24 IMPORTANCE OF WORKFLOWIN OPERATING ROOMS AND HYBRID OPERATING ROOMS
Regd.With RNI No.MAHENG/2007/22045.Postal Regd.No.MCS/162/2022 - 24.Printed and Published byVaidehi Thakar on behalf of The Indian Express (P) Limited and Printed at The Indian Express Press,Plot No.EL-208,TTC Industrial Area,Mahape,Navi Mumbai-400710 and Published at Mafatlal Centre,7th floor,Ramnath Goenka Marg,Nariman Point,Mumbai 400021.
Reproduction in anymanner,electronic or otherwise,in whole or in part,without prior written permission is prohibited.
India’s health insurance gold rush?
As new business models evolve in India’s private healthcare sector, what’s interesting is that the latest strategies in the private sector are on the health insurance side. Even as India’s national health insurance scheme i.e.
Ayushman Bharat Pradhan Mantri Jan Aarogya Yojana (PMJAY) expands to include senior citizens over 70 years irrespective of income criteria, there are signs that more stakeholders are now willing to look at creative/collaborative health insurance models, to expand insurance coverage and finance health spends.
Our September edition had a detailed cover story on the shifting landscape of insurance in India. (https://www.expresshealthcare.in/insurance/indian-health-insurance-a-shifting-landscape/445736/) The latest healthcare provider to foray into health insurance, Narayana Health’s Aditi plan offers Rs 1 crore for surgeries and Rs 5 lakh for medical management at Narayana Health network hospitals.
Narayana Health is not the first healthcare provider to foray into health insurance. The question is, can it succeed when predecessors have had mixed results?
Way back in 2007, the Apollo Hospitals group’s insurance foray resulted in Apollo Munich Health in 2007. This was sold to HDFC in January 2020, and is now merged with HDFC’s general insurance arm, HDFC ERGO. Some media reports surfaced in December 2023 that Apollo Hospitals was contemplating another foray into insurance.
In 2008, Max India tied up with UK-based healthcare services expert, Bupa for a joint venture, Max Bupa Health Insurance. By end 2019, Max India had exited the health insurance JV, selling its stakes to Fettle Tone LLP, an affiliate of True North Fund VI LLP, with the health insurance business rebranded to Niva Bupa.
In 2012, Religare Health Insurance was established as a JV between Religare Enterprises, Union Bank of India, and Corporation Bank. Fortis Healthcare and Religare Health Insurance (renamed as Care Health Insurance in 2020), were both promoted by brothers Malvinder and Shivinder Singh. Today, Religare Enterprises,
The rationale for hospitals venturing into insurance and vice versa is the same: bridging the trust gap between the three Ps: patients, providers (hospitals) and payers (insurance companies)
the holding company of Care Health Insurance, is caught in the eye of a stormy takeover battle between the Burmans of Dabur and the Religare board.
In 2018, the Manipal Group formed a joint venture partnership with Cigna Corporation and TTK Group, resulting in ManipalCigna Health Insurance.
In the past week, insurance broker Policybazaar’s parent company PB Fintech’s announcement that it was earmarking up to $100 million for a 20-30 per cent stake in a new healthcare company, structured along the lines of a Health Maintenance Organisation (HMO) model, has garnered a lot of interest. Though this is still at the planning stage and will need board approval, it indicates a stirring of the health insurance pot in India. Could this set the stage for more such collaborations? It's fair to say that while many would like a shot at India's health insurance market, finding the right balance has been tricky. The proverbial pot of gold remains elusive, but as more people seek health insurance after the COVID shock, perhaps the time is finally right.
The rationale for hospitals venturing into insurance and vice versa is the same: bridging the trust gap between the three Ps: patients, providers (hospitals) and payers (insurance companies).
Prima facie, patients would benefit as hospitals would keep costs reasonable. Hopefully, the discharge and the claims process would also be a lot smoother. Payors and providers would be able to nudge the insured population to monitor their health parameters. Once incentivised to keep patients healthy to reduce claims, the focus should shift from ‘sick care’ to ‘health care’, with the aim to remain healthy and prevent, delay and manage the onset of disease conditions.
But that's in theory. Let's hope reality lives up to the stated mission/vision. And of course, revenue projections.
Dr Harshal Tambe ,Managing Trustee,SMBTEducational Trust shares SMBT's vision, expansion plans and more,in an exclusive interaction with Express Healthcare
Can you share your vision for the hospital and how are you driving the organisation towards achieving it?
It was truly a purpose-driven initiative for us. We began with a mission to serve the underserved. Our journey started with a small unit in Sangamner, a Taluka place near Shirdi, where we established a 100-bed hospital for sugarcane workers. This hospital was closely aligned with our sugar factories and marked the beginning of our venture into healthcare.
As we developed this campus, the core purpose remained providing affordable healthcare. When I completed my studies and started looking into management, I realised that in the future, hospitals in India would fall into two models: large corporate hospitals with big setups, and extremely charitable models, driven by government initiatives.
I believed that aligning with national goals was crucial, so affordable healthcare became the primary vision for this hospital. Our mission at SMBT has always been to serve everyone, regardless of their socio-economic background, religion, or caste. 'Health for all' is our guiding principle at SMBT, and it remains central to our operations.
We ensure that no one entering the gates of SMBT leaves without receiving care, regardless of their financial situation. We are creating an ecosystem around affordable healthcare, ensuring we cater to every sector of the society. This was, and continues to be, the foundational vision of SMBT Hospital.
Can you elaborate on the initial facilities and how you expanded?
We started very small, focusing initially on education with pharmacy and Ayurveda
Whether it’s service expansion,technological advancements,community outreach,or sustainability,everything will be centered on patient outcomes and experiences.Sustainability, in particular,is vital to maintaining affordable healthcare,which requires us to continually improve our processes and operations
disciplines on this campus. We had a modest 100-bed Ayurveda hospital. When we decided to establish a modern hospital, we recognised that this area, a notified tribal and hilly region, lacked adequate healthcare facilities. Today, it might be the largest hospital in Maharashtra situated in such a region. Over the past 10 years, we've worked tirelessly to develop this area, which now has much better connectivity.
In the beginning, people questioned our decision to develop in this remote area, but we were determined. We started with a small outpatient department (OPD) with just four consultants in medicine, surgery, and radiology, who would come from Nashik for a few hours a day. From those humble beginnings, we have grown to nearly 350 consultants and expanded from 300 beds to almost 1,000 beds, including over 200 critical care beds.
It’s fascinating to see both an Ayurveda hospital and a multi-specialty hospital coexisting in the same campus. How do you balance both the practices?
It’s been challenging to balance both. Convincing our Ayurveda practitioners to stay focused on their core practices, like Panchakarma, while we develop a modern hospital alongside, was no small feat. They are achieving incredible results in their discipline, and simultaneously, we’ve been advancing the modern hospital.
Right from the start, I had the idea of emphasising super specialties. My goal was to introduce at least one new super specialty each year. When we began this hospital in 2013-14, the first super specialty we introduced was cardiology and cardiothoracic vascular surgery (CVTS).
Today, we’re performing over 200 to 250 procedures per
month in cardiology and more than 50 procedures in CVTS, which is a significant achievement.
We’ve continued to add new super specialties every year. Now, this hospital, located in a tribal and hilly region, is likely the first to have over 25 super specialties under one roof. The only specialty we’re yet to operationalise is radiation oncology, but it’s in progress and should be ready within the next eight or nine months. Once that’s complete, we’ll have a comprehensive range of specialties all in one place.
In what ways is your hospital leveraging technology to improve patient care and outcomes?
Despite being a large, affordable and charitable hospital, we have our challenges, but we've managed to become almost 90 per cent digital. We’re integrating HMIS, EMRs and EHRs across the hospital. Although implementing EHRs at such a large scale is challenging, we've started with a few pilot projects in some departments and aim to expand this further.
We’ve also digitalised many aspects of our operations, from diet plans to pharmacy services. For instance, we might be the first charitable hospital of this size to offer bedside delivery of medications. This means patients under specific schemes don’t need to visit the pharmacy; everything is delivered directly to their bedside. In terms of infrastructure, we have 12 to 14 modular theatres built to international standards. We've ensured that
even though we provide affordable services, the quality and class of our infrastructure meet global standards. Recently, we introduced Bone Marrow Transplant (BMT) services, which involve complex
treatments and significant investments in advanced technology. We’ve also conducted clinical trials with CAR T cells, a breakthrough in medical treatment.
With the high number of
surgeries we perform—over 1,400 monthly, including 150 joint replacements—we’re planning to bring in robotic technology within the next six months. This will be a significant advancement, especially for orthopaedic and general surgery, providing our students and surgeons with exposure to the latest technology. Our aim is to offer complex surgeries through advanced technologies at affordable rates without compromising on quality.
In cardiology, we were the first to bring the FD10 cath lab to North Maharashtra in 2015. Similarly, we were the first in the region to conduct CAR T cell treatments. Our future plans include introducing a state-of-the-art linear accelerator (LINAC) for radiation oncology, ensuring we stay at the forefront of medical technology.
Another major innovation we're focusing on is telemedicine. Our goal is to make telemedicine accessible on everyone’s mobile devices, with a simple, user-friendly interface. We’ve already launched pilot initiatives, and the feedback has been positive. Our vision is to provide free, easy access to consultations, especially for those in remote areas like Nandurbar and Palghar.
During the COVID-19 pandemic, we successfully ran a pilot for free video consultations, handling about
BMT - CELL & GENE THERAPY UNIT
AT SMBT HOSPITAL, SINCE 2014
INTERVIEW
100 consultations daily. Now, we're working on making this service even more streamlined and accessible. We aim to offer a simple link for appointments, avoiding complex procedures like multiple uploads, making it as easy as a video call.
This approach ensures that patients can receive the care they need without unnecessary complications, and we’re committed to making healthcare as accessible and straightforward as possible.
What role does the sustainability play in the hospital's operations and what steps are you taking to reduce the hospital?
The location is naturally conducive to sustainability, but we are very conscious about our environmental impact. At SMBT, we adhere to a strict 'no vehicle' policy on campus, reflecting our commitment to a vehicle-free environment. Additionally, we’ve implemented a no-plastic policy and several other initiatives that align with our values of environmental consciousness and sensitivity.
For the hospital specifically, we’re focusing on energy efficiency. We are gradually replacing older systems with more energy-efficient alternatives, including expanding our use of solar energy, which we already have on campus. Water conservation is another priority for us, even though we are in a region blessed with natural resources. We’ve implemented measures to conserve water and ensure that we manage waste according to the highest standards, including proper segregation and disposal as required by law.
When it comes to our building practices, we are integrating sustainable architecture into all our new constructions. This includes green building concepts like maximising natural light and ventilation, which not only benefit the environment but also improve the healing environment for our patients. Given the ample space and favorable surroundings we have here, we’re able to leverage these advantages fully.
We are also fortunate to have a location with excellent air quality, which has been validated by recent surveys. The air quality here at SMBT is significantly better than in urban areas, and this has a positive impact on our patients' health and recovery.
What are your future plans for the hospital's expansion, both operationally and geographically?
Operationally, one of our most significant breakthroughs is our MOU with Tata Memorial Hospital. This partnership is pivotal as we are now developing a 100-200 bedded dedicated cancer hospital at SMBT, which will house all surgical, medical and radiation oncology departments.
In addition to this, we are
focusing on integrating all government schemes at SMBT. While many claim to implement government schemes, our emphasis is on doing so religiously, without any additional costs to patients. This is crucial, as we want to ensure that the benefits of national and state schemes reach our patients directly. We've been particularly successful with schemes like MJPJAY in Maharashtra and Ayushman Bharat at the national level. In fact, for the past three years, we’ve been recognised as the best hospital in the Maharashtra region for implementing these schemes, with awards presented during the annual Republic Day celebrations by the regional commissioner and collector in Nashik.
In terms of service expansion, besides oncology, we are looking into other specialities as well.
Geographically, Nasik is a strategic location for us. Many doctors from Nashik city are engaged with SMBT, and it's my responsibility to maintain and enhance this engagement. We’re considering setting up facilities in Nasik city to cater to those seeking affordable healthcare. Furthermore, we are planning to expand in Thane and Mumbai regions. These are the two strategic locations we’ve shortlisted. If we move into these areas, our focus will be on super speciality care, with a primary emphasis on cardiology and oncology, given our established centers of excellence in these fields. We’ll
also consider joint replacements, as our numbers—150 per month— demonstrate our proficiency in this area.
For the new facilities, we are envisioning a minimum of 300 beds to support a multispeciality setup. Given our preference for a brownfield project over a greenfield one, we aim to complete this expansion within the next two years."
What are the top priorities for the hospital over next five years?
As I mentioned earlier, our first and utmost priority is patient experience. This is crucial, especially considering the challenges our country and state face within the healthcare ecosystem. I firmly believe that the patient comes first, and all our planning will revolve around patient treatments and patient experience.
Whether it’s service expansion, technological advancements, community outreach, or sustainability, everything will be centered on patient outcomes and experiences. Sustainability, in particular, is vital to maintaining affordable healthcare, which requires us to continually improve our processes and operations. This focus will remain consistent as we continue to expand.
Patient satisfaction is also a key component of our approach. We conduct various feedback exercises, including real-time feedback during hospital stays, post-discharge feedback, and follow-up calls after three to five days. If necessary, our team even visits patients at home, and we connect them directly with their treating doctors to resolve any issues or confusion.
This feedback mechanism is a critical part of our operational reviews, and we have seen positive results from these efforts over the past years. It’s a continuous process because, regardless of whether our services are provided free of charge, under a scheme, or through charity, we can never compromise on patient satisfaction and experience.
100+ CRITICAL ICU BEDS
SMBT CLINIC
INTERVIEW
Global suppliers continue to playa significant role in India's healthcare sector
Pradeep Mishra, Vice PresidentCentral Procurement & Supply Chain, Paras Healthcare
in an interaction with Express Healthcare talks about the healthcare procurement and supply chain industry
How has the Indian healthcare supply chain evolved over the past decade, and what key factors have driven this transformation?
The Indian healthcare supply chain has undergone a significant transformation over the past decade, driven by several key factors:
● Economic growth: Rapid economic growth has led to increased demand for healthcare services, driving the expansion of the healthcare sector and its supply chain.
● Government initiatives: Government initiatives such as the National Health Mission and Ayushman Bharat have played a crucial role in improving healthcare access and infrastructure, which has had a ripple effect on the supply chain.
● Technological advancements: The adoption of technology has revolutionised various aspects of the healthcare supply chain, from procurement and
INTERVIEW
inventory management to logistics and distribution.
● Increased competition: The entry of private players and increased competition has led to a focus on efficiency, cost-effectiveness, and quality in the healthcare supply chain.
What role is technology playing in transforming healthcare procurement and supply chain management in India? Which innovations are having the most significant impact?
Technology has become an integral part of healthcare procurement and supply chain management in India. Some of the most impactful innovations include:
● Electronic Health Records (EHRs): EHRs provide a centralised repository of patient data, facilitating better decision-making and streamlining procurement processes.
● Supply chain management software: Specialised software solutions help optimize inventory management, procurement planning, and logistics.
● Blockchain technology: Blockchain can enhance transparency, security, and traceability in the supply chain, particularly for pharma and medical devices.
● Artificial Intelligence (AI): AI can be used for predictive analytics, demand forecasting, and optimising supply chain operations.
The digitalisation of healthcare procurement is gaining momentum in India. What challenges do organisations face when transitioning to digital platforms, and how can these be overcome?
While digitalisation offers numerous benefits, healthcare organisations may face challenges when transitioning to digital platforms:
● Data security: Protecting sensitive patient data and ensuring data privacy is a top priority.
● Interoperability: Integrating different systems and ensuring data compatibility can be complex.
The development of digital health ecosystems will create new opportunities for collaboration and innovation in the healthcare supply chain
● Resistance to change: Overcoming resistance from employees who may be unfamiliar with new technologies.
● Cost: Implementing and maintaining digital solutions can be costly. To overcome these challenges, organisations can invest in robust cybersecurity measures, choose compatible systems, provide adequate training to employees, and carefully evaluate the longterm benefits of digitalisation.
What changes in procurement and supply chain management have become permanent due to the pandemic, and how are healthcare institutions preparing for future disruptions?
The COVID-19 pandemic has accelerated certain trends in healthcare procurement and
supply chain management:
● Increased focus on resilience: Healthcare institutions have become more focused on building resilient supply chains to withstand future disruptions.
● Telehealth adoption: The widespread adoption of telehealth has created new demand for medical devices and supplies that support remote patient care.
● Just-in-Time (JIT) inventory: Many organisations have shifted away from JIT inventory models to ensure adequate stock levels in case of future shortages.
● Domestic sourcing: There has been a renewed emphasis on sourcing supplies domestically to reduce reliance on foreign suppliers.
How is the role of global suppliers evolving in India’s
healthcare sector, and what opportunities and challenges do they present to local procurement processes?
Global suppliers continue to play a significant role in India's healthcare sector, offering a wide range of products and services. However, they also present challenges:
● Regulatory compliance: Ensuring compliance with Indian regulations can be complex.
● Quality concerns: Maintaining consistent quality standards can be difficult, especially for products sourced from different regions.
● Supply chain risks: Disruptions in global supply chains can impact availability and pricing.
Local procurement processes can mitigate these
risks by fostering relationships with reliable domestic suppliers and diversifying sources.
What are the most pressing challenges currently facing the healthcare supply chain in India, particularly for hospitals?
Some of the most pressing challenges facing the healthcare supply chain in India include:
● Drug shortages: Ensuring adequate availability of essential drugs, particularly those used in chronic diseases.
● Counterfeit drugs: Combating the proliferation of counterfeit drugs that pose serious health risks.
● Infrastructure constraints: Inadequate infrastructure, such as warehouses and cold storage facilities, can hinder efficient supply chain management.
● Price controls: Government price controls can impact the profitability and limit investment in research and development.
What trends do you foresee shaping the future of healthcare procurement and supply chain management in India over the next 5-10 years?
Several trends are likely to shape the future of healthcare procurement and supply chain management in India:
● Increased use of analytics: Data analytics will play a crucial role in optimising inventory management, demand forecasting, and supply chain planning.
● Sustainability: There will be a growing focus on sustainable procurement practices, including reducing waste, minimising environmental impact, and supporting ethical sourcing.
● Digital health ecosystems: The development of digital health ecosystems will create new opportunities for collaboration and innovation in the healthcare supply chain.
● Supply chain visibility: Advancements in technology will enable greater visibility and transparency throughout the supply chain, improving efficiency and reducing risks.
CEO CORNER
PPPs have the potential to make healthcare more affordable and accessible
Surendran Chemmenkottil, CEO,Metropolis Healthcare,discusses the company’s key goals for the coming years and more in an interaction with Kalyani Sharma
The diagnostic sector has witnessed substantial growth in recent years. What factors do you think are driving this growth, particularly in the postpandemic era?
There are several factors contributing to the growth of the diagnostic sector, especially after the pandemic. Firstly, there’s increased awareness about healthcare, and people are now more conscious of the need for regular and high-quality medical check-ups. The wellness segment has also grown, with more individuals proactively seeking regular health assessments. Additionally, chronic diseases and the aging population are fueling the demand for better healthcare services.
Expansion into tier 2 and tier 3 cities has also been a significant driver, with advanced diagnostics becoming more accessible across India.
How crucial are PublicPrivate Partnerships (PPPs) in expanding diagnostic services to tier 2 and tier 3 cities? What challenges do you face when collaborating with the government?
PPPs have the potential to be hugely beneficial in making healthcare more affordable and accessible. However, while there are opportunities, not many partnerships have gained traction. One challenge is ensuring a win-win situation where private players can operate sustainably.
Government processes, particularly around funding and payment timelines, can be slow, creating financial stress for private entities. Despite
Emerging infectious diseases will continue to play a role in driving growth.The trend toward early diagnosis is growing,and people are increasingly seeking tests even before diseases become critical
these challenges, we have successfully implemented a few PPPs and remain open to more as long as they make economic and operational sense.
Looking ahead, how do you see the Indian diagnostic sector evolving in the next five years, particularly in terms of market share and service offerings?
While it's hard to pinpoint exact market shares due to the lack of reliable industry data, organised players, including listed and regional chains, are poised to see a significant
increase in their share of the market. The demand for highquality diagnostics is rising, especially for specialised and high-end testing, which organised players can better deliver compared to smaller, unorganised labs.
Technological advancements, such as asset-light models and remote diagnostics, will also help organised players expand their reach. Additionally, investments in emerging fields like genomics and molecular diagnostics will further boost growth.
Emerging infectious
diseases are also becoming a concern. How do you foresee this area contributing to the sector’s growth?
Yes, emerging infectious diseases will continue to play a role in driving growth. The trend toward early diagnosis is growing, and people are increasingly seeking tests even before diseases become critical. The preparedness of private players like us to quickly scale up our capabilities when new diseases emerge is improving. For instance, with the Mpox outbreak, we can ramp up testing capabilities as soon as
we receive government guidelines.
What role do you see telemedicine and remote diagnostics playing in the future of healthcare, and how have technological innovations impacted your business model?
Telemedicine and remote diagnostics are already making a significant impact. At Metropolis, we've built fully digital systems over the last few years. Today, we can conduct remote diagnostics across borders, speeding up diagnosis and improving customer outcomes. Artificial intelligence is also helping us predict diseases and improve process efficiencies. For example, we can now analyse a customer’s past medical data and suggest proactive steps for their health management, offering a more personalised healthcare experience.
What are the key goals for Metropolis Healthcare in the coming years, particularly in terms of growth and innovation?
We aim to expand our services to cover at least 1,000 towns across India, up from the 650 we currently serve. Our focus remains on providing highquality diagnostic services, especially in specialty areas like oncology, neurology, nephrology, Women and Child health, and infectious and chronic diseases. We also plan to continue leveraging technology to enhance productivity and improve customer experiences, all while maintaining profitability.
Public health infrastructure,while improving,requires collaborative efforts to combat the threat of infectious diseases
ByKalyani Sharma
India’s battle with infectious diseases is a critical aspect of its healthcare journey, shaped by the nation’s vast, diverse population and socio-economic challenges. From tuberculosis to malaria, dengue, and more recently, COVID-19, infectious diseases remain a constant threat to public health, particularly in densely populated regions. The pandemic, however, acted as a tipping point, underscoring the urgent need for a comprehensive, futureready public health infrastructure capable of swift responses to outbreaks. In this cover story, we explore the current state of India’s public health infrastructure for infectious diseases, recent advancements, challenges, and a forward-looking roadmap for preparedness.
The existing state of public health infrastructure in India
A self-assessment done by the government in June 2024 has revealed that most public health facilities, including district hospitals and primary health centers, fall significantly short of essential standards. Only 20 per cent of these facilities meet the required benchmarks for infrastructure and resources, while a troubling 42 per cent have scored below 50 per cent. In response, the government has launched an initiative to upgrade 70,000 facilities within 100 days, with inspections and funding support provided under the National Health Mission. This underscores the urgent need for reforms to improve healthcare delivery and ensure equitable access to quality services across the country.
According to data from the Indian Public Health Standards (IPHS) dashboard, only about 20 per cent of the assessed facilities achieved a score of 80 per cent or higher, meeting essential standards for infrastructure, staffing, drugs, diagnostics, and equipment. This reflects a
India's public health infrastructure is like a neglected child - Health being a state subject - has traditionally not been looked after well by the centre and states have always had other priorities
Dr R Kishore Kumar
Founder Chairman, Pediatrician and Neonatologist, Cloudnine Group of Hospitals
Although the level of healthcare infrastructure is comparatively higher in urban areas,rural areas remain behind in terms of infrastructure facilities, which leaves them dragged behind in responding to infectious diseases in the first instance
Dr Avinash Phadke President and Mentor, Agilus Diagnostics
Adopting the ‘neighbourhoods of care’ model,which engages families and communities in prevention and early detection,is essential.It empowers communities with knowledge and skills for local action is built around supportive community networks and a knowledge system
Shyamal Santra Associate Director-Health and Nutrition, Transform Rural India
Strengthening the integration of digital tools in disease surveillance can improve granular and disease specific data capture and analysis,leading to faster and more effective responses
Dr Dileep Raman
Co-founder and Chief of Healthcare, Cloudphysician
widespread gap in basic healthcare provisions across most public health facilities.
Of the facilities assessed, 42 per cent—equating to 17,190 facilities—scored below 50 per cent, highlighting critical deficiencies in key healthcare areas. Additionally, 15,172 facilities fell within the 50 per cent to 80 per cent range, further indicating varying degrees of inadequacy throughout India’s public healthcare system.
Targeted investment in infrastructure and enhanced monitoring could fill the gaps.
Dr R Kishore Kumar, Founder Chairman, Pediatrician and Neonatologist, Cloudnine Group of Hospitals, Bengaluru mentions that India's public health infrastructure is like a neglected childhealth being a state subjecthas traditionally not been looked after well by the centre and states have always had other priorities.
“The country has made remarkable strides in eradicating diseases like smallpox and polio because it has been a directive of WHO and international organisations including Rotary International have contributed significantly, and it has established national programs for tuberculosis (TB), malaria, HIV/AIDS, and other communicable diseases - but research in these areas have been very slow and almost negligible for a country of our size. However, the COVID-19 pandemic exposed critical gaps in the health system, particularly in areas like disease surveillance, healthcare delivery, and resource allocation. Without research and data analysis - we won't be going anywhere.”
Dr Avinash Phadke, President and Mentor, Agilus Diagnostics mentions, “India has substantially improved its public health facilities over the years that exist; h owever, it still faces limitations due to high population density, geographic as well as economic division. It involves central and state schemes and
programs, which operate with different capacities and assign resources to Indian states. Although the level of healthcare infrastructure is comparatively higher in urban areas, rural areas remain behind in terms of infrastructure facilities, which leaves them dragged behind in responding to infectious diseases in the first instance.”
Primary Care Centers (PHCs) and Community Health Centers (CHCs) form the backbone of India’s healthcare system, but they often lack adequate resources, personnel, and technological integration, particularly in tier 2 and 3 cities and rural regions. Urban centers may have more advanced facilities, but the uneven distribution of healthcare services leaves rural populations particularly vulnerable.
Shyamal Santra, Associate Director-Health and Nutrition, Transform Rural India also share some stats and said, “Rural Health Statistics from 2021-22 reveal significant shortfalls: 25 per cent of Sub Centres (SCs), 31 per cent of Primary Health Centres (PHCs), and 36 per cent of Community Health Centres (CHCs) are lacking. There is a shortfall of 4,335 physicians and 294 pharmacists, with an even greater deficit in tribal areas. Specialist shortages are severe, with 83.2 per cent fewer surgeons, 74.2 per cent fewer obstetricians, and 81.6 per cent fewer paediatricians than needed. The acute shortage of trained health professionals and infrastructure impacts quick response.”
Dr Madhuri Somani, Consultant microbiologist and infection control Officer, PSRI Hospital, New Delhi throws light on a very relevant point. She mentions, “COVID-19 was testament to the potential of our public health capabilities. But, where do we currently stand in handling infectious diseases especially in the time of antimicrobial resistance and emerging threats like Monkeypox and Zika virus to
name a few”
She mentions that, “Currently, there is a huge disparity between urban and rural areas as microbiology and molecular diagnostics laboratories are primarily concentrated in the former. Strengthening them throughout the country should be the foremost prerogative ,because if an infectious disease diagnosis cannot be made , the clinician is left with no option
While the Indian government has initiated efforts like the Skill India Program,these need to be significantly scaled up to meet the growing demand, especially in infectious disease management
Garima Malhotra Associate Partner, Praxis Global Alliance
Currently,there is a huge disparity between urban and rural areas as microbiology and molecular diagnostics laboratories are primarily concentrated in the former.Strengthening them throughout the country should be the foremost prerogative
Dr Madhuri Somani
Consultant microbiologist and infection control Officer, PSRI Hospital
Challenges regarding data quality and integration persist with inconsistent reporting and a lack of standardised protocols hindering effective surveillance
Dr Gunisha Pasricha Principal Scientist, Infectious Diseases, MedGenome
but to treat an infection blindly. “Super bugs” : The drug resistant bacteria ,viruses ,fungi and parasites , can only be detected in Wellequipped laboratories ,with a gamut of tests like culture and sensitivity ,molecular diagnostics , ancillary serology to guide appropriate clinical treatment ,trained clinical microbiologists and paramedical staff with an indepth knowledge of Antimicrobial
resistance( AMR) . Research and public health funding into affordable diagnostic tests and Point of care tests should be prioritised. NAATs are molecular tests, which are being used in our National TB elimination programme ,is an apt example.”
Role of disease surveillance
and management
Effective disease surveillance
is crucial for identifying outbreaks early and mounting timely responses. While India has made strides in developing its surveillance systems, significant challenges remain. The Integrated Disease Surveillance Programme (IDSP) is an important initiative, but it suffers from inconsistent reporting, limited data integration, and reliance on outdated methods in some areas.
Talking about the challenges, Dr Gunisha Pasricha, Principal Scientist, Infectious Diseases, MedGenome said, “Challenges regarding data quality and integration persist with inconsistent reporting and a lack of standardised protocols hindering effective surveillance. Coverage in rural areas is often limited, primarily due to insufficient healthcare infrastructure and personnel. Furthermore, the lack of specialised training in infectious disease management limits healthcare providers' capacity to respond effectively to outbreaks. India continues to experience frequent outbreaks of diseases like dengue, cholera, and influenza, which strain the public health infrastructure. The rise of new infectious diseases and the resurgence of previously controlled diseases present significant challenges to surveillance and management efforts.”
“Gaps in the system include the need for comprehensive training programs in infectious disease management, such as expanded master's in public health (MPH) courses and specialised residency programs. Further genomic sequencing should be integrated into routine diagnosis and surveillance. Additionally, increasing public awareness about disease prevention and control can enhance community participation in surveillance efforts”, she added.
Dr Dileep Raman, Cofounder and Chief of Healthcare, Cloudphysician also opines that “Strengthening the integration of digital tools
in disease surveillance can improve granular and disease specific data capture and analysis, leading to faster and more effective responses. Expanding diagnostic capabilities will ensure more accurate reporting and reduce reliance on estimations.”
According to Dr Sandeep S Reddy, Consultant-Department of Infectious Diseases, Ramaiah Memorial Hospital, despite the advancements in technology and communication, the real-time data collection, analysis, and response mechanisms are not fully optimised, with many states still relying on manual methods, leading to delays in identifying and responding to outbreaks. Thereby existing in poor coordination between different levels of government (central, state, and local) and between public and private healthcare providers.
The strengths of India’s disease surveillance lie in the scale of its public health programs, particularly its ability to collect data from a wide range of sources. However, weaknesses are evident in terms of inter-agency coordination, data analysis capacity, and the use of predictive analytics to preempt future outbreaks. Improving infrastructure in tier 2 and 3 cities and rural regions should also be prioritised. By investing in regional healthcare facilities and enhancing their connectivity to national disease control centers, India can create a more resilient network to respond to health crises.
The role of technology and digital health Technology has the potential to revolutionise how India manages infectious diseases. Artificial Intelligence (AI) and machine learning (ML) are already being used to predict outbreaks based on climate data, migration patterns, and other factors. Moving forward, AI could help forecast disease trends, enabling proactive measures rather than reactive ones.
Dr Sunil Rana, Associate Director and Head- Internal Medicine, Asian Hospital, Faridabad shares, “To expedite data collection, processing, and dissemination, IDSP, for example, made use of information and communication technology (ICT) networks during H1N1 outbreak. These expenditures aided in the resolution of a number of issues, such as the capacity to reach out to isolated communities, increase private sector
Despite the advancements in technology and communication,the real-time data collection,analysis,and response mechanisms are not fully optimised, with many states still relying on manual methods,leading to delays in identifying and responding to outbreaks
Dr Sandeep S Reddy
Consultant-Department of Infectious Diseases, Ramaiah Memorial Hospital
To expedite data collection,processing, and dissemination,IDSP,for example, made use of information and communication technology (ICT) networks during H1N1 outbreak.These expenditures aided in the resolution of a number of issues
Dr Sunil Rana
Associate Director and Head- Internal Medicine, Asian Hospital
More government hospitals,medical colleges,and expansive healthcare infrastructure can help address the healthcare needs of India’s growing population
participation, and promote the use of other forms of communication including voicemail and email.”
Telemedicine is another critical component. During the pandemic, telemedicine provided an essential bridge between patients and healthcare providers. By expanding telemedicine infrastructure, especially in rural regions, India can make healthcare more accessible while ensuring infectious diseases are managed
without overcrowding urban hospitals.
Dr Phadke opines that what remains central to embracing technology is the ability to enhance India’s public health frameworks. New interventions in the field of digital health like the National Digital Health Mission (NDHM) are opening innovations towards better data integration and patient handling. Telemedicine has emerged as an important
means of providing healthcare to distant communities increasing the rate of diagnosis and treatment.
Dr Raman also shares, “Mobile health applications can also empower individuals to monitor and report symptoms, contributing to a more comprehensive surveillance network. Mathematical modeling and machine learning are particularly useful for predicting disease trends and outbreaks by analysing datasets and identifying patterns. Additionally, technology helps track antimicrobial resistance, providing data for developing new treatments and vaccines.”
Workforce capacityand training
A robust healthcare system depends on a well-trained workforce. Capacity building for healthcare workers, particularly in infectious disease management, is vital. The lack of trained personnel in rural and remote areas exacerbates India’s healthcare challenges. Malhotra stresses, “Over 75 per cent of healthcare professionals are in urban regions, leaving rural areas critically underserved. This urban concentration of healthcare providers, coupled with the limited availability of specialists in rural Community Health Centres (CHCs), poses a substantial challenge in managing infectious diseases. The shortage of trained public health professionals, including epidemiologists and microbiologists, further hampers effective disease monitoring and response. To address these gaps, enhancing training and skill development programs is crucial. While the Indian government has initiated efforts like the Skill India Program, these need to be significantly scaled up to meet the growing demand, especially in infectious disease management.”
Santra also suggest, “Adopting the ‘neighbourhoods of care’ model, which engages families and
communities in prevention and early detection, is essential. It empowers communities with knowledge and skills for local action is built around supportive community networks and a knowledge system, and emphasises that healthcare challenges cannot be addressed through medical or clinical interventions alone - it integrates the needs, values, and aspirations of individuals, families, and communities, providing a well-rounded solution to health concerns in under-resourced areas.”
Continuing medical education (CME) programs, combined with on-the-job training and digital learning platforms can also ensure that healthcare workers are up to date on the latest treatment protocols, surveillance technologies, and public health strategies.
Dr Ravishankar Polisetty, a former cardiac surgeon turned translational Ayurvedic researcher highlights that, “More government hospitals, medical colleges, and expansive healthcare infrastructure can help address the healthcare needs of India’s growing population. The creation of over 1,70,000 Ayushman Arogya Mandirs (family health centres) across the country is also a significant effort to improve access to primary healthcare in both rural and urban areas. A recent EYFICCI report on ‘Decoding In-
◆ India has ~41Kgovernment hospitals with ~849Kbeds,but this capacity remains insufficient for a population exceeding 1.4 billion.This results in a bed-to-population ratio of roughly 1.8 beds per 1,000 people,which falls short of the World Health Organization’s (WHO) recommendation of 3.5 beds per 1,000 people. Nevertheless, ongoing efforts to expand hospital infrastructure offer a promising avenue for improvement.
◆ Asignificant challenge lies in the distribution of healthcare professionals,with over 75 per cent concentrated in urban areas,which account for only ~37 per cent of the population.This urban concentration leaves rural regions,where the need is often greatest,particularly underserved.The shortfall of specialists in rural Community Health Centres (CHCs) is a critical issue,with an 80 per cent overall shortage and specific gaps of 83 per cent for surgeons and 79 per cent for physicians.Addressing this disparity is essential for improving the management of infectious diseases nationwide.
◆ India's healthcare expenditure,currently at 1.9 per cent of GDPfor FY24,is relatively low compared to other major economies.Although the National Health Policy (NHP) 2017 aims to increase this to 2.5 per cent by 2025, progress has been gradual.Public spending on healthcare is primarily directed towards curative care,with insufficient investment in preventive measures and infrastructure.
◆ The COVID-19 pandemic highlighted critical areas for improvement within India’s healthcare infrastructure,such as the availability of hospital beds,ventilators,and essential medicines.
◆ This crisis spurred significant international support,including a US$ 1B loan from the World Bank in 2023 to enhance pandemic preparedness and health service delivery.These developments indicate a proactive shift towards strengthening healthcare resilience in the face of future outbreaks.
◆ Financial barriers to healthcare access remain a concern,with a substantial portion of the population still lacking health insurance.Over 70 per cent of middle-income individuals do not have health coverage,leaving them vulnerable to catastrophic health expenditures.Expanding insurance coverage and making healthcare more affordable are key steps towards better managing infectious diseases.
◆ Sanitation and access to clean water are also crucial in the fight against infectious diseases.According to the National Family Health Survey (NFHS) - 5,while 70 per cent of households in India have access to improved sanitation,only 40 per cent treat their water before drinking,which is essential for preventing the spread of infections.Continued investment in sanitation and water treatment infrastructure will play a vital role in disease prevention.
dia’s Health Landscape’ states that by 2047, the country will require 12.5 million qualified doctors and 15 million nurses.”
Wayforward
Looking ahead, India’s strategy to combat infectious dis-
eases must focus on creating a comprehensive, multi-layered health infrastructure that integrates disease surveillance, technological innovation, and workforce capacity building.
Public health infrastruc-
ture, while improving, requires bold initiatives and collaborative efforts to effectively combat the threat of infectious diseases. The lessons learned from the COVID19 pandemic must shape a new era of preparedness, where rapid responses, technological inn ovations, and well-trained healthcare workers form the cornerstone of a future-ready system.
Dr Yash Javeri, Director- Critical Care and Emergency Medicine,Regency Health Lucknow emphasises that current trends in India's population and the demographics of critical care staff necessitate urgent changes in critical care
Critical care is starting to face some tough obstacles, and the ICU of the future will be shaped by these problems—namely an aging population, care gaps, digital dimension, and a disproportionately low number of ICU professionals. The supply-anddemand quandary is already apparent in the ICU. Because of these impending changes, in 20 or 30 years your hospital’s ICU must look different and work differently to handle a steady influx of patients. We have significant care gaps in the present functioning of ICUs. We have to examine future possibilities for staffing structure, introduction of critical care guidelines, and groundbreaking technical solutions. We also need to look at the challenges of the future while we reframe our concepts.
Core concept of ICU
What defines ICU is the ICU Team. What matters most is the intensivist and critical care nurses.
Nurses are the backbone of the ICU. Some are not numbers, and soon is not a time for ICU patients.
# Every life matters
The growth of ICU Beds
The rising number of beds and the severity of the disease are driving organic growth in ICU beds across the globe. The growth is more evident in LMIC countries where ICU beds are a scarce resource. We also need non-designated reserve areas that can be modified for the ICU. The growth of ICU beds puts pressure on already deficient ICU manpower.
Supplyand demand of critical care demands change
Current trends in India's population and the demographics of critical care staff dictate that critical care must change—and
fast. With millions of baby boomers aging, demand for designated critical care wards within hospitals will increase. The greying population already occupies a large chunk of ICU beds. The supply-and-demand quandary is now becoming challenging in the ICU. We also need to examine future possibilities for staffing structure, introduction of critical care guidelines, and groundbreaking technical solutions.
Market challenges
Despite promising growth, we face challenges related to the high costs of ICU stay, which poses financial strains on healthcare systems and patients. The high-cost ICU model can impede access, especially in low-resource settings. Cost-effectiveness and other financial models to share the financial burden are urgently required. Affordability and outcome-oriented services are needed urgently. ICU needs to reach where it’s required most.
Structure
The infrastructure of critical care needs to be transformed
and the focus must pivot to ways that enhance personalised medicine. Technology will continue to make strides which should provide us with the tools for redesigning processes of critical care management.
Less is more
The intensive care community is increasingly exploring; can “Less be More” in the management of the critically ill. It is worth pointing out that “Less is More” is not a lazy approach; rather, it is a well-researched and carefully thought-out strategy aimed at getting rid of the therapies that do not improve clinical outcomes. Now is the time to recognise that “more care is not always better”. Ensure that the practices we implement are intended to be high-value. A minimalistic approach is required and at the same time, we need to be aware that that one size doesn’t fit all.
Individualised and personalised
We are increasingly aware that in the ICU, as across all other medical fields, patients must be
treated as individuals and not as diseases. The concept should be applied not only to clinical management but also to other nonmedical needs. We can characterise patients better, and our ability to identify phenotype subgroups will help precision medicine.
Affordable care
Cost optimisation is an urgent need of the hour. Cost analysis of each intervention needs to be done with a conscious serious effort every time. Indigenous solutions need to be explored. We need to triage our resources and invest in areas of need.
Critical care going to places
Critical care is a concept, not a location, which frequently begins with ED intervention and culminates in ICU admission and continued management. Peter Safar ICU care at home (ICAH), transition care, and electronic ICU are the main strategies for the future. Digitisation is a must to improve workflow, efficiency, and outreach to newer territories. Critical care ‘outreach’ teams, in conjunction with noncritical care hospital personnel, could be leveraged as an effective strategy to extend ICU capabilities in and out of the hospital during a disaster. We should see shared resources globally.
Human resources
Critical care experts are the key to quality care in the ICU. ICU professionals are our asset and our responsibility. However, the population of specially trained intensivists and experienced ICU nurses is proportionately declining. The average-age ICU nurse is not replaced fast enough. Critical care nursing is brutally hard work; it’s physically, emotionally, and spiritually grueling.
The challenge is keeping experienced nurses from leaving because they’re burned out. We need to keep their knowledge and experience, possibly by creating new positions where their knowledge experience and accumulated wisdom can be used to benefit the next generations of patients and providers.
As for physicians, fewer are choosing critical care, which will likely lead to significant staffing issues. The number of doctors choosing a career in critical care is leveling off. Part of the problem is an educational system that helps medical students choose a specialty. We need to reemphasise critical care training pathways across all healthcare professionals.
Technology
Technology is there to serve the patient first, but most importantly, to serve the care alliance of patients and practitioners. Sophisticated presentation will evolve in the ICU to provide a safer environment that uses the available HR most efficiently. It won’t save on manpower, but it will greatly increase patient safety. Technology that doesn’t rely on human factors will be used commonly.
We miss things because we don’t notice them. AI/machine learning & automation of systems will push information to us as computerised analysis. This would help critical care preparedness and could be used in disaster settings. The evolution of ICU technology must focus on bridging the gap between limited staff and a growing patient population. Technology should help minimise the gap between adequate care and excellent care.
Digitisation
How do ICU professionals organise themselves and leverage
technology to address this gap and improve the quality of care? One solution to the staffing shortage is electronic ICUs—or eICUs, which allow an intensivist and ICU nurse to monitor and manage part or all of the patient population in their organisation’s ICU from off-site.
Advances in networking are likely to redefine the physical and organisational boundaries of the critical care unit. No longer a self-contained entity, tomorrow’s critical care units are likely to regularly draw on resources—both human and technological—located outside the unit’s physical space. Remote monitoring will help leverage existing manpower.
eICU with smart alerts, physiologic status boards, and color-coded assessments of response to protocolised care may help intensivist on-site manage increasingly busy and acute ICUs. The greatest impact will be to facilitate the transformation of data into information and to highlight factors that are of greatest immediate importance. In addition to maximising medical staff, eICU systems can leverage technical support. We foresee a day shortly when a network of hospitals might centralise its critical care application servers and patient record servers in one location to reduce IT staff overhead, standardise clinical protocols, and automate corporation-wide quality control mechanisms. With an eICU system, cameras, monitors, and communication devices
The infrastructure of critical care needs to be transformed and the focus must pivot to ways that enhance personalised medicine
provide information on each patient, and can even provide treatment recommendations or guidelines.
Role change
ICU care providers will take on more duties as managers of care or at least have that as a big additional responsibility.
ICU providers will go through an evolution like airline pilots did.These days, airline transport pilots don’t spend most of their time flying the plane. There are plenty of autopilots and subsystems that do that. The pilot now spends most of her time managing the system and intervenes as necessary to bring everything into harmony. Sophisticated digitalisation and AI will evolve the ICU to provide a safer environment that uses the available human resources most efficiently.
● Safety: Sophisticated presentation will evolve in the ICU to provide a safer environment that uses the available human resources most efficiently. It won’t save on manpower, but it will greatly increase patient safety. Technology that doesn’t rely on human factors will be used commonly. We miss things because we don’t notice them. Automation of systems that will push information to us as computerised analysis; postulate on that information. This
would help in critical care and could be used in disaster settings as well. The evolution of ICU technology must focus on bridging the gap between limited staff and a growing patient population.
● Surveillance: Surveillance technology can help identify a disease outbreak or other disaster faster than humans. Some hospital systems are using surveillance systems that link across their facilities to find patterns. These systems can be used to find medical errors, but they can also act as bio-disease surveillance systems, which can be used to identify a sudden outbreak.
● The critical care team of the future: We’ll see a reorganisation of physician services into an intensivist team model. “The development we’ve seen over the last 20 years is that outcomes are better with a unit-based special team that manages patients in cooperation with the primary care physician.
● Critical care guidelines: An integral component- Few critical care experts shy away from such buzzwords and phrases as “standardisation of care” regarding ICU practices. Professionals do agree that universal guidelines will be the norm in the future. We’ll see the development of drastically improved
outcomes and reduction in harm through reliable processes. With the development of reliable processes in place; we can see that we will close the gap between intent and actual execution.
Quality improvement care is ripe for integrating clinical practice guidelines. Certain types of interventions are nearly universal in ICUs. Systematic implementation of guidelines will be the difference between an average ICU and a great ICU.
Green ICU
GREEN ICU (GREater Environmental Sustainability in Intensive Care Units) is a multidisciplinary initiative that aims to develop evidence-based guidelines to reduce the environmental footprint of intensive care practice. Nowadays, we need a sustainable approach to our critical patient care that reduces the environmental impact of an ICU.
Global critical care
Critical care is under prioritised. A global call to action is needed to increase equitable access to care and the quality of care provided to critically ill patients. Advocacy at all levels is needed to achieve universal health coverage for critically ill patients. The global variability
in many aspects of critical care will forever remain, yet working to achieve this future vision for critical care organisations will lead to higher-quality care across systems and continents, including more humanistic and more personalised care with fewer errors and better quality, as the goal will always remain to provide the highest quality patient care and outcomes. The area of critical care may be moving more quickly toward the future than other hospital functions because it must do so to continue to work at all. The success of achieving a future of quality care, patient safety, and adequate staffing rests on a different approach with providers and technology. We should learn to work smarter to leverage new technology and the expertise of all other experts in other fields. Prospects for critical care may look questionable now, but solutions are available and the future just might be brighter than expected
References
Crawford AM, Shiferaw AA, Ntambwe P, et al. Global critical care: a call to action.Crit Care. 2023;27(1):28. Published 2023 Jan 20. doi:10.1186/s13054-02204296-3
Esper, A.M., Arabi, Y.M., Cecconi, M.et al.Systematized and efficient: organization of critical care in the future.Crit Care26, 366 (2022).
https://doi.org/10.1186/s13054022-04244-1
MEDTECH
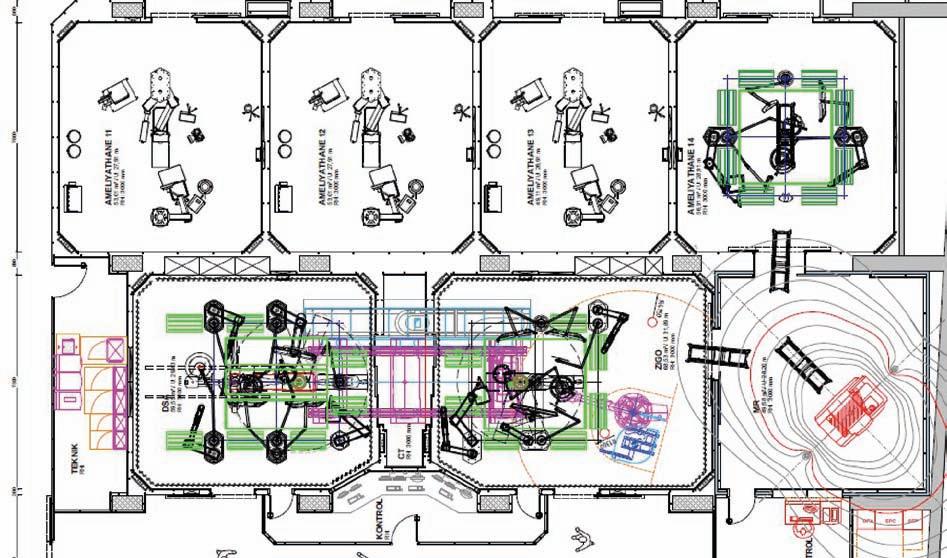
Importance of workflowin operating rooms and hybrid operating rooms
Bhavesh Bhatt, Director,Mediconz International highlights the importance of image guided operating room or hybrid operating room
With the advances in medical science surgeries are becoming lesser and lesser invasive accordingly the Operating Rooms are also changing to reflect this. Today, surgeries involve collaboration among various specialists working on a single patient, creating a demand for advanced operating rooms with Imaging systems , you can call it IGOR, “Image Guided Operating Room” or HOR “Hybrid Operating Room.”
The surgical world is undergoing rapid changes to reflect the advances in medical science. The explosion of knowledge that the advances brought led to minimally invasive surgeries with specialists in various medicine branches providing their expertise. In fact, surgeons nowadays increasingly prefer to perform minimally invasive or open procedures in HOR , which surpass medical disciplines and boundaries while enabling specialists like interventional cardiologists, cardiac surgeons, interventional radiologists, vascular surgeons, urologist, Neuro , Spine , Once and ortho surgeons to collaborate in performing surgeries.
Hospitals nowadays are constructing HORs equipped with X-ray modalities like Cathlab systems, CT scans, 3D C-arms & MRI. This is of benefit to the patients undergoing cardiac, vascular, trauma, Spine , Neuro Surgery and many more. It cannot be underestimated with regard to risk minimisation that it offers.
Workflow is extremely important while designing OR complex and it is highly recommended to consult domain expert right in the beginning
or at least when the first cut draft is ready. Over the years I have had opportunities to study many OR layouts and
surprisingly very few were perfect. Many of them had issues with workflow in change area, Clean and Dirty utility
movement, Staff & patient movement etc... to name a few. It was also observed that too many toilets were planned in the change room areas and in some cases they were planned close to sterile areas. It is always recommended to plan clean and dirty corridors well in advance so that a proper workflow can be designed with lots of natural lights in the operating room / corridors, this helps OR staff remain energetic and active.
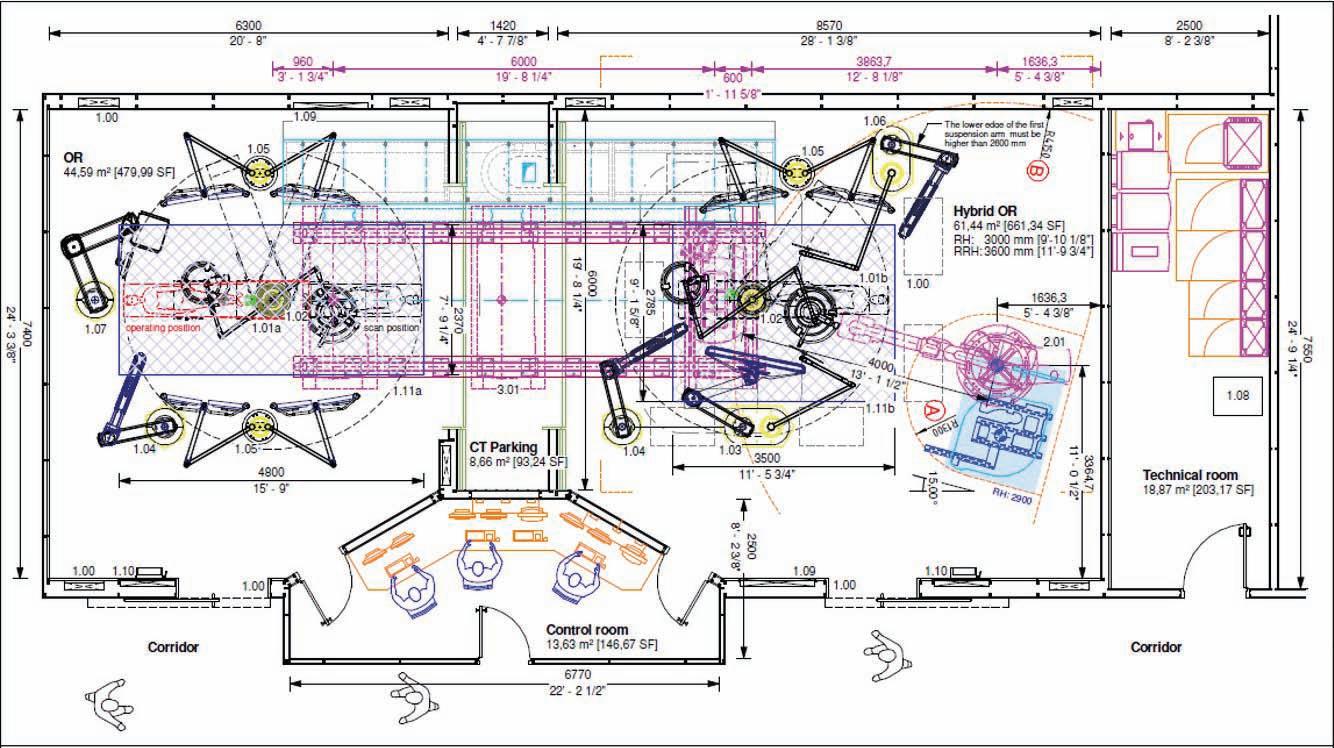
For Hybrid OR it is important to plan the modality well in advance which will help design the area and its workflow well; For example Cath lab type - Ceiling or Floor mounted will need different floor space and so is the height. Not to forget the proximity to technical room has to be planned in such a way that the sterile movement is not affected. For Computed Tomog-
raphy (CT) , it is important to know if it will be a sliding gantry or a mobile solution this will help plan room accordingly. However if hospital is planning a hybrid with Cathlab and a CT together as shown in pic 1, then this needs more attention and lot needs to be planned.
Whereas while planning an MRI Hybrid it is critical that the operating room has to be planned in such a way that the patient transfer is seamless and without any obstructions. In the time to come we can also have a OR complex with all three imaging modalities namely CT , Cathlab & MRI. This workflow is very interesting and can help minimise infection as patient doesn’t have to be moved out of complex as both soft and hard tissue scanning can be done within the OR complex as show in Pic 2.
In the near future we will talk about “Diagnostic Street “concept where we can add Navigation room and Robotics in the OR complex along with above modalities as shown in Pic 2 , Interventional physicians and surgeons can conduct wide range of procedures / treatments and examine their results using imaging modality in the OR complex without any delay.
The high-performance HOR is attributed to its phased and intensive planning and construction. It takes anywhere from 6 to 9 months to build a HOR in an existing setup. The challenge is to combine many individual medical systems to form a single, holistically functioning system.
In both, planning as well as implementation phases, hospitals greatly benefit from our many years of experience from room classification, room concept and configuration, to the viewing concept. We support hospitals, architects and planners with our extensive knowledge and expertise throughout all planning stages. This contributes greatly to the transparency of the project. Using the 3D presentation of the OR, the customer can check the positioning of various devices. Our most important concern is to ensure optimal work processes in the new HOR for all user groups. This is why we place such importance on workflow consulting during the planning phase. Getting everyone involved at an early
stage makes all the difference.
The operating room can only be equipped to optimally cater to everyone’s needs if it is clear from the onset which departments will ultimately make use of the HOR.
The heart of the HOR is the operating table and the imaging modality. The 360-degree radiolucent and flexible operating table turns the HOR into an interdisciplinary OR: the operating table system can be adapted to meet the requirements of cardiology, cardiac, vascular, neuro and orthopaedics surgeries. There are mobile radiolucent tables also available which
can be used for basic hybrid applications too with mobile imaging solutions. For MRI hybrid application Kevlar Board is compatible hence it should be planned, which will be transferred from system OT table to MRI examination table trolley for seamless transfer.
Besides optimal workflows and the technical interaction of all devices, one should also focus on creating an attractive workplace and appealing atmosphere. This involves the use of products that support ergonomic working methods for surgeons and surgical staff. In addition, colors, Nat-
ural lights and wall images are used to create a pleasant and positive working atmosphere.
In the design of HOR, we pay special attention to the integration of sustainable products and future-proof solutions. This is where we opt for the use of flexible wall and ceiling elements always enable quick retrofitting. We offer support in planning and in implementation as well as to the protection of hospital investment who wants to install HORs.
Mediconz International is an ISO certified Company, comprising of professionals with vast experience in multi-
ple fields of medical, engineering and architecture. With expertise in executing number of turnkey modern health care facilities are attributed to competency, knowledge and experience of our core team in the field of Design, Project Management and Execution. With more than 50 years of combined experience in the planning and designing of inter- disciplinary OR workflows and Hybrid ORs working in close collaboration with imaging equipment providers in healthcare sector we deliver the best possible outcomes.
Himanshu Baid,Managing Director,Poly Medicure Ltd highlights that the strategic vision for 2030 focuses on multiple pillars: innovation,manufacturing,regulatory frameworks,talent development, quality and increasing exports,preventive healthcare and cross-industry collaboration
The medical technology sector in India is undergoing a transformative journey, set against the backdrop of a burgeoning healthcare landscape and increasing government focus on fostering innovation. The vision for medtech in India by 2030 envisions a robust, self-reliant ecosystem that not only addresses domestic healthcare needs but also establishes the country as a global hub for medtech manufacturing and innovation. The government's initiatives to promote the medical devices sector in India are commendable and have significant potential to enhance healthcare accessibility and quality. By introducing various schemes and policies, the government is creating a conducive environment for domestic manufacturing, research, and development.
In India, the medical device industry is a rising star that is expanding quickly and has a great deal of potential to become self-sufficient and advance the cause of universal health care. The size of the Indian medical devices market is estimated at $16-17 billion and is expected to grow to $50 billion by 2030 and the sector has been growing steadily at over CAGR of 15 per cent for last 3 years. Thus, a comprehensive policy framework is urgently needed to spur this growth and realise the sector's full potential. The current policy strives to provide a coherent set of focus areas for the coordinated expansion of the sector.
Secondly, because the medical device industry is diverse and multidisciplinary, government laws, skill development programs, and trade promotion efforts are dispersed among multiple departments at both the federal and state levels. The variety of initiatives must be gathered coher-
India’s medtech sector holds enormous potential, owing to the country’s large population,growing middle class,and rising incidence of chronic diseases.The sector is expected to grow exponentially,driven by technological advancements,increasing healthcare expenditure, and government initiatives to make healthcare more accessible and affordable
ently in order to provide the sector with targeted, effective support and facilitation.
Strategic vision for 2030
India’s medtech sector holds enormous potential, owing to
the country’s large population, growing middle class, and rising incidence of chronic dis-
eases. The sector is expected to grow exponentially, driven by technological advancements, increasing healthcare expenditure, and government initiatives to make healthcare more accessible and affordable. The strategic vision for 2030 focuses on multiple pillars: innovation, manufacturing, regulatory frameworks, talent development, quality and increasing exports, preventive healthcare and cross-industry collaboration. These pillars aim to create a medtech ecosystem that is competitive, innovative, and sustainable, both in terms of economic growth and patient care.
Innovation
One of the cornerstones of the vision is fostering innovation and research and development (R&D) in the medtech space. Currently, India lags behind other developed nations in terms of medtech innovation due to a lack of significant investment in R&D, infrastructure, and collaboration between academia and industry. To achieve this, increased investment in R&D, both from the private sector and through public-private partnerships (PPPs) are crucial.
Increasing exports and reducing import dependency
India is already known for its prowess in pharma manufacturing, and there is no reason why the country cannot replicate that success in medtech manufacturing. The goal is to reduce India’s dependency on imports to 50 per cent by 2030, which currently account for over 70 per cent of the country’s medtech needs, by developing a strong domestic manufacturing base.
Increased investment in manufacturing There is a need for increased
investment in medtech manufacturing, focusing on highquality, affordable medical devices that can compete globally. It is required for developing specialised manufacturing clusters across the country, equipped with world-class infrastructure and supported by government incentives. This would not only reduce import dependency but also position India as a global manufacturing hub for medical devices, creating significant employment opportunities in the process.
Embracing a robust regulatoryframework
The New Regulatory Bill, the 2023 Drugs, Medical Devices and Cosmetics Bill aims to revolutionise India's pharmaceutical and medical device sectors. It introduces innovative components, including a risk-based classification system for medical devices, a dedicated regulatory framework for in vitro diagnostic medical devices, the establishment of Central Drugs and Central Medical Devices Authorities, online licensing processes, and stringent penalties for compliance. The bill has received acclaim for its forward-thinking regulation, offering benefits such as enhanced patient safety, innovation in vitro diagnostic medical devices and economic growth.
However, to unlock India's potential as a global medical
device hub, streamlined, robust and transparent regulations are crucial. Currently, India’s regulatory framework for medical devices is seen as fragmented, which can hinder innovation and delay the time-to-market for new products. The regulations can simplify and harmonise processes, reduce regulatory burdens, foster innovation, attract foreign investment, strengthen domestic manufacturing and enhance global competitiveness. The transformative New Drugs, Medical Devices and Cosmetics Bill of 2023 has the potential to reshape the medical device landscape.
Comprehensive talent development strategy
The future of India’s medtech sector hinges on the availability of skilled talent capable of driving innovation and growth. While India has a large pool of engineers and scientists, there is a gap in the availability of specialised talent for the medtech industry. To address this, a comprehensive talent development strategy that includes the establishment of specialised training institutes and the integration of medtechspecific courses into the curricula of engineering and medical schools is required. There is also the need for strengthening industry-academia collaboration to ensure that the skills being imparted are in line with in-
CONTRIBUTOR’S CHECKLIST
● Express Healthcare accepts editorial material for the regular columns and from pre-approved contributors/columnists.
● Express Healthcare has a strict non-tolerance policy towards plagiarism and will blacklist all authors found to have used/referred to previously published material in any form,without giving due credit in the industry-accepted format.
● As per our organisation’s guidelines,we need to keep on record a signed and dated declaration from the author that the article is authored by him/her/them, that it is his/her/their original work,and that all references have been quoted in full where necessary or due acknowledgement has been given.The declaration also needs to state that the article has not been published before and there exist no impediment to our publication.Without this declaration we cannot proceed.
● If the article/column is not an original piece of work, the author/s will bear the onus of taking permission for re-publishing in Express Healthcare.The final decision to carry such republished articles rests with the Editor.
● Express Healthcare’s prime audience is senior management and professionals in the hospital industry. Editorial material addressing this audience would be given preference.
dustry requirements. Furthermore, apprenticeship and internship programs must be created that provide hands-on experience in medtech manufacturing and R&D, thereby bridging the gap between education and employment. This focus on talent development is essential to ensure that India has the workforce needed to sustain the growth of its medtech sector.
Preventive healthcare
By focusing on early detection and prevention of diseases, preventive healthcare reduces the need for costly curative treatments, thereby stimulating demand for medical devices used in screening, diagnosis, and monitoring. This includes devices for routine check-ups, such as blood pressure monitors, glucose meters, and imaging equipment. Additionally, preventive healthcare initiatives can drive innovation in the medical devices sector as manufacturers develop new technologies and solutions to address specific needs.
Cross-sector collaboration
India's potential to be a major player in the global medical devices sector is hindered by the insufficient availability of quality raw material domestically. Just as an example, the country faces challenges in producing steel that meets the stringent quality standards required for
medical applications. To address this gap, effective crossindustry collaboration and alignment among different government ministries are essential. By streamlining regulatory procedures, providing incentives for investment, and improving infrastructure, India can foster a thriving domestic medical devices industry and reduce its reliance on imports.
Enhance ease of doing business
Increased government funding for medtech R&D and innovation, as well as tax incentives for companies that invest in medtech research is essential. Furthermore, to unlock the full potential of India's medtech industry, introducing specific legislation for medical devices can pave the way for robust growth.
Additionally, PPPs can play a crucial role in advancing the medtech sector. PPPs must be created to facilitate the development of medical device parks, research institutes, and training centres. These partnerships can help leverage private sector expertise and investment while ensuring that public health objectives are met.
To boost India’s medtech exports, the implementation of additional export-friendly policies and the development of trade agreements with key international markets is re-
● The articles should cover technology and policy trends and business related discussions.
● Articles by columnists should talk about concepts or trends without being too company or product specific.
● Article length for regular columns: Between 1300 - 1500 words.These should be accompanied by diagrams,illustrations,tables and photographs, wherever relevant.
● We welcome information on new products and services introduced by your organisation for our Products sections.Related photographs and brochures must accompany the information.
● Besides the regular columns,each issue will have a special focus on a specific topic of relevance to the Indian market.You may write to the Editor for more details of the schedule.
● In e-mail communications,avoid large document attachments (above 1MB) as far as possible.
● Articles may be edited for brevity,style,relevance.
● Do specify name,designation,company name, department and e-mail address for feedback,in the article.
● We encourage authors to send a short profile of professional achievements and a recent photograph, preferably in colour,high resolution with a good contrast.
quired. Also, fostering collaboration between various stakeholders, including the government, industry, academia, and healthcare providers, to create a holistic and supportive ecosystem is very much necessary for medtech innovation.
Wayforward
India’s medtech Roadmap 2030 presents an exciting opportunity for the country to emerge as a global leader in medical technology. By focusing on innovation, manufacturing, regulatory reform, and talent development, India can build a self-reliant medtech ecosystem that not only addresses the healthcare needs of its population but also positions the country as a major player in the global medtech industry. India, undoubtedly, has the potential, which now is being backed by a robust and coherent policy regime aimed at streamlining regulatory processes, fostering ease of doing business, adopting global standards, stimulating the development of local manufacturing as well as improved competitiveness for the sector. Now is the time when India, leveraging the government support, Industry participation and country's talent pool, will achieve new heights in terms of manufacturing and accessibility of high-quality medical devices, and set new standards for healthcare innovations globally.
Email your contribution to: viveka.r@expressindia.com viveka.roy3@gmail.com
Editor, Express Healthcare
HEALTHCARE TRACKER
Integrating haematologyand flowcytometrydata :
Asynergistic
approach
Vikram Patil, Deputy Product Manager-Flow Cytometry,Sales and Marketing,Sysmex explains about Sysmex's CyFlow WA,a middleware interface that integrates data from haematology and flow cytometry onto a single screen
In the field of haematopathology, diagnosing complex conditions such as leukemia and lymphoma requires both haematology and flow cytometry data. Haematology, which provides crucial parameters like CBC-DIFF (complete blood count with differential) and blood morphology, offers a foundational understanding of a patient’s health. Flow cytometry, on the other hand, provides detailed insights into specific abnormal cells & subtypes utilising specific marker panels.
Traditionally, haematology data such as CBC-DIFF results are analysed independently from flow cytometry in separate platforms. However, when these data streams are disconnected, clinicians need to cross-refer multiple platforms to manually gather insights and interpret scattered information. This increases manual work, and the risk of diagnostic delays or errors.
The importance of unified data integration
Integrating haematology and flow cytometry data enhances diagnostic precision and reduces the cognitive burden on the clinicians. By combining haematology insights such as WBC counts and blood smear morphology with flow cytometry’s ability to characterise cell surface markers, laboratories can create a more holistic and data-driven patient profile. This integration not only speeds up the diagnostic process but also supports more confident clinical decisions, ultimately leading to improved patient outcomes.
Sysmex’s CyFlowWA: Asolution for data integration
To address this need for streamlined diagnostics, Sysmex has
Integrating haematology and flow cytometry data is an essential & crucial evolution in the field of haematopathology
developed CyFlow WA (Work Area Manager), a middleware interface that integrates data from haematology and flow cytometry onto a single screen. CyFlow WA enables clinicians to view CBC-DIFF, morphology images, and flow cytometry data on a single screen, eliminating the need to toggle between different systems.
CyFlow WA’s bidirectional communication automatically receives panel information for clinical flow cytometry from the LIS, minimising manual data entry. This provides completely comprehensive patient data on
a single screen making it possible to choose flow cytometry panels based on haematology results in real time, offering a truly integrated diagnostic pathway.
Sysmex’s CyFlow WA enables smoother workflows, reduces the burden on lab professionals, and improves diagnostic accuracy, improving patient outcomes in haematological malignancies.
In conclusion, integrating haematology and flow cytometry data is an essential & crucial evolution in the field of haematopathology.
HEALTHCARE TRACKER
Introducing the HDFDialysis Machine SWS-4000 byHemant Surgical
The SWS-4000 stands out for its multi-functional design,offering customised curing modes tailored to meet the unique needs of individual patients
Hemant Surgical Industries Ltd., a leader in the field of dialysis solutions, proudly presents the SWS-4000 Hemodialysis (HDF) machine—a state-of-theart innovation designed to elevate patient care through precision, safety, and reliability. With a rich history of expertise, Hemant Surgical is renowned for its specialised Turnkey Dialysis setup projects across Africa and Asia. Over the past 25 years, the company has successfully installed over 4000 dialysis machines worldwide, reinforcing its position as a trusted name in the healthcare industry.
The SWS-4000 stands out for its multi-functional design, offering customised curing modes tailored to meet the unique needs of individual patients. This feature ensures that treatments are more effective and patient-centric, making dialysis a more comfortable experience. The machine is designed to adapt seamlessly to diverse clinical requirements, ensuring optimal care for every patient.
One of the most impressive features of the SWS-4000 is its Advanced Volume Balance Control System, which enables precise control of ultrafiltration.
Managing fluid removal during dialysis is critical, and this technology ensures it is performed with accuracy, reducing the risks of fluid imbalance and enhancing overall treatment outcomes.
To further enhance patient safety, the SWS-4000 is equipped with a double-stage intoxication filtration system, ensuring that the substitution fluid meets AAMI standards. This guarantees high-quality, contamination-free fluid for each treatment, safeguarding patients from potential complications.
The machine’s reliable sys-
tem is supported by cuttingedge safety features, including pressure detectors, conductivity detectors, air detectors, and blood leakage detectors. These integrated systems ensure constant monitoring and provide a secure treatment environment for patients and clinicians alike. In addition to offering cutting-edge dialysis machines, Hemant Surgical has a dedicated team of 45+ Bio-Medical Engineers stationed across the globe to provide seamless installation and after-sales services. The company has successfully completed numerous Turnkey projects in both
African and Asian countries, and proudly operates its own dialysis centers in Mumbai and Nairobi, Kenya. Hemant Surgical’s vision is to establish a global chain of dialysis centers, expanding its reach and continuing to deliver exceptional renal care solutions worldwide.
For institutions seeking advanced dialysis solutions with a proven track record of success, the SWS-4000 from Hemant Surgical is the ideal choice. Combining innovative technology, patient-centric features, and robust safety standards, the SWS-4000 sets a new benchmark in the dialysis industry.
PessaryRing byAmi Polymer
Atharwa Mishra,Officer,Ami Polymer Pvt Ltd.explains the benefits of Pessary Rings
What is a PessaryRing?
Apessary ring is a flexible, silicone device inserted into the vagina to support the pelvic organs. It primarily used to treat conditions such as pelvic organ prolapse and stress urinary incontinence. Think of it as a supportive brace for your
descends into the vaginal canal due to weakened pelvic muscles.
when the top of the vagina loses support and collapses. Pessary rings can support the vaginal walls and keep them in place.
Cystocele and rectocele
A cystocele is when the bladder prolapses into the
vagina, and a rectocele is when the rectum bulges into the vaginal canal. Pessaries provide the necessary support to alleviate these conditions.
Stress urinary incontinence
Stress urinary incontinence is the unintentional loss of urine during physical activities.
Pessaries can help support the bladder neck and reduce urine leakage.
Benefits of using Pessary Rings
Non-surgical solution
Pessary rings offer a noninvasive alternative to surgery, making them a suitable option for those who prefer or require conservative treatment.
Immediate relief
Once inserted, pessary rings can provide immediate symptom relief, improving the quality of life for many women.
Customisable and reusable
Pessaries come in various sizes and designs, allowing for a customised fit. They are also reusable, making them a cost-effective long-term
solution.
Ami Polymer Opthalmic product?
At Ami Polymer Pvt. Ltd, We are the manufacturer of silicone pessary rings. Our dedication to safety, quality, and performance is evident in every aspect of our product development and manufacturing process.
Call to action
We invite you to explore our range of women Hygiene & Sexual wellness solutions and discover how Ami Polymer Pvt. Ltd can help you create a safer, more efficient environment for your healthcare staff and patients. Contact us today to learn more or discuss your specific needs.
You can choose Ami Polymer with confidence:
Unmatched Safety & Quality:FDA Material Grade Materials
◆ TSE, BSE & BPA Free
◆ Reach Test & USP Class VI
Compliant Biocompatible
◆ 8 Extractable Studies Completed
Rigorous Manufacturing
Standards:
◆ Cleanroom Manufacturing
◆ ISO 9001 & ISO 13485 Certified
Beyond Safety & Quality:Leading-Edge Technology
◆ Unwavering Expertise
◆ Exceptional Customer Service
◆ Leading-Edge Technology
Conclusion In conclusion, As a leading manufacturer of silicone pessary rings, we are dedicated to empowering women with high-quality, non-surgical solutions for pelvic health. Our products offer comfort, durability, and effectiveness, helping women regain their confidence and live active lives. By choosing our pessary rings, healthcare providers can trust in our commitment to quality and innovation, ensuring the best outcomes for their patients. Join us in redefining women's health care and providing solutions that truly make a difference.
REGD.WITH RNI NO.MAHENG/2007/22045,POSTAL REGD.NO.MCS/162/2022 – 24,PUBLISHED ON 8TH EVERY MONTH, POSTED ON 14TH,15TH,16TH EVERY MONTH,POSTED AT MUMBAI PATRIKA CHANNEL SORTING OFFICE,MUMBAI – 400001