

























Findings
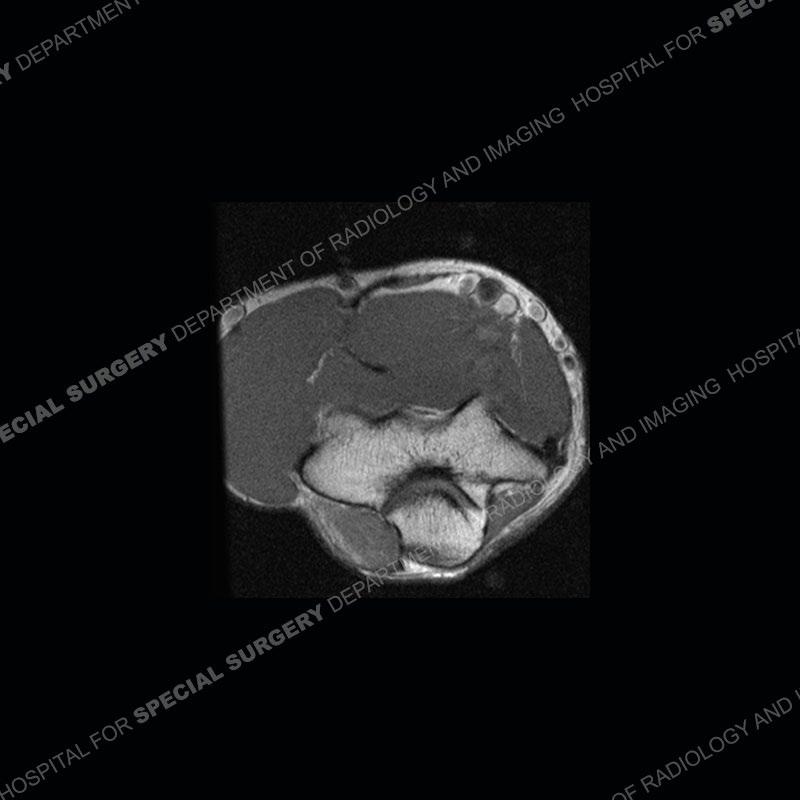
The radiographs are normal. On the MRI, the ulnar nerve has enlarged and T2 hyperintense fascicles proximal to and as it traverses the cubital tunnel. Just distal to the triceps attachment, a muscle is seen of the medial elbow, effacing the fat of the cubital tunnel and causing mass effect of the traversing ulnar nerve.




















Diagnosis: Ulnar Nerve Compression from Anconeus Epitrochlearis
Muscle
The anconeus epitrochlearis is considered an accessory muscle although it may have served some purpose in the ancient past. In most individuals it has become attenuated to form the roof of the cubital tunnel or Osborne’s ligament. In some individuals, the muscle persists and can cause an effacement of the fat of the cubital tunnel and it’s contents, the ulnar nerve. Just distal to the medial head of the triceps insertion, there should be fat present of the ulnar nerve and no muscle. The anconeus epitrochlearis may at times be associated with hypertrophy of the medial head of the triceps which can contribute to the mass effect upon the cubital tunnel and the ulnar nerve.
These patients may or may not be symptomatic. In this case, one can see the enlargement and T2 hyperintensity of the fascicles of the ulnar nerve. The imaging findings of the ulnar nerve do however remain somewhat nonspecific. There is a broad range of reported prevalence in the population but probably around 15% and with a relatively high frequency of bilaterality. In symptomatic patients, conservative measures can be attempted but unfortunately frequently fail. The surgical treatment is still debated as relates to releasing the muscle (myotomy), excision of the muscle (myomectomy), medial epicondylectomy, and the role of nerve transposition.
References
Cammarata, Michael J. BS; Hill, J. Bradford MD; Sharma, Sheel MD. Ulnar
Nerve Compression due to Anconeus Epitrochlearis: A Case Report and Review of the Literature. JBJS Case Connector 9(2):p e0189, April-June 2019.
| DOI: 10.2106/JBJS.CC.18.00189