stimulate them. Stimulation of A2A and A3 receptors by PEMFs in cells throughout the body reduces inflammation by lowering many pro-inflammatory tissue cytokines, including tumor necrosis factor-α (TNF-α), interleukins (IL-1β, IL-6, and IL-8 in microglial cells;IL-6 and IL-8 in cartilage and bone cells; IL-8 and NF-kappa B in skin cells), and synovial fibroblasts.
Most research to date has been done on PEMF stimulation of A2A receptors, which has been shown to be especially helpful for chronic inflammation. That’s because the A2A receptor, under normal conditions, is naturally stimulated by acute inflammation-producing molecules to inhibit or control the inflammation. Most notably, PEMFs, by increasing adenosine receptors, enhance adenosine’s functional efficiency, resulting in a stronger physiological action than the use of pain relief drugs. A PEMF intensity of about 15 Gauss (1.5 mT) has been found to be optimal to affect the ade-
63 Super Charge Your Health To Protect Yourself Against Cancer
nosine receptors. The anti-inflammatory effect of adenosine enhanced by PEMF is less likely to have the side effects, desensitization, and receptor resistance than drugs designed to be used to act on adenosine receptors.
Healthy Heart Function:
Helping to maintain healthy heart function is another of PEMF therapy’s significant benefits.
Because the heart is an electrically dynamic organ, it is most susceptible to PEMFs. The heart muscle itself, because of its dynamic electrical activity, also creates its own internal PEMFs that have their own healthful effects on cardiac tissue. The heart contributes between five and ten percent of the total electromagnetic field brought about in the human body by externally applied electric and magnetic fields.
The reaction of the cardiovascular system to external PEMFs includes direct responses of many tissues including cardiac muscle, the autonomic nervous system, blood vessels, and reflex responses processed by the central nervous system among others. Studies have shown that the natural PEMFs of the heart become much larger when exposed to external PEMFs. Studies also show that PEMFs can affect the function of the centers of the autonomic nervous system that control heart rhythm. In addition, PEMFs dilate the heart’s large blood vessels, acting just like nitroglycerin, a drug used for angina chest pain.
The heart has its own “nervous” system, the conductive pathways of the heart. This system controls the natural rhythmic and coordinated beating of the heart. PEMFs help to make this system function better and decrease its sensitivity to the external, body wide autonomic nervous system.
Another reason why PEMF therapy can support heart function is because of its beneficial effects on the functional state of the body wide nervous and endocrine systems, as well as on heart tissue metabolism. PEMF stimulation activates the parasympathetic nervous system, the part of the autonomic nervous system responsible for the body’s rest and repair mechanisms. This activation, in turn, causes heart rate and blood pressure to decrease and the cardiovascular system to become less reactive to adrenaline and acetylcholine, while also reducing the stress hormones cortisol and aldosterone. This likely explains why it is so common for people to report significant relaxation and feelings of stress reduction following treatments with whole-body PEMF systems. Such stress relief is another important aid for cancer patients as they progress through cancer.
PEMFs have also been shown to improve blood pressure levels and microcirculation in people with ischemic heart disease and vascular diseases in their extremities, and to also improve both lipoproteins and cholesterol levels.
64 Super Charge Your Health To Protect Yourself Against Cancer
Improved Circulation and Blood Flow:
The majority of the body’s functions are handled by blood cells moving freely throughout the various systems such as the neurological, cardiovascular, nervous, digestive, and many others. These cells need to be able to travel unimpeded by blockages and other issues which cause restrictions in flow. This can only occur when blood vessels are healthy and wide enough to allow blood cells to easily circulate.
Abnormal or diminished production of nitric oxide, which occurs in cancer and various other disorders, can cause blood vessels to constrict, adversely affecting blood flow and other vascular functions. In a healthy cellular environment, blood vessels continually produce nitric oxide. The inner lining of the blood vessel (endothelium) produces and uses nitric oxide to signal the adjacent smooth muscles in the blood vessel wall to relax, causing blood vessels to widen. The subsequent increase in blood flow leads to an immediate decrease in both blood pressure and heart rate. Research shows that therapeutic PEMFs improve circulations, and enhance delivery of nutrients as they pass through the bloodstream, repairing molecules, stimulating growth factors, increasing oxygen, eliminating waste, and achieve many other actions that support healthy circulation.
Improved Sleep and Better and Fuller Sleep Cycles:
Studies show that nearly two-thirds of all adults experience some level of sleep deprivation. Of those two-thirds, nearly one-third of them experience chronic sleep deprivation. Poor sleep is also a common issue chronically affecting many cancer patients. PEMF therapy not only helps people fall asleep easily, but also to stay asleep.
Research studies show that PEMF treatments before going to sleep and while sleeping on a PEMF mat during bedtime enhances and balances circadian rhythms. Sleep disturbances can affect daytime functioning, psychologically and cognitively. PEMFs can also improve psychological and cognitive daytime function through better sleep.
I have found that presenting the brain with one PEMF frequency of three Hertz (Hz) throughout the night anchors the brain into delta levels and lower theta levels. Not only does this result in better and deeper delta, you also get longer periods of delta, and you also then begin to have a deeper theta level of sleep. What wakes people up during the night the most is the fact that when you’re aware of your dreaming you are in high levels of theta. When you anchor or tether more of the brain in delta throughout the entire night using PEMF people get a much longer night’s sleep.
Improved Mental Focus, Concentration and Cognitive Function:
PEMF therapy around 10 Hz promotes the alpha state in neurological function, which is when the mind is relaxed, at its most aware and its senses are the most heightened. The alpha state is one of the peak times for learning and retaining information.
65 Super Charge Your Health To Protect Yourself Against Cancer
Unfortunately, one of the many issues that go along with blood cells that are not properly charged is the inability to create and maintain this state.
PEMFs between 14 to 30 Hz can also increase the brain’s beta waves. By doing so, PEMFs improve the brain’s ability to process information analytically, problem solve, and multitask much more efficiently.
PEMF stimulation impacts psychological and cognitive function both directly and indirectly. Indirect benefits are especially significant when other symptoms are present. For example, if you’re experiencing chronic pain, you’re more likely to also experience some depression or anxiety. As PEMF therapy addresses your pain, it will also improve your psychological function. Another indirect benefit is from improved sleep, as mentioned above.
Direct benefits result from PEMFs’ actions on the brain and nervous system. Whether these actions are because of changes to the brainwave levels or actions on the brain cells themselves, either way, the effects are measurable. Through entrainment, PEMFs can quickly shift dominant brainwaves from beta to alpha or theta, and even down into delta (deep sleep).
Since different parts of the brain function at different frequencies, stimulation at a given frequency will either simulate or depress brainwave frequencies to match the simulation frequency. PEMF exposure in the alpha and beta rhythms will likely have a positive effect on long-term memory. Even a single session of theta frequency (5-8 Hz) stimulation to the brain affects numerous measures of cognitive function.
Even weak PEMFs appear to help cognitive function, including short and long-term memory, word finding, attention, and concentration, all of which can be impaired by chemotherapy and radiation treatments, as discussed in Chapter 5. Recollection seems to improve more dramatically with higher intensity stimulation. Studies show this to be true even in cases of people with mild to moderate Alzheimer’s disease. In fact, PEMFs alone were better than PEMFs and medications together
Other people that benefit from lower frequency (alpha, theta, delta) PEMFs include those with stress-induced anxiety, surgery patients, ADHD children with behavior problems (up to 70 percent benefit), and women suffering with premenstrual symptoms.
Improved Muscle Performance
When all of the positive and negative electromagnetic charges are working properly in healthy cells, muscle performance improves. This includes everything from mobility and flexibility to increased stamina and strength. This is critical as you age and lose this type of function and ability, or after injuries requiring rehabilitation. Cancer can also negatively affect muscle function, mobility, and strength. PEMF therapy applied regularly can help prevent such losses and keep your muscles strong and healthy.
66 Super Charge Your Health To Protect Yourself Against Cancer
Reduction Of Stress and Anxiety
PEMFs not only offer incredible benefits for physical well being, but also for stress, anxiety, and other mental/emotional issues. This is especially necessary for the fears and anxiety commonly experienced by cancer patients.
PEMFs change the stress responses in the body, resulting in a more efficient function of the nervous and endocrine systems. In addition, in 2011, the FDA approved high intensity transcranial PEMF therapy to treat severe depression.
PEMFs help with stress in three basic ways. First, they reduce the brain’s reaction to it. Second, they help the body eliminate the neurotransmitters and hormones produced by stressful fight-flight reactions. Third, they help defend the cells and tissues of the body from the physical changes induced by stress chemicals and hormones.
In addition, PEMF stimulation of the kidneys accelerates the excretion of stress hormones. The same thing happens with the hypothalamus in the brain, which has a central role in controlling the brain’s responses to stress. In many individuals, the brain is in a heightened state of expectancy for stress.
In people prone to anxiety, alpha brainwaves appear to be lacking. PEMF therapy has been shown to help entrain alpha brainwaves, thereby alleviating anxiety.
Stress clearly causes significant disruptions in normal brain rhythms. Research in Germany found that 10 Hz PEMF stabilized circadian rhythms. Circadian rhythms control the body’s hormone balance. Stress is a clear example of how circadian rhythms and brainwave frequency patterns can become disrupted. PEMF therapy at 7 or 10 Hz can be useful for reducing many of the physical effects of stress, circadian rhythm disruption, and tissue regeneration.
Enhanced Healing, Repair, and Recovery Processes
This is one of the most common uses of PEMFs, and also of importance to cancer patients. In addition to the fact that PEMF therapy can improve muscle strength and endurance, as noted above, energy production in the muscles themselves can increase by as much as 500 percent with regular treatment sessions.
By triggering the production of heat stress proteins (natural tissue protective proteins) before exercise, PEMF therapy assists in not only preventing the wear and tear and breakdown of cells, it also promotes accelerated restoration and recovery. For people struggling with chronic injuries or continual pain, it means finally having the relief they so desperately seek. For fitness enthusiasts and athletes, it means performing at a higher level with less recovery time.
One of the most important research findings is that PEMF signals appear to have therapeutic effects on damaged tissue, but do not seem to affect normal tissue. Un-
67 Super Charge Your Health To Protect Yourself Against Cancer
der normal conditions, PEMFs interfere only moderately with enzyme activity, but greatly enhance activity when enzymes function under less than optimal conditions due to tissue damage. When tissue is damaged and ion leakage results in altered ionic concentrations at cell sites, data show that PEMFs markedly increase the enzymes’ activity.
Reduction of Inflammation and Swelling
Chronic inflammation is a major cause of cancer, as well as many other serious, degenerative diseases. When the body’s repair and recovery process are not working properly, inflammation and its associated swelling are often the main culprits. It is very hard for the body to heal inflammation and reduce swelling when there are issues with blood flow, as well as with the health of the blood cells themselves. As discussed above, PEMFs can improve blood flow, and also improve of the health of blood cells, most notably red blood cells. Regular home therapy produces more consistent and enduring results.
Cellular Restoration
Every function in the body relies on its cell membranes and their electromagnetic charges. When these charges are out of balance, any or all of the issues mentioned above can occur. Cells working properly are able to do everything from processing nutrition better to carrying much needed chemicals to the various parts of the body. This one improvement alone, which PEMF therapy can and does provide, can lead to better oxygenation, better circulation, and more efficient productivity in every aspect. All of these improvements can substantially improve responses to cancer treatments.
Other Health Benefits of PEMFs
In addition to the above benefits, PEMFs support health in other significant ways, as well, including:
● Antibacterial, Antifungal, Antiviral, and Antiparasitic Benefits: Research has shown that PEMFs can help the body resist harmful bacteria, fungi, viruses, and parasites, which is of great importance to cancer patients because of how cancer can increases susceptibility to infectious agents, as can chemotherapy and radiation therapy. A wide range of PEMF frequencies and intensities has been studied in regard these harmful microorganisms.
● Anticoagulant Effects: PEMF therapy addresses many of the mechanisms that lead to increased blood viscosity (thickness) and clotting, including the reduction of platelet adhesiveness, reduction of fibrinogen and improvement of fibrinolysis, improving the pliability of red blood cells (allowing them to move through capillaries more easily), and increasing the saline content of the blood, decreasing viscosity. PEMF therapy reduces the stickiness of platelets, thus decreasing the risk of unhealthy clotting by an amount almost equivalent to taking aspirin. In addition, PEMF therapy does not have the risks associated with aspirin use, particularly
68 Super Charge Your Health To Protect Yourself Against Cancer
gastric bleeding. These anticoagulant effects appear to be universal to virtually all types of PEMFs.
● Anti-Edema Activity: Edema is swelling caused by excess fluid trapped in tissue, and is a frequent occurrence in cancer patients, including pulmonary edema. Tissues with edema are deprived of oxygen, nutrients, and circulation, making them an ideal environment for cancer cells to thrive within. PEMF therapy has a positive effect on swelling and edema by improving cellular metabolism through direct actions on the sodium-potassium pump in the cell membrane. Any kind of cell or tissue damage causes edema due to leakage of fluids from the cells and blood vessels. Improving circulation helps to remove this excess fluid and prevent further fluid accumulation. Anti-edema effects happen rapidly after starting the use of PEMFs.
In addition to improving blood circulation, PEMFs also have a positive effect on lymphatic vessels, stimulating lymph drainage and reducing production of lymph edema, and therefore simulating the immune system and correcting the edema.
● Autophagy: Autophagy is the natural, regulated process in the body that disassembles and eliminates unnecessary or dysfunctional cellular components, resulting in the orderly breakdown and recycling of these components. Autophagy may also be responsible for clearing out dysfunctional cells in the body that, when they accumulate and clog up tissues, can lead to the development of cancer.
There is not much research at this point on the effects of PEMFs on autophagy, given how new the science is, but some experimental studies provide support for its use in helping to maintain healthy cells.
To assess the impact of PEMFs on autophagy, one study looked at their effects on human neuroblastoma cells. Neuroblastoma cells are often used in research into Alzheimer’s disease (AD). In these cells, a specific PEMF induced a pro-survival autophagy process that was cell-protective by removing damaged proteins and cell organelles and removing beta-amyloid cells. The same PEMF had previously been found to improve resistance to induced cellular oxidative stress, which is damaging to cells. This study not only demonstrated the potential benefit for PEMFs in protecting against and possibly slowing the progression of AD, but also that it does this through the improvement of autophagy.
If PEMFs can improve autophagy at a basic level, as they did in these studies, then they are likely to help with cancer, as well as many of the conditions of aging and cell breakdown and injury.
69 Super Charge Your Health To Protect Yourself Against Cancer
● ATP and Mitochondria: Mitochondria are often called the powerhouses of the cell because they are the major generators of ATP. Mitochondria are tiny and the number inside a cell vary significantly from cell to cell, depending on the level of activity of the cells.
Mitochondria are constantly regenerating themselves using their own DNA. Mitochondria dysfunctions are now known to be primary factors associated with cancer. In fact, and increasing number of researchers and physicians now regard cancer to be far the result of mitochondrial dysfunction and due to genetic predispositions and disruptions.
PEMFs have been found to increase of the number and size of mitochondria that then promoted cellular and intracellular regeneration. In addition, PEMF therapy enhances the production of ATP, and therefore the body’s energy supply. Research has shown that PEMFs can induce between 100 to 600 percent more ATP production within a short time after stimulation. People using PEMFs frequently report significant increases in energy, most likely due to the significant increases in ATP production.
● Detoxification: Detoxification is what your body constantly does to neutralize, transform or get rid of unwanted materials or toxins, in order to maintain optimal health. It is one of your body’s most important functions. Cancer arises in part because of impairments to the body’s ability to effectively eliminate toxins that act like carcinogens. This impairment also severely hinders the body’s ability to fight and recover from cancer.
The bulk of the detoxification work is done by the liver and the intestinal tract. The kidneys, lungs, lymphatic system, and skin are all also involved in this complex detoxification process.
Because PEMFs improve inefficient or suboptimal liver and kidney function, they clearly help the body to detoxify. PEMFs also improve cellular detoxification because they improve the ability of cell membranes to open and rebalance themselves. In addition, by optimizing the function of all cells in the body, PEMFs further enhance detoxification by improving blood and lymph circulation, decreasing inflammation, rebalancing cell energy, helping to restore cell function, improving skin respiration, and repairing damaged cells of tissues involved in detoxification.
● Growth Factors And Nitric Oxide: Growth factors are substances (primarily hormones and proteins) that regulate and stimulate various cellular processes. They are essential for the regeneration and healing of tissues after injury, including damage caused by cancer and other diseases. Typically, growth factors act as signaling molecules between cells, binding to receptors embedded in the cell membrane of their target cells. PEMF stimulation
70 Super Charge Your Health To Protect Yourself Against Cancer
fine-tunes growth factors in many ways, but one of the best-understood is by increasing nitric oxide production.
Calmodulin (CaM) is a messenger protein in the cell that binds calcium. It mediates various biologic processes. Once CaM binds to calcium (a process PEMF therapy increases by supporting the necessary electrical charge activity), the resulting cascade catalyzes the release of nitric oxide, and therefore improves growth factors.
A NASA PEMF neural stem cell stimulation study using a 10 Hz square wave PEMF signal found that this PEMF application increased production of over 160 different growth factors that may facilitate nerve regeneration. Evidence to date also shows that PEMFs can significantly increase growth factors throughout the body, whether in the brain, nerves, bones, etc., all contributing to tissue regeneration and healing.
● Healing and Regeneration
Of Tissue:
Basic regeneration is part of normal cell function. Cells are always dividing, growing, and eating up their older or injured neighbors (see Autophagy above). This does not require any outside stimulation, although it can enhance and ease the process. Injury-induced regeneration and wound healing, including the healing of injuries and wounds caused by biopsies and surgery to remove tumors, require significantly more energy and, therefore, more time. Regeneration and wound healing also require a great deal of cellular communication and adaptation to take place, along with the stimulation and production of stem cells and growth factors.
When it comes to healing and tissue regeneration, addressing and resolving the cause of the problem is the goal all physicians aspire to achieve. PEMFs go a long way in helping us to do that, whereas typical conventional treatments frequently cannot do not. In fact, physicians rely almost solely on the body’s natural capacity to heal, regardless of the age or health status of the person. This is basically like rolling the dice, hoping for the best to happen naturally. PEMFs dramatically improve on leaving healing to chance. The healing process can happen faster through the use of PEMFs, and in some cases in about half the time that it would normally take.
PEMF therapy has been used to heal bone, ligaments, and tissues in almost every imaginable situation. Therapeutic magnetic fields accelerate healing through their effects on reduced inflammation, improved circulation, streamlined cellular communication, and growth factors. Magnetic stimulation increases stem cell production, differentiation and maturation, and growth factors.
As mentioned above, PEMF signals have therapeutic effects on damaged tissue but do not seem to affect healthy tissue. This activity of PEMFs primarily on abnormal tissue or functions is another aspect of the appeal of PEMFs for healing.
71 Super Charge Your Health To Protect Yourself Against Cancer
● Immune Function: The body’s immune response to disease, especially cancer, serious infections, and other diseases, requires nitric oxide for a variety of reasons. PEMFs assist with this on a basic level by increasing nitric oxide production. This helps lay the foundation for a healthy immune system and is part of why PEMF therapy is so important for prevention.
PEMFs also positively affect cancer-fighting white blood cells (WBCs), which play important roles in the body’s immune response. In addition, PEMF stimulation can assist with “rolling adhesion.” Part of the body’s immune response involves a natural inflammatory response characterized by vascular permeability, which, in turn, allows white blood cells called leukocytes to move through tissues and collect at the site of injury or disease. During rolling adhesion, these WBCs bind to the inner wall of the vessel and slowly roll along its surface, inducing chemical changes in the surface of the vessel. These changes result in the WBCs migrating through the vessel wall and into the target tissue. The basic actions PEMFs have on transmembrane potentials and ion flow improve this process by increasing the adhesion properties of WBCs, and by improving the overall permeability of the vessel walls themselves.
Free radicals are known to interfere with cellular communication and mitochondrial function, damaging the immune system. Free radical damage is another major cause of cancer. PEMFs support cellular metabolism, making the body better able to adapt to the presence of free radicals.
Cytokines are chemical messengers in the body that are part of the inflammatory process. Wherever there is significant inflammation, whether it’s from cancer, trauma, infections, toxins, autoimmune disease, or other conditions, cytokine levels are elevated. PEMFs have been found to reduce cytokine levels in areas of inflammation.
● Oxygenation: Low oxygen levels (hypoxia) in the body cause cell injury, with the degrees and lengths of time tissues are oxygen-deficient determining the degree of damage. The vast majority of cellular functions depend on an adequate supply of oxygen. Hypoxia, as we have discussed, is a major cause of cancer, and creates an optimal microenvironment in the body within which cancer cells and tumors thrive.
PEMFs significantly increase oxygen levels in tissues by improving circulation, helping the body transfer oxygen from the air into the lungs and blood, affecting the ability of hemoglobin to carry oxygen, and helping the oxygen in hemoglobin to transfer into the tissues. One study focused on the effect magnetic fields have on the gas-transport function of blood during oxygen deprivation. The study’s researchers found that magnetic field therapy changed the shape of the hemoglobin molecule from a form that was less reactive to oxygen to a form that was more reactive, positively influencing the gas-transport function.
72 Super Charge Your Health To Protect Yourself Against Cancer
In bronchitis, emphysema, or pulmonary edema (a potential side effect of cancer), there is poor oxygen exchange from the air into the air sacs in the lung and then into the blood. PEMFs reduce the inflammation in these conditions allowing for better oxygen exchange and improving the saturation of oxygen in the blood.
One of the earlier demonstrations of the benefit of PEMFs in improving oxygenation was done in Germany in the early 1990s using a large PEMF plate. The researchers found that PEMF effects could be increased during periods of high muscle activity, after drinking alcohol, while sleeping, or after inhaling carbon dioxide (CO2). Hyperventilation and large meals would reduce the magnitude of the effects. In their studies, they found that blood volume increased, oxygen levels increased, and pH became more alkaline.
Ozone therapy is used to increase the delivery of oxygen into the body. There are other benefits from ozone therapy, as well, including as a potential treatment for cancer. Since both ozone therapy and PEMFs increase delivery of oxygen into the body, it makes sense to combine these therapies. There is research to show that PEMF therapy combined with ozone therapy produces better results than either one alone.
● Red Blood Cells: Red blood cells (RBCs) are the primary transporters of oxygen to tissues. They make up 70 percent of all the cells in the body. The sheer number of red blood cells we carry and produce is astounding: upwards of two million per second. Through all the basic mechanisms it affects, PEMF therapy help facilitate the formation, function, and reabsorption of RBCs.
The majority of oxygen transfer happens as red blood cells travel through the microcirculatory system, which is made up primarily of capillaries. Capillaries are so incredibly small that red blood cells often must contort themselves, almost folding in half, to squeeze their way through. A phenomenon known as the “rouleaux effect” makes this process difficult or impossible.
A rouleaux formation is a stack of red blood cells stuck together. It closely resembles a stack of coins and is therefore commonly referred to as “coining.” Capillaries can only accept a single RBC at a time, so healthy circulation requires that coining or rouleaux be prevented from happening as much as possible.
Because PEMF therapy facilitates a balanced cellular membrane charge, it has a direct effect on RBC activity. Properly charged red blood cells will repel from one another. There are many examples of this on the internet shown by practitioners using dark field microscope samples.
Aside from preventing rouleaux, PEMFs’ separation of RBCs allows for a greater available surface area for oxygen and nutrients to be absorbed and exchanged. PEMFs can enhance the release of oxygen from hemoglobin, with only ten to thirty minutes of exposure increasing the rate of oxygen release for several minutes to several hours.
73 Super Charge Your Health To Protect Yourself Against Cancer
For a much more in-depth discussion of the full range of the benefits of PEMF therapy and its mechanisms of action, I refer you to my book, Supercharge Your Health With PEMF Therapy, and my website, DrPawluk.com. More information can also be found in this eBook’s Appendix.
To summarize the health and wellness benefits that PEMF therapy that I shared with you in this chapter, the main thing to I want to emphasize is that enhancing even one of the above issues by using PEMF therapy can have a tremendous impact on the rest of your life. With so many possible benefits of using PEMF therapy, there is little reason not to at least consider it. The difference it can make for you could be life-changing. Because of the many benefits it provides, I am confident that appropriate PEMF therapy will supplant many traditional therapies and health maintenance approaches in the next few years.
In the next chapter, we will take a closer look at how PEMF therapy can help to prevent cancer, and aid in its recovery.
74 Super Charge Your Health To Protect Yourself Against Cancer
How and Why PEMF Therapy Aids Cancer Prevention and Recovery
I have never been a proponent of saying that PEMFs alone should be used to treat cancer. The most humbling thing I can say about the treatment of cancer is that there are no perfect solutions. I would also say that cures are rare.
Cancer in whatever form is a chronic illness. Even if you have been declared “cured” by a doctor, with “cure” usually defined as surviving beyond five years after diagnosis, there is almost always a need for lifelong vigilance and surveillance to be sure the cancer has not come back. Yes, you can effectively be in a state of long-term remission after an original diagnosis. Unfortunately, very many people do not live beyond five years or for that matter beyond 10 or even 15 years after their diagnosis. An example is breast cancer, which could be considered cured today, yet might show up 15 to 20 years later in the bones, with no indication that it was brewing there over the decades. Medicine today continues to search for answers in the war on cancer in order to find a cure using the most effective cancer treatment available.
To me, the real issue is not necessarily to find a cure, even though that is certainly a desirable goal, but rather to find ways of making our current therapies more effective in order to produce longer-lasting results with a better quality of life. So often, current medical therapies for cancer are brutal, making people very ill, yet too often producing poor results nonetheless, including distressing and demoralizing side effects like pain, nausea, vomiting, hair loss, bad fatigue, and other issues. Yes in many cases the therapies do produce somewhat long-lasting benefits, but this is often uncertain and unpredictable.
Accordingly, we may well ask if PEMF is a useful addition to the conventional arsenal of cancer therapies, both as an adjunct in the short term, and for preventive care in the long term.
How PEMF Therapy Enhances Existing Cancer Treatments
PEMF therapies may be one approach to enhancing the value of existing treatments for cancer. As you learned in Chapter 6, PEMFs provide many health benefits, including benefits related to improving healthy oxygen circulation, promoting the growth of healthy cells, and improving the quality of breathing, a benefit of particular benefit to individuals with lung cancer.
75 Super Charge Your Health To Protect Yourself Against Cancer CHAPTER 7
PEMF therapy may also help with pain. Cancer often brings with it one or more of four different types of pain.
First, there’s bone pain, which is generally caused by a tumor pressing on the bone. Patients experience this as extreme tenderness or unpleasant dull sensations that persist no matter how the individual positions his or her body.
Second, there’s nerve pain. This is a very common problem for cancer sufferers who undergo chemotherapy, as chemotherapy often produces neuropathy. When the treatment itself results in nerve damage, patients often experience tingling, numbness, or a burning sensation in their limbs.
Third, there’s soft tissue pain. This happens when cancer damages muscles, fascia, tendons, and ligaments. Often this particular source of pain is hard to identify as it is likely to accompany other forms of pain.
Finally, there’s phantom pain. In extreme cases, cancer treatments can require amputation. Phantom pain occurs when a patient feels as though he or she is experiencing pain in the limb that was amputated.
Patients are sometimes advised to take medication for these forms of pain. Pain relievers like aspirin and ibuprofen sometimes prove useful for relatively mild sensations. Codeine is sometimes used to address moderate pain, and morphine and other powerful opioids can be used to tackle overwhelming pain. There’s a chance, however, that the medication will prove ineffective, decline in effectiveness over time, cause side effects, or even, in the case of opioids, prove addictive or lead to lethal overdose.
PEMF therapy may offer a viable alternative to such medications. (Borea PA, Gessi S, Merighi S, Varani K. Adenosine as a Multi-Signalling Guardian Angel in Human Diseases: When, Where and How Does it Exert its Protective Effects? Trends Pharmacol Sci. 2016 Jun;37(6):419-434; Fernandez MI, Watson PJ, Rowbotham DJ. Effect of pulsed magnetic field therapy on pain reported by human volunteers in a laboratory model of acute pain. Br J Anaesth. 2007 Aug;99(2):266-9.) There is reason to believe that, just as it may ease other forms of pain, PEMF therapy may relieve pain resulting from cancer, as well.
76 Super Charge Your Health To Protect Yourself Against Cancer
Research Into PEMF Therapy As A Potential Cancer Treatment
Admittedly, the research available to support the use of PEMFs in the setting of cancer is still in its early stages. So, the question is what is the harm of adding PEMF to a cancer therapy plan? The fear of harm comes largely from uncertainty.
That said, conventional medical therapies still have a huge level of uncertainty as well, but they are sanctioned by society and the medical community. That makes them acceptable, even though they are very often ineffective. Because the benefits of PEMFs are not as widely known in the Western medical community, any risks are considered to be “unacceptable”.
Most doctors are completely ignorant about what PEMFs do biologically and physically. And, unfortunately, they are not willing to explore these approaches even in cases like cancer where complementary therapies are a vital part of treatment. Likewise, most doctors are not even willing to approach and consider nutritional aspects of managing cancer. As a result, patients suffering from cancer are largely left on their own when it comes to discovering how PEMF therapy might help them.
Perhaps we can shed a little bit of light on this issue by looking at the research. Various studies exist on PEMF therapy’s potential usefulness in addressing various forms of cancer, including breast cancer, ovarian cancer, prostate cancer, and lung cancer, which I discuss in more detail in chapters 8 and 9, as well as in the Appendix. For now, let’s focus on two recent studies. One study used human subjects and one used animals.
Even conventional medical oncology sometimes resorts to relying on animal studies in the absence of any available human studies. Since you can’t always conclude that the results from animal studies can be applied to humans, drawing conclusions from animal studies needs to be done with some caution. However, I’m of the belief that individuals are responsible for their own health and will ultimately make their own best personal decisions. If the information from animal studies figures into those decisions, that’s all right.
In the animal study, researchers examined the use of pulsed electric fields in breast cancer in mice. Very short pulse length pulsed electric fields, which didn’t create heating to destroy tissue, were used. The frequency was 4 hertz. MRI was used to assess the physical changes in the tumors. Two weeks after treatment, the growth of treated tumors had been inhibited by 79 percent. The pulsed electric fields caused apoptosis in the tumor cells, and various tumor growth factors, including the development of new tumor blood vessels, were strongly suppressed. As a control, normal skin was treated the same way as the tumors and showed no permanent changes.
77 Super Charge Your Health To Protect Yourself Against Cancer
The study’s outcomes shows that tumors react differently to PEMFs, in a positive fashion, than normal tissue does. The results suggest short pulse electromagnetic fields may be able to inhibit human breast cancer development and suppress tumor blood vessel growth and may therefore serve as a novel therapy for breast cancer. (Wu S, Wang Y, Guo J, Chen Q, Zhang J, Fang J. Nanosecond pulsed electric fields as a novel drug free therapy for breast cancer: an in vivo study. Cancer Lett. 2014 Feb 28;343(2):268-74.)
In a human study done in China, magnetic fields were studied in the treatment of patients with advanced cancers of various kinds. Unfortunately, the entire study is a written in Chinese, so it is not available in complete form to those not fluent in that language. In this study, 137 patients with advanced malignant tumors were exposed to a magnetic field of approximately 7 Hz, at 4000 Gauss, for two hours a day for between 30 to 50 days. The clinical benefit was 60 percent. 28 patients had a complete response and 54 had a partial response. The median overall survival was 12 months. The one-year, two-year, and three-year survival rates were 47 percent 11.8 percent, and 3.4 percent, respectively. Complications were minimal. In addition, there were no treatment-related deaths, which is also significant.
The conclusion of the study is that the PEMF therapy seems to have improved the quality of life of these individuals and in many cases probably prolonged their survival. It is not known if treatment extended beyond the 30 to 50 days used in this study would have produced even better results. Nonetheless, these results are very impressive despite the limited length of time the treatment was used. (Han JQ, Liu Q, Sun CT, Yao J, Zhao B, Wang H. [Efficacy and safety of low-frequency rotary magnetic fields in the treatment of patients with advanced malignant tumors]. Zhonghua Zhong Liu Za Zhi. 2013 Jun;35(6):468-71.) (Article in Chinese.)
These two studies show us that PEMF therapy has significant potential in helping patients with cancer, both advanced or otherwise. Obviously, a great deal more research needs to be done to discover the best signals and approaches.
Unfortunately, the survival rates in individuals with advanced cancers normally tend to be very poor. If life can be extended comfortably to even a limited degree, this could be a very important benefit.
While we don’t have commercially available PEMF devices that are exactly the same as those used in the above human study, we do have available PEMF systems that are of a comparable intensity with a similar frequency. However, these devices are often very expensive and need to be used for extended periods of time, typically up to two hours per day, on a daily basis for months, if not the rest of the person’s life. Since often these treatments are applied in doctors’ offices, the treatment durations there are probably too short.
78 Super Charge Your Health To Protect Yourself Against Cancer
Even if available PEMFs are not exactly comparable to those used in this study, the available devices have the potential to produce beneficial results. In the end, there is no harm in trying, based on what this human study shows. In my clinical experience, patients using PEMFs on an ongoing, long-term basis, in the home setting, with or without conventional therapies, do better and are much more comfortable.
Still, it remains for patients to determine whether using PEMF therapy along with other conventional approaches is something they might want to consider. As a physician, I can’t tell you whether this is your best option. But I feel comfortable saying, knowing what I know about PEMFs and their benefits, that PEMFs can be a very important addition to whatever approach to cancer treatment an individual may choose.
At this point, suffice it to say, nobody has a perfect solution, but in summary, we can say the following:
● PEMF therapy is safe to use. Neither the available research nor clinical experience indicates that low-intensity PEMF produces any side effects. Right now, across the country, people are using the pulsed magnetic fields of PEMF mats to provide therapy for a variety of ailments they experience, and even to help their children and pets.
● PEMF is non-invasive. There are no needles, IVs, or any other form of invasive therapy involved in PEMF. Generally speaking, you simply lie on a PEMF mat to experience the low-intensity pulsed magnetic fields and can do this in the comfort of your own home.
● PEMF brings no risk of toxicity. I alluded above to the harsh side effects that often accompany traditional chemotherapy (pain, nausea, hair loss, etc.) Patients experience these side effects because, while chemotherapy attacks cancer cells as it’s supposed to, it kills healthy cells as well. This can depress the immune system and leave the body more vulnerable to infectious illness.
In contrast, PEMF therapy produces no such harmful effects. Instead, there’s evidence to suggest that PEMF may actually oxygenate the blood, enhance the production and function of healthy red blood cells, and facilitate the repair of damaged red blood cells, thus potentially offsetting some of the damaging side effects of chemotherapy.
● PEMF combines readily with other types of cancer therapy. PEMF can be added to most if not all cancer therapy plans. Given that PEMF is safe, non-invasive, and non-toxic, there’s little no risk of an unfortunate interaction with any other therapy or treatment the patient is receiving.
In the next chapter, I discuss additional benefits that PEMF therapy can provide to cancer patients, including supporting the effectiveness of conventional cancer treatments, as well as recommended PEMF treatment protocols.
79 Super Charge Your Health To Protect Yourself Against Cancer
PEMF Therapy As An Aid To Conventional Cancer Care
In this chapter, I discuss how PEMF therapy might be used as an aid for cancer patients, and provide recommendations for its use for specific types of cancer, and in terms of the intensity of the PEMFs, the applicators that are best used, and recommended treatment times.
As I discussed previously in this eBook, an optimum diet with appropriate nutritional supplementation is essential for achieving the best results with PEMF therapy, as well as all other therapies, including conventional cancer treatments. I always emphasize the need for good nutrition and appropriate supplements in the setting of cancer. There is enough scientific evidence to emphasize this need.
It’s difficult to recommend specific diets and supplements, however, because they have to be individualized. I recommend consulting with a professional skilled in diet and nutrition to receive guidance on the supplements that should be used. There are many practitioners in this area who specialize in helping with cancer. Unfortunately, it is rare that oncologists would provide this guidance.
Developing PEMF treatment recommendations for cancer is complicated by the fact that there are many types of cancers, potentially in all areas of the body, and the conventional medical system treatments are many and varied, as well. In addition, cancer can be local, regional, and systemic. There is the primary cancer and metastatic cancer, with variable degrees and locations of metastatic activity. There are different degrees of severity, and aggressiveness, complicated by the underlying health status and age of the individual. Some people even have multiple cancers.
Cancers occur in many ways, with many different body systems involved. Cancers also have highly variable degrees of response to various therapies. Different tissues have different response rates to PEMFs. So, ultimately, PEMF treatment recommendations have to be highly individualized. A major goal of PEMF therapy is to help with the primary cancer as well as working to prevent spread or metastases.
The PEMF treatment recommendations below are highly generalized and only suggestive at best. While most people who look at PEMF therapy as an adjunctive or alternative approach for the specific cancer in the specific location, our goal should be not only focused on the short-term but also the long-term needs. The reality is that people often look for PEMF therapy after they have gone through multiple rounds of conventional approaches and have moved into a state of dire need. This limits the potential value of PEMF therapy.
80 Super Charge Your Health To Protect Yourself Against Cancer CHAPTER 8
There are also people with cancer who look to alternative approaches as a priority and avoid conventional therapies. Neither of these positions can be disputed. It’s always a matter of personal choice. No therapeutic approach is guaranteed to be completely successful, as success depends on the definition and goals of the individual. Most, but not all, of the time my experience has been that PEMF therapy provides some amount of value to people who have chosen this therapy as part of their healing journey. Sometimes it provides a great deal of value. Tailoring the right PEMF system to the individual’s situation and clearly defining expectations is very important to achieve good results.
Intensity of the PEMF
Most of the time the PEMFs will need to be medium or high intensity, applied either locally, regionally, or on the whole body. A high intensity whole body “magnetic sandwich” will normally achieve the best results most efficiently, both short-term and long-term. Local, superficial, and deeper, cancers can be managed well with local medium to higher intensity PEMF therapies. These would be most helpful for short-term needs, and may be all that is necessary for some cancers depending on the nature of the cancer. Primary cancers involving a larger organ, such as a lung, liver, bowel or bladder, can be considered regional in their activity and will typically need a higher intensity magnetic field, unless the cancer is very superficial and close to the applied magnetic field.
Applicators
Depending on the PEMF device that is used, the applicators available will determine the type of magnetic field it will produce. For local cancers, the recommended magnetic field applicator intensity should be able to produce no less than 500 gauss, as long as the cancer at its farthest distance from the applicator is less than two inches. Usually, regional cancers involving a larger area are deeper in the body.
Even though a cancer may appear to be less than an inch in diameter on imaging studies, that does not mean that its “sphere of activity” is less than an inch. It is almost always better to think deeper and wider than what the imaging shows. For regional cancers, the minimum magnetic field for a wider applicator would likely need to be between 4000-7000 Gauss. High intensity whole body, “magnetic sandwich” systems essentially remove all the guesswork and can be used for most aspects of cancer, including metastatic spread and long-term whole body needs.
81 Super Charge Your Health To Protect Yourself Against Cancer
Treatment Time
Always use the “low and slow” approach. The minimum treatment time should be no less than 30 minutes twice a day, to the primary cancer site. For multiple areas needing treatment, each significant area may need 30 minutes at a time. Using whole body “magnetic sandwich” PEMF allows for multiple areas to be treated simultaneously for 30 minutes twice a day. However, even with these whole body treatments, local or regional areas may need additional stimulation. Combined treatments may need to be done for several hours a day. How many times a day to repeat the treatment will depend on the cancer in the person. The minimum should be twice a day. In some cases, especially with cancer pain, the treatments may need to be many times a day for optimal results.
Cancer Bone/Metastases
There are primary bone cancers and secondary bone cancers. Primary bone cancers include multiple myeloma (the most common), osteosarcoma, chondrosarcoma, and Ewing’s sarcoma. Secondary bone cancers are those that are metastasized from primary cancers in other areas of the body. In both situations, the most common symptom is pain as a result of destruction of the bone and the nerves in the affected area. Fractures happen more easily in the affected bones and may involve collapse of the vertebrae.
The goal of PEMF therapy is to not only treat the underlying involved bone area or areas but also to help the rest of the body deal with the cancer. The earlier in the process that PEMF is started when cancer invades bone, the better and faster the results will be. Most of the time medical treatments may involve pain medications, radiation and medication to stimulate bone growth. PEMF therapy works well alongside other treatments. My experience over the years has shown that PEMFs can make a significant reduction in bone pain. PEMF therapy has been FDA approved for decades for the treatment of non-healing fractures, which is what bone metastases really are. Therefore, PEMF therapy may not only help with the underlying cancer bone pain, but also help to stimulate new bone formation and reduce progressive destruction of the bone.
Intensity of the PEMF: Medium to high intensity PEMFs are needed for specific local application at the primary cancer or metastatic sites. The lower the intensity of the magnetic field the more treatment time is needed. I usually recommend medium to high intensity fields, depending on where the cancer is, with higher intensity fields being preferred at an intensity of at least 4000 Gauss.
Applicators: The goal of therapy is not only to target the area of the bone with the cancer but also to help the whole body. When the whole body is treated, the body is healthier in general and has more physical healing and immune resources available
82 Super Charge Your Health To Protect Yourself Against Cancer
to target the sites of the cancer itself, and will not need as much for any of its other needs. A high intensity whole body PEMF system is recommended, preferably a whole body “magnetic sandwich,” dual applicator system. The dual applicator system provides whole body treatment for general health as well as an applicator available for the local cancer site. This type of dual system also makes treatment times more efficient, so that less treatment time would be necessary, as when individual applicators are used.
Treatment Time: 60 minutes two to three times a day, especially at the beginning, using a “low and slow” approach. Once the pain is controlled, treatment time may be able to be reduced. I recommend a minimum of 30 minutes twice a day for ongoing treatments. Repeat evaluations, including imaging studies and blood markers, and the status of symptoms and function, following the initiation of PEMF therapy will help to guide how to adjust the protocol. Treatment would be lifelong.
Suggested Supplements: New bone can’t be built without adequate nutrients to support bone development. At a minimum, these would include vitamin D3 5000 IU per day, a general bone building formula, DHEA 25 mg per day, vitamin K2, and curcumin 3000 mg/day. For other targeted supplements for bone cancer, I recommend consulting with a health practitioner who specializes in the use of supplements for cancer.
Cancer, Brain Radiation Therapy
Brain radiation therapy is most commonly used for metastatic brain cancers and also for acoustic neuromas and trigeminal neuralgia. But the radiation used to destroy cancer cells can also hurt normal cells in the area radiated. Side effects vary from person to person, depending on how much of the brain is being radiated, and are caused by the cumulative effect of radiation on the cells. This means they develop over time and most patients do not experience any side effects until a few weeks into their treatment. Side effects may be unpleasant and perhaps temporary, disappearing bit by bit after therapy is complete. Acute (short term) side effects include some of the most common side effects of radiation therapy for brain tumors:
● Fatigue is very common with radiation treatment and tends to begin a few weeks into therapy. Fatigue typically resolves slowly over the weeks and months following treatment.
● Hair loss may occur where you received radiation. Hair typically starts to regrow a month or so after treatment. However, your hair might not grow back exactly as it was before treatment and for some, the hair loss becomes permanent.
● Muffled hearing during treatment. This typically resolves in 2-4 weeks after finishing treatment.
● Skin irritation in the treatment area. It may include being red, irritated, dry, or sensitive, looking like a sunburn.
83 Super Charge Your Health To Protect Yourself Against Cancer
● Short-term memory loss and difficulty thinking can occur, especially with whole-brain radiation, but may also happen with local radiation depending on the area of the brain being treated.
● Brain tissue swelling can develop during treatment, resulting in a headache or pressure feeling. If this happens medications may be needed to decrease swelling.
● Side effects of radiosurgery are usually related to sending high doses of radiation to particular areas of the skull. For instance, if you are treated for an acoustic neuroma (a tumor involving the nerve that controls hearing), you might lose some hearing. Treatment for trigeminal neuralgia can lead to tingling or numbness of the face.
These side effects tend to occur during treatment, and can last up until a few months after treatment. Long-term effects can happen months to many years after cancer treatment and the risks vary depending on the areas included in the field of radiation and the radiation techniques used.
Long-term side effects after a few months following treatment, even up to years in some cases, include:
● Low risk of a second cancer in or near the radiation field from exposure of healthy tissue to radiation.
● Radiation necrosis of the tissue at the site of the tumor. Surgery may be needed to remove the necrotic tissue.
● Damage to healthy brain tissue can cause headaches, seizures, or even death.
● Harm to the pituitary gland and other areas of the brain which can affect hormone levels in the body, including thyroid and sex hormones, future fertility issues for women and cause sexuality concerns for men.
It may not be possible to use PEMF therapy during the course of radiation treatments. PEMFs may be used to treat the brain and head prior to radiation if there is adequate time. The intent is to try to get the tissues around the head and the brain as healthy as possible, even to the extent of reducing swelling around the tumor, prior to the radiation. There is a risk that magnetic fields may protect the tissues being radiated from the effects of radiation. The goal of radiation is to eliminate or significantly reduce the tumor. There is no point doing radiation if this cannot be achieved due to protection provided by the PEMF therapy.
It may be best to wait one or two weeks following radiation therapy before PEMF therapy is started. PEMF therapy can be done to the whole head or, in the case of very focused radiation therapy, to the area of the radiation field. On the other hand, because radiation cannot be completely isolated and laser focused, whole head stimulation of with PEMFs may be very reasonable. The goal of PEMF therapy is to reduce the amount of collateral inflammation in the head and brain caused by the radiation. There is no significant research to guide what the likely benefits would be in this spe-
84 Super Charge Your Health To Protect Yourself Against Cancer
cific setting. We are extrapolating from the general knowledge about what PEMFs would do with all tissues, including the brain.
Since PEMFs increase ATP in tissues, they may help significantly with brain fog, fatigue, memory, swelling, circulation, hair loss. and hearing issues. If there were seizures before the radiation started, PEMFs may help to decrease inflammation related to the seizures, since radiation may not eliminate seizures entirely. By improving the health of the brain in general, it’s possible that recurrences of cancer may also decrease. There is no guarantee with radiation therapy that it would reduce or eliminate the tumor completely, in which case it could potentially regrow. Adding PEMF therapy after radiation may decrease this risk of regrowth.
Intensity of the PEMF: Since whole brain/head PEMF therapy will be needed, and one of the goals of the therapies to reduce inflammation, the PEMF magnetic field needs to penetrate the entire head with at least 15 Gauss per the intensities in Appendix A. The average human head measures six to seven inches in width and eight to nine inches in length. This means that a PEMF intensity of about 7000 Gauss is needed or a minimum of 4000 Gauss. If a 4000 Gauss magnetic field is used, treatment would need to be done to the front and the back of the head. Treatment should follow the “low and slow” approach, meaning start slowly and use a low intensity. Generally, PEMFs can be used with other medications as needed. If anti-seizure medications are being used, it’s important to watch for side effects; the dose of these medications may need to be reduced. This may be true for other medications, as well.
Applicators: The best applicators will likely be a butterfly type coil or a loop coil placed on the top of the head. In the case of the butterfly coil, one loop (wing) of the butterfly coil would be on each side of the head, with the center of the butterfly at the top of the head. The loop coil would also be placed at the top of the head, like a halo. If the loop coil placed on top of the head is too large, one end of it can be squeezed together to make it a better fit. A paddle applicator is not as helpful, although it could be tried at the side of the head. This would require the paddle to be placed on each side of the head for a balanced treatment. It’s also possible with a “magnetic sandwich” to use two applicators at the same time on each side of the head. Since many of these brain cancers are spread from other parts of the body, making this a stage IV cancer, high intensity whole body PEMF is recommended separately, followed by a session with a lower whole body pad combined with a loop applicator applied to the head.
Treatment Time: Using the “low and slow” approach is very important for this type of treatment. Both time and intensity need to be gradually ramped up based on the body’s ability to tolerate the treatments. The goal would be to reach a minimum of 30 minutes twice a day, depending on symptoms, ability to tolerate the PEMF treatments, and other practical health and function constraints. PEMF therapy may like-
85 Super Charge Your Health To Protect Yourself Against Cancer
ly need to be continued indefinitely to get as much recovery from the radiation damage as possible.
PLEASE NOTE. Radiation oncologists frequently advise against nutritional supplements while ongoing radiation therapy. Consult with your radiation oncologist about the use of supplements during radiation. Experts believe that there is no harm in doing supplements after radiation is completed.
Cancer, Breast
PEMF therapy for breast cancer can be considered for prevention, during treatments, following treatments, and long-term after care.
Relative to prevention, inflammation in the breast over long periods of time is a highly likely stimulant to the development of breast cancer, although not necessarily in all cases. A strong family history of breast cancer, positive BRCA genes, significant chronic fibrocystic disease of the breasts, trauma or other significant insults to the breasts, breast implants, and significant obesity are all risk factors for breast cancer. Even the National Cancer Institute’s website (cancer.gov) writes, “Chronic inflammation may be caused by infections that don’t go away, abnormal immune reactions to normal tissues, or conditions such as obesity. Over time, chronic inflammation can cause DNA damage and lead to cancer.”
Any woman with any of these contributing factors should consider routine PEMF therapy for prevention, not only to the breast, but also for the whole body.
Typical breast cancer treatments include lumpectomy, mastectomy, chemotherapy, radiation, and longer-term hormone suppression therapy. Lymph node sampling creates its own issues with lymphedema. PEMF therapy has a significant role for anybody recovering from surgery, accelerating healing times and reducing the risk of complications. PEMF therapy has been found to often dramatically increasing the effectiveness of the chemotherapy in reducing side effects, especially neuropathy. PEMFs can be used before and after radiation therapy to reduce the collateral damage from the radiation to healthy tissues, including the heart, which is often in the path of the radiation field in the left chest. Routine use of PEMFs following these more aggressive procedures will also help reduce the risk of recurrences. While recurrence is more often in the same breast as the breast cancer, it also tends to recur more often than elsewhere in the opposite breast.
Another important aspect of using PEMFs is a long-term benefit to reduce the risk of metastases. Nearly 35 percent of women diagnosed with early-stage breast cancer will develop metastatic disease within 10 years. One breast cancer researcher from Northwest University in Chicago reports that 40 to 60 percent of women at the time
86 Super Charge Your Health To Protect Yourself Against Cancer
of initial diagnosis will have breast cancer stem cells in the bones. This is one of the reasons that bone metastases are common 10 or more years after initial treatment. Inflammation in the body is likely to be one of the more significant factors contributing to the breast cancer stem cells becoming activated in the bones. This information suggests that women having their initial diagnosis of breast cancer should strongly consider whole body PEMF therapy for the rest of their life following initial diagnosis and treatment. The purpose of the PEMF therapy in this setting is to continually work on reducing inflammation in the body, especially in the bones. Daily whole body PEMF therapy will help to restore health for other health problems as well.
Intensity of the PEMF: Therapy can be local, regional, or whole body. The intensities in general should be medium to high. Local therapy would be to the breast itself. Regional therapy would be to regional metastases, such as to the liver, the lungs, vertebrae and other regional bone metastases. The preferred and recommended treatment would be whole body, for the reasons mentioned in the previous paragraph. Given the investment required for adequate intensity magnetic fields, for local or regional use, it would be most cost-effective to proceed from the start to have a higher intensity whole body PEMF, particularly the “magnetic sandwich” approach.
Since many women with breast cancer, develop breast cancer post-menopause, they may also have osteopenia or osteoporosis, and therefore require higher intensity whole body PEMFs anyway. Having the right PEMF system from the start will provide many multiple benefits beyond the breast cancer. The minimum intensity magnetic field for local treatment is 1000 Gauss. For regional or whole body purposes, a minimum of 4000 Gauss would be better, given the depth into the body that the magnetic fields have to reach. A 6000+ Gauss allowing the “magnetic sandwich” approach would be the optimal intensity needed.
Applicators: To treat the breast or breasts only, a local small magnetic pad PEMF system is needed. For regional therapy, a half body pad of sufficient intensity, for example, 4000 Gauss, could work. A PEMF whole body system is the most recommended, allowing the “magnetic sandwich” treatment approach for optimal lifetime results.
Treatment Time: PEMF treatment around the time of procedures (chemotherapy and/or radiation) may need to be more intense. Typically, up to 60 minutes twice a day may be needed for the first few weeks or months after the end of conventional breast cancer treatments. After healing and recovery, PEMF therapy is geared to lifetime health maintenance and the typical recommendation is whole body PEMF stimulation twice a day in the morning and evening for 30 minutes. More time may be added if other needs arise.
Cancer, Chemotherapy Complications
Chemo drugs kill fast-growing cells, such as cancer cells. But because these drugs affect the entire body, they affect normal, healthy cells that are fast-growing, too.
87 Super Charge Your Health To Protect Yourself Against Cancer
Damage to cells causes side effects. The severity of side effects vary significantly from person to person and from one chemotherapy drug to another. Side effects are a very common aspect of chemotherapy.
Normal cells most likely to be damaged by chemotherapy are:
● Blood-forming cells in the bone marrow
● Hair follicles
● Cells in the mouth, digestive tract, and reproductive system
● Some chemotherapy drugs can damage cells in the heart, kidneys, bladder, lungs, and nervous system.
Doctors try to give chemotherapy at levels high enough to treat cancer, while keeping side effects at a minimum.
Common chemotherapy side effects include:
● Fatigue
● Hair loss
● Easy bruising and bleeding
● Infection
● Anemia (low red blood cell counts)
● Nausea and vomiting
● Appetite changes
● Constipation
● Diarrhea
● Mouth, tongue, and throat problems such as sores and pain with swallowing
● Skin and nail changes such as dry skin and color change
● Urine and bladder changes and kidney problems
● Weight changes
● Chemo brain, which can affect concentration and focus
● Mood changes
● Changes in libido and sexual function
● Peripheral neuropathy or other nerve problems, such as numbness, tingling, and pain
● Fertility problems
Some side effects of chemotherapy may not happen for several weeks to months after the chemotherapy is completed. Use of PEMFs during chemotherapy may not only help chemotherapy work better but may also help to reduce the side effects. Waiting to start PEMF therapy after symptoms have begun may not work as well as using it throughout the course of chemotherapy, or starting PEMF therapy afterwards.
While PEMF therapy may be targeted to specific problem areas with side effects, whole body PEMF therapy will produce the best and most efficient results. Additional focused PEMF therapy could be applied locally for problems caused by chemotherapy, such as urinary tract and kidney issues, nausea, fatigue, peripheral neuropathy, and fatigue.
Intensity of the PEMF: Most efficient treatment would be using high intensity whole body PEMFs with significant control of intensity. Whole body treatment will help in the
88 Super Charge Your Health To Protect Yourself Against Cancer
control of the cancer and healing of tissues damaged by the treatments. Treatment of local problems would require magnetic field intensities based on the depth of penetration needed to reduce inflammation.
Applicators: A whole body, magnetic field “sandwich” is the most efficient way to deal with problems in multiple areas the body. Additional local or regional treatment can be applied for problems not responding to whole body treatment. Frequency-based, medium to high intensity local PEMFs may be needed for brain entrainment purposes to reduce fatigue, brain fog, and neuropathy. Nausea may require both brain and abdominal treatments. PEMF therapy should be able to be used together with other therapies to reduce symptoms. Most other therapies that control symptoms do not help with healing, which is why combinations of PEMF therapy and medications can be expected to be more effective.
Treatment time: Because of the toxicities associated with chemotherapy, the “low and slow” approach is critical. Individuals in this situation often lack motivation to do treatment and may require their support system to help out with encouragement and applicator placements. The goal would be to reach the maximum intensity and up to an hour of total treatment at a time, two to three times per day. The success in managing symptoms, especially for how often they recur, will determine how long and how often treatments need to be done. Any treatments used for chemo side effects should help with the underlying cancer process, as well.
Cancer, Head, Neck, And Oropharyngeal
For cancer in these areas of the body, the general recommendations at the beginning of this chapter apply. PEMFs may be helpful to the primary cancer itself, but may be especially helpful following chemotherapy, and before and after surgery and/or radiation. The incidence of distant metastases in head and neck squamous cell carcinoma (SCC) is relatively small in comparison to other cancers. Metastases occur most often in the lungs.
Intensity of the PEMF: High intensity PEMFs are necessary for the head and neck area to be able to reach all the tissues equally throughout the hold had neck area, especially to be able to benefit lymph nodes.
Applicators: Local applicators would do best, particularly the butterfly coil or loop coil folded into any lips around the neck. Metastases can be treated with higher intensity regional applicators or whole body PEMF therapy.
Treatment Time: Between 30 to 60 minutes twice a day in the first stages of treatment. As significant improvement is seen, treatments may be cut back to 30 minutes twice a day indefinitely for health maintenance.
89 Super Charge Your Health To Protect Yourself Against Cancer
Cancer, Liver
Liver cancer can occur as a primary condition or a secondary condition from liver metastases. Regardless of whether it is primary or secondary, liver cancer should be treated generally as well as specifically. PEMFs are not expected to cure or kill the cancer. Occasionally, liver cancer may be seen to shrink.
Primary liver cancer can metastasize most commonly to the lungs and bones. As with all other cancers, high intensity whole body PEMF therapy is recommended, preferably at the earliest stages before obvious metastases have developed. Combination therapies will usually provide the best results. PEMFs can be used in combination with chemotherapy, surgery, embolization procedures and before and after radiation.
Intensity of the PEMF: Follow the intensity recommendations in Appendix A. Since the liver is a large organ, a magnetic field intensity of a minimum of 4000 Gauss is recommended.
Applicators: A regional applicator may be used but a whole body high intensity PEMF system is recommended. A regional applicator would include a half body pad or an elliptical coil applied over the liver on the front of the lower chest and upper abdomen. Whole body PEMF therapy should be done using a “magnetic sandwich” approach or if using a single pad with the bottom of the two pads and loop coil, apply the pad below the body as well as the loop coil on the front of the body.
Treatment Time: A “low and slow” approach should be used. The goal is to reach maximum intensity for an hour twice a day. Once significant results are achieved, treatment may be able to be reduced to 30 minutes twice a day while monitoring test results. It is likely that treatment will be required for months followed by a maintenance protocol.
Supplements. Liver and antiviral supplements should be combined. At a minimum, liver supplements can include milk thistle, alpha lipoic acid, and acetyl cystine, acetyl l-carnitine, zinc, selenium, tocotrienols, licorice root and vitamin C. There are many more possible anticancer supplements. As a result, I recommend consulting with a professional skilled in nutrition and supplements for cancer patients to give guidance on nutrition and the supplements that could be used. The PEMFs are expected to work synergistically with any supplements, as well as decreasing inflammation in the liver and improving liver function.
Cancer, Lung
There are many forms of both primary and secondary lung cancer, with primary starting in the lung itself and secondary from metastases from other cancers elsewhere in the body. The two major forms of primary lung cancer are non-small cell
90 Super Charge Your Health To Protect Yourself Against Cancer
and small cell. The overall five-year survival rate for all stages is 14 to17 percent for non-small-cell lung cancer and six percent for small-cell lung cancer.
Inflammation is a very important contributor to the development of lung cancer. The inflammatory components include a buildup of inflammatory white blood cells, promoting tumor progression by releasing a variety of cytokines, chemokines, and cell toxic mediators. Inflammation also affects many aspects of the cancer process, including the proliferation and survival of cancer cells, angiogenesis, tumor metastasis, and tumor response to chemotherapy and hormones.
One of the most important causes of inflammation in the lung is smoking. Other contributing factors include air pollution, autoimmune disease, radon, and recurrent infections. Because cancers thrive in low oxygen environments, they are more commonly seen in people with chronic obstructive pulmonary disease (COPD), who have lower than normal oxygen levels in their lungs.
Research is limited on the use of PEMFs for lung cancer but one study showed significant impact on cancer cells. Lung cancer tumor tissue obtained during surgery from twenty patients was evaluated for biochemical and physical changes using deep electron microscopy. All had PEMFs preoperatively to reduce tumor resistance to standard therapy. PEMFs caused cellular changes to the cancer cells, showing a marked antitumor effect. Changes were best after 20 to 30 treatment sessions. Highly differentiated (mature) adenocarcinomas were the most sensitive to the PEMFs.
The goal of PEMF therapy is to help to heal inflammation in the lung, which not only contributes to the development of the cancer, but also causes it to continue to grow and spread. In addition, PEMF therapy increases blood supply and oxygen exchange in the lungs, making the environment less hospitable to the cancer.
With metastatic cancer, the other parts of the body from which the metastases spread need PEMF therapy as well. Whole body high intensity PEMF therapy is the best and the most efficient use of treatment time. Individuals with cancer would be best served by considering long-term needs, for whatever health issues may unexpectedly arise. So the investment in a more efficient PEMF treatment system should be evaluated and considered. The cost, not just in dollars but also in health, of not considering future needs can be considerable and regrettable. PEMFs can be used along with surgery, chemotherapy and before and after any radiation therapy, as well as other medications.
Intensity of the PEMF: Because of the size of the lungs, high intensity PEMFs are needed. The average diameter of the chest from the front to the back is about 6-9 inches, depending on which part of the chest is measured. That means that a magnetic field intensity of between 4000-7000 Gauss is necessary to provide at least 15 Gauss of magnetic field intensity from the front to the back of the chest.
91 Super Charge Your Health To Protect Yourself Against Cancer
Applicators: Appropriate intensity regional applicators may be used. They would have to be applied to the side and back of the left chest, and the front and the back of the right chest to deliver the needed magnetic field intensity. If the lung cancer is secondary to cancer elsewhere in the body, the other parts of the body would need to be treated as well. A more efficient alternative would be to use a dual pad, whole body, “magnetic sandwich” PEMF system. The whole body system would also be helpful to maintain the general health of the body and work to prevent and deal with metastatic disease.
Treatment Time: Using the “low and slow” approach, the recommend treatment time is 60 minutes twice a day. Improvements in lab work, symptoms, and imaging studies may allow treatment time to be decreased to about 30 minutes twice a day, indefinitely.
Cancer, Pancreatic
The causes of or risks for pancreatic cancer include chronic pancreatitis, age, heredity (family cancer syndrome and BRCA2 gene), smoking, heavy alcohol use, excessive processed and red meat, other history of cancer, abdominal obesity, sedentary lifestyle, diabetes and chronic hepatitis. People often have several of these risk factors. Over 80 percent of cases occur between the ages of 60 and 80.
Pancreatic cancer can spread into other parts of the belly and the liver, and also to the lungs, bone, brain, and other organs. Because pancreatic cancer disseminates early and progresses locally rapidly, more than 75 percent of patients diagnosed with it cannot be offered curative treatment.
By the time somebody is diagnosed with pancreatic cancer, PEMF treatment, to have some value to either improve symptoms and perhaps to delay progression and dissemination, needs to be done aggressively and early. The temptation may be to simply do local high intensity treatments to the pancreas area, but because of the rapid dissemination, a high intensity whole body “magnetic sandwich” system should be strongly considered and used aggressively.
Intensity of the PEMF: 4000-7000 Gauss is recommended. Lower intensity systems may provide some general benefit for symptom relief and somewhat improve vitality, but the risk may be too high to bother.
Applicators: If the decision is made to do local treatment, a regional applicator over the whole upper abdomen would be better than a smaller local device just to treat the pancreas itself. Again, by the time the cancer is discovered it will have started causing problems in the whole upper abdomen, not just the pancreas itself. The best system is likely to be a high intensity “magnetic sandwich” PEMF system. Every treatment session could include treatment with the two whole body pads first, followed by
92 Super Charge Your Health To Protect Yourself Against Cancer
laying on the lower whole body pad combined with a loop coil to the upper abdomen.
Treatment Time: A ”low and slow” approach may be needed depending on the general status of the person. It may need to be advanced faster than used with other conditions, in order to be more aggressive. The minimum recommended treatment time is 60 minutes two to three times per day.
Cancer, Stage IV
The same issues that apply to stage IV cancer apply to cancer in general. The difference is that in stage IV, the cancer has now spread to another organ or multiple organs in the body from its original source. It may range from being mild to severe. There may be other significant health issues at the same time. Treatments for stage IV cancer are complicated and often challenging to deal with, and may include chemotherapy, immune modifying agents, surgery, and/or radiation. Life expectancy with stage IV cancer depends on many factors, as well. Five-year survival rates vary by cancer and range from 5.5 to 72 percent for the top 12 most common cancers, and vary by cancer type, grade, genetics, and many other traits.
The goal of PEMF therapy in the setting of stage IV cancer is to increase general health, reduce symptoms from the cancer or treatments, help the body to control the cancer at its current level or better, facilitate the effectiveness of any other standard or experimental conventional medical system treatments being used, help any other alternative approaches to be more effective, and/or reduce inflammation in the body that may make cancer growth more likely.
Since often, especially for solid organ cancers, cancer stem cells are already in many places of the body, the aim of PEMF therapy is to reduce local factors that may cause cancer cells to take root and grow. It is not a replacement for other therapies, especially rescue therapies with imminent organ failure. My experience has been that PEMFs help to support any other approaches being taken to deal with the cancer and other health conditions.
I believe it is important to work with integrative health practitioners to obtain the optimal benefits for the circumstances. Every health discipline has something to offer; no one type of practitioner is supreme or absolute. Survival of a person, in general and with stage IV cancer in particular, I believe is ultimately spiritually determined. After 50 years of medical practice and being part of the care of hundreds of stage IV cancer patients, I’m only one of the participants helping. I bow to the Ultimate Decision-Maker. After all, “nobody gets out of here alive.” Everyone leaves and shuffles off this mortal coil. We do the best we can to maintain our residence in these bodies, guided by spirit.
93 Super Charge Your Health To Protect Yourself Against Cancer
In my experience, combining PEMF therapies along with other integrative approaches in the stage IV cancer setting, a number of individuals with short term survival expectations have lived four years or more. Whether the PEMFs were a major contributing factor to their extended survival, we can’t say for certain. However, almost all were thankful for the benefits they received which made them feel considerably more comfortable in their journey.
It is a personal choice which path people want to take in dealing with stage IV cancer. There is no judgment. It’s impossible to know which path was right or not. I respect each person’s choice. If PEMFs are part of the choice to continue with various treatments, then I hope they can have an impact in helping.
Ultimately, the decision on which PEMF system to use has to be individualized. This often will require a consultation with a professional with clinical expertise with cancer, as well as in the use of PEMFs. A professional with expertise with only one particular PEMF system can still be very important and helpful, understanding the strengths and limitations of the system they are using. It may also be helpful to engage a professional who has wider knowledge of PEMFs and access to different types of PEMF systems to have flexibility in making the best recommendations. To take a quote from Dr. Abraham Maslow, “if your only tool is a hammer, you see every problem as a nail.”
I believe that stage IV cancer will require at least a whole body “magnetic sandwich” system and/or additional applicators for local use. Different PEMF systems can be configured in many ways to produce “magnetic sandwich” configurations. The better option, normally, would be to have two whole body pads running together. This makes treatment more efficient, decreasing total treatment time. Smaller applicators may be used for specific needs, often combining a whole body pad with a local applicator. It’s even possible to combine two local applicators in two different areas or in a “magnetic sandwich” approach.
The whole body approach is to decrease inflammation throughout the whole body, thereby decreasing the burden of the immune system with many fights in many locations. The whole body approach with the right magnetic field intensity will also help any local needs, while at the same time being able to use a local applicator where also needed.
Intensity of the PEMF: 4000 – 7000 Gauss either/or whole body and local. The need for these intensities is to reach deep into the body wherever an anti-inflammatory and support action is needed.
Applicators: Local, whole body, and preferably whole body “magnetic sandwich.” A local portable PEMF device may be needed for sleep or for other local treatments over extended treatment times.
Treatment Time: The “low and slow” approach will always be needed at the beginning of starting PEMF stimulation. I recommend 30-60 minutes twice a day at a min-
94 Super Charge Your Health To Protect Yourself Against Cancer
imum, morning and evening, combining local and whole body treatment time as needed. Depending on the amount of pain or other health issues present, more time may be added throughout the day.
For additional information about how PEMF therapies can support surgery, chemotherapy, and radiation treatments, please see the Appendix.
The next chapter provides further overviews of the research that demonstrates the usefulness of PEMF Therapy as a supportive cancer treatment.
95 Super Charge Your Health To Protect Yourself Against Cancer
PEMF Therapy and Cancer: What The Research Shows
In this chapter, I provide samplings and summaries of various studies that provide indications of the benefits PEMF therapy can provide for cancer. These studies fall into three categories: in vitro cell line studies, animal studies, and human studies. I begin with a comment that researchers wrote in a scientific paper that was published in 2016 in the medical journal Cancer Medicine:
““Cancer is one of the most common causes of death worldwide. Available treatments are associated with numerous side effects and only a low percentage of patients achieve complete remission. Therefore, there is a strong need for new therapeutic strategies. In this regard, pulsed electromagnetic field (PEMF) therapy presents several potential advantages including non‐invasiveness, safety, lack of toxicity for non‐cancerous cells, and the possibility of being combined with other available therapies. Indeed, PEMF stimulation has already been used in the context of various cancer types including skin, breast, prostate, hepatocellular [liver cells], lung, ovarian, pancreatic, bladder, thyroid, and colon cancer in vitro [cell line studies] and in vivo [animal and human studies]... Indeed, PEMF therapy can be used as an adjuvant treatment to chemotherapy and radiotherapy with the aim of reducing their dosage, mitigating any harmful secondary side effects, and enhancing patient’s prognosis.” (Vadalà M, Morales-Medina JC, et al. Mechanisms and therapeutic effectiveness of pulsed electromagnetic field therapy in oncology. Cancer Med. 2016 Nov;5(11):3128-3139.)
A Sampling of In Vitro (Cell Line) Studies
What follow are the outcomes of various studies that examined the effects of PEMFs on different types of cancer cell lines.
Human Breast Adenocarcinoma Cells Compared to Human Nontumor Cells:
In this study, “MCF7 breast cancer cells and their normal counterparts, MCF10 cells” were both exposed to PMEFs in a frequency range between 20 to 50 Hz, at intensities between 2 mT to 5 mT, for between 30 to 90 minutes each day. At the end of the third day, the researchers found that daily 60 minute PEMF exposure at 20 Hz and 3 mT increased apoptosis (cell death) in the breast cancer cells while having no harmful effects on the normal cells.
96 Super Charge Your Health To Protect Yourself Against Cancer CHAPTER 9
As a result of this finding, the researchers wrote, “Based on our data it appears that PEMF-based anticancer strategies may represent a new therapeutic approach to treat breast cancer without affecting normal tissues in a manner that is non-invasive and can be potentially combined with existing anti-cancer treatments.” (Crocetti S, Beyer C, et al. Low intensity and frequency pulsed electromagnetic fields selectively impair breast cancer cell viability. PLoS One. 2013 Sep 11;8(9):e72944.)
Human Breast Cancer and Colon Cancer Cell Lines:
In this study, both cells lines were exposed to PEMFs for between 24 to 72 hours at a frequency of 50 Hz and an intensity of 10 mT. The study “clearly showed disintegration of cells treated with a 50 Hz EMF, compared to untreated control cells. A large percentage of treated cells resulted in increased early apoptosis after 24 h[ours] and 72 h[ours], compared to the controls.” (Filipovic NDT , Radovic M, et al. 2014. Electromagnetic field investigation on different cancer cell lines. Cancer Cell Int. 14:1–10. )
Human Breast Cancer and Lung Cancer Cell Lines:
In this study, both human breast and lung cancer cells were treated with PEMFs for durations of two, six, eight, or 24 hours, with the PEMFs administered either alone or in combination with various chemotherapy drugs. The study found that PEMFs “induced apoptosis and gene expression changes that modestly inhibited breast and lung cancer cell growth.” These same researchers also found similar results when PEMFs were administered to mice with breast or lung cancer. (Chen MY, Li J, Zhang N, et al. In Vitro and in Vivo Study of the Effect of Osteogenic Pulsed Electromagnetic Fields on Breast and Lung Cancer Cells. Technol Cancer Res Treat. 2022 JanDec;21:15330338221124658.)
Human Ovarian Cancer Cell Lines:
In a study conducted by researchers in China, cultured human ovarian cancer cells were exposed to PEMFs of 8, 16, 32, and 64 Hz, respectively, at an intensity of 1 mT. The exposures lasted for 30 minutes and were administered twice a day at 12-hour intervals for three days. At the conclusion of the study, it was found that PEMFs of 8 Hz, 1 mT significantly induced apoptosis and inhibited the spread of the ovarian cancer cells. (Wang Q, Wu W, Chen X, He C, Liu X. [Effect of pulsed electromagnetic field with different frequencies on the proliferation, apoptosis and migration of human ovarian cancer cells]. Sheng Wu Yi Xue Gong Cheng Xue Za Zhi. 2012 Apr;29(2):291-5. Chinese. PMID: 22616177.)
Human Hepatocellular Carcinoma (Liver Cancer) Cells:
In this study, “hepatocellular carcinoma cells (HCCs) were exposed to 27.12 MHz radiofrequency electromagnetic fields using in vitro exposure systems designed to replicate in vivo conditions. Cancer cells were exposed to tumour-specific
97 Super Charge Your Health To Protect Yourself Against Cancer
modulation frequencies, previously identified by biofeedback methods in patients with a diagnosis of cancer. Control modulation frequencies consisted of randomly chosen modulation frequencies within the same 100 Hz–21 kHz range as cancer-specific frequencies.”
The study found that as a result of PEMF therapy, the growth HCCs “was significantly decreased”, without harming or interfering with the growth of normal liver cells. “These findings uncover a novel mechanism controlling the growth of cancer cells at specific modulation frequencies without affecting normal tissues, which may have broad implications in oncology,” the researchers concluded. (Zimmerman JW, Pennison MJ, et al. Cancer cell proliferation is inhibited by specific modulation frequencies. Br J Cancer. 2012 Jan 17;106(2):307-13.)
Animal Studies
A number of animal studies further demonstrate the potential benefits PEMF therapy has as a supportive treatment for cancer. A sampling of such studies follows.
Human Breast Cancer Grafted Onto Mice:
In this study, a specific type of human breast cancer was grafted onto female mice via injection into the fatty tissue of their mammary glands. The mice were then divided into four groups, with the first group untreated and acting as the controls. The second group received radiation treatment every other day, the third group received daily 10-minute PEMF treatments, and the fourth group received radiation therapy in combination with PEMFs.
At the end of the study, it was found that the group receiving radiation therapy or PEMFs “had significantly fewer lung metastatic sites and slower tumor growth than did untreated mice.” Moreover, no harmful side effects were attributed to the PEMF treatments, leading the researchers to conclude that PEMF therapy “provided a safe means for retarding tumor vascularization, growth and metastasis.” (Cameron IL, Sun LZ, Short N, Hardman WE, Williams CD. Therapeutic Electromagnetic Field (TEMF) and gamma irradiation on human breast cancer xenograft growth, angiogenesis and metastasis. Cancer Cell Int. 2005 Jul 26;5:23.)
Another Study of Mice Injected With Breast Cancer Cells:
In this study, mice were injected with metastatic mouse tumor cell line cells and then divided into four groups, with one group acting as the control. The other three groups were exposed to PEMFs of 1 Hz and 100 mT once a day for four weeks, for one hour, three hours, or four hours, respectively. At the study’s conclusion, the mice in the control group experienced a 500 percent greater increase in tumor growth during the four-week period, whereas the mice that received PEMF therapy for four hours a day “showed extensive areas of necrosis in their tumors.” However, there was no reduc-
98 Super Charge Your Health To Protect Yourself Against Cancer
tion in tumor size or growth in the mice that only received PEMFs for one or three hours, respectively. As the study’s authors noted, “the time of exposure of these tumors to magnetic fields is critical”.
They concluded their study by writing, “Our findings, along with the reports of others, support further exploration of the potential of magnetic fields in cancer therapeutics, either as adjunctive therapy or, in some as yet to be determined specific cases, as primary therapy. In particular, prolonged exposure times and different field strengths and waveforms should be explored.” (Tatarov I, Panda A, Petkov D, et al. Effect of magnetic fields on tumor growth and viability. Comp Med. 2011 Aug;61(4):33945.)
Rat Liver Cancer:
In this study, 60 rats were studied over a period of one month, and divided into six groups. The first three groups were used as normal controls. The other three groups were injected with the carcinogen diethylnitrosamine (DEN) in order to induce hepatocellular carcinoma (HCC).
Among the control groups, the first group received PEMF therapy (2-3 Hz, 0.0004 T) for 30 minutes a day, six days a week. The second group received PEMFs (<1 Hz, 0.6 T) for 15 minutes a day, six days a week, and the third group was left untreated.
Among the three groups of rats with induced HCC, the first group also received PEMF therapy (2-3 Hz, 0.0004 T) for 30 minutes a day, six days a week. The second group received PEMFs (<1 Hz, 0.6 T) for 15 minutes a day, six days a week, and the third group was left untreated.
At the study’s conclusion, the rats in each of the control groups treated with PEMFs showed no evidence of harm caused by the PEMFs. “Such results suggest the safety of the used magnetic fields. The lack of adverse reactions in normal cells suggested that the safety of this treatment may be related to its ability to influence preferentially and selectively with the transformed cells,” the researchers wrote.
Among the rats in the HCC-induced groups, those that received PEMF treatments showed a “significant decrease in AFP level and other blood tests”. AFP (alpha fetoprotein) is a tumor marker test for liver cancer. The researchers also found “slight improvement in dielectric properties of livers which suggests the anticancer activity of these magnetic fields”.
Based on these findings, the researchers concluded that their study “suggests a selective anticancer activity of magnetic fields from the exposure system through incorporating three main strategies: apoptosis, necrosis and inflammatory infiltration of the hepatocellular carcinoma.” They also noted that the PEMFs “did not affect the cancer cells directly but increased the host immune system against cancer.”
99 Super Charge Your Health To Protect Yourself Against Cancer
(Emara SO, EL‐Kholy SM, et al Therapeutic effects of low frequency pulsed electromagnetic fields on rat liver cancer. Res. Inventy Int. J. Eng. Sci. 2013 Apr;2(9):17–18.)
Two Studies of Induced Melanoma in Mice:
Melanoma is a skin cancer that can sometimes be fatal, which is why the following two studies are so noteworthy. In both of them, mice were injected with melanoma cells to induce melanoma.
In the first study, between two to four melanoma tumors were induced in 120 female mice. The mice then received 30-minute PEMF treatments (0.5 Hz, 0.2 T) three times a day over the course of six days. On average, the mice tumors shrunk by 54 percent within a few minutes after PEMF therapy was administered and by 68 percent three hours later. Within two weeks following exposure to PEMFs, the tumors had shrunk by 90 percent. The PEMFs also caused blood flow to the tumor sites to be reduced within the first 15 minutes of treatment, and to eventually stop over time. “A second treatment at this time can result in complete remission,” the researchers wrote. (Nuccitelli R, Pliquett U, et al. Nanosecond pulsed electric fields cause melanomas to self-destruct. Biochem Biophys Res Commun. 2006 May 5;343(2):351-60.)
In the second study, melanoma was also induced in four mice via injection of melanoma cells, causing a total of 17 melanoma tumors to form. The mice then received only six minutes of PEMF therapy (5-7 Hz, 0.2 T). The study found that the tumor cells began to shrink within an hour of treatment and were completely eliminated after a single treatment. (Nuccitelli R, Tran K, et al. Optimized nanosecond pulsed electric field therapy can cause murine malignant melanomas to self-destruct with a single treatment. Int J Cancer. 2010 Oct 1;127(7):1727-36.)
Note: In the second study above, PEMFs were delivered via suction needle electrodes, a method that is not used in treatments using standard PEMF devices. Still, the results certainly merit our attention.
Human Studies
Despite the encouraging results of the above in vitro and animal studies that provide indications of PEMF therapy’s potential benefits as a supportive treatment for cancer, few human studies on the use of PEMFs for cancer have been conducted so far. Among the most noteworthy ones that have is one that was published in 2009 in the Journal of Experimental & Clinical Cancer Research.
In that study, researchers first identified tumor-specific frequencies that could potentially be used as an aid for treating specific types of cancer. In all, a total of 1,524 electromagnetic frequencies were identified based on an examination of 163 cancer
100 Super Charge Your Health To Protect Yourself Against Cancer
patients. The frequencies ranged from 0.1 Hz to 114 kHz. According to the researchers, most of these frequencies (57 to 92 percent) were specific to a single tumor type.
The researchers then offered what was termed “compassionate treatment” using various of these PEMFs to 28 patients with advanced cancers who, because of their conditions, had limited other treatment options available to them. Seven of the patients had advanced breast cancer, five had ovarian cancer, three had pancreatic cancer, two had colorectal cancer, and two had prostate cancer. Among the other nine patients, there was one case each of brain cancer (glioblastoma multiforme), liver cancer (hepatocellular carcinoma), mesothelioma, neuroendocrine cancer, non-small-cell lung cancer, small-cell lung cancer, sarcoma, thyroid cancer, and oligodendroglioma, a cancer that affects the brain and central nervous system.
The patients were shown how to self-administer PEMF therapy, with each of them then giving themselves 60-minute PEMF treatments three times a day over an average of 278.4 months. During this time, none of the patients reported any side-effects from their use of PEMFs, with the exception of low grade (grade 1) fatigue, which was experienced by three of the patients during or immediately after each treatment .
Thirteen of these patients were able to subsequently be evaluated to determine how well they responded to the PEMFs. According to the study’s authors, “One patient with hormone-refractory breast cancer metastatic to the adrenal gland and bones had a complete response lasting 11 months. One patient with hormone-refractory breast cancer metastatic to liver and bones had a partial response lasting 13.5 months. Four patients had stable disease lasting for +34.1 months (thyroid cancer metastatic to lung), 5.1 months (non-small cell lung cancer), 4.1 months (pancreatic cancer metastatic to liver) and 4.0 months (leiomyosarcoma metastatic to liver).”
Based on these results, the authors concluded, “Cancer-related frequencies appear to be tumor-specific and treatment with tumor-specific frequencies is feasible, well tolerated and may have biological efficacy in patients with advanced cancer.” (Barbault A, Costa FP, et al. Amplitude-modulated electromagnetic fields for the treatment of cancer: discovery of tumor-specific frequencies and assessment of a novel therapeutic approach. J Exp Clin Cancer Res. 2009 Apr 14;28(1):51.)
In another noteworthy study, “ Forty‐one patients with advanced HCC [hepatocellular carcinoma, i.e., liver cancer] received very low levels of PEMFs modulated at HCC‐specific frequencies (100 Hz–21 kHz) and received three‐daily 60 min[ute] outpatient treatments. No adverse reactions were observed during PEMF treatment. Five patients reported complete disappearance and two patients reported decrease in pain shortly after beginning of treatment. Four patients showed a partial response to treatment, while 16 patients (39 percent) had stable disease for more than 12 weeks. This study shows that PEMF therapy provides a safe and well‐
101 Super Charge Your Health To Protect Yourself Against Cancer
tolerated treatment, as well as evidence of antineoplastic effects in patients with HCC.” (Vadalà M, et al. Mechanisms and therapeutic effectiveness of pulsed electromagnetic field therapy in oncology. Cancer Med. 2016 Nov;5(11):3128-3139.)
The results of these two studies demonstrate the potential that PEMF therapy has as a treatment for cancer. The studies also demonstrate that PEMFs are safe for cancer patients.
To learn about additional in vitro, animal, and human studies that have been conducted on PEMFs and cancer, please see the Appendix.
Hopefully, human clinical trials will continue to be conducted in order to further determine PEMF therapy’s benefits for cancer. In the meantime, because affordable PEMF devices increasingly available today, cancer patients now have the opportunity to support their primary cancer treatments with PEMF therapy at home.
In the next chapter, I explain how PEMF therapy can be combined with other complementary and alternative therapies to further enhance those therapies’ benefits.
102 Super Charge Your Health To Protect Yourself Against Cancer
Combining PEMFs With Other Complementary Cancer Treatment Methods
While PEMF therapies provide a large array of actions that support health and can potentially reduce the problems associated with cancer, these actions produce better results when PEMFs are part of a more comprehensive wellness approach, including optimal dietary nutrition support and, as necessary, various nutritional supplements.
In this chapter you will learn how and why PEMF therapy with other complementary cancer treatments can enhance these treatments benefits to help improve patient outcomes. First, though, let’s briefly discuss diet and nutrition, an essential cornerstone of health which is vitally important when it comes to preventing and recovering from cancer.
Diet—The Vital Cornerstone of Your Health
The foods and beverages you consume supply the fuel your body needs—in the form of vitamins, minerals, enzymes, amino acids, essential fatty acids, and other nutrients—to perform its vast number of daily functions. The better the quality of foods and beverages you consume, the better able your body will be to generate energy, repair itself, and resist cancer and all other diseases. Conversely, poor dietary habits diminish your body’s ability to maintain optimum health, and significantly increase cancer risk. They also reduce the degree of benefit you will gain from PEMFs and any other type of therapy.
The key to eating well is to eat foods that will provide your body with what it needs to maintain your health. In general, since inflammation is a significant component of cancer and most other health conditions, an anti-inflammatory diet which consists of more vegetables and fruits (eaten raw or lightly steamed) is generally the most anti-inflammatory and is what I recommend to all of my patients. Such a plantbased diet has also been shown to be a wise choice for both preventing and recovering from cancer.
Continuing to follow the standard American diet (SAD) and other unhealthy diets that promote inflammation and then trying to treat yourself with PEMF therapy is like trying to put out the fire of inflammation while continuing to pour gasoline on the fire. That’s not very smart and certainly not effective in terms of achieving and maintaining better health.
103 Super Charge Your Health To Protect Yourself Against Cancer CHAPTER 10
Another important aspect of healthy eating is nutrient density This has to do with how much nutrition there is in a food in comparison to how many calories it contains. Colorful foods tend to have the most healthful qualities, not only in terms of their vitamins and minerals, but also in antioxidants and cofactor phytochemicals like carotenoids that work synergistically with those nutrients, helping to make them more bioavailable.
The debate surrounding vegetarian and vegan diets versus an omnivore diet that includes meats, poultry, and other flesh foods is not one to put much stock in since it is possible to be very healthy or very unhealthy eating either way. If you choose to be vegetarian, be sure to supplement nutrients where needed, and consume plenty of sources of vegetarian protein. If you choose to eat meat, make it lean and not overcooked. It is generally accepted that fried or cooked fats derived from animals (meat, dairy, seafood) are strongly inflammatory in the body. To offset the free radical or oxidative stress caused by these foods, once again, raw fruits and vegetables eaten at the same meal are the answer.
If possible, also eat organic foods. Organic fruits and vegetables have been shown to have a higher nutrient content, compared to non-organic produce, and are also free of harmful pesticides, preservatives, and other chemicals used to grow non-organic, commercial food crops. Similarly, your meat and poultry food choices should ideally be free-range and free of the hormones and antibiotics that are commonly found in commercially harvested animal products.
Other healthy eating practices include eating plenty of fiber-rich foods (raw fruits, vegetables, and complex carbohydrates), and eliminating sugars and simple carbohydrates, “junk” foods, and unhealthy fats, especially trans-fatty acids and hydrogenated fats.
Finally, it is incredibly important to drink plenty of water, especially when using PEMF therapies, because energy transfers more easily in a body that is well-hydrated, with blood that is less viscous (thick). The magnetic signal will be the most robust in a body with adequate hydration levels.
For more dietary, as well as other lifestyle and detoxification recommendations to help prevent and recover from cancer, please refer back to the guidelines I provided in Chapter 2.
Supporting Your Diet With Nutritional Supplements:
Even if you eat fresh, organically grown food for all of your meals—something that is not easy to do for many people—such foods, although certainly richer in nutrients than non-commercial foods, are most likely still incapable of meeting all of your nutritional needs.
104 Super Charge Your Health To Protect Yourself Against Cancer
There are a number of factors that explain this, starting with the fact that the soil in which food crops are grown contains significantly reduced levels of vital minerals, compared to the level of soil minerals a century or more ago. Because of the commercial farming methods used by today’s agricultural industry, much of the minerals that had been abundant in our topsoil prior to the early 20th century have been greatly depleted. To compensate for the poor condition of the soil, current nonorganic farming methods rely on substantial quantities of synthetic chemical pesticides, herbicides, and fertilizers to help crops grow. These commercial farming methods have not only resulted in significant declines in the mineral content of crop soil, but also declines in the overall nutrient content of the foods grown under such conditions.
Compounding the problem is the fact that much of our modern day food supply, after it is harvested, takes weeks and even months before it reaches us. Comparatively few of us eat locally grown food these days. Instead, the food that we consume, even if grown organically, is shipped from other parts of the country, frozen, stored, and warehoused along the way. This further reduces the nutrient content of food. For all of these reasons, it makes good sense to augment your diet with various nutritional supplements.
Because of your usual dietary habits and the quality of the food you eat, as well as the normal stresses and demands of daily living, you never know on a day-to-day basis what essential nutrients you’re missing from your food. You often hear doctors say that supplements and vitamins only make for expensive urine. I say, better to have expensive urine than cheap urine. You absorb what you need and eliminate what you don’t. So, daily nutritional supplements and basic vitamins are necessary for almost everybody.
Supplement quality is directly related to supplement efficacy. The better the quality of your supplements, the better the job they will do for you.
To help ensure that you provide your body with sufficient amounts of the nutrients it needs to function at optimal levels, a good multivitamin/mineral is important. It will act as a security blanket, covering common diet deficiencies. In addition to a good multivitamin/mineral supplement, I recommend that most people take a basic foundation of nutritional supplements. However, I recommend that cancer patients work with an experienced nutritional specialist to best determine which nutritional supplements a person might need. There are many nutritional and other supplement products that can potentially benefit cancer patients, but as with cancer treatment itself, there is no specific one-size-fits-all nutritional supplement program for patients. Every patient is different and nutritional needs can vary greatly from one patient to another.
When using PEMF therapies, maintaining proper levels of magnesium in the body is vital because PEMFs cause a great deal of calcium ion movement in the body. Mag-
105 Super Charge Your Health To Protect Yourself Against Cancer
nesium is what calcium latches on to as it moves in and out of the cell, so a magnesium deficiency may undermine the effectiveness of PEMF treatments. Since most of us could use more magnesium, supplementation with it is recommended, especially when PEMF therapy is employed regularly.
In addition to the foundation supplements above, I recommend various other supplements to support detoxification and healthy sleep, as well as easing pain and pain-related conditions, and for managing stress.
Complementary Therapies That Can be Used With PEMFs
There are usually multiple factors that combine to cause and exacerbate most chronic health problems. This is especially true for cancer. For healing to be possible, each of these factors must be addressed and resolved.
Similarly, there are multiple factors that need our attention if we are to recover from disease and create and maintain good health. In addition to a healthy diet and appropriate nutritional supplementation, other essentials for health and recovery from illness include adequate amounts of restorative sleep, regular exercise, cultivation of positive emotions, and stress management, among other things. Unfortunately, not all oncologists and other physicians are trained to address all of these factors.
I take a broader approach, incorporating multiple therapies, so that I don’t leave anything to chance. This includes PEMF therapy because of the wide range of benefits it is proven to provide. Based on my experience, PEMF therapy can and should be combined with other therapeutic approaches in order to maximize patient recovery, especially since it is uncommon for complementary therapies to interfere with one another.
However, it can be difficult to find advice about combining therapies, primarily because physicians tend to have specialties. Practitioners of any discipline who only practice one discipline, even with excellence, tend to know little about other therapeutic options. The integrative medicine that I am trained in urges physicians and patients alike to know as much about health as possible, and to explore a wide range of therapeutic options to achieve optimum treatment results and well-being.
Because PEMF therapies work on such a basic level, their effects are almost always enhanced with the use of other modalities, and vice versa. That being said, there is usually a best practice in terms of sequence of use, duration of treatment, and time between applications. In addition, you should always consult your physician or other health professional before beginning a new therapy. This is especially important when it comes to using PEMF and other therapies in conjunction with conventional cancer treatments (surgery, chemotherapy, radiation).
106 Super Charge Your Health To Protect Yourself Against Cancer
Complementary Treatments For Cancer:
As I discuss in more detail in this eBook’s Appendix, a growing number of cancer patients elect to use complementary, alternative, and integrative (CAM) therapies to treat their condition. This is particularly the case when they are treated by integrative oncologists, who specialize in combining such therapies with conventional cancer treatments. In some cases, patients may chose to forgo chemotherapy or radiation altogether to avoid their side effects, choosing to only use complementary and alternative therapies. Overall, however, studies show that the best likelihood of a successful treatment outcome is greater when conventional treatments are combined with CAM therapies, compared to the use of CAM therapies alone. Still, there are documented cases of cancer patients who successfully achieved and maintained remissions by using only CAM therapies. Ultimately, the choice and responsibility for which treatment option to take belongs to the patients themselves.
Complementary Treatments That Can Be Enhanced By PEMF Therapies
Just as PEMF therapy can help to improve the effectiveness of surgery, chemotherapy, and radiation therapy, it can also enhance the effectiveness of various CAM therapies, whether they are used by themselves, or as part of an overall integrative treatment program that combines both conventional and CAM treatments for cancer.
What follow are some of the therapies that work well with and complement PEMF therapy. Because of space limitations, the descriptions below are fairly short and not in depth and serve mostly to highlight the relative aspects of these therapies and PEMFs.
Acupuncture:
Acupuncture is sometimes used for cancer patients because of its ability to reduce pain, boost immunity, and promote relaxation. Acupuncture has also been shown to reduce nausea caused by chemotherapy.
PEMF therapy can be used at the same time that acupuncture is being used. PEMF and other magnetic fields have been found to stimulate acupuncture points and meridians. Although acupuncture needles are temporarily stronger in action than magnetic fields, when the needles are applied along with PEMF, the therapeutic effects are even stronger.
Conversely, other acupuncture-related therapies, such as acupressure, cupping, and moxabustion, are not typically as strong in their actions as PEMF fields are. PEMF therapy is also an excellent alternative to acupuncture when acupuncture treatments are indicated for people who are not comfortable with the needles.
107 Super Charge Your Health To Protect Yourself Against Cancer
Since magnetic fields act more directly on cells and tissues through which they pass than acupuncture, acupuncture and PEMF can be used together to provide patients with the benefits of both modalities. For example, in the case of spinal arthritis, a deep joint problem that causes significant pain, multiple tissues are often involved. Edema can be, as well. PEMF therapy can effectively treat any edema in muscles, ligaments or nerves, as well as relax muscles and start cellular repair of both joints and other soft tissues.
At the same time, acupuncture will help reduce pain almost immediately and help a person relax. The secondary actions of acupuncture on the immune system and other hormone and repair mechanisms take more time to take effect and can easily be overwhelmed or reversed by other events in a person’s life or processes happening in the body after an acupuncture treatment. Combining both therapeutic systems will often result in the primary actions of both acupuncture and PEMF therapy being more active and more effective than waiting for the secondary actions of either therapy to kick in.
Based on my clinical experience as a practitioner of both therapies, I recommend that PEMF treatment be administered first, followed by acupuncture. However, many acupuncturists find benefits in doing both therapies at the same time. PEMF therapy will act on the body’s tissues directly, and rebalance all of its cells, while the acupuncture’s systemic actions will correct any blockages or imbalances in the body’s energy pathways (meridians) and organ systems. When the secondary effects of both therapies kick in, the overall therapeutic action of each therapy is greatly increased.
Chiropractic, Massage, and Physical Therapy:
Chiropractic manipulation and massage work directly on muscles, superficial soft tissues, and ligaments to reduce tightness, spasms, strains, and subluxations of the spine. These forms of bodywork help to stimulate acupuncture points and meridians, improve circulation to tissues, and relax muscles. Secondarily, massage works to flood the body with endorphins. Since many toxins and wastes are stored in muscles, along with a great amount of tension and related blockages of circulation, regular treatments with these therapies can help provide rapid structural relief and help most people to maintain better health. When appropriate, such therapies may be offered to cancer patients, although in some cases they may be contraindicated.
These therapies and PEMF therapy significantly improve the benefits of each other. As with acupuncture, when PEMF therapy is used in combination with these therapies, the greatest benefit will likely be achieved from using PEMF therapy first, followed by chiropractic manipulation, massage, or physical therapy. On the other hand, when there are mechanical problems, these may have to be resolved first before PEMF will be helpful to complete the work needed. For massage, PEMF therapy helps relax both
108 Super Charge Your Health To Protect Yourself Against Cancer
patients and their muscles before massage is started, thereby requiring less work on the therapist’s part to get deeper into tissues for much deeper stimulation.
Regular (ideally daily) use of whole-body PEMF therapy at home decreases the need for manipulation or massage by helping tissues remain detoxified and relaxed, while also keeping the cumulative physical effects of stress to a minimum. Even so, massage has more direct physical action on the muscles themselves than PEMF therapy, which is why the combination of regular local and/or whole body PEMF therapy and chiropractic, care, massage, or physical therapy treatments keep the body from aging as quickly and help to prevent musculoskeletal problems from developing or worsening. A growing number of chiropractors and other bodywork practitioners now offer PEMF therapy for this reason.
I would place osteopathic manipulation alongside these other therapies in terms of potential PEMF therapy use and how to think about it as discussed above.
Infrared Therapy:
Infrared is invisible radiant energy and is part of the electromagnetic spectrum. Its wavelengths are longer that those of visible light, but significantly shorter than the wavelengths used in PEMF devices.
The two types of infrared therapy are far infrared (FIR) and near infrared (IR). Infrared is primarily used to generate heat in tissues. In addition to generating heat, FIR/IR also introduces high frequency EMFs into the body. Infrared does not typically penetrate the body deeply, with a FIR/IR signal usually dissipated within one to two inches into the body because of the natural drop-off of the intensity of these high-frequency stimuli. High frequencies dissipate into the body very rapidly, while heating the tissues along the way. This is one of the reasons why FIR/IR is used in saunas to detoxify the body, primarily through the skin. Such detoxification strategies can sometimes be useful for helping cancer patients eliminate stored toxins in their body that can exacerbate cancer.
There are both passive and active FIR devices. The active infrared systems are driven by using electrical line current and tend to create more dynamic action in the body than the passive systems. Active systems are most commonly used in health practitioners’ offices. The passive systems are usually designed for personal or home use, and radiate FIR signals using either ceramic or fiber materials. FIR systems have been designed for whole-body applications, including in saunas, blankets, covers, clothing, and others. Active FIR, especially applied to the whole body, tends to generate more heat in the tissues than passive FIR. ELF PEMFs usually penetrate the body more completely without loss of signal, as opposed to higher frequency FIR/IR, which get absorbed by the tissues.
FIR/IR in all formats can be used alongside PEMFs to obtain additional health benefits. The person is essentially going to be getting a broader spectrum of frequencies and
109 Super Charge Your Health To Protect Yourself Against Cancer
intensities when these modalities are combined. FIR/IR will help local, superficial musculoskeletal problems more dynamically and quickly than many PEMFs, especially low PEMF intensity systems. This means that if someone owns a whole body PEMF system, they can still use an FIR sauna or a local FIR/IR treatment device.
For cases of acute arthritic or musculoskeletal problems I am more inclined to use FIR/ IR to start with for several treatment sessions, followed by longer-term PEMF management, especially if I think the underlying problem is or is likely to become more chronic.
Some FIR/IR systems use red colored diodes for their IR signals. In order to generate current to the diode, AC current may be modulated in such a way as to introduce ELFs as well as the diode frequencies into the body. This makes such a device a dual treatment system that uses IR and ELF simultaneously. This type of system would be expected to be even more dynamically acting than simple FIR/IR by itself, especially if it’s higher intensity.
As with many other therapeutic approaches, I recommend using PEMFs before using FIR/IR if they are going to be used on the same day. However, FIR/IR may help superficial acute problems more quickly than PEMF therapy, so in the case of an acute injury, I recommend using FIR/IR first and following that with PEMF treatment. If the FIR/IR creates a significant amount of tissue reactions, then PEMFs can also follow the FIR/IR treatment. Otherwise, PEMF therapy can be used first and FIR/IR therapy used afterward.
Laser Therapy:
There are two types of laser therapy systems. One system is tissue destructive and used for ablation of tumors, and to treat and remove skin lesions, including cancer lesions. The other system enhances tissue healing.
There are two types of this latter system: high intensity and low intensity. The low intensity systems are known as low-level or cold laser. The high intensity laser equipment tends to be very expensive and mostly affordable by practitioners. Most very effective low-level lasers are also expensive and are used primarily by professional health practitioners. There are some less expensive home-based systems available, which unfortunately also tend to be very low intensity and less effective.
Low-level lasers are often used in a similar way to FIR/IR. Their beam is very narrow and focused. Because of this level of intensity, they are able to penetrate the body more deeply than FIR/IR and can often even pass through less dense superficial areas of the body, such as the hands. More expensive professional models with much higher laser intensities are more likely to penetrate deeper, thicker body parts, such as the abdomen or lung. Lasers may be used with different colors and therefore have the combined benefits of the laser frequencies along with the color benefits. Most therapeutic lasers emit red.
110 Super Charge Your Health To Protect Yourself Against Cancer
Unlike FIR/IR, laser therapy is used primarily for local area applications that most typically have to be applied by professionals. PEMFs can be used alongside laser therapy. Because of the intensity, very high frequency, and focus of the laser beam, PEMFs are useful for wider and deeper areas of treatment and will interact with tissues at lower frequencies. Low-frequency PEMFs penetrate the body completely, but lasers tend to be more superficial in their depth of penetration. In addition, lasers cannot be used safely around certain body structures, such as the eyes and brain. For the most part, PEMFs do not have these limitations. PEMFs can be used simultaneously with low-level laser therapy, or before or after.
Light Therapy:
Active light therapy can include lights or lamps that radiate specific colors, having colored crystals applied, use natural spectrum lighting, and so on. Light therapy is generally administered as a whole-body treatment approach. Specific colors are used to generate specific actions and reactions in the body. Lighting systems, like with laser and infrared systems, are limited by the thickness of the tissues exposed. They are also often blocked by clothing.
When light therapy is administered, there is a significant amount of attenuation, absorption, and diffraction of light as it moves into the body. Many of the light’s resonant effects are due to the stimulation of the optical nervous system and not the tissue directly. For these reasons, PEMFs would not be expected to interfere with light therapies and may be used concurrently with them. Some research also indicates that PEMFs may act like light therapy, even though their frequencies are considerably lower.
To avoid frequency interference, I recommend that PEMFs be used prior to light therapy if used on the same day. When combined, both therapies would be expected to have a beneficial, synergistic effect.
Hypnosis, Counseling, and Psychotherapy:
Each of these categories of therapies can be extremely helpful for cancer patients in terms of managing their fears and anxieties related to their diagnoses, and for managing their stress levels. In addition, they can also aid in helping patients marshal their inner resources to create a more positive mindset and as an aid for visualization and guided imagery, the benefits of which for cancer patients was proven by Dr. O. Carl Simonton and others (see Chapter 4).
I have worked with many practitioners who combine PEMF therapies along with psychological approaches. Most PEMF systems cause people to become relaxed. There are specific PEMF devices which have selectable frequencies that can be specifically used to tune the brain into different levels of relaxation, from light to very deep. PEMFs can be also used for stress reduction. Then, because PEMFs help make people more relaxed, they can
111 Super Charge Your Health To Protect Yourself Against Cancer
more effectively participate in psychological therapy approaches. In this case, I recommend doing PEMF therapy before and/or during psychological therapies.
Ozone Therapy:
Ozone therapy is an increasingly common cancer treatment option employed by a growing number of integrative oncologists and other integrative physicians today. Many of the effects of ozone therapy are comparable to effects of PEMF therapy. Deep ozone therapy needs to be administered by a skilled professional.
Ozone works internally to create the production of oxygen in tissues. PEMFs also improve oxygenation and circulation.
To be effective, ozone has to be absorbed by the tissues, enter the circulatory system, then be distributed to tissues. By the time the ozone gets into the tissues, it may be diluted dramatically. Because PEMFs will assist in this dispersion, we recommend these therapies be combined to improve effectiveness.
Homeopathy:
Homeopathy is based on an almost completely different set of principles than magnetic field therapy, although both can be resonancy-based. Homeopathy relies on principles of similar resonance. To be effective, homeopathic remedies must resonate with the symptoms of the person being treated.
While homeopathy has not been proven to be effective as a treatment for cancer itself, research does show that it can help to boost immune function, improve energy and overall well-being, and ease certain side effects of chemotherapy and radiation therapy, such as nausea, infections, and mouth sores. (Kassab S, et al. Homeopathic medicines for adverse effects of cancer treatments. Cochrane Database of Systematic Reviews 2009, Issue 2. Art. No.: CD004845.; Frenkel M. Is There a Role for Homeopathy in Cancer Care? Questions and Challenges. Curr Oncol Rep. 2015 Sep;17(9):43 )
PEMFs produce frequencies or magnetic fields that could potentially interact with the frequencies of homeopathic remedies. In addition, PEMF frequencies are typically much lower than those of homeopathic remedies. This means that PEMF frequencies likely interact with homeopathic remedies as a result of harmonic resonance where their frequencies overlap. Even so, the likelihood of significant harmonic interaction is probably very low.
Since it is not known for certain whether homeopathic remedies can be canceled out by PEMFs, I recommend that homeopathics be used at different times. Preferably, patients should receive PEMF therapy first. In fact, several days of PEMF therapy use may very well help to clear the body’s internal terrain and “static” before homeopathy is used.
112 Super Charge Your Health To Protect Yourself Against Cancer
In addition to the above therapies, PEMF therapy can be used with many other therapeutic, energetic, and resonance therapies. Generally speaking, PEMF therapy is safe for use with most other modalities and is usually best applied before any other resonance therapies are used on the same day.
In my own clinical practice, I regularly employed or recommended PEMF therapy along with the therapies discussed above, and consistently found that adding PEMFs to my patients’ overall treatment plans improves the benefits of the other therapies. I also encouraged my patients to consider purchasing their own PEMF systems so that they can continue to obtain the benefits of PEMFs on their own, while also helping to sustain the benefits they receive from the other treatments they receive.
I hope that this chapter furthers your understanding of just how versatile and valuable PEMFs can be for improving your health.
113 Super Charge Your Health To Protect Yourself Against Cancer
Choosing PEMF Devices and Systems
Based on my many years of researching and using PEMF systems and experiencing the many health benefits they provide, both for myself and for my clients, I’ve learned that owning your own PEMF system is one of the best things you can do to maintain good health and help resolve any health problems you may have. As this book makes clear, PEMF therapy offers many supportive benefits for both preventing and helping to manage cancer, which is why I encourage all people with or at risk for cancer to consider PEMF therapy for home use.
Going for professional help can be extraordinarily useful. However, owning your own PEMF system that is right for your needs gives you the most flexibility to better control your health.
People buy PEMF systems for specific needs that make sense at the time, but PEMF systems are likely to be useful for unexpected, or even expected, health needs long into the future. This is particularly true for people dealing with cancer.
There are two major advantages of owning a PEMF system—convenience and cost savings over time.
The best results from PEMF therapy are achieved from daily treatments, ideally for at least 30 minutes twice a day. But in some cases treatments times may need to last much longer than that—in some instances, even 24 hours/day using portable, battery-operated devices—for meaningful and lasting results to occur. Having the ability to provide yourself with regular, ongoing treatments is simply not possible if you have to rely on your physician or other health care provider to administer PEMF treatments for you. Even scheduling treatments once a week with your provider may not be practical if he or she has a busy practice, as most clinicians do. Moreover, it is also unlikely that your scheduled appointment will last for the necessary amount of time required for a PEMF treatment to benefit you.
Then there is the cost factor involved in receiving professional PEMF treatments. Even if it were practical for your health care provider to provide you with daily PEMF treatments, the costs you would incur would be prohibitive over time, both because PEMF therapy is typically not covered by health insurance and has to be paid for out-ofpocket, and because of the fees providers charge for such treatments due to the expenses involved running a medical or health care practice, which are far greater than most patients realize.
114 Super Charge Your Health To Protect Yourself Against Cancer CHAPTER 11
Like all other patient and client services, when it comes to PEMF treatments, pricing structures must be based so that they help meet the economic needs of the overall medical/health care practice. This means that, even if it was possible for you to achieve daily PEMF treatments at your practitioner’s office, after a single month of five treatments per week, you would have paid at least $400.00, assuming a very low cost per treatment of $20.00, although in reality, the cost of a single professional treatment is likely to be more than that. At that rate, you could buy many of the various PEMF systems available for consumers in a matter of months.
Exceptional Price-Per-Day Value:
There is a large difference in pricing for the various PEMF systems I recommend. Units intended for use at home can range from as little as a few hundred dollars all the way up to $20,000 and more. Whole-body systems are more expensive, but they are also more complex and treat more of the body.
The true value of owning your own PEMF system is that it is a one-time purchase that can be used by you and your entire family for a vast range of needs in the comfort of your home for years to come. There are no refills, no co-pays, no fighting with insurance companies, no need for each family member to have a different system, and no need to take time off to schedule and travel to receive your treatments. When you factor in a lifetime of at-home daily, or at least regular, use of whichever system you might purchase, PEMF units are an exceptional value.
Whole-Body System Or Local PEMF System?
Because the purchase of a PEMF system is both a short-term and a long-term investment in your present and future health, it’s important to consider not only what is motivating your decision now but also to consider and plan for how the system you consider purchasing might help you with your future health needs.
Since the PEMF system you buy will be available to you for years to come, it is worthwhile to think about getting a system with more features and options than systems you might consider just for the short term. In line with that, once you decide to purchase a system, you next need to decide whether you need a whole-body PEMF system or a local PEMF system. A local system will have applicators that are basically only useful for treating one small area of the body at a time, such as a hand, knee, elbow, foot, part of the shoulder, part of the back, prostate, bladder, or neck, whereas a whole-body system with a long and wide pad applicator will typically treat your entire body.
Whole-body PEMF systems are usually used for health maintenance, and can provide more benefits more easily and quickly because they allow you to treat several local areas of your body at the same time. Another advantage of whole body PEMF
115 Super Charge Your Health To Protect Yourself Against Cancer
systems is that they have smaller pad-type regional applicators that can be used separately from the whole-body pad. This allows you to treat a local area of your body, such as your abdomen, chest, pelvis, hips, shoulders, or upper or lower back. Regional applicators are sometimes called pillow applicators and come in various sizes depending on the whole-body system you choose.
Deciding Which Magnetic Field Intensity Will You Need:
After deciding on whether you wish to purchase a local or whole-body PEMF system, your next most important decision will usually be determining what level of magnetic field intensity you need. Lower intensities may work well for superficial problems in tissues that are not deep in the body, such as the hands, elbow, shoulder tendinitis, carpal tunnel, heel spurs, eyes, teeth, or TMJ. Higher intensity local PEMFs are needed for problems deeper in the body, such as in the brain, spine, prostate, bladder, hips, knees, heart, lung, gallbladder, pancreas, kidneys, and bones. Local treatment PEMFs can range in maximum intensity from 10 Gauss to around 10000 Gauss. If you want to do whole body and regional treatments with the same PEMF system, intensity also becomes very important. Regional applicators can range in intensity from less than 1 Gauss to 7000 Gauss.
Long, body length pads that come with whole-body systems almost always operate on lower intensity fields than local or regional applicators or pads. Knowing the intensity of each applicator is therefore important before you decide which type of system to purchase. There are several choices among whole-body PEMF systems ranging in intensity from < 1 Gauss (< 100 micro Tesla) to 500 gauss or more. The general rule of thumb is that the higher the intensity, the faster the results, and the less the treatment time that will be necessary to achieve them.
Many people make their decision based on the cost of a PEMF system, often sacrificing results that might be better and more rapidly achieved by more expensive systems. Results are often promised by manufacturers and distributors of very low intensity PEMF systems that ignore the research studies showing that higher intensity is needed. To learn more about these proven intensities, please see my books Supercharge Your Health With PEMF Therapy and Power Tools For Health, as well as the blogs and videos available on my website, www.DrPawluk.com.
After you have decided on what type of PEMF system you want (whole-body versus local), and the magnetic field intensity you need, other factors to consider to further narrow down your choice of a specific system include frequencies, applicator shapes, whether the system is portable or AC powered, and whether rentals are available. Advice about the variety of PEMF options available to you can be obtained by contacting my team and me at www.DrPawluk.com. We will be more than happy to help you sort out all the PEMF options on the market.
116 Super Charge Your Health To Protect Yourself Against Cancer
Beware Of Scams And Outright Lies
Unfortunately, not all claims made by certain PEMF manufacturers and distributors are reputable. When people are misinformed, it is easy to be taken in by inflated claims and purchase PEMF systems that seem legitimate, but are in reality ineffective for the specific problem or problems that you may have. The truth is that any PEMF device is likely to have some benefit to health, but it may not provide the level of benefit you need or are looking for. Understanding this is most important for people with cancer or other serious illnesses.
Even medical professionals have to do extensive research to really understand the science behind PEMF therapy. Conventional medical training simply doesn’t include this information. If your only source of information about PEMFs is a general internet search, you probably won’t have the knowledge you need to make the best selection. Empowering you with that knowledge is why I wrote this eBook and my above-mentioned books, and created DrPawluke.com and its blog articles, videos, and much other informative and educational material on that site that is regularly expanding.
What follow are the most common claims made by some PEMF companies whose primary interest seems to be making money, not helping people.
FDA Approval Is Necessary/Best:
Most manufacturers of PEMF devices actually choose NOT to seek FDA approval. Why? Because such approval is far too limiting. If a device is FDA approved, there are strict parameters around what it can be marketed for. There must be clear research to support the claims and research is expensive to conduct. Moreover, if a PEMF device is FDA approved for a particular use, it manufacturer can’t claim it provides other benefits, even though most PEMFs do.
Also don’t be confused by claims of PEMF systems being FDA registered either. All that means is that the FDA knows the device is being imported into the USA, and all imported PEMF machines have to be registered, whether that information is part of the manufacturers marketing plan or not.
Claims That A PEMF Device/System Is The Best One On The Market:
The truth is there is no one best unit. You can’t find a one-size-fits-all model, or even a model that is best for most people. The PEMF device or system that is best for you will depend on what you need it for now, and perhaps how you might use it in the future. Manufacturers love to make claims that their machine is the best on the market. It might be for specific purposes, but not for the broadest range of needs.
PEMF Machines Can’t Be Used For Cancer and Other Specific Conditions:
PEMF devices are first and foremost wellness devices. Magnetic field therapies are safe for almost any application when used properly, even at very high intensities,
117 Super Charge Your Health To Protect Yourself Against Cancer
such as those used by an MRI machine. Although some people or manufacturers/ distributors might claim that you shouldn’t use PEMF therapy in conjunction with certain medications or with certain health conditions, including cancer, there is very little evidence that PEMF therapy causes any significant adverse effects. In fact, the opposite is true. Ample evidence exists that shows that PEMF therapy can be a very effective complement to most other treatments, including cancer, as you learned from the research studies I covered in Chapter 9.
Only One PEMF Device Will Work For You:
Again, some manufacturers will say almost anything to get you to buy their device. But the truth is there are many devices available on the market, and if you understand what signal intensity and coil configuration you need, many different PEMF systems can offer relief for cancer and other conditions. In making a purchasing decision you may want to be made more comfortable by knowing whether a device has research behind it or whether it can be effective for specific conditions. Unfortunately, even though there are thousands of research studies about PEMF effectiveness, there is never enough research to satisfy all questions. Research is expensive and it’s nearly impossible to find evidence for every PEMF system out there, which is why basically understanding frequency and intensity, as well as whether you need a whole-body system or a local, targeted system, is so important. I often say that whatever PEMF system you use will benefit your health at least to some extent, regardless of specific conditions. That’s because the overall positive effects on your body will at least indirectly help you cope with most specific conditions. Your body will decide what benefits it will see, and how quickly. This will depend on the PEMF being used, the starting point in the disease process, how aggressively treatment is done, and many other factors. But, you have to start somewhere.
Working With A Trained Professional Is The Best Way To Find The PEMF Device That’s Right For You
Because there are so many factors involved in selecting the best PEMF device, I always recommend that you work with a physician or medical team that is knowledgeable about and trained in the use of PEMF therapy. I have studied PEMF therapy for years, and I am always happy to help you make the right selection. Call my office or apply for a complimentary consultation if you are considering purchasing a PEMF device. (Visit www.DrPawluk.com/consultation.)
My team and I can help you make the best choice for you Scientific
118 Super Charge Your Health To Protect Yourself Against Cancer
Appendix
Electromagnetic fields (PEMFs) in the management of cancer:
A comprehensive review of the subject of cancer and PEMF therapy
I am one in the Love and in the Light of our Infinite Creator.
- Mantra
We shall not cease from exploration and the end of all our exploring will be to arrive where we started and know the place for the first time.
-T.S. Eliot, Little Gitting, 1942
We are not human beings having a spiritual experience, we are spiritual beings having a human experience.
- Pierre Teilhard de Chardin, philosopher and Jesuit priest
Summary
This e-book primarily focuses on the application of Pulsed Electromagnetic Field (PEMF) therapy in cancer care, with a particular emphasis on its role in modifying the cancer microenvironment. The book aims to educate both individuals with cancer and their care providers about the potential benefits of this relatively unknown, yet impactful, treatment option.
PEMF therapy, which has been available for over 40 years, is a complex concept that is often misunderstood due to the influx of equipment and misleading claims in the market. This confusion is further compounded by a lack of understanding of the extensive research available on the subject.
The book underscores the importance of PEMF therapy in all stages of cancer care, from prevention to palliative care. It highlights how PEMF therapy can effectively address many physiological actions, the breakdown of which are common to all health conditions, including cancer.
119 Super Charge Your Health To Protect Yourself Against Cancer
The therapy is particularly significant in the context of the cancer microenvironment. It relies on the body having adequate resources to make necessary changes in this microenvironment. PEMF therapies can contribute to the cancer care process by dealing with inflammation, supporting the immune system, improving tissue circulation and oxygenation, and decreasing the impact of physical contributing factors such as obesity and stress.
Moreover, PEMF therapies have been shown to have direct actions on cancers themselves by augmenting the body’s immune reactions. They also help to deal with the toxicities and damage caused by many of the therapies used in conventional cancer care today.
The is e-book also emphasizes the need for other lifestyle changes to give the body a better fighting chance against cancer. These include optimized nutrition, appropriate supplements, removing risk factors, adequate rest, effective mind-body interventions, and medical therapies as necessary.
We conclude by recommending daily home use of appropriately dosed PEMF equipment for optimal results. It also acknowledges the need for more research to further optimize the use of PEMF therapy in cancer care.
Introduction
I’m sure I don’t have to tell you how important cancer is to human health. It is the 2nd most common cause of death in North America behind heart disease. For now, very few cancers are curable and there is a constant search for new treatments in the continuing “war on cancer.” The war wages on.
Most conventional therapies for most cancers are best for the early stages of presentation. In the later stages, stages 3 and 4, most medical therapies fail and only, often at great cost, extend life by a matter of months. So, there is a huge need to find therapies that can help with the management of cancer, even though they may not cure them. This is especially important if these therapies are non-toxic, noninvasive, inexpensive and have value or benefit.
Chronic diseases are defined broadly as conditions that last 1 year or more and require ongoing medical attention or limit activities of daily living or both. Chronic diseases such as heart disease, cancer, and diabetes are the leading causes of death and disability in the United States. Six in 10 adults in the US have a chronic disease and for him 10 adults have two or more. (CDC) In the United States, 1.7 million people are diagnosed with cancer every year. 600,000 people will die from cancer every year. One in three people will have cancer in their lifetime.
In this e-book I have provided considerable background information on current biological considerations in the care of of cancer and most recent information relating
120 Super Charge Your Health To Protect Yourself Against Cancer
to the tumor microenvironment, the role of inflammation, the risks of inadequate circulation to and within tumors leading to low oxygen (hypoxia) environments, nutrition and complementary therapies, the use of HBOT (hyperbaric oxygen therapy), cancer stem cells, the role of obesity and metabolic syndrome, the development of bone metastases, and the possibility of spontaneous regression and the factors potentially contributing to that possibility. At the end, I reviewed the scientific research evidence supporting the use of PEMFs in the management of cancer. I have provided references to all of this information as well.
Breast cancer aspects and survival
Table 1 shows the overall survival (OS) and the breast cancer specific survival (BCSS) of women by age group. The % is that for each age group. The HR is the hazard ratio, that is, the risk of survival. And HR of 1 is neutral. A number below 1 favors survival whereas a number over one decreases the chances of survival. Clearly, someone over 80 has decreased chances of overall survival then someone under 40. Overall survival depends on many other factors that could contribute to dying, including other diseases, accidents, genetics, etc. BCSS is death specifically attributed to the breast cancer itself. As can be seen, the HR’s above age 60 are considerably less for BCSS than OS.
Table 1. Analysis of overall survival in breast cancer specific survival across different age groups
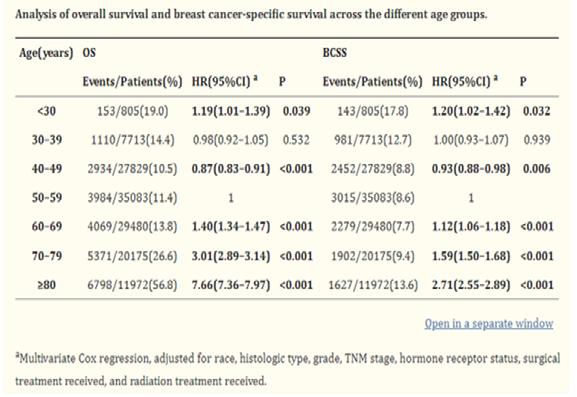
FROM: Chen
121 Super Charge Your Health To Protect Yourself Against Cancer
Figure 1. Cumulative overall and breast cancer specific survival probability over 120 months for young, middle-age, and elderly groups
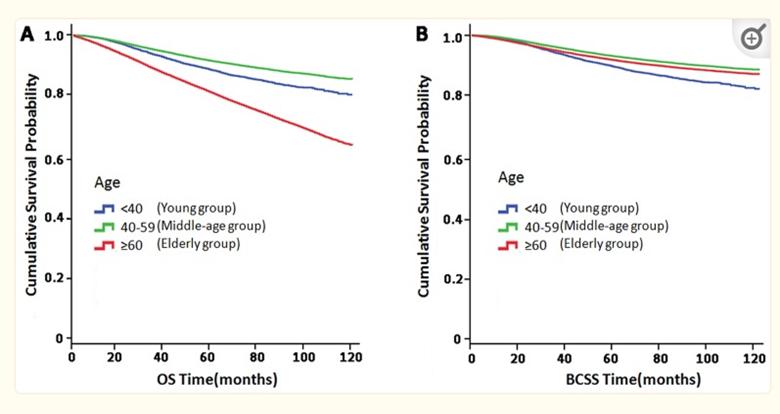 FROM: Chen
FROM: Chen
This figure shows graphically what was presented in table 1 above. The elderly group have lower survival rates than the other two age groups. For BCSS in figure B above shows a significantly smaller gap between the age groups, due to the risk to overall survival from other factors, other than breast cancer, being higher.
Figure 2 shows the effect of radiation therapy to the breasts after breast cancer surgery on isolated local cancer recurrence and breast cancer-related mortality over the next 15 years in 6097 women who were lymph node negative or 1214 women who were lymph node positive. In those with lymph node negative disease, 16% more women developed local recurrence at 5 years and 19% more at 10 years if there was no local radiation therapy and the difference in breast cancer mortality at 15 years was greater by 5%. In lymph node positive women, the difference was 30% at five years and 33% at 10 years and the difference in breast cancer mortality at 15 years was greater by 7%. This data was derived by combining results from 10 clinical trials. There is no information on whether any of these studies looked at the use of complementary and alternative medical (CAM) therapies in any of these women. There is more information later in this e-book on the use of CAM for cancer. To what extent CAM can impact these results and allow a woman to avoid radiation therapy without major risk to the development of recurrences or impact mortality is unknown. There is some information later in this book about studies done in Russia using PEMF therapies which may give some indication of the possible benefits of PEMF therapy and the associated risks of avoiding conventionally recommended care.
122 Super Charge Your Health To Protect Yourself Against Cancer
Figure 2. Effect of radiotherapy (RT) after breast cancer surgery on local recurrence and on breast cancer mortality – 15 year probabilities.
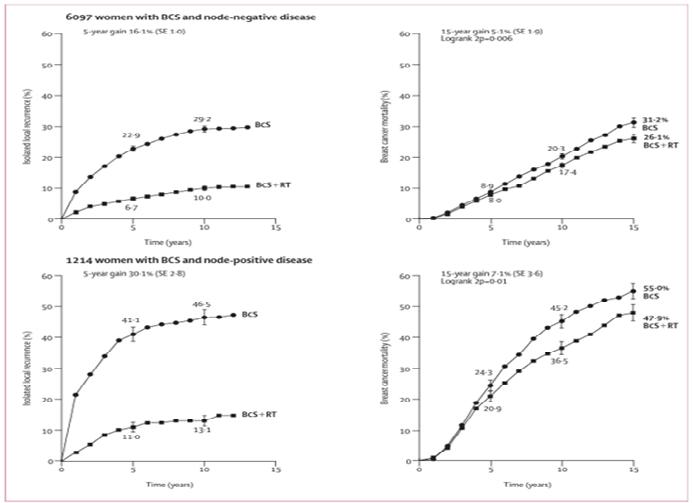
FROM: Clarke.
Characteristics of cancer cells
● Become self-sufficient and growth signaling and have a limitless potential to replicate.
● Become unresponsive to anti-proliferative signals.
● Evade apoptosis.
● Induce and sustain angiogenesis.
● Invade and metastasize.
● Sustain and grow by taking over the metabolism, hijacking, altering the microenvironment, starving healthy tissue: inducing hypoxia, anaerobic glyconeogenesis
Cancer cells/tumors’ influenceenzymes, gene proteins, and growth hormones, which in turn are most often over expressed/under at the fight.
The immune system: suppressing and/or blocking components of the immune system that can effectively attack cancer while increasing other components that enable cancer to multiply and spread [down regulating TH1 and up regulating TH2cancer cell adaptation.
Cancer cells crowd out other cells locally and cut them off from oxygen-carrying blood vessels necessary for their survival. When this happens, some cancer cells have developed the ability to bypass the need for oxygen and instead switch to the glu-
123 Super Charge Your Health To Protect Yourself Against Cancer
cose dependent glycolytic pathway. They use the glycolytic pathway even when oxygen is restored, by blocking one of the enzyme glycolytic [sugar feeding] pathways. Blocking lactose dehydrogenase-A (LDHA)may be an effective anti-cancer therapy. This is still investigational and there are no commercially available non-investigational products.
Cancer cells suppress or alter the immune system in order to facilitate growth and to avoid conflict.
Normal versus cancer cell growth factors
Normal cells: while similar to cancer cells, the amount is more in balance to produce a more normal level of activity.
Cancer cells:
● These cells have overproduced, require more chemicals [food - sugar/iron and copper], and are overactive.
● Compared to normal cells, cancer cells excrete increased levels of acid - related byproducts [acidosis], inducing a cancer conducive environment, and lactate. This alteration is one of the contributing causes of late-stage cancer-related pain.
In a paper called The Hallmarks of Cancer (Weinberg),it was recognized that cancers occurred through a series of mutations in many genes. Despite this, they listed six other essential alterations in cell physiology that characterized malignancy.
1. Self-sufficiency in growth signals: cancer cells acquire an autonomous drive to proliferate - pathological mitosis - by virtue of the activation of oncogenes such as ras or myc.
2. Insensitivity to growth-inhibitory (antigrowth) signals: cancer cells inactivate tumor suppressor genes, such as Rb, that normally inhibit growth.
3. Evasion of programmed cell death (apoptosis): cancer cells suppress and inactivate genes and pathways that normally enable cells to die.
4. Limitless replication potential: cancer cells activate specific gene pathways that render them immortal even after generations of growth.
5. Sustained angiogenesis: cancer cells acquire the capacity to draw out their own supply of blood and blood vessels - tumor angiogenesis.
6. Tissue invasion and metastasis: cancer cells acquire the capacity to migrate to other organs, invade other tissues, and colonize these organs, resulting in their spread throughout the body.
124 Super Charge Your Health To Protect Yourself Against Cancer
Breast cancer growth and development
This figure shows graphically a breast cancer tumor.
This drawing (FROM Camerondepicts a cross section of a human breast cancer tumor. The tumor has a well vascularized capsule. An outer cortex underlies the capsule for 100 to 150 μm. Immunohisto-chemistry shows that a hypoxia inducing factor (HIF)-α rich subcortex region is present at distances greater than 100 to 150 μm from blood vessels. The HIF producing region is thought to produce VEGFs causing an observed sprouting of endothelial cell growths and neo-angiogenesis. Cells further away from this neo-angiogenesis zone lack essential nutrients and oxygen and become necrotic (in the center of a cancer).Thus, this angiogenesis process is proposed to be hypoxia driven and is also proposed to be a main target of therapeutic PEMF therapy.
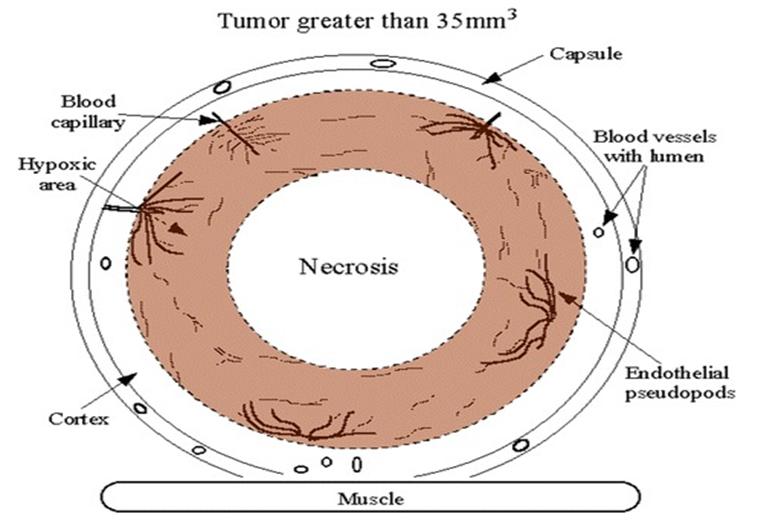
FROM: Cameron
The evaluation and time course of breast cancer growth and development is covered extensively by Engel. Growing and developing primary tumors (PTs) may have already disseminated DNA and circulating tumor cells (CTCs) to form local or distant small spots of cancer because of alterations in the local tumor microenvironment. The median growth periods for the primary tumor(PT) is 12.5 yrs, time to show metastases (METs) is ~9 yrs.,local recurrence shows up in ~5 yrs and regional lymph nodes show up in ~4 yrs. (Engel) Primary tumors can begin metastatic spread at from about
125 Super Charge Your Health To Protect Yourself Against Cancer
Figure 3: Cross section of a human breast cancer tumor.
1 mm tumor diameter. Even if 30% of METs only appear after 10 years, this follows a usual pre-diagnosis MET initiation pattern and does not indicate a delayed process. The growth times of PTs and METs vary by a factor of 10 or more but their ratio is robust at about 1.4. This means that faster growing PTs will end up having faster developing METs, by a ratio of 1.4.
In the case of breast cancer-related death, about 70% have a documented metastasis. It’s especially important to know that with every millimeter (mm) of primary tumor growth, more and more metastases are initiated. As PTs grow, they are associated with worsening prognosis. Until the initial tumor is resected, all tumor cells that can start secondary METs have already become disseminated. Only conversion to dormancy could delay the onset of METs.
When tumor cells leave the PT but remain close to the PT, they can initiate local recurrences. These usually occur within 3 cm of the original tumor. This 3 cm radius isthe usual target area of radiation therapy.If radiation is not used, 39% will have local recurrencesafter breast conserving surgery.The proportion of detected CTCs and micro-METs is a function of PT diameter.
About 13% of PT-related deaths happen in the first 15 years. When the PT tumor diameter is ~28 mm, the METs are already initiated up to a tumor size, and~25% of these new METs are not able to be destroyed by adjuvant therapies. When a local recurrence (LR) occurs, the time for METs to be found is about 4.2 years.
Different areas of a PT can be a source of circulating tumor cells (CTCs).Women with breast cancer patients have a 3-5 fold risk of developing secondary primary tumors compared to the normal population. Initial PT growth tends to generally be quite slow. When mammography screening begins at age 50 and over, 4% of PTs are not yet detectable although already present and will become obvious in the next 12.5 years.
The growth time of METs not only includes the time after the PT diagnosis but also time leading up to the PT diagnosis. For the simplest PTs, the total MET-free time in about 30% of METs is >10 years and a median of 6 years. MET growth varies similarly to PT growth. Post-MET diagnosis, survival is about 2 years and the time to initial MET diagnosis is estimated at 8.8 years. The ratio is 4.4. The longer a PT disseminates, i.e. the larger the PT, the longer the occult MET growth and the shorter the MET-free survival time. This is a growth-dependent metastasis principle.
The practical application of this information is that it appears to be best to remove a detected tumor as soon as possible, whether or not radiation or chemo are added.
126 Super Charge Your Health To Protect Yourself Against Cancer
METs occur 35% of the time without positive lymph nodes (LNs). The number of LNs is the most important clinical prognostic factor. When there are 0, 2, or 8–10 LNs, primary METs are diagnosed 0.7, 4, or 14% of the time, respectively.
Median post-MET diagnosis survivalis about 11 months. Complete pathological remissions of over 50% can be achieved with neo-adjuvant therapies (ATs) in a few weeks. LNs are not a cause of METs and therefore extended LN dissections cannot be justified. More aggressive diagnostics for METs during aftercare may not be useful because all secondary METs are already present, even if not obviously detected. This is the rationale for aromatase inhibitors. Thus, aromatase inhibitor (AI) prevention eradicates PTs quickly. Prevention with AIs successfully eradicates PTs of all sizes.
Overt METs are currently resistant to treatment. ATs over the past few decades have been able to achieve organ-specific MET eradication. As a result, METs in bone or lung are now about 50% or 30% less common. There is no evidence that liver and CNS METs can be eradicated. Much MET progression can now be explained by the effects of delays. If surgery is postponed, of great importance is that further METs and LNs are started with each additional millimeter of tumor diameter.
RADIATION: The eradication of occult local recurrences (LRs) by irradiation is excellent. Radiation therapies even make breast conserving surgery possible due to its efficacy in preventing faster growing LRs. Regional control of LNs is achieved with today’s surgical and neo-AT approaches making a LN relapse in < 5% during a time span of 15 years a rare event. Survival is optimal if no residual tumor remains after neo-AT primary and in the LNs. Thus, ATs also contribute to regional control because in the absence of an axillary dissection they act as neo-ATs on not removed LNs with isolated (tumor cell) TCs and micro-METs. The rapid eradications make intrinsic resistance in PTs and METs more likely than the concern for a therapy induced resistance.The CNS and liver are inaccessible.
Natural aromatase inhibitors
Neoadjuvant therapy (AT) is the use of therapy agents before a main treatment. One example is neoadjuvant hormone therapy prior to radical radiotherapy for cancer of the prostate. Neoadjuvant therapy aims to reduce the size or extent of the cancer before using a more radical treatment intervention. This is intended to both make procedures easier and more likely to succeed and to reduce the adverse consequences of a more extensive treatment, which would be required if the tumor were not reduced in size or extent.
Another related concept is that AT acts on any undetected micrometastatic disease dissemination present. This would be expected to result in improved longtime survival compared to a surgery and/or radiation alone strategy.
127 Super Charge Your Health To Protect Yourself Against Cancer
Aromatase inhibitors are prescription medicines that work by blocking the enzyme aromatase, the enzyme that converts androgens produced by the body into estrogen. Aromatase inhibitors are used in the treatment of breast cancer to reduce levels of circulating estrogen. This means that less estrogen is available to stimulate the growth of estrogen receptor (ER) positive breast cancer cells, slowing or inhibiting the progression of these cancers. About 80% of all breast cancers are ER positive. Aromatase inhibitors are unable to prevent the ovaries from making estrogen, which means that they are only used to treat breast cancer in postmenopausal women.
There are three aromatase inhibitors: anastrozole, exemestane, and letrozole. Use of synthetic AIs significantly increases risk of cardiotoxicity, osteoporosis, fractures, bone pain, arthralgia, myalgia and ≥ grade 3 hot flashes. Extended AI therapy can reduce the risk of localized and distant recurrence, contralateral BC and secondary cancer, and prolong disease-free survival compared with non-prolonged AI therapy. (Huifang).
Since this research indicates that hormone suppression, i.e. aromatase inhibitors (AIs), are very helpful in the treatment of breast cancer, the question becomes whether there are natural approaches to providing these AI’s without resorting to synthetic compounds. These natural products that inhibit aromatase may be clinically useful for treating postmenopausal breast cancer. AIs may also act as chemo-preventive agents for preventing secondary recurrence of breast cancer. They may also be useful for primary prevention of breast cancer in postmenopausal women, given their lower toxicity and long history of human use. (Mereles) AIs may also have a role in breast cancer chemotherapy for postmenopausal women. In addition, these natural products are known as polyphenols. Most polyphenols are known to be powerful antioxidants and have anti-inflammatory effects. Polyphenols help fight cell damage caused by free radicals and immune system components. In particular, polyphenols are credited with a preventive effect that helps protect the body from certain forms of cancer. (Sufianova) One of the best studied AI compounds is epigallocatechin-3-gallate (EGCG). The daily limit for this has been recommended to be EGCG 338 mg/day in supplement form. The outside limit could be 704 mg/day (Hu) EGCG has also been shown to have numerous other health promoting effects acting through different pathways, as antioxidant, anti-inflammatory and anti-atherogenic agent.
While this may be promising, it would be more so if there was actual research to support a value for the use of EGCG for breast cancer chemoprevention or treatment. I couldn’t find any controlled prospective studies on the use of natural AI’s either for active treatment after diagnosis of breast cancer or as chemoprevention. There was one retrospective study looking at green tea consumption in women in Japan diagnosed with breast cancer. (Nakachi They found that increased consumption of green tea was closely associated with decreased numbers of axillary lymph node metas-
128 Super Charge Your Health To Protect Yourself Against Cancer
tases among premenopausal patients with stage I and II breast cancer and with increased expression of PR and ER receptors among postmenopausal ones. Increased use of green tea was correlated with decreased recurrence of stage I and II breast cancer (P < 0.05 for crude disease-free survival); the recurrence rate was 16.7 or 24.3% among those consuming > or = 5 cups or < or = 4 cups per day, respectively, in a seven-year follow-up. However, there was no improvement in prognosis for those with stage III breast cancer.
It would have to be a personal decision whether to substitute EGCG for the pharmaceutical AI’s and perhaps it may be best to consider their use when undesirable side effects happen. It’s also possible that using natural AI’s along with PEMF therapy, lifestyle changes and other complementary therapies may enhance the value of the natural AI’s.
Limitations of conventional chemotherapy
The distribution of many anticancer drugs in tumor tissue is incomplete, and strategies are needed that might be used to improve drug penetration through tumor tissue. (Minchinton) The tumor diameter is a major determinant of the ability of the drugs to gain access to the deepest areas of the tumors.
Figure 4. Cancer survival rates up to 20 years after diagnosis and treatment using chemotherapy
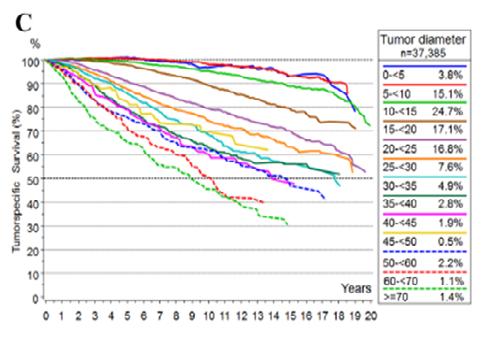 FROM: Minchinton
FROM: Minchinton
Survival clearly is worse as tumors get larger, ranging from less than 5 mm to over 70 mm (0.2 in-2.8 in)
Strategies that improve drug or even nutrient delivery or activity by targeting the tumor microenvironment, especially in low oxygen/hypoxic areas in tumors, represent an important future direction for cancer therapy. The possibility of improving therapy of solid tumors by increasing the tumor uptake of chemotherapeutic agents or other
129 Super Charge Your Health To Protect Yourself Against Cancer
therapeutics is by improving the tumor microenvironment and is getting major attention. While it is getting the most attention for chemotherapeutic drugs, the strategies using nutrients and supplements need to also consider these evolving oxygen enhancing strategies. (Choi)
Survivorship
Of the nation’s more than 10 million cancer survivors, more than six million have survived beyond five years, reports the National Cancer Institute. And some 14 percent, or more than 1.4 million, have lived more than 20 years beyond diagnosis.
(https://www.curetoday.com/view/what-five-years-really-means).
The reason people latch onto five-year survival stretches back to the years prior to World War II when very few people survived cancer. Five-year survival rates were introduced in the 1930s not to point patients toward notions of a cure, but because cancer specialists back then considered five-year survival a nearly unattainable goal.
When someone is first diagnosed with cancer one of the early questions will be “how long do I have?” For example, in colorectal cancer, 80% of the cancers recur within the first two years. In this setting, the concept of five-year survival may be reasonable to consider. As it is, the five-year survival rate for colorectal cancer 63%. For breast cancer, it’s about 86%. For lung cancer, about 15%. Prostate cancer has an even longer survival time span. For cancers with shorter-term likelihood of ”cure”, such as testicular cancer and some leukemias, if tumor markers are negative then it’s possible to consider the condition to be “cured” by the treatments. There are many factors involved in the likelihood of survival; not just the type of cancer, but also the aggressiveness of it, the age of the person and their background health, etc., when the treatments begin, subsequent lifestyle circumstances, and many more factors.
I have always had a concern about the term “cancer survivor.” In the fairly typical oncology community, survival is considered when somebody has survived death by five years or more. Many institutions do not routinely follow people beyond the fiveyear period, essentially claiming that beyond that time other causes of death become more prevalent. Therefore, surveillance and monitoring for recurrence and later progression to more advanced disease may not be deemed essential. The fact is that every day after the diagnosis of treatment, is important. Vigilance, optimism, and focusing on and implementing the many factors needed to better assure long-term survival are needed.
Most people who are diagnosed with cancer and treated become “different people” with many new factors in their lives becoming more important and with significant changes in lifestyle. These changed factors determine the environment or terrain of
130 Super Charge Your Health To Protect Yourself Against Cancer
the body that allowed the cancer to develop in the first place. “You” effectively become a different “you.” You need to shift from the “survivor state” to the “thriver state.” That is, you will need to shift your life to build many more positives into it and attempt to remove as many of the previous “negatives” as possible.
Your clinicians and professional team should be comfortable addressing and supporting the care of the long-term effects of the cancer and its treatment, including the toxicities from medications, radiation, hormone deficiency, chronic pain, fatigue, cognitive concerns, sleep issues and other psychosocial concerns. Your team should also promote health maintaining behaviors include a healthy lifestyle, treatment adherence and appropriate surveillance. All of this should be individualized to the “thriver’s” needs. (Moore)
Complementary or alternative care (CAM)
A high percentage of people with cancer use complementary, alternative and/or integrative care (CAM). Complementary medicine refers to treatments that are used in standard medical treatments, like using acupuncture to help with side effects of cancer treatment. Alternative medicine refers to treatments that are used instead of standard medical treatments. Integrative medicine is a total approach to care the combined standard medical treatment with the CAM practices that have been shown to be safe and effective. CAM among cancer patients in North America has been reported to be between 41-58%, depending on the specific patient population and the definition of CAM being used. (Horneber) However, these numbers can be somewhat misleading because CAM encompasses a wide range of therapies, including but not limited to dietary supplements, meditation, acupuncture, chiropractic care, and herbal medicines. When it comes to nutrition and dietary changes, these numbers may be considerably higher.
Effective CAM therapies – research-based evaluations
Based on a systematic review of scientific studies (Guerra-Martin), and nutrition is not considered, these were found to be effective CAM therapies, based on outcome comparisons:
● Auriculotherapy
● Acupuncture
● Laser
● Moxibustion
● Hypnosis
● Ayurveda
● Electroacupuncture
● Guided imagery
● Progressive muscle relaxation
● Phytotherapy
● Yoga
● Music therapy
● Traditional Chinese medicine
The US government provides regular “PDQ” updates on a number of CAM therapies (https://www.cancer.gov/about-cancer/treatment/cam/patient).
131 Super Charge Your Health To Protect Yourself Against Cancer
In another study from Yale (Johnson) where individuals refused CCT (7% refused surgery, 34% chemo, 53% radiation, 34% hormones), CAM was associated with poorer 5-year overall survival compared with use of CCT without CAM (82.2% vs 86.6%; P = .001). Figure 4 shows the survival curves over 84 mos.
Figure 5 Cancer survival results over 84 months for those refusing conventional cancer therapies (CCT) versus those receiving CAM.
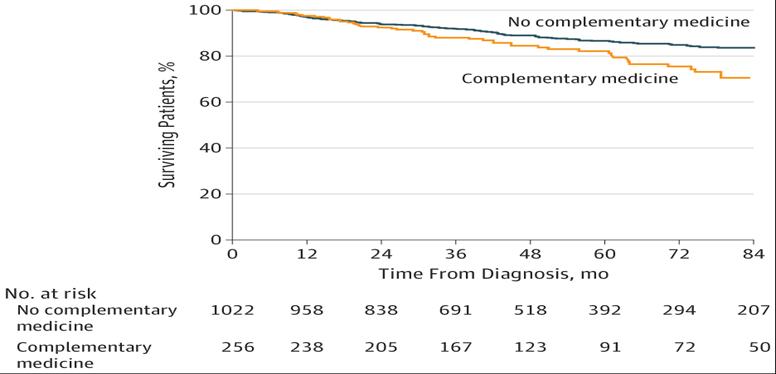 FROM: Johnson
FROM: Johnson
Not all is “bad news” for CAM use. A study of CAM use in 6 Phase III cancer therapy trials for Metastatic breast, colorectal, or lung cancers. Quality of life, adverse events, overall survival, and progression-free survival were compared between CAM users and non-users. 20% of participants in phase III trials were using CAM. (Wells) CAM use in breast cancer was 36%, colorectal cancer (CRC) 16%, and lung cancer 19%. The CAM group had more favorable baseline prognostic factors (ECOG 0-1, non-smoking status, younger age, and fewer metastases). They had lower adverse events (50% vs. 62%, P = .002); Quality of Life was similar. CAM had longer overall survival (OS) in those with lung cancer by about 20%, but not in CRC or breast cancer. The collective risk of progression was ~10% significantly lower with CAM (P = .024), especially in lung cancer ~20% (p= 0.005). But it was not lower in CRC or breast cancer.
Comparing CAM use with CCT for cancer is very complex and the results of these studies should be paid attention. CAM use is hard to define. There are certain to be significant differences among the various CAM uses and there appears to be significant opportunity for improving their value. Evidence-based technologies like PEMF may offer significantly better complementary, alternative and/or integrative care value.
Integrative cancer treatment is of substantial interest to many cancer patients. We report survival data for a consecutive case series of advanced metastatic breast
132 Super Charge Your Health To Protect Yourself Against Cancer
cancer patients who received a comprehensive clinical program combining conventional treatments with nutrition and supplementation, fitness and mind-spirit instruction at the Block Center for Integrative Cancer Treatment. Ninety consecutive patients with metastatic breast cancer diagnosed during 1984–1997 who received chemotherapy at the integrative cancer center were included. Prognostic factors, treatments and survival from onset of metastases were determined from analysis of scans, labs, pathology and medical records. The log-rank test and Cox proportional hazards analyses were used, and a Kaplan–Meier curve wascalculated. All patients had metastatic disease at baseline, 96% were relapsed and 52% had received prior chemotherapy for metastatic disease. Median age at onset of metastasis was 46 years. Median survival was 38 months. Published literature on populations with somewhat more favorable prognostic factors treated in conventional clinics showed median survivals of 20 to 23 months. Through the 1990s, median survival reported in metastatic breast cancer trials or observations generally ranged from 12 to 24months. Five-year survival was 27%forBlock Center versus 17% for comparison patients. Despite a higher proportion of younger and relapsed patients, survival of metastatic breast cancer patients at the Block Centerwas approximately double that of comparison populations and possibly even higher comparedtotrials published during this period. Explanations for the advantage relative to conventional treatmentalonemay include the nutritional, nutraceutical, exercise and psychosocialinterventions,individuallyorincombination;self-selectionof patientscannotberuledout. (Block)
Survival rates for cancer
Cancer.gov publishes survival rates in their SEER database. The five-year survival rates for all sites of cancer in 2011 or 66%. The lowest was for pancreas at 5.77%. Breast cancer was 89%, lung/bronchus 16%, colon 65%, and lymphoma 68%. The five-year survival rates can be dramatically impacted by comorbidities. For colorectal cancer for 2016, when there is no comorbidity the five-year probability of survival is 65% with about 35% dying from colon cancer. 14% will die from other causes. For those with severe comorbidities 34% will die from other causes. (From: https://seer.cancer.gov/ news/SEER-Cause-Survival.pdf)
So, when one is managing the care of cancer, the presence of comorbidities is critical to outcome, significantly complicating cancer care.
Mind-Body Medicine
I became aware of Dr. Carl Simonton’s work in the early 80’s. He was a radiation oncologist who noticed that patients given the same dose of radiation for similar cancers had different outcomes. He discovered that those who had a more positive attitude generally lived longer and had fewer side effects. He has been largely credited with starting the movement of the use of meditation and guided mental imagery in
133 Super Charge Your Health To Protect Yourself Against Cancer
cancer. He also recommended at least two years of counseling after diagnosis and treatment to lengthen survival. The thinking is that the whole process of diagnosis, treatment and so on are all very stressful. Stress leads to an increased risk of progression. This length of counseling helps to get past the shock of the diagnosis and treatment. In psychology, grief work often takes up to two years of counseling to resolve issues related to grieving. In a sense, the diagnosis and treatment of cancer, whether breast or otherwise, produces similar responses as the grieving process.
Subsequent to Dr. Simonton’s work, a study was published in the Lancet in 1989 that found similar results. (Spiegel)86 women with metastatic breast cancer were studied after 1 year of weekly supportive group therapy with self-hypnosis for pain. Both the treatment (n = 50) and control groups (n = 36) had routine cancer care. After 10 years only 3 were alive. Survival from time of randomization and onset of intervention was a mean 36.6 (SD 37.6) months in the intervention group compared with 18.9 (10.8) months in the control group, a significant difference. Survival plots indicated that divergence in survival began at 20 months after entry, or 8 months after intervention ended.
A common resource I recommend for guided imagery is https://www.healthjourneys. com/. They have CDs and MP3 files. Covering the following topics:
TABLE 1: Health Journeys’ audio guided imagery/meditation resource topics
● addiction & compulsive
● behavior
● anxiety relief creativity
● intuition & spirituality depression
● headache & migraine relief
● heart & cardiovascular health
● hospice & palliative care
● illnesses & conditions kids
● health
● military
● music
● pain relief
● performance & selfimprovement
● posttraumatic stress relationships
● relaxation & general wellbeing
● sleep & insomnia
● social & performance anxiety
● sports performance & rehab
Is there a “cancer personality”?
● stop smoking
● stress relief
● surgery & medical
● procedures
● teen stress
● anxiety & depression
● weight loss & fitness
● women’s health
● yoga
● convalescing from Covid
Is there a “cancer personality”? A 1984 study explored this by measuring the stress responses of three groups: melanoma patients, heart disease patients, and healthy controls. Using a dermograph, the study recorded electrical skin reactions as subjects viewed distressing statements like “You’re ugly.” Participants also self-reported their emotional stress levels.
134 Super Charge Your Health To Protect Yourself Against Cancer
Though all groups had similar physiological stress responses, the melanoma patients were more likely to deny feeling emotionally upset. This led to the idea of a “Type C” personality—traits like cooperativeness, patience, and passivity that are more common among those who develop cancer.
This study suggests that people can physically react to emotional stress while remaining unaware of it, fueling the ongoing debate on whether personality traits could influence cancer risks.
Researchers have sought to identify those personality characteristics that increased the risk of specific somatic diseases or were responsible for general susceptibility to diseases. One of the personality types claimed to be associated with cancer is the so-called Type C personality or Type C behavior (Greer) They did research on a sample of women with breast cancer and found the co-occurrence of cancer with a certain pattern of behavior associated with abnormal expression of emotions. Type C what considered associated with neuroticism and introversion, while coronary heart disease-prone personality is associated with neuroticism and extraversion. (Rymarczyk) A number of further studies on cancer patients revealed additional links between Type C and psychosocial factors but they were not always consistent either. Multiple studies have been done on this topic. In some studies, no association between any of the personality traits and cancer and cancer mortality was found. (Rymarczyk) in their research they evaluated a proposed two-facet structure of Type C, comprising Submissiveness (the interpersonal aspect) and Restricted Affectivity (the intrapersonal aspect) and found significant consistency.
Submissiveness manifests as abnormal levels of agreeableness, compliance, kindness toward others, uncritical adjustment to them, dependence, excessive patience, peacefulness, inability to refuse, and even in excessive focus on other people and sacrificing oneself for them at the cost of one’s own needs. Restricted Affectivity manifests itself in the repression and suppression of negative emotions (particularly anger), low awareness of the emotions experienced, inability to identify, name, and express them, anhedonia, passiveness, and helplessness in the face of adversities. Further research is needed to verify these personality traits and their relationship to a factorcontributing to cancer development in any given person.
These same traits have now been found in studies of many other cancers as well. In 1991, researchers in Melbourne, Australia, investigated whether personality traits were a risk factor in cancer of the colon. Over 600 people, newly diagnosed, were compared with a matched group of controls. Cancer patients, to a statistically significant degree, were more likely to demonstrate elements of denial and repression of anger. They appeared to be “nice” people who suppressed reactions to avoid conflict.
The characteristics associated with the “Type C personality” all represent emotional repression, a pushing down of necessary emotions. In contrast, self-assertion is im-
135 Super Charge Your Health To Protect Yourself Against Cancer
portant to having our needs met. Avoiding conflict and wanting to be liked lead to the denial of these needs. Even though there may not be a specific Type C personality, some personalities may be more prone to cancer than others. See Table 2
TABLE 2: Cancer personality types
Cancer-Prone Personality Types
● Becomes easily depressed or has feelings of hopelessness.
● Feels the need for approval and to please others.
● Is negative or pessimistic.
● Reacts adversely to and does not cope well with life changes.
● Represses both positive and negative emotions.
● Shows anger, resentment, or hostility towards others.
● Takes on extra duties and responsibilities, even when they cause stress.
● Worries often and excessively about others.
Cancer-Resistant Personality Type
● Controls anger and resolves anger issues positively.
● Copes well with stress and feels in control of situations.
● Does not become easily depressed.
● Does not worry excessively.
● Expresses emotions in a positive and constructive way.
● Is optimistic and hopeful.
● Knows when to say no.
● Likes to please, but does not seek approval as an emotional crutch.
● Seeks out and maintains social support networks.
FROM: https://www.psychologytoday.com/us/blog/how-the-mind-heals-the-body/201411/ is-there-cancer-prone-personality
How do emotional traits translate into cancerous skin lesions or other malignancies? The answer is that biology and psychology are not independent; each represents the functioning of a super system with components that can no longer be thought of as separate or autonomous mechanisms. The past quarter century of scientific inquiry has supplanted the traditional Western medical view of a split between body and mind with a truer, more unitary perspective. Our mind and body are one and our physiology, including our immune system, is directly affected by our emotions.
Thus, the repression of emotions threatens not only our psychological health but also our physical well-being. It does so by suppressing our immune response. In turn, immune suppression leaves us susceptible to bacterial or viral invaders, or to malignant changes from within.
Cancer treatment resistance
Resistance to cancer treatment applies to all currently available and known therapies. No therapies as currently known or immune to treatment resistance. Cancers have numerous mechanisms for maintaining their survival regardless of the attacks
136 Super Charge Your Health To Protect Yourself Against Cancer
thrown at them. Because resistance to treatment is a multifactorial process, treatment has to be multifactorial as well. Below are examples of resistance, that is, what factors have been identified to contribute to the resistance with the use of pharmaceutical drugs.
FROM: Ranji
Clearly, these are very complicated processes.
Cancer and bone metastases
Breast cancer and bone metastases
About 70% of breast cancer patients develop bone metastases (Mundy) The metastatic process sometimes occurs very early in the natural history of the disease but can occur at later stages. In either case, once the tumor has spread to the bone, the cancer is no longer “curable.”
Cancer and bone metastases
Bone is one of the most common metastatic sites. Many cancers can result in distant metastases; up to 70% of skeletal metastases originate from prostate and breast
137 Super Charge Your Health To Protect Yourself Against Cancer
Figure 6. Cancer drug resistance factors
cancers. It has been reported that only about 0.02% of cancer cells entering the circulation produce clinically detectable metastases, indicating the metastasis formation process is highly inefficient. Unfortunately, once metastases occur, they lead to 90% of cancer-associated mortality. (Shen)The 5-year-survival rate of prostate cancer decreases by ~30% when it metastasizes to the bone. (Yu)
Integrins have been the research focus of cell-extracellular matrix adhesion (ECM) and cytokine receptor activity. They are involved in the regulation of bone metabolism of bone precursor cells, mesenchymal stem cells (MSCs), osteoblasts (OBs), osteoclasts (OCs), and osteocytes. Cytokines activate bone metabolism through interaction with integrin receptors. Integrins mediate bone metastasis of breast, prostate, and lung cancer by promoting cancer cell adhesion, migration, and survival. (Mao)
Bone metastases are common in cancer and typically predict poor prognosis. The most common sites of bone metastasis are the skeleton, including the spine (87%), ribs (77%), pelvis (63%), and the forearms and femurs (53%). (Labedz) Cancers with a high prevalence of bone metastases, include prostate (85%), breast (70%), lung and kidney (40%, together).
In several types of cancer, including prostate, breast and lung cancer, bone metastases are associated with a much shorter survival. In spinal metastases, only 10–20% survive more than two years from diagnosis. Up to one-third of those with cancer develop spine metastases; in the US alone, there are about 180,000 annually.
The most common symptom from with spine metastases is severe pain refractory to treatment. Also, bone metastases lead to significant suffering, including pathological fractures, the need for radiotherapy to reduce pain or bone remodeling, the need for surgery to repair or prevent bone damage, spinal cord compression, and elevated calcium levels. These skeletal-related events (SRE) lead to worse mobility, reduced social functioning, and a lower quality of life. The treatment of spine metastases is mostly palliative.
Secondary bone cancers can be divided into osteolytic and osteoblastic lesions. Osteolytic lesions, have intensive bone resorption, are a more common form of metastasis, and especially frequent in breast, prostate and kidney cancer. Osteoblastic lesions, more often seen in prostate cancer, have abnormal bone formation, being weaker and more prone to fractures. Nevertheless, many lesions involve both bone formation and resorption processes; mixed lesions more common in breast cancer.
The multi-step process of metastasis to the bone involves migration and dissemination of cancer cells into the blood system, then (i) colonization of bone marrow by circulating tumor cells (CTCs), (ii) dormancy when cancer cells enter a quiet state after adapting to the bone marrow microenvironment, (iii) reactivation of dormant cells and then proliferation, and (iv) the reconstruction of the bone tissue by cancer
138 Super Charge Your Health To Protect Yourself Against Cancer
cells. Recruitment of osteoclasts by tumor cells is critical for metastatic bone remodeling. Cytokines and cytokine receptors affect these processes with crosstalk between cancer and bone cells.
Vertebral metastases are frequently managed by surgery, radiation or systemic therapy. Bisphosphonates are currently the standard of care to reduce bone loss; however, they have considerable side effects and rather limited usefulness. Therefore, new treatments are urgently needed to effectively manage metastatic disease in the spine.
Given the proven value of PEMFs for healing bone, whether for fractures, bone fusions and osteoporosis, and for pain management overall, PEMFs may well be an important tool for dealing with skeletal, and perhaps especially, spinal metastases.
The most studied cytokines include: Hepatocellular (HCC) - CX3CL1, CX3CR1; prostate– CXCL5, CXCL12, CXCR4, CXCR6, IL10; ?breast - CCL2, TGFbeta.
Table3: Cumulative incidence of bone metastasis among different solid cancers
FROM: Lo Bianco
In breast cancer, estrogen receptor (ER)+ tumors are more prone to metastasize into bone, while ER− tumors tend to go to visceral organs (e.g. lungs, liver, or brain), showing that tumor cell characteristics and the microenvironment of the primary tumor influence skeletal metastasis. (Salvador) Also, bone has unique structural and functional characteristics that supports metastasis. It not only creates an environment for cells to survive for long periods but also promotes colonization by disseminated tumor cells (DTCs). Most DTCs never evolve into metastases. Micro-metastases and/or DTCs in the bone marrow can be in and remain at very low levels after primary tumor resection. This is one of the reasons the cancer can resist treatment and reappear after long asymptomatic periods of inactivity, even for decades. This dormancy is basically tumor growth that has “arrested.” Because the DTCs have not adapted to the bone microenvironment, they can’t progress. When it does progress, it happens in a number of ways: autonomously in the DTCs themselves, through blood vessel growth (common to all growing tumors, ie, angiogenesis) and changing immune processes.
139 Super Charge Your Health To Protect Yourself Against Cancer
Cancer Type Incidence at Diagnosis (%) Lung cancer 49 Prostate cancer 15 Breast cancer 14 Gastrointestinal cancer 7 Kidney cancer 5
DTCs become dormant by various processes, either by tissue signals, such as hypoxia, biologic biochemical inhibitors of DTC growth, or by the lack of support for cell proliferation through normal tissue homeostasis. Under nutritional stress, cancer cells themselves induce dormancy and cell autophagy. Stress signals in the microenvironment itself induce dormancy in DTCs.
Circulating tumor cells (CTCs) in the blood are an indicator of metastatic progression, and show that many processes are involved in leading to metastasis. This means that a combination of proliferative and apoptotic activities is involved in the release of CTCs. Bone metastases may occur due to local tumor cell progression in the bone as well as releases of tumor cells from other non-bone metastatic lesions that end up in the bone.
Finally, those with malignancies may also end up having osteoporosis (16%) or osteopenia (44%), as found among 1041 patients affected by different malignancies.(Reuss-Borst)
Natural killer (NK) cells
What I was at a conference at Columbia University, researchers from China provided evidence of the impact of various medicines used routinely in cancer on the function of natural killer (NK) cells in the body. They noted that it was relatively common for people with a history of cancer to have surgery for an incidental problem, for example an appendectomy. Within some time after the surgery, there was evidence of spread of the cancer. They found that this was due to suppression of NK activity, either by reducing NK cell numbers or the function of NK cells. But they also discovered was that even one session of acupuncture (to the ST 36 point) prior to a surgical procedure could restore NK function. Subsequently I discovered a number of the medications frequently use around the time of surgery also had impact on NK levels.
Natural killer (NK) cells are a type of lymphocyte (a white blood cell) and play a crucial role in the host-rejection of both tumors and virally infected cells. Several medications and therapeutic agents can influence NK cell activity or levels, either as a primary effect or as a side effect.
As can be seen from this figure, even cancer related surgery causes major suppressive effects on NK function up to the seventh day postoperatively. However, NK induced interferon gamma (IFN gamma) is suppressed even beyond 28 days postoperatively.
Natural Killer (NK) cells are severely affected during this period in the postoperatively recovering cancer patient. NK cells play a crucial role in anti-tumor immunity because of their innate ability to differentiate between malignant versus normal cells. Therefore, an opportunity arises in the aftermath of cancer surgery for residual can-
140 Super Charge Your Health To Protect Yourself Against Cancer
cer cells, including distant metastases, to gain a foothold in the absence of NK cell surveillance. Here, we describe the post-operative environment and how the release of sympathetic stress-related factors (e.g., cortisol, prostaglandins, catecholamines), anti-inflammatory cytokines (e.g., IL-6, TGF-β), and myeloid derived suppressor cells, mediate NK cell dysfunction. (Angka) NK cells were found to be lower post-operatively along with T cells and NKT cells and this effect was more pronounced in patients undergoing major surgery versus minor surgeries.
Specific nutrients have been incorporated into peri-operative nutritional regimens with a specific focus on enhancing post-operative immune function and have therefore been called “immunonutrients”. These are glutamine, arginine, and omega-chain fatty acids.
In other research, women with breast cancer after having mastectomies had two cancer rate peaks (at the third and eighth year), while those untreated only had one peak (at the fourth year). These results indicate that surgery for breast cancer treatment accelerated mortality for a subset of patients as compared to those not receiving any treatment at all. Furthermore, in numerous preclinical animal studies, surgical stress has been shown to enhance metastases and reduce survival. (Angka) Even blood transfusions themselves will result in immunosuppression. Blood transfusions should be minimized to reduce the amount of post-surgical NK cell suppression.
Figure 7. This graph shows the relative change of NK levels and inflammatory cytokines following surgical stress. Pro-inflammatory cytokines and stress hormones peak very early. Anti-inflammatory cytokines take 1-2 days to kick in and gradually decrease over about seven days. NK cell cytotoxicity becomes quite depressed initially, gradually improving over about a week. NK related interferon gamma levels become depressed and don’t recover even after about four weeks
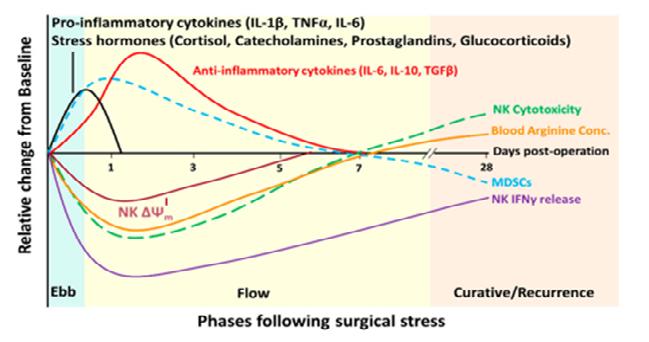 FROM: Angka
FROM: Angka
141 Super Charge Your Health To Protect Yourself Against Cancer
Figure 7: Relative change of NK levels and inflammatory cytokines following surgical stress
Medications that lower NK levels in the body
Here are some categories of drugs and specific agents that can affect NK cell levels or activity:
● Corticosteroids: These are well-known immunosuppressive drugs. Examples include:Prednisone, Methylprednisolone, and Dexamethasone.
● Immunosuppressive agents: These drugs are often used post-organ transplant to prevent rejection or in autoimmune diseases. They include:Cyclosporine, Tacrolimus (FK506), Azathioprine, Mycophenolate mofetil.
● Chemotherapy agents: Some chemotherapy drugs can suppress bone marrow function or have direct toxic effects on lymphocytes, which might lead to decreased NK cell levels. These include:Cyclophosphamide, Doxorubicin, Cisplatin, Methotrexate.
● Targeted therapies and monoclonal antibodies: Some newer cancer drugs, particularly targeted therapies, can influence NK cell activity. These drugs might not necessarily lower NK cell levels, but they can alter their function.Rituximab, for example, can influence NK cell-mediated antibody-dependent cellular cytotoxicity (ADCC).
● Biological agents for autoimmune diseases: Some drugs used to treat autoimmune conditions can influence the immune system, including NK cells.
● Tumor necrosis factor (TNF) inhibitors, like infliximab or etanercept, can influence the broader immune response, which may, in turn, affect NK cells.
● Antiretroviral therapy for HIV: Some antiretroviral therapies (ART) might impact NK cell function, though their primary target is the HIV virus itself.
It’s important to understand that the effect on NK cells can be direct or indirect, and the clinical significance of these changes varies widely.
Psychological stress
There is much evidence that psychological stress can adversely affect the human immune response. (Witek-Janusek) Stress-induced immunosuppression accompanies a variety of acute and chronic life stressors such as bereavement, depression, marital conflict, academic exam stress, and care giving in chronic disease. Stress-induced immune alterations were found in women newly diagnosed with invasive breast cancer (Stage II and III). Higher stress levels were predictive of lower NK cell activity (NKCA), diminished NK cell response to interferon (IFN), and decreased lymphocyte proliferation. Those with solid tumors (e.g., breast, cervix, endometrium, ovary, and lung) have reduced NKCA.
Narcotics lower natural killer cell levels
Narcotics or opioids,as as prescriptions, are known to have various effects on the immune system, including on natural killer (NK) cells. Research has indicated that opi-
142 Super Charge Your Health To Protect Yourself Against Cancer
oids can impact the immune system’s function and can suppress various immune responses, including the activity and levels of NK cells.
● Direct Effects: Some opioids, especially morphine, directly suppress NK cell cytotoxicity. NK cells’ ability to destroy target cells, such as tumor cells or virally-infected cells, is less.
● Indirect Effects: Opioids can also exert immunosuppressive effects indirectly by affecting other immune cells like T-lymphocytes or by altering the levels of cytokines.
● Clinical Relevance: The degree to which opioids impact immunity in clinical settings can be influenced by various factors, including the dose of the opioid, the duration of use, and the specific medical conditions being treated.
Sedatives, tranquilizers or SSRIs lower natural killer cell levels
Sedatives and Tranquilizers (Benzodiazepines and others):
Benzodiazepines, common sedatives/tranquilizers like diazepam (Valium), lorazepam (Ativan), and alprazolam (Xanax), have been studied for their effects on the immune system. Benzodiazepines can have immunosuppressive effects, impacting NK cell activity.
Other sedatives, such as certain anesthetics, might also have transient effects on immune function, including on NK cells, especially in the context of surgery or other major medical interventions.
Selective Serotonin Reuptake Inhibitors (SSRIs):
SSRIs, like fluoxetine (Prozac), sertraline (Zoloft), and paroxetine (Paxil). Studies suggest a potential modulatory effect on immune function, but the evidence is not consistent. Some research indicates that depression itself can alter immune function, so it can be challenging to disentangle the effects of the medication from the effects of the underlying condition.
PEMFs improve NK cells
End-stage cancer patients (N=15) were exposed at low intensity, coherent electromagnetic fields at radiofrequencies ranging from 600 kHz-729 Hz, for 8 h/day, 6 days/ week for 4 weeks. NK number and cytotoxicity of NK T-lymphocytes versus K562 cancer cell line were estimated by flow cytometry, before and after exposure. Data showed that the exposure of the end-stage cancer patients to the coherent electromagnetic fields resulted in a significant increase of the number and the cytotoxicity of the NK T-lymphocytes against cancer cells, in all patients. Exposure to coherent
143 Super Charge Your Health To Protect Yourself Against Cancer
EMFs at radiofrequencies increases the number and cytotoxicity of NK T-lymphocytes, which may contribute to the improvement of cancer patients’ status. (Evangelou)
No studies have shown that short- or long-term exposure to ELF-EMFs would compromise survival upon challenge with an infectious agent or tumor cells in animals whose NK cell function. Studies in humans (Rosado) focused mainly on NK cell counts in occupationally exposed individuals with contrasting results. Some authors observed an increase, others a decrease of peripheral blood NK cells after ELF-EMF exposure. One study reported the effects of ELF-EMF on NK activity in a group of 52 occupationally exposed workers. Individuals were stratified according to the ELF-EMF exposure dose in low (<0.2 μT/microT) and high (>0.2 μT/microT) exposed workers and NK function assessed as an ability to lyse target cells. Highly exposed workers showed no differences in peripheral blood NK cell number.
It’s likely that the primary effects of PEMF therapies on NK cells/activity in the setting of cancer will be through moderating the overall immune function and the imbalanced cancer microenvironment.
Testing for Cancers
This topic is too extensive to cover in this e-book.

However there is one new test that I recently became aware of that provides exciting opportunities to detect about 50 different cancers much earlier than usual. This is called the Galleri test. (galleri.com)
It is a multi-cancer early detection test that looks for a signal shared by 50+ types of cancer with a single blood test. If a cancer signal is detected, Galleri predicts the tissue type or organ associated with the cancer signal with 88% accuracy to help guide follow-up diagnostic testing which may include lab work or imaging to confirm cancer. The Galleri test is recommended for adults with an elevated risk for cancer, such as those aged 50 or older. The Galleri test is available by prescription only. Use of Galleri is NOT recommended in individuals who are pregnant, 21 years old or younger, or undergoing active cancer treatment.
Galleri checks more than 100,000 DNA regions and over a million specific DNA sites to screen for a signal shared by cancers that could be hiding. The Galleri test looks for
144 Super Charge Your Health To Protect Yourself Against Cancer
cell-free DNA and identifies whether it comes from healthy or cancer cells. DNA from cancer cells has specific methylation patterns that identify it as a cancer signal. Methylation patterns also contain information about the tissue type or organ associated with the cancer signal to guide next steps.
Small amounts of DNA shed from cancer cells may appear in the blood significantly sooner than circulating tumor cells, allowing detection much sooner than usual with most other testing.
The figure below shows that the lowest counts of ctDNA occur in the subclinical phase of disease, the optimal time for detection and developing strategies for preventing progression. The levels increase until clinical/radiologic sensitivity threshold is exceeded. Treatment then should decrease the levels, after which monitoring would occur for detection of residual disease and the early diagnosis of relapse. Relapse would include the identification of mutations related to resistance against treatment.
Figure 8. Circulating tumor DNA (ctDNA) applications for ovarian cancer management.
FROM:(Mari)
Detecting cancers at a subclinical stage is the most effective screening strategy.
Inflammation and cancer
Around 25% of cancers are related to chronic inflammation. Although the appropriate stimulation of inflammation can increase the immune response against cancer, studies have also found that inflammatory factors are involved in the tumor growth processes. Inflammatory processes participate in the initiation, promotion and metastasis of cancer through various mechanisms. (Lan)The initiation of a tumor requires a series of genetic mutations and epigenetic modifications that lead to the activation of the tumor growth pathway as well as the loss of the ability suppress tumors. The body needs to maintain a balance between tumor growth and suppression actions.
145 Super Charge Your Health To Protect Yourself Against Cancer
Screening/ early diagnosis Prognosis Treatment monitoring Detection of residual disease Early diagnosis of relapse Identification of resistance mutations Subclinical disease Clinical/radiological sensitivity threshold Tumor burden ctDNA sensitivity threshold Treatments Follow-up Relapse
In an inflammatory microenvironment, macrophages and neutrophils are active producers of reactive oxygen species (ROS) as well as reactive nitrogen (RNS), both of which can cause DNA damage. DNA damage is closely associated with the initiation of the tumor growth process. DNA damage can be induced by cytokines. The cytokine IL-22 can activate DNA damage by affecting a series of genes. Epigenetic responses that can increase oncogenes or decrease tumor-suppressor genes are orchestrated by pro-inflammatory cytokines. Thus, some aspects of cancer-related inflammation can provide a friendly environment for cancer initiation.
In particular, NF-κB plays an important role in the manipulation of the tumor microenvironment (TME). It controls the production of cytokines that regulate cell growth and migration. By invoking cytokines, transcription factors such as NF-κBset up an intricate system that allows the expansion of tumors. Mediators such as cells and other functional proteins and to angiogenesis, the inhibition of the immune response, the regulation of metabolism and other supportive activities for cancer promotion.
Also, inflammation is an important contributor to metastasis. Tumor metastasis requires cancer cells to migrate and be seeded, survive the early metastatic colony and establish ofa new TME. The metastatic process is very inefficient. Blocking every supportive factor for the process of metastasis is essential to improve the life expectancy of patientsindividuals with metastases. Particularly, inflammatory cytokines are important orchestrators of cancer–inflammation interactions and influence multiple aspects of cancer metastasis.
Together, inflammation and the cancer microenvironment modulated by the inflammatory response influence initiation, promotion and metastasis through an intricate network. A wide range of inflammatory factors, including cytokines, transcriptional factors, immune cells and stromal cells, are fundamental components of this system.
Cytokines in Cancer-Related Inflammation
Cytokines are a group of functional proteins produced by the immune system. They were initially described as controllers of immune response and inflammation. However, an increasing number of studies found that the elevations of some types of cytokines are associated with the induction and progression of tumors. Cytokines that promote or enhance cancer development are involved in a coordinated system.
Figure 9: Cancer promoting and cancer inhibiting cytokines.
146 Super Charge Your Health To Protect Yourself Against Cancer
FROM
: Lan
Many cytokines were found to be elevated in patients with cancer or tumor microenvironments.
Interleukins
IL-6 production is usually a result of infections and tissue injuries. The pro-tumor effects are seen in various cancer types: lung cancer, breast cancer and colorectal cancer, and some others. It inhibits apoptosis and release of ROS and RNS.
IL-2 and IL-12 possess anticancer effects. IL-2 gene therapy and cell therapy helped decrease tumor size. Possibly useful against pleural effusions caused by lung cancer. Capable of activating cytotoxic immune cells.
● Tumor Necrosis Factor Alpha (TNF-α) inflammatory, regulation multiple signaling processes, impacting tumor development via multiple mechanisms, EMT, boosting cell proliferation rate and accelerating angiogenesis. Found in Prostate cancer, ovarian cancer, liver cancer and breast cancer. May contribute to the migration of tumor cells.
● Transforming Growth Factor Beta (TGF-β) Produced by inflammatory cells, including neutrophils and macrophages; substantial role in tumor initiation and progression. Blocking TGF-β significantly increased anticancer treatments. Wide range of tumor-inductive or cancer-supportive mechanisms: EMT, immune escape, angiogenesis, suppression of apoptosis. Seen in breast, ovarian and prostate cancer TMEs.
● Chemokines (CKs) regulate activation and migration of multiple types of cells. Migration of WBCs to inflammatory sites mediated by CKs. Closely associated with cancer progression, metastasis and angiogenesis. Used in dendritic cells with adenovirus, then injected as an antitumor vaccine.
● Interferons (IFNs) Crucial for inflammatory processes. IFNs regulate the molecular, cellular and physiological processes that govern inflammatory responses. IFNs (type I, type II, type III). IFNs can affect metabolism and proliferation of cancer cells widely. Type I, strong tumor inhibitory ability. Already used for treatment of cancer or hepatitis C.
147 Super Charge Your Health To Protect Yourself Against Cancer
PEMFs reduce inflammation by lowering many proinflammatory tissue cytokines. These include reduction of the levels of tumor necrosis factor-α (TNF-α), interleukin (IL)-1β, IL-6, and IL-8, (Vincenzi, 2017) and NF-kappaB (Vianale). But very low intensity PEMFs between, 3 and 5 microTesla, do not affect some of these tissue cytokines (de Kleijn).
Inflammation and hypoxia
As for chemotherapy, oxygenated cells are essential for successful drug delivery. Thus, hypoxic cells, including CSCs, escape chemotherapy due to alterations in apoptotic pathways and DNA damage repair systems. Additionally, the restricted/abnormal vasculature of the hypoxic tumor environment contributes to inadequate transport of anti-tumor drugs into the tumor tissue. Immunotherapy is one of the more recent developments in cancer therapies. However, there is strong evidence that hypoxia suppresses T cells and supports tumor associated macrophage polarization.
Figure 10 Shows that various lifestyle factors increase the risk of many chronic diseases, including cancer, by acting on inflammation and the production of inflammatory biomarkers.
Figure 10. Lifestyle risk factors, pro-inflammatory biomarkers and major chronic diseases.
FROM: Gupta
148 Super Charge Your Health To Protect Yourself Against Cancer
There are many inflammatory molecules and transcription factors involved in inflammation some of these are: 5-LOX, adhesion molecules, chemokines, COX-2, C-reactive protein, cytokines, MMPs, NF-kB, prostatespecific antigen (PSA), STAT3, TWIST, and vascular endothelial growth factor (VEGF). These are known molecular links between inflammation and chronic diseases (See Figure above). The pro-inflammatory transcription factors (NF-kB and STAT3) are the crucial regulators of inflammation. For example, more than 500 cancer related genes are known to be regulated by NFkB. Epidemiological, genetic and pharmacological studies support the association of inflammation with chronic diseases. Accumulating evidence suggests that chronic inflammation is precursor to most tumors. Well-known examples include stomach inflammation leading to gastric cancer, bronchitis with smokers leading to lung cancer, ulcerative colitis leading to colon cancer, chronic cervical inflammation leading to uterine cancer, and so on.
Chronic inflammation plays a crucial role in various aspects of tumor development including cellular transformation, survival, proliferation, invasion, metastasis, and angiogenesis. (Gupta) Lifestyle factors such as alcohol, infectious agents, obesity, radiation, stress, tobacco, and toxicants are known
activators of inflammatory pathways. Chronic inflammation is a cause for most chronic diseases. Thus, chronic treatment is required for most chronic diseases. In addition, dysregulation in multiple inflammatory molecules contribute to the development of chronic diseases.
One of the most well-known effects of PEMF’s is the reduction of inflammation. One aspect of this, relating to effects of PEMFs on the adenosine receptor, is covered in the blog https://www.drpawluk.com/pain-inflammation-adenosine. This aspect of PEMF therapy has been reviewed in depth. (Ross)
Hypoxia
In addition to the benefit of PEMFs as a controlling factor to the development of cancer, PEMFs may contribute to the improvement of the microenvironment of developing cancer. Sites of inflammation tend to become depleted of molecular O2. (Watts) These findings have led to the concept of “inflammatory hypoxia,” in which inflammation and hypoxia are inextricably linked. This Wattspaper demonstrates mechanisms and outcomes of inflammatory hypoxia in vitro and in vivo and shows that infiltrating immune cells, principally neutrophils, shape the tissue microenvironment through depletion of local molecular O2. Polymorphonuclear cell (PMN)-dependent O2 depletion is critical to regulating the resolution of inflammation, through the “respiratory burst” process. Such localized O2 depletion was critical for effective mucosal protection and inflammation.
149 Super Charge Your Health To Protect Yourself Against Cancer
Fig 10a: Summary of thehypoxia-induced factors influencing cancer growth and progression
HYPOXIA
From: Moen
Hypoxia has proven to be a causativefactor in many pathophysiological events, includingcancer progression. (Moen) Research has demonstrated thatdecreased oxygen induces more malignant cellsand induces multiple cellular adaptations, which further sustainand foster cancer progression and thereby inducecancer growth (Fig. 10a). Hypoxia is reported to result incellular responses which improve oxygenation and viabilitythrough induction of angiogenesis, an alteration in metabolismby increased glycolysis and upregulation of genesinvolved in cell survival/apoptosis. Hypoxia has been shown to increase genetic instability, activate invasivegrowth, and preserve the undifferentiated cell state.
When activated, it is estimated that PMNs can consume up to 10 times more oxygen than any other cell in the body. Importantly, the PMN oxidative burst is not hindered by even relatively low oxygen concentrations (as low as 4.5%). Reactive oxygen species (ROS), damaging the cancer cells, can be generated in the relatively low oxygen environments, such as inflamed intestinal mucosa. Inflammatory lesions seen in mouse research were profoundly hypoxic or even anoxic,similar to that seen in some large tumors. Factors that predispose the inflamed intestinal epithelia to decreased oxygen delivery and hypoxia, include vasculitis, vasoconstriction, edema and increased oxygen consumption. These factors are commonly seen in the setting of cancer development. (Colgan)
Inefficient delivery of drugs is a main cause of chemotherapy failure in tumors low perfusion and oxygen levels. To enhance perfusion and drug delivery in these tumors, two strategies have been developed: vascular normalization, aiming at normalizing tumor vasculature and blood vessel leakiness, and alleviation of tissue stress, thus aiming at decompressing tumor blood vessels. Vascular normalization is normally based on the use of anti-angiogenic drugs, whereas stress alleviation is based on stroma-depleting chemicals. Reducing inflammation can normalize tumor vascula-
150 Super Charge Your Health To Protect Yourself Against Cancer
Growth Dedifferentiation Aggressiveness Angiogenesis Metastasis Therapy resistances Cell survival Glycolysis TUMOR PROGRESSION
ture, taking into accountthat malignant tumors tend to develop at sites of chronic inflammation.
While this focus has been on the delivery of chemotherapeutic drugs, the same most likely applies to the delivery of nutrients and chemotherapeutic/preventive herbs and supplements. Therefore, PEMFs would be able to help with the delivery of nutrients and supplements to tumor cells and their microenvironments.
Cancer Stem Cells (CSCs)
A few reasons for unsuccessful treatment outcomes are metastasis, recurrence, cancer heterogeneity, resistance to the treatment, and immunological escape. All of these factors can be attributed to the characteristics seen in CSCs present in the tumor environment. Therefore, CSCs are considered important targets for cancer treatment.
Which arose first, the cancer cell or the CSC? Tumor cells can arise either from transformeddifferentiated cells or transformed resident stem cells.Transformation is likely to arise from environmental inputs suchas tissue regeneration, infections, toxins, as well asintrinsic and non-intrinsic factors that lead to DNA mutations
The stem cell theory of cancer (Abd) includes two majorconcepts:
1. Cancer arises from stem cells that are present in thetissues of both children and adults; and
2. Cancer cells originatefrom the cells of normal tissues, including stem cells, proliferatingcells, and terminally differentiated cells.
In each of thehypotheses on the origin of cancer, including field theory,chemical carcinogenesis, infection, mutation, and genetic change,stem cells are considered the core generator of cancer.
According to the stem cell theory, cancer originates from thearrest in the maturation of stem cells into “normal” cells. CSCs and/orcancer cells can give rise and/or be composed of cells found innormal tissues including stem cells, transit amplifying cells, andterminally differentiated cells.
The solid tumor environment, also known as the tumormicroenvironment, refers to the surrounding cellular and non-cellular components thatinteract with and influence the behavior of solid tumors. It is a complex ecosystem thatplays a crucial role in tumor growth, progression, and response to therapy. Reacting to the presence of cancer cells, immune cells, such as T cells, B cells, natural killer (NK) cells,dendritic cells, and macrophages, infiltrate the tumormicroenvironment. Despite this extensive immune cell infiltration, tumorscan create an immunosuppressive microenvironment.
The solid tumor microenvironment is also shaped by the vascular supply. Thisblood supply is essential for the growth and survival of solidtumors. However, because the tumor blood ves-
151 Super Charge Your Health To Protect Yourself Against Cancer
sels can be abnormal this can lead to inadequate bloodflow and oxygenation in regions of the tumor.
The tumor microenvironment containsvarious “signaling” molecules, including growth factors, cytokines,and chemokines. These further enhance tumor cell proliferation,migration, invasion, and angiogenesis. There is a subset of cells within the heterogeneous tumor environment known as cancer stem cells (CSCs). These play a key role intumor growth, recurrence, and resistance to therapy. The percent of CSCs in a tumor can range from lessthan 1% to more than 50%, depending on the cancer type and stage. CSCs are especiallyimportant for the development and treatment of cancer clinically.
Photograph by Dennis Kunkel Microscopy/science Photo Library which was uploaded on September 25th, 2018. Hematopoietic stem cells isolated from human bone marrow (adult), colored scanning electron micrograph (SEM). These stem cells are part of the hematopoietic and reticuloendothelial systems and give rise to specialized blood cells (macrophages, histiocytes).
Cancer stem cells and hypoxia
Another important environmental factor, hypoxia, which refers toa deficiency in the amount of oxygen reaching the tissues, has beenfound to be related to the regulation of Yamanaka factors. Yamanaka factors can also induce the formation ofpluripotent stem cells (iPSCs), which have some similaritiesto CSCs and can be used to reprogram CSCs. Several studies haveshown that the overexpression of Yamanaka factors in cancer cellscan induce a “stem-like” state, which is associated with increasedcapacity to turn into tumors (tumor growth) and drug resistance. This means
152 Super Charge Your Health To Protect Yourself Against Cancer
Figure 11. Human Stem Cells from Bone Marrow
that reprogrammed cancer cells, becoming pluripotent and stem-like, increase their metastatic behavior.
As mentioned above, another important environmental factor, hypoxia, which refers toa deficiency in the amount of oxygen reaching the tissues, is a hallmark of the tumor environment. This is true especially in rapidly growing solid tumors where the oxygen levelscan range from 0% to 2% compared to normal physiological cell levelsof 4% to 9% oxygen.
Hypoxia has been found to be related to the regulation of Yamanaka factors. Yamanakafactors in cells can lead to the reprogramming of cells into apluripotent state. Hypoxia-inducible factor 1 (HIF-1) is atranscription factor that is activated under conditions of hypoxia, and ithas been found to regulate the expression of Yamanaka factors inresponse to low oxygen levels. However, a study usingzebrafish showed that HIF3a is degraded under normal oxygen levels (~21% O2)Furthermore, the activation of HIF-1 has been shown to be important for the survival and self-renewal ofCSCs, which are thought to be responsible for tumor initiation,progression, and resistance to therapy. It has been suggestedthat the upregulation of Yamanaka factors in response to hypoxia maycontribute to themaintenance of CSCs and the development of tumors. See Figure 12 below.
In 2006, Shinya Yamanaka, a stem cell researcher, discovered thatadult physical cells can undergo cellular reprogramming into anembryonic-like pluripotent state through transcription factorsknown collectively as Yamanaka factors (OCT3/4, SOX2, KLF4,and c-MYC) (17). Multiple studies have implicated CSCs in sharingcritical properties with embryonic cells through the elevatedexpression of Yamanaka factors, which supports the impact ofthese pluripotency factors in tumorigenesis.
Tumor vascularization via angiogenesis was considered the primary method of blood supply for tumor growth. In 1999, it was found that highly invasive and metastatic humanmelanoma cells had tumor growth independent of angiogenesis. This meant that these cancer cells generated vascular channels withoutthe involvement of blood vessel cells. This process was termedvascular mimicry (VM). Tumors with VM lead to a worseprognosis. Evidence has found that VM may be used by cancers as another independent prognostic factor for survival. In triple negative breast cancer, a hypoxic tumor microenvironmentincreased the population of CSCs, accelerating VM channelformation. This is an additional explanation for the invasive nature of treatment-resistant tumors.
While tumor hypoxia is considered one of the most inimical factorsthat leads to drug treatment resistance, it also contributes to radiation resistance. Radiotherapy generatesreactive oxygen species, causing irreversible cellular DNA damageand apoptosis. Currently, radiotherapy is most often used totreat head, neck, breast, cervix, prostate, and eye cancers. However,cancer cells experiencing hypoxia are likely to be
153 Super Charge Your Health To Protect Yourself Against Cancer
three-times moreresistant to radiation. But, CSCs, consideredto be the “seeds” of cancer, not killed by radiation may well be “awakened” withradiation, leading to recurrence and metastasis post-radiation.
Figure 12. Hypoxia stimulates various factors to increase tumor growth and metastasis
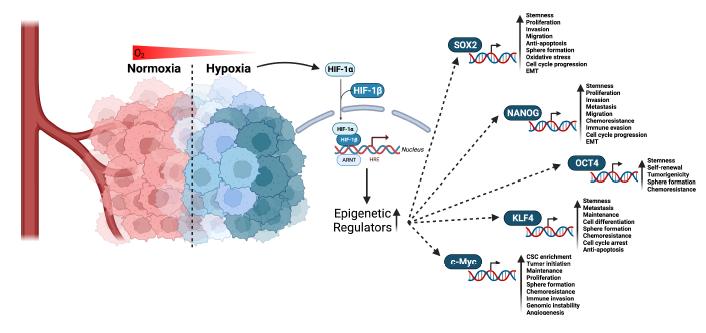 FROM: Abd
FROM: Abd
Mitochondria and Cancer
Introduction
Mitochondria are complex components (organelles) of the interior of all cells and are necessary to sustain life. However, mitochondria also influence the initial development of cancer, growth, survival and metastasis. Many facets of mitochondrial function, beyond energy production contribute to tumor development. These include mitochondrial density, dynamics, cell death regulation, acid-base (pH) homeostasis, metabolism control and intra-and extracellular communication. The interplay between these aspects of mitochondrial function results in coordination of mitochondrial effects on cellular physiology. These functions then extend to the role of mitochondria in cancer.
Mitochondria facilitate the flexibility of tumor cells, including supporting the use of fuel, energy production, cell death susceptibility, and oxidative stress. These supports facilitate cancer survival in the face of adverse environmental conditions, such as nutrient deficiency, and during anticancer therapies. Therefore, in order to effectively treat cancer, the cancer cell survival “escape routes” from therapies supported by mitochondrial functions must also be considered. This is yet another reason that combination therapies that remove this flexibility are critical to advance cancer treatment success.
154 Super Charge Your Health To Protect Yourself Against Cancer
Mitochondrion/mitochondria
Mitochondria is the plural of a single mitochondrion. A single mitochondrion is a small “organ” (organelle) in the cells of most organisms whose cells have a nucleus. This includes all animals, plants, fungi, and many unicellular organisms. Mitochondria have a double membrane structure and use oxygen-based respiration to generate adenosine triphosphate (ATP), which is used throughout the cell as a source of chemical energy. They were discovered by Albert von Kölliker in 1857 in the voluntary muscles of insects. The term mitochondrion was coined by Carl Benda in 1898. The mitochondrion is popularly nicknamed the “powerhouse of the cell”, a phrase coined by Philip Siekevitz in a 1957 article of the same name.
Mitochondria are typically round to oval in shape and range in size from 0.5 to 10 μm.
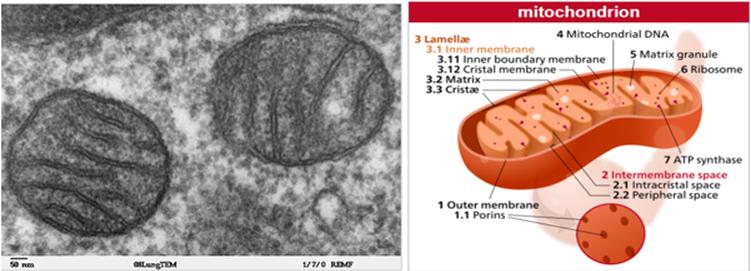
FROM: https://en.wikipedia.org/wiki/Mitochondrion. Two mitochondria shown by electron microscopy.
Number of mitochondria per cell
The number varies widely depending on the cell type and its energy needs.
● Red Blood Cells: have virtually no mitochondria, as they rely on glycolysis for energy.
● Liver Cells: may contain over 2000 mitochondria per cell.
● Muscle Cells: Highly variable, ranging from 100s to 1000s depending on muscle type and activity level.
● Neurons: in the brain each neuron can have up to 2 million, particularly at synapses where energy demand is high.
● Skin/other body cells: few hundred to around a thousand.
The number of mitochondria in cancer cells can be highly variable and is influenced by factors such as the type of cancer, the stage of the disease, and the metabolic characteristics of a specific cancer cell.
155 Super Charge Your Health To Protect Yourself Against Cancer
In general, however, some aspects are:
● Reduced Number: Some cancer cells have fewer mitochondria compared to their non-cancerous counterparts. These cells often rely more on glycolysis for energy, even in the presence of oxygen, known as the Warburg effect.
● Normal or Increased Number: On the other hand, some cancer cells have been found to have a normal or even increased number of mitochondria. These cells may rely more on oxidative phosphorylation for their energy needs and could be more aggressive or treatment-resistant.
● Metabolic Flexibility: Some cancer cells can switch between metabolic pathways (glycolysis and oxidative phosphorylation) depending on environmental conditions, and this could be reflected in varying numbers of mitochondria.
● Heterogeneity: Even within a single tumor, there can be a range of metabolic varieties, including variability in the number of mitochondria.
● Impact of Treatment: Certain cancer treatments may also impact the number and function of mitochondria in cancer cells.
Functions of mitochondria
In addition to producing energy, mitochondria store calcium for cell signaling activities, generate heat, and mediate cell growth and death. A major function of mitochondria is ATP production, hence its nickname ‘powerhouse of the cell’. However, mitochondria perform many roles beyond energy production, including the generation of reactive oxygen species (ROS), redox molecules and metabolites, regulation of cell signaling and cell death and biosynthetic metabolism. These multifaceted functions of mitochondria in normal physiology make them important cellular stress sensors, and allow for cellular adaptation to the environment. Mitochondria, a component of all cells, facilitate significant cellular flexibility, even to the point of tumor cell growth and their survival in otherwise harsh environments such as during nutrient deficits, hypoxia and cancer treatments. Therefore, mitochondria are key players in growth and development of tumors.
The functions of mitochondrial biology that contribute to tumor growth, include the genesis of the mitochondria and their turnover, breaking apart (fission) and fusion processes, affecting cell death, reacting to oxidative stress, controlling cellular metabolism and energy, intra-and extracellular signaling communication and changes in mitochondrial DNA.
The number of mitochondria in a cell (mitochondrial mass) is dictated by two opposing processes, cellular growth and development (biogenesis) and turnover (fission and fusion). This lifecycle process of mitochondria is now being seen as both a positive and negative regulator of tumor development. The role of mitochondrial biogenesis in cancer is dictated by many factors, including metabolic state, tumor variety, tissue type, micro-environment and tumor stage. Additionally, mitophagy, the selective autophagy process for mitochondrial turnover, controls a healthy mito-
156 Super Charge Your Health To Protect Yourself Against Cancer
chondrial population. Importantly, breakdowns in both mitochondrial production and mitophagy are central to cancer growth stimuli pathways.
Fission and Fusion Dynamics
While mitochondria appear to be quite fixed in their places in the cell, they are very dynamic and the balance of fission and fusion functional shape. Mitochondria exist as either fused, tubular networks or as fragmented granules depending on cellular state, with mitochondrial metabolism, respiration and oxidative stress regulating fission/fusion machinery. Mitochondrial morphology also affects susceptibility to mitophagy and apoptosis. Multiple studies have demonstrated an imbalance of fission and fusion activities in cancer, with elevated fission activity and/or decreased fusion resulting in a fragmented mitochondrial network. Restoring fused mitochondrial networks impairs cancer growth. The functionality of the mitochondrial network may impact the development of a shifting expression into multiple cancer types, further highlighting the role of mitochondrial dynamics in metastasis.
Genetic programs
Mitochondrial biogenesis is regulated by genetic transcriptional programs that coordinate stimulation of both mitochondrial and cell nucleus localized genes that produce mitochondrial proteins. The genes regulating mitochondrial biogenesis enhance cancer cell metabolic flexibility, allowing cancer cells to adapt to the stresses of cancer treatments and tumor microenvironments, resulting in treatment resistance and metastases.
Cancer cells can adapt their mitochondrial function according to the specific stress. For example, pancreatic cancer cells that increase their c-Myc and glycolytic gene expression enable them to be resistant to metformin treatment. These cancer cells actively use mitochondrial respiration for their energy. Metformin treatment would be expected to prevent their growth by decreasing their energy supply since it is a mitochondrial energy complex I inhibitor. Therefore, an important consideration in cancer therapeutics will be to impact routes of bioenergetic plasticity enabled by mitochondria.
Mitophagy
Clearance of damaged mitochondria via mitochondrial autophagy (mitophagy) is critical for cellular fitness since dysfunctional mitochondria can impair electron transport chain (ETC) function and increase oxidative stress. A major trigger for mitophagy is via a molecular pathway activated when the mitochondrial membrane changes its charge polarity. This depolarization is a signal of mitochondrial dysfunction that results from multiple causes including lack of oppositely charged molecules, hypoxia and impaired electron transport. An alternate pathway for mitophagy in-
157 Super Charge Your Health To Protect Yourself Against Cancer
duction is through HIF-1β target genes and adenovirus interacting protein, which inhibit mitochondrial respiration during hypoxic conditions that could result in excessive ROS.
Is mitophagy beneficial or harmful to cancers? Similar to cellular autophagy, which is shown to be both pro- and anti-tumorgenic based on context, the function of mitophagy in cancer transformation likely depends on tumor stage.
Thus, in certain stages of tumor development, decreased mitophagy may allow a threshold of dysfunctional mitochondria to persist, generating increased tumor-promoting ROS or other tumor promoting mitochondrial biochemical signals. In contrast, established tumors may require mitophagy for stress adaptation and survival.
A potential benefit of increased mitophagy for the clearance of increased levels of dysfunctional mitochondria can switch the fate of adenoma tumors from becoming carcinomas to becoming benign oncocytomas instead. An oncocytoma is a tumor made up of oncocytes, epithelial cells characterized by an excessive amount of mitochondria, resulting in an abundant cytoplasm. The cells and the tumor that they compose are often benign. For example, kidney oncocytomas represent 5-15% of surgically removed kidney tumors.
The bottom line is that mitochondria can influence cancer initiation, growth, survival and metastasis. Many facets of the actions of mitochondria go beyond energy production to actively contribute to cancer development. These include mitochondrial density, dynamics, cell death regulation, acid/base homeostasis, metabolic regulation and cellular communication. The interplay between these aspects of mitochondrial activity results in coordination of cellular physiology and contributes to the multiple actions of mitochondria in cancer. Mitochondrial adaptability translates to tumor adaptability, including alterations in fuel utilization, energy production, cell death susceptibility, and oxidative stress. All these, allow for cancer cell survival in the face of adverse environmental conditions such as nutrient deficiency and during chemotherapy and targeted cancer treatments. Therefore, the “mitochondrial escape routes” to cancer treatment need to also be considered. Combination therapies that reduce or remove this flexibility are needed to advance the success of cancer.
Cell Death
A hallmark of cancers is their ability to evade cell death, a phenomenon tightly linked to mitochondria. Tumor cells escape apoptosis by reducing pro-apoptotic gene proteins and/or increasing anti-apoptotic gene proteins. The balance of pro- and anti-apoptotic proteins affects a cancer cell’s susceptibility to apoptotic stimuli and would predict how a tumor will respond to chemotherapy.
Mitochondrial shape also dictates apoptotic susceptibility. The importance of mitochondrial shape in apoptosis is further supported by evidence that mitochondrial
158 Super Charge Your Health To Protect Yourself Against Cancer
hyper-fragmentation causes resistance to apoptosis stimuli on mitochondrial membranes. While the fission and fusion processes and outcomes by themselves do not necessarily regulate apoptosis, a balance generates a mitochondrial shape that improves responses to pro-apoptotic proteins.
Oxidative Stress
ROS, in the form of superoxide and hydroxyl free radicals and hydrogen peroxide, are produced from normal physiological metabolic reactions. Mitochondria are about the biggest contributors to cellular ROS. They have multiple antioxidant pathways to neutralize ROS, including superoxide dismutase (SOD2), glutathione, thioredoxin and peroxiredoxins.
Early on, it was seen that cancer cells have high ROS levels. This led to an overly simplistic conclusion that inhibiting ROS should be an important therapeutic strategy. But it’s much more complicated than that. ROS may increase signaling and tumor cell proliferation. But natural homeostatic increases in antioxidant responses prevent ROS-mediated cancer cell toxicity and may even enhance tumor survival. As a basis, multiple normal physiological reactions, including electron transport by the ETC and NAD(P)H oxidases, increase ROS production. However, these are often increased during the tumor development process by oncogenes, ETC mutations, and hypoxic microenvironments. ROS-influenced regulation of oncogene signaling also effects metastasis. Oxidation of the amino acid, cysteine, because of the increased ROS, increased its oncogenic ability, promoting tumor cell migration and metastasis across multiple tumor types. And, these different tumor expressions were blocked by a ROS scavenger.
In response to elevated ROS, many tumors increase their protective antioxidant pathways, to promote their growth. In a melanoma study, CTCs had higher levels of NADPH than primary tumor sites, probably to counteract the increased ROS caused by the stress of metastasis. In this research, antioxidants appeared to promote distant metastasis. Folate pathway inhibition prevented metastasis due to decreased NADPH production, but had no effect on the primary tumor.
Similarly, antioxidant treatment increased the number of metastases in a mouse model of malignant melanoma, causing increased invasiveness dependent on cells making glutathione. So, “successful” tumors maintain ROS levels within a window that stimulates proliferation without causing damage to them.
The balance of ROS production and antioxidant response is critical for maintaining a tumor-promoting ROS level. Combination therapy using glutathione and thioredoxin pathway inhibitors showed results in vitro and in vivo in breast cancer models (Harris), increasing ROS to slow cancer growth.
159 Super Charge Your Health To Protect Yourself Against Cancer
Reactive oxygen species (ROS) are normal byproducts of numerous cellular processes. At moderately increased levels, ROS damage DNA and promote mutagenesis in cells. To control oxidative stress, cells naturally generate antioxidants that convert ROS into benign molecules. The most abundant antioxidant within all cells is glutathione (GSH). Because generation of ROS is a byproduct of cell growth, cancer cells have much higher level of ROS production compared to normal cells. Therefore, to avoid the detrimental effects of oxidative stress, cancer cells must activate multiple antioxidant systems. By buffering ROS levels, cancer cells can restrict ROS within a range that is beneficial to promote tumor progression.
Results (Harris) show that antioxidants, such as GSH, are required for cancer initiation and suggest that reduced antioxidant activity can, counterintuitively, in fact be chemo preventive. These findings are consistent with significantly increased cancer incidences seen in clinical trials using antioxidants to prevent cancer. One study (Harris) looked at the impact of inhibiting the GSH antioxidant pathway on tumor development. Lack of GSH can prevent a tumor’s ability to drive malignant transformation. Inhibiting GSH works to suppress tumor development and malignant transformation and inhibiting GSH works best if delivered prior to cancer onset. At later stages of tumor progression GSH becomes less useful probably due to compensation from alternative antioxidant pathways. Remarkably, combined inhibition of GSH and thioredoxin antioxidant pathways synergistically leads to cancer cell death in vitro and in vivo.
Studying cancer metabolism in vivo.
Recent work has highlighted the importance of studying cancer metabolism in models comparable to the in vivo disease. For example, while glutamine fuels TCA cycle anaplerosis in vitro, this is not necessarily true of all tumors in vivo.
Metabolism
Alterations in glucose utilization
Many tumors divert glycolytic process products into the pentose phosphate pathway, serine biosynthesis and lipid biosynthesis, as opposed to complete oxidation by mitochondrial respiration. This is mitochondrial metabolic flexibility. Thus, mitochondria remain functional during aerobic glycolysis, and mitochondrial-dependent metabolic reprogramming can support bioenergetic homeostasis even during Warburg glucose vs oxygen-based metabolism.
Reprogramming of amino acid metabolism
Glutamine can be a substrate for TCA cycle oxidation and a starting material for macromolecule synthesis. . Transaminases, but not GDH, are upregulated in 3D cultures of proliferating mammary epithelial cells compared to quiescent cells, sug-
160 Super Charge Your Health To Protect Yourself Against Cancer
gesting that this pathway is important during cancer cell proliferation to support biosynthesis. As nutrients are oxidized to produce biosynthetic precursors, electrons are removed from carbon. Therefore, electron acceptors can quickly become limiting in highly proliferating cells. This observation was highlighted in a series of studies demonstrating that beyond ATP production, mitochondrial respiration is required to replenish electron-accepting cofactors NAD+ and FAD. Aside from coordinating fuel oxidation, mitochondria contribute to tumor progression through nucleotide synthesis via one-carbon metabolism. SHMT2 is expressed in ischemic tumor zones, providing proliferative advantage under hypoxic conditions (Kim et al., 2015). Additionally, serine hydroxylmethyltransferase (SHMT2) regulation of serine metabolism also contributes to NADPH production and detoxification of ROS under hypoxia, a function important for survival of MYC-driven cancers, which includes the most common human cancers.
Studying cancer metabolism in vivo
Recent work has highlighted the importance of studying cancer metabolism in models comparable to the in vivo disease. For example, while glutamine fuels the mitochondrial energy production cycle in vitro, this is not necessarily true of all tumors in vivo.
Classical oncogenic and tumor suppressive pathways regulate mitochondrial biology
The resurgence of mitochondrial research has led to the discovery that established tumor suppressors and oncogenes directly regulate mitochondrial biology. Several hallmark cancer signaling pathways that alter mitochondrial biology to promote transformation. In addition to promoting mitochondrial biogenesis, numerous studies have linked c-Myc with mitochondrial metabolism in cancer. Oncogenic K-Ras also promotes upregulation of mitophagy to preserve mitochondrial function under starvation conditions. Autophagy inhibition in cancers with active K-Ras results in a decline in mitochondrial respiration, TCA metabolite and energy levels during starvation, which may be important for tumor cell survival in nutrient-depleted microenvironments. p53 also has functions in the regulation of cellular metabolism via transcriptional activation of metabolic genes. p53 limits glycolysis and drives transcription of genes required for ETC assembly and maintenance. However, more recent work has suggested an alternate side to p53’s role in tumorigenesis, with its ability to allow for adaptation to metabolic stress resulting in pro-survival effects in tumor cells. These pro-survival effects are partially accomplished through upregulation of mitochondrial FAO and respiration, allowing cancer cells to adapt to starvation conditions (Jiang et al., 2015). In addition to transcriptional regulation of mitochondrial activity, p53 also directly functions at the mitochondria to induce apoptosis in response to stress. p53 mutations can also promote cancer survival through direct mitochondrial functions.
161 Super Charge Your Health To Protect Yourself Against Cancer
Microbiome and cancer
Few microbes (~a few dozen species) directly cause cancer. Many may be involved, and, perhaps several can promote host antitumor immunity. The gut microbiome has powerful effects on immunity by modulating primary and secondary gut lymphoid tissue against cancer and may be involved in tumor immune surveillance. There is also evidence of bacteria within tumors in at least 10 different cancer types. The implications of this are not yet known. Of the multiple billions of microbe species on the earth, just 11 are considered human cancer-causing agents, and account for about 13% of global cancer cases. (Sepiche-Poore) Large-scale clinical trials are underway to test the value of modifying the body’s microbe environment, ranging from dietary modifications to injecting engineered bacteria into tumors. These bacterial cancer therapies, if safe and effective, could tremendously expand cancer treatment options.

The human gut microbiome consists of four phyla: Bacteroidetes and Probacteria which are Gram negative; Acenetobacteria and Firmicutes which are Gram positive. Bacteroidetes and Firmicutes comprise over 90% of the microbiome, whereas their relationship and prevalence is determined by diet, BMI and other environmental factors. Obese mice, either genetically predisposed or diet-induced, tend to display an increase in Firmicutes and a decrease in Bacteriodetes. The link between microbiota, obesity and cancer can be classified in two overlapping groups: promotion of inflammation and production of cancer-promoting substances.
The first group is inflammation. Obesity-associated inflammation may well start in the in the gut. Death of bacteria, which is happening constantly, releases lipopolysaccharide (LPS). LPS then causes a downstream set of actions that include the release of cytokines, including NF-kB, IL-1, IL-6 and TNF-a. Under normal conditions the gut barrier allows only a minimal amount of LPS to enter circulation. LPS levels in obesity are at least doubled. Obesity leads to gut barrier dysfunction and other resulting cascading events, which eventually set the stage for cancer development.
The second group of microbiota-related cancer promotion is the generation of toxic metabolites. Obesity and high-fat diet associated changes in intestinal mi-
162 Super Charge Your Health To Protect Yourself Against Cancer
crobiome have been associated with altered bile acid metabolism, with increased production of deoxycholic acid (DCA). High fat diet fed mice had higher levels of serum DCA. DCA suppresses p53. (p53 is crucial in preventing cancer formation, functioning as a tumor suppressor. p53 has been described as “the guardian of the genome” because of its role in conserving stability by preventing genome mutation). Also, DCA causes DNA damage through ROS formation. The cancer promoting environment created by DCA, plus cytokines secreted from old and dying cells, favor HCC genesis and progression.
Microbes and microbial functions may help promote cancer development but can’t cause cancer by themselves. This happens because of the many immune modifying functions of microbiota and their active metabolites could affect tumor development and can be linked to the immune system’s role in the development of solid tumors. The immune system rarely initiates a lesion but can facilitate progression through tumor-tissue feedback loops, inflammation, or dysfunctional immune surveillance.
Of the trillions of microbes across the body, ~97% are in the colon, ~3% are everywhere else. Viruses may be more diverse and in greater numbers. Most of their related immune actions are in the gut, the largest immune organ in the body. There are something like 0.68% bacteria in cancer tumors across all cancers. Individual tumors range from no bacteria to 70% by cell count.
The gut microbiota can regulate the immune tone of the tumor microenvironment, now called the immune-oncology- microbiome (IOM). The gut microbiome can regulate many functions of the human bodies with tumors, typically through immunomodulation. Known microbial mechanisms can manipulate components of the gut cell barrier, modulate primary and secondary gut lymphoid tissue activities.
The gut microbiome has effects on adaptive immunity, the tumor microenvironment and effects on the use of anticancer drugs. The intestinal ecosystem can influence both local and distant cancers by impacting their immune context, influx of immune cells from the circulating blood, and inflammatory and metabolic patterns. Given that the intestinal barrier offers the largest host-microbial interface and greatest microbial diversity, investigations on the potential impact of the microbiota in oncogenesis or cancer prognosis have primarily focused on this barrier.
An intact gut microbiome has been shown to be necessary to prevent leukemia progression in genetically predisposed mice.
The use of antibiotics in cancer is limited to addressing or preventing known microbial carcinogens. This includes treating H. pylori-derived gastric lymphomas, using direct-acting antivirals against active Hepatitis C virus, and vaccinating against major human papillomavirus serotypes and hepatitis B virus to prevent urogenital, cer-
163 Super Charge Your Health To Protect Yourself Against Cancer
vical, head and neck, and liver cancers. But there is evidence that systemic antibiotics affect immune responses and decrease patient survival.
Prebiotics (molecules that promote growth of beneficial microbes) such as resistant starch, inulin, and mucin are promising in preclinical studies, improving antitumor immunity and therapy response in melanoma and colon cancer.
There are cause-effect relationships between microbiome composition changes and compromised tumor immunosurveillance, even affecting malignancies beyond the intestine. In other words, the gut microbiome can have both cancer inhibiting and promoting effects. Because the gut microbiome is so complex and vast, it becomes challenging to generalize about how to affect the microbiota with specific prebiotic/ probiotic recommendations.
Few commercially available probiotic formulations have been tested for impact on antitumor and systemic immunity, with certain formulations (VSL#3) increasing tumor growth in a study in mice. How relevant this is for humans is unknown. In critically ill patients, commercial probiotic use may even cause spread of the bacteria into the bloodstream, called bacteremia. Analysis of cases of Lactobacillus bacteremia in ICU patients at Boston Children’s Hospital showed that patients receiving Lactobacillus rhamnosus strain GG (LGG) probiotics had a markedly higher risk of developing Lactobacillus bacteremia than those who received no probiotics. (Yelin) Unfortunately, bacteremia may lead to sepsis or infections in organs. Therefore, indiscriminate administration of commercially available probiotics in cancer patients should be done with caution.
While there may be opportunities for enhancing the care of cancer with pre/probiotics, i.e., microbiome-based approaches, it should be done with caution as this point until there is more safety and value information.
Obesity and cancer
Worldwide, the burden of cancer attributable to obesity, expressed as the population attributable fraction, is 11.9% in men and 13.1% in women.Metabolic conditions like obesity and diabetes account for 6% of all new cancers worldwide. (Karra) There is convincing evidence that excess body weight is associated with an increased risk for cancer of at least 13 anatomic sites, including endometrial, esophageal, renal and pancreatic adenocarcinomas; hepatocellular carcinoma; gastric cardia cancer; meningioma; multiple myeloma; colorectal, postmenopausal breast, ovarian, gallbladder and thyroid cancers. (Avgerinos)
The prevalence of overweight and obesity has reached pandemic levels of 60-70% of the adult population in industrialized countries, with more in females and in urban areas. The global prevalence of overweight and obesity has increased by 27% in adulthood and 47% in childhood during the last several decades.
164 Super Charge Your Health To Protect Yourself Against Cancer
The table below provides a summary of the strength of the evidence for the risk of obesity causing specific cancers.
Evidence level
Strength of Relative Risk Increase for Obesity and Cancer Risk
Convincing/Sulficient High (RR tncrease>3)
Endometrial adenocarcinoma
Esophiageal adenocarcinoma
Modest (RR increase:1.50-2,99) Little (RR increase:1.00-1,49)
Renal adenocarcinoma
Hepatocellular cancer
Pancreatic adenocarcinoma
Gastric cardia cancer
Mulúple myetoma
Meningioma
Colorectal cancer
Postmenopausal breast cancer
Gall bladder cancer
Ovarian Cancer
Thiyroid Cancer
Limited
Advanced stage prostate cancer
Male breast cancer
Diffuse large B-cell Iymphoma
Table 4. Avgerinos
Epidemiologic evidence associating overweight/obesity and cancer risk by level of evidence and strength of Relative Risk increase for overweight/obesity in comparison to normal-range body mass index (18.5-24.9 kg/m2) defined by the WHO as synopsized by the IARC Working group in 2017.
Overweight and obesity are generally currently defined as a Body Mass Index (BMI) between 25-29.9 kg/m2 and over 30 kg/m2 respectively. Avoiding excess body weight reduces the risk of the above noted malignancies. There is some evidence of a probable protective effect, for premenopausal breast cancer, and cervix, oral, oropharyngeal and larynx cancers. The strongest evidence is for obesity and cancer is mostly for cancers of the digestive and hormone sensitive organs in women. Obesity is associated with improved survival in non-small cell lung, renal cell and metastatic colorectal (CRC) cancers.
Metabolic syndrome, which is usually part of the complex of factors associated with obesity is a metabolic dysfunction. Metabolic syndrome is diagnosed by having three or more of the following: increased waist circumference, triglycerides, fasting blood glucose, or blood pressure, and/or low HDL-cholesterol. These are independent cancer risk and prognostic factors, even among individuals with a body mass index (BMI) in the normal range.
165 Super Charge Your Health To Protect Yourself Against Cancer
Biological mechanisms linking overweight/obesity to cancer
The most important factors appear to be the contribution of the triad of overweight/ obesity, insulin resistance (IR) and adipocytokines (cytokines produced by fatty tissue) in cancer. The main pathways linking obesity and adipose tissue pathology to cancer are:
1. Hyperinsulinemia/ IR and abnormalities of the insulin-like growth factor-I (IGF-I) system and signaling;
2. Sex hormones biosynthesis and pathway;
3. Subclinical chronic low-gradeinflammation and oxidative stress;
4. Alterations in adipocytokine pathophysiology;
5. Factors deriving from ectopic fat deposition;
6. Microenvironment and cellular perturbations;
7. Factors causing obesity and cancer such as disruption of circadian rhythms and dietary nutrients;
8. Altered intestinal microbiome; and 9) mechanical factors.
In this Figure 13, a relative risk (RR) of one is considered neutral. Anything above that would be increased risk. For example, of 1.3 as seen for women with BMI between 30 – 34.9, indicates 30% increased risk over normal. An RR of ~1.6 would mean a 60% increased risk over normal. So, as a graph indicates increasing levels of BMI are associated with an increased RR for cancer death.
https://sphweb.bumc.bu.edu/otlt/MPH-Modules/PH/PH709_Cancer/PH709_Cancer10.html
166 Super Charge Your Health To Protect Yourself Against Cancer
Women Men Body-Mass Index 18.5 - 24.9 25.0 - 29.9 2.0 1.5 1.0 0.5 0.0 30.0 - 34.9 35.0 - 39.9 ≥40.0 Relative
Death
Risk of Cancer
Specifically, these are:
● Insulin-like growth factors (IGFs), are made in almost any tissue in the body, and are important in normal growth, development, and survival. Synthetic growth hormone and IGF are implicated in the
● Hormone and IGF are implicated in the development of cancer. IGF overexpression by cancer or tissue cells as well as IGF-I receptors made by the cancer cells could exert tumor growing actions by promoting cell cycle progression and inhibition of apoptosis. Increased serum IGFs levels have been seen as having an elevated risk for several cancers, particularly prostate, colorectal and breast cancer.
● Type 2 diabetes (DM II) consistently elevates the risk of pancreatic, biliary tract, and esophageal cancer in men; breast and endometrial cancer (EC) in women; and kidney, liver and CRC in both genders. Those with DM have a higher cancer mortality in a variety of malignancies compared with non-diabetic controls. Obesity is associated with increased adipose tissue inflammation manifested as the secretion of pro-inflammatory cytokines and alterations in the pattern of adipokine secretion.
● Insulin resistance (IR) is shown by elevated HbA1C and C-peptide serum levels. C-peptide serum levels are a more sensitive indicator of early phases, when HbA1C is still in the normal range. C-peptide levels have been associated with the risk of CRC. Insulin may promote cancer directly and indirectly; stimulation of cancer is by the insulin receptor or IGF. Insulin increases the metabolic activity of the cell, leading to increased oxidative stress that causes DNA damage.
Cancer cells are in a constant need of increased glucose supply which is supported by the high blood sugars seen in diabetes. The high blood sugars provide tumors with more glucose that then enhances their growth and progression, leading to decreased survival. High HbA1c’s have been positively associated with various malignancies; breast, colorectal, gastric, pancreatic, and liver cancers.
One of the common treatments for DM II is metformin. People who receive metformin appear to have a lower risk in cancer development. Metformin induces liver glucose production and reduces IR in peripheral tissues resulting in lower insulin and IGF1 levels. Moreover, it leads to activation of 5’ AMP-activated protein kinase (AMPK) affecting the mTOR pathway that is crucial for cell proliferation.
Sex hormones, commonly associated with increased risk of cancer, or produced in peripheral fatty tissue. Androgens and their precursors are converted to estrogen by aromatase. So, the higher aromatase levels in obesity lead to higher estrogen levels. Increased estrogen levels in women with higher BMI seem to account for the cancer risk associated with BMI in postmenopausal ER+/PR+ breast cancer. The reduced risk for breast cancer in obese premenopausal women is thought to be a result of increased ovarian androgen production. On the other hand, elevated androgens are associated with increased risk of breast cancer regardless of menopausal status.
167 Super Charge Your Health To Protect Yourself Against Cancer
Obesity is associated with a 2.6 fold higher risk of endometrial cancer (EC). Estrogen promotes EC by induction of IGF-I resulting in stimulation of cell proliferation and inhibition of apoptosis. Bioidentical progesterone opposes estrogen effects by binding IGF-I. So, it appears that unopposed estrogen is the main contributor to EC. High ovarian androgens may also be a contributing factor.
Biomarkers.
There are biomarkers linked to inflammation, insulin sensitivity, and liver function that are commonly dysregulated in metabolic disease. These are C-reactive protein (CRP), C-peptide, alanine aminotransferase (ALT) and aspartate transaminase (AST), and more comprehensive indicators of central adiposity (e.g., visceral to subcutaneous adipose tissue ratio (VAT:SAT)).
Metabolic obesity in thosewith normal weight.
Up to a third of lean individuals have metabolic syndrome parameters out of the clinical range that often go undiagnosed. Eight studies defined hyperglycemia according to HOMA-IR ≥ 2.5 or ≥ 3.0, elevated HbA1c ≥6.5%, or a diagnosis of diabetes. One study defined hyperglycemia as having a non-fasting blood glucose ≥125mg/dL.
Other than externally obvious fatty tissue, fatty deposits in other areas of the body, are called “ectopic fat deposition.” They surround organs and blood vessels and may make people less healthy. So, these individuals may be the metabolically unhealthy obese (MUO) versus metabolically healthy obese (MHO). MHO individuals have less local “ectopic” fatty tissue surrounding organs and blood vessels. Local ectopic fat tissue, such as in breasts, bone marrow, liver, and pancreas, can be toxic and cancer producing resulting in breast, bone marrow, liver and pancreatic cancers. These local fatty tissue deposits have more pronounced inflammatory environments that could lead to cancer development.
Several studies reported higher risk of obesity-related cancer among metabolically unhealthy (MUO) individuals independent of obesity status (i.e., across all BMI categories) with RRsfor cancer ranging from 1.06 to 3.47. In these studies, smoking and alcohol had to be adjusted for in 88% of the studies. Four studies evaluated HOMA-IR in relation to breast, colorectal, and thyroid cancer risk. Sixteen studies reported that even metabolic dysfunction relative to metabolic health among normal weight individuals (BMI <25 kg/m2) was associated with increased risk of colorectal, esophageal, pancreas, bladder, endometrial, thyroid, and breast cancer.(Karra)
So, people with insulin resistance independent of adiposity still experience a cancer-promoting low-grade inflammatory state.
Lean individuals with a “lipodystrophy-like picture” comprised of central adiposity and/or ectopic fat accumulation (i.e., in tissues not suited for fat storage) may be at
168 Super Charge Your Health To Protect Yourself Against Cancer
higher risk for metabolic dysfunction and concomitantly for cancer. True lipodystrophy is a disorder that affects how the body accumulates and stores fat. In a person with this condition, fat collects in certain areas, such as the torso, face, and neck, while the legs and arms have little to no fat. The “lipodystrophy-like picture” is not the true abnormal lipodystrophy, which needs more specific and endocrine or genetic evaluation.
Cancer survivors diagnosed with metabolic syndrome.
Multiple studies reported an increased risk of not only cancer-related mortality, but also cancer recurrence among those cancer survivors with metabolic syndrome compared with those who are metabolically healthy. Added risks of up to 90% have been reported for breast and digestive tract cancer mortality.
Cancer mortality among postoperative patients.
Having cancer surgery is not the end of the therapeutic process. Metabolic syndrome has been associated with colorectal cancer-specific mortality and overall mortality, and hepatocellular carcinoma (HCC)-specific mortality. One meta-analysis saw an association between metabolic syndrome and digestive tract cancer mortality even among postoperative patients, while another meta-analysis found an increased risk of cancer recurrence and all-cause mortality.
Subclinical chronic low-grade inflammation and oxidative stress.
Obesity is a state of chronic inflammation. There are many inflammatory components in the tumor microenvironment and promote cancer development. Obese subjects in one study without fatty inflammation and metabolic dysfunction had lower cancer and cardiovascular disease risk.
The role of adiponectin and leptin and the production of cytokines in fatty tissue is reviewed in the blog: https://www.drpawluk.com/overweight-obesity-and-pemfs/
Research has shown that there is increased mortality in individuals with insulin resistance and/or elevated high-sensitivity CRP (hsCRP). The effect of systemic inflammation in cancer-related mortality was found to be more significant. To back up these observations, studies have found that reducing weight leads to reductions in inflammation. The same holds true for drugs used to treat metabolic syndrome, which raise adiponectin levels and reduce inflammation.
Cytokines and adipokines produced by fatty tissue, induce inflammation which then causes adipose tissue hypoxia. As stated elsewhere in this e-book, hypoxia is both a cause and a consequence of cancer, in a vicious cycle.
Interestingly, fatty cells next to tumors may augment tumor growth. These are called cancer- associated adipocytes (CAAs) which change their structure to become
169 Super Charge Your Health To Protect Yourself Against Cancer
more invasive. In ovarian cancer, CAA’s increase their migration and invasiveness. To make this worse, cancer and adipocyte interactions increase fatty break down (lipolysis) which provides another energy source for cancer cells. Something similar happens in prostate cancer.
In obesity, the ratio of lectin and adiponectin are disrupted. When adiponectin is produced in fatty tissue it enters the circulation. Obese individuals have lower adiponectin levels. Adiponectin inhibits proliferation of several hormonally sensitive cancers, such as endometrial, breast, prostate and CRC. Adiponectin inhibits tumor development and growth by various cellular signaling effects. It seems to have its strongest effects in the setting of a high-fat diet. Adiponectin also has an insulin sensitizing and anti-inflammatory effect. Measures of adiponectin may be useful diagnostic and prognostic biomarkers in those with cancer
Longer-term calorie restriction
Prevents adipocytes in tumors and decreased cancer promoting hormones, growth factors, cytokines and epithelial-mesenchymal transition environment (EMT) which is more amenable to the development of cancer.
Bottom line, reducing or reversing obesity is an important goal in not only the prevention but also the management of cancers. “Starving” cancers with a low-calorie ketogenic diet may be very effective in the setting of obesity. (Talib; Seyfried)
The cellular matrix of tumors, akin to the connective tissue of skin, contains mesenchymal cells (MSCs). Mesenchymal cells are small spindle-shaped cells, which multipotent stem cells that can turn into progenitor (stem) cells for all types of connective tissue, such as fibroblasts, osteoblasts, chondroblasts and preadipocytes. MSC’s are in the circulation and can be recruited to tumor sites under the influence of various signals, including inflammation and/or hypoxia. While most of these are considered produced in the bone marrow, white adipose tissue in obese individuals is another site of production of MSC’s. These then can serve as a source for cancer stem cells and are able to migrate to various parts of the body.
Factors that contribute to the development of obesity and cancer
Some of these factors include:
● Sleep disruption which affects glucose regulation and energy balance and contribute to obesity.
● Diets and nutrition. Red and processed meat consumption, which is common among obese people, is strongly associated with stomach, colon and rectal cancer [165, 166]. In contrast, high fiber consumption (vegetables and fruits), not usually consumed by obese people, decreases the risk of developing CRC.
170 Super Charge Your Health To Protect Yourself Against Cancer
● Altered intestinal microbiome. The link between microbiota, obesity and cancer is discussed more extensively in the microbiome section further on in the e-book.
● Mechanical factors. Obesity increases abdominal pressure resulting in relaxation of the lower esophageal sphincter (LES). Due to a relaxed LES, the esophageal mucosa has more direct exposure to gastric acid leading to gastro-esophageal reflux (GERD). Chronic GERD then leads to Barett’s esophagus and eventually esophageal cancer.
Bottom line, reducing or reversing obesity is an important goal in not only the prevention but also the management of cancers. “Starving” cancers with a low-calorie ketogenic diet may be very effective in the setting of obesity. (Talib;Seyfried)
Adequate intensity level PEMF therapy of the abdomen can significantly decrease inflammation in the abdomen leading to other significant downstream benefits, not just for cancer. (See PEMF section below)
Hyperbaric Oxygen Therapy (HBOT) and cancer
I frequently recommend HBOT for individuals with cancer, at least for a few sessions, because it would be helpful for helping with the hypoxia frequently seen in cancers and they often compromise circulation around tumors.

The FDA has outlined the conditions for which HBOT is indicated, which doesn’t include any references to cancer, other than for delayed radiation injuries. Conditions for which hyperbaric chambers are cleared for marketing by the FDA. FDA clearance of a medical device includes a determination that the device has the same intended use as, and is as safe and effective as, another legally U.S.-marketed device of that type.
171 Super Charge Your Health To Protect Yourself Against Cancer
See: https://www.fda.gov/consumers/consumer-updates/hyperbaric-oxygen-therapy-get-facts
As of July 2021, the FDA has cleared hyperbaric chambers for the following disorders:
● Air and gas bubbles in blood vessels
● Anemia (severe anemia when blood transfusions cannot be used)
● Burns (severe and large burns treated at a specialized burn center)
● Carbon monoxide poisoning
● Crush injury
● Decompression sickness (diving risk)
● Gas gangrene
● Hearing loss (complete hearing loss that
occurs suddenly and without any known cause)
● Infection of the skin and bone (severe)
● Radiation injury
● Skin graft flap at risk of tissue death
● Vision loss (when sudden and painless in one eye due to blockage of blood flow)
● Wounds (non-healing, diabetic foot ulcers)
Once someone has their own higher intensity PEMF system for daily home use, HBOT may not be necessary. HBOTand PEMF therapy are expected to produce similar results by virtue of their action on increasing the delivery of oxygen into the tissues. Other than oxygen delivery and the downstream benefits of that, the list of benefits or actions from HBOT are much more limited than the right PEMF therapy.
Early in the history of HBOT, there had been concern that HBO could promote cancer growth because it would be providing oxygen to the growing cancer. However, in the early 2000s a couple of review studies determined that HBO did not promote cancer growth. (Moen) what the research has basically shown is that prolonged levels of high oxygen that increased reactive oxygen species (ROS) overwhelm the antioxidant defenses of cancers that led to cellular damage. There is some research to support that HBOT can induce apoptosis of cancer growth. One of the concerns for HBO is that it would increase angiogenesis, necessary for cancer growth. Multiple studies showed that there are no changes in angiogenesis. There was also a concern that HBO may increase metastatic spread. Likewise, there was no increase in metastatic spread after HBO. In fact one study showed that HBO may lead to a less aggressive tumor type in breast cancer. Likewise, HBO appears to reduce chemotherapy resistance by increasing tumor circulation and cell sensitivity. In fact, some researchers found that the uptake of chemotherapy is increased for the time of and immediately after HBOT. It appears that making chemotherapy work better relies on the HBOT being given during the time of chemotherapy or immediately after, when the oxygen levels are elevated. On the other hand, there may be some chemotherapy agents for which HBOT is contraindicated due to the potential for increasing toxicity of these agents. Relative to radiation, it appears that this should be done immediately after but not concurrently with HBOT. One of the tumor types that is especially susceptible to HBOT is breast cancer. It appears that HBOT has a strong
172 Super Charge Your Health To Protect Yourself Against Cancer
anti-angiogenic effect. There may be significant variation in the effectiveness of HBO with different cancer types. Further research is needed to clarify HBOT’s value in various types of cancer.
Combining HBOT and PEMF
On review of the PEMF literature, there was no research available that compared HBOTuse with or to PEMF therapy. Much of the research done on HBOT in the setting of cancer involved its use in reducing harm and damage from radiation therapy. There are few reports of the use of HBOT in the setting of cancer outside radiation therapy.
One report looked at the use of HBOT for lymphedema following breast cancer treatment (Ammitzboll), which includedsurgery, axillary dissection and radiotherapy. Those women receiving HBOT experienced improved QOL without consistently significant changes in arm mass, volume or lymphatic drainage. In another study looking at lymphedema after surgery or radiation (Teas) Ten healthy postmenopausal women (average age 58) with persistent (0.3-18 years) arm lymphedema following breast cancer surgery and radiation (n = 10) plus chemotherapy (n = 7) received 20 HBO treatments (90 minutes at 2.0 ATA five times a week for 4 weeks). End points included changes in upper extremity volume. We observed a 38% average reduction in hand lymphedema at the end of HBOT. For those 8 who benefited, the reduction was persistent from the end of treatment to a final measurement an average of 14 months after the last HBO treatment. However, total limb volume did not change significantly. These results are the opposite of those found in the Russian literature discussed below.
HBOT was not found helpful in preservation of erectile function after radical prostatectomy. (Chiles) A study on the use of HBOT preoperatively once prior to surgery for pancreatic ductal adenocarcinoma and compared to the control group, reduced the complication rate. (Bosco) HBOT was also studied in 232 individuals after resection of meningiomas who also had with conspicuous peritumoral brain edema (PTBE). (Tang) On the third day after operation, the Karnofsky performance score (KPS) and focal brain edema in the operative region between the HBOT Group and the Control Group were not significantly different (p > 0.05), but 15 days after surgery, compared with the Control Group, the KPS of the HBOT Group appeared obviously higher (p < 0.05), and the focal brain edema in the operative region was definitely smaller (p < 0.05). Six months after surgery, the volume of brain damage (encephalomalacia) in the operative region and the number of individuals with neurological deficits in the HBOT Group were significantly less than those in the Control Group (p < 0.05). Intraoperative blood loss and the need for postoperative transfusions is significant after resection of hepatocellular carcinoma (HCC).
A study was done (Ueno,2009 ) Forty-one consecutive patients who showed Hb level < 9.0 mg/dl at the end of hepatic resection were randomly assigned to a control
173 Super Charge Your Health To Protect Yourself Against Cancer
group (n = 21) or an HBOT group (n = 20). HBOT at 2.0 atm. with inhalation of 100% oxygen for a duration of 60 min was performed at 3, 24, and/or 48 h after the end of the hepatectomy. When compared to the control group, the HBOT group showed better changes in O2levels., serum lactate, and bilirubin levels for the first 3 postoperative days following surgery. Additionally, the HBOT group did not experience any fatal complications and had a lower incidence of postoperative hyperbilirubinemia than the control group. We also observed that postoperative NK cell activity and cancer-free survival in the HBOT group tended to be better than in the control group, in fact, six individuals in the HbO2 group experienced intraoperative bleeding and had O2 levels (<50%), had significant improvements in their O2 levels and serum lactate.
Work in an animal cancer model suggests that pretreatment with HBOT can improve tumor circulation to render chemotherapy more effective. (Heys) In follow-up, 32 women with locally advanced breast carcinoma (>5cm diameter) entered a randomized clinical trial where a course was administered of six intravenous pulses of chemo. In the case group this was preceded by 10, once daily, sessions of HBOT administered either at 2.4 or 2.0 atmospheres absolute. Eleven out of 15 subjects tolerated a full course of HBOT and chemotherapy. Tumor extravascular extracellular or edema fluid was reduced after HBOT but there was no reduction in tumor cell volume and no indication of increased vascularity on MRI. Clinical and pathological responses to chemotherapy were the same in both groups and there was no evidence of neovascularization. Five-year survival in those who tolerated the trial regime was 73% and did not differ between the groups. Unfortunately, this study shows that HBOT used this way does not seem to increase survival any better than usual care.
Cancer is common and radiation therapy (RT) is one well-established treatment for some solid tumors. HBOT may improve the ability of radiotherapy to kill hypoxic cancer cells, so the administration of radiotherapy while breathing HBOT may result in a reduction in mortality and tumor recurrence. A review (Bennett) of was conducted of published studies of randomized and quasi-randomized studies comparing the outcome of malignant tumors following radiation therapy while breathing HBOT versus air in November 2004 using The Cochrane Central Register of Controlled Trials (CENTRAL), Nineteen trials contributed to this review (2286 patients: 1103 allocated to HBOT and 1153 control). With HBOT, there was a reduction in mortality for head and neck cancers at both one year and five years after therapy of around 17 – 18%, as well as improved local tumor control at three months of 42% with HBOTT. There were variations in results with different radiation schemes. Local tumor recurrence was less likely with HBOT at one year (head and neck, 34%, two years (uterine cervix 40% and five years for head and neck at 27%. Unfortunately, there was a significant increase versus the control group in the rate of both severe radiation tissue injury (235%) and the chance of seizures during therapy (676%) with HBOT. These kinds of complications would not be expected with PEMF therapy, since any oxygen improvement would be induced without the use of pressure, that could
174 Super Charge Your Health To Protect Yourself Against Cancer
result in oxygen toxicity. Since there has been concern about increasing oxygen saturations in cancers, and the potential for interference for the benefits of radiation, this study seems to indicate that if anything, increasing oxygen saturation may sensitize the tissues to the effect of radiation.
The last reported study evaluated the effect of HBOT on post liver resection damage of liver cells by activated neutrophils. (Ueno, 2011) 12 non-cirrhotic patients (Group H), who underwent elective hepatectomy for liver cancer, were given 2 courses of HBOT: 2.0 atm with inhalation of 100% oxygen, for 60 min, at 3 hours and 24 hours after hepatectomy; they were then compared with the 12 patients (Group C) who had received usual treatment. The 12 group H individuals had lower leukocyte levels compared to group C. Group C individuals had a greater than 10% increase in the CD18 cancer maker at 12 hrs. After surgery. The group H CD18 levels were suppressed compared to group C. No individual in Group H had post-operative hyperbilirubinemia or hepatic failure; However, 3 in a group C had post-operative bilirubin elevation and 1 had intraperitoneal infection. This is an indication of HBOT helping with reduction of postop inflammation, and effect comparable to PEMF therapy.
Spontaneous Remissions of Cancers
I developed an interest in spontaneous remissions (SRs) in the 1970s after reading a book about evaluations of these phenomena that were being done on people treated at the Rosswell Park Cancer Center in Buffalo, New York. Also around that time a friend of mine had a colleague who reportedly had a spontaneous remission of a brain tumor. He did intensive guided imagery, significant lifestyle changes, self-hypnosis and meditation. At that time he had survived his lethal brain cancer by several years, without surgery, chemotherapy or radiation.
It was after this in 1992 that I read the Getting Well Again book by Dr. Carl Simonton. He was a strong proponent of guided imagery. In addition he listed a number of elements needed to be in place for an effective cancer care program, with a focus on the individual.
The following table shows the emphasis on many aspects of psychology and belief as part of the cancer care program.
175 Super Charge Your Health To Protect Yourself Against Cancer
Table5: Outline of chapters from Getting Well Again book by Carl Simonton
Part One: The Mind In Cancer
● The Mind-Body Connection: A Psychological Approach To Cancer Treatment
● Mysteries Of Healing: The Individual And His Beliefs
● The Search For The Causes Of Cancer
● The Link Between Stress And Illness
● Personality, Stress, And Cancer
● Expectations About Cancer And Their Effect On Recovery
● A Whole Person Model Of Cancer Recovery
Part Two: Pathways To Health
● The Program: Putting It To Work
● Participating In Your Health
● The “Benefits” Of Ilness
● Learn To Relax And Visualize Recovery
● The Value Of Positive Mental Images
● Overcoming Resentment
● Creating The Future: Setting Goals
● Finding Your Inner Guide To Health
● Managing Pain
● Exercise
● Coping With Fears Of Recurrence And Death
● The Family Support System
In 2011 Dr. Bernie Siegel wrote his book Love, Medicine and Miracles: Lessons Learned about Self-Healing from a Surgeon’s Experience with Exceptional Patients, building on the importance of beliefs and positive emotions in creating opportunities for healing, or even, miracles.
From a medical perspective, it was hard to explain SRs remissions. If these were better understood and less left to beliefs in “miracles,” it is assumed that these may be able to be more common and available to average people. Once researchers began to accumulate “cases” of spontaneous remissions, evaluate them for commonalities that may be explained from a medical perspective, these circumstances could be more readily duplicated through commonly available and acceptable techniques.
As a result, numerous studies have now been reported about SR’s and some sense has now developed about “medically understandable” reasons for them. SRs may happen in 1:60,000–1,00,000 cancers. Melanoma, lymphoma, leukemia, neuroblastoma, renal cell carcinoma, and germ cell cancers seem to be more common SRs.
176 Super Charge Your Health To Protect Yourself Against Cancer
However, not all SRs can be explained medically. Dr. Kelly Turner interviewed many holistic and integrative cancer clinicians and many individuals with reported SRs and summarize these findings in her book “Radical Remission.” She outlines 9 key factors that are most commonly associated with the possibility of an SR happening:
1. Radically Change Your Diet,
2. Taking Control Of Your Health,
3. Following Your Intuition,
4. Using Herbs And Supplements,
5. Releasing Suppressed Emotions,
6. Increasing Positive Emotions,
7. Embracing Social Support,
8. Deepening Your Spiritual Connection, and 9. Have A Strong Reason For Living.
Many more books are now beingpublished about people’s experiences with SRs. Many of the aspects of Dr. Turner’s findings are common through this literature and can become roadmaps for people healing or the least having a better journey in their cancer management program. Unfortunately, medical doctors, oncologists, radiation therapists and surgeons have no confidence in anything other than conventional medicine and rarely recommend alternatives.
177 Super Charge Your Health To Protect Yourself Against Cancer
In line with a scientific approach to SRs a large database has been developed and continues to collect cases, reports and evidence of SRs. This library is now being held at the Institute of Noetic Sciences. In 1993, they published Spontaneous Remission: An Annotated Bibliography. In this work, the authors, Caryle Hirshberg and the late Brendan O’Regan, defined spontaneous remission as “the disappearance, complete or incomplete, of a disease or cancer without medical treatment or treatment that is considered inadequate to produce the resulting disappearance of disease symptoms or tumor.”
Because there was no standard reference for the field of spontaneous remission before that time, the Remission Project cataloged the world’s medical literature on the subject and the resulting book was the largest database of medically reported cases of spontaneous remission in the world, with more than 3,500 references from more than 800 journals in 20 different languages. For the Online Spontaneous Remission Bibliography Project, they used the published original SR report work and provided additional data for an online copy of the Remission Database. Spontaneous Remission: An Annotated Bibliography
January 1, 1993. Marilyn Schlitz, PhD. https://noetic.org/publication/spontaneous-remission-annotated-bibliography/
Reviews of this science has shown that infection mediated immune system activation, biopsy procedures, and disruptions of the tumor microenvironment play pivotal roles in the self-healing of many tumors. Bacterial and viral infections are especially well documented in instances of SR. Even as early as 1868, William Busch reported spontaneous tumor regressions in patients with Streptococcus pyogenes infections. These concepts and findings are now being used as a bacteria mediated Bacillus Calmette-Guerin (BCG) approved treatment option for non-muscle-invasive bladder cancer (NMIBC). Similarly, there is now the first engineered cancer killing (oncolytic) herpes simplex virus (HSV) for some forms of advanced melanoma. A number of the immune stimulation strategies, often involved in SRs, include: endocrine factors, herbal medicines, transfusions, surgical removal of tumors, infections and fever. Again, most of these observations and findings relate to biomedical perspectives. (See Figure 13 below).
Investigating SR case reports in the light of diet and microbiome composition of the recovered patient may aid in developing novel therapies with reduced side effects. Further, insights from these studies may help predispose and orient one’s lifestyle towards conditions that are barren for cancer cells to flourish.
The increase in scientific interest in SR’s is helpful so that the medical oncological treatment community is becoming more accepting of the concept. Unfortunately, insurance coverage for comprehensive cancer care is limited mostly to the medical side of care and not the nutritional, supplement, mental, emotional and spiritual sup-
178 Super Charge Your Health To Protect Yourself Against Cancer
ports needed for the most effective cancer care. For these reasons, many of these support strategies need to be paid for out-of-pocket.
Factors that stimulate an immune response, including fever and infection, may promote SR. Similarly, disruption in the tumormicroenvironment, biopsy and ablation procedures and the induction of cell death by various means, may also induce SR.
Figure 14. Possible mechanisms involved in SR of cancers.
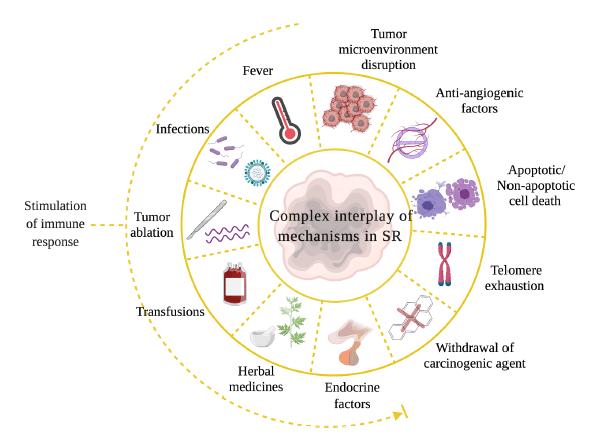 FROM: Radha
FROM: Radha
Dr. Dwight McKee holistic oncologist
I did some training with Dr. Dwight McKee, a holistic oncologist with 25 years of experience and being doubled certified in hematology and oncology, made some observations some interesting observations about the behavior of cancer during the Institute of Functional Medicine (IFM) Cancer Symposium.
The natural course of some cancers is to remain dormant or spontaneously regress.
Prostate cancer
60% of men in their 60s have cancer cells in the prostate in a large autopsy study. Only 3% of the men died of prostate cancer. There is a strong possibility that the natural course of some prostate cancers is to remain dormant through a man’s life or spontaneously regress.
Kidney cancer
80% of small kidney cancers remain stable or regress after three years. In metastatic stage IV kidney cancer, 6% of those given placebo treatments had stable disease or regression.
179 Super Charge Your Health To Protect Yourself Against Cancer
Cervical cancer
60% of the time, precancerous cervical cells revert to normal within a year; 90% revert in three years.
He stated that there is an old view and a new view of cancer.
Old view
Cancer is an inevitable linear process progressively accumulating mutations, until it grows into a tumor.
New view
Early cancers may spontaneously regress; established cancers may remain dormant.
Other observations:
● A 5 mm³ of tumor may have as many as 1 billion malignant cells.
● In early breast cancer, studies found 30-50% were positive for tumor cells in blood or bone marrow.
● In another study, they took multiple bone marrow samples from time of diagnosis to the end of treatment: at least one biopsy was positive in 100% of the individuals.
● Non-small cell lung cancer: 40% in stage I/II with positive bone marrows had a higher rate of recurrence.
● Micro-metastases in bone marrow may not be predictive of tumor recurrence.
● Cancer cells and terrain: permissive = tumor; nonpermissive = no tumor.
● Immunosuppression creates a highly permissive terrain.
● Tumors disable/inhibit the immune system. Reducing tumor burden allows the body’s own defenses to finish the job and to maintain residual tumor cells in a dormant state.
● Mind-body observation: “pilgrimage effect” – the further the patient travels to get to a clinical trial, the better the outcome. There was 1/3 the risk of dying if they lived > 15 miles away.
● Dean Ornish: there is a shift in tumor gene expression with diet and lifestyle changes. More available nutrients may directly affect tumor cells and/or the terrain/microenvironment.
Testing for Cancers
This topic is too extensive to cover in this e-book.However there is one new test that I recently became aware of that provides exciting opportunities to detect about 50 different cancers much earlier than usual. This is called the Galleri test. (galleri.com) It needs to be ordered by a doctor.
180 Super Charge Your Health To Protect Yourself Against Cancer
It is a multi-cancer early detection test that looks for a signal shared by 50+ types of cancer with a single blood test. If a cancer signal is detected, Galleri predicts the tissue type or organ associated with the cancer signal with 88% accuracy to help guide follow-up diagnostic testing which may include lab work or imaging to confirm cancer. The Galleri test is recommended for adults with an elevated risk for cancer, such as those aged 50 or older. The Galleri test is available by prescription only. Use of Galleri is NOT recommended in individuals who are pregnant, 21 years old or younger, or undergoing active cancer treatment.
Galleri checks more than 100,000 DNA regions and over a million specific DNA sites to screen for a signal shared by cancers that could be hiding. The Galleri test looks for cell-free DNA and identifies whether it comes from healthy or cancer cells. DNA from cancer cells has specific methylation patterns that identify it as a cancer signal. Methylation patterns also contain information about the tissue type or organ associated with the cancer signal to guide next steps.
Small amounts of DNA shed from cancer cells may appear in the blood significantly sooner than circulating tumor cells, allowing detection much sooner than usual with most other testing.
The figure below shows that the lowest counts of ctDNA occur in the subclinical phase of disease, the optimal time for detection and developing strategies for preventing progression. The levels increase until clinical/radiologic sensitivity threshold is exceeded. Treatment then should decrease the levels, after which monitoring would occur for detection of residual disease and the early diagnosis of relapse. Relapse would include the identification of mutations related to resistance against treatment.
Figure 8. Circulating tumor DNA (ctDNA) applications for ovarian cancer management.
181 Super Charge Your Health To Protect Yourself Against Cancer
FROM: (Mari)
Detecting cancers at a subclinical stage is ultimately the most effective screening strategy.
Combining cancer therapies
Comprehensive cancer management is amazingly complex. (Aljurf) there are an extraordinary number of therapeutic tools available. Because the cancer process itself over the entire spectrum of cancer, from prevention, acute care, health maintenance, chronic care, palliative care and end-of-life care, multiple approaches are the most likely to provide the best results. A “one-size-fits-all” approach is not possible. In addition, various parts of the health care “universe” often communicate and coordinate poorly with each other. In the end, life is “terminal” for all. There is no “cure” for life. The diagnosis and journey of cancer and its care is highly individual and unique. All care systems need to recognize and respect this. Most of the time results cannot be guaranteed.
Recognizing the above, it’s very important, and even necessary, to combine various therapies, modalities and support approaches. The above information provides a fragment of a picture on approaches to consider in the management of cancer. No one modality is paramount over any other. Sequencing modalities and dosing of therapies in a useful order is important.
After 50 years of practicing medicine, most of that as a family physician, and about 20 years of practicing holistic medicine, I have realized how little control I have over the care process and the results. People do poorly, who I wouldn’t expect, and people do exceptionally, likewise. Most of the time it’s about taking one step at a time.
All of this applies to the use of PEMF therapies, not only for general health, a myriad of medical problems and health conditions, but also in the care of individuals with cancer. The best outcomes happen when there is coordination between PEMFs, nutrition changes, nutritional therapies (whether oral and/or intravenous), medical therapies
182 Super Charge Your Health To Protect Yourself Against Cancer Screening/ early diagnosis Prognosis Treatment monitoring Detection of residual disease Early diagnosis of relapse Identification of resistance mutations Subclinical disease Clinical/radiological sensitivity threshold Tumor burden ctDNA sensitivity threshold Treatments Follow-up Relapse
if necessary, preferred or desired, psychological/emotional counseling, physical therapies (such as HBOT, laser, infrared, light therapies, photo-biomodulation, IPT, ozone, bio resonance treatments, etc.), mind-body treatments (including but not limited to guided imagery, meditation, hypnosis, yoga, EMDR, tapping, etc.), acupuncture (and its related modalities), homeopathic approaches, and spiritual practices (including the help of healers, shamans, channeling, spiritual guides), Chi Gong, and others. At a minimum, I recommend nutritional and supplement approaches as a foundation, and combining it with home based daily PEMF therapy to, at the very least, control inflammation and hypoxia, increasing tissue energy and helping with tissue repair. All of these modalities are fundamentally compatible and synergistic.
How does cancer kill?
There are various ways cancer can result in death.
1. Cancer is uncontrolled growth of tissues resulting in a high metabolic demand. This often leads to anorexia and weakness.
2. Cancer cells lack normal function and can disrupt the normal body functions. For example, patients with leukemia are predisposed to infections since the white blood cells cannot function properly.
3. Patients with cancer who are also taking chemotherapy are often immunocompromised, predisposing them to infections and increasing mortality.
4. Distant spread of tumor cells is often associated with increased mortality.
5. Compression of structures by tumor cells can disrupt the normal function of vital organs.
6. Tumor cells often produce inflammatory mediators causing anorexia and pain; they also produce ectopic hormones (Para neoplastic syndromes), which causes hormonal dysfunction.
PEMF actions in the body
PEMFs stimulate the body in noninvasive and non-toxic and very safe ways.Their actions are created by the stimulation of “charge” in the tissues is the magnetic field passes through. Magnetic fields pass through the body as if it didn’t even exist, in other words, there is no difference in the motion of the magnetic field whether a body’s present or not. That is, the body is transparent to a magnetic field.
Based on Faraday’s law of charge being produced by the motion of a magnetic field, the magnetic field interacts with ions in the tissues of the body. These interactions what creates the charges. Charges are then used by the body to induce a vast range of reactions, or physiologic actions that stimulate the body to rebalance, energize or repair itself.
183 Super Charge Your Health To Protect Yourself Against Cancer
Physiologic actions of PEMFs
The specific PEMF actions that are relevant to cancer management include: acupuncture stimulation, antibacterial, anticoagulant, antiedema, autophagy, ATP, detoxification, nitric oxide, healing and regeneration, immune function, nerves, oxygenation, red blood cells and pain control.
● Acupuncture stimulation may help with symptoms specifically and in general with balancing the energy pathways of the body. Anytime a magnetic field is used on the body it will stimulate acupuncture points and meridians because the acupuncture system is a DC current system. So, not only does PEMF therapy provide all the other actions of PEMFs but stimulates the acupuncture meridian system at the same time for all the benefits derived from acupuncture therapy. The degree of stimulation of the acupuncture system will depend on the intensity of the magnetic field.
● Antibacterial actions would help with any secondary infections that often happen in those with cancer and in particular those who have been on immunosuppression.
● Anticoagulant actions are very important because cancers are associated with a lot of inflammation and therefore increase the thickness of the blood and the risks of clotting. The anticoagulant actions are also important for helping to improve circulation.
● Antiedema actions are important because of the problems associated with circulation, risks of infection, poor healing, poor tissue health in general and challenges with immune function.
● Autophagy is important for the body in general to help to recycle cells that are not healthy. Cancers often associated with unhealthy cells continuing to reproduce. Autophagy would have helped to recycle those damaged cells.
● ATP depletion in people with cancer is common because of all the different negative aspects of the cancer process. This is particularly true when chemotherapy, radiation and surgery have been used.
● Detoxification is necessary because toxicities in the body and damage cells are more prone to lead to cancerous changes. The opposite of detoxification is the PEMF-induced increased ability of cells to absorb nutrients and supplements as well as any desired medications.
● Nitric oxide is important for vasodilatation, circulation, and immune function.
● Healing and regeneration are necessary from all the damage caused by various cancer therapies and the cancer associated inflammatory process which damages tissues. Damaged tissues are more prone to progression of cancer.
184 Super Charge Your Health To Protect Yourself Against Cancer
Physiologic Actions
1. Acupuncture Stimulation
2. Anti-bacterial, - fungal, -viral, Parasitic
3. Anticoagulant Effects
4. AntiEdema Activity
5. Anti-Spasm Activity
6. Autophagy
7. ATP and Mitochondria
8. Circadian Rhythms
9. Collagen, Hyaluronic Acid, GAGs
10. Detoxification
11. Gamma Waves
12. Growth Factors And Nítric Oxide
13. Healing and Regeneration
14. Immune Function
15. Nerves and Nerve Conductivity
16. Oxygenation
17. Red Blood Cells
18. Skin
19. Stem Cell Stimulation
● Immune function is stimulated by PEMF therapy in various ways, particularly in reducing pro-inflammatory cytokines.
● Benefits to nerves happen due to damage to the nerves caused by radiation and chemoand also in helping with pain problems, particularly with the more likely to be stubborn skeletal pain.
● Oxygenation, like circulation, is very important to improve and reverse the low oxygen environments seen in solid tumors and improve the health of the tissues of the rest of the body.
● Red blood cells function better and absorb and release more oxygen, in addition to reducing the risk of anemia.
● Stress and anxiety reduction are common benefits of PEMF therapy by virtue of their effects on the brain and the hormone functions and the nervous system.
The biggest value of PEMF therapy comes from the fact that the body decides what it will do with the magnetic stimulation. It is very hard to overstimulate the body, except in circumstances of significant toxicity and energy depletion. To deal with these risks we usually recommend a “low and slow” protocol to allow the body to gradually increase its defensive and recovery capabilities. See the blog: https://www.drpawluk. com/going-low-and-slow/. Routine use of PEMF therapy helps the tissues of the body to remain in a more optimal state of functioning, therefore becoming resistant to the growth and expansion of cancers.
A common question I get asked is whether PEMF therapy will stimulate the cancer to grow? If anything, it’s well proven that PEMF therapies do not promote cancer development and in fact help the body and any other therapies work better to reduce the growth, development and spread of cancers. They clearly make any other therapies, including chemotherapy, radiation, and surgery work even better.
185 Super Charge Your Health To Protect Yourself Against Cancer
the physiologic
PEMFs
Table 6.Partial list of
actions of
PEMFs can increase the blood supply in the area of the cancer, which then flood the cancer with reactive oxygen species (oxidative stress) which are very damaging to cancer cells. While there may be a temporary increase in blood flow to a cancer, this increased blood flow also brings with it better penetration and availability of immune factors. This potential temporary increase in the size of the tumor is really only a concern when tumors are in a very tight space, such as the brain, or next to a major nerve or blood vessel. If that is the situation, then close monitoring is important to reduce any risks.
So, while the basic functions of PEMFs appear to be very desirable in helping with the fight against cancer, PEMFs need to be supported with many of the other strategies needed to help with cancer. These include proper nutrition, supplements, adequate rest, a positive mental attitude and spiritual support. I will frequently and routinely recommend IV vitamin C,ALA, and immune building supplements. HBOT, infrared, EWOT can be made even more effective with PEMF therapy.
The primary value of PEMF therapy would be daily home use, started as soon as possible in the cancer care process and continued lifetime. Daily use of PEMF therapy does not allow gaps in therapy. Even though high intensity professional use of PEMF therapy can be temporarily helpful, it is the continual daily use is the most important for ensuring a reasonable level of probable success.
Besides the conceptual and theoretical basis for the use of PEMF therapy it’s even more important that there is research to support its use and effectiveness. As will be seen in the review below, almost any other therapies will be made to work better and combined with PEMF therapy. PEMF therapy can potentially be used alone if necessary but it would be best and most effective to combine it with other treatments as mentioned above.
PEMF research in cancer
Pulsed electromagnetic fields (PEMFs) have been studied fairly extensively in the setting of cancer. I will say right at the outset, that PEMFs are not expected to cure cancer. I have treated many patients with PEMF therapies while they have been undergoing all the other therapies that medicine has to offer as well as complementary approaches. Generally, PEMFs help to sustain people through their cancer treatment process, to allow less discomfort, more effectiveness of the therapy of their choice, and a better quality of life.
How can I say this? What is the evidence for how PEMFs work in the setting of cancer? And, how can we use them to their greatest benefit?
Below I present numerous studies that have been done on PEMFs, whether in animals or humans. The amount of scientific literature on the effects of PEMFs in cancer is
186 Super Charge Your Health To Protect Yourself Against Cancer
huge and it is not possible to devote enough space in this book to the topic. So, I will, of necessity, summarize some of the more relevant studies.
Human studies are usually based on prior animal studies, so the animal studies serve as a rich resource of information for us on how cancer behaves and how various therapies may be used. Conventional medicine relies on animal and laboratory studies heavily to guide the development of human therapies. Animal studies cannot be used as absolute evidence of effectiveness, because animal physiology and cancers in animals are often different than in humans. But there are many similarities.
Animal and laboratory studies
This is a summary of the results from numerous animal and laboratory studies of how PEMF/ PEMFs:
Breast Cancer
● Inhibition of spread and growth of lung metastases in mice with human breast tumor
● Significantly reduce the growth of breast cancer tumors in mice
● Led to earlier death of breast cancer cells because of PEMF-increased mitochondrial activity
● Co-exposure of breast cancer cells to PEMFs and 7 chemo agents compounded the chemo-induced decreases in mitochondrial activity, to 15.0%, 39.5%, 11.5%, 6.0%, 18.5%, 30.5%, and 12.5% of the control for an average of 39% reduction over the chemo agents
● Reduced mouse breast cancer tumor growth, reduced vascularization and increased tumor necrosis
● Human breast cancer cells unlikely to induce breast cancer
● Do not appear to act as a promoter or DNA-damaging agent for human breast cancer cells
● Increased mitochondrial activity and caused morphological changes in breast cancer cells
Other
● Influence free radical recombination processes that activate p 53 gene dependent survival mechanisms
● Inhibit tumor growth in mice
● Static MF enhances chemotherapy in mice
● 40-50% tumor growth inhibition of human colon adenocarcinoma in mice
● MF treatment significantly increases survival time (31%)
● Affect early tumor growth as well as advanced tumors
● Affect the metastatic processes
● Inhibit preneoplastic lesions chemically induced in the rat liver
● Inhibition of angiogenesis
● Decreased growth and reduced vascularization, alone or in combination with radiation, of tumors
● Reduced the proliferation of several cancer cell types due to increased mitochondrial activity, increased energy demand, with long-term exposure to ELF-EMF
● Showed lack of adverse responses in normal cells and tissues
● Increased survival and inhibited tumor growth in mouse colon cancer
● Decreased the proliferative activity of myeloma cells by 42%
● In endometrial, ovarian and prostate cancers no change to cisplatin toxicity
187 Super Charge Your Health To Protect Yourself Against Cancer
● Affected endometrial and prostate (endocrine-related) cancers more than ovarian
● Decreased the rate of proliferation of cervical cancer HeLa cells by 15%
● Increased SOD activity two-fold after PEMF exposure for 20 min; 40 min caused even more increase, but only in lymphocytes.
The studies show that PEMFs frequently inhibit tumor growth, work cooperatively with chemotherapy to enhance the effects of chemotherapy and work across many kinds of cancer.
Effect of magnetic fields on implanted breast tumor growth and viability in mice
Commonly studied T-cell–immunodeficient Swiss mice were treated to investigate the effect of magnetic fields on tumor growth and viability. (Tatarov) A preliminary study was done to assess the impact on general health. Magnetic field exposures were 100 mT for 60, 180, or 360 min. After determining that no ill effects happened to the mice, the study mice were divided into four groups, with three mice per group, based on the above times of exposure. Mice were injected with mouse breast cancer cells. Mice in the negative control group (NCG) were inoculated with the cancer cell line but were not PEMF-exposed. Mice in the remaining 3 groups were exposed daily to 100-mT, 1-Hz PEMF for as long as 4 wk. Times of exposure were 60 min (group G60), 180 min (G180), or 360 min (G360).
Mice were monitored for tumor growth once every 2 to 4 d over the course of 4 wks with whole body bioluminescence imaging using a live imaging system. This imaging system allowed real-time monitoring of tumor growth and spread in the mice. Injected mice not exposed to the magnetic field (NCG group) developed very large tumors. NCG mice had a 500-fold increase in tumor growth at week 4 compared with week 1. Tumor growth in mice in the G60 and G180 groups also showed significant increases (900 and 200 times, respectively) at week 4 when compared with week 1. See Figure 15. The G360 group showed only a 44-fold increase in their tumor growth at week 4 vs week 1. NCG mice had the largest tumors, followed by the mice in the G360, G60, and G180 groups. The G360 group tumors had obvious signs of failing tumor growth. Cell death in these tumors was likely due to apoptosis, with fragmented nuclei characteristic of programmed cell death. Mice not inoculated with cancer cells but exposed to magnetic fields did not show microscopic changes in their lungs, liver, or skin (mammary gland) tissues.
Figure 15: Multi-fold level of luminescence increase (mean ± SEM compared with week 1 value) in tumors under different magnetic field treatment times.
188 Super Charge Your Health To Protect Yourself Against Cancer
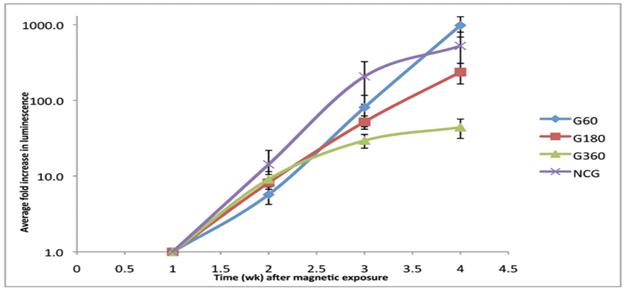 FROM: Tatarov
FROM: Tatarov
In Figure 15, the vertical line indicates the 100X, ie, the fold, change in tumor growth. 10-fold would be 10x100 times (1000%) baseline growth.
Mouse breast tumor cells grew more rapidly into grossly visible tumors in the unexposed group of mice when compared with those exposed to magnetic fields. Tumors were largest (caliper measurements) and most rapidly growing (imaging results) in non-PEMF exposed (NCG group) mice. Although tumor sizes were comparatively larger in mice exposed to magnetic fields for 360 min daily (G360 group) than in those exposed for 60 or 180 min, the G360 mice showed progressively slower decreases in the rates of tumor growth and ultimate progression. In addition, this group of mice had the most extensive areas of necrosis, as evidenced by the histopathology data. Because the imaging system detects only live tumor cells, the bioluminescence values of G360 mice were less than those of the other groups. Tumors in mice belonging to the NCG, G60, and G180 groups showed increases in tumor size and growth when measured over a period of 4 wk. In Figure 14 in the top two lines at the right (NCG/G60), the size of the tumors was the greatest followed by the third highest line (G180). The lowest growth was in the G360 line, which began a slower rise at about the 2 ½ week timeline, showing just above ten-fold growth with the next three higher lines ranging from about 100-fold to 1000-fold growth.
This study clearly shows that for a 100 mT/1000 G three times longer times of use produced better results in slowing cancer growth than lower treatment times. I have always had a concern expressed about the risks of longer exposures with PEMFs. Mice without breast cancer had no ill effects with these extended treatment times. Even with a 1000 Gauss whole body exposure of mice, who are typically more sensitive to PEMFs, there were no apparent ill effects and yet very strong tumor growth suppressing action.
One previous study by this same group found that PEMFs significantly reduced tumor growth and the amount of tumor vascularity, with a correlated increase in the amount of tumor necrosis. That study used lower strength field exposures (15 and 20 mT) and much shorter exposure periods (10 min per day). The optimal exposure regime remains unknown. We believe
189 Super Charge Your Health To Protect Yourself Against Cancer
that weaker and briefer exposures to magnetic fields are less likely to have an effect, compared with longer and stronger exposures.
A group of researchers did a study to identify tumor-specific frequencies and test the impact of administering these frequencies to patients with advanced cancer of the brain, pancreatic, ovarian, breast, prostate, lung, and bladder. (Barbault) They examined individuals with various types of cancer using a noninvasive biofeedback method to identify tumor-specific frequencies. They offered treatment to some of these individuals with advanced cancer and limited therapeutic options. In 163 patients with cancer, a total of 1524 frequencies ranging from 0.1 Hz to 114 kHz were identified. Most frequencies (57-92%) were specific for a single tumor type. Of the 28 who received these frequency exposures for 278 months (60 min treatment, 3 times/day) none had significant side effects. Three patients experienced grade 1 fatigue during or immediately after treatment. There were no significant toxicities. 13 were evaluable for response. One woman with hormone-refractory breast cancer metastatic to the adrenal gland and bones had a complete response lasting 11 months. Another woman patient with hormone-refractory breast cancer metastatic to liver and bones had a partial response lasting 13.5 months;one with non-small cell lung cancer 5.1 months; one with pancreatic cancer metastatic to liver - 4.1 months and one with leiomyosarcoma metastatic to liver - 4.0 months.
The same group of researchers studied people with advanced hepatocellular carcinoma (HCC) who had severely impaired liver function and did not qualify for standard chemotherapy or direct liver treatments. Therefore, a Phase I/II compassionate care clinical study was conducted. (Costa) In this study, 41 participants were treated with an in-the-mouth PEMF applicator PEMFs (100 Hz – 21 kHz) for 60 min (three times/day) until disease progression or death.The generator of the amplitude-modulated PEMF is a battery-driven radiofrequency (RF) PEMF generator with a stainless-steel spoon-shaped mouthpiece. The carrier is 27.12 MHz.Imaging studies were performed every 8 weeks. The primary end point was progression-free survival ⩾6 months. Secondary end points were progression-free survival and overall survival.A total of 31 individuals (76%) had radiological evidence of disease progression at the time of enrolment as defined by comparison of baseline imaging studies, with imaging studies obtained within the previous 6 months before enrolment. In all, 14 patients (34.1%) had stable disease for more than 6 months. Median progression-free survival was 4.4 months and median overall survival was 6.7 months, with one surviving 10 mos. There were three partial and one near complete responses.Estimated survival at 12, 24 and 36 months was 27.9%, 15.2%, and 10.1%, respectively.Estimated 60-day mortality was 27.8%.
Another study (Zhang) investigated the effect of PEMF treatment on tumors in mice injected with sarcoma ascites cells. Sarcomas tend to be very aggressive tumors. Sarcomas formed 4 to 5 d after inoculation. Mice were exposed to PEMF of 0.6 to 2.0 T with a gradient of 10 to 200 T/m, pulse width of 20 to 200 ms, and frequency of 0.16 to 1.34 Hz for 15 min daily for 28 d. The weights of the treated mice increased from 38
190 Super Charge Your Health To Protect Yourself Against Cancer
gms on day zero up to 50 gms by day 20. The control group weights went down from 38 gms to 37 gms. The mean tumor weight of treated animals was 1.4 gms compared with 2.4gms for control animals, a statistically significant difference. Microscopy showed extensive necrosis in tumor sections and associated evidence of apoptosis in samples from treated animals.The sarcomas from the treated mice were smaller and harder than the controls. There were more isolated from the surrounding tissues, having a thicker capsular membrane. In the control group the sarcomas were larger, softer had no membrane and appeared tightly bound to the surrounding tissues, indicating a strong immune response. The blood vessel cells were swollen in the treated mice, which seemed to block blood vessels, decreasing oxygen and nutritional supplies to the tumors. The mitochondria and intracellular volume expanded due to the PEMF. The PEMF appeared to lower the degree of malignancy of the sarcomas cells and inhibited their rapid growth. They also had more evidence of programmed cell death. There were many more dying cells, packed with debris, being digested by immune cells. These immune cells were more prominent and greater in number around PEMF exposed cells than controls.
This study is important in showing the immune and vascular changes induced by PEMFs against cancer cell growth, causing the tumors to shrink and helping to destroy the tumor.
Other studies on the tumor-reducing effects of magnetic fields represent a great variety in cell culture systems, animal models (mice), field sources, waveforms, field strengths, and exposure protocols. Many of the cell culture studies of tumor lines report significant cell death after magnetic. exposure compared with that of control cultures. With a few exceptions, most in vivo studies have reported a relative reduction in tumor size in tumors exposed to magnetic fields compared with controls. Reduction in tumor size occurs across a broad variety of field strengths, waveforms, exposure durations, animal models, tumor lines, and other procedural aspects.
Table 7 below shows other studies that have been done exploring the effects of PEMFs in animal hosts.
Based on the whole discussion above, we see that the optimal PEMF exposure regimen remains unknown. We also see that weaker and briefer exposures to magnetic fields are less likely to have an effect, compared with longer and stronger exposures.
TABLE: 7 PEMFs and impact on various cancers
191 Super Charge Your Health To Protect Yourself Against Cancer
A SAMPLE OF LITERATURE REPORTS ON EFFECTS OF ELECTROMAGNETIC FIELD TYPES ON GROWTH OF CANCEROUS TUMORS IN ANIMAL HOSTS
FROM: Cameron. The references are in the Cameron article.
Human studies
What about human studies, which are ultimately the most important for understanding to what extent PEMFs could help with human cancer management?
Breast Cancer
Many of these studies were conducted in Russia usinga “Magnetoturbotron” wholebody PEMF device. It is a rotating magnetic field device, intensity ranging from 0 to 3 mT (30 G) sequentially and then back to zero every 2 mins, typically for 1 hour daily over 30 days.
192 Super Charge Your Health To Protect Yourself Against Cancer Type of tumor Frequency Hz and (pps) Intensity Tesla Exposure min (m), (hr), or sec/day (d) Significant growth retardation yes or no References Melanoma 25 2-5 mT 3 hr/d Yes Hu et al. 2010 [4] Hepatoma 100 0.7 mT 1 hr 3x/d Yes Wen et al. 2011 [5] Colon 50 2.5 & 5.5 mT 70 m/d Yes Tofani et al. 2002 [6] Mammary 12 & 460 9 mT 10 m on alternate days Yes Bellossi & Desplasi 1991 7 MX-1 50 15-20 mT 3 hr/d Yes Berg et al. 2010 [8] Carcinogen induced 0.8 100 mT 8 hr/d Yes Seze et al. 2000 [9] Mammary 120b 10-20 mT 10 m/d Yes Williams 2001 [2] Mammary 120b 10 & 20 mT 3 to 80 m/d Yes Cameron et al. this report Mammary 120b 15 mT 10 m/d Yes Cameron et al. 2005 [1] Mammary 1 100 mT 60 to 180 m/d No Tataova et al. 2011 [10] 1 360 m/d Yes Sarcoma 0.16 - 1.3 0.6 - 2.0 T 15 m/d Yes Zhang et al. 2002 [11] Melanoma 50 5.5 mT 70 m/d Yes Tofani
2003
Sarcoma 50 250 mT 80 sec/d Yes Yamaguch
et al.
[12]
et al. 2006 [13]

Breast Cancer - PEMF Russian Research - Magnetoturbotron - SUMMARY by Stage
I 53 maste ctomy 0 30 rxs pre-op; 30 rxs post-op
II/III 73 pre-op rads; mastectomy; post-op rads rads only pre-op; 2wks post-op
III/MO 114 pre-op rads/chemo/ PEMF; radical; post-op chemo +/PEMP pre-op+/-PEMF
IV 51 usual therapies
IV 68 usual therapies
Stage I
2 mos after final rx + pogression; 30 rxs
2 mos after final rx + pogression; 30 rxs
PEMF alone ~hugely effective W long term use; ?higher intensity, better and faster
PEMF sig. benefit for pre-op W 30% reduced tumor size. higher intensity and longer term
PEMF sig. additive benefit to chemo/ rad'n pre/post-op W reduced rad'n SE's and future mets
PEMF sig. additive benefit to chemo/ rad'n pre- op W better tumor size reduction pre-op and better pathologic stage
PEMF sig. benefit for Stage IV state; CR 4%, 2X less tumor/mets 1 mo post 32%; 25-50% less 17%; ^Hgb
PEMF sig. benefit for Stage IV state; 50% less tumor/mets in 30%; 25-50% less 16%; best W soft tissue mets; remissions 0.3-14 yrs
Those with only local breast cancer (N=53) had Magnetoturbotron PEMF 30 times prior to operation and 30 times after it. Preoperative tumor size decreased by about 30%. (Bakhmutskii, 1993)
193 Super Charge Your Health To Protect Yourself Against Cancer
Stage N Intervention Control PEMF rx/s Condusion IIIb
therapies 0
1 usual
30;60;110rxs
0
0
Stages II and III
A controlled trial is described of 73 patients with stages II and III operable breast cancer. Prior to surgical removal of the tumor, the PEMF therapy group patients received combined PEMF and radiation therapy. PEMF therapy was for 5 days, 30-60 min/day, whole body, 100 Hz, with the field strength gradually and periodically changing from 0-3 mT; the duration of a single cycle was 120 sec. Each PEMF procedure was immediately followed by an exposure to radiation treatment of the breast and regional metastatic areas. Mastectomy was performed 24-72 hr after the last exposure. In the control group, 3 were operated without any preliminary treatment, and the rest received the same course of radiation therapy as described above, but without magnetotherapy. Two weeks after surgery, patients with stage III disease received an additional course of PEMF and radiation therapy (therapy group), or radiation therapy only (control group). Subsequently, patients could be ordered adjuvant hormoneand chemotherapy treatment. It was found that PEMF therapy reduced the negative effects of radiation therapy on cellular immunity, repaired the lymphocyte ratio, and returned the production of hormones to normal. PEMF therapy patients did not see the same degree of drop of lymphocyte counts as would be normally seen with radiation. The oxidative stress typically caused by surgery was prevented by PEMF therapy by almost threefold. Patients were followed for 12-30 mo after surgery. Metastases were found in 12% of patients treated with the magnetic field, and in 19% of patients treated without it. In patients with initial stages IIB and III cancers, within 1 yr after surgery, metastases appeared in 8% and 22% of cases, respectively. The authors concluded that treatment with PEMFs was well tolerated, did not have any adverse side effects, normalized immune and hormonal functions and decreased the probability of metastasis. (Milevskaya)
Another investigation was carried out on a group of 114 women less than 65 years of age with stage III local breast cancer without distant metastasis (stage M0). They all had (a) preoperative radiation of the breasts and adjacent areas in a total dose of 40- 46 Gy plus chemotherapy (per Cooper’s protocol) and the “Magnetoturbotron” (10-12 procedures each lasting 40-50 min long, (b) radical mastectomy and (c) postoperative adjuvant chemotherapy. The women were followed with x-ray looking for changes in the primary tumor and regional lymph nodes, and with biopsy histological changes in the primary tumor tissue (degree and depth of pathology). There were no significant unexpected side-effects or complications. The impact of the preoperative treatment on regional metastasis was 97% in cancers with PEMF and 52% without it. Preoperative versus post primary (a)-phase mammographic examination, including exposure to the PEMF revealed complete tumor regression in 42%, 46% with partial tumor regression and regression or reduction of regional metastasis volume of 90%. Histological examination of the tumor tissue specimens obtained during the tumor resection in the patients having received the pre-operative chemo/radiotherapy and PEMF treatment showed the following results: prominent pathologic change
194 Super Charge Your Health To Protect Yourself Against Cancer
(down to degree 3 and 4) of the tumor in 56% with PEMF and 48% without the PEMF. (Dobrynin; Rybakov)
Stage IIIB
This is a case report of a 48-year-old woman with a prior history of cancer the right breast with metastases to the axillary lymph nodes. She was treated with resection, radiation and chemotherapy. Ten months after she completed chemotherapy, she was discovered to have a recurrent tumor stage IIIB in the left breast. Because she had a very low white blood count, she was not a candidate for further chemotherapy or radiation. Instead, she had Magnetoturbotron therapy. After 30 exposures, the infiltration in the breast decreased considerably; after 60 exposures, one of the metastatic nodes disappeared while others became soft and reduced in size. After 110 magnetic field exposures there was complete regression of the tumor and metastases. More than 12 years after PEMF therapy, the patient was reported in good health. While this is a single case it is illustrative of the potential for PEMF therapy. It should also be noted extended treatments are likely to be needed to produce the best results. In this case, it took 110 hours, or about 15 weeks of daily therapy. (Bakhmutskii)
Stage IV
51 women (28-66 yr old) with advanced breast cancer were studied. All patients had incurable primary tumors with regional and distant metastases. Ten women were not previously treated. Others had mastectomy, radiation, chemotherapy, or combinations. The PEMF started at least 2 mos after the completion of treatment and evidence of progression. Magnetoturbotron 1 hr daily over 30 days. Complete tumor and metastases regression in 2 patients (4%); drastic improvement (more than a 2-fold decrease in tumor and metastases size for at least 1-mo after treatment in 16 (32%), and considerable improvement (25-50% decrease in the size of tumor and metastases) in 9 (17%). All had improvements in general health, pain and appetite and sleep. Also, recovery of blood hemoglobin content and tissue benefits for tissues altered by previous therapy. (Bakhmutskii,1991)
Another study included 68 women with generalized breast cancer. In those with incurable generalized tumor (tumor relapse, metastases to the other breast, lungs, lymph nodes, skin, brain, etc.), PEMF was started at least 2 mos after the completion of previous treatments and if there was evidence of further cancer progression. After a course of 30 exposures, a pronounced favorable effect (more than 50% regression of tumor and metastases) was found in 21 patients, and considerable tumor regression (25-50%) in 11 patients. PEMF treatment was more effective in those with metastases into soft tissues, i.e. into lymph nodes, skin, and subcutaneous areas. Remissions lasted from 4 mos to 15 yrs, depending on follow-up. (Bakhmutskii, 1993)
Postoperative care
195 Super Charge Your Health To Protect Yourself Against Cancer
Postoperative lymph drainage after radical mastectomy is universal and can delay recovery and discharge. This outcomeof mastectomy is caused by the removal of the axillary lymph nodes so that the normal amount of lymph in the breast accumulates without the ability to adequately drain itself through the axillary lymph nodes. After basic recovery from the surgery many patients go home with drains so that the fluid does not accumulate so much that healing can’t happen. This outcome was studied in a group of 106 patients who were allocated to either the usual care group or usual care plus PEMF therapy. 87 patients had metastasis of the regional lymph nodes. Preoperatively all the patients received radiation to the breast and the adjacent axillary area combined with chemotherapy. In addition to mastectomy, all patients had their regional lymph nodes removed. Postoperatively, the daily accumulation of lymph could reach the level of 200-600 ml. When the level of post-operative drainage was sufficiently stable, PEMF therapy was begun. This included 5-12 PEMF therapy sessions of 3.0 mT, 100 Hz, for 40-60 minutes. The average duration of lymph drainage in the control group was 13 days. In the PEMF group the duration of lymph drainage was an average of 8 days. The 24- hour lymph drainage in the PEMF group decreased from 200-300 ml to 50 ml or evenabsolutely stopped within 2 weeks. In 8 patients who had 600 ml’s of lymph drainage, after 5-6 PEMF treatments the drainage stopped completely. Therefore, PEMF therapy can be very useful in the recovery of women postoperatively who have had radical mastectomies or partial mastectomies with extensive removal of lymph nodes. (Letiagin)
Tissue changes
The “Magnetoturbotron” whole-body PEMF was studied in 20 patients with breast cancer, stages II or III. Samples of tumor tissue were isolated during surgery and were processed and stained using conventional techniques, then analyzed. Analysis revealed that PEMF induced significantly abnormal changes in the cancer cells in 100% of cases. These pronounced alterations often caused cell death which in turn caused formation of dead areas in cancer tissue, and cancer cells in such areas were replaced by fibrous tissue. Overall, the tumor characteristics demonstrated slowing of its development or its regression. The authors suggested that PEMFs affect the nucleus of malignant cells, decreasing their ability to proliferate. (Frolov)
Post-operative radical breast cancer surgery recovery
Another study by the same group evaluated this device on the postoperative treatment of lymph drainage after radical breast procedures (mastectomy or lumpectomy). 106 women, ages 32-68 yrs with only local breast cancer. 56 were in the standard care control group and 50 in the PEMF group. 87 had regional lymph nodes metastasis. All received preoperative radiation to the breast and adjacent axillary tissue (total dose of 40-46 Gy) and chemotherapy, using the Cooper’s modified protocol. The majority had radical mastectomy with pectoral muscle preservation. Regional lymph nodes were dissected. Drains were placed and removed when blood
196 Super Charge Your Health To Protect Yourself Against Cancer
flow stopped and evidence of drainage decreased. Any further accumulation of lymph was drained by needle puncture. Daily accumulations of lymph could reach 200-600 ml. There was a gradual reduction in lymph accumulation. PEMF was applied during this lymph accumulation period daily (3.0 mT, 100 Hz for 40-60 min). All the patients stood the procedures well. The control group of the patients did not receive PEMF. In this group the duration lasted from about 6-34 days with an average of 13 days. In PEMF group the general duration of the drainage was 3-33 days and an average of 8 days. In a 24 hr period, PEMFs decreased drainage volume from 200-300 mlto 50 ml over 24 hr or even absolutely stopped within 2 wk. In 8 women drainage of 600 ml in a day one day stopped completely after 5-6 PEMF sessions. (Letiagin)
In vivo animal studies
More intensive research examined the antitumor activity of the Magnetoturbotron PEMF in vivo in mice, with a particular focus on possible mechanisms of its action. They used 3 mT, 50- 200 Hz, for between 5 and 90 hrs. Focus was on the growth of transplanted tumors (leukemia, breast cancer, lung cancer, melanoma and uterine cancer. Lymphoid leukemia and uterine cancer were not sensitive to the PEMF. The most sensitive to this PEMF were breast carcinoma and melanoma with 70% inhibition of tumor growth. Lewis lung cancer (LLC) was less sensitive at 50% inhibition. Combining PEMF’s with the anticancer drugs (sarcolysine, 6- mercaptopurine) had a more enhanced antitumor effect. The anticancer effect of the PEMF was thought to be due to its inhibitory action on the tumor cells themselves or to the action of the PEMF’s on stimulating the cancer destroying effects of the body’s natural tumor resistance system, that is, neutrophils and macrophages.
When they looked at the PEMF effects on cultured human ovarian cancer cells they found modest inhibition of DNA synthesis by 22% in only 13 out of 45 experiments. The inhibition was not due to cell cycle arrest. Therefore, the data only showed weak and variable inhibitory effects of PEMF on tumor cells outside the body (ex vivo). Neutrophils and macrophage white blood cells may produce highly toxic reactive oxygen species (ROS) on contact with a tumor cell. These free radicals, including hydrogen peroxide, act as tumor cell killing factors. Examinations of spleen cells of tumor bearing mice and healthy donors with exposure of 1 hr 20 min significantly stimulated ROS by 58%. PEMF reliably stimulated ROS production by whole blood white cells of healthy donors; being maximal within 10 min after the beginning of PEMF action. ROS production by blood cells melanoma tumor growth in mice, exposure for 10 days, 2 hr/day, resulted in nearly a two-fold increase of ROS. The ROS of neutrophils was also additionally increased when combined with antitumor drugs (sarcolysine, 6-mercaptopurine). Based on these data the in vivo inhibitory action of PEMF to different types of tumors is not due to the specific direct action upon the tumor cells, rather the anti-cancer action is from activation of tumor destroying white blood cells. (Dobrynin, 1998a)
197 Super Charge Your Health To Protect Yourself Against Cancer
General
Case series
A case series is described where a PEMF system was used in the treatment of 151 cancer patients (45% stomach cancer, 20.5% lung cancer, 25.2% breast cancer, 5.3% Hodgkin’s disease (lymphogranuloma), and 3.5% melanoma). The whole body was exposed to a sinusoidal field, 1.65-3.5 mT, from 50-165 Hz, 15 cycles lasting from 1-20 minutes. PEMF therapy always supplemented other methods, including major surgery. In 52 patients, PEMF therapy was performed before operation; 50 patients noted pain relief and improvement in their general health and appetite. In 47 patients PEMF therapy was provided on the third day after surgery. It alleviated complications of the postoperative period, decreased pain and weakness. In 19 patients who had upper extremity lymphedema following mastectomy for breast cancer, a combination of PEMF therapy was given along with compression therapy. These therapies decreased or entirely cured the lymphedema. 31 patients had surgery for stomach cancer and the use of PEMFs following surgery improved their rehabilitation and decreased dyspeptic problems. Their body weight increased by 0.7-4 kg. They also had improved white blood counts and a significant increase in immunoglobulins. During the follow-up period, metastases were observed only in 2 patients at 3 mo and 9 mo after the operation. The authors concluded that the whole-body magnetotherapy had a favorable effect on the general state of cancer patients, facilitated repair processes in the postoperative period, and improved their immune status. (Lubennikov)
As can be expected with any therapeutic system, not everybody with cancer can benefit, especially with late-stage cancers. A case series was described of 74 patients with advanced malignancies, that could not be treated by established techniques, or with progressive asymptomatic disease, where aggressive conventional treatments were not indicated. They were treated with 4-6 mT, 8 or 20-Hz sinusoidal magnetic fields, at home 1 hour 3 times daily for at least 3 months and longer if possible. 28 patients had metastatic bone cancer, 25 pelvic tumors, 17 pulmonary tumors, and 4 brain tumors. All the patients were followed by x-ray, CT, MRI, clinical evaluations and self-rated quality of life. About 16% stopped using the PEMF system during the first 6 weeks because of problems with immobilization and positioning of the stimulator, the time-consuming course of the treatment, and depression that occurred because treatment was a constant reminder of their disease. Another 25% had their therapies stopped because of the rapid progression of their cancer. Nobody exhibited a clear effect of the magnetic fields on a tumor or an unequivocal tumor response, such as a partial remission. Lasting pain relief, which could be explained only by the action of the PEMF therapy, was reported by 3 patients with severe pain associated with growing tumor masses. While these results are disappointing, they are not unexpected given the late-stage of the cancers evaluated. It is also possible that these results may be more specific to this particular PEMF system and other systems, particularly higher intensity, may produce better results in late-stage cancers. (Sauerwein)
198 Super Charge Your Health To Protect Yourself Against Cancer
Ovarian cancer
Stage IV ovarian cancer was evaluated in a small controlled study on patients with inoperable ovarian tumors. PEMF therapy consisted of 0.3-30 uT, 0-10 Hz treatments 20 minutes daily for 2 weeks. They also received standard chemotherapy. 5 patients served as controls and only received the chemotherapy. Another 5 received chemotherapy and PEMF therapy. The results showed that the patients who had PEMF treatment had no subjective complaints of nausea, weakness and loss of appetite in contrast with control group where these typical side-effects of chemotherapy were pronounced. PEMF treated patients also have increases in lymphocytes and sedimentation rate, which returned to normal 2 weeks later. The control group showed no reactions in these parameters. No difference between exposed and control groups was observed in tumor size (MRI, sonography). (Goritskaya)
Complications from chemotherapy
Complications from chemotherapy are extraordinarily common. Conventional medical therapies often leave much to be desired. One group presented the results of use of PEMFs for treatment of two kinds of anti-cancer chemotherapy complications in adults and children. Research describing the use of PEMFs in children is rare. One group studied was those with local injuries of skin, underlying tissues, and veins, which frequently develop after IV injections or chemo agents leaking outside the blood vessel wall (extravasations); and the other was bowel obstruction from intestinal adhesions. Patients studied had phlebitis (inflammation of a vein) or thrombophlebitis (vein inflammation with associated thrombosis (clot formation), clots in veins without inflammation of the wall, infiltrations of the chemo agents into the surrounding skin outside the blood vessel, ulcers, indurations (heart and blood vessels), and tissue breakdown (necrosis). The first group received traditional therapy (local application of medicines, and compresses). The second group was treated with magnetic therapy. PEMF therapy was either with an alternating MF sinusoidal wave, continuous mode, 50 Hz, 40 mT in adults, and 10-30 mT in children or pulsed continuous mode, 25 Hz, 4.5 mT both in adults and children. PEMF therapy was once a day for 15 minutes. Applicators were positioned over the chemotherapy drug injection site or along the injured vein. Evaluations were done after 2 weeks. In phlebitis, traditional care patients, about 60% had improvement, though vein hardening persisted for 3-4 months. In the PEMF group, the phlebitis was cured in 12-14 days in 100%. Phlebothrombosis developed into sclerosed vein (vein closed down by inflammation in the clot) in 2 patients of the first group, and in none of the PEMF patients. Infiltrations and hardened veins gave rise to ulcers in 67% of cases in the first group, whereas PEMF therapy eliminated these problems in 12-30 days. Healing of ulcers and necroses in the standard care group proceeded slowly at an average rate of wound surface area decrease per day of 1%, and 30% needed surgical care. In the PEMF group, the average daily reduction of the wound surface area was 3%, and wounds were healed in 100% of patients in at most one month. The pulsed MF was more effective in treatment of ul-
199 Super Charge Your Health To Protect Yourself Against Cancer
cers and necroses, whereas alternating MF was better in phlebitis, phlebothrombosis, infiltrations, and tissue indurations. In PEMF-treated children, healing of extravasation-induced wounds happened faster than it did in adults, despite a worse initial condition of the injuries.
Intestinal adhesions
One of the most important parts of this study, which I’ve never seen reported before, is the effectiveness of PEMF therapy in abdominal adhesions. Abdominal adhesions lead to major health care costs and sickness, and result from almost any kind of abdominal surgeries and abdominal inflammation or infection. These often necessitate hospitalizations, intestinal decompression tubes, and even surgery to break down the adhesions. Unfortunately, even with corrective surgery for breakdown (lysis) of the adhesions, they often recur. This results in a cycle of multiple hospitalizations over a person’s lifetime for the adhesion problem.
Intestinal obstruction
In this study, the group with intestinal obstruction due to adhesions included 18 children (aged 3 to 12 yr) who had been treated for lymphosarcoma with involvement of the small bowel. In all cases, initial surgical operation for the lymphoma was followed by cycles of chemotherapy. Intestinal obstruction developed one or several months after the operation. The treated children with obstruction were exposed to an alternating sinusoidal wave, continuous mode, 50 Hz, 10-30 mT PEMF device, 15-20 min per day. Although complete elimination of pains and return to normal of bowel function were achieved after 2-4 exposures, the treatment course was extended to 10-12 days. No relapses of adhesion related intestinal obstruction were observed during a 0.5-6 yr follow-up period. (Kiselev)
Brainradiation therapy
Patients about to undergo brain radiation therapy, particular to the brain, are usually warned away from PEMFs, because of the lack of knowledge regarding their interaction and the concern that PEMFs may decrease the benefits from radiation therapy. A pilot study was conducted to investigate the clinical efficacy of PEMF stimulation combined with radiotherapy for treating inoperable metastatic brain cancer. 23 patients with inoperable secondary brain tumors had cobalt radiation to the brain area 48 hours apart. Immediately after each cobalt treatment, each patient’s brain received PEMF stimulation (1.5 mT; 75 Hz) for 12 hours. They were to return for evaluations 30 days after the second PEMF treatment. Thirteen patients had follow-up evaluations. In 10, the original tumor had occurred in the lung, in the 3 remaining cases the primary tumor was a seminoma, a breast cancer, and a melanoma. More than 1 metastasis was present in 4 patients. Comparison of pre- and post- CT scans showed progression of the metastases in 1 case, no change in 2 cases, partial remission in 8
200 Super Charge Your Health To Protect Yourself Against Cancer
cases, and complete remission in 2 cases. The authors thought that the results seemed to be slightly better in the treated group when compared with a previous group treated with cobalt radiation only. There were no negative side effects. The authors noted that exposure to PEMF has been shown in previous studies to increase the damage caused by X radiation in mice, with similar effects reported for PEMF with cytotoxic agents, cyclophosphamide and mitomycin c. (Mandolini)
Premalignant lesions
The search for treatment of early tissue changes that result in the development of cancer anywhere in the body is still pressing. For the most part, existing methods of local and symptomatic treatment are not sufficiently effective and do not lead to permanent cure; these methods are almost ineffective in the case of abnormal tissue alterations. To this end, the use of PEMFs in the therapy of premalignant pathology of the stomach was studied in 18 patients with a chronic peptic ulcer involving abnormal tissue development at the second or third stage. Whole-body exposure was with a rotating sinusoidal MF from 0-60 mT for 20 min, 15-20 times. Endoscopy after treatment revealed complete ulcer healing in 60% of patients, partial healing in 18%, and no changes in 22%. Even in the last group, PEMF exposures had a pronounced analgesic effect. Tissue alterations regressed in 43% of the patients, and the tissue reverted to the first stage. The PEMF increased the total number of T-lymphocytes (from 58% to 65%). These data indicated the immunomodulating effect of PEMF therapy. The authors ended up saying that PEMFs were an effective and promising method for the treatment of premalignant stomach pathology. (Kolomietz)
Advanced cancer
A group of researchers who had done previous cancer studies found that PEMFs at 50 Hz, average intensity higher than 3.6 mT, had antitumor efficacy in mice. In fact, in their prior research inhibition with PEMFs was significantly greater than that seen with chemotherapy. As a result, they studied 11 patients with advanced cancer, already heavily pretreated. Their PEMF stimulation was to the neck, thoracic and abdominal area of the patients, 5 days a week, for four weeks using two different treatment schedules: 20 min daily and 70 min. daily, at 5.5 mT. They concluded that PEMFs can be safely administrated without acute negative side effects in patients with cancer. (Ronchetto)
Head neck, oropharyngeal cancers
Therapies for cancers of the head neck, oropharyngeal cancers, are among the most disfiguring and functionally disabling. As a result, PEMF therapies could be very beneficial in this setting. One of the questions regarding these therapies is what can be done prior to radiation and/or surgery to reduce the complications and side effects? The goal of PEMF therapies is to reduce tumor size prior to surgical resection to pro-
201 Super Charge Your Health To Protect Yourself Against Cancer
long survival and improve function. Previous studies have shown that the survival rate of patients with stage 2 and 3 oral squamous cell carcinomas depended on the size of the tumor. In this setting, therapy consisted of giving the patients antioxidants supplemented by PEMFs. This therapeutic system was tested in 2 patients diagnosed with squamous cell carcinoma of the tongue. In both patients, the tongue developed a softer consistency and became more mobile after 3 wk of treatment. Speech improved and pain control achieved after only a few days of treatment. Surgery only required minimal resection of the tongue tip together with neck surgery, carried out 7 wk after therapy. Biopsies of the surgical tissues found no tumor cells. Another 11 patients with stage 3 tumors treated with combined radiation and chemotherapy were also treated with this therapy. The PEMF treatment improved their tolerance for radiotherapy and chemotherapy. Minimal skin and mucous membrane changes were seen in the PEMF treated patients. (Randoll)
Magnetic field therapies in the setting of otolaryngology or ENT have shown some promise. Alternating and constant magnetic fields have shown benefit. Static magnetic fields in magnetic rings, plates, or rods at 10-15 mT were used in the treatment of patients with non-purulent ear diseases and otitis media. Thay reduced inflammation and purulent discharge from the ear. A clinical effect was seen after 10-15 applications. PEMFs (50 Hz, 50 mT) were used successfully in the treatment of patients with acute and chronic laryngitis, postoperative inflammation of the larynx and trachea, or radiation cartilage damage of the larynx. Clinical improvement was recorded in 22/34 (65%) patients. PEMFs showed marked anti-inflammatory effects in patients with cancer of the larynx with 50 Hz, 50-60 mT prior to radiation therapy and decreased post radiation edema of the larynx. (Ozinkovskii)
“TAMMAT”therapy
Advanced techniques of magnetic field therapy of tumors (“TAMMAT”) was launched in 1992. TAMMAT was assigned to PEMF devices which generate virtually uniform rotating extremely-low-frequency magnetic fields of 0.4-4 mT, 0.3-160 Hz. This frequency range includes the bands of major physiological rhythms (cardiogram, encephalogram, rate of firing of neurons, etc.). For the chosen frequency range, the presence of biological tissues does not alter the field structure. This is an advantage of low-frequency PEMF therapy compared to UHF, laser, or millimeter-wave therapy. The treatments are done in an out-patient setting, 15-25 minutes of exposure daily for 3-4 wk. Preliminary data showed PEMFs to be an effective remedy for malignancies at stages up to T2-T3. Promising results were obtained for cancer of breast, lungs, intestines, oral cavity, and some others. PEMF therapy was employed either alone or in combination with traditional techniques. In the latter case, it reduced or eliminated the adverse side effects of radiation therapy and chemotherapy. In T4 stage tumors, PEMF exposures reduced pain, temporarily decelerated tumor growth, and increased life span. (Kovalchuk)
202 Super Charge Your Health To Protect Yourself Against Cancer
Bone cancer surgical grafts
As part of the treatment for bone cancer, whether metastatic or primary, often large tumor resections are carried out. As a result, large bone grafts from the person’s own bone (allograft) are needed to cover the defect and replace the lost bone. Healing the replaced bone is very slow and can take a long time to get union of the grafted bone with the healthy bone, even though it’s from the host. Many factors negatively affect this healing rate. A double-blind study was done (Capanna) to see if PEMFs could help with healing. 83 grafts in 47 patients were studied. The overall graft healing rate was the same (67%) in both control and active stimulated participants. There was a positive effect of PEMFs for the host graft junctions between allograft and host bone. When postoperative chemotherapy was not done, the healing time decreased by about 3 mos, from 9.4 mos in the control group to 6.7 mons in the active PEMF-stimulated group (p < 0.001). This effect would have been lost if chemotherapy was used. It is well known that chemotherapy delays healing, whether it’s bone or other tissues. This is why often surgery is delayed or done before chemotherapy to assure healing.
Lung cancer
Lung cancer tumor tissue from 20 patients was evaluated, using tissue biopsies, tissue, chemical and physical, changes and very deep electron microscopy. All these individuals were exposed to PEMFs preoperatively to enhance antitumor resistance. PEMFs produced nonspecific adaptation reactions, resulting in physical changes to the cancer cells which indicate a marked antitumor effect of magnetic fields. These changes were best after 20-30 sessions. Highly differentiated (mature) adenocarcinomas proved to be mostly sensitive to the magnetic field action. (Ogorodnikova)
Millimeter wave or microwave resonance therapy (MRT)
While most of our emphasis is on extremely low frequency PEMFs, the Eastern Europeans have done a considerable amount of work with millimeter wave or microwave resonance therapy (MRT). 149 patients were treated with this modality. 51 with cancer of the large intestine, 12 with stomach cancer, 3 with breast cancer, 4 with other malignant tumors, and 79 with polyps in the intestinal tract. Millimeter wave (MMW) radiation was applied to selected acupuncture points. Use of MRT during the pre-operative period arrested some accompanying diseases (duodenal and gastric erosions and ulcers, aggravations of chronic pulmonary and gastrointestinal diseases) and decreased the risk of the operation in 21 patients (88%). MRT was useful for early postoperative aggravations (hemorrhage, atony syndrome), in 68% patients. MRT used at the same time as radiation and chemotherapy significantly reduced the tissue toxic effects on healthy tissues and organs in 75%. Stage IV cancer patients had their problems stopped, that is, pain, toxic, and asthenic syndromes, in 67%. MRT in patients with polyps substantially eased recovery by 33% and helped recovery of bowel function and prevented relapse of polyps in an up to 24 months follow-up period. MRT did
203 Super Charge Your Health To Protect Yourself Against Cancer
not stimulate tumor processes and was tolerated by patients. Thus, MRT can be successfully used in patients with tumors and pre-tumor diseases as a modifying factor which increases the efficacy of conventional therapeutic means. These are assertions commonly made for PEMFs.
Advanced hepatocellular carcinoma
Treatment options for patients with advanced hepatocellular carcinoma (HCC) are limited. There is evidence that the growth of primary liver cancer cells may be altered by very low levels of PEMFs modulated at specific frequencies. These types of fields were tested in 41 patients with advanced HCC. Three-daily 60-min outpatient treatments were given until disease progression or death. Imaging studies were performed every 8 weeks. The goal was to see an impact on reducing the progression and survival over 6 months. Treatment was well tolerated and there were no significant toxicities. In all, 34% had stable disease for more than 6 months. Median progression-free survival was 4.4 months and median overall survival was 7 months. Treatment administered in the mouth with amplitude-modulated electromagnetic fields is safe, well tolerated, and shows evidence of antitumor effects in patients with advanced HCC. (Costa)
PEMFs and chemotherapy
Morphine is widely used as an analgesic in cancer and often in combination with chemotherapy. Chemo has DNA damaging effects not only on targeted cancer cells but also on non-chemo targeted cells. A study (Sanie-Jahromi) evaluated the effect of morphine in combination with 50-Hz electromagnetic field (PEMF) and co-treatment with cisplatin plus morphine and EMF on genes involved in DNA repair. Breast cancer and neuroblastoma cells were treated with morphine and then exposed to 50-Hz/0.50 mT PEMF, 15 min-on/15 min-off. Gene expression, cisplatin and bleomycin cytotoxicity were measured. Morphine treated cells showed significantly reduced genes, while “Morphine + PEMF” treatments did not significantly change the genes. The potential for the lethality level of cisplatin was significantly increased for both cell lines when co-treated with “Morphine + PEMF” compared with morphine only treated cells. Other related genes were significantly decreased in co-treatment of cisplatin and “Morphine + PEMF” which led to higher bleomycin cytotoxicity in SH-SY5Y not in MCF-7. This combination therapy provides data for promising use for increased sensitization of these types of cancers.
Combination treatment was studied (Omote) for potentiation of the therapeutic effect involving PEMF and the antitumor drug, mitomycin C (MMC), on fibrosarcoma (KMT-17) and hepatocellular carcinoma (KDH-8) in rats. On day 7 after tumor implantation into the thighs of rats, the area of the tumor received the PEMF (frequency 200 Hz, 40 gauss) for 1 h immediately after iv injection of the MMC. Survival at day 90 of KMT-17 implanted rats was 0% (0/10) in the non-treated group, 34% (4/12) in the
204 Super Charge Your Health To Protect Yourself Against Cancer
MMC-treated group, 47% (6/13) in the PEMF-treated group and 77% (10/13) in the MMC/ PEMF combination group. The increase of life span (ILS) of KDH-8-implanted rats in the combination group was significantly longer (% ILS, 18%) vs the MMC-only (% ILS 3%) and the PEMF-only (% ILS 8%) groups. So, PEMF potentiated the antitumor effect of mitomycin C for implanted fibrosarcoma and hepatocellular carcinoma.
A very thorough and interesting in vitro study was done to explore chemo treatment resistance. (Miyagi) Dunn osteosarcoma cells were treated to develop Adriamycin (ADR) resistance. These ADR-resistant cells were harvested. They had more than 10 times resistance than their nonresistant parent cells. They compared the growth rates of these ADR-resistant osteosarcoma cells for those exposed to PEMF versus those that were not. The PEMF was 10 Hz; rise time, 25 μsec, peak intensity, 0.4–0.8 mT. The growth rate in the resistant cells exposed to PEMF was significantly lower than that in the non-exposed resistant cells at all ADR concentrations, including ADR-free culture (P≤0.0114).
Combining PEMFs with other modalities as well as a chemotherapy agent would produce even stronger results. K-562 myelogenous leukemia cells and histiocytic lymphoma U-937 cells were studied in vitro. (Traitcheva)Three types of treatment: A) an ELF pulsed sinusoidal 50 Hz, 10-55 mT; B) the PEMF field and a cytostatic agent (actinomycin-C); and C) the PEMF, the cytostatic agent, and a halogen lamp. The results show a decreasing vitality of human K-562 and U-937 cancer cells in suspension with each additional treatment. Fifty-five mT exposuresused a Helmholtz coil and 39 mT. For a 10 mT treatment, 6 hrare necessary to strengthen the cytostatic ACM effect. For 55 mTamplitude, only 20 min is needed for productionof necrosis. With a halogen lamp, causing a rise in temperature from 370 to 420C, the lethal effect by ACM and PEMFincreases from 16% dead cells to 40%. This means that increasing the body temperature by about 5°C could potentially have an almost doubling effect of chemo and PEMF cancer killing. So, combining these modalities with a sauna could be quite useful. Other research has indicated that these kinds of benefits would be more likely to be seen when the modalities were combined very closely together in time.
Table 8 is a summary of in vitro laboratory studies where PEMFs were combined with chemotherapy. This demonstrates the potential usefulness of combining PEMF therapy with chemotherapy. The studies show that benefits from the combination of the two therapies is usually stronger than either one alone.
Table 8: PEMFs used for use in vitro cancer treatment studies combined with chemotherapy
205 Super Charge Your Health To Protect Yourself Against Cancer
Author Magnetic field Cancer Chemo Result
Yuan
5 mT/50Hz; 2 h/d static+PEMF; separately vs combo
Hao 8.8 mT Static MF for 12 Hr
Gray Static Mag Field 13 days ???
Li High intensity magnetic pulse (EMP)
Akbarnejad 100Hz, 100G
Barbault
RuizGómez
7 d rxs: 7 G static, 5hr daily only, DOX only, DOX+MF, control
PEMF 1.5 mT/ 1/25 Hz
a) Drug/PEMF 1 h same time vs drug 1 h then
b) PEMF for next 2 d 2 h/d; vs sham
Nephroblastoma/ Neuroblastoma Cells
myelogenous leukemia cells
transplanted breast CA in mice
Glioblastoma Multiforme (GBM)
Glioblastoma multiforme (GBM) cells
Ehrlich tumor IP injection
Cisplatin (DDP) – in vitro+in vivo; DDP/ PEMF – alone ea or combo
adriamycin (ADM)
>3d 17-22% inhibited growth and ^ apoptosis; > smaller tumor; less SE’s
Combo vs alone > Sig inhibition metabolic fctn; cell structure/DNA damage
adriamycin (ADM) Combo best; p<.0001
CCNU
enhance the delivery CCNU to tumor, aid apoptosis, inhibit growth
Temozolomide (TMZ) Combo > ^ apoptosis; ^ROS
Doxorubicin (DOX)
multidrug resistant human colon adenoCA (HCA) cell
vincristine (VCR), mitomycin C (MMC), and cisplatin (DDP)
Inhibition 82% DOX + MF vs 60% MF vs 31% DOX. , only. In combo 2/3 no tumor
Cytotoxicity: a) survival
VCR 6%, sham 20% @1Hz. MMC 19%, sham 5.3% @ 25 Hz. DDP 44–39% @25 Hz; b) min change
References above are in the Reference section below.
A double blind PEMF study was done in people with biopsy proven non-operable advanced lung cancer. (Zhu) They had to have a chemotherapy performance score (PS) between 0 to 2, no organ failure, and receiving or about to receive chemotherapy. The PEMF combined a static magnetic field with a rotational application. The static field peak intensity was 0.4T (4000 G) MF, with a rotating frequency of 7.5 Hz. Participants would lie down, with face up, on the treatment bed, for the chest to be exposed in the middle of the PEMF, 2 hrs/day daily for 21 days. The control group received sham treatment.
Numerous measures were evaluated: Functional Assessment of Cancer Therapy-Lung Questionnaire (FACT-L) is a questionnaire aimed at evaluating the life quality of lung cancer patients, pain Visual Analogue Scale, Objective Response Rate (ORR) and Disease Control Rate (DCR) and progression free survival (PFS).
Seventy people enrolled and 60 completed the study. Day 0 when randomized. Participants received blood routine testing (BRT), blood biochemistry test (BBT), urine and stool tests, tumor marker, brain MRI and chest CT between day -14 and day 0. On
206 Super Charge Your Health To Protect Yourself Against Cancer
day 0, they had FACT-L and PVAS questionnaires, and were randomized and assigned into PEMF group (PEMF therapy and chemotherapy) or control group (sham PEMF therapy and chemotherapy). From day 1 to day 21, participants received PEMF or sham PEMF treatment 2 hrs/d together with chemotherapy. On day 21, after finishing the whole treatment, they took the questionnaires again, and took their blood tests. On day 42, they once again finished questionnaires and had a chest CT scan. After that they were followed up every 3 weeks until their disease progressed, they died, or were lost to follow up. In addition, blood was collected on day 0 and 21 for cytokine array analysis.
Compared to the control group, more individuals in the PEMF group (67% vs 26%) had quality of life improvement on day 21. The two groups had similar ORR, DCR and PFS after treatment. PEMF treatment did not increase adverse events. They concluded that PEMF therapy could be applied as an adjuvant therapy along with chemotherapy.
PEMFs and radiation therapy
PEMF therapy combined with radiation therapy for liver cancer – an in vivo study
Based on previous cellular research by their group (Wen) that a 100 Hz magnetic field PEMF was effective at enhancing apoptosis of liver cancer cells induced by X-ray irradiation (IR) they extended this work. This time they explored the possible synergism between 100 Hz PEMF and IR in the treatment of hepatoma-implanted mice. 100 Hz PEMF exposure with a mean flux intensity of 0.7 mT was used inside a solenoid coil, lasting 60 min, with 12 hrs between. Sham 100 Hz PEMF exposure was performed by turning off the power supply to the solenoid coil. The IR was 6 MV, 4 Gy IR. (Gy, the symbol for gray is the dose, that is, the unit of ionizing radiation dose in the International System of Units, defined as the absorption of one joule of radiation energy per kilogram of matter.)
There were 6 groups: (n = 10). In each case IR was immediately followed by PEMF 100 Hz:
Group Description
I Sham IR IR and five periods of sham 100 Hz PEMFs (each period of 100 Hz PEMF exposure lasted for 60 min and the interval between each period of PEMF exposure was 12 hr)
II Sham IR and 5 periods of active PEMFs
III 4 Gy IR (within half an hour) followed by 5 periods of sham PEMFs
IV 8 Gy IR then 5 periods of sham PEMFs
V 4 Gy IR then 5 periods of PEMFs
VI 8 Gy IR then 5 periods of PEMFs
207 Super Charge Your Health To Protect Yourself Against Cancer
Mice were allowed to live up to their natural death.
To determine whether additional 100 Hz PEMF exposure periods could have a greater synergistic effect with IR than fewer periods of PEMF, three groups of tumor-implanted mice were examined (n=20). In each case IR was immediately followed by PEMF 100 Hz:
Group Description
I Gy IR then 5 periods of sham PEMFs;
II 4 Gy IR then 3 periods of PEMFs and two periods of sham PEMFs; and
III 4 Gy IR then 5 periods of PEMFs.
Mice were allowed to live up to their natural death.
Treatment and measurement of tumor diameter (maximum diameter at 10th day) and overall survival days were performed in a double-blind manner.
The addition of 4 Gy IR, but not 8 Gy, to 100 Hz PEMF could significantly improve survival time compared to IR or 100 Hz PEMF alone, indicating that 100 Hz PEMF could synergize with only lower dose IR.
TABLE 9: Survival Days and Tumor Diameters at 5th Day of Mice
aP < 0.05, siginificantly different in comparasion with Group II.
bP < 0.05, siginificantly different in comparasion with Group III.
cP < 0.05, siginificantly different in comparasion with Group IV.
dP < 0.05, siginificantly different in comparasion with Group I.
As shown in Table 9, compared to Group I (sham-exposed control group), IR (4 or 8 Gy) alone significantly reduced tumor size, but at the same time shortened overall survival days of tumor-bearing mice; moreover, 8 Gy IR alone significantly shortened survival time compared to 4 Gy IR alone. This suggested that besides reducing the tumor size, the whole-body irradiation caused significant cytotoxicity to the mice and this cytotoxicity should be dose-dependent. However, the addition of 100 Hz MF to IR (4 or 8 Gy) could significantly extend overall survival time compared to IR alone, sug-
208 Super Charge Your Health To Protect Yourself Against Cancer
w PEMFs or IR Alone or a Combination of IR and PEMFs Groups N Tumor diameter (cm) (±SD) Median Survival Days Group I (sham group) 10 4.97 ± 0.21 a,b,c 17 b,c Group II (5 MFs) 10 4.53 ± 0.35 b,c,d 20 b,c Group III (4 Gy X-ray) 10 3.81 ± 0.42 a,c,d 12 a,c,d Group IV (8 Gy X-ray) 10 3.01 ± 0.22 a,b,d 7 a,b,d Group V (4 Gy X-ray + 5 MFs) 10 2.69 ± 0.37 a,b,c,d 23 a,b,c,d Group VI (8 Gy X-ray + 5 MFs) 10 2.31 ± 0.39 a,b,c,d 14 a,b,c,d
Treated
gesting that EMF might possibly alleviate the harm to the tumor-bearing mice caused by IR.
TABLE 10: Survival Days and Tumor Diameters at 10th Day of Mice treated w Different PEMF Exposures When Combined With 4 Gy IR
Groups
aP < 0.05, siginificantly different in comparasion with Group II.
bP < 0.05, siginificantly different in comparasion with Group I.
As shown in Table 10, compared to fewer periods of 100 Hz PEMF exposure, more periods of PEMF exposure could significantly extend the overall survival time and reduce the tumor size of mice when combined with 4 Gy IR, indicating a synergistic mechanism between 100 Hz MF and 4 Gy IR in terms of their influence on the survival time and tumor inhibition. The maximum number of MF exposure periods in this experiment was no more than 5; further research is needed to explore the effects of more than 5 MF exposure sessions to demonstrate that a further increase in the number of 100 Hz MF exposure periods could achieve even better results.
The conclusion from this research is that these findings indicate that 100 Hz MF could possibly synergize with 4 Gy IR in terms of survival improvement and tumor inhibition in hepatoma-implanted mice.
When DNA damage was checked after exposure to ELF-EMFs in both normal and tumor cells, higher level of DNA damage was found in neoplastic cells. This was associated with defects in repair mechanisms, a common feature of tumor cells. These authors also found that antioxidant treatment (α-tocopherol at 10 μM) prevented stimulation of cell proliferation in normal cells, but not in tumor cells. Differences in DNA damage were also described for normal and tumor cells after this antioxidant treatment. These results show a differential EMF effect between tumor and normal cells.
Taking into account the impaired repair capacity of tumor cells, this differential effect could be extended to ionizing radiation treatment, thus supporting the view that the outcome for tumor cells exposed to ionizing radiation could be strengthened by EMF.
Experiments carried out on hepatoma-implanted mice have shown that five periods of combined 100 Hz frequency MFs and 4 Gy X-ray could significantly extend the overall days of survival and reduce the tumor size, compared to MF or X-ray treatment alone [79], suggesting that 100 Hz frequency MF could synergize with X-ray treatment
209 Super Charge Your Health To Protect Yourself Against Cancer
N Tumor diameter (cm) (±SD) Median Survival Days Group I (4 Gy X-ray + shaum MFs) 20 5.0 ± 0.42 a 17 a Group II (4 Gy X-ray + 3 MFs) 20 4.3 ± 0.33 b 19 b Group III (4 Gy X-ray + 5 MFs) 20 3.1 ± 0.52 a,b 23 a,b
in terms of survival improvement and tumor inhibition in hepatoma-implanted mice. In another study, the combination of EMF and γ-ray exposure produced a synergistic effect by triggering stress response, which increased reactive oxygen species [99].
PEMF therapy combined with radiation therapy for breast cancer – an in vivo study
One group did a well-designed in vivo study on mice of the combined effects of PEMF therapy with radiation therapy. (Cameron) The used a rectified semi-sinewave signal (15 mT/120 Hz), alone and in combination with gamma irradiation (IR) therapy in mice with an implanted breast cancer, injected into the breast fat pad of young female mice. Six weeks later, mice were randomly divided into four treatment groups:
1. Untreated controls,
2. 10 minute daily whole body (WB) PEMF,
3. 200 cGy of whole-body IR every other day (total 800 cGy),
4. Whole body IR plus daily TEMF. Some mice in each group were biopsied 24 hours after the end of IR. PEMF treatment continued for an additional 3 weeks.
Results: Most tumors <35 mm3 were white but tumors >35 mm3 were pink and had a capsule with blood vessels. The cortex within 100 microns of the capsule had little vascular supply. Blood vessels, capillaries, and endothelial pseudopods were found at >100 microns from the capsule (subcortex). Tumors >35 mm3 treated with IR 24 hours previously or with PEMF had decreased blood vessels in the subcortex and more endothelial pseudopods growing into hypoxic, HIF positive areas than tumors from the control group. Mice without being biopsied were followed for up to 70 days for tumor growth. Those that had either IR or PEMF had significantly fewer lung metastases and slower tumor growth than did untreated mice. No harmful side effects were attributed to PEMF.
Figure 16: Illustrates the effect on tumor growth ofthe 8-day course of gamma irradiation therapy (IR), the daily exposure to the TEMF therapy (TEMF), a combination of gamma irradiation and TEMF therapy (TEMF/IR), and no treatment (Control).
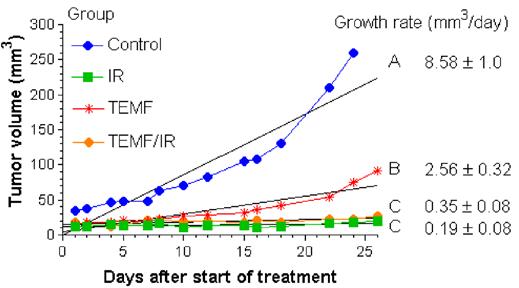
210 Super Charge Your Health To Protect Yourself Against Cancer
The tumors were all 35 mm3 or less at the start of treatment. The growth rate is the slope of the linear regression of the tumor volumes at each time. It can be seen that tumor growth was beginning to deviate from the linear fit about 18 days after the start of TEMF or radiation treatments however there was still a reasonable linear fit. ANOVA was used to determine any statistical differences in growth rates between treatment groups. Different letters demonstrate significant differences. Gamma irradiation alone (IR) or in combination with TEMF (TEMF/IR) reduced the tumor growth. The TEMF therapy resulted in a slower tumor growth rate than the untreated controls but not as slow as the gamma irradiated mice.
There was a synergistic reduction of the growth rate of breast cancer grafts in EMF/ ionizing radiation mice, compared with ionizing radiation therapy. Continued daily use of PEMFs following a course of IR therapy suppressed tumor blood vessel density, vs mice given IR alone. Although IR initially interferes with tumor vascularity, leading to tumor hypoxia, in turn enhancing IR resistance of tumor cells. These hypoxic areas produce HIF-1, leading to angiogenesis growth factors, further stimulating tumor growth. This known sequence of events following ionizing radiation treatment has led researchers to consider ionizing radiation treatment schedules coupled with the use of an anti-angiogenesis agent.
These results indicate that either IR therapy or PEMF therapy suppresses tumor growth. The IR therapy proved to be more effective at suppressing tumor growth than did the PEMF therapy, but not significantly, while the IR therapy but not the EMF therapy had harmful side effects. Both IR therapy and EMF therapy reduced blood vessel volume density within the tumor when measured one day after the end of the whole-body IR therapy but blood vessel volume density in tumors of the IR treated mice returned to pre-IR treatment levels. The continual use of daily EMF therapy in the IR treated mice did suppress the return of blood vessel volume density within the tumor following IR therapy. The combination of both therapeutic modalities therefore led to a sustained and significant reduction in the extent of tumor blood vessel volume density. This combined therapy and continuing the PEMF therapy long after IR may be likely to produce even better results than antiangiogenic therapy alone, while in addition providing all the other benefits of PEMFs.
So, sustained PEMF therapy by itself reduced: the extent of tumor blood vessel volume density, the tumor growth rate and tumor cell metastasis to the lung, without harmful side effects. Per the author, PEMF therapy alone may therefore be a useful alternate therapy for those with cancer who decide not to undergo standard radiation or for chemotherapy. The combination of IR therapy and continued TEMF therapy markedly suppressed the return of blood vessel volume density and tumor growth.
The study effectively pointed out that PEMF therapy can be combined even with whole body radiation therapy. Human studies are needed to verify these results.
211 Super Charge Your Health To Protect Yourself Against Cancer
PEMFs and surgery
One of the classic benefits of PEMF therapy is in improving wound healing. Surgery, obviously, creates surgical wounds. On the other hand, surgery is clearly used for repair of nonsurgical wounds as well. Surgery in the setting of cancer is used to remove tumors, restore damage from the cancer, for palliative care and to recover body functions. Surgery is often done in the context of other cancer therapies including chemotherapy, radiation therapy immune therapies and nutritional support. Timing of the surgery around chemotherapy and radiation therapy is very important to achieve adequate healing.
Most of the time, surgical practice does very little to enhance the healing process. Essentially, recovery from surgery is left to chance, that is, the natural ability of the body to heal itself without any other form of stimulation of the healing process. Healing is negatively affected with cancer care with both radiation and chemotherapy, but it is also impacted by the nutritional status, age factors, immune suppression, the nature of the cancer and its effects on the body, other medical therapies, and other factors.
To eliminate or significantly reduce reliance on “chance” to recover from surgery, PEMF therapy is well known to help the body heal better and faster with reduced likelihood of complications. A body that is stressed and overwhelmed in its health maintenance and repair needs is more prone to slower healing and complications, both of which are involved in not only the cancer process itself but also the treatments for it. The goal then is to create as healthy a body as possible and stimulate and support healing and recovery.
The actions of PEMFs in the body are covered in the “PEMF actions in the body,” specifically Table 6. They are also covered more extensively in the Power Tools for Health and the Supercharge Your Health with PEMF Therapy books. These are the basic actions of PEMF therapies without specific regard to the setting of cancer. However, all these actions still apply for their value and benefits before and after surgery in the setting of cancer care.
It’s important to emphasize that all these actions are not individually independent but are coordinated, synergistic and complementary to and with each other. All these actions may be seen and the body will use whatever resources it has or wants, to accomplish its natural goals of healing. PEMFs, fundamentally support and stimulate the body’s own natural healing functions. The PEMF cannot induce a function that the body is not capable of creating. In other words, PEMFs were not usually specifically created to produce these specific actions. The actions were discovered by studying the impact of PEMFs on the body. It will certainly be true that different PEMFs will have different actions or amounts of the different actions. Part of that variation will have to do with the magnetic field intensity mostly. Some of the varia-
212 Super Charge Your Health To Protect Yourself Against Cancer
tion will also be affected by the magnetic field pulse rates and, in some cases, the frequencies of the applied fields.
In this section, I will restrict the information to some of the specific studies done with surgery, not all of which are cancer related. Some of the cancer related surgery studies were in the Human Studies, Breast Cancer, section above.
The most important actions relating to support for and recovery from surgery, include:
Table 11. PEMF Actions for Surgery
● Acupuncture Stimulation
● Anti-bacterial/-fungal/-viral Actions
● Anti-coagulant Effects
● Anti-Edema Activity
● Anti-Inflammatory Response
● ATP and Mitochondria
● Autophagy
● Circulation
● Collagen hyaluronic acid and GAGs
● Growth factors and nitric oxide
● Healing and regeneration of tissue
● Immunology
● Oxygen
● Pain
● Red Blood Cells
● Skin
● Stem cell stimulation
● Stress response
For more detailed discussion of each of these actions either refer to the books or read the section above “Physiologic actions of PEMFs.”
Table 12. Below, summarizes several studies that evaluated surgical outcomes combined with PEMF therapies. There were no cancer surgery studies. The Russian studies above did include some that combined surgery with or without radiation and chemo. Some of the studies below were reviews of studies. Several studies used non-heating diathermy-type PEMFs with significant benefits. Since these are often circular PEMF coils of relatively low intensity, placement of these coils becomes critical to wound healing. Many clinicians place the wounds in the center of the coil where the magnetic field intensity drops dramatically. Ideal placement would be at the ring of the coil, with the magnetic field is the strongest.
PEMF therapy relative to surgery should be considered prior to elective surgery to precondition the tissues, especially increasing heat shock proteins, resulting in less appreciable trauma impact from the surgical wound and, consequently, had faster and better recovery, with lower likelihood of complications, especially infectious and circulatory. Because of edema of the wound area caused by the surgical procedures, circulation is compromised and rapid recovery of edema is important for faster recovery.
213 Super Charge Your Health To Protect Yourself Against Cancer
Table 12. Summary of PEMF Studies Evaluating Surgery Outcomes –
Author PEMF
Zorzi Randomization. Knee arthroscopy; 1.5 mT
Fiani Review – spinal fusion surgery
Ehnert
Review - various intensities of PEMFs for Bone Regeneration after Trauma and Orthopedic Surgery
Sorrell Lumbar surgery pain
Khooshideh C-Section
Heden Breast augmentation
Perumal Appendectomy
Zhang Mammaplasty –review of breast reconstruction and augmentation surgery studies
Sutbeyaz Fibromyalgia
PEMF use
Recovery after arthroscopic surgery; 3 yr follow-up
Spinal fusion; low intensity
1.6/50/100/105 uT; 3 mT; 1.3– 2 T for 3-5x/wk; 10-60 mins; 2-6 wks
2x/d, 60 days; 42 μs vs 38 μs; μs is the symbol for which microseconds
Recoveryrx device; (very weak) 27.12 MHz; continuous postop 7 days
Bilat active; bilat sham; 1 breast active; opposite none; 7 days
Recoveryrx device; (v weak) 27.12 MHz; continuous postop 7 days; active vs inactive
Review of 4 pain reduction trials. Mostly MHz devices.
30 mins 2x/d forwks. Very low intensity Whole Body PEMF
PEMF Benefit
Surgery scale sig better at 990 days; NDAIDs 26% active; 75% control; 3 yrs active best outcomes
84 active rx vs 69% control
Pain, stiffness, mobility, quality-oflife improvements
Back pain less – 42μs 40% v 38μs 19% v sham 25%; leg pain 45% v 17% vs 25%.
Sev pain 36% v 72%; meds 1.9x lower; at 7 d post-op better wound healing.
Active 3x better pain from POD3; pain meds better X3 b POD3
12 hr pain score and IV fentanyl use no different. Device placement not right - scar in center of loop vs at edge.
Day 1 mean difference in pain scores were p<0.003; Day 3 p<0.008.
Fibromyalgia score change PEMF 52% Sham 11%
The intensity of the magnetic fields required for surgical aftercare may be less than would be needed for deeper infectious situations, since often the wounds are relatively superficial. For deeper wounds, such as liver surgery, renal, cardiac and intestinal surgeries stronger magnetic fields may be needed because of the loss of intensity of the magnetic field deeper into the body, that is considering the inverse square or inverse cube laws. Experience indicates that tissue healing and recovery would be expected to be about half the usual time. While there is no reference for this, a study I read several decades ago about use of PEMFs in a trauma unit in Europe, the length of stay of the individuals receiving PEMF therapy after extensive trauma was shortened by at least a week. In fact, research in Russia following the Afghan war, found that dogs recovering from explosive heat trauma to the extremities were 1/3 more likely to survive after surgery went PEMF therapies were used.
214 Super Charge Your Health To Protect Yourself Against Cancer
cancer-related
not
Recommended PEMF devices
PEMF therapy does not have to be complicated or extravagantly expensive. Guidance for the proper use of PEMFs is available on DrPawluk.com in various blogs, podcasts and videos and in the book “Supercharge Your Health with PEMF Therapy” . In addition, consultations are available through DrPawluk.com for individuals with cancer looking at the possible use of PEMF therapy in the home setting.
215 Super Charge Your Health To Protect Yourself Against Cancer
References
1. Abd GM, Laird MC, Ku JC, Li Y. Hypoxia-induced cancer cell reprogramming: a review on how cancer stem cells arise. Front Oncol. 2023 Aug 8;13:1227884.
2. Akbarnejad Z, Eskandary H, Dini L, et al Cytotoxicity of temozolomide on human glioblastoma cells is enhanced by the concomitant exposure to an extremely low-frequency electromagnetic field (100Hz, 100G). Biomed Pharmacother, 92 (2017), pp. 254-264
3. Aljurf M, Majhail NS, Koh MBC, et al., editors. The Comprehensive Cancer Center: Development, Integration, and Implementation.Cham (CH): Springer; 2022
4. Ammitzbøll G, Hyldegaard O, Forchhammer M, et al. Effects of an early intervention with Hyperbaric Oxygen Treatment on arm lymphedema and quality of life after breast cancer-an explorative clinical trial. Support Care Cancer. 2023 May 1;31(5):313.
5. Angka L, Khan ST, Kilgour MK, et al. Dysfunctional Natural Killer Cells in the Aftermath of Cancer Surgery. Int J Mol Sci. 2017 Aug 17;18(8):1787.
6. Avgerinos KI, Spyrou N, Mantzoros CS, Dalamaga M. Obesity and cancer risk: Emerging biological mechanisms and perspectives. Metabolism. 2019 Mar;92:121-135.
7. Bakhmutskii NG, Golubtsov VI, Pyleva TA, et al. A case of successful treatment of a patient with breast cancer using a rotating electromagnetic field. Sov Med (8):86-87, 1991.
8. Bakhmutskii NG, Pyleva TA, Frolov VE, et al. The assessment of the efficacy of the effect of an eddy magnetic field on the Course of tumor progression in patients with generalized breast cancer. Lab. for Magnetic Field Applications in Oncology, Kuban’ Medical Inst., Krasnodar, Russia. Sov Med (7):25-27, 1991.
9. Bakhmutskii NG, Sinitskii DA, Pyleva TA, et al. Use of a magnetic eddy field in the treatment of mammary tumor. All-Union Symposium: Laser and Magnetic Therapy in Experimental and Clinical Studies, A. Tsyb, M. Kaplan, eds., 16-18 June, Obninsk, Kaluga Region, Russia, 203-204, 1993.
10. Balunas MJ, Su B, Brueggemeier RW, Kinghorn AD. Natural products as aromatase inhibitors. Anticancer Agents Med Chem. 2008 Aug;8(6):646-82.
11. Barbault A, Costa FP, Bottger B, et al. Amplitude-modulated electromagnetic fields for the treatment of cancer: discovery of tumor-specific frequencies and assessment of a novel therapeutic approach. J Exp Clin Cancer Res. 2009 Apr 14;28(1):51.
12. Bennett M, Feldmeier J, Smee R, et al.. Hyperbaric oxygenation for tumor sensitisation to radiotherapy. Cochrane Database Syst Rev. 2005 Oct 19;(4):CD005007.
13. Block KI, Gyllenhaal C, Tripathy D, et al. Survival impact of integrative cancer care in advanced metastatic breast cancer. Breast J. 2009 Jul-Aug;15(4):357-66.
14. Bosco G, Casarotto A, Nasole E, et al. Preconditioning with hyperbaric oxygen in pancreaticoduodenectomy: a randomized double-blind pilot study. Anticancer Res. 2014 Jun;34(6):2899906.
15. Cameron IL, Sun LZ, Short N, Hardman WE, Williams CD. 2005. Therapeutic electromagnetic field (TEMF) and γ irradiation on human breast cancer xenograft growth, angiogenesis, and metastasis. Cancer Cell Int 5:23–36.
16. Campbell EL, Bruyninckx WJ, Kelly CJ, et al. Transmigrating Neutrophils Shape the Mucosal Microenvironment through Localized Oxygen Depletion to Influence Resolution of Inflammation, Immunity, 40(1), 2014, 66-77.
17. Capanna R, Donati D, Masetti C, et al. Effect of electromagnetic fields on patients undergoing massive bone graft following bone tumor resection. A double blind study. Clin OrthopRelat Res. 1994 Sep;(306):213-21.
18. CDC - https://www.cdc.gov/chronicdisease/about/index.htm
216 Super Charge Your Health To Protect Yourself Against Cancer
19. Chen HL, Zhou MQ, Tian W, et al. Effect of Age on Breast Cancer Patient Prognoses: A Population-Based Study Using the SEER 18 Database. PLoS One. 2016 Oct 31;11(10):e0165409.
20. Chiles KA, Staff I, Johnson-Arbor K, et al. A Double-Blind, Randomized Trial on the Efficacy and Safety of Hyperbaric Oxygenation Therapy in the Preservation of Erectile Function after Radical Prostatectomy. J Urol. 2018 Mar;199(3):805-811.
21. Choi IK, Strauss R, Richter M, Yun CO, Lieber A. Strategies to increase drug penetration in solid tumors. Front Oncol. 2013 Jul 26;3:193.
22. Clarke M, Collins R, Darby S, et al.; Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005 Dec 17;366(9503):2087-106.
23. Colgan, S., Taylor, C. Hypoxia: an alarm signal during intestinal inflammation. Nat Rev Gastroenterol Hepatol 7, 281–287 (2010).
24. Costa FP, de Oliveira AC, Meirelles R, et al. Treatment of advanced hepatocellular carcinoma with very low levels of amplitude-modulated electromagnetic fields. Br J Cancer. 2011 Aug 23;105(5):640-8.
25. de Kleijn S, Bouwens M, Verburg-van Kemenade BM, et al. Extremely low frequency electromagnetic field exposure does not modulate toll-like receptor signaling in human peripheral blood mononuclear cells. Cytokine. 2011 Apr;54(1):43–50.
26. Dobrynin Y, Letiagin VP, Rybakov Yu L, et al. The effect of the turbulent magnetic field (TMF) in the preoperative combined therapy of human breast cancer (meeting abstract). Russian Cancer Res. Center of the Russian Acad. of Medical Sciences, Res. - Production Center “Zdorovye,” Moscow, 115478, Russia. Bioelectromagnetics Society, 23rd Annual Meeting, 11-14 June, St. Paul, MN, Abstract No. P-77, p. 164-165, 2001.
27. Dobrynin YV, Mescherikova VV, Nikolaeva TG, et al. Radioprotective effect of the turbulent magnetic field generated by Magnetoturbotron (meeting abstract). Blokhin Cancer Res. Center of the Russian Academy of Medical Sciences, Res.-Production Center “Zdorovye”, 115478 Moscow, Russia. Bioelectromagnetics Society, 20th Annual Meeting, 7-11 June, St. Pete Beach, FL, Abstract No. P-195A, p. 267-268, 1998b.
28. Dobrynin YV, Nikolaeva TG, Sedakova LA, et al. Antitumor effect of turbulent magnetic field (TMF) in experimental systems and possible biological mechanisms for its action (meeting abstract). Blokhin Cancer Res. Center of the Russian Academy of Medical Sciences, Res.-Production Center “Zdorovye”, 115478 Moscow, Russia. Bioelectromagnetics Society, 20th Annual Meeting, 7-11 June, St. Pete Beach, FL, Abstract No. P-194B, p. 266-267, 1998a.
29. Ehnert S, Schröter S, Aspera-Werz RH, et al. Translational Insights into Extremely Low Frequency Pulsed Electromagnetic Fields (ELF-PEMFs) for Bone Regeneration after Trauma and Orthopedic Surgery. J Clin Med. 2019 Nov 20;8(12):2028.
30. Engel J, Eckel R, Halfter K, Schubert-Fritschle G, Hölzel D. Breast cancer: emerging principles of metastasis, adjuvant and neoadjuvant treatment from cancer registry data. J Cancer Res Clin Oncol. 2023 Feb;149(2):721-735.
31. Evangelou A, Toliopoulos I, Giotis C, Metsios A, Verginadis I, Simos Y, Havelas K, Hadziaivazis G, Karkabounas S. Functionality of natural killer cells from end-stage cancer patients exposed to coherent electromagnetic fields. Electromagn Biol Med. 2011 Mar;30(1):46-56.
32. Fan W, Qian F, Ma Q, et al. 50 Hz electromagnetic field exposure promotes proliferation and cytokine production of bone marrow mesenchymal stem cells. Int J Clin Exp Med. 2015 May 15;8(5):7394-404.
33. Fiani B, Kondilis A, Runnels J, Rippe P, Davati C. Pulsed Electromagnetic Field Stimulators Efficacy for Noninvasive Bone Growth in Spine Surgery. J Korean Neurosurg Soc. 2021 Jul;64(4):486494.
217 Super Charge Your Health To Protect Yourself Against Cancer
34. Frolov VE, Bakhmutskii NG, Sinitskii DA, et al. Morphology of breast tumor in patients after combined therapy using pre-operation treatment with a magnetic eddy field. All-Union Symposium: Laser and Magnetic Therapy in Experimental and Clinical Studies, Tsyb A and Kaplan M, eds., 16-18 June, Obninsk, Kaluga Region, Russia, p. 204-206, 1993.
35. Ghannam MM, Al-Otaibi HA, Alanazy ES, et al. Magnetic field potential effects on the doxorubicin therapeutic activity in Ehrlich tumor growth. Saudi J Biol Sci. 2021 Apr;28(4):2566-2574.
36. Gkretsi V, Zacharia LC, Stylianopoulos T. Targeting Inflammation to Improve Tumor Drug Delivery. Trends Cancer. 2017 Sep;3(9):621-630.
37. Gorgun SS. Studies on the interaction between electromagnetic fields and living matter. Front Perspect 7(2):44-59, 1998.
38. Goritskaya I, Vinokurov V, Uritsky V, et al. The treatment effect of elf magnetic fields on patients with ovarian tumors. Bioelectromagnetics Society, 17th Annual Meeting, 18-22 June, Boston, MA, Abstract No. P-16A, p. 99, 1995.
39. Gray JR, Frith CH, Parker JD. In vivo enhancement of chemotherapy with static electric or magnetic fields. Bioelectromagnetics. 2000 Dec;21(8):575-83.
40. Greer S., Watson M. (1985). Towards a psychobiological model of cancer: psychological considerations. Soc. Sci. Med. 20, 773–777.
41. Guerra-Martín MD, Tejedor-Bueno MS, Correa-Casado M. Effectiveness of Complementary Therapies in Cancer Patients: A Systematic Review. Int J Environ Res Public Health. 2021 Jan 24;18(3):1017.
42. Gupta SC, Kunnumakkara AB, Aggarwal S, et al. (2018) Inflammation, a Double-Edge Sword for Cancer and Other Age-Related Diseases. Front. Immunol. 9:2160.
43. Hao Q, Wenfang C, Xia A, et al. Effects of a moderate-intensity static magnetic field and adriamycin on K562 cells. Bioelectromagnetics. 2011 Apr;32(3):191-9.
44. Harris IS, Treloar AE, Inoue S, et al. Glutathione and thioredoxin antioxidant pathways synergize to drive cancer initiation and progression. Cancer Cell. 2015 Feb 9;27(2):211-22. If
45. Hedén P, Pilla AA. Effects of pulsed electromagnetic fields on postoperative pain: a double-blind randomized pilot study in breast augmentation patients. Aesthetic Plast Surg. 2008 Jul;32(4):660-6.
46. Heys SD, Smith IC, Ross JA, et al. A pilot study with long term follow up of hyperbaric oxygen pretreatment in patients with locally advanced breast cancer undergoing neo-adjuvant chemotherapy. Undersea Hyperb Med. 2006 Jan-Feb;33(1):33-43.
47. Horneber M, Bueschel G, Dennert G, et al. How many cancer patients use complementary and alternative medicine: a systematic review and metaanalysis. Integr Cancer Ther. 2012 Sep;11(3):187-203.
48. Hu J, Webster D, Cao J, Shao A. The safety of green tea and green tea extract consumption in adults - Results of a systematic review. Regul Toxicol Pharmacol. 2018 Jun;95:412-433.
49. Huifang L, Jie G, Yi F. Neuro-immune-endocrine mechanisms with poor adherence to aromatase inhibitor therapy in breast cancer. Front Oncol. 2022 Dec 12;12:1054086.
50. Johnson SB, Park HS, Gross CP, Yu JB. Complementary Medicine, Refusal of Conventional Cancer Therapy, and Survival Among Patients with Curable Cancers. JAMA Oncol. 2018;4(10):1375–1381.
51. Karra P, Winn M, Pauleck S, et al. Metabolic dysfunction and obesity-related cancer: Beyond obesity and metabolic syndrome. Obesity (Silver Spring). 2022 Jul;30(7):1323-1334.
52. Khooshideh M, Latifi Rostami SS, Sheikh M, et al. Pulsed Electromagnetic Fields for Postsurgical Pain Management in Women Undergoing Cesarean Section: A Randomized, Double-Blind, Placebo-controlled Trial. Clin J Pain. 2017 Feb;33(2):142-147.
218 Super Charge Your Health To Protect Yourself Against Cancer
53. Kiselev AV and Grushina TI. Use of artificial magnetic field for rehabilitation of children with malignant tumors. VoprOnkol 46(4):469-472, 2000.
54. Kolomietz A, Suslova TE, Savina EV, et al. Clinical-immunological effects of magnetotherapy. All-Union Symposium: Laser and Magnetic Therapy in Experimental and Clinical Studies, Tsyb A and Kaplan M, eds., 16-18 June, Obninsk, Kaluga Region, Russia, p. 208-209 1993.
55. Kolomietz LA, Velichko SA, Stukanov SL, et al. Effect of laser and magnetic therapy on hormonal balance in patients with premalignancy of stomach (meeting abstract). Res. Inst. of Oncology, Tomsk Res. Center, Tomsk, Russia All-Union Symposium: Laser and Magnetic Therapy in Experimental and Clinical Studies, A. Tsyb, M. Kaplan, eds., 16-18 June, Obninsk, Kaluga Region, Russia, p. 49-50, 1993.
56. Kovalchuk VI, Ahtirskii VI, Dubovoi LV. Use of weak extremely-low-frequency magnetic fields in treatment of oncological diseases. FizicheskaiaMeditzina 4(1-2):93-95. Abstracts of All-Russian Conference “Use of Low-Level Laser Radiation and Magnetic Fields in Biology and Medicine,” Obninsk, Russia, 21-23 June 1994.
57. Labędź W, Przybyla A, Zimna A, Dąbrowski M, Kubaszewski Ł. The Role of Cytokines in the Metastasis of Solid Tumors to the Spine: Systematic Review. Int J Mol Sci. 2023 Feb 14;24(4):3785.
58. Lan T, Chen L, Wei X. Inflammatory Cytokines in Cancer: Comprehensive Understanding and Clinical Progress in Gene Therapy. Cells. 2021 Jan 8;10(1):100.
59. Letiagin VP, Dobrynin YV, Rybakov YL, et al. Application of the turbulent magnetic field (TMF)-influence for decrease of the postoperative lymphorrhea after surgical treatment of the locally spread breast cancer. Bioelectromagnetics Society, 24th Annual Meeting, 23-27 June, Quebec City, QC, Canada, Abstract (poster) No. P-26, p. 162, 2002.
60. Li K, Zhang K, Xu S, et al. EMP-induced BBB-disruption enhances drug delivery to glioma and increases treatment efficacy in rats. Bioelectromagnetics. 2018 Jan;39(1):60-67.
61. Lo Bianco G, Lanza E, Provenzano S, Federico M, Papa A, Imani F, Shirkhany G, Laudicella R, Quartuccio N. A Multimodal Clinical Approach for the Treatment of Bone Metastases in Solid Tumors. Anesth Pain Med. 2022 Jun 21;12(3):e126333.
62. Lubennikov VA, Lazarev AF, Golubtsov VT. First experience in using a whole-body magnetic field exposure in treating cancer patients. VoprOnkol 41(2):140-141, 1995.
63. Mandolini G, Santantonio M, Zucchini P, et al. The association of PEMF and 60co irradiation for the treatment of patients suffering from brain metastases not surgically removable. Electromagnetics in Biology and Medicine. Brighton CT, Pollack SR, eds. San Francisco, CA: San Francisco Press, p. 343-346, 1991.
64. Mao L, Wang L, Xu J, Zou J. The role of integrin family in bone metabolism and tumor bone metastasis. Cell Death Discov. 2023 Apr 10;9(1):119.
65. Mari R, Mamessier E, Lambaudie E, et al. Liquid Biopsies for Ovarian Carcinoma: How Blood Tests May Improve the Clinical Management of a Deadly Disease. Cancers (Basel). 2019 Jun 4;11(6):774.
66. Mereles D, Hunstein W. Epigallocatechin-3-gallate (EGCG) for clinical trials: more pitfalls than promises? Int J Mol Sci. 2011;12(9):5592-603.
67. Miasoedov DV, Biniashevskii EV, Bundiuk LS, et al. Experience with the use of microwave resonance therapy as a modifying factor in oncological therapy. Fundamental and Applied Aspects of the Use of Millimeter Electromagnetic Radiation in Medicine. Abstracts of the 1st AllUnion Symposium with International Participation. 10-13 May, 1989, Kiev, Ukraine, p. 313-315, 1989.
68. Milevskaya TG, Shitikov BD, Prohorova VI, et al. Eddy magnetic field therapy as a part of combined therapy for breast cancer. Mammologia (2):51-55, 1997.
69. Minchinton AI, Tannock IF. Drug penetration in solid tumors. Nat Rev Cancer. 2006 Aug;6(8):58392.
219 Super Charge Your Health To Protect Yourself Against Cancer
70. Miyagi N, Sato K, Rong Y, Yamamura S, Katagiri H, Kobayashi K, Iwata H. Effects of PEMF on a murine osteosarcoma cell line: drug-resistant (P-glycoprotein-positive) and non-resistant cells. Bioelectromagnetics. 2000 Feb;21(2):112-21.
71. Moen I, Stuhr LE. Hyperbaric oxygen therapy and cancer--a review. Target Oncol. 2012 Dec;7(4):233-42.
72. Moore HCF. Breast cancer survivorship. Semin Oncol. 2020 Aug;47(4):222-228.
73. Mundy GR. Metastasis to bone: causes, consequences and therapeutic opportunities. Nat Rev Cancer. 2002 Aug;2(8):584-93.
74. Nakachi K, Suemasu K, Suga K, et al. Influence of drinking green tea on breast cancer malignancy among Japanese patients. Jpn J Cancer Res. 1998 Mar;89(3):254-61.
75. Ogorodnikova LS, Gairabed’iants NG, Ratner ON, et al. Morphological criteria of lung cancer regression under the effect of magnetotherapy. VoprOnkol 26(1):28-34, 1980.
76. Omote Y, Hosokawa M, Komatsumoto M, et al. Treatment of experimental tumors with a combination of a pulsing magnetic field and an antitumor drug. Jpn J Cancer Res. 1990 Sep;81(9):95661.
77. Ozinkovskii VV. The use of low frequency alternating and constant magnetic fields in otolaryngology. ZhUshn Nos GorlBolezn (6):74-77, 1981.
78. Parida S, Siddharth S, Sharma D. Adiponectin, Obesity, and Cancer: Clash of the Bigwigs in Health and Disease. Int J Mol Sci. 2019 May 22;20(10):2519.
79. Perumal M, Abdul Latib AI, Samy MP, Zainal Abidin MRB, Nagandran E, Wan TS, Francis P, Foo CY. Pulsed electromagnetic fields for post-appendicectomy pain management: a randomized, placebo-controlled trial. Trials. 2022 Oct 14;23(1):874.
80. Radha. G, Lopus M. The spontaneous remission of cancer: Current insights and therapeutic significance. Transl Oncol. 2021 Sep;14(9):101166.
81. Randoll UG and Pangan RM. The role of complex biophysical-chemical therapies for cancer. BioelectrochemBioenerg 27(3):341-346, 1992.
82. Ranji P, Heydari Z, Alizadeh AM. Nanobiotechnological Approaches to Overcome Drug Resistance in Breast Cancer. Curr Cancer Drug Targets. 2015;15(7):544-62.
83. Reuss-Borst M., Hartmann U., Scheede C., Weiß J. Prevalence of osteoporosis among cancer patients in Germany: Prospective data from an oncological rehabilitation clinic. Osteoporos. Int. 2012;23:1437–1444.
84. Ronchetto F, Barone D, Cintorino M, et al. Static and extremely low frequency (ELF) magnetic fields to treat cancer: a pilot study on patients with advanced neoplasm to assess safety and acute toxicity. Bioelectromagnetics Society, 25th Annual Meeting, 22-27 June, Wailea, Maui, HI, Abstract No. 14-1, p. 137, 2003.
85. Rosado MM, Simkó M, Mattsson M-O, et al. (2018) Immune-Modulating Perspectives for Low Frequency Electromagnetic Fields in Innate Immunity. Front. Public Health 6:85.
86. Ross CL, Harrison BS. The use of magnetic field for the reduction of inflammation: a review of the history and therapeutic results. Altern Ther Health Med. 2013 Mar-Apr;19(2):47-54.
87. Ruiz-Gómez MJ, de la Peña L, Prieto-Barcia MI, et al. Influence of 1 and 25 Hz, 1.5 mT magnetic fields on antitumor drug potency in a human adenocarcinoma cell line. Bioelectromagnetics. 2002 Dec;23(8):578-85.
88. Rybakov YL, Kazanov AN, Gerasimenko VN. The effect of the turbulent magnetic field (TMF) in the preoperative combined therapy of human breast cancer. Bioelectromagnetics Society, 23rd Annual Meeting, 11-14 June, St. Paul, MN, Abstract No. P-77, p. 164-165, 2001.
89. Rybakov YL, Wainson AA, Mescherikova VV. Dobrynin, Ya.V. Radioprotective action of the turbulent magnetic field (TMF) when local x-ray irradation on the mice feet skin (meeting abstract).
220 Super Charge Your Health To Protect Yourself Against Cancer
Russian Cancer Res. Center of Medical Sciences, Res. Production Center “Zdorovye,” Moscow, Russia. Bioelectromagnetics Society, 25th Annual Meeting, 22-27, Wailea, Maui, HI, Abstract No. P-16-A, p. 177, 2003.
90. Rymarczyk K, Turbacz A, Strus W, Cieciuch J. Type C Personality: Conceptual Refinement and Preliminary Operationalization. Front Psychol. 2020 Sep 16;11:552740.
91. Salvador F, Llorente A, Gomis RR. From latency to overt bone metastasis in breast cancer: potential for treatment and prevention. J Pathol. 2019 Sep;249(1):6-18.
92. Sanie-Jahromi F, Saadat M. Effects of electromagnetic field, cisplatin and morphine on cytotoxicity and expression levels of DNA repair genes. Mol Biol Rep. 2018 Oct;45(5):807-814.
93. Sauerwein W, Heselman I, Olthoff K, et al. Can low frequency, low intensity magnetic fields be used in cancer treatment? BioelectrochemBioenerg 27(3):347-359, 1992.
94. Sepich-Poore GD, Zitvogel L, Straussman R, Hasty J, Wargo JA, Knight R. The microbiome and human cancer. Science. 2021 Mar 26;371(6536):eabc4552.
95. Seyfried T.N., Shelton L.M. Cancer as a metabolic disease. Nutr. Metab. 2010;7:1–22. doi: 10.1186/1743-7075-7-7.
96. Shen F, Huang J, Yang K, Sun C. A Comprehensive Review of Interventional Clinical Trials in Patients with Bone Metastases. Onco Targets Ther. 2023 Jun 29;16:485-495.
97. Shen F, Huang J, Yang K, Sun C. A Comprehensive Review of Interventional Clinical Trials in Patients with Bone Metastases. Onco Targets Ther. 2023 Jun 29;16:485-495.
98. Sieber WJ, Rodin J, Larson L, Ortega S, Cummings N, Levy S, Whiteside T, Herberman R. Modulation of human natural killer cell activity by exposure to uncontrollable stress. Brain Behav Immun. 1992 Jun;6(2):141-56.
99. Skyler B Johnson and others, Use of Alternative Medicine for Cancer and Its Impact on Survival, JNCI: Journal of the National Cancer Institute, Volume 110, Issue 1, January 2018, Pages 121–124.
100.Sorrell RG, Muhlenfeld J, Moffett J, Stevens G, Kesten S. Evaluation of pulsed electromagnetic field therapy for the treatment of chronic postoperative pain following lumbar surgery: a pilot, double-blind, randomized, sham-controlled clinical trial. J Pain Res. 2018 Jun 22;11:1209-1222.
101. Spiegel D, Bloom JR, Kraemer HC, Gottheil E. Effect of psychosocial treatment on survival of patients with metastatic breast cancer. Lancet. 1989 Oct 14;2(8668):888-91.
102. Standish LJ, Sweet E, Kim E, et al. Recurrence of Breast Cancer After Primary Treatment: A Matched Comparison Study of Disease-Free Survival in Women Who Do and Do Not Receive Adjunctive Naturopathic Oncology Care. Integr Cancer Ther. 2021 Jan-Dec;20:15347354211058404.
103. Sufianova G, Gareev I, Beylerli O, Wu J, Shumadalova A, Sufianov A, Chen X, Zhao S. Modern aspects of the use of natural polyphenols in tumor prevention and therapy. Front Cell Dev Biol. 2022 Sep 12;10:1011435.
104. Sutbeyaz ST, Sezer N, Koseoglu F, Kibar S. Low-frequency pulsed electromagnetic field therapy in fibromyalgia: a randomized, double-blind, sham-controlled clinical study. Clin J Pain. 2009 Oct;25(8):722-8.
105.Talib WH, Mahmod AI, Kamal A, et al. Ketogenic Diet in Cancer Prevention and Therapy: Molecular Targets and Therapeutic Opportunities. Curr Issues Mol Biol. 2021 Jul 3;43(2):558-589.
106. Tang X, Yin X, Zhang T, et al. The effect of hyperbaric oxygen on clinical outcome of patients after resection of meningiomas with conspicuous peritumoral brain edema. Undersea Hyperb Med. 2011 Mar-Apr;38(2):109-15.
107. Tatarov I, Panda A, Petkov D, et al. Effect of magnetic fields on tumor growth and viability. Comp Med. 2011 Aug;61(4):339-45.
108. Traitcheva N, Angelova P, Radeva M et al. ELF fields and photooxidation yielding lethal effects on cancer cells. Bioelectromagnetics 24:148–150, 2003.
221 Super Charge Your Health To Protect Yourself Against Cancer
109. Ueno S, Sakoda M, Kurahara H, et al. Safety and efficacy of early postoperative hyperbaric oxygen therapy with restriction of transfusions in patients with HCC who have undergone partial hepatectomy. Langenbecks Arch Surg. 2011 Jan;396(1):99-106.
110. Ueno S, Tanabe G, Kihara K, Aoki D, Arikawa K, Dogomori H, Aikou T. Early post-operative hyperbaric oxygen therapy modifies neutrophile activation. Hepatogastroenterology. 1999 MayJun;46(27):1798-9.
111. Vianale G, Reale M, Amerio P, et al. Extremely low frequency electromagnetic field enhances human keratinocyte cell growth and decreases proinflammatory chemokine production. Br J Dermatol. 2008 Jun;158(6):1189-96.
112. Vyas S, Zaganjor E, Haigis MC. Mitochondria and Cancer. Cell. 2016 Jul 28;166(3):555-566.
113. Watts ER, Walmsley SR. Inflammation and Hypoxia: HIF and PHD Isoform Selectivity. Trends Mol Med. 2019 Jan;25(1):33-46.
114. Weinberg R, Hanahan D. The Hallmarks of Cancer. Cell 2000;100(1):57-70.
115. Wells JC, Sidhu A, Ding K, et al. Complementary Medicine Use Amongst Patients with Metastatic Cancer Enrolled in Phase III Clinical Trials. Oncologist. 2022 Mar 11;27(3):e286-e293.
116. Wen J, Jiang S, Chen B. The effect of 100 Hz magnetic field combined with X-ray on hepatoma-implanted mice. Bioelectromagnetics. 2011 May;32(4):322-4.
117. Witek-Janusek L, Gabram S, Mathews HL. Psychologic stress, reduced NK cell activity, and cytokine dysregulation in women experiencing diagnostic breast biopsy. Psychoneuroendocrinology. 2007 Jan;32(1):22-35.
118. Yelin I, Flett KB, Merakou C, et al. Genomic and epidemiological evidence of bacterial transmission from probiotic capsule to blood in ICU patients. Nat Med. 2019 Nov;25(11):1728-1732.
119. Yu Y, Li K, Peng Y, Wu W, Chen F, Shao Z, Zhang Z. Animal models of cancer metastasis to the bone. Front Oncol. 2023 Apr 5;13:1165380.
120. Yuan LQ, Wang C, Zhu K, et al. The antitumor effect of static and extremely low frequency magnetic fields against nephroblastoma and neuroblastoma. Bioelectromagnetics. 2018 Jul;39(5):375-385.
121. Zhang L, Ding W, Ji Y. Analgesic effect of pulsed electromagnetic fields for mammaplasty: A meta-analysis of randomized controlled studies. Medicine (Baltimore). 2020 Aug 28;99(35):e21449.
122. Zhang X, Zhang H, Zheng C, et al. Extremely low frequency (ELF) pulsed-gradient magnetic fields inhibit malignant tumour growth at different biological levels. Cell Biol Int. 2002;26(7):599603.
123. Zhu, M., Yang, Z., Yu, H., et al. (2020). The Efficacy and Safety of Low-frequency Rotating Static Magnetic Field Therapy Combined with Chemotherapy on Advanced Lung Cancer Patients: A Randomized, Double-blinded, Controlled Clinical Trial. International Journal of Radiation Biology, 1–26.
124. Zorzi C, Dall’Oca C, Cadossi R, Setti S. Effects of pulsed electromagnetic fields on patients’ recovery after arthroscopic surgery: prospective, randomized and double-blind study. Knee Surg Sports TraumatolArthrosc. 2007 Jul;15(7):830-4.
List of abbreviations
222 Super Charge Your Health To Protect Yourself Against Cancer
ADCC: Antibody-dependent cellular cytotoxicity
Al Aromatase inhibitor
Akt: v-Akt murine thymoma viral oncogene homolog
ALA Alpha lipoic acid
ALT: Alanine Immuno Transferase
AMPK: 5* AMP-activated protein kinase
APC Adenomatous Polyposis Coli
ART: Antiretroviral therapies
AST: aspartate transaminase
AT: Neoadjuvant therapy
BC: breast cancer
BCG: Bacillus Calmette-Guerin
BCSS: Breast cancer specific survival
BMI: body mass index
Ca cancer
CAA Cancer-Associated Adipocyte
CAM Complementary or alternative medicine
CCT: Conventional cancer therapy
CD18: cluster of differentiation antigen 18 - tumor adhes
CK: Chemokine
CNS: Central nervous system
COX: Cyclooxygenase
CR Complete remission
CRC: Colorectal Cancer
CRP: C-Reactive Protein
CSC: Cancer stem cell
CT: Computer tomography scan
CTC: Circulating tumor cell
ctDNA Circulating tumor DNA
CVD: Cardiovascular Disease
DCA Deoxycholic Acid
DM diabetes mellitus
DNA Decoyribonuoleic Acid
DTC: Disseminated tumor cell
EC: Endometrial Cancer
HbA1c Hemoglobin A1c
HBOT Hyperbaric oxygen therapy
HCC: Hepatocellular Cancer
HIF: Hypoxia inducible factor
HIV: human immunodeficiency virus
HOMA-IR: Homeostatic Model Assessment for
HR Hazardratio
HRT: Hormone Replacement Therapy
hsCRP: high sensitivity C-Reactive Protein
HSV: Herpes simplexvirus
Hz Hertz
IFN: Interferon
IGF: insulin-like growth factor
IGFBP: Insulin-like factor-binding protei PPAR Peroxisome
Proliferator-Activated Receptors
IL: Interleukin
In: inch
IOM Immune-oncologymicrobiome
IPSC Pluripotent stem cells
IPT: Insulin potentiation therapy
IR: Insulin Resistance
KPS: Karnofsky performance score
LES Lower Esophageal Sphincter
LGG: Lactobacillus rhamnosus
strain GG
LHDA Lactose dehydrogenase-A
LN Lymph node
LPS: Lipopolysaccharide
LR Local recurrence
LTB-4 Leukotriene B4
MAPK mitogen-activated protein kinase
MET: Metastasis
MHO: Metabolically Healhy Obesity
microT: MicroTesla
ml milliter
mm Millimeter
MMP metalloproteinase
NMIBC: non-muscle-invasive bladder cancer
NSAIDs Non-steroidal antiinflammatory drugs
NSCLC Non-Small Lung Cancer
O2: Oxygen
OB: Osteoblast
OC: Osteoclast
OS Overall survival
p: probability
PAF: Population Attributable Fraction
PAK1 p21-activated kinase 1
PEMF: Pulsed Electromagnetic Field
PI3K: phosphatidylinositol
PMN Polymorphonuclead (White
PR progesterone receptor
PSA Prostate specific antigen
PT: Primary tumor
PTBE peritumoral brain edema
RCT: Randomized Controlled Trial
RNA Ribonuoleic acid
RNS Reactive nitrogen species
ROS Reactive oxygene species
RR Relative risk
RT: Radiation therapy, radiotherapy
SAT: Subcutaneous Adipose Tissue
SD: Standard deviation
SSR Selective serotonin receptor inhibitor
STAT: Signal Transducer and Activator of Transcription
TC: Tumor cell
TGF: Transforming growth factor
THE T lymphocyte helper type 1 cytokines
TH2: T lymphocyte helper type 2 cytokines
TLR: Toll-like receptor
TME: Tumor microenvironment
TNF-a: tumor necrosis factor-a
223 Super Charge Your Health To Protect Yourself Against Cancer
ECM Extracellular matrix
ECOG: Eastern Cooperative Oncology Group
EGCG epigallocatechin-3-gallate (from green tea)
ELF-EMF:Extremely low-frequency electromagnetic fiel MSC: Mesenchymal Cell
EMOR Eye movement desensitization and reprocessing mT: miliTesla
EMT: Epithelial-Mesenchymal Transition
ENT: Ear, nose and throat
ER: Estrogen receptor
ERK 12: extracellular signalregulated kinase 12
EWOT: Exercise with oxygen therap
FFA: Free Fatty Acid
G Gauss
GERD Gastro-Esophageal Reflux
GLP: Glucagon Like Peptide
GSK3: Glycogen Synthase kinase-3
About the Author
MMW: Millimeter wave
Treg: Regulatory T cell
MRI Magnetic Resonance Imaging Type C: Cancer personality
MRT: Microw ave resonance therapy
mTOR mammalian target of rapamycin
MUO: Metabolically Unhealthy Obesity
N: Number
NAFLD: Non-alcoholic Fatty Liver Disease
Nampt Nicotinamide phosphoribosyltransferas
VEGF: vascular endothelial growth factor
NASH: Non-Alcoholic SteatoHepatitis
NF-kB: nuclear factor-B
NK: Natural Killer
NKCA NK cell activity
NLR: Nucleotide Oligomerization Domain-line Repector
VAT: Visceral Adipose Tissue
VEGF: vascular endothelial growth factor
VM Vascular mimicry
WAT: White Adipose Tissue
WC: Waist Circumference
WHR: Waist-to-Hip Ratio.
VAT: Visceral Adipose Tissue
VM Vascular mimicry
WAT: White Adipose Tissue
WC Waist Circumference
WHR Waist-to-Hip Ratio
William Pawluk, MD, MSc is a formerly American Board-Certified family physician with a practice near Baltimore, Maryland. In addition to being recognized as the foremost authority on the medical use of Pulsed Electromagnetic Field (PEMF) therapy in North America, with over 30 years of experience, he has also trained in the clinical use of acupuncture, bodywork, energy medicine, homeopathy, and hypnosis. During the course of his medical career, he has had academic faculty appointments at a number of universities, including Johns Hopkins, and was the Clinical Director of the University of Maryland’s Complementary and Alternative Medicine Program. While continuing to practice functional and holistic medicine in Baltimore, Maryland, he also routinely consults and teaches other health care practitioners, as well as the public, about the use of PEMF therapy.
Dr. Pawluk is also the author of the books Supercharge Your Health With PEMF Therapy and Power Tools For Health. He has also written book chapters and articles, and has been featured in numerous TV, radio, podcast, and magazine interviews, in addition to being the founder and chief content creator of the authoritative PEMF therapy website, DrPawluk.com
224 Super Charge Your Health To Protect Yourself Against Cancer
