THE LONG EMERGENCY: NAVIGATING COVID'S NEXT STAGE
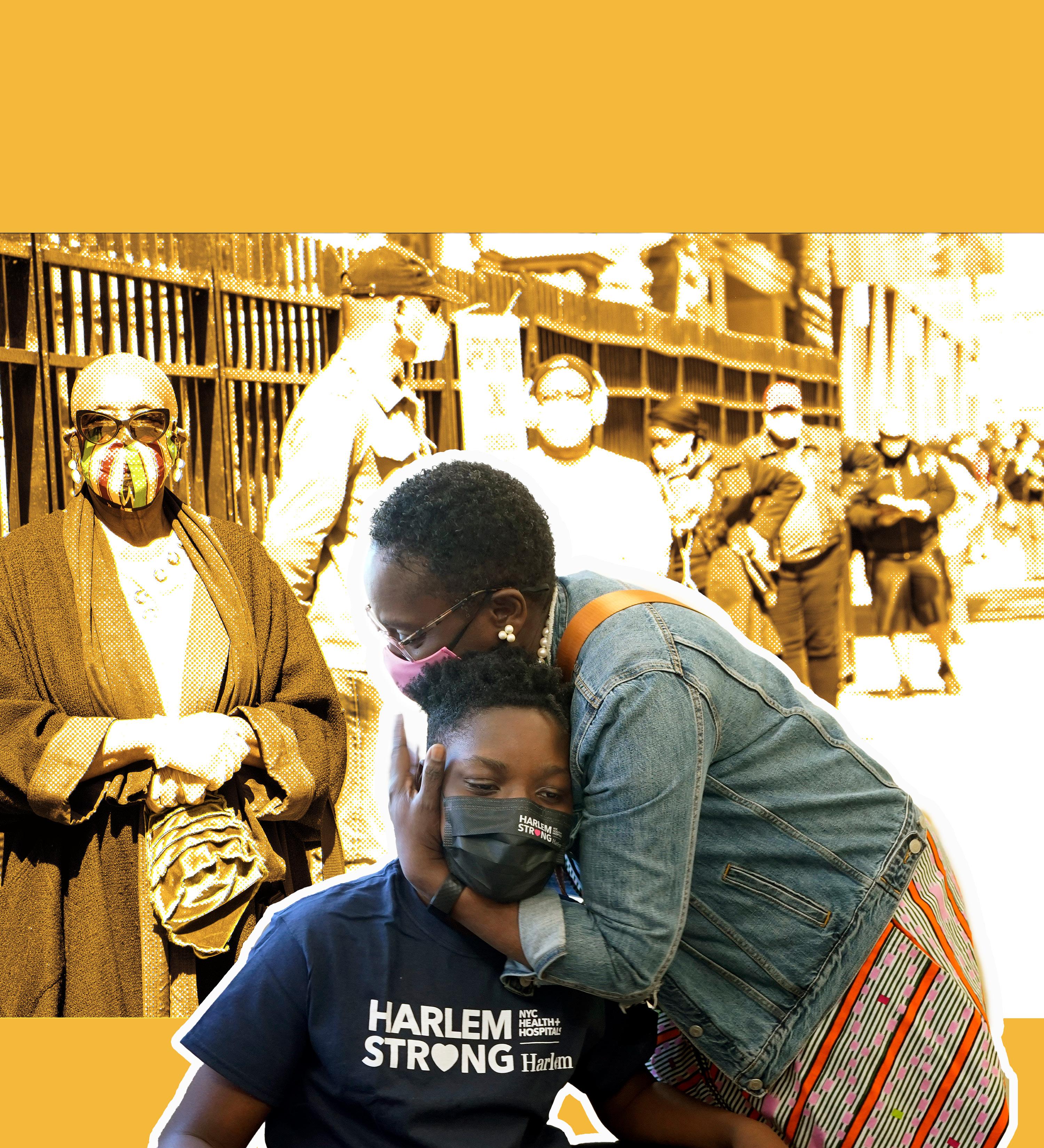 Illustration by Amanda Ulloa (AP Photo/Richard Drew) (AP Photo/Mary Altaffer)
By HELINA SELEMON Blacklight Science Reporter
Illustration by Amanda Ulloa (AP Photo/Richard Drew) (AP Photo/Mary Altaffer)
By HELINA SELEMON Blacklight Science Reporter
More than three years into the pandemic, our understanding of the extent of COVID-19’s impact on Black and brown communities remains incomplete due to a lack of federal data on race and ethnicity.

The Centers for Disease Control and Prevention (CDC) has reported over 104 million COVID-19 cases in the United States, but only 66% of those cases include race or ethnicity information. For comparison, the same data misses only 2% of sex data. Demographic data like race and ethnicity tells agencies and policymakers who’s vulnerable at different stages of the pandemic and helps them decide how and where to allocate resources like vaccines and testing. Researchers have been raising the alarms for years, and many are concerned that this can have serious implications in the years and even decades to come.
“Although race and ethnicity for testing and cases have become more complete since reporting began, a significant portion of both testing and case data continue to lack racial and ethnic information,” a CDC spokesperson said in a statement. But why is it missing in the first place?

TESTING OVERLOAD
It might come down to how the data was collected. In the early months of the pandemic, the surge of patients filling hospitals, clinics, and makeshift testing sites overwhelmed healthcare systems, making data collection on patients difficult to complete, let alone enforce.
Sarita Shah, an epidemiologist at Emory University, says the main issue early on was that data on COVID-19 cases that health departments received largely came from labs that received COVID-19 testing samples since they were quicker and most consistent at reporting information to local health departments than clinics and hospitals.
But unlike clinics and hospitals, labs don’t usually have much information about the patients they’re testing to pass on to health departments.
“The form does not typically include race and ethnicity since this is not crucial for the lab to conduct the test,” Shah told the Amsterdam News. They actually get very little information: name, DOB, address, and ordering physician.
This actually isn’t normally a problem for most diseases on an epidemic scale, Shah said. With other diseases like Ebola or tuberculosis, health de -
partments would have more time to report on it, gathering data from multiple sources to fill in gaps. COVID-19 was different, she said.
“We didn’t really have that time,” said Shah. “And the systems that we have in place for data reporting for public health purposes are huge operations and they’re not very easy to modify, adapt, pivot. They’re certainly not fast enough for the pace that COVID-19 needed.”
In April of 2020, New York City’s health department was trying to connect data from labs and hospital systems together. Celia Quinn, the deputy commissioner of disease control at the Department of Health and Mental Hygiene (DOHMH), said their best method for getting demographic data was actually to investigate each case, “which is a huge burden on us,” she said. “People don’t always want to talk to us.”
The frantic rush in the first few months of the pandemic might explain early data gaps, but continuing trends of missing race and ethnicity data and rising trends in some states, including New York, make little sense.
“It is quite concerning to see that this remains a persistent barrier and maybe even a worsening barrier,” Shah said.
IN FORMS WE DISTRUST
The CDC uses COVID-19 data to track outbreaks and trends across the country and to assess whether public health actions are working. While the agency mandated that state and local health departments report data on the virus’s spread and impact, each state had its own way of collecting that data.
When it comes to turning over data, the CDC has no enforcement mechanism in place to make sure that health departments report this information. Testing forms asking for name, age, sex, race, and ethnicity often remained incomplete or partially complete. Doctors noted that from the start of the pandemic it was these forms required by the CDC that went unfilled by patients and providers.
“I think we were trying to put in place Band-Aids, I guess, on a system that couldn’t really handle the stress but needed to have this information,” Shah said.
It’s not clear why these problems persisted in each state, but some researchers cite issues with community trust. Historical mistrust of medical institutions from Black and brown Americans contributed to hesitancy on sharing race and ethnicity
Continued on page S3
May 11, 2023May 17, 2023 • THE NEW YORK AMSTERDAM NEWS 2 S
COVID-19 DATA IS MISSING LOTS OF RACE AND ETHNICITY INFO. HERE IS WHY.
A woman with a face mask walks past a mural in Brooklyn on Friday, March 27, 2020. (AP Photo/Wong Maye-E)
with healthcare providers, contact tracers, and healthcare systems collecting COVID19 patient information.
As a result, the communities most impacted by the virus are usually the least likely to identify in health surveys or fill in the race and ethnicity questions.

One study found that 28% of surveyed patients were uncomfortable providing their race and ethnicity to healthcare providers, while another points to greater reluctance among those who’ve experienced discrimination.
Emil Coman, a statistician and researcher for the Health Disparities Institute at the University of Connecticut, said that collection of racial and ethnicity data in the U.S. is becoming more important than in other cultures and countries.
“Racial and ethnic minorities have inherited a set of burdens that makes the study of their health status compared to white U.S. residents somewhat more challenging,” he said.
Coman understands the skepticism people feel. Personal information that is collected by agencies, like a person’s name, birth date, and address, can feel less sensitive to share than race and ethnicity. While data systems commonly collect information about us like name and address, race and ethnicity are often excluded or requested less frequently.
“That’s the issue,” he said. “Race is a very stable characteristic of a person, and once it’s recorded in one place it should be available.”
To reduce missing data, it becomes important that public health and providers restore some of that trust by providing patients with the information they need to understand why those details are being asked of them in the first place.
Quinn said the burden is on providers to collect that information accurately and to do it in a way that’s sensitive and encourages people to report instead of simply checking “not interested” or “not applicable.”
“That’s a really high burden,” she added.
Quinn said the city’s health department is working on improving the way that they get information so that they can get as complete a picture of the virus as they can. “That’s something that we’ve worked on with providers and with labs to make sure that we have the infrastructure to receive that information,” she said.
The more passive the process is for getting this vital information, the more completeness we can start to see with race and ethnicity data, Quinn says. Testing systems at pharmacies like CVS or Walgreens make getting demographic data collection easier.
“That’s one way that we kind of work with the provider and the testing side to make sure that that information is collected so that it can come to us,” she said.
FILLING IN THE GAPS
Some researchers have tried to fill in the gaps. Chicago’s public health department teamed up with DePaul University and attempted to identify race and ethnicity in data that was previously unknown. A team at Emory University, including Shah, worked with Fulton County in Georgia to show fuller disparity by factoring for statistical biases.
“I think the best way forward is to have the actual data collected… that’s our first choice,” Shah said. “In the absence of that, though, these are tools we can use to fill in some of those gaps.”
It’s not perfect, she says, “but we do have statistical methods we can use.”
“I don’t think COVID is the [main] reason for missing race and ethnicity, I think the way it’s being collected in this country is flawed,” said Ofer Harel, professor of statistics and associate dean for research at the University of Connecticut. He added that there are a number of models that statisticians use to answer questions from data, but many researchers without this background may not know how best to apply them.
Research about missing data has been going on since the 1970s, said Harel, who researches methods for handling incomplete data. As science evolves, we may be able to develop better methods. “We’re getting better, but we don’t know everything yet,” he said.
Some states are missing more race and ethnicity data than others. According to April 2022 data from the Kaiser Family Foundation, places with sizable Black and Hispanic/ Latinx populations like Louisiana (22% cases with unknown race or ethnicity), District of Columbia (22% unknown) and Massachusetts (28% unknown) had less missing data than most. (As of April 2023, California has 18% cases with unknown race or ethnicity.) Other states like Maryland (39% unknown), Texas (50% unknown), New York (51% unknown), and Connecticut (69% unknown) saw an increase in missing data as the pandemic rolled on.
Delaware had both. Delaware started off with a huge amount—78% of missing race and ethnicity data—in July 2021. That number dropped to 39% almost a year later.
Delaware Health and Social Services said that the department issued an order in March of 2020 requiring labs reporting to the state to include race and ethnicity data in their results. They credited contact tracing for filling in the gaps and manually updated information when it was missing.
New York state’s percentage of missing race and ethnicity case data was dropping until around fall 2021 when missing data started to increase again. By April 2022, New York State’s Department of Health (NYSDOH), which depended on labs to report race and ethnicity, had missed 51% of race and ethnicity data.
According to the DOHMH, New York City started out missing 60% of race and ethnicity data for cases, 17% for hospitalizations, and 10% for deaths. The amount of missing race data for new COVID-19 cases is now down to 20% and Quinn cred-
in the fall of 2021 to when the city stopped doing test and trace in the spring of 2021.
“We stopped calling people to ask them their demographics,” she said. “We never got 100% completion even on that demographic question because I think it was put at the end of the interview just to make sure that we got some of the more critical pieces of, you know, who were your contacts so that we could do the contact tracing piece of it.”
It was at that time that Quinn said the department started focusing their investigations on cases that were in congregate settings or more like high-risk locations.
Pandemic-related hospitalizations and deaths tend to be better collected because of how they’re documented. Race and ethnicity data is the least complete for cases and continues to get more difficult with athome testing being more commonplace. The only people who get counted are those who are coming to a public health laboratory that are then going to end up in the reporting system, Shah says.
WHAT HAPPENS TO DATA WITH COVID-19 EMERGENCY ENDING?
The public health emergency ends this May and so will the way that state and local health departments monitor COVID19 as the federal government won’t require reporting of testing data. Without a federal requirement, the ways that the virus is monitored by cities and states will likely vary even more.
Persistent gaps in data can lead to inequitable distribution of resources. As policymakers in New York City navigate decisions to transition the city “back to normal,” incomplete data will continue to inform those decisions.
Quinn said that the demographic data for COVID-19, like the 80-some maladies the city health department tracks, helps the agency know what’s happening with the disease, where it is coming from, whether the disease requires an emergency response, who is being most impacted, and how they communicate with communities most impacted to keep them safe.
design better systems that talk to each other and surveys that are uniform and represent people’s identifiers well. Where data like race and ethnicity are unknown, he suggests a sensitivity analysis, a statistical approach that measures the potential impact of a complete data set, would help health departments analyzing data convey a greater sense of scope for the burden on people of different races and ethnicities.
Coman said in an attempt to be broad and general, federal demographic survey questions miss out on the complexity and nuances of who we are and our lived experience. “Trying to create categories that are very general and that apply everywhere equally gets you into this trouble,” he said.
There might be some federal movement to address this issue, not specifically for COVID-19 surveillance but more widely for how the federal government collects demographic data for public responses. The federal government announced late January that they’ve begun seeking proposals for revising the federal race and ethnicity standards.
But as people and governments start to move on from the pandemic, federal and local health agencies will be rolling back how often and how much they report data on COVID-19. What’s more, states won’t be required to report cases, and the CDC will stop tracking community-level spread, focusing on deaths and hospitalizations. Less data along with missing race and ethnicity data for COVID-19 will continue to hinder our ability to understand the true impact of the pandemic on different communities. Luisa Borrell, a Distinguished Professor of Epidemiology and Biostatistics at CUNY’s Graduate School of Public Health and Health Policy, said obtaining better data, is crucial to effectively addressing racial and ethnic inequality.
“So I think we have to put our money where our mouth is,” she said. “We have to definitely get better data.”
THE NEW YORK AMSTERDAM NEWS 3 S
COVID-19 DATA IS MISSING LOTS OF RACE AND ETHNICITY INFO Continued from page S2
Penny Pierce fills out forms with the help of Taiwan McCall before getting tested for COVID-19 in Harlem in April of 2020. Getting patients to fill out demographic information has been a challenge during the pandemic. (AP Photo/Seth Wenig)
THE LONG EMERGENCY
Is the pandemic over? Public health experts say not yet
By HELINA SELEMON Blacklight Science Reporter
New York is as back to normal as it has ever been since the start of the COVID19 pandemic more than three years ago. After years of unprecedented disruption, restaurant-goers are squeezing indoors for brunch, catching up on lost time with friends and family. Commuters and tourists are filing back into the subway, rushing to and from work and exploring the city. And with spring in full swing, parks and convention centers are alive with energy once again. But while many in the city are moving on from the pandemic, there’s one major milestone that signifies a true turning point in America’s fight against COVID-19: the expiration of the federal public health emergency on May 11.
“The end of the COVID-19 public health emergency will mean an end to policies that made access to testing, treatment, and vaccines free or affordable,” Lesley Green-Rennis, chair and professor of health education at Borough of Manhattan Community College (BMCC) tells the Amsterdam News.
While the expiration of the federal public health emergency doesn’t signify the end of the pandemic, which is currently killing more than 1,000 Americans a week, it does mark the beginning of reductions in national emergency support.
Some of these rollbacks have already taken place: in February, Congress reduced SNAP emergency allotments, and President Joe Biden signed a congressional resolution in early April to end the
coinciding national emergency that was originally slated to expire with the national public health emergency. On the global stage, the World Health Organization (WHO) recently decided to lift its COVID19 emergency.
Grappling with these policy changes includes understanding what support remains to carry Americans through a pandemic that still isn’t over, and how to make choices on the best ways to stay safe in the months ahead.
THE PANDEMIC LINGERS ON
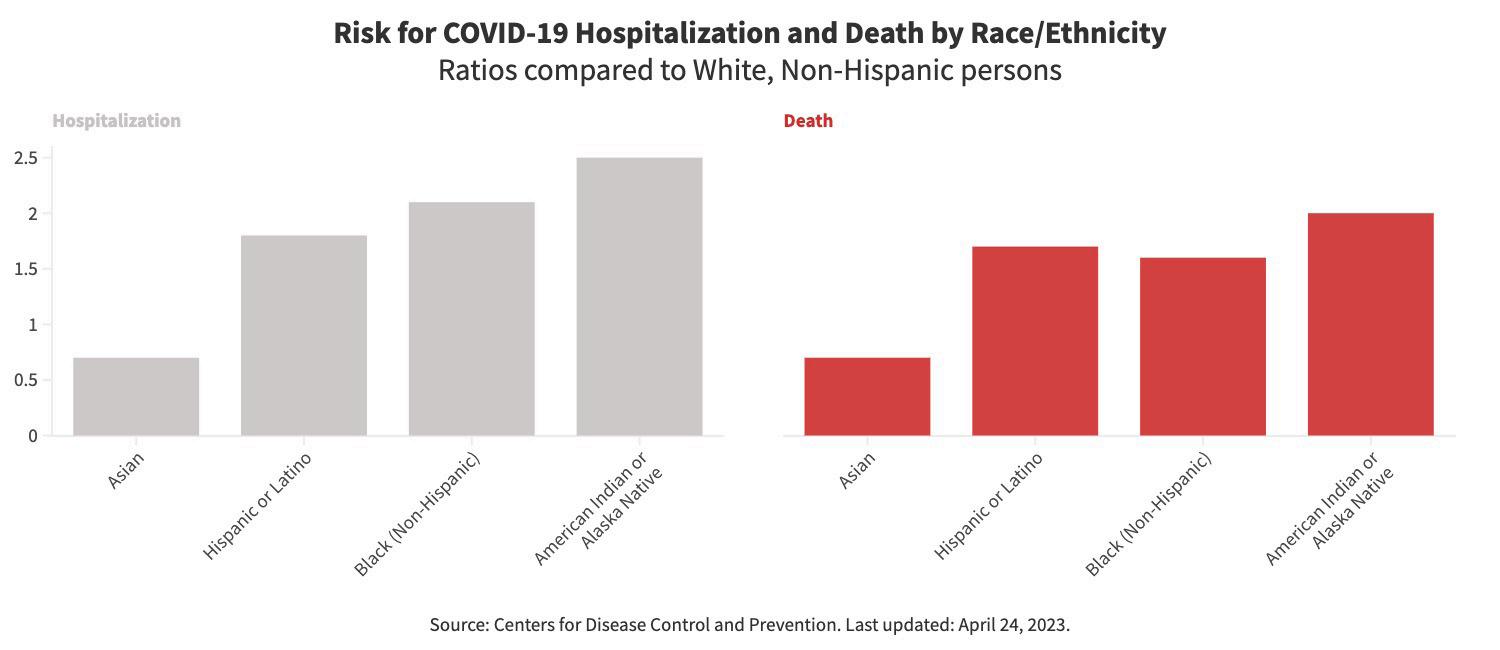
Three years into the pandemic, much of the anxiety and fear has been quelled since its early days. Case numbers and deaths have dropped to record lows. According to the Centers for Disease Control and Prevention (CDC), the U.S. is now experiencing more than 150 deaths a day and 1,375 hospitalizations a week, down from the most recent peak in early 2022 of about 2,500 deaths per day and 21,525 hospitalizations per week. Yet Black, Indigenous, Hispanic, and Latinx Americans are some of the most vulnerable. Black people are 60% more likely to die of COVID-19 compared to white people, according to the latest data from the CDC. Similarly, Hispanic and Latinx people are 70% more likely to die of the virus, and American Indian or Alaska Native people are twice as likely to die. More than 326,000 Black, Hispanic, and Latinx Americans have died since the pandemic started.
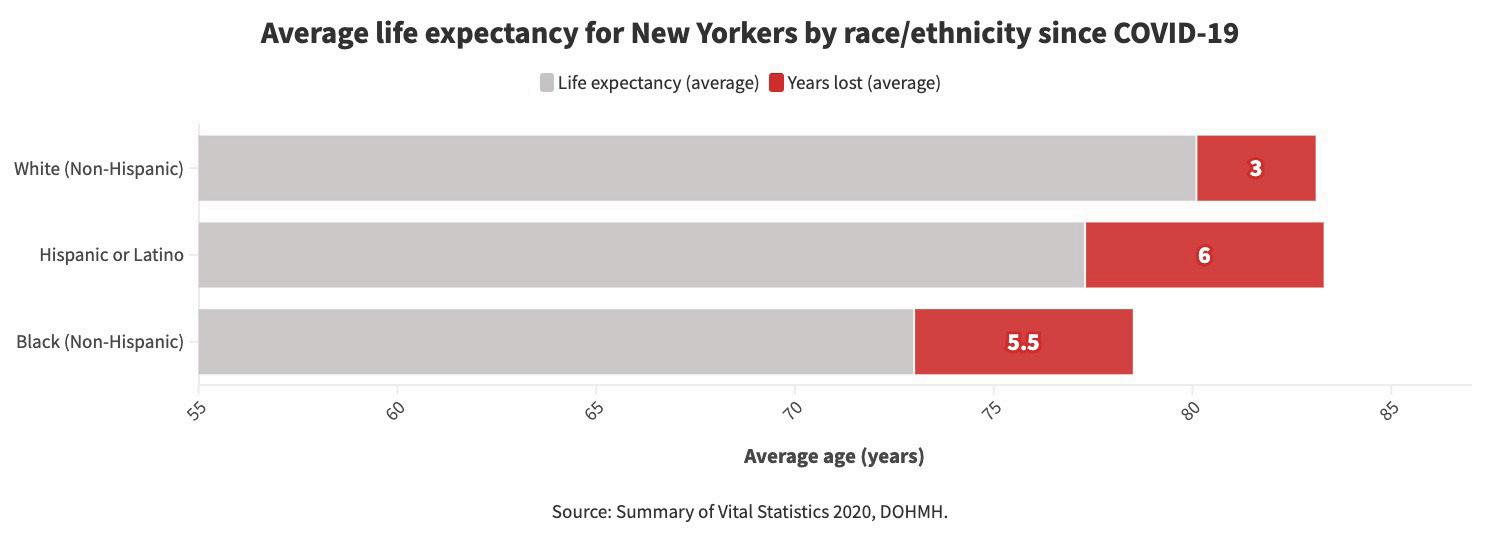
The pandemic also took years off of New Yorkers’ lives. A recent study from the
New York City Department of Health and Mental Hygiene found that the average life expectancy of Black New Yorkers is down five and a half years to 73 years, and Hispanic and Latinx New Yorkers are down six years to 77.3 years old. For comparison, life expectancy dropped three years, down to 80.1 years, for white New Yorkers.
In the 1950s, the average life expectancy for Black Americans was 63.6 years. Every fraction of a year in life expectancy can take years to gain. Luisa Borrell, a Distinguished Professor of Epidemiology and Biostatistics at CUNY’s Graduate School of Public Health and Health Policy, says it will take us decades to get those years back.
“Look at how long it [took] for African American [sic] to have a decent life expectancy,” she says. “And look at how long it took to get to 70.”
It will be an uphill battle to regain lost life expectancy in the years ahead. GreenRennis says it’s important to be vigilant to protect vulnerable people in our lives. This includes people of color over 50, people who are immunocompromised, pregnant people, or people living with comorbidities that make people vulnerable to COVID-19 like heart disease, high blood pressure, and asthma.
POLICY (AND COST) CHANGES TO COVERAGE AND ACCESS
The end of the public health emergency will change the cost and accessibility of preventing and treating COVID-19 for many people. Leighton Ku, Professor and Director of the Center for Health Policy Research at George Washington University, says that the three big elements he’ll be watching for
will be changes to Medicaid coverage, testing access, and SNAP benefits. Medicaid recipients will likely see the most drastic change since the health emergency allowed for continuous enrollment throughout the pandemic and prevented states from taking people off of insurance. The Kaiser Family Foundation estimates that between 5 and 15 million people could lose their Medicaid coverage if states no longer deem them eligible. Ku estimates that the number of people losing coverage is likely higher, between 15 to 18 million people, with many of these policy changes affecting Black and Latinx adults and children.
This dis-enrollment or “unwinding” of Medicare enrollment lists will take place over the next 14 months, sooner in some states than others. Ku says it is important that people insured through Medicaid have updated their contact information, including their address, with their state so that they don’t miss updates on their insurance.
VACCINES: MOSTLY FREE FOR NOW
On April 18, the Department of Health and Human Services announced a program to keep vaccines free for uninsured Americans. Some of the changes include paying for COVID-19 vaccines if you get your shot out-of-network and likely paying more for future shots. Those on Medicaid and with Medicare Part B will continue to have free shots, thanks to a provision in the CARES Act. According to Ku, COVID-19 vaccines are still free for anyone who has public or Continued on page S5
May 11, 2023May 17, 2023 • THE NEW YORK AMSTERDAM NEWS 4 S
private health insurance. So if you have Medicaid, private insurance, or Medicare, your COVID vaccine will still be covered and insured Americans will not need to pay for that as a preventive benefit. Just make sure to get your shot from an in-network provider, as private insurance companies may require people to pay for COVID-19 vaccines if they are out of network.
New Yorkers can still get a free vaccination by appointment at a NYC Health + Hospitals or Gotham Health center by calling 1-844-NYC-4NYC.
TESTING AND TREATMENT: COSTS DEPENDS
For testing, private insurance companies will no longer be required to cover up to eight rapid COVID-19 tests per month, as they were during the public health emergency. Most insurance will cover costs for COVID-19 PCR testing, but uninsured Americans – 27.5 million people, or 8% of the national population – will probably have these costs come out of their pocketbooks.
At-home test kits are still available all over the city while supplies last. With the end of mobile testing centers, New Yorkers can make an appointment to get free PCR testing at one of the city health department’s express sites, or pick up at-home testing kits at their nearest NYC Health + Hospitals and Gotham Health center. The city’s COVID hotline (212-268-4319) is available to help find free PCR testing and at-home testing kits.
For treatment, New Yorkers can go to NYC Health + Hospitals and Virtual ExpressCare or call 212-COVID19 (212-2684319) for a free prescription and delivery of the antiviral treatment Paxlovid. The medication will remain free to all Americans as long as government supplies last.
SNAP: LIKELY LESS ACCESS THAN BEFORE
At the beginning of March, SNAP allotments fell considerably for millions of people around the country, Ku says. Emergency allotments made on a sliding scale over the pandemic to meet family needs have returned to pre-pandemic amounts, a difference of up to a couple hundred dollars, depending on your household size. For those close to the poverty line, this amounts to even less than before the pandemic. “As we all know, food inflation is really high right now,” Ku says. It also halted work requirements during the pandemic and the government will be returning to a policy of only non-disabled people being allowed to receive SNAP benefits for three months unless they’re working 80 hours a week.
THE BEGINNING OF THE END OR THE END OF THE BEGINNING?
Some public health experts are concerned that this might give people the indication that the pandemic is over. The World Health Organization hasn’t yet declared the
pandemic over. Sentiments about the pandemic have eased, though attitudes are mixed about the end of the pandemic.
“I think the crisis phase is definitely over,” says Celine Gounder, an epidemiologist and infectious disease specialist and editor-at-large for public health at the Kaiser Family Foundation. “Hospitals are not overflowing with COVID patients [and are] able to now balance COVID care with other kinds of care… but we haven’t really learned the lessons of COVID-19.”
A recent survey found that 59% of adults in America think the public health emergency ending will have no impact on them, and almost half think that it won’t have an impact on the country. The public health emergency ending drew greater concern from groups of Americans who have been more negatively affected by the pandemic. Medical and public health officials are clear that the virus is still among us, and still mutating, so there’s still some risk, Green-Rennis says. “Our primary concern is that people will forget that, or not believe it and fail to practice preventive measures.”
This includes hand washing, refraining from interacting with others when we are sick, masking, getting tested when appropriate, and staying up to date with vaccinations, especially those who are particularly vulnerable.
Jorge Moreno, a physician and assistant professor of medicine at Yale University, says that seniors should get the latest bivalent booster if they haven’t gotten COVID-19 or had any boosters in the last four months.
“I cannot stress that enough. Get your booster, if possible,” he tells the Amsterdam News. “It’s still time, it’s not gone, it will protect you.”
Gounder says that immunocompromised folks should consider getting vaccine boosters every four to six months. She also recommends masking and opening doors and windows to create better ventilation at home when the weather allows and testing before going to big events. “It’s still
a really good tool to reduce risk,” she says. According to the CDC, only 16.7% of Americans have gotten an updated booster.
The antiviral drug Paxlovid continues to reduce the risk of COVID-19 progressing to severe disease, hospitalization, or death. “I think that’s a tool that’s really underutilized,” she says.
Moreno is looking ahead at the next few months with cautious optimism but urges people to stay up-to-date on changes with COVID-19 through the CDC, their state and local public health departments, and their doctors or community health centers.
“Educate yourself, not from Facebook, not from WhatsApp, not from social media,” he says. “There’s still a ton of misinformation out there…. I think getting the right information from the right resources will help you make decisions for you and your family.” New Yorkers, for example, can check local data maps to track COVID-19 trends in their area and follow our reporting on pandemic misinformation.
Moreno says it’s also important to notice when people in your community and schools are getting sick, and take some cues to mask and protect yourself. “Whether it’s kids out sick or more people around [you] getting sick, really [be] aware of that,” he says.
Ku says it’s fine to embrace some of what’s helping people feel normal these days. That said, Ku still carries masks with him wherever he goes.
“When in doubt, fall on the side of caution,” he says. “I have a mask in my pocket. I have masks in my car. So I am ready at any given moment.”
WHERE DO WE GO FROM HERE?
Dr. Gounder, an infectious disease specialist and epidemiologist, says when she thinks back to the early days of 2020, she remembers early conversations with her residents and medical students about a novel coronavirus when she was on service at Bellevue Hospital. At one point, she pulled out the first published epidemio-
logical report of AIDS.
“I said ‘We are at a similar moment with this new coronavirus,’” she says. Her students were skeptical, she recalled. “We haven’t really learned some of the lessons of COVID,” she says. “I think unfortunately, we’re not preparing ourselves for the next pandemic,” she added.
Gounder and others have outlined policy issues and next steps that still need to be addressed to curb this disease, like deciding what level of virus spread that we can live with, fixing our data collection systems for diseases, and addressing the ongoing shortage of public health workers.
Epidemiologist and Emeritus Professor of Public Health at Hunter College Philip Alcabes says the pandemic was an opportunity to completely reform the medical care system in America so that people could get access to the care they need. He says that some of his peers want more intensive and extensive disease surveillance systems to help us prepare for the next pandemic, but he’s thinking about how public health systems will be there for us the next time.
“I know there are people… who feel like ‘Well, what we have to do is create early warning systems so we’ll know when the new virus is coming,’” he says. “But that seems to leave unanswered the question of, well, what do we do once we know?”
The end of the public health emergency raises many questions about how we will handle the pandemic in the months and years ahead. However, experts agree that our success in dealing with the next pandemic will in large part be due to how successfully we learn, and implement, the lessons from the one we are all still living through.
For additional resources about COVID19, visit www1.nyc.gov/site/coronavirus/index.page or call 212-COVID19. COVID-19 testing, masks, and vaccination resources can also be accessed on the AmNews COVID-19 page: www.amsterdamnews.com/covid/.
May 11, 2023May 17, 2023 • THE NEW YORK AMSTERDAM NEWS 5 S
from page S4 THE LONG EMERGENCY
Continued
AFTER THE EMERGENCY ENDS:
What will stay and what will go?
not go back to pre-COVID times. But what impact will the end of the Federal Health Emergency on May 11 have on our lives?
Ziyad Al-Aly, MD is a clinical epidemiologist and Director of the Clinical Epidemiology Center for St. Louis, MO. He spoke with the AmNews about where we are currently regarding COVID-19 infections and why individuals must continue to stay vigilant.
“It’s actually hard to find someone who has not been infected [with COVID],” he says, adding that “it’s more common to find people who’ve been at least infected once, maybe some twice, and in some instances, really four or five times.”
Al-Aly says it’s very important for people to realize that COVID is still a novel virus and has not been on Earth for more than three or four years. “It still can wreak havoc with your body, so to the extent
sity School of Medicine “COVID-19 was something that was a tremendous learning experience for the world and we had the opportunity to come together to work together in a way that I think we probably hadn’t done previously,” she says.
“Unfortunately I think it also revealed some of the [structural inequality] . . .underlying some of the real issues in healthcare. So from my perspective some of the benefits of COVID were that we came together to look at science and companies that previously didn’t work together.”
Some of the aspects of COVID-19 that will stay with us are the therapies and treatments that were created, according to Gebo. A vaccine was developed in only 11 months and “we developed new therapies for treatment such as plasma, Paxlovid. So all of those things I think were real positives,” she says.
was already very clear.
The authors noted that “[a]s the COVID19 epidemic scales exponentially across the world, calls for expanded use of telehealth as innovative solutions, clearly highlights unmet needs” in the world healthcare system.

They say that telehealth has the potential to address many of the key challenges in providing health services during the outbreak of COVID-19: avoiding direct physical contact, minimizing the risk of COVID transmission, and continuous care. Clinicians and patients are strongly recommended to apply telehealth tools as an appropriate option to prevent and contain COVID-19 infections.
Dr. Gebo also spoke on the importance of telehealth and telemedicine. “People who were working or people who were unable to come to clinic on a regular
ers on their phones and have a face-toface visit… and I think that that actuallyular check-ins with some of my patients that I’m more concerned about instead of having them come to clinic, particularly some of my populations of patients who it’s difficult to get to clinic.”
Gebo continued, “I think that telehealth is something that we have to get better at and will be something that we move forward with. We have also gotten better with employing mobile medical devices so sending blood pressure cuffs to people at home glucometers so they can check their blood glucose. . . .It has built a health care system that is remote that is allowing people to do more interactions and more self-measurement and interactions with their health care provider to make decisions as opposed to waiting three months or six months for their next healthcare interaction.”
Other items that will “stay,” according to Gebo, include specific hospital and healthcare procedures, many of which Continued on page S7
-
May 11, 2023May 17, 2023 • THE NEW YORK AMSTERDAM NEWS 6 S
Medical director of Doctor on Demand Dr. Vibin Roy prepares to conduct an online visit with a patient from his workstation at home in April of 2021 in Keller, Texas. Telemedicine visits grew substantially during the pandemic and some doctors are advocating for it to expand. (AP Photo/LM Otero)
were available prior to COVID, but now have become deeply entrenched.
“I think one of the other things that will potentially continue is the idea of wearing masks in the hospital or medical facilities for high risk respiratory flu season or other seasons…. the fact that we as healthcare providers are now wearing masks is an important thing as we care for people who are high risk because they have symptoms so from my perspective I anticipate that during seasons where we have high flu rates or high COVID rates that we will re-implement these probably mandatory masks for healthcare providers in various situations at different times during the year.”
JD Davids is the Co-Director of Strategies for High Impact (S4HI), and is a health justice strategist for networks of disabled and chronically ill people and a queer and trans person living with myalgic encephalomyelitis (ME/CFS), Long COVID, and other complex chronic conditions.
January 2022 to really crystallize work that some of us have been doing before and during this ongoing pandemic as chronically ill and disabled people so our work is to build the power of chronically ill and disabled people to fight for and win the policies and programs that help us and our communities have healthy and safe and dignified lives. So in the course of this pandemic even as the pandemic was approaching, the conventional wisdom or the myth was that COVID wouldn’t be that big of a deal because it would only hurt people who are only sick or chronically ill already or are elderly. We think that our lives actually matter and that everyone was talking about us but not to us.”
The centering of people, coupled with the need for more trust, is something that Gebo cited as a real issue in the COVID-19 pandemic during her interview with the AmNews : “I think some of the things that were really complicated where we didn’t understand how it was transmitted and that led to some confu
health precautions that should be taken and as we learned more and changed our recommendations that led to feelings of that the government couldn’t be trusted or that people weren’t given the truth. As a scientist, it was very difficult because we were giving what we thought was our best advice at that time. . . with COVID, it was changing on a weekly, if not monthly basis.”
Gebo continued, stating “it developed this misinformation distrust because we were learning more and as we changed our messaging people felt that we were trying to hide things or we weren’t being forthcoming.”
As to where we are headed, according to Dr. Al-Aly, “the pandemic is not over. People are dying every day… people [are] getting infected and the virus is evolving… there’s really no guarantee that the next one around the corner will be milder and might be actually more severe so we have to be cautious… our situation today is certainly much better than what we were in March 2020… but

I really think that people need to be cautious… we’re asking for common sense measures for people to really take care of themselves and their families.”
Gebo also spoke to another aspect of the COVID crisis that may go namely specific health coverage, which could lead to equity issues.
“I think that there’s going to be some states that are going to really have significant swaths of the population who had coverage during COVID that are not going to and we had universal testing and treatment vaccines which rolled out, you know, very quickly, and I think it was well accepted and I think people appreciated that going back to the old system if you have health insurance and you can get coverage is going to continue those fissures in the healthcare system.”
For additional resources about COVID19, visit www1.nyc.gov/site/coronavirus/index.page or call 212-COVID19. COVID-19 testing, masks, and vaccination resources can also be accessed on the AmNews COVID-19 page: www.amsterd
May 11, 2023May 17, 2023 • THE NEW YORK AMSTERDAM NEWS 7 S
AFTER THE EMERGENCY ENDS:
Continued from page S6
Harlem resident Eleanor Kennedy, left, waits in line during a COVID-19 antibody test drive at the Abyssinian Baptist Church in May of 2020 in Harlem (AP Photo/Mary Altaffer)
By HEATHER M. BUTTS, JD, MPH, MA Special to the AmNews
As we continue to learn to live with and survive COVID-19, patients, policymakers, and doctors are still asking key questions. How should we as a society be serving people as the COVID-19 pandemic continues? How should individuals affected by COVID-19 be protected after the end of the public health emergency on May 11?
Dr. Andrew Pekosz, a virologist at the Johns Hopkins University Bloomberg School of Public Health, spoke with the AmNews about one group in particular that needs to be protected: those with Long COVID.
“I think Long COVID is a spectrum of a couple of different kinds of diseases,” he says. “We’re starting to really pay attention to [the fact] that some people have maybe more respiratory long-term side effects, some people have some neurological side effects, others have this general malaise feeling across their entire body.” Pekosz says that most people control infections and their bodies come back to a level that was exactly the same as it was before the infection. “But under certain conditions, and with certain viruses, there’s a larger portion of people that never make it back to that starting point,” he says. “And that’s where you can have some of these longterm effects.”
Pekosz says that one of the challeng-
es with studying and treating these longterm effects is the conflation of Long COVID into one disease when he believes that it is really various diseases. “I think it’s important to note that there’s probably a lot of different kinds of Long COVID that we’re now lumping together that I think we as scientists have to really separate out and study individually,” he says.
Lisa McCorkell, a co-founder of the Patient-Led Research Collaborative, an organization made up of Long COVID patients who are also researchers in fields such as biomedical research, public policy, and health activism, spoke with the AmNews about individuals that are chronically ill and suffering with Long COVID.
“I tell everyone, all patients, that they
know their body best, so if a provider tells you something that doesn’t align with what you’re experiencing, you’re not in the wrong,” she said. “There is a large community online that are experiencing exactly what Long COVID patients are going through, so trying to find that support can be really helpful.”
McCorkell says that many of the conditions that patients were getting diagnosed with like myalgic encephalomyelitis (also known as chronic fatigue syndrome or ME/ CFS) and Postural Orthostatic Tachycardia Syndrome (POTS), a blood circulation disorder, are generally lifelong conditions.
“I would say we are seeing people recover from Long COVID within a year but
Continued on page S9
May 11, 2023May 17, 2023 • THE NEW YORK AMSTERDAM NEWS 8 S
IMPACTED BY COVID-19
PATIENTS AND CAREGIVERS
WILL CONTINUE TO FACE CHALLENGES
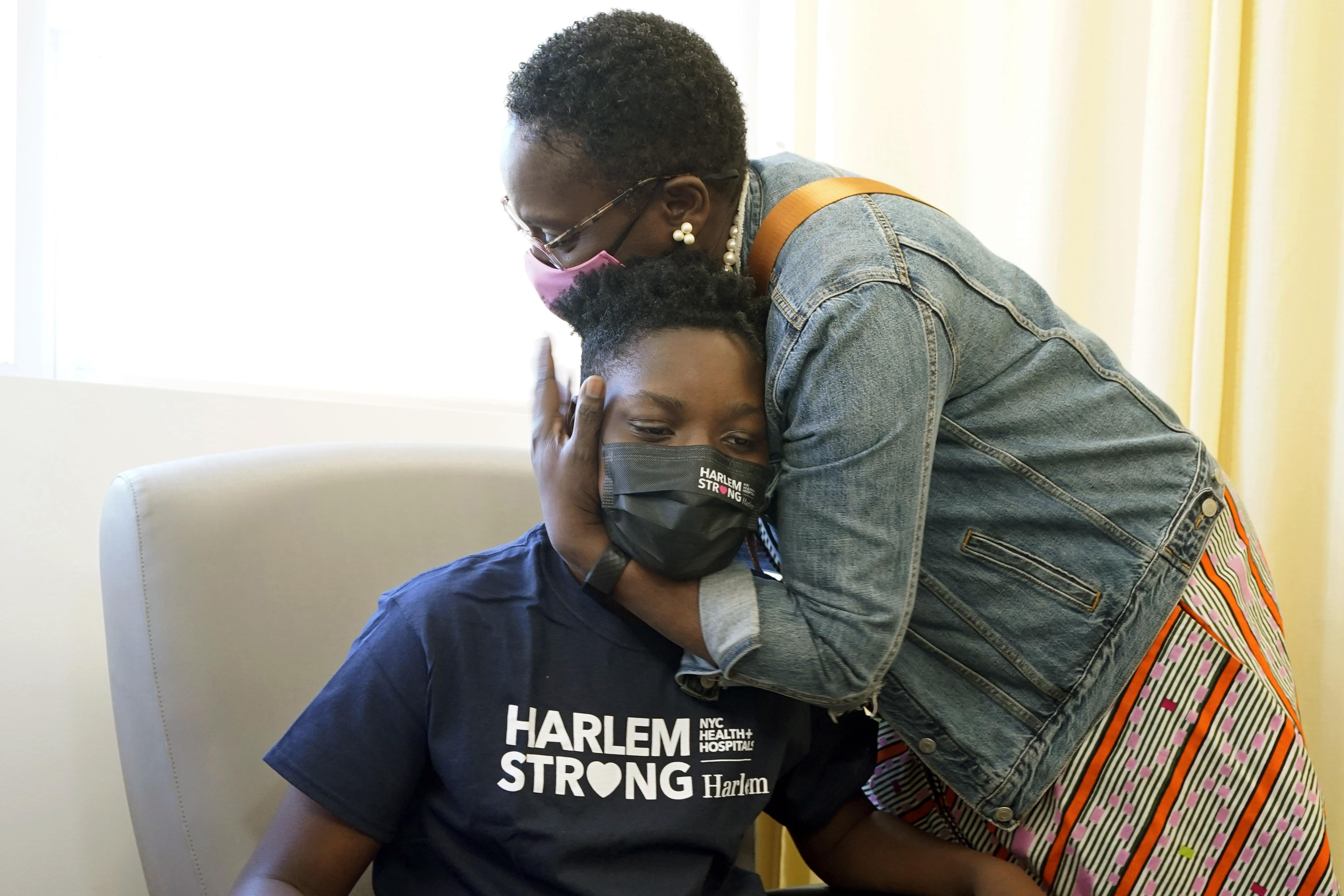
Julian Boyce, 14, gets a hug from his mother, Satrina Boyce, after he received his first Pfizer COVID-19 vaccination dose at NYC Health + Hospitals/Harlem, in 2021. (AP Photo/Richard Drew)
many of us have not. It’s a pretty significantly high number of us that are not,” she said.
“We’re all hitting our three-year anniversary and I don’t anticipate recovery,” she added. “It’s whether I get a treatment or not that helps me manage my symptoms so that’s definitely a myth that you recover from Long COVID [after] a few months because it’s possible people do but, [some] of us are not recovering within a year and if you don’t recover within a year, especially in things like ME/CFS and POTS, you’re more likely for it to be a lifelong illness.”
The continued struggle for many is not lost on experts like Dr. Kelly Gebo, Professor of Medicine and Epidemiology at the Johns Hopkins University School of Medicine.
“There are pockets of our population with people who have chronic diseases or who are caring for people with chronic diseases that are trying to continue to self-protect and there’s a real stigma associated with that,” Gebo says.

People with Long COVID are not the only ones facing pandemic-related challenges such as fighting for benefits, managing other chronic diseases, and dealing with food insecurity.
According to Gebo, there is a particularly vulnerable population in the aftermath of COVID-19: those who have been orphaned during the pandemic. Gebo highlights the significant needs of this group, emphasizing that losing a caregiver can have a profound impact on a child’s life.
People with disabilities are another impacted population. According to a report by the Center for Law and Social Policy, the backlog of applications at the Social Security Administration is “a hindrance for long COVID applicants, and others.”
The report recommends that programs like “TANF and SNAP be available to help people with Long COVID and other disabilities avoid hunger and hardship.”
Instead, disabled people face significant challenges in getting access to these essential support systems. The report highlights a concern that the systemic inequities of being denied benefits or losing them disproportionately can harm disabled people of color, individuals with low incomes, and those with marginalized identities. According to JD Davids, the Co-Director of Strategies for High Impact, we’ve been down this road before with other diseases.
“On the one hand we’ve seen what has happened with HIV with strategic investments and pushed by activists,” he says. “Over four decades, we’ve taken an almost universally fatal condition and been able to have it be a mostly manageable chronic condition if people get the treatment and care they need and it’s now even more readily a preventable condition.”
Davids says that we have a lot to learn
from past epidemics and the question is whether we will take those lessons and utilize them during the COVID-19 pandemic.
“So we have a choice here: we can go down the road of what we’ve done with HIV, or we could look at what . . .happened with myalgic encephalomyelitis . . .where we have …drastic lack of care and actual disbelief and doubting of those who have it who can be profoundly disabled.”
As for the end of the public health emergency on May 11, according to Davids, this is another place where looking to the past and HIV can be instructive. “It’s hard to call something an emergency for 40 years but when you look at the way that HIV has been and continues to be handled, it’s with specific and dedicated ongoing resources that has allowed us to have this success and that’s what we need for COVID and Long COVID,” he says.
Specific solutions that Davids gives in cludes creating long term federal fund ing similar to the Ryan White Care Act, which Davids says helps people get into and stay on the care and treatments that they need with all the support that helps them be able to do that. Training medi cal providers, funding for research, and national strategies are other solutions from Davids.
“What’s happening is right and left, measures are being dropped and it hap pened way before May 11th,” he says. “So what we’re going to see is basically at best a return to business as usual.”

Dr. Gebo is also an expert in the HIV arena, and spoke to some of these sim ilarities with the AmNews.

“I think the other thing [COVID-19] exposed was the difficulties and dispar ities in our health care system. There are populations that don’t get the same medical care as others and it’s important to try to engage everyone to make sure that we’re providing . . .the best possible care. Having done HIV medicine for 20 years, it wasn’t a shock to me, but I think having a global pandemic that affected everybody at the same time really exposed some significant flaws in our Healthcare system.”
Ultimately, Dr. Lisa McCorkell emphasizes the importance of taking measures to reduce the risk of experiencing these issues before, during, and after being diagnosed with COVID-19.
“It’s still worth it to try to not get COVID, to then try to not get Long COVID, and then if you are experiencing symptoms after COVID infection, it’s really important, especially if you’re having chest pain or anything that could be indicative of a stroke or a heart attack, to make sure to get that checked out and to not normalize that,” she says.
For additional resources about COVID19, visit www1.nyc.gov/site/coronavirus/index.page or call 212-COVID19. COVID-19 testing, masks, and vaccination resources can also be accessed on the AmNews COVID-19 page: www.amsterdamnews.com/covid/.
May 11, 2023May 17, 2023 • THE NEW YORK AMSTERDAM NEWS 9 S
Continued from page S8 PATIENTS AND CAREGIVERS IMPACTED BY COVID WILL CONTINUE TO FACE CHALLENGES
SCAN HERE nyc.gov/jointheboldest Start Building Your Career REGISTER FOR EXAM 3317 MAY 3 - May 23, 2023
THE TOUGHEST MOST REWARDING JOB IN LAW ENFORCEMENT
DECLINING ACCESS TO COVID-19 SERVICES WILL WORSEN HEALTH DISPARITIES
By
For much of the COVID-19 pandemic, New York City has offered a variety of services to support its residents who got infected. New Yorkers could get tested for free at sites across the city, even without health insurance; they could receive Paxlovid prescriptions from the same sites where they were tested; they could call a hotline for treatments or care advice; and they could even receive a free hotel room to isolate themselves from family members.
Those services have declined over the last year, however, culminating with the shutdown of many public testing sites this spring in time with the ending of federal emergency measures. In late March, NYC Health + Hospitals announced that it would end its mobile program for testing and Paxlovid prescriptions by May 11; testing will still be available at hospital sites, by appointment. For New Yorkers who are at higher risk of COVID-19, the change will make it harder to stay safe as the virus continues to spread.
Health + Hospitals provided a “vital resource and safety net” for New Yorkers throughout the last three years, said Dr.
The public health system primarily serves Black and Latino communities, including many New Yorkers who are low-income, don’t have health insurance, and are undocumented, she said. For these groups, the city’s free COVID-19 programs provided services that they may not have been able to access anywhere else.
Steven Thrasher, a professor at Northwestern University and author of the book “The Viral Underclass,” told the Amsterdam News that the city has been “a leader in a lot of ways” during the pandemic. City institutions quickly built a COVID-19 service infrastructure that didn’t exist in other parts of the U.S., he explained.
But now, much of that infrastructure has been dismantled, both in New York City and across the country. The local closures come as healthcare organizations nationwide prepare for the federal public health emergency to end on May 11.

The combination of local and national changes is “a perfect storm,” Blackstock said. “It really feels like an abandonment of public health.”
At this point, while the federal govern-
insurance companies to provide free tests, and insurance coverage of treatments and vaccines is likely to change as well.
After May 11, many New Yorkers may not know where or how to get COVID19 care—and this will lead fewer people to seek it out, experts say. Still, one important program remains intact: people will still be able to connect with doctors for COVID-19 care through calling the Health + Hospitals hotline, 212-COVID19, or making an appointment by calling 1-844-NYC-4NYC.
In response to questions, Health + Hospitals and the city health department both referred to its March press release announcing the site closures. “As we transition out of the emergency phase of the pandemic, the Health Department and NYC Health + Hospitals will continue to provide services and support to New Yorkers and ensure access to lifesaving COVID19 care,” Health Commissioner Dr. Ashwin Vasan said in a statement.
The federal public health emergency “bolstered” New York State’s response to COVID-19, a spokesperson for the state
health department said. After it ends, “thegoing access to vaccines, COVID-19 tests, and treatments.”
COVID-19 SERVICES REMAIN VALUABLE
While COVID-19 may not be spreading across NYC as much now as it was in 2020, the disease still kills hundreds of Americans every day and has led to long-term symptoms for millions. Testing remains important as a preventative measure, said Dr. Wafaa El-Sadr, a professor of epidemiology and global health at Columbia University’s Mailman School of Public Health. A positive test result can lead the patient to isolate, breaking potential chains of transmission, El-Sadr said. This may be particularly helpful for reducing outbreaks in workplaces that require in-person attendance. At the same time, the patient can seek out Paxlovid or other COVID-19 treatments.
Paxlovid, the most effective treatment against currently-circulating variants, is more effective when patients receive it quickly after becoming sick. “So the easier it is to get tested promptly, the better,” ElContinued on page S11
May 11, 2023May 17, 2023 • THE NEW YORK AMSTERDAM NEWS 10 S
A worker wearing a protective face shield checks for open windows at a New York City Health + Hospitals COVID-19 testing site in Brooklyn in November of 2020. (AP Photo/Kathy Willens)
Sadr said. The New York health system is also still distributing Paxlovid for free through its ExpressCare hotline at 212COVID19 (212-268-4319).
The ExpressCare program has sent about 40,000 Paxlovid prescriptions as of April 2023, according to a spokesperson at Health + Hospitals. Nearly 43% of the hotline’s patients live in communities that the city’s Taskforce on Racial Inclusion & Equity has determined most impacted by COVID-19.
As PCR testing sites across the city close, healthcare providers have directed New Yorkers to utilize at-home, rapid tests instead. Health + Hospitals, for example, continues to distribute free at-home tests at a number of locations around the five boroughs, and will keep the program going as long as supplies last.
However, PCR tests are more accurate than the at-home tests, particularly as the coronavirus continues to mutate.
Elana Levin found out that she had COVID-19 this past December through a PCR test at a mobile site in her Brooklyn neighborhood of Sunset Park. The PCR result allowed her to isolate soon after her symptoms started, she said, while an at-home test she took the same day was negative.
sites also showed New Yorkers that they could easily access COVID-19 care if they needed it. These sites were highly visible, outdoors, and required no appointments; all of these qualities implicitly encouraged people to take advantage of the sites.
Their absence “will change the perception of access” to COVID-19 services, ElSadr said.
CLOSURES WILL WORSEN DISPARITIES
As the Health + Hospitals walk-in sites close and the federal health emergency ends, New Yorkers will have to work harder to get a PCR test if they need one. Health + Hospitals still offers free testing at its hospital sites, but patients now need to make an appointment for the service. They might need to make an appointment with a doctor, pay a $100 fee, or even risk COVID-19 exposure by entering a healthcare clinic to get tested, as outdoor options will no longer be available.
Many healthcare settings have also dropped their mask requirements after a statewide rule expired in February, increasing the risk that someone might get COVID-19 while seeking a test. The advocacy group Mandate Masks NY has compiled a list of organizations across the state that still require masks.
Jasmin Smith, a former contact tracer who lives in Brooklyn, worries that di-
it harder for people with existing health conditions to participate in common activities, like taking the subway or going to the grocery store.
COVID-19 safety measures “make the world more open to people like myself who are COVID-conscious and people who might be immunocompromised, disabled, chronically ill,” Smith said. “When those things go away, your world becomes smaller and smaller.”
The ending federal public health emergency has also contributed to widespread confusion and anxiety about COVID-19 services, El-Sadr said. “People have so many questions about this transition,” she said, and local leaders could do more to answer these questions for New Yorkers. The near future of COVID-19 care in the U.S. could reflect existing health disparities for other endemic diseases, like the seasonal flu and HIV/AIDS, Thrasher said. For example, people with insurance and a primary care physician are more likely to get their annual flu shots, he said, while those without are more likely to face severe outcomes from the disease.
After May 11, COVID-19 outcomes are likely to fall along similar lines. “More people have died of AIDS after there were HIV medications,” Thrasher said. “More people have died of COVID when there were vaccines in this country than before.”
COVID-19 services for people who need them most. This might include giving out free masks and rapid tests, requiring masks in crucial locations like healthcare settings, and improving awareness of COVID-19 and long COVID through public campaigns.
Some of the infrastructure built during COVID-19 may also be valuable in responding to other health crises. Health + Hospitals has maintained its ExpressCare hotline (631-397-2273), initially developed to provide COVID-19 services; New Yorkers can now contact this hotline 24/7 for a variety of health needs. According to the website: “For medical urgent care, self-pay patients will pay a flat $125, and insured patients will pay a copay amount based on their plan.” Health + Hospitals has a policy to not deny care to those who are uninsured and can help those who qualify sign up for coverage.
The mobile testing sites similarly provide a model for easily-accessible care in future crises. “We need to be meeting people where they are,” Blackstock said, whether organizations are providing COVID-19 tests, treatment for substance use disorder, or anything in between.
For additional resources about COVID19, visit www1.nyc.gov/site/coronavirus/index.page or call 212-COVID19. COVID-19 testing, masks, and vaccination resources can also be accessed on
May 11, 2023May 17, 2023 • THE NEW YORK AMSTERDAM NEWS 11 S
Continued from page S10 DECLINING ACCESS TO COVID-19 SERVICES WILL WORSEN HEALTH DISPARITIES

S AM News 01424 AM News 01524 AM News 01114 AM News 01434 AM News 01014 AM News 01124 AM News 01444 AM News 01024 AM News 01134 AM News 01454 AM News 01034 AM News 01144 AM News 01464 AM News 01044 AM News 01154 AM News 01474 AM News 01054 AM News 01164 AM News 01424 AM News 01064 AM News 01174 AM News 01484 AM News 01074 AM News 01184 AM News 01494 AM News 01084 AM News 01194 10/13/22 12/29/22 03/16/23 10/20/22 01/05/23 03/23/23 10/27/22 01/12/23 03/30/23 11/3/22 01/19/23 04/06/23 11/10/22 01/26/23 04/13/23 11/17/22 02/02/23 04/20/23 11/24/22 02/09/23 04/27/23 12/1/22 02/16/23 05/04/23 12/8/22 02/25/23 05/11/23
The Apollo Theater is closed due to the coronavirus pandemic but carries the message "Be Well," Thursday, April 16, 2020, in the Harlem neighborhood of New York. Most entertainment venues nationwide are closed during the pandemic. (AP Photo/Mark Lennihan)
