




















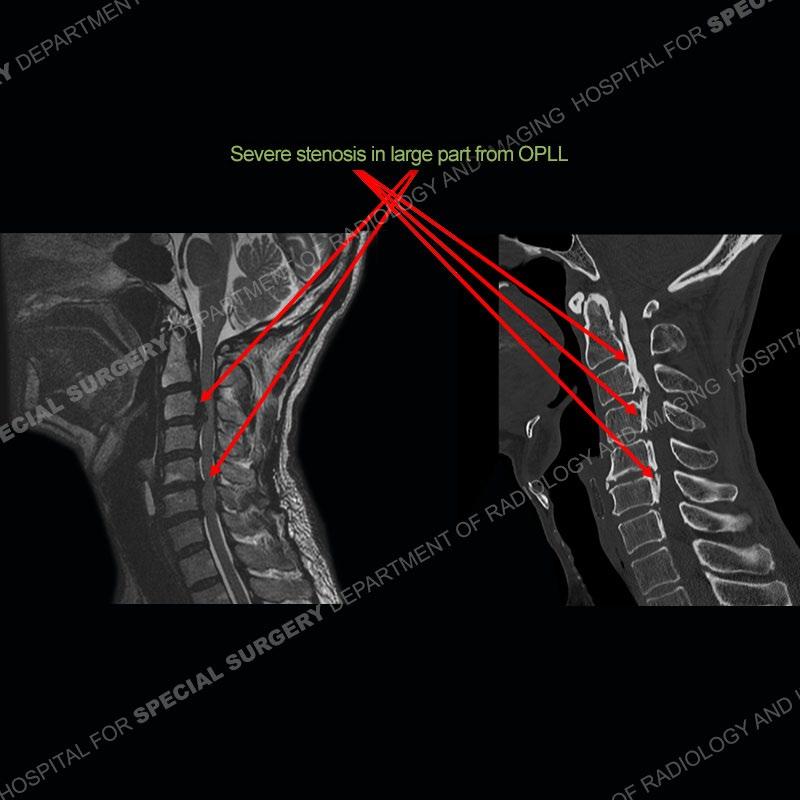
Findings
Preoperative imaging shows severe central canal stenosis at many levels of the cervical spine, in large part related to ossification of the posterior longitudinal ligament (OPLL). On the preoperative MRI, there is trace T2 hyperintensity/edema of the cord. The patient is seen to have undergone posterior fusion and decompression at C2-C3 and decompression via laminoplasty of C4-C6. Expected positioning of the hardware on the radiographs. Post-operative MRI demonstrates post-operative changes of recent surgery (earlier the same day) particularly of the posterior soft tissue. There is very good decompression of the cervical spine. However, now seen is marked edema of the cord especially about C3-C4.








Diagnosis: White Cord Syndrome (WCS)
A thankfully uncommon complication that occurs in the setting of long standing central canal stenosis as in the case of OPLL. It is postulated that during the decompression, there is reperfusion to previously injured cord which produces oxygen-derived free radicals. These then can damage the cord through so called “oxidative stress”. Not originally described in the history but in this case and is often the situation, motor potentials can be lost at the time of surgery. Patients wake up with loss of motor function or quickly develop a loss of motor function. Sensory dysfunction can also occur.
On imaging, there is marked edema or T2 hyperintensity of the spinal cord at the area of decompression. This edema represents the injury caused by the aforementioned oxidative stress. This entity is a diagnosis of exclusion with hematoma or other more common post-operative complications needed to be excluded. Predicting who may have this complication is not well understood at this time. As in this case, quick recognition of motor/sensory potential abnormalities is critical as is rapid evaluation with MRI. Unfortunately, treatment is still limited and not well delineated with high dose steroids being the current mainstay treatment. As of this time, this patient has begun to improve and is undergoing rehabilitation therapy.
References
Yen Hsin L, Samynathan C VV, Yilun H. White Cord Syndrome: A Treatment Dilemma. Cureus. 2023 Apr 26;15(4):e38177. doi: 10.7759/cureus.38177. PMID: 37252488; PMCID: PMC10224717.
Dahapute AA, Balasubramanian SG, Annis P. White cord syndrome following posterior decompression and fusion for severe OPLL and an acute traumatic cervical injury - A case report and review of literature. Surg Neurol Int. 2022 Oct 28;13:501. doi: 10.25259/SNI_692_2022. PMID: 36447894; PMCID: PMC9699864.