
What’s the Diagnosis Case 174 1

What’s the Diagnosis Case 174 2
What’s the Diagnosis Case 174 3

What’s the Diagnosis Case 174 4

What’s the Diagnosis Case 174 5

What’s the Diagnosis Case 174 6

What’s the Diagnosis Case 174 7

What’s the Diagnosis Case 174 8

What’s the Diagnosis Case 174 9

What’s the Diagnosis Case 174 10

What’s the Diagnosis Case 174 11
What’s the Diagnosis Case 174 12

What’s the Diagnosis Case 174 13

What’s the Diagnosis Case 174 14

What’s the Diagnosis Case 174 15

What’s the Diagnosis Case 174 16

What’s the Diagnosis Case 174 17

What’s the Diagnosis Case 174 18

What’s the Diagnosis Case 174 19

What’s the Diagnosis Case 174 20

What’s the Diagnosis Case 174 21

What’s the Diagnosis Case 174 22

What’s the Diagnosis Case 174 23

What’s the Diagnosis Case 174 24

What’s the Diagnosis Case 174 25

What’s the Diagnosis Case 174 26

What’s the Diagnosis Case 174 27

What’s the Diagnosis Case 174 28

What’s the Diagnosis Case 174 29

What’s the Diagnosis Case 174 30

What’s the Diagnosis Case 174 31

What’s the Diagnosis Case 174 32

What’s the Diagnosis Case 174 33

What’s the Diagnosis Case 174 34

What’s the Diagnosis Case 174 35

What’s the Diagnosis Case 174 36

What’s the Diagnosis Case 174 37

What’s the Diagnosis Case 174 38

What’s the Diagnosis Case 174 39

What’s the Diagnosis Case 174 40

What’s the Diagnosis Case 174 41

What’s the Diagnosis Case 174 42

What’s the Diagnosis Case 174 43
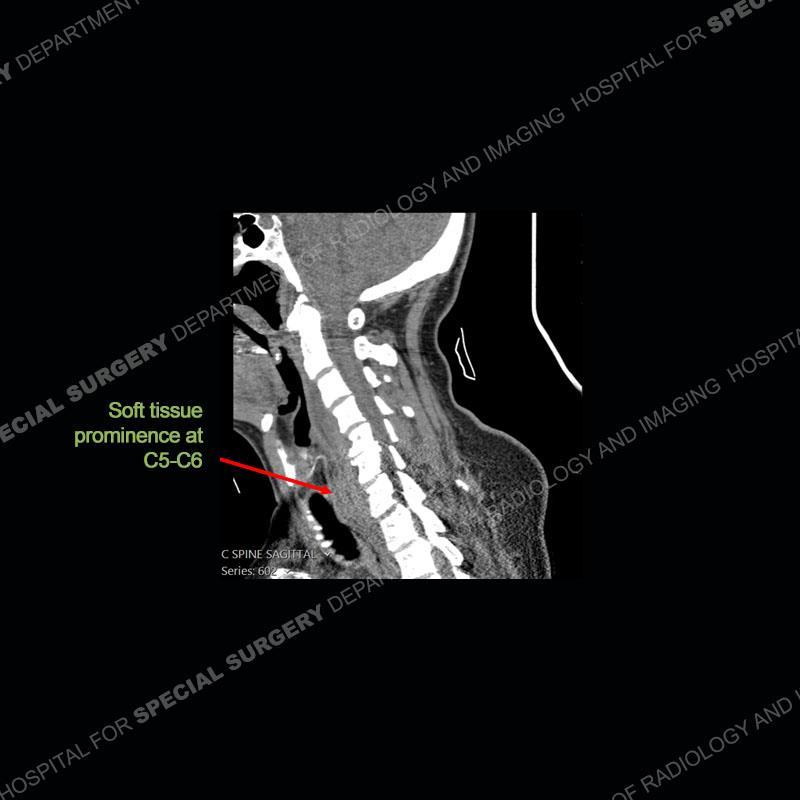
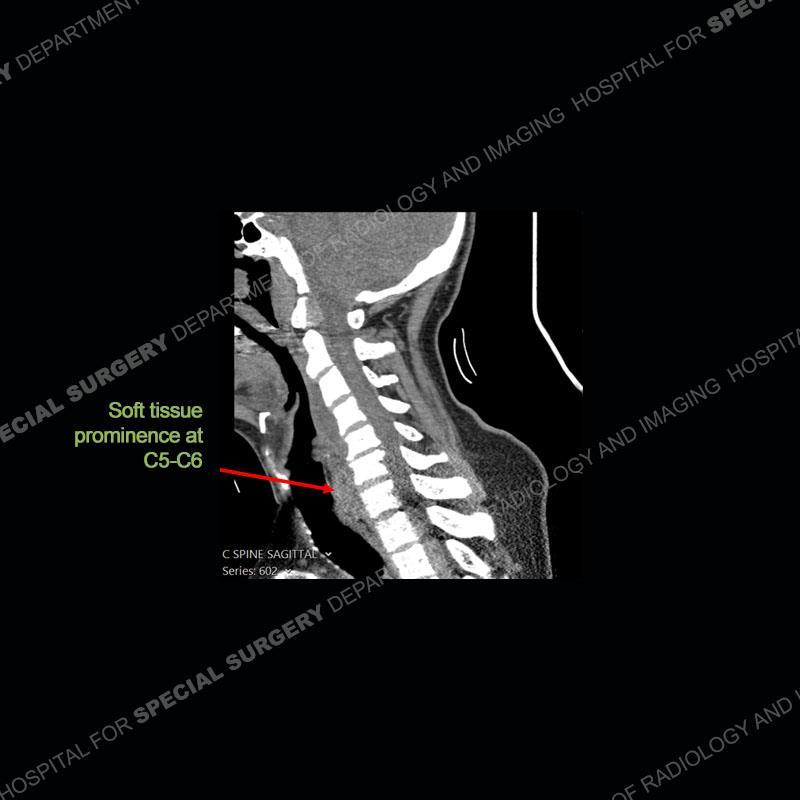
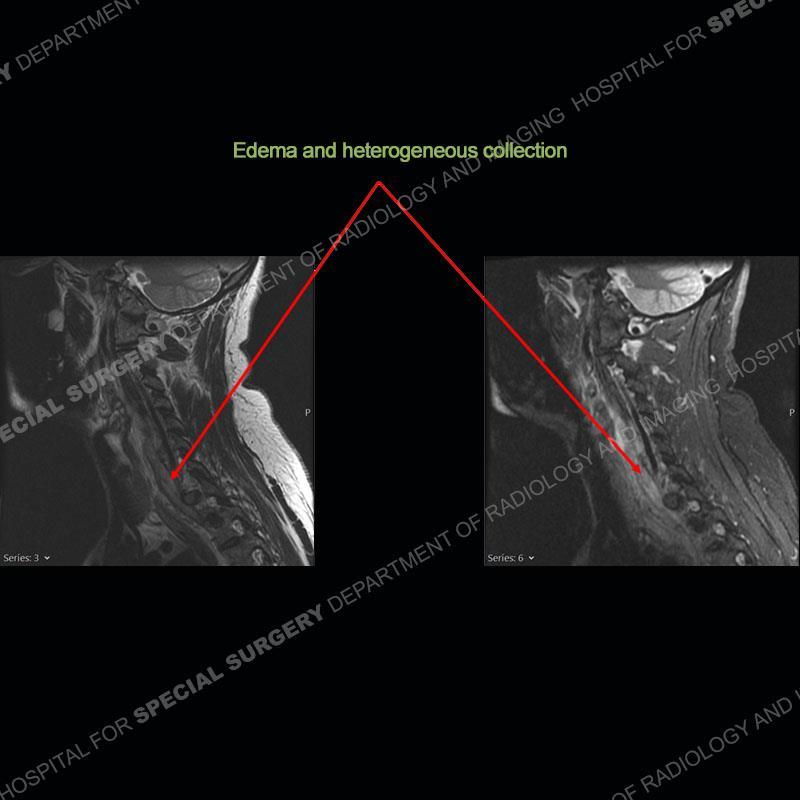
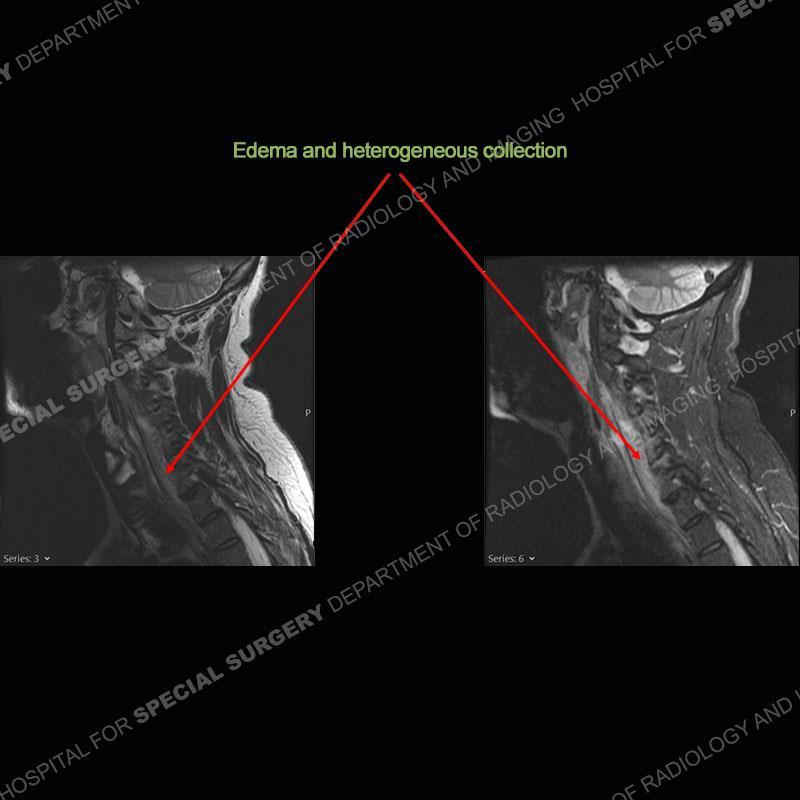
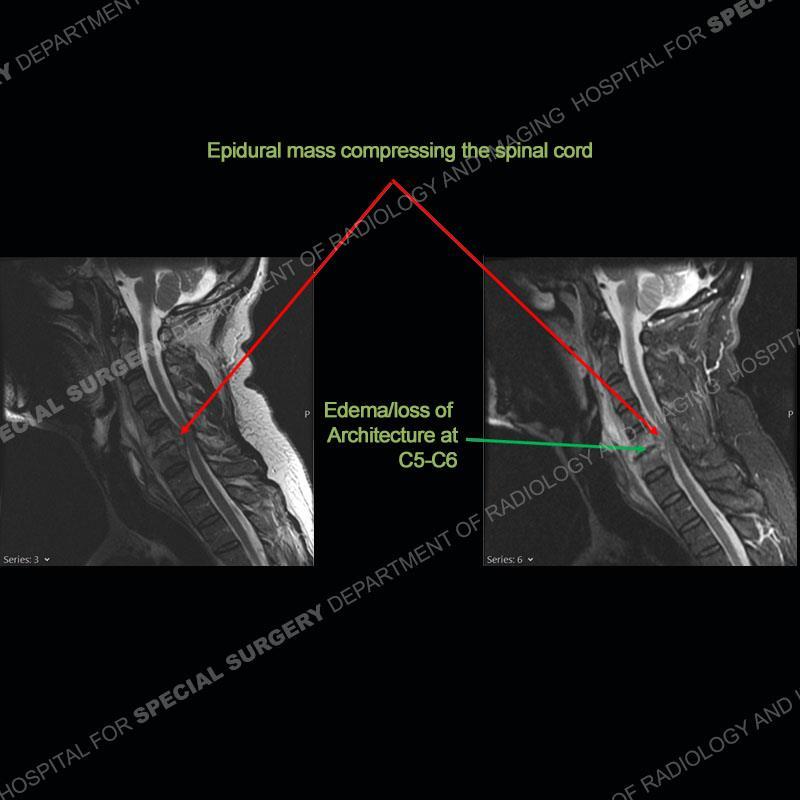
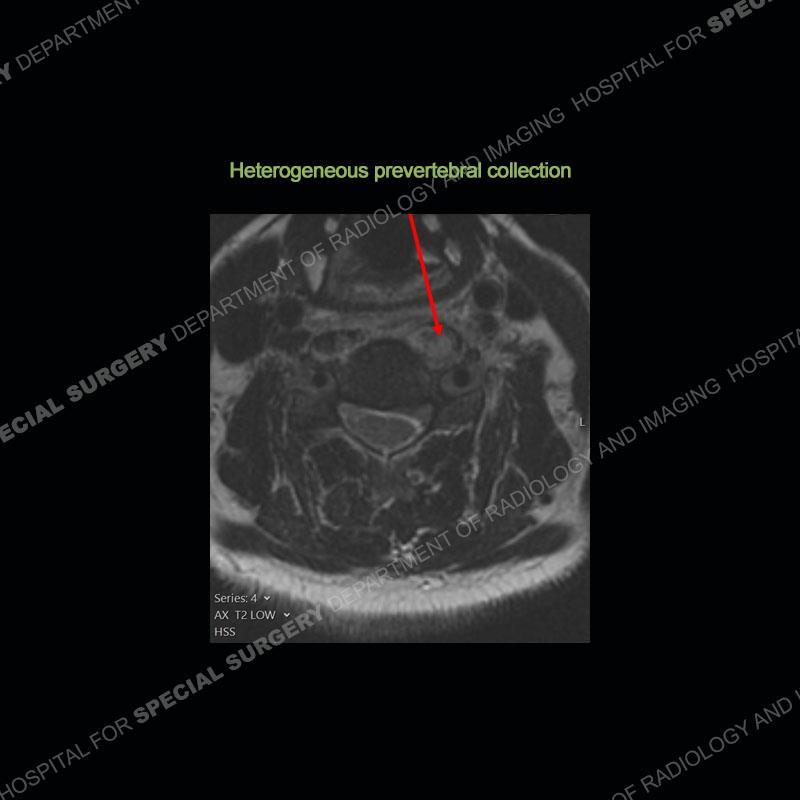
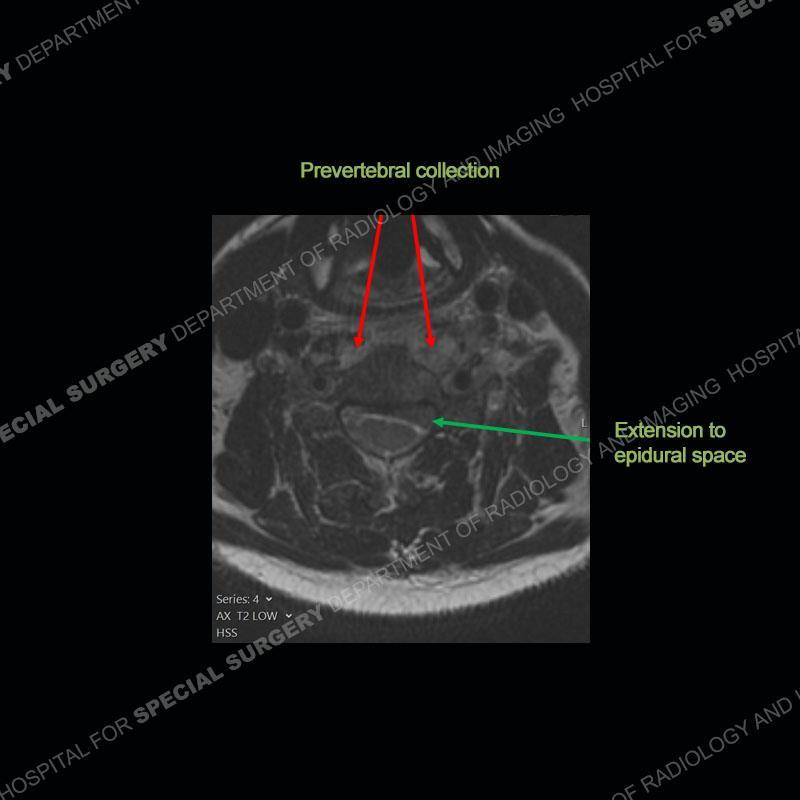
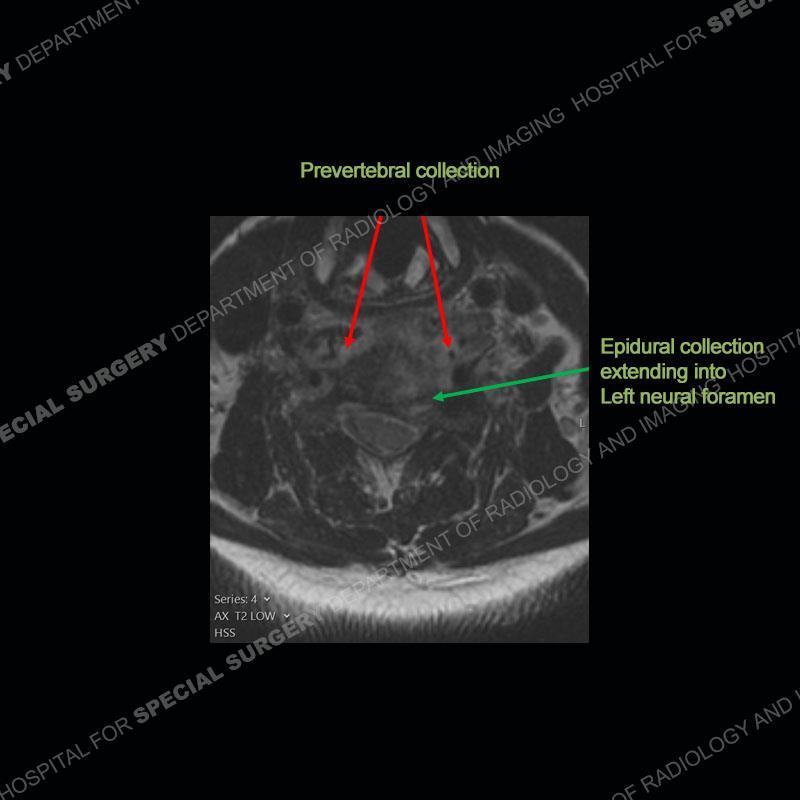
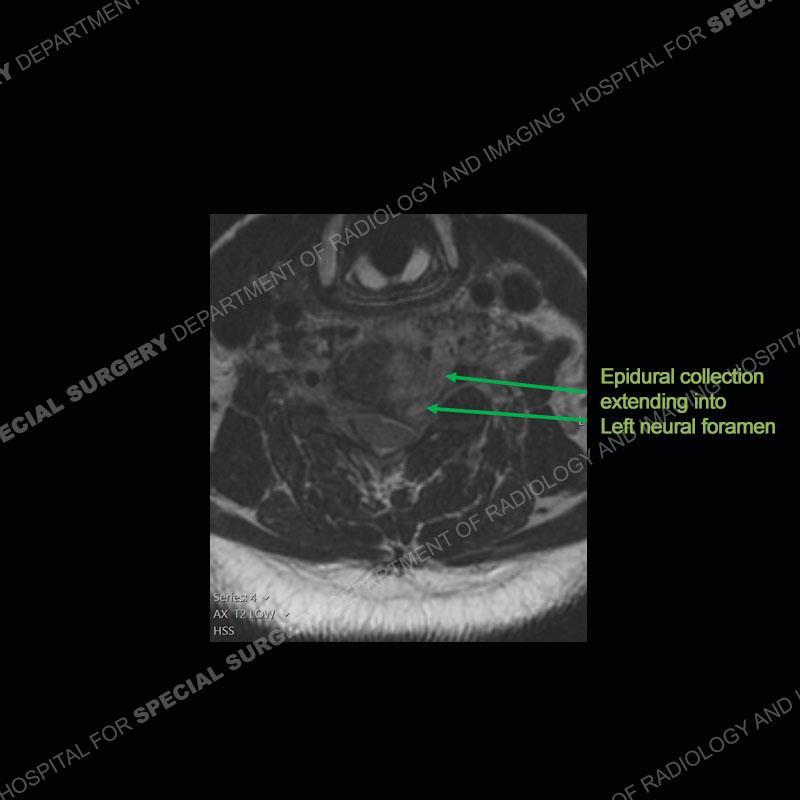
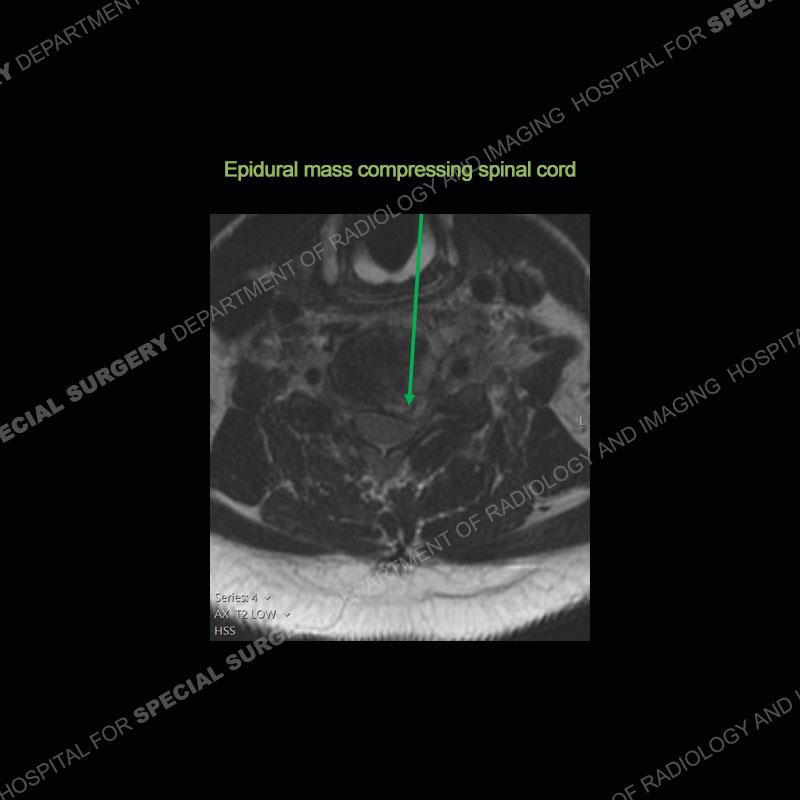
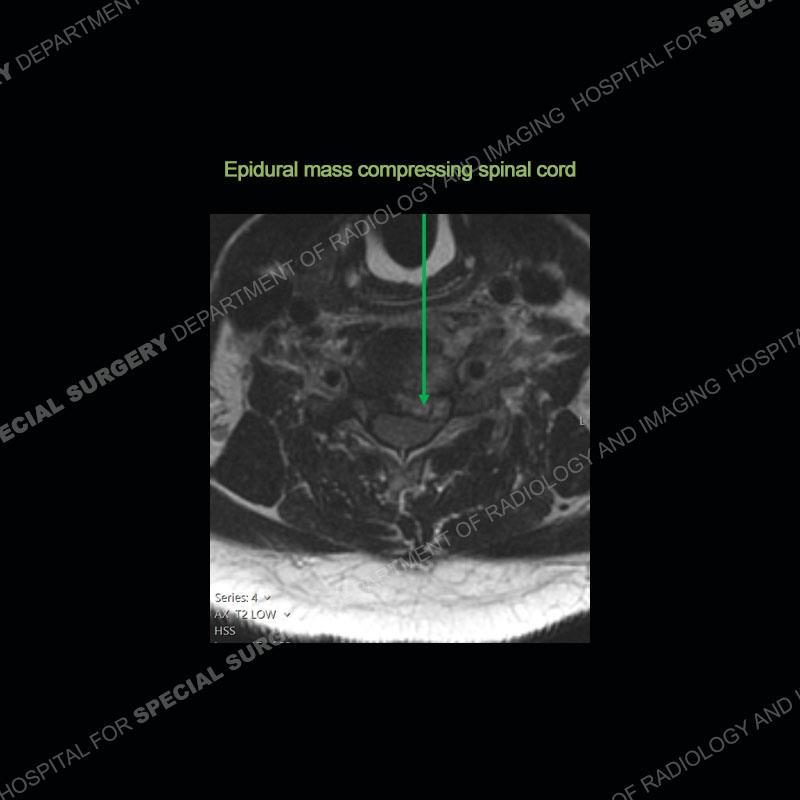
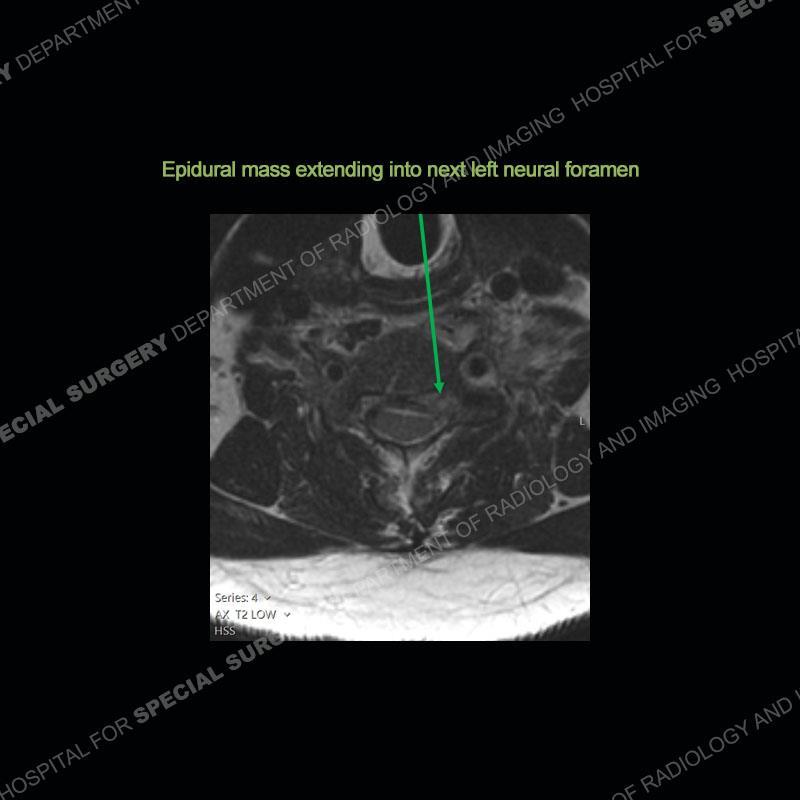
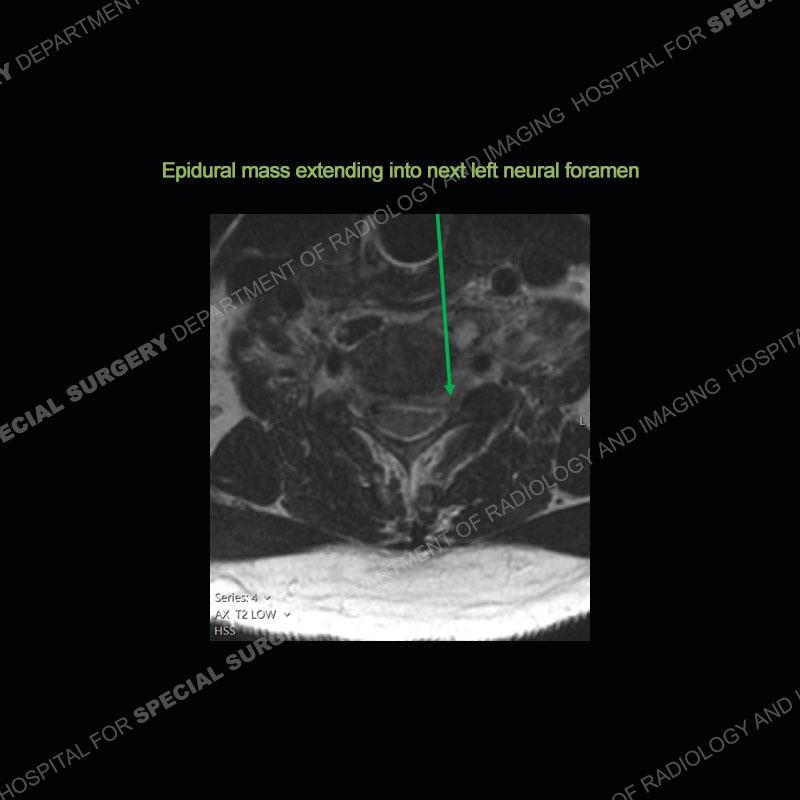
Findings
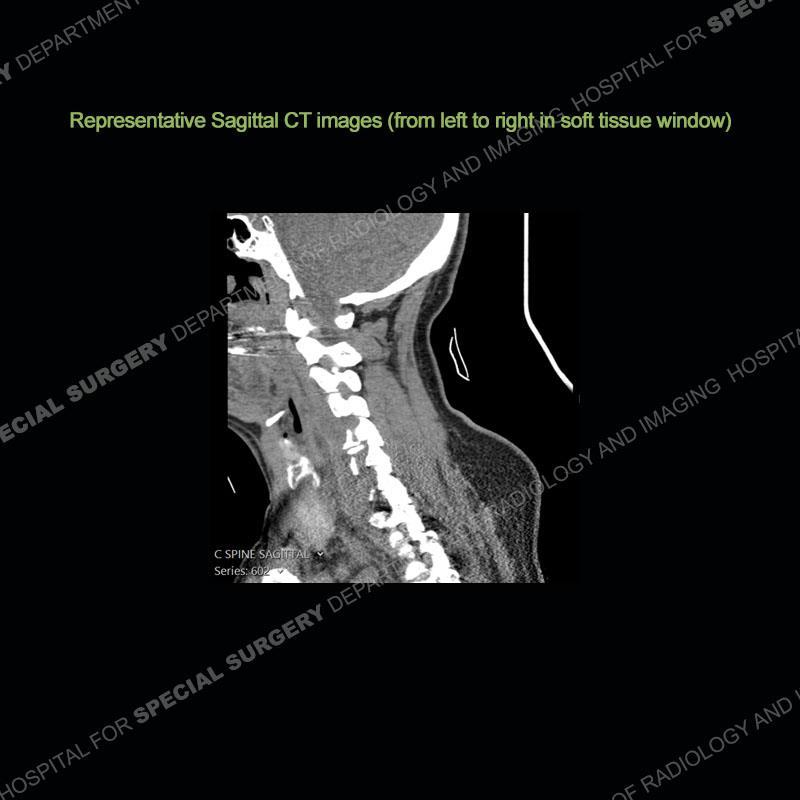
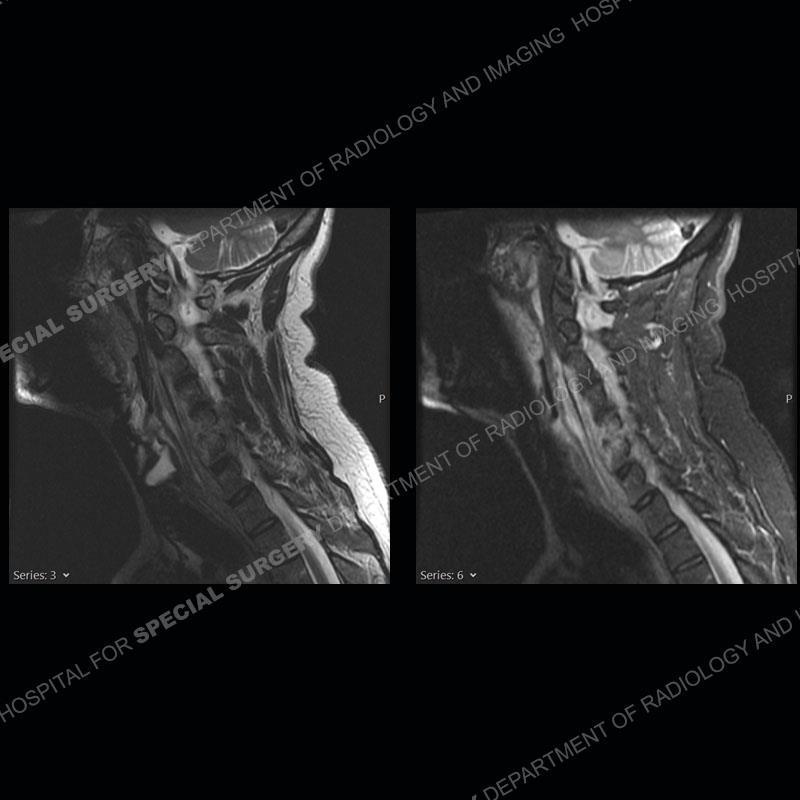
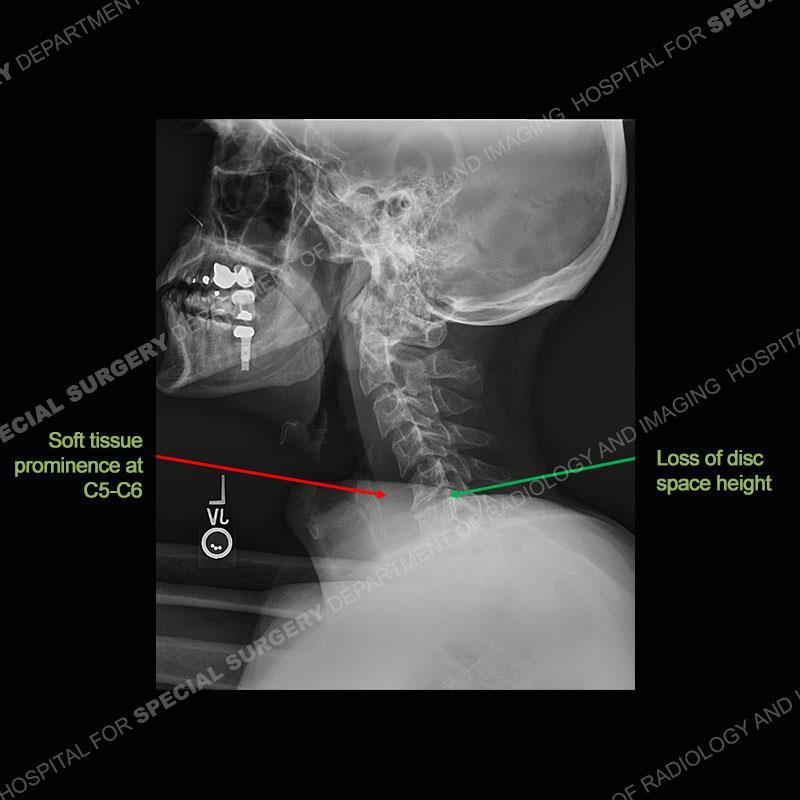
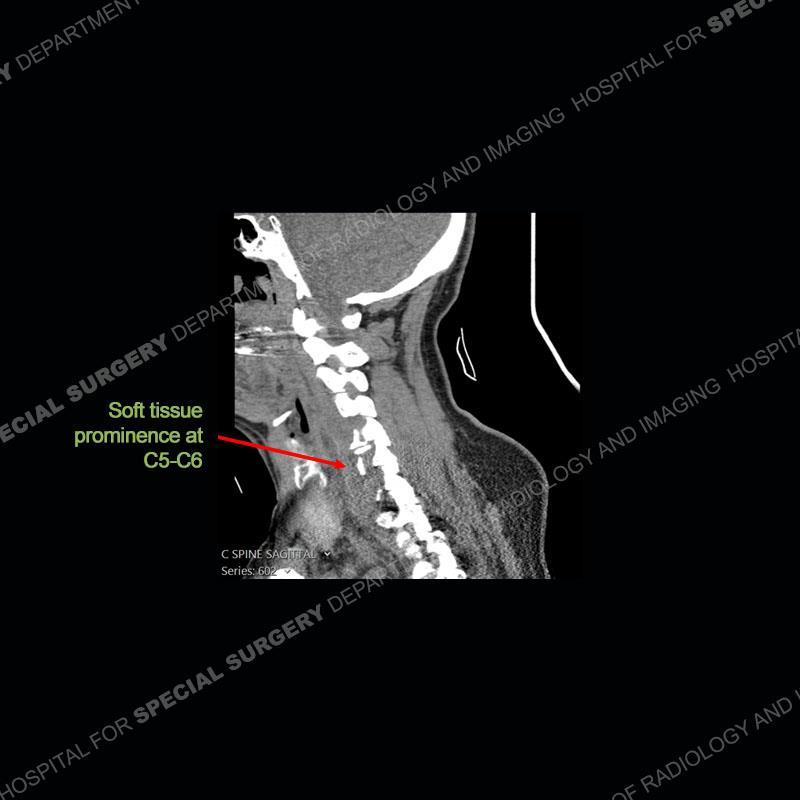
The radiographs demonstrate a prevertebral soft tissue fullness centered at C5-C6 that persists even on extension. There is a slight loss of disc height at C5-C6. The CT more readily shows the prevertebral soft tissue swelling at C5C6 where there is a punctate focus of gas. On the MRI, there is a marked amount of edema and a heterogeneous collection in the prevertebral soft tissue at C5-C6. Edema is present of the C5 and C6 vertebral bodies with a loss of the normal architecture about the disc space. A heterogeneous epidural collection has formed that causes compression of the spinal cord asymmetric to the left side and also precipitates severe left sided neural foraminal stenosis.

What’s the Diagnosis Case 174
44
What’s the Diagnosis Case 174 45
What’s the Diagnosis Case 174 46
What’s the Diagnosis Case 174 47

What’s the Diagnosis Case 174 48
What’s the Diagnosis Case 174 49

What’s the Diagnosis Case 174 50
What’s the Diagnosis Case 174 51
What’s the Diagnosis Case 174 52

What’s the Diagnosis Case 174 53
What’s the Diagnosis Case 174 54
What’s the Diagnosis Case 174 55
What’s the Diagnosis Case 174 56
What’s the Diagnosis Case 174 57
What’s the Diagnosis Case 174 58
What’s the Diagnosis Case 174 59
What’s the Diagnosis Case 174 60

What’s the Diagnosis Case 174 61
What’s the Diagnosis Case 174 62
What’s the Diagnosis Case 174 63
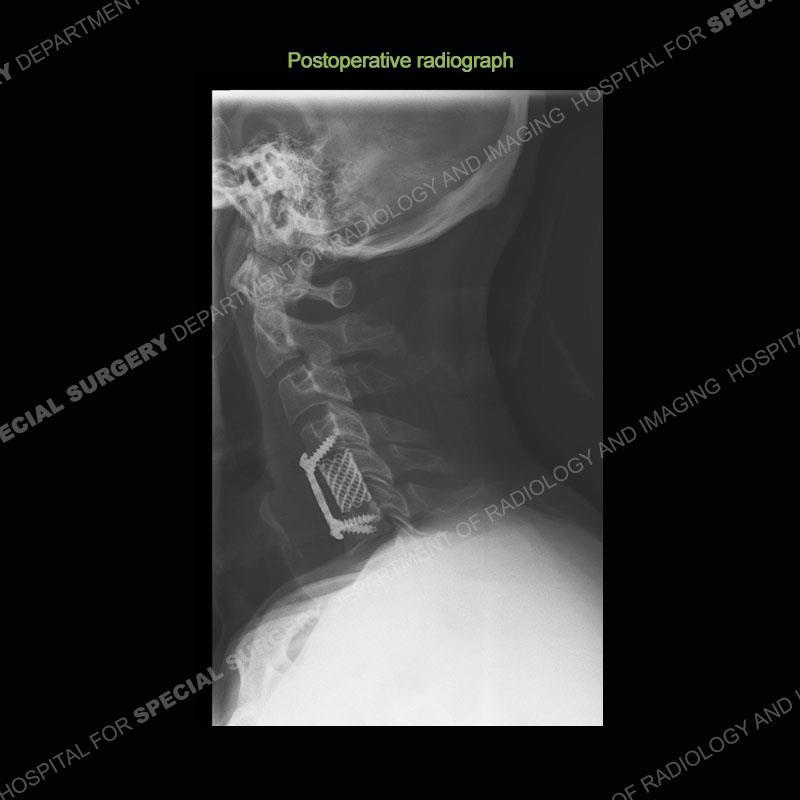
Diagnosis: Spontaneous Retropharyngeal Abscess (RPA) with Discitis/Osteomyelitis, Epidural Abscess, and Cord Compression
Spontaneous RPA in the non-immunocompromised, adult population is an extremely rare occurrence. RPA most frequently occurs in young children and most typically after a URI. It may be associated with torticollis in Grisel syndrome. In the adult population, the pathomechanism is not well understood with some suggesting a hematogenous spread or perhaps a seeding from the adjacent aerodigestive tract. The abscess as in this case can extend to involve the vertebral column and then the neural elements. At times, this process can be treated with antibiotic therapy alone but when there are neurologic symptoms and especially progression of neurologic symptoms, surgical intervention is warranted. In this case, given the extent of the process and the patient’s clinical situation, a corpectomy with fusion was performed in addition to antibiotics.
What’s the Diagnosis Case 174
64
What’s the Diagnosis Case 174 65
References
Spontaneous, Non-Traumatic Retropharyngeal Abscess Complicated by Spinal Osteomyelitis and Epidural Abscess in Immunocompetent Adult: Management and Proposal Pathophysiological Mechanism. Giorgos Sideris ,Thomas Nikolopoulos, Nikolaos Papadimitriou. Cureus. 2020 Jul; 12(7): e9028. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Sang Do Kim, Rojeh Melikian, Kevin L Ju, David Zurakowski, Kirkham B Wood, Christopher M Bono, Mitchel B Harris. Spine J. 2014 Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30.
Retropharyngeal abscess with secondary osteomyelitis and epidural abscess: proposed pathophysiological mechanism of an underrecognized complication of unstable craniocervical injuries: case report. Carlos R Goulart, Tobias A Mattei, Mariano E Fiore, William J Thoma, Ehud Mendel. J Neurosurg Spine. 2016 Jan;24(1):197-205. doi: 10.3171/2015.4.SPINE14952.
Surgical treatment of spondylodiscitis in the cervical spine: a minimum 2-year follow-up. Christoph E Heyde , Heinrich Boehm, Hesham E Saghir, Sven K Tschöke, Ralph Kayser. Eur Spine J. 2006 Sep;15(9):1380-7. doi: 10.1007/s00586-006-0191-z. Epub 2006 Jul 26.
What’s the Diagnosis Case 174
66
