Scientists are bringing to light the many ways sleep influences our physical and mental well-being

HARVARD AUTUMN 2022

Scientists are bringing to light the many ways sleep influences our physical and mental well-being
WAITING PATIENTLY: In August, welcome week ceremonies were once again back on campus. Days were filled with classes, clinics, and activi ties, all designed to help members of the incoming medical and dental school classes settle themselves in their new home. The week’s cap stone event, the white coat ceremony, was held under a large tent on campus. During the ceremony, students officially pledged themselves to the ideals and tenets of their respective professions. In the days and evenings preceding the much-anticipated ceremony, however, the tent stood silent, ready, and bathed in calming lights.


FOR THE PEOPLE: Third-year medical student Anjali Misra may aspire to bring music to audiences at the Hatch Shell in Boston, but her greater hope is to use the political stage to bring change to health care and people’s lives.

Researchers home in on how the sleeping brain consolidates memories.
20 Deep Trouble by Stephanie Dutchen
Floods, exacerbated by climate change, deposit disease and distress.

22 Clocking In by Charles Schmidt
Sleep researchers who study circadian rhythms are uncovering intricate links to health and disease.
28 The Land of Nod by Elizabeth Gehrman
The quiet of a sleeping child gives little hint of the growth and development going on in the brain.
34 The Limits of the Lullaby by Ann Marie Menting

An interview with a pioneer in pediatric sleep medicine.
38 Blavatnik Harvard Life Lab Longwood
The School opens a muchanticipated incubator space for academic and industry scientists.
4 Commentaries Letters from the dean and our readers

7 Discovery Research at Harvard Medical School
13 Noteworthy News from Harvard Medical School
42 Five Questions by Ekaterina Pesheva Pranav Rajpurkar on the exquisite possibilities of medical artificial intelligence
43 Roots by Catherine Caruso
Dzifa Kpodzo on her love of the art and practice of plastic surgery — and the difference her work can make in the lives of her patients
44 Student Life by Elizabeth Gehrman MD candidates on melding advocacy with medicine
The residency placements for members of the Class of 2022
Alumni share titles of books that have influenced them professionally or personally
ACCORDING TO THE U.S. CENTERS FOR DISEASE CONTROL AND PREVENTION, an estimated 1 in 3 U.S. adults are sleep-deprived. In addition, the Institute of Medicine’s Committee on Sleep Medicine and Research posits that more than 50 million people in this country are affected by sleep disorders. Clearly, there is a critical need to better understand sleep and circadian biology.
Fortunately, at HMS sleep medicine and chronobiology have been areas of active research for more than fifty years. In 1997, HMS established the Division of Sleep Medicine. Directed by Charles Czeisler, the Frank Baldino, Jr., PhD Professor of Sleep Medicine at HMS and the chief and senior physician of the Division of Sleep and Circadian Disorders in the Departments of Medicine and Neurology at Brigham and Women’s Hospital, the division brings together sleep researchers and clinicians from across Harvard and throughout the School’s affiliate hospitals to advance knowledge on sleep, circadian biology, and neurobiology; make evidence-based contributions to clinical care, public health policies, and workplace safety guidelines; and foster the next generation of sleep medicine physicians.
A notable example of work to advance the discipline is the National Sleep Research Resource. This data-sharing resource is funded by the National Heart, Lung, and Blood Institute and co-led by Susan Redline, the Peter C. Farrell Professor of Sleep Medicine at HMS and director of the Programs in Sleep and Cardiovascular Medicine and Sleep Medicine Epidemiology at Brigham and Women’s. As of 2020, this global resource hosted data from about 30,000 overnight sleep studies that are searchable and can be analyzed along a range of research queries related to physi cal, psychiatric, and cognitive health.
Our sleep researchers continue to contribute to the body of evidence on the effects of sleep deficiency on mental acuity, research that is vital to understanding the effects of shift work on the cognitive performance of firefighters, police officers, railroad workers — and the more than 140,000 resident physicians across this country. Large-scale surveys conducted by the Harvard Work Hours Health and Safety Group, a pan-Harvard group directed by Czeisler, have backed the call to curtail the number of allowable work hours for trainees in order to decrease medical errors and improve decisions on patient care. The group’s work also informs another troubling problem for our profession: physician burnout. A 2020 article co-authored by Czeisler in JAMA Network Open reported that sleep deficiency and sleep disturbance are predictors of depres sion and could be underlying factors in poor mental health among physicians.
Sleep, specifically the effects of daylight saving time on health, will also be featured in Harvard Radcliffe Institute’s 2022-2023 Exploratory Seminar series. Czeisler, together with Elizabeth Klerman, MD ’86 PhD ’90, a professor of neurology at Massachusetts General Hospital, will discuss the health-related advantages and disadvantages of both standard and daylight saving time with members of the legislative and executive branches of the U.S. government and leaders from business, communications, education, and other sectors of our society. The outcomes of this learning session could affect nearly every person in the nation.
I am confident that sleep researchers throughout HMS will continue to produce research that will better inform physicians, policymakers, and the public of the importance of a good night’s sleep on our overall health.
medicine
Catherine Caruso, Stephanie Dutchen; Elizabeth Gehrman; Ekaterina Pesheva; Charles Schmidt
JudyAnn Bigby, MD ’77; Emery Brown, MD ’87 PhD ’88; Rafael Campo, MD ’92; Elissa Ely, MD ’87; Timothy G. Ferris, MD ’92; Alice Flaherty, MD ’94; Atul Gawande, MD ’94; Donald Ingber, PhD; Sachin H. Jain, MD ’08; Perri Klass, MD ’86; Jeffrey Macklis, MD ’84; Victoria McEvoy, MD ’75; Barbara McNeil, MD ’66 PhD ’72; Lee Nadler, MD ’73; James J. O’Connell, MD ’82; Nancy E. Oriol, MD ’79; Anthony S. Patton, MD ’58; Mitchell T. Rabkin, MD ’55; Eleanor Shore, MD ’55
George Q. Daley, MD ’91
Kenneth Bridges, MD ’76, president

Louise Aronson, MD ’92, president-elect
Chasity D. Jennings-Nuñez, MD ’95, vice president
Douglas Chin, MD ’94 MMSc ’94; David Cohen, MD ’86 PhD ’87; John F. Cramer III, MD ’74; Sitaram Emani, MD ’97; Jessica Ann Holman, MD ’13; Elbert Huang, MD ’96; Kristy Rialon, MD ’08; Michelle Rivera, MD ’92; Margaret Liu, MD ’81; Numa Pompilio Perez Jr., MD ’15; Coleen Sabatini, MD ’04; Nancy Petersmeyer, MD ’80; Douglas Zipes, MD ’64
Chair of Alumni Relations
A. W. Karchmer, MD ’64
Harvard Medicine magazine is published two times a year, with online editions appearing monthly.
PUBLISHERS: Harvard Medical Alumni Association and Harvard Medical School
© The President and Fellows of Harvard College
EMAIL: harvardmedicine@hms.harvard.edu
WEB: hms.harvard.edu/magazine ISSN 2152-9957 | Printed in the U.S.A.
George Q. Daley Dean of Harvard Medical School
WE WANTED TO TAKE A MOMENT to remember Preston Phillips (Class of ’88) on these pages. Over the many years this magazine has been bringing news to alumni about alumni, it has chronicled lives lost to wars and conflicts of global scale. It is sobering to realize that we now salute one of our own taken by the scourge of gun violence in this country. Phil lips was killed while doing what he loved and what he excelled at: caring for his patients. We are all the poorer for this loss.
THE ARTICLE “ALTERED PERCEPTIONS” in the Spring 2022 issue of Harvard Medicine informs us of Harvard’s “troubled past,” refer ring to Timothy Leary’s Harvard Psilocybin Project of the early 1960s. A few years earlier, however, there was a foray into psychedel ics, specifically lysergic acid derivatives, by three highly respected Harvard investigators. One of them was Henry Knowles Beecher, MD ’32, the Henry Isaiah Dorr Professor of Research in Anesthesia at Massachu setts General Hospital and, later, professor emeritus at HMS. The trio wished to inves tigate whether LSD, which was then legal, induced mood alterations. Indeed, Beecher had proposed that LSD reflected and/or expanded a person’s preexisting mindset, which, along with “setting” (environment), was later echoed by Leary and colleagues, and is integral to current psychedelic therapeutic research protocols.
Beecher’s interests in LSD can be traced to his work as a battlefield physician during World War II, where he became aware of the essential role played by the subjective response to the effects of analgesic drugs. Indeed, he pioneered studies on the placebo effect. It is noteworthy that the United States Army Research Council and Central Intelli
gence Agency later supported Beecher’s clas sified LSD studies, allegedly to test various drugs for their property to influence human behavior, such as while extracting the truth from recalcitrant prisoners during interroga tion. It is likely that these government agen cies were not as interested in the mysteries of the mind as they were with mind control.
Perhaps of greater interest is Beecher’s apparent moral distress resulting from his involvement in what many later would consider to be unethical human LSD studies; the researchers had not obtained informed consent from the healthy college students who participated. Nonetheless, in a 2007 paper in International Anesthe siology Clinics, George Mashour, a scholar who has written on Beecher’s life and work, notes that Beecher evolved into a seminal, influential, and respected bioethicist who made groundbreaking contributions to the ethics of human experimentation while also serving as “a conscience for the psychedelic research movement.”
In fact, Beecher’s ideas and opinions were complex, and on occasion contradictory and enigmatic, yet inevitably open to his own reconsideration and public deliberation.
STEPHEN JACKSON, MD ’64 MONTE SERENO, CALIFORNIA
I READ THE ARTICLE ON the potential thera peutic uses of psychedelics in the Spring 2022 issue of Harvard Medicine. I am a master’s student at Harvard Divinity School, and I study Christianity and psychedelics, having spent a substantial portion of my life in the psychedelic movement.
With respect to those interviewed for the piece on psychedelics, I contin ue to find myself disappointed in over ly optimistic psychedelic discourse. As the psychedelic movement argues for its legitimacy, I believe it is not educat ing the public about significant scientific and ethical concerns around psychedelics. The leading research group, Multidisci plinary Association for Psychedelic Stud ies (MAPS), has set the tone that strategy is more important than honesty; as founder Rick Doblin once noted, “We don’t actu ally do science, we do political science.”
Doblin also has asserted that psychedelics can bring “net zero trauma” by 2050 and “spiritualize humanity” by 2070, which I believe displays a religious fervor instead of equipoise. I fear the excitement outpaces the unknowns, including long-term risks of psychological side effects.
I am not a scientist, so I rely on scientists to at least try to be committed to scientific equipoise. I am grateful to researchers who are beginning to offer more critical perspectives. For a sample of further read ing, I invite you to search online for the
blog post by Leiden University clinical psychologist Eiko Fried, Treating depres sion with psychedelics: red flags and FAQ I share this perspective because I am increasingly anxious about the unintend ed consequences of a societal psychedel ic pendulum swing when the movement lacks a culture of transparency and rigor ous self-criticism. Thank you for taking the time to read and consider.
JOE WELKERMASTER’S CANDIDATE
HARVARD DIVINITY SCHOOL
CAMBRIDGE, MASSACHUSETTS
IN THE ARTICLE ON THE EFFECTS OF HEAT on older adults in the Autumn 2021 issue of Harvard Medicine, you quote Francesca Dominici as saying, “Clinicians best serve patients when they stay abreast of the litera ture on risk factors and, when heat looms in the forecast, consider warning, checking in with, or adjusting relevant medications of the vulnerable.”
I think it is irresponsible to include this quote. I’m not sure this person, a profes sor of biostatistics, has any understanding of clinical medicine or should be making such recommendations.
Do you really mean to imply that a busy clinician, in the midst of a normal work day, should review the chart on every patient in their panel, review every single one of their potentially harmful medica tions, then reach out and call each elder ly patient and the person who manages their medications to explain recommend ed medication changes, every single time the temperature looks like it might rise above the potentially harmful threshold of 80 degrees Fahrenheit? Implying that this should fall to individual clinicians sets up unreasonable expectations and puts the blame for these deaths on physicians for not “doing everything they can” to prevent them. These types of expectations are exactly what lead to physician burnout
and the self-blame that is behind so many clinician suicides.
Another look I READ WITH INTEREST “A Place in the Room” and “Cri de Coeur,” two articles in the Spring 2021 issue of Harvard Medicine. Both pertain to inadequate consideration of major and common women’s health issues in clinical research programs, even in recent times.
Curiously, this is a legitimate complaint despite the fact that our esteemed NIH undertook a massive research initiative targeted at just such concerns three decades ago. The Women’s Health Initiative was begun in 1991, initially under the direction of the newly appointed first female NIH director, Bernadine Healy, MD ’70. A total of 160,000 postmenopausal women partici pated in a series of studies over fifteen years.
The most consequential of these studies had to do with the use of estrogen replacement therapy in postmenopausal women, a thera peutic modality that had become common and popular prior to 1990. This particu lar study was terminated abruptly in 2004 because of a failure to demonstrate benefit with regard to prevention of coronary heart disease. Little consideration was given to the clear benefit that occurred regarding prevention of osteoporosis. No consider ation was given to quality-of-life issues, such as control of menopausal symptoms. Data regarding breast cancer occurrence were variable, depending upon use or non-use of medroxyprogesterone in conjunction with estrogen replacement.
Along with termination of the estrogen replacement therapy study in 2004 came the stern recommendation that this ther apy be largely eliminated as a therapeutic option. This recommendation was prompt ly endorsed by OB-GYN physicians nation wide and has been conventional wisdom ever since. Seldom has a single study reversed therapeutic decision-making so quickly and completely.
Advocates for more sympathetic consid eration regarding major and common women’s health concerns do, however, have the opportunity to revisit and reinterpret the data of this Women’s Health Initiative study. Possibilities exist for segmental analysis in order to identify substantial subpopulations in which estrogen replacement therapy can be used safely, perhaps with limitations and restrictions, but with the prospect of signifi cant symptomatic and other benefits. These potential quality-of-life benefits were widely appreciated prior to 1990, although excluded from consideration in this landmark NIHsponsored program of studies.
Harvard Medicine welcomes letters to the editor. Please email your letter to harvard medicine@hms.harvard.edu. Letters may be edited for length, clarity, or to conform to HMS style.
HMS
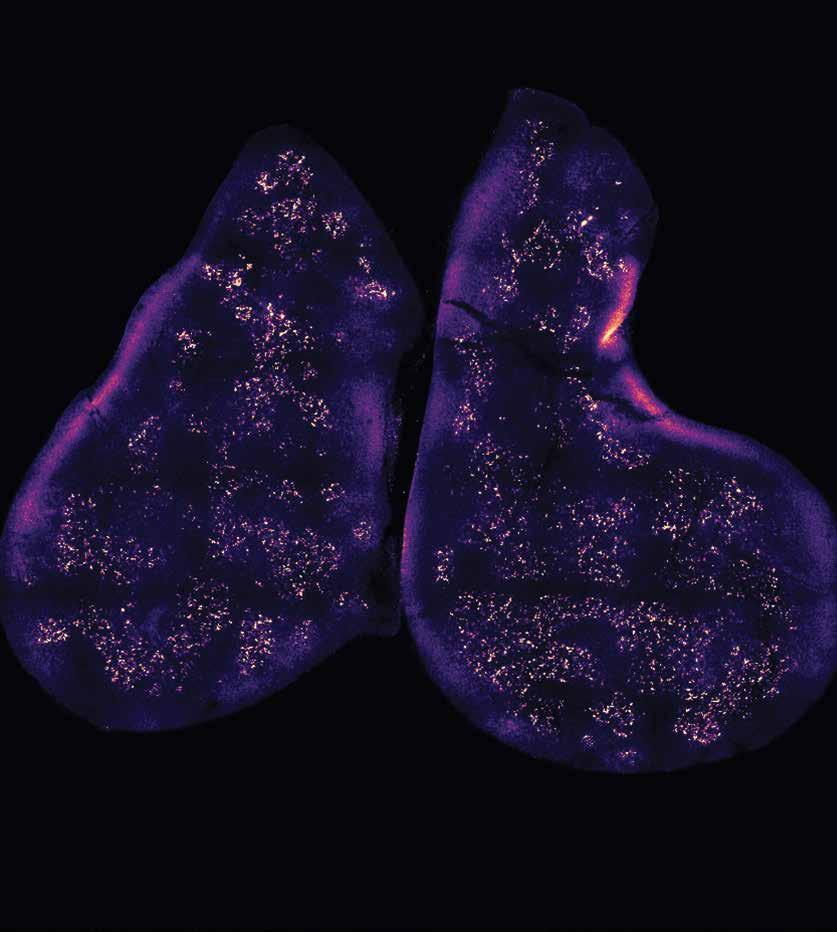
The thymus gland, shown here, produces T cells and teaches them to recognize foreign proteins.
THE MECHANISM BY WHICH CELLS in the thymus gland prepare T cells to discern self from non-self has been described by immunologists in the Blavat nik Institute at HMS. Their research shows that T cells, powerful immune cells produced in the thymus gland, are exposed to thymus-produced proteins that mimic proteins from various tissues throughout the body. These previews of the proteins that T cells will normally encounter help them learn to recognize foreign proteins. The investigators say the work could inform research on autoimmune diseases.
A COMPREHENSIVE INVESTIGATION of national trends in cardiovascular mortality among Black and white women and men across multiple sociodemographic domains conducted by HMS scientists at Beth Isra el Deaconess Medical Center has found that, although cardiovascular mortality rates across all groups declined over the past 20 years, Black people in this country continue to experience higher mortality rates than their white counterparts. This mortality disparity was especially evident in Black women younger than 65 and Black women and men living in commu nities with high levels of racial segregation.
The research team used publicly avail able data from the National Center for Health Statistics provided by the U.S. Centers for Disease Control and Prevention to examine more than 17 million cardiovas cular deaths in Black and white adults 25 years or older living in the United States from 1999 to 2019. The researchers crossreferenced the mortality data with informa tion from the U.S. Census Bureau divisions, which divide the nation into four sections: the Northeast, Midwest, Southeast, and West. They also used the NCHS urban–rural classification scheme to classify counties as urban or rural.
The researchers found that during the study period, age-adjusted mortality rates declined for Black adults as did the abso lute rate difference between Black and white adults. However, the cardiovascular mortality rate remained higher for Black adults. The relative gap between Black and white women and Black and white men was greatest in the younger subgroups, indicating higher rates of premature death from cardiovascular disease in Black women and men.
The team also found that, although mortality rates declined across all groups in all regions, relative reductions in mortal ity were greatest among white individuals,

A team of HMS researchers at Massachusetts General Hospital and Brigham and Women’s Hospital has shown that compared with an adenovirus vaccine, mRNA vaccines elicit more function al antibodies specific to SARS-CoV-2 in both pregnant individuals and their children. Furthermore, the team found that mRNA vac cines administered during the first and third trimesters provided greater maternal immune responses than did vaccines given in the second trimester and that the placenta-to-fetus transfer of antibodies specific to SARS-CoV-2 was most efficient after firstand third-trimester vaccinations. The results were consistent for all known variants of concern.
A TEAM made up of HMS researchers at Hebrew SeniorLife and Massachusetts General Hospital and colleagues at the Fram ingham Heart Study and the University of South Carolina has found a link between depression, diet, and the development of frailty. Frailty, defined as a recognizable state of increased vulnerability that occurs because of a decline in function across multi ple physiological systems, affects 10 to 15 percent of older adults and often co-occurs with other health conditions, such as depres sion. Diet is thought to be a major contribu tor to frailty development and depression. Although previous studies established a link between an inflammatory diet and the risk of frailty, this study sought to determine wheth er individuals with depressive symptoms are more vulnerable to frailty development in response to dietary inflammation.
while Black adults had higher mortality rates than their white counterparts in both rural and urban settings. The researchers speculate that, in rural areas, distance to health care clinics, food insecurity, and high rates of tobacco use, obesity, and diabetes may play roles. In more urban settings, rising income inequality and envi ronmental stressors may be associated with cardiovascular mortality.
About 1,700 individuals from the Fram ingham Heart Offspring Study cohort partic ipated in the study. During an 11-year followup period the participants, all determined to be non-frail at the start, reported their diet and depressive symptoms, then had their frailty status reassessed. The study showed that an association between inflammatory diet and increased odds of frailty was some what stronger among those with depressive symptoms. The researchers hypothesize that since individuals with depressive symp toms typically have higher levels of inflam mation, adding dietary inflammation on top of that accelerates the development of frail ty. In addition, the data suggest that when middle-aged and older adults consume a pro-inflammatory diet, they are more likely to simultaneously develop new depressive symptoms and frailty rather than develop either condition alone.
Kyalwazi AN et al., Circulation, July 2022
Millar CL et al., The Journal of Gerontology, July 2022
Atyeo CG et al., Nature Communications, June 2022
A TEAM LED BY RESEARCHERS at HMS and the Broad Institute of MIT and Harvard has identified the pathway by which a specific gut bacterium, Akkermansia muciniphila, helps control inflam mation. By identifying the molecules the bacte rium produces, detailing their actions in the gut, and describing the biological outcome — inflam mation control — the team achieved what may be a first: a soup-to-nuts understanding of the metabolic activity of a gut bacterium. Complete characterizations of bacterial activity, say the scientists, are essential if we are to learn how to manipulate gut bacteria to treat or prevent illness.
Bae M et al., Nature, July 2022
IN EXPERIMENTS using a mouse model, HMS researchers at Boston Children’s Hospital have developed a new technique that could lead to “offthe-shelf” CAR T therapies, potentially making treatments available to more patients who need them. This scalable technique uses induced pluripotent cells to generate generic CAR T cells.
In CAR T-cell therapy, T cells from a patient’s blood are engineered to carry so-called chime ric antigen receptors, or CARs, that enhance the T cells’ ability to attack and kill tumor cells.
Although the therapy successfully treats certain leukemias and lymphomas, it’s not available for many who need it.
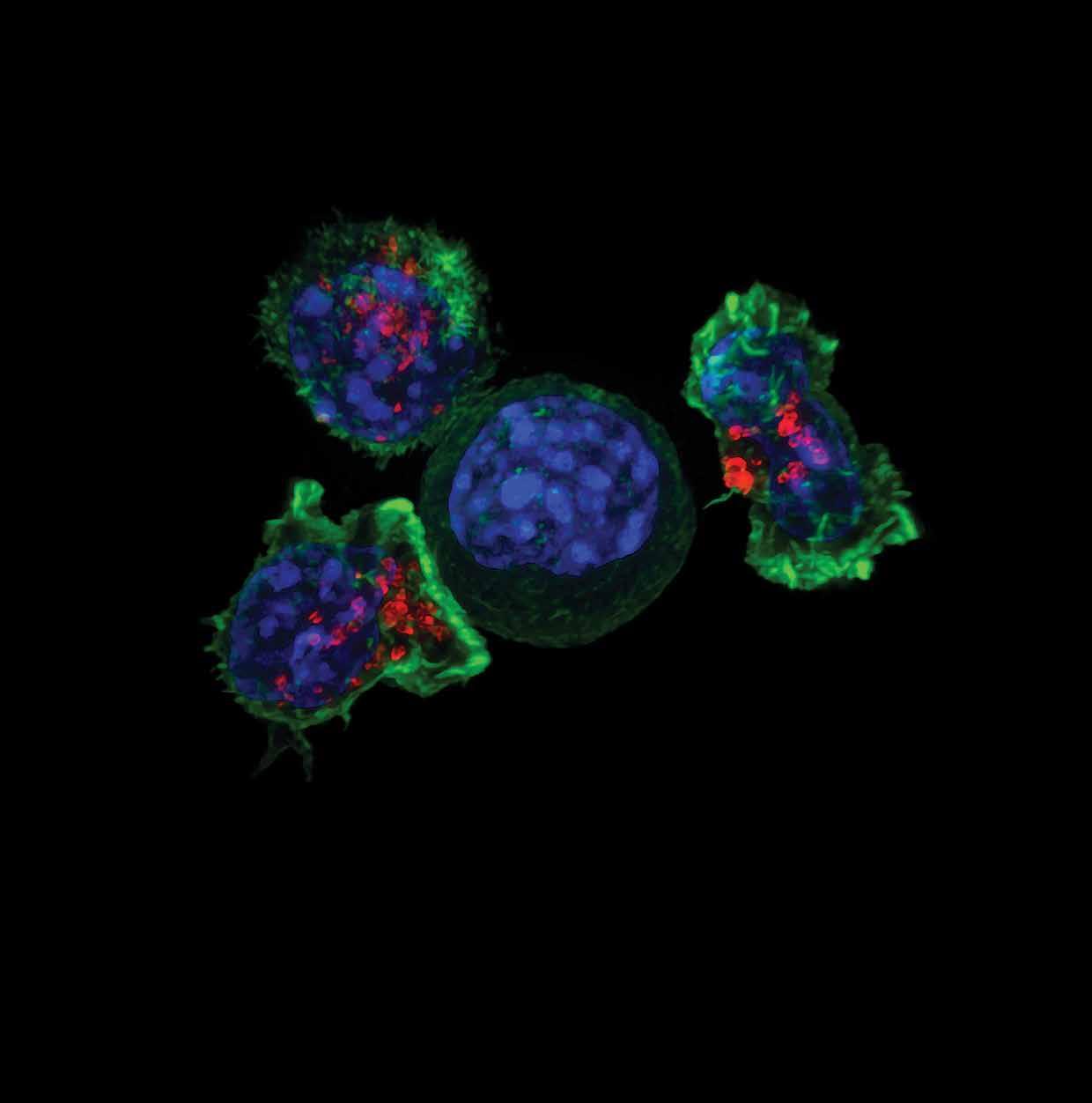
Jing R et al., Cell Stem Cell, August 2022 ALEX RITTER, JENNIFER LIPPINCOTT SCHWARTZ, AND GILLIAN GRIFFITHS/NATIONAL INSTITUTES OF HEALTH Microscopic image showing killer T cells (red and green) surrounding a cancer cell (blue, center).INFLAMMATION, THE BODY’S FIRST LINE of defense, occurs when immune cells rush to the site of injury or acute illness to make repairs and stem further damage. When successful, inflammation helps the body survive and heal, but when recovery following an inflammatory response goes awry, damage continues — and the inflammation itself can cause further injury, increased disease severity, or death.
Clues to what could predict the road to a good inflammatory recovery have recently been uncovered by scientists at HMS and Massachusetts General Hospital.
The team of researchers identified univer sal features of the inflammatory responses of patients who successfully recovered after surgery or acute illnesses such as COVID-19, heart attack, and sepsis. These features, they discovered, include precise trajectories that white blood cell and platelet counts follow as they return to normal.
For their study, the researchers sought to isolate common features they would need to study inflammatory recovery, an aim that led them to focus on patients who under went nonemergency cardiovascular surgery, such as coronary bypass, valve replacement, or some combination. By examining data from more than 4,600 such patients, the team found two measurements that reliably identified a successful inflammatory recov ery: a precise rate of decrease in white blood cell count and a precise rate of increase in platelet count.
Furthermore, when the scientists math ematically analyzed the trajectories for a successful recovery, they found that in patients with successful inflammation recov eries, white blood cell counts underwent exponential decay while platelet counts increased linearly after a short delay.
To determine whether these trajectories held for patients with other medical condi tions, the team assessed data from patients
who had other types of surgeries — limb amputations, hip replacements, cesarean sections, partial colon removals, and complex pancreas surgery — and who had experienced conditions such as COVID-19, Clostridium difficile, colitis, and sepsis. Patients who had successful inflammatory recoveries showed the same white blood cell and platelet count trajectories as patients who recovered well from cardiovas cular surgery. The indicators for inflamma tion recovery also held for patients who had experienced heart attacks and strokes, conditions that can prompt inflamma tion. The findings held true regardless of a patient’s condition or age.
Foy BH et al., Nature Communications, August 2022which then passes those signals to the brain. How well the cochlear nerve relays these signals contributes to the clarity, or intelligi bility, of sound processed within the central nervous system.
For years, scientists and clinicians believed hair-cell deterioration was the primary cause of hearing loss and that cochlear nerve damage was widespread only after hair cells were destroyed. Audio grams, long considered the gold standard of hearing exams, provide information about the health of hair cells, not the health of the auditory nerve. This fact, say the research ers, explains why many patients with normal audiograms report having difficulties hear ing in noisy environments, a characteristic of hidden hearing loss.
Maison SF et al., Scientific Reports, June 2022 OTOLARYNGOLOGYA TEAM OF HMS RESEARCHERS at Mass Eye and Ear has developed a model capable of esti mating the amount of hidden hearing loss in humans. After comparing two large sets of data, one that showed average speech scores collected during hearing tests as a function of age and one that tracked the aver age loss of cochlear nerve fibers as a func tion of age, the team was able to construct a model that estimates the relation between speech scores and nerve survival in people.
According to the scientists, the model offers ways to gauge the effectiveness of hear ing loss interventions, including the use of personal sound amplification products and hearing aids. Its use could also lead to better evaluations of cochlear nerve damage and the speech-intelligibility deficits that result.
Two main factors determine how well a person can hear: audibility and intelligibility. Hair cells, the sensory cells inside the inner ear, contribute to the audibility of sounds—or how loud a sound must be for a person to detect it.
Upon detecting a sound, hair cells pass electrical signals to the cochlear nerve,
When placed near the ear or against the skull, a vibrating tuning fork, such as the one shown above, is sometimes used to determine hearing loss. Studies have shown, however, that results of such tests can be subjective, with mixed hearing loss and conductive hearing loss being difficult to distinguish.

IN A NATIONWIDE STUDY that compared outcomes of pregnant patients who gave birth in the 14 months before the advent of COVID-19 and the first 14 months of the pandemic, HMS researchers at Beth Israel Deaconess Medical Center and the Harvard T.H. Chan School of Public Health found that during the pandemic the rates of maternal death during deliv ery hospitalization increased, as did the rates for cardiovascular disorders and obstetric hemorrhage among this patient population.
The study analyzed data from 1.6 million pregnant patients who gave birth in 463 U.S. hospitals. There were no statis tically significant differences in the two groups’ demographic characteristics, including age, race and ethnicity, insur ance types, and comorbidities.
Consistent with reports from the U.S. Census Bureau, the team saw a 5.2 percent reduction in total live births during the pandemic period. Their analysis also found that maternal deaths during in-hospital delivery increased from 5.17 deaths per 100,000 pregnant patients prior to the pandemic to 8.69 deaths per 100,000 pregnant patients during the pandemic, a small but statistically signif icant increase. They also saw increases in the odds of developing hypertensive disor ders and hemorrhage, a difference they suggested may indicate how the pandem ic heightened stress and adversely affect ed obstetric care and pregnancy-related outcomes.
The researchers found that during the pandemic, hospital stays, particularly after cesarean births, were shorter as obstetric teams worked to minimize the spread of infection, and rates for sepsis declined, an outcome they linked to enhanced hand hygiene and masking.
Molina RL et al., JAMA Network Open, August 2022
For decades, it’s been known that skin pigmentation can affect a pulse oximeter’s ability to accurately measure oxygen satu ration. Pulse oximeters measure how much light passes through the skin to render an estimate of how much oxygen is in a patient’s red blood cells. The most accurate way to measure true blood hemoglobin oxygen saturation levels is by analyzing a sample of a patient’s arterial blood. Yet the procedures for drawing these blood samples can cause discom fort for patients, so they are not performed routinely.
Recent findings from a study of the effects of taking large doses of vitamin D show such supplements do not decrease fracture risk in healthy middle-aged and older adults, upending the idea that older people should take extra vitamin D to ward off agerelated osteoporosis and loss of bone mass. The study was led by HMS researchers at Brigham and Women’s Hospital and is part of the large Vitamin D and Omega-3 Trial (VITAL). The results, say the researchers, indicate that only small to moderate amounts of vitamin D are needed to preserve bone health and that those amounts can be found in foods that have been fortified with vitamin D.
For the recent study, the researchers investigated whether pulse oximeter read ings affected the delivery of care in hospi tal intensive care units. They found that, compared to white patients, Black, Hispanic, and Asian patients had greater discrepancies between oxygen saturation levels detected using pulse oximeters and levels detected in blood samples: specif ically, pulse oximeter readings for the Black, Hispanic, and Asian patients indi cated oxygen saturation levels higher than levels found in analyses of their blood samples. As a result, these patients were less likely to receive supplemental oxygen than white patients in the study.
Such discrepancies can have dire consequences. Falsely elevated oxygen saturation readings can obscure the fact that a patient may be at heightened risk for hidden hypoxemia, a condition associ ated with higher mortality rates and one that occurs at higher incidence among racial and ethnic minority patients.
PULSE OXIMETERS, the clinical devices used to measure a person’s oxygen saturation levels, may be contributing to disparities in care, says a team of HMS researchers from Brigham and Women’s Hospital and Beth Israel Deaconess Medical Center.
The researchers say the findings offer a cautionary tale, for they highlight the biases that exist in real-world data, noting further that such data are increasingly being used in medical artificial intelli gence efforts to train algorithms to assist clinicians with decision-making.
Gottlieb ER et al., JAMA Internal Medicine, July 2022LeBoff MS et al., New England Journal of Medicine, July 2022
On August 1, David Ginty ( fig. 1), the Edward R. and Anne G. Lefler Professor of Neurobiology, became chair of the Depart ment of Neurobiology in the Blavatnik Insti tute at HMS. He succeeds Michael Greenberg, the Nathan Marsh Pusey Profes sor of Neurobiology, who announced last November that he would step down after 14 years as chair.
“The department stands for excellence and inclusion in neuroscience research, training, and education,” said HMS Dean George Q. Daley, MD ’91, in his announce ment of Ginty’s appointment, “and I am confident that David will further strength en and evolve what is arguably the nation’s, if not the world’s, preeminent neurobiology department.”
Ginty is the seventh chair to lead the department. Founded in 1966, it is consid ered to be the first neurobiology depart ment established in the world. Today, the department includes thirty research labo ratories in which scientists study neurosci ence at the molecular, cellular, circuit, and systems levels.
“It is an honor and privilege to have this opportunity to lead the department during this period of extraordinary discovery,” said Ginty.
Ginty did postdoctoral work in neurobi ology at HMS in the early 1990s. In 2013, he returned to the department as a member of its faculty and has served as associate direc tor of the Harvard Program in Neurosci ence and as a primary mentor to numerous graduate students and postdoctoral fellows who have gone on to posts in academia and industry. Ginty also is a Howard Hughes Medical Institute investigator, a member of the National Academy of Sciences and the American Academy of Arts and Sciences, and a fellow of the American Association for the Advancement of Science.
In his announcement, Daley thanked Greenberg “for his incredible vision and leadership of the department, and for
being a thoughtful and trusted advi sor to countless colleagues, including me.” Greenberg will remain a faculty member in the neurobiology department.
Members of the Class of 2026 welcomed to campus
In August, HMS and the Harvard School of Dental Medicine celebrated a defining tradi tion: a week of welcome for new students together with the presentation of the white coats that signify their entrance into the professions of medicine and dentistry ( fig. 2).
In his greeting to the students, George Q. Daley, MD ’91, dean of HMS, told the students that despite challenges they may face, each of them possesses what they need to achieve their goals.
“Let me assure you that if you remain focused on what you came here to do — to discover what it means to be a good doctor, to absorb the latest in biomedical science, and to cultivate effective leadership skills — you will go far,” Daley said.
The 164 students who make up the incoming MD class include 92 women, 69 men, and 3 people with different gender identities. The total number of entering dental students is 35, with 21 women and 14 men.
Twenty percent of the entering MD class are members of groups underrepresented in medicine. Twenty-one students iden tify themselves as LGBTQ. The entering students hail from Brazil, Canada, Mexico, New Zealand, and thirty-six U.S. states.
Within the MD class, 135 students are enrolled in the Pathways curriculum, which incorporates early clinical experience and advanced clinical and student-tailored science courses, as well as collabora tive, case-based pedagogy. Twenty-eight students are enrolled in the Health Scienc es and Technology program, a Harvard University, HMS, and MIT collaboration focused on translational medical science and engineering. Fourteen students are enrolled in the Harvard/MIT MD-PhD Program, indicating that they plan to earn an additional advanced degree while completing their medical studies.
Coursework for the students’ first week was designed to give them a shared funda mental understanding of key concepts that will be important in their future careers, while first clinical experiences provided them an introduction to the doctor-patient relationship.
The Biden administration announced in early August that Monica Bertagnolli ( fig. 3), an HMS faculty member who has dedicated her career to improving the lives of patients with cancer, will be the next director of the National Cancer Institute, the nation’s lead agency for cancer research.

Bertagnolli is the HMS Richard E. Wilson Professor of Surgery in the Field of Surgical Oncology at Brigham and Women’s Hospital. She also serves as a clini cal researcher and a surgical oncologist at the Dana-Farber Brigham Cancer Center and as a member of the Gastrointestinal and Sarcoma Treatment Centers at DanaFarber Cancer Institute.
In an interview following her appoint ment, Bertagnolli reflected on this new opportunity. “I hope to do everything possible to get the very best tools in the hands of colleagues. That’s what our patients need. The exciting thing about the NCI is that it truly reaches every part of our society. It enables new discoveries in basic science laboratories and it works to translate them into findings that trans form patient care for everyone in America, including those in the most underserved communities. It’s the thrill of a lifetime to be able to join the team at NCI.”
Although Bertagnolli thinks there is much promise in oncology now, from basic science research to work by the biotech industry, she does see challenges. The most critical, she said during her interview, is getting research results translated directly into benefits for all patients, not just those who have advantages.
“There is both incredible excitement and promise, but it’s also a huge challenge.”

The Lagoon Nebula, shown here in a photograph taken in 2018 by the Hubble Space Telescope, lies 4,000 light-years from Earth. It is filled with radiation, high-speed particles, and dense clouds of gases — in short, the stuff that stars are made of. Through an ages-long process of consolidation, stars are built. When ready, they take their places in the celestial expanse.

J. ALLAN HOBSON, MD ’59, USED TO SAY that the only known biological function of sleep was to cure sleepiness. It was the only biological drive that humanity didn’t yet understand the purpose of. Hunger and thirst propel people to sustain their bodies; sex perpetuates the species. But sleep? Nothing. n Then his team found evidence of a far larger role for sleep.
Ithappened in 1999. Study participants sat one at a time at a computer in Hobson’s lab at HMS, where he was a profes sor of psychiatry. Between blank screens, an image flashed for mere milliseconds: a grid of horizontal dashes, 19 across and 20 down, uniform except that one dash was switched out for a letter — either T or L — and three dashes in a row were slanted.
Robert Stickgold, at the time an HMS assistant professor of psychiatry in Hobson’s group, asked each participant to report which letter they’d seen and whether the trio of slant ed lines had been arranged horizontally or vertically. As the test repeated for 60 to 90 minutes, he adjusted the speed of the screens and tracked the participants’ accuracy.
Stickgold had some participants repeat the task later the same day. They didn’t improve much. Those tested the next day after a full night of sleep, however, did significantly better.
Looking further, the team found that it took at least six hours of sleep for a participant to achieve significant improvement. The more sleep they got beyond six hours, the better they did on the test.
Taking some participants into the sleep lab revealed that improvement depended on how much deep, slow-wave sleep participants
experienced in the beginning of the night and how much rapid eye movement, or REM, sleep they got toward dawn.
When Stickgold and his colleagues published their findings in the Journal of Cognitive Neuroscience in 2000, they provid ed some of the first convincing evidence that sleep was not merely useful to memory and learning, as had been shown before, but in fact required for both.

“It might have been the first study that hit the scientific community hard enough that they believed it,” says Stickgold, now an HMS professor of psychiatry at Beth Israel Deacon ess Medical Center and a global leader in sleep, dream, and memory research. “It was so care fully done, with so many ridiculous control groups, that it really landed.”
Before he died, in 2021, Hobson saw scien tists confirm sleep as a critical player not only in memory consolidation, but in immunity, endocrine function, and mood regulation. Recent work suggests other roles, such as clearing disease-associated waste products from the brain. It all started with memory, and memory started with that grid of dashes.
Stickgold vividly remembers the hope and fear of those initial findings. “I was driv ing home, sitting at a stoplight, having an imagined conversation with Terry Gross on NPR and saying, I hope it doesn’t turn out that the function of sleep is to help you see diagonal bars,” he quips. “Because that’s all we could say as a fact.”
He didn’t worry for long. Within months, studies began tumbling in one after anoth er. Stickgold and HMS colleagues went on to show in 2000 alone that participants deprived of sleep the first night after the test didn’t improve overnight as much as those allowed to rest, even after they were given two nights of catch-up sleep; that it didn’t matter what time of day participants were tested or how much they’d slept the night before their first training; and that partici pants learning to play Tetris dreamed about it over the following night. Studies since then have established other connections: those who take a nap after learning some thing new remember it better than those who don’t nap, people with amnesia dream about tasks they just learned even though they don’t consciously remember them, and people who dream about a task after first learning it improve more after sleep ing than those who didn’t dream about it.
Over the past two decades, these and other studies involving healthy sleep, disor dered sleep, and sleep deprivation, both in humans and in animal models, have persuaded most experts that sleep plays an essential role in consolidating all sorts of memories. That includes what are techni cally known as declarative memories, such as your relatives’ names, your most embar rassing moment, and what a cat looks like, as well as implicit memories, such as how to walk or play an instrument.
“I don’t think we’ve run across any type of memory processing that isn’t preferen tially or exclusively the province of sleep,” says Stickgold.
Consolidation refers to the second of three steps involved in memory process ing. The first is acquisition or encoding, when information comes into the brain. The murky phenomenon of consolidation was once conceptualized as the conver sion of short-term memories to long-term ones but is now understood to be a more complex process in which the brain sorts out what should be retained and what can be discarded from the day’s experiences, stabilizes the keepers, and begins filing them away and integrating them into existing knowledge. The third step has
JOHN SOARES (THIS AND FACINGtraditionally been considered recall, but a growing number of specialists, including Stickgold, view consolidation and recall as an ongoing state of memory evolution. While researchers have found that acquisi tion occurs mostly or entirely while awake, consolidation appears to happen primarily during sleep, with a still-unclear propor tion taking place when awake.
“Early on, memory researchers didn’t want anything to do with sleep,” says Stick gold. “Now they’re all looking at it.”
Today the question has turned from whether sleep enables memory consolidation to where, when, and how it does. Research ers are puzzling out which areas of the brain and which stages of sleep are involved in consolidating each type of memory and what happens at the molecular level to make it possible. At the same time, they’re reveal ing how sleep and memory consolidation go awry in conditions such as schizophrenia and post-traumatic stress disorder — and investigating how to intervene.
“Sleep has been relatively neglected as a target for treatment,” says Dara Manoach, PhD ’89, an HMS professor of psychology and director of the Sleep, Cognition and Neuropsychiatry Laboratory at Massachu setts General Hospital. “Maybe it’s the new frontier for intervention for cognitive deficits in a range of disorders and even healthy aging.”

Healthy sleeping brains appear to process memories all night long.
It’s become clear in recent years that nonREM and REM sleep each contribute to memory consolidation throughout the night. Non-REM sleep, which begins as the sleeper drifts off and then descends into slow-wave or deep sleep before rising to transition into REM, seems to do more consolidating of declarative memory. REM sleep, marked by dreaming, seems more important for consolidating implicit memory. But that’s a simplification, and plenty of details remain to be pinned down, like how consolidation varies between early night and late-night REM and for the many different kinds of declarative memory.
Ever more sophisticated tools point researchers to the parts of the brain most likely doing the work. Electroencephalography, or EEG, traces the electrical signals of messages traveling between neurons. Implanted elec trodes capture such signals deeper within the brain than surface EEG can reach. Imaging such as functional MRI shows which areas are active in a given sleep stage, while a single-cell light-activation technique known as optoge netics allows researchers to zoom in on the activity of individual neurons. Biochemistry and genetics flesh out the picture with clues about the neurotransmitters, genes, and gene expression patterns at play.
Earlier this year a group of HMS research ers discovered something never seen before in sleeping humans.
The researchers, led by Sydney Cash, an HMS associate professor of neurology and co-director of the Center for Neurotechnol ogy and Neurorecovery at Mass General, and Leigh Hochberg, an HMS senior lecturer on neurology, part-time, at Mass General, were testing a brain–computer interface for people with injured or missing limbs when they made the discovery.
The study included a participant with tetraplegia who played a game in which a computer “pressed” colored buttons in a certain sequence and then the participant would try to press the buttons in the same order by envisioning his paralyzed hand moving the cursor. Using electrodes they’d implanted in the participant’s motor cortex, the researchers watched as his motor neurons fired in corresponding patterns.
“Sleep has been relatively neglected as a target for treatment.
Maybe it’s the new frontier for intervention for cognitive deficits in a range of disorders and even healthy aging.”
The remarkable part came the following night: Those patterns repeated as the partic ipant slept. His unconscious brain appeared to be practicing the game in a phenomenon known as replay, which in the motor cortex had previously been observed only in labo ratory animals. This potential indicator of memory consolidation happened repeat edly during the night, largely during slowwave sleep. The team reported its findings in June 2022 in The Journal of Neuroscience.
“What we found was pretty incredible,” said Daniel Rubin at the time the paper was released. Rubin is an HMS instructor in neurology at Mass General and co-author on the paper. “This is the most direct evidence of replay from the motor cortex that’s ever been seen during sleep in humans.”
How much the participant’s perfor mance improved after his replay-filled sleep remains a tricky question; subsequent scores were lower, but the team believes that’s because he got too good at the game and moved the cursor faster than the computer was programmed to register it.
More than a dozen brain structures have been implicated in the larger story of memory processing, ranging from the most primitive — such as the cerebellum and the basal ganglia, major players in implicit “muscle memory,” and the amygdala, which modulates the emotional components of memories — to the evolutionarily recent, such as the prefrontal cortex, which orches trates working memory.
In the phase of non-REM sleep that fills most of the night, the cerebral cortex, thala mus, and hippocampus take center stage for memory consolidation. The cortex produc es long-cresting and briefly dipping elec trical waves. At the peak of some of these waves, the thalamus emits a short electri cal burst called a spindle that propagates to the cortex. With each spindle, the hippo campus, one of the most important struc tures in memory processing and the place where declarative memories form, sends out a sharp electrical ripple. Current theories hold that this triad represents memories being transferred from the hippocampus
to long-term storage in the cortex. Recent work suggests that the thalamus coordinates this dialogue of sleep rhythms.
Manoach’s empirical focus began in the thalamus. She studies schizophrenia, specifi cally its cognitive deficits that can cause people to struggle with memory, attention, and learning. Such deficits can be debilitat ing, yet treatments for them aren’t nearly as effective as those for the disorder’s psychot ic symptoms. Stickgold suggested in 2001 that Manoach look at sleep. The two quick ly discovered, in a study they collaborated on, that following sleep, controls got better at a computer keyboard-related task but that the same was not true for participants with schizophrenia. Sleep had no effect on their ability to perform the task; they didn’t get better at all. Manoach and Stickgold’s experiment, reported in 2004, was the first to demonstrate that schizophrenia involves a failure of memory consolidation during sleep. They soon traced the failure to a dearth of sleep spindles.
The finding made sense. Studies have shown that participants with more sleep spindles tend to show greater improvement
in memory-related tests the next day than do those with fewer spindles; brains busy consolidating memories overnight tend to produce more sleep spindles, spindle defi cits go hand in hand with consolidation troubles, and boosting spindles can allevi ate the problem.
A new drug seemed to offer a chance for Manoach’s team to help in schizophre nia. The sleep aid eszoplicone, approved by the FDA in 2004 and marketed as Lunesta, was known to boost the activity of GABA receptors in the thalamus, which have been linked to spindle generation. To the researchers’ delight when they ran a clinical trial, the drug increased spindle numbers and density in participants with and without schizophrenia, but to their bewilderment it didn’t improve memory.

Further studies provided an answer: the drug had unwanted effects on cortical waves and hippocampal ripples and disrupted the three-part synchrony.
“We learned that for an intervention to be successful, it has to preserve all three oscillations and their coordination,” says Manoach.
Manoach and Stickgold’s experiment was the first to show that schizophre nia involves a failure of memory con solidation during sleep.JOHN SOARES
So Manoach’s focus expanded to include the cortex and hippocampus. Led by Dimi trios Mylonas, an HMS instructor in psychi atry in Manoach’s lab, her team is now exploring the GABA receptor-targeting sleep drug zolpidem, marketed as Ambi en, which they found increases spindles and preserves hippocampal ripples in rats where eszoplicone suppressed them.
Researchers are exploring other noninva sive therapies to improve memory consolida tion during sleep. One type uses stimulation that the brain registers without waking up — electrical pulses, soft sounds, gentle vibra tions, light — to trigger spindles, which initiate fresh cortical waves. Bryan Baxter, an HMS instructor in psychiatry in Manoach’s group, is leading an auditory stimulation project for schizophrenia with an eye toward develop ing it for use with at-home wearable devices.
Studying sleep-dependent memory consoli dation has led Manoach and Stickgold to upend conventional views of sleep, memory, and certain neurological and psychiatric disorders.
Rather than starting with the idea that sleep abnormalities and cognitive issues arise as part of the natural progression of schizo phrenia, for example, Manoach hypothesiz es that they contribute to the illness. Many people with schizophrenia sleep poorly long before diagnosis. In 2014 Manoach reported that low sleep spindle rate activity is present early in the course of schizophrenia, before people start taking medications, and she and others have observed spindle and cognitive
deficits in unaffected family members. She joins a subset of researchers in suggesting that schizophrenia be reclassified as a cognitive disorder, one in which the symptoms typi cally associated with disease onset — hallu cinations, delusions, and disordered thinking and behavior — instead represent late-stage consequences that may be preventable.
Manoach and Stickgold also wonder whether PTSD is a disorder of memory consolidation. Clues arose when Stickgold and others noted that whereas ordinary dreams during REM sleep blend and riff on lived and imagined experiences, PTSD nightmares play back traumatic events like a movie. In talking with his wife, a trauma therapist, Stickgold realized that what goes wrong in the disorder — the brain’s failure to tamp down the emotional response to the memory, its holding on to detail instead of extracting the gist, its inability to incorpo rate the trauma into the person’s life story in a way that lets them move forward — indicates that the “things sleep does par excellence” have faltered.
“Your brain can’t do the integrative work,” he says. “It’s locked out of some of those consolidation processes.”
But what is it really?
As the saying goes, if you want to under stand something in biology, watch how it breaks. Efforts at HMS to illuminate sleep-dependent memory consolidation in disease span autism spectrum disorder, epilepsy, Alzheimer’s disease, narcolepsy, bipolar disorder, and more. Memory draws an unlikely connection among them.
“We conceptualize all these neurolog ical, psychiatric, and neurodegenerative disorders as different things, but sleep is involved in memory consolidation in all of them,” says Baxter. “We can ask whether sleep-dependent memory deficits in schizo phrenia are similar to those in Alzheim er’s. We can look at biomarkers that might be common across these conditions and try to develop interventions to target the biomarkers.”
Findings in the clinic provide new insights that guide basic scientists and vice versa. The hope now, sources say, is for greater dialogue between those focused on memory processing during conscious ness and those who study sleep.
“We haven’t paid enough attention to studying memory in both states together,” says Manoach.
“Instead of thinking of wake and sleep as binary, we need to look at how they link to each other,” agrees Mylonas. “Memoryrelated processes that happen in one state have consequences during the other.”
Collaboration across specialties is neces sary not only to tackle the complexity of memory consolidation but to complete the age-old pursuit to conclusively identify a memory in the brain.
“We don’t even know what a memory is,” says Stickgold. “It would be really excit ing to understand that.” He and colleagues are driven by deep desires to understand human memory and to make life better for people along the way.
“As a family member, I understand the suffering these illnesses cause,” says Mano ach, whose mother was diagnosed with a psychotic disorder while Manoach was studying schizophrenia in graduate school. “It’s a complex puzzle, this circuitry. I want to figure out how it works and how we can fix it.”
Answers tantalize on the horizon: How does something that happens when we’re largely unaware of the world help establish nothing less than who we are?
Stephanie Dutchen is manager of feature content and multimedia in the HMS Office of Communications and External Relations.
“We conceptualize all these neurological, psychiatric, and neurodegenerative disorders as different things, but sleep is involved in memory consolidation in all of them.”

T STARTS WHEN THE WATERS RISE, but it doesn’t end there.
Floods take lives, accounting for about half of all deaths related to natural disasters around the world each year. Greater still are their effects on survivors’ physical and mental health, which can last long after the waters recede.
Flooding is “by far the most pervasive risk” of climate change, states a June 2022 article in Nature Communications. Climate change spins up more frequent and fierce hurricanes. It helps fuel other storms that dump recordbreaking, riverbank-bursting rains like those that inun dated Kentucky, Missouri, Montana, and Texas this summer. Rising sea levels worsen storm surges and turn ordinary high tides into coastal floods. Accord ing to a 2013 review in Disaster Health, flooding events doubled worldwide from 1997 to 2006.
“Areas that traditionally haven’t experienced floods are going to experience them, including every coastal city in the U.S.,” says Patrick Vinck, an HMS assistant profes sor of emergency medicine at Brigham and Women’s Hospital and director of research at the Harvard Human itarian Initiative. “Many emergency health systems are not ready to cope with that type of disaster.”
While some people in a flood’s path are injured by swirling debris or die from drowning, the heaviest toll on health occurs in the days, weeks, and sometimes years that follow.
Health care providers can help reduce this longterm suffering by understanding the range of potential flood-related illnesses and being prepared when they encounter them in their clinics.
Infections top the list of illnesses — no surprise since floodwaters are usually filthy, picking up everything from sewage and animal waste to industrial pollutants to disease-causing organisms that flourish in warming seas, lakes, and rivers. Waterborne bacteria, viruses, and parasites can infect the skin, eyes, lungs, gastroin testinal tract, nerves, and other organ systems of those exposed to contaminated floodwaters or whose food or drinking water becomes compromised. The inci dence of diarrheal, respiratory, soft tissue, and systemic diseases, some mild and others life-threatening, often soars after floods. People may similarly fall ill if they touch or ingest toxic materials in floodwaters.
Mosquito-borne diseases can also follow as the insects breed in standing water. An outbreak of West Nile virus occurred in New Orleans after Hurricane Katrina hit in 2005.

“You have to be open-minded about vector- and waterborne infections in terms of understanding that we may see things in places we haven’t seen them before,” says Regina LaRocque, an HMS associate professor of medicine at Massachusetts General Hospi tal. “It’s very important to take a good patient history.”
Arguably the most underappreciated health conse quences of floods are not physical but psychological. This is particularly true in high-income countries, says a 2017 paper in Lancet Planetary Health. Clini cians and researchers have documented swells in depression, anxiety, post-traumatic stress disorder, substance use, suicide, and violence after floods.
The incidence and severity of mental illnesses tend to rise with more severe and longer-lasting floods, but Vinck notes that experiencing repeated, smaller flood events can erode mental health and quality of life too.
Ronald Kessler, the McNeil Family Professor of Health Care Policy in the Blavatnik Institute at HMS, contributed to our understanding of flood-driv en mental illness through his long-term work with people who survived Hurricane Katrina.
“Major disasters have enormous mental health effects,” he says. “There’s potential for permanent damage — you lose loved ones, your job, your house. Your community and way of life are gone. Depression, anxiety, uncertainty about the future, it’s scary stuff.”
Shifts in land use and population growth further increase the potential for floods to damage lives. Each year, tens of millions of people worldwide lose their homes to flooding, according to the 2022 Nature Communications paper. Displacement can drive refugeeism, which brings its own set of health risks.
Nor do people need to experience flooding them selves to feel the effects. Politico reported in 2017 that depression and anxiety can spread to those who are repeatedly exposed to news about flooding on tele vision or social media.
Post-flood infrastructure and behavior affect health as well. People may not be able to access health facilities to manage chronic conditions. Using gener ators in a power outage raises the risk of carbon monoxide poisoning. Gathering in mass evacua tion shelters can drive infectious diseases such as norovirus and COVID-19; influenza swept through a packed shelter after Hurricane Harvey inundated Houston in 2017.
Alongside diagnosis, clinicians can participate in research. Vinck wants to see long-term cohort studies analyze climate change, health, and human behavior, gathering evidence that can help reduce casualties from extreme weather events.
“We need to know how to effectively engage so people can protect themselves,” he says. “So they can decide how to react to conditions they haven’t experienced before.”
Then doctor and patient alike can be better prepared when floods arrive.
Stephanie Dutchen is manager of feature content and multimedia in the HMS Office of Communications and External Relations.

NE DAY WHILE HE WAS A GRADUATE STUDENT at Stanford University, Charles Czeisler embarked on an experiment that would alter the course of his career. It was 1974, and Czeisler was studying cortisol, a stress hormone that spikes during bouts of acute anxiety. Scientists were aware that cortisol also ebbs and flows in circadian cycles, and Czeisler wanted to profile the hormone’s daily rhythms in the body. So, he outfitted human volunteers with devices that sample blood repeatedly over time, anticipating that cortisol levels would not be affected by sleep. He found, however, that cortisol levels plunged when volunteers fell asleep later than usual, delaying the normal rise that occurs a few hours after bedtime. This showed that sleep interacted with circadian rhythms to affect the hormone’s secretion.
“The results blew me away,” says Czeisler, the HMS Frank Baldino Jr., PhD, Professor of Sleep Medicine at Brigham and Women’s Hospital and director of the Division of Sleep Medicine at HMS. “And they launched me on a lifelong quest to understand the properties of the human circadian pace maker and how it’s regulated.”
BY CHARLES SCHMIDTCzeisler and other scientists have since gone a long way toward advancing our knowledge of circadian rhythms, which are known to regulate essential functions ranging from hormone release to body temperature, sleep, and metabolism. The body’s inner clocks are exquisitely tuned to environmental cues and optimized for the natural world. That also means they can
be thrown off track by life in the modern world. Circadian disruptions are increas ingly linked to sleep deficiency, as well as chronic illnesses such as diabetes. But as scientists learn more about how circadian rhythms affect health, “we’re also finding new opportunities for clinical translation,” says Frank Scheer, a professor of medicine in the Division of Sleep Medicine at HMS and a senior neuroscientist in the Divi sion of Sleep and Circadian Disorders at Brigham and Women’s. “Understanding circadian biology is the key to developing novel targeted therapeutic interventions and protective lifestyle modifications.”
Robert Thomas, MMS ’03, an HMS asso ciate professor of medicine at Beth Israel Deaconess Medical Center, who studies sleep epidemiology with the Framingham Heart Study and the Korean Genome and Epide miology Study, would agree. “Sleep is holistic, affecting the heart, brain, lungs, metabo lism, truly all parts of the body, and its study involves all the body’s systems. Research is identifying these interactions so that clinicians can develop a broad and deep knowledge of how sleep affects the health of their patients.”
The study of circadian rhythms, chronobi ology, draws on a long evolutionary history. Billions of years ago photosynthetic cyano bacteria evolved the ability to follow circadian clocks to anticipate and respond to sunshine at dawn, and as more complex plants and animals spread over the planet, they too evolved rhythmic functions that provide adaptive advantages. Birds evolved circadian clocks to orient themselves to the sun’s posi tion during migration, and small mammals, such as chipmunks and squirrels, developed an innate sense to forage at times that mini mize their chances of being hunted and killed. Some of the earliest evidence for circadian rhythms was generated during experiments performed more than 300 years ago, when scientists discovered that certain plant species move their leaves at the same time of day even if they are subjected to total darkness. The term “circadian” was later coined to describe biolog ical rhythms that cycle in 24-hour periods, even in the absence of environmental prompts.
In mammals, circadian biology is to a large extent governed by a pinhead-sized bundle of nerve cells in the brain called the suprachiasmatic nucleus (SCN). This so-called master clock presides over a host of physiological processes. Scientists used to think the SCN was tied to its cycli cal rhythms by the sleep/wake schedule and social interactions. But in what he describes as his most important discovery, Czeisler reported in 1986 that the SCN is in reality activated by light impulses traveling along retinal nerve cells into the human brain. Light synchronizes the SCN to the solar day, prompting it, for instance, to coordinate cortisol release to increase during the night several hours after bedtime preceded by the release of the sleep hormone melatonin, which begins an hour or two before bedtime and peaks in the middle of the night.
At first scientists assumed that the SCN controlled all aspects of circadian biology and behavior in mammals. But during the late 1990s, scientists made another crucial discovery: Individual organs and cells contain their own circadian clocks, each of them similarly operating on 24-hour schedules driven by a cell-governed molec ular clock.
“If you take a cell from the heart, or skin, or liver and put it in a dish, it will happily tick along and exhibit rhythmic behav iors, even without external input from the environment or a neural network,” Scheer explains. An isolated liver cell, for instance, fires up the genes required for metabolism at hardwired intervals, regard less of whether it’s communicating with the SCN or not. Scheer describes these cell- and organ-specific clocks as members of an orchestra. As the central clock, the SCN plays the role of a conductor, he says, synchronizing other clocks to the light/ dark schedule through its hormonal and neuronal signaling. But the other “periph eral” clocks can still be reset by behavioral cues specific to their functioning, such as the timing of meals.
Charles Weitz, the Robert Henry Pfeiffer Professor of Neurobiology in the Blavatnik Institute at HMS, says the circadian clocks

in our cells are composed of several selfassembling protein structures thought to have properties like those of human-made machines. Comparable protein machines performing other functions “have moving parts and error control,” says Weitz. “They can recognize when something goes wrong and then fix it.” Weitz points out that up to several thousand genes in any human cell are under circadian clock control and that half of all human genes are under circadian clock control somewhere in the body.
“The most important processes of every organ system are regulated by their circadi an clocks,” Czeisler says. “Circadian clocks in lung tissue regulate respiration, and in the heart, they regulate cardiac function ing.” Elucidating how the clocks work was considered such a major advance that the scientists who accomplished this feat — Michael Rosbach and Jeffrey Hall, both geneticists at Brandeis University, and
In the late 1900s, scientists found that individual organs and cells contain their own circadian clocks, each operating on 24-hour schedules driven by a cellgoverned molecular clock. JOHN SOARES
Michael Young, a geneticist at Rockefell er University — were awarded the Nobel Prize in Physiology or Medicine in 2017.

But when the body’s clocks fall out of synch with each other, problems arise. That’s what is happening today, as modern technologies decouple us from the solar day to which our bodies evolved. We fly through time zones, obscuring our internal ability to distinguish day from night, resulting in jet lag. Most of us spend the evening hours bathed in artifi cial light that signals daytime to the SCN — shifting circadian clocks later in time, often to our detriment. Czeisler cites research showing that premature infants exposed to 12-hour alternating cycles of light and dark in the neonatal intensive care unit gain more weight, achieve better oxygen levels, and are discharged weeks earlier than babies kept in continuously illuminated NICUs, signifying how solar rhythms are hardwired into the human genome.
Indeed, researchers have found that light is the most potent disrupter of circa dian biology. That is especially true of the blue light emanating from our computer screens, “which has much bigger impacts on the circadian system than light of longer wavelengths,” says Jeanne Duffy, an HMS associate professor of medicine at Brigham and Women’s. “In addition to these effects on the circadian system, the light shines directly into your eyes, producing an alert ing effect.” During one study, Duffy and her collaborators found that people who nightly read e-books set at a typical brightness had suppressed melatonin levels, took longer to fall asleep, and were less alert the next morning. Duffy’s team concluded that using portable light-emitting devices at night disrupts circadian rhythms and perpetu ates sleep deficiency, a chronic problem for one in every three U.S. adults, accord ing to the U.S. Centers for Disease Control and Prevention.
Sleep serves many crucial functions in humans: excess synapses are pruned during sleep, and lymphatic channels open to carry waste products out of the brain, including amyloid proteins, which are damaging to nerve cells. “We also replay many of the
“Sleep is holistic, affecting the heart, brain, lungs, metabolism, truly all parts of the body, and its study involves all the body’s systems.”Robert Thomas
experiences we had during the day while sleeping and reinforce pathways by which these memories are stored,” Czeisler says. Sleep deficiency, by contrast, which occurs when adults get less than 7 to 9 hours of sleep per night, is a performance killer. “It lengthens reaction time and impedes judgment and problem-solving,” Czeisler says. “Someone who averages four to five hours of sleep a night for several days in a row develops the same level of cognitive impairment as if they’d been awake for 24 hours, which is equivalent to being legally drunk.” Indeed, research by Czeisler’s team has shown that irregular sleep and light exposure patterns in Harvard undergrads are linked to delayed circadian rhythms and lower academic performance. The irregular sleepers spent less time asleep between 10 p.m. and 10 a.m. and napped more during the day than regular sleepers.
Artificial light is far from the only circa dian disrupter — the body’s other clocks are similarly affected by their own ill-timed exposures. Clocks in the gut, for instance, were primed by evolution to receive food during the day; nighttime snacking and meals causes them to “reset.” Clocks in muscle tissue evolved to facilitate daytime physical activity, not nighttime workouts at the gym. If the timing of light, meals, and exercise conflict “your central timekeeper in the brain can be in Boston, while your liver clock is in Paris, and your muscle clock runs on Tokyo time,” Scheer says.
Scheer has found that such circadian misalignment puts people at risk of chron ic illnesses. He and other researchers have developed lab protocols for decoupling circa dian clocks from their environmental cues and behavioral cycles such as the sleep/wake cycle, so they can zero in on how disrupted rhythms affect health in human volunteers. During one study, Scheer’s team found that human participants living under conditions during which their mealtimes, sleep times, and light/dark schedules had been repeat edly altered exhibited worrisome metabolic changes: Within a few days, their glucose levels after meals were dramatically elevated, blood pressures rose, cortisol levels peaked at bedtime rather than upon awakening, and

leptin levels decreased. Leptin is a hormone that suppresses hunger, and low levels stimu late appetite and make people sluggish. All these outcomes are risk factors for diabetes, cardiovascular disease, and obesity.
These and other lab-based findings, Scheer says, help support epidemiologi cal evidence linking nighttime shift work to higher risks for obesity, heart disease, and diabetes that can’t be fully explained by other factors, such as lifestyle or fami ly history. Scheer proposes that nighttime eating habits are at least partly to blame. His team recently reported that nighttime meals disrupted glucose levels and circadian alignments of participants in a carefully controlled study that simulated nighttime work conditions for several days. Partici pants exposed to simulated night work ate at night to mimic typical shift work behav ior, while another group ate during the day.
Scheer and his colleagues tracked central rhythms in the participants by measuring
their endogenous circadian rhythm in core body temperature, a rhythm governed only by the SCN. They also tracked peripheral circadian rhythms in blood insulin and glucose levels.
They found that core body tempera ture was unaffected by evening mealtimes, “meaning your central clock doesn’t care when you eat,” Scheer says. However, among nighttime eaters, the endogenous circa dian rhythm in glucose shifted by about 12 hours. This shift was not seen in the daytime eating group. Glucose levels also differed in the two groups, with levels in those eating at night elevated while their peers in the daytime eating group showed no such increases. Restricting meals to daylight hours thus prevented these effects.
Precisely why nighttime eating boosts glucose levels isn’t clear. Accumulating evidence, however, suggests that delayed
Evidence suggests that delayed mealtimes coupled with the normal increase in melatonin levels at night may play a role in boost ing glucose levels.
mealtimes coupled with the normal increase in melatonin levels at night play a contrib uting role. Scheer’s findings also point to an opportunity: Both day and night workers might minimize their diabetes risk, he says, by eating at times that align better with their circadian biology. Elizabeth Klerman, MD ’86 PhD ’90, an HMS professor of neurology at Massachusetts General Hospital, agrees, adding that this type of evidence helps bring circadian concepts into mainstream medi cine and policy.

Western medicine has long turned a skepti cal eye toward circadian interventions, in part because the results were thought to lack scien tific rigor. Now this is changing. That research describing the inner workings of circadian clocks was deemed worthy of a Nobel Prize was a huge boost to the field, “and people are increasingly starting to do the necessary trans lational and implementation studies,” Kler man says. “We need more proof of efficacy in appropriate populations and conditions for real-world applications of circadian research to be incorporated into health strategies.”
Klerman’s own studies have direct impli cations for obstetrics. With collaborators at Brigham and Women’s, Klerman investigated the relationships between light exposure, melatonin levels in blood, and the frequency of uterine contractions during childbirth. Uterine tissue contains melatonin receptors that are upregulated during late-term preg nancy. Klerman’s findings associated high circulating levels of melatonin with more frequent contractions. Exposure to artificial light — especially the short-wave, blue-green variety — suppresses melatonin, and may therefore have a clinical role in lengthening the duration of labor, with implications for mother, baby, and hospital resources.
Czeisler’s research, meanwhile, has impli cations for improving alertness among the shift workers who arguably need it most: medical residents making life-and-death decisions in the hospital. Shifts lasting 24 hours or more are a rite of passage in medi cal training. But sleep deprivation lowers the alertness and performance of residents, and Czeisler’s own research has shown that it can increase the number of medi cal errors made by residents. Shifts lasting
through the day and night, Czeisler says, require residents to work during circadian phases when their subjective sleepiness is at its highest levels. He and his colleagues recently reported that residents working on shifts capped to no more than 16 hours have better scores on neurobehavioral tests, are not as sleepy, and commit fewer medical errors than residents working longer sched ules. The evidence is still a work in progress, however. In a separate study, Czeisler found that residents working shorter shifts made more medical errors if they were overbur dened with patients. Czeisler points out that the discrepancy confounds the results.
Finally, on the policy side, circadian researchers are weighing in on a looming change that could affect people living in near ly all fifty U.S. states: a congressional move to establish permanent daylight saving time starting in November 2023. A bill called the
Sunshine Protection Act passed in the Senate in March 2022, but has yet to clear the House of Representatives. Daylight saving time begins in spring, when clocks are advanced by one hour so that darkness falls later by clock hour without any change in the amount of sunshine. Then clocks are set back an hour in autumn, thereby restoring standard time. Daylight saving was established decades ago as an energy-saving measure that would cut electrical power use at night — a premise that was later shown not to be true. Those who want to make it permanent say brighter afternoons stimulate more economic activity. Yet daylight saving time has some harmful effects, notably shorter sleep duration, which has in turn been linked to poorer health and cognitive problems. The American Academy of Sleep Medicine, which opposes the bill, has stated that standard time “aligns best with human circadian biology and provides distinct benefits for public health and safe ty.” Klerman agrees, arguing that making daylight saving permanent “is a horrible idea that puts us forever on the wrong time zone.”
While this debate is being played out, researchers and the public are becoming increasingly aware of how circadian rhythms influence health and behavior. Duffy points out that most people who experience jet lag or the consequences of night-shift work “under stand and relate at some level to the influ ence the circadian system has on our bodies and minds.” But behaviors that disrupt our rhythms, she adds, such as keeping irregular sleep schedules, being exposed to artificial light at night, and eating at irregular times of the day and evening, can take a lot of effort to change. Still, over the past two decades, clini cians and experts in other fields have become “accepting and even enthusiastic about pros pects for new countermeasures against the effects of circadian disruption,” Scheer says.
“Important work lies ahead, and there’s a criti cal need for multicenter clinical trials testing the effects of circadian-based treatments. But the tide is turning, and the more we under stand the underlying mechanisms, the better the opportunity to design circadian-based approaches that improve health.”
Daylight saving time has harmful effects, most notably shorter sleep duration, which has been linked to poorer health and cognitive problems.Elizabeth Klerman
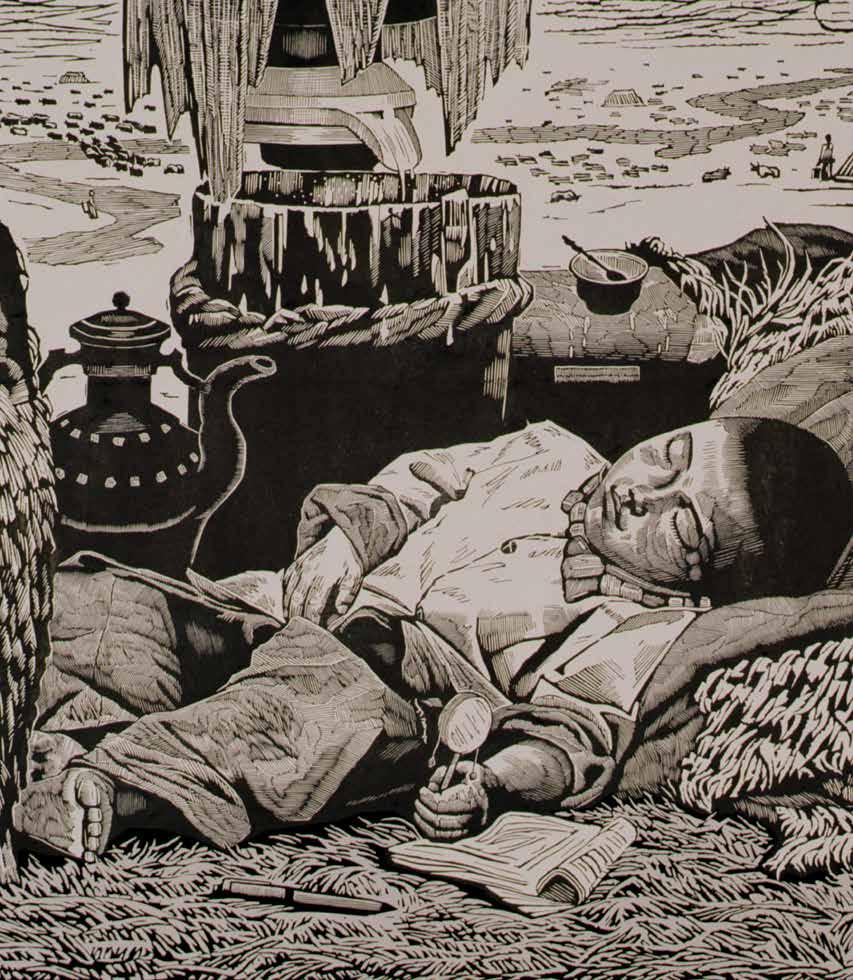

EY PARENTS! Tired of those out-ofcontrol kids, throwing embarrass ing tantrums wherever they go?” starts a YouTube parody video.
“You’ve had it with parenting,” the infomercial-style voiceover exclaims as a fed-up mother shakes her head. “But wait! There is a solu tion! Introducing Naptime! — the latest, most effective tool for child-tantrum prevention!” Cut to scenes of bedraggled parents instantly quieting their children with a few sprays from a bottle full of the fictional product.
With almost 26 million views, the video, written and directed by the cheeky Brooklyn-based producer Chris Capel, has clearly struck a chord. But to millions of parents, naptime is no joke.
“It’s always been one of the huge core issues for people living with infants, toddlers, and small children,” says Perri Klass, MD ’86, a pediatrician and the author, most recently, of The Best Medicine: How Science and Public Health Gave Children a Future. “We go through different cultural moments in terms of where our major anxieties are, but sleep training and sleeping through the night versus daytime napping are a constant.”
According to Matthew Walker, a professor of neuroscience and psychology at the University of California, Berkeley, and author of Why We Sleep: Unlocking the Power of Sleep and Dreams, preindus trial societies in Western Europe, Africa, the Middle East, South Asia, and Latin America arranged their routines around biphasic sleeping. In some regions, people began their “first sleep” when the sun set, waking during the night to read, write, pray, social ize, or have sex and squeezing in a “second sleep” in the hours before chores beckoned at dawn. But Walker writes that this sleep pattern was likely a cultural phenomenon. More often, he writes, “the true pattern of biphasic sleep — for which there is anthro pological, biological, and genetic evidence … is one consisting of a longer bout of continuous sleep at night, followed by a shorter
The quiet of a sleeping child gives little hint of the growth and development going on in the brain
Qijia Dawa (b. 1946) Midday (Zhengwu) Woodcut
midafternoon nap.” Because of this behav ior, children’s sleep patterns were not seen as significantly different from those of grownups, with little ones presumably fulfilling their need for two to ten additional hours a day, depending upon their age, however and whenever they could.
Once factory work came along in the late 1700s, adult schedules began to become more regimented and children’s sleep patterns followed suit. In the years since, advice on child-rearing has become an industry, and scientists have learned more about how much sleep children really need, when they need it, which sleep pattern is best, and what happens to young brains during sleep.
Much is still unknown, but it has become clear that sleep is essential to learning, memory formation, emotional regulation, and physical and mental development and that naps are an essential part of a child’s health and well-being.
Children need a lot of sleep — up to 17 hours a day for infants under three months to 10 hours per night for 18-year-olds, according to the U.S. Centers for Disease Control and Prevention.
While naps count toward total sleep necessary at any age, they play a special role for young children because of the interaction of their circadian rhythms and the homeostatic process known as sleep pressure, or, in lay terms, tiredness. Scientists still aren’t sure why sleep pres sure builds more quickly in children than adults, but some suggest it’s because they usually can’t get 13 or 14 hours of unin terrupted sleep, in part because they must eat frequently, and they need naps to make up for the sleep they don’t get at night.
But there’s more to it than simply getting enough sleep in a 24-hour cycle. Numer ous studies have shown that napping clears the brain — specifically the hippo campus, a seahorse-shaped structure in each hemisphere that plays an important role in learning and memory — so that it can be filled again with new information. Rebecca Spencer, a professor of cognitive neuroscience at the University of Massa
chusetts Amherst, describes the hippo campus as a short-term filing system.
“All the new things you encounter in a day get thrown in there before being sorted into the cortex — which is a bigger, longterm filing system that can sort things by type — during sleep,” she says. “So if you learn grandma used to be a ballerina and you already know she likes to knit, then those two things are integrated into your concept of grandma, which helps you create generalities and also makes each memory easier to find. Kids are constantly bombard ed with new information. They’re not only learning their alphabet, for example, but also that the sky is blue and bunnies are furry — things that adult brains take for granted — so we think their hippocampus just needs to be cleaned out more often.”
Spencer’s research has found that chil dren who nap soon after learning new words, for example, remember the words 80 percent of the time, as opposed to 30 percent for those who don’t nap. Children who don’t nap also score an average of 10 percent lower on word retention tests compared to children who do nap. What surprised Spencer, though, was that the ability to remember what was learned continued into the next day. “What that tells us is that sleep has to take place shortly after learn ing for the learning to take root,” she says.
Emotional memory and reactivity are affected by naps in basically the same way, as any parent confronted by a grumpy toddler knows. “Kids are exposed to emotional
scenarios all morning long,” says Spen cer, “at the level of ‘mom made me put my shoes on and I didn’t want to,’ or ‘I didn’t get my favorite food for breakfast.’ Our studies show that if they take a nap, they’re cool as a cucumber. It gives them a clean slate when they wake up because all the emotional memories from the morning are cleaned out. So if they see a classmate acting up in the corner, they’re less bothered by it. If there’s no nap, the emotional load is never released, and they may overreact too.”
Not getting their naps can cause big prob lems for little kids. “We see attention issues, emotional disruption, academic difficulties, mental health problems, weight gain, even changes in growth,” says Laura De Girolami, MD ’05, a Brookline pediatrician who says she discusses sleep with parents every time they come for a visit. Almost all human growth hormone is produced during slowwave, or deep sleep, which a 45-minute nap is long enough to produce. “Lack of sleep can result in decreased growth hormone secretion and cortisol levels,” De Girolami adds. “I generally don’t tell parents that because it will completely freak them out, and the problem is usually temporary.” Chil dren whose sleep routines are disrupted because of illness, according to Spencer, will often experience a growth spurt once they recover their normal sleeping regimen.
Kids who are already at increased risk for challenging social behaviors may have a
“All the new things you encounter in a day get thrown in the hippocampus before being sorted into the cortex during sleep.”
Spencer’s research has found that children who nap soon after learning new words remember the words 80 percent of the time, as opposed to 30 percent for those who don’t nap.

harder time sleeping, which can then create a vicious cycle resulting in more challeng ing behaviors. And that’s true not just for younger kids. While children mature at different rates, most grow out of the need for a nap by around age 5, but now “we live in such a sleep-deprived culture that naps can be beneficial longer,” says Denise Clark Pope, a senior lecturer at Stanford’s Gradu ate School of Education and an alumna of Harvard’s Graduate School of Education. In 2001, Pope authored Doing School: How We Are Creating a Generation of Stressed-Out, Materialistic, and Miseducated Students.
A paper presented at the American Academy of Pediatrics (AAP) 2019 confer ence found that only about half of U.S. children aged 6 to 17 are getting enough sleep and that those who aren’t are defi cient in measures of “childhood flourish ing,” such as showing curiosity about new things, caring about their schoolwork, staying calm when faced with a chal lenge, and finishing tasks they’d begun.
Research published in Lancet Child & Adolescent Health in July bears this out and highlights the neurological outcomes of insuf ficient sleep. The analysis drew on data from the NIH’s ongoing Adolescent Brain Cogni tive Development study, looking at more than 8,000 9- and 10-year-olds, about half of whom got less than nine hours of sleep a night. The sleep-deprived children had more mental health and behavioral issues than their peers who slept nine or more hours a night and were more likely to be depressed, anxious, and aggressive. Furthermore, brain imaging showed that the less-rested children had a smaller volume of gray matter in the areas of the brain responsible for attention, memory, and inhibition control. And these neurological deficits didn’t diminish quickly; the research ers found that the lower volumes were still evident two years after the initial evaluation.
A 2018 CDC study found that up to 73 percent of high schoolers are getting too little sleep. “In older kids, we know that when this happens bullying goes up,” says Pope, “their abilities to self-regulate and to make deci sions become impaired, and their metabo lism is affected.” One study Pope conducted with more than 135,000 students found that
about 20 percent of teens slept an average of five hours or less at night — about half of the eight to ten hours recommended by the AAP. On top of the problems already noted, this may help explain the spike in ADHD diagnoses since the late 1990s, Spencer notes. “Sleep can improve inhibitory control,” she says, “and that’s the core deficit in kids with ADHD: they lack inhibitory control and sustained attention. Kids with ADHD generally need 45 minutes more sleep to get the same benefit as typically developing kids. So if we find underlying sleep apnea, for example, once that’s treated, ADHDlike behaviors will decrease significantly.”
Teens’ circadian rhythms and school sched ules often work against them. The hormonal shifts that come with puberty make teens stay awake longer — till 11 p.m. or so rather than the 8 p.m. or 9 p.m. bedtimes their younger siblings are probably sticking with. On average, high schools in the United States start around 8 a.m., with some ringing in as early as 7:30. The result is chronic sleep deprivation for the teens. “How often do teachers see kids asleep at school in the library, in lectures, during assembly?” says Pope. “They’re absolutely tired during the day, and then when they go home, they have homework, after-school activities, socializ ing with friends. Many of them have work or family responsibilities, too. Although some of them would really benefit from naps, they don’t always have time for one.”
That coffee shops are now on every corner and energy drink companies are marketing to teens only exacerbates the issue, doctors say, as, of course, does elec tronic media. “Young people have poorer impulse control,” says De Girolami. “Adults might not respond to a text because they know it can wait, but kids don’t feel that way. Especially with apps like Snapchat, where the text is only there for twenty-four hours, and their friends saying, ‘Why didn’t you open my Snap right away? Why didn’t you Snap back?’ This teenage phenomenon of immediacy means you can never get a screen break so your mind can quiet down.”
A 2019 survey by the nonprofit Common Sense Media found that almost a third of teens sleep with their phones in their beds, and a review of twenty studies published in JAMA Pediatrics in 2016 found that use of mobile devices after lights-out was associ ated with less sleep and poorer sleep quality.
“There’s a reason you’re supposed to dim the lights an hour or so before bed,” says Pope, “never mind not looking at your phone. Light suppresses the release of melatonin, which helps induce sleep by calming the brain. But for young people now, checking their phones is Pavlovian.”
Family situations can sometimes disrupt sleep as well, says Klass. “Most physicians are aware that inequities can play out in all kinds of ways both subtle and unsub tle,” she says. “Sleep patterns don’t happen in a vacuum. Is there a quiet place for the child to sleep during relevant hours?
“Kids are sitting for hours on end these days — on buses, in class, maybe at their jobs. The body needs to be active to have better sleep.”
A 2019 survey by Common Sense Media found that almost a third of teens sleep with their phones in their beds.ELISABETH FALL (FACING
It could be way different if the family is in a shelter or renting a single room in someone’s house, or if the parents work nights. I think we’re more aware of these things than we used to be, but we’re prob ably never sufficiently aware of them.”
Pediatric sleep specialists sometimes recommend certain medications to help children with neurodevelopmen tal disorders fall asleep and stay asleep, or, for neurotypical kids, melatonin for a short period until they return to regular sleep schedules after a disrup tion, but most experts prefer the use of natural methods whenever possible.

Young children can sometimes be lulled to sleep at naptime by a caregiver placing a hand on their back, rubbing their feet, or simply sitting beside them, because, as Spencer points out, if they know they’re being watched they’re more likely to settle down. De Girolami actually recommends against naps for teens because they can “just keep the cycle of sleep imbalance going.” Instead, she suggests older kids learn to practice better sleep hygiene, perhaps by meditating, having a bath before bedtime, or sipping chamomile tea. “It’s essentially about having a ritual to cue your body it’s time for bed,” she says. Exercise, too, can make a big difference. “Kids are sitting for hours on end these days — on buses, in class, maybe at their jobs,” says Pope. “The body needs to be active to have better sleep, even though it can seem counterintuitive.”
Parents, these physicians agree, are often yearning for the one right answer, and, as with so many health matters, there simply isn’t one. “Children are really different temperamentally and in terms of patterns,” says Klass. “Anybody who’s had more than one child knows this. You may have an easy kid, a hard kid, a good sleeper who happily naps whenever and wakes up smiling, or one who’s harder to put down and harder to wake up. It’s impor tant not to look at this as a one-size-fitsall situation and to give parents the sense that they’re doing something wrong. Some parents just have a harder assignment.”
 SLEEP
SLEEP
THE GENESIS AND DEVELOPMENT of the field of pediatric sleep medicine in the United States owe much to the work of Richard Ferber, MD ’70. As a co-founder and former director of the Center for Pediatric Sleep Disorders at Boston Children’s Hospital, Ferber was instrumental in introducing clinicians to the ways of identifying and treating children’s sleep problems, from general sleeplessness to more complex medical conditions such as sleep apnea.
Ferber served on the American Board of Sleep Medicine, where he advocated for incorporating pediatric sleep medicine compe tencies into certification exams, and on the board of the American Academy of Sleep Medicine, where he was involved in crafting standards related to research, education, and care in the field. He received the AASM’s Nathaniel Kleitman Distinguished Service Award as well as the organization’s Excellence in Education Award and held positions on three notable journals: an editor of Sleep, an associate editor of Sleep Medicine, and the editor-in-chief of Frontiers in Sleep Medicine. Now retired, Ferber is a correspond ing member of the Faculty of Neurology at Boston Children’s and a founding and continuing member of the HMS Division of Sleep Medicine and its faculty executive committee.
INTERVIEW BY ANN MARIE MENTING FINKENSTAEDTIn addition to these professional accomplishments, Ferber is widely known for his book Solve Your Child’s Sleep Problems, first published in 1985 and revised and expanded in 2006. Compre hensive in content and approachable in style, the book includes discussions of the neurology of sleep, normal sleep rhythms for children and strategies for supporting them, and biological condi tions that might prevent children from getting a good night’s rest.
Harvard Medicine magazine talked with Ferber about his career. What follows is an edited version of that conversation.
A pioneer in the field of pediatric sleep medicine discusses helping children and families get a good night’s rest
HarvardMedicinemagazine: You dedicated SolveYour Child’sSleepProblemsto your two sons, noting that they taught you how to be a parent and reminded you of how important it is to remember being a child. Did the spirit in that dedication express itself in your clinical work?
Richard Ferber: It must have. One of my favorite parts of working in the Center for Pediatric Sleep Disorders at Chil dren’s was working directly with children. When parents would come in with their child, especially if it was a young child, they really didn’t expect me to talk very much to their child or try to solve the problem directly with the child. But I found this direct conversation approach was the most fun and often the most productive, especially when working with a child who had problems going to bed or sleeping through the night. What did the child think they could do to help with their own prob lem, what steps could they take, and what changes were they not ready to accept?
In these situations, I would try to work out a plan directly with the child. Then we would go over it. This repetition would help them remember it, their parents understand it, and the child feel empowered as a planner. The kids were surprised and often really excited about helping to form the plans and pleased that it was not just someone telling them what was going to be done and how. I found this process to be effective.
I obviously couldn’t take this approach in every situation, say, when the child was an infant or when the underlying cause could not be addressed behaviorally, but when I could, and I got the youngster to share in the decision, there was a good chance that things would go well quickly.
HMM: So the treatment became a family effort.
RF: Absolutely. It had to be. The child wasn’t complaining that they were waking up. It was the parents who were concerned and, even more than their child, not getting the rest they needed. I always felt that a sleep-deprived parent could not be as good a parent as one who was well rested. Being able to, in effect, give parents their sleep back while also giving the child their sleep was a goal in most sleeplessness situations.
Sometimes, of course, the problem that parents were observ ing was something that required more extensive treatment than a change in schedule or bedtime sleep practices — disorders like sleep apnea or narcolepsy. But regardless of the specifics of the problem, we would work to identify the root or roots of the problem and devise appropriate treatments or treatment options.
HMM: You mention that helping a family learn what behavior or schedule is normal could lead to a reso lution of a child’s sleeplessness. What would you tell parents?
RF: Often the conversation started with clarifying some misun derstandings about children’s sleep behavior. Many people do not realize that all children wake up occasionally throughout
the night — just as adults do. Sleeping through the night is something of a myth; we all wake up at night, turn over or move around, get comfortable, and then fall back asleep.
A child’s nighttime rousing can resolve itself if the child is allowed to complete the cycle and simply fall back to sleep, espe cially if the child always seems well when checked. But many times, parents intervene and the child becomes accustomed to the intervention, so instead of following the normal course of semi-rousing then falling back asleep, they would seem to require a parent’s intervention. This leads to poor sleep for both child and adult.
Another frequent misunderstanding is what a child’s sleep needs actually are. This can lead to parents’ concerns their child is not getting enough sleep and thus to mistaken concepts of when their child should go to bed at night, how late they should sleep in the morning, and how long they should nap during the day.
As a result, parents may put their child to sleep too early — during the end-of-the-day period of increased wakefulness — or try to get them to sleep too late in the morning or allow them to nap too much during the day. For these children, the night is simply ‘too long.’ Helping parents learn just what normal amounts of sleep are and correcting the schedule could often readily resolve the perceived problem.
The reasonable amount of time that one can expect a child to sleep day plus night varies considerably by age. And bedtime should ideally coincide with when the child feels sleepy: We all have an internal clock that tells our body when it’s time to gear down and rest. Expecting a child to sleep from 7 p.m. to 7 a.m. when they have a ten-hour nighttime sleep requirement can mean it takes them two hours to fall asleep or they wake two hours too early in the morning — or that they are awake for two hours during the night.
The good thing is that the body is built to adapt to a regular and age-appropriate schedule, and children can adapt even more quickly than adults, so once a proper schedule is instituted, a related sleeplessness problem can be resolved.
HMM: The Center for Pediatric Sleep Disorders was the first full-service sleep center in the world devoted to the treatment of sleep problems in children, wasn’t it?
RF: It was. We started it at Children’s in 1978. Sleep medicine as a clinical discipline was relatively new at that time. There might have been around fifteen sleep centers in the country, but all of them were focused on adults. I had done a pediatric internship and residency at Children’s and a fellowship there in psychiatric research that focused on the development of sleep and motor rhythms in infants. I also spent a year at the hospital as the pedi atrician to the psychosomatic unit. I learned a great deal there about how to interact with patients and their families.
It was during the year on the psychosomatic unit that Myron Belfer, then the acting head of the Department of Psychiatry at Children’s; Patricia Boyle, a senior psychologist at the hospital;
The amount of time that one can expect a child to sleep day plus night varies considerably by age.
and I established the sleep clinic. The sleep laboratory was set up at the same time in the Department of Neurophysiology, where Cesare Lombroso took me on to develop and supervise its opera tion. Their interests stemmed from the number of sleep problems they were seeing among patients in their psychiatry program and the frequency with which seizures occurred at night during sleep.
My own interest derived from my work with Peter Wolff, direc tor of psychiatry research and my mentor. It was from him that I gained my interest in all aspects of sleep and sleep rhythms. From him and my studies there, I learned a great deal about sleep in infants and children. I decided that I wanted to focus my career in those areas.
Initially the center’s clinic was in the psychiatry department and the sleep laboratory was in the neurophysiology depart ment. But we were able to combine the program and, later, to greatly expand it.
For a long time, we were basically the only operating sleep laboratory in Boston, and we were referred patients of all ages for study — we might study a newborn one night and a 90-year-old the next. It was an extraordinary opportunity to see the develop ment of sleep across the life span. Eventually, as we built a larger referral base for children, and when Beth Israel Hospital set up its own sleep laboratory for adults, we were able to shift our stud ies to just children.
Operating a sleep program seemed to bring together all my interests: working with children and their families, learning how to develop a specialized history aimed at determining causes, developing new treatment approaches, and using modern tech nology to better understand many of the problems we faced.
HMM: What findings came out of work done at the sleep center that you think helped advance the field of pediat ric sleep medicine?
RF: First, and very fundamentally, the work helped us understand the various causes of sleeplessness in children. Clarifying what was normal sleep, what were normal nighttime wakings, and what habits influenced sleeplessness — overfeeding, needing to be rocked, inappropriate napping, incorrect schedule — turned out to be huge. We also conducted a good deal of research on the disorders of circadian timing for sleep in children.
We found that obstructive sleep apnea was much more common in children than originally thought. Usually, when a physician would see a child in their office and the child looked fine and breathed normally, the doctor would have no idea that the child was having difficulty breathing while sleeping. But our studies, including videos we produced of such children during sleep, helped show other practitioners that obstructive apnea was common. The children had difficulty breathing in sleep just as adults who have obstructive apnea do.
It had long been known that children diagnosed with pediatric obesity-hypoventilation syndrome, also known as Pickwickian syndrome, can suffer from obstructive apnea. We helped show
that obstructive apnea was more commonly present in children because of large tonsils and adenoids, not weight. In our hospital we also saw many children whose obstructive apnea was due to congenital facial abnormalities.
We described and named the disorder of “confusional arous als,” which joined sleepwalking and sleep terrors as a category of so-called arousal disorders. Children who experience these would wake up in the middle of the night, confused and scream ing inconsolably. And in younger children, their behavior more closely resembled confusion or temper tantrums than the terror seen in teenagers and adults. Parents often assumed their children were having nightmares. But a researcher in Canada had already shown that sleepwalking and sleep terrors were incomplete arous als from the deepest stage of nondreaming, or non-REM, sleep and that they had nothing to do with dreaming. The children acted as they did because their arousal systems were being activated but their sleep systems were only slowly giving way to full waking.
Although arousal disorders could be treated with medication, we found that for young children, confusional arousals often had behavioral triggers and could be treated behaviorally. We found that explaining to parents what was happening and reassuring them that it was nothing bad helped them let events run their course with minimal intervention. This helped the child complete the arousal process more quickly and kept the parents from worry.
HMM: I was hoping we could take some time to talk about your days as a medical student at Harvard. What do you recall from that time?
RF: I still remember some of the advice we were given. In particu lar I remember a talk that the late Judah Folkman, MD ’57, gave a group of us at Children’s, long before he became chief of the Department of Surgery at the hospital.
During the talk, he told us the story of a young child on a cancer ward at Children’s who had just died. The child’s father arrived at the hospital, picked up the child, and began walking the halls with the child in his arms. He had walked back and forth but would not relinquish the baby. The staff tried to reason with him to allow them to take the child, but nothing worked. They decided to call another physician at the hospital, one they knew was skilled in such situations. The doctor came and just started walking up and down the hall next to the man who kept hold ing his child. The doctor talked to the father about the child. He mentioned how beautiful the baby was and generally talked about the child as if the baby were still alive. Then he asked the father if he could hold the baby for a while. The father handed the baby to the doctor and then sat down and wept.
That story was very striking to me. It told me you have to understand where the parents are cognitively and emotionally before you can help them and their child.
Ann Marie Menting is the editor of Harvard Medicine magazine.
We might study a newborn one night and a 90-yearold the next.


“The Blavatnik Harvard Life Lab Longwood will be the conduit that takes our science into the world to help humanity.”
— MARK NAMCHUK, EXECUTIVE DIRECTOR OF THERAPEUTICS TRANSLATION AT HMS
Years of dreams and plans came to fruition in October when the School opened a collaborative space for early-stage, high-potential biotechnol ogy and life sciences start-ups with either Harvard or HMS origins. It is a space in which scientific idealism and business pragmatism join forces to improve the health and well-being of people the world over.
Considered a crucible of ideas and a nexus of support for ventures focused on developing new medicines, the Blavatnik Harvard Life Lab Longwood is part of an intellectual ecosystem at HMS dedicated to bringing therapeutics conceived in Harvard labs to the patients who need them.

Together with their partners at LabCentral, a Cambridge-based nonprofit that manages the lab, the leadership of the HMS Therapeutics Initiative and the Blavatnik Life Lab are dedicated to perpetuating the innovative research that the world expects from HMS, allowing the School to expand upon its tradition of taking today’s ideas and turning them into tomorrow’s medicines.
Photography by John SoaresThe HMS Therapeutics Initiative and the Blavatnik Harvard Life Lab Longwood work in tandem to inspire the next generation of scientists, those who will likely play leading roles in developing the medicines of tomorrow.


The Therapeutics Initiative supports the education of graduate students by providing them with the tools and skills that will help them become productive therapeutics researchers.
The Blavatnik Life Lab extends this educational mission by offering fellowships to early- and mid-career researchers from diverse disciplines, and, for faculty seeking to advance their careers in therapeutics research and drug discovery, an academia–industry bridge program that connects HMS experts with their peers in the pharmaceutical and biotechnology industries.

Scientists in the start-ups benefit from an integrated infrastructure and governance provided by the leaders of the Therapeutics Initiative and the Blavatnik Life Lab and their partners at LabCentral. In addition to providing tenants with business-building guidance and expert advisors and mentors from industry and academia, the researchers are located in the heart of the School’s core facilities, several of which can offer the start-ups the highly specialized services, equipment, and staff neces sary for complex biomedical research and translation.



During freshman orientation at Stanford, I heard Andrew Ng from Stanford’s artificial intelligence lab give a talk on AI. He spoke with such enthusiasm about the effects AI would have on our lives. I emailed him, telling him of my hope to get involved in AI research. He invited me to join his lab, which I did during my freshman year. I stayed for the rest of my undergrad career as part of a team building artificial intelli gence for autonomous driving. His lab was a playground with a lot of talented people I worked with and learned from. I found my calling during the second year of my PhD program when I worked at the intersection of AI and medicine: I started building arti ficial intelligence tools to detect abnormal heart rhythms in electrocardiograms and later built AI tools across different medi cal specialties for disease diagnosis, risk prediction, and therapy recommendations.
What do you see as the greatest promises and hurdles of medical AI?
The central promise of medical AI — which is also the mission of my lab — is the idea that AI can safely automate many clini cal decision-making tasks. This should help improve patients’ lives. The quest to develop high-performance medical AI algo rithms that can help doctors in their work is an important pursuit. But designing the consummate AI doctor will require us to tackle challenges on three fronts: algorithm design, dataset curation, and implementa tion design. Right now, high-performance algorithms are built using human-labeled data, but in the future, we will need to lever age the vast swaths of unlabeled data when
designing these algorithms. On the dataset front, we must build ones that work reli ably for a variety of patient populations and clinical settings worldwide. For implemen tation design, the focus rests on enhancing the interaction between the AI algorithm and the clinician so that the AI tools allow clinicians to make optimal decisions. We need to design these systems to extract the good while safeguarding against the bad.
One of my main interests is creating communities around AI and medicine. At HMS, I founded the Medical AI Bootcamp, a joint Harvard–Stanford mentored research program for college students that involves AI in medicine. I also try to bring people into medical AI by curating materials that appeal to any level of interest and background. I’ve taught an online course series on AI and medicine, I co-host the AI Health Podcast, and I co-write Doctor Penguin, an AI and health care research newsletter.
My parents instilled in me a love of science and reading at an early age. My love of research and teaching was shaped by several advisors in AI and computer science, including Ng, Percy Liang, and Michael Bernstein at Stanford, and my longtime mentors in medical AI at Stanford, Matt Lungren, Curt Langlotz, and Eric Topol, the Scripps Research Translational Insti tute founder.
I enjoy walking around Boston, mostly to coffee shops. I also like to cook and try new recipes. I’m currently in the groove of weight lifting but occasionally enjoy golf and tennis.
 —Ekaterina Pesheva
—Ekaterina Pesheva
A conversation with Pranav Rajpurkar, assistant professor of biomedical informatics in the Blavatnik Institute at HMSin JOHN SOARES; JUSTIN CHAN (FACING
DZIFA KPODZO DIDN’T EXPECT to end up in plastic surgery. In fact, she entered HMS “determined not to be a surgeon. It was the only thing I thought I would never do.”

However, that all changed during her first surgical experience, when she placed her hand on a patient’s aorta. “That was it. Feeling some one’s blood circulating under my hand was unbelievable,” she recalls. “People let you into their lives in a whole different way as a surgeon.”
Her training at HMS was the first step in an impressive career arc that recently led to a new job: chief of the Division of Plastic and Recon structive Surgery at Albany Medical College.
Kpodzo describes her experience at HMS as one largely shaped by people: her classmates, who remain close friends and confidants, as well as her many mentors in surgery and medical education at the School. “The common thread was their level of engagement and their passion for education. These are people who are so brilliant and talented, and they took the time to listen and give advice.”
There are many reasons Kpodzo loves plastic surgery: the detail and discipline of the work; the chance to see results unfold before her eyes; and the opportunity to operate on every body part and tissue type. However, asking her why she chose plastic surgery is akin to “asking somebody why they fall in love with someone. It’s this visceral thing. Plastic surgery just fits me.”
Kpodzo considers her patients to be her most important collabo rators. “I have to listen and talk to patients to understand and eluci date and interpret what their wishes are,” she says. She also feels her specialty exists at the intersection of medicine and art: She applies her creativity within the basic surgical parameters to achieve a result that is aesthetic and functional and suits the individual.“Every body has its art,” she explains, and it is her job to connect the two.
This is especially true in one of her surgical passions, top surgery for transgender patients, which usually involves removing breast tissue to achieve a more typically masculine appearance. When performing top surgery, she says, she has the privilege of “helping patients really reflect who they are on the inside. It’s pretty special to come along for that journey.” When Kpodzo first became interested in top surgery, she turned to Richard Bartlett, an HMS assistant professor of surgery, part-time, at Beth Israel Deaconess Medical Center, for additional train ing. One of her current goals is to create a multidisciplinary health care experience for transgender patients.
Kpodzo considers relationships and talking to people to be central to everything she does. Having grown up all over the world, she came to realize that “human beings at their core are pretty straightforward and have consistent desires, beliefs, and values.”This notion, she says, helps her whether she is mentoring a resident or counseling a patient.
Kpodzo credits her mother, who moved from Ghana to Germany to become a dentist and oral surgeon in the 1970s, with showing her what is possible. “There are always challenges for me being a Black woman. I am never the person anybody is expecting in the room. But I think about women like my mother who have paved the way and that’s a huge motivation.”
—Catherine CarusoDzifa Kpodzo, MD ’06 | Chief, Division of Plastic and Reconstructive Surgery, Albany Medical College
COMPETING IN TENNIS since the age of 7 gave Maryann Zhao the “mental fortitude to stay determined and not falter,” she says. “When you’re out there playing on your own, you have to figure out how to solve whatever’s happening in the match at that moment. It gave me the confidence to feel there’s no problem I can’t overcome.”

What led this rising third-year medical student to con sider science as a career was the other side of the same coin. “There’s a lot of problem-solving in science,” she says. “There’s so much in science that is not yet understood, and as a researcher you’re trying to figure out how the world works. That part is really satisfying to me.”
Zhao had always done well in her science classes in middle school and high school, but it wasn’t until her undergrad years at Pomona College, a small liberal arts institution in Clare mont, California, that her future came into focus. “I took biology, chemistry, math, physics, computer science, and eco nomics,” she says, “but my real interest was in how science affects people and their health, so that started pushing me toward pre-med.”
As the daughter of parents born in China — her father has a PhD in physics and her mother has worked as a software engineer — Zhao volunteered for a program called Health Bridges, which helps new immigrants in the emergency department gain access to health insurance.
She got involved with Partners In Health and learned more about advocacy, community outreach, and global health, including “what it means to advocate for patients, to make calls to Congress, to organize people at a grassroots level.” She and her classmates started talking about how physicians can influence politics after witnessing the inequities exposed by COVID.
“As physicians,” she says, “we’re privileged to be able to connect with patients and hear what issues are impacting them most and then advocate for change to improve those issues. Medical students come in with bright eyes seeing things they want to change, but it’s hard to actually have the skills to make a change on a systemic level.”
Zhao believes it’s important to enhance medical students’ policy and political literacy and “pull back the curtain on the political process.” She’d like to see the “innovative research” being done in areas like gene therapy translate into helping more people. “These innovations are incredibly expensive when they hit the market,” she says. “How can we ensure that the very patients these therapies are designed for are able to access them?”
She sees her future as a clinician involving some aspect of research and interaction with the legislative process to influ ence policy as an expert in her field. “What that field is going to be is something I’m still trying to figure out,” she says.
—Elizabeth Gehrman“IN COLLEGE I WAS INTERESTED IN science but also in social science and public policy,” says Inam Sakinah, a rising thirdyear medical student. “I wanted to approach my future less in terms of what title I wanted to hold than what problems I wanted to solve.” She chose to get an MD because she saw it as placing her at the intersection of medicine, health policy, and advocacy — and she chose HMS because when she inter viewed at the School, “one of the administrators talked about the concept of the ‘physician-and.’ He said, we want you to practice medicine but also go beyond that to make a differ ence in another field that can benefit the lives of your patients. That’s what I was looking for.”
Sakinah comes by her advocacy bent naturally. Her parents were both “on the front lines of civil rights efforts working to protect our rights as Muslim Americans,” Sakinah says. Watch ing them work on humanitarian and civil rights advocacy initia tives — and discussing the issues that led to their actions with her and her younger brother during family dinners — gave her a clear sense that she wanted a career working toward a more equitable country.
She built a mentorship program for a low-resource school in Gadsden County, Florida, and worked in the Florida Department of Health as one of twelve college students selected statewide for a gubernatorial fellowship. A service trip she led in college was especially formative for it brought her to the Edmund Pettus Bridge in Selma, Alabama, on the 50th anniversary of the Bloody Sunday march from Selma to Montgomery. “It crystallized for me,” she says, “that we have a collective responsibility to bring the promise of America into being.”
While in pandemic lockdown at HMS, Sakinah helped found Future Doctors in Politics, along with Anjali Misra, Maryann Zhao, and several other classmates, and she serves as the group’s national president. “COVID-19 forced a reckoning among a new generation of students to think of the consequences of not advocating,” she says. “We saw in stark terms that the decisions our politicians make can often have a bigger impact on patient outcomes than anything physicians do at the bedside.”

She thinks the joint MD-MBA she’s pursuing will be crucial in moving toward her ultimate goal: to establish an ideas lab that will “position physicians with the advocacy, leadership, and man agement skills to drive progress toward equity in health care.”
“If we train the next generation of physicians to have the mindset and skillset to be physician-advocates, we can empower them to be the change we need to ensure better, more equitable health outcomes for all.”
—Elizabeth Gehrman“MY PARENTS HAVE DEFINITELY had a big influence on me,” says third-year medical student Anjali Misra. Her mother, a journalist, taught her “how every interaction is an oppor tunity to learn someone’s story.” Her father, a physician in India before moving to the United States, was working as a gastroenterologist in Cedar Rapids, Iowa, when he died unexpectedly. Misra was still in high school. “It’s hard for me to talk about that,” she says. “But his empathy for and understanding of his patients is something I continually try to emulate. His people skills — special doesn’t seem like a big enough word to describe them. He gave so much to his patients, but it was also clear how much he got out of his work.”
Misra came to Boston to attend MIT, where she received her bachelor’s in brain and cognitive sciences and worked with the mobile clinic The Family Van and in a student-run ambulance service. Then, a Mitchell Scholarship, which aims to facilitate connection between Ireland and the United States, took Misra to the Emerald Isle. “I always had an interest in rural medicine and in learning about health systems that are different from our own,” she says, “so I got an MPH at University College Cork. I wanted to be primed to understand the bigger picture all the way through medical school.” She also solidified her interest in emergency medicine while overseas, working as a certified EMT.

At HMS, her paths are coalescing. “There’s often a separation between public health and emergency medicine,” she says, “but they come together downstream, when people end up in the emergency department with something that could have been prevented. Better understanding the care people receive outside of the hospital will help us care for them when they end up in the ED. This ties in with my interest in legislative advocacy and politics, which are major factors that shape health.”
Misra believes emergency medicine physicians can be effec tive policy advocates because “they see so much of what is hap pening in the community and affecting people’s health,” she says. The ED is also a good place to reach patients without creating barriers. She cites Vot-ER, an organization founded by an HMS graduate that works to integrate voter education and registra tion into health care settings, as a perfect example of the kind of bridge that can be built during hospital visits. “Emergency departments can make things accessible, available, and easy,” she says. “I get excited thinking about that.”
Misra says that being an advocate is “just as important to me as being a clinician. I plan to continue to engage in public health research and legislative advocacy throughout my career.”
—Elizabeth GehrmanNiyi Odewade, Bezaye Teshome, and Aser Abrha (left to right) have their Match Day results captured for posterity.

Andrew Bartuska Stanford Health Care
Mary Decker Brigham and Women’s Hospital
Agustin Oneto Massachusetts General Hospital
DERMATOLOGY
Travis Benson Hospital of the University of Pennsylvania
Sidharth Chand University of California Irvine Medical Center
Michael Chang Massachusetts General Hospital
Bina Kassamali Massachusetts General Hospital
Michelle Lee Massachusetts General Hospital
Danny Linggonegoro Stanford Health Care
Renajd Rrapi New York University Grossman School of Medicine
Jordan Said Stanford Health Care
EMERGENCY MEDICINE
Aser Abrha Massachusetts General Hospital
Maya Ball-Burack (facing camera) hugs a classmate after receiving her Match Day news.

Hannah Bougleux Gomes Massachusetts General Hospital
Sarah-Ethel Justus Beth Israel Deaconess Medical Center
Cray Noah UCLA Medical Center
Niyi Odewade Brigham and Women’s Hospital
David Severson Duke University Medical Center
Julia Song Brigham and Women’s Hospital
Benjamin Vierra University of Washington Affiliated Hospitals
Aaron Wickard Naval Medical Center San Diego
Alice BosmaMoody Brigham and Women’s Hospital
David Bunn Brigham and Women’s Hospital
Fang Cao Stanford Health Care
Jennifer Cloutier Massachusetts General Hospital
Sam Doernberg Brigham and Women’s Hospital
Parsa Erfani Brigham and Women’s Hospital
Sanjay Raaj Gadi Duke University Medical Center
Reid Grinspoon New YorkPresbyterian Hospital/Columbia and Cornell
Thuy-Lan Lite Massachusetts General Hospital
Derek Liu Stanford Health Care
Karine Liu Massachusetts General Hospital
Albert Park Stanford Health Care
Alexandra Pourzia Stanford Health Care
Rifat Rahman New YorkPresbyterian Hospital/Columbia and Cornell
Azucena Ramos Massachusetts General Hospital
Farees Saqlain Hospital of the University of Pennsylvania
Henry Ashworth Alameda Health System-Highland Hospital
Samuel Lyon Augusta University
Emily Witt Massachusetts General Hospital
INTERNAL MEDICINE
FAMILY MEDICINE
Mara Farcasanu Cambridge Health Alliance
Maahika Srinivasan Hospital of the University of Pennsylvania
Moustafa Abdalla Massachusetts General Hospital
Chukwuma Eruchalu Massachusetts General Hospital
Radhika Agarwal Brigham and Women’s Hospital
Yuri Ahuja New York University Grossman School of Medicine
Chidiebere Akusobi Massachusetts General Hospital
Lestat Ali Massachusetts General Hospital
Caroline Behr University of Colorado School of Medicine
Catherine Gutierrez Massachusetts General Hospital
Kristi Hill
The Johns Hopkins Hospital
David Iskhakov Massachusetts General Hospital
Sebastian Koochaki Brigham and Women’s Hospital
Kameron Kooshesh Massachusetts General Hospital
Dylan Kotliar Brigham and Women’s Hospital
Juhi Kuchroo Brigham and Women’s Hospital
Rebecca Lewinsohn Stanford Health Care
Sarah Shareef DartmouthHitchcock Medical Center
Jiunn Song Massachusetts General Hospital
Bruce Hamilton Tiu Stanford Health Care
Nishant Uppal Brigham and Women’s Hospital
Julie Urgiles New YorkPresbyterian Hospital/Columbia and Cornell
Lianet Vazquez Massachusetts General Hospital
Zain Virk Vanderbilt University Medical Center
Leia Wedlund New YorkPresbyterian Hospital/Columbia and Cornell
Ottavia Zattra Hospital of the University of Pennsylvania
Jade Connor Massachusetts General Hospital
Jonathan D’Gama Brigham and Women’s Hospital
Suhas Gondi Brigham and Women’s Hospital
Catherine Mankiw Brigham and Women’s Hospital
Smiles abound as Chidiebere Akusobi, Jiunn Song, and Catherine Gutierrez (left to right) display the letters announc ing where they matched for their residencies.

Justin Reynolds Yale New Haven Hospital
Raquel Sofia Sandoval Johns Hopkins Hospital
Hannah Smati Baylor College of Medicine
Derek Soled Brigham and Women’s Hospital
Suk Joon Lee Massachusetts General Hospital
William Curley Brigham and Women’s Hospital
Mark Nagy University of Colorado School of Medicine
Milana Bochkur Dratver Hospital of the University of Pennsylvania
Ashley Goreshnik Yale New Haven Hospital
Kimberly Schaefer Oregon Health and Science University
Bezaye Teshome Northwestern University McGaw Medical Center
Ryan Sameen Meshkin Massachusetts Eye and Ear
Jade Moon University of Minnesota
OBSTETRICSGYNECOLOGY
Emily Adams Johns Hopkins Hospital
Sonya Bharadwa Northwestern University McGaw Medical Center
Mugdha Mokashi Northwestern University McGaw Medical Center
Juliet Musabeyezu Brigham and Women’s Hospital
Ayotomiwa Ojo Northwestern University McGaw Medical Center
Caitlin Radford New York-Presbyterian Hospital/Columbia and Cornell
Yuexin Wang University of Washington Affiliated Hospitals
Sanchay Gupta Baylor College of Medicine
Omar Halawa Wilmer Eye Institute
Edward Lu Massachusetts Eye and Ear
Blake Oberfeld University of Florida
Rachel Tandias Massachusetts Eye and Ear
Christine Xu University of California, Davis
Paul Zhou University of California Irvine Medical Center
Samuel Finlayson University of Washington Affiliated Hospitals
Yonina Frim Massachusetts General Hospital
Jon Hochstein
Boston Children’s Hospital
Pinky Langat Boston Children’s Hospital
Hannah Olsen Boston Children’s Hospital
Olivia Plana Children’s National Medical Center
Alexander Pomerantz Boston Children’s Hospital
Sigurast Olafsson New York University
Grossman School of Medicine
Catherine Wu University of California Irvine Medical Center
Andrew Chun Massachusetts General Hospital
Josie Francois Brigham and Women’s Hospital
Shadaab Kazi Cambridge Health Alliance
Alexander Reed Stanford Health Care
UROLOGY
Maheetha Bharadwaj University of Washington
Logan Briggs Mayo Clinic
Wesley Chou Oregon Health and Science University
Thomas Hwang Brigham and Women’s Hospital
Felix Hong Massachusetts General Hospital
Elaina Pullano Massachusetts General Hospital
Sarah Wicheta Massachusetts General Hospital
SURGERY
Mihir Dekhne Hospital for Special Surgery
Aliya Feroe Mayo Clinic School of Graduate Medical Education
Rachel Flaugh Hospital of the University of Pennsylvania
Bailey Ingalls University of Washington Affiliated Hospitals
Fatima Mubarak Baylor College of Medicine
Atousa Nourmahnad UCLA Medical Center
Evan Stieler Massachusetts General Hospital
Lillian Dattilo Massachusetts Eye and Ear
Anne Feng Rutgers New Jersey Medical School
Betzamel Lopez University of Miami/ Jackson Health System
Kameron Kooshesh (left) and Bailey Ingalls flash the “I Matched!” cards that detail the specialty and institution in which they will train.

Elizabeth Noyes Massachusetts Eye and Ear
Annette Wang University of Maryland Medical Center
PATHOLOGY
Katherine Latham Massachusetts General Hospital
Hannah Resnick Massachusetts General Hospital
Edgar Garcia Saiz Boston Children’s Hospital
Katherine Shaffer University of Washington Affiliated Hospitals
Priya Shah Children’s Hospital of Philadelphia
Mimi Yen Li University of California San Francisco
Ricky Madhavan Yale New Haven Hospital
Margaret Okobi University of California San Francisco
Samuel Petrie Vanderbilt University Medical Center
OTHER Melaku Arega Bain Capital Life Sciences
Shivangi Goel Iterative Scopes
Natalie Guo Thrive Capital
Travis Hughes nference
Alexander Munoz Boston Consulting Group
Maya Ball-Burack University of Washington Affiliated Hospitals
Okechi Boms Hospital of the University of Pennsylvania
Kendall Carpenter Boston Children’s Hospital
Allison Fialkowski Boston Children’s Hospital
PHYSICAL MEDICINE AND REHABILITATION
Gregory Galeazzi Spaulding Rehabilitation Hospital
Grant Schleifer Spaulding Rehabilitation Hospital
Ken Chang Stanford Health Care
Moses Flash Hospital of the University of Pennsylvania
Showly Nicholson Massachusetts General Hospital
Michael Snyder Northwestern University McGaw Medical Center
Nathan Nakatsuka New York Genome Center
Emory Werner RA Capital Winston Yan Arbor Biotechnologies
Institutions listed represent categorical residency matches and their locations. Locations of prelimi nary or transitional programs are not included.
What book has had a profound influence on you, professionally or otherwise?
Thinking, Fast and Slow, by Daniel Kahn eman. This is a summary of Kahneman’s research that led to his receiving the 2002 Nobel Prize in Economics. It is a fascinating reminder of the mistakes we all make in the process of critical thinking, often the result of old habits, inherent biases, and resorting to common heuristics. I use examples and anecdotes from the book when teaching second-year medical students as they make their transition from the basic science years into their clinical rotations, where clinical reasoning becomes so important. The book fosters the discipline to always stop and think slowly about the validity of one’s criti cal analysis of complex problems.
Cancer Ward, by Aleksandr Solzhenitsyn; General Pathology, by Howard Florey; Mechanisms of Disease, by Ruy PérezTamayo; Pathology of the Kidney, by Robert Heptinstall; and many, many more.
Nneka Azikiwe Holder, MD ’97
Caste, by Isabel Wilkerson. It reframes the conversation about racism and is a much better explanation of how systemic it is and why it continues to exist.
Jan Polissar, MD ’61
Years after graduation, I’m OK—You’re OK, by Thomas Harris, and What Do You Say After You Say Hello, by Eric Berne, finally made sense of psychiatry, my chosen field. I also greatly appreciated the twenty-fourvolume collected works of Sigmund Freud, which won the Goethe Prize in 1930.
The Unwinding of the Miracle, by Julie YipWilliams. I read this book because she and I are both Williams College alums. Thank God I did. It is her memoir of her fiveyear battle with colon cancer. There was no happy ending; this brilliant, talented woman died at age 42. Brilliant writing deal ing with hopes, dashed hopes, joy, anger, family dynamics, interactions with her docs. This is a must-read for any physician. Keep a hanky nearby.
A book I have given, perhaps at this point a dozen times, to medical students, other doctors, or bright youngsters interested in medicine, art, history, life: The Heal ing Hand: Man and Wound in the Ancient World, by pathologist Guido Majno, one of our very best teachers at HMS. Try to find the hardcover—the better to enjoy the illus trations. And try to experience medicine, art, and life as he did.
Ellen Weber, MD ’83
Heartsounds: The Story of a Love and Loss, by Martha Weinman Lear. This is the true story of a middle-aged physician who has a major heart attack with subsequent severe heart failure. His wife, the author, describes not just the terrifying course of his disease but the profound lack of empathy and atten tion they received from his physicians. As
you go through med school and intern ship, it is easy to get tired and cynical. This book will remind you why you became a physician and will keep you listening to your patients.
William Goodson, MD ’71
These books illustrate how to learn from stories. The Early Diagnosis of the Acute Abdomen, by Sir Zachary Cope, explains the skill of diagnosis using a history and a physical before everyone just ordered a CAT scan. From Fish to Philosopher: The Story of Our Internal Environment, by Homer Smith, posits that kidneys are necessary for philosophers to sit around talking, details the evolution of the kidney, and answers the lifeboat question on the renal exam. Hint: Give away the vintage wine and drink the beer for hydration.
Beyond Halftime: Practical Wisdom for Your Second Half, by Bob Buford. This book helped me adjust to my retirement after 30-plus years as a general surgeon. The main message is that one needs to transi tion from success to significance (i.e., pay it forward by sharing your experience with younger colleagues).
There are many books, but one object that profoundly influenced me was a small porce lain that my chairman of medicine, Walter Bauer, had gracing his desk. It was of a child kneeling down, perhaps to look at an ant on the sidewalk. It epitomized his advice, that one should always have the curiosity of a child.
Madeleine L’Engle’s A Wrinkle in Time describes an impossible quest by helpless children, a clinging to family and love in the face of an overwhelming darkness, no one saves you but you—these are themes I keep returning to over and over in my life, professionally and personally.
The Rack, by A.E. Ellis; it’s a sanatorium/ disease novel. The subject is human suffering.
To better understand Russia and its ruthless leaders, The Sinner and the Saint: Dostoevsky and the Gentleman Murderer Who Inspired a Masterpiece, by Kevin Birmingham.
Stephen Grund, MD ’91
The House of God, by Samuel Shem (Stephen Bergman, MD ’73). I read it between my first and second year of med school. I was so dismayed by it that I told my wife I had made a big mistake (I hadn’t). The wisdom of the Fat Man helped me navigate medical school, residency, and fellowship relatively unscathed and not surprised or shocked by anything I witnessed. Also read his followup book Mount Misery, about his psychia try residency at McLean. I used humor to get me through and not take everything to heart.
Michael Quinones, MD ’86
The House of God, by Samuel Shem. The absolute irreverence and the fact that the characters were based on real-life attend ings made it a nice break from the reality of the hard work we needed to do.
James MacDonald, MD ’96
There are many books: No one book would fit here. But I think two which come to mind are Graham Greene’s The Quiet American and Robert Penn Warren’s All the King’s Men, both of which I have read over five times. They are always relevant. In The Quiet American we declare ourselves “the greatest country ever” and a champion of democ racy but we wreak havoc too often. All the King’s Men is a wonderful description of the power and danger of populism in Ameri can democracy.
Kenneth Bridges, MD ’76
Blindspot: Hidden Biases of Good People, by Mahzarin Banaji, addresses the issue of intrinsic biases arising from the racial chasm in the United States. Most people have an inward feel for their conscious racial biases although they may avoid admitting them. Unfortunately, a thoughtful desire to be nonracist does not necessarily eliminate negative behavior around race. Blindspot highlights the ways in which intrinsic bias molds social interactions and shapes rela tionships, thoughts, and actions.
Ann Cathcart, MD ’21
Nina Riggs’ The Bright Hour: A Memoir of Living and Dying. As a mother, my heart is always torn when I kiss my son goodbye in the morning before putting in the long hours that a career in medicine requires. But I have found a calling in helping other mothers have more time and better time with their children. Riggs’ gorgeous post humously published memoir of living with incurable breast cancer illuminates and motivates that calling.
Kenneth Franklin, MD ’78
Sapiens: A Brief History of Humankind, by Yuval Noah Harari. It lifted my gaze again to the big picture.
Bruce Barnett, MD ’75
Doctor and Patient is a collection of essays by Francis W. Peabody, MD 1907, that includes his highly regarded 1926 address to students at HMS, “The Care of the Patient.” His words, “the secret of the care of the patient is in caring for the patient,” have informed me and guided my practice.
George Hill, MD ’57
John Farquhar Fulton’s Harvey Cushing: A Biography. In 1950, I was taking embryol ogy as a sophomore at Yale. The graduate student who was guiding us thought I would be interested in Cushing’s career and loaned me his copy of Fulton’s book. I was hooked. I wanted to follow Cushing from Yale to HMS and then to become a surgeon at the Brigham. At HMS, I learned that Cushing was a bril liant man but also a man with personal flaws.
“Most people have an inward feel for their conscious racial biases although they may avoid admitting them.”
Craig Comiter, MD ’92
Born a Crime: Stories from a South African Childhood, by Trevor Noah. This book made me realize how all races can be discrimi nated against for absolutely no reason.
George Lewinnek, MD ’67
Everyone should look at the Handbook of Epictetus for an idea of Stoic philosophy. Erik Erikson’s Childhood and Society is a wonder ful and humbling look at the values of soci eties other than our own. The Spirit Catches You and You Fall Down: A Hmong Child, Her American Doctors, and the Collision of Two Cultures, by Anne Fadiman, looks at the Hmong people in California. A recent book I read, The Price of Peace: Money, Democ racy, and the Life of John Maynard Keynes, by Zachary D. Carter, gives an economic perspective on the history of the past century that expanded my view.
Mark Hochberg, MD ’73
Forgive and Remember: Managing Medi cal Failure, by Charles Bosk. As a cardiac surgeon, I could not help feeling personally responsible for the death of every patient of mine. I cannot remember the more than 3,000 successes, but even now I can recite the names of most of the mortalities. When ever guilt overwhelmed me, I pulled this book out. It was given to me by my mentor, Judah Folkman, MD ’57, at HMS gradua tion. I was not sure then why Judah gave it to me, but I now regard it as an incredibly thoughtful gift.
So many, but two that immediately come to mind are Evelyn Waugh’s Brideshead Revis ited, which I have read perhaps ten times in my life. This quotation has always stuck with me: “To know and love one other human being is the root of all wisdom.” Heirs of General Practice, by John McPhee, is the book that motivated me to enter family medicine, and I’ve never regretted it.
The Cry and the Covenant, by Morton Thompson, was an old book by the time I read it as a teenager, but the story of how Ignaz Semmelweis saved so many lives by reducing deaths from puerperal fever despite having his findings rejected and ridiculed for years remains in my memory as a story of the power of simple observa tion and perseverance.
Few of us had time for nonmedical read ing while at HMS or as residents. Now that those years are in the past, I try to read nightly for an hour or two after dinner. The Story of San Michele, by Axel Munthe, should be read by every physician. First published in 1929 and written by a physi cian who shared memories of Pasteur and Charcot, it describes diseases we no longer see. Preet Bharara’s Doing Justice: A Prosecu tor’s Thoughts on Crime, Punishment and the Rule of Law gives insight into the criminal justice system from a learned and empa
thetic attorney. Jonathan Sacks’ Morality: Restoring the Common Good in Divided Times is a thought-provoking work by the late chief rabbi of Great Britain. Harriet Washington’s Medical Apartheid: The Dark History of Medical Experimentation on Black Americans from Colonial Times to the Pres ent shows the poor care afforded African Americans in the nineteenth century and, lamentably, into our time. Lawrence Muel ler’s Jungle Surgeon describes the effect that a volunteer surgeon had while working under adverse circumstances. Learning something new or being introduced to a different insight is enhancing.
Robin Yuan, MD ’78
I must selfishly say the books that have influ enced me the most were books I authored on midlife, cosmetic surgery, marriage, and my grandfather. They forced me to organize experiences and thoughts on these various topics that shaped the way I live, how I prac tice plastic surgery, and how I remember my family and ancestors. Outside of that, the classic book Principlization of Plastic Surgery, by my mentor D. Ralph Millard, MD ’44, gives structure to life as a plastic surgeon and a human being.
Thanks to all who shared recollections of books that have been influential in your personal or professional life.
We hope you will share your thoughts on some of the upcoming questions: How would you most like others to remember you as a physician? and What skills would you recommend clinicians learn today to better prepare for tomorrow? Responses for these will appear in print, online, or both in the coming months.
Responses can be submitted online: hms.harvard.edu/rounds or via email: hmsalum@hms.harvard.edu.
1940s
1943
McLemore Bouchelle, MD January 3, 2016
1947
Fred D. Fowler, MD April 19, 2022
1948
Modestino Criscitiello, MD June 24, 2022
John A. MacLeod, MD February 25, 2022
Clarence T. Thompson, MD June 17, 2022
1949
Louis D. Browning Jr., MD February 4, 2022
1950s 1950
Hart Achenbach, MD March 10, 2022
Renee Gelman, MD June 1, 2022
1951
Hoke V. Bullard Jr., MD June 19, 2022
1952
John J. Martin, MD March 22, 2020
David P. Michener, MD January 17, 2022
John B. Thomas, MD July 14, 2022
1953
Aaron B. Stevens, MD January 13, 2022
1954
Richard B. Cattell, MD November 15, 2020
James E. Cavanagh Jr., MD May 7, 2022
Edgar R. Miller Jr., MD February 19, 2022
1955
Maurice B. Burg, MD April 24, 2022
James A. Greene Jr., MD June 14, 2022
Hugh McDevitt, MD April 28, 2022
Walden B. Whitehill, MD June 7, 2022
1956
Francis A. L’Esperance Jr., MD February 1, 2022
Anthony P. Monaco, MD August 22, 2022
James Snow, MD May 28, 2022
1957
Manuel G. Herrera-Acena, MD January 19, 2022
John L. McNay Jr., MD June 19, 2022
Richard A. Norton, MD June 9, 2022
1958
Donald Butterfield, MD May 21, 2022
Murray Goldstone, MD July 18, 2022
Sheila Hafter Gray, MD December 21, 2021
George A. Jacoby Jr., MD February 14, 2022
Charles S. Kahn, MD April 9, 2022
John W. Madden, MD March 10, 2022
Rudolph W. Pierce, MD March 22, 2022
Irene L. Solomon, MD May 20, 2022
1959
Carl M. Beiles, MD March 28, 2022
Walter T. Gilsdorf, MD May 6, 2022
Arthur B. Kieger, MD March 23, 2022
William Reed, MD May 24, 2022
Gordon Murray Shepherd, MD June 9, 2022
Carl G. Silverman, MD April 24, 2022
1961
Alan B. Gazzaniga, MD June 17, 2022
Glenn Y. Lee, MD March 30, 2022
Royce Moser Jr., MD March 26, 2022
1962
William M. Colaiace, MD February 26, 2022
Robert G. Dluhy, MD May 25, 2022
1963
Jaime Gutierrez-Gongora Jr., MD October 4, 2021 1964
Elmer M. Cranton, MD November 28, 2021
Rob Roy MacGregor, MD May 12, 2022
1965
Kirk Avent, MD July 1, 2022
Stephen R. Crespin, MD January 29, 2021
1968
J. Kathleen Greenacre, MD March 25, 2022
Daniel Onion, MD July 6, 2022
William Ensminger, MD March 11, 2022
Jay Gold, MD June 1, 2022
1977
Stephen D. Thompson, MD February 15, 2021
Armando Samaniego, MD May 21, 2022
Preston J. Phillips, MD June 1, 2022
1960s
1960
Richard R. Kelley, MD February 24, 2022
Robert E. Kleiger, MD January 21, 2022
Edward B. Gilmore, MD August 8, 2022
1967
Mark S. Horwich, MD January 20, 2022
This listing of deceased alumni includes those whose notices of death were received between March 1 and August 31, 2022.
“RESOLVE” AND “RESILIENCE” BEST CAPTURE the spirit of the Spring 2022 meeting of the HMAA Alumni Council. Throughout the year, I was humbled by the unstinting dedication of departing Council members Oni Blackstock, MD ’05, Tamara Calla han, MD ’95, Carmon Davis, MD ’90, Erik Gaensler, MD ’84, Elizabeth Garner, MD ’94, Tim Russell, MD ’74, Nina TolkoffRubin MD ‘68, and student representative, MD candidate Nicky Joseph. Typical of this great alumni body, however, new councilors are poised to move our mission forward. Resolve.
Members reflected on the loss of the innovative and resource ful leadership of Paul Farmer, MD ’90 PhD ’90, and the establishment of a memorial scholarship fund in his name. At the same time they were heartened by the creativity of Council student representative and MD candidate Lash Nolen whose We Got Us commu nity empowerment project weaves a tapestry of support organizations into a coherent force for health care education, awareness, and activism. Resilience.
Dean George Q. Daley, MD ’91, reviewed the HMS Vision for 2040, which includes the Blavatnik Harvard Life Lab Longwood. This facility will cement the School’s leadership as a builder of partnerships between academia and industry in the life sciences. Moreover, anticipated Gordon Hall renovations, which highlight accommodations for flexwork and other sweeping hybrid workplace changes, will ensure HMS retains and attracts a work force that will sustain its continued primacy in health care innovation and implementa tion. The reimagined Countway Library embodies the emerging work/study/relaxation concept for communal spaces with meditation rooms, holographic anatomy projections, and parallel study spaces that join computer stations with the venerable stacks of journals and books (accessible at https://bit.ly/3rrrIZF).
The dean also reflected on the sobering Report of the Presidential Committee on Harvard & the Legacy of Slavery. Unvarnished and searing, the report goes beyond a tally of bondsmen held in Cambridge and highlights a lasting legacy that includes Harvard endowments derived from fortunes amassed from the sweat and suffering of enslaved men, women, and children. Addressing lingering effects will require resolve.
Persistent underrepresentation of people of color at HMS is one lingering effect of that legacy. It is a problem that is being tackled resolutely. Led by Andrea Reid, MD ’88, associ ate dean for student and multicultural affairs, a new mentoring partnership between the Office of Recruitment and Multicultural Affairs and HMAA already is paying dividends, with a webinar for premed students drawing 27 alumni, 6 HMS students, and 167 premed students from thirty-eight different institutions, including at least five historically Black colleges and universities. A networking event for alumni and HMS students from underrepresented minority groups included thirty-four alumni and forty-nine students. Participants in both events were enthusiastic; future participation surely will grow. The partnership will explore additional in-person connections and mentorship opportunities that can enrich the HMS experience for all, exemplified by the advocacy and mentorship work of DeWayne Pursley, MD ’83 (Class of 1982), for which he received the 2022 Distin guished Service Award for HMS Alumni. Resilience.
Our spring meeting was the first in-person program in two years but prudent safety measures allayed concerns and rewarded attendees with an event that warmed the hearts of all. Resolve and Resilience.
Kenneth Bridges, MD ’76, is vice president of external affairs for Global Blood Therapeutics, Inc., in South San Francisco.

Are you inspired by a peer who deserves recognition for their dedication to the School? The Alumni Council is seeking nomi nations for the 2023 Distinguished Service Award for HMS Alumni. This award was established in 2019 to recognize MD alumni who have demonstrated loyalty, service, and commit ment to HMS through volunteering, community building, service as an ambassador for the School, or otherwise sup porting HMS and its mission. Submit your nomination by December 31 at alumni.hms.harvard.edu/nomination.
MD graduates selected six new Alumni Council members during the 2022 election. Three of the individuals will repre sent the third (classes of 2007–2011), sixth (1992–1996), and tenth (1976 and beyond) pentads, respectively: Kristy Rialon, MD ’08; Elbert Huang, MD ’96; and Douglas Zipes, MD ’64. Michelle Rivera, MD ’92, will represent all classes as councilorat-large. Louise Aronson, MD ’92, was selected as the presi dent-elect, and Chasity Jennings-Nuñez, MD ’95, will serve as vice president. Learn more about the new representatives at alumni.hms.harvard.edu/election
Philanthropic support from 2,688 alumni enabled our faculty, staff, postdocs, and students to continue their unremitting pursuit of the School’s mission to alleviate suffering and improve health and well-being for all. MD alumni can view each class’s Honor Roll of Donors — the lists of individuals who made gifts during fiscal year 2022, which ran from July 1, 2021, to June 30, 2022 — at alumni.hms.harvard.edu/honor-roll.
Classes ending in “3” and “8” are celebrating June 1 – 3. Join your Reunion Committee to help plan a personalized class event and encourage your classmates to participate in 2023 activities. For more information, contact the alumni engage ment team at 617-384-8520 or hmsalum@hms.harvard.edu
Following the death of Paul Farmer, the HMS community rallied to create an endowed scholarship in his name that will support students interested in global health and social medi cine for generations to come. If you would like to contribute to this fund and help carry on Farmer’s legacy, visit hms.harvard.edu/farmer-scholarship.
When you include Harvard Medical School in your estate plan, you create a legacy of helping to secure a healthier tomorrow.
By following these tips, you can make a larger gift to the School while maintaining control over your assets in your lifetime.
Without a will, the laws of your state will decide how your estate is divided.
TIP: Work with an attorney to create a will or living trust that accomplishes your personal and philanthropic goals.
Including HMS in your will or living trust is a simple way to make a gift—it costs nothing now but provides future support for the causes most important to you.
•
your financial, tax, and estate planning goals
or eliminate estate tax
health and well-being
Contact us in confidence: Kate Murphy | 1-800-922-1782 giftplanning@hms.harvard.edu
A retirement account can be the most highly-taxed asset that people pass to heirs.
TIP: Leave other types of assets to your heirs and gift retirement assets to a charitable organization such as HMS.
Designating HMS as a beneficiary of your individual retirement account, investment account, savings account, or donor-advised fund is as easy as filling out a form.
Learn more at hms.harvard.edu/future-gifts
U.S. Postage PAID Burlington, VT 05401
Permit No. 391 25 Shattuck Street Boston, Massachusetts 02115
Each year, floods account for nearly half of all deaths from natural disasters worldwide. They also exact a lasting toll among survivors. Infections caused by pathogens or pollutants in floodwaters can lead to long-lasting illnesses, and debris and other hazards can result in injuries that change lives forever. The psychological consequences may be even more insidious. Experiencing a flood can cause trauma that lingers for a lifetime, while repeated exposure to news of flooding-induced plights of others can cause depression and anxiety in the wider population.

