THE POTENTIAL OF PULSED ELECTROMAGNETIC FIELDS (PEMF)
FOR SLOWING OR REVERSING HEART FAILURE




As a holistic physician, I am committed to helping people find real, lasting solutions for managing chronic health conditions. During my years in family medicine, I realized that a lot of the conventional treatments used, particularly in conditions requiring long-term management, were ineffective at best and harmful at worst. I knew there had to be a better way.
The more I learned about alternative modalities, the more I knew I was right. There is a better way, one that gets to the root cause of health issues rather than just masking the symptoms with prescriptions or jumping right to risky procedures that may cause more problems if they don’t address what actually caused the condition.
I was determined to find the best ways to help my patients and received training in functional medicine, nutrition, acupuncture, homeopathy, hypnotherapy, bodywork, and energy medicine as I sought the best solutions. When I discovered pulsed electromagnetic field therapy (PEMF), read the research, and saw firsthand the results my patients enjoyed, I knew I’d found what I’d been looking for.
For more than 30 years, I’ve been exploring the clinical use of PEMFs for healing, regeneration, and holistic pain management. My book, Power Tools for Health, is a comprehensive overview of the research and usage of PEMFs in healing. This book covers the basic concepts in the application of PEMFs, mechanisms of action, an extensive clinical section on 50 different health conditions, and more than 500 references on laboratory findings and clinical trials.
I have authored professional book chapters and journal articles and provided over 10050 interviews for radio, podcasts, magazines, and TV.
I’ve been cohost of a two-hour holistic health radio show for the past ten years. I’m also the host of the Pain Solution Summit at www.painsolutionsummit.com.
In 2019, I was honored to receive the ACIM Lifetime Achievement Award for my work on magnetic field therapy.
Beyond clinical applications, I have discovered that my patients see even better results upon purchasing a PEMF device for home use. Owning a unit allows them to enjoy the ongoing benefits of PEMF therapy for a wide range of conditions far beyond what brings them to me initially.
I’ve done the research on PEMF devices so that I can recommend the best unit for each person's unique situation. I have purchased, tested, and validated approximately 100 different PEMF devices over the 30 years I’ve worked in this field.
Based on my experience, a number of devices are recommended and available for purchase on my website, drpawluk.com. These include local and whole-body systems, both battery and AC-powered devices, and devices ranging from very low intensity (<1 Gauss), medium intensity (10–1,000) Gauss, to high intensity (2,000-8,000 Gauss) machines, including devices that can cause muscle contractions.

with basic educational information, more than 40 blogs with references, numerous videos, and a virtual store from which devices may be purchased. Once devices are purchased, my staff and I provide significant ongoing support for both initial use and subsequent informational needs.
In this e-book, I am pleased to offer a snapshot of the incredible potential of PEMFs specifically in slowing or even reversing heart failure.
Dr. William Pawluk drpawluk@drpawluk.com www.drpawluk.com

fraction, the mechanisms that contribute to it can include fibrosis (scarring), adenosine triphosphate (ATP) depletion, imbalanced neuroendocrine reactions, poor heart muscle contractions, reduced nitric oxide (NO) sensitivity, increased reactive oxygen species (ROS), increased sympathetic nervous system activity, and elevated heart cell death rate (apoptosis).
Pulsed electromagnetic fields (PEMFs) are known to have a safe impact on these mechanisms and can be used alone or to augment the benefits of conventional medical treatments.
It is even possible for individuals, with known or unknown heart or cardiovascular problems, to reduce the likelihood of heart failure by taking advantage of PEMFs for preventive health maintenance.
I first became aware of the potential of PEMF therapy to help individuals with heart failure about two decades ago. That was when I saw a woman, a previously active and avid golfer, confined to a wheelchair because of her late-stage heart failure.
I learned through a colleague that she received around 12 hours of therapy daily with a professional high-intensity static magnetic device over about two weeks.
It was astonishing to see her not only be able to walk again but also be back on the golf course by the end of that treatment time.
I had been a medical doctor for three decades, but I had never seen such a dramatic recovery even without relying on heavy medications.

Heart failure syndrome refers to the inability of the heart to deliver adequate blood to the body in order to meet metabolic needs. There are two types: left-sided heart failure and right-sided heart failure.
This type of heart failure occurs when the left ventricle no longer pumps enough blood around the body and must work harder than normal to pump the same amount of blood. There are further two types of left-sided heart failure: systolic and diastolic.
Also known as heart failure with reduced ejection fraction, systolic failure occurs when the left ventricle loses its ability to contract normally and is unable to pump with adequate force to push enough blood into circulation. The most prominent characteristics of systolic heart failure include hypertrophy, scarring between and among cells (interstitial fibrosis), and sporadic heart cell (cardiomyocyte) death.
This type of left-sided heart failure is also known as heart failure with preserved ejection fraction. It occurs when the left ventricle stiffens and loses its ability to relax normally. It restricts the heart from filling fully with blood properly during the resting period between each beat. The hallmarks of diastolic heart failure include impairment of the cardiac blood vessels themselves, which affects coronary flow reserve and microvascular perfusion.
Right-sided heart failure usually occurs as a result of initially developing left-sided failure. It is when the right side of the heart sustains damage because of the fluid pressure transferred back to the lungs from the failing left ventricle. The blood then backs up in the veins of the body when the right side loses pumping power, causing swelling or congestion in the legs, ankles, gastrointestinal tract, or liver. When both ventricles fail, that is usually an indicator of an end-stage clinical situation of heart failure syndrome.
Heart failure is a progressive disease that has a significant impact on quality of life. It usually worsens with time. Statistics indicate that 80% of men and 70% of women with heart failure under the age of 65 can be expected to die within eight years of the diagnosis. The mortality rate in those with heart failure over the age of 65 is even higher and occurs sooner. This is the reason for the increased urgency to find better solutions for heart failure than currently available in conventional healthcare.
Heart failure occurs as a result of abnormal function of many or even all different parts of the heart. These parts include the pericardium, the myocardium, the endocardium, cardiomyocytes, valves, and the macro and micro cardiac blood vessels.
The most common causes of heart failure include ischemic heart disease, hypertensive heart disease, cardiomyopathy, and rheumatic heart disease.
The leading cause of the condition for those over the age of 50 is hypertension at 60%.
Heart failure is generally found in older adults, as less than 10% of the population between 60 and 79 has been diagnosed with the condition. This number rises between 11% to 14% for those over the age of 80.
It is estimated that the prevalence of heart failure will increase by 46% from 2012 to 2030. That translates to eight million people with heart failure in the United States.
Starting medical therapy for heart failure may lead to some control of the condition, which is referred to as the stability phase. Months to years following the stability phase, heart function may decline, leading to multiple hospitalizations. Eventually, the condition may not respond to treatment when relatively permanent physical changes in the heart ventricles set in.
The longer it takes for treatment to be started from the onset of symptoms and the initial diagnosis, the worse the outcomes. So there is an urgency to start aggressive early management of heart failure much earlier in the course of the condition..
If the condition becomes unmanageable, with much more severe symptoms and disability, therapy becomes more intense with heart failure is medically managed by continuous adjustments of pharmaceuticals and may end up with the use of left ventricular assist devices (LVADs) and cardiac transplantation.
Unfortunately, only a small percentage of people is a candidates for these invasive end-stage treatments.
There are multiple factors, whether acting alone or together that contribute to the development and progression of heart failure.
Adenosine triphosphate is known as the fundamental currency for supplying energy for muscle contractions and producing molecules. The action of cells anywhere in the body requires ATP.
Most of the ATP the heart uses comes from the metabolism of oxygen in the mitochondria, which are essentially the powerhouses of cells. Mitochondria take up about 40% of the volume of heart muscle cells. In contrast, they take up only 20% to 25% of the cell volume in liver cells.

ATP molecules are recycled between 1,000 to 1,500 times every day. That means the human body turns over its weight in ATP daily, translating to about 65 kilograms per day in a resting adult (Zimmerman). Meanwhile, the amount of ATP stored in the body at one time is only about 80 to 100 grams, which is enough energy for five to eight seconds of maximum effort.
Oxygen consumption and cardiac work need a constant supply of ATP (Ventura-Clapier). So it is worth noting that the heart uses more than 90% of its maximal oxidative availability capacity during high-intensity exercise. That means there is minimal extra capacity over what is being used for the exercise.
Individuals with heart failure experience an imbalance between the work the heart must do and the energy available it takes to fulfill its needs. In other words, a failing heart has energy starvation.
The human heart contains less than a gram of ATP, but it uses around six kilograms of these molecules a day to maintain normal cardiac electrical action and continuous contractions. This number amounts to around 10% of the total need of the whole body for ATP per day.
The ATP in a normal heart renews roughly every 20 seconds. If the production of these molecules were to stop abruptly in a healthy human heart, the stored ATP would only be able to keep the heart beating for a few seconds. Therefore, the rate of ATP use must match the rate of ATP production beat-to-beat.
The heart is considered a metabolic omnivore and can use multiple sources to produce ATP (Zhou). There are many metabolic pathways that must be controlled and integrated to supply the ATP needed for cell processes, such as ion transport, muscle contraction, nerve impulses, and phosphorylation (Dunn). It is for that reason heart muscle cells need ATP to maintain normal heart rates, pump blood, and support increased work demands or recruit its contractile reserve.
It is also worth noting that there is an ATP paradox in heart failure. failing heart is mostly maintained until the end stage despite a mismatch between energy supply and demand. That means the heart continues on a downward spiral to failure despite relatively stable levels of ATP.
The mitochondria work to keep energy balance during cardiac remodeling. Still, an adequate supply of ATP alone is not enough to stop the other non-energy-dependent processes in heart failure from leading to the vicious cycles of the condition (Zhou)
Given these considerations, ATP plays a critical role when there is ischemia or a lack of blood supply to the heart, as well as in the development and maintenance of cardiac hypertrophy and subsequent heart failure. Improving the ATP environment of the heart is a major consideration in the use of PEMFs in the setting of heart failure.
Cardiac hypertrophy or heart enlargement is the abnormal or pathologic remodeling of heart tissue and is an early indicator of possible heart failure.
This remodeling increases energy demand because of unfavorable heart shape, increased neurohormonal stimulation, and impaired calcium function (Zhou).

An abnormal calcium ion imbalance is a hallmark of heart failure since the movement of calcium ions is impaired in failing hearts.
This imbalance results in reduced energy charge during the normally unceasing cardiac electrical activity.
The mitochondria act as a calcium ion sink under pathological conditions, resulting in a calcium ion overload that contributes to mitochondrial dysfunction. These ions are important regulators of mitochondrial function, but their uptake into mitochondria is reduced in failing hearts (Zhou).
Pulsed electromagnetic fields have been shown to increase intracellular calcium ions, demonstrating another potential pathway to help manage heart failure (Barbier).
The production of beat-to-beat cardiac ATP occurs through mitochondrial oxidative metabolism using fatty acids as the primary fuel (Zhou).
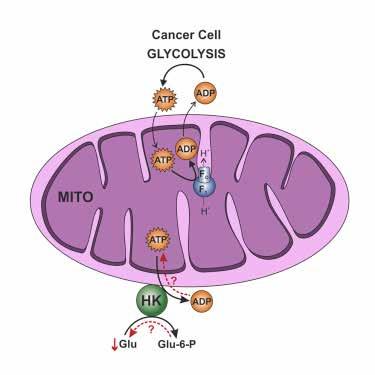
It is during the pathological cardiac remodeling during the development of cardiac hypertrophy that cardiac metabolism shifts toward glucose as fatty acid oxidation and metabolism decrease.
Adenosine triphosphate generated from the use of glucose alone is less than 5% of the total used in a normal adult heart.
An increase in reliance on glucose also reduces the efficiency of ATP production and worsens pathological remodeling.
Moreover, since fatty acid metabolism is not as efficient, lower fatty acid oxidation increases the accumulation of damaging incompletely oxidized fatty acids. This mismatch between fatty acid supply and oxidation is seen early in heart failure.
The cardiac output of individuals with heart failure may be lower, but it does not necessarily indicate a decreased ejection fraction.
It is often the case that symptoms are due to a decreased forward blood flow or the output of blood into the rest of the body.
The body tries to compensate for the low output through physiological responses that increase the amount of blood coming into the heart and going out into the rest of the body.
These compensatory mechanisms lead to a vicious cycle that worsens heart malfunction and increases heart failure symptoms.
Reduced heart muscle function can result from the inability of the heart muscles to contract properly or the stiffening of the muscle walls. Blood builds up when the heart chambers are unable to get rid of all the blood with each contraction and relaxation.
The backward pressure in the blood vessels from the backup leads to fluid leakage into the lungs and throughout the body, resulting in congestion. Hence the reason for the older term congestive heart failure.
Heart enlargement or cardiomegaly occurs in heart failure in order to cope with the effects of the condition. It affects the flow of electrolytes in and out of the heart muscle, which is essential to preserve cardiac function.
The endothelium is a fragile lining of metabolically active cells inside the blood vessel walls.
A common cause of heart failure is impaired cardiac blood vessel endothelial function, which is related to local and systemic microvascular inflammation.
It is often due to underlying coexisting conditions such as hypertension, obesity, ischemia, diabetes, metabolic syndrome, lung disease, and iron deficiency.
It is also well known that autoimmune diseases can contribute to systemic inflammation that leads to endothelial inflammation.
The effects of heart failure are cumulative and increasingly irreversible as the heart remodels itself, so the longer the condition has been in place, the more rapid the decline. Moreover, longer heart failure duration is independently associated with advanced and irreversible myocardial damage (Sugiura).

The large coronary arteries are responsible for feeding the heart muscle (macrovascular circulation), but it is the tiny capillary blood vessels that do most of the work to supply circulation to the heart tissue, down to the cellular level (microvascular circulation).
The density of capillaries in a given area of tissue is critical for blood supply at the tissue level, as both low capillary density and obstructed vascular flow can impact cardiac function.
Individuals with heart failure can have body-wide macrovascular or microvascular constriction and reduced peripheral blood supply.
The benefits of improving blood flow in heart failure have been known for a long time (Luxán).
For example, nitroglycerine and other nitrates, or nitrites that release nitric oxide, have been used for managing heart disease since 1847 because of their vasodilating abilities (Lee).
Angiotensin-converting enzyme inhibitor drugs, commonly used in treating heart failure, stimulate the release of nitric oxide, and PEMFs have been found to increase the activity of these drugs (Sadeghzadeh).
Macrovascular narrowing or occlusion of the coronary arteries results in reduced blood supply to the myocardium, leading to secondary microvascular problems.
However, microvascular dysfunction can still occur without coronary artery occlusion, as metabolic syndromes, diabetes, and hypertension can all affect coronary microcirculation.
Cardiac hypertrophy, which is maladaptive, is also associated with reduced vessel density because fewer capillaries lead to decreased oxygen supply to the enlarged heart muscle.
The blood vessels of the heart also control cardiac cell metabolism in addition to regulating local blood flow. The metabolic requirements of the heart to fulfill its pumping function are immense, so the vasculature is essential for regulating cardiac metabolism and protecting against heart failure.
In diastolic heart failure from coronary artery disease, there is also an increase in reactive oxygen species, a decrease in nitric oxide, and inflammatory activation in the microvasculature.
These complications lead to reduced microvascular circulation and endothelial dysfunction, causing the endothelium to start shedding itself. The restoration of endothelial function should also restore vascular flow and oxygen supply and rescue dysfunctional cardiomyocytes.
Recovering microvascular function is especially important for patients with stunned or hibernating myocardium.
A stunned myocardium occurs as a result of the coronary blood supply improving after prolonged postischemic dysfunction, such as in heart ischemia episodes or myocardial infarction. Meanwhile, hibernating myocardium is chronically ischemic and supplied by a narrowed coronary artery in which ischemic cells have not died, and, being chronically dysfunctional, leading to contraction that is chronically depressed.
It is worth noting that diastolic heart failure is becoming the predominant form of heart failure among the aging population. There is an important link between coronary microcirculatory dysfunction and diastolic heart failure as this condition involves all the muscular structures of the heart.
The cardiac microvascular endothelial cells are responsible for regulating the relaxation of cardiomyocytes, especially through nitric oxide activity. There is some evidence that PEMFs induce nitric oxide activity in various circumstances, contributing to increased microvascular blood flow and secondarily to reduced development of hypertrophy (McKay).
It is known that heart failure is associated with measures of systemic inflammation (Murphy). However, clinical trials of conventional anti-inflammatory therapies have been shown ineffective at managing the this progressive condition.
Therefore, targeted anti-inflammatory therapies with non-conventional approaches have the potential to improve the prognosis for heart failure.
Inflammation in the heart is a hallmark of heart failure, but there is more inflammation in those with diastolic heart failure.
That is because diastolic heart failure is more associated with obesity, diabetes, hypertension, chronic obstructive pulmonary disease, and chronic kidney disease. These conditions are similar in that they involve high levels of inflammation.
That means the therapeutic target in diastolic heart failure should be the reduction of systemic inflammation, rather than just cardiac inflammation.
In one study, 57% of individuals with heart failure had elevated serum c-reactive protein (CRP), a common measure of systemic inflammation (Redfield).
Those in stable chronic heart failure with reduced and preserved ejection fraction had a median elevated hs-CRP (high sensitivity C- reactive protein) between 6.6 milligrams per liter and 8.5 milligrams per liter, with optimal levels being less than one milligram per liter (Watanabe).
Meanwhile, systemic inflammation is even greater in acute heart failure, with hsCRP concentrations of 12.6 milligrams per liter.
Other markers of inflammation are also elevated in individuals with heart failure. These include tumor necrosis factor-a, interleukin-1b, interleukin-6, and galectin-3. Tumor necrosis factor-a is associated with both impaired systolic and diastolic function as well as adverse cardiac remodeling.
Injury of cardiac cells leads to increased interleukin-1 (IL-1), which reduces energy production and myocardial contractility through direct effects on mitochondria. Moreover, IL-1interleukin-1 impairs diastolic function by affecting intracellular calcium reuptake, inhibiting cardiomyocyte relaxation, and decreasing nuclear factor kappa B.
The decrease of nuclear factor kappa B is significant as it is necessary for reducing inflammation, apoptosis, extracellular matrix remodeling, and mitochondrial dysfunction.
It also induces antioxidant effects.
The use of anti-interleukin-1 therapy has been evaluated in those with recently decompensated heart failure, and the death or hospitalization rate after long-term therapy was lower (Murphy)
However, it may take longer for anti-inflammatory therapies to deliver benefits than conventional medical therapies with heart function action-altering mechanisms, but the benefits of the latter are shorter-acting.
The reduction of interleukin-12 and interleukin-23 can also be helpful. That is because interleukin-12 can induce autoimmune myocarditis and microvascular endothelial dysfunction, while interleukin-23 has shown to increase myocardial remodeling and decrease survival post-myocardial infarction in animals.
Bottom line, targeting these said inflammatory factors is crucial in adequately managing heart failure.
Excess body fat is another important target in reducing body inflammation, as it also increases the risk of heart failure (Harada).
Adipose tissue, such as belly fat, secretes a variety of cytokines or adipokines, which have a high likelihood of pro-inflammatory actions. In contrast, the production of adiponectin, an anti-inflammatory adipokine that inhibits cardiac hypertrophy, inflammation, and fibrosis, is suppressed in obesity.
In addition to the increased cardiovascular risk from visceral obesity, it has been found that increased fat around the heart, called epicardial adipose tissue, creates an additional risk for the heart (Mookadam).
The epicardial adipose tissue is also often referred to as the pericardial fat pad. There is evidence of a correlation between the amount of visceral obesity and the pericardial fat pad. So the risk factors contributing to visceral obesity also apply to the pericardial fat pad.
The pericardial fat pad is known to increase the mechanical load on the heart.
It releases adipokines and cytokines, metabolically modulates adjacent cardiac tissue, diffuses free fatty acids directly into adjacent heart cells, and contributes to the overall metabolic burden of obesity.
A pericardial fat pad thicker than five millimeters is associated with left atrial enlargement, lower ejection fraction, increased size of the left ventricle, and abnormal diastolic function, all of which contribute further to heart failure.
The activation of the innate immune system contributes to the inflammatory milieu in heart failure (Murphy). The toll-like receptor four, of which has the highest amount in the heart, contributes to the myocardial inflammation that occurs in heart failure, myocarditis, ischemia-reperfusion injury, aortic valve disease, hypertension, and atherosclerosis. Moreover, toll-like receptor four expression is increased in patients with advanced heart failure, and failure and inhibiting it has been found to reduce interleukin-1b and interleukin-6 concentrations and lessen cardiomyocyte hypertrophy in response to pressure overload in animal models of heart failure. Statistics indicate that 70% of patients with end-stage heart failure have anti-cardiac antibodies, which may be directed against various cardiac proteins or enzymes (Murphy). While less than 1% of the healthy population have autoantibodies against b1-adrenergic receptors, up to 60% of patients with nonischemic cardiomyopathy and more than 90% of those with implanted LVADs have them. Reducing these antibodies has been shown to improve cardiac function and left ventricular ejection fraction.
The negative impact of inflammatory cytokines extends beyond the heart itself but also to the skeletal muscle oxygen extraction during exercise.
Inflammation also worsens anemia and loss of muscle mass, promotes sodium retention in the kidneys, and increases pulmonary pressures during exercise because of pulmonary vasoconstriction.
These effects, additionally to cardiac effects of heart failure, can cause manifest in shortness of breath and reduced exercise tolerance. These are yet, another reason why addressing whole-body inflammation is necessary for a comprehensive approach to managing heart failure.
The hemodynamic stress of heart failure induces a state of sterile inflammation.
In this state, increased heart muscle wall tension and mechanical stretch trigger the release of various pro-inflammatory cytokines by cardiomyocytes and cardiac fibroblasts. These include tumor necrosis factor-a, interleukin-6, interleukin-1b, angiotensin II, and myostatin (Murphy).
Heart failure itself also triggers mitochondrial dysfunction and generates reactive oxygen species. These lead to the activation of the NOD - like receptor protein 3 inflammasome and the maturation of pro-inflammatory cytokines such as interleukin-1b and interleukin-18. Simultaneous with the production of inflammatory cytokines from within the heart, inflammation occurs as a result of innate immune system activation, neurohormonal activation, oxidative stress, and through cross-talk with other organ systems.
Advanced heart failure is often associated with ischemia of the intestinal mucosa by either a decrease in cardiac output or venous congestion in right-sided heart failure. This state allows the crossing over of endotoxins, microbial components, and metabolites into the systemic circulation.
The released endotoxins decrease following diuretics or after the successful treatment of decompensation.
Heart failure is also associated with dysbiosis of the gut microbiome, causing low bacterial diversity and depletion of butyrate-producing bacteria, which exert anti-inflammatory effects.
Senescence is a protective response against stress that limits the proliferation of aged non-functional cells.
However, senescent cells tend to accumulate in fibrotic regions, and there is evidence that senescence is closely related to cardiovascular disease (Gevaert). Indeed, endothelial cell senescence is associated with augmented dysfunction and vascular inflammation.
There are also recent studies that further demonstrate how endothelial senescence contributes to diastolic heart failure.
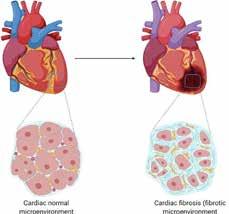
Fibrosis or fibrotic scarring is a form of wound healing in which connective tissue replaces normal tissue. If left unchecked, it can lead to significant tissue remodeling and the formation of permanent scar tissue.
Cardiac remodeling is a key mechanism of heart failure, and it has two aspects: cardiomyocyte injury and myocardial fibrosis (Liu).
Cardiomyocyte injury presents as cardiomyocyte hypertrophy, necrosis, and apoptosis. Repeated cellular injuries and chronic inflammation and repair are susceptible to fibrosis as the excessive accumulation of extracellular matrix components leads to permanent fibrotic scarring and thickening of the affected tissue.
Fibrosis deposits connective tissue, which can interfere with or altogether inhibit the normal structure and function of the organ or tissue. One of the contributors to fibrosis is the accumulation of mast cells.
The density of mast cells increases in ischemic cardiomyopathy and hypertension, so the accumulation of mast cells in heart muscle can lead to fibrotic and inflammatory reactions.
There are two types of heart fibrosis: replacement and interstitial fibrosis. Replacement fibrosis usually occurs after heart cell necrosis from myocardial infarction, but it can also stem from hypertrophic cardiomyopathy, sarcoidosis, myocarditis, chronic renal insufficiency, and toxic cardiomyopathies.

Meanwhile, interstitial fibrosis is diffuse and includes reactive and infiltrative interstitial fibrosis. Reactive fibrosis is often seen in numerous conditions, such as hypertension and aging. In contrast, infiltrative fibrosis is less common and caused by the progressive deposition of amyloidosis or glycolipids in the spaces between cells. Interstitial and infiltrative fibrosis can eventually lead to heart cell apoptosis and replacement fibrosis. Either form of fibrosis is damaging to the heart.
Blood markers or cardiac magnetic resonance imaging (MRI) can evaluate the degree of fibrosis.
The two myocardial fibrosis blood markers are galectin-3 and soluble suppression of tumorigenicity-2, and these can be used for risk stratification and risk detection even without heart failure.
Cardiac resonance imaging can also detect and evaluate the degree of edema and other problems associated with heart failure (Liang).
The blood marker N-terminal pro–B-type natriuretic peptide (BNP) is commonly used to monitor heart failure. The concentration of plasma BNP increases with the severity of heart failure. Heart failure:
▪ is unlikely if plasma BNP levels are less than 100 picograms per milliliter.
▪ is more likely if plasma BNP levels are between 100 to 500 picograms per milliliter.
▪ or cardiac dysfunction is probable if plasma BNP levels are greater than 500 picograms per milliliter (Cao).
Meanwhile, heart failure is more likely in individuals:
▪ below 50 years of age with NT-proBNP levels greater than 450 picograms per milliliter
▪ between 50 and 75 years of age with NT-proBNP levels greater than 900 picograms per milliliter; and
▪ over 75 years of age with NT-proBNP levels greater than 1,800 picograms per milliliter.
The reduction of plasma BNP and NT-proBNP levels in heart failure predicts an improvement in clinical symptoms. A study of acute myocardial function patients found that BNP and NT-proBNP levels predicted sudden cardiac death and were the strongest predictors, even after adjusting for clinical variables, including ejection fraction. Plasma BNP and NT-proBNP can also be used as prognostic indicators to help clinicians adjust their therapy strategy, but they are still underused in managing heart failure.
The New York Heart Association Classification provides a simple way of classifying the extent of heart failure. It classifies those with the condition into one of four categories based on their limitations during ordinary (e.g., climbing stairs) and less-than-ordinary (e.g., walking short distances) physical activity, as well as varying degrees of shortness of breath and angina pain.
Class I
Class II
Class III
Class IV
No symptoms and no limitations in ordinary physical activity.
Mild symptoms (mild shortness of breath or angina) and slight limitation during ordinary activity.
Marked limitations in activity due to symptoms, even during less-than-ordinary activity. Comfortable only at rest.
Severe limitations. Experiences symptoms even while at rest. Mostly bed-bound individuals.
The conventional medical treatments for heart failure are based on the stage of the condition.
▪ Oxygen
▪ Water pills
▪ Vasodilator pills
Acute Decompensated Heart Failure
▪ Angiotensin-converting enzyme inhibitor drugs
▪ Muscle contraction enhancers
Chronic Heart Failure
▪ Hypertension control
▪ Water pills
▪ Angiotensin receptor blockers
▪ Aldosterone antagonists
▪ Angiotensin-converting enzyme inhibitor drugs
Advanced Heart Failure
▪ Heart transplant
▪ Left ventricular assist device implantation
The Potential of Pulsed Electromagnetic Fields (PEMF) for Slowing or Reversing Heart Failure
In chronic heart failure, angiotensin receptor blockers, angiotensin-converting enzyme inhibitor drugs, and aldosterone antagonists are considered the golden triangle of heart failure treatment.
If the severe symptomatic state is persistent in advanced heart failure with decreased cardiac function despite guideline-based medical therapy, considerations are given to advanced options such as heart transplant, implantation of a LVAD, or even initiation of end-of-life care.

The conventional treatments above focus primarily on the medical aspects of heart failure. There are non-conventional strategies that target the other pathophysiological aspects of the condition, but their application is rarely explored. Targeting these specific aspects can help improve function and extend the life of individuals with heart failure.
The hallmarks of heart failure, as discussed throughout this resource, can be addressed with multiple coordinated strategies such as:
▪ enhancing cardiomyocyte relaxation, endothelial metabolism, medication effectiveness, nutrient transport, and rehabilitation;
▪ improving afterload reduction and autophagy;
▪ increasing protection from atherogenesis, ATP production, circulation, glycosaminoglycans production, and oxygenation;
▪ reducing abnormal angiogenesis and collateral formation, growth factors, infection, and inflammation; and
▪ stimulating muscle and vascular repair.
When atherosclerotic plaque obstructs coronary blood vessel flow, the heart attempts to increase angiogenesis and collateral formation. These reactions may be valuable self-preservation strategies initiated by the heart, but they are a double-edged sword as they also enhance the development of hypertrophy. Reducing the other pathophysiologic aspects of heart failure may decrease the need for the heart tissue to make these vascular changes.
In terms of anti-fibrosis medication, there are no proven safe and effective options available yet, but herbal therapies may have some effectiveness in decreasing cardiac fibrosis (Li and Wang). The current best strategies are preventative, aside from the probable effectiveness of PEMFs described in a later chapter of this resource.
A key aspect of controlling inflammation is stimulating a ubiquitous molecule called adenosine, acting through its generalized receptor, the adenosine receptor. This molecule regulates the function of every tissue and organ in the body and is considered a guardian angel in human disease (Borea). Studies show that the release of adenosine can be enhanced with PEMF stimulation (Varani).
The concentrations of adenosine are naturally at physiological levels in body fluids between the cells of unstressed tissues. These concentrations increase rapidly in response to cell injury-causing stress conditions such as low oxygen, lack of blood supply, inflammation, or trauma. PEMFs stimulate the activation of adenosine receptors while also increasing their functionality and augmenting chemical agents that stimulate these receptors.

PEMFs influence A3 and A2A adenosine receptors, with the latter being the predominant receptor subtype responsible for coronary blood flow regulation. The stimulation of A2A adenosine receptors dilates coronary arteries in both an endothelial-dependent and endothelial-interdependent manner (Mustafa). Moreover, stimulating A2A and A3 adenosine receptors through PEMFs can help reduce inflammation as it lowers many pro-inflammatory tissue cytokines.
Pulsed electromagnetic field therapy has immunomodulatory effects of decreasing the production of pro-inflammatory cytokines while stabilizing or increasing the production of anti-inflammatory cytokines. This therapy also helps restore inflammatory cascades to homeostatic production levels (Ross).

PEMFs have been shown to reduce inflammation associated with obesity (Baranowska and Du).The visceral fat compartment is the greatest source of inflammation in obesity, so using PEMFs over the abdomen with sufficient intensity should aid in reducing inflammation.
It can also prevent the damaging consequences of the secondary inflammation caused by abdominal cytokines released throughout the body.

It would also be beneficial to apply PEMFs with sufficient intensity to the whole body to address the systemic effects of inflammation resulting from excess fat.
There is more on this topic at https://www.drpawluk.com/blog/overweight-obesity-and-pemfs.
Pulsed electromagnetic fields have been shown to cause numerous physiological reactions that address many of the known pathophysiologic aspects of heart failure (Pawluk). Therefore, PEMFs can be very useful as a sole therapy or as a complement to other approaches in treating heart failure, especially when controlling cardiac hypertrophic remodeling.
PEMF therapy should be started in the early stages of heart failure or when cardiac hypertrophy has already set in even before diagnosis. It can also be useful when the ejection fraction is already seen to decrease or before symptoms of heart failure remodeling become evident. If heart failure has already been diagnosed and medication has begun, PEMF therapy should make the medications even more effective and may allow the reduction of dosages, thus limiting side effects (Pawluk).
There is a significant need to increase the production of ATP and improve mitochondrial function in heart failure, and PEMFs can help meet this need. Studies have shown that using PEMFs for 20 minutes can stimulate ATP production by up to 600% (Zhang).
It is worth noting that since ATP is recycled constantly, frequent PEMF treatment to the heart may be necessary to maintain production and utilization. Moreover, it is still unknown how long and how much of the ATP produced through PEMF stimulation can last.
If significant benefits are seen in cardiovascular function with PEMF therapy, attention should be paid to how long those benefits last and how often the therapy should be repeated. It is possible that with higher-intensity PEMFs, treatment times could be reduced to 10 to 15 minutes, multiple times a day, depending on the response.
The heart constantly makes stem cells for health maintenance and the replacement and repair of cells, especially in the presence of ischemia. Pulsed electromagnetic fields have been found to increase neural stem cells (Goodwin). They have also been shown to increase other types of stem cells in the body (Maziarz and Poh). Moreover, studies indicate that extremely low-frequency PEMFs tuned by ion cyclotron resonance for the calcium ion can be used to drive cardiac-specific differentiation in adult cardiac progenitor cells without any pharmacological or genetic manipulation of the cells, increasing the lifespan of cardiomyocytes (Gaetani).
Disruption of the natural, coordinated tissue growth and angiogenesis in the heart contributes to the progression from adaptive cardiac hypertrophy to heart failure. Supplementation of angiogenic factors during progression from adaptive to maladaptive cardiac hypertrophy preserves cardiac function. Cardiac microvascular endothelial cells increase myocardial angiogenesis, and cardiac myocytes also play a crucial role in myocardial angiogenesis. Pulse-burst magnetic field stimulation could augment angiogenesis, with associated improvement in ventricular function and reduced infarct size, as found when studied in vitro in rats (Li). The PEMF promoted the proliferation and migration of cardiac microvascular endothelial cells and cardiac myocytes directly. The PEMF also had an effect on the intercellular communication between cardiac microvascular endothelial cells and cardiac myocytes.
These results show novel cardiac cell mechanisms for PEMF action, indicating potential application in treating ischemic myocardial disease and pathological cardiac hypertrophy. Thus, using PEMFs to promote angiogenesis in hypertrophic myocardium becomes a new therapeutic target of heart failure. Therefore, PEMFs may potentially improve pathological myocardial hypertrophy and ischemic myocardial disease.
As far as the development of cardiac fibrosis is concerned, PEMFs have been shown to decrease the development of fibrosis in orthopedics (Huegel). PEMFs have not been studied directly on cardiac fibrosis, but they can indirectly affect the development of cardiac fibrosis by decreasing the cardiac inflammation that leads to fibrosis.
Arrhythmias and atrial fibrillation are common in those with heart failure, either as a cause or consequence. Pulsed electromagnetic field therapy may help control or reduce the frequency and severity of these arrhythmias.
Low-frequency, high-intensity PEMF could suppress atrial fibrillation by mediating the natural autonomic nervous system of the heart. Left stellate ganglion autonomic neural activity can also affect ventricular arrhythmia, as studies have shown that left stellate ganglion hyperactivity appears to predispose to the development of ventricular arrhythmia. The effect of low-frequency, high-intensity PEMF stimulation has been studied in acute heart attack research. It has been shown to reduce both the neural activity of the left stellate ganglion and the incidence of ventricular arrhythmia (Wang). Therefore, this form of PEMF stimulation could be a novel non-invasive substitute for the existing implant device-based electrical stimulation or sympathectomy approaches conventionally used in treating arrhythmias. Other research has also shown that lower-intensity PEMFs applied directly to the heart in a dog model decrease the risk of episodes of atrial fibrillation (Scherlag).

The generalized functional capacity in heart failure can be severely limited and debilitating. It can be due to many factors not directly related to heart muscle function but because of peripheral muscle changes (Sbruzzi). These peripheral changes include decreased blood supply in the periphery, reduced capillary function, the transformation of slow-twitch type I to fast-twitch type II fibers, and changes in general metabolic and nutritional status that include reduced skeletal muscle size and muscle strength. These changes are predictors of exercise intolerance and the poor prognosis of the value of muscle training. If able to be accomplished, functionally useful muscle training has the potential benefit of increased maximum oxygen consumption, muscle mass, oxidative enzyme levels, endothelial function improvement, and better performance in functional tests.
Neuromuscular electrical stimulation (NMES) improves peak oxygen, walking distance, quality of life, muscle strength, endothelial function, and depressive symptoms in patients with heart failure.
Therefore, it could be important in cardiac rehabilitation for heart failure patients (Neto). However, NMES can be painful and uncomfortable. To provide adequate results, higher intensity levels of NMES are needed.
One study also found that NMES in individuals with heart failure produced only about one-quarter of the peak intensity muscle contraction compared to maximum voluntary muscle contraction (Sbruzzi).
While this may be useful in individuals with very weak local muscles and the inability to contract these muscles voluntarily, it would not be sufficient for whole-body rehabilitation.
In contrast, neuromuscular magnetic stimulation (NMMS) is much more tolerable, especially for larger and deeper muscular enhancement. Neuromuscular magnetic stimulation was studied in 40 healthy volunteers, 20 receiving active neuromuscular magnetic stimulation, and 20 controls (Yang).
The active group received 15 minutes of quadriceps NMMS at maximum tolerable intensity three times per week for five weeks. The maximum magnetic field output intensity was 3.1 T/s. Visible muscle contractions were seen in all participants. The tolerated NMMS intensity was about 45% of the maximum possible. Even so, the isometric maximum and average peak torque of the NMMS group increased significantly by 22% and 23%, respectively. The speed of straightening the knee after stimulation also improved between 20 and 27%. The control group had no changes in their peak torques.
This research indicates that the high-intensity PEMFs indicated for heart stimulation in those with heart failure would also be useful in peripheral muscular rehabilitation.

Heart failure is an increasingly common and lethal health condition for which there is no current cure. Conventional medical and procedural therapies have improved survival but, clearly, safe and effective innovative therapies are still needed. Continued research into the pathophysiologic mechanisms of heart failure has discovered numerous physiologic changes that are be amenable to more innovative broad-spectrum approaches such as PEMFs. Some of these cardiac changes include poor heart muscle contractions, reduced general heart muscle health, increased sympathetic activity in the body and related neuroendocrine reactions, reduced nitric oxide levels and sensitivity, ATP depletion, increased reactive oxygen species, elevated heart cell death rate, and an increased rate of autoimmune diseases.
The root causes for some of these changes, whether acting solely or together, include inflammation, fibrosis, cardiac hypertrophy, endothelial dysfunction, reduced ATP supply, tissue calcium imbalance, poor tissue metabolism, cardiac vascular changes, metabolic tissue stress, dysregulated intestinal function, muscle weakness, and hypoxia.
As it happens, an innovative physiologically broad-spectrum strategy that addresses many of these dysfunctions, both as a cause and a consequence of heart failure, is the use of PEMF therapy. Evidence is accumulating for the value of PEMF therapy in addressing many of the pathophysiologic changes in cardiac disease in general and heart failure in particular. Fortunately, there is increasing availability of the right PEMF devices. So research is desperately needed to determine the value of PEMF therapy as a complementary modality specific to the treatment of heart failure.

▪ Baranowska A, Skowron B, Gil K, et al.. Obesity related adipokines release in rat adipose derived stem cell cultures influenced by pulsed electromagnetic field. Folia Med Cracov. 2018;58(2):131–145.
▪ Barbier E, Dufy B, Veyret B. Stimulation of Ca2+ influx in rat pituitary cells under exposure to a 50 Hz magnetic field. Bioelectromagnetics. 1996;17(4):303-11.
▪ Cao Z, Jia Y, Zhu B. BNP and NT-proBNP as Diagnostic Biomarkers for Cardiac Dysfunction in Both Clinical and Forensic Medicine. Int J Mol Sci. 2019 Apr 12;20(8):1820.
▪ Du L, Fan H, Miao H, et al.. Extremely low frequency magnetic fields inhibit adipogenesis of human mesenchymal stem cells. Bioelectromagnetics. 2014 Oct;35(7):519–30.
▪ Dunn J, Grider MH. Physiology, Adenosine Triphosphate. 2021 Feb 27. In: StatPearls (Internet). Treasure Island (FL): StatPearls Publishing; 2021 Jan–.
▪ Gaetani R, Ledda M, Barile L, et al.. Differentiation of human adult cardiac stem cells exposed to extremely low-frequency electromagnetic fields. Cardiovasc Res. 2009 Jun 1;82(3):411-20.
▪ Gevaert AB, Shakeri H, Leloup AJ, et al. Endothelial Senescence Contributes to Heart Failure With Preserved Ejection Fraction in an Aging Mouse Model. Circ Heart Fail. 2017 Jun;10(6):e003806.
▪ Gomes Neto M, Oliveira FA, Reis HF, et al. Effects of Neuromuscular Electrical Stimulation on Physiologic and Functional Measurements in Patients With Heart Failure: a systematic review with meta-analysis. J Cardiopulm Rehabil Prev. 2016 May-Jun;36(3):157-66.
▪ Goodwin T and Dennis R. Physiological and molecular genetic effects of time-varying electromagnetic fields on human neuronal cells. NASA Johnson Space Center, Houston, TX, United States. NASA/TP-2003-212054.
▪ Harada T, Obokata M. Obesity-Related Heart Failure with Preserved Ejection Fraction: Pathophysiology, Diagnosis, and Potential Therapies. Heart Fail Clin. 2020 Jul;16(3):357-368.
▪ Huegel J, Chan PYW, Weiss SN, et al.. Pulsed electromagnetic field therapy alters early healing in a rat model of rotator cuff injury and repair: Potential mechanisms. J Orthop Res. 2021 Oct 17.
▪ Lee PM, Gerriets V. Nitrates. In: StatPearls (Internet). Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK545149/
▪ Li F, Yuan Y, Guo Y, et al. Pulsed magnetic field accelerate proliferation and migration of cardiac microvascular endothelial cells. Bioelectromagnetics. 2015 Jan;36(1):1-9.
▪ Li X, Li L, Lei W, et al.. Traditional Chinese medicine as a therapeutic option for cardiac fibrosis: Pharmacology and mechanisms. Biomed Pharmacother. 2021 Oct;142:111979.
▪ Liang K, Baritussio A, Palazzuoli A, et al. Cardiovascular Magnetic Resonance of Myocardial Fibrosis, Edema, and Infiltrates in Heart Failure. Heart Fail Clin. 2021 Jan;17(1):77-84.
▪ Liu T, Song D, Dong J, et al. Current Understanding of the Pathophysiology of Myocardial Fibrosis and Its Quantitative Assessment in Heart Failure. Front Physiol. 2017;8:238. Published 2017 Apr 24.
▪ Luxán G, Dimmeler S. The vasculature: a therapeutic target in heart failure? Cardiovasc Res. 2021 Feb 23:cvab047.
▪ Maziarz A, Kocan B, Bester M, et al. How electromagnetic fields can influence adult stem cells: positive and negative impacts. Stem Cell Res Ther. 2016 Apr 18;7(1):54.
▪ McKay JC, Prato FS, Thomas AW. A literature review: the effects of magnetic field exposure on blood flow and blood vessels in the microvasculature. Bioelectromagnetics. 2007 Feb;28(2):81-98.
▪ Mookadam F, Goel R, Alharthi MS, et al. cross-sectional observational study. Heart Views. 2010;11(3):103-108.
▪ Murphy SP, Kakkar R, McCarthy CP, et al. Inflammation in Heart Failure: JACC State-of-the-Art Review. J Am Coll Cardiol. 2020 Mar 24;75(11):1324-1340.
▪ Mustafa SJ, Morrison RR, Teng B, et al. Adenosine receptors and the heart: role in regulation of coronary blood flow and cardiac electrophysiology. Handb Exp Pharmacol. 2009;(193):161-188.
▪ Mustafa SJ, Morrison RR, Teng B, Pelleg A. Adenosine receptors and the heart: role in regulation of coronary blood flow and cardiac electrophysiology. Handb Exp Pharmacol. 2009;(193):161-188.
▪ Pawluk W, Layne CJ. Power Tools for Health: how magnetic fields PEMFs help you. Publ. Friesen Press. 2017.
The Potential of Pulsed Electromagnetic Fields (PEMF) for Slowing or Reversing Heart Failure
▪ Poh PSP, Seeliger C, Unger M, et al. Osteogenic Effect and Cell Signaling Activation of Extremely Low-Frequency Pulsed Electromagnetic Fields in Adipose-Derived Mesenchymal Stromal Cells. Stem Cells Int. 2018 Jul 12;2018:5402853.
▪ Redfield MM, Chen HH, Borlaug BA, et al. Effect of phosphodiesterase-5 inhibition on exercise capacity and clinical status in heart failure with preserved ejection fraction: a randomized clinical trial. JAMA 2013;309:1268–77.
▪ Ross CL, Zhou Y, McCall CE, et al. The Use of Pulsed Electromagnetic Field to Modulate Inflammation and Improve Tissue Regeneration: A Review. Bioelectricity. 2019 Dec 1;1(4):247-259.
▪ Sadeghzadeh F, Entezari AA, et al. Characterizing the Binding of Angiotensin Converting Enzyme I Inhibitory Peptide to Human Hemoglobin: Influence of Electromagnetic Fields. Protein Pept Lett. 2020;27(10):1007-1021.
▪ Sbruzzi G, Schaan BD, Pimentel GL, et al. Effects of low frequency functional electrical stimulation with 15 and 50 Hz on muscle strength in heart failure patients. Disabil Rehabil. 2011;33(6):486-93.
▪ Scherlag BJ, Yamanashi WS, Hou Y, et al. Magnetism and cardiac arrhythmias. Cardiol Rev. 2004 Mar-Apr;12(2):85-96.
▪ Sugiura A, Kitahara H, Iwahana T, et al. Association of heart failure duration with clinical prognosis in advanced heart failure. Clin Res Cardiol. 2020 Mar;109(3):350-357.
▪ Varani K, Vincenzi F, Ravani A, et al. Adenosine receptors as a biological pathway for the anti-inflammatory and beneficial effects of low frequency low energy pulsed electromagnetic fields. Mediators Inflamm (2017) 2017:2740963.
▪ Ventura-Clapier R, Garnier A, Veksler V, et al. Bioenergetics of the failing heart. Biochim Biophys Acta. 2011 Jul;1813(7):1360-72.
▪ Wang J, Li F, Zhou X, et al. Clinical observation of modified zhenwutang in treatment of chronic heart failure patients with yang deficiency syndrome, Chin. J. Exp. Tradit. Med. Formula (2018) 3–8.
▪ Wang S, Zhou X, Huang B, et al. Noninvasive low-frequency electromagnetic stimulation of the left stellate ganglion reduces myocardial infarction-induced ventricular arrhythmia. Sci Rep. 2016 Jul 29;6:30783.
▪ Watanabe E, Arakawa T, Uchiyama T, et al. High-sensitivity C-reactive protein is predictive of successful cardioversion for atrial fibrillation and maintenance of sinus rhythm after conversion. Int J Cardiol 2006;108:346–53.
▪ Yang SS, Jee S, Hwang SL, Sohn MK. Strengthening of Quadriceps by Neuromuscular Magnetic Stimulation in Healthy Subjects. PM R. 2017 Aug;9(8):767-773. Ts
▪ Zhang S, Clark M, Liu X, et al. The Effects of Bio-inspired Electromagnetic Fields on Healthy Enhancement with Case Studies. Emerging Science Journal 2019 Dec;3(6):369-381.
▪ Zhang Y, Li L, Liu X, et al. Examination of the Effect of a 50-Hz Electromagnetic Field at 500 μT on Parameters Related with the Cardiovascular System in Rats. Front Public Health. 2020 Apr 7;8:87.
▪ Zhou B, Tian R. Mitochondrial dysfunction in pathophysiology of heart failure. J Clin Invest. 2018 Aug 31;128(9):3716-3726.
▪ Zimmerman JJ, von Saint André-von Arnim A, McLaughlin J. Chapter 74 – Cellular Respiration, Editor(s): Bradley P. Fuhrman, Jerry J. Zimmerman. Pediatric Critical Care (Fourth Edition), Mosby, 2011, 1058-1072.
The Potential of Pulsed Electromagnetic Fields (PEMF) for Slowing or Reversing Heart Failure