14 minute read
ATOPIC DERMATITIS – is it just bad


Products & Procedures under the microscope
With Gaynor Wooldridge
Advertisement
Chair of the Medicines and Procedures Panel (MaPP) of the Institute of Chiropodists and Podiatrists
ATOPIC DERMATITIS – IS IT JUST BAD LUCK?
Introduction
Atopic dermatitis (eczema) is a pruritic, inflammatory skin barrier disease (Koh et al. 2021). It affects approximately 20% of children and 10% of adults in developed countries. An analysis of the 2017 Global Burden of Diseases (Langan et al. 2020), highlighted that atopic dermatitis is the leading contributor of all skin-related disability, affecting approximately 4% of the global population (Laughter et al. 2021). It is a disease that affects people of all ages and ethnicity, and has a significant psycho-social impact on patients and their relatives. In this article, we will look at the historical precursors to atopic dermatitis (AD), and the reported treatments of the time; a brief comparison of atopic dermatitis and psoriasis; current understanding and treatments of AD; and exciting new discoveries and future treatment pathways.
Old disease, new name
Fred Wise (1881-1950) and Marion Sulzberger (1895-1983) are credited with introducing the term ‘atopic dermatitis’ in 1933 (Kramer et al. 2017). Atopy was actually a term created in 1923 by Arthur Coca (1875-1959) and Robert Cooke (1880-1960), when they recognised an association between allergic rhinitis and asthma (Diaz-Cabrera et al. 2021). The definition, based on ‘atopy’, from the Greek word ‘atophos’ meaning ‘second placed’ (Thomsen, 2014), and dermatitis, again Greek in origin, with ‘derma’ meaning skin, and ‘itis’, inflammation.
However, despite this fairly recent introduction into our medical lexicon, the historical precursors of atopic dermatitis can actually be dated to at least 69-140 AD/CE (Bhattachaya et al. 2016). Travelling further back in time, the ancient Greek physician, Hippocrates (c460 BC/BCE - c370 BC/BCE), was to describe the condition of chronically itchy skin. Prevailing thoughts of ‘humors’ guided medical therapy throughout the majority of history, and treating eczema in patients was unpopular (Calvus, 1525). In fact, the oozing often present was thought to be an essential part of the healing process. The term ‘ekzema’ was first used in 543 BC/BCE by the Greek physician Aatius of Amida, and means ‘to boil out’ (Kramer et al. 2017). Ekzema was further described by Girolamo Mercuranali (1572) in his De Morbis Cutaneous, which was the first handbook of dermatological illness at the time. We had to wait until the mid- nineteenth century for Hebra, the first chair of dermatology in Venice, to describe a recurrent, chronic skin disorder which was characterised by intensely pruritic ‘papules and nodules’ on the skin and trunk. He termed this condition ‘constitutional prurigo’, (Hebra et al. 1866), although many other terms were also used during these times, including eczema rubrum, prurigo diatesique and prurigo’ Besnier (1881). Dermatologist: I can’t decide whether I want to specialise in psoriasis or dermatitis. I don’t want to make a rash decision.
Moving into the 20th century, the French dermatologist LuisAnne-Jean Brocq (1903) proposed that atopic dermatitis was linked to nerves, and termed it ‘neurodermatitis’. This, bizarrely, was widely accepted by doctors, and the concept that neurodermatitis was a psychosomatic illness flourished (Duncan, 1959). It became the official name for AD for a few decades, and is still a term widely used in America and Germany.
Experts continue to disagree on the appropriate name for atopic dermatitis, and it is clear that this may not be the term that will ultimately be used. The name and condition will continue to change, together with the development of molecular biology and immunology, and with the advances in the aetiology of the disease (Kramer et al. 2019).
Early treatments (if any!)
Throughout history, individuals have had a myriad of dermatologic conditions. The first documented treatments of AD were found on papyrus in Ancient Egypt. Wright and
Goldman (1979) found that eczema of the head was treated by painting the broken skin with rotting food, mixed with warm fat, fish oil, rotten cereal and breadmeal, covered with bandages and left over night. The idea of introducing potential pathogens into damaged skin would seem to us now, to be fraught with danger!

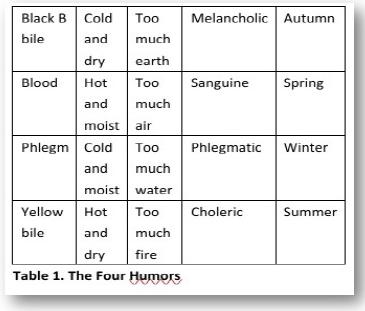
Prior to the 19th century, medical practice was based largely on what the ancient Greeks termed the ‘four humours’. Hippocrates postulated the humoral theory in the 5th Century BC/BCE in his Corpus Hippocraticum. In this vast work, he described multiple dermatologic diseases, with recommendations of spring water, or sea water, baths, and topical application of a fatty substance, as well as treatments using sulphur (Sgontzos et al. 2015). In 1799, when George Washington (first US president) developed epiglottitis, he was such a proponent of the humoral theory that he insisted on being treated with the established practice of blood letting. He lost an estimated 5-7 pints of blood in less than 16 hours; this proved detrimental to his chances of survival, and he died shortly after (Cohen 2012).
Which Humor are you? This is an interactive personality test of the ‘Four Temperamants’, an idea from Ancient Greek medicine. https://openpsychometrics.org/tests/ O4TS/1.php
Coal tar is a thick, dark coloured liquid, which is a by-product from coke making, and coal gas from coal (Hamilton, 2015); it was discovered around 1665 (Roelofzen et al. 2007). In a previous Podiatry Review (October, 2021) we examined the history of phenol, and it’s discoverer, Friedlieb Ferdinand Runge (1794-1867). Runge termed phenol ‘ Karbolsaure’ (coal-oil-acid or carbolic acid). This incredible German analytical chemist, who sadly died in poverty, also became the first person to isolate quinine from cinchona bark; he accidentally found that belladonna extract could cause pupils to dilate (after a chance splash in the eye); isolated caffeine from coffee beans; and invented the first coal tar dye (Anft, 1955). Coal tar began to be used for medical purposes in the early 1800s (Diez and Garcia, 2019), and is still used today. Despite its longstanding clinical use and efficacy, the molecular mechanism is unknown. However, in 2013 Van der Bogaard et al. found that its use in patients with atopic dermatitis completely restored the expression of major skin barrier proteins, including filaggrin.
Atopic Dermatitis vs. Psoriasis
It can be easy to confuse AD and psoriasis. Both are thought to have a similar cause: an immune system that kicks into overdrive and attacks the body. However, this process is different for each condition. (Gardner, 2018).
In psoriasis, immune system chemicals cause the outer layer of skin cells to go through their life cycle in days, rather than a month. This process causes cells to create a super fast layer to build up on the skin, creating a thick coat of red, silvery scales characteristic of plaque psoriasis (GuttmanYassly et al. 2017). People suffering with eczema tend to have overly reactive immune systems when triggered by a substance (internal or external), which causes inflammation. Research has also shown that some people with atopic dermatitis have a mutation gene which leaves skin more vulnerable to dryness, irritants and allergens (Ballard, 2021). More about this fascinating discovery later in the article.
Atopic dermatitis is approximately four times more common than psoriasis, although it is possible to suffer with both conditions (psoriasis-dermatitis). Both atopic dermatitis and psoriasis can affect people of all ages, but AD typically first appears in babies and children, often between the ages of 15-35. Only 1% of babies suffer with psoriasis (Krupka at al. 2020). Children with AD may find that their symptoms go away or improve as they get older, whilst psoriasis tends to be a lifetime condition.
Current Understanding and Treatment Pathways of Atopic Dermatitis
Most of the current treatments for AD target the immune system with the use of corticosteroids, calcineurin inhibitors
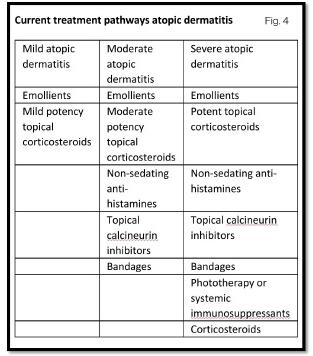
(immunosuppressants) and UVB radiation, with emollients used as an adjuvant to improve skin barrier function. Atopic dermatitis is frequently refractory to topical treatments,and long term treatment with oral immunosuppressive therapy is often required to control the burden of disease, prevent flare-ups and to achieve a better quality of life outcomes (Napolitano et al. 2018).
Standard treatments currently include topical treatments, such as emollients and corticosteroids. If these are not effective, systematic immunosuppressants such as methotrexate, azathioprine and ciclosporin can be added. If there is still no improvement, targeted systemic therapies, such as dupilumab (biologic) and baricitinib (JAK inhibitor) are the next step (Wise, 2022). Gokaimen (2016) determined that atopic dermatitis was actually a random vestige of evolution. This research included the genomes of more than 2,500 people from around the world. The gene at the heart of the research was the filaggrin gene. Filaggrin, a large protein, was discovered in 1977 by Beverley Dale, but its critical role in skin barrier preservation was not understood until 2006 by Professor Irwin McLeen. The relationship with atopic dermatitis was a significant breakthrough in the understanding of eczema pathogenesis and it was found that patients with atopic dermatitis had loss of function mutations in the filaggrin gene (Brown, 2012). Filaggrin has been shown to be a crucial epidermal protein, vital for the formation of the corneocyte, and the generation of intracellular metabolites (Thyssen and Kezic, 2014); this contributes to the hydration and pH of the stratum corneum. (Filaggrin’s first function is to activate the tenofilaments, hence the name: filament aggregating protein). The faulty epidermal differentiation gene results in the reduced production of filaggrin, and more than 50% of people suffering with atopic dermatitis, have been found to have the faulty gene. In our ancestors, this gene helped ‘natural vaccination’ against small pox and cow pox. This gene has persisted, but modern lifestyles with overuse of detergents on our skin, exposes the weakness and causes AD (Gupta et al. 2020).
Atopic dermatitis can also be caused by a proliferation of staphylococcus aureus on the skin. This displaces helpful bacteria and disrupts the skin barrier function. This weak barrier function can trigger an immune system response that causes inflamed skin and other symptoms (George et al. 2019). Clausen et al. (2017) suggested that increased staphylococcus aureus colonisation in patients with AD, as well as filaggrin mutations, show how vital host-microbe interactions are. This research was supported by Koh, Ong and Omman (2021) who stated that skin microbiome is a complex and constantly evolving community that interacts across the skin barrier. There is much research regarding the use of bleach (dilute sodium dichlorite/Dakin) for patients with AD. Bleach baths do seem to improve clinical symptoms, and also restore surface microbiome by eradicating staphylococcus aureus (Maarouf and Shi, 2018, and Silverwood et al. 2021).
Emerging New Treatments and Future Therapeutics
Atopic dermatitis is a common, inflammatory, chronic skin disorder with a constellation of symptoms. Currently, there are many therapies, in various phases of drug development, that specifically target the pathogenesis of AD (Edwards et al. 2018). These include oral, injectable and topical novel therapies, all having a diverse range of mechanistic action (Patel and Strowd, 2017).
AD is frequently refractory to topical treatments, and long term treatment with oral immunosuppressive therapy is often required to control the burden of disease, prevent flare-ups and achieve a better quality of life (Napolitano et al. 2018).
JAK inhibitors (janus kinase inhibitors) target several pathways, instead of a single one (Schuttelaar, 2022). Currently, other medications such as Dupilumab, and other human monoclonal antibodies (biologics) thogenesis of AD, are also in the process of being approved for its management (Tameez etal. 2020).
Several other emerging treatments are expected to play an important role in therapy, and a number of JAK inhibitors (baricitinib, upadacitinib and abrocitinib) have recently been approved by the UK Medicines and Healthcare regulatory agency (MHRA) for atopic dermatitis.
HOW DO JAK INHIBITORS WORK?
• Stop activity and response of one or more JAK enzymes • KAK inhibitors block JAK enzymes to halt auto-immune process • Block messages coming from cytokines (proteins that promote inflammation • JAK inhibitors calm over reactive immune systems
Many inflammatory cytokines are involved in the pathogenesis of atopic dermatitis, and these JAK inhibitors would appear to have the potential for a broad therapeutic benefit within dermatology.
However, more robust studies are needed to assess long-term safety, and also to establish future treatment guidelines. JAK inhibitors certainly seem poised to be an important addition for the future treatment of this complex, chronic, very old, skin disease.
TABLES
Table 1: Table created by Gaynor Wooldridge from information provided by research on the four humours. Photo of dermatitis to patient’s foot with permission granted 01/08/22 Fig 1: Free image from Shutterstock: http://www.shutterstock.com/imagephoto/four-eggs-eggbox-types-temperaments-sanguine-1040693363 Fig 2: Personal clinic image. Permission granted by patient. Atopic dermatitis vs psoriasis. Fig 3: Normal skin vs dermatitis. Shutterstock: Designua ID 275935922. Accessed 09 August 2022 Fig 4: Atopic Dermatitis, current treatment pathways. Created by Gaynor Wooldridge based on information provided by research on current treatments. Fig 5: How do JAK inhibitors work? Created by Gaynor Wooldridge, based on information provided by research on JAK inhibitors.
REFERENCES
Anft, B. 1955. Friedlieb Ferdinand Runge: A forgotten chemist of the nineteenth century. J Chen Edu. 32(11): 566 Ballard, A. 2021. JAK inhibitors are coming and they are the biggest eczema development in years. Available at: https://nationaleczemasociety.org/blog/jakinhibitors-research/ Accessed: 09 August 2022 Besnier, EH. 1892. Première note et observations preliminare pour service d’introduction a l’etude des prurigoa diatesique (dermites Multiforms pruringineises chromiques exacerbates et paroxystiquea du type du prurigo’ de Hebra. Amales de dermatologic et de syphiligraphie. Paris. 3: 634-648 Bhattachaya, T et al. 2016. Historical perspectives on atopic dermatitis: eczema through the ages. Pediatr Dermatol. Bozek, A, Zaja, M and Krupta, N. 2020. Atopic dermatitis and psoriasis as overlapping syndromes. Medicines of Inflammation Vol 2020, Article ID 7527859 4 pages Brocq, LAJ, Besnier, E and Jacquet, L. 1900-1904. La pratique dermatologique: traite de dermatologie appliquée. Paris: Masson et Cie Calvus, MF. 1525. Hippocrates (c460-370BC/BCE) attributed to. Octoginta Volumina. The Hippocratic Corpus translated from Greek into Latin by Calvus (c14401527). Rome: Franciscino Minutius Calvus Clausen, ML et al. 2017. Staphylococcus aureus colonisation in atopic eczema and it’s association with filaggrin gene mutations. Br J Dermatol Cohen, J. 2012. A brief history of bloodletting. History Magazine. May 2012. Dale, BA et al. 1981. Similarities between stratum corneum basic protein and histidine-rich protein 11 from newborn rat epidermis. Biochem Biophys Acta 668, 98-106 Diaz-Carera, NM, Sanchez- Borges, MA and Ledford, DK. 2021. Atopy: a collection of comorbid conditions. The Journal of Allergy and Clinical Immunology in Practice. Vol 9 Iss 11 pp 3862-3866 Diez, MA and Garcia, R. 2019. Coal tar: a by-product in coal making and an essential raw material bin in carbochemistry. Eds: Suarez-Ruiz, I, Diez, MA, Rubiera, F. New Trends in Coal Conversion. Cambridge. Woodland Publishing pp. 439-487 Duncan, MC. 1959. Neurodermatitis -a psychosomatic approach. Med J. 116: 247-54 Edwards, T et al. 2018. Insights into future therapeutics for atopic dermatitis. Expert Opin Pharmacother 19(3): 265-278 Gardner, A. 2018. Key differences between eczema and psoriasis you need to know. https://www.health.com/condition /psoriasis/eczema-psoriasisdifference#:~:text=%E2%80%9C Accessed 3 August 2022 George, SMC et al. 2019. Treatments to reduce infection with the bacteria Staphylococcus aureus in eczema. Cochrane Library Gokaimen, O. 2016. Itchy skin is a random vestige of evolution. Genome Biology and Evolution. Gupta, J et al. 2020. Filaggrin gene mutations with special reference to atopic dermatitis. Curr Treat Options Allergy Guttman-Yassly, E et al. 2017. Atopic dermatitis and psoriasis: two different immune diseases or one spectrum. Curr Opin Immunol 48: 68-73 Hamilton, R. 2015. Coal Tar. Tarascon Pocket Pharmacopoeia. Deluxe Lab Coat Edition. Burlington, Massachusetts. Jones and Bartlett Learning Hebra, FR von. 1866. On diseases of the skin, including the examination. Editor’s: Ferdinand Hebra and Moriz Kaposi. London. The New Sydenham Society. Vol. 3-5 Hippocrates, of Los. c460BC/BCE. Corpus Hippocraticum Koh, LF, Ong, RY, Omman, JE. 2021. Skin mocrobiome of atopic dermatitis. Allergology International Vol 71 Kramer, ON et al. 2019. The history of atopic dermatitis. Clinics in Dermatol Vol 35: Iss 4 pp 344-348 Langan, SM and Irvine, AD. 2020. Atopic dermatitis. The Lancet Vol 396 Iss 10247 pp 345-360 Laughter, MR et al. 2021. The global burden of atopic dermatitis: lessons from the GBD study – 1990 to 2017. Br J Dermatol 184: 304-9 Maarouf, M and Shi, VY. 2018. Bleach for atopic dermatitis. Dermatitis 29(3):120-126 Mercuranali, G. 1572. De Morbis Cutaneous, et omnibus corporis humani extrementis tractatus locupletissi. Venice Napolitano, M et al. 2018. Adult atopic dermatitis: new and emerging therapies. Expert Rev Clin Pharmacol 11(9): 867-878 Patel, N and Strowd, LC. 2017. The future of atopic dermatitis treatment. Ader Exp Med Biol 1027: 185-210 Roelofzen, JH et al. 2007. Coal tar in dermatology. J Dermatolog Treat 18(6): 329-34 Sgontzos, M et al. 2015. Hippocrates on paediatric dermatology. Paediatric Dermatology 32(5): 600-603 Silverwood, RJ et al. 2021. Atopic eczema in adulthood and mortality UK population based cohort study, 1998-2016. The Journal of Allergy and Clinical Immunology Vol 147 Iss 5 pp 1753-1763 Schuttelaar, MLA. 2022. A new avenue for the treatment of chronic hand eczema. Br J Dermatol 197(1): 7-8 Tameez Ud Din, A et al. 2020. Dupilumab for atopic dermatitis. The silver bullet we have been searching for? Cureus 12(4) Thomson, SF. 2014. Atopic dermatitis natural history, diagnosis and treatment. ISRN Allergy 2014: 1-7 Thyssen, JP and Kezic, S. 2014. Causes of epidemal filaggrin reduction and their role in the pathogenesis of atopic dermatitis. Allergy and Clinical Immunology Vol 134 Iss 4 pp 792-799 Van den Boggard, EH. 2013. Coal tar induces AHR-dependent skin barrier repair in atopic dermatitis. The Journal of Clinic Investigation 123(2): 917-927 Wise, J. 2022. NICE recommends three more treatments for atopic dermatitis. BMJ 377 Wright, RC and Goodman, L. 1979. Contact dermatitis: a historical perspective. Int J Dermatol 28(8): 665-8







