
10 minute read
VA Prosthetics: Status and Advances


By J.R. Wilson
ANCIENT TEXTS – POETRY, HEROIC TALES, HISTORIES – make reference to prosthetic limbs dating back as far as 1500 B.C., although the oldest physical evidence is an artificial leg dated at around 300 B.C. Unearthed at Capua, Italy, in 1858, the bronze and iron device, with a wooden core, appears to have been used after a below-the-knee amputation.
For the next 1,500 years, little progress was made and prosthetics primarily were cosmetic in nature, aside from those designed to help a horse-mounted knight hold a sword or lance. The only “advances” were the development of the peg leg and hook hand during the “Dark Ages” (476 B.C. to 1000 B.C.).
The Renaissance (14th-17th centuries) saw a renewed emphasis, based on resurrected Greek and Roman medical texts, to fit amputees with more functional prosthetic legs and hands, most made of iron, steel, copper, and wood. Increased functionality and lighter, more adaptable materials led to the first real advances during the 16th century. The next three centuries saw incremental improvements in articulation, materials, and functionality, but artificial limbs essentially remained little more than “placeholders” for the amputated limbs.
It was not until post-World War II military amputees began demanding greater functionality that researchers again improved the weight and durability of prosthetics and, with the development of transistors and microprocessors, began the modern evolution of technologically advanced components and systems.
While significant advances were made in both design and functionality from 1950 through the post-Desert Storm era of the 1990s, all of the factors for a “perfect storm” in prosthetics – from smaller, faster electronics to advanced new lightweight materials to high demand to strong public support – came together at the turn of the century and the beginning of America’s longest war in Southwest Asia.
Improved, ubiquitous body and vehicle armor, universal basic medic training for all warfighters, medics trained to EMT levels, and the presence of surgical teams on the front lines made Operation Iraqi Freedom and Operation Enduring Freedom (Afghanistan) the lowest killed in action (KIA) conflicts in history. But they also led to more amputations and more major loss of limb functionality than at any time since the U.S. Civil War.
The Department of Veterans Affairs (VA), the Department of Defense (DOD), and civilian academic and medical research facilities all are involved in – and cooperating with each other on – the constant advancement in prosthetics, especially lower limbs, arms, and hands, the latter being by far the most difficult. Prosthetic legs have advanced to the point where some wounded warfighters, told advanced battlefield care has saved their legs – but with only 80 to 90 percent of the functionality they originally had – have asked DOD or VA surgeons to amputate and give them the latest prosthetic leg, which may offer more than 100 percent of a natural leg’s functionality.
Even so, artificial legs still are not perfect, with different people experiencing different levels of pain and difficulty adapting to them.
Although the number of U.S. warfighters now deployed to Southwest Asia is only a fraction of those there at the peak of the war, interest in further prosthetic technology development and funding for it has remained relatively stable, as has the pace of research, development, test, and evaluation (RDT&E). “Some areas are moving faster than others at different points in the development pipeline,” according to Brian Schulz, PhD, scientific program manager, VA Office of Research and Development. “Multigrasp hands have come a long way, microprocesser knees and ankles have made advances. Most [of those advances] have been on the inside [of the prosthesis], such as neural interfaces and a lot of surgical techniques that show immense promise for the future.
“It’s more a steady process of small advances than a big leap. There are some things on the cusp, such as modular implantable neural prosthetic systems that interface the nerves with the prosthetic limb. That doesn’t have full FDA [Food and Drug Administration] approval yet, but once it and others are approved, they will come together in the future to enable much more capability.”
The level of funding and research, combined with advances in other technologies that are applicable to improving some part of prosthetic development, such as smaller, faster microprocessers, also have led researchers to take another look at ideas previously shelved because all of the necessary technologies were not there to support them.
“A fair amount of funding has gone into trying to improve the socket interface due to the discomfort and skin issues prosthetic users experience. Despite a lot of effort and some incremental advances, I don’t think we’ve really solved the intended issues, which is why some of the internal efforts have become more attractive,” M. Jason Highsmith, PhD, national director, VA Orthotic & Prosthetic Clinical Services, told Veterans Affairs & Military Medicine Outlook. “There may be some additional things [impacting the future evolution of prosthetics], such as the concept of wearable technology. Another is the smartphone, where you can connect to an app to make an adjustment.”

Despite great strides in prosthetic technology, especially since the turn of the century, the process of adapting to and property fitting prosthetics can still be challenging.
The vast majority of military amputees from Southwest Asia have been in their late teens or early 20s, raising another concern for researchers and clinicians.
“These largely impact the younger end of the spectrum, and we don’t really have a good handle on what will happen as they grow older,” Highsmith warned. “We need more studies.”
That is one reason it takes so long to move a new technology or prosthesis from the lab to the FDA to the wounded warrior. And the amount of red tape involved will only increase as researchers seek to link new levels of prosthetic electronics to the human nervous and muscle systems.
That is why translating implantable and invasive systems to market is slower than developing the enabling technologies.
“So many advances in the lab look promising, but take so long to get out to the patient. Any implantable device requires full FDA approval as a Class 3 implantable device, which is far more difficult,” Schulz said. “Some level of red tape is necessary because these are invasive devices, but they also are a hurdle we have not had to get past with simpler external devices.
“The implants would be permanent, with the prosthetic attaching to it. The problem there is you have a hole in your skin with metal coming through it that could be an avenue for infection.”
This slower, more difficult process also will have an impact on public perception and the expectations of amputees. Advances in artificial limbs, especially legs, have been so fast and dramatic since the turn of the century that those outside the development chain have come to expect new, sci fi-level capabilities on a regular, fast-track basis. Lately, however, new technologies under investigation are facing a much longer and more rigorous approval cycle before becoming commercially available.

advertisement
Which is not to say there are no exceptions, the most notable of which is the LUKE Arm, under development for the past 15 years by DEKA Research & Development Corp., a New Hampshirebased company founded by Segway inventor Dean Kamen. Named for the prosthetic hand given Star Wars hero Luke Skywalker after a light saber battle with Darth Vader, it became the first invasive prosthesis approved by the FDA in May 2014.
The arm translates signals from the wearer’s muscles to perform multiple complex, simultaneous, powered movements. Individual motors in the wrist and fingers enable it to adjust its positions to perform six different user-selectable grips, while force sensors allow precision control of its grasp.
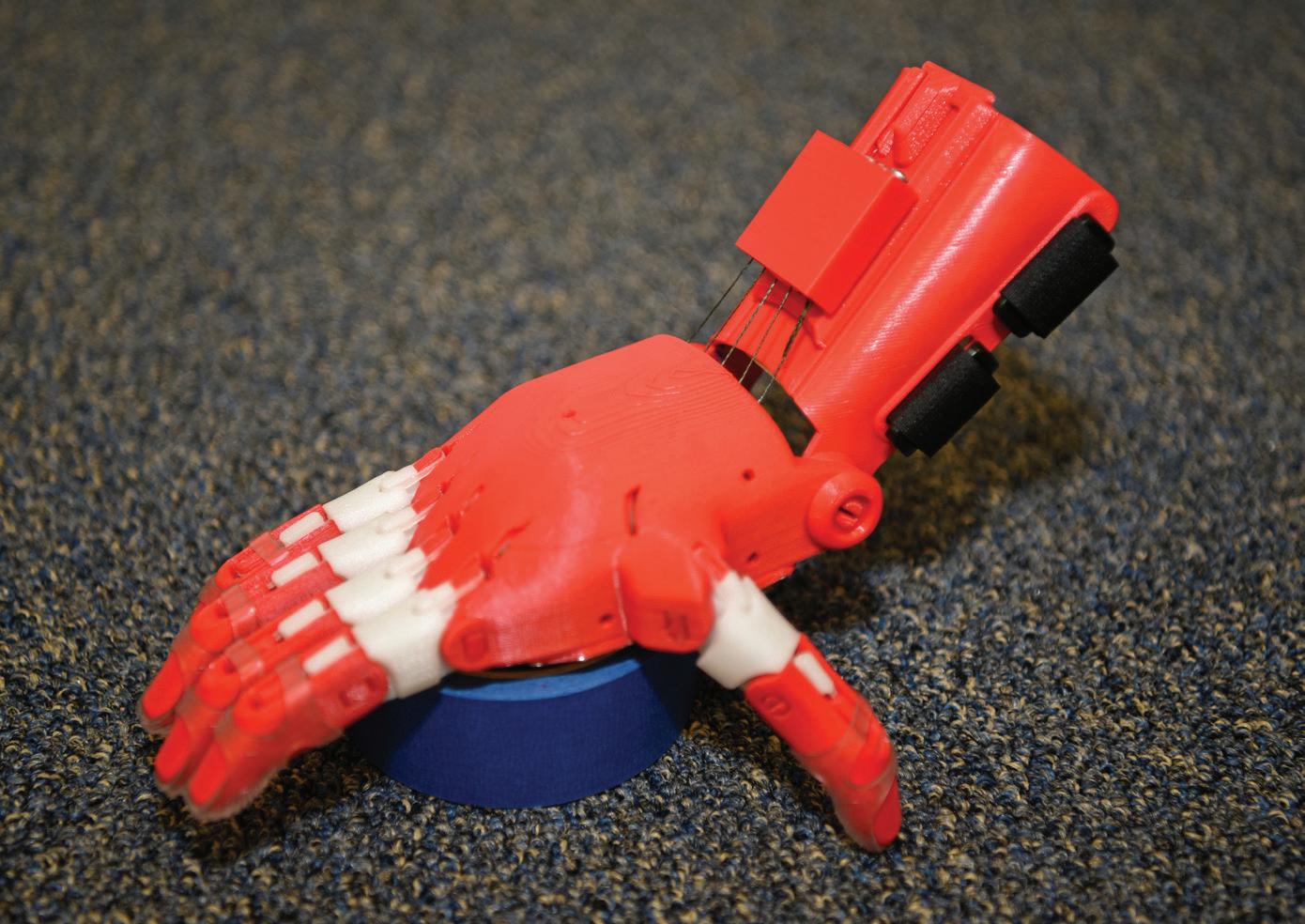
A prosthetic 3-D printed hand is made by Tech Sgt. Zachary Zilm, 582nd Operation Support Squadron NCO in charge of group training, July 3, 2018, on F.E. Warren Air Force Base, Wyoming. Zilm works through the organization Enabling the Future, a global network of passionate volunteers using 3-D printing to give the world a “helping hand.” The hands go to children who do not have the option for traditional prosthetic devices. Additive – or 3-D – printing and the ways it can potentially be used to improve care for patients with prostheses is of great interest to the VA.
Continuing development of the LUKE Arm also has given the wearer a rudimentary sense of touch by tying sensors in the artificial fingers to nerves at the point of amputation. Special software translates the signals to mimic those coming from a real hand, enabling the patient to “feel” and send signals back to the hand with the appropriate movements and pressure to open an envelope or pick up an egg without breaking the shell.
Hands and feet/ankles are the most difficult to replicate, although feet/ ankles, when part of a complete leg prosthetic, have shown significant improvement in recent years.

Utah Gov. Gary Herbert meets with Enduring Freedom and Iraqi Freedom veterans Ed Salau, left, and Bryant Jacobs, right, in February 2016 at the VA Salt Lake City Health Care System. In December 2015, Salau and Jacobs became the first Americans to undergo surgery – part of an FDA-approved study – to receive percutaneous osseointegrated prostheses (POPs), titanium implants in their residual limbs to which prosthetic limbs attach.
“The anatomic level of amputation matters greatly, especially what happens at the foot level versus the legs. Prosthetic feet began moving out in the 1990s, and in the last decade and a half, we’ve seen powered feet and ankle systems and microprocessor knee systems. Upper limbs also have incorporated more of those during that time, reintegrating large muscle groups to have more control over the terminal device, such as a hand,” Highsmith noted.
“A lot of advancements have been made in a lot of areas. Sadly, the partial foot amputation problem has not moved as much as other areas. There were some advancements a decade ago, but nothing recently. The other levels have seen significant advancements, but there is always both an up and downside, in terms of cost, training, pain, etc.”
Research to advance and improve the sense of touch and balance – which are closely linked in feet and legs – reduce pain, and give the patient a greater sense of “wholeness” remain primary goals in improving the patients’ ability to reintegrate into their routines and lives.
As with many new technologies, an advance in one area often leads to advances in others. Such is the case with sensor restoration for lower-limb amputees. Schulz said the same technology could be used to restore sensation in neuropathic feet, a growing problem among veterans.
advertisement

advertisement
advertisement
The success of any new technology also depends on determining the best balance between accommodation and training.
“Folks have been paying more attention to this, looking at how much training is actually needed to fully and maximally use these technologies and be sure you’re actually studying the patient’s utilization to see if there is a real difference between the current technologies and previous technologies,” Highsmith said.
“Some higher technologies may be issued without proper training, and we’re very interested in making sure if we are going to issue technology that has novel features, the patient is getting the training to understand what the technology is capable of and how to properly use it. That could be understanding specific modes, for example, such as running or climbing.”

The LUKE Arm prosthesis translates signals from the wearer’s muscles to perform complex, simultaneous, powered movements. In May 2014, it became the first invasive prosthesis to receive FDA approval.
Other fast-evolving technologies not directly related to prosthetics also will have an impact on future VA and DOD efforts to improve patient care. One of those is additive – aka 3-D – printing.
“From a material science perspective, conventional methods and materials will likely be a strong product, but we have a number of clinicians who use this technology to make their delivery of care more efficient,” Highsmith said. “That may not be the actual product, but check-fits along the way.
“There could be lots of different ways to integrate 3-D printing, and we don’t want to limit what our clinicians can imagine for using these techniques. We have a group looking at where these tools are around the network, how many clinicians are using it, what it is doing for practice in the VA. It’s of great interest.”
The materials available for 3-D printing today are not of sufficient quality for the rigors of a prosthetic limb, but new, stronger materials are being developed at a fast pace. And there are some applications where current materials might play a role.
“There are some circumstances where having a softer material is better, such as printed airsoles that are softer in some areas than others,” Schulz noted. “Another group is looking at 3-D printing methods that would allow women to wear high heels, which standard prosthetics are not designed to do.”
Mechanical and biomechanical orthotics are not likely to be the only avenue of treatment for amputees in the future. Transplants of hands or feet, for example – not from another person but using replacements grown in the lab from the patient’s own cells – also are a growing part of 21st century medical research as is regeneration, where the body is stimulated to regrow a severed part. But both are far behind mechanical and even biomechanical prosthetics.
“Hand transplants will improve as technology and immune suppression improve, but in the forseeable future, it’s too difficult a problem to really take over. It can be done, but not without challenges and setbacks,” Schulz said. As to what will be the dominant approach by mid-century: “I would say neural mechanical, increasing integration with our neural system. Possibly with some elements of regeneration.
“The future will see better integration of bio, improved control, improved neural interfaces, better skeletal attachments, more durable, commercial external components. Many of these advances can be used together to restore a limb. When people can feel, they tend to call it ‘their’ hand, not the ‘prosthetic’ hand.”





