IFMSA-Egypt Research Methodologies Manual





Because of expense, time, and accessibility, collecting data from the whole target population is almost always unfeasible. Thus, researchers use techniques (sampling techniques) to decide on a subset or a smaller group, a sample, from the target population to collect data from. These sampling techniques are designed so that the data collected from the sample is representative of the whole target population. (Cohen, Manion & Morrison, 2007).
1. Population: is the entire group of people (or any other elements) who possess specific attributes that a researcher is interested to study. There are two types of population:
A. Target population: population under study to which the researcher wants to generalize the research findings.
B. Accessible population: part of the target population that is available to the researcher. (Phillips & Stawarski, 2016)
2. Element: Is the single member of the population under study. It is also called subjects, respondents, or participants.
3. Sampling: It is the process of selecting a portion of the population to obtain data regarding a research problem.
4. Sample: A portion of the population that has been selected to represent the population of interest, and from which data will be collected.
5. Sampling frame: It is a comprehensive list of all the sampling elements in the accessible population. The sample is selected from the sampling frame.
6. Representativeness: It is how well the sample represents the variables of interest in the target population, as well as other demographic characteristics.
The sample should replicate the population in approximately the same proportions as it occurs in the target or accessible population. This is achieved by randomization.

7. Sampling bias: It occurs when the researcher shows a preference in selecting one participant over another. This bias increases when random selection is not used.
8. Inclusion criteria: The characteristics that each sample element must possess in order to be included in the sample.
9. Exclusion criteria: The characteristics that an element may possess and could confound or contaminate the results of the study. Such elements should not be included in the sample.
10. Sampling plan: It is a description of the strategies that will be used to obtain the sample of the study, It should include the sample size, type, as well as inclusion and exclusion criteria.
11. Randomization: Randomization is a systematic process where the researcher can specify the chance of each element of the population to be selected for the sample. It is used to ensure that selections are made independent of each other and there is no bias in selecting the sample. Randomization is employed to ensure that the variable of interest will be present in the sample to the extent as it would be in the whole population. (Phillips & Stawarski, 2016).
There are two main types of sampling techniques: Probability Sampling and Nonprobability Sampling.
It is a sampling technique in which each element or member in the accessible population has an equal chance to be selected and included in the sample. To obtain a probability sample, the researcher has to identify every element in the accessible population. That is to develop a sampling frame.
There are four types of probability sampling: Simple, Stratified, Cluster, and Systematic. (Polit & Hungler, 1978)
It Is the most basic probability sampling method. To achieve a simple random sampling the researcher first identifies the elements of the accessible population. The elements are randomly selected from the sampling frame. This could be achieved through a variety of procedures. In one procedure, names are written on slips of papers, placed in a container, mixed well, and then elements are drawn one at a time until the desired sample size is reached.
Although this procedure is sufficient to achieve simple random sampling, it could be time consuming and tiresome when a large sample size is desired. Thus, the most common way of achieving simple random sampling is using a table of random numbers. This table is usually computer-generated, and a number is assigned to each name in the sampling frame.
Numbers then are selected randomly to obtain a sample. Simple random sampling, however, has a couple of downsides which make it inconvenient to use: a complete list of accessible population is needed, which is impossible in many situations, and It does not guarantee a high representation level with very high population sizes. (Phillips & Stawarski, 2016).
This method is used when the researcher knows some of the characteristics of the population (variables) that are critical in achieving representativeness. Here, the researcher divides the accessible population according to mutually exclusive variables.
Mutually exclusive means that each sample element belongs to only one group or stratum. Then, the researcher selects a sub-sample from each group or stratum randomly.
Moreover, Proportional stratified random sampling is a method that increases representativeness of variables in the sample. In this method, the number of elements taken from each stratum is proportional to the number of elements in the accessible population. This sampling technique ensures the representation of each sub-group in the accessible population. However, it requires specific information about the population in order to stratify it accurately, and a complete list of accessible population is required. (Polit & Hungler, 1978).
Here, the population to be studied is too large and/or geographically scattered over a grand space (Polit & Hungler, 1978). Therefore, it is difficult or impossible to obtain a sampling frame for randomization. For example, if a study is to be conducted over all doctors in Egypt.
To select a random sample from this population, multistage/cluster random sampling is appropriate because simple and stratified techniques would be inconvenient. Cluster sampling is carried out through dividing the large populations in clusters using simple or stratified. Then, the researcher obtains sample frames out of these clusters to select the sample from. This process could be repeated until a reasonable cluster is reached where the researcher can obtain a sample frame and select a sample from that frame.
Because selecting a sample from clusters is done in two or more stages, cluster sampling is also referred to as Multi-stage random sampling. These multiple stages also contribute to increased sampling error. (Phillips & Stawarski, 2016).
Like both simple and stratified random sampling, this method requires an ordered list of all members of the accessible population. This technique depends on selecting every kth subject from the sample frame (Phillips & Stawarski, 2016). To achieve this, the researcher would divide the population sum by the sample size desired to get the sampling interval (k).
For example, if a researcher wants a sample of 50 from a population of 400 subjects, the sampling interval (k)=400/50=8. This means that the researcher will choose every 8th subject from the population. While this technique is easy and inexpensive, the researcher needs to be careful when listing the population elements in the sample frame. Unless elements on the sample frame are randomized and do not have a certain order whatsoever, bias will occur. (Polit & Hungler, 1978).
In non-probability sampling, random selection is not used. Thus, each element or participant in the accessible population does not have equal chance to be included in the sample. Accordingly, the sample may not be representative of the population, and the study results therefore cannot be generalized to the general population. However, this sampling technique is less expensive and less complicated. There are three types of non-probability sampling: Convenience, Quota, and Purposive Sampling. (Phillips & Stawarski, 2016)
This technique uses participants who are easily accessible to the researcher and who meet the criteria for inclusion. Thus, subjects/elements are included in the study just because they are available at a certain time in a certain place.
For example, a researcher might select a sample by choosing every fifth patient who enters the clinic on a certain day.
It Is a type of convenience sampling. Snowball sampling is when the researcher gets assistance from subjects to bring more subjects who meet the inclusion criteria into the study. (Phillips & Stawarski, 2016)
This method is similar to the stratified random sampling in that the participants are divided into strata based on specified characteristics to provide representativeness of different groups within the accessible population. Yet, this differs from stratified random sampling in that the elements are not randomly selected from each group/stratum (Polit & Hungler, 1978). The researcher first determines which strata are to be studied. A stratum can be age group, sex, educational level, diagnosis, etc. Then, the researcher will calculate the quota (or number) of participants needed for each stratum. This quota can be computed proportionally to the population. Members are then selected from each quota conveniently and not randomly.
In this technique, the researcher (based on his knowledge and/or experience) selects the elements of the study sample. According to the researcher, the chosen elements are thought to best represent the phenomenon being studied.
Sampling
This sampling technique is usually used in qualitative research. This technique allows the researcher to handpick, so it is easy, simple, and time saving. However, the generalizability of the research findings is very limited. (Polit & Hungler, 1978)
To choose an appropriate sampling technique, the researcher should identify the research goals and select the sampling methods that would achieve these goals.
Next the researcher should test each method for satisfying the research goal and then choose the best method. Also the researcher should consider the inclusiveness of the sample and representability.
Also, the feasibility, resources and access to population play great roles in the final decision for a sampling strategy.
A cross-sectional study is defined as a type of observational research that analyzes data of variables collected at one given point in time across a sample population or a pre-defined subset like a snapshot.
Researchers can conduct a cross-sectional study with the same set of variables over a set period.
Similar research may look at the same variable of interest, but each study observes a new set of subjects.
The cross-sectional analysis assesses topics during a single instance with a defined start and stopping point, unlike longitudinal studies, where variables can change during extensive research.
Cross-sectional studies allow the researcher to look at one independent variable as the focus of the cross-sectional study and one or more dependent variables.
In which the investigator measures the outcome and the exposures in the study participants at the same time.
Cross-sectional studies can be classified as descriptive or analytical, depending on whether the outcome variable is assessed for potential associations with exposures or risk factors and there is another type which is repeated (or serial) cross-sectional study.
Descriptive
1. Assesses how frequently, widely, or severely the variable of interest occurs throughout a specific demographic.
2. Simply characterizes the prevalence of one or multiple health outcomes in a specified population.
3. Generates hypotheses.
4. Answers what, who, where, and when questions.
Analytical
1. Investigators collect data for both exposures and outcomes at one specific point in time for the purpose of comparing outcome differences between exposed and unexposed subjects
2. Investigates the association between two related or unrelated parameters
3. Tests hypotheses
Data collection is conducted on the same target population at different time points.
At each time point, investigators take a different sample (different subjects) of the target population, thus, repeated cross-sectional studies can be used for analyzing population changes over time (also known as aggregate change over time).
They cannot be used to look at individual change (as in a cohort study).
For example, Zito et al.
Using annual cross-sectional surveys, Zito et al. reported that the prevalence of prescription psychotropic drug use among youth (people <20 years old) increased more than threefold between 1987 and 1996 in a mid-Atlantic Medicaid population. This is not a cohort design because it does not follow a single group of people over time; there are changes in the population over time due to births, deaths, aging, migration, and eligibility changes.

Learn about characteristics such as knowledge, attitude, and practices of individuals in a population.
Used to collect all variables at one time.
Multiple outcomes can be researched at once.
Prevalence for all factors can be measured which can be assessed at either one point in time (point prevalence) or over a defined period (period prevalence).
Suitable for descriptive analysis.
Researchers can use it as a springboard for further research.
Monitors trends over time with serial cross-sectional studies.
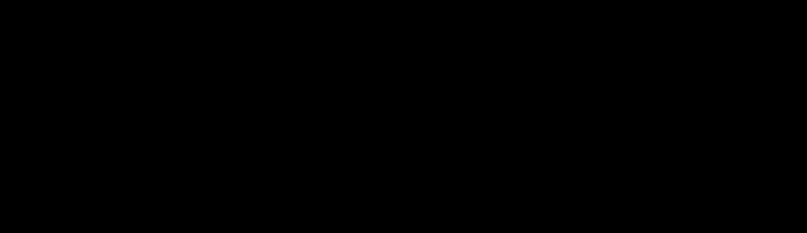
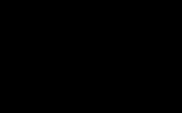
We define a population and determine the presence or absence of exposure and the presence or absence of disease for everyone at the same time. Each subject then can be categorized into one of four possible subgroups.
Design of a hypothetical cross-sectional study: I. Identification of four subgroups based on presence or absence of exposure and presence or absence of disease.
There will be (a) persons who have been exposed and have the disease; (b) persons who have been exposed but do not have the disease; (c) persons who have the disease but have not been exposed; and (d) persons who have neither been exposed nor have the disease. If we use (a) and (b), we can compare the prevalence of exposure in persons with the disease to the prevalence of exposure in persons without the disease.
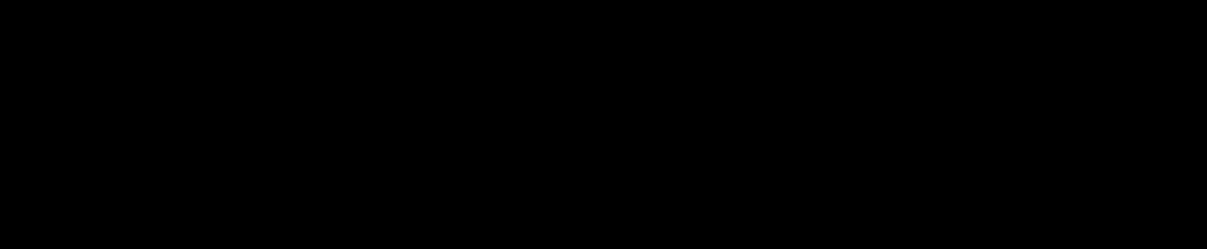
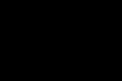
Design of a hypothetical cross-sectional study II: (top) A 2 × 2 table of the findings from the study; (bottom) two possible approaches to the analysis of results: (A) Calculate the prevalence of disease in exposed persons compared to the prevalence of disease in non-exposed persons, or (B) Calculate the prevalence of exposure in persons with disease compared to the prevalence of exposure in persons without disease.
Fast and Inexpensive.
No ethical difficulties.
There is no loss to follow-up.
These studies are conducted either before planning a cohort study or a baseline in a cohort study. These types of designs will give us information about the prevalence of outcomes or exposures; this information will be useful for designing the cohort study.
They may be useful for public health planning, monitoring, and evaluation.
Data on all variables is only collected once.
Able to measure prevalence for all factors under investigation.
Multiple outcomes and exposures can be studied.
The prevalence of disease or other health related characteristics are important in public health for assessing the burden of disease in a specified population and in planning and allocating health resources.
Good for descriptive analyses and for generating hypotheses.
It is difficult to derive causal relationships from cross-sectional analysis.
As cross-sectional studies measure prevalent rather than incident cases, the data will always reflect determinants of survival as well as etiology.
Unable to measure incidence.
Associations identified may be difficult to interpret.
Susceptible to bias either due to low response and misclassification due to recall bias, temporal bias, survival, or selection bias.
Generalizability limited by sampled population and population definition
Study sought to determine the prevalence of asthma in children and analyze its association with being a passive smoker, being exposed to vehicular traffic (both risk factors) and the intake of dehydrated fruit (a possible protective factors) the researchers found that the prevalence of asthma increased with the number of smokers with whom they lived, but it was not associated with living near the main avenue or the consumption of dehydrated fruits. Thus, in the cross-sectional study, there are both descriptive (an estimate of prevalence) and analytical components (study of association between variables).
Receiving voluntary family planning services has no relationship with the paradoxical situation of high use of contraceptives and abortion in Vietnam.
Patient-Related Factors Influencing Satisfaction in the Patient-Doctor Encounters at the General Outpatient Clinic of the University of Calabar Teaching Hospital, Calabar, Nigeria.
Cross-sectional pilot study of antibiotic resistance in Propionibacterium acnes strains in Indian acne patients using 16s-RNA polymerase chain reaction: A comparison among treatment modalities including antibiotics, benzoyl peroxide, and isotretinoin.
A representative study of a specific population to collect information on what is known, believed, and done in relation to a particular topic
It is a quantitative method (predefined questions formatted in standardized questionnaires) that provides access to quantitative and qualitative information. It is also Conducted to collect information on the knowledge (i.e., what is known), attitudes (i.e., what is thought), and practices (i.e., what is done) about general and/or specific topics of a particular population.
The knowledge part is normally used only to assess the extent of community knowledge about public health concepts related to national and international public health programmes. Investigation of other types of knowledge, such as culture-specific knowledge of illness notions and explanatory models, or knowledge related to health systems, e.g., access, referral, and quality, is highly neglected.
Measuring attitudes is the second part of a standard KAP survey questionnaire. However, many KAP studies do not present results regarding attitudes, probably because of the substantial risk of falsely generalizing the opinions and attitudes of a particular group.(Cleland 1973, Hausmann-Muela et al. 2003)

The act of measuring attitudes via a survey has been criticized for many reasons. When confronted with a survey question, people tend to give answers which they believe to be correct or in general acceptable and appreciated, sensitive topics are particularly demanding.
The survey interview context may influence the answer: whether the interview is conducted at a clinic or in a village, whether there are other people present, etc. The question formulation can be manipulative towards a favorable answer. Sometimes, the respondents may be uninformed about the issue and thus find it strange, but their attitudes are nonetheless measured. On occasion, the attitude scales (numbers/verbal) may fail to reflect the respondents' answers. (Cleland 1973, HausmannMuela et al. 2003, Pelto and Pelto 1994)
A third and integral part of KAP surveys is the investigation of health-related practices.
Questions normally concern the use of different treatment and prevention options and are hypothetical.
KAP surveys have been criticized for providing only descriptive
data which fails to explain why and when certain treatment prevention and practices are chosen. In other words, the surveys fail to explain the logic behind people's behavior.
1. Gather information about general practices and beliefs.
2. Measure the extent of a known situation, confirm or disprove a hypothesis, or provide new tangents of a situation’s reality.
3. Enhance the knowledge, attitude, and practices of specific themes; identify what is known and done about various health-related subjects.
4. Establish the baseline (reference value) for use in future assessments and help measure the effectiveness of health education activities' ability to change health-related behaviors.
5. Suggest an intervention strategy that reflects specific local circumstances and the cultural factors that influence them; plan activities that are suited to the respective population involved.
6. To assess and identify communications processes and sources important for program implementation and effectiveness.
7. To help set program priorities and make program decisions.
8. To generate baseline levels and measure changes that result from interventions.
Number of Staff Required:
The team will be composed of surveyors and supervisors. The number of supervisors is directly dependent on the number of surveyors, which is determined by the size of the survey and the resources available. Each supervisor should have daily face-to-face contact with each of the surveyors that s/he supervises. For 10-15 surveyors, for example, two supervisors work quite well.
Training:
Training surveyors is crucial. The training lasts two-to-four days depending on the complexity of the survey and questionnaire and the experience level of surveyors recruited.
The training should allow surveyors to master the knowledge, skills, and expertise specific to the KAP survey.
1. Step One: Define the survey objectives: Review existing information, determine the purpose of the survey, identify the areas of enquiry, identify the survey population, and create a sampling plan.
2. Step Two: Develop the survey protocol: Organize the contents of the survey protocol, define the key research questions, determine whether the survey needs ethical review, create a work plan, and develop a budget.
3. Step Three: Design the survey questionnaire: Develop the survey questionnaire, make a data analysis plan, and pre-test and finalize the questionnaire.
4. Step Four: Conduct the KAP survey: Choose survey dates and timeline, recruit survey supervisors and interviewers, train supervisors and interviewers, and ensure the quality of data collected.
5. Step Five: Analyze the data: Clean the data, implement a data analysis plan, and interpret the findings.
6. Step Six: Use the data: Translate findings into action, write the survey report, disseminate findings, and use KAP survey data in programming.
A KAP survey takes between six and twelve weeks.
1. Constructing the survey protocol.
2. Preparing the survey.
3. Course of the KAP survey in the field.
4. Data analysis and presentation of the survey report.
5. Conclusion, references, and abbreviations.
KAP surveys can identify knowledge gaps, cultural beliefs, or behavioral patterns that may facilitate understanding and action, as well as pose problems or create barriers to development efforts.
They can identify information that is commonly known and attitudes that are commonly held.
To some extent, they can identify factors influencing behavior that are not known to most people, reasons for their attitudes, and how and why people practice certain behaviors.
Data can be hard to interpret accurately.
Lack of standardized approach to validate findings.
Analyst biases in KAP surveys.
Other Criticisms such as:
Their findings generally lead to prescriptions for mass behavior modification instead of targeting interventions towards individuals, For example:
A study which used KAP surveys to study the AIDs epidemic found that “these unfocused inquiries into diffuse behaviors in undifferentiated populations are not productive in low-seroprevalence populations, especially when the objective is to design interventions to avert further infection. The failure of KAP surveys to distinguish conceptually between the relevance of AIDS-related behavioral data for individuals and for populations makes them fundamentally flawed for such purposes.
The investigators use the surveys to explain health behavior under the assumption that there is a direct relationship between knowledge and action.
A popular means of gauging people’s opinion of a particular topic, such as their perception or reported use of an eHealth system. The process of conducting research using surveys that researchers send to survey respondents, the collected data is statistically analyzed to draw meaningful research conclusion
Often the terms “survey” and “questionnaire” are used interchangeably as if they are the same. But strictly speaking, there is a difference.
A research approach where subjective opinions are collected from a sample of subjects and analyzed for some aspects of the study population that they represent.
According to the purpose
One of the data collection methods used in the survey approach, where subjects are asked to respond to a predefined set of questions.
Used to investigate and understand a particular issue or topic area without predetermined notions of the expected responses
The design is mostly qualitative in nature, seeking input from respondents with open-ended questions focused on why and/or how they perceive certain aspects
-Crosssectional
-Longitudinal
Used to describe the perception of respondents and the association of their characteristics.
The design is mostly quantitative and involves the use of descriptive statistics such as frequency distributions of Likert scale responses from participants.
Used to explain or predict one or more hypothesized relationships between some respondent characteristics.
The design is quantitative, involving the use of inferential statistics such as regression and factor analysis to quantify the extent to which certain respondent characteristics lead to or are associated with specific outcomes.
-Single cohort of respondents.
-Multiple cohorts of respondents.
-Nominal
-Ordinal
-Interval or ratio
-Questionnaire surveys: May be mail-in, groupadministered, or online surveys
Instruments that are completed in writing by respondents
-Interview surveys: May be personal, telephone, or focus group interviews
Completed by the
interviewer based on verbal responses provided by respondents
1. Online/ Email/ SMS:
The most popular survey research methods these days.
Their cost is extremely minimal.
The responses gathered are highly accurate.
2. Phone:
Useful in collecting data from a more extensive section of the target population.
There are chances that the money invested in phone surveys will be higher than other mediums, and the time required will be higher.
3. Face-to-face:
The response rate for this method is the highest.
It can be costly.
Surveys can be conducted faster and cheaper compared to other methods of primary data collection such as observation and experiments.
Surveys are an excellent vehicle for measuring a wide variety of unobservable data, such as people’s preferences (e.g., political orientation), traits (e.g., self-esteem), attitudes (e.g., toward immigrants), beliefs (e.g., about a new law), behaviors (e.g., smoking or drinking behavior), or information (e.g., income).
Survey research is also ideally suited for remotely collecting data about a population that is too large to observe directly.
Due to their unobtrusive nature and the ability to respond at one’s convenience, questionnaire surveys are preferred by some respondents.
Interviews may be the only way of reaching certain population groups such as the homeless or illegal immigrants for which there is no sampling frame available.
Large sample surveys may allow detection of small effects even while analyzing multiple variables, and depending on the survey design, may also allow comparative analysis of population subgroups (i.e., within-group and between-group analysis).
It is subject to many biases such as non-response bias, sampling bias, social desirability bias, and recall bias.
In some cases, unwillingness, or inability of respondents to provide information.
Differences in understanding: it is difficult to formulate questions in such a way that it will mean exactly the same thing to each respondent.
Survey research is economical in terms of researcher time, effort, and cost than most other methods such as experimental research and case research.
Simply put, clinical trials are experimental studies on humans. Their purpose is to determine how effective a certain treatment is in patients with a certain diagnosis. Results from a sample of patients are used to draw conclusions on a population of present and future patients.
Most clinical trials are conducted by pharmaceutical companies to investigate the effects of certain drugs. However, clinical trials may also be used to investigate other modes of treatment, like surgery, counseling, or radiation therapy.
A procedure in which one or more parties in a trial are kept unaware of which treatment arms participants have been assigned to, i.e. which treatment was received in order to avoid bias.
The focus of conducting a randomized controlled trial (RCT) is the elimination of bias. Unconscious information bias may be introduced if the investigators or participants are aware of who is getting the intervention and who is not.
Unblinded or open label: All are aware of the treatment the participant receives.
Single blinded: A single stakeholder is blinded i.e. they do not know which group the participants have been assigned to or what treatment they are receiving. Usually, the participant is blinded, and only the data collectors and the researchers know which group they’ve been assigned to.
Double-blinded: Two stakeholders are blinded, usually the participants plus the data collectors OR the researchers. Neither of the two blinded parties knows which group the participant falls in.
Triple blinded: The participant, the researchers, and the data collectors are all blinded. None of the parties know which group the participant falls in.
Participants in a trial: Awareness of group assignment will influence their behavior in the trial and their responses to subjective outcome measures if participants are not blinded. A participant who is conscious of not receiving active therapy, for example, maybe less likely to conform with the trial procedure, more likely to pursue further treatment beyond the trial, and more likely to exit the trial without presenting outcome results
Clinicians: Blinded clinicians are far less inclined than unblinded clinicians to shift their behaviors to participants or have preferential care for the active and placebo classes.
Data collectors and Outcome adjudicators: To ensure unbiased ascertainment of outcomes, blinding of data collectors and outcome adjudicators (sometimes the same individuals) is crucial.
For example, in a randomized controlled study of cyclophosphamide and plasma exchange in multiple sclerosis patients, when examined by blinded neurologists, no successful therapy regimen was superior to placebo, however, there was an obvious advantage from cyclophosphamide, plasma exchange, and prednisone treatment when evaluated by unblinded neurologists
Data analysts: By selective use and reporting of statistical measures, bias can also be added during the statistical study of the trial. This may be a subconscious process motivated by researchers willing to see a good outcome, but there are profound implications.
Placebo: intervention indistinguishable from the experimental intervention
“Double‐dummy” : design (i.e., comparing active A + placebo B with active B + placebo A)
Sham surgery: which is a fake surgery that omits the step, is thought to be therapeutically necessary. But, it is ethically controversial in some surgeries where control group patients might be at risk when exposed to operations.
N.B
- Experiments are sometimes simply defined as 'blind' or 'double-blind' and do not indicate who was blinded, which suggests that one or more patients, healthcare professionals, result evaluators, and observers were blinded. Thus, it
- As part of the technique, all blinding techniques should be clarified and gain ethical consent from scientific ethics committees.
Blinding is used to prevent conscious or unconscious bias in the design of a clinical trial and how it is carried out. It is used to ensure the objectivity of trial results. Lack of blinding has been found to be consistent with more exaggerated predicted intervention results in randomized controlled trials (RCTs), by 9 percent on average. (In a systematic analysis of 250 RCTs found from 33 meta-analyses, researchers noticed a substantial gap in the magnitude of the predicted treatment effect between studies that reported double-blinding relative to nonblinding studies (p = 0.01), with an average odds ratio of 17 percent greater in studies that did not mention blinding.)
The placebo effect is often addressed or regulated by blinding (placebo effect: a mechanism in which a virtual -and ineffective- therapy will often improve the health of a patient, merely because the individual believes it to be helpful. In the placebo effect, anticipation is central.)
In some cases, blinding is not possible such as some surgeries or due to unethical considerations.
Conceals randomization sequences.
Eliminate selection bias during the process of recruitment and randomization.
Done when participants enter trials (during the recruitment).
A procedure in which one or more parties in a trial are kept unaware of which treatment arms participants have been assigned to, i.e., which treatment was received in order to avoid bias.
Seeks to reduce performance and ascertainment bias after randomization.
Done after the participants entered the trail (after recruitment)
Differences between sampling and allocation into groups
The method by which the participants were selected for the trial
Random allocation is how participants were allocated to treatment.
Randomization eliminates accidental bias, including selection bias, and provides a base for allowing the use of probability theory.
It promotes the comparability of the sample groups and provides the basis for statistical inference for the quantitative evaluation of the impact of medication as it is used to create similarity of groups.
Simple randomization
It is a process that guarantees Participants in the trial have a fair probability of being allocated to a group of therapies. The techniques of sequence generation by simple randomization procedure include:
Tossing of a coin
Die throwing
Card shuffling
Using table of random numbers
The major disadvantage of simple randomization is that the treatment groups can, by chance, end up being dissimilar both in size and in prognostic factors; these imbalances might be substantial in small sample trials.
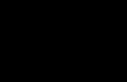
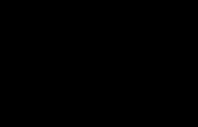
It operates by randomizing participants inside blocks such that each therapy is given an equal number.
For example,
With a block size of 4, there is an assurance that the group is balanced each time the 4th patient is enrolled. With a block of size 4, there are six ways in which we can allocate treatments so that two subjects get A and two get B:
Treatment groups will be equal in size and tend to be distributed uniformly according to key characteristics related to the results. In time, smaller block sizes will result in more balanced groups than larger block sizes.
That when the research groups are unmasked, the allocation of participants can be predictable and result in selection bias. That is, the care assignment that has happened so far the least often in the block is likely to be the next one selected.
N.B: By using random block sizes and holding the investigator oblivious to the scale of each block, selection bias can be minimized.
Stratified random allocation
This is a procedure that splits the trial Participants into strata according to meaningful Prognostic factors linked to results; follow-up The classification and distribution process takes place. The participants are inside each stratum by which they are assigned to treatment groups using separate treatment groups Schedules of randomization. Importance:
Simple randomization sometimes fails to establish equilibrium in baseline prognostic variables between therapies groups, especially when the sample size is low; The first stratified random allocation constitutes the first effort to correct the template for this.
Stratification reduces variance, Both power and precision are inversely related to the variance.
It has been suggested that the drug effect estimation can be more reliable and has more strength in a limited sample size study following a stratified random allocation process.
Increased efficiency, facilitation of subgroup analysis, and protection against type I error.
It is a way of changing the probability of allocation according to the study's progress and position. It can be used both to minimize the imbalance between treatment groups, and to alter the probability of allocation based on the therapeutic effect.
To minimize the disparity, covariate adaptive randomization changes the distribution of a subject, taking into consideration the imbalance of the prognostic variables.
One example is the minimization randomization (minimization) strategy to establish metrics that jointly assess and distribute the distributional imbalance of different prognostic variables to mitigate the imbalance.
To balance the prognostic factors, minimization was first adopted as a covariate adaptive process.
By simple randomization, the first subject is allocated, and the following ones are allocated to match the prognostic factors. In other words, to assign the newly recruited subjects and reduce the imbalance of the prognostic variables, the data of the subjects that have already participated in the analysis is used to. One of drawbacks From a statistical point of view, it does not satisfy randomness, which is the underlying hypothesis of statistical inference.
In order to select participants, certain eligibility criteria are used. Eligibility criteria describe the specific parameters of the population to be studied, including the age range, the diagnosis, prior therapy allowed, and organ function requirements.
Each of the eligible participants should have an equal chance to be allocated the intervention or not. One way of achieving this is by the parallel-group design. Here, each group of participants is exposed to only one of the study interventions.
Another way of achieving this is by using a crossover design. In a crossover design, all the trial participants sequentially receive both interventions. The only component being assigned here is the order of intervention. A participant can receive the experimental treatment followed by the placebo, or the other way around.
The protocol should be reviewed and approved by an independent ethics committee before starting the trial. For clinical trials, it is now obligatory that protocols are registered with a publicly available trial registry before recruiting any participants to the trial.
The patient is registered using a procedure that is described in the protocol. In order to register, the patient has to go to the central registration office of the trial, usually in a healthcare setting. Eligibility will be checked by conducting laboratory tests, weighing the patient, etc. This data is documented prior to the start of the trial. Informed consent, usually through a written form, is also obtained to ensure that the study proceeds in an ethical manner. Each participant is assigned a unique identification number.
A randomized controlled trial (RCT) is a study design in which participants are randomly assigned to an experimental group or a control group. It is the most commonly used clinical study, because it measures the efficacy of a certain treatment or intervention on a group of patients with the same diagnosis.
The experimental group receives the new intervention or drug that is being tested. On the other hand, the control group receives the conventional intervention or drug or receives no treatment at all (i.e. a placebo).
The two groups are then followed up to see if there are any differences between them in the outcome. If the experimental group shows a greater improvement in their health condition, then the new intervention or drug is said to be effective. The results and subsequent analysis of the trial are used to assess the effectiveness of the intervention.
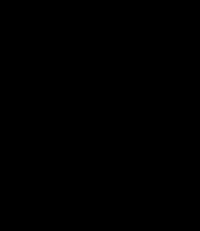
Because the outcomes are measured, randomized controlled trials are considered quantitative studies. They are one of the simplest, yet most effective study designs. They also provide high-quality evidence with low levels of bias. On the pyramid of evidence, RCTs fall near the very top, or apex, right below systematic reviews and meta-analyses of RCTs.
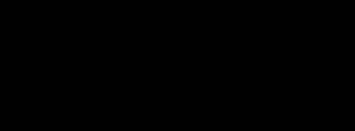
Pre-clinical phase: In this phase, researchers test the drug on non-human subjects, usually animals. The effects of the drug on the animal are studied. Rodent and non-rodent mammalian models are used to determine the drug’s pharmacokinetic profile, safety, and adverse effects. One or more species may be used. This phase can last for several months.
Phase 0: This is the very first phase of the trial that involves human subjects. In this phase, researchers aim to learn how a drug is metabolized in the body and the effects it exerts. A very small dose of a drug is given to about 10 to 15 healthy people. This phase lasts several months.
Phase I: In this phase, a trial is conducted on a small group of patients with the same disease or condition. Its purpose is to study the toxicity and side-effects of the drug. Typically, there are 10-30 participants, but some phase I trials can include up to 100 participants. Like phase 0, phase I also lasts several months.
Phase II: Small groups of patients are used to study the effects of various doses of a drug. When a drug is believed to have shown promising effects in these early phases of its development, it is desirable to test the new treatment against the standard treatment. Like Phase I, Phase II also uses patients with the same disease or condition. Phase II can involve up to several hundred people. The length of this phase ranges from several months to two years.
Phase III: Phase III comprises larger clinical trials that compare the effects of the experimental (new) drug with a placebo or a conventional drug typically used for treatment. These trials are used to document the effects of a new drug and compare its efficacy to a standard drug. This is the last phase before the manufacturer applies for marketing authorization, or for the drug to be licensed for selling. Phase III trials are those that most often come to mind when clinical trials are mentioned; because they use the RCT study design. Phase III can involve anywhere from 300 to 3,000 participants, and usually lasts from one to four years. There are some exceptions as regards to the duration, like the Covid-19 vaccine, whose phase III trials lasted only six months due to the urgent state of the pandemic.
Phase IV: This is the postmarketing phase. It covers both long-term studies of safety and pure marketing studies. Phase IV trials test new drugs after they’ve been approved. The drug is tested in several thousand patients. The advantage of using a large group of participants is that it increases the probability of discovering rare side effects. This allows for better research on short-lived and long-lasting side effects and safety. Doctors can also learn more about the efficacy of the drug and its effect when used with other treatments.
The research protocol is the plan for the researcher’s project, or what they will accomplish when they start the study with their research team. It describes the reasoning behind and the process of the research project, including what the researcher hopes to accomplish and how they will accomplish it.
In drafting a research protocol, the researcher must answer a few questions:
1. What: What is the research question? What methods will be used to answer the research question?
2. Where: Where will the research project take place?
3. When: When, or over what period of time, will the research project take place?
4. Why: Why is this research project/study being conducted?
5. How: How will the research question be answered? How will the research project be conducted?
1. Project title and date
2. Personal information: of the primary investigator and their co-investigators
3. Background and rationale: The background and rationale are equivalent to the introduction in a research report.
The background describes the studies, results and references that are relevant to the design and conduct of the study.
The rationale specifies the reasons for conducting the research project.
4. Research Objectives and Hypothesis: This section states the precise objectives of the study in the form of a hypothesis. The rest of the protocol should be designed to answer the hypothesis posed here.
5. Study design: The study design describes the type of study proposed (observational, RCT, etc.). It also describes the sequence of the study. It includes information on the type of study, the research population or the sampling frame, who can take part, and the expected duration of the study.
6. Methodology: The methodology section is the most important part of the protocol. It should include detailed information on the procedures to be used, measurements to be taken, observations to be made, etc.
7. Safety Considerations: Safety aspects of the research should always be kept in mind and information must be provided on how the safety of research participants will be ensured.
8. Follow-up (applies to RCTs)
9. Data Management and statistical analysis: The statistical methods proposed to be used for the analysis of data should be clearly outlined. For qualitative data, specify in sufficient detail how the data will be analyzed.
10. Expected outcomes of the study
11. Quality assurance and ethical considerations
A research proposal describes an idea for a project. It focuses on the research question the researcher hopes to answer. A research proposal tells how a researcher might attempt to answer the question, and how they will obtain the data they need. It may also include a focused literary search, and might include the results of a pilot project.
A research protocol is the next stage, representing a detailed road map showing how the researcher will successfully complete the project. It answers more questions than the research proposal, like the duration of the project and where it will be conducted. A research protocol also further elaborates on how the research question will be answered, and what methods will be used.
Institutional review board:
It’s a group federally mandated to review and monitor research involving humans to ensure protection of their rights and welfare as research participants.
IRB approval is required for all research involving human participants, whether living individuals, data, or specimens.
Mostly include researchers, but also, include community members and persons who are known about ethical and legal issues of research.
Ensure that the research is ethically acceptable and that the welfare and rights of research participants are protected.
Each local committee has its federal regulations according to its discipline and the type of research that need the approval, but there are some ethical issues should be determined by IRB when approving the research protocol:
Participants’ autonomy through their informed consent or their representatives after explaining all things about the expected results of these studies.
Maximizing the benefits for participants.
Minimizing the harms and risks.
Selection of participants is equitable.
Confidentiality is adequately maintained.
The moral principles and actions guiding and shaping research from its inception to its completion; the dissemination of findings and the archiving, future use, sharing and linking of data.
Research ethics in the social sciences initially drew on the “patient protection” model of medical research. More recently, it has broadened in scope to include consideration of benefits, risks and harms to all persons connected with and affected by the research and the social responsibilities of researchers.
Throughout history, evidence suggests that ethical issues in human experimentation had been recognized and addressed as early as the late 1800s.
The 1947 Nuremberg Code is commonly cited as the first document to govern the conduct of human research. The main cause of that is the war trials of Nazi physicians accused of conducting “murderous and torturous human experiments” on prisoners in concentration camps in the name of medical science in 1946/1947. This code included 10 ethical principles.
Link:
https://media.tghn.org/medialibrary/2011/04/BMJ_No_7070_Volume_313_Th e_Nuremberg_Code.pdf
The World Medical Association published the “Declaration of Helsinki” in 1964. This declaration expands on the ten ethical principles of Nuremberg code, but excludes 2 of the 12 items to address perceived deficiencies in the Nuremberg Code. This declaration continuously undergoes revisions.
Link:
https://www.who.int/bulletin/archives/79(4)373.pdf
The 1947 Nuremberg Code is commonly cited as the first document to govern the conduct of human research. The main cause of that is the war trials of Nazi physicians accused of conducting “murderous and torturous human experiments” on prisoners in concentration camps in the name of medical science in 1946/1947. This code included The National Research Act in 1974 was enacted in response to the Tuskegee Study of Untreated Syphilis carried out from 1932 to 1972 that withheld effective therapy for syphilis from hundreds of African American men to observe the progression of syphilis, presumably for the sake of medical research without telling them about the threats of these trails.
This act created the National Commission for the Protection of Clinical Subjects of Biomedical and Behavioral Research to oversee human experimentation in the United States.
Link:
https://www.govinfo.gov/content/pkg/STATUTE-88/pdf/STATUTE-88Pg342.pdf
In 1979, the commission drafted the Belmont Report that describes the basic ethical principles underlying the conduct of research: respect for persons beneficence, and justice
Link:
https://www.hhs.gov/ohrp/sites/default/files/the-belmont-report508c_FINAL.pdf
The Common Rule , a set of federal regulations necessitating oversight of government-funded research in the United States, was drafted in 1991. Elements of its policy center on the presence and procedures of institutional review boards (IRBs) and general requirements for informed consent
Link:
https://www.hhs.gov/ohrp/sites/default/files/ohrp/policy/frcomrul.pdf
There are three objectives in research ethics:
The first and broadest objective is to protect human participants.
The second objective is to ensure that research is conducted in a way that serves the interests of individuals, groups and/or society.
Finally, the third objective is to examine specific research activities and projects for their ethical soundness, looking at issues such as the management of risk, protection of confidentiality and the process of informed consent.
Basic Principles
Respect for people’s autonomy through informed consent, and people with diminished autonomy should be protected.
Beneficence through doing no harm, maximizing benefits for participants, and minimizing risks for them.
Justice through fairness.
Other Principles
Honesty and Integrity.
Objectivity.
Openness.
Carefulness.
Confidentiality.
Legality.
Animal Care in animal studies.
There are seven main principles that guide the conduct of ethical research involving human subjects:
Social and clinical value: The answers to the research question should contribute to scientific understanding of health or improve our ways of preventing, treating, or caring for people with a given disease to justify exposing participants to the risk and burden of research.
Scientific validity: A study should be designed in a way that will get an understandable answer to the important research question. The question asked should be answerable, the research methods must be valid and reliable, and the study has to be designed with accepted principles, clear methods, and reliable practices. Invalid research is unethical because it is a waste of resources and exposes people to risk for no purpose.
Fair subject selection: The primary basis for recruiting participants should be the scientific goals of the study. Participants must not be chosen on the basis of vulnerability, privilege, or other unrelated factors. Participants who accept the risks of research should be in a position to enjoy its benefits. Specific groups of participants (ex. women or children) should not be excluded from the research opportunities unless there is a good scientific reason or a particular susceptibility to risk.
Favorable risk-benefit ratio: Everything should be done to minimize the risks and inconvenience to research participants, while also maximizing the potential benefits. Efforts should also be made to determine that the potential benefits are proportionate to, or outweigh, the risks.
Independent review: To minimize potential conflicts of interest and make sure a study is ethically acceptable before it starts, an independent review panel should review the proposal. The independent panel ensures that the study is free of bias, ethically designed, and ensures the protection of research participants.
Informed consent: Potential participants should make their own decision about whether they want to participate or continue participating in research. This is done through a process of informed consent in which individuals:
Are accurately informed of the purpose, methods, risks, benefits, and alternatives to the research.
Understand this information and how it relates to their own clinical situation or interests.
Make a voluntary decision about whether to participate.
Respect for potential and enrolled subjects: Individuals should be treated with respect from the time they are approached for possible participation, throughout their participation and after their participation ends. Even if they refuse enrollment in a study, they should still be respected. This includes monitoring their welfare, respecting their privacy, keeping their information confidential, and informing them of new information that might emerge from the course of the study.
Ethical guidelines for animal participants are generally based on the three R’s of animal research: Replace, Reduce, and Refine.
Respect for animals’ dignity: researchers must have respect for animals' worth, regardless of their utility value, and for animals' interests as living, sentient creatures.
Responsibility for considering options: researchers are responsible for studying whether there are alternatives to experiments on animals. Alternative options must be prioritized if the same knowledge can be acquired without using laboratory animals. If no good options are available, researchers should consider whether the research can be postponed until alternative methods have been developed.
Responsibility for considering and balancing suffering and benefit: Researchers must consider the risk that laboratory animals experience pain and other suffering and assess them in relation to the value of the research for animals, people or the environment. Researchers are responsible for considering whether the experiment may result in improvements for animals, people or the environment. Suffering can only be caused to animals if this is counterbalanced by a substantial and probable benefit for animals, people or the environment.
Responsibility for considering reducing the number of animals: Researchers are responsible for considering whether it is possible to reduce the number of animals the experiment plans to use and must only include the number necessary
to maintain the scientific quality of the experiments and the relevance of the results.
Responsibility for minimizing the risk of suffering and improving animal welfare: Researchers are responsible for assessing the expected effect on laboratory animals. Researchers must minimize the risk of suffering and provide good animal welfare. Suffering includes pain, hunger, thirst, malnutrition, abnormal cold or heat, fear, stress, injury, illness and restrictions on the ability to behave normally/naturally.
Responsibility for maintaining biological diversity: Researchers are responsible for ensuring that the use of laboratory animals does not endanger biological diversity. The use of endangered and vulnerable species must be reduced to an absolute minimum.
Responsibility when intervening in a habitat: Researchers are responsible for reducing disruption and any impact on the natural behavior of individual animals, including those that are not direct subjects of research, as well as of populations and their surroundings.
Responsibility for openness and sharing of data and material: Researchers are responsible for ensuring that there is transparency about research findings and facilitating the sharing of data and material from experiments on animals. Such transparency and sharing are important in order to avoid unnecessary repetition of experiments.
Requirement of expertise on animals: Researchers and other parties who handle alive animals must have adequately updated and documented expertise on animals. This includes specific knowledge about the biology of the animal species in question, and a willingness and ability to take care of animals properly.
Requirement of due care: There are national laws and rules and international conventions and agreements regarding the use of laboratory animals, and both researchers and research managers must comply with these.
Validity: The research design must address specific research questions. Hence, the conclusions of the study must correlate to the questions posed and the results. The methods used must relate specifically to the research questions.
Efficient: makes the best source of the resources used.
Study designs and variables: it’s unethical to test some variables by specific study designs e.g: smoking and interventional study designs.
Sampling: The design must explain why the study can only be conducted on a particular group of participants. Likewise, it should explain why certain people or groups are excluded. In addition, if the study design includes children or special needs individuals, additional requirements, like parental permission, must be addressed.
Voluntary Participation and Consent: The chosen design must not, under any circumstances, coerce or pressure any subject to participate. This includes any type of persuasion or deception in attempting to gain an individual’s trust.
Confidentiality: Information provided by the research subjects must remain confidential, and the anonymity of respondents must be respected. However, if a participant is at risk of harm, their information might have to be released.
Risk of Harm: There should be a keen focus on the risk-to-benefit ratio. If possible risks outweigh the benefits, the study design must be redesigned or even abandoned altogether.
When choosing the right research methods, the investigators must ensure they are taking the most ethical approach that simultaneously yields the most accurate results. To do so, they must ask the following questions:
1. Which methods most effectively fit the aims of your research?
2. What are the strengths and restrictions of a particular method?
3. Are there potential risks when using a particular research method?
Naming authors on a research paper ensures that the appropriate individual receives credit and is held accountable for their work. Generally, an “author” is considered to be an individual who has made a significant intellectual contribution to the study.
To be credited as the author of their study, the researcher must meet these four criteria:
1. The researcher must have made a significant contribution to the study design and data analysis.
2. The researcher must have drafted or revised the research article.
3. The researcher must give their approval for the final version.
4. The researcher must agree to be held accountable for all aspects of their work, including accuracy and integrity.
That being said, there are forms of authorship widely deemed unacceptable by the research community. They are a major contributor to authorship disputes, because their participation violates ethics of research publication, they are:
1. Ghost authors, or authors who contribute substantially to the research paper but are not acknowledged for their work. They are often paid. Not acknowledging a writer’s contribution is deemed dishonest, and therefore, unethical.
2. Guest authors, or authors who make little to no contribution to the research paper but are listed to increase the probability of the paper being published. Because they make no discernable contribution to the research paper, their inclusion is unethical.
3. Gift authors, or authors whose only contribution is being affiliated with the study. Like guest authors, their inclusion is unethical.
When an investigator, author, editor, or reviewer has a financial/personal interest or belief that could affect his/her objectivity, or inappropriately influence his/her actions, a potential competing interest exists. The most obvious competing interests are financial relationships, such as employment, grants, and paid expert testimony.
Undeclared financial interests may seriously undermine the credibility of the journal, the authors, and the science itself. However, competing interests can also exist as a result of personal relationships, academic competition, and intellectual passion.
Plagiarism is defined as deliberately using the work of another person or entity without permission, credit, or acknowledgement. It is one of the most common types of political misconduct, and, unfortunately, the most damaging.
As the name suggests, it is the reproduction of a publication word for word.
An entire publication or part of it may be copied, without the acknowledgment or crediting of the original author or publisher.
Substantial copying is the copying of the research materials, processes, tables, or equipment. It differs from literal copying in that the offender here is plagiarizing the idea, or essence, of the research paper. In literal copying, the offender plagiarizes the words and paragraphs of the research paper, or the literary components.
Paraphrasing is reproducing someone else's ideas while not copying word for word; the offender writes them down in their own words or according to their understanding. It is done without permission and acknowledgment of the original source. Paraphrasing is only acceptable if the original source is properly referenced.
Text recycling occurs when a researcher reproduces their own publication word for word, and submits it as an entirely new publication.
It is similar to literal copying, except that the offender is plagiarizing their work instead of another publisher’s work.
After deciding on a fitting journal to publish your research, you should start formulating your manuscript.
A manuscript is the reporting of your study in an organized manner that correlates to the guidelines of the journal of choice. A manuscript is the file you submit to the journal to be published. Writing the manuscript employs the scientific writing style explained in the previous section.
1. Read the author guidelines: Every journal has a guide for authors printed at least once a year. This guide will include information regarding the aim and scope of the journal, the different types of manuscripts the journal accepts, and specific details about formatting a manuscript before submitting it.
2. Write the Methodology section: The methods section should state everything you did during the study. (the contents of the methodology section were discussed in the previous section).
3. Write the Results section: The results section should include all the findings you gathered from conducting your research.
4. Discuss your results: In the discussion section, the author should compare his/her findings to the existing knowledge and to findings of previous studies to put the results in a meaningful context.
5. Write a Conclusion: The author should write a comprehensive yet concise conclusion that accurately sums up the study, its findings, their interpretation, its implications, and limitations.
6. Write the Introduction section: The introduction should include the purpose, aim, and significance of the study. It should also include a review of existing literature on the topic under investigation.
7. References: In this step, the author should ensure that each citation is in its correct location in the manuscript. Next, the author should formulate a list of references that follows the guidelines of the journal. Guidelines in writing references include the type of citation used, the format the references are written in, and the order of the references.
8. Write the Abstract: The abstract is a presentation of your study, the methods you used, the findings you gathered, and their interpretation. An abstract is used to inform prospective readers about your study without them reading the full paper. The abstract should usually follow a distinct limit of words.
9. Create a title page: The title page should include the title of the paper, author(s) name(s), their affiliations, and their institutions.
Scientific writing is a technical form of writing that is used to communicate data among scientists in any given field. Scientific writing can vary slightly based on what it is you are trying to communicate, a journal article, a research proposal, a literature review article, etc.
Writing a research report varies based on the type of research, quantitative or qualitative. However, both types of research have similar sections within which the data differs. These major sections are introduction, methods, results, and discussion.
Introduction: The introduction of a quantitative research report includes the research problem, the purpose and significance of the study, and a comprehensive review of previous literature. Moreover, depending on the type of the study, the framework, objectives, questions, and hypothesis can be included in this section.
Method: The methods section should be very concise; it should include the research design used in the study, the sampling technique and the sample, the setting of the study, the data collection tool, the methods of measurement, and a discussion of the data collection process.
Results: The result section includes the data analysis process and all the findings of the conducted study. The results section is usually organized depending on the study objectives, questions, or hypothesis, if present, or the research purpose. The results are usually presented in a narrated form with reference to a table or figure that includes all of the results gathered from the study.
Discussion: The discussion section is where the data, literature, and results provided earlier on the study tie together to produce a valuable conclusion that gives them meaning and answers the research question. The discussion section includes major findings, which are identified through the interpretation of the results, limitations to the study, conclusions drawn from the findings, implications of the study, and recommendations based on the conclusion of the study. The major findings are usually presented in comparison to the research question, objective, or hypothesis (if present). Moreover, the findings are compared to findings of previous studies and the theoretical knowledge base, usually present in the introduction n section.
Introduction: The introduction section of a qualitative research report identifies the phenomenon to be investigated and the type of qualitative study to be conducted. Also, this section includes the study purpose, the study question or aims, and the significance of the study. Because qualitative research is based on assumptions and philosophies, they are included in this section to provide a basis for the methods, results, and discussion sections. Some qualitative studies include the literature review in the introduction section or as a separate section, while others include a literature review in the discussion section.
Methods: As the researcher serves as the primary data collection instrument and is responsible for the data analysis which depends solely on the researcher’s reasoning, the researcher’s credentials are included in this section. This section also includes the setting and population included in the study. Moreover, the role of the researcher is described including the entry to the setting, selection of the study subjects or sample, and the ethical considerations presented to the subjects. Finally, the data collection process is described. This includes all of the data collection tools the researcher used and the dynamic way the researcher collected the data including the time consumed, how the data was recorded, and the amount of data collected.
Results: In this section the data collected, in the form of tapes, notes, observations and other materials from interviews, etc., is transformed into meaningful categories or common themes by the researcher. The data analysis procedures used and the process of implementing them is detailed in this section. Results, which include patterns and theories derived from life experiences, historical events, etc., are presented in a way that clarifies the phenomenon being studied.
Discussion: This section includes conclusions, derived from the findings, that answer each research question and link the findings with existing theoretical and empirical literature. Moreover, this section includes implications of the study and recommendations based on the study’s findings.
Citation is the way of giving credit to authors’ original work when you decide to use it in your own research. Citation is crucial to the respect of authors’ copyrights. Typically, a citation can include the author's name, date, location of the publisher, journal title, or DOI (Digital Object Identifier). There are two parts to referencing: in-text citation and reference list. There are a plethora of citation styles that are established, each of which has its own format and uses. The major citation styles are APA, MLA, Chicago, and Vancouver.
This style is usually used by Education, Psychology, and Sciences.
The APA referencing style is an "author-date" style, so the citation in the text consists of the author(s)’ surnames and the year of publication given wholly or partly in round brackets.
No distinction is made between books, journal articles, internet documents or other formats. In the reference list: the author(s) full names, publication year, title, edition (if applicable), and publisher are written in this order.
The references are then arranged alphabetically by the author.
Examples
In-text:
Author Surname(s), Year of Publication,
Page(s)
(Cervone & Pervin, 2017, pp. 13-16)
In the reference list:
Author(s). (Year of Publication).
Title: Subtitle
This style is used mainly in Humanities.
(Edition.). Publisher.
Cervone, D., & Pervin, L.A. (2017). Personaity: Theory and Research (13th ed.). Wiley.
The aim of the MLA style is to be brief and to provide only as much detail as is necessary to identify the work cited and the location of the information in that work.
The flow of the text should not be interrupted. In in-text citations, the author(s)’ surnames and the pages of the cited work are written between brackets.
In the reference list, the author(s)’ full names, title of the work, edition (if applicable), publisher, and publication year are written in this order.
No distinction is made between books, journal articles, internet documents or other formats.
Reference lists in MLA are arranged alphabetically by the author.
Examples
In-text:
Author Surname(s)
(Burns
Page(s)
In the reference list:
Author(s).
Year of Publication
Burns, Lynette Shiredan, and Benjamin J Mattews. Understanding Journalism. 3rd ed. Sage, 2018.
Title.
Chicago
Edition. Publisher,
This style is generally used by Business, History, and the Fine Arts.
Chicago style is an "author-date" style, so the citation in the text consists of the author(s) name and year of publication given wholly or partly in round brackets.
In in-text citation the author(s) surnames and the year of publication are written.
You can include page numbers, chapter or section numbers, preceded by a comma, if you need to be specific.
In the reference list, the Author(s)’ full names, publication year, title of work, edition (if applicable), and place of publication and publisher should be written in this order.
Reference lists in Chicago are arranged alphabetically by the primary author's surname.
Examples
In-text:
Author Surname(s)
(Tuten
In the reference list:
Page(s)
Year of Publication,
This style is used mainly by the Health Sciences. Vancouver Style uses a notational method of referencing when referring to a source of information within the text of a document.
In in-text citations, a number between brackets is used to refer to the reference.
This number correlates to the reference list at the end that is arranged in the order of citation in the text, the first reference cited is labeled number 1 and so on.
In the reference list, the number of the reference, the author(s)’ full names, title of the work, edition (if applicable), and place and place, publisher, and publication year are written in this order.
In-text:
(Reference Number).
…provides an overview of the principles of immune response (1).
In the reference list:
You can always use online tools and desktop applications to help you generate citations in just a few clicks; we highly recommend Mendeley for such a purpose.




Kirollus Nagah
RSDD DA 20/21


RSDD GA 20/21
Salma Elnoamany
Aya Elsayed Abdelwahed


KMSA Kafr El-Shiekh
Moustafa Elsayed

MSSA Menofia
ASSA Alexandria
Mahmoud Nagy MSSA Mansoura SWG Coordinator
Mohamed Ehab Eid
HMSA Helwan
Mirna Hussein
Yahya Mohamad
HMSA Helwan





