Pulmonary function testing for social security disability
Metabolic measurements: indirect calorimetry
Summary
Case studies
Self-assessment questions
Entry-level
Advanced
Chapter 11: Pulmonary Function Testing Equipment
Volume-displacement spirometers
Flow-sensing spirometers
Peak flowmeters
Body plethysmographs
Breathing valves
Pulmonary gas analyzers
Blood gas analyzers, oximeters, and related devices
Computers for pulmonary function testing
Summary
Self-assessment questions
Entry-level
Advanced
Chapter 12: Quality Systems in the Pulmonary Function Laboratory
Quality manual
Quality system essentials
Path of workflow
Summary
Case studies
Self-assessment questions
Entry-level
Advanced
Chapter 13: Reference Values and Interpretation Strategies
Selecting and using reference values
Establishing what is abnormal
Pulmonary function testing interpretation, “bringing it all together”
Interpretation algorithm
Summary
Case studies
Self-assessment questions
Entry-level
Advanced
Appendix A: Answers to Self-Assessment Questions
Chapter 1, Indications for pulmonary function testing
Chapter 2, Spirometry
Chapter 3, Diffusing capacity tests
Chapter 4, Lung volumes, airway resistance, and gas distribution tests
Chapter 5, Ventilation and ventilatory control tests
Chapter 6, Blood gases and related tests
Chapter 7, Cardiopulmonary exercise testing and field tests
Chapter 8, Pediatric pulmonary function testing
Chapter 9, Bronchoprovocation challenge testing
Chapter 10, Specialized test regimens
Chapter 11, Pulmonary function testing equipment
Chapter 12, Quality systems in the pulmonary function laboratory
Chapter 13, Reference values and interpretation strategies
Glossary
Back Cover
Inside Front Cover
Symbols and Abbreviations Used in Pulmonary Function Testing*
General Symbols
P Pressure, blood or gas
V Gas volume
Gas volume per unit time, or flow
F Fractional concentration of gas
I Inspired
E Expired
A Alveolar
T Tidal
D Dead space
Q Blood volume Blood flow
C Content in blood
S Saturation
a Arterial
c Capillary
v Venous
Mixed venous
BTPS Body temperature and pressure saturated with water vapor
ATPS Ambient temperature and pressure saturated with water vapor
STPD 0°C, 760 mm Hg, dry
Lung Volumes
VC Vital capacity
IC Inspiratory capacity
IRV Inspiratory reserve volume
ERV Expiratory reserve volume
FRC Functional residual capacity
RV Residual volume
TLC Total lung capacity
RV/TLC (%) Residual volume to total lung capacity ratio expressed as a percentage
VTG Thoracic gas volume
VT Tidal volume
VA Alveolar volume
VD Dead space volume
VL Lung volume
Ventilation and Ventilatory Control
Expired volume per minute, minute volume (BTPS)
Alveolar ventilation per minute (BTPS)
Dead space ventilation per minute (BTPS)
fb, f Respiratory rate per minute, breathing frequency
VD/VT Dead space to tidal volume ratio
P100, P0.1 Pressure in the first 100 msec of an occluded breath, occlusion pressure
Spirometry
FVC Forced vital capacity with maximal expiratory effort
FIVC Forced inspiratory vital capacity with maximal inspiratory effort
FEVT Forced expiratory volume for a specific interval T
FEVT/FVC%, FEVT% Forced expiratory volume to forced vital capacity ratio expressed as a percentage
FEFx Forced expiratory flow related to some specific portion of the FVC, denoted as subscript X, referring to the volume of FVC already exhaled at the time of measurement
FEF25%–75% Forced expiratory flow during the middle half of the FVC (formerly the MMF)
FEF50%/FIF50% Forced expiratory flow to forced inspiratory flow at 50% of VC expressed as a ratio or a percentage
FET Forced expiratory time
PEF Peak expiratory flow
MEFV Maximal expiratory flow-volume curve
MIFV Maximal inspiratory flow-volume curve
PEFV Partial expiratory flow-volume curve
Forced expiratory flow related to the actual volume of the lungs denoted by subscript X, referring to the lung volume remaining when measurement is made
MVVX Maximal voluntary ventilation as the volume of air expired in a specified interval, denoted by subscript X (formerly MBC)
Pulmonary Mechanics
C Compliance, volume change per unit of pressure change
Cdyn Dynamic compliance, measured during breathing
* Where two symbols are given, both are commonly used
Copyright
3251 Riverport Lane
St. Louis, Missouri 63043
RUPPEL’S MANUAL OF PULMONARY FUNCTION TESTING, ELEVENTH EDITION
No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, or any information storage and retrieval system, without permission in writing from the publisher. Details on how to seek permission, further information about the Publisher’s permissions policies and our arrangements with organizations such as the Copyright Clearance Center and the Copyright Licensing Agency, can be found at our website: www.elsevier.com/permissions.
This book and the individual contributions contained in it are protected under copyright by the Publisher (other than as may be noted herein).
Notices
Knowledge and best practice in this field are constantly changing. As new research and experience broaden our understanding, changes in research methods, professional practices, or medical treatment may become necessary.
Practitioners and researchers must always rely on their own experience and knowledge in evaluating and using any information, methods, compounds, or experiments described herein. In using such information or methods they should be mindful of their own safety and the safety of others, including parties for whom they have a professional responsibility.
With respect to any drug or pharmaceutical products identified, readers are advised to check the most current information provided (i) on procedures featured or (ii) by the manufacturer of each product to be administered, to verify the recommended dose or formula, the method and duration of administration, and contraindications. It is the responsibility of practitioners, relying on their own experience and knowledge of their patients, to make diagnoses, to determine dosages and the best treatment for each individual patient, and to take all appropriate safety precautions.
To the fullest extent of the law, neither the Publisher nor the authors, contributors, or editors, assume any liability for any injury and/or damage to persons or property as a matter of products liability, negligence or otherwise, or from any use or operation of any methods, products, instructions, or ideas contained in the material herein.
Library of Congress Cataloging-in-Publication Data
Names: Mottram, Carl D.
Title: Ruppel’s manual of pulmonary function testing / Carl D. Mottram, RRT, RPFT, FAARC, Technical Director, Pulmonary Function Labs and Rehabilitation, Associate Professor of Medicine, Mayo Clinic College of Medicine, Rochester, Minnesota. Other titles: Manual of pulmonary function testing
Description: Eleventh edition. | Maryland Heights, Mo. : ELSEVIER, [2017]| Revision of: Manual of pulmonary function
testing / Gregg L. Ruppel. 10th ed. c2013. | Includes bibliographical references and index.
Identifiers: LCCN 2016048605 | ISBN 9780323356251 (pbk.)
Subjects: LCSH: Pulmonary function tests–Handbooks, manuals, etc.
LC record available at https://lccn.loc.gov/2016048605
Content Strategist: Yvonne Alexopoulos
Content Development Manager: Billie Sharp
Publishing Service Manager: Deepthi Unni
Project Manager: Andrea Lynn Villamero
Design Direction: Amy Buxton
Printed in the United States of America
Last digit is the print number: 9 8 7 6 5 4 3 2 1
Contributors/Reviewers
Contributors
Susan Blonshine, BS, RRT, RPFT, FAARC, AEC President/CEO, TechEd Consultants, Technical Director, Michigan State University Pulmonary Function, Laboratory Mason, Michigan
Katrina M. Hynes, MHA, RRT, RPFT Supervisor Pulmonary Function Laboratory, Mayo Clinic Rochester, Minnesota
David A. Kaminsky, MD Professor of Medicine, Pulmonary and Critical Care, University of Vermont, Attending Physician Medicine, Pulmonary, and Critical Care, Fletcher Allen Health Care, Burlington, Vermont Reviewers
Ellen A. Becker, PhD, RRT-NPS, RPFT, AE-C, FAARC Professor, Respiratory Care, Cardiopulmonary Sciences, Rush University, Chicago, Illinois
Sarah Gabua, DNP, RN, CNE Nursing and Allied Health Consultant, Adjunct Faculty, Nursing and Allied Health, School of Nursing, 2nd Act Consulting, LLC, Ferris State University, Las Vegas, Nevada, and Big Rapids, Michigan
Janet Czermak Russell, MA, MS, APN-BC Associate Professor of Nursing, Essex County College Newark, New Jersey
Foreword
This text began as a series of notes for respiratory therapy students who were interested in learning to perform pulmonary function tests. In the 1970s, a great deal of time was devoted not only to performing the physiologic measurements but also to manually measuring graphic recordings and calculating the results. Much has changed over the past 40 years in regard to performing pulmonary function studies. Most notably, microprocessors have supplanted the drudgery of measuring and calculating, so that the results of complicated tests are available almost as soon as the patient has completed the maneuver. While this permits the person conducting the test to concentrate on acceptability and repeatability, it may allow the tester to give minimal attention to the physiology responsible for the patient’s symptoms. With few exceptions, the physician treating the patient no longer performs the test but relies on a technologist to make the measurements that will determine a course of therapy or whether additional studies might be needed. Understanding respiratory physiology has taken a back seat to learning how to navigate sophisticated computer software.
Previous editions of the Manual have attempted to bridge the gap between making standardized physiologic measurements of lung function and interpreting the results of those tests to answer the clinical question being asked. This latest edition continues with that intent by updating the content and expanding the best practices as new techniques become available. The new material is directed at helping those interested in lung function testing learn not only how to do each test but also why a specific test is important. More than ever, this requires individuals who have a solid understanding of
respiratory physiology and the clinical skills to deal with symptomatic patients in the testing environment. Well-prepared technologists are more likely to avoid misclassification of disease states and to relate the results of pulmonary function tests to important patient outcomes. This edition of the Manual aspires to contribute to that preparation.
Carl D. Mottram, RRT, RPFT, FAARC, took responsibility as the author/editor beginning with the tenth edition. He has continued in this role to significantly expand and improve the eleventh edition. There is no one better qualified to continue improving the content and the format of the text. The Manual should continue to be a useful resource for students of lung function testing, whether they are therapists, technologists, or physicians.
Gregg L. Ruppel, MEd, RRT, RPFT, FAARC, Division of Pulmonary, Critical Care and Sleep Medicine, Saint Louis University School of Medicine, St Louis, Missouri
Preface
The primary functions of the lung are oxygenation of mixed venous blood and removal of carbon dioxide. Gas exchange depends on the integrity of the entire cardiopulmonary system, including airways, pulmonary blood vessels, alveoli, respiratory muscles, and respiratory control mechanisms. A few pulmonary function tests assess individual parts of the cardiopulmonary system. However, most lung function tests measure the status of the lungs’ components in an overlapping way.
This eleventh edition describes the most common pulmonary function tests, their techniques, and the pathophysiology that may be evaluated by each test. Topics covered include the following:
• Basic tests of lung function, including spirometry, lung volume measurements (i.e., body plethysmography, nitrogen washout and helium dilution), diffusing capacity, and blood gas analysis
• Ventilation and ventilatory control, cardiopulmonary exercise tests, and pediatric and infant pulmonary function testing
• Specialized test regimens that focus on exhaled nitric oxide measurements, forced oscillation techniques, metabolic studies, disability determination, and preoperative evaluation
• Bronchial challenge tests that assist the clinician in characterizing the hyperreactivity of the airways
• Pulmonary function testing equipment, quality assurance, and reference values and interpretation
Distinctive features
The eleventh edition includes many of the features from the
previous editions:
• Learning objectives for entry-level and advanced practitioners are again included at the beginning of each chapter.
• Each test section includes criteria for acceptability and repeatability, as well as interpretive strategies with criteria that are organized to help those who perform pulmonary function tests adhere to recognized standards.
• Most of the testing criteria are based on the American Thoracic Society (ATS) and European Respiratory Society (ERS) statements, with a few based on the clinical practice guidelines of the American Association for Respiratory Care.
• The interpretive strategies are presented as a series of questions that can be used as a starting point for test interpretation. In this edition, we included a flowchart process for systematically interpreting the basic lung function tests.
• Case Studies with real-life patient scenarios, questions, and discussion topics are included at the end of the chapters.
• How To boxes populate specific testing chapters. These are a stepby-step guide to performing function tests. When possible, we’ve provided illustrations. These procedures take the guesswork out of performing an accurate test.
• The Evolve Learning Resources feature updated Case Studies in PPT format so instructors can utilize them during class discussions. Clinical Scenario slides, organized by disease process, provide an in-depth case analysis with figures and charts noting lab values and treatment options. Instructors and student study groups can use these to supplement their own clinical experiences.
As in previous editions, each chapter includes self-assessment questions. The questions in this edition are divided into entry-level and advanced categories. The answers may be found in Appendix A. A selected bibliography at the end of each chapter is arranged according to topics within the chapter, including standards and guidelines.
Changes to this edition
The following changes to this edition reflect suggestions of the
users of previous editions, as well as new developments in pulmonary function testing.
• Updated references and American Thoracic Society and European Respiratory Society Standards. The test criteria are based largely on these standards/recommendations.
• Chapter 4 includes additional discussion on the multiple breath nitrogen washout tests and the lung clearance index.
• Chapter 7 reviews the new ATS-ERS standards for Field Testing. In this section we discuss the update of the 6-minute walk test and both the incremental and endurance shuttle walk tests. Chapter 12 incorporates the new Clinical and Laboratory Standards Institute’s quality management system model and its application in pulmonary diagnostic testing.
Using this book
This manual is intended to serve as a text for students of pulmonary function testing and as a reference for technologists and physicians. Because of the wide variety of methods and equipment used in pulmonary function evaluation, some tests are discussed in general terms. For this reason, readers are encouraged to use the selected bibliographies provided. The presentation of indications, pathophysiology, and clinical significance of various tests presumes a basic understanding of cardiopulmonary anatomy and physiology. Again, readers are urged to refer to the General References included in the selected bibliographies to refresh their background knowledge of lung function. The terminology used is that of the American College of Chest Physicians (ACCP)-ATS Joint Committee on Pulmonary Nomenclature. In some instances test names reflect common usage that does not follow the ACCP-ATS recommendations.
Evolve ancillaries
Evolve is an interactive learning environment designed to work in coordination with Ruppel’s Manual of Pulmonary Function Testing, eleventh edition. For the student, our Evolve Learning Resources include:
• Practice Tests to help students apply the knowledge learned within the text
• Conversion and Correction Factors
• Helpful Equations
• Reference Tables
• Sample Calculations
For the instructor, our Evolve Learning Resources include:
• PowerPoint presentations of Case Studies and Clinical Scenarios
• Test Bank containing approximately 600 questions
• Electronic image collection consisting of images from the textbook Instructors may use Evolve to provide an Internet-based course component that reinforces and expands the concepts presented in class. Evolve may be used to publish the class syllabus, outlines, and lecture notes; set up virtual office hours and e-mail communication; share important dates and information through the online class calendar; and encourage student participation through chat rooms and discussion boards. Evolve allows instructors to post examinations and manage their grade books online. For more information, visit http://evolve.elsevier.com or contact an Elsevier sales representative.
Acknowledgments
Carl D. Mottram, RRT, RPFT, FAARC
I would like to acknowledge a few key colleagues and friends who have contributed to my professional success. First, I had the honor of being educated and mentored by Drs. Fred Helmholtz and Robert (Bob) Hyatt, both of whom have passed since the tenth edition. Dr. Helmholtz, along with colleagues, assisted in the development of the G-suit during World War II and the nitrogen washout test for measuring lung volumes. After retirement he continued to have a significant impact on pulmonary medicine through a variety of professional activities, including spending a month teaching the respiratory therapy students basic pulmonary physiology. Dr. Helmholtz was also very active in the NBRC and AARC, championing the field of respiratory care.
Dr. Hyatt hired me into the pulmonary function laboratory. He was a soft-spoken, very intelligent man with a commanding presence when I first met him. He was the first to describe the flowvolume curve, a discovery that revolutionized the interpretation of spirometry and had a profound impact on patient care, yet he was very humble about this fact. I was told the story of a colleague describing his first encounter of meeting Dr. Hyatt. He queried, “So you invented the flow-volume curve?” Dr. Hyatt replied, “No, it was there. I just found it.”
Both these gentlemen were giants in the field of pulmonary diagnostic testing who shared their passion and knowledge about respiratory physiology with me during my early and mid-career development, and contemporary mentors Drs. Paul Scanlon, David Driscoll, Bruce Staats, and Ken Beck treated me as an equal and
helped me understand pulmonary physiology through their tutelage. Mr. Jeff Ward, Mayo Clinic’s former RT program director, started me on my professional journey with the mindset of inquiry and yearning for knowledge. Susan Blonshine, Gregg Ruppel, Jack Wanger, and I “grew up” together. We supported each other professionally as champions of quality pulmonary diagnostic testing. I continue to be honored that Gregg has entrusted me with the Manual and hopefully, I’ll be able to continue to enhance this classic text. I would like to thank contributors to this edition Susan Blonshine, Dr. David A. Kaminsky, and Katrina M. Hynes for their excellent subject contributions. I would also like to thank the 45 staff members of the Mayo Clinic Pulmonary Function Laboratories a laboratory of 24 procedure rooms that meet, yet more often exceed, the expectations of the 150 to 250 patients each day that walk through our doors. None of my professional or educational activities would be possible without their unsurpassed dedication to Mayo’s primary value “the needs of the patient come first.” Finally, I would like to acknowledge my family for their love and support.
CHAPTER 1
Indications for Pulmonary Function Testing
CHAPTER OUTLINE
Pulmonary Function Tests
Airway Function Tests
Lung Volume and Ventilation Tests
Diffusing Capacity Tests
Blood Gases and Gas Exchange Tests
Cardiopulmonary Exercise Tests
Metabolic Measurements
Indications for Pulmonary Function Testing
Spirometry
Lung Volumes
Diffusing Capacity
Blood Gases
Exercise Tests
Patterns of Impaired Pulmonary Function
Obstructive Airway Diseases
Restrictive Lung Disease
Diseases of the Chest Wall and Pleura
Neuromuscular Disorders
Congestive Heart Failure
Lung Transplantation
Preliminaries to Patient Testing
Before Patient Testing
Patient Preparation (Pre-Test Instructions)
Withholding Medications
Smoking Cessation
Other Patient Preparation Issues
Anthropometric Measurements
Physical Assessment
Pulmonary History
Test Performance and Sequence
Technologist-Driven Protocols
Patient Instruction
LEARNING OBJECTIVES
After studying the chapter and reviewing the figures, tables, and case studies, you should be able to do the following:
Entry-level
1. Categorize pulmonary function tests according to specific purposes.
2. List indications for spirometry, lung volumes, and diffusing capacity.
3. Identify at least one obstructive and one restrictive pulmonary disorder.
4. Relate pulmonary history to indications for performing pulmonary function tests.
Advanced
1. Identify three indications for exercise testing.
2. Name at least two diseases in which air trapping may occur.
3. Describe the use of a technologist-adapted protocol for pulmonary function studies.
KEY TERMS
β2 agonist body plethysmograph
bronchial challenge capnography
diffusing capacity (Dlco)
edema
forced vital capacity (FVC)
hypercapnia
hyperventilation
hypoventilation
maximal expiratory flow volume (MEFV)
maximal midexpiratory flow rate (MMFR)
maximal voluntary ventilation (MVV)
oximetry
pulse oximetry
resting energy expenditure (REE)
spirometry
vital capacity (VC)
The chapter provides an overview of pulmonary function testing. Common pulmonary function tests are introduced, and the indications for each test are discussed. Diseases that commonly require pulmonary function tests are described, and guidelines regarding patient preparation and assessment are presented.
Adequate patient preparation, physical assessment, and pulmonary history help the tests provide answers to clinical questions. The importance of patient instruction in obtaining valid data is discussed. These topics are developed more fully in subsequent chapters.
Pulmonary function tests
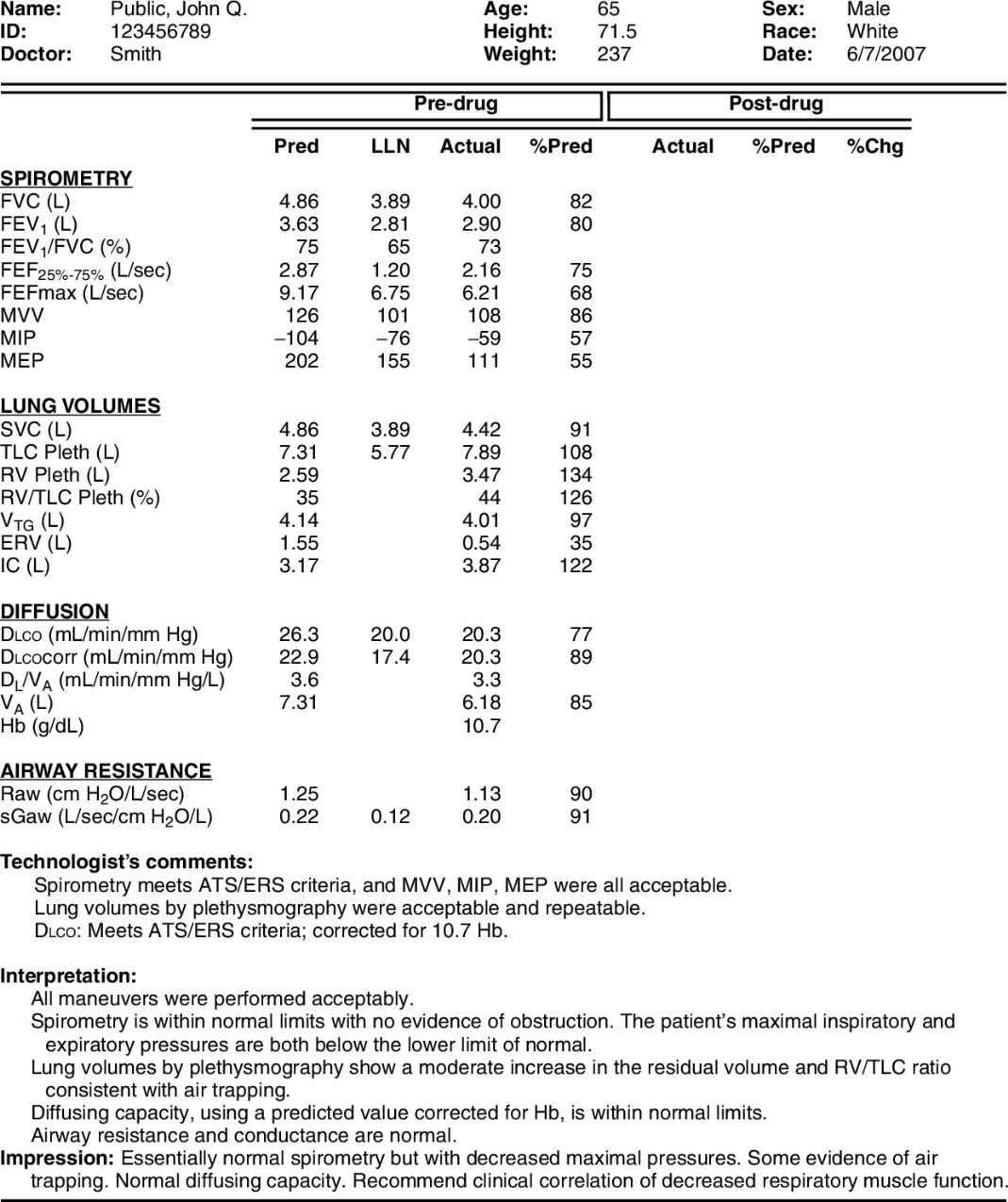
Many different tests are used to evaluate lung function. These tests can be divided into categories based on the aspect of lung function they measure (Box 1.1). Although the tests can be performed individually, they are often performed in combination. Fig. 1.1 shows a sample pulmonary function test report that includes spirometry, lung volumes, diffusing capacity, and airway resistance (Raw) measurements in a commonly used format. Determining which tests to do depends on the clinical question to be answered. This question may be explicit, such as “Does the patient have asthma?,” or less obvious, such as “Does this patient who needs thoracic surgery have any pulmonary diseases that might complicate the procedure?” In either case, indications for specific tests are useful (see Boxes 1.2 through 1.6).
Box 1.1
Categories of Pulmonary Function Tests
A. Airway function
1. Simple spirometry
a. VC, expiratory reserve volume (ERV), inspiratory capacity (IC)
2. Forced vital capacity maneuver
a. FVC, FEV1, FEF, PEF
(1) Prebronchodilator and postbronchodilator
(2) Pre-bronchochallenge and post-bronchochallenge
b. MEFV curves
(1) Prebronchodilator and postbronchodilator
(2) Pre-bronchochallenge and post-bronchochallenge
2. Total lung capacity (TLC), residual volume (RV), RV/TLC ratio
3. Minute ventilation, alveolar ventilation, and dead space
4. Distribution of ventilation
a. Multiple-breath N2
b. He equilibration
c. Single-breath techniques
C. Dlco tests
1. Single-breath (breath holding)
2. Steady state
3. Other techniques
D. Blood gases and gas exchange tests
1. Blood gas analysis and blood oximetry
a. Shunt studies
2. Pulse oximetry
3. Capnography
E. Cardiopulmonary exercise tests
1. Simple noninvasive tests
2. Tests with exhaled gas analyses
3. Tests with blood gas analyses
4. Tests with flow volume loops
5. Tests with direct laryngoscopy
F. Metabolic measurements
1. Resting energy expenditure (REE)
2. Substrate utilization
FIG. 1.1 Sample pulmonary function test report. Lung function tests are grouped by category in the left column. The post-drug columns are blank because the patient was not retested after the bronchodilator LLN, Lower limit of normal.
Airway Function Tests
The most basic test of pulmonary function is the measurement of
vital capacity (VC). This test simply measures the largest volume of air that can be moved into or out of the lungs. In the mid-1800s, a surgeon named Hutchinson developed a simple water-sealed spirometer that allowed measurement of what he named vital capacity, or “vital breath,” as he noted its relationship to survival. Hutchinson popularized the concept of using VC to assess lung function and named several other lung compartments that are still used today. He observed that VC was related to the standing height of the patient. He also developed tables to estimate the expected VC for a healthy patient. The VC was usually graphed on chart paper, which allowed subdivisions of the VC to be identified (see Chapter 2).
PF Tip 1.1
Pulmonary function data are usually grouped into categories (Fig. 1.1). The patient’s demographic data (age, height, gender, race, weight) are usually at the top of the report. The PFT data are presented in several columns. These columns show the predicted (expected) values, the lower limit of normal (LLN) or upper limit of normal (ULN), measured values obtained during testing, and the percent of predicted values for each test (actual/predicted × 100). Be sure to identify which column is actual and which is predicted.
Forced vital capacity (FVC) is an enhancement of the simple VC test. During the 1930s, Barach observed that patients with asthma or emphysema exhaled more slowly than healthy patients. He noted that airflow out of the lungs was important in detecting obstruction of the airways. Barach used a rotating chart drum (kymograph) to display VC changes as a spirogram. He even evaluated the effects of bronchodilator medications using the FVC traced as a spirogram.
In 1947, Tiffeneau described measuring the volume expired in the first second of a maximal exhalation in proportion to the maximal volume that could be inspired (FEV1/IVC [inspiratory vital capacity]) as an index of airflow obstruction (i.e., the Tiffeneau index). Around 1950, Gaensler began using a microswitch in conjunction with a water-sealed spirometer to time FVC. He observed that healthy patients consistently exhaled approximately