
What’s the Diagnosis Case 175 1

What’s the Diagnosis Case 175 2

What’s the Diagnosis Case 175 3

What’s the Diagnosis Case 175 4

What’s the Diagnosis Case 175 5

What’s the Diagnosis Case 175 6

What’s the Diagnosis Case 175 7
What’s the Diagnosis Case 175 8

What’s the Diagnosis Case 175 9

What’s the Diagnosis Case 175 10

What’s the Diagnosis Case 175 11

What’s the Diagnosis Case 175 12

What’s the Diagnosis Case 175 13

What’s the Diagnosis Case 175 14
What’s the Diagnosis Case 175 15

What’s the Diagnosis Case 175 16

What’s the Diagnosis Case 175 17

What’s the Diagnosis Case 175 18

What’s the Diagnosis Case 175 19

What’s the Diagnosis Case 175 20

What’s the Diagnosis Case 175 21

What’s the Diagnosis Case 175 22

What’s the Diagnosis Case 175 23

What’s the Diagnosis Case 175 24

What’s the Diagnosis Case 175 25

What’s the Diagnosis Case 175 26

What’s the Diagnosis Case 175 27

What’s the Diagnosis Case 175 28

What’s the Diagnosis Case 175 29

What’s the Diagnosis Case 175 30

What’s the Diagnosis Case 175 31

What’s the Diagnosis Case 175 32

What’s the Diagnosis Case 175 33
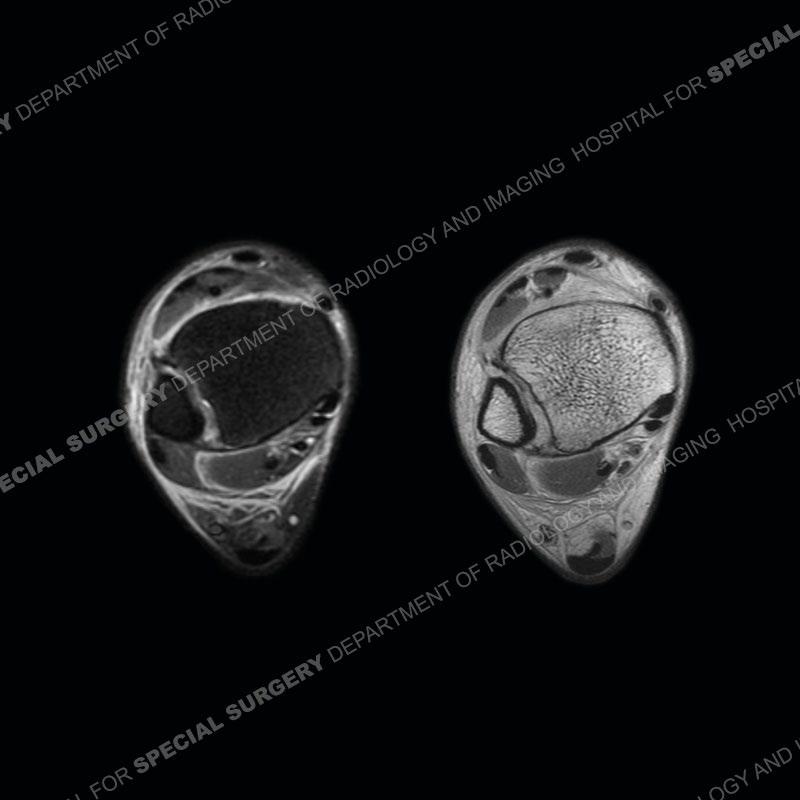
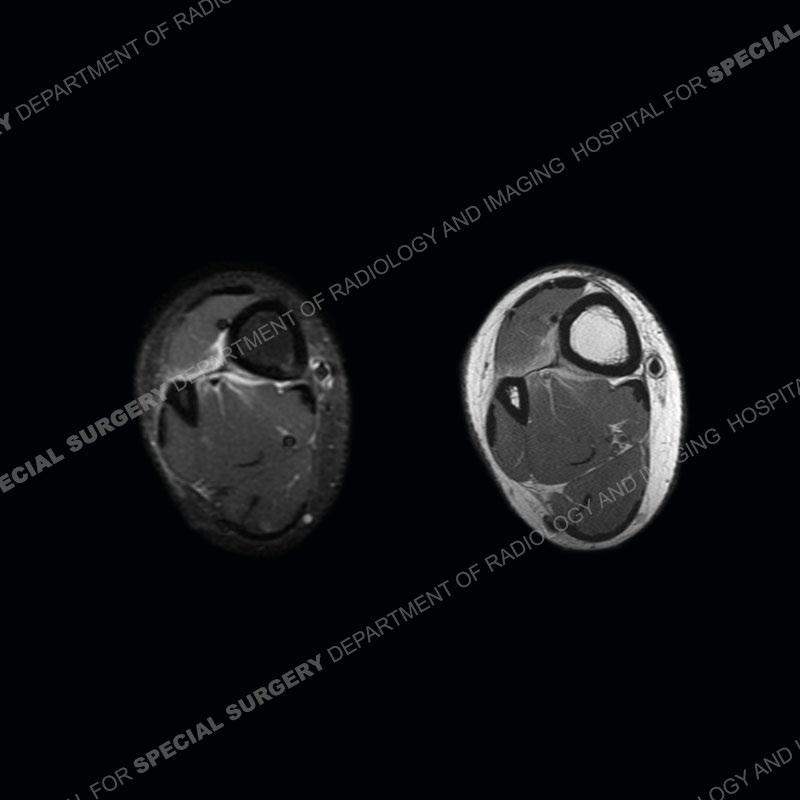
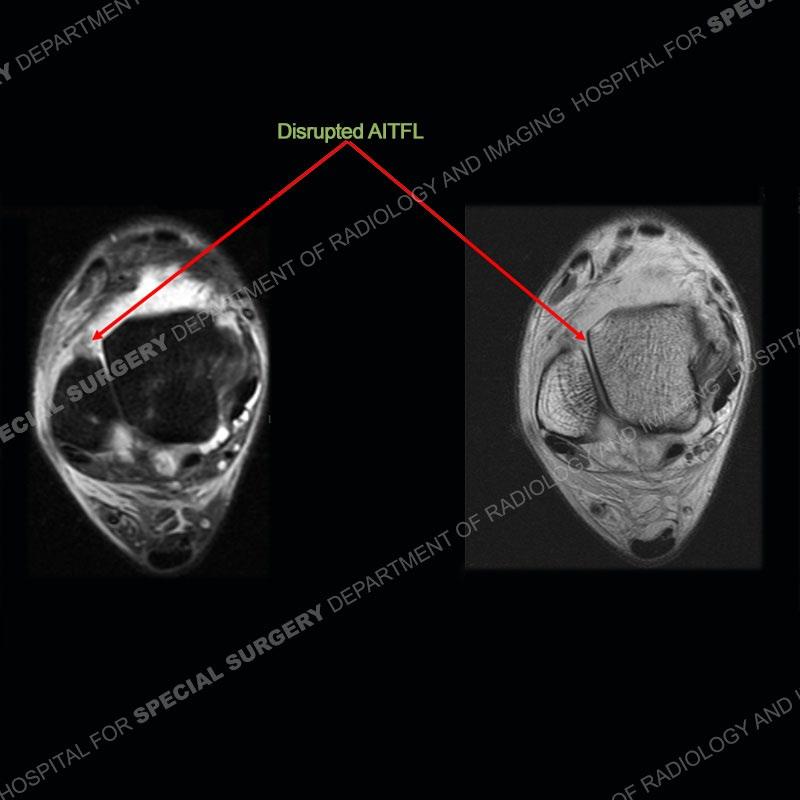
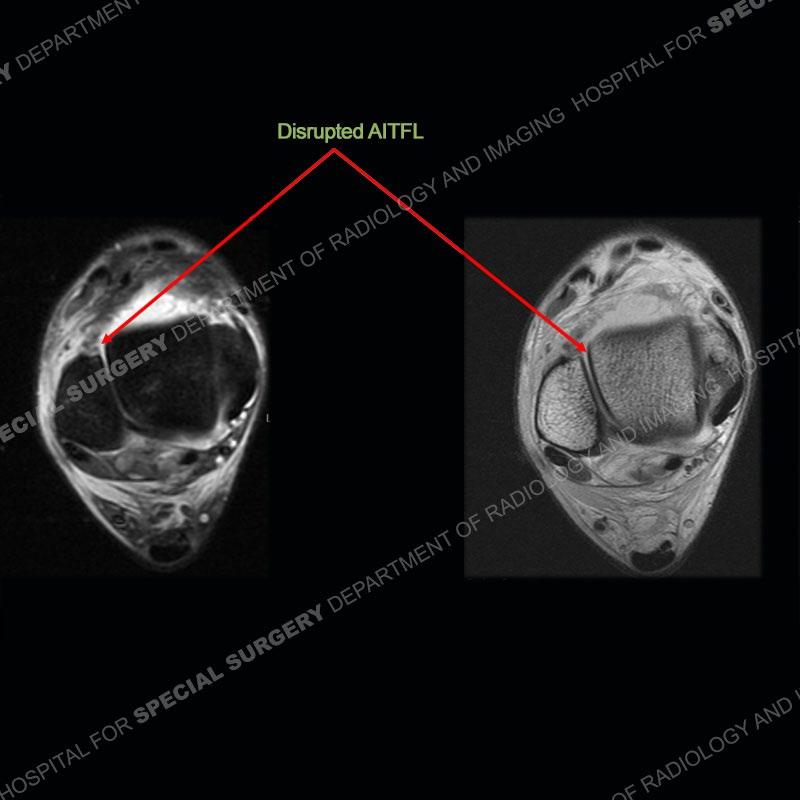
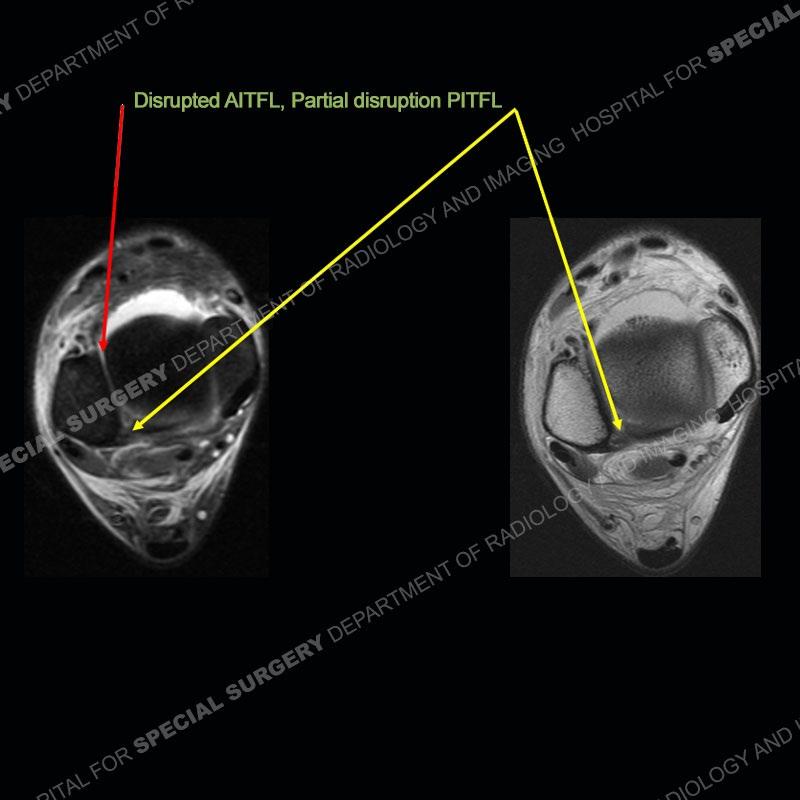
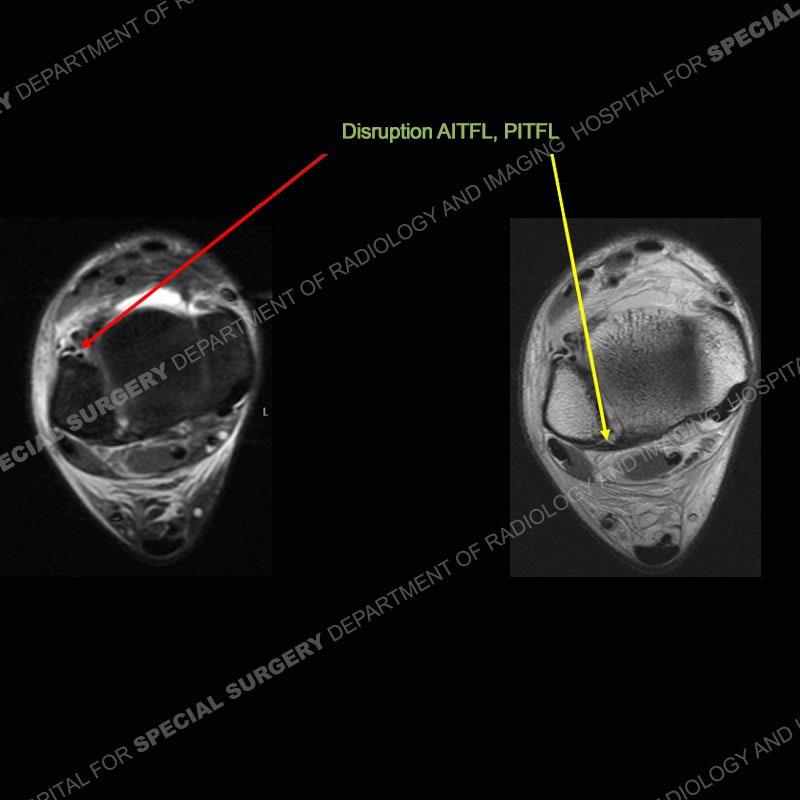
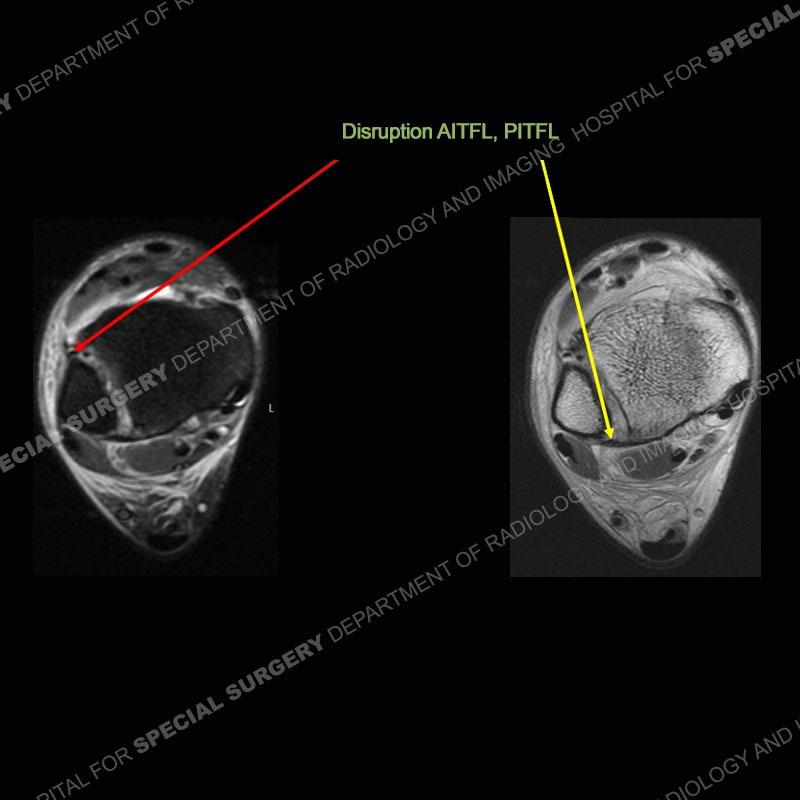
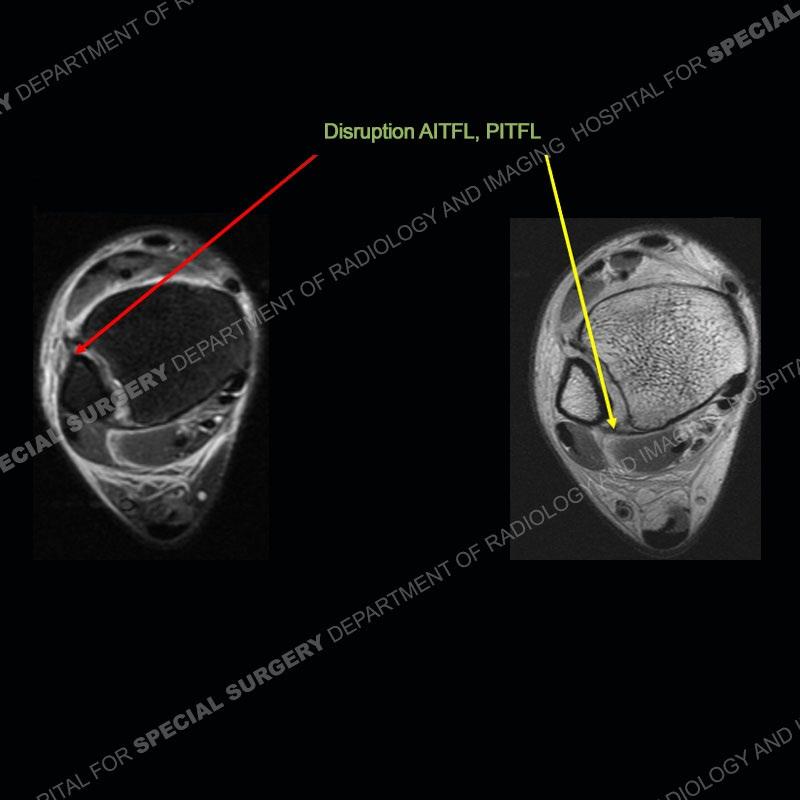
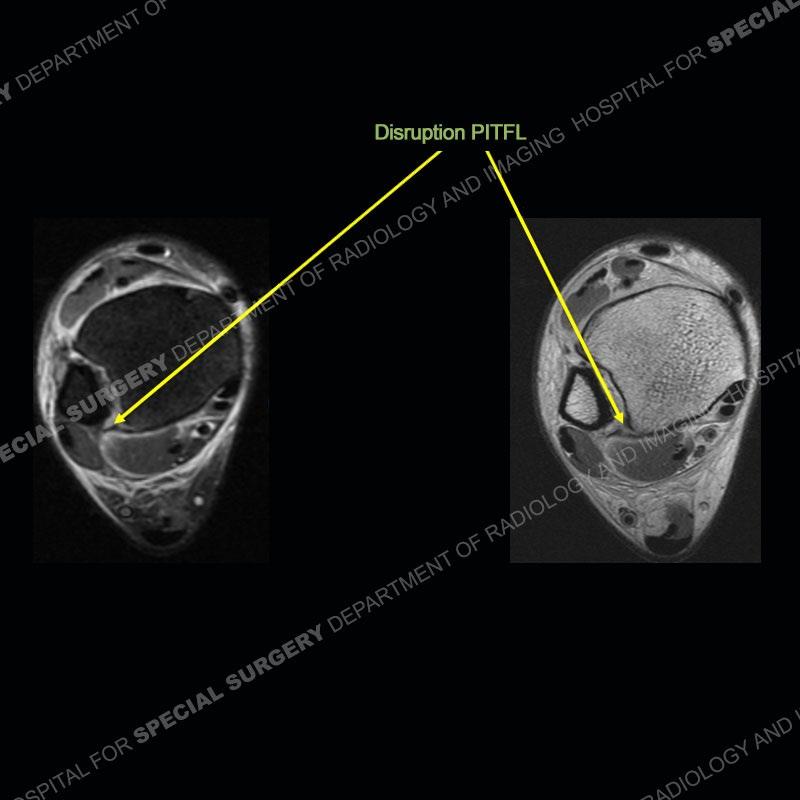
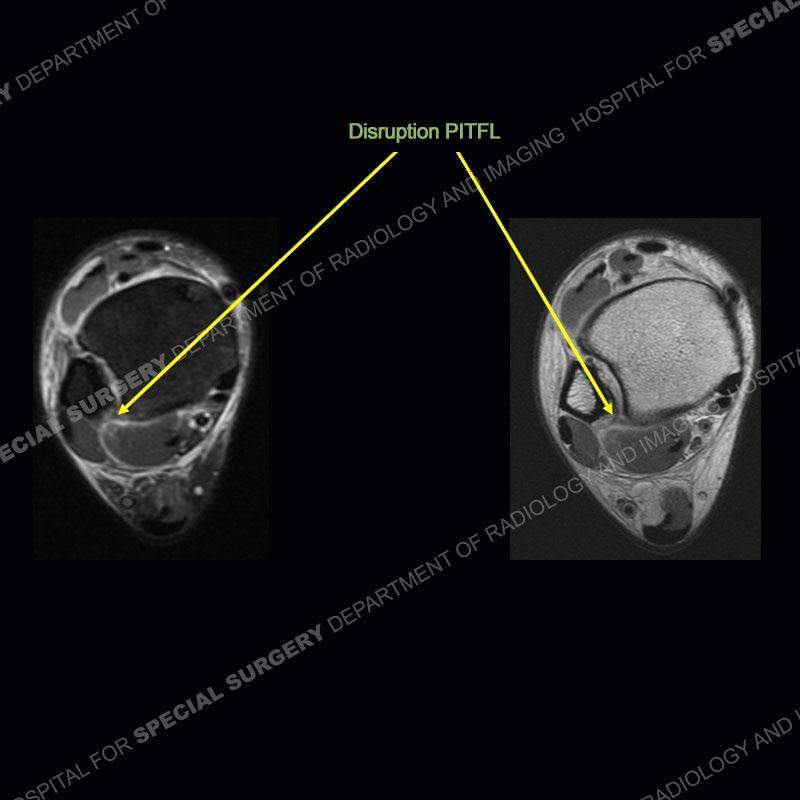
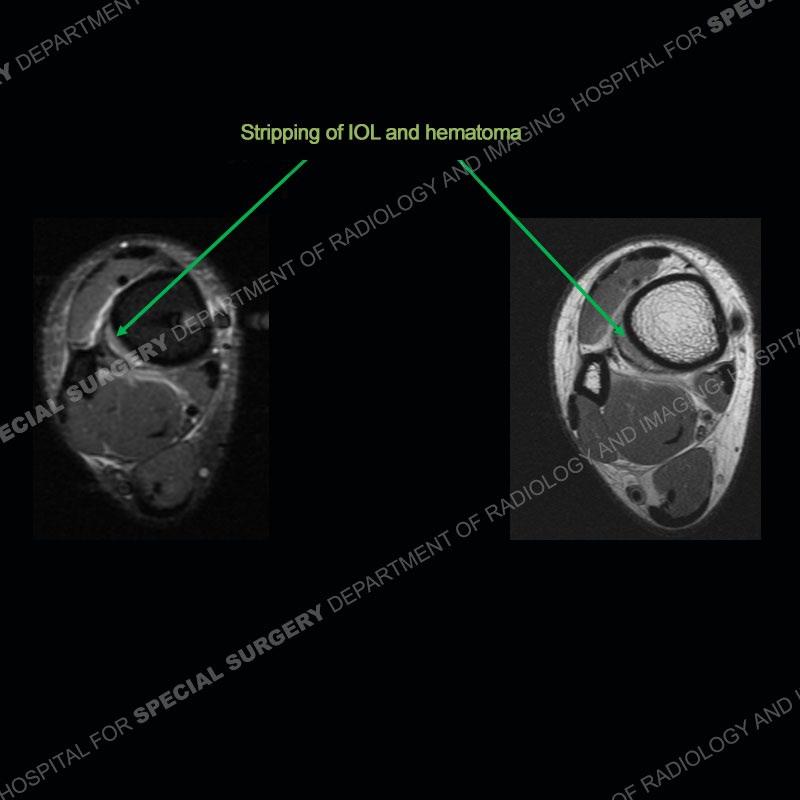
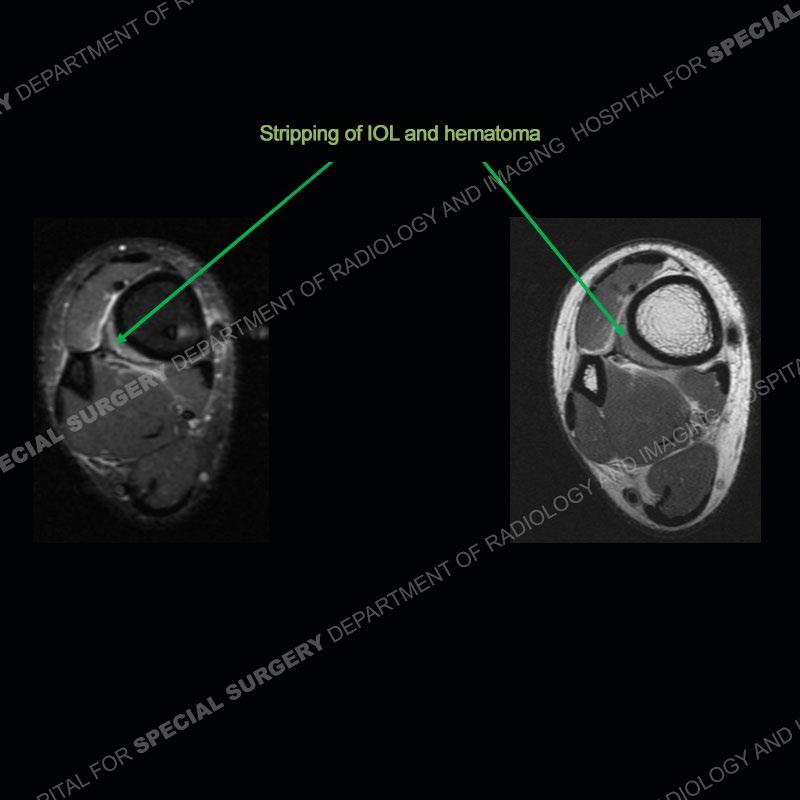
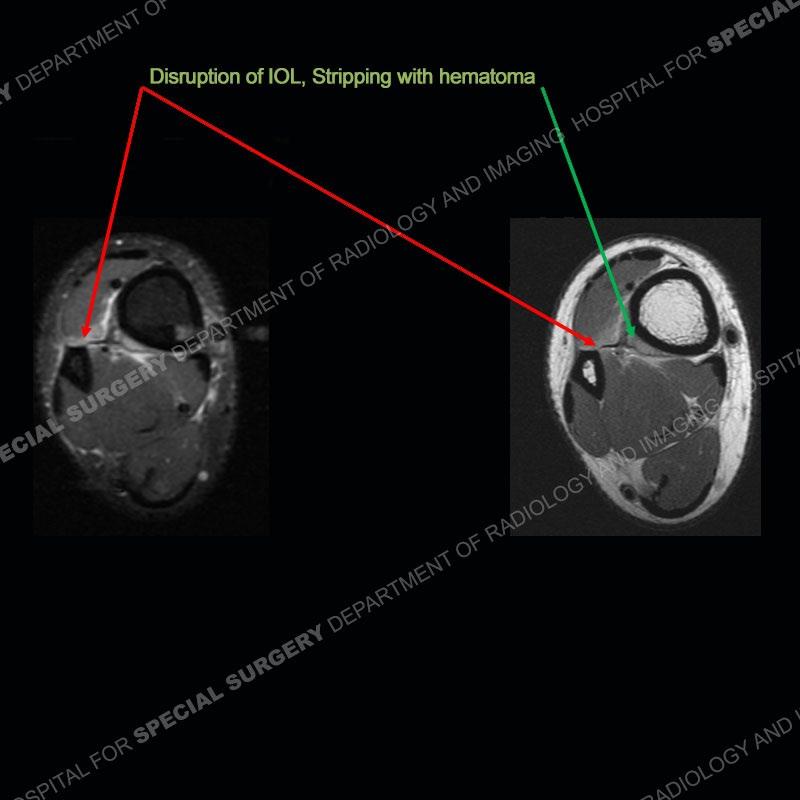
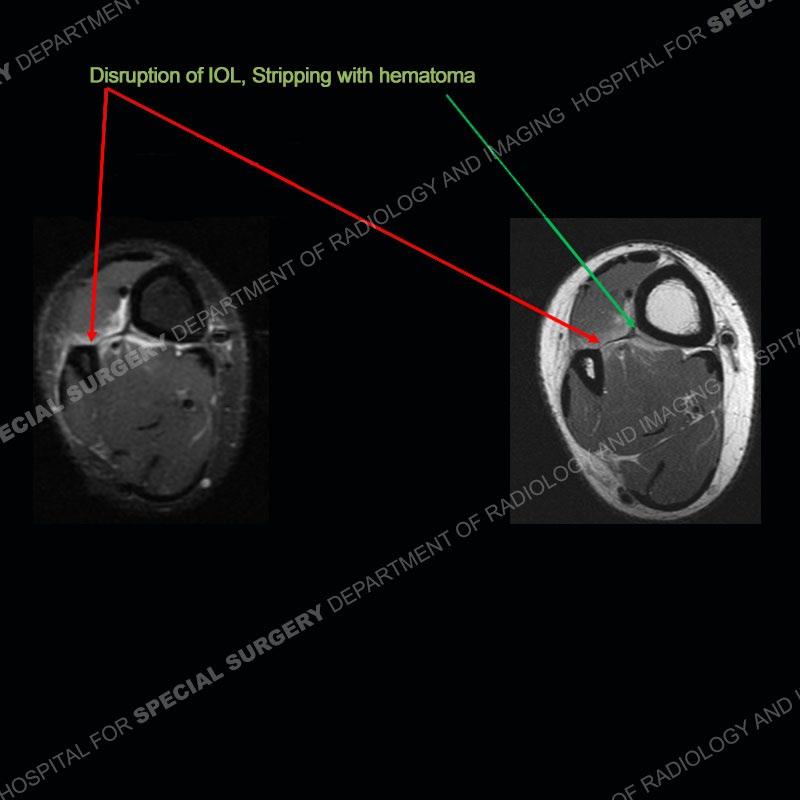
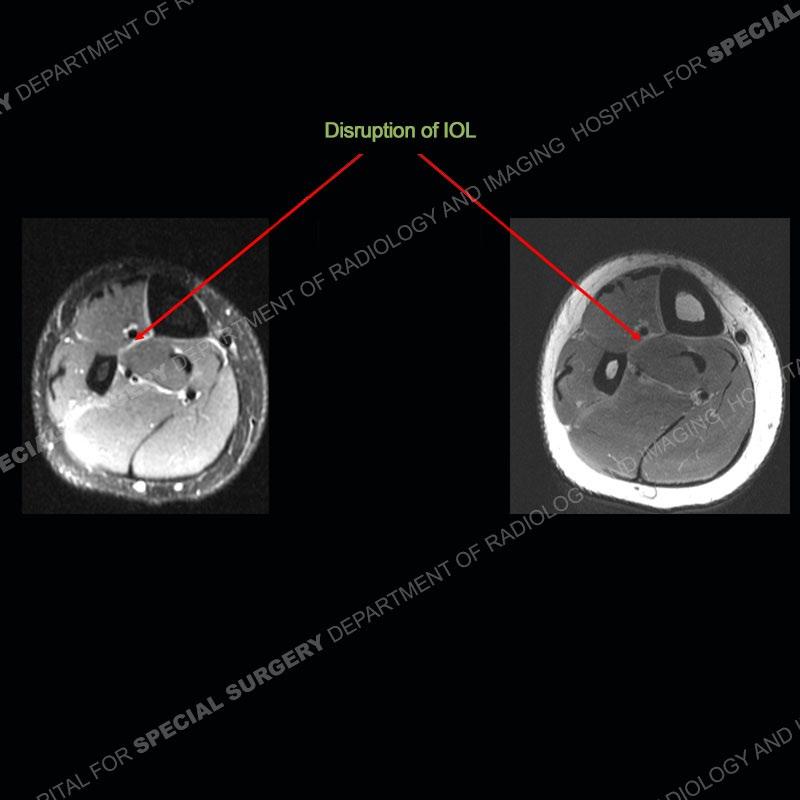
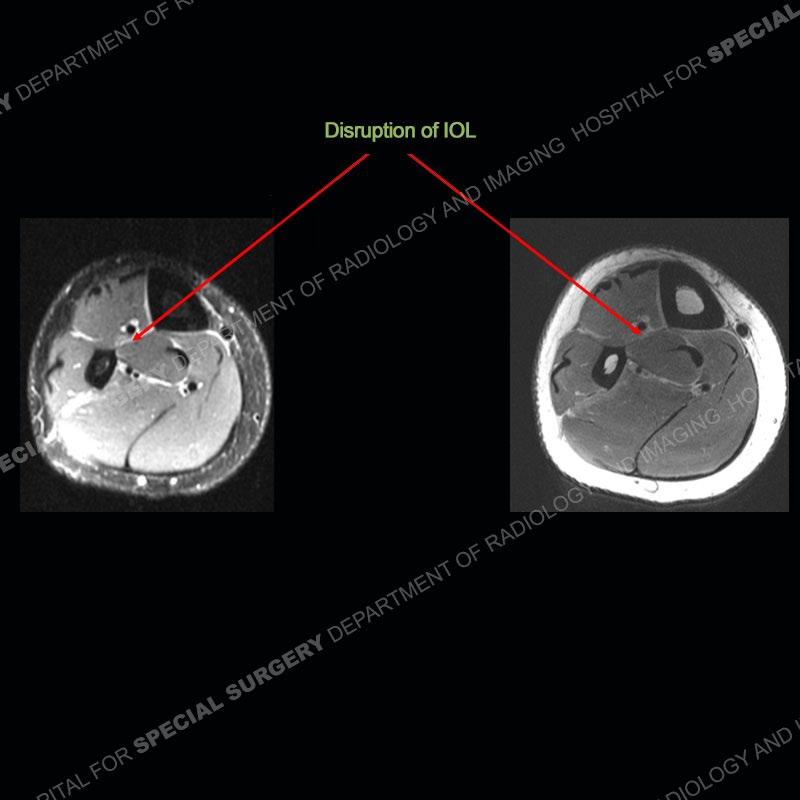
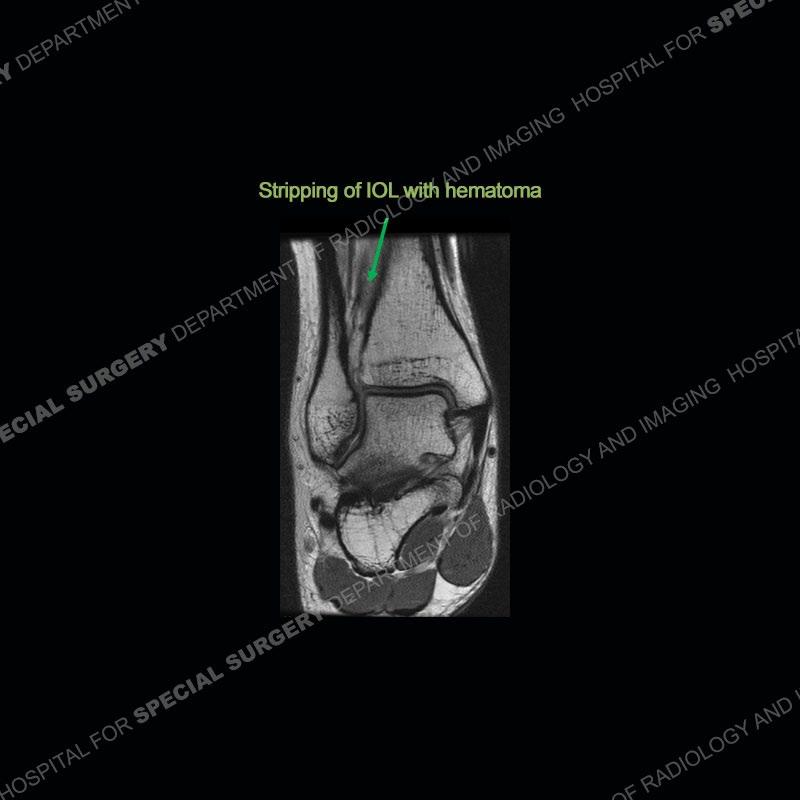
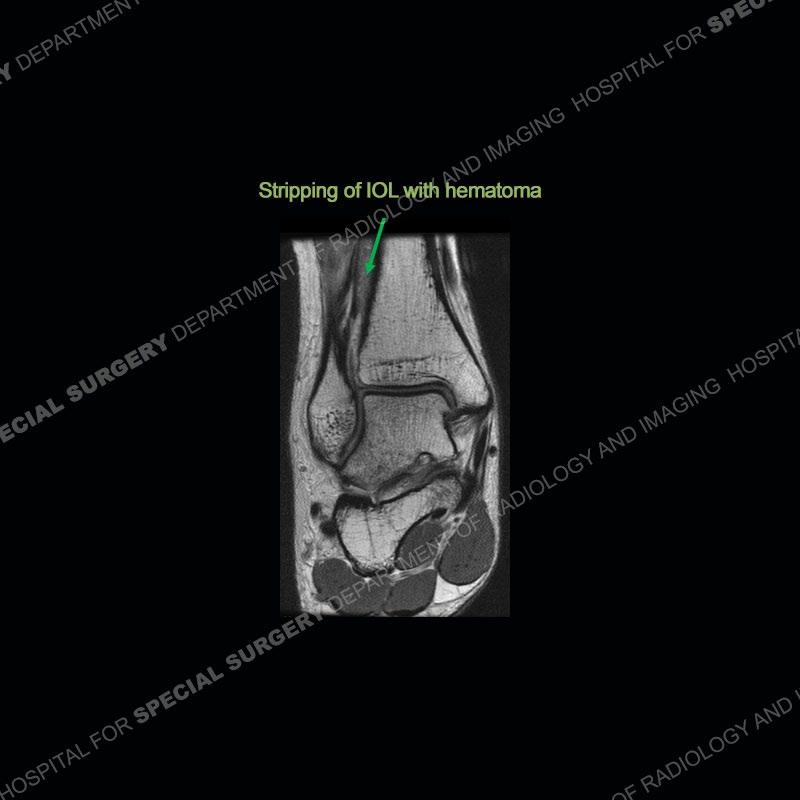
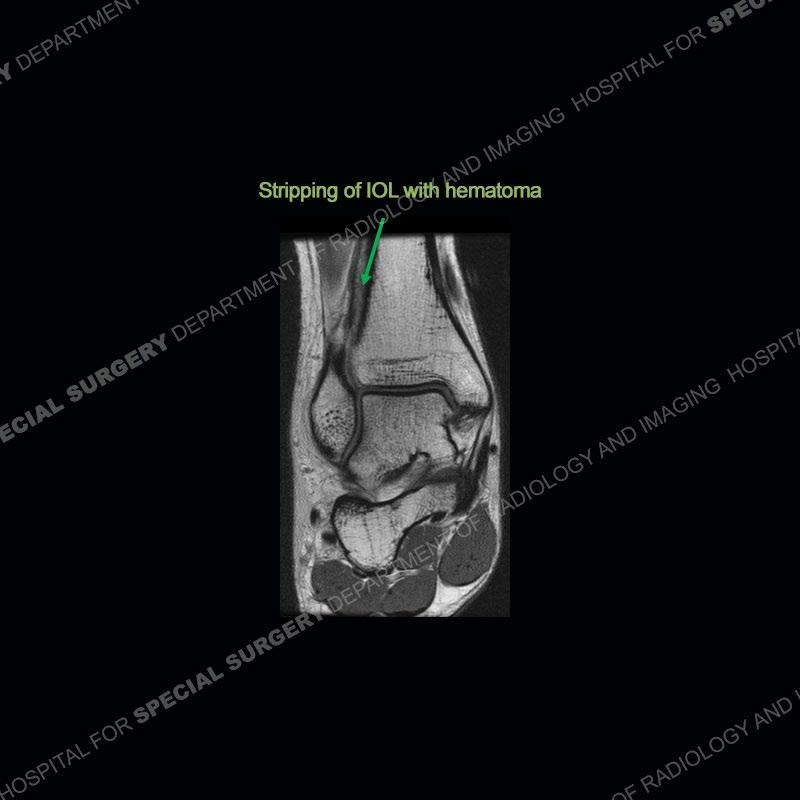
Findings
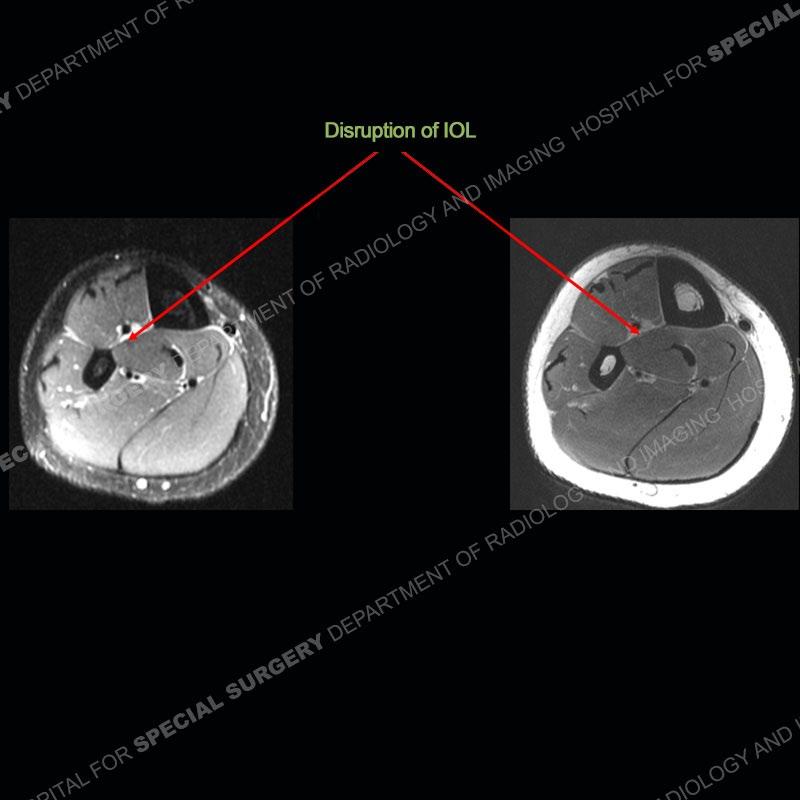
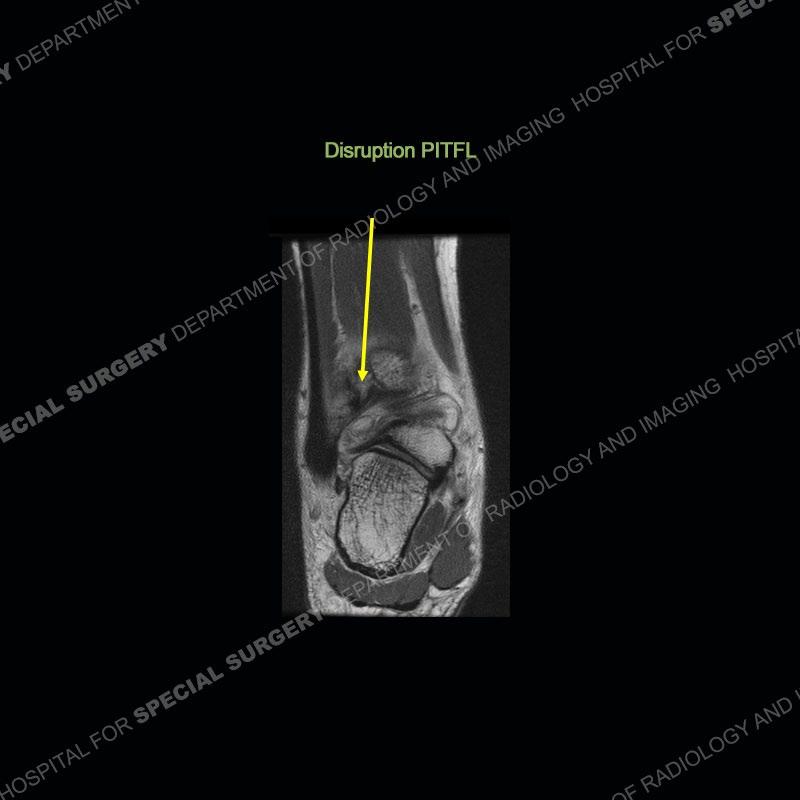
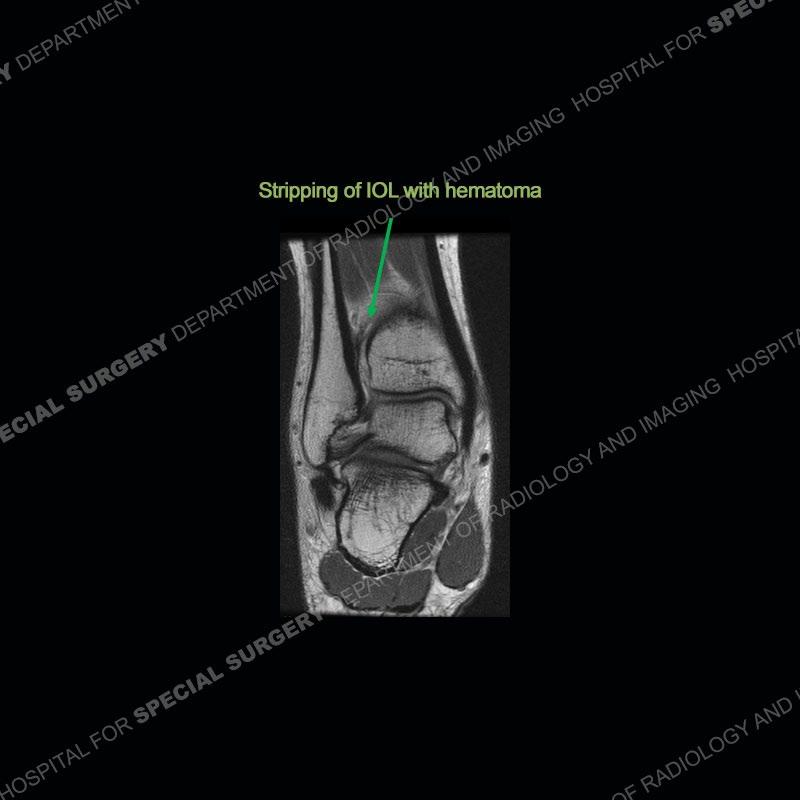
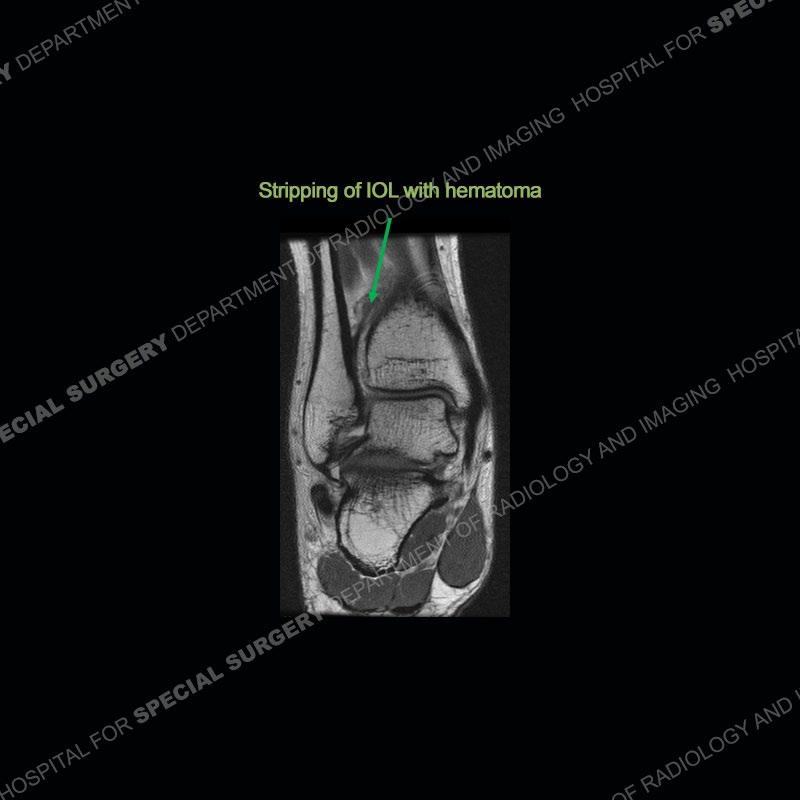
On the AP radiograph there is a diminished overlap of the distal tibia and fibula (normal is at least 10mm overlap). On the mortise view there is no overlap of the distal tibia and fibula and an increased distal tibial fibular clear space (normal is less than 5 mm and measured 1cm superior from the ankle joint). The MRI shows a disruption of the anterior inferior tibiofibular ligament (aitl), a disruption of the posterior inferior tibiofibular ligament (pitfl), and a disruption of the interosseous ligament. There is also a stripping of the distal interosseous ligament (IOL) from the tibia and a precipitated subperiosteal hematoma.

What’s the Diagnosis Case 175
34

What’s the Diagnosis Case 175 35

What’s the Diagnosis Case 175 36
What’s the Diagnosis Case 175 37
What’s the Diagnosis Case 175 38
What’s the Diagnosis Case 175 39
What’s the Diagnosis Case 175 40
What’s the Diagnosis Case 175 41
What’s the Diagnosis Case 175 42
What’s the Diagnosis Case 175 43
What’s the Diagnosis Case 175 44
What’s the Diagnosis Case 175 45
What’s the Diagnosis Case 175 46
What’s the Diagnosis Case 175 47
What’s the Diagnosis Case 175 48
What’s the Diagnosis Case 175 49
What’s the Diagnosis Case 175 50
What’s the Diagnosis Case 175 51
What’s the Diagnosis Case 175 52

What’s the Diagnosis Case 175 53
What’s the Diagnosis Case 175 54
What’s the Diagnosis Case 175 55
What’s the Diagnosis Case 175 56
What’s the Diagnosis Case 175 57
What’s the Diagnosis Case 175 58

What’s the Diagnosis Case 175 59

What’s the Diagnosis Case 175 60

What’s the Diagnosis Case 175 61

What’s the Diagnosis Case 175 62
Diagnosis: Ankle Syndesmotic Injury (“high ankle sprain”)
As compared to the more typical ankle sprain of the lateral collateral ligaments, this can be a much more significant injury requiring much greater time away from sport and necessitating surgical intervention. This case was just a nice example of classic findings on radiographs and MRI. The radiographs can be enhanced with external rotation stress views to demonstrate abnormal widening of the ankle joint. On MRI, the AITFL, PITFL, and IOL can all be especially well seen on axial images to evaluate the extent of injury. In this case, the transverse tibiofibular ligament (or deep portion of the PITFL) was maintained and not highlighted. The AITFL is the first ligament to be injured with subsequent injury to the remainder of the ligaments if greater force is imparted.
Given the looser attachment of the periosteum in children, subperiosteal hematoma around the area of the metaphysis can frequently be seen. This accounts for the finding in the current exam. The mechanism of injury is typically external rotation rotating the talus laterally to cause a force between the distal tibia and fibula and then disruption of the ligament complex. The treatment of these injuries including when surgery should be performed as well as what surgery should be performed continues to evolve and be somewhat controversial.
What’s the Diagnosis Case 175
63
References
Acute and Chronic Syndesmotic Instability: Role of Surgical Stabilization. Derek S Stenquist, Michael Y Ye, John Y Kwon. Clin Sports Med. 2020 Oct;39(4):745-771. doi: 10.1016/j.csm.2020.06.002. Epub 2020 Aug 13. Management of Syndesmotic Ankle Injuries in Children and Adolescents. Shore, Benjamin J. MD, MPH, FRCSCKramer, Dennis E. MD. Journal of Pediatric Orthopaedics June 2016, Volume 36p S11 S14 Copyright © 2016 Wolters Kluwer Health, Inc. All rights reserved. DOI: 10.1097/BPO.0000000000000767 ISSN: 0271-6798
What’s the Diagnosis Case 175
64
