Aprenda dónde leer esta historia en español en la página 7
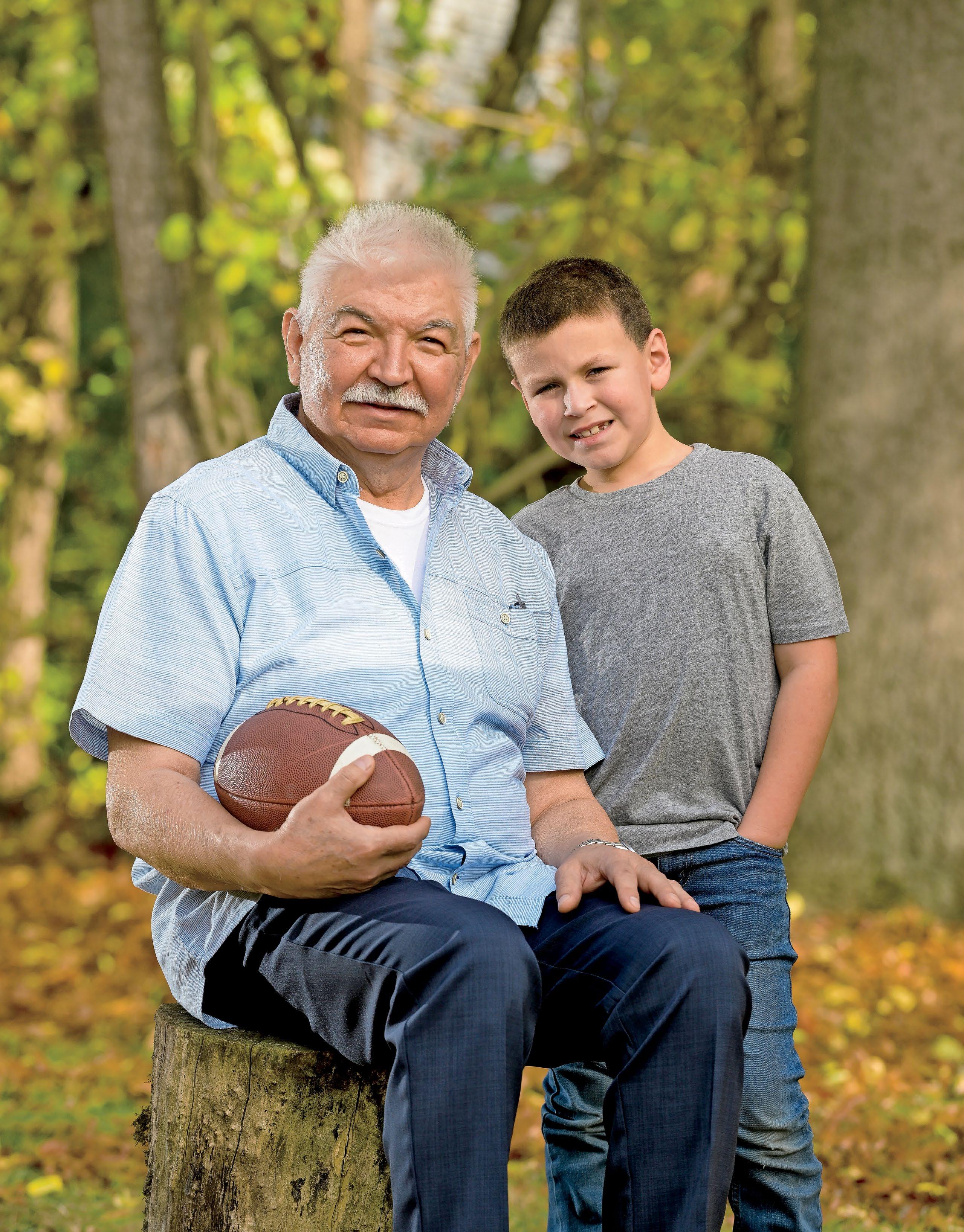
Bensabio Guajardo, pictured with his 8-year-old grandson, Kevin, is thriving after transplant surgery.
About 26 million people in the United States have limited English proficiency, with 62% of these adults speaking Spanish, according to the nonprofit health policy research group KFF. As a total of the U.S. population, 8% of people age 5 and older have limited English proficiency.
Adults with limited English proficiency are almost twice as likely to report that their physical health is poor compared with adults who are English proficient, KFF reports. They also report less use of care, greater barriers to accessing care and are almost five times as likely to report being uninsured.
UChicago Medicine’s Latino Transplant Program is one of the only programs in the country dedicated to supporting Latino and Hispanic transplant patients and their families. In contrast to the language barriers these patients often face, our hepatologists, surgeons, nurses, pharmacists and financial counselors speak fluent Spanish. (Read more about the program and transplant patient Bensabio Guajardo on Page 7.)
The ability to speak with providers in a patient’s preferred language goes far beyond simply understanding what a provider is telling the patient. It impacts the amount of time spent with the patient and whether they felt their cultural beliefs were respected.
When adults can speak in their preferred language, they are more likely to feel comfortable asking questions and being involved in decision-making.
Our transplant program fills a much-needed gap in the Latino and Hispanic communities, which face socioeconomic inequities and other factors that place them at a much higher risk of diseases that lead to organ failure. With our new program, we aim to help patients navigate the many complexities of securing a transplant, while also empowering them to be strong advocates for their health and the health of their community.
Tom Jackiewicz President, University of Chicago Health System
Spot and treat the ‘winter blues’
Seasonal affective disorder (SAD) is a type of depression prompted by a change in seasons — mainly fall and winter — when we experience less daylight and sunshine, and it affects as many as 5% of people in the United States each year.
Anita Davis, LCPC, a therapist at UChicago Medicine Ingalls Memorial Hospital, answered common questions about SAD.
WHAT CAUSES SAD?
Although the direct cause of SAD isn’t known, the arrival of earlier sunsets affects the body’s circadian rhythms that help regulate essential functions such as sleep, metabolism and immunity.
“Our internal biological clock is triggered by sunlight and darkness,” Davis said. The onset of SAD can increase melatonin (a sleep-related hormone) and decrease serotonin (a mood-related hormone), which leads to less activity, sleeping more and feeling low or depressed.
HOW IS SAD DIAGNOSED?
It takes a two-year period to diagnose a patient with SAD. The reason? “You have to see a pattern happening around the same time each year that’s not connected to a significant loss or traumatic event,” Davis said. “Generally, the person feels better in other seasons.”
WHAT TREATMENTS ARE AVAILABLE?
While medications and therapy are options, Davis shared several approaches to try first that can boost serotonin:
» Buy a light box or light therapy lamp
» Put higher-watt bulbs in household lights
» Eat proteins and high-fiber foods
» Increase your outdoor activity on sunny days
» Exercise regularly to boost endorphins
» Have your vitamin D levels checked
» Get up earlier to experience more daylight
SHOULD I SEE A DOCTOR FOR SAD?
If symptoms last for more than two weeks, or if they intensify and impair daily life, a medical professional may help. Ingalls Behavioral Health Department has an intensive outpatient therapy program at four locations to address a range of emotional health issues, including SAD. Free assessments are available, Davis said.
If you are having thoughts of suicide, go to your nearest emergency department or call 988 to reach the 988 Suicide & Crisis Lifeline (previously known as the National Suicide Prevention Lifeline). You can also text HOME to 741741 to reach the Crisis Text Line.
To make an appointment at the UChicago Medicine Ingalls Memorial Behavioral Health Department, call 708-332-1991 or visit UChicagoMedicine.org/seasonal-info
KEY
SYMPTOMS OF SAD
» Low moods
» Low motivation to get things done
» Fatigue
» Sleeping more
» Eating more
» Feeling of helplessness, hopelessness and low self-worth
» Trouble concentrating or focusing
» Feeling sad most of the day
Emergency care in Northwest Indiana
The new emergency department (ED) at UChicago Medicine Crown Point* is here to help Northwest Indiana residents get critical treatment quickly — and closer to home. Michael Kurz, MD, Professor of Medicine and Chief of the Section of Emergency Medicine at UChicago Medicine, shared several benefits of the new ED, which is open 24/7 and staffed by faculty physicians.
AN EXPERIENCED EMERGENCY CARE TEAM
Together, our staff has over 300 years of experience in emergency medicine.
SCREENING TOOLS, SHARED EXPERTISE
Our world-class team collaborates with UChicago Medicine clinicians in Hyde Park.
From registration to seeing a physician, our efficiency shines when seconds count.
AMBULANCES CAN GO TO UCHICAGO MEDICINE CROWN POINT
Need emergency transport? When appropriate, you can ask to be taken to our facility.
Michael Kurz, MD
3 reasons to see a primary care doctor
Seeing a primary care physician (PCP) is an easy way to take care of your health. A doctor who knows you can make a big difference in the quality of your care, said UChicago Medicine Medical Group family medicine physician Paulo Aranas, MD*, who practices at UChicago Medicine Orland Park and UChicago Medicine at Ingalls - Tinley Park. Here’s why:
‘We’re here to prioritize
your health’
Meet the advanced practice providers at UChicago Medicine
Nurse practitioners and physician assistants are commonly referred to as advanced practice providers (APPs). These and other highly trained individuals provide much of the same patient-focused care as doctors.
Nearly 600 APPs work at all University of Chicago Medicine locations* and in almost every specialty — including cardiology, critical care, gastroenterology, transplant medicine and surgery.
Brooke Schweitzer, DMSc, MSPA, PA-C, Executive Director of Advanced Practice Providers at UChicago Medicine, spoke more about APPs and their roles in patient care.
WHAT IS AN ADVANCED PRACTICE PROVIDER?
APP is the umbrella term for physician assistants, nurse practitioners, certified registered nurse anesthetists, certified nurse midwives and clinical nurse specialists. We work with each other and our physician partners to provide care in both inpatient and outpatient settings.
WHAT DOES AN APP DO?
Depending on their specialty, APPs spend their time assessing and diagnosing patients, developing treatment plans, prescribing medications, ordering and interpreting tests,
and educating patients. APPs can also do procedures, performing everything from lumbar punctures and chest tube insertions to skin biopsies, and they may assist surgeons in the operating room.
HOW DO APPS SUPPORT PHYSICIANS?
Our work isn’t to replace physicians but to increase access and equity by giving them more time to see patients who need specific expertise. You may see an APP in the emergency department to diagnose and care for your injury or as a primary care provider in our outpatient family medicine clinics.
WHY SHOULD PATIENTS TRUST AN APP?
Our APPs go through rigorous training, and they’re held to the same credentialing and privileging process as our UChicago Medicine physicians. They obtain a master’s degree and complete thousands of hours of patient care training, and they participate in ongoing education to stay up to date on the latest treatments.
*APPs are not agents or employees of the Ingalls Memorial Hospital.
KNOWLEDGE OF YOUR HEALTH HISTORY
Building a long-term relationship with your PCP helps ensure careful, coordinated care over time, especially for older patients who see many doctors and specialists. PCPs can provide oversight by consolidating all the information and explaining it in plain language.
PERSONALIZED ADVICE AND TREATMENT
Because they learn a lot about you, your PCP can be a well-informed advocate. “Maybe I know that a patient likes biking but not the treadmill,” said Aranas, who also practices weightloss medicine. “Patients aren’t as resistant to suggestions; they know we understand the situation.”
JUDGMENT-FREE CONVERSATION
Patients may see doctors as authority figures — and they might worry about being scolded for unhealthful habits — but Aranas assures that PCPs won’t judge anyone seeking care. “We want to help you figure out the issue and we’ll solve it together,” he said.
To make an appointment with a UChicago Medicine primary care physician, call 866-724-1137 or visit UChicagoMedicine.org/PCP-info
*Paulo Aranas, MD, is a UChicago Medicine Medical Group provider. UChicago Medicine Medical Group is comprised of UCM Care Network Medical Group, Inc., and Primary Healthcare Associates, S.C. UChicago Medicine Medical Group providers are not employees or agents of The University of Chicago Medical Center, The University of Chicago, the Ingalls Memorial Hospital, UChicago Medicine Orland Park or UChicago Medicine at Ingalls — Tinley Park.
Paulo Aranas, MD
The number of advanced practice providers working at UChicago Medicine
From left: Bridget McGrath, PA; Frank Umbriaco, AGACNP-BC; Laura Urciuoli, FNP-BC; and Alisa Heitman, MSN, N-C.
U.S. News: Cancer, ENT programs rated best in Illinois
Food hall offers hip, healthful options
Expanded dining options are available in a new food hall located at the University of Chicago Medicine’s Center for Care and Discovery. The food hall, which debuted in September, brings two Chicago-based brands and a celebrity-cheffounded eatery to UChicago Medicine’s Hyde Park medical campus: Sip of Hope Coffee, Burrito Beach and Root & Sprig.
The University of Chicago Medical Center's cancer and ear, nose and throat programs are ranked the best in Illinois, according to U.S. News & World Report’s 2024-25 Best Hospitals list. The Medical Center received “high performing” ratings in 16 common adult procedures and conditions, and it has 10 specialties rated among the nation’s best.
» Ear, nose and throat (11)
» Cancer (12)
» Gastroenterology and GI surgery (25)
» OB-gynecology (25)
» Diabetes and endocrinology (30)
» Cardiology, heart and vascular surgery (32)
» Pulmonology and lung surgery (35)
» Neurology and neurosurgery (36)
» Urology (36)
» Geriatrics (40)
40 years of critical care by air
The UChicago Medicine Aeromedical Network (UCAN), the only hospital-based medical helicopter transport program in Chicago, is marking 40 years in operation. Although UCAN’s twin-engine Airbus EC-145 helicopter can land at accident scenes, most transports take place between hospitals to bring ill patients to UChicago Medicine for a level of care or expertise they can’t get elsewhere, said Ira Blumen, MD, the medical and program director for UCAN.
New facility opens in Hinsdale
$75 million donation supports new cancer pavilion
The AbbVie Foundation, a nonprofit dedicated to addressing health inequities, has donated $75 million to the University of Chicago to support construction of UChicago Medicine’s new cancer pavilion. The building, to be named the AbbVie Foundation Cancer Pavilion, will provide a hub for world-class research, pioneering clinical treatments and personalized care. The donation will help fund the $815 million, 575,000square-foot space, which is scheduled to open in 2027.
A new outpatient center staffed by UChicago Medicine and Comer Children’s Hospital clinicians has opened in Hinsdale. The center, located at 11 Salt Creek Lane, offers care in pediatric and adolescent gynecology, digestive diseases, and ENT, as well as transplant services for adult patients; Comer Children’s experts provide neurology, digestive diseases and cardiology services. Three existing UChicago Medicine sites in Hinsdale have closed and relocated into the new center.
When is the flu an emergency?
Know the warning signs and what to do next
Each year, thousands of people flood hospital emergency departments seeking treatment for flu symptoms — but most of the time, that step isn’t necessary. Zoheb Osman, DO*, a family medicine physician with UChicago Medicine AdventHealth Medical Group, offers a primer to navigate flu season.
COMMON SIGNS OF FLU
In general, it’s safe to assume you have the flu — and not a cold — if your symptoms are severe and accompanied by a fever (typically 100 to 104 degrees Fahrenheit). Symptoms may include:
» Chills
» Dry cough
» Runny or stuffy nose
» Fatigue
» Headache
» Muscle pain/body aches
» Sore throat
An annual flu shot can help reduce your risk of getting the flu and related complications. Treating symptoms with over-the-counter medications such as acetaminophen for pain or fevers, getting plenty of rest and drinking lots of fluids provide enough relief for most people.
There are times when you should go to a hospital’s ED for the flu. A key sign is when you or a loved one experiences severe dehydration, which can show up as:
» Confusion
» Dark-colored urine
» Weakness
» Dizziness
» Limited appetite
» Extreme thirst
» Severe or consistent vomiting
Other signs of a flu-related emergency include severe chest or abdominal pain, difficulty breathing or shortness of breath.
DANGERS IN CHILDREN AND INFANTS
Warning signs of flu complications are slightly different for children and infants. If you have a child experiencing any of the following symptoms with the flu, go to an ED:
» Bluish color to the skin
» Severe headache
» Stiff neck
» Inability to take in fluids
» Trouble urinating
Infants under 3 months old who have a fever over 100.3 degrees Fahrenheit, an absence of tears while crying, fewer wet diapers than normal, an inability to eat and/or inconsolable crying or irritability also should be taken to an ED immediately.
UChicago Medicine offers walk-in flu testing and treatment. Or visit UChicagoMedicine.org/ UrgentCare to reserve your spot.
HOSPITAL CARE FOR SEVERE FLU
*Zoheb Osman, DO, is a UChicago Medicine AdventHealth Medical Group provider. UChicago Medicine AdventHealth Medical Group providers are not employees or agents of The University of Chicago Medical Center, The University of Chicago, UChicago Medicine Medical Group or the Ingalls Memorial Hospital.
Up-close look at ulcerative colitis
Ultrasound technology guides IBD treatment for teen athlete
Gage Wimmer recently started college as a happy, healthy, 180-pound lacrosse player. But just one year earlier, the towering athlete had withered down to 115 pounds.
“I thought it was food poisoning,” said Wimmer, now 18. “And then it didn’t go away.”
Doctors diagnosed Wimmer with severe ulcerative colitis, an inflammatory bowel disease (IBD) that inflames the digestive tract and causes pain and severe diarrhea.
Wimmer became so sick that he could barely get out of bed. The Chesterton, Indiana, teenager missed three months of school and an entire lacrosse season.
After the medicines his doctor prescribed didn’t help, Wimmer was referred to the University of Chicago Medicine’s Inflammatory Bowel Disease Center, one of the oldest centers of its kind.
Gastroenterologist Noa Krugliak Cleveland, MD, prescribed a new medication and brought in a dietitian to help Wimmer determine what he could and couldn’t eat.
Krugliak Cleveland also performed regular intestinal ultrasounds — a new, noninvasive tool used at UChicago Medicine to help patients monitor their IBD.
Gel is applied to the abdomen and a probe is rolled over the area to provide a detailed, real-time look at the small bowel and colon, allowing doctors to quickly spot inflammation, active disease or other complications.
This state-of-the-art approach is much easier than an endoscopy or a colonoscopy.
“Intestinal ultrasound doesn’t hurt — it doesn’t expose you to radiation, there’s no prep, you can eat or drink before, and you can do it as often as you need to,” said Krugliak Cleveland, who also offers the ultrasound screenings at UChicago Medicine's Northbrook location and at Comer Children's Hospital. “Based on the ultrasound, we came up with a treatment catered to Gage.”
Wimmer, active and energetic again, is now enjoying lacrosse and classes in the electro-mechanical technology program at College of DuPage.
UChicago Medicine pioneers new use of drug for ulcerative colitis
A University of Chicago Medicine patient became the world’s first to receive the drug guselkumab (Tremfya) since it was federally approved for treating moderate to severe ulcerative colitis. Tremfya, already used to treat plaque psoriasis and psoriatic arthritis, was also proven to be an effective treatment for ulcerative colitis in a global study led by UChicago Medicine’s David T. Rubin, MD, Chief of the Section of Gastroenterology, Hepatology and Nutrition. The study contributed to the U.S. Food and Drug Administration’s approval in September. Rubin is a paid consultant of Johnson & Johnson, the maker of Tremfya.
To make an appointment with UChicago Medicine’s Inflammatory Bowel Disease Center, call 866-643-8419 or visit UChicagoMedicine.org/IBD-info
With his IBD under control, Gage Wimmer has returned to sports and school.
David T. Rubin, MD
Noa Krugliak Cleveland, MD
New lungs, new life
Latino Transplant Program offers Spanish-speaking patients comfort and coordinated care
As images from his chest X-ray flashed on the computer screen, Bensabio Guajardo was comforted by his nurse’s words.
“¡Mira tus hermosos pulmones nuevos! ” the nurse said in Spanish — which, in English, translates to “Look at your beautiful new lungs!”
Just a few weeks earlier, 68-year-old Guajardo received a double lung transplant through the University of Chicago Medicine’s Latino Transplant Program. It is one of the only programs in the country dedicated to supporting Latino and Hispanic transplant patients and their families.
Almost everyone on a patient’s team — including hepatologists, surgeons, nurses, pharmacists and financial counselors — speaks fluent Spanish. No translators are required.
“There’s a certain amount of relief when we can communicate directly in their native language,” said Pablo G. Sanchez, MD, PhD, a native Argentinean and surgical director of the lung transplant program at UChicago Medicine. “It feels more personal, like you’re closer to home.”
(CONTINUED ON NEXT PAGE)
Pablo G. Sanchez, MD, PhD
Bensabio Guajardo is cherishing time with his family after a double lung transplant.
(CONTINUED FROM PREVIOUS PAGE)
Guajardo, who is from Mexico, speaks English fluently but still chose to speak both languages with his transplant team. The bilingual staff was particularly helpful for his wife, Juanita, who oversees his care.
“It allowed her to speak freely and understand everything that was happening,” Guajardo said.
PATH TO TRANSPLANT
After retiring from a 34-year career at U.S. Steel, Guajardo started feeling short of breath while doing routine tasks. He stubbornly insisted he was fine.
Soon, Guajardo’s breathing became so strained that he agreed to see a doctor. In 2017, he was diagnosed with severe sleep apnea and pulmonary fibrosis, a chronic lung disease that would gradually worsen his breathing.
Within a year, Guajardo needed to use a transportable oxygen tank with a mask to help him breathe. The pulmonary fibrosis
continued to worsen. Even a walk from his bed to the couch would exhaust him.
“I was trying to be strong-headed because I didn’t want to accept that I was really sick,” Guajardo said. “But my health was going down, down, down.”
After frustrating experiences at other hospitals, Guajardo, who lives in Trail Creek, Indiana, found his way to UChicago Medicine in Hyde Park — the same place where two of his four children had major surgeries decades earlier.
A pulmonary team that included Anila Khan, MD, and Kevin Tsui, MD, studied Guajardo’s case and determined he needed a lung transplant. Guajardo was referred to the
Latino Transplant Program and added to the waitlist for donor lungs in August 2023.
As he waited, the then-278-pound Guajardo worked with UChicago Medicine’s ACTNOW clinic, which helps transplant patients lose weight in order to have a successful surgery. By changing his diet and using a semaglutide weight-loss drug, he lost nearly 100 pounds over 10 months.
Still, Guajardo’s lungs were getting worse. He landed in the UChicago Medicine emergency department in April and spent several weeks in the intensive care unit. Sanchez described him as “very, very sick.”
‘AN ABSOLUTELY NEW MAN’
Just in time to save Guajardo’s life, a set of donor lungs became available in early May. A “bloodless” transplant surgery — a specialized procedure that uses precise surgical techniques to minimize blood loss — quickly followed.
Although bloodless transplant surgeries were developed to treat patients with certain religious beliefs, they’re now widely performed. UChicago Medicine’s transplant
Guajardo with his granddaughters Camila, 2, and Emmaline, 2.
Anila Khan, MD Kevin Tsui, MD
412
Number of organ transplant surgeries (heart, lung, liver, kidney, heart, pancreas and islet) performed at UChicago Medicine in FY24
1 in 4
People awaiting a transplant in the U.S. who are Hispanic
No. 1
Hispanic/Latino lung transplant recipients have the highest fiveyear adjusted survival rate compared to other racial and ethnic groups
Sources: UChicago Medicine, U.S. Department of Health and Human Services, The Journal of Heart and Lung Transplantation
team has adapted these techniques for lung transplants; Sanchez said they result in better outcomes and a lower risk of graft dysfunction, infection, arrhythmias and stroke.
Guajardo’s 10-hour surgery was a success.
“The day after, he looked like an absolutely new man,” Sanchez said.
Two days later, Guajardo was walking the hospital halls without needing oxygen. He hasn’t needed it since. He returned home 19 days after his transplant, which is weeks earlier than normal.
Flor Cerda, the UChicago Medicine nurse practitioner who worked with Guajardo, partially attributed the recovery to strict compliance with aftercare instructions.
“They’re just wonderful people to take care of,” Cerda said.
FINDING
A NEW NORMAL
Guajardo’s prognosis is excellent, but now he must take care of his lungs, Sanchez said. That means being cautious about viruses and knowing the side
effects of his medication, including a higher risk of skin cancer.
Still, Guajardo can now resume his beloved fishing hobby — but he must wear a hat, long sleeves and sunscreen.
“We want to give our patients normalcy back, but it’s a new level of normal with more precautions,” Sanchez said.
Guajardo said he feels blessed to have received a double lung transplant at UChicago Medicine.
In a matter of weeks, he went from being in critical condition to living a normal life. Just a few weeks ago, he walked down the aisle at his son’s wedding — no oxygen canister needed.
“My grandson, who is 7, said, ‘Grandpa, when the doctor fixes you, can you go outside and play football with me?’” Guajardo said. “I told him the doctor hasn’t cleared me to do that, but I said, ‘I’m going to do it real soon.’”
To make an appointment with UChicago Medicine’s Latino Transplant Program, call 773-923-1934 or visit UChicagoMedicine.org/transplant-info
Identifying disparities in transplant care
Latinos account for nearly 20% of the U.S. population, according to the U.S. Census Bureau. But many who need organ transplants face socioeconomic inequities that can hinder the process.
Latinos also have a higher risk of diseases that lead to organ failure — including liver diseases, Type 2 diabetes, high blood pressure and kidney disease.
In 2020, only about one-third of Hispanics (the demographic measured by the U.S. Department of Health and Human Services) waiting for any organ transplant received one, compared to nearly half of white patients, federal data shows. That gap includes lung transplants, according to a 2023 study in the Annals of Thoracic Surgery.
The Latino Transplant Program at UChicago Medicine aims to help patients “navigate the clinical, surgical, emotional and financial complexities of transplantation,” said Pablo G. Sanchez, MD, PhD, a lung transplant surgeon and the program’s director.
Members of the Latino Transplant Team speak fluent Spanish to help patients and their families.
‘One-and-done’ skin cancer treatment
Supercharged cells are used in novel immunotherapy to fight the disease
For 15 years, Alla Pinzour traveled the country seeking treatment for her advanced melanoma. Some efforts would bring temporary remission, but her skin cancer always returned.
“Surgeries, chemo, radiation — you name it, I had it done,” said Pinzour, who lives in north suburban Hawthorn Woods. “Nothing seemed to work.”
By early 2024, Pinzour’s skin cancer had spread to other places in her body, including her lungs and stomach, causing her health to deteriorate further.
That’s when Pinzour’s oncologist told her about a groundbreaking new melanoma treatment that would soon be offered at the University of Chicago Medicine.
The approach is called tumor-infiltrating lymphocyte therapy, or TIL therapy, and it works by boosting a person’s cancerfighting cells to help their own immune system kill the cancer.
That concept, known as immunotherapy, trains the body’s immune system to attack a disease, similar to how it might fight a cold.
In mid-February, the Food and Drug Administration approved the use of TIL therapy for advanced melanoma. Weeks later, Pinzour became the first person in the Midwest — and one of the first in the country — to have the commercially approved treatment.
“We did a lot of planning and training with the research team and the operating room nurses and staff, so as soon as the FDA said ‘Go,’ we were the first ones to do it,” said UChicago Medicine surgical oncologist Mecker G. Möller, MD.
QUICK, STRONG RESULTS
For Pinzour, the results have been dramatic. Soon after receiving TIL therapy, the cancerous tumors under her skin started to shrink. Pinzour’s latest scan, in July, showed even more positive clinical response, Möller said.
Daniel Olson, MD
Mecker G. Möller, MD
How TIL therapy works
Removal and reengineering
Fighter cells go to work
Follow-up monitoring
For an appointment, call 844-482-7823 • Or to learn more, visit uchicagomedicine.org/defeatcancer
A patient’s own cancerfighting T cells (tumorinfiltrating lymphocytes, or TILs) are surgically removed from their tumor. The cells are sent to a lab, where they’re strengthened and multiplied into the billions.
The supercharged TILs are frozen and returned to the hospital. Put back into the body via an IV, the cells contain an excessive number of TILs — far more than typically found in a person’s body — to provide the power to destroy the tumor.
“If it continues to work, this might be the only treatment she ever needs,” said UChicago Medicine oncologist Daniel Olson, MD, who helped administer Pinzour’s TIL therapy. “An infusion of these cells can sometimes drive melanoma into remission – it’s a one-and-done treatment.”
“I’ve been waiting for this for many, many years,” said Pinzour, a mother of two. “I would have gone anywhere in the world to get this, but I was able to get it right here in Chicago.”
call 844-482-7823 • Or to learn more, visit uchicagomedicine org/defeatcancer 3 While the T cells multiply in the lab the patient receives chemotherapy to reduce the number of cancer cells
Patients will see their oncologist once or twice a week for the first month to monitor blood counts and check for complications. At three months, they will receive an imaging scan to see if the tumors are shrinking.
“Still, for patients with melanoma who don’t respond to the standard therapy, it’s the best thing out there,” he said.
That’s good news for patients like Pinzour, who in 2009 noticed a tiny mole on her leg. When it started to grow, she saw a doctor who confirmed it was melanoma.
At the time, there was only one drug to treat melanoma and Pinzour didn’t tolerate it well. But she kept taking it, and her cancer went into remission until 2015.
UChicago Medicine doctors have since used TIL therapy on other patients with advanced melanoma, and more are scheduled in the coming months. UChicago Medicine is now one of the highest-volume centers in the country for the treatment.
“TIL therapy gives patients hope when there wasn’t any before,” Olson said.
PROGRESS AND CHALLENGES
Despite seeing positive results in his patients, Olson notes that TIL therapy doesn’t work for everyone. Only one-third to one-half of all patients will see a benefit, he said, and most advanced melanoma patients will not get long-term remission.
When Pinzour heard about TIL therapy, she immediately reached out to UChicago Medicine, where medical oncologists and scientists at the David and Etta Jonas Center for Cellular Therapy continue to study the use of TIL therapy for other types of tumors, including cervical cancer.
“TIL therapy has changed the landscape of how we treat melanoma,” said Möller, who also directs the Regional Cancer Therapies Program at UChicago Medicine.
To make an appointment with a University of Chicago Medicine Comprehensive Cancer Center expert, call 855-397-3327 or visit UChicagoMedicine.org/TIL-info
Periods, pregnancy, Pap smears
Pediatric and adolescent gynecology myths debunked
Gynecologic care isn’t important only for adults.
Experts recommend an initial visit during the teenage years to establish a line of care for the future. It’s also an opportunity for young patients and their caregivers to ask questions when the body is rapidly changing.
Julie Chor, MD, MPH; Jessica Long, MD; and Shashwati Pradhan, MD; are physicians from the pediatric and adolescent gynecology team at the University of Chicago Medicine.
They addressed myths and misconceptions that often come up during appointments — and the answers they give to put minds at ease.
MYTH: I DON'T NEED TO SEE A GYNECOLOGIST UNLESS I'M SEXUALLY ACTIVE
FACT: We suggest seeing a gynecologist for the first time between ages 13 and 15. This allows younger people to get accustomed to talking about things like their periods. It destigmatizes coming to the gynecologist, and it’s a low-stakes, low-pressure visit that can help us establish care and perform preventative counseling.
UChicago Medicine pediatric and adolescent gynecologist Shashwati Pradhan, MD, consults with a patient.
FACT: Tampons will not stretch out the vagina. Individuals who want to use tampons as a way of managing their menstrual flow should use them if they’re comfortable doing so. There are different sizes created for comfort and levels of menstrual flow. Another myth we often hear is that you’re not a virgin if you use tampons, which is simply not true.
MYTH: YOU CAN’T GET PREGNANT WHILE ON YOUR PERIOD
FACT: Not all bleeding is an indicator that your period has started. Many people with irregular periods may experience spotting while they’re ovulating. While it’s unlikely to get pregnant while on your period, it can still happen if you’re having bleeding for other reasons. In general, bleeding isn’t a reliable way to confirm that you’re not at risk for pregnancy.
MYTH: I NEED TO DOUCHE OR CLEAN OUT MY VAGINA
FACT: We talk about the vagina being a self-cleaning entity. In general, that means you don’t need to do anything to clean out the inside. In some cases, we might recommend things like a sitz bath (a warm, shallow bath), but douching itself actually causes more harm than good because it flushes away healthy bacteria that are part of the vaginal environment.
MYTH: I NEED A PAP SMEAR EVERY YEAR
FACT: Per CDC guidelines, your first Pap smear typically starts at age 21. If results are normal, meaning the cells in the cervix do not show signs of cancer or any unusual changes, then we usually test every three years
gynecologist on your period. It won’t faze us and it’s very normal.
MYTH: IUDS ARE DANGEROUS
until age 30. After that, we start looking at the cells on the cervix and whether the human papillomavirus (HPV) is present, which influences how often we test.
MYTH: IF I GET HPV, IT WILL CAUSE CERVICAL CANCER
FACT: While the majority of cervical cancer cases develop in people with HPV, most people with HPV are not going to develop cervical cancer. If you have a positive HPV test, it’s important we monitor you closely afterward to prevent abnormal cells from progressing to cancer. It’s also important to get your HPV vaccines, ideally before you become sexually active.
MYTH: IF I'M ON MY PERIOD, I HAVE TO CANCEL MY GYNECOLOGY APPOINTMENT
FACT: As OBGYNs, we’re very comfortable dealing with menstrual blood. If you have a heavy period on the day of your Pap smear, the red menstrual blood cells may lead to an insufficient sample of cervical cells. But if you’re not coming for a Pap test, you can absolutely still come to the
FACT: Decades ago, there was a type of IUD that was dangerous, and it came with an increased risk of serious infection. The types we use today (hormonal and copper) are very safe. Risks of bleeding, infection and injury are well below 1%. We’re also trying to address pain management during IUD insertion. The CDC recommends a lidocaine injection or gel to decrease pain.
MYTH: BIRTH CONTROL WILL MAKE IT HARDER FOR ME TO GET PREGNANT IN THE FUTURE
FACT: Once you stop using most hormonal contraception (and the copper IUD), you return to fertility quite quickly. The one exception to this is Depo-Provera, or “the shot.” It can take longer for your body to clear that hormone. But it does not change your body’s overall ability to become pregnant.
MYTH: ACCESS TO BIRTH CONTROL WILL PROMPT YOUNG PEOPLE TO START HAVING SEX
FACT: This concept is called the moral hazard: If you provide something upfront, it will increase risky behavior. That comes up in a lot of different contexts, including contraception, and it’s just not true. The same thing applies with providing condoms — something that we know leads to safer sexual behavior, not earlier or increased exposure to risk.
To make an appointment with a UChicago Medicine pediatric and adolescent gynecologist, call 773-377-3434 or visit UChicagoMedicine.org/PAG-info
U.S. News ranks Comer Children’s No. 2 in Illinois
UChicago Medicine Comer Children’s Hospital has been recognized as the No. 2 pediatric hospital in the state for four consecutive years by U.S. News & World Report. The 2024-25 Best Children’s Hospitals rankings put Comer Children’s at No. 17 in the Midwest, up three spots from last year, and include placements in four specialties: cancer (33), neurology and neurosurgery (37), urology (49) and behavioral health (top 50). U.S. News debuted behavioral health as a pediatric specialty this year, giving equal recognition to all of the top 50 programs.
Big flex
Orthopaedic surgery, therapy help nurse achieve bodybuilding dream
Yolanda Lake had plenty of reasons not to enter her first bodybuilding competition.
The mother of three coaches her daughter’s volleyball team and recently began pursuing a master’s degree. She also works full time as a nurse at University of Chicago Medicine Ingalls Memorial Hospital.
Also, just months earlier, Lake had surgery at Ingalls Memorial to repair tears in her bicep and rotator cuff — a group of muscles and tendons surrounding the shoulder joint — caused by a variety of activities.
A full recovery takes months, or even one year, her doctors said.
But as she began physical therapy sessions at UChicago Medicine Ingalls-Calumet City, Lake decided she’d go for it anyway. She signed up to compete in the USA Natural Chi-Town Showdown bodybuilding competition in June.
“When I say I’m going to do something, I have to do it,” said Lake, 42, who lives in the south suburbs.
In early January, with her care team’s blessing, Lake began an intense training regimen. She went easy on her shoulders and arms, slowly increasing the weight to avoid injury.
When the big day arrived, Lake competed in two categories: Bikini Novice, where she placed second; and Bikini Wellness, where she took first place.
“The night Yolanda won, she messaged me and said, ‘I could not have done this without you by my side,’” said Pamelanie “Lanie” Pacatang, PT, CLT, who was Lake’s physical therapist at UChicago Medicine. “I had goosebumps. I was so proud.”
SAFE, STEADY RECOVERY
UChicago Medicine Medical Group orthopaedic surgeon Joseph Thometz, MD*, performed Lake’s 90-minute surgery at Ingalls Memorial in October 2023. He
Yolanda Lake poses with her bodybuilding awards at her gym in Glenwood.
reattached Lake’s tendons — the parts of the muscle that tore away from the bone — in her shoulder and bicep.
Because she was young, in good health, and had “good quality” tissue, Lake made a quicker than normal recovery, Thometz said.
“Surgery is one part of the process, but it’s just as important to have a skilled physical therapist and a patient who’s committed to improving, which she was,” Thometz said.
EXERCISING AFTER SURGERY
Lake’s first few weeks of physical therapy were painful and frustrating, which is normal. Progress is slow during the first six weeks, Thometz said, but shoulder and arm muscles begin to strengthen after that.
Pacatang recalled a time — one she and Lake laugh about now — when Lake cried about her slow progress, smearing her makeup, fearing she’d never regain the ability to move her arm without discomfort. Pacatang comforted Lake, reminding her that a safe recovery takes time.
Lake pushed on, never missing her twice-weekly sessions.
“She trusted her physical therapist to help her heal correctly — that was key,” Pacatang said. “By collaborating with her orthopaedic surgeon, her physical therapist and her personal trainer, Yolanda was able to safely achieve a full range of motion in her arm and had the power to become a competitive bodybuilder.”
Lake gradually ramped up her workouts, doing many of them before dawn and even in the snow. She ran up and down the bleachers at her local football field and did lunges, side shuffles and backward shuffles across the turf.
Today, she reflects on her journey with pride. At a bodybuilding competition in 2023, Lake sang the national anthem and cheered on participants from the sidelines. This time, she was onstage and winning.
“I look forward to doing it again and being even better,” Lake said.
*Joseph Thometz, MD, is a UChicago Medicine Medical Group provider. UChicago Medicine Medical Group is comprised of UCM Care Network Medical Group, Inc. and Primary Healthcare Associates, S.C. UChicago Medicine Medical Group providers are not employees or agents of The University of Chicago Medical Center, UChicago Medicine Comer Children’s Hospital, The University of Chicago, the Ingalls Memorial Hospital or UChicago Medicine Ingalls — Calumet City.
4 ways to prevent bone and joint disease
Sara Shippee Wallace, MD, MPH, an orthopaedic surgeon at the University of Chicago Medicine, shared easy steps you can take at any age.
MAINTAIN A HEALTHY WEIGHT
This is the biggest way to slow or prevent the progression of arthritis. Additional stress on the joint is magnified when patients gain weight, so maintaining a healthy weight is vital for lower extremity joint health and for weight-bearing joints. It also helps prevent osteoporosis, a weakening of the bones commonly associated with aging.
ADJUST YOUR DIET
Patients with mild arthritis may benefit from an anti-inflammatory diet. A Mediterranean diet with vegetables, grains and healthy fats promotes joint health, and it can boost cardiovascular health, help you maintain a healthy weight and lower the risk of Type 2 diabetes. Calcium and vitamin D are key to strong bones (and they’re best absorbed together).
ADD WEIGHT-BEARING EXERCISE
Get active by running, walking, dancing or playing sports — or try Pilates, weightlifting or yoga. These all support bone density and bone health, and they benefit your cartilage. High-impact activity may not be best for people with arthritis, or those with previously injured ligaments who have some degree of osteoarthritis.
4
KNOW YOUR RISK AND GET SCREENED
While there are no screenings for arthritis, knowing your risk factors — and family history — can aid in early detection and getting medication to slow the disease. To detect osteoporosis, which is otherwise usually diagnosed after a fracture, a screening test called a DXA scan is recommended for all women over 65, as well as some higher-risk women under 65.
A slow and steady recovery allowed Lake to amp up her workouts.
Drive-Thru Baby Shower delivers for local mothers
Patty Siuda and her granddaughter waited nearly four hours in their minivan to attend the fifth-annual Drive-Thru Baby Shower in south suburban Harvey, where 300 backpack diaper bags filled with essentials were being distributed.
Siuda, who was first in line, received a crate filled with baby clothes and other items donated by an employee at UChicago Medicine Ingalls Memorial Hospital, which hosted the event.
“It means the world to me,” Siuda said.
The shower began in 2020 during the uncertainty of the COVID-19 pandemic, and its mission to help expectant mothers feel safe and more prepared continues today.
“Being able to offer patients top-of-the-line supplies for their baby speaks volumes about what we can do, and it’s a reflection of the care we provide here at our hospital,” said Shanice Williams, OB Program Manager at Ingalls Memorial.
Williams is also the coordinator for the Healthy Baby Network, a free program at Ingalls Memorial that connects residents with medical, nutritional and financial assistance. She partnered with area nonprofits and
Stepping out for heart health
corporate sponsors to stock the bags and on other giveaways.
Attendee Brittany Fort hugged the event’s volunteers after receiving a baby walker — one of several big-ticket items given away.
“Babies are expensive, and the first time around you’re so overwhelmed with everything,” Fort said. “To have something like this where you could just get a little help is amazing.”
Part of Ingalls’ Family Birth Center, the Healthy Baby Network program bridges the gap between local residents and healthcare resources through partnerships with local retailers, government agencies and other organizations.
Ingalls Memorial offers 23 private birthing
The University of Chicago Medicine registered 585 participants for the American Heart Association Metro Chicago Heart Walk in September, raising $100,000 for cardiovascular research and lifesaving initiatives. Many walked the 1- and 3-mile routes near Soldier Field in honor of loved ones or to celebrate UChicago Medicine’s scientific contributions that help people live longer, healthier lives.
suites and a staff dedicated to making a woman’s birthing experience comfortable and special.
“We have quality care and all of the resources so patients don’t have to travel so far,” Williams said.
The Drive-Thru Baby Shower is a key part of Ingalls Memorial’s efforts to improve maternal and child health in South Side communities where Black women face healthcare barriers and suffer disproportionately high rates of pregnancy-related complications and deaths.
In fiscal year 2023, 93% of mothers who used Healthy Baby Network resources delivered babies of normal weight, and 96% were full-term deliveries, according to the UChicago Medicine’s annual Community Benefit Report.
The event provided free baby supplies for 300 moms-to-be.
Sisterhood in action
Foundation gift funds triple-negative breast cancer research
As Tara Boland underwent treatment for triple-negative breast cancer (TNBC), she befriended others facing the disease.
“Tara got into the habit of chatting to the person next to her in the chemotherapy chair,” said Tara’s husband, Matt.
“She would hear their stories, and some of them were pretty dire — they didn’t have jobs or didn’t know how they were going to pay rent — and she would help them.”
The stories inspired Tara to found the TaTa Sisterhood Foundation, which provides direct support to women with TNBC, shortly before she passed away from the disease in 2013.
It recently offered a gift to fund the work of Rita Nanda, MD, director of the breast oncology program at the University of Chicago Medicine. Tara met Nanda while seeking treatment for a subtype of TNBC known as androgen receptor-positive triple-negative breast cancer (AR+ TNBC).
NEW PATHS TO TREATMENT
Because TNBC lacks expression of the three major breast cancer drug targets (estrogen, progesterone and HER2 receptors), the disease is notoriously hard to treat. It doesn’t respond to hormone therapy or targeted anti-HER2 drug therapies.
Nanda, a nationally renowned expert in TNBC, is focused on identifying new and better treatment options, seeking the right therapy for an individual patient.
“Tara came to UChicago Medicine to enroll in a clinical trial of the anti-androgen receptor therapy enzalutamide, which is FDA-approved for prostate cancer — a cancer that is frequently androgen-receptor positive,” Nanda said. “What we found in that trial was that a percentage of patients with AR+ TNBC benefited from this well-tolerated oral treatment.”
The foundation’s gift will fund a correlative study of Nanda’s current clinical trial
studying the effectiveness of enzalutamide with or without mifepristone, another hormone-blocking targeted agent, compared to chemotherapy.
If either approach proves to be better than chemotherapy, then patients with AR+ TNBC could have new options for treatment.
FUNDING SUPPORTS LEGACY
The clinical trial is funded by the Breast Cancer Research Foundation, but Nanda and her team wanted to analyze a particular biomarker associated with a poor response to enzalutamide in prostate cancer patients — research that would not have been possible without philanthropy.
“We don’t know how common this
biomarker is in breast cancer, or if it might also predict resistance to enzalutamide in AR+ TNBC,” Nanda said. “That’s why the work the TaTa Sisterhood Foundation is supporting is so critical.
“I thought this research would be perfect to do in Tara’s memory.”
The expansion of a research project seeking to improve patient options reflects the spirit of the woman who inspired the sisterhood, Matt Boland said.
“When my coworkers raised money for us, Tara wanted to turn around and pass it on to the people who needed it,” he said. “She was helped by a lot of people when she was sick. She wanted to give back. She was someone who never lost hope.”
Tara Boland, pictured with her children and husband, Matt.