7 minute read
Ocular manifestations of


COVID & the Eye
Ongoing research seeks possible ocular connections. Howard Larkin reports
Since Li Wenliang MD first warned colleagues of a cluster of SARS-like pneumonia cases in late December 2019, ophthalmologists have been involved with COVID-19. Perhaps most urgently, Dr Li’s subsequent death from the disease, which he contracted from an asymptomatic glaucoma patient, dramatically illustrated the need for universal precautions to combat COVID19 in clinical practice.
In the months since, ocular manifestations of SARS-CoV-2 infection and COVID-19 have been the subject of much study. One recent review estimated the pooled prevalence of ocular manifestations at 7%, with SARS-CoV-2 confirmed present on conjunctival swabs by PCR tests at about 1% (Taiwan J Ophthalmol. 2020 Jul-Sep; 10(3): 153–166.).
However, other research suggests ocular involvement may be more common depending in part on how it is defined. For example, a standardised questionnaire of daily COVID-19 symptoms administered to patients served by hospitals in Strasbourg, Dijon, Nice, Brest and Colmar in France found that 36.7% reported ocular symptoms, and these were statistically associated with all major systemic manifestations, including flu-like illness, respiratory, neurological and digestive, said Tristan Bourcier MD, PhD, professor of ophthalmology at Strasbourg University Hospital.
“The symptoms reported by the patients resembled to a non-specific mild conjunctivitis confirming the possibility that SARS-CoV-2 targets ocular surface cells creating a potential entry portal. Moreover, SARS-CoV-2 has also been detected in the tears of COVID-19 patients suffering from conjunctivitis during illness,” said Dr Bourcier, who has been supporting patients with COVID19 acute diseases along with ICU and infectious diseases colleagues since the pandemic entered France early last year.
But while COVID-19 anterior infections could theoretically trigger corneal graft rejections, uveitis or neuritis episodes, the reality is different, Dr Bourcier said. “Most of the COVID-19 patients suffer red eye and eyelid swelling with or without discharge. In the very majority of cases there is no visual impairment neither anatomical sequels.”
This observation coincides with the clinical experience of José Güell PhD, Professor of Ophthalmology at Autonoma University of Barcelona, Spain, and Director of Cornea and Refractive Surgery at IMO Barcelona. But while he has seen many cases of diffuse conjunctivitis in COVID-19 patients, and these cases are often referred to him, he has yet to see a conjunctival swab positive for the virus.
Because these patients also are exposed to other eye-drying circumstances, such as spending much more time looking at computer and smart phone screens, and staying indoors, “it is really difficult to assign the cause to COVID”, he said. Generally, these cases resemble a mild viral conjunctivitis and respond well to low-dose topical corticosteroids. He is much more concerned with the risk of contagion for the staff in treating patients.
HIDDEN INFECTION Still, SARS-CoV-2 virus may be in the eye that cannot be detected by a conjunctival swab, said Ashok Kumar PhD, associate
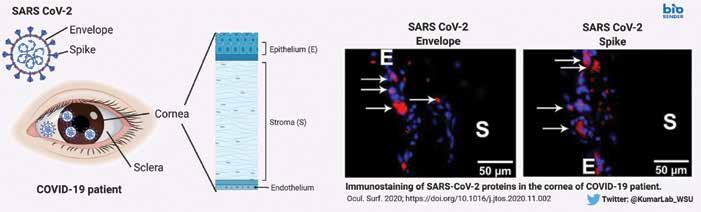
Schematic of corneal tissue indicating different layers and detection of SARS CoV-2 Spike and Envelope proteins in cornea of COVID-19 donor eyes.
professor in the Department of Ophthalmology, Visual and Anatomical Sciences at Wayne State University School of Medicine, Detroit, USA. Research in his laboratory on post-mortem ocular tissues of patients who died of COVID-19 found SARS-CoV-2 RNA on the posterior corneas (endothelial layer) of four patients and in the vitreous of one who was negative for the virus in the conjunctiva (Sawant OB et al. The Ocular Surface in press, online 8 November 2020).
Dr Kumar noted that no live virus has yet been isolated from ocular tissues, and suggested that conjunctival swabs taken later in the course of disease may be negative because the viral load drops off quickly. Indeed, four of the patients his laboratory examined who died of COVID-19 had no detectable viral RNA in their nasopharyngeal swabs. Virus was also detected in small numbers of patients who tested positive within two weeks of death who died of other causes. He emphasised the need to test tissues intended for transplant.
ROLE OF INFLAMMATION While both the conjunctiva and the cornea express the ACE2 receptors and Furin protease required for SARS-CoV-2 to enter cells, it remains uncertain whether the ocular surface could be another entry route, Dr Kumar said. One of the unique aspects of his study is the presence of SARS-CoV-2 viral antigens (i.e., Spike and Envelope proteins) in the corneal epithelium of COVID-19 donor eyes. This provides a stronger evidence than viral RNA detection and suggest potential susceptibility of ocular surface cells to SARS-CoV-2 infection. With colleagues at the University of California – Los Angeles, USA, he is conducting a study involving mice that express human ACE2 on the cornea to see if they can contract systemic SARS-CoV-2 infections through the eye, establishing a theoretical animal model for this transmission route. They are also examining the virus’ effect on cultured human corneal epithelial cells, particularly the induction of antiviral and inflammatory responses. These experiments are needed to conclusively prove or refute whether eye is a gateway for SARS-CoV-2 entry – he further added.
Sezen Karakus MD and colleagues at the Johns Hopkins Wilmer Eye Institute, Baltimore, Maryland, USA, are taking another approach to detecting whether COVID-19 can manifest solely or initially as an ocular infection. They are testing patients who present with viral conjunctivitis to determine how many are associated with the SARS-CoV-2 virus. Following these patients may also shed light on whether such infections remain isolated in the eye, or can develop into systemic disease. “If SARS-CoV-2 associated conjunctivitis is more common than we thought, patients presenting with conjunctivitis might need to be tested and isolated,” said Dr Karakus, who is an assistant professor of ophthalmology at the Johns Hopkins University School of Medicine.
While the involvement, if any, of SARSCoV-2 in the front of the eye mostly seem asymptomatic, however, the infection at the posterior segment of the eye may be a different matter, Dr Kumar said. In addition to his research with the cornea, he and his UCLA colleagues are examining how the virus affects retina and retinal cells using cell culture and animal models of SARS-CoV-2 infection, again looking for inflammation and antiviral responses.
While there is no current evidence of visual impairment resulting from retinal involvement in COVID-19, longer-term inflammation of retinal blood vessels “could lead to complications down the line”, Dr Kumar said.
RETINAL IMAGES AS DIAGNOSTIC TOOL Retinal blood vessel dilation associated with COVID-19 might also play a role in assessing the severity and stage of the disease, said Alessandro Invernizzi MD, assistant professor and head of the Uveitis and Ocular Infectious Diseases Service at the Eye Clinic – Department of Biomedical and Clinical Science “Luigi Sacco”, University of Milan, Italy. Research he conducted with other colleagues from the Eye Clinic, infectious diseases and emergency medicine departments found that both retinal veins and arteries were dilated in 54 COVID-19 patients compared with 133 SARS-CoV-2 negative subjects, and the degree of vein dilation significantly correlated positively with disease severity, and negatively with time from symptom onset. “If our data will be confirmed, retinal veins diameter could represent a useful parameter to monitor the inflammatory response and/ or the endothelial damage in COVID19,” the article said. (Invernizzi et al. EClinicalMedicine published by The Lancet, 20 September 2020.)
The group’s current research is focused on converting these preliminary findings into a clinical process that may be useful in predicting which patients will progress to severe disease, Dr Invernizzi added. “Just by taking a single picture of the fundus we can get a lot of information about the impact of COVID-19 on the vascular system. It’s quite early to say whether this will change the way we manage patients but there is a lot of potential.”
Dr Invernizzi’s study also found a higher than expected incidence of other retinal abnormalities in the COVID19 patients compared to SARS-CoV-2 negative subjects, including haemorrhages in 9.25%, cotton wool spots in 7.4% and tortuous vessels in 12.9%. While these findings were not disease specific and did not appear to compromise vision, they suggest an avenue for further research on the possible effects of SARS-CoV-2 on the retinal microvasculature. Further research is also needed to determine whether the blood vessel dilation observed was directly due to the virus or the product of a massive systemic inflammatory response, he said.
One thing his findings do suggest is COVID-19 patients should have a fundus examination, Dr Invernizzi said. “Most of these patients were not complaining of ocular symptoms. We cannot really rely on patient complaints to tell whether it is worth screening their fundus.”







