-Test-TakingAdvice
Bythispointinyourlife,youhaveprobablygainedmoretest—takingexpertisethan youcaretoadmit.Nevertheless,hereareafewtipstokeepinmindwhentakingthe exam:
Arrive30minutesearlyforyourtest.Youwanttoberelaxedandreadytostarton time,notrushedandstressedbytraffic.Bringsnacksanddressinlayerssothatyou willbecomfortableallday.
Avoidaheavylunch!Manytest—takershavereportedthatitcanbedifficulttofocus ontheexamafteraheavymeal.
Forlongvignettequestions,readthequestionstemandscantheoptions,andthen gobackandreadthecase.Youmaygetyouranswerwithouthavingtoreadthrough thewholecase.
'l‘here’snopenaltyforguessing,soyoushouldneverleaveaquestionblank.Ifyou aren’tsure,askyourself,WhatwouldIdoifthisclinicalsituationreallypresented itselftomeandlwasalonemanagingit?Yourgutinstinctisoftenright. Goodpacingiskey.Youneedtoleaveadequatetimetogettoallthequestions.Even thoughyouhave1minuteperquestiononaverage,youshouldaimforapaceof45 secondsperquestion.Ifyoudon’tknowtheanswerwithinashortperiodoftime, makeaneducatedguessandmoveon.Youcanflagthatquestiontocomebackto ifyouhavetimeattheend.
It’sokaytosecond-guessyourself.Researchshowsthatour“secondhunches"tend tobebetterthanourfirstguesses.
Don’tpanicover“impossible”questions.Thesemaybeexperimentalquestions thatwon’tcountinyourscore.Again,takeyourbestguessandmoveon. Notetheageandraceofthepatientineachclinicalscenario.Whenraceorethnicity isgiven,itisoftenrelevant.Knowthesewell,especiallyformorecommondiagnoses. Questionsoftendescribeclinicalfindingsinsteadofnamingeponyms(eg,theycite “ ,, “ ,, KEYFACT tender,erythematousbumps1nthepadsofthefingerratherthanOslernodes inafebrileadolescent). Never,everleaveaquestionblankIThereis
Asnotedabove,visitwww.theabfm.org/cert/exampreparationaspxforstudystrate— nopenaltyforguessing. giesspecifictotheABFMcertification/recertificationexam.
ITestingandLicensingAgencies
AmericanBoardofFamilyMedicine 1648McGrathianaParkway,Suite550 Lexington,KY40511 859-269-5626or888-995-5700
SupportCenter:877-223-7437 vvwwtheabfrnorg
EducationalCommissionforForeignMedicalGraduates(ECFMG) 3624MarketStreet,FourthFloor Philadelphia,PA19104—2685 215—386—5900
Fax:215—386—9196 www.ecfmg.org
FederationofStateMedicalBoards(FSMB) 400FullerWiserRoad Euless,TX76039
817-868-4000
Fax:817-868-4099 wwwfsmb.org
IPreventiveMedicine
1°prevention:Diseasepreventionmeasuressuchascounselingforat—riskbehaviors, immunizations,andchemopreventionthataretakenbeforethediseasedevelops.
2°prevention:Definedasearlydetectionandtreatmentofasymptomaticdisease, includingriskassessment.
3°prevention:Managementofchronicdiseasestopreventorminimizecomplications.
Characteristicsthatmakeadiseaseappropriateforscreeninginclude: Diseaseleadstosignificantmorbidityandmortality. Effectivetreatmentisavailable. Diseaseisdetectableintheasymptomaticperiod. Testingisaccurateandsimple. Treatmentadministeredduringtheasymptomaticperiodyieldsabetterout— comethantreatmentinthesymptomaticperiod.
Characteristicsofriskfactorsthatwouldbeappropriateforscreeningare: Highprevalenceoftheriskfactorinthepopulationtobescreened. Largeportionsofthosewiththeriskfactorareunidentified. Associateddiseaseshouldhaveahighincidenceinthepopulationtobe screened.
Diseaseshouldhaveseriousconsequences. Readilyavailabletreatmentthatcanmodifytheriskfactor. RiskmodificationshouldIdiseaseincidence.
ADULTIMMUNIZATIONS
Table2.1outlinescommonadultimmunizationsandtheirindications.Forinformationonimmunizationofpediatricpopulations,refertotheChildandAdolescent Medicinechapter.
CANCERSCREENING
ThefollowingguidelinesarebasedonrecommendationsfromtheUnitedStatesPreventiveServicesTaskForce(USPSTF)andtheAmericanAcademyofFamilyPhysicians(AAFP).TheUSPSTFdescribestheirstrengthsofrecommendationasgrades (Table2.2)thatcommunicateboththeimportanceoftherecommendationandhow itshouldbeincorporatedintopractice.Rememberthattheserecommendationsare updatedannually.
SkinCancer
Insufficientevidence(gradeI)forwhole—bodyskinexaminationbyaprimarycare clinicianorpatientskinself—examinationfortheearlydetectionofcutaneousmela— noma,basalcellcancer,orsquamouscellskincancerintheadultgeneralpopula— tion.
However,thereisgradeBevidencerecommendingcounselingchildrenadolescents andyoungadults(ages10—24)whohavefairskinaboutminimizingtheirexposure toultravioletradiationtoreduceriskforskincancer.
CervicalCancer
RoutinelyscreenforcervicalcancerwithaPapanicolaousmearallwomen21years ofagewhohavebeensexuallyactiveandhaveacervix(gradeAstronglyrecommended).
Repeatscreeningatleastevery3years,butthisintervalcanbelengthenedtoevery 5yearsinwomenaged30to65yearsiftheyarebeingscreenedwithacombination ofcytologyandHPVtesting.
TABLE2.1
RecommendedAdultImmunizationSchedule
VACCINE SCHEDULE
Td/Tdap
Givethecomplete1°seriesifthepatienthasnotbeenpreviouslyvaccinated(firstdose,Tdap;seconddose,Td4weekslater;
thirddose,Td6monthslater)
TdapcansubstituteforonlyoneofthethreeTddosesintheseries
Boosterdosesodshouldbegivenevery10yearsthereafter
Humanpapillomavirus
Varicella
Herpeszoster
Measles,mumps, rubella
Influenza
Pneumococcal (polysaccharide):
PPSV23(older)
PCV13(newer)
HepatitisA
HepatitisB
Meningococcal: 4—valentconjugate meningococcalB
DatafromtheCDC.
Vaccinategirlsandboysat11or12years(orasearlyas9years)withcatch—upvaccinationforyoungwomenandyoungmen between13and26years,andformenaged22—26yearsifimmunocompromised(includingHIV)andmenwhohavesexwith men(MSM)
lfthepatienthasahistoryofchickenpox,considerimmune;otherwise,vaccinatewithtwodosesgiven1—2monthsapart
Singledoserecommendedforadults260yearsregardlessofwhethertheyreportapriorepisodeofherpeszoster
lfthepatientwasbornbefore1957,considerimmune
lfthepatientwasbornafter1957,twodosesshouldbegivenatleast1monthapart
Forrubellaspecifically,ensurethatwomenofchildbearingpotentialhaveimmunity
Onedoseannuallyrecommendedforallpersonsaged26months,includingalladults
Givetoalladults265years:PCV13,thenPPSV2312monthslater
Adults19—64yearswithcomorbidconditions(chronicpulmonarydisordersexcludingasthma,CVD,DM,chronicliverorrenal disease):PPSV23vaccineonly,giveseconddose25yearslater
Adultswithaspleniaorimmunosuppression:Bothvaccines(PCV13first,thenPPSV238weekslater)
Vaccinateanypersonseekingprotectionorpeopleofthefollowingindications:MSM,chronicliverdisease,personstraveling orworkinginendemicareas
Twodoses6—12monthsapartorthreedosesat0,1,and6months
Vaccinateanypersonseekingprotectionorpeopleofthefollowingindications:personsathighriskforSTIs,healthcare personnel,end—stageliverdiseasepatients,HIV—infectedpatients,chronicliverdiseasepatients
Threedoses(0,1-2months,4-6months)
Givetoadultswithasplenia,first—yearcollegestudentsindormitories,militarypersonnel
1—3dosesdependingontypeofvaccineandindication;consideraseconddoseat5yearsforthosegivenpolysaccharide vaccine
Routinescreeningisnotrecommendedforwomen>65yearsofagewithahistory ofadequate9screeningandwhoareotherwisenotathighrisk.Theevidence isinsufficienttorecommendfororagainsttheroutineuseofnewtechnologiesor HPVtestingalonetoscreenforcervicalcancer.
OvarianCancer
Donotroutinelyscreenforovariancancerbyultrasound,measurementoftumor markers,orpelvicexamination.Althoughthespecificityforscreeningstrategiesis high,thepositivepredictivevalueislowbecauseofthelowprevalenceofovariancan— cerinthegeneralpopulation.Further,theinvasivenatureoftestingthatfollowsa C9screeningtestledtheUSPSTFtoconcludethatthepotentialrisksoutweighthe
potentialbenefits(gradeD,againstrecommendation).
BreastCancer
Breastself-examination:Generalconsensusamongexpertgroupsisnottorecommendbreastself-examination.
TABLE2.2. DefinitionofUSPSTF Grades
A—Stronglyrecommendsservice
B—Recommendsservice
C—Recommendsselectivelyoffering servicebasedonprofessional judgmentandpatientpreference
D—Recommendsagainstservice l—lnsufficientevidence
Mammography:
Womenaged50to74years:Screenforbreastcancerevery2yearswithmam— mography(gradeBrecommendation).
Women<50years:Individualizeyourdecisiontostartregular,biennial screeningmammographybasedonpatientcontext,includingthepatient’s valuesregardingspecificbenefitsandharms.(GradeCrecommendationto screenwomenaged40—49years.)
Women275years:Donotroutinelyscreenwithmammography.
Germlinepredisposition(BRCAIorBRCAZ):Althoughafamilyhistoryofbreast canceriscommoninwomenwhodevelopbreastcancer,only5%to6%ofallbreast cancersareassociatedwithgermline(inherited)geneticmutations.Themajority oftheseinvolvetwogenes,BRCA1andBRCA2.Affectedpatientswhomeetthe NationalComprehensiveCancerNetwork(NCCN)criteriaforBRCA1andBRCA2 screeninginclude:
Femalebreastcancerdiagnosed<50yearsold. 'l’riple—negativebreastcancerdiagnosed<60yearsold. Invasiveovarianorfallopiantubecanceror1°peritonealcancer.
Malebreastcancer.
AshkenaziJewishdescentwithbreast,ovarian,orpancreaticcancerdiagnosed atanyage.
Patientswithbreastcancer(anyage)whohavefirst—,second—,orthird—degree relativeswithbreastcancerdiagnosed<50yearsoldinoneormorerelatives; invasiveovarian,fallopiantube,orlOperitonealcancerinoneormorerela— tives;breast,prostate,orpancreaticcancerdiagnosedintwoormorerelatives. Womenwhotest(-9forBRCAIorBRCAZmutationsareatIriskforbothbreast andovariancancer.Suchwomenshouldbereferredforappropriatecounselingto consideroptionsforreducingriskandintensifiedsurveillance.
TheNCCNguidelinesrecommendthatBRCAcarriersbeofferedprophylacticbilat— eralmastectomy;however,thatdecisionismadebasedonpatientpreference.Also, bilateralsalpingo—oophorectomyshouldbeofferedtowomenwhohavecompleted childbearing.Inwomenwhooptnottohaveprophylacticbilateralmastectomy, annualmammogram(startingatage30years)andannualbreastMRI(startingat age25years)isrecommended.Additionally,selectiveestrogenreceptormodula— tors(tamoxifenorraloxifene)canbeusedtoItheriskofinvasivebreastcancerin high-riskwomenwhooptagainstsurgicaloptions.Inpostmenopausalwomen,an aromataseinhibitor(suchasanastrozole)mayalsobeused.
ProstateCancer
TheUSPSTFrecommendsinformed,individualizeddecision-makingaboutscreeningforprostatecancerinmenages55to69yearsbasedontheman’svaluesand preferences(gradeC).PSA-basedscreeningisnotrecommendedformen70years andolder(gradeD).Withearlydetectionofasymptomaticdisease,veryfew,ifany, patientshaveimprovedsurvivalandtherewillbemoreharmdonebyfalselyelevated PSAlevelsandthesubsequentadditionaltestingandtreatment.
ColonCancer
Screenadults50to75yearsofageforcoloncancerwithanannualfecaloccultblood test,sigmoidoscopyevery3to5years,orcolonoscopyevery10years(gradeArecommendation).Screeningadultsaged76to85yearsisagradeCrecommendation. ScreenearlierifthereisIriskforcolorectalcancer—eg,ifthepatienthasapersonal orstrongfamilyhistoryofcolorectalcancer,adenomatouspolyps,orafamilyhistory ofahereditarysyndrome(familialadenomatouspolyposis,hereditarynonpolyposis coloncancer).
Donotscreenforcolorectalcancerinadults>85yearsofage(gradeDrecommen— dation).
LungCancer
Therearecurrentlydifferingopinionsregardinglungcancerscreening.
USPSTFrecommends(gradeB)annualscreeningforlungcancerwithlow-dose CTinadultsages55to80witha30—packyearsmokinghistoryandcurrentlysmoke, orhavequitinthelast15years.Screeningshouldbestoppedwhenthatpatienthas ceasedsmokingfor15yearsordevelopsalife-limitingconditionorthewillingness tohavecurativelungsurgery.
AAFPfindsthatthereisinsufficientevidencetosupportthisrecommendation, citinghighnumberneededtoscreen,lackofreproducibilityoftheseresultsinall settings,andhighcost.
ADULTHEALTHMAINTENANCE
Tables2.3listsrecommendedclinicalpreventiveservicesfordifferentadultpopulationsbasedonthegradeAandBrecommendationsfromtheUSPSTFandtheAAFP. Male-andfemale-specificscreeningrecommendationsarediscussedbelow.Table2.4 listsclinicalpreventiveservicesforpregnantwoman.Seecancerscreeningandimmunizationrecommendationsabove.
TA8LE2.3. RecommendedClinicalPreventiveServicesforAllAdults
A30—year—oldwomanwhoisotherwise healthypresentstoyouforthefirsttime becauseshewantstobetestedforthe ”breastcancergene.”Sheisconcerned becauseher527yeareoldmotherwas diagnosedwithmetastaticbreastcancer at38yearsofage.Howwouldyouanswer thispatient?
218 Alcoholmisuse ScreenandcounselbehaviortoIalcoholmisuse Depression Screenalladults,includingpregnantandpostpartumwomen;implementscreeningwithadequatesystemsinplace toensureaccuratediagnosis,effectivetreatment,andappropriatefollow—up
HBV/HCV Screenadultsathighriskforinfection;one—timescreeningforHCVinfectiontoadultsbornbetween1945and1965 HIVinfection Screenadolescentsandadultsaged18-65years
ScreenforhighBP;obtainmeasurementsoutsideoftheclinicalsettingfordiagnosticconfirmationbeforestarting treatment
ReferpatientswithBMI230kg/m2forintensive,multicomponentbehavioralinterventions
Physicalinactivity/ unhealthydiet
OfferorreferadultswhoareoverweightorobeseandhaveadditionalCVDriskfactorstointensivebehavioral counselinginterventionstopromoteahealthfuldietandphysicalactivity;cliniciansmaychoosetoselectively counselpatientsaboutthebenefitsofahealthfuldietratherthanincorporatecounselingintothecareofalladults inthegeneralpopulation
CounselsexuallyactiveadolescentsandcounselalladultsatTriskforSTls
Askalladultsabouttobaccouse,advisethemtostopusingtobacco,andprovidebehavioralinterventionsandFDA— approvedpharmacotherapyforcessationtoadultswhousetobacco
ScreenforlatentTBinfectioninpopulationsatIrisk
Screenforabnormalbloodglucoseaspartofcardiovascularriskassessmentinthosewhoareoverweightor obese;cliniciansshouldofferorreferpatientswithabnormalbloodglucosetointensivebehavioralcounseling interventionstopromoteahealthfuldietandphysicalactivity
AdultswithoutahistoryofCVD(ie,symptomaticCADorischemicstroke)usealow—tomoderate—dosestatinforthe preventionofCVDeventsandmortalitywhenthefollowingcriteriaaremet:
Theyareaged40—75years
TheyhaveoneormoreCVDriskfactors(ie,dyslipidemia,diabetes,hypertension,orsmoking)
Theyhaveacalculated10—yearriskofacardiovasculareventof10%orgreater
Identificationofdyslipidemiaandcalculationof10—yearCVDeventriskrequiresuniversallipidsscreeninginadults aged40—75years
Low—doseaspirinisrecommendedforadultswith210%10—yearCVDriskwhoarenotatIriskforbleeding,havea lifeexpectancyofatleast10years,andarewillingtotakelow—doseaspirindailyforatleast10years
ExerciseorphysicaltherapyandvitaminDsupplementationincommunity—dwellingadultswhoareatTriskforfalls
Youadviseherthatsheislikelyacandidate forBRCAI/BRCAZmutationtesting,given thatshehasafirstrdegreerelativewith premenopausalbreastcancer,andreferher forgenetictesting
ScreeninginMen
AbdominalAorticAneurysm:Offerone-timescreeningbyultrasonographyformen 65to75yearsofagewhohaveeversmoked.
ScreeninginWomen
Chlamydiaandgonorrhea:Screensexuallyactivewomenage24yearsandyounger andolderwomenwhoareatTriskforinfection.
Intimatepartnerviolence:Screenwomenofchildbearingageforintimatepartner violence(gradeB).Therewasinsufficientdatatorecommendfororagainstscreeningotherpopulations(gradeI).SeetheDomesticViolencesectionbelowformore information.
Osteoporosis:Screeninwomenaged265yearsandinyoungerwomenwhosefractureriskis2thatofa65-year-oldwhitewomanwhohasnoadditionalriskfactors. TheFRAX(FractureRiskAssessment)toolcanbeusedtoestimate10-yearrisksfor fracturesforallracialandethnicgroupsintheUnitedStates.
ScreeningforSTI
Chlamydiaandgonorrhea:Screensexuallyactivewomen£24yearsandolder womenwhoareatTriskforinfection.
TheUSPSTFrecommendsthatallpregnantwomenbescreenedforhepatitisB, HIV,andsyphilis.
TABLE2.4. RecommendedClinicalPreventiveServicesforPregnantWomen
CONDITION RECOMMENDATION
Bacteriuria, Screenwithurinecultureat12-16weeks’gestationoratthefirstprenatalvisit asymptomatic
Breastfeeding
Depression
GestationalDM
HBVinfection
HIVinfection
Neuraltube defects
Preeclampsia
Rh(D) incompatibility
Syphilis
Tobaccouse
Provideinterventionsduringpregnancyandafterbirthtopromoteand supportbreastfeeding
Screenpregnantandpostpartumwomen,implementscreeningwithadequate systemsinplacetoensureaccuratediagnosis,effectivetreatment,and appropriatefollow—up
Screenasymptomaticpregnantwomenafter24weeksofgestation
Screenatthefirstprenatalvisit
Screenallpregnantwomen,includingthosewhopresentinlaborwhoseHIV statusisunknown
Allwomenplanningorcapableofpregnancyshouldtakeadailysupplement containing0.4—0.8mg(400—800pg)offolicacid
Low—doseaspirin(81mg/d)aspreventivemedicationafter12weeksof gestationinwomenwhoareathighriskforpreeclampsia
OrderRh(D)bloodtypingandantibodytestingatthefirstprenatalvisit;repeat antibodytestingforallRh(D)—negativewomenat24—28weeks’gestation
Screenallpregnantwomen
Providesmokingcessationbehavioralinterventionsforallpregnantsmokers
MSM:TheCDCrecommendsscreeningforHBsAg,syphilis(annually),gonorrhea, chlamydia,andHIV.HepatitisCscreeningshouldbedonewhenotherriskfactors arepresent.AnalPapanicolaoutestingisavailable,butevidenceandguidelinesfor itsuseareinconsistent.
AdditionalscreeningforSTIsuchasHIVandsyphilisarerecommendedforallmen andwomen(regardlessofsexualorientation)engaginginhigh-risksexualbehavior. Athoroughsexualhistorytoassesspatientsexualbehaviorisimportant.When determiningpatientsatriskforSTIs,alsoconsiderdemographicsofthepopulation served(eg,ifthereisahighcommunityprevalenceofsyphilis).
PREVENTIONOFDENTALCARIESINPRESCHOOLERS
Atotalof19%ofchildren2to5yearsofageand52%ofchildren5to9yearsofageexperiencedentalcaries.Ethnicminorityandeconomicallydisadvantagedchildrenare atTrisk.Despiterecommendations,fewpreschool-agedchildrenevervisitadentist.
Guidelinesforthedentalcareofpreschoolchildrenareasfollows: Prescribecurrentlyrecommendeddosesoforalfluoridesupplementationto preschoolchildren>6monthsofagewhose1°watersourceisfluoridedeficient (USPSTFgradeBrecommendation).
Youmayusetopicalfluoridevarnishes,whichareeasiertouse,acceptedwidely bypatients,andhaveIpotentialfortoxicity,asadjunctstooralsupplementation. Thesecanbeappliedevery3to6monthsfromthetimeoffirsttootheruptionuntil theageofS(USPSTFgradeBrecommendation).
Monitorfordentalfluorosis,amildadverseeffectoffluoridesupplementationpri— marilyofcosmeticsignificance.
ENDOCARDITISPROPHYLAXIS
Offerantimicrobialprophylaxisfordentalandotherprocedurestopatientswithcar— diacconditionswiththehighestriskofadverseoutcomefrominfectiveendocarditis.
Endocarditisprophylaxisisrecommendedforthefollowingcardiacconditions: Cardiacvalvulopathyinacardiactransplantrecipient.
Congenitalheartdefectcompletelyrepairedwithintheprevious6monthswith prostheticmaterialordevice,whetherplacedbysurgeryorbycatheter.
Repairedcongenitalheartdiseasewithresidualdefectsatthesiteoradjacentto thesiteofaprostheticpatchordevice.
Unrepairedcyanoticcongenitalheartdisease,includingpalliativeshuntsandconduits.
Previoushistoryofinfectiveendocarditis. Prostheticheartvalves.
Donotofferantimicrobialprophylaxistopatientswithanyotherformofcongenital oracquiredheartdiseasesuchasbicuspidaorticvalve,acquiredaorticormitralvalve disease(includingmitralvalveprolapsewithregurgitation),orhypertrophiccardio— myopathy.
Offerantimicrobialprophylaxistopatientswiththecardiaclesionscitedabovewhen theyundergoprocedures,suchasthefollowing,likelytoresultinbacteremiawitha microorganismthathasthepotentialtocauseendocarditis: Alldentalproceduresthatinvolvemanipulationofgingivaltissueortheperiapical regionofteethorthatperforatetheoralmucosa.
Proceduresoftherespiratorytractthatinvolveincisionorbiopsyoftherespiratory mucosa.
ProceduresinpatientswithongoingGIorGUtractinfection. Proceduresoninfectedskin,skinstructure,ormusculoskeletaltissue.
A45—year—oldmalenonsmokerpresents foraroutineannualphysicalexam,Heis generallyheaIthyandofanormalweight withnocurrentmedicalcomplaints,He exercisesbyjogging30minutestwotimes aweek,onaverage.Hisfamilyhistory includeshighbloodpressure(BP)andan olderbrotherwithMIatage48years,He isworriedthatthismighthappentohim, Whatpreventiveservicescanyouofferthis patient?
' KEYFACT
Threeyearsaftersmokingcessation, theriskofrecurrentMi~Ltothatofa nonsmoker.
[~—
The”5A’s”approachtotobacco cessationadvocatedbythe NationalCancerInstitute:
IAskaboutsmokinghabits
lAdviseallsmokerstoquit
IAssesspatient’sreadinesstoquit
IAssistwithnonpharmacologic measuressuchascounselingand pharmacotherapy(asappropriate)
IArrangefollow—upandsupport
SMOKINGCESSATION
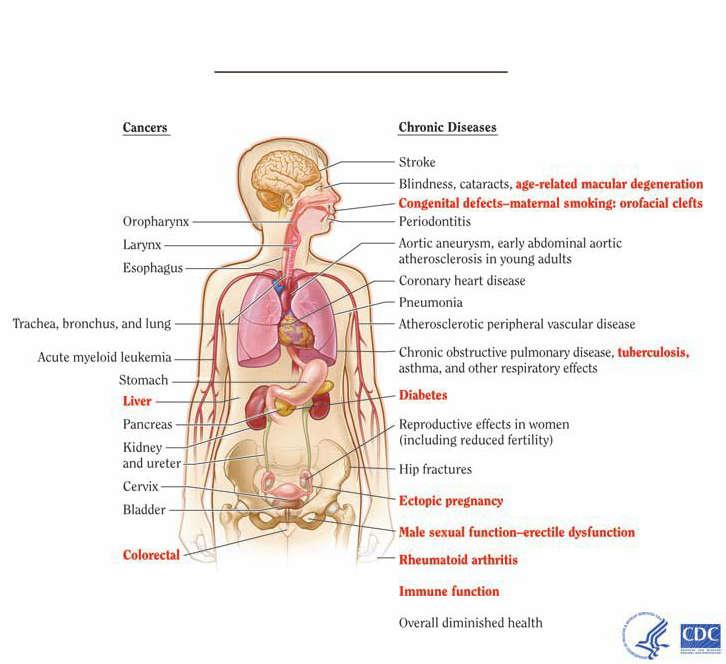
PrevalenceofcigarettesmokingamongadultsintheUnitedStateswasestimatedby theCDCtobe17%in2014.Smokingcausesasmanyas480,000deaths/yearandis themostcommonpreventablecauseofdeath(Figure2.1).
Smokingcessationisknowntoconferthefollowinghealthbenefits: MI:J,mortalityrisk.Theriskofrecurrentcoronaryeventsisprogressively\Ltonear thatofanonsmokerby3yearsafterquitting.
Stroke:AssociatedwithaJ,riskovertime.
Pulmonarydisease:SlowedprogressioninthedeclineofFEV1inpatientswith COPD.Alsoassociatedwithalriskofpulmonaryinfectionssuchasbacterial pneumoniaandTB.
Malignancy:1/riskoflung,kidney,bladder,stomach,andcervicalcancers,among others.
PUD:1/riskofdevelopingPUD;acceleratedrateofhealing.
Osteoporosis:lriskofbonelossandfracture(begins10yearsafterquitting).
CessationMethods
Evaluatethepatient’scigaretteuse,assesshisorherinterestinquitting,andfind outaboutpreviousattemptsatquitting
Oncethepatientisready,offerstrategiessuchassettinga“quitday"andhelpdefine alternativeoralbehaviorstosubstituteforthecigarette(eg,gum,throatlozenges). Manybehavioralmethodshavebeenadvocatedtoencouragepatientstoworktoward quitting.Discussandagreeuponmethodsforcessation(Table2.5)inadvanceof thequitday.
RisksfromSmoking
Smokingcandamageeverypartofyourbody
9mm; .Qhr-zniskigsiée
3!mice
Blindness,cataracts.age-relatedmaculnrdegenemtinn __—'Congenitaldefects—maternalsmoking:orofacial:Icfls l'eriodonlilis (Irupharynx J
larynx
Esophagus
InadditiontocheckingBPaspartofhis physicalexam,youorderalipidpanel anddiscussthebenefitsofahealthydiet.
Evidenceisinsufficientforrecommending low—doseaspirintopreventCVDinadults <50years.
‘ Aorticaneurysm.varlyabdominalaortic f atherosclerosisinyoungadults T 22,“ Coronaryheartdisease
' ‘7\‘ r7Pneumonia
“trachea.bronchus,andlung l :3“l" Alhernsclcmlicperipheralvasculardisease ,4 r. I “ Chronicobstruclivupulmonarydisease.lubcrculosls.
Acutenn‘clnitlleukemia asthma.andnthurrespiratoryenacts
Stomach 1‘ "- d p Liver /I z), A ntlheten
Pancreas "IIf! 2' Reproductiveeffectsinwomen [includingreducedfertility)
Kidney f é I 'i ll andureter‘ H ,1.- l
Cervix“.7 R q I).
Hipfractures
Eclupicpregnancy
Bladder “m}(‘«9i4:“/ Malesexualfunctionwmctiledysfunction
Colorectal
Rheumatoidafihn’tis
lmmunefunction
(Iveralldimil‘iis‘hedhwllh I. " a
TABLE2.5.
MethodsforSmokingCessation
METHOD DESCRIPTION
EFFICACY
Groupcounseling Lectures,groups,exercises,strategies Associatedwitha20%1—yearquit rate
Nicotine Suppresseswithdrawalsymptoms: Whenusedwithabehavioral replacement depressedmood,insomnia, program,gumandpatchmethods (gum,patch,nasal irritability,restlessness,weightgain doublethequitrate spray,inhaler)
Bupropion Enhancescentralnoradrenergic Greaterefficacythannicotine anddopaminergicfunctionwhen replacement administeredatadosageof150mg
Bupropionusedtogetherwith twicedaily nicotinepatcheshasbeenshown tohave>50%efficacy
Varenicline Partialagonistofthenicotinic
Aseffectiveasormoreeffectivethan acetylcholinereceptor bupropion Casereportsofsuicidalthoughtsand aggressiveanderraticbehavior havebeenreported
Hypnosis, Noevidencetosupporttheefficacy acupuncture,and oftheseprocedures electriccigarettes
IObesity
IntheUnitedStates,theprevalenceofobesityisnowabout34%inadultsand17%in children.Screenalladultpatientsforobesityandofferintensivecounselingandbehavioralinterventionstopromotesustainedweightlossinobeseadultsandchildren andpreventmorbidityandmortalityassociatedwithobesity,including: Triskofbothcardiovascularandoverallmortality.Inaddition,thereareclear associationsbetweenobesityandTmorbidity
Triskofcardiovasculardisease,hypertension,stroke,type2DMandinsulinresistance,dyslipidemia,cancer(includingcancersofthecolon,kidney,andgallbladder),sleepapnea,gallbladderdisease,GERD,andkneeosteoarthritis. I,qualityoflife,includingImobilityandsocialstigmatization.
Diagnosis
OverweightandobesityarediagnosedbasedonthecalculationofBMI(kg/m2): BMI:weight(kg)/heightZ(m2)
SeeTable2.6forthecategoriesofBMI.
Management
Considerthefollowingmodalitiesinthetreatmentofobesity: Dietandexercisecounselingwithbehavioralstrategiestohelppatientschange eatingpatternsandbecomephysicallyactive.Thismayleadtosmall/moderate degreesofweightloss(1-6kg)typicallysustainedforatleast1year.
A32—year—old5—ft,4—in,203—lbwoman presentsforherannualphysicalexam.She wouldliketolosesomeweightandasks aboutuseofguargumforweightloss. Whatisthenextstepinthemanagement ofthispatient?
A47ryearroldhomelessmanpresentsto yourclinictoestablishcare,Hisknown medicalconditionsincludediabetes, hypertension,andarecently63purified proteinderivative(PPD),forwhichheiscur rentlytakingisoniazid(INH).Hecomplains ofsomecough,diarrhea,andtinglingin hisfeet.Onexam,hisBPisl56/97mmHg, andyounotethathesmellsofalcohol.He haspaleconjunctivae,aredtongue,and fissuresatthecornersofhismouth.Healso appearstohavesomelossofsensationto lighttouchinhisfeetbilaterally.Howdo youproceed? '
KEYFACT
ABMI230isassociatedwithTriskofboth deathfromCVDandoverallmortality Intentionalweightlossof25lbhasbeen associatedwithaIinCVD,cancer,and overallmortality.
TABLE2.6. BMICategoriesfor OverweightandObesity
Overweight 25—29
Obese 30—39
Morbidlyobese 40—49
Super—obese 50—59
CalculateBMI,whichforthispatientis 35kg/mZ,andofferreferralforintensive, multicomponentbehavioralinterventions, asperUSPSTFandAAFPrecommenda tionsforpatientswithBMI230kg/mz.You explainthatguargumhasnotbeenshown tobeeffectiveforweightlossandrecom— mendadietandexerciseregimen.
Medication(Table2.7):MaybeconsideredforpatientswithBMI>30whendiet andexerciseattemptshavefailedand/orwhenthepatienthascomorbidities.Weight lossresultingfrommedication: Ismodest(average3—5kg),anddiscontinuationofmedicationsmayleadto rapidweightgain.
Willonlybesignificantwhencombinedwithlifestylechanges Isconsideredsuccessfulwhena5%to10%reductionininitialweight.Ifthat amountofweightlossisnotachievedwithaparticularagent,themedication shouldbediscontinuedtoavoidadverseeffects.
Surgery:
Youcheckhematocrit,peripheralblood smear,and8,2andfolatelevelsAlso considercheckinganl-lk,ashisloss ofsensationcouldbecausedbydiabetic neuropathy.Hisalcoholuseshouldbe addressedaswellincludingtheriskof thiaminedeficiency.
' KEYFACT
Medicationsforthetreatmentofobesity allowforsustainedweightlossonlyifthey areusedincombinationwithlifestyle changes.
Considerpatientsforgastricbypassandverticalbandedgastroplastyifthey haveaBMI>40orBMI>35withcomorbidities,havefailedtorespondtopre— viousnonsurgicalweightlossattempts,andarewellinformedandmotivated. Discusswiththempostoperativecomplications,whichmayincludeamortal— ityrateof0.2%,woundinfection,re—operation,vitamindeficiency,diarrhea, andhemorrhage.
Referforbariatricsurgerytohigh—volumecenterswithexperiencedsurgeons. Preparepatientsandofferappropriatesupport,includingpsychological screeningandadietandexerciseprogram,forsuccessfulsurgicalweightloss. PatientswhoundergoRoux—en—Ygastricbypasswillrequirelifelongvitamin supplementation(multivitamin,B127iron,zinc,magnesium)andyearly screeninglabsfornutritionaldeficiencies.
Nutrition
MALNUTRITION
Table2.8outlinestheclinicalmanifestationsandtreatmentofseveremalnutrition.
TABLE2.7. MedicationsUsedtoTreatObesity
Sympathomimeticdrugs
Phentermineanddiethylpropion Stimulatessympatheticnervous CanIBP,contraindicatedinCAD,HTN system Useupto12weeksonly(scheduleIVdrugswithabusepotential)
Drugsthatalterfatdigestion
Orlistat Inhibitspancreaticlipase Canbeusedonalong—termbasis,averagelossof8%initialweight
Antidepressants Sideeffectsincludeabdominalcramps,flatus,andoilyspotting
Fluoxetine Actsasanappetitesuppressant NotFDAapprovedforweightloss;mustuse260mg/day
Bupropion Actsasanorepinephrinemodulator NotFDAapprovedforweightloss
Antiepilepticdrugs
Topiramate Alsoapprovedfortreatmentof NotFDAapprovedforweightlossasasingleagent;availablein migraine combinationtreatmentwithphentermine
Zonisamide Hasserotonergicanddopaminergic NotFDAapprovedforweightloss activity
TABLE2.8. PresentationandTreatmentofSevereMalnutrition
MARASMUS KWASHIORKOR
Definition
Totalcaloriemalnutrition Proteinmalnutrition
Etiologies COPD,HF,cancer,AIDS Trauma,burns,sepsis
(indevelopedcountries)
Symptoms/Exam
Weightloss/wasting
Treatment Correctfluidandelectrolyte
Normalweight;edema,ascites
Treatmentisthesameasthatfor abnormalities;treatinfections; marasmus givevitaminsandminerals Startwithigprotein/kgand30
Complications kcal/kg,preferablyenterically
Immunosuppression,poor woundhealing,impaired growthanddevelopment,
Sameasthoseformarasmus muscleatrophyleadingtoorgan dysfunction
KEYFACT
Thinkaboutfat—solublevitamindeficiencies inpatientswithanysortofintestinal malabsorption(IBD,CF).
Ifneurologicdeficitsarepresent,think
vitaminB,2deficiency.Immediate treatmentisnecessarytoprevent irreversibleperipheralneuropathy,balance problems,dementia.
VITAMINDEFICIENCIES
Vitamindeficienciesmaybemorecommonindevelopedcountriesthanisgenerally believed.Vitaminsareneededforbasicmetabolism,butsincemostofthemcannot besynthesized,theymustbepresentinourdiets.Thepresentationandtreatmentof fat—andwater-solublevitamindeficienciesaresummarizedinTables2.9and2.10.
TABLE2.9. PresentationandTreatmentofFat-SolubleVitaminDeficiencies
VITAMIN ETIOLOGY
SYMPTOMS/EXAM
TREATMENT
A(retinol) Foundinurbanpoor,elderlypatients,and Nightblindness,xerosis,Bitotspots(white High-dosevitaminA thosewithfatmalabsorptionsyndrome patchesontheconjunctivae)leading tokeratomalacia,endophthalmitis,and blindness
D Foundinelderlypatients,thosewith Children:Rickets(restlessness, High-doseoralvitaminD insufficientsunexposureormalnutrition/ craniotabes,costochondralbeading, malabsorption,breastfeedinginfants,and bowlegs,kyphoscoliosis) anticonvulsantusers Adults:Osteomalacia
E Associatedwithseveremalabsorption Areflexia,peripheralneuropathy, OralvitaminE gaitabnormality,ophthalmoplegia, Iproprioception
K Poordiet,malabsorption,antibiotics Clottingfactordeficiencies(II,VII,IX,X) VitaminKSQ
TABLE2.10. PresentationandTreatmentofWater-SolubleVitaminDeficiencies
VITAMIN ETIOLOGY
B1(thiamine) Themostcommoncauseisalcoholism
B2(riboflavin) Usuallyoccurswithotherdeficiencies
SYMPTOMS/EXAM TREATMENT
Anorexia,musclecramps,paresthesias‘ Oralthiamine Dryberiberileadingtoneuropathy andWernicke—Korsakoffsyndrome;wet beriberileadingtohigh—outputheart failure
Nonspecificsymptoms(eg,mouth OralvitaminB2 soreness,glossitis,cheilosis,weakness, irritability)plusseborrheicdermatitis andanemia
33(niacin) Associatedwithalcoholism
Nonspecificsymptoms(seeabove); Oralnicotinamide pellagra(Figure2.2)(dermatitis, diarrhea,dementia)
B6(pyridoxine) Associatedwithmedicationinteractions Nonspecificsymptoms(seeabove); Oralorintramuscularvitamin36 (INH,OCPs)orwithalcoholism;fat peripheralneuropathy,anemia,and malabsorptionsyndromesmay seizures contribute Levelscanbemeasured(normal>50 ng/mL)
B12 Foundinvegans,gastrectomypatients, Megaloblasticanemia,glossitis, VitaminB,2administered (cyanocobalamin) gastricbypasspatients,andthosewith anorexia,diarrhea intramuscularly perniciousanemia Peripheralneuropathy,balance problems,dementia(reversibleif treatedwithin6months)
C(ascorbicacid) Foundinurbanpoor,elderly,alcoholics, Scurvy:Poorwoundhealing,easy
OralvitaminC cancerpatients,smokers,andthosein bruising,bleedinggums,subperiosteal renalfailure hemorrhage,andanemialeading toedema,oliguria,neuropathy,and intracerebralhemorrhage
Biotin Causedbyeatinglargequantitiesof Myalgias,dysesthesias,anorexia,and Oralbiotin raweggs nausealeadingtodermatitisand alopecia
Folicacid
Causedbyinadequatedietaryintake
Megaloblasticanemia,neuraltube
Oralfolicacid defects
NUTRITIONALANDHERBALSUPPLEMENTS
VitaminandMineralsinDiseasePrevention Currentevidenceisinsufficienttoassessthebalanceofbenefitsandharmsoftheuse ofthefollowing:
MultivitaminsforthepreventionofChronicdiseasesuchascardiovasculardisease andcancer.
VitaminDandcalciumsupplementationforpreventionoffracturesinpremenopausalwomenormenandinpostmenopausalwomen.
Becautiousinofferingseveralvitamins,includingA,C,andE,withantioxidant functionsforprotectionagainstcancer,heartdisease,andAlzheimerdiseasesince studiesreportequivocalresultsfortheseeffects,andseveralvitaminshavebeen showntobedetrimentalathighdoses.
HerbalSupplements
Morethan40%oftheUSpopulationusessometypeofcomplementaryoralternativemedicine.Effectsofherbalsupplementsaredifficulttoevaluateduetoproblems inisolatingtheactivecomponent.Table2.11listsherbalsupplementswithdemonstratedsafety.Certainherbalremedieshavebeenassociatedwithdeleteriouseffects andshouldbeusedwithcaution.Examplesinclude:
Blacklicorice:Causeshypertension.
Chromium:\I/bloodsugar.
Garlic,ginger,gingko,ginseng,feverfew,C0910:ProlongINR.
IDomesticViolence
INTIMATE-PARTNERABUSE
Definedasintentionalcontrollingbyorviolentbehaviorfromapersonwhowasor isinanintimaterelationshipwiththevictim.Thisbehaviormaybephysicalabuse, sexualassault,emotionalabuse,economiccontrol,and/orsocialisolation. Womenaremorelikelythanmentobethevictimsofchronicphysicalabuse. Violenceingayandlesbianrelationshipsappearstobeascommonasinheterosexualrelationships.
Moststatesdonotcurrentlyrequiremandatoryreportingofdomesticviolence againstcompetentadults.Table2.12outlinesriskfactorsforintimate-partnerabuse.
TABLE2.11 EffectsofSelectedHerbalSupplements
SUPPLEMENT DISEASE/CONDITION NOTES
Garlicpowder
Highcholesterol
Gingerroot Nausea,motion
Hasmodesteffect;prolongsINR
Studiesareconflictingonwhethergingeriseffectivefor sickness motionsickness;probablysafebutmayinteractwithmany medications
Glucosamine Osteoarthritis
Horsechestnut Venous
Usewithcautioninthepresenceofseafoodallergy
Bescin,amixtureoftriterpenesaponinsisolatedfrom insufficiency thehorsechestnutseeds,hasbeenshowninrandomized controlledtrialstohaveefficacyinchronicvenous insufficiency;itsmechanismofactionremainsunknown
Peppermintoil IBS
Sawpalmetto BPH
StJohn'swort Depression
Usesupportedbydatafromclinicaltrials
Giveatadoseof160mgBIDor320mgonceperday
ComparableefficacyandsafetywhencomparedwithSSRls inpatientswithmildtomoderatedepression;cautionwith useisadvisedduetomultipledruginteractions
FGURE2.2. Pellagra.Characterized byanerythematousrashinsun—exposed skin.Findingsrangefromobviousscaly erythematosubtlechangesthatareoften mistakenforthephoto—damagetypically seeninelderlypatients.(Reproducedfrom OldhamMA,etal.Pellagrousencephalopathy presentingasalcoholwithdrawaldelirium:Acaseseries andliteraturereview.AddictSciClinPract.2012;7(1):12; courtesyofRichardJohnson,MD,Departmentof Dermatology,MassachusettsGeneralHospital,Boston, MAUSA,2012.)
' KEYFACT
Beawareofherbalremediesthatinteract withwarfarin,includinggarlic,ginger, gingko,ginseng,feverfew,andClO.
' KEYFACT
Bealertforsignsandsymptomsof intimate—partnerviolence.Womenabused bytheirintimatepartnersaremore vulnerabletocontractingHIVorotherSTIs duetoforcedintercourseorprolonged exposuretostress
A30—year—oldbusinessmanwhoisrelocat— ingtoIndiain5weekspresentsforapre travelcheckeup.Hehasnosignificantmedie calhistoryandisgenerallyingoodhealth. Heprovideshisimmunizationrecord,Heis worriedaboutcontractingmalariaandhav— ingboutsofdiarrhea.Howdoyouaddress hisconcerns?
Whenreviewinghisimmunizationrecords, lookspecificallyforthedateofhislast tetanusboosterandWhetherhehasbeen immunizedagainstHAVandHBV;otter generaltraveladviceregardingfood, water,andinsectrepellant;andprovide prescriptionsforbothmalariaprophylaxis andtraveler’sdiarrhea,withstrictandclear instructionsonwhenandhowtheyshould betaken.
TABLE2.12. RiskFactorsforIntimate-PartnerAbuse
RISKFACTORS
Femalegender
Youngage
Lowsocioeconomicstatus
Pregnancy
WHENT0SUSPECT
Inconsistentexplanationofinjuries
Delayinseekingtreatment
Multiplesomaticcomplaints
Gynecologicconditionssuchaspremenstrual
Mentalhealthproblems syndrome,STls,unintendedpregnancy,or
Substanceabuseonthepartofvictimsor chronicpelvicpain perpetrators
Separatedordivorcedstatus
Historyofchildhoodabuse
CHILDABUSE
Latenessforprenatalcarevisits
FrequentEDvisits
Patientnoncompliance
Centraldistributionofinjuries(breasts, abdomen,genitals)
ThisimportanttopicisaddressedintheChildandAdolescentMedicinechapter.
TravelMedicine
Travelisassociatedwithpotentialmorbidityandevenmortalityfrominfectious sources,modesoftransportation,environmentalexposures,andadversemedicalout— comesfromillnessesindependentoftravel.Inaddition,alwaysaddresssafesexstrategieswhenapatientwillbetraveling.Offerthefollowingguidelinesandrecommendationstothosecontemplatingorplanningtraveltoreducetheriskofadverseevents. PleaseseetheCDCWebsiteforup—to-dateinformationregardingspecificlocations.
PRETRAVELASSESSMENT
Determinethepatientshealthstatus(eg,infants,elderlypersons,pregnantwomen, orthosewithchronicillnessesorunderlyingmedicalconditions).
Identifypotentialmedicalneeds(eg,allergytovaccinecomponents,medication use,immunosuppression).
Evaluatethepatient’stravelitinerary(eg,planneddestinations,climateandaltitude, ruralvsurbanenvironment,durationofstay,accommodations,purposeoftravel).
GENERALGUIDELINESFORSAFETRAVEL
Food:Advisepatientsthatfruitsaresafeonlywhenpeeledandthatvegetablesneed tobefullycookedtopreventcontaminationfromfecallypassedorganismsinthe soil.Unpasteurizeddairyproductsandinadequatelycookedfishormeatshouldbe avoided.
Water:Counselpatientstoavoidicecubesandthatwaterissafeonlyafterithas beenboiled.Chlorinationwillkillmostviralandbacterialpathogens,butprotozoal pathogenssuchasGiardialambliacansurvive.Carbonateddrinks,beer,wine,and drinksmadefromboiledwateraresafe.
Insectrepellents:Advisetravelerstouseatleast20%DEETonclothingandexposed skintopreventmosquito-borneinfectionssuchasmalaria,yellowfever,dengue fever,andZikavirus.ProtectionwithDEETlastsforseveralhoursbutismitigated byswimming,washing,sweating,wiping,andrain.Travelersmayalsochooseto