
12 minute read
Imaging Technology


By Scott R. Gourley
FEW AREAS OF MILITARY MEDICINE are evolving faster and more dramatically than medical imaging. And few locations reflect this evolution better than Brooke Army Medical Center (BAMC) in San Antonio, Texas. Comprising 10 separate organizations, BAMC has been described as “the Flagship of Army Medicine.” In addition, ongoing coordination with both veteran and civilian medical facilities provides BAMC practitioners with a unique perspective across a broad spectrum of medical care.
In terms of medical imaging, Col. James Wiedenhoefer, USAF, chief of BAMC’s Department of Radiology, points to “the full scope of radiologic services” and related imaging technologies.
“We span everything from the most basic, which is just plain film, to some of the more complex nuclear medicine and MRI [magnetic resonance imaging] imaging,” he explained. “So we do plain film, ultrasound, CT [computerized tomography], MRI, and nuclear medicine imaging, some of which is fused with cross-sectional imaging such as CT. And along those same lines, we also do interventional radiology work with angiography, fluoroscopy, and mammography.”
Elaborating on the example of mammography imaging, he offered that it uses “basic X-ray technology” that has been “modified slightly and specifically for imaging breast tissue.”
He noted that recent mammography developments at BAMC involve the introduction of 3-D breast tomosynthesis, which applies computer technology to achieve 3-D imaging of the breast tissue, which he characterized as a significant enhancement over “plain film 2-D imaging.”
Wiedenhoefer pointed to CT scanning as “the workhorse” of imaging at BAMC, largely due to the fact that “it’s quick and it’s detailed.”
“With our radiology services, we probably do more here than anywhere else in the DOD,” he said, adding, “and we have a lot of specialty applications that we also use for both CT and MRI.”
Asked for an example of those specialty applications, he pointed to “functional cardiac MRIs.”
“That’s basically like looking real time at the function of the heart, while using MRI,” he said. “And that’s been a big thing added just in the last year, where we’ve been able to identify disease states that we previously couldn’t.”
He pointed to the recent example of a service member who was attempting to reclassify specialties to become an air traffic controller.
“Through our functional MRI program, we found a condition that’s called cardiac non-action, which is basically where the heart muscle isn’t as dense as it should be and predisposes this kid to be like one of these cases of just sudden cardiac death in a young person. … Our functional MRI program has allowed us to identify some of these cases and really make a big difference,” he said.
Col. Kyle Walker, MC, USA, chief of Diagnostic Radiology and Trauma/ER Radiology at BAMC, highlighted the use of dual-energy CT, identifying it as “where different strengths of photons are utilized to characterize specific types of pathology and actually render a specific diagnosis.”
Walker said that the amount of patient radiation exposure in CT scans “is always an issue,” and that it is always addressed through practice of the “as low as reasonably achievable” (ALARA) radiation principle.
“ALARA means balancing the amount [of radiation] given versus the optimal diagnosis,” he said. “In reality, the equipment does a lot of that for us because it basically modulates the strength of the beam based upon the thickness of the person. But we’re also cognizant of that with the techniques we pick and the number of times a patient is scanned. So the fact that we have modern equipment really cuts down on the dose given. “But every dose that’s administered is actually documented with the scan,” he added. “It’s part of the medical record. It’s accessible and can be quantified.”
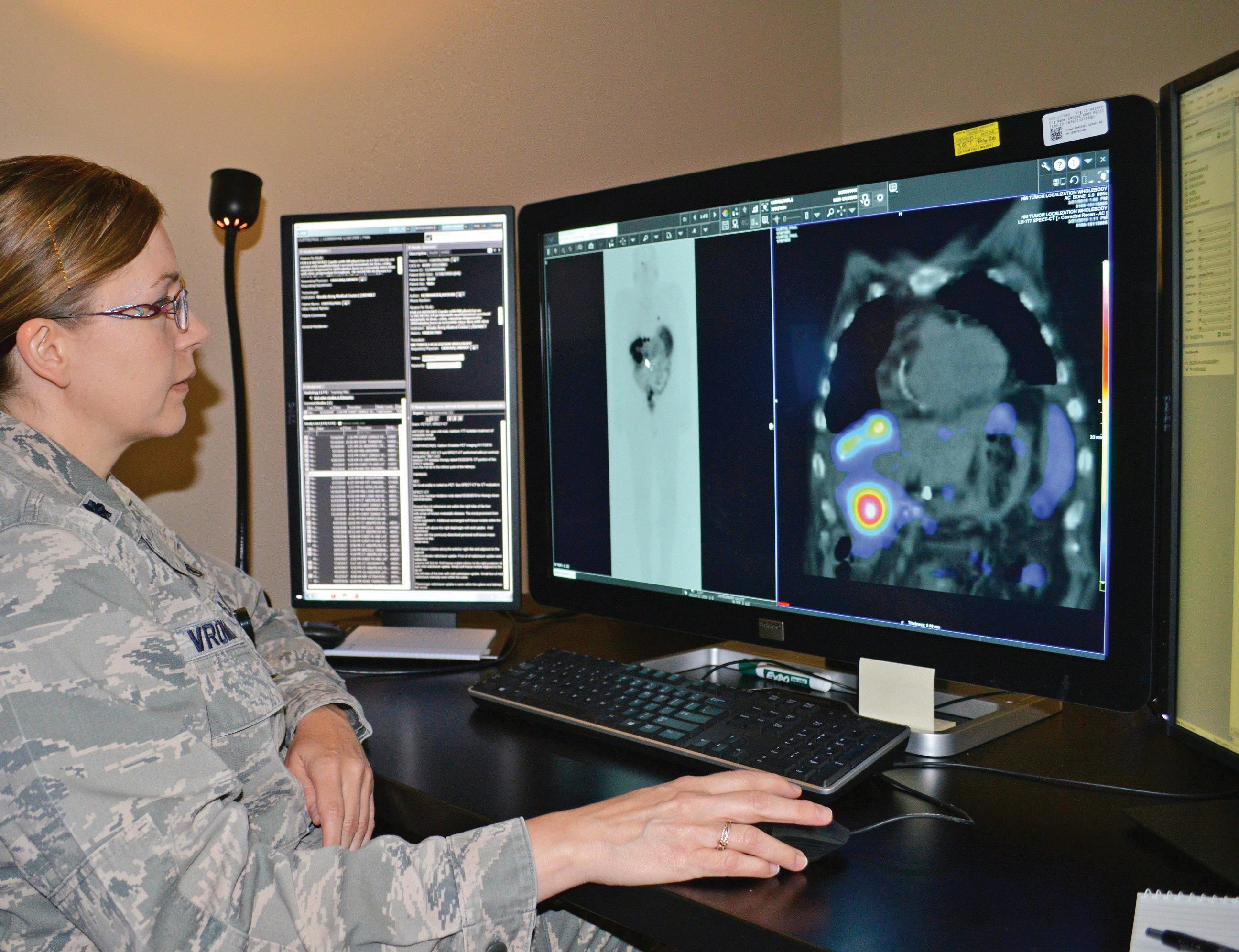
Air Force Lt. Col. Penny Vroman, Brooke Army Medical Center Nuclear Medicine Department chief, looks at scans of a patient with neuroendocrine tumors June 26, 2019, to ascertain if a radiopharmaceutical that was administered is targeting the tumors.
In parallel with this documentation, BAMC plans to acquire new software that will monitor and track the amounts of radiation doses on patients that may be reoccurring into the system. Walker said that the recent introduction of new CT technologies at BAMC didn’t change employment of the technology but did serve to make CT scanning more efficient.
“That’s because the new technology takes advantage of a wide number of detectors on the scanner, which means virtually half of the dose is administered for each scan, with computer programming basically reconstructing the other part for us,” he said.
In addition to reducing radiation dosages, Walker offered that another advantage is the ability to get very detailed information on complex anatomic structures that would otherwise be susceptible to motion.
“The best example of that is the heart. I mean, we can essentially freeze the heart with a heartbeat and be able to visualize all the detailed anatomic structure,” he said. “That also goes for the brain, for the solid organs, and for the gastrointestinal tract.”
advertisement
Walker described BAMC as “on the cutting edge in the sense that we actually use alternative imaging techniques for fertile-age females,” stating, “For acute abdominal pain, for example, we use a lot more MRIs than are used in the civilian sector to diagnose those disease processes rather than exposing them to radiation with CT. And that’s also true with kids.”
Noting his own background as an obstetrician-gynecologist with a fellowship in women’s imaging, Wiedenhoefer echoed those sensitivities to radiation exposure for fertile-age females, adding that other recent changes include new breast biopsy techniques that utilize the Affirm ® breast biopsy system, which allows patients to sit upright during the procedure.
“So we’re applying many of the technologies that we have had in the past,” he said. “We just have better equipment.”
Reflecting on coordination efforts between BAMC and the Veterans Health Administration (VHA), Walker highlighted the area of interventional radiology.
“We treat a lot of the patients with the Y90 Radioembolization,” he said. “Basically they have liver cancer and they can have an endovascular treatment for their liver cancer that has a relatively low side-effect profile and pretty good efficacy. And that’s a good joint venture. Those collaborations occur, but it’s kind of more driven by the subspecialists that are out there rather than us specifically. But we do collaborate with them frequently.”
While acknowledging that cooperation, Wiedenhoefer offered his personal belief that there is room for improvement.

Cardiac magnetic resonance imaging technologists observe a patient during a cardiac MRI scan at Wilford Hall Ambulatory Surgical Center, Joint Base San Antonio-Lackland, Texas. Cardiac MRI is noninvasive, takes approximately 20-45 minutes, and enables an assessment of the function and structure of the heart.
“We had a case just recently where someone from the VA reached out to us to try and help acquire some imaging for an inpatient at the VA,” he explained. “They didn’t have a table that was able to support the weight of the particular patient. And we were working with them, trying to coordinate getting the patient over here. But it didn’t work out for that particular incident, meaning that they just ended up taking them over to university hospital. However, there are more and more circumstances where we’re trying to cover all of San Antonio and all of these military-related components working better together to take care of our patients.”
Looking at the possible evolution of imaging technologies over the next five years, Lt. Col. Nathan E. McWhorter, DO, a nuclear medicine physician at BAMC and assistant professor of radiology at the Uniformed Services University of the Health Sciences, pointed to the hope for the release of new “theranostic” imaging and treatment agents.
“Theranostic combines the words ‘therapy’ and ‘diagnostic’ into one word,” he said. “We call it a radiopharmaceutical, where it’s just designed to target a specific type of tumor. And you can put one type of radioactive particle on it, inject it into the patient, and then do imaging. And then, once your diagnosis is made and that this patient indeed has that treatable type of cancer, then we put a different type of radioactive particle on the exact same radiopharmaceutical – you can just think of it as a medication, really – and it goes in the same way by injection and kind of bombards the tumor from the inside while the patients just kind of sit there in the chair and really don’t feel anything.”
McWhorter said that BAMC currently uses a theranostic called Lutathera ® , offering, “Our hospital was the first to do this in the DOD and the first here in San Antonio as well. It’s for a specific type of carcinoid tumor, where we have the agent, the best type of PET [positron emission tomography] imaging for diagnosing it, and can categorize where the disease is throughout their body. Then from that, we follow up and treat them with a very small radioactive dose of a medication.”
He continued, “This was a huge breakthrough. We’re at a new age in nuclear medicine. In fact, there’s hopefully another type of theranostic coming up for treating prostate cancer. It’s under research right now, but it’s showing some very promising results. And as it achieves FDA approval, we will be looking to adapt that capability very quickly.”

advertisement
In his own perspective on future developments, Wiedenhoefer noted an expansion of breast-specific gamma imaging to look at metabolically active breast tumors as well as the use of elastography, which can be applied in both MRI and an ultrasound to assess the stretchiness, sponginess, or compressability of an organ.
“We’re doing that with ultrasound and with MRI,” he said. “And that helps lower the number of biopsies that need to be done for these tissues and may actually reduce the number of invasive diagnostic tests that need to be done.”
However, Wiedenhoefer was quick to assert that few areas hold greater promise than the introduction of new information technologies (IT).

U.S. Air Force Airman 1st Class Faith Brown, a diagnostic imaging phase II student assigned to the 6th Medical Support Squadron, uses the brand-new General Electric Revolution HD computed tomography (CT) machine at MacDill Air Force Base, Florida, June 13, 2019. The images produced during scans from the new CT machine are more detailed than before, allowing radiologists to better diagnose more patients.
“Everything is computer-based now,” he observed. “It’s all ones and zeros. It’s no longer a photograph. It’s all digital information. And because of that, it can be transmitted over much larger distances and manipulated better. We’re merging more and more of that and our doctors are working more and more together. We’re covering a larger scope of things, and really trying to consolidate those, with the hope that in the next five years what is now limited to San Antonio could be more throughout CONUS and the world, where these subspecialty radiologists like Dr. McWhorter or Dr. Walker can actually provide support to other places just by sending the images to them.”
As the chief of the Informatics Division in the BAMC radiology department, Rik Guinther was also quick to highlight digital benefits ranging from the continuity of information from the battlefield to a reduction in medical errors or misdiagnoses.
“The digital information is also important in 3-D reconstruction,” Wiedenhoefer echoed. “In fact, just this past week, Rik Guinther and his team were working with the maxillofacial surgeons here. The current technology that we have allows us to do better 3-D reconstructions and allows them to do their surgery better. Orthopedics is similar. They can do a lot of 3-D reconstructions just to make sure that alignment of joints and so forth, and fracture planes, are well visualized and conceptualized before they go and take them to do surgical repair.”
The same imaging technologies and approaches that hold so much promise also present new challenges for the medical community. One of those challenges involves what some might see as information overload.
Wiedenhoefer explained that 10 or 15 years ago, a CT scan of the head involved 16 images reflecting slice thicknesses of 1-1.5 centimeters.

Ezra Poetker, radiology informatics system administrator, monitors radiology information systems for irregularities at Brooke Army Medical Center, Fort Sam Houston, Texas, Oct. 4, 2019. Radiology Informatics supports all radiology sections and is essential in the interpretation of more than 275,000 patient studies each year.
“But now the slices look at every millimeter, and that same exam might result in 2,000 images. And they all need to be looked at. So it’s easier for us to acquire images at a lower radiation dose, but yet they become more complex in the interpretation of them.”
He added, “Right now, when we have a trauma patient come in, they’ll get a head CT, neck CT, and CT of aorta, chest, abdomen, pelvis, cervical spine, thoracic spine, and lumbar spine. When one person comes through, they may easily have 10,000 images for radiologists to look at. With that same patient 10 years ago, it would have been 115 images – maybe. So patients are coming through and the radiologists are having to read, in an eight-hour shift, maybe 130 exams or more. It’s really getting to a point where they may not be able to get through all the images. So, from that standpoint, we are better and better, but we also have a ton more to do. And it’s getting to the point where we are maxed out in what we can get through in the interval of time.”

advertisement
Moreover, Walker pointed out that the reality for radiologists reading that imagery is that it is a 24/7 requirement. “It never ever stops,” he said. “And the problem is the complexity doesn’t change regardless of time of day or night. So a big challenge is having personnel to keep up.”
“That’s absolutely true,” Wiedenhoefer added. “And that person has to be skilled enough to do the work and to get through it. And that’s going to continue. The technology is going to continue to get more complex.”
He referred to the application of new IT “imaging modalities,” and BAMC’s use of systems called Vitrea and TeraRecon, to break the CT scans into individual elements.
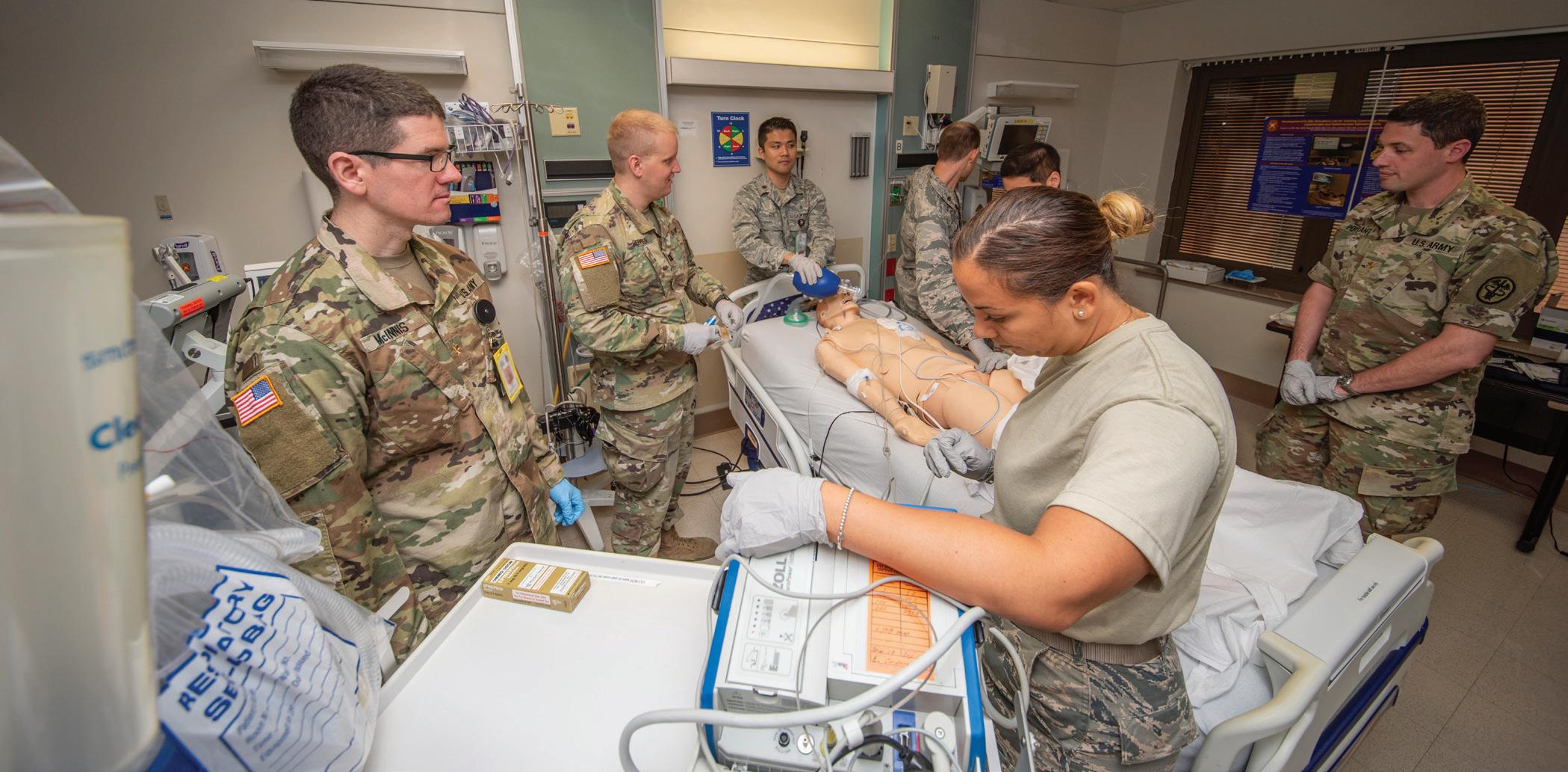
Army and Air Force doctors assess a simulated trauma patient at Brooke Army Medical Center, Fort Sam Houston, Texas, Sep. 4, 2019. A trauma patient today might generate 10,000 images for a radiologist to look at.
“So if we were interested in just looking at the bone or looking at the heart or something, we can take that and then do 3-D reconstructions of that thing,” he explained. “Nuclear medicine does this a lot with cardiac exams. But then it requires somebody skilled enough to do all the post-processing in order to make usable information out of that. … It takes some really skilled people to do it. And meanwhile the patients are coming through faster than we’re able to even do the processing.”
In addition to the processing, Guinther highlighted associated IT challenges based on both digital storage and the bandwidth necessary to open the images to other providers and other hospitals as necessary.
“We went from 16 images on a piece of film to a couple of thousand digitally and now we’ve got to transfer these to another hospital or to other workstations around the hospital,” he said. “So storage becomes a big issue as we continue with digital mammography and those types of things. That’s one of our biggest challenges on the IT side, just to make sure that we keep up with the amount and volume of information that we acquire, and to present it back to the radiologist in a timely fashion. And it’s not just radiologists today; it’s anybody that needs to see that image. And that can be hundreds of clinicians a day viewing thousands of studies.”
Wiedenhoefer closed with acknowledgement of one more potential issue hovering on the digital horizon.
“I have read about, and we haven’t had any direct issues here, but one thing I could see becoming a problem in the future involves malware and viruses incorporated into imaging systems,” he said, “because it’s all computer software now. And there are reports actually of people who have added malware and viruses into the system that then falsely place tumors into organs. So people get cross-sectional imaging and they’re interpreted as a tumor, when in reality it isn’t a tumor. It’s a virus that’s intentionally in there to look like a tumor. They insert false tumors into these things to wreak havoc within the systems. Again, we haven’t had any issues with that, to my knowledge, but they are out there.”





