2 Application of Duplex Ultrasound in Conjunction with Computed Topography Angiography to Identify Native Carotid Artery Stenosis
Evan Bair, Evan Ryer, and Gregory Salzler
11 The Impact of Race, Socioeconomic Status and Fragmented Care on Textbook Outcomes in Rectal Cancer
Olivia B. Granja, Theresa Koch, Madison B. Gladfelter, Ayobami M. Fatunmbi, Shengxuan Wang, Rebecca L. Hoffman, and Joseph A. Blansfield
17 Interprofessional Communication in Healthcare Systems: Analysis and Solutions
Yousef Raslan Hakim, Yonis Hakim, and Ali Abdelhady
20 A Two-Year Prospective Study on Medical Student and Mobility Specialist Intervention on Patient Mobility
Christopher D. Manko, Tyler Zlupko, Benjamin Krouse, Dylan Bertovich, Burke Beauregard, Shuyi Chen, Tyler Depalma-Shields, Marc Incitti, Stephanie Miller, Susan Sinay, Keiran Soprano, and John Pamula
25 Effects of Antipsychotics on Brain Structure in Patients with Psychotic Disorders
Daniel J. Seok, Maneesha Thomas, Pranav K. Selvan, Sonal Arora, John S. Yoo, and Brian J. Piper
30 Effect of Bilateral Truncal Vagotomy at the Time of Primary Roux-En-Y Gastric Bypass on Postoperative Marginal Ulcer Rates
Benjamin J. Smith, Mark Mahan, Vladan Obradovic, David Parker, Alexandra Falvo, James Dove, and Anthony T. Petrick
37 Induced Pluripotent Stem Cell (IPSC) Therapy: A Novel Method to Treat Degenerative Diseases?
Maria Y. Tian
46 Construction of a Patient-Empowering, Financially Sustainable Implementation Framework in the Emergency Department: Geisinger ProvenCare Pneumonia
Niraj Vyas, Mark White, and Chadd Kraus
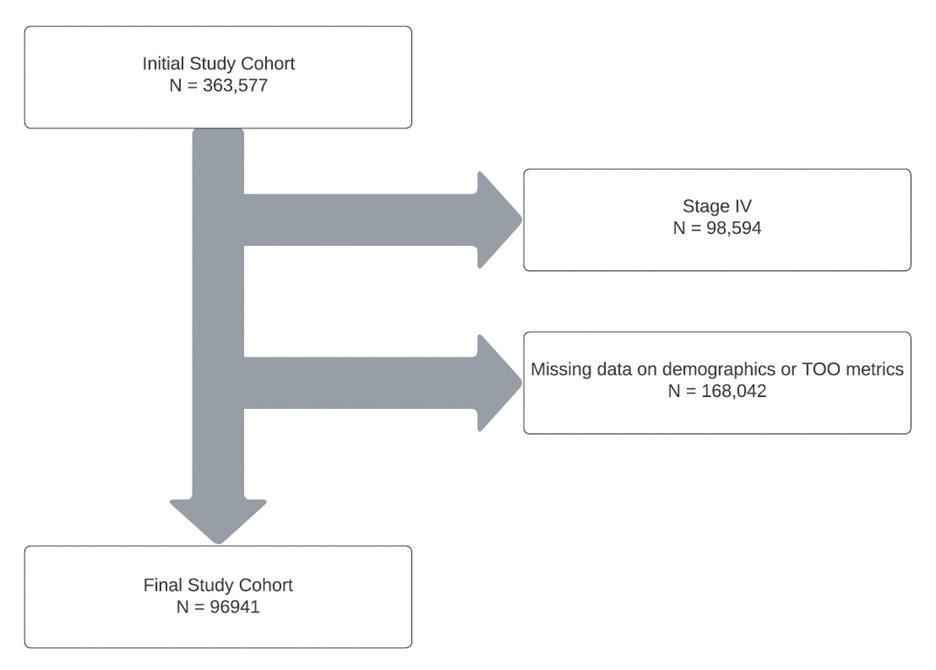
56 Impact of Fragmented Care on Survival and Textbook Outcomes in Rectal Cancer: A NCDB Study
Theresa Koch-Tran, Madison Wivell, Olivia Granja, Ayobami Fatunmbi, Shengxuan Wang, Rebecca Hoffman, and Joseph Blansfield
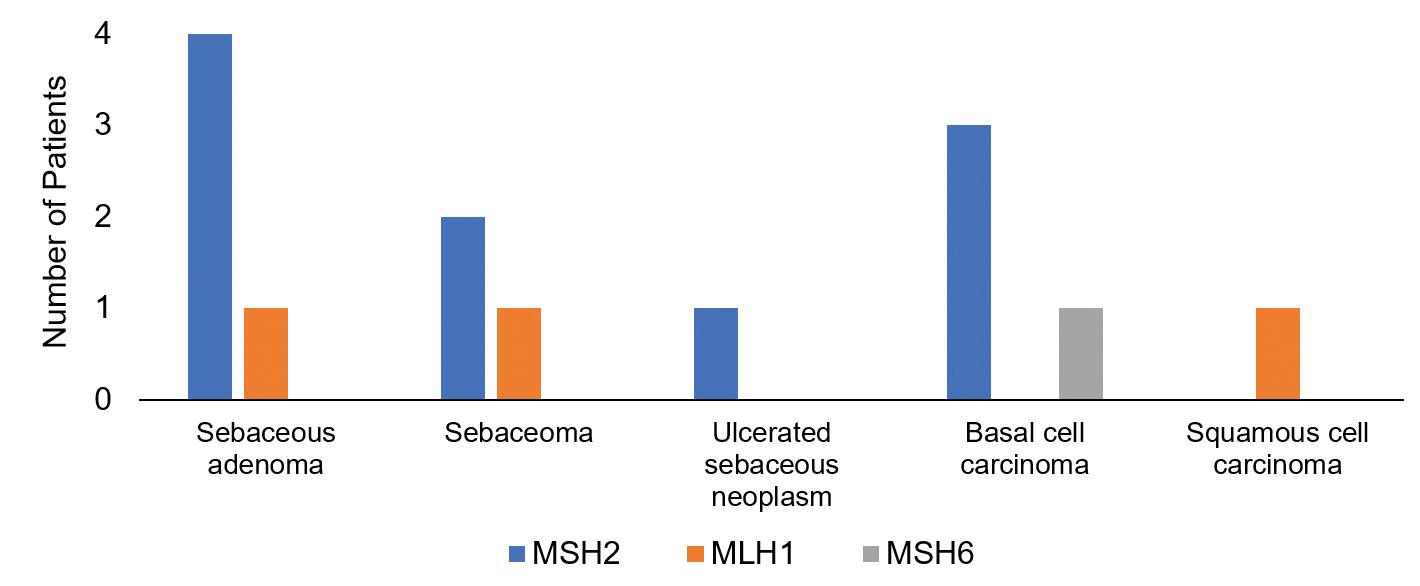
65 An Analysis and Outcomes of Skin Cancer Screenings Among Lynch Syndrome Patients in Geisinger’s Inherited Gastrointestinal Malignancy Clinic
Alexandra Yudiski, Heather Rocha, Matthew Dzeda, Edward Liu, Olivia Granja, Nicholas Haynes, Hannah Wooley, Shane Conklin, Cassandra Pisieczko, Kaitlyn Sweeney, Amanda Leicht, Thomas Moreland, Bradley Confer, and Heinric Williams
69 2025 Summer Research Immersion Program
70 Medical Research Honors Program
71 Finding your way: Opportunities for student funding
72 Cover art submissions
A message from the editor-in-chief
Welcome to the eighth edition of the Journal of Scholarly Research in Progress (SCRIP). As the editor, I am pleased to present this latest compilation of scholarly work, showcasing the dedication and passion of our talented students at Geisinger College of Health Sciences.
This edition features articles by recent graduates of the Medical Research Honors Program (MRHP)—Evan Bair, Niraj Vyas, and Benjamin Smith. These students undertook hypothesis-driven, long-term research projects intended to develop their competence in a topic not specifically taught in medical school. Starting in their first year, they conducted research under the guidance of a mentor and advisory committee, gaining independence and building their professional network throughout the four-year program. Upon successfully defending and submitting their final theses, they graduated from Geisinger Commonwealth School of Medicine with distinction in research. In total, 11 medical students from the class of 2024 have graduated from the MRHP. Collectively, their theses, modeled after scientific manuscripts, were submitted to SCRIP or other scholarly journals.
Excitingly, SCRIP will now be more accessible to the scientific community as we transition to the open-access Scholastic publishing platform. Our new website (scrip.scholasticahq.com) optimizes articles for online reading, mobile-friendly pages, social media integration, and enhanced discoverability through online browsers and indexes. This transition will elevate the scholarship of our students and aligns with our commitment to advancing knowledge and supporting our students’ academic and professional growth.
I extend my sincere appreciation to the dedicated students, mentors, reviewers, and our marketing, communications, and design team who have made this edition possible. I hope this journal, focused on student research, embodies the spirit of inquiry and scholarly excellence that aligns with Geisinger College of Health Sciences’ strategic plan to transform health through research, inspiration, value, and education. Suggestions from our contributors and readers to further develop or improve the journal are more than welcome; if you’d like to share your thoughts, email me at slobo1@geisinger.edu.
Sincerely,
Sonia Lobo, PhD, RYT Editor-in-Chief
Student editors
Carolyn Young, MD Class of 2026
Christopher Manko, MD Class of 2025
Niraj Vyas, MD Class of 2024
Jaclyn Podd, MD Class of 2024
Marketing, Communications, and Design
Jessica L. Martin, Managing Editor
Geisinger Marketing & Communications
Heather M. Davis, MFA
Director, Marketing & Communications
Elizabeth Zygmunt
Director of Public Relations and Media
Shannon Lesniak
Graphic Designer
Acknowledgments
The SCRIP journal would not be possible without the contributions of faculty, staff, and student volunteers committed to the review and assessment of submitted articles. Their feedback provides student authors with an opportunity to strengthen their writing and to respond to critiques. We gratefully acknowledge the following faculty members for their support in providing peer review.
Greg Shanower, PhD
Zachary Salvati, LGC
Tracey Pratt, MPH
Scott LeMaire, MD
Thomas Churilla, MD
Cyamatare Felix Rwabukwisi, MD, MPH
Anthony Gillott, MD
Mathangi Rajaram-Gilkes, MBBS, MSc, MS, MEd
Bruce Levy, MD, CPE
Saishravan Shyamsundar, MS
Julian Burwell
Elizabeth Kuchinski, MPH
Margrit Shoemaker, MD, FACP
Brian Piper, PhD
John Arnott, PhD
Ying Sung, PhD
Office of Research & Scholarship
MSB, Suite 2024, 2nd Floor West 570-504-9662
Sonia Lobo, PhD, RYT
Associate Dean for Research & Scholarship
Professor of Biochemistry
Michele Lemoncelli
Program Coordinator, Research & Scholarship
Tracey Pratt, MPH
Manager, Research Education Resources
Laura E. Mayeski MT(ASCP), MHA Manager, Research Compliance
Application of Duplex Ultrasound in Conjunction with Computed Topography Angiography to Identify Native Carotid Artery Stenosis
Evan Bair1†, Evan Ryer2, and Gregory Salzler2
1Geisinger Commonwealth School of Medicine, Scranton, PA 18509
2Geisinger Medical Center, Danville, PA 17822
†Doctor of Medicine Program
Correspondence: ebair@som.geisinger.edu
Abstract
Doppler ultrasound (DUS) examination is used to determine degree of stenosis by comparing patient records to threshold values of peak systolic velocity (PSV) through the internal carotid artery (ICA). DUS often overestimates the severity of stenosis. Computed tomography (CT) angiography (CTA) serves as the standard for diagnosis of stenosis, yet significant discrepancies remain between the DUS threshold values and the degree of stenosis determined by CTA analysis, especially for patients in the 50%–69% stenosis range. Therefore, standardization of stenosis diagnostic criteria between CTA and DUS findings is incomplete. Results from qualifying patients in the Geisinger medical system who underwent CTA and DUS analysis within a 3-month period were reviewed retrospectively by two blinded physicians to assess the concordance between current DUS parameters and degree of stenosis determined by CTA. Our data indicated significantly elevated PSV values as being the appropriate thresholds for determining both 50%–69% and >70% stenosis. The PSV values recorded were greater than 240 and 270, respectively. This study also showed some of the limitations that exist with CTA and DUS analysis in determining the percentage of ICA stenosis. Future studies will examine modified selection criteria to see if a more dependable PSV value can be elucidated.
Introduction
Internal carotid artery (ICA) stenosis is an abnormality often associated with atherosclerosis, the buildup of plaque on the artery walls. The ICA is particularly susceptible to atherosclerosis near its origin due to the bifurcation of the common carotid artery (CCA). At areas of bifurcation, turbulent blood flow allows for
greater deposition of calcified residue which, over time, leads to greater luminal narrowing due to shear stress alterations of the arterial walls (1). Due to restricted blood flow or embolic debris traveling to the brain, potentially severe complications may occur. These can range from transient ischemic attacks (TIA) to debilitating strokes. It is estimated that carotid atherosclerosis is responsible for up to 20% of ischemic strokes (2). Primary preventive strategies, close monitoring, and medical and surgical management are all elements of ensuring optimal patient outcomes.
Monitoring of ICA stenosis includes four primary modalities, including carotid duplex ultrasound (CDUS), magnetic resonance angiography (MRA), computed tomography angiography (CTA), and catheter angiography. CDUS uses doppler waves to give a report on both the velocity of the blood through the lumen of the artery as well as some basic information of the morphology of the arterial lumen. CTA and MRA both allow for direct visualization of a substantial amount of vasculature ranging from the aortic arch to the intracranial vessels where the imaging can be used to study direct morphology. These methods are extremely useful tools of measurement, but their specific measurement values in determining the risk of future strokes in asymptomatic patients is uncertain.
Of these modalities, two frequently used in conjunction with one another are CTA and CDUS. CDUS can provide insight into the velocity of blood flow through areas of stenosis. This velocity can then be correlated within a range of the degree of stenosis. CDUS can accomplish this in an inexpensive, noninvasive, and radiation-free manner. There is limited direct imaging from CDUS, however, and its quality depends on the individual recording the test; thus, this is where CTA’s application can aid providers. CTA allows for
Area of higher internal pressure; lower flow velocity
Area of lower internal pressure; high flow velocity
visualization of the vasculature, and this can provide more direct measurement of stenosis, albeit with radiation exposure and exposure to iodinated contrast dye (3).
DUS measurements were originally compared to patient angiography records to use the peak systolic velocity (PSV) as a measure of degree of ICA stenosis. The basis for this measurement is Bernoulli’s pressure dynamics (Figure 1). Bernoulli’s equations show the relationship between the pressure inside the lumen and the result of that pressure on the correlating velocity. As lumen diameter increases, internal pressure increases and fluid velocity decreases. As lumen diameter becomes smaller, such as in the case of carotid atherosclerosis, the internal pressure decreases and fluid velocity increases.
Based on Bernoulli’s pressure equations, higher PSV will correlate with a greater degree of stenosis. While CTA and CDUS are sound measurement devices, there exist inconsistencies in certain ranges where CDUS and CTA measurements do not correspond to one another as strongly as would be preferred in patient management.
Barlinn et al. demonstrated this in their 2016 study where CTA and DUS measurements strongly correlated with one another in determining the degree of stenosis across all stenosis ranges. To further test these findings, Barlinn et al. conducted Bland-Altman analysis. This is a technique where two modes of measurement in medical settings are compared in a visual manner to assess differences between the averages of the two measurement modalities and interpret an agreement interval. This analysis showed large incongruences between DUS and CTA stenosis measurements. In terms of correlation, there was a difference of 3.57%.
While this was an encouraging finding, the Bland-Altman analysis showed a 95% confidence range of -29.26 to 22.84, demonstrating the concerningly high levels of
Area of higher internal pressure; lower flow velocity
Figure 2. A comparison of the North American Symptomatic Carotid Endarterectomy (NASCET) method and European Carotid Surgery Trial (ECST) measurement methods. NASCET measures the widest portion of the ICA lumen distal to the plaque to the area of greatest stenosis. ECST measures the greatest area of the carotid bulb to the area of greatest stenosis.
variability between the two measurement types (4, 5). Similarly, in the 2023 study by Simann et al., their findings showed that CTA was the superior measurement device, and there existed substantial differences between the measurements recorded when comparing CTA and DUS. The range of degree of stenosis in which the greatest differences existed was in the patient population that had an ICA stenosis between 50% and 69% (6). This range represents important threshold values for determining whether a patient requires medical or surgical management, especially if they are symptomatic. In addition to these inconsistencies in evaluation, limitations and sources of measurement error exist in each. For example, high degrees of calcified plaque can interfere with CDUS signal and give artificially low-velocity flow volumes. CTA imaging results can be influenced by the angle with
Figure 1. Pictorial representation of Bernoulli’s pressure dynamics.
which the artery is viewed, the interpretation of the viewer, and the quality of the image itself.
Guidelines for determining the degree of ICA stenosis are detailed in the North American Symptomatic Carotid Endarterectomy Trial and the European Carotid Surgery Trial (7). The NASCET trial based the severity of stenosis off the lumen diameter of the region of greatest disease burden and compared this lumen diameter of the unaffected region distal to the stenosis (Figure 2). When compared to the ECST, which determined stenosis by comparing the most affected region to the carotid bulb, the NASCET guidelines often produce a less severe result. While these guidelines have served as the usual source for interpreting PSV values and concurrent treatment regimens, they have fallen under scrutiny, especially in the determination of stenosis in the 50%–69% range in asymptomatic patients (8).
Currently, treatment guidelines suggest that patients with a history of stroke or TIAs and 50%–69% stenosis may benefit from surgical intervention, such as stenting or CEA. Those with less than 50% stenosis will not benefit from surgery. Older individuals, men, and those with stenosis exceeding 70% are at greatest risk and would most likely benefit from surgery. Ultimately, the decisions on managing patients with 50–69% stenosis are determined by the patient’s clinical features, associated comorbidities, and overall health (9). History of a TIA is a useful clinical indicator for the need for intervention, but, per a 1996 study by Hankey, only 15% of stroke victims have a preceding TIA (10). Therefore, many of those patients who ultimately suffer a stroke would be considered to have asymptomatic carotid stenosis. These are the patients for whom intensive medical intervention, as described previously, would be especially beneficial, and medical intervention would be more beneficial to these patients than surgical procedures such as CEA and CAS. Medical management of stenosis would include controlling hypertension, smoking cessation, switching to the Mediterranean diet or other heart-healthy diets, reduced sodium intake, antiplatelet medications, lipid-lowering agents, and ACE inhibitors (11).
Current NASCET guidelines give a PSV value of 125 cm/ sec as the threshold value for a stenosis equal to or greater than 50%. This threshold value has been tested with several rigorous trials, and there is significant concern that the value does not appropriately hold up. This can have significant ramifications for the management of ICA stenosis, as patients may undergo
unnecessary and invasive procedures such as stenting or carotid endarterectomy (CEA) when medical management may be sufficient. Beach et al., in their 2012 analysis, proposed an even higher value at 165 cm/sec utilizing scatterplot data of 3,000 different data points (12). In their 2021 study, Gornik et al. found that a PSV value of 180 cm/sec was more consistent with a stenosis of 50%–69% than was the value given in the NASCET guidelines (13). In their study, they compared these PSV values to the more robust catheter angiography measurement as opposed to CTA. Given that the 50% stenosis value represents such an important marker for potential intervention strategies in symptomatic patients and potentially the start of more aggressive medical management in asymptomatic patients, it is important to define a value distinguishing this degree of stenosis as thoroughly as possible.
While it is also of high clinical relevance to best distinguish these values in the guidance of treatment for the sake of efficacy in a treatment regimen, it is also just as imperative to use proper guidance in overseeing resource management. In a 2007 study by Pawaskar, it was shown that stenting was significantly more expensive than CEA, most of which was due to procedural cost (14). Even more inexpensive was the ability to medically manage patients with asymptomatic stenosis of 50% or greater. Ultimately, best medical treatment (BMT) is the most optimal approach in management of both asymptomatic and symptomatic stenosis. Whether in using statins for hyperlipidemia, smoking cessation, hypertension management, or antiplatelet therapy, these interventions are significantly less invasive, have less side-effects, and are usually more cost-effective (15). Other factors favoring medical management as opposed to surgical management in terms of financial burden included elderly patients above the age of 75 with lower life expectancy following the procedure, which was noted to be of value as the degree of atherosclerosis increased proportionally to age. While comparisons of demographics and surgical methods does not fall directly under the purview of this study, it is important to note that the monitoring of the degree of ICA stenosis does dictate medical and surgical strategies.
In our study, we looked to find a more robust measurement of PSV that correlates with a stenosis value of 50%–69% as seen in CTA. This was done by comparing the values of PSV to the degree of stenosis determined via CTA by two board-certified vascular
surgeons in patients receiving both a CTA and a DUS reading within 3 months of each other prior to any surgical intervention. Furthermore, we explored detailing more robust threshold PSV values for >70% stenosis in a similar manner. From this, we gained better understanding for guiding proper medical and surgical management of these patients with a goal of increased efficacy and decreased financial burden.
Methods
Four board-certified vascular surgeons at Geisinger Medical Center conducted a blinded review of the CTA of patients who had CDUS within a 3-month period from a pool of patients in the Geisinger medical system. Patient data came from a retrospective chart review of patients who had a CTA and DUS within 3 months of each other from January 2021 through May of 2021. Approval for this study was obtained from Geisinger’s Institutional Review Board (2020-0119). Patients who were used for measurement could not have a procedure in the intervening time interval between when the CTA and DUS were collected. Furthermore, an artery’s data was not used if it was found on the CTA that the region of stenosis had been previously stented, was contained in the common carotid artery, or had any influence from a previous intervention. Patients were disqualified from use if the quality of the image was poor. Examples of where this occurred include CTAs with significant image distortion due to movement or other artifacts and an excessive buildup of calcified atherosclerosis that made measurements difficult and unreliable. These various factors defined our exclusion criteria from the study. From DUS reports, the PSV was recorded for each artery, and if available the end-diastolic velocity (EDV) was recorded as well. If available, a ratio of the ICA to the CCA was recorded. The patient’s age, surgical history, medical history, and substance use history, including tobacco and alcohol use, were recorded for demographic analysis.
For direct visualization of the CTA, the threedimensional Aquarius iNtuition Viewer TeraRecon (TeraRecon, Durham, NC, USA) platform was used. A centerline through the artery under study was created by a member of the research team who was not part of the final measurement process. These centerlines were created using TeraRecon prior to review. Each physician measured an artery using the same centerline to avoid any deviations in the measurement of the lumen due to differences in the centerline itself. Two board-certified
vascular surgeons measured the degree of stenosis from the CTA, and if there was a greater than 40% discrepancy between their measurements, a third physician would review the CTA. This reading would replace the values that were most significantly different from the other two. Arteries with 25% stenosis or less were deemed clinically insignificant and treated in a similar fashion to arteries with no evident stenosis. The stenosis values were analyzed in three different categories of measurement that were available on the iNtuition platform: the average area of the residual lumen and stenotic lumen, the diameter of the residual lumen and stenotic lumen, and the minimum and maximum diameters of the arterial lumen. To determine which of these categories provided the most robust measurements, receiver operating characteristics (ROC) and area under the curve (AUC) analysis were performed. ROC-AUC analysis also utilized other variables collected from the patient tests to determine which provided the most reliable measurements. These other variables included peak systolic velocity (PSV), end-diastolic velocity (EDV), common carotid artery to internal carotid artery ratio, PSV + ratio, EDV + ratio, and PSV + EDV + ratio. After finding the most robust predictor of degree stenosis, a PSV value that represented each threshold of clinically relevant stenosis was produced.
Results
The initial data includes 126 patients (252 arteries). Cases were excluded if the difference between two measurements of stenosis on computed topographic angiography (CTA) was 40% or higher, or the absolute difference was 25% or greater if one of the two measurements obtained demonstrated a stenosis of zero. Cases were also excluded if both measurements were zero or if the patient met any exclusion criteria, such as a surgery between the time of the CTA and the duplex ultrasound DUS, poor CTA image, or stenosis of the common carotid artery. Of these, 187 individual arteries from 121 patients met the inclusion criteria and were included in the final analysis.
Table 1 showed the characteristics of the 121 patients. The mean age was 68.2 years and 67.8% of the patients were male. Among the patients, 43.8% received either a CAS, CEA, or both procedures prior to recording a PSV from their DUS. All other comorbidities are detailed in Table 1.
Prior large arterial bypass, endarterectomy, PVI, n% 8 (6.6%)
Prior amputation of leg, foot, or toe,n% 2 (1.7%)
Prior TIA or stroke, n% 38 (31.4%)
Prior CEA by side, n%
Table 1. Patient characteristics and demographics.
Table 2 showed the AUC from each ROC analysis. Score ranges are between 0.5 and 1.0, with 0.5 being an uninformative test and 1.0 being a perfect test. Scores of 0.5–0.6 were unsatisfactory, 0.6–0.7 satisfactory, 0.7–0.8 were seen as reliable, 0.8–0.9 were highly reliable, and 0.9–1.0 were ideal. AUC scores were reliable to highly reliable for all velocity parameters for classification of CTA stenosis < 50% vs 50%–69% for average vessel diameter measurement (AUC < 0.8). AUC was reliable for all velocity parameters for classification of CTA stenosis < 50% vs 50-69%, for minimum vs maximum vessel diameter measurement and reduction in vessel lumen area measurement (AUC 0.7-0.8). The AUC was reliable for classification of CTA stenosis 50%–69% vs ≥ 70% when the parameters included EDV for average vessel diameter measurement. When using the minimum vs maximum vessel diameter measurement, the AUC was reliable
when then model included PSV only or PSV and ratio combination. The AUC was higher in reliability for classification of CTA stenosis 50%–69% vs ≥ 70% for all parameters except ratio only for reduction in vessel lumen area measurement. None of the parameters, unfortunately, were within the optimum category for reliability.
Of the different modalities the most robust predictor for <50 – 50%–69% stenosis was the average vessel diameter measurement, specifically utilizing the PSV and ratio of the internal carotid artery to the common carotid artery. Overall, average vessel diameter provided the most robust predictors of <50 – 50%–69% stenosis throughout all categories. For predicting degree of stenosis for 50%–69% vs ≥70%, the reduction in vessel lumen area measurement provided the most robust measurements. Specifically, using the PSV and ratio of the ICA to the CCA was the most robust of these measurement modalities.
Given that average vessel diameter provided the most robust measurements, ROC analysis was conducted to determine the threshold PSV values for determining the degree of stenosis. The bolded values in Table 3 represent the optimum cutoff points. Overall, specificity was poor while sensitivity was higher with higher than anticipated cutoff points. There was a greater negative predictive value (NPV) as opposed to positive predictive value (PPV) for these points. Youden’s index captures the performance of these values in predicting degree of stenosis. The Youden’s index for these threshold values was poor, indicating that a high degree of inaccuracy and false positives and false negatives would occur.
Ultimately, the highest-sensitivity cutoff point with the greatest NPV was a PSV of ≥ 240. This value had a concurrent specificity of 71.1%, a PPV of 63.6%, NPV of 92.9%, and a Youden’s index of 0.614, indicating one of the highest levels of reliability of our compiled measurement parameters but a lower degree of reliability overall.
Table 4 similarly provided an elevated value for the PSV that was most sensitive and specific for stenosis greater than 70%. The number of patients was low, with only 12 total falling in this range. The suggested PSV value was a velocity greater than or equal to 250 cm/s. This carried a sensitivity of 87.9% and a specificity of 71.4%, a positive predictive value of 90.9%, and negative predictive value of 64.5%. Overall, the reliability of these scores was low, with a Youden’s index value of 0.593.
Discussion
The determination of the degree of ICA stenosis is usually done with CTA and CDUS. The PSV gathered from the CDUS is often used in gauging degree of stenosis via the NASCET guidelines. These threshold values, however, may not be optimum in determining management in asymptomatic patients who have a stenosis of 50%–69%. Furthermore, the use of CTA and CDUS have provided unreliable and surprisingly low levels of certainty when determining degree of stenosis when utilizing the values obtained from CDUS in comparison to CTA. CTA remains the most reliable modality for measuring stenosis outside of catheterbased carotid angiography but does come with other risks such as radiation exposure and greater financial burden. A 2021 study by Samarzija et al. showed that CTA measurements showed a positive correlation with PSV values from CDUS studies, however, this correlation coefficient was unable to tell absolute values between the measurements. This study also showed that CTA severely underestimated the degree of stenosis throughout all ranges of stenoses, and that there was a high degree of standard error determined from the measurements (16). Similarly, our study showed that the threshold values determined by average vessel diameter measurements were poor. In Table 2, ROC-AUC comparative analysis determined that average vessel diameter measurements provided the most robust results. When this method was used to determine PSV threshold values most indicative of 50%–69% stenosis, the findings resulted in a PSV of ≥ 240 cm/sec, as shown in Table 3. This was higher than anticipated and while associated with a high degree of sensitivity (90.3%) and high NPV (92.9%), it had a low specificity (71.1%), PPV (63.6%) and a low Youden’s index (0.614). This value is therefore effective at ruling out patients who may be thought to have 50%–69% stenosis but will carry with it a high degree of false negatives and false positives. This has poor implications for its use in determining medical and surgical management in patients with 50%–69% stenosis.
A similar trend was observed in our values for determining stenosis values
Table 2. Area under the curve for ROC analysis of velocity parameters for prediction of CTA stenosis.
Table 3. ROC analysis table predicting <50% and 50%–69% stenosis using average vessel diameter measurement.
0.0.Modified
Table 4. ROC analysis – diagnosing a 50%–69% versus > 70% stenosis using reduction in vessel lumen area measurement.
greater than 70%. Our PSV value was a velocity greater than or equal to 250 cm/s. This carried a sensitivity of 87.9% and a specificity of 71.4%, a PPV of 90.9%, and NPV of 64.5%. Overall, the reliability of these scores was low, with a Youden’s index value of 0.593. Similarly, these scores would not be clinically reliable for use as markers for determining stenosis greater than 70%. The current gold standard is a PSV of 230 cm/s or greater.
Determining degree of stenosis is paramount to managing patients to reduce the risk of ischemic stroke and prepare for worsening of stenosis. A stenosis of 50% is particularly important since patients with a 50% or greater degree of stenosis are at higher risk of stenosis progression and therefore at higher risk of ischemic stroke. Risk of stenosis progression is positively associated with the stenosis grade; higher degrees of stenosis may continue to worsen, and this includes patients who are asymptomatic (17). Once it is determined that a patient has a 50% or greater stenosis, the onus of follow-up becomes much more critical. A 2012 study by Dua et al. showed that out of 288 patients, 26 (9%) developed symptoms or had a severe increase in their stenosis to >75%. The comorbidities most associated with stenosis increase included coronary artery disease (8.1%), hyperlipidemia (7.3%), and hypertension (6.7%) (18). Our study, and others, show that our current methodology for predicting 50%–69% stenosis is unreliable, and this confounds the ability to appropriately gauge the risk of patients for ischemic events, provide appropriate treatment plans, and accurately determine risk of disease progression. Aside from carotid angiography, the gold standard of accurately determining degree of stenosis, albeit invasive, current noninvasive measurement techniques
are not sufficiently diagnosing stenosis risk with an acceptable degree of accuracy. Better defining threshold values for PSV is a start, and determining proper follow-up for patients who are asymptomatic and in this vague degree of stenosis of 50%–69% is necessary.
Ischemic events are debilitating and require high degrees of resource utilization. Medical management of patients determined to have 50% stenosis or higher should be aggressive. Current optimal management for patients who are not requiring surgery or are poor candidates is multifactorial. Medically, aspirin daily of 75–325 mg/d, with rivaroxaban at 2.5 mg bid, or Clopidogrel 75 mg OD or ticagrelor 90 mg BID (if ASA-intolerant or allergic to ASA) is beneficial to reducing ischemic events in patients. Lipid lowering therapies with a goal LDL <1.8 mmol/L (70 mg/dL; <1.4 mmol/L [54 mg/dL] for very high risk) via a highdose statin with ezetimibe or PCSK9 inhibitors is beneficial. Antihypertensives with ACEi/ARBs for a blood pressure goal <130/80 is ideal. Glucose-lowering therapy to a HbgA1c <7% further reduces risk. Finally, and least costly to patients, are lifestyle modifications including smoking cessation, transitioning to a healthier diet such as the Mediterranean diet, and moderateintensity exercise 4–7 times a week to prevent atherosclerosis (19).
While this may appear to be a great deal of medical intervention, prevention of stroke not only maintains a patient’s health and independence, but it also prevents financial burden from hospitalizations and interventional procedures in addition to the medical expenses for necessary follow-up. Data from 2006–2008 showed that the financial burden for patients suffering either a hemorrhagic or ischemic stroke was an average of $20,396 ± $23,256 (20). Further financial burden following a stroke include transportation concerns, household expenses, relocation, property loss, informal and formal home care, and potential disability causing job loss. Furthermore, the cost of inpatient management of a stroke vastly outweighed outpatient preventive measure (21).
Given the health and financial benefits that early detection of ICA stenosis of 50% or greater incurs in better managing patients, it is clearly imperative to better diagnose, monitor, and effectively treat. Of these, diagnosis and accurately gauging the degree of stenosis continues to present challenges. As seen in our study,
and others like it, the threshold values outlined in NASCET do not appear to accurately gauge the degree of stenosis, and the current modalities available are flawed. Further studies challenging these thresholds are necessary and determining better ways to determine ICA stenosis in a cost-efficient and non-invasive manner will benefit patients greatly.
Conclusions
In conclusion, our data does not give a reliable PSV value for determining accurately a degree of ICA stenosis. Our data yielded a PSV value of greater than or equal to 240 cm/s for determining 50%–69% stenosis and PSV value of 250 cm/s for stenosis greater than 70%. Our results, along with other studies cited here, however, do indicate that the value for determination of ICA stenosis as put forth by the NASCET is too low in determining the accurate degree of stenosis. We propose that the best PSV value for determining 50%–69% stenosis will be higher than 125 cm/s. Further studies evaluating PSV values to CTA findings are needed to better refine the diagnosis and management of ICA stenosis in a costeffective and efficient manner.
Disclosures
We have no disclosures.
Acknowledgments
I would like to acknowledge the Geisinger Medical Center Department of Vascular Surgery. A special thanks to Evan Ryer, MD, Gregory Salzler, MD, and James Elmore, MD, for their mentorship and support in this project. Furthermore, I would like to thank the MRHP advisory board, Gabi Waite, PhD, and Abhishek Yadav, MBBS, MSc.
References
1. Dhawan SS, Avati Nanjundappa RP, Branch JR, et al. Shear stress and plaque development. Expert Rev Cardiovasc Ther 2010;8:545-56.
2. Liu J, Zhu Y, Wu Y, Liu Y, Teng Z, Hao Y. Association of carotid atherosclerosis and recurrent cerebral infarction in the Chinese population: a metaanalysis. Neuropsychiatr Dis Treat. 2017 Feb 20;13:527-533.
3. Adla T, Adlova R. Multimodality Imaging of Carotid Stenosis. Int J Angiol. 2015 Sep;24(3):179-84.
4. Barlinn K, Floegel T, Kitzler HH, Kepplinger J, Siepmann T, Pallesen LP, Bodechtel U, Reichmann H, Alexandrov AV, Puetz V. Multi-parametric ultrasound criteria for internal carotid artery disease-comparison with CT angiography. Neuroradiology. 2016 Sep;58(9):845-51.
5. Giavarina D. Understanding Bland Altman analysis. Biochem Med (Zagreb). 2015 Jun 5;25(2):141-51.
6. Simaan N, Jubeh T, Wiegler KB, Sharabi-Nov A, Honig A, Shahien R. Comparison of Doppler Ultrasound and Computerized Tomographic Angiography in Evaluation of Cervical Arteries Stenosis in Stroke Patients, a Retrospective SingleCenter Study. Diagnostics (Basel). 2023 Jan 26;13(3):459.
7. Ferguson GG, Eliasziw M, Barr HW, Clagett GP, Barnes RW, Wallace MC, Taylor DW, Haynes RB, Finan JW, Hachinski VC, Barnett HJ. The North American Symptomatic Carotid Endarterectomy Trial: surgical results in 1415 patients. Stroke. 1999 Sep;30(9):1751-8.
8. Warlow CP. Symptomatic patients: the European Carotid Surgery Trial (ECST). J Mal Vasc 1993;18(3):198-201. PMID: 8254241.
9. Louridas G, Junaid A. Management of carotid artery stenosis. Update for family physicians. Can Fam Physician. 2005 Jul;51(7):984-9.
10. Hankey GJ. Impact of treatment of people with transient ischemic attacks on stroke incidence and public health. Cerebrovasc Dis. 1996;6(Supp1):26–33.
11. Spence JD. Management of asymptomatic carotid stenosis. Ann Transl Med. 2020 Oct;8(19):1262.
13. Gornik HL, Rundek T, Gardener H, Benenati JF, Dahiya N, Hamburg NM, Kupinski AM, Leers SA, Lilly MP, Lohr JM, Pellerito JS, Rholl KS, Vickery MA, Hutchisson MS, Needleman L. Optimization of duplex velocity criteria for diagnosis of internal carotid artery (ICA) stenosis: A report of the Intersocietal Accreditation Commission (IAC) Vascular Testing Division Carotid Diagnostic Criteria Committee. Vasc Med. 2021 Oct;26(5):515-525.
14. Pawaskar M, Satiani B, Balkrishnan R, Starr JE. Economic evaluation of carotid artery stenting versus carotid endarterectomy for the treatment of carotid artery stenosis. J Am Coll Surg. 2007 Sep;205(3):413-9.
15. Mohd AB, Alabdallat Y, Mohd OB, Ghannam RA, Sawaqed S, Hasan H, Ellebedy M, Turkmani K, Al-Ezzi S. Medical and Surgical Management of Symptomatic and Asymptomatic Carotid Artery Stenosis: A Comprehensive Literature Review. Cureus. 2023 Aug 10;15(8):e43263.
16. Samaržija K, Milošević P, Jurjević Z, Erdeljac E. Comparison of Carotid Stenosis Grading by CT Angiography and Doppler Ultrasonography: How the Statistical Methods Applied Influence the Results. Acta Clin Croat. 2022 Feb;60(3):457-466.
17. Ong CT, Wong YS, Sung SF, Wu CS, Hsu YC, Su YH, Hung LC. Progression of Mild to Moderate Stenosis in the Internal Carotid Arteries of Patients with Ischemic Stroke. Front Neurol. 2018 Dec 3;9:1043.
18. Dua A, Patel B, Kuy S, Seabrook GR, Tondravi N, Brown KR, Lewis BD, Rossi PJ. Asymptomatic 50% to 75% internal carotid artery stenosis in 288 patients: risk factors for disease progression and ipsilateral neurological symptoms. Perspect Vasc Surg Endovasc Ther. 2012 Dec;24(4):165-70.
19. Hackam, Daniel G. Optimal Medical Management of Asymptomatic Carotid Stenosis. AHA Journals. Stroke. 2021;52:2191–219
20. Wang G, Zhang Z, Ayala C, Dunet DO, Fang J, George MG. Costs of hospitalization for stroke patients aged 18-64 years in the United States. J Stroke Cerebrovasc Dis. 2014 May-Jun;23(5):861-8.
21. Rochmah TN, Rahmawati IT, Dahlui M, Budiarto W, Bilqis N. Economic Burden of Stroke Disease: A Systematic Review. Int J Environ Res Public Health 2021 Jul 15;18(14):7552.
The Impact of Race, Socioeconomic Status and Fragmented Care on Textbook Outcomes in Rectal Cancer
Olivia
B. Granja1†, Theresa Koch1†, Madison B. Gladfelter1†, Ayobami M. Fatunmbi2, Shengxuan Wang2, Rebecca L. Hoffman2, and Joseph A. Blansfield2
1Geisinger Commonwealth School of Medicine, Scranton, PA 18509
2Geisinger Surgery Institute, Danville, PA 17822
Correspondence: ogranja@som.geisinger.edu
Abstract
Background: Due to the multimodality treatment strategy needed to treat most patients with rectal cancer, fragmentation of care (receiving care at more than one institution) can be common in these patients and may present barriers for those from disadvantaged groups. Textbook oncologic outcomes (TOO) have recently been shown to be a marker for defining the quality of care for cancer patients. The aim of this study was to determine if socioeconomic status and race affect the fragmentation of care and achievement of TOO in rectal cancer patients.
Methods: A retrospective cohort study was performed on rectal cancer patients who received care at one institution (integrated care) and those treated at more than one institution (fragmented care) using the National Cancer Database (NCDB) NCDB (20062018). TOO was defined as: no 90-day mortality, R0 resection, ≥ 12 lymph nodes evaluated, non-length of stay outlier, no 30-day readmissions, and receiving guideline-appropriate therapy. Disparities in care based on race and socioeconomic variables were studied. Univariate and multivariate analyses were performed to look for associations between TOO and fragmented care.
Results: A total of 96,941 patients were included; 86.2% were white, 7.8% Black, and 3.0% Asian. In terms of ethnicity, 90.1% of patients were non-Hispanic, and 6.2% Hispanic. Fragmented care was associated with improved TOO in rectal cancer treatment (OR: 1.423, 95% CI: 1.377-1.471). Black patients were less likely to have TOO compared to white patients (OR: 0.843, 95% CI: 0.793-0.896). Patients in the income bracket of (≥$63,333) were more likely to achieve TOO compared with patients in lower income brackets. There are disparities in which patients receive care at more than one institution. Patients of non-white race were more
likely to have care at one institution compared to white patients. Private insurance and higher income were also associated with care at more than one institution. Hispanic patients are less likely to receive fragmented care (OR: 0.743, 95% CI: 0.693-0.796).
Conclusion: Socioeconomic and racial disparities exist and impact the achievement of TOO for patients with rectal cancer. Receiving care at more than one institution improves the receipt of TOO; however, vulnerable populations may not have access to care at higher-level care centers, which affects their ability to receive textbook outcomes. Further studies are needed to maximize care for this patient population.
Introduction
Worldwide, colorectal carcinoma remains one of the leading causes of death (1). With the advancements in surgical techniques, as well as adjuvant and neoadjuvant therapy, patients receive treatment guided by a multimodal approach involving radiation, chemotherapy, and surgery (2). Measuring the quality of care by various parameters is a vital tool to ensure delivery of patient-centered, evidence-based care.
Given the complex nature of multi-disciplinary treatment, many patients ultimately receive parts of their therapy at different institutions. Various factors may lead to a patient’s decision to receive treatment in a specific location. Freischlag et al. analyzed how fragmentation of care (FC) between academic hospitals and community hospitals in locally advanced rectal carcinoma affected patient mortality. Patients who received oncologic surgery at academic institutions were more likely to receive part of their care at different hospitals (3). Surprisingly, the study also demonstrated that patient outcomes were more favorable with FC at academic hospitals
when compared to receipt of fully integrated care at community hospitals (3). Other factors that may impact rectal carcinoma outcomes are racial disparities, socioeconomic status, and medical mistrust. These patients are presented with several obstacles that may impede higher quality treatment, and can ultimately affect long-term survival. Lu et al. evaluated the effect of racial inequality and survival in rectal cancer patients treated in minority- and non-minority-serving hospitals. They found that although treatment guidelines have improved in the last several years, many barriers to care persist for minority populations seeking rectal cancer therapy (4).
Disparities in race and socioeconomic status can severely impact a patient’s ability to seek care at higher level centers farther away from their communities. Some of the variables that affect this include traveling cost, transportation, lack of knowledge about treatment options at higher volume centers, and lack of referrals from providers. Patients from underrepresented backgrounds may be intimidated to ask questions during a visit, especially if there is a language barrier and a proper translator is not provided. It is extremely important to evaluate and attempt to improve on these disparities, as the number of patients under the age of 50 diagnosed with rectal carcinoma continues to increase throughout the United States (5).
Textbook oncologic outcomes (TOO) is a multifactorial metric for defining the quality of care in cancer patients (6). It represents the ideal outcome for patients undergoing cancer treatment. TOO is defined as a negative margin resection, no 30- day hospital readmission, adequate lymph node resection (N≥12), non-length of stay (LOS) outlier, no 90-day mortality. As institutions aim to achieve TOO in their patients, this can potentially lead to improvements in quality of care. No study has specifically examined whether FC and TOO are impacted by race and socioeconomic status. Thus, the aim of this study was to determine if socioeconomic status and race affect the FC and achievement of TOO in rectal cancer patients.
Methods
To analyze whether fragmentation of care (FC) and textbook oncologic outcomes (TOO) are impacted by socioeconomic status and race, a retrospective cohort study was performed utilizing the National Cancer Database (NCDB). This database uses hospital’s registry and database to track the diagnosis, progress,
and outcomes of patients diagnosed with malignant neoplastic diseases. The NCDB is a joint project of the Commission on Cancer of the American College of Surgeons and the American Cancer Society. The NCDB, established in 1989, is a nationwide, facilitybased, comprehensive clinical surveillance resource oncology data set that currently captures 72% of all newly diagnosed malignancies in the U.S. annually (7).
The data used in the study are derived from a deidentified NCDB file. The American College of Surgeons and the Commission on Cancer have not verified and are not responsible for the analytic or statistical methodology employed, or the conclusions drawn from these data. Due to the deidentified nature of the data, this study was deemed to be exempt from Institutional Review Board oversight. Rectal cancer patients who received care at one institution (integrated care) and those treated at more than one institution (fragmented care) between the years 2006 to 2018 are included in this study.
All demographic and surgical information is fully described throughout this study. The TOO variable included patients with the following parameters: ≥ 12 lymph nodes evaluated, no 90-day mortality, a nonlength of stay outlier, R0 resection after surgery, no 30day readmissions, and received guideline-appropriate therapy. Guideline-concordant therapy consisted of the receipt of neoadjuvant chemotherapy and radiation therapy for clinical locally advanced disease; or receipt of adjuvant chemotherapy and radiation therapy within 180 days after diagnosis for non-clinically locally advanced with pathologic locally advanced disease. Categorical variables are summarized using frequency and percentages. Comparisons by fragmented care were performed using Chi-square test for categorical. Multivariate logistic regression was developed to identify the impact of fragmented care, race, and SES factors on textbook outcome. Survival analysis techniques and log-rank test were used to test the null hypothesis of no difference in survival probability between two groups. Statistical analysis was conducted using SAS® Enterprise Guide 8.2: User’s Guide (SAS Institute Inc., Cary, NC, USA). Results were considered statistically significant if P value was 0.05 or less.
The greater circle distance variable is defined by the distance traveled (in miles) by the patient from their home to their care facility. This variable was assessed along the patient’s race. Additionally, treatment started days from diagnosis was also measured based on race.
Kaplan-Meier survival plots were performed to look at overall survival (OS) in this patient population.
Results
Demographics
A total of 96,941 patients were included in this study. Of these, 86.2% were white, 7.8% Black, and 3.0% Asian. In terms of ethnicity, 90.1% of patients were non-Hispanic, and 6.2% Hispanic (Table 1). Almost half of the patients in the study (49%) had private insurance. Seven percent of the patients in the study had Medicaid. Eighteen percent of patients had an income of less than $40,227. Twenty-six percent of the overall patient population had FC. Of these patients, 27% were white compared to 23.5% Black patients and 20% Hispanic patients.
Factors that Were Associated with Textbook Oncologic Outcomes
A multivariate analysis was performed for the achievement of TOO in this patient population (Table 2). FC was associated with improved TOO in rectal cancer treatment (OR: 1.423, 95% CI: 1.377-1.471). Black patients were less likely to have TOO compared to white patients (OR: 0.843, 95% CI: 0.793-0.896). Patients in the income bracket of (≥$63,333) were more likely to achieve TOO when compared with patients in lower income brackets.
Factors that Were Associated with FC
There were disparities among the patient population in regard to FC. A multivariate analysis was performed to evaluate these factors (Table 3). All patients of non-white race were more likely to have care at one institution when compared to white patients. Private insurance and higher income were also associated with care at more than one institution. Hispanic patients were less likely to receive fragmented care (OR: 0.743, 95% CI: 0.693-0.796).
Time to Treatment Start and Distance Traveled for Treatment
Table 4 evaluated the greater circle distance traveled for treatment and the time from diagnosis to treatment. In this study population, overall, the greater circle distance traveled was 31.1 miles. Black patients traveled least with a mean distance traveled of 20 miles versus 32 miles for white patients, 22 miles for Asian
0.994
Table1. Race and socioeconomic status
Table 2. Multivariate analysis: Associations with Textbook Oncologic Outcomes
patients and 39 miles for other races (p<0.0001). The time to start treatment from diagnosis overall was 35 days. This was longest in black patients, with a mean of 42 days, and shortest in white patients, with a mean of 34.5 days (p<0.0001).
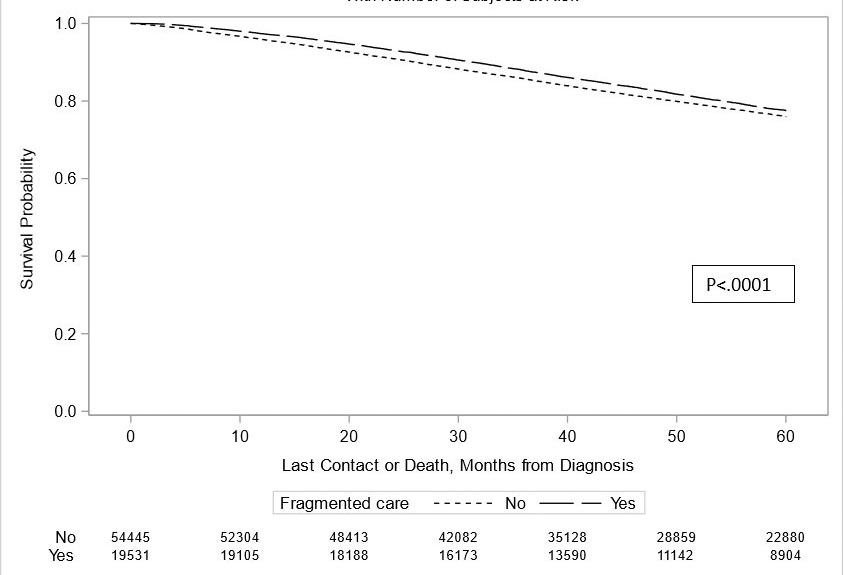
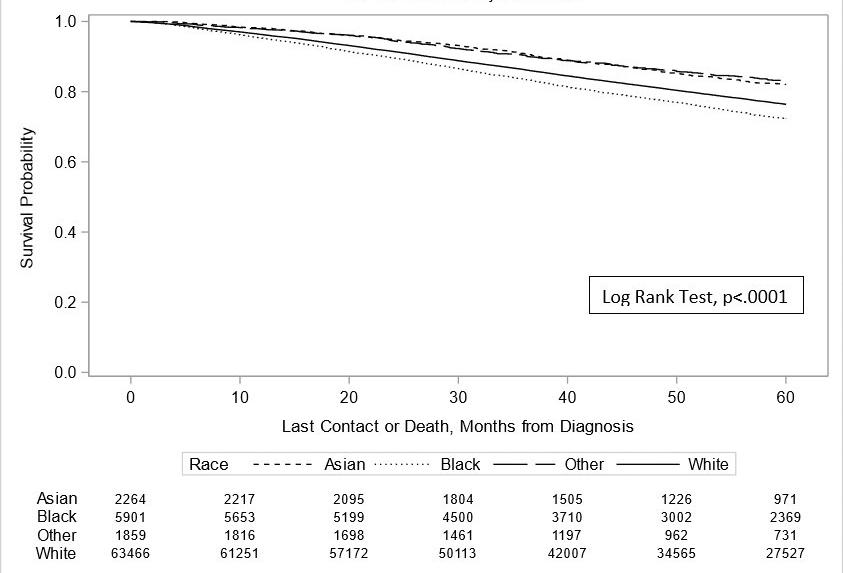
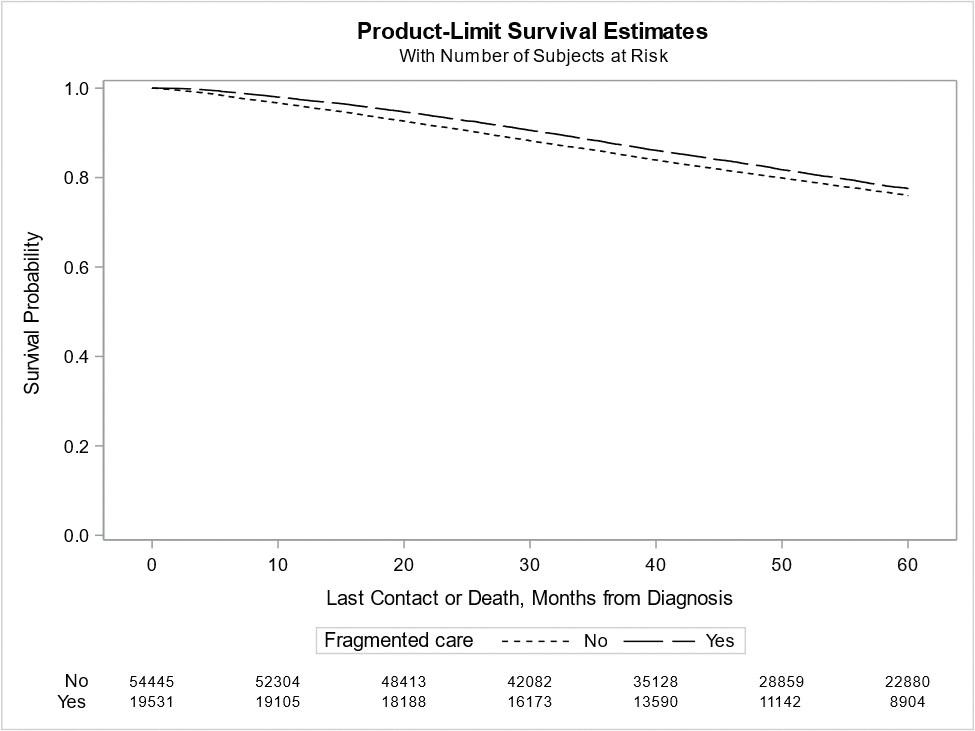
OS Based on FC and Race
Kaplan-Meier (KM) curves were performed to evaluate OS based on FC and race. Figure 1 compared FC to IC in this study population. Five-year survival rates were lower in patients who received IC care versus those who received FC (p<0.0001). Figure 2 shows 5-year survival probability based on race. Black patients had the worst OS rates, and Asian patients had the best OS rates for this study population (p<0.0001).
Discussion
This retrospective NCDB study is the first study, to our knowledge, to characterize what racial and socioeconomic factors affect FC and the ability to achieve TOO in rectal cancer patients. This study showed that FC is associated with TOO in rectal cancer patients. There appear to be socioeconomic and racial disparities associated with FC and TOO. Black patients were less likely to achieve a TOO compared to their white counterparts. Patients in the highest income quartile (≥$63,333) were more likely to achieve TOO, while lower-income quartiles attained fewer TOO. There are disparities in which patients have FC. Patients of non-white race are more likely to have IC compared to white patients. Private insurance and higher income also are associated with FC.
Overall, for this study population, FC is associated with a higher likelihood of achieving a TOO and therefore, it appears that FC is beneficial for patients. Racial and socioeconomic disparities appear to keep patients from having care at different institutions which is associated with a decrease in TOO. There has been a trend toward centralization of surgical care to institutions with higher volumes over the years (8). This centralization of care has been shown to improve outcomes for cancer operations. This study suggests that lower socioeconomic groups and minorities are not seeking care at more than one institution and instead are staying at one institution for their care. Future studies are needed to identify the reasons why certain groups are more likely to have FC versus IC.
This study did show an association with OS based on the receipt of FC and also based on race. Overall FC was associated with an increased OS. In addition, black patients had worse OS compared to white or Asian patients. More studies are needed to identify why race may play a role in OS; however it appears that FC does have an association with survival outcomes. FC may be one of the drivers for this improvement in OS.
Some of the negative effects on FC are delays in care and care that is farther from home (9). For this study, Black patients traveled the shortest distance for their care, followed closely by Asian patients. This correlates with more Black and Asian patients having IC. Despite traveling shorter distances,
Table 4. Great circle distance and treatment started days from diagnosis by race
Table 3. Multivariate analysis: Associations with fragmented care
Black patients had the longest time from diagnosis to treatment start. It is uncertain why these patterns are present, but more research is needed to identify the cause of these delays in treatment.
Although previous studies may have focused on rectal cancer mortality, fragmented care, and disparities in care post-surgical resection, no study has analyzed how fragmented care and textbook oncologic outcomes are impacted by race and socioeconomic status. Our data
showed that disparities exist between socioeconomic status based on income quartiles. Most importantly, disparities in outcomes, survival, and delay to care based on a patient's race were found. Additionally, our data showed that FC offers a significant benefit for better outcomes versus integrated care, demonstrating disparities with white patients receiving the highest rates of FC and better outcomes overall. Whereas in the past FC was viewed negatively, now with the centralization of care to higher-volume centers, FC is showing better outcomes for patient care.
This study is a vital piece of literature, as it highlights the racial and socioeconomic impact the access rectal care patients have and further how it ultimately impacts a patient's 5-year survival. This study demonstrates the unfortunate reality that not all patients receive the same care access. It can be used as a guide for physicians, community leaders, and public health workers to construct methods to break down the barriers to care for these patients. Additionally, this study can help guide individualized patient care for patients from disadvantaged groups. Health care providers can use the patient's economic and social factors to construct a treatment plan that will help optimize oncologic care and improve outcomes.
Some of the limitations of this study included the database itself. The National Cancer Database proportionally reports more cancer data on patients of white race over non-white patients. This is a limitation to getting more accurate data from a proportionate number of racial groups. Another limitation is the median income variable, this variable is measured by the zip code of the patient at the time of diagnosis. However, it does not account for the patient moving, temporary housing, or the actual household income of the individual patient versus a category based on area. Due to the limitations
Figure 1. Overall survival for the study population, stratified by fragmented care
Product-limit survival estimates with number of subjects at risk
Figure 2. Overall survival for the study population, stratified by race
Product-limit survival estimates with number of subjects at risk
of the database, there is no information regarding why patients chose a specific treatment regimen, nor is their information as to why they had care at one institution versus another. Therefore, more research is needed to identify these trends.
Nonetheless, this study is relevant as rectal cancer remains one of the largest public health issues in the United States and worldwide. Therefore, this study addressed an important topic: addressing disparities in treating this aggressive cancer. By understanding the issues that impact patient outcomes from various groups, we can further expand the literature on improving access to care and survival outcomes in these patients.
Further steps are needed to decrease disparities in care and improve all aspects of rectal cancer care. Future studies can also analyze how improving access to care may affect survival and prognosis in rectal cancer.
Conclusion
Socioeconomic and racial disparities exist and impact the achievement of TOO for patients with rectal cancer. Receiving care at more than one institution improves the receipt of TOO; however, vulnerable populations may not have access to care at higher-level care centers, which affects their ability to receive textbook outcomes. Further studies are needed to maximize care for this patient population.
Disclosures
The authors declare no conflicts of interest. This research did not receive any funding from agencies in the public, commercial, or not-for-profit sectors.
Acknowledgments
All authors made substantial contributions to either the concept and/or design of this study. SW collected and analyzed the data for the present study. OG, TK, MG, AF, RH, and JB all interpreted the data and drafted and/ or edited the manuscript. OG, TK, MG, AF, SW, RH, and JB reviewed the manuscript for errors and provided feedback for changes. All authors approved this version of the manuscript and agreed to be accountable for all aspects of the article.
References
1. Rawla P, Sunkara T, Barsouk A. Epidemiology of colorectal cancer: incidence, mortality, survival, and risk factors. Prz Gastroenterol. 2019;14(2):89-103. doi:10.5114/pg.2018.81072
2. Chiu CG, Hari DM, Leung AM, Yoon JL, Sim MS, Bilchik AJ. Are community hospitals meeting the same standards as academic hospitals for the multimodal management of rectal cancer? Am Surg 2012;78(10):1172-1177.
3. Freischlag K, Olivere L, Turner M, Adam M, Mantyh C, Migaly J. Does Fragmentation of Care in Locally Advanced Rectal Cancer Increase Patient Mortality? J Gastrointest Surg. 2021;25(5):12871296. doi:10.1007/s11605-020-04760-x
4. Lu PW, Scully RE, Fields AC, et al. Racial Disparities in Treatment for Rectal Cancer at Minority-Serving Hospitals. J Gastrointest Surg. 2021;25(7):18471856. doi:10.1007/s11605-020-04744-x
5. Sifaki-Pistolla D, Poimenaki V, Fotopoulou I, et al. Significant Rise of Colorectal Cancer Incidence in Younger Adults and Strong Determinants: 30 Years Longitudinal Differences between under and over 50s. Cancers (Basel). 2022;14(19):4799. Published 2022 Sep 30. doi:10.3390/cancers14194799
6. Aquina CT, Hamad A, Becerra AZ, et al. Is Textbook Oncologic Outcome a Valid HospitalQuality Metric after High-Risk Surgical Oncology Procedures? Ann Surg Oncol. 2021;28(13):80288045. doi:10.1245/s10434-021-10478-0
7. Mallin K, Browner A, Palis B, et al. Incident Cases Captured in the National Cancer Database Compared with Those in U.S. Population Based Central Cancer Registries in 2012-2014. Ann Surg Oncol. 2019;26(6):1604-1612. doi:10.1245/ s10434-019-07213-1
8. Aquina CT, Probst CP, Becerra AZ, et al. High volume improves outcomes: The argument for centralization of rectal cancer surgery. Surgery. 2016;159(3):736-748. doi:10.1016/j. surg.2015.09.021
9. Abelson JS, Bauer PS, Barron J, et al. Fragmented Care in the Treatment of Rectal Cancer and Time to Definitive Therapy. J Am Coll Surg. 2021;232(1):27-33. doi:10.1016/j. jamcollsurg.2020.10.017
Interprofessional Communication in Health Care Systems: Analysis and Solutions
Yousef Raslan Hakim1†‡, Yonis Hakim2†‡, and Ali Abdelhady3∆‡
1Geisinger Commonwealth School of Medicine, Scranton, PA 18509
2Tulane University School of Medicine, New Orleans, LA 70112
3The Ohio State University College of Medicine, Columbus, OH 43210
∆Doctor of Medicine
†Doctor of Medicine Program
‡Authors contributed equally
Correspondence: yhakim@som.geisinger.edu
Abstract
Communication and networking are areas of emphasis for establishing better teams and systems in the fast-paced health care environment. Communication and networking between health care professionals, students, and community members provide ample opportunities to strengthen connections and share insights, advice, and experiences. Communication and networking also allow for establishing better rapport with community members. To optimize communication within health care, as well as between health care professionals and the larger community, health care professionals should provide longitudinal and culturally competent care for community members, organize and participate in educational and engaging community events, and hold regular meetings with other health care professionals. These methods will allow health care systems to become more positive working environments and will enable health care professionals to become more connected to their communities.
Introduction
Communication and networking between health care professionals, students, and the community need to be optimized to enhance the quality of care delivered to patients. When communication and networking between health care professionals are improved, health care professionals benefit from each other’s insights and experiences, resulting in more efficient health care teams. The literature shows that regular communication, which allows team members to share ideas and information openly, is a hallmark of teamwork and efficient teams (1, 2). Also, when connections between health care professionals and the community are strengthened, health care professionals can have stronger rapport with their patients.
Current Gap between Health Care Professionals
When passing by staff members, physicians, or students from other teams; fellow health care professionals may not greet them. Since greetings are among the basics of communication, it is expected that other aspects of communication and networking are also in need of improvement. It is observable that health care professionals have limited contact and meetings with each other, especially when they belong to different teams or departments. It is certainly true that time is limited and of the essence, especially in health care. Nonetheless, extending greetings and reaching out to those who need help may not require a significant amount of time. Unfortunately, limited communication and networking result in health care professionals’ missing opportunities to learn from the experiences, insights, and advice of colleagues and senior staff members.
Overall, poor communication results in a loss of opportunity to become better health care providers and establish stronger health care systems with positive work environments. This conclusion is well-founded in the literature. A research study on 2,000 incident reports showed that over 80% of medical incidents and accidents were attributed to human errors, including communication errors (3). Another study mentioned that anesthesiology residents reported that negative outcomes could have been prevented if they, as trainees, were allowed to contribute with their knowledge and skills (4). These studies highlight the association between communication and medical care outcomes. Another study showed that there was a strong, positive correlation between job satisfaction and having a sense of being a part of the team (5). This sense of being a part of the team can occur when there is
open communication between team members. These aforementioned studies show the need to optimize communication, an integral component of teamwork, in order to strengthen health care systems and allow them to become positive work environments that deliver high quality of care to the patients.
Building Rapport: Culturally Competent Care
Communication and networking can also be optimized outside of the clinical space — in the larger community. One of the factors that improve quality of care is building rapport between physicians and their patients. This can be accomplished when patients have longitudinal visits to a culturally competent physician who understands the cultures of the patients and with whom patients can relate. For many patients, receiving care from a physician who understands their individual cultures would be similar to attaining a distant dream. This dream is one that has long been forgotten, and nothing remains of it except for a transient thread of lingering hope. Allowing patients to attain this dream by enabling them to have longitudinal visits to a culturally competent physician is essential. Research has shown that culturally competent interactions improve patient satisfaction, resulting in improvements in treatment compliance (6, 7). Other research studies underscored that continuity of care was important to patients (8). Studies also found that patients who were treated by race-discordant physicians believed that they had less engagement in decision making (9). On the other hand, research showed that Black patients who were treated by race-concordant physicians had higher treatment compliance and patient satisfaction (10, 11). The researchers noted that one reason behind this higher satisfaction was culturally sensitive communication (11). These aforementioned research studies highlight the importance of receiving longitudinal and culturally competent care. Such care improves patient satisfaction, treatment compliance, and quality of care.
In many types of communities, practicing physicians may not be easily known or identified. There may be awareness that the community has members who are health care professionals and physicians, but they may not be known. If community members tried to search for these physicians in hospital directories, they would not be certain that they had found the correct doctor. Calling the clinic to ask about a physician’s cultural background or asking the physician directly are problematic. Physicians and health care professionals should be more integrated into their communities.
This would allow members of the community to easily find doctors of similar backgrounds and who might better understand their cultural needs. In addition, when health care professionals are wellintegrated into the community, they can learn more about the cultures or backgrounds of members in the community and become more culturally competent. Health care professionals can also attain this valuable cultural competency by benefiting from the insights and experiences of more senior colleagues. They can speak with senior colleagues about such insights and experiences during lunch breaks or social events for health care teams.
Bridging the Gap between Health Care Professionals
There are multiple solutions for the lack of communication and networking in clinical spaces. Health care systems can allocate regular times on a monthly or weekly basis to allow health care professionals to meet. Once scheduled, these occasions would naturally gather health care professionals and open opportunities for networking. In addition to this, health care professionals can arrange weekly gatherings after their shifts, with or without the help of health care systems. These do not need to be lengthy. They can be merely 30 minutes of meet-and-greet gatherings. Another solution that we saw enacted is the formation of a group on social media. With this solution, the bigger the group, the more difficult it becomes to effectively communicate and network. Hence, if the group is large, smaller groups should be made, in conjunction with the larger group, and members should attempt to meet in person once a month.
Engaging the Community: Communal Events
Regarding integration into and connecting with the community, health care professionals can arrange events that interest community members of different ages and levels. They can organize a health fair, for example. This can be done on a small scale or a large scale, and it can be open to community members of all ages. We attended such a health fair, and it was successful and well-attended. Health care professionals can also arrange a “play a doc” event for kindergarten and elementary school students or a science fair for middle and high school students. To attract college students and professionals, health care professionals can organize events to provide professional and academic development advice. Mentorship programs can also be started for community members of various
ages, and the mentorship programs may be general in scope and not restricted to medicine. Through these efforts, community members can recognize the presence of health care professionals in the community and that they are not just professionals in health care systems but also individuals with a sense of community.
Conclusion
One of the ways to develop better health care teams is improving communication and networking within these teams and with their communities. Through the implementation of the aforementioned methods, health care systems can foster better working environments and health care professionals can become more connected to and integrated into their communities.
Disclosures
The authors have nothing to disclose.
References
1. Mickan SM, Rodger SA. Effective health care teams: a model of six characteristics developed from shared perceptions. J Interprof Care. 2005;19(4):358-370. doi:10.1080/13561820500165142
2. Xyrichis A, Ream E. Teamwork: a concept analysis. J Adv Nurs. 2008;61(2):232-241. doi:10.1111/ j.1365-2648.2007.04496.x
3. Williamson JA, Webb RK, Sellen A, Runciman WB, Van der Walt JH. The Australian Incident Monitoring Study. Human failure: an analysis of 2000 incident reports. Anaesth Intensive Care. 1993;21(5):678-683. doi:10.1177/0310057X9302100534
4. Bould MD, Sutherland S, Sydor DT, Naik V, Friedman Z. Residents' reluctance to challenge negative hierarchy in the operating room: a qualitative study. Can J Anaesth. 2015;62(6):576586. doi:10.1007/s12630-015-0364-5
5. Cantarelli P, Vainieri M, Seghieri C. The management of healthcare employees' job satisfaction: optimization analyses from a series of large-scale surveys. BMC Health Serv Res. 2023;23(1):428. Published 2023 May 3. doi:10.1186/s12913-023-09426-3
6. Coelho KR, Galan C. Physician cross-cultural nonverbal communication skills, patient satisfaction and health outcomes in the physician-patient relationship. Int J Family Med 2012;2012:376907. doi:10.1155/2012/376907
7. Leach MJ. Rapport: a key to treatment success. Complement Ther Clin Pract. 2005;11(4):262265. doi:10.1016/j.ctcp.2005.05.005
8. Dang BN, Westbrook RA, Njue SM, Giordano TP. Building trust and rapport early in the new doctorpatient relationship: a longitudinal qualitative study. BMC Med Educ. 2017;17(1):32. Published 2017 Feb 2. doi:10.1186/s12909-017-0868-5
9. Harvey VM, Ozoemena U, Paul J, Beydoun HA, Clemetson NN, Okoye GA. Patient-provider communication, concordance, and ratings of care in dermatology: Results of a cross-sectional study. Dermatol Online J. 2016;22(11):13030/ qt06j6p7gh. Published 2016 Nov 15.
10. Adamson AS, Glass DA 2nd, Suarez EA. Patientprovider race and sex concordance and the risk for medication primary nonadherence. J Am Acad Dermatol. 2017;76(6):1193-1195. doi:10.1016/j. jaad.2017.01.039
11. Gorbatenko-Roth K, Prose N, Kundu RV, Patterson S. Assessment of Black Patients' Perception of Their Dermatology Care. JAMA Dermatol. 2019;155(10):1129-1134. doi:10.1001/ jamadermatol.2019.2063
A Two-Year Prospective Study on Medical Student and Mobility Specialist Intervention on Patient Mobility
Christopher D. Manko1,2†, Tyler Zlupko1,2†, Benjamin Krouse1,2†, Dylan Bertovich1,2†, Burke Beauregard1,2†, Shuyi Chen1,2†, Tyler Depalma-Shields1,2†, Marc Incitti1,2†, Stephanie Miller1,2†, Susan Sinay2, Keiran Soprano2, and John Pamula2
1Geisinger Commonwealth School of Medicine, Scranton, PA 18509
2Guthrie Robert Packer Hospital, Sayre, PA 18840
†Doctor of Medicine Program
Correspondence: cmanko@som.geisinger.edu
Abstract
Background: It is important to emphasize and promote mobility to patients in the inpatient setting given its positive effects in improving overall health. The Johns Hopkins Highest Level Mobility (JH-HLM) score provides a method of tracking patients’ mobility. The goal of this study is to understand the effects that medical students and mobility specialists have on improving patient mobility in the inpatient setting with the Johns Hopkins mobility tools. Interventions involving the medical students aimed to increase JHHLM score increases by 5% and non-negative changes by 2.5%.
Methods: Mobility specialists and medical students met with and provided mobility education to increase mobility in medical and trauma patients. Mobility specialists also directly assisted patients in mobilizing. Aggregate data for the patient floor was gathered to assess trends in mobility scores over time with the inclusion of these interventions. Percentages of JH-HLM score increases which track increases in amount mobilized, non-negative changes which track improvement from patient baseline, and patients who had 3+ mobility attempts were tracked in this study.
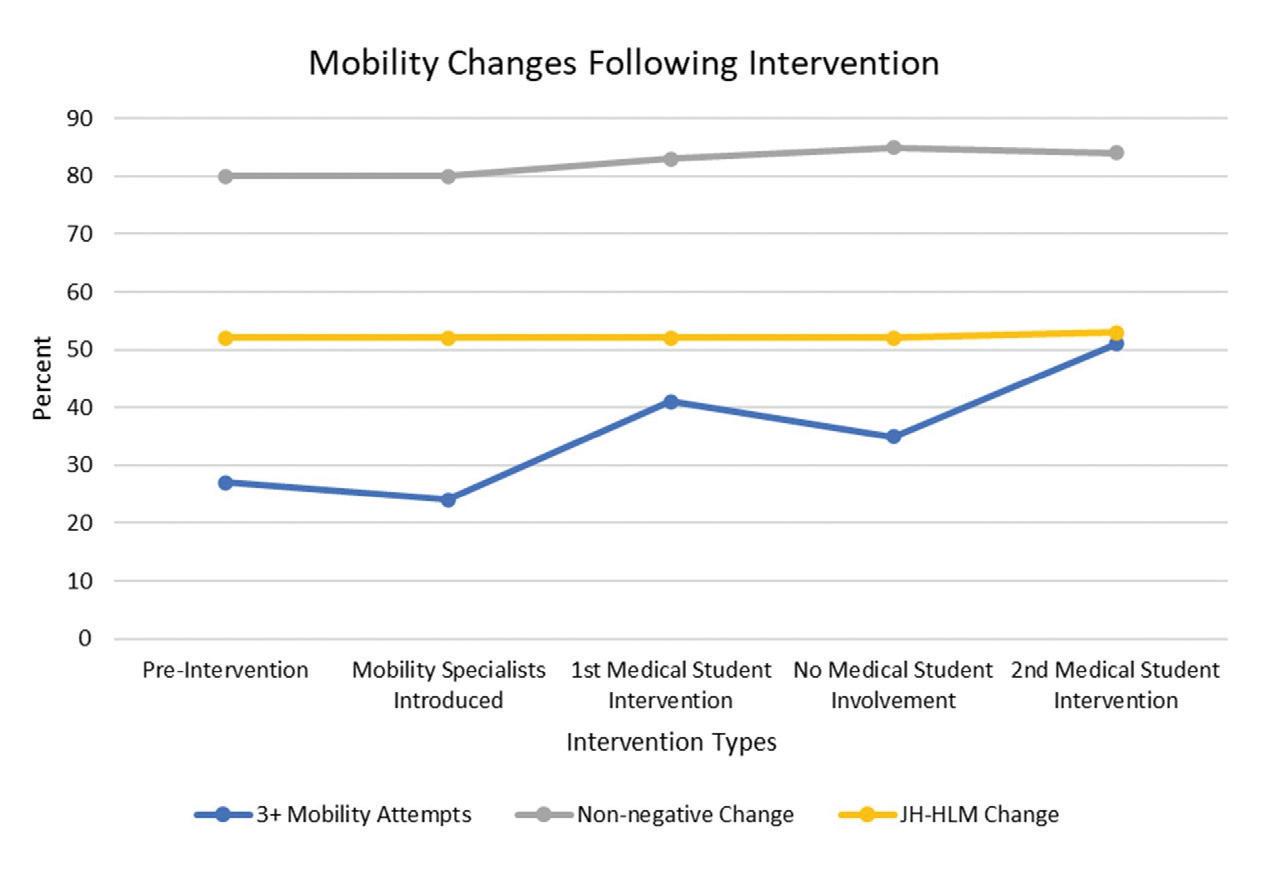
Results: From baseline to the second medical student intervention, there was a notable increase in mobility attempts (27% to 51%) with smaller increases by comparison in non-negative changes (80% to 84%) and JH-HLM score increases (52% to 53%).
Conclusion: Overall, medical student and mobility specialist intervention positively correlated to an increase in mobility attempts. Future work should focus on improving JH-HLM score increases and nonnegative changes, as well as investigating individuallevel effects with statistical analysis.
Introduction
One critical component to the success of patient outcomes in patient and provider control is mobility. Numerous studies have shown the clear benefits of mobility toward a patient’s recovery (1–10). In particular, mobility has shown benefits in decreasing postoperative complications as well as hospital length of stay (4, 6). For postoperative outcomes in older patients, early mobilization can decrease risk of readmission and death (11). A previous study at Johns Hopkins demonstrated that medical intensive care unit patients benefited from increased mobility which contributed to lower lengths of stay (12). The results of this study led to the development of the Johns Hopkins Activity and Mobility Promotion Program and the Johns Hopkins Highest Level of Mobility (JH-HLM) scoring system, which is an effective way to assess patient mobility (13).
The JH-HLM scoring system is a valuable tool which has shown excellent inter-rater reliability (14). This tool, which can be found on the Johns Hopkins Medicine website, enables providers to rate a patient’s mobility level to determine patient-specific mobility recommendations (13). The JH-HLM scoring system provides a score from 1 to 8. Patients who are, at most, able to sit on the edge of their beds receive a JH-HLM score of 3 and are recommended to have a sitting support device present (13). For a patient who can walk 25 feet or more, they receive a JH-HLM score of 7 and are recommended to use walkers as ambulatory support systems (13).
However, multiple studies have suggested that there is a need to better mobilize patients (15–17).
A recently published paper investigating barriers to mobilizing found staffing to be a perceived barrier (18).
Understanding the benefits of patient mobility and the JH-HLM tool, this study aims to improve and track patient mobility for medical and trauma patients through mobility specialists and medical student intervention by providing patient education on the importance of mobility, facilitating mobility exercises, and tracking mobility progress. Both medical student groups involved in the project aimed to improve JH-HLM score increases by 5% and nonnegative changes by 2.5%.
Methods
Act
● Consider encouraging rotating students to include mobility education as a standard practice while seeing patients
● Investigate ways to further improve JH-HLM score increases and non-negative changes
● Investigate intervention effects in other inpatient departments
Study
● Overall, mobility attempts increased from 27% to 51%, non-negative changes increased from 80% to 84%, and JH-HLM score increases increased from 52% to 53%
Medical and trauma patients admitted at Guthrie Robert Packer Hospital, a rural community hospital, were selected as the population for this study. Mobility specialists and medical students acted as intervention to improve patient mobility. Two groups of medical students met with patients in the inpatient setting to provide patient education and motivation related to the importance of mobility. Mobility specialists were hired to both motivate and mobilize patients through patient-tailored mobility exercises. Inclusion criteria included patients in the Robert Packer Hospital on floor 6 northwest or southwest that were 18 years or older. Exclusion criteria included patients that were pregnant.
Mobility evaluations with scoring were completed preand post-intervention and documented on the hospital’s Qlik data platform. Data was collected in aggregate for the inpatient floor setting. Mobility evaluations included percentage of patients completing 3+ mobility attempts a day, JH-HLM score improvements, and non-negative changes. JH-HLM scores track the amount mobilized by a patient. Non-negative changes measure improvement in mobility from baseline score. Additionally, the number of patients seen by the medical students groups was tracked. Pre-intervention mobility data was collected between December 2021 to April 2022 (5 months). Mobility specialists began their intervention in May
Plan
● Improve the mobility of patients on the inpatient floor
● Improve JH-HLM score increases by 5% and nonnegative changes by 2.5% with each student intervention
Do
● Mobility specialists aided in mobilizing and motivating patients, and medical students aided in motivating patients
1. Plan-Do-Study-Act figure for project set-up and execution.
2022. The mobility specialists participated during the entire intervention period. The first group of medical students participated between October 2022 and March 2023 and the second group of medical students participated between August 2023 and November 2023. This study was approved by The Guthrie Clinic Institutional Review Board (approval number 2307-33) and conducted in accordance with relevant guidelines and regulations. This study acts as both a quality improvement and research study. Figure 1 outlines the setup and execution of the project with a Plan-DoStudy-Act figure (19).
Results
The first medical student group saw 120 patients. Eight could not be confirmed due to documentation issues. The second medical student group saw 79 patients, with 15 being unconfirmed or excluded due to either incorrect documentation, patient floor selection, or not having confirmed documentation via electronic health records. All months in the intervention were tracked,
Figure
excluding August and September 2022 due to issues with pulling the data set in aggregate from the Qlik program utilized.
During the pre-intervention phase, 27% of patients completed 3+ mobility attempts, which paradoxically decreased to 24% with the addition of mobility specialists. The introduction of the first group of medical students then led to 41% of patients making the 3+ mobility attempts, with a follow up decrease (to 35%) after they ended their intervention. After the addition of the second medical student group there was a subsequent increase to 51%. For nonnegative changes, it was 80% to 80% to 83% to 85% to 84% respectively from pre-intervention to each chronological intervention. Finally, for JH-HLM score increase it was: 52% to 52% to 52% to 52% to 53% respectively. Figure 2 illustrates these changes over time.
decreased during periods in which there was no medical student intervention. This overall increase is consistent with a prior study which demonstrated the positive physical activity effects of motivational interviewing on patients with hip fractures (20). Medical students in the study presented here were able to elicit the patient’s goals, many of which were to “get better” and “go home.” The students could then educate and motivate the patients on the importance of movement in achieving their goals, while forming a patient-provider relationship.
Discussion
This study aimed to understand the effects mobility specialists and medical students could have on patient mobility. Throughout the 2-year intervention period there was an overall positive change in the number of mobility attempts (27% to 51%). Multidisciplinary patient interviewing with education may have had a positive contributory effect to this, as the scores
With this overall increase in mobility attempts, medical students working in a multidisciplinary team with mobility specialists may have an overall positive effect on patient mobility. Hospitals that face difficulty with staffing and/or challenges with encouraging patients to mobilize could look towards medical students to encourage mobility attempts. The unique position medical students hold allow them to spend more time with their patients. This can enable them to educate and motivate the patients they see while pre-rounding. Additionally, this has the added effect of enabling medical students to better understand the importance and effects mobilizing can have, which may act as transferable skills to other services they later rotate on. As noted previously, mobility specialists initially did not have a strong positive effect, which may have been due to delays in fully engaging with the patients due to onboarding the new mobility specialists in the program and developing the new program. Over time, however, the mobility specialists interventions led to improved patient mobility. When comparing the effect of mobility specialists prior to their intervention to the period between student interventions, there was an increase from 27% to 35% in mobility attempts indicating improvement in patient mobility.
Although there were notable improvements seen in the overall scores of mobility attempts, the percent increase in non-negative changes and JH-HLM score increases was minor. This indicates that the student
Figure 2. Trends of different mobility characteristics tracked over time.
Mobility changes following intervention
and specialist intervention had limited overall impact on increasing patient mobility from their admission baseline. An explanation for this may be that the medical and trauma patients that were included often had limiting diagnoses that limited the possibility of notable improvements in these mobility metrics.
To the authors’ best knowledge, this is the first study to investigate the effects medical students combined with mobility specialists can have on patient mobility in a rural hospital setting. Additionally, this study includes data where medical students were not involved, as well as multiple student groups, which strengthens the effects seen with this intervention given potential variability in patient-medical student interactions.
The most notable limitation in this study was that the data was sourced only in aggregate and could not be separated per patient into intervention and nonintervention groups. Given the changes in mobility variables between intervention periods, it is possible that this study’s intervention influenced trends documented. However, medical student interviews amounted to only 176 confirmed patients, a likely small percentage of the total eligible admitted patients during the study period, thus inhibiting the ability to make a true claim on effectiveness and statistical significance. Additionally, the mobility specialists also only met with a subsection of the floor’s patients. Even so, these trends may still follow intervention given that nearby patients in shared rooms or on the floor may be positively influenced when overhearing or seeing mobility education/motivational strategies. An additional limitation was that variability in patient condition and hospital course was not controlled for. Future work should pull direct patient information via the electronic health record and compare this with a pre-intervention group with similar health status/ risk factors. Future work should also expand to see if a greater positive effect in intervention could be seen with patients on other specialty services given differences in patient characteristics and differences in prognoses. Finally, future work should investigate other methods to further increase JH-HLM score increases and non-negative changes, in addition to targeting the limitations noted above.
Conclusion
Overall, the addition of mobility specialists and medical students correlated to a notable increase in mobility attempts for inpatient medical and trauma patients
at the Guthrie Robert Packer Hospital demonstrating a potential synergetic influence of multifaceted mobility intervention. By comparison, there was very little increase in percent of JH-HLM score increases and non-negative changes over the 2-year study. Future work should assess patient-specific mobility information in the intervention group and compare this to a similar health status control group to better assess the effects of each intervention, as well as aim to better improve non-negative changes and JH-HLM score increases.
Acknowledgments
The authors would like to express their sincere gratitude to Vicky L. Hickey for her help with this study. Her help regarding the institutional review board policies and advice on improving presentation of the study helped to efficiently start and improve the project. The authors would also like to thank the faculty and staff at Geisinger Commonwealth School of Medicine for their guidance and education on quality improvement for students in the phase 2 curriculum. Their efforts helped to support the creation and execution of this project.
Disclosures
The student authors were awarded monetary awards for their quality improvement presentations of their respective portions of the project. The mobility specialist authors (Susan Sinay and Keiran Soprano) are employed by the Robert Packer Hospital. No funding was utilized for this study.
References
1. Rath S, Schreuders TAR, Stam HJ, Hovius SER, Selles RW. Early active motion versus immobilization after tendon transfer for foot drop deformity: a randomized clinical trial. Clin Orthop 2010;468(9):2477–84.
2. Pearse EO, Caldwell BF, Lockwood RJ, Hollard J. Early mobilisation after conventional knee replacement may reduce the risk of postoperative venous thromboembolism. J Bone Joint Surg Br 2007;89(3):316–22.
3. Mundy LM, Leet TL, Darst K, Schnitzler MA, Dunagan WC. Early mobilization of patients hospitalized with community-acquired pneumonia. Chest. 2003;124(3):883–9.
4. Padula CA, Hughes C, Baumhover L. Impact of a nurse-driven mobility protocol on functional decline in hospitalized older adults. J Nurs Care Qual. 2009;24(4):325–31.
5. Kurabe S, Ozawa T, Watanabe T, Aiba T. Efficacy and safety of postoperative early mobilization for chronic subdural hematoma in elderly patients. Acta Neurochir (Wien). 2010;152(7):1171–4.
6. Oldmeadow LB, Edwards ER, Kimmel LA, Kipen E, Robertson VJ, Bailey MJ. No rest for the wounded: Early ambulation after hip surgery accelerates recovery. ANZ J Surg. 2006;76(7):607–11.
7. Rezaei-Adaryani M, Ahmadi F, Asghari-Jafarabadi M. The effect of changing position and early ambulation after cardiac catheterization on patients’ outcomes: A single-blind randomized controlled trial. Int J Nurs Stud. 2009;46(8):1047–53.
8. Price P, Fowlow B. Research-based practice: Early ambulation for PTCA patients. Can J Cardiovasc Nurs J Can En Soins Infirm Cardio-Vasc. 1994;5(1):23–5.
9. Hunter A, Johnson L, Coustasse A. Reduction of Intensive Care Unit Length of Stay: The Case of Early Mobilization. Health Care Manag 2020;39(3):109–16.
10. Wang J, Ren D, Liu Y, Wang Y, Zhang B, Xiao Q. Effects of early mobilization on the prognosis of critically ill patients: A systematic review and meta-analysis. Int J Nurs Stud [Internet]. 2020 Oct 1 [cited 2024 Jun 8];110:103708. Available from: https://www.sciencedirect.com/science/article/pii/ S0020748920301942
11. Pederson JL, Padwal RS, Warkentin LM, HolroydLeduc JM, Wagg A, Khadaroo RG. The impact of delayed mobilization on post-discharge outcomes after emergency abdominal surgery: A prospective cohort study in older patients. PLoS ONE [Internet]. 2020 Nov 6 [cited 2024 Mar 23];15(11):e0241554. Available from: https:// www.ncbi.nlm.nih.gov/pmc/articles/PMC7647086/
12. McLaughlin KH, Friedman M, Hoyer EH, Kudchadkar S, Flanagan E, Klein L, et al. The Johns Hopkins Activity and Mobility Promotion Program: A Framework to Increase Activity and Mobility Among Hospitalized Patients. J Nurs Care Qual. 2023 Jun 1;38(2):164–70.
13. Tools, Resources and Research [Internet]. [cited 2024 Mar 23]. Available from: https:// www.hopkinsmedicine.org/physical-medicinerehabilitation/education-training/amp/toolkit
14. Hiser S, Chung CR, Toonstra A, Friedman LA, Colantuoni E, Hoyer E, et al. Inter-rater reliability of the Johns Hopkins Highest Level of Mobility Scale (JH-HLM) in the intensive care unit. Braz J Phys Ther. 2021;25(3):352–5.
15. Callen BL, Mahoney JE, Grieves CB, Wells TJ, Enloe M. Frequency of hallway ambulation by hospitalized older adults on medical units of an academic hospital. Geriatr Nurs N Y N 2004;25(4):212–7.
16. Kalisch BJ, Landstrom GL, Hinshaw AS. Missed nursing care: a concept analysis. J Adv Nurs [Internet]. 2009 Jul [cited 2024 Mar 23];65(7):1509–17. Available from: https:// onlinelibrary.wiley.com/doi/10.1111/j.13652648.2009.05027.x
17. Kamel HK, Iqbal MA, Mogallapu R, Maas D, Hoffmann RG. Time to ambulation after hip fracture surgery: relation to hospitalization outcomes. J Gerontol A Biol Sci Med Sci. 2003 Nov;58(11):1042–5.
18. Crooks E, Rampley T, Weeks DL, Billings C, Stengem D, Rangel T. Perceived Barriers to Patient Mobilization Among Therapy and Nursing Acute Care Staff: A Multi-Site Survey Study. Arch Phys Med Rehabil. 2024 Feb;105(2):243–50.
19. Plan-Do-Study-Act (PDSA) Directions and Examples [Internet]. [cited 2024 Jun 9]. Available from: https://www.ahrq.gov/health-literacy/ improve/precautions/tool2b.html
20. O’Halloran PD, Shields N, Blackstock F, Wintle E, Taylor NF. Motivational interviewing increases physical activity and self-efficacy in people living in the community after hip fracture: A randomized controlled trial. Clin Rehabil. 2016;30(11):1108–19.
Effects of Antipsychotics on Brain Structure in Patients with Psychotic Disorders
Daniel J. Seok1*‡, Maneesha Thomas1*‡, Pranav K. Selvan1*‡, Sonal Arora1*, John S. Yoo1*, and Brian J. Piper1,2
1Geisinger Commonwealth School of Medicine, Scranton, PA 18509
2Center for Pharmacy Innovation & Outcomes, Danville, PA 17821
*Master of Biomedical Sciences Program
‡Authors contributed equally
Correspondence: seokdanielsu96@gmail.com
Abstract
Psychosis is a mental disorder characterized by a disconnection from reality occurring as a result of a psychiatric illness such as schizophrenia. Possible symptoms include delusions, hallucinations, talking incoherently, and agitation. In addition, physical changes in brain volume have been found to be a common finding in magnetic resonance imaging studies of patients with psychosis. Several longitudinal studies were conducted to assess the effects of antipsychotics on brain structure. As there are animal and human data suggesting that antipsychotics are associated with changes in brain structure, this review examines whether these changes are driven by the underlying illness or represent the iatrogenic effects of antipsychotic medications. There are clear indications that psychotic illness and antipsychotic exposure exert distinct and spatially distributed effects on brain volume. However, various limitations and questions to be answered remain for these findings to be considered clinically significant for use in real-time treatment.
Introduction
In the United States, 1 in 5 adults suffer from a mental illness, with 52.9 million Americans diagnosed with a disorder in 2020 (1). The diagnosis of a mental illness is broken into two broad categories: any mental illness (AMI) or a subcategory called serious mental illness (SMI), which is defined as a mental disorder that severely interferes with major life activities (1–4).
Approximately 14.2 million, or 5.6%, of American adults suffer from SMI, while 3 in 100 Americans experience psychosis, disruptions in thoughts and perceptions that deviate from reality, every year (2–4). One of the most common illnesses of SMI is schizophrenia, with 1% of the population worldwide and 0.25% of Americans diagnosed per year (4). A common part of treatment for schizophrenia and
related psychotic disorders is antipsychotic medication. First-generation antipsychotics, known as typical antipsychotics, block about 72% of D2 dopamine receptors as well as noradrenergic, cholinergic, and histaminergic receptors (5, 6). These medications are used to alleviate symptoms of psychosis in acute halogenic episodes in schizophrenia, acute mania, and major depressive disorder (MDD) (5, 6). Secondgeneration (atypical) antipsychotics, block D2 dopamine and 5-HT2A serotonin receptors and are approved to treat psychosis and mood disorders such as anxiety and MDD (5, 6). It may be difficult for doctors to know what type of antipsychotic medication to prescribe to patients, especially due to the possibility of severe side effects for various mental illnesses. Some effects of typical antipsychotics include low efficacy among patients with multiple hallucinogenic episodes and extrapyramidal symptoms such as tardive dyskinesia (7). Serious side effects include brain cell loss and smaller brain volume (7).
The effects of antipsychotic medications on brain structure are determined in vivo through magnetic resonance imaging (MRI), an imaging technique used to observe brain size and structural changes. It is commonly used in antipsychotic medication studies to determine brain changes in vivo (7, 8). Most antipsychotic medication studies have found changes in the amount of gray and white matter, which are different components that make up the nervous tissue in the central nervous system (7–9). Gray matter consists mostly of neuron somas and is not heavily myelinated, while white matter is heavily myelinated (7, 9). These neurons help with signaling, as they create a pathway where white matter sends new information to gray matter to process it (7, 9). With increased use, a better understanding of the risks and benefits of antipsychotic medications became crucial. The focus has been on weighing the risk of metabolic adverse
effects with the benefit of effectiveness in symptom management. Despite their risks, antipsychotics remain the first line of treatment for psychotic disorders because of their effectiveness in protection against untreated psychosis. To better appreciate the relative risks and benefits, the effects of antipsychotic medications on brain structure require further analysis.
Methods
To assess the effects of antipsychotics on brain structure, a literature review was conducted using the online databases PubMed and Google Scholar. Initial criteria for our search included articles published between 2010 and 2024 and articles with an impact factor greater than 2. Also, key terms such as “antipsychotics,” “neuroleptics,” “schizophrenia,” “psychosis,” “major depressive disorder,” “MDD,” “brain,” “brain structure,” and “neuroimaging” were used in the search field. The search queries combined the terms with Boolean operators for granulation of the results, e.g., “antipsychotics AND (brain structure OR neuroimaging) AND schizophrenia.” Only English articles and peer-reviewed articles were selected. Case studies and editorials were excluded. Data from selected articles went through a focused analysis to look for data pertaining to changes in gray and white matter volume, and the effects of antipsychotics on brain structure.
Discussion
Antipsychotics and Brain Structures in Animals
Even though increasing data suggests that antipsychotic drugs might influence brain structures directly, the specific anatomical loci of these effects and their underlying cellular basis remain uncertain. To investigate this, a research team led by Vernon et al. from the Department of Neuroscience and Psychosis at King’s College London developed a rodent model that uses clinically relevant doses and serial MRI, followed by postmortem histopathological analysis (Table 1). Among antipsychotics, haloperidol and olanzapine were continuously administered to rats via osmotic minipumps to maintain clinic-like steady-state levels for 8 weeks. Longitudinal in vivo MRI was carried out at baseline, 4 weeks, and 8 weeks after the perfusion (10). Results of the investigation showed that there was a decrease in the volume and thickness of the anterior cingulate cortex after chronic treatment, regardless of the medication administered. Postmortem analysis
confirmed these volumetric findings and demonstrated that chronic antipsychotic treatment had no effect on the total number of neurons or astrocytes in the anterior cingulate cortex, but an increase in the density of these cells was observed (11). Another team from the department of psychiatry at the University of Pittsburgh had reported that chronic exposure of macaque monkeys to haloperidol or olanzapine was associated with a 10%–18% lower glial number in the parietal gray matter (12). Later, they also found a significantly lower astrocyte number with a nonsignificant lower oligodendrocyte number in the exposed monkeys, suggesting that glial alterations in psychosis must be considered an effect of antipsychotic treatment (13). While researchers need to be careful when extrapolating results from animals to patients, these reports highlight the power of the approach to link MRI findings to histopathological origins and that clinically relevant dosing regimens cause structural brain changes in experimental animals.
Changes in Brain Structure Post Antipsychotic Treatment in Humans
A study by Voineskos et al. examined how olanzapine affects an individual’s brain structure consisted of 88 participants with a known history of MDD with psychotic features including psychotic depression. These participants were prescribed olanzapine and sertraline. Olanzapine is a thienobenzodiazepine classified as a second-generation antipsychotic used to treat mental disorders including schizophrenia and bipolar disorder (14). Sertraline is a selective serotonin reuptake inhibitor used to treat MDD, social anxiety, and many other psychiatric disorders (14). Participants were started on this regimen for 12–20 weeks, including 8 weeks of remission of psychosis, and either continued the same regimen or switched to a placebo and sertraline for a subsequent 36-week period. MRI was done at the beginning of the study and a second MRI at the end of the 36 weeks. Findings showed participants (who sustained remission) exposed to olanzapine compared with placebo had a significant reduction in cortical thickness in bilateral hemispheres (14). Participants exposed to olanzapine lost approximately 1.2% of their cortex and for context, the mean annual change in cortical thickness across an adult lifespan is approximately 0.35%–0.59% from age 60 to 91 (14).
A longitudinal study evaluating the predictors of brain volume changes post antipsychotic treatment found
correlations between antipsychotic dosage and brain volume reduction (15). Patients recently diagnosed with schizophrenia had MRIs of their brain taken before starting treatment with clozapine and then subsequently underwent imaging longitudinally as they continued their antipsychotic treatment. Results showed that longer periods of treatment resulted
Authors Year Objective
Goff DC, et al.
Analyze the long-term effects of antipsychotic medication in schizophrenia.
in increased total brain volume loss. Within these patients, higher dosage resulted in a lower gray matter volume percentage overall (15). After being separated into dosage groups, the patients that received the highest dosage of clozapine over the specific time had the largest lateral ventricles, lowest baseline brain volume, and highest reduction rate of gray matter
Longitudinal observational study
Review the effects of antipsychotic treatment on brain structure in firstepisode schizophrenia oatients. Systematic
Vernon AC, et al. 2014 Analyze the effects of chronic antipsychotic treatment on brain structure (rodent model).
Vernon AC, et al. 2011 Link MRI findings with histopathological origin in rats treated with antipsychotics.
Konopaske GT, et al. 2008
Voineskos AN, et al. 2020
Boonstra G, et al. 2011
Assess the effect of chronic antipsychotic exposure on cell numbers in macaque monkeys.
Examine the effects of olanzapine on brain structure in patients with MDD + psychotic features.
Analyze brain volume changes after withdrawal of atypical antipsychotics in patients with first-episode schizophrenia.
Battistella G, et al. 2014 Review the long-term effects of cannabis on brain structure.
Fusar-Poli P, et al. 2012
Experimental study with MRI and histopathology
Experimental study
Experimental study
Randomized placebo-controlled clinical trial
Longitudinal study
Longitudinal study
Evaluate the onset of psychosis and associated brain changes. Voxel-wise meta-analysis
Lawrie SM 2018 To review the evidence behind brain changes in patients with schizophrenia are related to antipsychotic medication.
Chopra S, et al. 2021
Lieberman JA, et al. 2005
Evaluate the effect of antipsychotic medication and illness on brain volume in first-episode psychosis.
Assess antipsychotic drug effects on brain morphology in first-episode psychosis.
Narrative review
Longitudinal, triple-blind, placebocontrolled MRI study
Longitudinal study
Long-term antipsychotics use impacts brain structure though needed for disease management.
Decreased gray matter volume over time was noticed in patients with schizophrenia that were taking antipsychotics.
Chronic antipsychotic treatment led to volume reduction of the anterior cingulate cortex. (10)
Increased neuronal cell density after treatment. (11)
There was decreased astrocyte numbers due to chronic antipsychotic treatment. (13)
Olanzapine led to a reduction in cortical thickness. (14)
The higher the dosage of antipsychotics, the greater the brain volume loss. (15)
Neuroanatomical changes were noticed at the onset of psychosis. (17)
There is mixed evidence showing the role of antipsychotics and brain structural changes. (18)
Initial increase in pallidal gray matter volume with treatment, leveling off over 12 months. (19)
Both medicated and non-medicated patients showed significant gray matter volume loss. (20)
Table 1. Literature Review Summary. The table includes articles that provided study data relevant to antipsychotics and/or mental illness and brain structure.
(6)
Yang C, et al.
(7)
within the brain over time in comparison to the other dosage groups (15). The study found that the relationship as given: “antipsychotic dosage × time” is the best predictor for brain volume loss (15).
Is It the Disease or the Drug?
Mental disorders like schizophrenia are known to cause changes to brain structure by their own manifestation, along with other health-life factors that affect the magnitude of these changes (11). Alcoholism and family history all can play a role in the changing brain structures of a person with schizophrenia (15). Studies have shown that reductions of brain matter have been evident in patients around 2 years before schizophrenia diagnosis (7).
While antipsychotic medications may not be the cause for structural changes within the brain, they play a role in accelerating the reduction of already deteriorating structures. To examine the relationship between antipsychotics and brain structure, a study was done to view how changing doses of antipsychotics can play a role in the level of brain structure loss in patients that have been diagnosed with schizophrenia (7). With increasing dosage of clozapine, there was a correlation with increasing brain structure loss within the frontal, temporal, and parietal lobes. Also, comparable results were seen within the lateral ventricles, thalamus, and cerebellum (15). It was concluded that while antipsychotic medications work to decrease the level of brain deterioration brought on by mental disease, they can exacerbate the pathology of the illness in the long term (7).
Although the effects of antipsychotics on brain volume are inconsistent (17, 18), a few studies have found differences in gray matter volume associated with antipsychotics (6, 19). An investigation demonstrated that there was an antipsychotic-induced increase in pallidal gray matter volume within the study group taking antipsychotic medication compared to the placebo group within the first 3 months of being diagnosed with schizophrenia (19). An increase in pallidal gray matter volume was associated with greater reductions in symptom severity (19). However, by the 12-month period, there was no significant difference in total gray matter volume detected between the study groups, suggesting antipsychotic related brain volume changes could be significant when given earliest in treatment (19). Although another study observed that antipsychotic medication played a role in changing
brain structure (15), the results indicated that mental illness also had a significant role in altering brain structure and size. One study had results consistent with the observation that gray matter volume loss over a 12-month period did not differ between patients on medication and patients not on medication (15). However, both medicated and non-medicated patients displayed significant gray matter volume loss (15). The degree to which the overall decrease in brain structure volume is mostly related to the progression of the illness or medication related remains unclear (20).
Based on the complexity of these findings, it is noted that antipsychotic medications are crucial in treatment of psychiatric disorders but do provide some contribution to the exacerbation of pre-existing brain structure changes.
Conclusion
In conclusion, antipsychotic medications and mental illnesses both affect brain structure. While antipsychotic medications could have neuroprotective effects during the early stages of illness, prolonged use can result in a reduction in brain structure volume and may exacerbate pre-existing deteriorating brain structures from the mental illness. Antipsychotic medication has been shown to cause changes in brain structure over time in patients with diagnosed psychosis. In these patients, however, there has been evidence indicating that brain structural changes can be caused by the manifestation of the diagnosed psychotic disease. Decreases in brain matter volume are associated with the manifestation of psychotic illnesses and certain antipsychotic medications, but studies have been inconclusive in pinpointing whether the antipsychotic medications played a singular role in decreasing brain gray matter volume. As developments in distinguishing medicinal versus disease related brain structural changes advance with further research, it will be important to note the specific effects different antipsychotics have on brain structure. Furthermore, this information will be crucial to exploring the mechanisms behind their brain structure–altering functions.
References
1. U.S. Department of Health & Human Services. Mental illness [Internet]. [cited 2024 Mar 19]. Available from: https://www.nimh.nih.gov/health/ statistics/mental-illness
2. National Alliance on Mental Illness. Early psychosis and psychosis [Internet]. 2020 [cited 2022 May 7]. Available from: https://www.nami.org/AboutMental-Illness/Mental-Health-Conditions/ Psychosis
3. Viron MJ, Stern TA. The impact of serious mental illness on health and healthcare. Psychosom Med 2010;51(6):458-65.
4. Chan V. Schizophrenia and psychosis: diagnosis, current research trends, and model treatment approaches with implications for transitional age youth. Child Adolesc Ment Health. 2017;26(2):341-66.
5. Chokhawala K, Stevens L. Antipsychotic medications [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 [cited 2022 May 5]. Available from: https://www.ncbi.nlm.nih.gov/ books/NBK519503/
6. Goff DC, Falkai P, Fleischhacker WW, Girgis RR, Kahn RM, Uchida H, et al. The long-term effects of antipsychotic medication on clinical course in schizophrenia. Am J Psychiatry. 2017;174(9):840-9.
7. Yang C, Tang J, Liu N, Yao L, Xu M, Sun H, et al. The effects of antipsychotic treatment on the brain of patients with first-episode schizophrenia: a selective review of longitudinal MRI studies. Front Psychiatry. 2021;12:587013.
8. Chiao CC, Lin CI, Lee MJ. Multiple approaches for enhancing neural activity to promote neurite outgrowth of retinal explants. Methods Mol Biol 2020;2092:65–75.
9. Lee D-K, Lee H, Park K, Joh E, Kim C-E, Ryu S. Common gray and white matter abnormalities in schizophrenia and bipolar disorder. PLoS ONE 2020;15(5):e0232325.
10. Vernon AC, Crum WR, Lerch JP, Chege W, Natesan S, Modo M, et al. Reduced cortical volume and elevated astrocyte density in rats chronically treated with antipsychotic drugs-linking magnetic resonance imaging findings to cellular pathology. Biol Psychiatry. 2014;75(12):982-990.
11. Vernon AC, Natesan S, Modo M, Kapur S. Effect of chronic antipsychotic treatment on brain structure: a serial magnetic resonance imaging study with ex vivo and postmortem confirmation. Biol Psychiatry 2011;69(10):936-944.
12. Konopaske GT, Dorph-Petersen KA, Pierri JN, Wu Q, Sampson AR, Lewis DA. Effect of chronic exposure to antipsychotic medication on cell numbers in the parietal cortex of macaque monkeys. Neuropsychopharmacology. 2007;32(6):1216-1223.
13. Konopaske GT, Dorph-Petersen KA, Sweet RA, Pierri JN, Zhang W, Sampson AR, Lewis DA. Effect of chronic antipsychotic exposure on astrocyte and oligodendrocyte numbers in macaque monkeys. Biol Psychiatry. 2008;63(8):759-765.
14. Voineskos AN, Mulsant BH, Dickie EW, et al. Effects of antipsychotic medication on brain structure in patients with major depressive disorder and psychotic features: neuroimaging findings in the context of a randomized placebocontrolled clinical trial. JAMA Psychiatry 2020;77(7):674-683.
15. Boonstra G, van Haren NE, Schnack HG, Cahn W, Burger H, Boersma M, et al. Brain volume changes after withdrawal of atypical antipsychotics in patients with first-episode schizophrenia. J Clin Psychopharmacol. 2011;31(2):146-153.
16. Battistella G, Fornari E, Annoni JM, Chtioui H, Dao K, Fabritius M, et al. Long-term effects of cannabis on brain structure. Neuropsychopharmacology 2014;39(9):2041-8.
17. Fusar-Poli P, Radua J, McGuire P, Borgwardt S. Neuroanatomical maps of psychosis onset: voxelwise meta-analysis of antipsychotic-naive VBM studies. Schizophrenia Bulletin. 2012;38:1297-307.
18. Lawrie SM. Are structural brain changes in schizophrenia related to antipsychotic medication? A narrative review of the evidence from a clinical perspective. Ther Adv Psychopharmacol 2018;8(11):319-26.
19. Chopra S, Fornito A, Francey SM, O'Donoghue B, Cropley V, Nelson B, et al. Differentiating the effect of antipsychotic medication and illness on brain volume reductions in first-episode psychosis: A longitudinal, randomised, triple-blind, placebocontrolled MRI Study. Neuropsychopharmacology 2021;46:1494-1501.
20. Lieberman JA, Tollefson GD, Charles C, Zipursky R, Sharma T, Kahn RS, et al. Antipsychotic drug effects on brain morphology in first-episode psychosis. Archives of General Psychiatry. 2005;62(4):361-70.
Effect of Bilateral Truncal Vagotomy at the Time of Primary Roux-En-Y Gastric Bypass on Postoperative Marginal Ulcer Rates
Benjamin J. Smith1†, Mark Mahan2, Vladan Obradovic2, David Parker2, Alexandra Falvo2, James Dove2, and Anthony T. Petrick2
1Geisinger Commonwealth School of Medicine, Scranton, PA 18509
2Department of Surgery, Geisinger Health System, Danville, PA 17822
†Doctor of Medicine Program
Correspondence: bsmith@som.geisinger.edu
Abstract
Background: Marginal ulcer (MU) disease is a relatively common complication following Roux-en-Y gastric bypass that is associated with multiple comorbidities and requires surgical intervention for cases that are refractory to medical management. The primary study objective was to compare MU incidence in patients who underwent Roux-en-Y gastric bypass (RYGB) with and without bilateral truncal vagotomy (BTV). BTV reduces gastric acid and is typically reserved for patients with higher risk of gastric acid related complications. BTV has also been associated with weight loss. The secondary aims were to understand differences in MU complication rates, prevalence of gastroesophageal reflux disease (GERD), proton pump inhibitor (PPI) use and percent body weight loss (%BWL) between the two cohorts.
Methods: A retrospective cohort review of patients at a tertiary academic medical center was completed. All patients who underwent primary RYGB, with or without BTV, from 2015 through 2020 were included. Patients with incomplete outcome data were excluded (n=101 for RYGB without BTV and n=11 for RYGB with BTV). Patients without post-operative esophagogastroduodenoscopy (EGD) were considered asymptomatic and therefore deemed negative for MU. Fisher’s exact test was used to assess the statistical significance of study aims.
Results: A total of 1,940 patients underwent RYGB without BTV, while 55 patients underwent RYGB with BTV. Median follow-up was 32.8 months for patients with BTV and 38.0 months without BTV. Patients who underwent RYGB without BTV were younger (44.5 vs 47.7 years, p=0.034) and had higher preoperative BMIs (46.1 vs 44.1 kg/m2, p=0.044).
MU incidence with BTV was the same as without BTV (1.80 vs 1.82%, p= 0.999). Major complication rates were significantly lower without BTV (1.9 vs 9.1%, p=0.005). Major complications that occurred in the BTV group included postoperative organ space surgical site infection, ventilation within 48 hours, acute renal failure, sepsis, septic shock, bowel obstruction, and unplanned ICU admission. Patients without BTV also had significantly greater %BWL at 1 year (30.37 vs 25.18%, p<0.0001) and 2 years (30.56 vs 25.82%, p= 0.003). There were no significant differences in minor complications, gastro-jejunal anastomotic stenosis, bleeding, or gastro-gastric fistula. In patients who underwent post-operative EGDs for GERD, there was no significant difference between non-BTV and BTV cohorts in esophagitis (p=0.213) or PPI use up to 2 years (p=0.999).
Conclusion: Despite being implemented in patients with higher risk for ulcer-related complications, RYGB with BTV has similar MU incidence and gastro-jejunal anastomosis complications as RYGB without BTV. RYGB without BTV was superior for weight loss up to 2 years, but BTV demonstrated equitable weight loss potential after 2 years despite a lower initial cohort BMI. However, BTV is associated with higher rates of major complications following RYGB.
Introduction
Roux-en-Y gastric bypass (RYGB) is currently the second most common bariatric procedure in the United States, with more than 210,000 cases from 2016 through 2020 (1). Primary RYGB has demonstrated efficacy in both weight loss and obesity associated comorbidity reduction and is consequently considered the gold standard in bariatric surgery. Despite these benefits, marginal ulcer (MU) formation remains a
relatively common complication of primary RYGB with incidence ranging from approximately 0.6%–16% of all patients (2). Risk factors for MU development include smoking tobacco, NSAID use, corticosteroid use, diabetes mellitus, and large gastric pouches (3–5). Of all patients who undergo primary RYGB, 1% will require surgical revision to address MU disease (6). Furthermore, approximately 9% of patients who develop marginal ulcers will require surgical intervention due to failure of medical management (3).
A known surgical option for treating postoperative MU disease is bilateral truncal vagotomy (BTV). BTV is typically reserved for MU disease that fails medical management (7). The physiologic mechanism of BTV for treating MU disease is related to reduced vagal stimulation of gastric acid production from gastric parietal cells. Stimulation of gastric acid release is achieved via multiple pathways including direct stimulation of parietal cells via vagal acetylcholine (ACH) release, increased gastrin release from G-cells, increased histamine release from enterochromaffinlike (ECL) cells, and inhibition of somatostatin release from D-cells. Consequently, the removal of vagal innervation to parietal cells via vagotomy disrupts one of the mechanisms responsible for gastric acid production (8, 9). Of these mechanisms, gastrin appears to be the primary stimulant for gastric acid secretion in most obese patients. Interestingly, in postRYGB patients with low gastric pH, gastrin levels are relatively low. This paradigm suggests that gastric acid secretion in post-RYGB patients is primarily regulated by vagal stimulation and ACH which would be directly influenced by BTV (10). While evidence suggests the utility of vagotomy for treating recalcitrant MU following RYGB, there is a lack of data regarding the outcomes of index RYGB with concomitant BTV. BTV further offers the additional benefit of augmenting weight loss following insufficient weight reduction with bariatric procedures (11). However, this benefit has not been demonstrated in the setting of primary RYGB. In fact, a limited amount of literature suggests that vagotomy does not augment weight loss when performed at the time of index RYGB (12).
The primary objective of this study was to compare MU incidence in patients who underwent RYGB with and without BTV. It was hypothesized that BTV would reduce MU incidence after index RYGB. Secondary objectives included comparison of gastro-jejunal (GJ) anastomosis bleed and stenosis rates, gastro-gastric
(GG) fistula formation, prevalence of gastroesophageal reflux disease (GERD), proton pump inhibitor (PPI) use, and the percent body weight loss (%BWL) between cohorts.
Methods
A retrospective cohort review of patients at a tertiary academic medical center was completed. All patients who underwent primary RYGB, without or with BTV, from 2015 through 2020 were included. Patients with incomplete outcome data were excluded. Patients selected for BTV included those at a high risk for gastric acid related disease. This was defined as patients on low-dose preoperative PPI therapy with continued symptomatic GERD or patients on high-dose preoperative PPI therapy.
Patients without postoperative esophagogastroduodenoscopy (EGD) were considered asymptomatic for gastric acid related disease and therefore deemed negative for MU disease. MU was diagnosed by evidence of ulceration, erosion, or friable mucosa at or near the GJ anastomosis on EGD. Chart review of patients with postoperative EGD was completed to evaluate for post-procedure PPI use at 6 months, 1 year, and 2 years in addition to evidence of GERD on EGD. Evidence of GERD on EGD was defined as documentation of erythema at the gastro-esophageal junction. The percentage of patients with postoperative PPI use at each previously identified follow-up period was calculated accordingly with the quantity of patients with follow-up at the selected time interval throughout the study duration. The incidence of MU was determined by the number of patients with evidence of MU on EGD divided by the total number of patients in each respective cohort.
The standard technique utilized in all primary RYGB cases consisted of gastric pouch confection, GJ anastomosis creation with linear or EEA 21-mm stapler, a 50-centimeter-long biliopancreatic limb, and a 150-centimeter-long Roux limb. The technique for BTV consisted of identification of the anterior and posterior vagal nerves as they traversed the esophageal hiatus, with excision of a 2-centimeter segment proximal to the gastroesophageal junction with harmonic scalpel.
Major complications were defined as the presence of anastomotic bleed, gastrointestinal bleed, organ space surgical site infection, unplanned ventilation, placement on a ventilator within 48 hours of surgery, acute renal
failure, cerebral vascular accident, cardiac arrest, myocardial infarction, sepsis, septic shock, unplanned ICU admission, or bowel obstruction following the procedure. Minor complications were defined as superficial incisional surgical site infection, deep incisional surgical site infection, wound disruption, pneumonia, pulmonary embolism, progressive renal insufficiency, urinary tract infection, blood transfusion, venous thromboembolism, or Clostridium difficile infection following the procedure. Fisher’s exact tests were used to assess the statistical significance of study aims. Statistical analyses were performed using SAS Software (version 9.4) and p-values <0.05 were considered significant.
The study protocol has been approved and overseen by the Institutional Review Board under IRB number 2018-0594. This study was conducted in accordance with relevant guidelines and regulations of the IRB, including the Helsinki Declaration.
Results
The total number of patients that underwent RYGB without BTV and RYGB with BTV from 2015 to 2020 were 2,041 and 66 patients, respectively. Following the application of exclusion criteria, the cohorts for analysis consisted of 1,940 patients who underwent RYGB without BTV and 55 patients who underwent RYGB
Total patient cohort: RYGB = 2014 patients RYGB with BTV = 66 patients
Excluded patient charts:
RYGB = 101 patients
RYGB with BTV = 11 patients
Patient cohort for analysis:
RYGB = 1940 patients
RYGB with BTV = 55 patients
Patient without post-operative EGD:
RYGB = 1855 patients
RYGB with BTV = 47 patients
Patient with post-operative EGD:
RYGB = 85 patients
RYGB with BTV = 8 patients
with BTV. Additionally, 85 patients in the RYGB without BTV group and 8 patients in the RYGB with BTV group underwent postoperative EGD (Figure 1).
Median follow-up was 38.0 months for patients without BTV and 32.8 months for those with BTV. Patients who underwent RYGB without BTV were younger (44.5 vs 47.7 years, p=0.034) and had higher preoperative BMIs (46.1 vs 44.1 kg/m2, p=0.044). There were no other significant differences in the demographic characteristics between the two cohorts (Table 1).
MU incidence was the same without BTV versus with BTV (1.80 vs 1.82%, p= 0.999) and major complication rates were significantly lower without BTV versus with BTV (1.9 vs 9.1%, p=0.005). The major complications that occurred in the BTV group included postoperative organ space surgical site infection, placement on a ventilator within 48 hours, acute renal failure, sepsis, septic shock, bowel obstruction, and unplanned ICU admission. Patients without BTV had significantly greater %BWL at 1 year (30.4 vs 25.2%, p<0.001) and 2 years (30.6 vs 25.8%, p= 0.003). There was no significant difference in %BWL at 3 years postprocedure. There were no significant differences in minor complications, GJ anastomotic stenosis, GJ anastomosis bleeding, or GG fistula between cohorts (Table 2).
For patients who underwent RYGB without BTV and had a postoperative EGD, patient follow-up at 6 months, 1 year, and 2 years was 85, 61, and 47 patients, respectively. For patients who underwent RYGB with BTV and had a postoperative EGD, patient follow-up at 6 months, 1 year, and 2 years was 8, 7, and 6 patients, respectively. There were no significant differences between non-BTV and BTV cohorts in the prevalence
Figure 1. Patient cohorts.
Table 1. Patient demographics. BMI indicates body mass index; COPD indicates chronic obstructive pulmonary disease.
of GERD (p=0.213) or PPI use up to 2 years (p=0.999) (Table 3).
Discussion
In this investigation, a retrospective review of all patients who underwent index RYGB, with or without concomitant BTV, was conducted at a single tertiary academic center from 2015 to 2020. The data showed that there was no difference in MU incidence between
Table 2. Postoperative patient outcomes. a) Minor complications were defined as superficial incisional surgical sight infection, deep incisional surgical site infection, wound disruption, pneumonia, pulmonary embolism, progressive renal insufficiency, urinary tract infection, blood transfusion, venous thromboembolism, or Clostridium difficile. b) Major complications were defined as anastomotic bleed, gastrointestinal bleed, organ space surgical site infection, unplanned ventilation, placement on a ventilator within 48 hours of surgery, acute renal failure, cerebral vascular accident, cardiac arrest, myocardial infarction, sepsis, septic shock, unplanned ICU admission, or bowel obstruction. GJ indicates gastro-jejunal; GG indicates gastro-gastric.
RYGB without BTV versus RYGB with BTV. RYGB without BTV demonstrated superior weight loss up to 2 years post-procedure compared to RYGB with BTV. Furthermore, BTV did not improve postoperative GERD prevalence or PPI use and resulted in a higher rate of major complications.
The current recommendation for MU management consists of prophylactic postoperative PPI treatment for 6–12 months for low-risk patients. Longer therapy courses can be indicated for patients with an increased risk of MU disease. In cases where MU disease is confirmed, treatment consists of 8 weeks of high-dose PPI therapy and possible addition of cytoprotective barrier medications such as sucralfate (13). While the effect of BTV at the time of primary RYGB on MU incidence has not been previously investigated, the utility of vagotomy for the management of postoperative MU disease has been documented. In cases of MU disease that are recalcitrant to medical management, surgical interventions, including BTV and GJ anastomosis revision, were previously considered viable treatment options. The physiology of vagotomy in treating MU disease is due to the disruption of the direct vagal stimulation of parietal cells via M3 ACH receptors. While vagal stimulation represents one of multiple mechanisms responsible for gastric acid secretion, other mechanisms of acid production include reduced somatostatin mediated inhibition of acid secretion, enhanced release of histamine from
Table 3. Patients with postoperative EGD outcomes. a) Number of patients with follow-up at 6 months post index procedure for RYGB vs. RYGB with BTV was 85 and 8, respectively. b) Number of patients with follow-up at 1 year post index procedure for RYGB vs. RYGB with BTV was 61 and 7, respectively. c) Number of patients with follow-up at 1 year post index procedure for RYGB vs. RYGB with BTV was 47 and 6, respectively. d) Calculated according to the total number of patients who underwent EGD following RYGB and RYGB with BTV. The number of patients in the RYGB and RYGB with BTV were 85 and 8, respectively. PPI indicates proton pump inhibitor; GERD indicates gastroesophageal reflux disease; EGC indicates esophagogastroduodenoscopy.
ECL cells, and potentiating gastrin secretion of G cells (14). When comparing surgical options for managing MU disease, Bonanno et al. showed that BTV was similar in efficacy to GJ anastomosis revision for treatment of recalcitrant MU disease (15). Hunter et al. supported these findings and further demonstrated fewer comorbidities associated with truncal vagotomy relative to GJ anastomosis revision (7).
In contrast to the established efficacy of vagotomy in treating recalcitrant MU disease following RYGB, this study demonstrated that BTV at the time of index RYGB does not improve MU incidence. However, this result must also be considered in the context that RYGB with BTV was only performed in cases with a high risk for postoperative MU disease. Furthermore, in this investigation, there was no difference in GJ anastomosis stenosis or bleed between cohorts. One hypothesis for the unchanged MU incidence between BTV and non-BTV cohorts relates to the multitude of physiologic mechanisms that influence gastric acid secretion, as previously discussed. Interestingly, while gastrin levels are low following RYGB, vagotomy has been associated with hypergastrinemia. This results from G-cell hyperplasia induced by loss of the direct vagal stimulation of parietal cells and disrupted negative feedback of gastric acid secretion. This paradox suggests gastric acid secretion may be stimulated by gastrin following RYGB with BTV due to hypergastrinemia despite the reduction of gastrin levels often seen post-RYGB. An additional consideration for the potential reason that BTV did not improve MU incidence is related to the anatomic location of acid-producing parietal cells. These cells are concentrated in the gastric fundus and body, which comprise much of the gastric pouch postoperatively.
This may consequently predispose the GJ anastomosis to continued gastric acid exposure despite division of the vagus nerve if alternative acid producing mechanisms are able to adequately stimulate parietal cells.
Furthermore, there is limited research demonstrating non-ulcer related effects of BTV at the time of primary RYGB. In regard to postoperative weight loss, Okafor et al. found no significant difference between patients who underwent RYGB without vagotomy and those who underwent RYGB with vagotomy at the time of the index procedure (12). In contrast, there is evidence that supports weight loss augmentation with vagotomy when performed with other bariatric procedures. Kral and colleagues showed that in a comparison of patients that underwent vertical banded gastroplasty, with or without vagotomy, the vagotomy cohort had significantly increased weight loss (11). This apparent difference in the effect of vagotomy on weight loss in the aforementioned procedures may be due to gastrointestinal tract continuity status. Specifically, in RYGB the gastrointestinal tract is disrupted at the gastric level, with portions of the distal stomach and proximal small intestine being bypassed by ingested contents, whereas the gastrointestinal tract remains continuous in vertical banded gastroplasty. Consequently, vagotomy may enhance early satiety in vertical banded gastroplasty via potentiating delayed gastric emptying. In contrast, RYGB results in a significantly reduced gastric volume and disruption of pylorus-mediated gastric emptying, thus limiting the ability of vagotomy to enhance early satiety through delayed emptying. This study further supports Okafor’s findings, that BTV does not improve weight loss when performed concurrently with RYGB. In fact, the data showed that RYGB without BTV resulted in superior weight loss up to 2 years post-procedure. These results must be considered in the context that patients in the RYGB without BTV cohort had higher preoperative BMIs and subsequently greater excess body loss potential than patients in the RYGB with BTV group.
In this study, the data showed that patients who underwent RYGB with BTV were more likely to experience the following complications: postoperative organ space surgical site infection, placement on a ventilator within 48 hours, acute renal failure, sepsis, septic shock, bowel obstruction, and unplanned ICU admission. While there is no proposed mechanism for these complications as they relate to BTV within this
study, these complications may be related to operative time. However, operative time was not assessed in this study. While no existing literature relates vagotomy to the observed complications, the addition of vagotomy to bariatric procedures does predispose patients to other well-documented adverse effects. These complications include dumping syndrome, diarrhea, and delayed gastric emptying (14). Post-vagotomy dumping syndrome most often occurs when performed with a concomitant procedure that disrupts pyloric controlled gastric emptying, such as RYGB. In these settings, the combination of anatomic and physiologic disruptions of gastric emptying results in relatively rapid emptying of large volumes of hyperosmolar contents into the jejunum. This causes intestinal hypermotility and associated symptoms, such as nausea, tachycardia, abdominal distention, and abdominal cramping (16). Similarly, diarrhea can occur following vagotomy due to intestinal hypermotility, in addition to colonic exposure to unconjugated bile acids (14, 16). While vagotomy causes delayed gastric emptying secondary to increased pyloric tone, gastric division, as in RYGB, reduces concern for this complication by removing pylorus mediated control of gastric emptying. Other complications associated with vagotomy include increased bleeding and injuries to the stomach or esophagus. However, these complications may also be inherent to the bariatric procedure being concurrently performed at the time of vagotomy (14).
The findings of this study must be considered in the context of the following limitations. A major limitation of this study was the evaluation of a limited number of patients who underwent primary RYGB with concomitant BTV. Another limitation of this study was that EGD was only performed in patients who were symptomatic for GERD. Consequently, asymptomatic MU disease would not have been identified. However, the consequence of this limitation is likely not clinically relevant as patients without symptomatic disease would not have required treatment. Furthermore, patients who underwent postoperative EGD that was not captured in our system would have been incorrectly accounted for in the asymptomatic cohort. Additionally, low patient follow-up limited the evaluation of postoperative PPI use. In patients who underwent postoperative EGD, the percentage of patients with follow-up at 2 years was 55% and 75% in the RYGB versus RYGB with BTV cohorts, respectively. This may have influenced actual PPI use rates due to patients who were asymptomatic for GERD potentially being
less inclined to continue with post-procedure follow-up. However, comparison of the percent of patients with PPI use was similar between RYGB without BTV and with BTV cohorts at all examined time intervals and it is therefore unlikely that patient follow-up rates would influence this evaluation.
Considering these results, index RYGB with BTV is advised against in patients at high risk for gastric acid-related complications. A future adaptation of this study would be to collect a larger cohort of patients who underwent index RYGB with BTV for analysis as this study was limited to 55 patients. Another future suggestion would be to examine the relationship of operative time as it relates to RYGB without BTV and RYGB with BTV postoperative complication rates.
Conclusion
Despite being implemented in patients at a higher risk for gastric acid related complications, RYGB with BTV had similar MU incidence and associated GJ anastomosis complications as RYGB without BTV. RYGB without BTV had superior weight loss up to 2 years post-procedure. Importantly, RYGB with BTV was further associated with a higher risk for major postoperative complications. RYGB with BTV is consequently advised against.
Disclosures
The authors have no conflicts of interest or financial ties to disclose.
Acknowledgments
Thank you to Dr. Anthony Petrick for contributions as research honors thesis mentor. Thank you to Dr. Anthony Petrick, Dr. Vladan Obradovic, and Dr. David Parker for contributions as members of the thesis advisory committee. Thank you to Dr. Mark Mahan for formatting and editing contributions. Thank you to James Dove for data-gathering and analysis contributions.
References
1. American Society for Metabolic and Bariatric Surgery. Estimate of Bariatric Surgery Numbers, 2011-2021 [internet]. Newberry, FL: ASMBS; 2022. Available from https://asmbs.org/resources/ estimate-of-bariatric-surgery-numbers/.
2. Süsstrunk J, Wartmann L, Mattiello D, Köstler T, & Zingg U. Incidence and prognostic factors for the development of symptomatic and asymptomatic marginal ulcers after Roux-en-Y gastric bypass procedures. Obesity Surgery. 2021; 31(7):3005-3014.
3. Azagury DE, Dayyeh BA, Greenwalt IT, Thompson CC. Marginal ulceration after Roux-en-Y gastric bypass surgery: characteristics, risk factors, treatment, and outcomes. Endoscopy. 2011; 43(11):950-4.
4. Sverdén E, Mattsson F, Sondén A, Leinsköld T, Tao W, Lu Y, Lagergren J. Risk factors for marginal ulcer after gastric bypass surgery for obesity. Annals of Surgery. 2016;263(4):733-7.
5. Coblijn UK, Lagarde SM, de Castro SM, Kuiken SD, van Wagensveld BA. Symptomatic marginal ulcer disease after Roux-en-Y gastric bypass: incidence, risk factors and management. Obesity Surgery 2015;25:805-11.
6. Di Palma A, Liu B, Maeda A, Anvari M, Jackson T, Okrainec A. Marginal ulceration following Roux-en-Y gastric bypass: risk factors for ulcer development, recurrence and need for revisional surgery. Surg Endoscopy. 2020 ; 35(5):2347-2353.
7. Hunter J, Stahl RD, Kakade M, Breitman I, Grams J, Clements RH. Effectiveness of thoracoscopic truncal vagotomy in the treatment of marginal ulcers after laparoscopic Roux-en-Y gastric bypass. The American Surgeon. 2012 ; 78(6):663-668.
8. Rabben HL, Zhao CM, Hayakawa Y, Wang TC, Chen D. Vagotomy and Gastric Tumorigenesis. Current Neuropharmacology. 2016; 14(8): 967–972.
9. Debas HT, Carvajal SH. Vagal regulation of acid secretion and gastrin release. Yale J Biol Med 1994;67(3-4):145-51.
10. Palermo M, Acquafresca PA, Rogula T, Dduza GE, Serra E. Late surgical complications after gastric by-pass: A literature review. Arquivos Brasileiros de Cirurgia Digestiva. 2015;28(2):139-143.
11. Kral, JG, Görtz L, Hermansson G, Wallin GS. Gastroplasty for obesity: Long-term weight loss improved by vagotomy. World Journal of Surgery 1993; 17(1):75-78; discussion 79.
12. Okafor, PN, Lien C, Bairdain S, Simonson DC, Halperin F, Vernon AH, Linden BC, Lautz DB. Effect of vagotomy during Roux-en-Y gastric bypass surgery on weight loss outcomes. Obesity Research & Clinical Practice. 2015; 9(3):274-80
13. Choi J, Polistena C. Management of Marginal Ulceration. Complications in Bariatric Surgery 2018;45-58.
14. Seeras K, Qasawa RN, Prakash S. Truncal Vagotomy. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Dec 11 [accessed 2023 Apr].
15. Bonanno A, Tieu B, Dewey E, Husain F. Thoracoscopic truncal vagotomy versus surgical revision of the gastrojejunal anastomosis for recalcitrant marginal ulcers. Surgical Endoscopy 2019; 33(2), 607–611.
16. Ukleja A. Dumping syndrome. Practical Gastroenterology [internet]. 2006 Feb [accessed 2023 Jun];30(2):32. Available from: https://med. virginia.edu/ginutrition/wp-content/uploads/ sites/199/2015/11/UklejaArticle-Feb-06.pdf
Induced Pluripotent Stem Cell (IPSC) Therapy: A Novel Method to Treat Degenerative Diseases?
Maria Y. Tian1*
1Geisinger Commonwealth School of Medicine, Scranton, PA 18509
*Master of Biomedical Sciences Program
Correspondence: mtian@som.geisinger.edu
Abstract
Embryonic stem cell therapy is an effective method to treat nonregenerative diseases due to its potential for diverse differentiation and limitless proliferation. However, the extraction of stem cells from early-stage embryos is faced with ethical concerns. Recently, a novel method was developed to overcome this issue by generating stem cells from somatic endothelial cells. These stem cells, known as induced pluripotent stem cells (IPSCs), have features similar to embryonic stem cells with many therapeutic and non-therapeutic applications including treating degenerative diseases, disease modeling, and increasing wound healing efficiency. However, there are currently limitations in the development and applications of IPSC therapy. This review will discuss the challenges, promises, clinical applications, and developing directions in IPSC therapy.
Introduction
Induced pluripotent stem cells (IPSCs) are stem cells generated from normal somatic endothelial cells. Like embryonic stem cells (ESCs), they are capable of multi-lineage differentiation including all three primary germ layers (endoderm, mesoderm, and ectoderm) (1). IPSCs can also proliferate and self-renew indefinitely in vitro, and develop into germ cells that give rise to gametes, which makes its use preferable to ESCs through bypassing unethical tissue extraction from early-stage embryos (1). Some of the promising uses of ISPCs include treating degenerative diseases, disease modeling, drug discovery, limb regeneration with function restoration, increased wound repair efficiency, and advancing personalized medicine.
Shinya Yamanaka discovered in 2006 that IPSCs can be generated by expressing four main transcription factors in normal somatic cells: Sox2, Oct3/4, c-Myc, and Klf4, collectively named “Yamanaka factors” (1). Using these transcription factors to induce pluripotency is known as the OSKM method (1). Oct3/4, Sox2,
and Klf4 were later discovered to work as positive regulators for gene networks that help maintain ESC pluripotency and inhibit the expression of genes that promote differentiation (1). The fourth factor, c-Myc, is found to play a non-essential role, but its inclusion may dramatically enhance the reprogramming efficiency (1). To date, the OSKM method is most preferred to generate IPSCs (2).
Observed in all types of cell lines, there are multiple challenges in the IPS cellular reprogramming and proliferation process. To increase transformation success rates, cell lines with the highest potential for differentiation and proliferation are chosen. To achieve this, there are a series of tests that are used to access the quality of these cell lines (3). Currently, the teratoma assay is the only assay capable of assessing IPSC pluripotency through predicting the differentiation capability and malignant potential of the cell line (3). This assay works by injecting stem cells into immunodeficient mice and accesses the quality of stem cells through the growth of tumors in the mice (3). This assay is an important tool for the pre-clinical safety assessment of the cells (3). However, due to its time-consuming and costly nature, as well as requiring trained specialists and animal usage, it is not practical as a routine screening tool (3).
The PluriTest is a bioinformatics assay that assesses the pluripotency of undifferentiated cells by comparing the transcriptome of the experimental cell line to the transcriptome of a larger pluripotent cell line (3). This assay can rapidly screen for cells that meet or deviate from pluripotent profiles and can be carried out with a small number of cells, which can be beneficial in the early stages of establishing new pluripotent cell lines (3). However, unlike the Teratoma assay, it cannot assess differentiation capacity (3). The EB in vitro assay provides quantitative information on the differentiation potential of a cell line (3). Unlike the Teratoma assay, it can quickly assess the differentiation potential without requiring a trained specialist. Similar to PluriTest, it
cannot predict the malignant potential in a transformed cell line (3). However, if direct confirmation of the differentiation capacity is needed, then the EB in vitro assay combined with PluriTest is recommended (3).
Finally, artificial intelligence is rapidly improving in its ability to classify the quality of IPS cell lines. A novel method using multi-source feature ensemblelearning, also known as the multi-source feature fusion (MsFF) model, has shown a 95.55% accuracy in identifying good, medium, and bad cell lines by sorting and processing 46,500 images of IPSC colonies (4). These results were further verified using living cell fluorescent staining, currently an optimal biological method (4). This model provides a quick and efficient method to judge the biological quality of a single IPSC colony (4).
The assays mentioned above are critical to ensuring the quality of cell lines and have revealed some of the challenges discussed later in this review including the mutagenic properties of IPSCs and an inefficiency in the differentiation and proliferation process. While previous reviews discussed IPSC therapy at various stages in stem cell transformation in different experiments, this review will seek to provide a holistic and up-to-date review on the challenges and promises, clinical applications, and directions for IPSC therapy improvement and advancement.
Methods
Literature review on IPSC therapy and its clinical applications were conducted using a variety of sources and credible databases including PubMed, EMBO journal, and Google Scholar, using search terms “IPSC therapy,” “IPSC applications,” “limitations and challenges of IPSC therapy,” "benefits and promises of IPSC therapy," “IPSC wound therapy,” “IPSC therapy to treat cardiovascular diseases,” “IPSC therapy to treat neurodegenerative diseases,” and “clinical implications for IPSC therapy.” Primary articles evaluating preclinical and clinical trials were examined within the past 5 years.
Discussion
Current Challenges of IPSC Therapy
Inefficient Cellular Reprogramming and Differentiation
One major issue in IPSC therapy is the slow and inefficient induction of pluripotency in somatic cells.
Only one in every 1,000 somatic cells using the OSKM method is successfully induced into a pluripotent state (5). While pluripotency is typically determined in the first few hours of reprogramming after transformation, what causes the shift to pluripotency remains unknown (5). Presently, there are two dominant models that seek to explain for the low efficiency.
One model is the elite model, which proposes that inherently, only a limited number of superior cells are capable of being reprogrammed into IPSCs. However, this model was proven inaccurate when mature IPSCs in mice was generated from terminally differentiated cells including pancreatic cells and B-lymphocytes (2). The second model is the stochastic model, which proposes that all cells have the potential to become IPSCs, but many will fail to complete the process.
Currently, this model has accrued greater support from research that demonstrates reprogramming takes place as a series of events and a failure to complete any one of these events can lead to a failure in reprogramming (2).
Research from the Hochedlinger laboratory also supports the stochastic model by demonstrating that IPSC differentiation is affected by DNA methylation of the Dlk-Dio3 (delta-like homolog one gene and the type III iodothyronine deiodinase) gene clusters, which is a genomic region that is associated with stem cell regulation and cancer progression (2). Reduced DNA methylation of the Dlk-Dio3 gene cluster produced viable IPSC clones but hypermethylation of the Dlk1-Dio3 gene promoters generated few IPSC clones (2). Rudy Jaenisch’s laboratory also supports the stochastic model by discovering that enhancing OCT3/4 expression and reducing SOX2 expression in somatic cells improves the pluripotency reprogramming efficiency (2). Collectively, these experiments identified that increased efficiency of IPSC induction is not dependent on the cell type but rather in the process of cellular transformation such as the nuclear programming of somatic cells via epigenetic modifications and expression of transcription factors.
Mutagenesis
Given the high proliferative ability of stem cells, it may come as no surprise that there is an increased risk for DNA mutations which could lead to genomic instability. Interestingly, on their own, Yamanaka factors can become oncogenes if they are overexpressed, especially c-Myc, which is often found to be mutated in cancerous tumors and acts as a driver mutation (6). In one study by Yamanaka and his team, c-Myc acted as
an oncogene, where the activation of c-Myc in chimeric mice led to frequent tumor developments but an inactivation of c-Myc did not (1).
Several additional factors can increase the risk of IPSCs induced tumorigenesis. First, if undifferentiated somatic cells remain in the differentiated IPSC colony, there is a chance that the DNA from the somatic cells can initiate tumor development (6).
Second, if Yamanaka factors are still active in the IPSC colony after all the cells are reprogrammed, tumor development may occur (6). Mutagenesis can be further augmented by the frequent use of viral vectors, such as lentivirus and retrovirus, to generate human IPSCs by inserting the reprogramming factors into the host DNA (7). Common issues associated with using these vectors include chromosomal instability, copy number variations (CNV), and point mutations (8).
Fortunately, several methods have been reported to overcome the mutagenic properties of IPSC colonies. One method is to express Yamanaka factors using non-inserting adenovirus vectors or plasmids for transient expression in somatic cells (9). Another method involves adding reprogramming proteins to cells directly instead of inserting transgenic constructs containing the Yamanaka genes (9). While these methods may avoid genomic alterations, they are currently inefficient (9).
A recent and promising model to advance IPSC therapy is the organ-on-a-chip (OoC), which is sensitive to in vitro culturing (1). This technology is a bioengineered system that reproduces the physiology and activity of an organ or organ system through presenting the tissue on a microfluidic chip. OoC can be useful to develop patient-specific cell colonies and tissue, as well as to test for mutagenesis, which can increase our ability to develop targeted methods to reduce mutagenesis.
Being able to detect, control and reduce mutagenesis in IPSCs is essential if these cells are used as therapeutic agents. Thus, reducing mutagenesis is one of the most important areas in IPSC research.
Transplantation Concerns
After reprogramming, a variety of challenges can arise in the pre- and post-transplantation phases. One of the most concerning issues involve the low yield and limited survival of IPSC tissues in vivo (1). For example, recent experiments suggest that IPSC-derived neurospheres, which are free-floating clusters of neural stem cells, can survive for up to 1 year in immunosuppressed
allograft models after transplantation (10). However, the survival of these cells drastically drops to 14 days in active immune allograft models (10). This result indicates an active immune system can play a significant role in the survival of IPSC transplants.
To increase graft survival, one in vitro study showed that induced mesenchymal stem cells (iMSC) suppress the immune response and reduce graft rejection (2). Thus, iMSC may be a useful therapeutic choice to increase post-transplantation survival since it impairs the proliferation of the natural killer cells and inhibits their cytolytic capability (2).
One outstanding question in IPSC graft transplants is whether these tissues are immunogenic. One hypothesis states that an organism’s immune system will target IPSC-induced tissues due to the high level of mutations contained in the nuclei. However, this hypothesis is doubtful due to the observations from a few experimental results. One result came from Guha and his colleagues, who did not detect the immunogenicity of iPSC-derived differentiated cells in vitro and in vivo (1). Another observation came from Araki et al., who transplanted multiple IPSC-generated skin and bone marrow tissue into mice but did not observe T cell infiltration or engraftment differences between IPSC and ESC (1). This indicates that like ESC, IPSC tissues may not induce dynamic changes in the body, despite the differences in origin and reprogrammed cellular changes. Thus, further research is needed to evaluate the immunogenicity response.
Current Promises of IPSC Therapy Disease Modeling
Disease modeling is important to understand the mechanism of disease, study patient-specific vulnerabilities, and screen for potential therapeutic drugs (11). Prior to the development of IPSC technology, there was an urgent and unmet need for human disease modeling. Model organisms such as mice were extensively utilized to study human disease. However, the genetic differences between mice and humans precluded accurate modeling (11). For instance, transgenic mice models used in human Alzheimer's research could not replicate the human disease pathology — this is most likely due to the inherent differences between mice and human neurons (12). Subsequent approaches then focused on cell culture methods. However, studying heart and nerve cells in vitro using this method is notoriously
difficult, since these cells do not proliferate well unless programmed to. Once taken out of their normal cellular context, these cells may not function like they do in an in vivo environment. Thus, IPSC technology becomes highly attractive to supply a variety of tissue models using minimally invasive methods. Compared to traditional cellular screens, IPSC-based disease modeling has additional advantages in easy accessibility, human origin, multi-lineage differentiation, and advancing personalized medicine (1).
Currently, IPSC-based disease modeling is used for a variety of diseases. One example is modeling spontaneous diseases (10). In Alzheimer's disease, where 95% of disease onset results from spontaneous cases (13), IPSC-based disease modeling is a good method to help us understand the genetic constitution and cellular physiology behind the origin of this degenerative disease.
A large focus of IPSC-based disease modeling is also toward studying single gene mutations with an early onset, because late-onset diseases may have increased cellular aging with greater DNA mutations that disrupt the differentiation process and decreased embryoniclike properties (11). In general, modeling spontaneous diseases is more challenging than modeling single gene mutations because multiple genetic variants in collaboration with environmental factors make reprogramming more complicated and harder to control. Interestingly, these factors also can contribute to disease progression.
A recent technology that is rapidly advancing IPSCbased disease modeling is CRISPR-Cas 9 technology (11). CRISPR-Cas 9 enables the genetic editing and transformation of IPSCs into various disease-causing mutations (11) and is used to generate much-needed precision models for human diseases (14). One concern with CRISPR-Cas 9 is the risk for off-target effects, which have been frequently observed in normal and cancer cell lines (11). However, multiple recent studies using whole-genome sequencing have reported that off-target gene modifications are rare in IPSCs (11). These studies show off-target gene modifications may be low and not a concern for disease modeling (11). CRISPR-Cas 9 is also used to correct mutated IPS cell lines (14), which further helps in the investigation of disease pathology and discovery of therapeutic options. In a study from 2017, CRISPR-Cas 9 was used to successfully correct pathogenic mutations in IPSC derived hepatocytes (14). Unfortunately, CRISPR- IPSC
research currently faces several limitations, including low editing efficiency, and is costly and labor intensive, but there is much optimism that this technology can transform modern medicine. In the future, we are likely to see CRISPR-Cas 9 not only model and correct greater number of human diseases, but may observe CRISPR-Cas 9 produce healthy and fully functioning organs to be transplanted into patients one day.
Diverse Applications
The promise of IPSC clinical therapies revolves around the cells' ability to differentiate into many cell types, including germ cells. The first clinical study in 2014 transplanted IPSC-induced retinal pigment epithelium (RPE) sheets into two patients with macular degeneration (11). While the therapy decreased the symptomatology of macular degeneration and improved vision, the onset of mutagenesis in the second patient put a stop to the study (11).
Currently, mouse IPSCs corrected with gene editing have found success to transplant hematopoietic progenitors and treat sickle cell anemia in mouse models (12). Additionally, with the help of threedimensional (3D) organoids, IPSC therapy could generate organ-like tissues, which suggests a promising direction in organ-replacement therapy. In a study, an IPSC-induced liver organoid was successfully used to produce functional human-like tissues in mice models. However, given the inherited differences between mice and humans, further studies are needed to confirm this result in humans.
Other hypothesized applications of IPSCs are in vaccine development as well as in generating protection against cancer (15). Due to its ability to generate immune cells, researchers are optimistic IPSC therapy can be used to develop personalized immunotherapies against cancer (15).
The organ-on-a-chip technology further expands the possibilities of IPSC therapy. One way it achieves this is facilitating the examination of multiple organs on a highly reproducible scale. Additionally, this technology allows for the study of simultaneous organ interactions, which can greatly advance understanding and predictions of IPSC therapeutic results and the boundaries of graft rejection or acceptance.
Drug Discovery
Drug screening is necessary to test the efficacy and toxicities of a drug (11). An early method for drug
testing is known as target-based screening. This method first identifies a known gene that codes for a protein target involved in a disease and subsequently screens compounds against the target to test for effective drugs (11). While this method is simpler to implement than the later-developed phenotypic screening, it has low success rates and is not suitable for clinical translation (11). Phenotypic screening does not identify a target and directly tests compounds on cells to screen for drugs that produces a favorable phenotypic result. IPSC technology can benefit phenotypic screening by providing human-like cells and tissues, which can increase the accuracy of predicting how the drugs may act in the body. Additionally, IPSC technology can provide limitless supply of cell lines, which can further reduce costs and resources compared to extracting the cells from humans (11). This can help mitigate costly expenses associated with often unanticipated side effects in the late stages of clinical trials (11).
Another benefit of IPSC technology is drug repurposing, in which approved drugs for certain diseases are retested and applied for application to other diseases (11). This will also be a cost-effective method to quickly reassign drugs for new clinical use as well as help develop multi-targeted therapeutic strategies (11). However, one of the main limitations in using IPSC technology for drug screening is the long duration (several weeks or greater) it takes to reprogram IPSCs into diseased states.
Cardiovascular Remodeling
Human cardiomyocytes can no longer divide after development. As a results, patients with damaged, weakened, or stiff heart tissue are at a greater risk of heart failure and may live with chronic heart failure symptoms such as shortness of breath, fatigue, weakness, and chest pain (16). Consequently, there is a great need for research and advancement in repairing damaged heart tissue. Since IPSC-generated cardiomyocytes are derived from the patient’s own skin cells, it is a promising option to help reproduce and restore lost cardiomyocytes while decreasing the risk of immune system rejection compared to foreign cells and tissues. To date, cardiomyocytes have been successfully generated from human hair follicle keratinocytes with well-developed cellular organelles and exhibiting cardiac-like transmembrane action potentials (17). Recent research has also successfully used rat hair follicles derived from pluripotent stem
cells to generate mature beating cardiomyocyte sheets (17). A major benefit of hair-follicle-induced cardiomyocytes is that they do not form tumors (17), unlike skin-induced cardiomyocytes, which could bypass one of the largest issues with mutagenesis.
In general, IPSC-derived cardiomyocytes are better than mesenchymal stem cells and skeletal myoblast derived cardiomyocytes due to the improved regional contractile function and cardiac bioenergetic efficiency (18). A recent study also observed favorable results by co-culturing various types of stem cells. In their study, a mixture of IPSC-derived cardiomyocytes and mesenchymal stem cells enhanced cell-cell interactions, prolonged survival of cells and promoted the structural framework of cardiomyocytes after cell sheet transplantation into athymic nude rats in a 2-week-old myocardial infarction model compared to cell sheets of just IPSC derived cardiomyocytes (1). Direct injection of stem cells at the site of injury can also successfully heal small, damaged areas in the heart, but this is problematic for large areas, as the needle injection of a cellular suspension can induce necrosis and clumping of the injected cells (19). Thus, one area of focus is to improve adhesion between the transplanted and host cells to form dense tissues. One promising method is to use stem-cell-derived sheet engineering due to its ability to form vascularized networks to generate thickened cardiac tissue. Thus far, this engineered cell sheet transplantation has shown improvements in the clinical manifestations of heart failure in myocardial infarction and has played a significant role in minimizing cardiac dysfunction (19). In future research, strategies to support the transplanted cardiomyocyte tissues by promoting their functionality, maturity, and efficient production should be identified (18).
Modeling of Neurodegenerative Diseases
Neurodegenerative diseases are characterized by the progressive loss of neurons and brain tissue, which can lead to impairment in physical movement and cognition (2). Currently, neurodegenerative diseases are difficult to study and diagnose, given that the majority of cases are spontaneous. The sudden onset in largely elderly adults also suggests that both extrinsic factors, such as the environment, and intrinsic factors, such as abnormal cellular activity, contribute to the disease. There has been tremendous progress during the past few years in using IPSCs to target neurodegenerative diseases. One successful area is in disease modeling
which allows the studying of neural diseases by generating disease-induced neurons from IPSCs. For instance, Alzheimer's disease (AD) induced neurons that mimic the pathological characteristics and responses of the disease provide a promising platform for compound screening, studying disease mechanisms, and drug development and discovery (20).
Disease modeling has also advanced our understanding of other neuronal diseases. In one study, 17 genes have been identified to cause Parkinson’s disease when mutated through using IPSC reprogrammed cells (20). Another recent study discovered in Huntington’s disease-IPSC-derived neurons that FOXO transcription factors modulated proteasome activity, which could become a therapeutic target for the disease (20). In amyotrophic lateral sclerosis (ALS) IPSC-derived motor neurons, deficiencies in mitochondrial function are suggested to play a role in the onset of the disease (20).
Aside from recapitulating disease, IPSC has been successfully reprogrammed into healthy neurons. Endogenous cellular mechanisms and transcriptional feedback are retained in IPSC-derived cells, which is important for disease modeling. One recent study found IPSC-derived motor neurons to have similar efficiency and electrophysiological properties as cells derived from ESCs and brain-derived neural stem cells. Additionally, self-renewable, neural stem cells can be quickly generated (around 2 weeks) in large quantities with high reproducibility from IPSCs, although the purity of the colonies is unclear (20). These stem cells can be further differentiated into specific neuron types, including cortical neurons, GABAergic neurons, motor neurons, sensory neurons, serotonergic neurons, glutamatergic neurons, dopaminergic neurons, astrocytes, and oligodendrocytes (20). In the future, this technology may be further used to replenish and replace brain tissue and treat certain inherited or induced brain disorders caused by a lack of functional neurons.
Currently, most of the research involved in using IPSCs for neurodegenerative diseases is disease modeling and drug discovery rather than developing brain tissue for therapeutic applications. However, the successful reprogramming of IPSCs into neurons and the continuous recognition of limitations bring optimism for the future to move beyond the petri dishes and into therapeutic development and application to cure and reverse neurodegenerative diseases.
Wound Repair
As a human ages, the capacity to self-regenerate tissues and repair scar-free wounds diminishes. One study found that the transition from scar-free healing to scarring may occur as early as 24 weeks after human gestation (21). This capacity can be further affected through the genetic makeup and the development of an individual. Furthermore, the immune system plays a significant role in the efficiency of wound repair, affecting the remodeling of the extracellular matrix, restoring tissue homeostasis through clearing cellular debris, and producing cytokines and growth factors (21). Macrophages are also important in the woundhealing process, and dysfunctional macrophages have been observed to decrease the efficiency of wound repair through an abnormal production of growth factors and inflammatory mediators and a deficiency of anti-inflammatory factors (21). Consequently, the loss of tolerance in the immune system associated with the development of the adaptive immune system may affect the diminished capabilities of wound regeneration (21).
Before the transition to scarring, wound healing is characterized by minimal inflammation and increased expression of anti-inflammatory cytokines such as interleukin-10 (21). Unlike adult wound healing, other wound repair factors unique to the embryo include higher levels of type III collagen in the extracellular matrix, high levels of high-molecular-weight hyaluronic acid, and high expression of transforming growth factor beta-3 which is created by keratinocytes and fibroblasts (21).
Some major issues in the chronic wound healing environment are that it inhibits stem cell proliferation rate, expresses lower levels of growth factor receptors, and changes the expression of genes needed for wound healing in the cells (22). This slows down the generation and ability of new cells to repair a wound (22).
Excitingly, a diverse array of somatic cells have been successfully reprogrammed to treat open wounds. Human IPSC-derived smooth muscle cells (hiPSC-SMC) are demonstrated to promote angiogenesis, accelerate diabetic wound healing, and increase epidermal and muscle thickening to improve wound architecture through directly injected cells (23). Delivery of hiPSCSMC-containing collagen scaffolds accelerated diabetic wound healing and is associated with increased total macrophages (21).
Comparatively, adipose-derived stem cells (ADSC) can promote angiogenesis and vascularization, secrete growth factors, modulate immune responses, and induce epithelialization in the wound, and are shown to be safe and effective to treat radiation ulcers, Crohn's disease, and severe trauma (4). It also possesses the least limitations in clinical applications (4). However, it does not secrete as many pro-angiogenic cytokines and promote epidermal and muscle thickening as hiPSC-SMCs. Additionally, ADSC research is early in the stages and has not demonstrated consistent pure extractions which further limits its clinical use with low confidence in the mechanism of ADSC wound repair (4).
Ma and his team demonstrated that hair follicle dermal sheath-derived mesenchymal stem cells could fully close a wound in 18 days through direct injection of the cells to the site of injury (22). During this time, the cells stimulated angiogenesis, proliferation, and migration of keratinocytes and fibroblasts to the wound site which promoted epithelial growth (22). Another study showed that IPSC-derived endothelial cells could stimulate angiogenesis, increase fibroblast infiltration and collagen deposition (which is vital for health healing) to accelerate wound closure (24).
Despite the successful repair of wounds from IPSC-derived cells, earlier issues mentioned with IPSC therapy apply to IPSC wound repair including mutagenesis, potential immunogenicity, and inefficient reprogramming with low cell count (4). Additionally, poor cell survival and engraftment limit the long-term use of IPSC therapy where most cells die in the first 48 hours after administration (24). In addition to improving the efficiency and purity of IPSC therapy, one potential direction to advance wound repair is to increase the proliferation and localization of progenitor cells as the cells have been extensively studied to recruit other necessary cells like macrophages and keratinocytes and produce collagen types I and III (21).
Conclusion
Since the discovery of IPSCs, a plethora of research has pushed IPSC research in exciting and diverse directions. Unlike ESCs, IPSCs bypass ethical concerns by extracting cells from the patient without lasting harm. Additionally, IPSC therapy can be applied to a broad range of patients, as well as develop therapies for individuals, which may be revolutionary in both precision and personalized medicine.
Currently, a widely used application with IPSC technology is disease modeling which facilitates drug discovery and development, understanding disease mechanisms, and testing for adverse effects in therapeutic strategies. Specifically, the organ-on-achip method allows for simultaneous single or multiple organ observations as well as their interactions. This method can also reproduce human clinical responses to drugs, diseases, toxins, and pathogens. The supply of IPSC tissues and organs provides cost-effective and ethical modeling, reducing the need for testing in animal models and primary cell cultures (25).
Additionally, IPSC technology is applied to treat a diverse spectrum of diseases. Some of the most ambitious promises are treating chronic and degenerative diseases such as cardiovascular and neurodegenerative diseases which have been endorsed through disease modeling and the successful generation of neurons and cardiomyocytes. Another major advancement is observed in using IPSC therapy to accelerate the healing of chronic open wounds and ulcers.
Although cellular transformation has been successful, there are currently many limitations that prevent its clinical feasibility. Given the high mutagenesis rate, we must develop an efficient method to detect and purify the successful IPSC-induced cells apart from the mutated cells. Additionally, IPSC reprogramming, and proliferation are slow and inefficient, so it is not a reliable method to treat some conditions such as spinal cord injury and spontaneous diseases (26). Given the high influence of reprogramming factor expression and environmental stimuli, one potential area of focus is controlling and manipulating these external influences to increase efficiency and success.
Comparatively, little is known about the mechanisms that induce the IPSC reprogramming process. Increased understanding of this area in research will also lead to better control of mutagenesis and increase the efficiency of IPSC transformation.
Another limitation of IPSC therapy is the low survival rate of IPSC grafts. To date, there is very limited research exploring the long-term outcomes of IPSC engraftment which should be encouraged to account for potential adverse effects and overall feasibility.
In the industrial market, more funding and recognition are needed to support IPSC research. Currently, pharmaceutical industries do not endorse IPSC
research. High expenses not only come from a large amount of research and tissue samples required to successfully produce a small pool of healthy cells, but the extraction and long-term storage of patient cells increases expenses, currently requiring around six months in the reprogramming phase. This long duration will also not be feasible to treat certain illnesses that have a rapid fatality such as brain and heart tissue damage.
One potential area to improve IPSC therapy is to learn from the physiology and chemistry of embryonic development. As discussed previously, embryos possess different characteristics from adults in their immune responses that stimulate scar-free healing. In one study, increasing high-molecular-weight hyaluronic acid as seen in scar-free healing was found to be a safe and effective compound to increase the efficiency and epithelial growth in adult skin repair (21).
Identifying the weaknesses and limitations in IPSC research is a major step in the right direction. Further understanding the mechanism of IPSC reprogramming as well as the role of external influences is crucial to not only improve the process itself but to ensure successful long-term integration. The recent plethora and rapid diversification of IPSC research brings great optimism in the advent of lifesaving, cost-effective, and personalized therapies.
Acknowledgments
A special thank you to Gregory Shanower for his support and mentorship on this project.
References
1. Yamanaka S. Pluripotent stem cells-based cell therapy-promise and challenges. Cell Stem Cell 2020;27(4):523-531.
2. Karagiannis P, et al. Induced pluripotent stem cells and their use in human models of disease and development. Physiological Reviews. 2019;99(1): 79-114.
3. International Stem cell Initiative. Assessment of established techniques to determine developmental and malignant potential of human pluripotent stem cells. Nature Communications 2018;9(1).
4. Hassanshahi A, et al. Adipose-derived stem cells for wound healing. Journal of Cellular Physiology 2018;234(6):7903–7914.
5. New steps forward in cell reprogramming. Hsci. harvard.edu, hsci.harvard.edu/new-steps-forwardcell-reprogramming.
6. Gorecka J, et al. The potential and limitations of induced pluripotent stem cells to achieve wound healing. Stem Cell Research & Therapy. 2019;10(1).
7. Rowe G, George D. Induced pluripotent stem cells in disease modeling and drug discovery. Nature Reviews Genetics. 2019.
8. Bar S, Nissim B. Epigenetic aberrations in human pluripotent stem cells. The EMBO Journal 2019;38(30).
9. Okita K, Shinya Y. Induced pluripotent stem cells: Opportunities and challenges. Philosophical Transactions of the Royal Society B: Biological Sciences. 2011;366(1575):2198–2207.
10. Yokoi T, et al. Long-term survival of transplanted induced pluripotent stem cells-derived neurospheres with nerve conduit into sciatic nerve defects in immunosuppressed mice. Biochemistry and Biophysics Reports. 2021;26(100979).
11. Shi Y, et al. Induced pluripotent stem cells technology: A decade of progress. Nature Reviews Drug Discovery. 2016;16(2):115–130.
12. Hanna J, et al. Treatment of sickle cell anemia mouse model with iPS cells generated from autologous skin. Science. 2007;318(5858):1920-3.
13. Masters C, Bateman R, Blennow K. et al. Alzheimer's disease. Nat Rev Dis Primers. 2015.
14. Next-generation disease modeling: CRISPR editing in iPSCs. Synthego. 2024.
15. Zhao C, Makoto I. Generation and applications of induced pluripotent stem cells-derived mesenchymal stem cells. Stem Cells International 2018;2018:1–8.
16. Mayo Clinic. Heart failure - Symptoms and causes. Mayo Clinic, Mayo Clinic. 2021.
17. Takaoka N, Yamane M, Obara K, et al. Hairfollicle-associated pluripotent. HAP, stem cells differentiate into mature beating cardiomyocyte sheets on flexible substrates in vitro. Med Mol Morphol. 2022;55: 248–257.
18. Yoshida S, et al. Maturation of human induced pluripotent stem cell-derived cardiomyocytes by soluble factors from human mesenchymal stem cells. Molecular Therapy. 2018;26(11):2681–2695.
19. Guo R, Morimatsu M, Feng T. et al. Stem cellderived cell sheet transplantation for heart tissue repair in myocardial infarction. Stem Cell Res Ther 2020;11(19).
20. Farkhondeh A, et al. Induced pluripotent stem cells for neural drug discovery. Drug Discovery Today 2019;24(4):992–999.
21. Xia H, Li X, Gao W, et al. Tissue repair and regeneration with endogenous stem cells. Nat Rev Mater 3. 2018;174–193.
22. Kucharzewski M, et al. Novel trends in application of stem cells in skin wound healing. European Journal of Pharmacology. 2019;843(15):307–315.
23. Clayton Z, et al. Induced pluripotent stem cellderived endothelial cells promote angiogenesis and accelerate wound closure in a murine excisional wound healing model. Bioscience Reports 2018;38(4).
24. Nourian D, Mirahmadi B, Chehelgerdi M. et al. Skin tissue engineering: wound healing based on stemcell-based therapeutic strategies. Stem Cell Res Ther. 2019;10(111).
25. Paik D, et al. Patient and disease–specific induced pluripotent stem cells for discovery of personalized cardiovascular drugs and therapeutics. Pharmacological Reviews. 2019;72(1):320–342.
26. Doss X, Agapios S. Current challenges of iPSC-based disease modeling and therapeutic implications. Cells. 2019;8(5):403.
A Patient-Empowering, Financially Sustainable Implementation Framework in the Emergency Department: Geisinger ProvenCare Pneumonia
Niraj Vyas1†, Mark White1, and Chadd Kraus2
1Geisinger Commonwealth School of Medicine, Scranton, PA 18509
2Lehigh Valley Health Network, Allentown, PA 18103
†Doctor of Medicine Program
Correspondence: nirajjvyas@wustl.edu
Abstract
Background: The implementation framework for Geisinger ProvenCare to be created in this study aims to be scalable, utilizes identified facilitators, accounts for identified barriers, and maintains financial sustainability while effectively treating patients with pneumonia.
Methods: ProvenCare pneumonia (PNA) assigns patients to hospitalization or emergency departmentto-home (EDTH), leveraging non-hospital resources (e.g., care management, remote monitoring) to avoid hospitalization using clinical judgment combined with objective risk stratification tools (e.g., pneumonia severity index/PSI). Care algorithms aim to standardize care, including antibiotic stewardship. EDTH patients are discharged with a PNA kit, including pulse oximetry, and close follow-up with care management and home care resources.
Results: This study evaluated 3,338 patients, all of whom were hospitalized. ProvenCare PNA has enrolled 883 patients. The mean age of patients was 68.4 years (SD = 18.4). The mean length of stay was 3.981 days (SD = 3.039). Patients enrolled in ProvenCare PNA were hospitalized for significantly longer (p < 0.001) and were more likely to be re-hospitalized (p < 0.001) compared to the non-enrolled group. Patients enrolled in ProvenCare PNA had a significantly higher mortality at every interval up to 90 days (p < 0.001). However, there was a larger total amount of savings for patients enrolled in ProvenCare PNA (p = 0.011).
Conclusion: Implementation of an evidence-based, resource-dedicated EDTH program for patients with PNA is challenging. All patients were hospitalized. Barriers to implementation include defining pneumonia diagnoses, determining illness severity, adapting inpatient order sets, and showing financial and quality
measure outcomes. Future research should focus on adaptations of the model with a larger sample of patients to ensure sustainability. The creation of an innovation center would help with this endeavor.
Introduction
Geisinger ProvenCare
In 2005, the executive leadership of Geisinger Health (Geisinger) accepted a challenge to prove that a large integrated health care system, supported by EMR, could successfully transform a complex clinical process to decrease unnecessary differences in care and consistently provide evidence-based treatment for patients with a specific medical condition (1).
They began with elective coronary artery bypass grafting (CABG) and showcased that an improvement model incorporating evidence-based medicine into the workflow, applying reliability science principles such as standardization, error prevention, and redesigning failure modes to the process, utilizing effective data feedback strategies, and involving patients in their care, leads to the consistent delivery of appropriate care with improved patient outcomes (2). This model was named ProvenCare and was subsequently extended to elective total hip replacement and cataract surgery (3).
In 2007, Geisinger applied the ProvenCare model to percutaneous coronary intervention (PCI) (3), which required multiple interconnected microsystems to establish a reliable pathway. A clinical microsystem refers to a small group of individuals working together regularly to provide care to specific patient subpopulations. It encompasses clinical and business goals, interconnected processes, a shared information environment, and yields performance outcomes. These interlinked microsystems formed a new PCI mesosystem, supporting the provision of care to
this patient population. A mesosystem represents an interconnected collection of peer microsystems that provide care or support care for specific patient populations. The purposeful integration of care microsystems into ProvenCare mesosystems (such as CABG and total hip replacement) through the application of reliability science-driven redesign has enabled Geisinger to consistently deliver evidencebased care, one patient at a time (4).
Geisinger's ProvenCare serves as evidence that the integration of multiple improvement concepts (evidence-based guidelines, data feedback, reliability science) within a unified design model can effectively reduce unnecessary variations in health care delivery. The aim of ProvenCare has three components: decrease complication and mortality rates, increase the efficacy of health care delivery, and eliminated unwarranted variation in providing evidence-based care (1).
Defining Pneumonia
Generally, pneumonia (PNA) is defined as an infection of pulmonary parenchyma caused by various organisms. Harrison emphasized that PNA comprises a group of distinct infections, each with its own unique epidemiology, pathogenesis, presentation, and clinical course (5). While the textbook acknowledges the differentiation between lobar and bronchopneumonia based on pathological characteristics, it suggests that PNA classification should primarily revolve around the specific microorganism responsible for the infection. Furthermore, the microbial cause remains unidentified in over a third of patients, particularly in children, where a blood culture is often the sole diagnostic test performed. However, it is important to note that this blood culture test yields a positive result in only 5%–10% of patients and possibly up to 20% in severely ill individuals (6).
The absence of a widely accepted and commonly understood definition for PNA presents a significant challenge in accurately categorizing diverse pathologies and clinical manifestations. This lack of clarity hinders clinical decision-making and may lead to poorly designed research studies. The extent of this issue becomes apparent when health care professionals struggle to identify the infectious agents responsible for lung infections, resulting in the need for empirical antibiotic treatment. If a specific diagnosis could be established, targeted therapy with comparable effectiveness to broad-spectrum empirical treatment
could be administered, thereby reducing the unnecessary prescription of broad-spectrum antibiotics and the associated risks of antibiotic resistance (7).
To assess short-term mortality in individuals with community-acquired pneumonia (CAP), the Pneumonia Severity Index (PSI) was initially developed as part of the Pneumonia Patient Outcomes Research Team (PORT) project (8). Additionally, the intent was to identify patients with CAP who have a low risk of mortality upon presentation utilizing easily accessible clinical information. There were 20 prognostic variables associated with mortality that physicians routinely had access to during a patient's initial examination: 3 demographic characteristics (age, sex, and nursing home residence), 5 concurrent illnesses (active neoplastic disease, congestive heart failure, cerebrovascular disease, renal disease, and liver disease), 5 physical examination findings (pulse rate, respiratory rate, systolic blood pressure, temperature, and mental status), 6 laboratory measurements (blood urea nitrogen, glucose, hematocrit, sodium levels, partial pressure of arterial oxygen, and arterial pH), and 1 radiographic finding (pleural effusion). The primary outcome measured was in-hospital mortality within 30 days after admission. The PSI was developed in two steps to better align with physicians' decisionmaking processes in the office or ED. Step 1 identified a subgroup of patients at an extremely low risk of death (classified as risk class I) solely based on the presence or absence of 11 medical history and physical examination findings. In Step 2, the risk of death was assessed for the remaining patients (non-risk class I) by incorporating the same findings used in Step 1, along with the laboratory and radiographic variables that constitute the PSI. Each prognostic variable was assigned an integer-based weight, and the total point score was calculated by summing these weights for a given patient. Based on the total point score, patients were then categorized into four additional risk classes (II–V), each indicating an increased probability of mortality (9).
Implementation Science
Implementation science (IS), while existing as a scientific field for over 20 years, has only emerged into the spotlight within medicine in the last decade. IS is “applied research that aims to develop the critical evidence base that informs the effective, sustained, and embedded adoption of interventions by health systems and communities” (10). In other words, the aim
is to study the method by which research findings and evidence-based interventions (EBIs) are incorporated into routine practice and analyzing this process to improve quality of care and delivery (11). As a result, IS works closely with translational science to increase the likelihood of EBIs incorporation in patient care.
IS aims to gain understanding of the procedures involved in bringing about practice transformation and the results derived from such changes. Effective research methodologies combine the assessment of clinical effectiveness with appropriate implementation research. These integrated research designs evaluate the process of change and assess patient outcomes within the same study. The approach to implementation may vary, and hybrid designs — those taking into account clinical effectiveness and implementation — have been proposed. These hybrid designs include features such as simultaneous evaluation of relevant outcomes during data collection, testing of both clinical and implementation processes, and evaluation of the implementation process based on the EBI’s impact (12, 13). Irrespective of the specific approach, all hybrid research designs deliberately strive to systematically document both patient and process outcomes, ideally predetermined as part of the experimental design (14).
The evaluation of EBI implementation is accomplished via the concept of a framework, which use metatheoretical language to compare theories, provide organization to diagnostic inquiries, and identify components of systems that require analysis and reevaluation. A framework is one of three levels utilized in IS; the other two are theories and models. Frameworks are used to identify elements and relationships between them. Additionally, they provide a general list of variables, as well as metatheoretical language for comparing theories, organizing diagnostic and prescriptive inquiry, and generating questions for analysis (15). Frameworks can be extensive paradigms that emphasize professional consensus within a scientific community. They do not need to specify the direction of relationships or identify critical hypotheses (16). Theories make general working assumptions about specific elements of a framework. Theories can be utilized to diagnose phenomena, explain their processes, and predict outcomes. Several theories can function within a single framework. Models are used to systematically assess the consequences of assumptions made about a limited set of parameters and variables (17). They can be used to test conceptual coherence between different levels of IS (16).
In the absence of systematic, comparative evaluations of institutions, recommendations and interventions may rely on superficial notions rather than performance analysis. In this case, institution refers to shared concepts utilized by actors in action situations with repetitive patterns of interaction defined by appropriate exogenous variables. It is crucial to utilize a shared framework encompassing a suitable range of theories to tackle reform-related inquiries. Subsequently, customized models are employed to forecast the outcomes of these simplified structures. Errors may arise when unsuitable models are utilized to examine complex situations that deviate from the model's assumptions. Consequently, institutions face difficulties in adapting to dynamic environments, leading to a negative impact on the sustainability of resources and investments.
Previous Attempts at Framework Creation
Various frameworks have been developed for medical use, but they tend to either focus on specific procedures or lack practicality for everyday application. One widely used framework is the Promoting Action on Research Implementation in Health Services (PARiHS), which is broad but criticized for its limited utilization of theory (18). Another framework, the Exploration, Preparation, Implementation, Sustainment (EPIS) model, lacks scalability and detail necessary for clinical use, and its user networks and factor operationalization could be improved (19). The Consolidated Framework for Implementation Research (CFIR) lacks a method to evaluate financial aspects, leading to frequent mention of economic barriers (20). Similarly, the Triple P Implementation (TPI) framework faces economic obstacles in its implementation (21).
Health care workers' perceptions and experiences play a crucial role in framework assimilation, often outweighing established guidelines or contraindications (22). Therefore, stakeholder input and medical education are vital in the framework development process. However, a framework should not be a rigid algorithm but rather integrate stakeholder experience to enhance patient outcomes (21). Balancing flexibility and rigor can be achieved by applying Weiner's theory of organizational readiness for change (23). Lastly, highlevel leadership support is crucial for sustainability and effective framework implementation. Establishing a research department, such as an innovation center, has been shown to improve patient outcomes by enhancing care quality and reducing costs, thus increasing the
likelihood of leadership buy-in through improved economic efficiency and research grants (24).
Interventions in Emergency Medicine
Emergency implementation science (EIS) is a rapidly expanding subfield of IS. EIS encompasses various sectors, subjects, and changes occurring at individual, service unit, organizational, or systemwide levels. It involves coordinating multilevel changes as well as rapid modifications to computer systems, including database linkage, simulation models, and the application of machine learning and artificial intelligence for learning and feedback (25).
There are three components to implementation of changes in an emergency setting: 1) decision-makers must act with limited information; 2) the changes often lack testing or strong supporting evidence; and 3) researchers must swiftly find and provide evidence on rapidly implementable changes, offer feedback during and after the change, and monitor the process to ensure immediate utility for decision-makers (25).
An implementation framework is crucial for the field of emergency medicine and the patients treated in EDs. Previous EBPs in this area have often overlooked IS or faced obstacles that hindered their effective integration. For instance, Kotter's Change Management Model (KCMM) has been proposed as a means to bring about change in emergency medical education, particularly in didactic settings. However, there is a lack of quantitative and objective evaluation methods, such as assessing training exam scores or medical knowledge milestones, to measure its effectiveness (26). Likewise, the Milestone Project, which aimed to implement changes in emergency medical education, encountered challenges related to resource limitations and inadequate execution at various levels (27).
There are several aspects within emergency medicine that could greatly benefit from the adoption of an implementation framework. For example, the assessment of cardiopulmonary resuscitation (CPR) quality by most ED physicians relies solely on visual observation, with no established procedures for obtaining quantitative CPR feedback (28). Similarly, there is a dearth of standardized and validated measures for end-of-shift handovers in the ED, and previous attempts to develop tools for this purpose have failed to account for scalability beyond a single site (29). Clinical workflow also varies across different EDs, even within the same health care system, due to
diverse patient populations. Consequently, there is a lack of a framework that defines the data elements within electronic medical records (EMR) for quantifying ED patient outcomes (30).
One of the identified barriers to initiating the implementation of EBPs in these areas is the discomfort experienced by health care workers in the dynamic clinical environment (31). Additionally, certain EBPs have encountered technical barriers that impeded effective communication (32). If the proposed complex implementation framework were to be implemented, it would necessitate significant redevelopment within the field of emergency medicine. Therefore, a comprehensive reassessment of the current system and meticulous planning involving all stakeholders would be essential to ensure successful integration (33). New research designs, evaluative methods, collaboration systems with stakeholders are just some of the opportunities that EIS has to offer. EIS showcases the potential of IS to stakeholders by delivering quick and credible information that lends to quick implementation. Most importantly, this science directly impacts patient care, allowing for increased positive outcomes (25).
Objective
The implementation framework for Geisinger ProvenCare to be created in this study aims to be scalable, utilizes identified facilitators, accounts for identified barriers, and maintains financial sustainability while effectively treating patients diagnosed with pneumonia in the emergency department (ED). After the creation and validation of the framework, this work would propose the introduction of an innovation center to manage implementation and alteration of evidencebased practices (EBPs) via the proposed framework to increase positive patient outcomes in the ED.
Methods
Study Setting
Geisinger is an integrated health delivery system that serves a population of approximately 1 million patients in central and northeastern Pennsylvania. The framework created in this study was implemented at EDs at all Geisinger hospitals.
Study Population
All patients 18 years and older with a PNA diagnosis in the ED were included in this study.
Study Design
Upon arrival to the ED, patients are evaluated via standard of care and assigned a clinical diagnosis of PNA. PNA presents with a number of signs and symptoms: cough, dyspnea, purulent sputum, nausea, vomiting, diarrhea, hemodynamic instability, increasing oxygen requirements, and fever. A chest X-ray may demonstrate lung infiltrates or pleural effusions. However, there is no specific set of signs and symptoms that must be present. A patient may be considered for enrollment if the evaluating physician determines that PNA is the most likely diagnosis based on clinical judgment.
An ED provider performed objective risk stratification via PSI to assign patients to hospitalization or the ED-to-home (EDTH) arm. These providers received training to ensure appropriate order sets are used for the study.
Patients determined to be Risk Class I were discharged to home with a scheduled follow-up appointment with their primary care provider (PCP). Risk Class II or III patients were discharged to home with a PNA kit, including pulse oximetry, and close follow-up with case management and home care resources. Risk Class IV or V patients were hospitalized with post-discharge case management follow-up.
Data Collection and Analysis
Patients with a PNA diagnosis in the ED were automatically selected via EMR data collection. Additional demographic information included age, ED location, length of stay in the hospital, diagnosis code, readmission up to 90 days, PCP follow-up scheduling and completion, mortality up to 90 days, total amount of savings, and whether the patient had Geisinger health insurance. Considered intervals for the data included in-hospital, 30 days, 60 days, and 90 days. The collected data was stratified into two groups: patients enrolled in ProvenCare PNA and patients who were removed or not enrolled.
Continuous variables were descriptively summarized using mean and standard deviation and were displayed using violin plots. To compare continuous variables, notably length of stay and total amount in saving, between the enrolled and non-enrolled groups, linear ANOVA was performed. Categorical variables, with the exception of ED location, had binary outcomes. They were reported using percentages and were displayed using stratified bar charts. Pearson’s chi-squared test
was performed to compare categorical outcomes between the enrolled and non-enrolled groups. All analyses were performed in the R statistical package (R Core Team 2023).
Results
This study evaluated 3,338 patients, all of whom were hospitalized after evaluation in the ED (Table 1). Of those patients, 833 were enrolled in ProvenCare PNA. The remaining 2,455 patients were either removed or declined ProvenCare participation. The mean age of patients was 68.4 years (SD = 18.4), and 1,199 patients (35.9%) had Geisinger health insurance. The mean length of stay was 3.981 days (SD = 3.039). One thousand and three patients were re-hospitalized, and 361 patients died within 90 days after discharge. Follow-up was scheduled with a PCP within 1 week of discharge for 454 patients (14.8%); 274 patients completed this scheduled visit. It should be noted that an additional 228 patients visited their PCP within 1 week of discharge, despite not having an appointment scheduled at time of discharge. When comparing the outcomes of patients enrolled in ProvenCare PNA to those who were not enrolled, there was not a difference in proportion of patients who had Geisinger insurance. Compared to the non-enrolled group, patients enrolled in ProvenCare PNA were more likely to be re-hospitalized at every measured interval up to 90 days (p < 0.001) (Figure 1A) and were hospitalized for significantly longer (p < 0.001) (Figure 2). There was no difference in in-hospital mortality, 7-day follow-up scheduling, or 7-day follow-up completion between the two groups. Patients enrolled in ProvenCare PNA had a significantly higher mortality at every interval up to 90 days (p < 0.001) (Figure 1B).
Discussion
There are many lessons to be learned from the challenges encountered during the creation of this framework. Many of these barriers were encountered during the initial integration of the framework into the clinical space. A clear definition of a PNA diagnosis has been a longstanding controversy in medicine, particularly in the ED where the condition may present similarly to upper respiratory infections, congestive heart failure, and chronic obstructive pulmonary disease. This framework utilized PSI as a method of objectively determining risk class, likelihood of mortality, and the need for hospitalization. However, PSI is not a perfect tool. In some instances, patients
may have received a presumptive PNA diagnosis with high enough severity for hospitalization but were found to have a different etiology once admitted to the floor. Conversely, some patients may have received a different primary diagnosis requiring hospitalization but were found to have PNA during their admission. The latter scenario became a particular concern for patients admitted with COVID-19, as they may have developed subsequent PNA.
The incorporation of order sets for each arm of the study was a significant barrier. Stakeholders in both the emergency and information technology departments are required to determine the items that should be included in each order set. A large amount of time and resources are required for the integration of the order sets into the EMR software. Additionally, ED physicians received training to ensure the appropriate order set utilization for patients enrolled in ProvenCare PNA.
Table 1. Comparison by enrollment in ProvenCare PNA
No patients were enrolled in the at-home arm of ProvenCare PNA due to a number of challenges encountered. Without any patients in this arm, it is impossible to determine facilitators of implementation or the extent of scalability of the framework in the outpatient realm. In fact, the at-home arm was discontinued entirely and reincorporated into the
Geisinger Acute Care at Home (ACaH) program. This transition addressed many of the barriers faced by the ProvenCare program; however, it should be noted that ACaH does not require the same metrics as ProvenCare, notably financial data. Additionally, ACaH utilizes the same inclusion criteria as ProvenCare PNA with an additional requirement that the patient lives within a 20-mile radius of Geisinger Wyoming Valley Medical Center. The exclusion criteria limits the severity of patients eligible for ACaH. Patients with PSI score greater than 130, no evidence of lung infiltrate on chest imaging, active lung cancer undergoing chemotherapy or radiation, endstage renal disease on dialysis, severe immunosuppression, new pulmonary embolism, cavitary lesions or empyema, or pulmonary fibrosis were excluded from enrollment. These restrictions narrowed the complexity of patients, an important limitation to the ProvenCare program.
ProvenCare PNA was created with the intention to be financially sustainable, meaning the implementation of this framework would reduce financial costs to both the patient and the system. Unfortunately, it is difficult to clearly describe facilitators and scalability of this framework at this time. While patients enrolled into ProvenCare PNA were more likely to have negative outcomes compared to those enrolled, there is no distinction in the complexity of the patients between the two groups. Without access to patient comorbidity or illness severity, there is no way to determine if the enrolled, hospitalized patients were, by the nature of their medical complexity, at a higher risk of mortality and rehospitalization.
Figure 1. A) Readmissions by ProvenCare PNA enrollment. B) Mortality by ProvenCare
enrollment
As a result, there is no way to determine the true patient and organizational cost of a patient’s stay with current information technology infrastructure in place. Further research and having this additional information would help assess the true efficacy and financial outcomes of ProvenCare PNA.
Lastly, there is a limitation in the patient population (northeastern and central Pennsylvania) sampled and its generalizability. There was a significant difference in the proportion of people enrolled into ProvenCare PNA between the various Geisinger hospitals. This difference may be a result of inconsistent education or knowledge about the new ProvenCare PNA program or enrollment may have been skipped due to other pressing clinical concerns. Additionally, it is possible that these patients have a PCP outside of the Geisinger system. As a result, scheduling and follow-up with their PCP would not be able to be tracked.
Conclusion
This study aimed to create an implementation framework that is scalable, utilizes identified facilitators, accounts for identified barriers, and maintains financial sustainability. While this framework was not able to accomplish all these goals, there is a good foundation with a potential to meet the goals with continued work. This framework identified many barriers and overcame some of them. Many others can still be addressed with changes, especially regarding data collection. There are numerous facilitators identified in the hospitalization arm, but none were identified in the EDTH arm. Similarly, there is evidence to show that the inpatient arm is scalable across the health system, but there is no information about the EDTH arm. Restructuring of the EDTH arm with increased resources to track metrics in the outpatient realm may address these concerns.
Figure 2. Length of stay by ProvenCare PNA enrollment
ProvenCare
Secondly, this project assessed a proposal for the creation of an innovation center. Given the barriers encountered during the creation of this framework, this health system would benefit greatly from an innovation center, where staff dedicated to identifying EBPs can systematically create ProvenCare programs. These individuals would be tasked with quality assurance and evaluation of the implementation systems in place. Previous studies have demonstrated that a center of this type is at minimum financially self-sustaining, if not more, with the savings to the system and the patient from the process (34–36). With such a system in place, Geisinger and ProvenCare can look to expanding on the framework created in this study and work toward patient-empowering designs.
Acknowledgments
I would like to express my deepest appreciation to the committee members: Dr. Chadd Kraus, Dr. H. Lester Kirchner, and Dr. Mark White. You all have provided invaluable guidance and feedback throughout this four-year journey. Without your wisdom, expertise, and patience, I would not have been able to complete this work, which will undoubtedly define my research career.
Disclosures
The author has no financial disclosures to report.
References
1. Katlic MR, Facktor MA, Berry SA, McKinley KE, Bothe A, Steele GD. ProvenCare lung cancer: A multi-institutional improvement collaborative. CA Cancer J Clin. 2011;61:382–96.
2. Casale AS, Paulus RA, Selna MJ, Doll MC, Bothe AE, McKinley KE, et al. “ProvenCareSM”: A provider-driven pay-for-performance program for acute episodic cardiac surgical care. Ann Surg 2007;246:613–21.
3. McKinley KE, Berry SA, Laam LA, Doll MC, Brin KP, Bothe A, et al. Clinical microsystems, Part 4. Building innovative population-specific mesosystems. Jt Comm J Qual Patient Saf 2008;34:655–63.
4. Nelson EC, Batalden PB, Godfrey MM. Quality by design: A clinical microsystems approach. 2007.
5. Levison ME. Pneumonia, including necrotizing pulmonary infections (lung abscess). Harrison’s Principles of Internal Medicine, 1994, p. 1184–91.
6. McNally LM, Jeena PM, Gajee K, Thula SA, Sturm AW, Cassol S, et al. Effect of age, polymicrobial disease, and maternal HIV status on treatment response and cause of severe pneumonia in South African children: A prospective descriptive study. Lancet. 2007;369:1440–51.
7. Van Der Eerden MM, Vlaspolder F, De Graaff CS, Groot T, Bronsveld W, Jansen HM, et al. Comparison between pathogen directed antibiotic treatment and empirical broad spectrum antibiotic treatment in patients with community acquired pneumonia: A prospective randomised study. Thorax. 2005;60:672–8.
8. Fine MJ, Auble TE, Yealy DM, Hanusa BH, Weissfeld LA, Singer DE, et al. A prediction rule to identify low-risk patients with community-acquired pneumonia. Pneumologie. 1997;51:834.
9. Aujesky D, Fine MJ. The pneumonia severity index: A decade after the initial derivation and validation. Clin Infect Dis. 2008;47 Suppl 3:S133–9.
10. Allotey P, Reidpath DD, Ghalib H, Pagnoni F, Skelly WC. Efficacious, effective, and embedded interventions: Implementation research in infectious disease control. BMC Public Health 2008;8.
12. Curran GM, Bauer M, Mittman B, Pyne JM, Stetler C. Effectiveness-implementation Hybrid Designs. Med Care. 2012;50:217–26.
13. Landes SJ, McBain SA, Curran GM. An introduction to effectiveness-implementation hybrid designs. Psychiatry Res. 2019;280:112513.
14. Williams JK, Feero WG, Leonard DGB, Coleman B. Implementation science, genomic precision medicine, and improved health: A new path forward? Nurs Outlook. 2017;65:36–40.
15. Ostrom E. Institutional Rational Choice: An Assessment of the Institutional Analysis and Development Framework. Theories of the Policy Process, 1999.
16. Kitson AL, Rycroft-Malone J, Harvey G, McCormack B, Seers K, Titchen A. Evaluating the successful implementation of evidence into practice using the PARiHS framework: Theoretical and practical challenges. Implementation Science. 2008;3.
17. Ostrom E. Institutional Rational Choice: An Assessment of the Institutional Analysis and Development Framework. Theories of the Policy Process, 2019, p. 21–64.
18. Ullrich PM, Sahay A, Stetler CB. Use of implementation theory: A focus on PARIHS. Worldviews Evid Based Nurs. 2014;11:26–34.
20. Merlo G, Page K, Zardo P, Graves N. Applying an Implementation Framework to the Use of Evidence from Economic Evaluations in Making Healthcare Decisions. Appl Health Econ Health Policy 2019;17:533–43.
21. McWilliam J, Brown J, Sanders MR, Jones L. The Triple P Implementation Framework: the Role of Purveyors in the Implementation and Sustainability of Evidence-Based Programs. Prevention Science 2016;17:636–45.
22. Zubkoff L, Carpenter-Song E, Shiner B, Ronconi JM, Watts B V. Clinicians’ Perception of Patient Readiness for Treatment: An Emerging Theme in Implementation Science? Administration and Policy in Mental Health and Mental Health Services Research. 2016;43:250–8.
23. Malterud K, Aamland A, Iden KR. Small-scale implementation with pragmatic process evaluation: A model developed in primary health care. BMC Fam Pract. 2018;19.
24. Allen K, Hazelett S, Martin M, Jensen C. An Innovation Center Model to Transform Health Systems to Improve Care of Older Adults. J Am Geriatr Soc. 2020;68:15–22.
25. Øvretveit J. Emergency Implementation Science. Implementation Science: The Key Concepts, 2022, p. 127–9.
26. Haas MRC, Munzer BW, Santen SA, Hopson LR, Haas NL, Overbeek D, et al. #DidacticsRevolution:
Applying Kotter’s 8-Step Change Management Model to Residency Didactics. West J Emerg Med 2019;21:65–70.
27. Sheng AY. Trials and tribulations in implementation of the emergency medicine milestones from the frontlines. West J Emerg Med. 2019;20:647–50.
28. Wright N, Lin Y, Cheng A. How is quality of cardiopulmonary resuscitation being assessed? A national survey of Canadian emergency medicine physicians. Canadian Journal of Emergency Medicine 2019;21:744–8.
29. Kwok ESH, Clapham G, White S, Austin M, Calder LA. Development and implementation of a standardised emergency department intershift handover tool to improve physician communication. BMJ Open Qual. 2020;9:e000780.
30. Tan A, Durbin M, Chung FR, Rubin AL, Cuthel AM, McQuilkin JA, et al. Design and implementation of a clinical decision support tool for primary palliative Care for Emergency Medicine (PRIM-ER). BMC Med Inform Decis Mak. 2020;20:13.
31. Chuang E, Cuartas PA, Powell T, Gong MN. “We’re Not Ready, But I Don’t Think You’re Ever Ready.” Clinician Perspectives on Implementation of Crisis Standards of Care. AJOB Empir Bioeth. 2020;11:148–59.
32. Weston BW, Gaither J, Schulz K, Srinivasan S, Smith JJ, Colella MR. Innovative approaches to emergency medical services fellowship challenges. West J Emerg Med. 2020;21:429–33.
33. Thomas TL. Developing and implementing emergency medicine programs globally. Emerg Med Clin North Am. 2005;23:177–97.
34. Bhattacharyya O, Shapiro J, Schneider EC. Innovation Centers in Health Care Delivery Systems: Structures for Success. J Med Internet Res 2022;24:e33961.
35. Lewis CC, Hannon PA, Klasnja P, Baldwin L-M, Hawkes R, Blackmer J, et al. Optimizing Implementation in Cancer Control (OPTICC): Protocol for an implementation science center. Implement Sci Commun. 2021;2:44.
36. Glasgow RE, Ford BS, Bradley CJ. Implementation science for cancer control: One center’s experience addressing context, adaptation, equity, and sustainment. Transl Behav Med. 2023.
Impact of Fragmented Care on Survival and Textbook Outcomes in Rectal Cancer: An NCDB Study
Theresa Anne Koch-Tran1†‡, Madison Wivell1†‡, Olivia Granja1†, Ayobami Fatunmbi2, Shengxuan Wang2, Rebecca Hoffman2, and Joseph Blansfield2
1Geisinger Commonwealth School of Medicine, Scranton, PA 18509
Background: Rectal cancer is treated with multimodal therapy. This leaves patients vulnerable to receiving fragmented care (FC). The goal of therapy is to achieve a textbook oncologic outcome (TOO). TOO is a composite quality metric that takes into consideration several variables that are used to define optimal outcomes for patients undergoing oncologic surgeries. The aim of this study was to determine if receiving FC has an impact on rectal cancer patients’ likelihood of achieving a TOO.
Methods: Patients diagnosed with rectal cancer between 2006 and 2018 and had their data reported to the National Cancer Database were included in this retrospective cohort study. Univariate and multivariate analysis were performed.
Results: This study included 96,941 patients; 26% received FC. Overall, 28% of patients achieved a TOO; 33% of patients who received FC achieved a TOO versus 26% of patients who received IC achieved a TOO. Patients who received FC traveled slightly farther than their IC counterparts (33.6 versus 30.2 miles, p<0.001). Treatment for FC patients was also slightly delayed (36.5 versus 34.9 days from diagnosis to treatment, p<0.001). FC was associated with a higher likelihood of TOO (OR 1.36, 95% CI: 1.32-1.41). Patients who had FC had an improved overall survival with a P<0.0001.
Conclusion: Fragmented care is associated with improved survival in patients treated for rectal cancer. Fragmented care also improves the likelihood of achieving a TOO for these patients. While traveling to more than one institution for cancer care can be inconvenient for patients, it appears that it improves patient outcomes.
Introduction
Rectal cancer is a complex malignancy and is associated with high mortality rates (1,2). Over the years an increase in the use of multimodality treatments — chemotherapy, radiation and surgery for locally advanced disease — have improved the survival rate, however the overall survival rate is still below 70% (3). Rectal resection is a critical component of the multimodality treatment, but surgery can be complex and is typically performed by specialists (4). The complexity of rectal cancer operations has led to the centralization of care for rectal cancer patients, allowing patients to receive treatment at high-volume centers specializing in the care of rectal cancer patients. Centralization of this complex procedure has led to improved surgical morbidity; however, centralization of care may come at the cost of potential care fragmentation (1, 4–8).
Fragmentation of care (FC) is defined as receiving various aspects of cancer care at more than one health system or hospital. FC has been shown to impact patients negatively by increasing the travel distance for care, as well as to delay the time to start treatment (9). Therefore, although it seems that centralization of surgical care to high-volume hospitals may improve outcomes, fragmentation of multimodality care may diminish these effects (7, 8).
The measurement of quality has become a key factor for the evaluation of cancer care delivery. There have been multiple ways to define the quality of care, but all metrics have positives and negatives. Textbook oncological outcomes (TOO) has recently become a well-studied quality metric for comparing cancer care because it considers multiple factors important in cancer care delivery. TOO takes postoperative complications, hospital length of stay, readmission rates, morbidity, and mortality into account and
therefore encompasses the entire gamut of patient care (10). As such, it may be a better-quality metric. The achievement of TOO has been shown to improve overall survival for patients with cancer (11, 12).
To date, no studies have determined the impact that FC has on TOO. Thus, the aim of this study was to examine the impact fragmentation of care has on the achievement textbook oncological outcomes for rectal cancer.
Methods
The National Cancer Database (NCDB) is a joint project of the Commission on Cancer (CoC) of the American College of Surgeons (ACS) and the American Cancer Society. The NCDB, established in 1989, is a nationwide, facility-based, comprehensive clinical surveillance resource oncology data set that currently captures 72% of all newly diagnosed malignancies in the U.S. annually (13). The data used in the study are derived from a de-identified NCDB file. The American College of Surgeons and the Commission on Cancer have not verified and are not responsible for the analytic or statistical methodology employed, or the conclusions drawn from these data. Due to the deidentified nature of the data, this study was deemed to be exempt by the Institutional Review Board.
Patients who received a diagnosis of primary rectal cancer between 2006 and 2018 were included in this study. Patients who were missing demographic information, information for TOO criteria, data for the
time between diagnosis and surgery/chemo, patients who were missing survival data, and nonsurgical candidates were excluded from this study (Figure 1).
Patient demographic information, treatment facility type, staging, treatment, outcome information, and information regarding fragmented care were collected from the NCDB. Fragmented care (FC) was defined as a patient receiving care at >1 facility while integrated care (IC) was defined as receiving care at a single institution.
Great circle distance was calculated based on the number of miles between the patient’s zip code and the address of the treatment center. This is a variable in the NCDB to evaluate distance patients travel to receive care.
The primary outcome variable of this study was to evaluate the impact of FC to achieve a TOO. The secondary outcome was overall survival. TOO was defined as meeting all the following criteria: no mortality within 90 days of surgery, achievement of an R0 resection (all margins grossly and microscopically negative), having 12 or more lymph nodes evaluated, being a non-length of stay (LOS) outlier (>8 days), no readmissions within 30 days of surgery and having guideline-concordant therapy. Guideline-concordant therapy consisted of the receipt of neoadjuvant chemotherapy and radiation therapy for clinical locally advanced (cT3–T4b and/or cN1–N2b) disease or receipt of adjuvant chemotherapy and radiation therapy within 180 days after diagnosis for nonclinically locally advanced (cT1–T2 and cN0) with pathologic locally advanced (pT3–T4b and/or pN1– N2b) disease. Guideline-concordant therapy was also defined as receipt of neoadjuvant multiagent chemotherapy (total neoadjuvant therapy) or both neoadjuvant and adjuvant chemotherapy for clinically locally advanced (cT3–T4b and/or cN1–N2b) disease.
Comparisons by FC were performed using Chi-square test for categorical variables. A multivariate logistic regression model was developed to identify the impact of FC and other potential factors on TOO, and stepwise selection was applied to remove insignificant variables.
Figure 1. Flow chart illustrating the number of patients excluded from the study and the reason for exclusion.
Table 1. Demographics and outcomes of study cohort
1Chi-Square
Survival analysis was performed using KaplanMeier methods and log-rank test were used to for a difference in survival probability between two groups. Statistical analysis was conducted using SAS® Enterprise Guide 8.2: User’s Guide (SAS Institute Inc., Cary, NC, USA). Results were considered statistically significant if the p value was ≤0.05.
Results
Demographics
This study included 96,941 patients; 25,499 patients (26%) received FC while 71,442 (74%) received IC (Table 1). Overall, 83,610 (86%) of the study population were white, 59,383 (61%) were male, and the majority of patients had limited medical comorbidities (91,089, or 94%, had a CharlsonDeyo Score of 0 or 1). Most patients (96,941; 75%) underwent low anterior resections for their cancer and 37% had surgery at comprehensive community cancer programs.
Textbook Outcome Data
Overall, 28% of patients (26,971) achieved a TOO; 33% (8,510) of patients who received FC achieved a TOO versus 26% (18,461) of patients who received IC achieved a TOO. Table 2 and Figure 2 show a
Table 2. Post-operative outcomes based on TOO parameters
Figure 2. The rates of individual parameters for FC and IC percentages of textbook outcome compared to overall percentage.
breakdown of TOO based on each individual component of the metric. Mortality for the group overall was 2% (1,986), however there was a statistically significant increase in 90-day mortality in patients who had IC compared to FC (2.3% versus 1.3%, p<0.001). Each individual component of TOO was significantly improved in patients who had FC versus IC except for the rate of R0 resection, which was equivalent (Table 2).
Factors Associated with Achievement of a TOO
A multivariate analysis was performed to identify factors that were associated with the achievement of TOO (Table 3). FC was shown to be associated with the achievement of TOO (OR 1.36, 95% CI: 1.32-1.41).
Facility type was also associated with achievement of TOO, as care at a non-community cancer program being associated with increased TOO.
Patients who received FC traveled slightly farther than their IC counterparts (33.6 versus 30.2 miles, p<0.001) (Table 4, Table 5). Treatment for FC patients was also slightly delayed (36.5±28.3 days versus 34.9±31.1 days from diagnosis to treatment, p<0.001).
Factors Associated with FC
A multivariate analysis was performed to identify factors that were associated with FC (Table 4). With increasing age, patients were significantly less likely to have FC (OR 0.991, 95% CI: 0.99-0.993). Patients who underwent surgery at academic (OR 0.692, 95% CI 0.648-0.739) or comprehensive community programs (OR 0.675, 95% CI 0.633-0.720) were less likely to have FC than patients who underwent surgery at community cancer programs.
Table 3. Multivariate analysis of factors associated with
Table 4. Additional variables associated with achieving a TOO
FC and Overall Survival
Overall survival was evaluated for patients who had FC versus those who had IC. A Kaplan-Meier curve along with a cox proportional hazard model demonstrates that patients who had FC had an improved overall survival compared to those with IC (P<0.0001) (Figure 3, Table 6).
Discussion
This study examined the impact that fragmentation of care has on textbook oncological outcomes in locally advanced rectal cancer. We have demonstrated that patients in this study who had FC were 36% more likely to achieve a TOO as well as have an improved overall survival compared to patients with IC. Older, more medically complex patients, Black patients and those treated at an academic institution were less likely to receive fragmented care.
Many patients have care at multiple institutions and therefore it is important to study whether FC affects the overall quality of care. In this study, FC was associated with better outcomes and should be considered as a positive predictor of quality care. This is possibly due to the centralization of cancer care at higher volume centers. In this study, there were several demographic characteristics associated with FC. Older patients, nonwhite and uninsured patients were less likely to have FC. Our study, like other studies, show that there are disparities for high-risk populations. Wasif et al. studied socioeconomic and racial differences in cancer surgery and found that Black, uninsured, and less-educated patients were less likely to have surgery at high-volume centers and therefore less likely to have FC (14).
Overall, in the literature, FC has shown mixed results regarding the effects on overall survival. Hester et al. investigated the impact of care fragmentation in the treatment of hepatocellular carcinoma, reporting that fragmentation of care was associated with worse overall survival (8). Brown et al. reported that fragmentation of care in patients with pancreatic cancer was not associated with worse survival outcomes (15). Finally, Khan et al. showed an improvement in 30-day, 90day, and overall survival in patients with pancreatic ductal adenocarcinoma with FC compared to patients with IC (16). In rectal cancer specifically, Freischlag et al. examined fragmentation of care in patients with stage II and III disease and found that receiving integrative care at an academic institution had improved survival outcomes when compared to patients with
1Two sample t-test
Table 5. Multivariate analysis of factors associated with fragmented care
Table 6. Cox proportional hazards model on 5-year survival
fragmentation of care at academic institutions (7). More studies will be needed to identify the actual causes of FC and to delineate if there are disparities in the care of patients based on FC. Given the mixed messages of the current body of FC literature, further research is needed.
Rectal cancer surgical care has become more centralized, which has been shown to improve surgical outcomes. High-volume centers show improved outcomes when compared to lower-volume centers (4–6). This centralization of care might be one of drivers of FC. Although some outcomes including surgery related outcomes might be improved, patient comfort may come at a cost. Our study shows that FC was associated with an increase travel distance and longer time to start treatment. Longer time to treatment and travel can increase patient anxiety, stress, and cost of care. Other studies have also shown an increase in costs with FC (1). Stitzenberg et al. found a proportional relationship
between centralization of care and travel distance. Their study showed that as cancer care becomes centralized to high volume centers the travel distance will increase (17).
In this study, a minority of patients (28%) achieved quality cancer care and as such there is much room for improvement. In the literature the achievement of TOO varies based on histological type and have slowly improved over time (18). For colectomy, one study published overall rates of 55% with large variations based on site of care (19). Our study shows comparable results with achievement of TOO with other studies looking at the rectal cancer patient population (20).
Overall, this study’s data supports the centralization and care fragmentation in the treatment of rectal cancer. Although fragmentation of care increases the travel distances and time to treatment, it also increases the likelihood of achieving a TOO, a driving factor for increased overall survival. More studies are needed to further define what aspects of FC lead to the highest
Product-limit survival estimates with number of subjects at risk
3. Kaplan-Meier Curve on 5-year survival stratified by receipt of fragmented care. Diagnosis year from 2006-2018.
Figure
quality of care as defined by TOO. By defining how to improve TOO, centers can bring the best care to patients closer to their homes and potentially allow treatment at one site, making care easier and potentially more cost-effective for patients.
This study is not without limitations that should be considered. First, the nature of the retrospective cohort study allows for the possible introduction of bias. Additionally, great circle distance was calculated using the patient’s zip code rather than address, thus there are individual variations in distance traveled that are not accounted for. However, we believe the great circle distance provides a good estimation of the travel requirements for patients. Due to the limitations of the database the reasons for FC are not known. Therefore, no conclusions can be made as why patients received care at multiple institutions or why which institutions were associated with fragmented care. While TOO seems to serve as a good quality metric, it is not without limitations. TOO is a composite variable, which means it places equal weight on all endpoints. One could argue that the endpoints examined with TOO are not equal, such as 90-day mortality vs less than 12 lymph nodes excised. With the multiple complexity of TOO that includes multiple factors and fragmented care, the authors did not choose to include additional inclusion criteria to the analysis. Therefore, there are differences in the sequencing of care between clinical and pathologic stages that are not addressed in this manuscript. This study did not assess for the sequencing of chemotherapy or radiotherapy thus no conclusions can be made regarding the role of TNT as it relates to receiving FC or IC. Finally, the NCDB only reports on CoC accredited institutions, thus these findings may be limited in their generalizability with non-CoC institutions.
Conclusion
In conclusion, while traveling to high-volume centers for oncologic surgery may pose a greater inconvenience to rectal cancer patients, this may provide a greater likelihood of achieving a TOO and increasing survival. This study supports fragmentation of care in rectal cancer patients.
Disclosures
The authors declare no conflicts of interest. This research did not receive any funding from agencies in the public, commercial, or not-for-profit sectors.
Acknowledgments
All authors made substantial contributions to either the concept and/or design of this study. SW collected and analyzed the data for the present study. TK, MG, OG, AF, RH, and JB all interpreted the data and drafted and/ or edited the manuscript. TK, MG, OG, AF, SW, RH, and JB reviewed the manuscript for errors and provided feedback for changes. All authors approved this version of the manuscript and agreed to be accountable for all aspects of the article.
References
1. Hussain T, Chang HY, Veenstra CM, Pollack CE. Fragmentation in specialist care and stage III colon cancer. Cancer. 2015 Jun 4;121(18):3316–24.
2. Xu Z, Mohile SG, Tejani MA, Becerra AZ, Probst CP, Aquina CT, et al. Poor Compliance with Adjuvant Chemotherapy Use Associated with Poorer Survival in Patients with Rectal cancer: an NCDB Analysis. Cancer. 2016 Aug 25;123(1):52–61.
3. American Cancer Society. Survival Rates for Colorectal Cancer [Internet]. Cancer.org. American Cancer Society; 2014. Available from: https://www. cancer.org/cancer/colon-rectal-cancer/detectiondiagnosis-staging/survival-rates.html
4. Aquina CT, Probst C, Becerra AZ, Iannuzzi JC, Kelly KN, Hensley BJ, et al. High Volume Improves outcomes: the Argument for Centralization of Rectal Cancer Surgery. Surgery. 2016 Mar 1;159(3):736–48.
5. Stitzenberg KB, Meropol NJ. Trends in Centralization of Cancer Surgery. Annals of Surgical Oncology. 2010 Jun 18;17(11):2824–31.
6. Birkmeyer JD, Siewers AE, Finlayson EVA, Stukel TA, Lucas FL, Batista I, et al. Hospital Volume and Surgical Mortality in the United States. New England Journal of Medicine. 2002 Apr 11;346(15):1128–37.
7. Freischlag K, Olivere LA, Turner MC, Adam MA, Mantyh CR, Migaly J. Does Fragmentation of Care in Locally Advanced Rectal Cancer Increase Patient Mortality? Journal of Gastrointestinal Surgery. 2020 Aug 4;25(5):1287–96.
8. Hester CA, Nishika Karbhari, Rich NE, Augustine MM, Mansour JC, Polanco PM, et al. Effect of Fragmentation of Cancer Care on Treatment Use and Survival in Hepatocellular Carcinoma. Cancer 2019 Jul 12;125(19):3428–36.
9. Lin CC, Bruinooge SS, Kirkwood MK, Hershman DL, Jemal A, Guadagnolo BA, et al. Association between Geographic Access to Cancer Care and Receipt of Radiation Therapy for Rectal Cancer. International Journal of Radiation Oncology*Biology*Physics. 2016 Mar;94(4):719–28.
10. Aquina CT, Hamad A, Becerra AZ, Cloyd JM, Tsung A, Pawlik TM, et al. Is Textbook Oncologic Outcome a Valid Hospital-Quality Metric after High-Risk Surgical Oncology Procedures? Ann Surg Oncol 2021 Aug 15;28(13):8028–45.
11. Lin CC, Bruinooge SS, Kirkwood MK, Hershman DL, Jemal A, Guadagnolo BA, et al. Association between Geographic Access to Cancer Care and Receipt of Radiation Therapy for Rectal Cancer. International Journal of Radiation Oncology*Biology*Physics. 2016 Mar;94(4):719–28.
12. Sujay Kulshrestha, Bunn C, Patel PM, Sweigert PJ, Eguia E, Pawlik TM, et al. Textbook Oncologic Outcome Is Associated with Increased Overall Survival after Esophagectomy. Surgery. 2020 Nov 1;168(5):953–61.
13. Sweigert PJ, Eguia E, Baker MS, Paredes AZ, Tsilimigras DI, Dillhoff M, et al. Assessment of Textbook Oncologic Outcomes following Pancreaticoduodenectomy for Pancreatic Adenocarcinoma. Journal of Surgical Oncology. 2020 May;121(6):936–44.
14. Mallin K, Browner A, Palis B, Gay G, McCabe R, Nogueira L, et al. Incident Cases Captured in the National Cancer Database Compared with Those in U.S. Population Based Central Cancer Registries in 2012–2014. Annals of Surgical Oncology. 2019 Feb 8;26(6):1604–12.
15. Nabil Wasif, Etzioni D, Habermann EB, Mathur A, Pockaj BA, Gray RJ, et al. Racial and Socioeconomic Differences in the Use of High-Volume Commission on Cancer-Accredited Hospitals for Cancer Surgery in the United States. Annals of Surgical Oncology 2018 Feb 15;25(5):1116–25.
16. Brown ZJ, Labiner HE, Shen C, Ejaz A, Pawlik TM, Cloyd JM. Impact of Care Fragmentation on the Outcomes of Patients Receiving Neoadjuvant and Adjuvant Therapy for Pancreatic Adenocarcinoma. Journal of Surgical Oncology. 2021 Oct 2;125(2):185–93.
17. Khan H, Heslin MJ, Crook ED, Mehari K, Johnston FM, Fonseca AL. Fragmentation of Care in Pancreatic Cancer: Effects on Receipt of Care and Survival. Journal of Gastrointestinal Surgery. 2022 Oct 11;26(12).
18. Stitzenberg KB, Sigurdson ER, Egleston BL, Starkey RB, Meropol NJ. Centralization of Cancer Surgery: Implications for Patient Access to Optimal Care. Journal of Clinical Oncology. 2009 Oct 1;27(28):4671–8.
19. J. Madison Hyer, Beane JD, Gaya Spolverato, Tsilimigras DI, Diaz A, Paro A, et al. Trends in Textbook Outcomes over Time: Are Optimal Outcomes following Complex Gastrointestinal Surgery for Cancer Increasing? Journal of Gastrointestinal Surgery. 2021 Sep 10;26(1):50–9.
20. Sweigert P, Eguia E, Baker MS, Link C, J. Madison Hyer, Paredes AZ, et al. Assessment of Cancer Center Variation in Textbook Oncologic Outcomes following Colectomy for Adenocarcinoma. Journal of Gastrointestinal Surgery. 2020 Aug 10;25(3):775–85.
21. Naffouje SA, Ali MA, Kamarajah SK, White B, Salti GI, Dahdaleh FS. Assessment of Textbook Oncologic Outcomes following Proctectomy for Rectal Cancer. Journal of Gastrointestinal Surgery. 2022 Apr 19;26(6):1286–97.
An Analysis and Outcomes of Skin Cancer Screenings Among Lynch Syndrome Patients in Geisinger’s Inherited
Gastrointestinal Malignancy Clinic
Alexandra Yudiski1†‡, Heather Rocha2‡, Matthew Dzeda1†, Edward Liu1†, Olivia Granja1†, Nicholas Haynes1†, Hannah Wooley1†, Shane Conklin1†, Cassandra Pisieczko3, Kaitlyn Sweeney2, Amanda Leicht2, Thomas Morland2, Bradley Confer2, and Heinric Williams2
1Geisinger Commonwealth School of Medicine, Scranton, PA 18509
According to the National Comprehensive Cancer Network (NCCN) guidelines, patients with germline mutations in the DNA repair genes (MLH1, MSH2, MSH6, PSM2) should consider full-body skin exams every 1–2 years due to increased risk of sebaceous neoplasms. Lynch syndrome (LS) is associated with an increased lifetime risk to develop sebaceous neoplasms. At Geisinger’s Inherited Risk
Gastrointestinal Malignancy (IGRI) Clinic, patients received counseling including discussions regarding the increased lifetime risk for dermatologic diseases and solid organ malignancies. A chart review was completed for LS patients in the IGRI clinic from 2016 to 2022 (N=134). Patient contact occurred through in-person and telemedicine visits. Dermatology clinic visits, skin pathology reports, patient’s age, and genetic variants were reviewed. Overall, 65.7% of patients had at least one full-body skin exam with a dermatologist between 2016 and 2022. Completion among MLH1, MSH2, MSH6 and PSM2 carriers were 61.9%, 67.5%, 68.1% and 61.5% respectively. Incidence of patients diagnosed with at least one sebaceous neoplasm was 2.6% and 1.1% per year in MSH2 and MLH1 germline mutations between 2016 and 2022, respectively, and no sebaceous neoplasms were identified in MSH6 or PSM2 carriers. During the study period, 6 patients were diagnosed with a sebaceous neoplasm, 4 patients were diagnosed with basal cell carcinoma and 1 patient was diagnosed with squamous cell carcinoma. To date, there is currently limited evidence of an increased risk for basal cell or squamous cell carcinoma in LS compared to the general population. In conclusion, patients’ completion of full-body skin
screenings is most likely attributed to patient education from a genetic counselor with offer of dermatology referral. Based on our findings and current literature, more individualized counseling for specific germline mutations and patients with family history of sebaceous neoplasms may be worthwhile due to the association with these lesions.
Introduction
Lynch syndrome (LS) is caused by a mutation in mismatch DNA repair genes: MLH1, MSH2, MSH6, PMS2, and EPCAM. Inheritance is autosomal dominant with strong evidence of reduced penetrance among patients with PMS2 variants. These patients have an increased risk for multiple malignancies, including colorectal, gastrointestinal, endometrial, ovarian, urologic, pancreatic, and sebaceous carcinoma of the skin (1). The reported risk for sebaceous neoplasms among patients diagnosed with LS is highest for MSH2 (up to 9%) (2). Based on NCCN guidelines, patients should consider full-body skin exam every 1 to 2 years with a dermatologist with no recommended age to begin surveillance, as this should be individualized to patient and provider concern coupled with family history. In the literature, loss of MSH2 and MLH1 expression has the strongest association with sebaceous neoplasms (3).
Sebaceous lesions can be categorized as sebaceous hyperplasia, sebaceous adenoma, sebaceoma, and sebaceous carcinoma. Sebaceous hyperplasia is an overabundance of normal-appearing sebaceous lobules upon histopathology and typically requires no further treatment, unless for cosmetic purposes. There is
currently no strong evidence for an association with sebaceous hyperplasia and LS. Sebaceous adenomas, sebaceomas, and sebaceous carcinomas are associated with LS. Sebaceous adenomas and sebaceomas appear indistinguishable based on clinical features. A lesion is considered a sebaceoma if more than 50% of cells are basaloid in appearance, while lesions with less than 50% are categorized as sebaceous adenomas. These are benign, but are excised to rule out cancerous lesions, including basal cell and sebaceous carcinomas (4).
Sebaceous carcinomas are highly aggressive malignancies with a 5-year survival rate of 78.0% (5). In a systemic review of 380 LS cases, basal cell carcinomas (BCC) in 10% of patients and squamous cell carcinomas (SCC) in 23% of patients were identified within this patient population, but there is currently no evidence of a strong link to LS in comparison to sebaceous neoplasms since BCC and SCC are relatively common among the general population. If patients have a strong family history of skin malignancies or are diagnosed at an earlier than expected age, screening for LS using immunohistochemistry may be warranted and aid risk management of visceral malignancies such as colorectal cancer (6).
At IGRI clinic, patients meet with a genetic counselor who provides education on increased risk for cutaneous sebaceous neoplasms among LS patients in comparison to the general population and are asked to consider full-body skin exams by a dermatologist. Patients are followed annually with either an in-person or telemedicine visit. Given the lack of a recommended age to begin skin screening, all LS patients were referred to dermatology for full body skin evaluation (unless with previously established dermatological care).
Methods
Procedures
We completed a retrospective review of all patients from April 2016 through December 2021 (N=134), with at least one follow-up, through December 2022.
Parameters evaluated included: age of diagnosis, sex, mismatch repair mutations, completion to recommended screening, and follow-up guidelines with IRB approval provided by Geisinger. Reviewers followed the same
standard of procedure instructions for initial review, and a quality control analysis was completed by randomly assigning 20% of charts to be re-reviewed by a different reviewer to ensure the accuracy and precision of the initial chart review. Dermatological pathology reports, dermatology visits, and primary skin cancers were reviewed in LS patients’ electronic health records.
Statistics
For data analysis, completion of a full-body skin exam was defined as an LS patient that attended at least one dermatology appointment and had a skin examination documented. A chi square analysis was completed using excel to evaluate parameters. Figures were constructed utilizing Excel software.
Results
Patients’ ages range from 20 to 81, with an average of 48.1 years of age. Patients assigned female at birth account for 73.1% of the study population. Within this population, 65.7% of patients completed a full-body skin screening. Chi square analysis was performed for sex (X²= 0.022, p= 0.88), age (X²= 9.39, p= 0.009154), mismatch gene mutation (X²= 0.51, p= 0.92) with completion of at least one skin exam, revealing no statistical significance (p-value < 0.05) for sex and germline mutations. The chi square analysis did reveal that age has a statistical significance (p-value <0.05) in association with completion to skin exams. The percent completion among patients less than 40 years, between 40 and 60 years, and more than 60 years were 48.8%, 71.0%, and 81.4%, respectively. Average age of patients at first diagnosis of sebaceous neoplasm associated with LS was 57 years (range 43–76), and all these patients had full-body skin exams every 1–2 years per recommended guidelines.
Table 1 shows the incidence of sebaceous neoplasms, BCC, and SCC among patients with MSH2, MLH1, MSH6, and PMS2 germline mutations. Out of the 88 patients that completed a full-body skin examination,
Table 1. Incidence of sebaceous neoplasms, BCC, and SCC among LS patients with MSH2, MLH1, MSH6, and PMS2 germline mutations between 2016-2022.
5 patients (5.8%) were found to have sebaceous adenomas confirmed by biopsy. Of those 5 patients, 3 of them also had one or more sebaceomas confirmed by biopsy. Based on previously diagnosed germline mutations, 4 of these patients had lesions that demonstrated loss of MSH2 expression, and 1 patient had a loss of MLH1 expression. One patient with a loss of MSH2 expression had an excised lesion that was described as an ulcerated sebaceous neoplasm but could not be excluded from sebaceous carcinoma according to the pathology report.
Table 2 lists the specific subtype of each germline mutation that had at least one sebaceous neoplasm diagnosis and their family history of sebaceous neoplasms. An additional 4 patients had a diagnosis of basal cell carcinoma and 1 patient had two squamous cell carcinomas diagnoses that were all completely excised and confirmed by biopsy. Figure 1 illustrates the number of patients that had a diagnosis of sebaceous neoplasms, BCC, and SCC within 2016-2022.
Discussion
Despite discussing the risk of skin lesions with each patient, the completion of at least one skin exam was 65.7%. There is currently no reported data on skin screening completion rates in this patient population. One possible reason is phrasing of the NCCN guidelines, which states “consider” full-body skin exam rather than “recommend” as it does for colonoscopies
for colon cancer screening. Other reasons may include comorbid disease status, as some patients have multiple chronic health problems for which they follow up. Other patients may have a perceived lower risk for sebaceous lesion with germline PMS2 variants conferring an overall lower degree of risk for more serious solid tumor malignancies (e.g., colorectal, uterine, and ovarian cancers). In addition, the lack of convenience of traveling to another clinic site for a referral versus completing all recommended screenings at the time of clinic could be a barrier. At future appointments, the care team could explore reasons of refusal for additional insight regarding barriers to completion of skin checks.
The germline mutation with the most patients diagnosed with at least one sebaceous neoplasm with a total of 5 patients was MSH2, which corresponds with what was found in literature (6). Although there is limited evidence in the literature depicting a higher
MSH2 1384C>T
MSH2 1384C>T
MSH2 942+3A>T
MSH2 1760-1G>A
MLH1 298C>T
Table 2. Germline mutations of patients with at least one diagnosis of a sebaceous neoplasm that was confirm by histopathology and associated family history
1. The number of LS patients with at least one diagnosis of sebaceous neoplasm, BCC, or SCC that was excised and confirmed by histopathology with associated germline mutations MSH2, MLH1, and MSH6
Figure
risk for BCC or SCC in LS due to these lesions being relatively common in the general population, these cancers were caught during these skin screenings as well. At future appointments, the care team could explore discussing the increased incidence among MSH2 and MLH1 for sebaceous neoplasms with this patient population and current risk for other skin cancers like BCC and SCC. Three patients with sebaceous neoplasms diagnoses also had first-degree relatives that had a previous sebaceous neoplasm, while the other 3 patients had no family history of these skin lesions. Hence, utilizing a patient’s family history when talking about their personal risk may be warranted for sebaceous neoplasms.
At IRGI clinic, patients have access to subject experts and specialists in the individual malignancies associated with LS. In developing countries with less resources, patients may not have access to care where genetic testing is limited or not available. In one study completed at a public cancer center in Brazil, only 62.5% of patients underwent genetic counseling who had abnormal clinical-based screening for LS and 18.7% underwent genetic testing to confirm an LS-associated mutation between 2012 and 2018 (7). In a national survey of gastroenterologists completed in 2018, a multivariable analysis depicted that physicians perceived that barriers including cost of germline testing and availability of genetic counseling were associated with non-academic and rural-based hospitals (8).
Conclusion
Based on these findings and the current literature, targeting patients specifically based on germline variants and/or with a family history of sebaceous neoplasms may be the most practical strategy to apply risk management to those at the highest degree of risk. A stronger recommendation for gene-based surveillance mutations may be indicated, but further evidence is needed.
References
1. Bansidhar BJ, Silinsky J. History and Pathogenesis of Lynch Syndrome. Clinics in Colon and Rectal Surgery [Internet]. 2012 Jun 1 [cited 2020 Jun 3];25(2):63–6. Available from: https://www.ncbi. nlm.nih.gov/pmc/articles/PMC3423881/
2. Giardiello FM, Allen JI, Axilbund JE, Boland CR, Burke CA, Burt RW, et al. Guidelines on Genetic Evaluation and Management of Lynch Syndrome: A Consensus Statement by the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology [Internet]. 2014 Aug 1 [cited 2021 Apr 4];147(2):502–26. Available from: https://www.gastrojournal.org/article/S00165085(14)00448-X/fulltext
3. Le S, Ansari U, Mumtaz A, Malik K, Patel P, Doyle A, et al. Lynch Syndrome and Muir-Torre Syndrome: An update and review on the genetics, epidemiology, and management of two related disorders. Dermatology Online Journal. 2017;23(11).
4. Lazar AJF, Lyle S, Calonje E. Sebaceous neoplasia and Torre–Muir syndrome. Current Diagnostic Pathology. 2007 Aug;13(4):301–19.
5. Tripathi R, Chen Z, Li L, Bordeaux JS. Incidence and survival of sebaceous carcinoma in the United States. Journal of the American Academy of Dermatology [Internet]. 2016 Dec 1 [cited 2023 Feb 4];75(6):1210–5. Available from: https://pubmed. ncbi.nlm.nih.gov/27720512/
6. Aziz S, O’Sullivan H, Heelan K, Alam A, McVeigh TP. Characterization of sebaceous and non-sebaceous cutaneous manifestations in patients with lynch syndrome: a systematic review. Familial Cancer 2022 Nov 23;22(2):167–75.
7. Kozak VN, de Souza Fonseca Ribeiro EM, Kozonoe MM, Ioshii SO, Casali da Rocha JC. When guidelines face reality – Lynch syndrome screening in the setting of public health system in a developing country. J Community Genet. 2022 Feb;13(1):19-29.
8. Noll A, J Parekh P, Zhou M, Weber TK, Ahnen D, Wu XC, Karlitz JJ. Barriers to Lynch Syndrome Testing and Preoperative Result Availability in Earlyonset Colorectal Cancer: A National Physician Survey Study. Clin Transl Gastroenterol. 2018 Sep 20;9(9):185.
2025 Summer Research Immersion Program
Each summer the Geisinger Commonwealth School of Medicine Summer Research Immersion Program (SRIP) brings together first year medical students for an opportunity to gain research experience in basic science, clinical science, public/community health, behavioral health, or medical education under the guidance of a research mentor. The summer research experience includes a $2,500 educational stipend. At the end of the program, students present their research in a poster session. In addition to research, SRIP students participate in a variety of complementary enrichment activities:
• GCSOM and Geisinger faculty research seminars
• GCSOM Grand Rounds and clinical seminars at our hospital partners
• Special events or conferences related to your research topic
• Clinical exposure
• Scientific writing & communication workshops
SRIP program goals:
• Provide students with an immersive research experience under a mentor’s guidance
• Enhance students’ knowledge of the scope and types of research relevant to improving health in the region, nationally, and globally
• Provide research opportunities that span the translational continuum from laboratory based biomedical studies to clinical and public health research conducted with community partners
• Engage students in peer learning and networking
• Enhance students’ skills in oral and written scholarship
Program dates:
SRIP 2025 will be an 8-week program held June 2 – July 25, 2025.
For more information, contact: Sonia Lobo, PhD SRIP Program Administrator Associate Dean for Research & Scholarship slobo1@geisinger.edu
Elizabeth Kuchinski, MPH SRIP Director eckuchinski@geisinger.edu
Medical Research Honors Program
Current first-year medical students are eligible to join the Medical Research Honors Program (MRHP). With a mentor’s guidance, you will drive this long-term, thesis focused research experience. By completing the requirements while remaining in good academic standing, you’ll graduate with an honors distinction.
Through the MRHP, you will:
• Advance fundamental scientific knowledge
• Stand apart in competitive residency application fields
• Refine scholarly communication
• Gain a mindset of continual growth and learning
To complete this 4-year program, you must submit a research project proposal, write a thesis, and deliver an oral defense. You will also write abstracts, present posters, and publish findings while building towards your thesis defense. Your research experience is guided by a research mentor, a thesis advisory committee, and the program director. We encourage you to participate in the Summer Research Immersion Program as well.
Application deadline:
Early consideration deadline: April 28, 2025
Final deadline: Sept. 15, 2025
Application packet must include:
• MRHP application form
• Letter of support from research mentor
• CV
• Acknowledgment of mentor’s expectations
• Project proposal: project title, specific aims, hypothesis, background, preliminary data (if available)
Be a mentor
If you would be willing to have a medical student work with you on a long-term, thesis driven research project, email us at mrhp@geisinger.edu or scan the QR code. Be sure to indicate your willingness to commit time, facilities, and resources to a student as needed throughout the program.
Questions about the MRHP program or mentoring?
Contact: Sonia Lobo, PhD Associate Dean for Research and Scholarship slobo1@geisinger.edu
Tracey Pratt, MPH MRHP Program Manager tpratt@geisinger.edu
Finding your way: Opportunities for student funding
You can find assistance in searching for funding opportunities specifically designed for students at the Office of Research and Scholarship. Funding opportunities may include support for fellowships, internships, research, programming, and collaboration.
The Office of Research and Scholarship can help you locate and qualify funding opportunities as well as assist in application review. Be sure to call or stop by early in the proposal development process so we can work with you to meet your deadline.
Geisinger Clinical Research Fund
Geisinger Commonwealth School of Medicine is pleased to support student research and professional development through the Clinical Research Fund (CRF). The Office of Research & Scholarship administers GCSOM’s CRF allocation by providing funding for research costs and subscriptions, conference travel reimbursement, and publication fees. As a GCSOM student, you may apply for up to $5,000 per calendar year (January – December) from the CRF to support the use of Geisinger research cores (Investigator Initiated Research Operations, Biostatistics, Phenomic Analytics & Clinical Data Core). In addition, you may be able to obtain funds to cover the costs of a research subscription, such as statistical software. You may receive travel support up to $1,000 per calendar year to present your research at a scientific conference.
Finally, if your work has been accepted for publication in a scholarly, peer-reviewed journal, you may be eligible for support with publication fees. Publication support falls under the conference/publication support category, with a cap of $1,000 per student for combined conference/publication support per calendar year.
All student research support must be preapproved by Research & Scholarship staff. Funding is dependent on an annual budget allocation and is not guaranteed. If you’re considering applying for research support, contact mrhp@geisinger.edu early in your planning and preparation.
Contact information:
Tracey Pratt, MPH Manager of Research Education Resources Office
of Research and Scholarship
Phone: 570-558-3955
Internal extension: 5335
Email: tpratt@geisinger.edu
Cover art submissions
This year’s call for SCRIP cover art yielded several creative and noteworthy submissions from our talented students which are showcased below. The image chosen for the SCRIP cover was submitted by Julian Burwell, MD Class of 2027, and is an artistic interpretation of a DNA double helix. The painting represents the recent developments in genomics and Geisinger’s MyCode® Community Health Initiative to enhance preventive care for patients.
Lynzi Smith, MD Class of 2025
“A chance to cut is a chance to cure.”
A watercolor painting highlighting a surgeon’s most important tool: their hands.
Melissa Endy, MD Class of 2025
This is an acrylic painting of an anonymous Geisinger Commonwealth student wearing their hospital-issued green scrubs as they work during the night on Epic. The student is highlighted by the light from their screen as they look through their patient’s chart, and a glimpse of the night sky is visible through a window in the upper right corner. This piece reflects the long periods of intense studying and research in physiology, pharmacology, and pathology, as well as the many hours dedicated to the art of patient care that students engage in throughout their education.
Finn Gustav Rieker, MD Class of 2026
1. A high-magnification, H&E-stained section of vaginal epithelium from a cadaveric histological study of the connective tissue bridging the posterior urethral and anterior vaginal walls—the urethrovaginal septum.
2. A high-magnification, trichrome-stained section of urethral epithelium from a cadaveric histological study of the connective tissue bridging the posterior urethral and anterior vaginal walls—the urethrovaginal septum.
1
2
Zachary Rieker, MD Class of 2027
A yellow butterfly against a blue background. The left wing is a normal, yellow butterfly’s wing, while the right is composed of a leopard eye and daisy.
525 Pine St.
Scranton, PA 18509
570-504-7000
geisinger.edu/gcsom studentresearch@geisinger.edu
From left: William Adams, Hugh Johnson, Chukwuemeka Ene, Jennifer Bekker, Calvin Kiniale, Kelly Barr, Truong An Pham, and Julian Michael Burwell received Excellence in Research Awards for their outstanding abstract submissions at the 2024 Summer Research Symposium.