C.R.U. Malawi crisis response unit

Addressing the Road Traffic Fatality Rate in Malawi
by Hardi Shah
project Title: crisis response unit - c.r.u. malawi
by hardi shah
Project presented to the Faculty of the Department of Architecture College of Architecture and the Built Environment, Thomas Jefferson University
In partial fulfillment of the requirements for the degree of BACHELOR OF ARCHITECTURE
Arch-508 / Design 10: Research and Design Faculty
Associate Professor Chris Harnish
Philadelphia, Pennsylvania
May 2019
table of contents
abstract & research question thesis statement & intentions research & design methods research findings & conclusions design proposal : crisis response unit : c.r.u. design findings & conclusions design proposal development reflection assessment works cited bibliography 06 08 12 20 22 26 48 76 78 80
benefits of strategy 4
AMBULANCE TRAILER CARETENT
AMBULANCE TRAILER CARETENT
THE AMBULANCE IS ITS OWN ENTITY.
THE CARE TENT & TRAILER ARE ONE ENTITY. This allows the ambulance to leave with a critical patient while the emts handle other victims with minor injuries.
Simple triage and Rapid Treatment
Also known as (S.T.A.R.T). This is a method used by rescuers , EMS and first responders to efficiently evaluate and categorize all of the victims during a multiple casualty event. The method was developed in 1983 by the staff members of the Newport Beach
Fire Department located at Hoag Memorial Hospital in Newport Beach, CA.
The first medical personnel arriving at a mass casualty incident will use a triage tag to categorize the victims by the severity of their injury, in some cases the will move victims to areas noted by triage tarps.
FOUR TRIAGE CATEGORIES
MINOR
DELAYED CARE / CAN DELAY UP TO THREE HOURS
DELAYED
URGENT CARE / CAN DELAY UP TO ONE HOUR
IMMEDIATE
IMMEDIATE CARE / LIFE-THREATENING
DECEASED
VICTIM IS DEAD OR MORTALLY WOUNDED / NO CARE REQUIRED
To ensure clear understanding and organization for the victims at a chaotic scene, the tent should be able to organize the scene in terms of the colors of the triage tags that are given to victims according to the S.T.A.R.T. method.
46
“First Aid Product™.” First Aid Product: Wholesale Direct to the Public! Why Pay Retail?™. Accessed March 05, 2019. https://first-aid-product.com/disaster-survival/triage-supplies-s-t-a-r-t-triage-kits.html. “BP Medical Supplies.” Accessed March 05, 2019. https://www.bpmedicalsupplies.com/products/Disaster-Relief-MCI/Triage-Supplies/. findings
program needs for s.t.a.r.t. phases
The immediate category according to the S.T.A.R.T. system requires emergent attention and must be transported to the healthcare facility before treatment is given to anyone else in the other categories. This means that square footage and beds that are accounted for the immediate category will be transferrable to the delayed category upon the immediate’s transfer to the hospital.
The minor category is for individuals who can still walk and so they may be able to assist the EMTs recover patients from the crash. Due to time purposes in Malawi, we will address the deceased only after the injured are treated.
47
“First Aid Product™.” First Aid Product: Wholesale Direct to the Public! Why Pay Retail?™. Accessed March 05, 2019. https://first-aid-product.com/disaster-survival/triage-supplies-s-t-a-r-t-triage-kits.html. “Mass Casualty, START Triage and the SMART Tag System.” Lecture, Boston, March 06, 2019. Accessed March 6, 2019. https://www.blessinghealth.org/sites/default/files/users/user15/EMS_START_Triage_SMART_Tags_2017.pdf. 36 SQFT 250 SQFT 180 SQFT 160 SQFT 0 SQFT 2-4 critical patients @ 30sqft per patient (including 4 beds) 1-2 EMTs @ 20sqft per EMT 2-6 very low risk patients @ 6sqft per patient (sitting room) 12-14 low risk patients @ 8sqft per patient (sitting room) ; 2 beds @ 18sqft per bed 1-2 EMTs @ 20sqft per EMT
findings
MINOR CIRCULATION DELAYED IMMEDIATE DECEASED
program studies: adjacency analysis
The programmatic adjacencies in these diagrams were assigned to study possible variations of the mobile facility. The delayed and immediate categories are most emergent in a triage system and so must be given highest priority.
Studying variations of the programmatic adjacencies, it is clear that another set of criteria must be developed to analyze the positive and negative outcomes of each.
48
2 4 IMMEDIATE MINOR DECEASED SUPPLIES DELAYED IMMEDIATE MINOR DECEASED SUPPLIES DELAYED IMMEDIATE MINOR DECEASED SUPPLIES DELAYED MINOR DECEASED SUPPLIES DELAYED IMMEDIATE “First Aid Product™.” First Aid Product: Wholesale Direct to the Public! Why Pay Retail?™. Accessed March 05, 2019. https://first-aid-product.com/disaster-survival/triage-supplies-s-t-a-r-t-triage-kits.html. “Mass Casualty, START Triage and the SMART Tag System.” Lecture, Boston, March 06, 2019. Accessed March 6, 2019. https://www.blessinghealth.org/sites/default/files/users/user15/EMS_START_Triage_SMART_Tags_2017.pdf. case studies
1 3
crisis response unit criteria
As the tent is developed, it is critical to set up criteria which can be used to assess the success or failure of the proposed solution.
However, we must also accept that not all of the criteria might be able to be incorporated into a solution. The challenge of this proposal lies in the question of compromise.
49
“First Aid Product™.” First Aid Product: Wholesale Direct to the Public! Why Pay Retail?™. Accessed March 05, 2019. https://first-aid-product.com/disaster-survival/triage-supplies-s-t-a-r-t-triage-kits. html. “BP Medical Supplies.” Accessed March 05, 2019. https://www.bpmedicalsupplies.com/products/Disaster-Relief-MCI/Triage-Supplies/. 00 rate of assembly repetitive deployment triage adjacencies & prioritization required manpower Simple triage and Rapid Treatment compaction ability weight of overall structure appropriate lighting affordable materiality clear signage for triage waterproof materials storage room for supplies provides sunshading utility connections square footage storage & energy capability volume of stored structure weight of tent structure type of internal space flexibility of vehicles DEPLOYMENTCRITERIA STRUCTURALCRITERIA PROGRAMMATICCRITERIA MINOR DELAYED IMMEDIATE conclusions
proposal
driver & emt timelines on-site
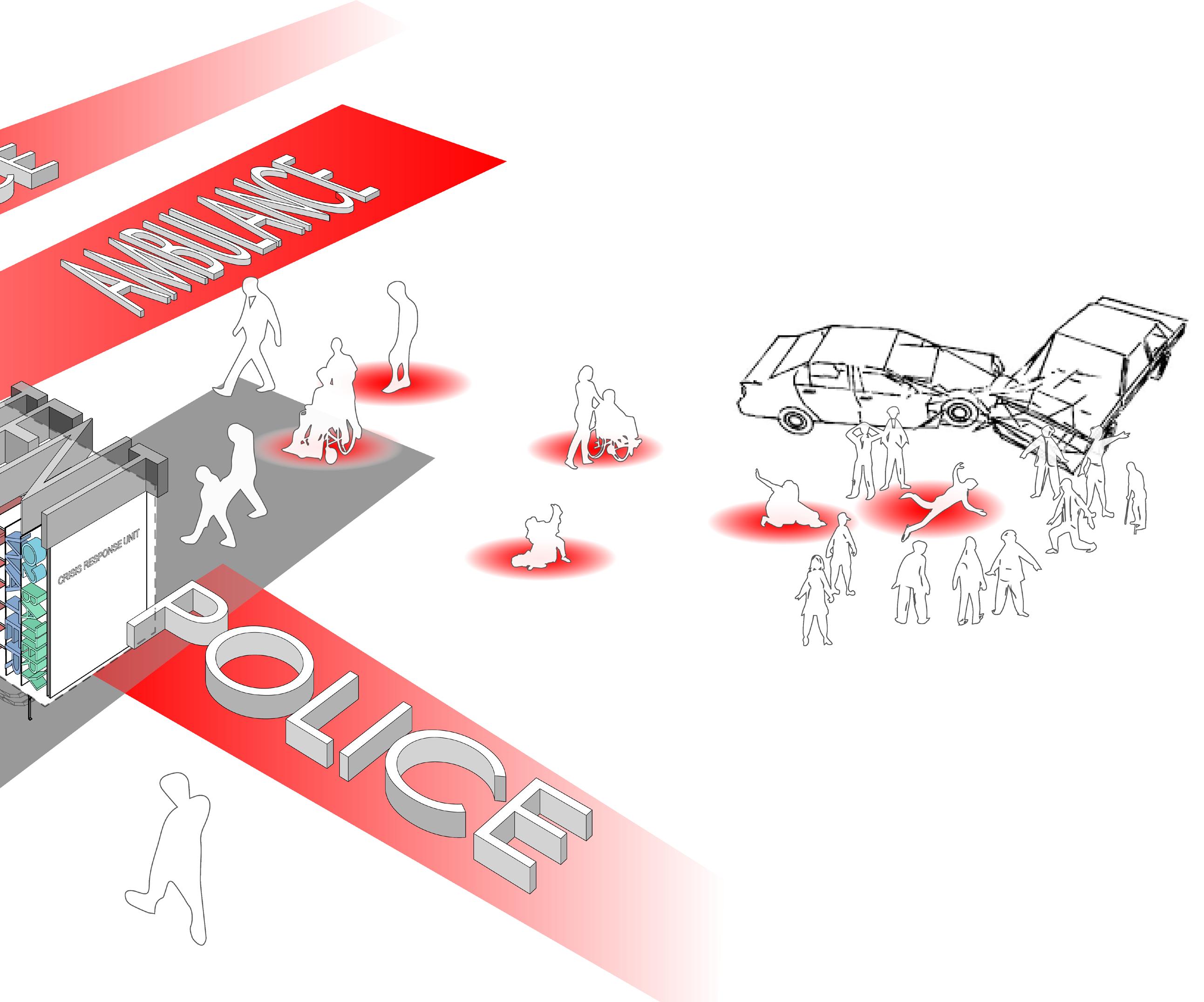
The crash-site is a chaotic situation within which the triage, treatment, and emergency services must be provided simultaneously. This requires some type of organization or delagation of tasks to occur on site. The timeline is an example of how roles can be taken and distributed between the driver, the EMTs, and the low-risk victims.
While EMTs provide essential medical services, the driver can take over tasks such as tent deployment and setup. Low-risk victims may also be able to provide some organization by directing high-risk victims to the tent.
50
51 “Mass Casualty, START Triage and the SMART Tag System.” Lecture, Boston, March 06, 2019. Accessed March 6, 2019. https://www.blessinghealth.org/sites/default/files/users/user15/EMS_ START_Triage_SMART_Tags_2017.pdf.
prefab & shipping strategy
ONE OF THE GOALS FOR THIS PROJECT WAS TO CREATE A PREFABRICATED, SHIPPABLE DESIGN.
2 C.R.U.s
ALL COMPONENTS OF A 2-UNIT SET WOULD BE ABLE TO FIT INSIDE A
45’ LONG SHIPPING CONTAINER.
structure supplies tent fabric supplementary
52
2 C.R.U.s with the detached tent modules fit into a shipping container
findings
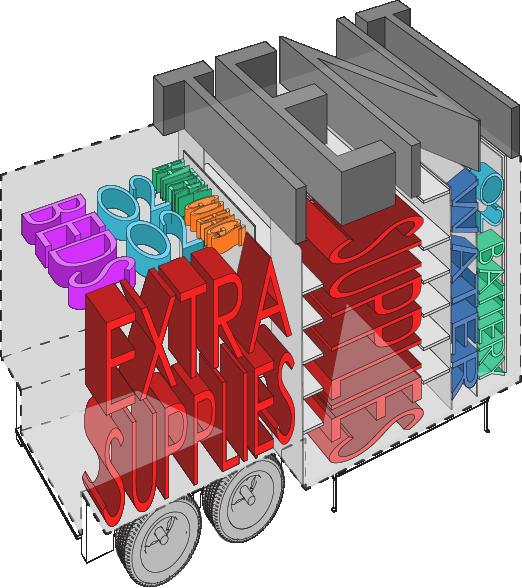
foldable stretchers
portable oxygen, batteries, extra firstaid supplies
EMS go-bags supplies for: minor treatments burns, sutures, & fractures
oxygen connection
electric connection
crisis response unit -c.r.u contents
water connection
The C.R.U. is divided into two phases: the treatment zone & the storage zone
The deployable tent is located on top of the treatment zone of the C.R.U.
The electric, oxygen, and water connections are located towards the front of the trailer over the hitch to ensure the most stability and safety.
53
proposal
c.r.u. exploded axon features
Based on multiple conditions that the system could encounter, various features were included in the C.R.U.
Things such as a fabric which allows some light transmission but definitively stops rain and a light system along the top of the C.R.U. for night-time emergencies are included.
PVC fabric allows for pliability, durability, and wide temperature and humidity conditions
3’ walkable space with doors at both ends
structural corner joints are fabricated using shipping container modules
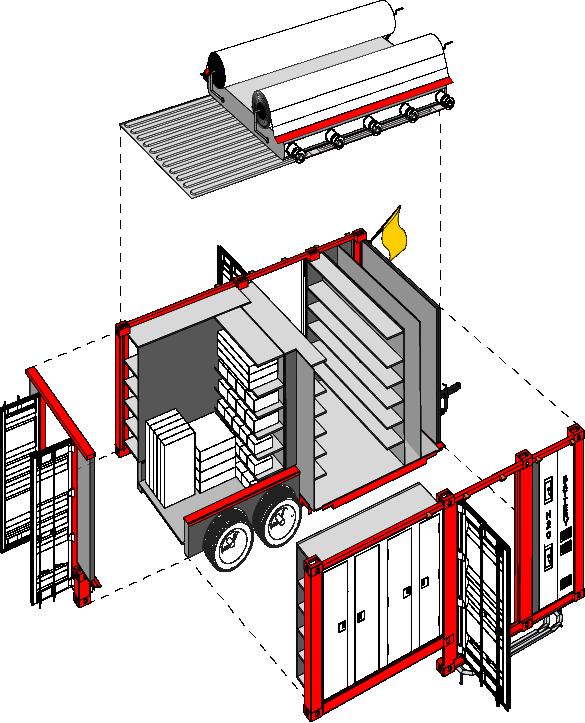
lever to crank fabric back into a roll rod connecting telescopic members for easy deployment
flag signifies triage category being treated
aluminum metal plate walls to lighten the weight of the trailer
trailer hitch to attach to the vehicle
flood lights provided for nightime usage double doors allow for ease in unloading and reloading
footrails provide steps to the taller trailer
folded stands to allow for stabilization on uneven ground
54
proposal
c.r.u. floor plan
55
O 2 O BATTERY BATTERY HO 2 O 2 2 HO2 O 2 A B 16’ 10’ proposal
proposal
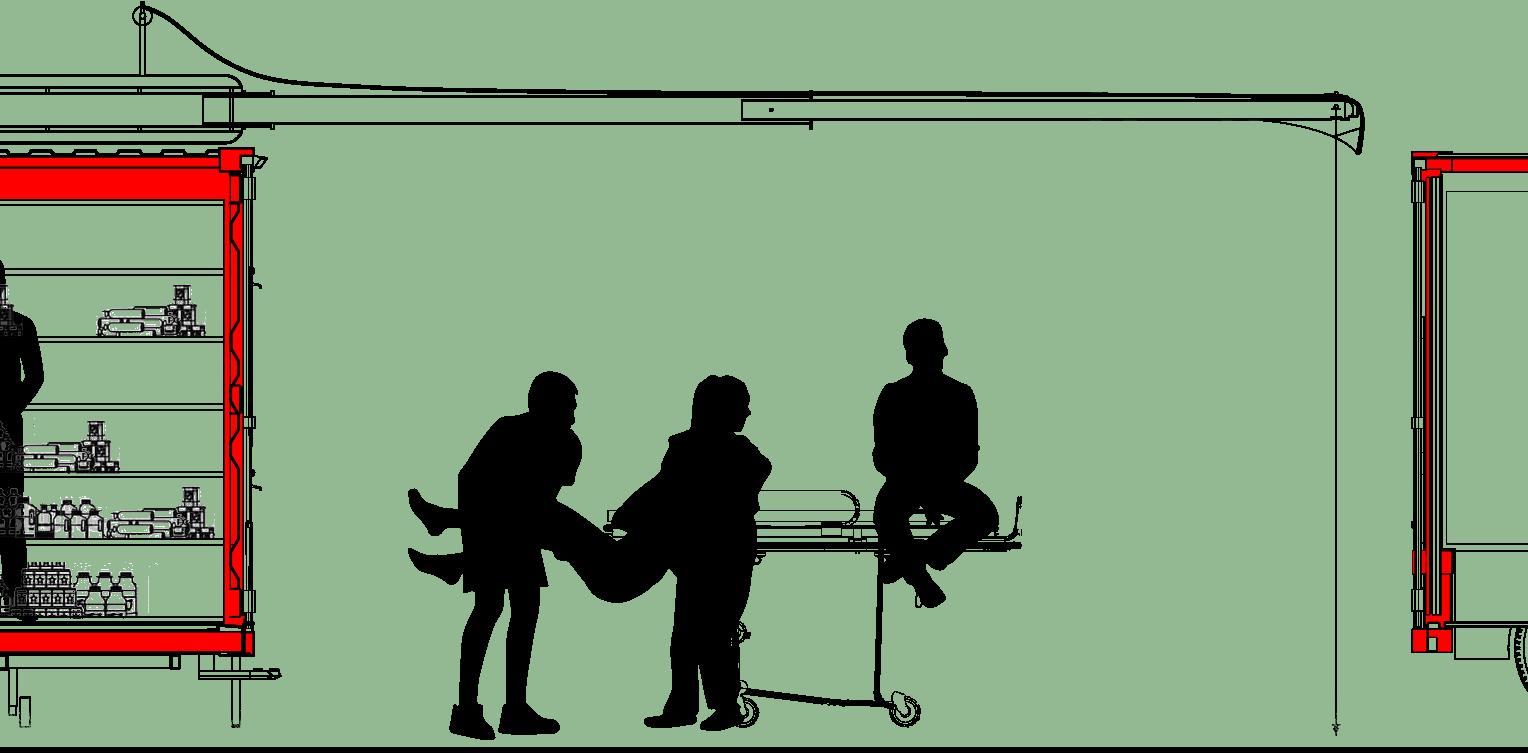
c.r.u. elevation
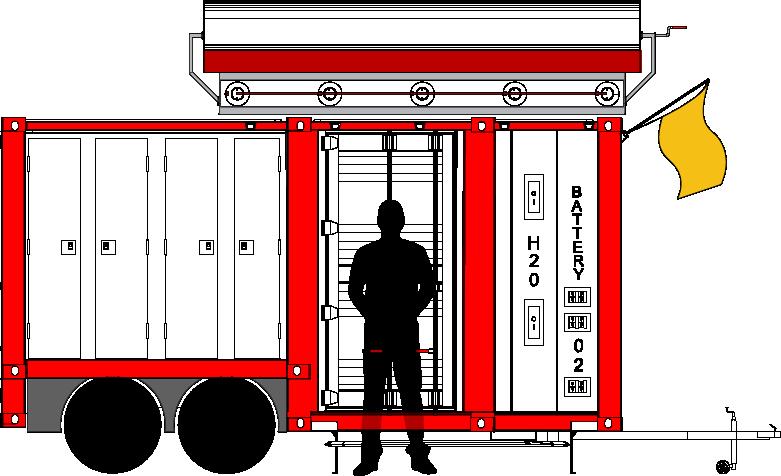
56
proposal
c.r.u. section a
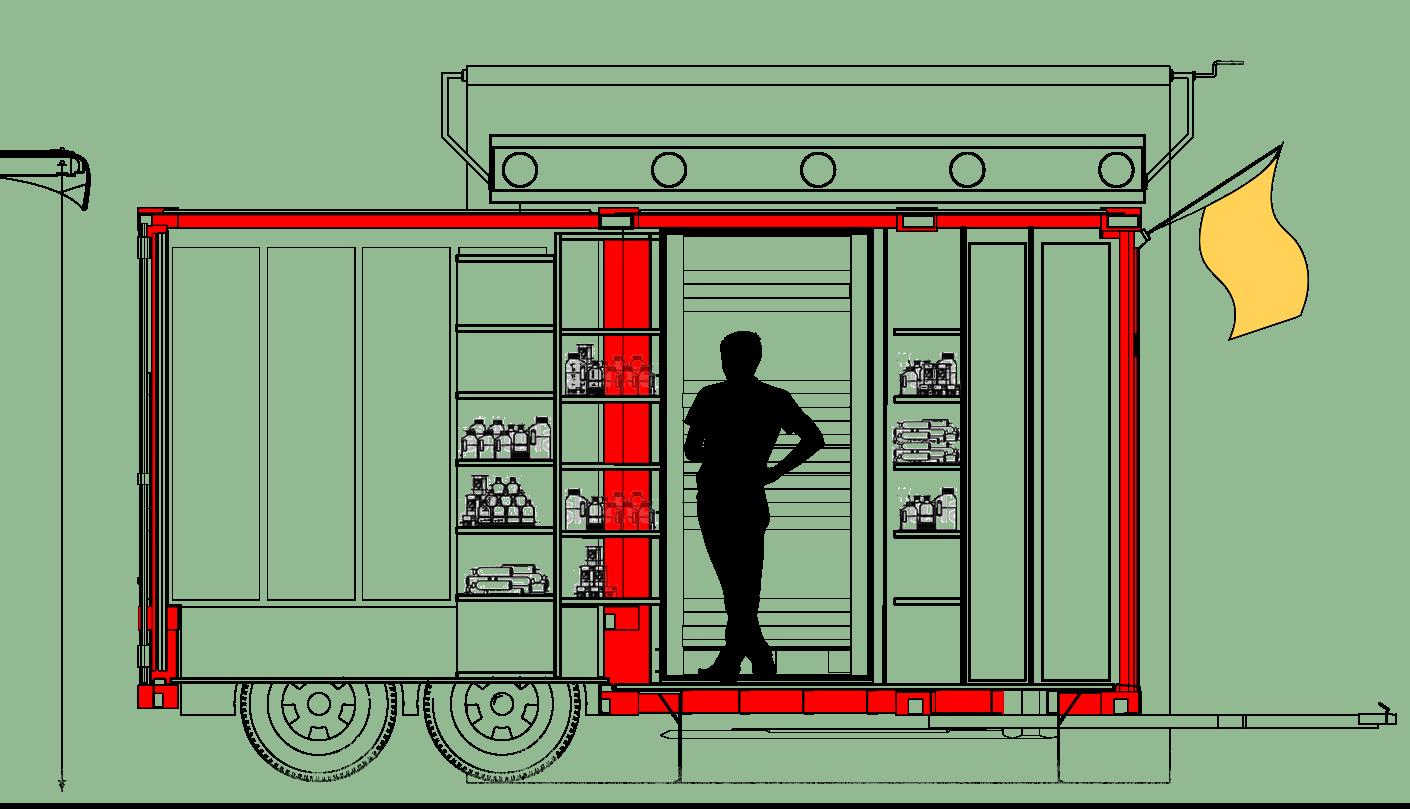
57
O O HO O HO O
proposal
c.r.u. section b
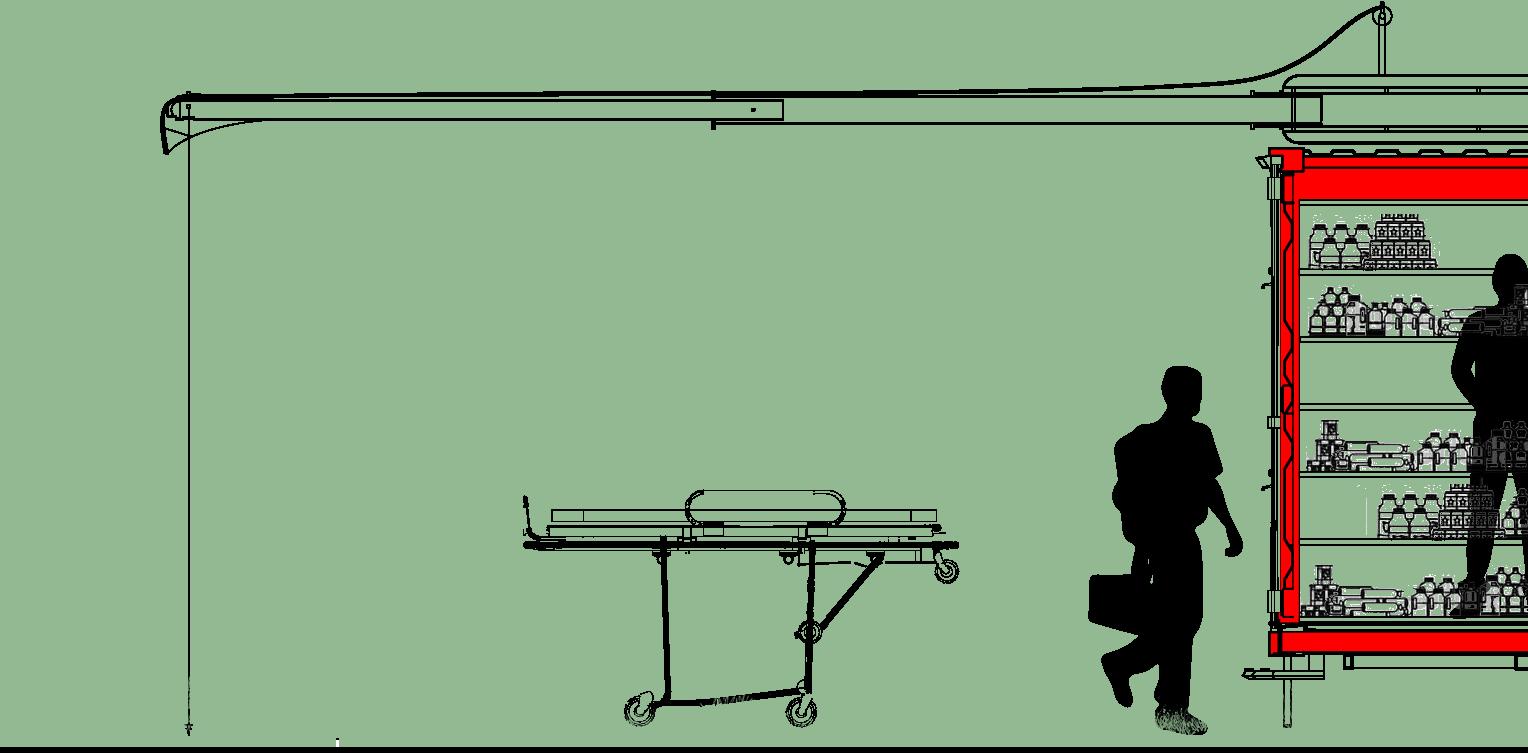
58
59 O O HO O HO O
c.r.u. section b
diagram
WIND UPLIFT
60
load
weight loads torque tension compression
proposal wind
tension
61 weight O O HO O HO O wind
torque tension compression tension
loads
overall system

proposal
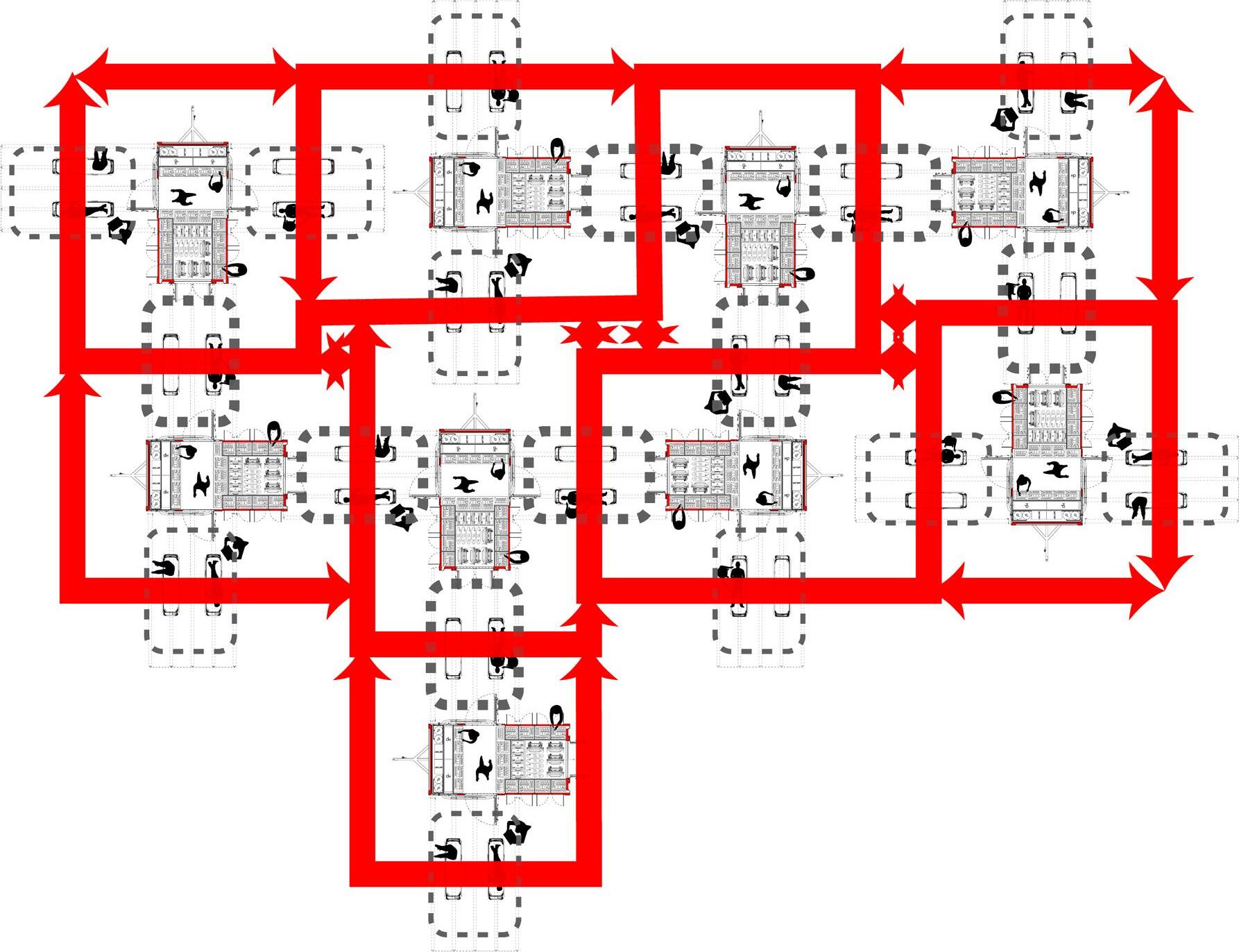
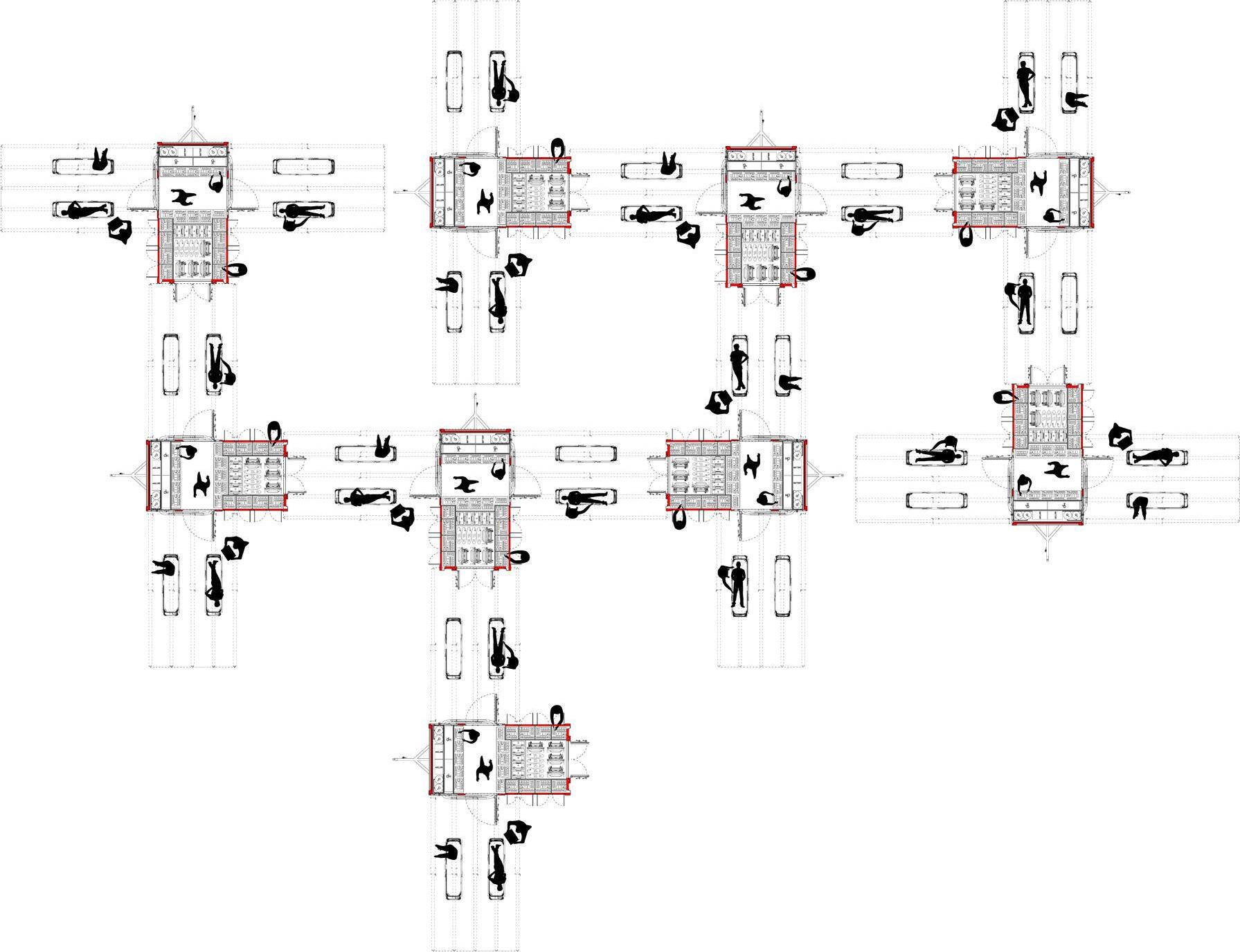
circulation through c.r.u. on-site
The crisis response units are designed to be able to be walked through and create a continuous circulation path on-site.

The deployed tent structure covers the area of treatment directly above the utility connections and supply corridor. The circulation flows through the supply corridor of one C.R.U. to a treatment area in front of the storage space with portable oxygen tanks, batteries, and go-bags.
i.e. the treatment zones are perpendicular to the storage zones creating a space with all available supplies in the perimeter: the critical zone.
64
65
proposal
mass casualty clinic set-up
In event of a much larger mass casualty situation, there is a possibility to organize a layout of the Crisis Response Units such that a makeshift clinic could be created.
C.R.U. System Unit
66
zones created using c.r.u.
The layout of the supply and storage zones determines the types of treatment areas.
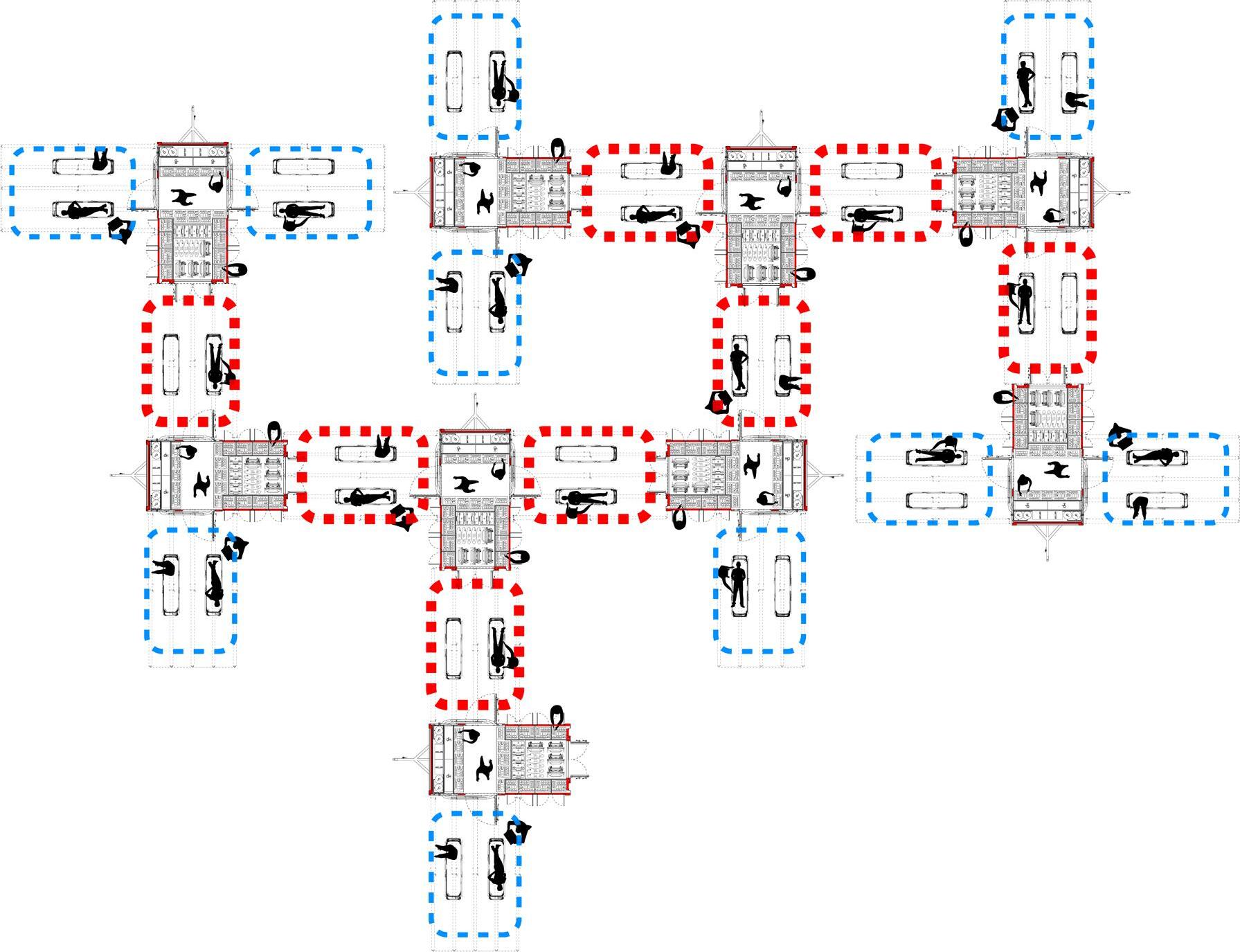
Critical treatment areas, adjacent to every resource available, can be created where the supply and utility zone is located adjacent to the storage zone.
Supply & Utility Zones
Storage Zones
Critical Treatment Zones
Treatment Zones
67
proposal
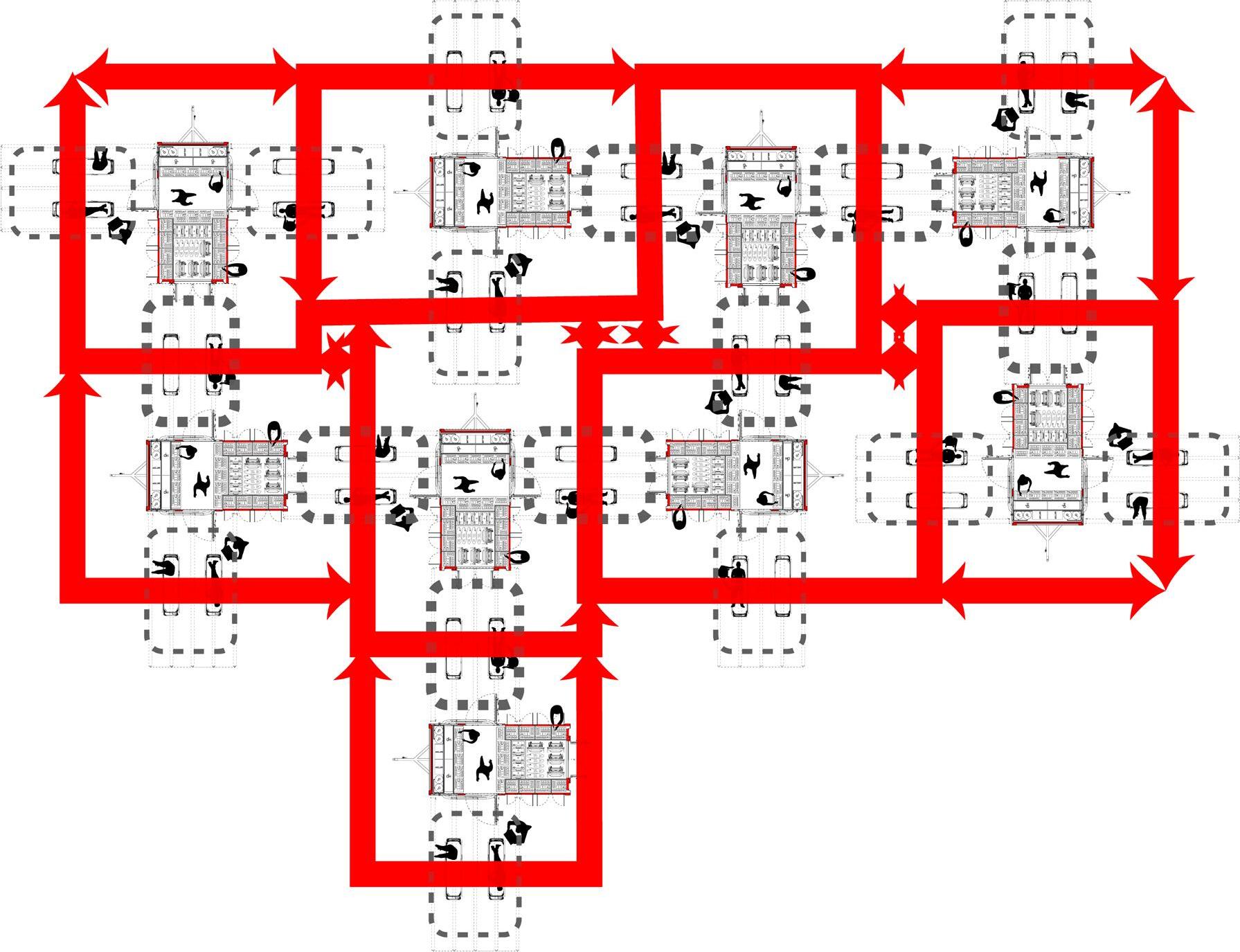
patient circulation within c.r.u.
This creates a grid like organization on an otherwise chaotic site. While patients travel along this grid. The staff can travel along a different grid utilizing the corridors within the unit.
Supply & Utility Zones
Storage Zones
Patient Circulation
68
proposal
proposal
staff circulation within c.r.u.
This creates a grid like organization on an otherwise chaotic site. While patients travel along this grid. The staff can travel along a different grid utilizing the corridors within the unit.
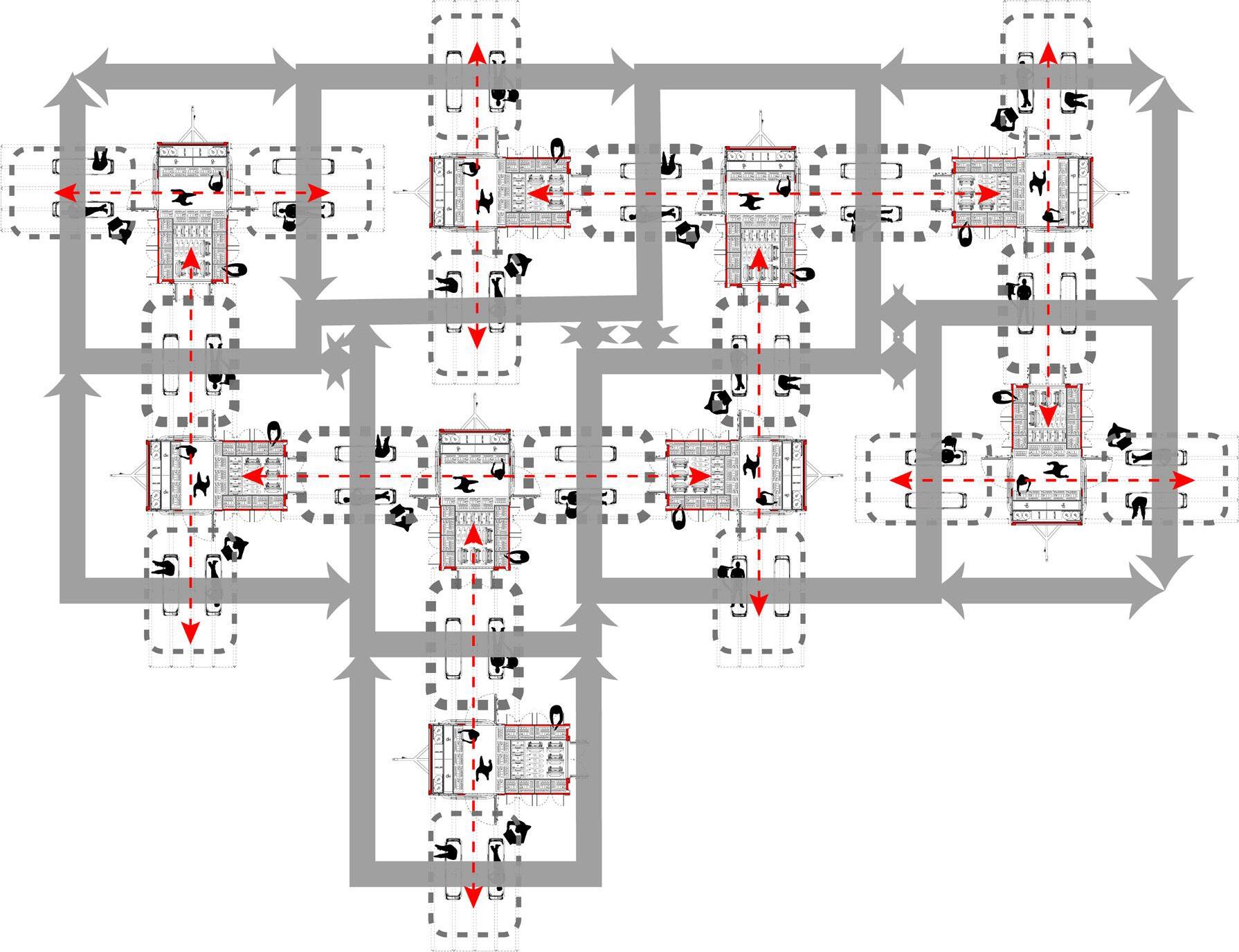
Supply & Utility Zones
Storage Zones
Staff Circulation
Patient Circulation
69








analysis/ critique of completed project
The strengths of this project lie in the research done regarding the manufacturing, deployment, and programmatic criteria. Once a scale was set for the project determined by the possibility to mass produce the Crisis Response Unit and ship it in pairs, it became easier to delve into details of medical program and various uses. Once the overall proportions of the unit were established, the form of the unit was able to be researched in terms of functionality as well as structural stability during transport. The form of the trailer with the tires paired towards the back and the hitch located towards the front was created once the program of the trailer was established. The utilities were located directly above the hitch to ensure the most stability for the most delicate items. The contents and utilities of the unit were key in driving the circulation and connectivity of one unit to another.
The various uses and flexibilities of the Crisis Response Unit could have been documented and expressed better within this project. The usage of this unit could have substituted, in cases of acute emergency and resource deficiency, the need for an ambulance as it can be attached to a vehicle and easily transported. The integration
of the Police and the Ministry of Health could have been developed more broadly within this project. I went forth past that subject because I knew that ambulatory circulation was being developed currently in Malawi. The graphic incorporation of existing infrastructure would have been an excellent addition to this project had I gotten more time. In theory I had created a system wherein the existing police infrastructure could be used to house these C.R.U.s and I also included a timeline in which this is mentioned briefly but I do wish that I had elaborated on that subject.
In terms of peer review and interviews, if I had more time with this project I would love to be able to conduct a survey with medical professionals in the emergency medicine department and test out the system that the Crisis Response Unit creates. Because this project was so user-centric, it would have made all the difference if I could personally sit down with a number of professionals and conduct a survey to gain more insight into the intricacies of on-site emergency care and their immediate needs when treating a patient.
works cited
Branas, C. C., E. J. MacKenzie, and C. S. ReVelle. 2000. A trauma resource allocation model for ambulances and hospitals. Health Services Research 35 (2): 489-507.
“Goal 3: Good Health and Well-being.” UNDP. Accessed February 10, 2019. http://www.undp.org/content/undp/en/home/sustainabledevelopment-goals/goal-3-good-health-and-well-being.html#targets.
Harrison, Hooi-Ling, Nigel Raghunath, and Michele Twomey. 2012. Emergency triage, assessment and treatment at a district hospital in malawi. Emergency Medicine Journal : EMJ 29 (11): 924-5.
HDT Global. Accessed February 27, 2019. http://www.hdtglobal. com/series/medical-mergency-operations/.
Lynn, Mauricio. “Hospital Planning and Response to Sudden Mass Casualty Incidents.” Mass Casualty Incidents, 2016, 25-55. doi:10.1007/978-1-4939-3496-6_3.
“Malawi.” World Health Organization. February 01, 2015. Accessed February 11, 2019. https://www.who.int/gho/countries/mwi/en/.
“Model Comparison Chart.” Demers Ambulances. Accessed February 27, 2019. https://www.demers-ambulances.com/model-comparisonchart/.
Mohammed-Najeeb Mahama, Ernest Kenu, Delia Akosua Bandoh, and Nuhu Zakariah Ahmed. “Emergency Response Time and Pre-Hospital Trauma Survival Rate of the National Ambulance Service, Greater Accra (January – December 2014).” BMC
Emergency Medicine 18, (2018). doi:http://dx.doi.org/10.1186/ s12873-018-0184-3.
“New UN Regulation on Automatic Emergency Call System for Road Traffic Accidents Will Reduce Response Times, Save Lives.” Targeted News Service, Nov 23, 2017.
“Rapid Deployment Shelters For Sale | HTS.” Roder HTS USA. Accessed February 11, 2019. https://www.hts-usa.com/products/rapiddeployment-shelters/.
Rivas-Adrover, Esther. (2015). Deployable Structures.
“Road Traffic Deaths.” World Health Organization. March 11, 2016. Accessed February 12, 2019. https://www.who.int/gho/road_safety/ mortality/en/.
Schlottmann, Francisco et al. “Road traffic collisions in Malawi: Trends and patterns of mortality on scene” Malawi medical journal : the journal of Medical Association of Malawi vol. 29,4 (2017): 301-305.
“SHELTERPOD (RED) Limited Edition.” SHIFTPOD | Advanced Shelter Systems Inc. Accessed February 11, 2019. https://store. advancedsheltersystemsinc.com/responsepod/shelter/shelterpod-r.
Sion, Melanie, MD, and Anthony Charles, MD, MPH, FACS. Central Malawi District Hospital Surgical Capacity Assessment. Report. Department of Surgery, Thomas Jefferson University Hospital.
Tyczynska, Nicole E. Online interview by Hardi Shah. February 06, 2019.
“What Is a Mass Casualty Incident?” Classification of Social Media Platforms. Accessed February 27, 2019. https://delvalle.bphc.org/ mod/wiki/view.php?pageid=89.
https://www.who.int/bulletin/archives/80(11)900.pdf
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
final presentation script
The goal of this project was to analyze and combat the high road traffic accident mortality rate in Malawi with a special focus on mass casualty incidents.
To express the weight of this issue, malawi ranks 1st in Africa in road traffic accident mortality rate at 35 fatalities per 100,00 people. The United Nations recognized this as a global issue and set a sustainable development goal which has not been met.
1/3rd of all injury related deaths are caused due to road traffic accidents and 30% of all accidents result in at least 1 fatality. The cause for this has been identified to be the delay in emergency medical attention, lack of ambulance services, and a shortage of pre-hospital teams. This identifies the main issue to lie in the response system for road traffic accidents.
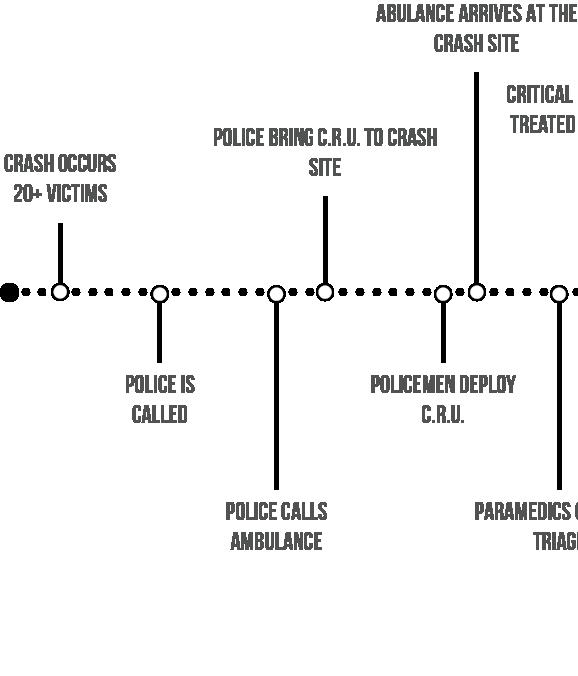
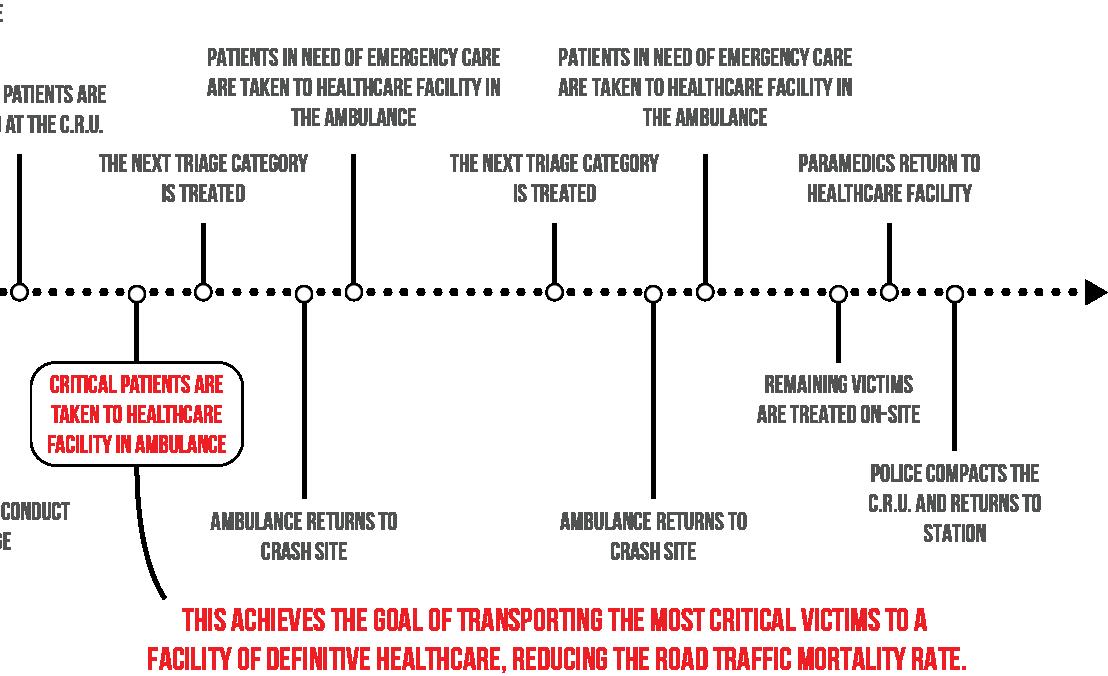
I first looked at the timeline for a typical road traffic accidents and identified the issues in the process in red.
I then looked at the timeline for a mass casualty road traffic accident. A mass casualty is defined as an accident which results in more patients than the local resources are able to handle. In red, I have identified issues that are faced in addition to the ones identified for a typical accident.
As stated before, the main issue lies in the response system for road traffic accidents. This includes the initial triage and urgent care, which is the area of intervention.
This brings me to my thesis question:
Could a deployable prefabricated mobile emergency response unit help reduce the on-site road traffic accident fatality rate?
By enabling the first responders to conduct efficient triage, the medical staff is able to quickly recognize victims in critical condition. These victims could then be transported to a healthcare facility where they will have access to definitive care, while other victims may be treated on site. This will reduce the amount of time that it takes for a critical patient to be recognized and taken to a hospital.
To assist healthcare providers on a chaotic crash site, the crisis response unit, or CRU, will be a deployable emergency unit which will provide a space for the responders to recognize and treat patients.
I studied the three main components of the system: the ambulance, trailer, and tent and established their uses and relationships on the site.
I also established a set of deployment, structural, and programmatic criteria to assess the success or failure of the proposed solution within the context of Malawi.
A goal for this project especially within the context of Malawi, was to be able to design the CRU to be a prefab and efficiently shippable design. A 2-unit set would aim to be fit into a 45 long shipping container.
The timeline of the crash was then reanalyzed as the response system was recreated. After a crash occurs, the police is contacted. As the police race to arrive at the crash-site and deploy the Crisis Response Unit, the ambulance makes it’s way to the crash site. This way, the medical staff is not wasting precious time deploying the tent when they could be triaging
the victims. Once the critical victims are identified, they are stabilized and taken to the healthcare facility while the rest of the patients are addressed on site.
The unit is divided into two sections: the primary treatment zone and the secondary storage zone. The primary zone is home to the emergency supplies, and the connection to oxygen, electricity, and water. The secondary zone contains the larger units needed on site such as the foldable stretchers, go bags, portable batteries, portable oxygen, and extra supplies.
When dealing with a mobile unit, there had to be a flexibility in the features to be able to exist in different conditions. Things such as a PVC fabric for durability, the choice to make a mechanically deployable tent to ensure multiple deployments without causing strain on the physical material, and a structural frame which is modeled from the structure of a durable shipping container were all considered. There also had to be features included to increase the ease in use such as a lever to crank the fabric back into the roll, the walking space within the unit between the supplies, and the footing to assist with the circulation within the site.
The floor plan further clarifies the organization of the components within the unit.
The elevation expresses the location of the utilities with respect to the hitch. To ensure more stability during transport for the utilities, it is located directly above the hitch. The flag is placed to signify the triage category which is being addressed at that time.
The sections express the relationship between the treatment areas and the supplies. Creating the walkway within the unit allows the treatment areas to connect and bleed into each other.
The loads affecting the unit were addressed when the structure was being created. The tension cables at the ends of the telescopic structures are
incorporated to offset the wind uplift.
The overall system can be created using multiple units.
CRU is designed to be able to be walked through and create a continuous circulation within the site for the staff. The circulation flows through the supply corridor of one unit into a covered treatment area in front of the storage space with portable utilities.
The CRU system could also be utilized in case of a larger mass casualty situation such as a flood or fire. A makeshift clinic can be created using these units.
The layout of the supply and storage zones determines the types of treatment areas. Critical treatment areas can be created where the supply and utility zone is located adjacent to the storage zone as that area has access to resources available in both zones of the unit. Other treatment areas are adjacent to only the supply & utility zone.
This creates a grid like organization on an otherwise chaotic site. While patients travel along this grid.
The staff can travel along a different grid utilizing the corridors within the unit.
CRU strives to be able to provide an effective area for treatment and create some organization on an incredibly chaotic site.
By establishing this organization, it is easier for medical staff to be able to triage critical victims quickly and administer emergency stabilization.
The response time which could otherwise be wasted attempting to transport each victim to a healthcare facility to then await triage in an overwhelmed facility, is now cut to a fraction by providing an organized space to conduct that triage initially on site.
bibliography
“Rhino RT/R5 Telescopic Bollard.” Rhino Security. Accessed May 06, 2019. http://www.rhinosecurity.co.uk/post-barriers/steel-telescopicposts/137-2/.
“Specification for Rigid Stretchers.” doi:10.3403/00259128. https:// techlemstretchers.com/wp-content/uploads/2018/11/Techlem-Cataloguerev4-webNA.pdf
“Strap Drive | Telescoping Field Mast | 8 to 18 Meters | MIL-STD-810.” The Will-Burt Company. Accessed May 06, 2019. https://www.willburt.com/ products/telescopic-masts/qeam/hdtm/.
“3G Aluminum Alloy Stretcher.” Medical Stretchers - Ambulance Stretchers - Mobi Medical Supply. Accessed May 06, 2019. https://medicalstretchers.com/2-ambulance-stretchers.
“ASAP® RAPID SHELTER SYSTEMS.” Deployed Logix. Accessed May 06, 2019. https://deployedlogix.com/asap-rapid-shelter-systems/#tab-id-1.
“ETFE and PTFE Structures.” Fabric Architect. Accessed March 26, 2019. https://www.fabricarchitect.com/material-choices.html.
“First Aid Product™.” First Aid Product: Wholesale Direct to the Public! Why Pay Retail?™. Accessed March 05, 2019. https://first-aid-product.com/ disaster-survival/triage-supplies-s-t-a-r-t-triage-kits.html.
“Mass Casualty Management Systems.” World Health Organization. April 2007. Accessed March 3, 2019. https://www.who.int/hac/ techguidance/tools/mcm_guidelines_en.pdf?ua=1.
“Mass Casualty Oxygen System (MCOS).” First Line Technology. Accessed May 06, 2019. https://www.firstlinetech.com/product/mcos/.
“Mass Casualty, START Triage and the SMART Tag System.” Lecture, Boston, March 06, 2019. Accessed March 6, 2019. https://www. blessinghealth.org/sites/default/files/users/user15/EMS_START_Triage_ SMART_Tags_2017.pdf.
“Telescoping Mast | Unlimited Deployment | No Maintenance.” The WillBurt Company. Accessed May 06, 2019. https://www.willburt.com/ products/telescopic-masts/pneumatic-locking/non-military/.
“BP Medical Supplies.” Accessed March 05, 2019. https://www. bpmedicalsupplies.com/products/Disaster-Relief-MCI/Triage-Supplies/.
“Goal 3: Good Health and Well-being.” UNDP. Accessed February 10, 2019. http://www.undp.org/content/undp/en/home/sustainabledevelopment-goals/goal-3-good-health-and-well-being.html#targets.
“Malawi.” World Health Organization. February 01, 2015. Accessed February 11, 2019. https://www.who.int/gho/countries/mwi/en/.
“Model Comparison Chart.” Demers Ambulances. Accessed February 27, 2019. https://www.demers-ambulances.com/model-comparison-chart/.
“New UN Regulation on Automatic Emergency Call System for Road Traffic Accidents Will Reduce Response Times, Save Lives.” Targeted News Service, Nov 23, 2017.
“Rapid Deployment Shelters For Sale | HTS.” Roder HTS USA. Accessed February 11, 2019. https://www.hts-usa.com/products/rapiddeployment-shelters/.
“Road Traffic Deaths.” World Health Organization. March 11, 2016. Accessed February 12, 2019. https://www.who.int/gho/road_safety/ mortality/en/.
“SHELTERPOD (RED) Limited Edition.” SHIFTPOD | Advanced Shelter Systems Inc. Accessed February 11, 2019. https://store. advancedsheltersystemsinc.com/responsepod/shelter/shelterpod-r.
“What Is a Mass Casualty Incident?” Classification of Social Media Platforms. Accessed February 27, 2019. https://delvalle.bphc.org/mod/ wiki/view.php?pageid=89.
Branas, C. C., E. J. MacKenzie, and C. S. ReVelle. 2000. A trauma resource allocation model for ambulances and hospitals. Health Services Research 35 (2): 489-507.
Chokotho, Linda, Wakisa Mulwafu, Kathryn H. Jacobsen, Hemant Pandit, and Chris Lavy. 2014. The burden of trauma in four rural district hospitals in malawi: A retrospective review of medical records. Injury 45 (12): 206570.
Haac, Bryce E., Jared R. Gallaher, Charles Mabedi, Andrew J. Geyer, and Anthony G. Charles. 2017. Task shifting: The use of laypersons for acquisition of vital signs data for clinical decision making in the emergency room following traumatic injury. World Journal of Surgery 41 (12): 306673.
Harrison, Hooi-Ling, Nigel Raghunath, and Michele Twomey. 2012. Emergency triage, assessment and treatment at a district hospital in malawi. Emergency Medicine Journal : EMJ 29 (11): 924-5.
HDT Global. Accessed February 27, 2019. http://www.hdtglobal.com/ series/medical-mergency-operations/.
https://www.who.int/bulletin/archives/80(11)900.pdf
Lynn, Mauricio. “Hospital Planning and Response to Sudden Mass Casualty Incidents.” Mass Casualty Incidents, 2016, 25-55. doi:10.1007/978-1-
4939-3496-6_3.
Mohammed-Najeeb Mahama, Ernest Kenu, Delia Akosua Bandoh, and Nuhu Zakariah Ahmed. “Emergency Response Time and Pre-Hospital Trauma Survival Rate of the National Ambulance Service, Greater Accra (January – December 2014).” BMC
Repoussis, Panagiotis P., Dimitris C. Paraskevopoulos, Alkiviadis Vazacopoulos, and Nathaniel Hupert. 2016. Optimizing emergency preparedness and resource utilization in mass-casualty incidents. European Journal of Operational Research 255 (2): 531-44.
Rivas-Adrover, Esther. (2015). Deployable Structures.
Samuel JC, Akinkuotu A, Villaveces A et al. (2009) Epidemiology of injuries at a tertiary care center in Malawi. World Journal of Surgery 33, 1836–1841.
Samuel, J. C., E. L. P. Campbell, A. G. Charles, and B. A. Cairns. 2010. Burn epidemiology and burn care in malawi: Outlining prevention strategies. Injury Prevention 16 (Supplement 1): A61-.
Schlottmann, Francisco et al. “Road traffic collisions in Malawi: Trends and patterns of mortality on scene” Malawi medical journal : the journal of Medical Association of Malawi vol. 29,4 (2017): 301-305.
Sion, Melanie, MD, and Anthony Charles, MD, MPH, FACS. Central Malawi District Hospital Surgical Capacity Assessment. Report. Department of Surgery, Thomas Jefferson University Hospital.
Tyczynska, Nicole E. Online interview by Hardi Shah. February 06, 2019.
Yu, Christopher, Keenan Crane, and Stelian Coros. “Computational Design of Telescoping Structures.” ACM Transactions on Graphics36, no. 4 (2017): 1-9. doi:10.1145/3072959.3073673. https://www.cs.cmu. edu/~christoy/Projects/Telescopes-sig2017.pdf