The Godolphin and Latymer School
Cover by Angelina Kim LVI
DR DOLPHIN
SPRING 2021
Message from the editors Hello, and welcome to the Spring Edition of Dr Dolphin, G&L’s biomedical magazine! In this edition you will find a collection of fascinating articles, lectures and art! We would also like to thank everyone who contributed to this edition of Dr Dolphin: your submissions were all brilliant and greatly appreciated! We hope you enjoy this magazine as much as we enjoyed your articles. If you would like to submit any pieces of work, please send an email to us at rfahid@godolphinandlatymer.com, rzahaki@godolphinandlatymer.com, and cgilardi@godolphinandlatymer.com. Happy reading! Rojin, Roxanna and Clara :)
1
DR DOLPHIN
SPRING 2021
CONTENTS New Frontiers ……………………………………………....…..………………………………………………………………………………………………….... 3 The Potential of AI in Medicine Today Ovarian Cancer Detection by Dogs Birth and Bacteria Biomaterials: Changing the Face of Dentistry Creativity and Science: How Andrew Pelling’s experimental lab is redefining the limits of medicine Obesity: is it all to do with overconsumption? Current Affairs …………………………………………………………………….………………………………………………………………………………….. 16 Should Vaccines be Compulsory? Implications of COVID-19 on the Lungs The Importance of Vaccines in Medicine Lectures ……………………………………....….…………………………………………………………………………………………………………….. 23 BMJ ‘Born Equal - Racism in Medicine’ Who thinks about ‘Doctors in Distress’? Key Concepts ……………………………………....….…………………………………………………………………………………………………………….. 32 Why do we have Different Blood Types? The Neuroscience Behind PTSD The Theory of Natural Selection The truths to obesity Art …………………………………....….…………………………………………………………………………………………………………...... 38 Flower by Isabella Davidson Medical Word Search …………………………………....….…………………………………………………………………………………………………………...... 39
New Frontiers
2
DR DOLPHIN
SPRING 2021
The Potential of AI in Medicine Today The use of artificial intelligence in healthcare has always been a hot topic, one debated for years due to its ethical, legal and social standpoints. However, while we look at artificial intelligence as a construct of the future, one would be surprised to realise how prevalent it is in the present day and how each individual has most probably engaged with at least one form of medical AI sometime in the past six months! However, don’t be fooled into thinking that we have embraced very much of it, AI holds an enormous amount of potential in the medical field and these possibilities can only unfold with time. Before we start, let me explain the true nature of the AI I am referring to in this article, and how it is used in this field of practice. Medical AI fundamentally refers to the use of artificial intelligence technology in the healthcare system through automated processes. Essentially, it holds the potential to completely transform the practice of medicine by helping doctors more accurately treat patients, make more precise predictions about a patient's future health and additionally, recommend the most suitable and beneficial treatments through logical constructs. Moreover, it should be noted that studies have shown that an astonishing 50% of practices carried out by medical professionals have the potential to become automated with the use of AI - a rather frightening figure! The question will always be asked - why would we want to use technology instead of humans? And what are some examples of ways that we have already started doing so? Essentially, what issues might arise from these technological advancements in
the world of medicine - is technology always better? There are a myriad of duties that medical professionals face every single day, a large proportion under the umbrella term of ‘patient care.’ This care consists of gathering data from consultations, processing this data and retrieving results to then generate a diagnosis for the patient by using other sources of data as a reference. Then comes determining the appropriate treatment method, preparing this treatment, monitoring the progress of the patient and finally, ensuring the patient is provided with the correct aftercare through appointments, etc. Yes, it is a lot of work that these healthcare professionals are faced with daily - all for one problem, one patient. A study in 2016 showed that physicians spend a lot more time on entering data and general desk work than actually engaging with their patients! Therefore, I think we’d all be relieved to know that the large majority of the above care has the potential to become automated using AI. Now, what benefits does this hold? Creating automated systems that can carry out these tasks without a human having to do so manually results in more efficient and faster task completion, freeing up a great deal of time for doctors, thus enabling them to focus on other things that cannot be automated. There will always be certain tasks better done by humans, while others more efficiently done by computers by preventing human calculation errors, saving time, etc. By using AI for certain tasks, the medical system won’t just become more efficient but may also help us move towards more ‘precision medicine’. If experts are able to find a good balance between the use of AI
3
DR DOLPHIN
SPRING 2021
and the skills of highly trained medical professionals - healthcare as a whole would benefit and be transformed even further into a highly innovative and successful system. At present, technology has already completely revolutionised the way in which we seek care. It may seem normal to us now, but in the UK most medical records are now digitised. We can schedule appointments online instead of calling in and we can even check into clinics using our own personal mobile phones - all quite modern concepts! Furthermore, programs like Germwatcher designed to detect, track and investigate infections in patients in hospitals, now exist and can help us gain knowledge that otherwise we might have trouble understanding. There exist decision support systems that use inputted symptoms and special algorithms to generate potential diagnoses. Furthermore, a more fascinating, and some might even say frightening, technology is the use of robotic surgical systems like the Da Vinci robot - equipped with robotic arms, precise movement and magnetised vision. All of these forms of AI seem generally beneficial, so what could possibly go wrong? The relationships built between physicians, nurses and other clinicians with their patients assumes a system built on human care and interaction. However, nowadays electronic health records and data collection in computers seem to be getting the way of this. Doesn’t the idea of talking to a doctor while they type furiously
Ovarian Cancer Detection by Dogs
into their computer, trying to keep up with what you are saying as they update your records, seem too familiar an image? Critics may argue that healthcare is slipping into an artificial state and becoming too impersonal. Additionally, the legal issues with sensitive personal data being stored on online databases does make people nervous. Some people do not trust that their data is being stored securely on computers, instead of manually recorded and kept in secure, physical filing systems. While there are a few issues with the use of AI in the medical system, overall the benefits are astronomical and outweigh the negatives. Personally, I think we should all be excited for what the future holds in the healthcare sector. Furthermore, whilst many believe that doctors could risk being replaced, that will never be the case. We are heading towards evolution not extinction, and while the role of healthcare professionals will most certainly change and adapt, it will ultimately grow alongside technology and shape a brighter future for medicine as a whole. Nadia Baghai LVI References: https://bjgp.org/content/68/668/143 https://healthitanalytics.com/news/arguing-t he-pros-and-cons-of-artificial-intelligence-inhealthcare Dogs are known to have a highly evolved sense of smell, having up to 300 million olfactory (smell) receptors in their nose compared to just 6 million in humans. Studies have further shown
4
DR DOLPHIN
SPRING 2021
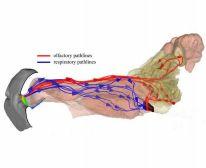
that their noses function differently to ours. We smell, inhale, and breathe through the same airways within our nose, whereas dogs have a fold of tissue just inside their nostrils that separates the air to perform two different functions: olfaction and respiration. 12% of inspired air diverts to a recessed area in the back of the nose (red), which is dedicated to olfaction.
The rest of the air (blue) continues past this area and performs the expected function and enters the lungs via the pharynx (black). In addition, dog’s have a part of their brain that is devoted to analysing smells, which is 40 times greater than ours. As a result, their sense of smell is overall 10,000 to 100,000 times more acute.
Have dogs been successful in detecting ovarian cancer? The short answer to this question is
yes, and with high rates of success too. A dog’s incredibly strong sense of smell enables them to smell the cancer odour molecules emitted by cancer cells that have been taken from patients. This has led to numerous studies being set up, for example, a study in 2018 worked with dogs from Penn Vet Working Dog Centre, training them to detect malignant ovarian cancer using plasma samples from people at the Perelman School of Medicine. One German Shepherd, Osa, was presented with dishes of blood containing a benign sample, malignant sample, and normal samples, as well as other irrelevant samples to act as “distractors”. Whilst smelling these different samples, Osa suddenly froze and stared at one sample- she had correctly identified the cancer.
Similar research in 2013 has been carried out such as one that aimed to see how well trained dogs could accurately detect cancer odour in the blood of ovarian cancer patients. It also wanted to study whether their ability to detect this smell was affected by treatment to reduce the tumour burden, including surgery and five courses of chemotherapy. This study found that dogs showed high sensitivity (97%) and specificity (99%) in recognizing viable cancer cells thus concluding that canine detection gives a very good assessment of the prognosis of the study patients. However, their reliability did decrease with blood samples that had been through chemotherapy, which is most likely explained by the fact that reducing the number of cancer cells
5
DR DOLPHIN
SPRING 2021
also reduces the number of odour molecules, making the cancer harder to smell and detect. How were dogs able to detect these malignant cancer cells? Through investigating the chemistry of human body odours, it has been found that dogs detect changes in volatile organic compounds (VOC) in plasma. The VOC changes take place in the early stages of ovarian cancer and produce a specific odour. A further step into these findings. It is hoped that these ordourants can be collected and/or isolated and are able to be translated into a device and electronic system. The Nano/Bio Interface Centre is creating an electronic nose made of nanosensors that mimic the abilities of a canine nose, producing a tool that could be used in the future for use in ovarian cancer detection.
abdominal cavity so patients are unlikely to feel a tumour. At a later stage, when it is eventually easier to detect, it is much harder to treat with there thought to be around 4,200 ovarian cancer deaths in the UK each year (11 per day). Therefore, this research using canine detection could be life-saving as it has the ability to detect cancer reliably and easily at a much earlier stage than before. This should result in lower mortality rates in the treatment of ovarian cancer. Anneliese Mayer LVI References https://www.pbs.org/wgbh/nova/article/dog s-sense-of-smell/ https://www.vet.upenn.edu/about/press-ro om/bellwether/bellwether-magazine/bellwe ther-fall-2018/sniffing-out-ovarian-cancer https://www.ncbi.nlm.nih.gov/pmc/articles/ uPMC3765942/
What is the significance of this research?
https://www.healthline.com/health/cancer/ ovarian-cancer-early-signs#types
Currently, ovarian cancer is easy to treat in its early stages, however, extremely hard to detect due to the ovaries being located deep within the
https://www.cancerresearchuk.org/health professional/cancer-statistics/statistics-by
6
DR DOLPHIN
SPRING 2021
Birth and Bacteria In a world obsessed with hygiene and cleanliness, science and technology have provided us with cleaner alternatives for just about everything. But in the case of childbirth, maybe it wasn’t designed to be pristine. When women give birth vaginally, their baby is exposed to a vast array of microflora and bacteria, not only during their passage through the birth canal, but also through contact with the mother’s skin and any faeces passed during the birth. While it may seem counterintuitive that evolution and natural selection has facilitated immediate contact with its mother’s excrement, it creates a microbiome of bacteria that helps the baby develop a strong immune system. However, in the UK, it is estimated that 30% of infants are born via caesarean section, with almost half being elective. In recent years scientists have begun to investigate how different modes of delivery can affect a newborn’s immune system. A 2011 study found that the mode of newborn delivery contributes not only to variation in the infant microbiome, but also the diversity of bacteria introduced. According to the study, vaginally delivered babies possessed similar microbiomes to the maternal vaginal and fecal flora. The babies’ gut bacteria consisted primarily of lactobacillus and within months showed a strong proportion of bifidobacterium, both of which are considered by biologists to be health promoting bacteria. The study goes on to demonstrate that the microbiomic composition of caesarean born
infants’ had lower distributions of bifidobacterium and alarmingly contained staphylococcus, which is potentially pathogenic. Their bacterial profile also had much higher levels of hospital bacteria, which in some cases made up 30% of their total microbiome. Several studies have concluded that over time these differences largely disappear, to the extent that caesarean born and vaginally born infants’ microbiomes become indistinguishable by 9 months. However, it appears that by this point each birth type has already acquired certain predispositions. Low diversity of bacterial microbes in the gut has been linked to an increased risk of several diseases including inflammatory bowel disease, asthma, coeliac disease and obesity. It can also have a lifelong effect on the body’s response to medicinal drugs, and can increase the propensity for allergies by a staggering 800%. Additionally, there is evidence from both human and rodent studies that highlights the key roles played by the gut microbiome in the development of brain functioning, cognition, anxiety and sociability. In most cases the increased risk posed by these conditions is very minor and the cause may be hard to distinguish from other correlating factors. For instance, diversity of gut flora can be compromised as antibiotics are more frequently used to prevent infection in a caesarean birth. It is more likely (especially in emergency c sections) for caesarean born babies to be separated from their mothers for longer periods which reduces exposure to the maternal skin microbiome, potentially limiting the development of a robust and varied immune
7
DR DOLPHIN
SPRING 2021
system. When faced with the task of trying to replicate the bacterial exposure during natural births, one of the first methods researchers investigated was ‘vaginal seeding’ by which vaginal swabs from the mother were applied to the infant’s face. Clinical bodies quickly rejected this idea. Rather than just deeming it ineffective, it was concluded that this method was actually harmful. However, trials later undertaken by Willem de Vos and Sture Andersson at the University of Helsinki may have unearthed a promising but unorthodox solution. Their infant group sample each received a dose of their mother’s gut bacteria, delivered via a highly diluted breast milk solution containing traces of carefully screened fecal microbiota from the mother. Amazingly, the cohort went on to develop a bacterial population that resembled that of a vaginally born infant, almost perfectly.
-different-micr obiome-but-not-for-long/ 3. https://www.bbc.co.uk/news/health-4974 0735 4.https://digital.nhs.uk/data-and-inform ation/publications/statistical/mater nity-services monthly-statistics/january-2019#ke y-facts 5.https://www.nhs.uk/conditions/caesare an-section/risks/ 6.https://pubmed.ncbi.nlm.nih.gov/3300 7265/ 7.https://www.economist.com/science-a nd-technology/2020/10/17/how-to-ar m-caesare an-babies-with-the-gut-bacteria-they -need
As modern medicine advances and along with it our ever-growing antiseptic capability and desire, it is almost ironic that the introduction of bacteria could be just what we’re looking for. Maybe in this case a little bit of dirt is exactly what we need. Aimee Wong Rogers LVI Sources 1. https://www.ncbi.nlm.nih.gov/pmc/a rticles/PMC4681407/#:~:text=Infant s%20born%2 0vaginally%20have%20a,et%20al. %2C%202010). 2. https://www.newscientist.com/articl e/2216818-c-section-babies-have-a 8
DR DOLPHIN
SPRING 2021
Biomaterials: Changing the Face of Dentistry Like in so many fields of science, technological advancements are the reason for improved efficiency and increased opportunities in treatment. Dentistry is no different, and this has brought exciting prospects of utilising biomaterials- a creative regenerative discovery. Kangaroos, elephants, sharks and alligators- what do they all have in common? Their teeth! Not the shape or quantity, or ease of mutilating their prey, but the ability to regrow. These polyphyodonts are capable of replacing their teeth when tissue that supports them, known as the periodontium, is worn down. This leaves gaps (more scientifically referred to as diastemas) which permit the teeth growing behind the original as a result of their abundance of stem cells to be able to move forwards and take their place. This cycle can continue as there is room at the back for new teeth to grow and so their chewing, which is an imperative part of their digestive process, will never be compromised due to a lack of a full set of robust teeth.
Humans, on the other hand, do not possess this hugely advantageous traitwe are mere diphyodonts. We have just two successive sets of teeth: milk teeth (also known as deciduous teeth) and adult (or permanent) teeth. Though these have evolved to be much more durable so they can last our entire lives and our diet has changed resulting in less strain on our teeth through mechanical breaking down of our food,
that is not to say they always do last for that long. In the case of damaged or missing teeth, there are numerous restorative measures that can be taken: veneers and crowns for the former as well as prosthetics such as implants, dentures and bridges to treat edentulism (toothlessness). Although some provide a more long-term remedy, a permanent solution requiring no further maintenance or replacement is yet to be available. However, biomaterials may be the future of regenerative dentistry. These synthetic substances, alongside stem cells, have the potential to repair and stimulate the growth of pulp and surrounding dentin tissues that make up the central chamber of the tooth as well as the crown and root which form the main structure. Despite being inserted like a dental filling, biomaterials differ from the existing material used to fill cavities in their properties of being compatible with pulp tissue and non-toxic to cells. Using translational therapy, they can modify the behaviour of the stem cells as the cellular microenvironment is imitated to allow optimum conditions for differentiation and so development of these tissues to occur. This, effectively, enables an affected tooth to heal itself or regrow completely. This would prevent the need for extensive drilling to remove decay and insert a filling which is only a temporary solution and, if unsuccessful, would require a root canal causing further impairment of the tooth. Biomaterials offer a significantly more benign treatment plan with longer-lasting results that do not require additional management and support; this ultimately reduces the cost and time of the process. Although stem cells have already shown huge potential in the field of science,
9
DR DOLPHIN
SPRING 2021
further research and trialling is needed before this treatment can be clinically approved. Testing on rats has been carried out but humans have yet to be involved in experimentation. However, this biological therapy brings exciting possibilities to restorative dentistry which is so essential in maintaining dental health. Therefore, it is crucial that creativity and innovation continues to grow and be such a prominent aspect of science to allow more incredible and revolutionary advancements in this branch of research.
https://www.ncbi.nlm.nih.gov/pmc/articles/P MC5126784/
Dahlia Levin UVI
https://www.ncbi.nlm.nih.gov/pmc/articles/P MC5370483/ https://www.sciencedirect.c om/science/article/pii/B978 0081024768000013 https://dentistinodenton.co m/animal-replacement-teet h/ https://www.labroots.com/trending/plants-an d-animals/14456/animals-regrow-teeth-hum ans https://link.springer.com/chapter/10.1007/97 8-3-319-14845-8_8
10
DR DOLPHIN
SPRING 2021
Creativity and Science: How Andrew Pelling’s experimental lab is redefining the limits of medicine Andrew Pelling is an award winning scientist who runs one of the most experimental labs in the world, based at the University of Ottawa. His goal is nothing short of ambitious: to build novel materials for next generation medical innovations and speculative living technologies of the future. In his lab, this involves making ears out of apples and regenerating spinal chords out of asparagus. Controversial, no? Now, it might sound ridiculous and impossible, and many more ‘rational' scientists have dismissed his research because of its straight forward of concepts. Yet, sometimes we can solve the biggest problems with the simplest solutions. Maybe the answers have been in front of us the whole time- even as close to us as our kitchens. In the early 1800s, Hungarian physician Ignaz Semmelweis was shunned for his suggestion that a micro biome of microscopic harmful cells lived on our hands and skin, urging other surgeons to wash their hands regularly. For years scientists were certain that the Sun orbited the Earth. History is a reminder that we need to keep an open mind, at the end of the day there is technically no certain known ‘limit’ to the potential of science. Andrew Pelling began to rethink how we use materials to reconstruct damaged or diseased human tissues. His lab stripped plants of their cells and DNA, leaving behind natural fibres that acted as scaffolds for human tissue. He talked about his love of finding broken machine parts and mixing them together to build
something new- and his lab did just that. They took an apple, removed all apple cells and DNA and implanted human cells into the cellular scaffolds which worked very similarly to our organs and tissues. The human cells divide by mitosis and fill the structure, and what fascinated him was when he observed that once implanted, the body treats it like its ownsending cells and blood supply that keeps it alive. Encouraged by these findings, he asked his wife, a musical instrument carver, to carve human ears out of apples. By treating biology ‘like hardware’, and using only soap and water, his lab offered an alternative to commercial scaffolds which scientists have been working on for decades which use proprietary products, animals or cadavers. He put his research into an online open research and started a company determined to develop kits so that in the future, we might be able to augment our bodies from our own kitchens. His next revolutionary idea emerged when he was cutting asparagus in the kitchen, noticing the amazing vascular bundles which reminded him of one of the most spectacular tissues in our bodies- the spinal cord. There is currently a global bioengineering effort aimed at treating spinal cord injuries as ½ a million a year suffer from pain or numbness to paralysis- a complete and utter loss of motor function.Most research has been using synthetic polymers, animal products or human caradures to solve this
11
DR DOLPHIN
SPRING 2021
problem.
Pelling’s Lab noticed the asparagus scaffold had microchannels which may guide regenerating neurons like those in our spinal cord. It moves and bends and has the same texture and flexibility as human tissue. But humans aren’t plants, our cells haven’t evolved to grow on plant tissues and have no business in our spinal cord. At least according to many critics of his research. These guiding structures should disappear over time, but humans lack the enzymes to break these tissues down. However, this proved to be more beneficial than restraining- the inertness of plant tissue made it biocompatible as the body doesn’t detect or reject it, while at the same time cells which are regenerating can benefit from its shape and stability. He became wrapped in doubt - he felt like an outsider, did he have the right to work on such a complex problem? So he surrounded himself with wire neurosurgeons, clinicians, biochemists and bioengineers and began to start planning experiments. In the experiment which was repeated several times he took a rat and anaesthetised it so they could sever its thoracic region slightly, enough to paralyse its lower body. They then implanted the scaffold between ends of severed spinal cords which acted like a bridge and he began to see that they recovered some mobility. No stem cells, electric stimulation, pharmaceuticals, exoskeletons or physical therapy had been used- and the rats were showing signs of a regenerating spinal cord.
This was no easy experiment, it at times felt morally wrong to paralyse the rats, but the team was encouraged by constant positive results. They were still sceptical about them and repeated the experiment until his lab was nearly bankrupt- just to be certain that his findings were true. This is the start of something extraordinary and they are just beginning to be translated into the clinic, the new technology was designated a breakthrough medical device by the FDA. Human clinical trials are set to begin in two years. As scientists, we spend our lives living on a knife’s edge,” he explained, “on the one hand, it’s our job to fundamentally broaden the horizon of human knowledge. But at the same time, we’re trained to doubt: to doubt our data, to doubt our experiments, to doubt our own conclusions. We spend our lives crushed under the weight of constant, unrelenting, never ending anxiety, uncertainty and self doubt. This is something I really struggle with. But I think almost every scientist can tell you about a time they ignored those doubts and did the experiments that would ‘never work’, and the thing is, every now and then, one of those experiments works out. The challenge we face is that while doubt can be destructive to your mental health it's also the reason why scientific rigour is such a potent tool for discovery. It forces us to ask the difficult questions and repeat experiments, nothing about that is easy. Often it becomes our responsibility to bear the burden of the hard and sometimes heart wrenching experiments. This ultimately leads to the creation of new knowledge, and in some really rare cases
12
DR DOLPHIN
SPRING 2021
the type of innovation that just might change a person’s life.” Andrew Pelling’s work has made many scientists reflect on the role of creativity in science as well as bravery it requires to suggest what has never been suggested before. It can be daunting, but thanks to the risk he took humans now have the potential to design
References: Ted talks: https://www.ted.com/talks/andrew_pelling_t his_scientist_makes_ears_out_of_apples?l angua ge=en https://www.google.co.uk/url?sa=t&rct=j&q= &esrc=s&source=web&cd=&ved=2ahUKEwj klNS
the architecture of plant tissues in such a way that they can encourage cell growth, meeting unmet medical needs we face now or in the future. Chiara Champeaux Year 11
y5JbvAhULHxoKHXh9DeUQtwIwAXoECAU QAw&url=https%3A%2F%2Fwww.ted.com %2Ft alks%2Fandrew_pelling_could_we_treat_sp inal_cord_injuries_with_asparagus%2Ftrans cript %3Flanguage%3Den&usg=AOvVaw3MfHlb 3jYvwwr83obk9SLt Pelling’s Lab website: https://www.pellinglab.net
13
DR DOLPHIN
SPRING 2021
Obesity: Is it all to do with overconsumption? Obesity is currently associated with the leading causes of death worldwide including diabetes, ischaemic heart disease and cancer, with at least 2.8 million people dying each year a result of being overweight or obese. It has reached epidemic proportions globally - an increasingly concerning problem for not only high income but also low income country governments to mitigate as food becomes further accessible to citizens. By 2030, more than 2.16 billion individuals are expected to be overweight. Overweight and obesity are defined as abnormal or excessive fat accumulation that presents a risk to health and is prevalent in environments which promote physical inactivity and mass consumption of high calorie foods. However, not all people living in such environments will become obese, nor will all obese people have the same body fat distribution or suffer the same health problems. The link between obesity and genetics is still somewhat debated, the most widely accepted cause of obesity lying in environmental factors. Although genetic changes in humans occur too slowly to be the prime factor in the obesity crisis, the imbalances in how people respond to the same environment implies that genes do in fact play a role in the occurrence of obesity. Other factors that influence the heritability of obesity include epigenetic marks. Genes code for specific proteins to be made within cells in response to changes in our environment. Studies of resemblances and differences among family members and twins have shed light on evidence that explains the large quantity of the differences
in weight among adults. Additional research between obese and non obese people have pinpointed variants in several genes that potentially contribute to obesity by increasing hunger and food intake. In most cases obesity probably results from interaction between a multitude of genes, more than 50 different genes, and environmental factors (multifactorial obesity). Very rarely does obesity occur in families in line with one clear inheritance pattern as a result of changes in a one single gene (monogenic obesity). But how do genes influence obesity? The brain controls food intake by reacting to signals transmitted from adipose tissue (fat), the pancreas and the digestive tract. These signals are carried by hormones such as insulin (regulates blood glucose concentration) and leptin (controls appetite). The brain then coordinates these signals and responds to the instructions of the body - to eat more and reduce energy or the opposite. Genes are the basis for the signals and responses that control food intake and small changes in these genes can affect their activity. Genes that have been linked to obesity include: A) FTO GENE - this a protein found on chromosome 16. The presence of this gene has a direct influence on obesity as it promotes food intake; those with this gene have a 30% higher chance of being overweight. B) MC4R GENE ( melanocortin-4 receptor) - contributes to metabolism. This gene regulates the quantities of energy we use from what we eat and stimulates our appetite. Those with a variant of this gene are likely to be overweight.
14
DR DOLPHIN
SPRING 2021
C) ADIPOQ GENE - mutations of this gene are associated with adiponectin deficiency which can lead to obesity and insulin resistance (diabetes). One possible hypothesis to our current obesity epidemic is the prevalence of “energy-thrifty genes”. Energy is vital for survival and human energy regulation is directed towards protecting and preventing weight loss rather than controlling weight gain. The tendency of humans to store energy in the form of fat is more beneficial than storing it in another form as they can hold more energy and are hydrolysed much slower. The storage of energy as fat is hypothesised to result from thousands of years of evolution in environments with limited food supplies. This is where the “energy thrifty gene” comes in. These genes would have helped our ancestors survive famines to much better extent than those who did not have the “thrifty genotype” by storing the energy from food much more efficiently and in greater quantities as fat. These genes are now being challenged by our current environment where food is plentiful and easily accessible all year round. Another proposed hypothesis includes epigenetics. Epigenetic marks or “imprinting” affect gene expression without actually changing the DNA sequence. Changes or failures in imprinting can not only cause extreme forms of obesity but also are associated with human’s susceptibility to obesity. Epigenetic marks are affected by changes in surrounding environments during critical development periods e.g growth of a foetus and are caused by DNA methylation and histone
modifications which regulate the imprinting. As many imprinted genes are growth factors, disorders within imprinting often lead to obesity. As well as growth, imprinted genes are involved in differentiation, development and metabolic functions. Imprinting is regulated by DNA methylation which arises through the addition of a methyl (CH3) group to a cytosine nucleotide. Methylation causes the silencing of gene expression which stops genes from being transcribed during protein synthesis. These methylation patterns can be passed down to children. Histone modifications also control imprinting where the DNA in cells can be packaged as heterochromatin which is tightly stored. This will prevent gene expression as the DNA base sequences are inaccessible to transcription factors. To bring this into perspective, if a mother were to be malnourished during the first half of pregnancy, the child would be more likely to be obese due to inherited epigentic marks from mother to store any food received as fat.
To conclude, it is probable to say that both genetic and environmental effects on epigenetics will in turn be associated with obesity. Clara Gilardi LVI
15
DR DOLPHIN
SPRING 2021
Current Affairs Should Vaccines Be Compulsory? Vaccines are essential in reducing the number of deaths caused by infectious diseases, and are the solution to the current global pandemic. Some of the world’s most major health concerns have been dramatically reduced, almost to the point of eradication, by vaccinations, such as smallpox, polio and measles. However, ever since vaccinations were developed by Edward Jenner in 1796, they have been subject to various ethical debates, the most prevalent being whether vaccinations be a personal choice. Since the outbreak of smallpox in the early 19th century, vaccination mandates have been established, especially for children, to ensure herd immunity is achieved. Herd (or population) immunity is reached when the majority of the population is vaccinated, which provides indirect protection to individuals who are not vaccinated. With the potential to prevent 6 million deaths worldwide each year, vaccinations are a crucial means of ensuring infectious diseases are prevented from spreading rapidly in populations. In the UK, parents have the choice whether to vaccinate their children, but should vaccinations be made compulsory? How do vaccines work? There are various different types of vaccines, however the principle remains the same. Vaccines capitalise on the adaptive immune system, which when exposed to an infection, can respond much more quickly and effectively when exposed to the same
pathogen again. By allowing the immune system to recognise something as a threat by mimicking an infection, and safely allowing the immune system to respond, the immune system can then kill the pathogen extremely quickly when exposed to it again. T-lymphocytes are a type of white blood cell which attack pathogens in the body. After the vaccine imitates an infection, the body retains a few T-lymphocytes, called memory cells, which, if exposed to the same pathogen, can kill the cells more quickly and effectively. B-lymphocytes are another type of white blood cell which are responsible for producing antibodies which attack the pathogens. Vaccines are specifically designed to develop immunity by imitating an infection, without causing an illness. There are five main types of vaccines: live, attenuated vaccines, inactivated vaccines, toxoid vaccines, subunit vaccines, and conjugate vaccines. However, over the last few years, mRNA vaccines have been at the forefront of medical research. The Pfizer-BioNTech vaccine uses this technology, which has been used to vaccinate millions of people in the UK over the last few months. These vaccines work by injecting the nucleic code (mRNA) for the spike protein of SARS-CoV-2 which is contained in a lipid nanoparticle. The nucleic code is incorporated into our cells, which will then begin to produce the spike protein. The body can then recognise this protein as foreign, so amounts an immune response, similarly to the other types of vaccines.
16
DR DOLPHIN
SPRING 2021
Why are vaccines not compulsory? By harnessing the power of the immune system, vaccines are able to save millions of lives every year, however some people refuse to be vaccinated, despite the overwhelming evidence about the safety and efficacy of vaccines. These people are commonly referred to as “anti-vaxxers”, and have dramatically risen in prominence since Andrew Wakefield published false claims about the MMR vaccine leading to autism. The World Health Organisation views vaccine hesitancy as one of the top ten global threats, which can be seen when in 2016 there were more than 500 cases of measles reported in England, which was more than five times the number of cases reported in 1996. Another group of people who oppose vaccinations are certain
religious groups. For example, some Christians argue that if God has decided that someone will die from smallpox, it would be a sin to stop God’s will by vaccination. Some people are also medically unable to have vaccinations due to compromised immune systems, or allergic reactions in response to certain vaccines. These three groups of people will make it very difficult for vaccines to ever be compulsory, as there will always be people who either strongly oppose vaccinations, or physically cannot be vaccinated due to the health risks. Should vaccines be compulsory? Although vaccines provide the solution to infectious disease which can quickly spread across the world, it is not right to impose compulsory vaccinations on a population, as not only will it be very difficult to enforce, but people should be given the choice due to religious or medical reasons. Instead of enforcing vaccinations, the problem of vaccine hesitancy should be solved by educating people on the safety, efficacy and abundant benefits of vaccines, whilst highly recommending that everyone who is offered a vaccine should take this opportunity. Jess Gilbert LVI6 References https://www.bbc.com/news/world-48186856 https://www.cdc.gov/vaccines/hcp/conversations/dow nloads/vacsafe-understand-color-office.pdf\\ https://en.wikipedia.org/wiki/Vaccine_hesitancy#Religi onhttps://www.genengnews.com/insights/mrna-addre ssing-the-blind-spot-of-enzyme-replacement-therapy/ https://www.theguardian.com/world/2020/dec/02/howdoes-the-pfizerbiontech-covid-vaccine-work-and-whowill-get-it https://www.bbc.co.uk/news/world-481868
17
DR DOLPHIN
SPRING 2021
Implications of COVID-19 on the lungs The coronavirus. A chaotic pandemic that has dominated our lives for nearly a year now. It has been established that COVID-19 is a respiratory disease, and can cause a range of breathing problems- from mild to extremely severe- but as we approach the anniversary of lockdown in the UK, what exactly does this virus do to potentially devastate such a vital organ? How does it even get inside our system? And what makes this disease so spreadable? The coronavirus enters the body through the nose or mouth via a receptor called ACE2, which is important for controlling blood pressure and electrolyte levels and it is also found in the lungs, the back of the throat, tongue and nose. Researchers have also found a supply of protease in the nose, which chemically removes the top section of the coronavirus spike, allowing it into nasal cells. Because of this splitting off, COVID-19 can bind 10 times more tightly to insert its RNA into the cell, which can explain why the virus spreads so easily around the body. In fact, the viral content in the upper respiratory tract has been found to be at its highest at day one, suggesting that its peak preceded any symptoms and highlights how the virus can be transmitted without the onset of symptoms. Inside the lung, the ACE2 receptor sits on top of lung cells and are essential for producing surfactant- a compound that coats the alveoli, and plays an important role in gas exchange. Reduced surfactant from the viral destruction of lung cells means it is harder to keep the alveoli open. White blood cells are sent here as an immune response, however blood vessels
around these air sacs become leak fluid in response to inflammatory chemicals that the white blood cells release, which puts pressure on the alveoli from outside and, in combination with the lack of surfactant, causes them to collapse, leading to pneumonia and difficulty breathing. While most people fully recover from pneumonia, lung injury associated with COVID-19 may result in long-term breathing problems. More severe inflammation can lead to acute respiratory distress syndrome (ARDS), where patients require a ventilator. Some people also react to the virus’ presence by producing an intense immune response- a cytokine storm. The body replaces damaged cells with scar tissue and potentially leads to pulmonary fibrosis, making people breathless and patients may have long-term pulmonary scarring. What factors increase lung damage? By now it is obvious that age, smoking, and other underlying health conditions play an immense role in the risk of severe infection and how likely a person is to recover. Inhalation of cigarette smoke irritates the lungs, unleashing the immune system to fight said irritation. Adding on a coronavirus infection with that further amplifies the
symptom response, putting smokers at risk
18
DR DOLPHIN
SPRING 2021
of a more severe case. Older people may have less elastic lung tissues and a weakened immune system that occurs with advanced age. Also, timely support and proper care of patients can massively minimise the long term effects. Lastly, disease severity. This could be down to pure luck whether the person has a mild or a severe case. Milder cases are far less likely to cause lasting scars in the lung tissue.
Over time, the tissue will naturally heal, but it can take up to a year for a person’s lung function to return to pre-covid levels and respiratory therapists will be very much needed to help COVID-19 survivors. Unfortunately the virus doesn’t only impact the lungs, researchers and doctors have found there to be other effects on the brain, kidney and liver, to name a few. Even with the development of a vaccine, there is still so much left to discover about this virus
Tabitha Iliffe LVI
https://www.hopkinsmedicine.org/health/con ditions-and-diseases/coronavirus/what-coro navir us-does-to-the-lungs
References and further reading: https://www.medicalnewstoday.com/articles/ covid-19-what-happens-inside-the-body#Ph ase4:-Acute-respiratory-distress-syndrome,thecytokine-storm,-and-multiple-organ-failure https://theconversation.com/coronavirus-can -cause-lasting-lung-damage-but-the-effectsmay -ease-over-time-140398
https://www.weforum.org/agenda/2020/04/th is-graphic-shows-what-covid-19-does-to-yo ur-b ody/
19
DR DOLPHIN
SPRING 2021
The Importance of Vaccines in Healthcare Smallpox, tetanus, diphtheria, meningitis and polio to name but a few are prime examples of the pivotal role vaccinations play in combating the most dangerous diseases not only in childhood, but also in major epidemics and pandemics, like Ebola and, most recently, COVID-19. While vaccines remain “the most effective tool for preventing infectious diseases and improving global health” and are “relevant to people of all ages and in all countries”’ as mentioned in the Vaccine Innovation article within the New England Journal of Medicine in which Professor Chris Witty illustrates how “celebrating vaccines is really celebrating the power of our immune system”. With further research, we are able to see that vaccines do not actively kill or defeat the virus, but instead we do. I think it is important to begin with analysing why vaccines are actually necessary. While the human anatomy consists of physical barriers such as that of the skin, mucous membranes and expulsive reflexes such as that of coughs and sneezes, we also have the nonspecific immune system. While the non-specific immune response, which includes processes such as phagocytosis, is highly effective, it provides the body with no “memory” of the pathogen and is therefore not what the vaccine seeks to initiate. Instead, vaccines stimulate the specific or acquired immune system. Acquired immunity is dependent on the specialized white blood cells known as lymphocytes. Lymphocytes originate from stem cells in the bone marrow and divide continuously to
release immature lymphocytes into the bloodstream. Some of these travel to the thymus to differentiate into T cells, while others remain in the bone marrow- these are called B cells. Both T and B cells recognize and help eliminate foreign pathogens (with antigens), but do so in very different ways and are essential to the vaccination process. Antigen presenting cells, produced in the non-specific defence system, present the foreign antigen (vaccine antigen) to T Helper cells. The receptors on the T helper cells fit the antigens and become activated to produce interleukins, stimulating T cells to divide rapidly via mitosis, forming clones of activated T cells. These are able to develop into killer T cells which are specific to the presented antigen and destroy infected cells. These interleukins, produced by T cells, are also able to activate B cells which produce specific antibodies to fit the antigens on the surface of the pathogen (acting as opsonins or agglutinins). Some of these B cells, however, develop into memory cells which would be able to wipe out the pathogen rapidly should it ever return. This is known as the secondary immune response. But, what is the importance of this timeline in vaccination? Well, it allows us to understand why some vaccines require a second or third dose to maintain protection. While the primary vaccination can be likened to a “first infection”, there is a “lag phase” after which B cells and T cells initiate their immune response. The response to the second vaccine, however, is like a “second infection” and is therefore faster. This vaccination schedule leads to longer lasting and more powerful immune responses.
20
DR DOLPHIN
SPRING 2021
However, in order to appreciate the complexity and application of this immense science, it is vital to look at that of the arguably most notable immunization-related accomplishment- the eradication of smallpox, which was verified by the World Health Organisation in 1980. Edward Jenner, a country doctor (roughly equivalent to a GP) made the intelligent observation that dairymaids, who had cowpox, did not get smallpox. Perhaps this is more clearly highlighted in Jenner’s own small experiment. When Jenner inoculated a small sample of cowpox from Sarah Nelms, who was infected, and transferred it into James Phipps (an eight year old) he showed mild symptoms of the disease and then proceeded to recover. However, when he was soon after infected with smallpox, he showed no symptoms at all. What Jenner took from this was that a milder disease provided immunity to a more severe one. But, Jenners observations did not stop there. He also noticed that in history, and with the smallpox vaccine, that vaccine protection often diminished as time went on. This knowledge is still extremely relevant today. While vaccines can prevent infection, they are also able to prevent the significance of the disease should someone become infected with the disease. With this, they essentially reduce the severity of the disease and prevent mortality rates worldwide. This knowledge is extremely relevant to the current COVID-19 pandemic and its vaccine- perhaps a revaccination might be necessary? This contributes greatly to the deployment of a vaccine. For this, there are several “main” strategies. The first was used
effectively in smallpox and Ebola outbreaks. For this, a rapid vaccine is used and is initiated by identifying extreme cases and vaccinating their close contacts, and the contacts of the contacts essentially forming a “ring” and the technique is thus titled “ring vaccination”. While this has been proved successful, it is not applicable to the current pandemic as often symptoms are minimal or not present at all. The second, however, might be more relevant. This technique begins by identifying those at high risk of dying, catching and spreading the virus and vaccinating these individuals. These include the elderly, the immunosuppressed or front line workers. However, it would be inappropriate not to mention how vaccines are dependent on the trust and efficiency of the products themselves. In addition, in the administers and scientists. Failure or mistakes in the vaccination would have “substantial long term public health consequences” according, again, to Vaccination Innovation. This pattern can be easily seen also from Andrew Wakefield and his colleagues’ now discredited study. Since the 1970s there has been skepticism on the safety of vaccines e.g. against pertussis or whooping cough, however the retracted paper in The Lancet is arguably the most famous. The paper that was built on the work of 12 children promoted the non-existent connection between the MMR vaccine and Autism. This catalysed the anti-vaccine movement for those who are afraid of complications related to the vaccine. With this, people fear their DNA may be altered to produce cancer. To overcome this, education efforts have been put in place and public health experts have focused on
21
DR DOLPHIN
SPRING 2021
the benefits of mass vaccination to the general population. In conclusion, incredible progress has been made since Jenner’s smallpox vaccine discovery including the control of childhood diseases (such as measles, mumps, rubella and polio). These scientific breakthroughs have led to the rapid expansion of knowledge of the complex immune system at a molecular level and has allowed for the COVID-19 vaccine to be developed at the fastest rate in history. With this, it can be clearly seen the huge possibility for discovery in controlling pathogens and providing effective vaccines to the pathogens of all nature including cancers. Chris Witty explains that there is “good theoretical reason for thinking that we could use vaccines to help prevent or treat cancers” which is an interesting area for future research. Nicole Monaghan LVI References: https://www.ncbi.nlm.nih.gov/pmc/articles/P MC1200696/ https://www.nejm.org/doi/10.1056/NEJMp20 29466 https://www.gresham.ac.uk/lectures-and-ev ents/vaccination
22
DR DOLPHIN
SPRING 2021
Lectures BMJ ‘Born Equal - Racism in Medicine’ Lecture In this lecture on the process of putting together the British Medical Journal (BMJ) ‘Born Equal-Racism in Medicine’ issue, Zosia Kmietowicz (news editor), Navjoyt Ladher (head of education) and Juliet Dobson (opinion and bmj.com editor) discussed the dilemmas they encountered whilst compiling articles for the journal and the steps they took to resolve them in order to publish and shed light on the experiences of doctors and patients from minority ethnic backgrounds and how little progress has been made in combating racism and prejudice within medicine. With the senior editor team responding positively once the idea of an issue dedicated to the topic was proposed, the team invited guest editors Victor Adebowale (chair of the NHS Confederation, crossbench member of the House of Lords, former NHS board member) and Mala Rao (senior clinical fellow at Imperial College London and medical adviser to NHS England’s workforce race equality, both of whom have been extremely vocal in their calls to hold the healthcare system accountable for the racism that is perpetuated within it. In this way, every decision that was made would be well-informed from all angles with advice from the most influential voices.
With this in mind, they engaged in many conversations surrounding the various ethical dilemmas. One such dilemma they faced was naming the prejudice experienced by doctors and patients from minority ethnic backgrounds from various areas of the medical sphere, be that medical schools, the NHS and/or regulators etc. This question, the editors explained, was quickly resolved with a unanimous decision that there should be no hesitancy to call it what it is - racism. However, what dominated the majority of discussions was the collective terms to be used within the issue. During the lecture, the speakers pinpointed the various collective terms that were brought up in the meetings and their reasoning for their conclusion, which was to use the term ‘ethnic minority’, ensuring that specificity is maintained throughout i.e. avoiding use of umbrella terms as much as possible. Some of the terms that were mentioned included Black and Minority Ethnic (BME); Black, Asian and Minority Ethnic (BAME); Person of Colour (POC); Black, Indigenous and People of Colour (BIPOC); non-White and ethnic minority. Collective terms such as
23
DR DOLPHIN
SPRING 2021
these mask specificities and individual details, which are vital to comprehend when discussing the impacts of ethnicity within medicine. To illustrate this point, Zosia Kmietowicz brought up the very topical example of COVID-19, reasoning that during the first wave, the poorest outcomes were seen in those of a South Asian background, particularly individuals with familial roots in Pakistan and Bangladesh and by using collective terms such as BAME, these crucial details will be lost and therefore effective action cannot be taken to minimise the disproportionate impact on the aforementioned groups. Moreover, acronyms such as BAME and BME are UK specific and accessibility is a key factor of the language used within the journal. Not only are they UK specific, however, even within the UK, studies have found that out of 300 people only a couple had a vague understanding of what the terms stood for. Kmietowicz went on to explain that the media is also beginning to recognise this with The Sun tweeting that they would no longer be using the term BAME declaring it “outdated” and saying it “obscures important differences between ethnic groups” on 5th March 2021. Using this language would have therefore made the journal inaccessible and would have ultimately minimised the impact of the content within it. Another factor that had to be taken into consideration were the opinion pieces. An overwhelming number of pieces were submitted and deciding which to publish proved to be a difficult task, not only because of the sheer volume but also because of the process of distinguishing which would have the most impact and relevance. Among those submissions were
many pieces targeting religious discrimination, which although highly important and impactful were not as relevant to the issue. Others, although descriptive and emotive, were not productive and analytical pieces and so were also deemed unsuitable for this particular issue. Within the topic of opinion pieces also lies the issue of the contributors. The BMJ editors originally decided not to ask for contributions from their two regular weekly columnists, both of whom are White but were encouraged by Adebowale (one of the aforementioned guest editors) to allow them to write their weekly column suggesting that this issue should feature voices from all backgrounds. The editors went on to explain the range of feedback they received and the discussions this generated. One of the aforementioned columnists had taken to twitter to ask for advice and guidance on their piece. They were originally applauded for their initiative, however later received backlash for using others’ experiences and ideas and publish them as their own. The shift in response to this piece can be attributed to a range of factors whether it be the political climate or another factor entirely, but it was an interesting point nonetheless. The final point of significance was the question of how to keep the conversation going beyond the special issue with the most enlightening topics breached in the lecture being the extent to which racism is present at medical schools, the implications this could have on future medical advancements such as within the realms of AI and how the shifts in politics leads to further disparity within the medical profession e.g. after Brexit there was an
24
DR DOLPHIN
SPRING 2021
exponential increase in attendance of Eastern European doctors to support groups. All of which are discussed at length within the journal itself, which can be accessed at https://www.bmj.com/racism-in-medicine. To end with, the panelists provided some reading recommendations, which I have included below for your interest: Medical Apartheid - Harriet Washington Political Determinants of Health - Daniel Dawes The Immortal Life of Henrietta Lacks Rachel Skloot Overall, this lecture was highly valuable. The perspective of journal editors was one that I, personally, had neglected to
consider when reading pieces from medical journals, however is something that is worth reviewing. Moreover, gaining an insight into the process of creating a journal with the purpose of maximum impact, reach, and accessibility is interesting to keep in mind, especially while actually reading the pieces and recognising the impacts of this on its language, contributor and content. One final note. Combating racism in medicine will not only improve outcomes for patients, however will have enormous implications on the medical practitioners and wider society. It is a conversation that, as the editors highlighted, should not be limited to “special issues”, however, should be at the forefront of discussions about the healthcare system. Rojin Zahaki LVI-16
References: Kmietowicz, Z., Ladher, N. and Dobson, J., 2021. BMJ ‘Born Equal-racism in medicine’. Zamila Bunglawala (2019). Please, don’t call me BAME or BME! - Civil Service. [online] Blog.gov.uk. Available at: https:// civilservice.blog.gov.uk/ 2019/07/08/ please-dont-call-me -bame-or-bme/ [Accessed Mar. 2021]. Bmj.com. (2021). Racism in medicine | The BMJ. [online] Available at: https://www.bmj.com/racism-in-medicine [Accessed Mar. 2021].
25
DR DOLPHIN
SPRING 2021
Who thinks about ‘Doctors in Distress’? I recently attended a virtual webinar by Dame Clare Gerada where she spoke about the charity, Doctors in Distress. Alongside this, she mentions the book, Beneath The White Coat: doctors, their minds and mental health. This book talks in great detail about doctors’ mental health. I feel really strongly about discussing the importance of managing mental health and I feel that it isn’t discussed enough in a scientific, social or political setting. Since Year 8 the idea of questioning if doctors take care of us, who takes care of doctors has been deep within my mind. I had previously worked on a presentation about it with my friend, which ultimately led to the basis of my EPQ title. My main aim for my EPQ is to investigate what systems are in place or can be put in place to assess the mental health of a medical practitioner. I use the word ‘assess’ broadly, less of judging a doctor’s mental health but more in a way to see if they need extra support or someone to talk to. The Doctors in Distress charity is exactly that; a place where medical practitioners can attend group sessions and a form of psychological PPE (personal protective equipment) is provided. The word PPE is usually used to describe physical equipment e.g. masks, gloves, hazmat suits so I found it intriguing that Dame Gerada used it to describe something that affects us both physically and mentally. She is right of course, mental health illnesses and problems affect us
in more ways than one. Especially during COVID-19, now is the time to think even more deeply about the people taking care of us, all front-line medical workers. To provide some more information about what Doctors in Distress entails, here is the basis and principle upon which it was founded by Amandip Sidhu. The Doctors in Distress charity was inspired by a tragic case of a cardiologist doctor who passed in November 2018. He experienced what is commonly referred to as ‘burn out’ and felt he had only one way to escape the suffering. The founder of the charity passed ownership to Dame Clare Gerada who has helped expand its influence and community. The charity’s aim is to raise awareness of the value of medical professionals' health and well-being.
"IT WILL TAKE TIME AND THERE IS MUCH TO ACCOMPLISH BUT WE BELIEVE THE RIGHT THING TO DO IS TO HELP THOSE THAT CARE FOR US ALL." - Amandip Sidhu I chose to write this article to share my experience of this virtual talk that I attended, as well as raise awareness of the importance of mental health and how common it really is. Especially for a high intensity, stress filled environment that doctors and other medical practitioners work in, managing mental health is crucial. It can be the breaking point of so many young doctors. I want to expand the awareness about how common mental illness is, how people manage it, what the causes might be and how people can help?
26
DR DOLPHIN
SPRING 2021
The term ‘burnout’ is often used when a doctor describes their mental illness. Here is the definition; burnout is a state of emotional, physical, and mental exhaustion caused by excessive and prolonged stress. Even Dame Clare Gerada expressed that she experienced burnout. It can be small or big but signifies a change from the normal routine. For example, one of her main principles that she constantly upheld was to always have curiosity about a patient. As soon as this is not present something is going wrong. How can one treat a patient you’re not interested or curious about? On one occasion she realised that she indeed had lost curiosity and she felt that something was different. This caused her to believe that she experienced burnout.
One of the key points that Dame Clare Gerada touches on is how challenging it
is for a doctor to admit a change in their identity that has evolved over the years. She mentions how a doctor’s identity begins to form from medical school. Understandably, this is where their journey begins; the start of a lifetime to become a doctor. However, as this identity forms so early on, it would only become more concrete as they grow older and to change that identity would get even harder. For example, to go from doctor to patient. She suggests how this is one of the reasons doctors find it so hard to even admit they have a mental illness, let alone get help for one. Once you have obtained such significant training and respect for your position, admitting that you have an illness is extremely challenging. Furthermore, when thinking about the frequency of mental illness we may have to consider the specialty. A statistic Dame Gerada touches up on is the fact that in recent years the number of paediatricians with mental health problems has risen significantly. Whereas, the figures that depict surgeons’ mental health problems is much lower. This could be because surgeons are more prone to handling high pressure situations, or it could equally be that they are more unwilling to report an illness. Why might this be? Does the specific work you do make way for an increase or decrease in likelihood of mental health problems? From what I can infer, different specialties handle varied situations and challenges. However, in the end each Individual is different and will handle a problem differently. The main message that I discovered while researching this, is that doctors are human.
27
DR DOLPHIN
SPRING 2021
Having a mental health problem doesn’t mean that it is untreatable. With the right help you can get better over time. You can often help someone by talking to them, conversing through their problems. Just showing that you care and are there for them can help significantly. Doctors are incredibly skilled humans who can change the fate of life and death with their own hands, but still humans. Humans can get sick, they can also get better, but it is time to stop forgetting that doctors are human as well. We should notice and be aware of the fact that we might need to take care of the ones caring for us. Angelina Kim LVI
28
DR DOLPHIN
SPRING 2021
The Theory of Natural Selection English naturalist Charles Darwin had been working on the idea of natural selection for years, collecting research, making observations, and testing his hypothesis during a five-year voyage to study plants, animals, and fossils in South America and on islands in the Pacific. In 1859, he brought this idea to the attention of the world in his best-selling book, On the Origin of Species. Natural selection is the process through which populations of living organisms adapt and change. Individuals in a population are naturally variable, meaning that they are all genetically different in some ways. This variation means that some individuals have traits better suited to the environment than others. Individuals with adaptive traits — traits that give them some advantage — are more likely to survive and reproduce. These individuals then pass the heritable traits on to their offspring. Over time, these advantageous traits become more common in the population and transmitted through generations. This process happens over many years and multiple generations. It is an ongoing process that leads to small changes throughout all species throughout several years. It can also lead to speciation, where one species gives rise to a new and distinctly different species; this is a process that drives evolution and helps to explain the diversity of life on Earth. Darwin chose the name natural selection to contrast with “artificial selection,” or selective breeding that is controlled by humans. He pointed to the pastime of pigeon breeding, a popular hobby in his day, as an example of artificial selection. By choosing which pigeons mated with others, hobbyists created distinct pigeon breeds, with fancy feathers or acrobatic flight, that were different from wild pigeons. He
explained that a process much like artificial selection happened in nature, without any human intervention and claimed that natural selection explained how a wide variety of life forms developed over time from a singular common ancestor. Before this theory was brought to light, scientists were under the impression that uniformitarianism (the idea that Earth has always changed in uniform ways and that the present is the key to the past) was the key to how evolution occurred. Several other theories had been discredited by whichever scientist had a more accurate and provable theory. The theory of uniformitarianism was what brought Charles Darwin to his conclusion of natural selection. Through the discovery of Darwin’s theory, scientists were able to better understand how species were able to evolve and become more suited to their environments over time, and light was shed on new leads for understanding humankind. After his theory was deemed to be true, scientists only then discovered DNA three years after. Several advances came about after Darwin proved his theory. Without the discovery of natural selection, these advances may not have been possible. An example of natural selection could be the distinction between polar bears and black bears. Although they are both from the same genetic make, they share very different heritable traits that make them suited for their environments. Polar bears are well adapted to the cold environments of Antarctica and do not fare well if they are placed somewhere that differs in temperature. A black bear, however, generally lives in warmer areas that experience four distinct seasons and hibernates during the winter months. A black bear could not survive if it was placed in an area that was cold year-round because it’s heritable traits are not designed
29
DR DOLPHIN
SPRING 2021
for that environment. This is an example of how one in the same population has branched off through the process of evolution and has become more adapted to the environments they are in, causing a new variation of species to be formed. Although natural selection is one of the main driving forces of evolution, there are a few others that play a part as well. These factors are mutation, genetic drift, and gene flow. Mutations are changes in DNA that form genes. The mutation of genes is an important source of genetic variation within a population. Mutations can be random (for example, when replicating cells make an error while copying DNA), or happen as a result of exposure to something in the environment, like harmful chemicals or radiation. Mutations can be harmful, neutral, or sometimes helpful, resulting in a new, advantageous trait. When mutations occur in gametes, they can be passed onto offspring but they are one of the less common occurrences to happen in evolution. The previously mentioned example of polar bears and black bears is proof of genetic mutation. The most distinctive difference is the colour between the two: polar bears are white while black bears are black and other types of bears can be brown. Genetic drift is where certain advantageous traits do not carry on to the next generation and essentially die out. Gene flow is where certain heritable traits are shared between more than one variation of the same species. This process can lead to big changes fairly quick, unlike natural selection where changes occur at a slow prolonged pace. Once again, the example of polar bears and black bears could serve as a model for gene flow. They both share the same heritable traits of hunting, a trait needed to survive in both variations and environments. If the environment changes rapidly, some species may not be able to adapt fast
enough through natural selection. Through studying the fossil record, we know that many of the organisms that once lived on Earth are now extinct. An invasive species, a disease organism, a catastrophic environmental change, or a highly successful predator can all contribute to the extinction of species. Today, human actions such as overhunting and the destruction of habitats are the main cause of extinctions and seem to be occurring at a much faster rate today than they did in the past. Despite the wealth of evidence from the fossil record, genetics and other fields of science, some people argue that evolution altogether is false. But all this information continues to support its validity and humans are one of the best manifestations of this theory. We have evolved into a very intelligent and intellectual population, who started as quite the opposite. Fossil "links" have also been found to support human evolution. In early 2018, a fossilized jaw and teeth found that are estimated to be up to 194,000 years old, making them at least 50,000 years older than modern human fossils previously found outside Africa. Through the process of natural selection, we have thrived and became an incredible population of many varieties. Evolution is happening all around us every day in every part of the world. Darwin was discredited for a long time even after he was dead by those who believed evolution was false and that God was the only factor behind the variations in species and how they change. Some now believe that God is the creator, and still, accept that natural selection plays a hand in the differentiation of species. Charles Darwin was not the founder of evolution, but he did play a role in finding out how evolution occurs and what the
30
DR DOLPHIN
SPRING 2021
driving factors behind it were. If his theory had not been formed, how far would our knowledge of evolution have come? Maybe everyone would still believe in creationism or that uniformitarianism was the only process behind evolution. We have come a
long way since those theories were first introduced, and we continue to move forward daily with advances in the topic. Juliette Desbiez LVI
References
World Transformation Movement. (1998). ‘Natural Selection’ allowed the human condition to be explained. Retrieved from https://www.humancondition.com/fre edom-expanded-book1-natural-Sele ction/?ref=adgrants-search_biology& gclid=Cj0KCQjwov3nBRDFARIsANg sdoFRSuRTAHPOog_ghwVtuH_8t2 XOqKJq720ZPdulkQJOxP0NShnuE AaAginEALw_wcB
All About Science, (2002). Darwin’s Theory of Evolution. Retrieved from https://www.darwins-theory-of-evolut ion.com/ Doc, T. (2015, November 24). Home. Retrieved from https://www.famousscientists.org/ev olution-theories-before-darwin/ Live Science Staff, (2007, August 15). Forces of Evolution. Retrieved from https://www.google.com/amp/s/amp.l ivescience.com/1796-forces-evolutio n.html
31
DR DOLPHIN
SPRING 2021
Key Concepts Why do we have Different Blood Types? If you’re in an accident and a panicked bystander asks you your type, here’s why you don’t respond with tall, dark-haired and charismatic. Much like your potential significant other, there’s a few options to choose from: A, B, AB and O. Why does this occur? Red blood cells, like all cells (except white blood cells), have small globular proteins on their surface called antigens. These antigens act as markers to white blood cells, which have antibodies on their surface, to tell them that they are not pathogenic so that your white blood cells don’t attack them. This works because each antigen has its own complementary antibody. If a pathogen does enter the body, a white blood cell with the matching antigen binding site will come along and recognise it as a foreign threat and alert the white blood cells to destroy it. People have different antigens depending on their genetic makeup and these types can be categorized into the blood types mentioned above. An Austrian doctor, Karl Landsteiner, identified the most common blood antigens in 1901, which he called A and B. He also found that some people had neither antigen (type O), and in 1902 two of his students discovered that some people have both antigens (type AB). Blood can also be classified using the Rhesus system, or Rh for short. Funnily enough, it was named after the rhesus monkey in which it was first discovered. In this system, if a person has RhD antigens on the surface of their red blood cells, they
are Rh positive, if they don’t, they’re Rh negative. In Australia, around 83% of people are Rh positive. The two systems are usually combined in order to achieve maximum precision, giving us 8 possible blood types. As a result, it is vital that blood transfusions occur between people of the same blood type. If not, the recipient’s antibodies will detect an impostor in the new blood’s different antigens and alert the white blood cells to attack in a process called haemolysis (when the red blood cells are destroyed). As the body wages an internal civil war, the patient may experience a dangerously high fever, blood in the urine, and kidney failure. Not fun. Luckily, nowadays, blood is meticulously screened before being administered to patients to avoid rejection; not only does it put the patient at risk, it’s a waste of a precious donation. One difference between the Rhesus system and the ABO group system is that Rh negative people don’t usually possess antibodies against RhD (unless they have been previously exposed to it), whereas in the ABO group system if the antigen is absent from the red blood cell, the antibody against it is present in the plasma. Testing to see if you’re Rh positive or negative is routinely done during pregnancy, blood donation and before a blood transfusion. If a mother is Rh negative but her baby is Rh positive (which can happen if the father is Rh positive), the mother could produce antibodies that fight the baby’s red blood cells. This can happen if blood from the unborn baby enters the mother’s circulation. When there is a risk of this happening an injection called anti-D can be given to the
32
DR DOLPHIN
SPRING 2021
mother to help prevent these antibodies against Rh positive blood being produced. As you can see, your blood is far more complicated than a simple red liquid and you should probably make sure you know your type. Blood type, that is. Roxanna Fahid LVI References: https://www.sciencefocus.com/the-human-b ody/why-do-we-have-different-blood-types/ https://www.ncbi.nlm.nih.gov/books/NBK268 84/#:~:text=Each%20B%20cell%20produce s%20a,and%20antibody%2Dsecreting%20e ffector%20cell. https://medlineplus.gov/ency/article/001303. htm#:~:text=A%20hemolytic%20transfusion %20reaction%20is,the%20process%20is%2 0called%20hemolysis. https://www.mydr.com.au/tests-investigation s/blood-typing#:~:text=The%20rhesus%20( Rh)%20system,be%20Rhesus%20positive %20(Rh%2B).
33
DR DOLPHIN
SPRING 2021
The Neuroscience Behind PTSD The brain is composed of 3 main parts the cerebrum, the cerebellum and the brainstem. The cerebrum is the largest part of the brain, consisting of the two main hemispheres. It is responsible for body functions such as movement, the 5 main senses (touching, seeing, hearing, tasting and smelling), speech and emotions. The cerebellum is the smaller bulb-shaped part of the brain located directly under the cerebrum. It is responsible for body coordination, general muscle movement and balance. The brainstem runs from the cerebrum, through to the cerebellum and connects them into the spinal cord. It performs automatic responses such as sneezing, regulating body temperature, regulating the sleep cycle and digestion. Post traumatic stress disorder is defined as an anxiety disorder caused by very stressful, frightening or distressing events. Like all psychological disorders, the trauma which causes PTSD, has significant effects on brain structures and their functions. Where your body is experiencing trauma, the amygdala (located in the cerebrum) initiates an immediate, automatic response which alerts the body to be prepared to brace a threat. As a result, the hypothalamus (which detects this response) releases the stress hormone, cortisol, which keeps the body hypervigilant and alert. Eventually, when the prefrontal cortex (also in the cerebrum) has realised that the threat is no longer dangerous, it helps the body to calm down and return to its normal state.
However, if someone experiences too much trauma over a period of time or a highly traumatic experience in a very short period of time, the amygdala can be overactivated and therefore too many stress hormones are being released and the prefrontal cortex cannot settle the body fast enough. This is why one of the main symptoms of PTSD is being constantly stressed, hypervigilant or excessively on edge. Moreover, the hippocampus (located in the cerebrum) is also significantly impacted by trauma. It is responsible for memory processes, and when it is overworked (from extreme trauma experiences) it can also essentially “malfunction” resulting in memory loss, memory flashbacks and repetitive memories of the event- all more common symptoms of PTSD. On a molecular level, the molecule glutamate is a chemical messenger of brain signals between nerve cells and normally, it is responsible for sending nerve signals as well as playing a key role in memory. A study recently done by NCPTSD, a Yale psychologist and PET scanner Irina Esterlis showed that patients with PTSD had a significantly higher amount of glutamate (specifically mGluR5) being released in their brain than usual. As tested on animals, an increase in mGluR5 caused fear and stress-related behaviours, demonstrating another reason as to why people with PTSD share some of these behaviours. The PET scan image here shows the difference
34
DR DOLPHIN
SPRING 2021
between a normal patient and a patient with PTSD- specifically the difference in amount of mGluR5 present in their brains. It is interesting to note that similar amounts of glutamate has also been found in people suffering from Huntington’s disease: a genetic, neurological disease
with similar symptoms such as memory lapses and increased aggressive/irritable behaviour. Aya Kodmani LVI
References: https://www.nhs.uk/conditions/post-tra umatic-stress-disorder-ptsd/ http://www.mayfieldclinic.com/pe-anatb rain.htm https://www.verywellmind.com/wh at-exactly-does-ptsd-do-to-the-brai n-2797210
https://news.yale.edu/2017/07/17/ new-ptsd-study-identifies-potential -path-treatment https://hopes.stanford.edu/about-gl utamate-toxicity/
35
DR DOLPHIN
SPRING 2021
The Truths to Obesity
your brain.
Many of us think we are in control of what we eat, and this coupled with how we keep active dictates our shape and size. With the proliferation of exercise videos and meal plans for “all shapes and sizes”, a belief that obesity is a personal choice has been established. Millions of people, especially children, are bullied daily due to their weight and size . But what if they are not in control? What if our universal belief towards obesity is incorrect ?
Let the cavemen eat cake….
Reaching for that serotonin sweet spot As you may have noticed, we have the tendency to eat a lot when we feel emotional. There are times when we are sad or depressed and this can lead to emotional eating-- eating more than the required calories you would need in a day. In a fast paced life, people tend to feel isolated and that's when they find solace in food and primarily junk food. According to an American Medical Association study, researchers have found a connection between eating chocolate and being depressed. It is said that cocoa raises the level of serotonin, a neurotransmitter that produces feelings of happiness. But what is it that triggers the brain to reach out to high-fat foods despite knowing the fact that they may harm you in the long run? Many people turn to sugary and high-fat foods to comfort themselves. According to a study published in the Nature Neuroscience, eating such foods triggers the release of dopamine, another “feel-good” neurotransmitter in the brain. So, the more such foods you eat, the brain starts getting addicted to them, making you crave for more. It becomes a cycle and a trap for
Our crave for calorific food is biological, developed through evolution. When we were cavemen we never knew when we would eat again and famine was a constant threat. Therefore even when we had eaten a full meal, fearing hunger, our brain signalled that we were still hungry and that we wanted to eat more. In modern times, this has evolved into the concept of ‘dessert tummy’-- after a meal your body starts to crave food that is higher in calories as your body wants to store up in fat for the future. For example, grizzly bears after eating a full meal of fish, will have “dessert” by just eating the skin, as this has the highest fat and calories. The concept of ‘dessert tummy’ has been conserved through evolution and throughout the animal kingdom. This self preservation now has led to weight gain. But if everybody is preparing themselves for ‘famine’ then why isn’t everyone overweight? While self preservation and fear of starvation has developed an evolutionary tendency towards calorie hoarding, there has never been a historic abundance of food, and therefore we all have different responses to too much food. My leptin’s broken….
Scientists discovered Leptin, a hormone that regulates your energy, including the number of calories you eat and expend, as well as how much fat you store in your body . The leptin system has evolved to keep humans from starving or overeating. Today, leptin is very effective at keeping us from starving. But there is something wrong with the mechanism that is supposed to prevent
36
DR DOLPHIN
SPRING 2021
us from overeating. In 1994 researchers found that the cause of obesity was in fact a mutation in this hormone. Leptin is produced by your body’s fat cells. The more body fat cells, the more leptin is produced. Leptin is carried by the bloodstream into your brain, where it sends a signal to the hypothalamus — the part that controls when and how much you eat. The fat cells use leptin to tell your brain how much body fat they carry. High levels of leptin tell your brain that you have plenty of fat stored, while low levels tell your brain that fat stores are low and that you need to eat. When you eat, your body fat goes up, leading your leptin levels to go up. Thus, you eat less and burn more. Conversely, when you don’t eat, your body fat goes down, leading your leptin levels to drop. At that point, you eat more and burn less. So how does it cause obesity? People who are obese have a lot of body fat and therefore very high levels of leptin, which should in theory cause them to naturally limit their food intake. In other words, their brains should know that they have plenty of energy stored. However, scientists discovered that leptin signals in obese patients often do not work. While leptin may be present, the brain doesn’t see it .This condition is known as leptin resistance and it is now believed to be one of the main biological contributors to obesity. To understand what was really going on, an experiment was done with obese children who had a mutation in their leptin hormone . This experiment included a variety of three year olds and a 3000 calorie breakfast. Most 3 year olds as you would expect, had
one bite of toast whereas the children with the mutation were able to eat a lot more .This proved to scientists how this mutation can severely affect children today as not only was the quantity of food higher but they also had a preferred taste for fat. Interestingly, this same mutation causes food motivation in dogs as well. You probably know of Labradors, the familyfriendly dogs that are highly food motivated. Eighty percent of all Labradors have a similar leptin mutation which makes the dog very food motivated and consequently, why they are great guide dogs. Although we can see there are biological and evolutionary factors which can lead to obesity, doctors would highlight the importance of personal responsibility for your own health . There are always ways to improve your condition, whether going on a brisk walk everyday, planning a low calorie diet or joining a weight loss group, small actions like these can significantly and rapidly increase your health and reduce the risk of obesity. Specialists would argue the most important step in preventing obesity is understanding your health situation and actively seeking help to improve . We can see that there are genetic and biological reasons why people tend to be obese . The fast food, fast paced society we live in makes it even harder . People who find themselves here are already fighting a tough battle, and this is why it is important to realise and understand that obesity is not a personal choice. However this does not mean their situations cannot be improved. While genetics predispose a person to major challenges, learning about healthy diet, exercise and emotional support can help people regain control of their body and mind. Riya Nathan Year 11
37
DR DOLPHIN
SPRING 2021
Flower “I chose to paint it because I like using nature as the inspiration for my artwork, mainly individual plants and animals, as I like the idea of being able to preserve living things in their most vibrant state; the flower in the painting will continue to look as it does in full bloom, while the real flower will wither. This emphasises the idea of the cycle of life, reminding us that all living organisms die, contrasting starkly with objects, which remain unchanged.”
Isabella Davidson LVI
38
DR DOLPHIN
SPRING 2021
Wordsearch
39