
WhyLow-levelRadiationExposureShouldNotBeFeared AlanE.Waltar,1 AbelJ.Gonzalez,2 andLudwigE.Feinendegen3
Abstract Thepurposeofthispaperistoaddressthepublicfear thatisusuallyassociatedwithlow-levelradiationexposuresituations.Itsultimateobjectiveistoprovidepersuasiveassurances toinformedbutskepticalmembersofthepublicthatexposuresituationsinvolvinglow-levelradiationarenottobefeared.Unfortunately,justacquiescingtoanunsupportivepublicfearoflow-level radiationisnotwithoutconsequences.Itiscausingseveredisruptionstothebenefitsthatharnessedradiationcanproduceforthe well-beingofallhumanity.Inthispursuit,thepaperprovidesthe scientificandepistemologicalbasisneededforregulatoryreform byreviewingthehistoryinquantifying,understanding,modeling, andcontrollingradiationexposure,includingsomeoftheevolving contributionsoftheUnitedNationsScientificCommitteeonthe EffectsofAtomicRadiation,theInternationalCommissiononRadiologicalProtection,andthemyriadofinternationalandintergovernmentalorganizationsestablishingradiationsafetystandards.It alsoexploresthevariousinterpretationsofthelinearno-threshold modelandtheinsightsgainedfromradiationpathologists,radiation epidemiologists,radiationbiologists,andradiationprotectionists. Giventhatthelinearno-thresholdmodelissodeeplyimbeddedin currentradiationexposureguidance,despitethelackofasolidscientificbaseontheactuallyprovenradiationeffectsatlow-doses,thepapersuggestsnear-termwaystoimproveregulatoryimplementation andbetterservethepublicbyexcludingand/orexemptingtrivial low-dosesituationsfromtheregulatoryscope.Severalexamplesare givenwheretheunsubstantiatedpublicfearoflow-levelradiation hasresultedincripplingthebeneficialeffectsthatcontrolledradiationofferstoamodernsociety.
HealthPhys.125(3):207–227;2023
Keywords:InternationalCommissiononRadiationProtection (ICRP);linearhypothesis;radiation,low-level;UnitedNationsScientificCommitteeontheEffectsofAtomicRadiation(UNSCEAR); linearhypothesis;LNT
1RetiredProfessorandHead,DepartmentofNuclearEngineering, TexasA&MUniversityandPastPresidentoftheAmericanNuclearSociety;12449IngallsCreekRoad,Peshastin,WA98847; 2NuclearRegulatoryAuthority(Argentina),RepresentativeatUNSCEARandMember oftheIAEACommissionofSafetyStandards;formerlyDirectorofradiationsafetyattheIAEA;Vice-PresidentofIRPAandVice-ChairofICRP; BuenosAires,Argentina; 3NuclearMedicine,Heinrich-HeineUniversity, Dusseldorf,Germany;Lindau,Germany.
Theauthorsdeclarenoconflictsofinterest.
Forcorrespondencecontact:AlanWaltar,12449IngallsCreek Road,Peshastin,WA98847,oratemailat alan.waltar@gmail.com
(Manuscriptaccepted 9 March 2023) 0017-9078/23/0
Copyright©2023HealthPhysicsSociety
DOI:10.1097/HP.0000000000001703
www.health-physics.com
INTRODUCTION
IFPROPERLY harnessed,ionizingradiation(orradiation,inshort) hasyieldedextraordinarybenefitsintheworldofmedicine, agriculture,andgeneralindustry.Ifleftuncontrolled,however, highlevelsofradiationexposurecanleadtoseverehealtheffects.Butthisdoesnotjustifyfearingsituationsinvolvinglow levelsofradiationexposure.Thisdichotomyisusualtomany humanendeavors.Weprotectourselvesagainsthighlevelsof harmfulagents,butontheotherhand,weliveinharmonyand areunconcernedwithlowerlevelsofthesameagents.
However,experiencehasshownthatunpleasantemotionsareoftencausedwithinthepublicatlargeandintheir representativesbythemerementionoftheword “radiation.” Thereappearstobeafeelingofthreatfromradiationatany level evendowntoverylowlevelsofradiationexposure. Inspiteofearlyeffortstoputradiationinperspective(Ander andGonzalez1989),thisphysicalphenomenon,whichis strangeformanypeopleinspiteofitsnaturalism(perhaps becausetheycannottouch,see,orsmellit),hasbecomethe nemesisofmanybeneficialendeavorsforsociety.
Thepurposeofthispaperistoaddressthepublicfear thatisusuallyassociatedwithlow-levelradiationexposure situations.Itsultimateobjectiveisprovidingpersuasiveassurancestoinformedbutskepticalmembersofthepublic thatexposuresituationsinvolvinglow-levelradiationare nottobefeared.
Assuch,wefeelakeystepistoprovidescientificand epistemologicalargumentsforpersuadingourcolleaguesin theradiationprotectioncommunityandtheregulatorswho receivetheiradvicethatthecurrentsituationhascreateda stateoffearoflow-levelradiationexposureandthatthis couldbecausingmoreharmthanbenefit,violatingabasic ethicalprincipleofourprofession.Thismightinturnprovidestepsforchangingthewayregulationsareestablished andimplemented.Suchchanges,properlycommunicated, shouldeasethefearthatpermeatesalargesegmentofthe generalpublic.
Unfortunately,justacquiescingtoanunsupportivepublicfearoflow-levelradiationisnotwithoutconsequences.It iscausingseveredisruptionstothebenefitsthatharnessedradiationcanproduceforthewell-beingofallhumanity.
QUANTIFYINGRADIATION
Usually,physicalphenomenaaffectingourlivesarenot quantifiedwithsuchdetailandcontrolledsoconservatively asradiationexposure.Intheireffortstoprovidesuchcontrol, radiationhealthprofessionalshavedevelopedaratherelaboratebutsomewhatbewilderingsystembasedonaquantitythat isconfusedlytermed[radiation] dose,whichisunderstoodby mostpeopleasaquantityofamedicineordrugtakenatone time.Butforradiation,suchadoseexpressestheamountof energydeliveredbytheemittedradiationtoaunitmassoftissue.Achallengeindefinitionarisesbecausethehumanhealth effectsofradiationexposuredependuponnotonlythedoseincurredbutalsoonthetypeofradiation(i.e.,alpha,beta, gamma,etc.),theenergyoftheradiation,andthesuspected sensitivityoftheparticulartissuebeingexposed.
Toaccountforthesevariables,radiationisusuallynot controlledintermsofeitherthedoseitdeliversortheamount ofradioactivitythatgenerates suchradiation.Rather,itis “measured” intermsofanon-physicalentitythat “weights” thephysicaldose.Stateddifferently,thisphysicalradiation doseismodifiedbysubjectiveweightingfactors(i.e.,factors thatareconjecturedratherthanprovenfacts)thatestimatethe influenceofthetypeofradiationinvolvedintheexposuresituationandtheradiosensitivityofthedifferentorgansinthe bodybeingexposed.Suchweighteddoseistermed “effective dose,” butusuallyitissimplycalled “dose.”
Itistobenotedthatconventionally,theterm “dose” is generallyusedtomeantheamountofsubstanceinteracting withatargettissue.Inradiobiology,dosemeansanamount ofa “substance-equivalent” perunitmass.Thistranslatesinto aratiocausingobservedeffectsintheexposedsystem.In pharmacology,forinstance,doseisamassperbodyweight, whereasinradiationbiology,doseisaweightedratioofenergyabsorbedperexposedunitmass,whichroughlyexpressestheweightedamountoftheenergythatdifferentparts ofthehumanbodyabsorbfromradiationexposure.
Butdifferentlythanforotherbodilyattacks,itisnotthe doseincurred(i.e.,theamountreceivedinagivenperiodof timeorduetoaparticularaction)thatisassessedbutrather theso-called “committeddose.” Thisisthelifetimedoseexpectedtobeincurredasaresultofanexposure.Moreover, controlisnotevenexercisedoversuch “committeddose” butratheroverwhatisconfusedlytermed “dosecommitment.” Thisisdefinedasthetotalcommitteddosesthatwouldeventuallyresultfromanyendeavorinvolvingradiationexposure.
IntherecentCongressoftheInternationalRadiation ProtectionAssociation(IRPA),acritiquewaspresentedincludingthepotentialdifficultieswiththesystemofradiation quantitiesandunits recognizingtheconfusionitgenerates eveninprofessionalaudiences(Gonzalez2021).Suchradiationdefinitioncomplexitiesarelikelyresponsibleformisunderstandingandevenpuzzlementamongmembersofthe publicandare,therefore,partiallyresponsibleforthefear causedbyradiation.
RADIATIONHEALTHEFFECTS
Aswithotheragentsinvolvedinourdailylife,radiationis quantifiedandradiationexposureiscontrolledbecauseofits potentialhealtheffects.Thehealtheffectsofradiationhave beenmeticulouslystudiedforwelloveracentury with farmorein-depthinvestigationsthanforanyotherknown bodilyattack.
Infact,thehealtheffectsofnootheragentarestudiedand agreeduponatthehighestinternationalandintergovernmental levelasisthecaseforradiationhealtheffects.TheinternationalintergovernmentalorganizationchargedwiththeestimationofradiationhealtheffectsistheUnitedNationsScientific CommitteeontheEffectsofAtomicRadiation(UNSCEAR), whichreportsitsestimatesannuallytotheUnitedNations GeneralAssembly(UNGA)ofthe194countriesthatare membersoftheUnitedNations.UNSCEARwasestablished bytheUnitedNationsin1955withthemandatetoassessand reportlevelsandeffectsofexposuretoionizingradiation (UN1955).Governmentsandorganizationsthroughoutthe worldrelyonUNSCEAR´sestimatesasthescientificbasis forevaluatingradiationriskandforestablishingprotective measures.Nootheragentsaffectingpeoplehavethebenefit ofasimilarlevelofscientificsupport.
Asaresult,theradiationhealtheffectsthatshouldbeof concernforsocietyarewellknown.Itisundisputablethat exposuretohighlevelsofradiationdose,deliveredatrelatively highlevelsofchangingdoserates,causeharmfulacuteeffects tothehumanbody.Thesehealtheffectsareobservableanddiagnosableinindividualsexposedtosuchhighdosesandcan beunequivocallyattestedbyaradiationpathologistasbeing attributabletoradiationexposure.Theindividualsexposedto suchhighdosesexperiencetissuereactions(oftenreferredto as “deterministic” effects,becauseabovecertainlevelsofdose, theseeffectsare “determined” tooccur)forwhichdifferential pathologicaldiagnosisandattestationareachievablethateliminatepossiblealternativecauses.Theoccurrenceofsuchadeterministiceffectisuncommoninpractice.Somedeterministic effectshavebeensufferedbyworkersasaresultofhighradiationexposuresinseriousaccidents;someothersoccurredin patientsduetotheerroneousadministrationofradiationdose inradiotherapeutictreatmentsandininterventionalradiology. Radiationsafetymeasuresareundertakentopreventsuchexposuresand,asaresult,suchadverseeffectsareexceedinglyrare, giventheusualsafetyendeavorsinvolvingradiationexposure.
Belowcertainthresholdhighdoselevels,suchacuteradiationhealtheffectsthatcanbediagnosedinindividuals andattributedtotheradiationexposuredonotoccur.However,atmodestlyhighandmediumdoselevels,somedelayedlimitedincreasesinthebackgroundincidenceofother healtheffectshavebeenobserved,suchasmalignanciesthat havebeenassociatedwithsignificantradiationexposure.These effectsoccurrandomlyandthereforearetermed “stochastic”
(fromtheGreekstokhastikós, “aimat,guess”),meaninghavingarandomprobabilitydistributionorpatternthatcanbeanalyzedstatisticallyinacohortofexposedpeople.Potentially radiation-induciblemalignanciesareindistinguishablefrom genericbackgroundmalignancies,whicharerathercommon (aroundaquarteroftheworldpopulationsufferamalignancy duringtheirlife),andtherefore:
• Theycannotbeunequivocallyattributedtoradiationexposureinanexposedindividualbecauseradiationexposureis nottheonlypossiblecauseoftheiroccurrence;and
• Theirincidenceinacohortofexposedpeopleisextremely difficulttodetectatmediumdosesandimpossibletoobserveatlowdosesbecauseofthepresenceofahighbackgroundincidence.
Itshouldbenotedthatthereareatpresentnobiomarkers ofmalignanciesthatarespecifictoradiationexposure.Evenif thesebiomarkerswerediscovered,theywouldmostprobably beunabletodistinguishpotentialeffectsfromhuman-maderadiationexposuresvis-à-visbackgroundexposure,whichis usuallyhigherthanthatcausedbyhumanactivities.
Thepresenceofsuch “stochasticeffects” hasbeenidentifiedthroughoutepidemiologicalstudiesoflargecohortsof peoplewhohaveincurredhighandmediumdoses,delivered atrelativelyhighandhighlychangingdoserates notablythe survivorsofthenuclearbombingoftheJapanesecitiesof HiroshimaandNagasaki.Theirincidenceisrelativelylow, butitisstatisticallymeasurableifthecohortofexposedpopulationislargeandtheirradiationdosesarerelativelyhigh.
Insummary,
• Attributionofstochasticeffectstoexposuresituationsis notpossibleinindividuals;
• Attributionisonlyachievablecollectivelyforalargecohortexposedtorelativelyhighdoses,anditisusually expressedasanincreaseinthebackgroundincidenceof thestochasticeffectsinthatcohort;but
• Suchcollectiveattributionis notachievableforlow-dose radiationexposuresituations;namely,forthosesituations involvingexposurelevelstypicaloftheglobalrangeofradiationbackgroundlevels.(Theselevelsarearoundthose usuallyestablishedaslimitsbyregulatoryauthoritiesand ininternationalstandards.)
UNSCEARhasissuedareportthatrecapitulatesand clarifiestheepistemologyaswellasthescientificknowledgeforattributingobservedhealtheffectsinindividuals andpopulationstoradiationexposureanddistinguishesthat frominferringconjecturalrisks(i.e.,aneducatedguess,inferredfromincompleteevidence)toindividualsandpopulationsfromanexposure(UNSCEAR2012a).Itconcluded thatincreasesintheincidenceofhealtheffectsinpopulations cannotbeattributedreliablytochronicexposuretoradiation
atsuchlowlevels.UNGAhasendorsedthisreport (UN2012).
Simplyput,inthenormalradiationexposuresituations thatarecontrolledbyregulators,theoccurrenceofradiation healtheffectscannotbeattested,eitherindividuallyorcollectively. “Risks” canbeonlysubjectivelyinferred.Effects, ifany,wouldbeunobservableduetobothepistemicand statisticallimitations.Whereasthereremainsconsiderable controversyregardingtheactualmechanisticbiologicalresponsestolow-doseexposure,theultimateeffectsonhealth (ifany)andthesubjectivelyinferredriskwouldbesosmall thattherewouldbenoreasontoharboranyfear.
DEVELOPINGTHERADIATION PROTECTIONPARADIGM
Theradiationprotectionparadigm,ormodel,usedfor controllingradiationexposureisgloballyaccepted.Basedon thisparadigm,auniqueinternationalandintergovernmental systemofradiationprotectionstandardsisbeingestablished inco-sponsorshipbyallrelevantorganizationswithintheUnited Nationssystem.Asimilarapproachdoesnotexistforany otheragentaffectingpublicsafety.
Suchinternationalandintergovernmentalfocus-in-depth onradiationhealtheffects,alongwiththeassociateddevelopmentofasophisticatedsystemofsafetystandards,should havebeenareasonforreassuringthepublicthatradiationis verywellunderstoodandproperlycontrolledforpublicprotection.Unfortunately,suchanextensivefocus evenonlow radiationdoseswherenodetrimentaleffectshaveeverbeen seen maybehavingtheoppositeeffect.
Fromahistoricalperspective,assoonasxraysandradioactivitywerediscoveredbytheendofthenineteenthcentury,thenewprofessionalcommunitiesofradiologistsbecameawareofthedetrimentaleffectsofhigh-levelradiation exposure.Theyrealizedtheneedforaparadigmormodelfor theprotectionofthemselves.In1928,afewdecadesafter thesediscoveries,theInternationalX-rayandRadiumProtectionCommitteewascreatedbythe1928SecondCongress ofRadiologyinStockholm.ThisCommitteewouldeventuallyevolveintotoday’sInternationalCommissiononRadiologicalProtection(ICRP)(Lindell1996;ClarkeandValentin 2008).ICRPisanon-governmentalinternationalcharitythat providesrecommendationsonradiationprotectiontoprofessionalsusingradiationandto agenciesresponsibleforregulatingtheuseofradiation.
TheICRPactivitiesgeneratedtheprofessionofradiation-protectionists.Thisisalargecommunityofspecialists whoareinternationallygroupedundertheIRPA.Their workisgovernedbythreeprinciplesdevelopedbytheICRP sincethemid-1970s,whichhavesinceevolvedintothecurrentlyrecommendedparadigm(ICRP2007a).Theseare basedonfoundedethicaldoctrines(Gonzalez2011a;ICRP
2018):namely,thejustificationofactionsthatresultin changesoftheradiationexposuresituation;theoptimization ofradiationprotectionbyselectingthebestprotectionoptionsundertheprevailingcircumstances;andthelimitation ofthecommittedindividualdoses.Afourthprincipleonprotectionofthefutureandtheenvironmentwasimplicitin ICRPrecommendations,butitwasspecificallyaddedby theintergovernmentalinternationalorganizationsandreads asfollows: “Peopleandtheenvironment,presentandfuture, mustbeprotectedagainstradiationrisks” (IAEA2006).This universalparadigmwaselaboratedoveranumberofyears, becomingdefactouniversalaroundthe1990s(ICRP 1991).Itiscommensuratewiththe “precautionaryprinciple” recommendedbytheUnitedNationsEducational,Scientific andCulturalOrganization(WC2005).
Theinternationalandintergovernmentalradiationsafety standardsbasedontheICRPparadigmareestablishedincollaborationwiththeEuropeanCommission(EC),theFood andAgricultureOrganizationoftheUnitedNations(FAO), theInternationalAtomicEnergyAgency(IAEA),theInternationalCommissionofRadiationUnitsandMeasurements (ICRU),UnitoftheInternationalLabourOrganization(ILO), theOrganizationforEconomicCo-operationandDevelopmentNuclearEnergyAgency(OECD/NEA),thePan AmericanHealthOrganization(PAHO),theUnitedNations EnvironmentProgramme(UNEP),andtheWorldHealth Organization(WHO),allundertheaegisoftheIAEAthat issuesthestandards.Thefirststandardswereissuedin1962 (IAEA1962).Theywereverymuchimprovedattheendof lastcentury(IAEA1996a),andtheyhavebeenupdatedrecently(IAEA2014).
intherisk(i.e.,probability)ofincurringeffectsattributable toradiation.
TheICRPparadigmwasinitiallydevelopedtobesuitableforpracticaloperationalprotectionforoccupationalexposuresituationswhereinternationallegallybindingobligationsforlabormaybeinvolved(ILO1980).
InICRP’songoingeffortstoimprovetheirguidanceinresponsetoincreasingscientificinput,aformalquantitativeuncertaintyanalysishasbeenusedtocombinetheuncertaincomponentsofestimatingthechanceofincurringradiation-related malignancieswithandwithoutallowingfortheuncertain possibilityofauniversallow-dosethreshold.Whereasthe existenceofsuchalow-dosethresholdintherisk-doserelationshipisnotseenbyICRPasunlikelyforradiation-related cancersofcertaintissues(ICRP2005),itconcludedthatthe evidencedoesnotfavortheexistenceofauniversalriskthreshold.However,bothUNSCEAR(UNSCEAR2012a)and ICRPconsideredthatsucheffectsinthislow-doseregionbe referredtoasonlynotionaleffects.
Onsuchbasis,aso-called “detriment-adjustednominal probability” perunitdosecoefficientwasdevelopedby ICRP,thevaluebeingaround5%Sv 1 ofdose.Thus,dose restrictionsforradiationprotectionpurposesarecurrently implicitlyrecommendedonthebasisofariskcoefficient of0.005%mSv 1 (athousandthofaSievertistermed millisievertormSv).Itistobenotedthatwhile5%Sv 1 is mathematicallyequivalentto0.005%mSv 1,thesetwofactors areepistemologicallyverydifferent.Thefirstisbasedonmeasureddataandthesecondonconjecturalexperts’ judgments.
THECURRENTPARADIGM
TheICRPparadigmiscurrentlyusedworldwide.Itimpliesaconservativeassumption:thattheprovenriskofradiationathighdosescanbeconjecturedforlowdosesaswell, despitealackofdirectevidencesupportingsuchaconjecture andinspiteofaUNSCEARpronouncementthathealtheffects atsuchlowdosescannotbeattributed(seelastparagraph under “Radioepidemiologists” inthesectiontitled “The LinearNo-ThresholdRegulatoryApproach”).
TheICRPpurportstobeawarethattherearerecognizedexceptionstosuchanassumptionembeddedintheir paradigmbutstilljudgesthatforthepurposesofradiation protectioninthedoserangebelowabout100mSv,itisplausibletoassumethattheincidenceofdetrimentaleffectsmay riseindirectproportiontoanincreaseinthedoseintherelevantorgansandtissues.Therefore,theparadigmrecommendedbytheICRPisbasedupontheassumptionthatat anydose,includingdosesbelowabout100mSv,agivenincrementindosewillproduceadirectlyproportionateincrement
Itiscrucialtoemphasizethisimportantdifference.This paradigmisbasedonepidemiologicalfactualdatausually obtainedfromexposuresituationsinvolvinghighdoses,high dose-rate,andinmanycaseslargevariationsinthedose-rate change,andwhereanepidemicofattributableradiationeffectsisevidentandscientificallyquantifiablebyprofessional radioepidemiologists.ThiscouldbedonewellwiththecohortoftheHiroshimaandNagasakibombingsurvivorsand withthechildrenaroundChernobylcontaminatedwithhigh levelsofradioiodineviamilkingestion,justtoshowtwoexampleswhereanepidemicofradiationeffectswassuffered. Forsuchwhole-bodyradiationexposures,theprobabilityof someoneinthecohortdevelopinganattributablemalignancy isconsideredtobearound10 2 Sv 1 ofeffectivedoseincurred(basedonnothresholdbutincludingvariationswith sex,conditionsofexposure,etc.)(IAEA2014;ICRP2007a).
Butacritiquetothiscoefficientisthatexpressingit withthequantityeffectivedoseandtheunitSievertisequivocalbecausethisquantityandthisunitweredefinedforlow doses.Anevenmoreseriousproblemarisesduetothescientificdatabeingaccumulatedfromsituationswheretherewas anepidemicofradiationeffectsbeingextrapolatedtoradiationexposuresituationswherethereisnoobviousepidemic,
www.health-physics.com
thedosesarelow,thedoserateislow,andthechangeinthe doserateisverylow.
Theparadigmthenconjecturesthatfactualepidemiologicaldatasupportingtheriskof10 2 Sv 1 areapplicable tolow-radiationdose,lowdose-rate,lowchangesindoserate,andsituationsimposinga detriment-adjustednominal riskcoefficient of10 5mSv 1.Theequation10 2 Sv 1 =10 5mSv 1 isatthecoreofaconceptualproblemthatthispaperaimsto underline:whereasthisequationismathematicallycoherent,itcanbestronglyarguedthatitisepistemologicallyincoherent.Theleftrepresentsaprovenfact;namely,atruth demonstratedbyevidence,whiletherightrepresentsaninferredconjecture;namely,anopinionorconclusionbased onincompleteinformation.
Nevertheless,ontheICRPbasisoutlinedabove,atheoreticaldose-responserelationshiphasbeensynthesizedby theUnitedNationsEnvironmentalProgramme(UNEP 2016)asinthegraphshowninFig.1.
Thedosesareexpressedas:
•“Highdoses” (afewthousandsofmSv);
•“Moderatedoses” (afewhundredsofmSv);
•“Lowdoses” (afewtensofmSv);and
•“Verylowdoses” (afewmSv).
• Itshouldbenotedthattheglobalaveragenaturalbackgrounddoseis2.4mSvy 1 (UNSCEAR2008c).Typical highbackgroundvaluescouldbearound10mSvy 1,and veryhighnaturalbackgroundvalueshavebeenfoundina fewareasoftheworldwheretheyareevenwellabove 100mSvy 1 (UNSCEAR2008c).
• Theprobabilitiesareexpressedinpercentagesbetween 0%and100%,where:
• 100%correspondstothecertaintythattheeffectwilloccur;and
• 0%correspondstothecertaintythattheeffectwillnotoccur.
Ithastobenotedthattheprobabilitiesareoftwo distinguishabletypes:
• Frequentistprobabilities,whichareinthehigh-dosearea, arebasedonevidence;namely,onthetruthfulandverifiableexistenceofanincreaseinthefrequencyofradiation healtheffectsinacohortofexposedpeopleandaredefinedasthelimitoftherelativefrequencyofincidence oftheeffectinaseriesofcertifiableepidemiologicalstudiesonsuchcohorts;and
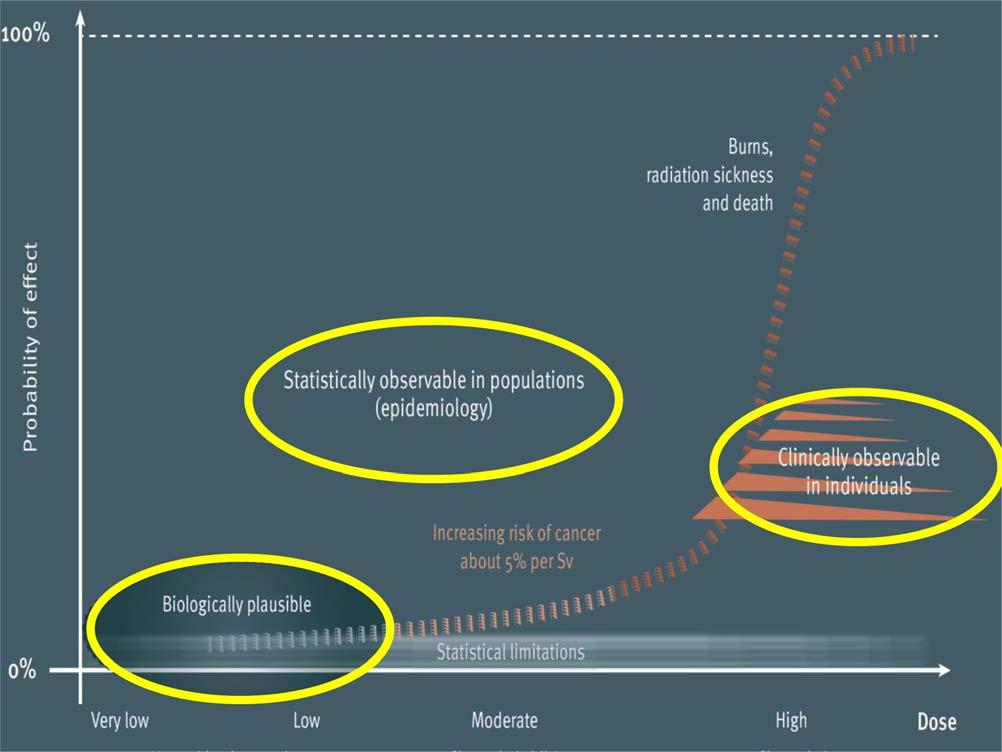
• Subjectiveprobabilities(sometimesalsoconfusedlytermed “Bayesian”),whichareconjecturedforthelow-dosearea, expressedasapossibleexpectationthatradiationhealtheffectsmightoccur,andarequantifiedbyapersonalbeliefor expert’sjudgement;thatis,notnecessarilysubstantiatedby thefrequencyorpropensitythattheeffectsactuallyoccurat suchlevelsofdose.
Bothfrequentistandsubjectiveprobabilitiesaremathematicallycompatiblebutepistemologicallyverydifferent: thefirstisbasedonfactualevidence,andthesecondis basedonsubjectiveconjectures(i.e.,extrapolationsthat lackexperimentalevidence).
Wefurthernotetheimportanceofdistinguishingbetweenthefollowingfactors:
• Verifiedobservationsofhealtheffectsinexposedindividualsandpopulations,whichallowtheiroccurrence tobeattestedbyqualifiedprofessionalsand,therefore, sucheffectstobeunambiguouslyattributedtotheexposuresituationsthatgeneratedthem;and
• Theoreticalprojectionsofhealtheffects(markedasbiologicallyplausibleinFig.1),forwhichoccurrenceisfeasible butnotverifiable;namely,thoseprojectionsallowingonly someconjecturalinferenceofrisks.
Asindicatedbefore,giventhecurrentstateofknowledge, radiationhealtheffectsinindividualsexposedtoradiationcan onlybeattributedwithconfidenceiftheywerediagnosedand theiroccurrenceattestedbyaradiopathologicalspecialist.These deterministiceffectsareusuallyacuteandoccurearlyinindividualsexposedtohighdosesofradiation.Theydonotoccur unlessthedoseexceedsacertainhighthresholdvalue.
Inthelow-andmedium-doseregions,thereiscurrently nofactualwaytoattributeradiationhealtheffectstoaspecificindividualwhoispartofanexposedcohortbecause, forthetimebeing,therearenobiomarkersthatallowthat determination.Notwithstanding,collectiveincreasesinthe backgroundincidenceofhealtheffectsassociatedwithradiationexposurecanbedeterminedasaresultofepidemiologicalstudies.But,asemphasizedbefore,statisticaland epistemicuncertaintiesmakeanyfactualdeterminationof suchdamageunfeasiblewhenthedosesarelow.Itisonly throughradiationbiologythatsomemechanisticinsightis
possible.Researchoverthepastcoupledecadeswithinthe radiobiologycommunityhasprovidednewinsightsregardingtheexistenceofhealtheffectsatlowdoses,including claimsondetrimental,beneficial,ornoeffects.Additionalresearchislikelynecessarybeforesuchfindingscanachievethe reproducibilityandreliabilityrequiredtoincludethecomplexitiesnecessaryindevelopingauniversallyacceptedradiobiologicalmodelforevaluatingtheultimatehealtheffectsoflow-doseradiationexposure.
Thissituationhasresultedinadilemmaforregulators duringtheimplementationstage.Therandomnatureofstochasticeffects,alongwiththeparadigmrecommendedby ICRPandestablishedininternationalandintergovernmentalsafetystandards,makeitimpossibletoderiveacleardistinctionbetween “safe” and “dangerous.” Thishascreated difficultiesinexplainingthecontrolofradiationexposures, howeversmalltheymaybe,andhaslikelybeenasignificant causeofthepublicfearofradiation.Themajorimplication oftheICRPparadigmandoftheconsequentinternational andintergovernmentalsafetystandardsisthatsomeriskis assumed notwithstandingtheclearevidencethatfactual healtheffectsfromlowradiationdoselevelshavebeen conjecturedbutnotproveninpeople.
DOSERATEANDDOSE-RATECHANGE
Theradiationprotectionparadigmanditsderivedsafety standardsarebasedonthequantitydose,incurredorcommittedoveraperiodoftime,usually1y.However,oneareathat hasreceivedlittlefocustodateistheinfluenceofboththe doserateandtherateofchangeofthedoserate(namely,of thefirstandsecondtime-derivativesofdose)ontheultimate healtheffectsofradiationexposure,and,therefore,onthe protectionparadigmanditsderivedstandards.Thedoserate
seemstobecertainlyrelevant,andtherateofchangeofdose ratemayberelevantaswell,buttheinformationavailableon thelatterisminimal,althoughsomeexperimentalevidence onitsinfluenceexists(Brehwensetal.2010).
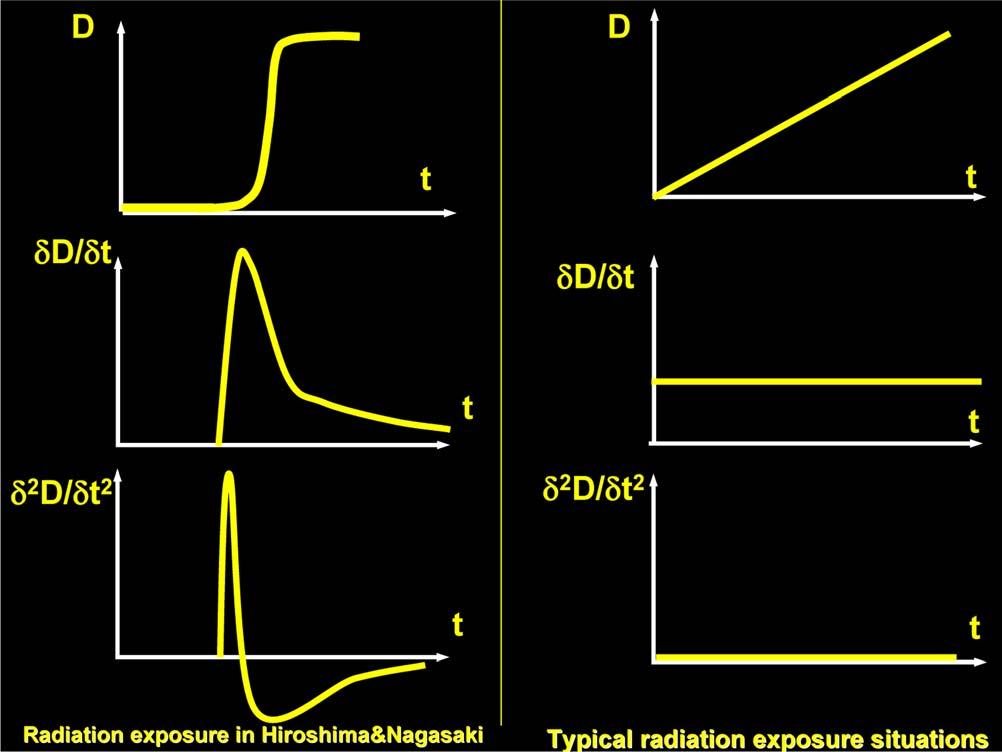
Muchofourdatabaseforhighradiationdosecomes fromtheatomicexplosionsinJapan,anditisabundantly clearthatnotonlythedosebutalsothedoserateandtherate ofchangeofthedoserateforthosesituationswasenormous. However,inmostradiationexposuresituations,thedose,the doserate,andthedose-ratevariationarelow,andthustherate ofchangeofdoserateisbasically zero.Fig.2illustratesthese importantdifferences.
Oneofthefewexposuresituationsthatfeatureschanges inthedoserateistheexposureofaircrewandpassengersto cosmicraysduringsomeminutesfollowingdepartureand beforelanding,whereboththedoserateandtherateof changeofdoseratevary.Butthechangeisprotractedover timeand,furthermore,theavailableepidemiologicaldata forthesecohortsisminimalforestimatinghealtheffects. Hence,weremainopentolearningmoreabouthowthis mayhavefactoredintoourunderstandingoftheactualhealth effectsofionizingradiationatlowdoses.
ATTRIBUTIONVS.INFERENCE
Fromthediscussionabove,itcanbeconcludedthatthere arecurrentlytwodomainsinthedose-effectsrelationship,namely:
• Adomainaboveacertaindoserange,inthemoderateand highdosearea,whereeitherpathologicaldiagnosisorepidemiologicalevidencecanbegatheredinordertoattributetoradiationeitherdeterministiceffectsinindividuals orstochasticeffectsincohortsofexposedpeople;and
• Adomainbelowthisrangewherethereisbiologicalinformationsuggestingthatradiation healtheffectsmightbeplausibleandthatariskcouldbesubjectivelyinferred,e.g.,for regulatorypurposes.Inthislowandverylowdomain,the risksinthecurrentregulatoryframeworkaregenerally inferredbytheexpertjudgmentofradio-protectionists.
Unfortunately,theattributionoffactualeffectsoflow-level radiationexposure(usuallytermedepistemology)isfartoo oftenbasedonconjecturedestimates;namely,opinionsor conclusionsinferredfromincompleteinformation.Thisisa seriousproblem.Understanding thatsuchriskisconjectural iscrucialforthedebateontheperceptionoflowradiation
4GonzalezAJ.Attributionsofhealtheffectstoradiationvis-à-visinference ofradiationrisk:ICRPrecommendationsandUNSCEARreporting.In: InternationalJointConferenceRadio2017.VCongressoBrasileirode ProteçãoRadiológica,VICongressodeProteçãoContraRadiaçõesde PaísesdeLínguaPortuguesaeVIICongressoInternacionaldeRadioproteção Industrial.OrganizadopelaSociedadeBrasileiradeProteçãoRadiológicaem cooperaçãocomaAgênciaInternacionaldeEnergiaAtômica,Sociedade PortuguesadeProteçãocontraRadiaçãoeABENDI,CidadedeGoiânia, 25
29September2017.
Fig.2. Ontheleftthefigurepresentstheidealizedtimevariationofdose (D),doserate(dD/dt)andchangeofdoserate(d2D/dt2)causedbytheexplosionsinHiroshimaandNagasaki;ontherightthesamevariablesare presentedforatypicalradiationexposuresituation.dosesbecausethishasnotbeenexplainedtomembersofthe publicandtheirrepresentativesinpositionsofauthority.The epistemologicallimitsaroundtheradiationsciences,which areessentialforclarifyingtheradiationprotectionparadigm, havebeenamplydebatedintheliterature(Gonzalez2011b, 2014aandbWielandandGonzalez2018)4 andrecently havebeenaddressedbytheIAEA(IAEA2022a).
STUDYINGRADIATIONEFFECTS
Therearefourprimaryprofessionalspecialtiesfocused onstudyingradiationhealtheffects:
• Radiation-pathologists.Expertswhoareabletodiagnose,attestandattributetoparticularexposuresituations theendresultofradiation-induceddiseases inexposed individuals.Theseexpertsdiagnoseonthebasisoftheir professionalexperienceandalsousinglaboratorysamplesofbodytissuefordiagnosticorforensicpurposes. Theirfieldofcompetenceandpossibilityofdiagnosis, attestation,andattributionarelimitedtodeterministiceffects,andthereforeonlytohighdoses;
• Radiation-epidemiologists. Expertswhousemedical statistics(specificallythestatisticsofepidemics)toestimatetheprevalenceofhealtheffects,suchasstochastic malignancies,thatcouldbeassociatedtoradiationin exposedcohortsofpeople(notinindividuals).Sincethese effectsusuallyhavearelativelyhighbackgroundincidence,epidemiologistsaimatquantifyingincreasesin suchincidenceinacohortfollowingtheirradiationexposure.Bothepistemicandstatisticallimitationsrestrictthe possibilitiesofepidemiologicalestimatesofstochasticradiationeffectstomediumandhighdosesincurredbycohortsof people.However,epidemiologists’ competenceforestimationandattestationshouldinprincipleberestrictedtosituationswherethereisanepidemicinthecohort,namelywhere changesintheincidenceofeffectscanbeobservedandmeasured(asitwasthecaseintheHiroshimaandNagasakicohort).Alas,manyradiationepidemiologistshaveextended theirestimatestothelow-doseregionbyconjecturingthat thesameepidemicsthattheycanobserveandquantify athighdosesalsooccuratlowdoses–despitethatsuch anepidemiccannotbeseenbutonlyconjectured;
• Radiation-biologists.Expertswhofocusonthemechanisticbiologicalchangesattributedtoradiationexposure (e.g.,evaluatingtheprogressionofmolecularchanges causedbyradiationupthroughcells,tissue,andorgans). Theycanprovidescientificinsighttothemechanismsof inductionofradiationhealtheffects,andtheyarealsoable toattesttheoccurrenceofradiationexposureinindividualsbyusingbiologicalindicators.However,theycannot yetreliablyattesttotheoccurrenceofultimatehealtheffectsineitherexposedindividualsorincohorts;and
• Radiation-protectionists.Expertsassociatedwithconjecturingandinferringradiationrisksonthebasisoftheinformationprovidedbyradiation-pathologists,epidemiologists,and biologists,inordertoprovideguidancefortheprotectionof peopleandtheenvironmentagainstexposuretoradiation.
Afterincludingasummaryofwhatismeantbythe term “risk,” thisarticlewillthenfocusonsomeofthekey issuesrelatedtotheabovedisciplines.Itisnotedthatitis uncommonthatspecialistsinthesefourverydifferentdisciplinesdirectlyinteractwithanopeneartounderstandthe fullcomplexityoftheeffectsoflow-levelradiation.Asaresult, thelackofconvergenceintheirworkhasledtosomeconfusionand,understandably,haslikelybecomeanotherelement leadingtothecurrentunnecessarypublicfearoflow-levelradiation.Amongseveralattemptstobringthesedisciplinestogether,theAmericanNuclearSocietyjoinedwiththeHealth PhysicsSocietyinsponsoringaconferencein2018(Health Physics2020)tobringtogetherkeyinternationalspecialistsinthesefour(plusrelated)disciplines.Asummaryof theconferenceoutcomeisreferenced(Feinendegen2020).
RADIATIONRISK
Theword “risk” canmeanmanydifferentthingstomany differentpeople,includingprofessionals.Followingisashort overviewofthisconceptinrelationtoradiation,whichhasbeen amplydiscussedattheinternationallevel(Gonzalez2019).
Fortheprofessionalcommunity, riskisformallydefined ininternationalsafetystandards(IAEA2007)as,alternately:
• Theprobabilityofaspecifiedhealtheffectoccurringina personorgroupasaresultofexposuretoradiation;
• Themathematicalmean(expectationvalue)ofanappropriatemeasureofaspecified(usuallyunwelcome)consequence;and
• Amulti-attributequantityexpressinghazard,danger,or chanceofharmfulorinjuriousconsequencesassociated withactualorpotentialexposures.
Theseareverydifferentconcepts,andtheusebyprofessionalsofallofthemhascertainlynothelpedtofacilitate theunderstandingofriskatlowdoses.
Butforthenon-professionals,themeaningofriskcan beverydifferentthanthedifferentconceptsusedbyprofessionals.Thegeneralpublicoftenassociateriskwithavariety ofconnotationsincludingchance,plausibility,likelihood, prospect,hazard,imperiling,jeopardizing,gambling,betting, wagering,venturing,danger,peril,threat,menace,fear,and endangering.Threat,menace,andfearhavebeenthemain publicconnotationsofradiationriskandhavefueledthepublicfearofradiation.
Historically,thequantificationof “risk” wasformedon aretrospectiveanalysisofactualexperienceonfactual
www.health-physics.com
frequenciesofpastoccurrencesandwasthusquantified witha “frequentist” probability;namely,aprobabilitycalculatedfromthefrequenciesoffactualoccurrenceoftherisky event.However,overtime,theconceptof “risk” evolved,particularlyforradiationprotection,andisnowoftenalsoreferredtoasasubjectiveprobabilityofoccurrenceresulting fromexperts’ judgments,whicharesometimesbasedonestimatesoffrequentistprobabilitiesbutfromdifferentsituations.Thus,dueinlargeparttothelackoffactualdataof healtheffectsatlowdoses,conjecturesaremadeextrapolatingriskestimatesfromhigh-doseradiationexposuresituationstolow-dosesituations.
Theconceptoffrequentistprobabilitywasandcontinues tobethebasisforepidemiologicalestimatesandshouldprovidethecorescientificbasisforradiationprotectionatdoses abovethelevelsatwhichstochasticeffectsareseen.Originally, radioepidemiologicalestimatesweregenerallyperformed usingdataonfrequenciesofsuchactualhealtheffectsfactually incurredintheaftermathofpastradiationexposuresituations. Sucheventsusuallyinvolvedrelativelyhighdosesandhigh andhighlychangingdoserates,suchasthoseaffectingthe cohortofHiroshimaandNagasakisurvivors.Alas,this frequentistradioepidemiologicalpracticewasextendedto low-doseradiationexposuresituationsforwhichaprevalenceofradiation-induceddiseaseisnotidentifiable;namely, wheretherearenotfrequenciesprovidingabasisfortheassignmentoffrequentistprobabilities.Thesesituationswould epistemologicallybeconsideredtobeoutsidethedomain ofradioepidemiology.However,extrapolationsfromthe frequentistexperiencehavebeenusedforprovidingestimates and,withthehelpofexperts’ subjectivejudgments,notional radiationriskshavebeeninferredasasubjectiveprobability quantifyingapotentialincrementoverthebackgroundprevalenceofeffects.
Onthesebases,bothfrequentistandsubjectiveradiation risksareexpressedinradioepidemiologyindistinctlyasexcess absoluterisk,meaningtherateofdiseaseinanexposedpopulationminustherateofdiseaseinanunexposedpopulation.They arealsoexpressedasexcessrelativerisk,i.e.,therateofdisease inanexposedpopulationdividedbytherateofdiseaseinanunexposedpopulationminusone.Inadditiontothesetwomain denotations,alargenumberofrisk-relatedterminologiesare somehowconfusedlyusedinradioepidemiology,anotation thatmaybecontributingtopublicfear.
Thepuzzlementcausedbythedifferentdenotations andconnotationsoftheword “risk” havepermeatedthe fieldofradiationprotection.Inthedescriptionsoftheradiationprotectionparadigmandintheradiationsafetystandards,thewordriskisusedprolificallyandindissimilar ways,withoutspecificallydescribingthemeaningofthe termeachtimeitisused.Notably,adetriment-adjustedrisk isdefinedastheprobabilityoftheoccurrenceofastochastic healtheffect,modifiedtoallowforthedifferentcomponents
ofsuchdetrimentinordertoexpresstheseverityoftheconsequence(s).Thedetrimentisamultidimensionalconcept includingstochasticandconjecturalcomponents,suchas probabilityofattributablefatalcancer,weightedprobabilityofattributablenon-fatalcancer,weightedprobabilityofsevereheritableeffects,andlengthoflifelostifthe harmoccurs.
Thus,theradiationprotectionparadigmisbasedona radiationweightedrisk-dosemodelestimatedbyextrapolationofhigh-dosedata,withoutadosethreshold.
Initspublication60,ICRPhadengagedinasophisticatedanalysisoftheconceptofriskbutavoidingthecrucial distinctionbetweenfrequentistandsubjectiveprobabilities. Thatrecommendationincludedtheformulationofprecise, butagainconjectural,quantitiesdefiningrisk,including thetotalprobabilityofdeath(usedasareference)andthe conditionalandunconditionaldeathprobabilityrates.These quantitieswouldeventuallyevolveintoseveraltypesofestimatesthatcanbeusedtocalculateconjecturallifetime risk;namely,thesubjectiveprobabilitythatindividualswill develop,ordiefrom,aspecificdiseasecausedbyradiation exposure.Theseestimatesinclude:
• Theexcesslifetimerisk,whichisthedifferencebetween theproportionofpeoplewhodevelopordiefromthediseaseinanexposedpopulationandthecorresponding proportioninasimilarpopulationwithouttheexposure;
• Theriskofexposure-induceddeath,whichisdefinedas theincrementinacause-specificdeathrateaccumulated overalifetime,asanadditionalcauseofdeathintroduced byradiationexposure;
• Theriskoflosinglifeexpectancy,whichdescribesthe decreaseinlifeexpectancyduetotheexposureofinterest;and
• Thelifetimeattributablerisk,whichisanapproximation oftheriskofexposure-induceddeathanddescribesexcess deaths(ordiseasecases)overafollow-upperiodwith populationbackgroundratesdeterminedbytheexperienceofunexposedindividuals.Thelifetimeattributable riskisusedbyICRPtoestimatelifetimerisksandforestablishingdoserestrictions,butunfortunatelyitwasnot clearlyindicatedthatlifetimeattributableriskisaconjecture(i.e.,basedonopinionsorconclusionsinferredfrom incompleteinformation).
Itistobeemphasizedthatthedistinctivenessofthe frequentistvis-à-vissubjective interpretationofriskisnotspecificallyrecognizedintheICRPparadigm.Thefrequentist probabilitiesarisingfromtheepidemiologicalstudiesofpopulationsexposedtorelativelyhighdosesandhighdoseratesare usedtofiguresubjectiveradiationriskestimatesforlow-dose low-dose-rateexposuresituations,andnospecificdistinctions aremadebetweenthesetwoprobabilities.
Itiscleartherearemanynuancesthatcomeintoplay whendiscussingrisks,andradiationrisksinparticular.A comprehensivediscussionofsuchnuancesisaddressedin theliterature(Gonzalez2015).Forthepurposeofthispaper, itshouldbesimplyrecognizedthatallfourfieldsoftherelevantsciences,i.e.,radiationepidemiology,radiationbiology,radiationpathology,andradiationprotection,playan importantroleinunderstandingtheactualhealtheffectsof radiation.Whereasdisagreementoftenexistswithinthese fieldsregardingtheinterpretationofthehealtheffectsresulting fromradiationexposure,thereisampleandconvincingevidencethatthereisnolegitimatereasonforthepublictoremain fearfulofexposuretolowradiationlevels.
Insummary,
• Aprovableradiationriskforindividualsoccursonlyfor exposuretohigh-doseradiation(thedeterministicdomain andthemediumandhighdose-epidemiologicaldomain).
Peopleoughttofearriskduetotheeffectsresultingfrom highandmediumdoses,butsucheffectsarenotattributablefollowingexposuretolowradiationdoses.
LEGALCONSIDERATIONS
Theabilitytoattributehealtheffectstospecificradiation exposuresituationscaninfluencethelegalcapabilitytoimputedamagesfromthosesufferingdetrimentaleffectsto thoseresponsiblefortheexposure.Theimputationmayincludeassigningliabilitiesforphysicalinjuriesorharmful effectsinflictedonthosewhoreceivedtheexposure.
Fordeterministiceffects,thelegalprocessisstraightforward,andtheradiopathologistdiagnosingtheeffectisaproper andsufficientexpertwitnesswhocanlegallyattestincourtto thefactualoccurrenceoftheeffects.Butforstochasticeffects, individualattributionisnotfeasible.Insomelegaljurisdictions (Gonzalez2022),collectiveimputation(sometimestermedas “classaction”)isfeasible,andradioepidemiologistswouldbe appropriateexpertwitnesses.However,suchclassactionsare notobtainableinalljurisdictions(Gonzalez2022).
Forsituationswheretheradiationexposureisinthe loworverylowregion,thereisnofactualbasistoimpute damagesincetheinferencesofriskarebasedonlyonsubjective(conjectural)expertjudgment.Fartoooften,thiscaveatismissedinlegalproceedings,andawardsforworkers ormembersofthepublicsubjectedtotheselow-doseexposuresarebasedonemotionsorpoliticalconveniencerather thanscience.Thesesituationsareoftenpublicizedandhave alsolikelycontributedtothepublicfearofradiation.
Insomejurisdictionswherelegislationisnotcodifiedand foroccupationalcases,ithasbeenagreedtousefactualexposuredatatodetermineaconjectural “assignedshare” oftheradiationdamages.This “assignedshare” isdeterminedbyfirst evaluatingthehypotheticalrelativeriskofthesituation.The
excessriskisthentheriskincurredbeyondtherelativerisk, andtheassignedshareissimplydeterminedastheexcess relativeriskdividedbytherelativerisk.
Theoverallissueofattributingworkers’ harmtooccupationalexposurewasaddressedbytheInternationalLabor Organizationwithoutaclearoutput(ILO2010).Thewider issueofimputingharmtoradiationexposuresituationshad beendiscussedintheinternationallegalliterature(Gonzalez 2002,2014c)andhasbeenoneofthetopicsofarecent IAEAbookonnuclearlaw(IAEA2022b).
Adefinitiveclarificationoftheimputabilityofharmto radiationexposuremightbecrucialforlimitingthepublic fearoflowradiationdoses.
THELINEARNO-THRESHOLD REGULATORYAPPROACH
Duringtheearlyyearsfollowingthediscoveryofradiation,thisnewphenomenonwasgenerallyreveredasanexcitingnewmethodologyfordiagnosingbrokenlimbsduringWorldWarIandevenasa “tonic” forimprovinghealth. Butlikemanyothernewdiscoveries,itwassometimesused inexcess causingskinburnsandotherhealthimpairments andthispromptednewexperimentstodeterminesafe doselevels.
PerhapsthemostinfluentialworkwasdonebyHerman Muller(Calabrese2019)whenheirradiatedfruitfliesand concludedthattherelationshipbetweendoseanddamage waslinear,withnothreshold.Eventhoughhisdatawereobtainedatveryhighdoserates(thousandsoftimeshigher thanlow-levelradiation),hewaslaterawardedaNobel Prizeforrelatedmutationalstudies,providingahighmeasureofnotoriety,withafollow-upendorsementofhislinear modelbytheNationalAcademyofSciences(NAS)inthe mid-1950s(CalabreseandGiordano2022).
Althoughtheremayhavebeenotherfactorsinaddition toMuller’searlyworkthatcameintoplay,hisworkleddirectlytotheacceptanceofthelinearno-threshold(LNT) model.Thus,inspiteofthemanycaveatsintheICRPrecommendations,LNThasbeenadoptedininternationalsafety standardsandalmostuniversallyusedwithintheinternational radiationprotectioncommunityasapracticaltoolforregulatingradiationexposure.
Butamajorcontroversyisbuildingwithintheradiation protectioncommunity.Someresearch(Calabreseetal.2022), alongwithanextensivevideoseriespioneeredbytheHeath PhysicsSociety(Cardarellietal.2023),provideconsiderablesupportforhowprofessionaldeceptionmayhavecrept intotheadoptionoftheMuller’soriginalLNTpremise.
GiventhequestionableethicsrevealedintheCalabrese investigations(Cardarelli2023),itisnotsurprisingthatthe meaningoftheLNTmodelismultipleandimprecise.Itis intendedtomean “alineardose-responserelationshipwith
nothresholdofdose,” butthereisambiguityinitsprecise understanding,withinterpretationsincludingthefollowing:
• Forsomeitisa premise;namely,anunderlyingassumptionthatradiationcarriesariskatanylevel;
• Forothersitisa hypothesis;namely,asuppositionor proposedexplanationoftherelationbetweenhealtheffectsandincurredradiationdose,whichismadeonthe basisoflimitedevidenceasastartingpointforfurtherinvestigation;and
• Forothersitisa model;namely,asimplifieddescription ofacomplicatedphenomenonthatisusefulonlyfor practicaloperationalpurposes.
ThesevariousviewsoftheLNThavepermeatedthe differentprofessionalcommunitiesinvolvedintheissue. Giventhiscontroversy,LNThasbeenusedwithdifferent denotationsbytherelevantprofessionalcommunitiesand withmanyconnotationsabsentspecializedaudiences,thus likelybecomingasignificantcauseofconfusioncontributingtothepublicfearofradiation.
LNThasbeenviewedbythevariousradiationprofessionalcommunitieswiththefollowingsimplifieddescriptions.
Radiopathologists
Forradiopathologists,LNTisneitherapparentnorneeded, neitherasa premisenorasa hypothesisnorasa model. Radiopathologistslookforfactuallydiagnosedeffectson individualswhohavebeenexposedtohighradiationdoses. Thedose-responserelationshipisasigmoidcurvepresentingadefactodosethreshold.
Belowthedosethreshold,radiationeffectsare,fora radiopathologist,neitherdiagnosablenorattributableinindividuals.Itshouldbenoted,however,thatradiopathologists mayusespecializedbioassayspecimens(suchassomehematologicalandcytogeneticsamples)asbiologicalindicatorsof radiationexposure,evenatdosesbelowthethreshold.Nonetheless,UNSCEARhasindicatedthatthepresenceofsuchbiologicalindicatorsinsamplestakenfromanindividualdoes notnecessarilymeanthattheindividualwouldexperience healtheffectsduetotheexposure(UNSCEAR2012b).
Radioepidemiologists
Forradioepidemiologists,LNTisa hypothesis,anepidemiologicalconjecturebywhichchangesinthebackgroundincidenceofdeleteriouseffectsassociatedwithradiation,suchasmalignancies,perunitdose,canbemeasured. Indeed,radiationexposuresituationsinvolvingrelatively highdoses,deliveredatrelativelyhighdoseratesandinvolvingsubstantivetimechangesofthedoserate,havebeen made.Butalltoooften,radioepidemiologistshavepresumedsuchchangesoccurequallyatradiationexposuresituationsinvolvinglowdosesandlowdoserateswithno changeinthedoserate inspiteofthefactthatepidemio-
logicalevidenceisnotachievableinsuchsituationsdueto epistemicandstatisticallimitations.
Stateddifferently,forradiation-epidemiology,LNT meansthattheincidenceofeffectsperunitdoseathighdoses, highdoserates,andhighdose-ratechanges,whichisbacked upwithepidemiologicalevidence,remainsthesameatlow dosesandlowdoserateswithnosignificantchangesinthe doserate,inspiteoftheabsenceofepidemiologicalevidence. Epidemiologyisaveryserviceablesciencewherean epidemicexists,suchastheepidemicofradiationeffects thatfollowedthebombingofHiroshimaandNagasakior theepidemicofpediatricthyroidcancerthatfollowedthe highthyroiddosesincurredbychildrenthatingestedhighly contaminatedmilkfollowingtheChernobylaccident (UNSCEAR2008c).Butsuchanepidemichasnotbeen visibleforlow-levelradiationexposuresituations.Itisonly presumedtoexist.Theexistenceofeffectsisjustconjectured because shouldtheyexist theycannotbeseenduetothe epistemicandstatisticallimitationsofepidemiologicalsciences.Itissimplyunfeasible(namely,impossibleandimpracticaltoachieveeasilyorconveniently)toaccruesufficientstatisticaldataforlow-doseexposuresituationsinorder toobserveactualhealtheffectsduetothoseepistemological constraints.
UNSCEARhasbeenevaluatingepidemiologicalstudies ofcancerandcardiovasculardiseasesforyears(UNSCEAR 2006a).Inrecentyears,UNSCEARconductedareevaluation forinferringcancerrisktoexposureatlowdoseratesfromenvironmentalsources(UNSCEAR2017a).Theoverallresults ofthosestudiesimplythattheriskofcancerperunitdoseis smallerforlow-dosethanforhigh-dosesituations although uncertaintystillexistsduetothelowstatisticalpowerassociated withlow-doseradiation.Environmentalradiationexposuretypicallyresultsinlowandmoderatedoses,andtherefore,potential excesscancerrisksmaybeexpectedtobesmallornonexistent. Theestimationofsuchsmallandinferredincremental risksofcancerfromprotractedradiationexposurescould easilybeaffectedbyconfoundingduetoothercancerrisk factors.Itisimportanttoemphasizethatradiationisjust oneoftheriskfactorsforcancer.Itisunlikelythatradiation actsindependentlyfromotherriskfactorsincancerdevelopment(suchassmoking,diet,etc.).Thismaycontribute tothedifferencesbetweenstudyresultsbecausetheexistenceofconfoundersandtheirassociationwithradiationexposurecanvary.Ananalysisaccountingfortheeffectsof confoundersalsosetsrequirementsforsamplesizeina study.Butevenwithinthiscontext,meta-analysisorpooled analysisofpiecemealdatahaslimitationsnomatterhow largethesamplesize.Demonstratingtheinsignificanceof low-doseexposurecomparedtootherlifestylefactorsin well-organizedepidemiologicalstudies(e.g.,Kudoetal. 2022)willbemoremeaningfulasreal-lifeevidence.Precise estimatesofhealtheffectsandtheirfrequenciesneedsufficient
follow-up,caseascertainmentthroughhigh-qualitycancer registrysystems,andaccurateinformationonriskfactorsother thanradiationexposure.Thisemphasizestheneedforprospectivelong-termstudieswithhigh-qualitydosimetry,aswell ascomprehensiveandaccurateoutcomedataandinformation oncancerriskfactorsotherthanradiationexposure.
Thequalityofradioepidemiologicalstudiesisakeyissue. Thecurrentpreferredmethodsofevidencesynthesisaresystematicreviews,meta-analyses,andpooledanalyses,which areregardedasthestate-of-the-artscientificstandardsfor poolingresearchdataandaredeemedsuperiortotraditionalnarrativereviews.Thereareprinciplesandcriteriaforensuringthe qualityofthereviewsofepidemiologicalstudiesthattakeinto accountthesescientificdevelopments.Itshouldbenotedthat thespecificnatureandscientif iccontentsofsuchstudiesdo notallowforamechanisticapplicationofgenericqualityassurancecriteriaand,therefore,UNSCEARhasdevelopedanapproachtoassessthequalityofsuchstudiesandtosynthesize thefindingsfrommanystudiesintoitsinferenceofradiation risks.Thisispublishedasareportonprinciplesandcriteria forensuringthequalityoftheUNSCEAR’sreviewsofepidemiologicalstudiesofradiationexposure(UNSCEAR2017b).
UNSCEARhasdiscussedtherelevanceofthedoseand thedose-rateeffectivenessfactor(DDRF),aradiationprotectionconcept,inthecontextofscientificevaluationsofepidemiologicalstudiesofcancerriskfromlowdose-rateexposure. Itconcludedthatthedose-responserelationshipsdependona largenumberoffactorssuchthatthescientificevidenceregardingapossiblereductionintheradiation-inducedeffects perunitdoseatlowdosesandlowdoseratesrelativetoacute exposureswithmoderateorhighdosescannotbeexpressedby asinglevalue.Duetothisplethoraoffactors,theappropriatenessandneedoftheDDRFconcepthavebeendeeply questioned(Gonzalez2017).
UNSCEARcontinuestoreviewthedevelopmentsin epidemiological,biologicalandstatisticalanalysesthatcontributetoimprovedinferenceofrisk,ifany,following low-doseandlowdose-rateenvironmentalexposures.Meanwhile,UNSCEARencouragesapplyingradiobiologicaldata derivedoverthepastcoupledecadestohelpunderstandthe lackofobservablecancerincidentsfollowingtheexposure tolowdoses,evenwithoutknowingwithcertaintytheprecisemechanismsinvolved.
Insummation,theradioepidemiologicalmeaningof LNTshouldreflectthefactthattheepidemiologicaloutcomes fromlow-doseradiationexposuresituationsareonlyconjecturalinferences;namely,theeffectsarenotattestableandcannotbeattributed.Lookingtothefuture,UNSCEARrecommendscombiningamechanisticunderstandingoflow-dose radiationcarcinogenesiswithepidemiologicalstudiesusing mathematicalmodelingintegratingdatafromexperimental systems(e.g.,dose-responsedataforinductionofkeymutationsorepimutations).
Radiation-protectionists
Forradiation-protectionists,LNTrepresentsa model,i. e.,asimplifieddescriptionofreality,whichispracticaland workableformanagingoperationalradiationprotection, particularlyinoccupationalradiationprotection,byexercisingprotectionagainstadditionaldosesregardlessofthe levelofaccumulateddose.
Ifthismodelisnotusedfortheprotectionofworkers,it maynecessitateassigningdifferentprotectionforthesame increaseindoses,dependingontheaccumulateddose.This couldunavoidablycreatediscriminationamongworkers, suchasage-relatedconsiderations,whichispreventedby thecurrentinternationallaborlegislation.
Radiobiologists
Forradiobiologists,LNTwasoriginallytakenasa premisepostulatingthatatlowradiationdoseexposures,a givenincrementindosewouldproduceadirectlyproportionateincrementintheprobabilityofincurringcellulareffectsthatwouldevolveintomalignanciesorheritableeffectsattributabletotheradiationexposure.
Theearlyradiobiologicalassumptionwasthatthemain interactionsofradiationwithlivingmatterwere “targeted” directandindirectinteractingeffectswiththecellularDNA causingmutationsthatcouldevolveintoassociateddetrimentaleffectssuchasmalignancies.However,biologicalresearch overthepastfewdecadeshasincreasedtheunderstandingof howradiationinteractswiththenon-linearcomplexitiesoflivingtissue.Accordingly,itisimportanttodelveabitdeeper intothebiologicalaspectsofradiationexposureatlowlevels, sincethedevelopmentofascientifically-basedpremisetoreviewandeventuallyrevisetheLNTpremisecanonlybeaccomplishedandacceptedbythebroadradiationhealthprofessionalcommunitywhenthedetailedbiologicalprocessesare understood(Brooksetal.2023).
Detailedradiationbiologyresearchoverthepastfew decadeshasrevealedmanysecondary, “non-targeted,” effects,includingthefollowing(UNSCEAR2006b):
• Radiation-inducedgenomicinstability,inwhichifasingle cellisirradiatedandsurvives,itmayproducedaughtercells thatovergenerationshaveincreasingnumbersofmutations;
• Adaptiveresponse,whichexpressestheprovenabilityof cellsandtissuesinallorganismstorespondtoanumber ofdifferentchallengestobetterresiststressdamage,e.g., alsocausedbyradiationexposure(inthiscontext,adaptiveprotectionappearstooperatebypreventionofDNA damage,repairofdamage,andbydamageremoval);
• Bystandereffects,namelytheabilityofirradiatedcellsto conveymanifestationsofdamagetoneighboringcellsnot directlyirradiated;
• Abscopaleffects,whicharesaidtooccurifthereisasignificantresponseinatissuethatisphysicallyseparate fromtheregionofthebodyexposedtoradiation;and
Inducedclastogenicfactors,whichresultfromalargebody ofevidencethatbloodplasmafromirradiatedanimalsand humanscancontainso-called “clastogenicfactors” capable ofinducingchromosomaldamageinunexposedcells.
Intheearlyphasesofresearch,therewasaconcernfor heritableeffects,i.e.,effectsthatmightbeobservedinoffspringbornafteroneorbothparentshavebeenirradiatedprior toconception,andUNSCEARstudiedtheissueindepth (UNSCEAR2001).However,suchheritableeffectshave notbeenseeninhumans,andUNSCEARhasconcludedthat “althoughdemonstratedinanimalstudies,anincreaseintheincidenceofhereditaryeffectsinhumanpopulationscannotat presentbeattributedtoradiationexposure” (UNSCEAR2012b).
Someofthemanifestationsofthesenon-targetedand delayedeffectscaninprinciplearisespontaneouslyandafter exposuretootheragents.Theseeffectshaveledtodifferent assumptions,rangingfrom(1)thepossibilitythatlowradiationdosesproducebeneficialeffects(hormesis)ratherthan damage,to(2)thepossibilitythatlow-doseexposurebrings higherrisksthanhypothesizedfromepidemiologicalstudies.
Thecausesofthevarioustypesofresponsestoirradiationdependontheinteractionofenergydepositionevents withsensitivestructuresatthevariouslevelsofbiological organization(ICRP2015;UNSCEAR2021).Thus,exposuretofieldsofionizingradiationcreatesenergydepositionsalongtracksofsubatomicparticlesofmicroscopicdimensions.Suchenergydepositioneventsaredistributedby chanceinexposedmattersuchasbiologicaltissues.Atthe molecularlevel,theenergydepositionsoccurstochastically. Forexample,inaradiationfieldof100kVxrays,anaverage energydepositioneventpernanogramtissue(anaveragecell mass)constitutesaroundtheequivalentof1mSv.Thus,the typicallimitinglevelsofradiationdosesbeingregulatory controlledformembersofthepublic,namely1mSvperyear, wouldleadtooneenergydepositioneventpernanogramper year;namely,aroundoneinteractionpercellperyear.
Themajorconcernsofsuchexposureareanyespecially seriousdamagingchangesofthegeneticmaterial,theDNA, withimmediateattemptsofrepair,andsubsequentalterations ofcellularsignalingcontrolmechanisms.
Ingeneral,biologicalresponsestolowdosesofionizing radiationaretwofold:primaryeventsfollowingenergydeposition,andsecondaryresponsestotheprimaryevents.These latterresponsesappearwithinhoursafterexposureandmay lastoverlongtimes.Sincethetypesanddegreesofsecondaryresponsesareundergeneticcontrol,variousdegreesof radiosensitivityexistamongthehumanpopulation.
Theissueofradiosensitivityiscomplex.Theeffectsofradiationupthroughthechainofcellstructuretocomplexorganscanvaryamongindividuals,includingtheageandgenderofeachindividual.However,theICRPhasaddressedsuch effects(ICRP1998),principallythegeneticvulnerabilitiesfor
cancer,andhasconcludedthatsuchvariableshavebeenwell accountedforintheiroverall guidance.Whereasvariations inradiosensitivitycouldbeofimportanceifradiationdoses arehigh,itishighlyunlikelythattheycanbeofsignificant concernforlow-doseradiation.Anyeffectsoflow-doseradiation,ifany,arealmostcertainlyoverwhelmedbyotherfactors. Regardingthemajoreffectsfromlow-doseandlow dose-rateradiation,thefollowingreporting(Feinendegen andCuttler2018)summarizeskeyoutputsfromconsiderablebiologicalresearch:
• Lowdosesofionizingradiationtoexposedcells,quite differentfromhighdoses,causeinexperimentalbiologicalsystemspotentialprotectivecellularsignalingchanges thatarefairlylargeincomparisonwithrelativelyveryfew potentiallyseriousDNAdamages,andmostsuchdamage isbasicallyrepairedrelativelyrapidly.Asdoseratesincrease,thenumberof “hits” increaseinalinearfashion. Butthesignalingchangesthatfollowaremanifestina non-linearfashionincomplexbiologicalsystems.Inparticular,adaptiveresponse-protectionswithbeneficialconsequenceshavebeenmeasuredtoreducespontaneous damageintheexposedsystem.Othersecondaryresponses(referredtoearlier)includegenomicinstability, bystandereffects,andabscopaleffectsthathavebeenobservedathigherdoses(Brooksetal.2016);
• Atchroniclowdose-rateexposure,repairmechanisms andsecondaryresponsesreduceorpreventcellulardamageaccumulation.Anycelldamagethatdoesoccurneeds tobecomepropagatedthroughtheincreasinglycomplex levelsofbiologicalorganizationinordertocauselatedetrimentalhealtheffects.Such damage,ifany,andthepropagationofsuchdamage,isaninherentlynon-linearprocess(Feinendegenetal.2010);
• Secondaryresponsestolowdosesofradiationhavebeen unequivocallyobservedinthehumanbody.Yet,thesignificanceforthemtocauseclinicalhealtheffectsisstill beingdebated.Whereassomeconjectureremains,ithas beenarguedthatessentiallyallbiologicalsystemscontributepositivehealthresultsatlowdoses(e.g.,medications, vaccinations,traceelements,etc.)butresultinconsiderable damageathighdoses;simplyput,thepoisonisinthedose;
• Radiationbiologydataindicatethattheprobabilityofaclinicalmalignancyinthehumanbodyfollowinglow-doseexposure,ifitoccursatall,issmall.Spontaneousdamagefrom physiologicalreactiveoxygenspecies(ROS),thekeyreactionprovidingessentialenergyforlifeitself,isfar morefrequent.Yetourbodilyprotectivesystem(immune system)clearlyaccommodatesandeffectivelyrepairs suchdamage.Furtherdiscussionofthispowerfulimmune systemisincludedbelow;
• Contrarytoearlierconcernsthatcellulardamagecanoccurevenatlowlevelsofradiation,recentexperimental
www.health-physics.com
evidencehasrevealedjusttheopposite;namely,thatbiologicalsystemsapparentlyrequireacertainlowlevelof radiationtosurviveandthrive(WaltarandFeinendegen 2020);and
• Ingeneral,livingsystemsprotectthemselvesagainstdamagebypreventingdamagetoarise,repairingdamagethat occurs,andremovingdamagethatescapesrepair.Theremovalisakeycomponentoftheimmunesystem.
Anissuethathasbeenwidelydiscussedbytheradiobiologycommunityistheeffectofionizingradiationonthe immunesystem.Theissuehasbeendeeplyreviewedby UNSCEARsince1972(UNSCEAR1972).Theimmune systemisoneofthemostcomplexsystemsofthehuman body.Itreliesonhighlyspecializedcellswiththeirspecific functionofprovidingaverycomplexsetofbiochemicalreactionsthatyieldseveraltypes(lymphocytesandaccessory cells)strategicallyspreadthroughoutthebody,perfectlypositionedtorecognizeantigens(non-selforforeignsubstancesandcells)andtoneutralizeordestroythem.This systemprotectsagainstinfectionsandcancer.Thereare twodifferentbutinterrelatedformsofimmunity:innate andacquiredimmunity.Innateimmunityisfullyfunctional beforeanyforeignagententersthebodyandtherebyprovidesarapiddefense.Acquiredimmunitydevelopsaftera pathogenhasenteredthebodyandmaintainsmemoryof previousexposures,yieldingastrongerresponsefollowing subsequentexposuretothesameantigen.Acquiredimmune responsesaremainlyexecutedbyB-lymphocytes(humoral responses)andT-lymphocytes (cell-mediatedresponses) (Feinendegenetal.2011).
Theeffectsofionizingradiationontheimmunesystem canbeassessedbyestimatingchangesincellnumbersorby usingavarietyoffunctionalassays.Theimpactofsuchalterationsinimmuneresponsedependsonfactorssuchasthedose ofradiation,itstemporalrelationtoimmunization,andgenetic disposition.Thereisnodoubtthathighdosesofradiationproduceimmunosuppression,mainlyduetothedestructionof cells.Lymphocytesareveryradiosensitive,andtheirreduction iscurrentlyusedasanearlyindicatorofthelevelofanaccidentalacuteexposure.Radiation-inducedchangesinimmune parametersseemtobemoredependentontotaldosethanon doserate(Liuetal.2020).Persistingeffectsontheimmune systemhavebeenobservedafterexposuretohighdoses.
Atlowdosesandlow-doserates,lowdose-ratechanges, andtheeffectsofionizingradiationontheimmunesystem mightbesuppressiveorstimulatoryornone.Someexperimentaldataappearstorevealthatusinglow-levelradiation tostimulatetheimmunesystemwouldlimitflusymptoms (CalabreseandDhawan2013),butthelong-termimpacts oftheselowradiationdosesontheimmunefunctionsinrelationtohumanhealthhavenotbeenevaluated.Manypeople throughouttheworldroutinelyvisitradiationhealthspas(e.g.,
mineswheretheradiationleveliswellabovenaturalbackground) andclaimconsiderablerelieffromnagginghealthissues.
UNSCEARhasconcludedthatwhilethesuppressive effectsofhighdosesofionizingradiationarewelldocumented(UN2014),uncertaintyexistsregardingtheeffects oflowradiationdosesontheimmunesystemsinceboth stimulatoryandsuppressiveeffectshavebeenreported.
Inspiteofthisnewinformation,therecontinuestobe considerabledebateregardingthecausalrelationshipbetween thenon-targetedeffectsandtheobservedhealtheffectsattributabletoradiation.UNSCEARconcludedseveralyearsago (UNSCEAR2006c)thattheestimationofthehealtheffects ofradiationshouldbebasedonepidemiologicalobservations wherethereisastatisticallysignificantdose-relatedincreasein diseaseincidence.Thesedirectobservationsofadversehealth outcomeswouldimplicitlytakeaccountofmechanisticelementsrelatingnotonlytothetargeted(direct)effectsofirradiationbutalsotothenon-targetedanddelayedeffects.
RecentUNSCEARestimates(UNSCEAR2019)onthe biologicalmechanismsrelevantfortheinferenceofcancer risksfromlow-dose,lowdose-rateradiationacknowledges theexistenceofsecondaryresponsesfollowinglow-doseradiationexposureasdescribedabove.Butbecauseoftheuncertaintiesofthesesecondaryresponses,whicharesmall anddifficulttodetectaccuratelyforlow-dosesituations, UNSCEARremainscautiousregardingtheirconsistency, disposition,andreproducibility.
Giventheseuncertainties,UNSCEARjudgesthereis stillinsufficientjustificationtorecommendchangesinthe currentradiobiologicalparadigmonthebasisofthesesecondaryresponses.Here,UNSCEARclaimsthatsofar,there isaconsiderabledegreeofuncertaintyregardingthemechanismsbridgingsecondaryresponsestoclinicalcancer.In thiscontext,itshouldbeemphasizedagainthattheincidenceofcanceratverylowdosescannotbemeasuredfor epistemologicalreasonsunlesslargepopulations(enough tobestatisticallysignificant)arebeingstudied.Further, giventheheterogeneityofindividualsforvariousaspects, theriskofcanceratverylowdosescouldnotbeevidenced evenifalargenumberofindividualswerestudied.
Insummarizingtherecentresearchwithintheradiationbiologycommunity,despiteremaininguncertainties astowhetherandtowhatdegreeadaptiveprotectionalways operatesagainstradiogenicandnon-radiogenicdamage, anyradiationhealtheffectsatlowdose,iftheyexistatall, arealmostalwaysdwarfedbyothertoxinsthatwelivewith everyday,suchasthenaturalbodilyburningofoxygenso essentialtolife.
MISUSEOFLNTANDRADIATIONFEAR
ThewideandimpreciseuseoftheacronymLNT,withoutclarificationofitsrealmeaning,haslikelybeenacause
www.health-physics.com
ofseriousconfusionaboutthehealtheffectsattributableto radiationexposuresituationsinvolvinglowdose,lowdose rate,andlowdose-ratechange.Thisismostdisturbingbecausethesearesomeradiationexposuresituationsassociatedwiththemanybeneficialusesofradiation.
Thewiderbutepistemologicallywrongconnotationof LNThasbeentheimproperuseofthequantitytermed collectivedose.Thecollectivedoseisanextensivequantity (differentlyfromtheintensivequantitydose),whichisdefinedasthetotalradiationdoseincurredbyapopulation. Animproperuseofthisquantityhasbeentointegratethe lowdoseofanindividualcohortmemberandmultiplyit bythetotalnumberofpeopleinthatcohort resultingina largehypothesizednumberofcasualties.BothUNSCEAR andICRPhavewarnedthatthisapproachisimproper.This misuseofcollectivedosehasbeendoneevenatacademic levels,e.g.,wronglyattributingtotheChernobylaccident aroundonemilliondeaths(Yablokovetal.2009)!Thisabsurdcalculationhasbeenwithdrawn,butthedamagewas done,andpublicfearofradiationwasincreased.
Giventhemisuseofsuchradiationriskcalculations, UNSCEAR,followingaspecificrequestfromtheUnited NationsGeneralAssembly,addressedtheissueofattributionofhealtheffectstodifferentlevelsofradiationexposure.Itreachedanumberofconclusions,significantlynotingthatincreasesintheincidenceofhealtheffectsinpopulationscannotbeattributedtolow-doseradiationexposure situations.Only notionalrisksfromplannedsituations maybeprospectivelyinferredforpurposesofradiationprotectionandallocationofresources.
EventheHolySeehasweighedinonthisissue.Areportonbiologicalimplicationsofoptimizationinradiation protectionfromthePontificalAcademyofSciencesindicatedthat “Therearereasonstobelievethattheassumptions inherentintheLNTmodelarelikelytooverestimatethereal riskatthelowdosesofinterest” (PontificalAcademyof Sciences1983).
THELNTMODELASCURRENTLYUSEDFOR REGULATORYPURPOSES
Asnotedearlier,thetermLNTusedbytheradiation protectioncommunitysimplyreferstoapracticalmodel formanagingoperationalradiationprotection.Thismodel assumesradiationexposureshouldbelimitedbycertain doselevels.Belowtheselevels,protectionshouldfollowa processofoptimizationofprotectionbyselecting(among theavailableprotectionalternatives)thebestprotectionoptionundertheprevailingcircumstances.Itsimplyassumes thatradiationrisksmightbeconjecturedandinferredat anylevelofdose.
However,iftheseconjecturalinferenceswithinthe practicalLNTradiationprotectionmodelareunderstood tobeprovenfacts,agapinunderstandingiscreatedthatis
likelyresponsibleforcreating publicfear.Theseriousepistemologicallimitationsofthebiologicalandepidemiological sciencesforvalidatingtheLNTmodelmustberecognized.
Despitetheseclearreservations,theLNTradiationprotectionmodelisrecognizedasrathereasytoadministerand servesasthegenerallyacceptedradiationprotectionmodel inmostnationsontheglobe.However,aswesumuptheevidencefromtheperspectiveofeitherradiationepidemiologyorradiationbiology,thereisnovalidreasontofear low-doseradiationexposures inspiteofthevariousinterpretationsoftheLNT.
Manyprofessionalsintheradiationcommunitynow arguethattheLNTmodelasusedbytheregulatorycommunityshouldberevisedanditspurposeclarified atleastfor radiationlevelsinthelow-dose,lowdose-ratedomain.They basetheirargumentsalongthelinesoutlinedabove.
Anewresearchanddevelopmentprogramiscurrently beingdesignedbytheUSNationalAcademiesofScience, Engineering,andMedicine(NASEM2022)toseekthedata neededtoevolveamorescientificapproachtotheregulationofradiationexposure.Hopefully,sufficientdatawill bederivedtoprovideawidelyacceptablemodeltobeembeddedinregulationapproachesworldwide.Butthismay takeseveralyears,anditisdependentonasustained fundingbasethatisoftendifficulttomaintainforthedurationneeded.
So,whatshouldwedointhemeantimetohelpremovethe unnecessaryanddestructivepublicfearoflow-doseradiation?
POTENTIALREGULATORYSOLUTIONFORTHE LOW-DOSECONUNDRUM:EXCLUSIONS
ANDEXEMPTIONS
Theconundrumofprotectionagainstlow-doseexposure,oftencausedbymisunderstandingsandmisapplicationsderivedfromtheLNTmodel,couldbesolvedthrough abetterformulationofthecurrentregulatoryapproach withoutenteringintocontroversialbiologicaland epistemologicaldiscussions.
Ontheissueofthedoselimits
Forinstance,takingintoaccountthecurrentdoserestrictionsestablishedininternationalprotectionstandards,itisalreadyestablished(albeitnotnecessarilyclear)thattheannual doseofsomeindividualsshouldnotexceed100mSvunder anycircumstance(namely,thefactualdose “limit”).ThecurrentvaluesforprotectioncriteriarecommendedbyICRP andestablishedininternationalsafetystandardsincludesuch afactuallimitforsomeemergencyexposuresituations.But theword “limit” isusedratherdifferentlywhenreferringto plannedexposuresituations.Itthenreferstoa “limit” ofanincrementofdoseaboveabackgrounddosethatishigherthan thestated “limit.” Tosuchapeculiar “limit,” thepublished lowvalueof1mSvy 1 forthepublichasbeenassigned.That
www.health-physics.com
isacauseofmajorconfusion.Itisquitereasonablethatthis leadsthepublictobelievethatreceivingadoseaboveornear 1mSy 1 isverydangerous.Theybecomesurprised(andperhapsrelaxed)whentheylearnthattheyarecontinuallyexposedtobackgroundnaturalradiationatdosesconsiderably higherthansucha “limit.”
Itshouldbenotedthatthe1mSvlevelwassomehow arbitrarilyselectedasanannualdoselimit.Ittracesback toapreviouslevelof5mSv,whichwasreducedbyafactor offivefollowingachangeinthedosimetryofthecohortof HiroshimaandNagasakivictims.Butthat5mSvhadbeen subjectivelyselectedasonetenthoftheoccupationaldose limitatthetime,whichwas50mSvy 1;namely,1order ofmagnitudelowerthanavalueconsideredsafeforanindividualworker.The50mSvy 1,inturn,hadbeenderived froman “indexofharm” developedbyICRP(ICRP1977).
Overtimethe “1mSvlimit” wasperceivedasapurposelylowextradoserestrictionofferedforthesakeofthe precautionaryprincipleduringa plannedexposuresituation involvingmembersofthepublic.Itshouldbenotedthata plannedexposuresituationisasituationofexposurethat arisesfromtheplannedoperationofaradiationsourceor fromaplannedactivitythatresultsinanexposureduetoa source.Sinceprovisionforprotectionandsafetycanbe madebeforeembarkingontheactivityconcerned,associatedexposuresandtheirprobabilitiesofoccurrencecanbe restrictedfromtheoutsettolowprecautionarylevels.In fact,theprimarymeansofcontrollingexposureinplanned exposuresituationsisbygooddesignofinstallations, equipment,andoperatingprocedures.
Constructingtheideathatareal “limit” [i.e.,apointbeyondwhichanindividualdoseshallnotpass(aterminal pointorboundaryforindividualdoses;namely,therealregulatoryrestrictiononthelevelofdoseincurredbyindividuals)]shouldbe,andinfactalreadyis,somethingcloser tothe100mSvy 1 level.Thisisrecognizedincurrentstandardstobeanacceptablesafelimitbecauseitisallowedto beincurredundersomeconditions,whicharespecifiedin theinternationalstandards.Adoptingthisinterpretation wouldconstituteahugestepingreatlyamelioratingtheunnecessarypublicfearoflow-levelradiation.
Ontheissueofoptimizingprotection
Inaddition,thestandardsrequirethatprotectionbeoptimized;namely,thatthebestoption(amongtheavailableprotectionoptions)beselectedundertheprevailingcircumstances. Optimizationinthegeneralsenseisintendedtofindtheprotectionsolutionthatprovidesthemaximumbenefitwiththeminimumdisadvantages.Unfortunately,mainlyduetohistoricalreasons,optimizationofprotectionissometimesconfusedwith minimizationofindividualdoses.Thisissimplywrong.
Amostunfortunateexampleofplacingunduefocuson radiationdosewastheevacuationproceedingsfollowingthe
Fukushimaaccident.Asnotedinthenextsectiondealingwith socialconsequences,thedeathtollduetothelong-termevacuationprocessresultedinahighnumberofactualfatalities, butnonewereduetotheradiationexposureitself.
Ontheissueofregulatoryscope
Thelow-doseconundrumcouldwellbesolvedthrough acleardefinitionofthescopeofwhathastoberegulatedby introducingthekeyconceptsofexclusionfromregulations andexemptionsfromregulating.Theconceptofexemption fromregulatorycontrolwascarefullyconsideredmanyyears ago(LinsleyandGonzalez1988),anditwasintroducedin Europeveryearly(EC1993);however,aninternationalconsensushasbeenelusive.
Regulationofradiationexposurehasnotincludeda cleardefinitionoftheregulatoryscope.ICRPhasmadeclear recommendationsinthisregard(ICRP2007b),buttheyhave beengenerallyignoredbyregulators.Forinstance,thereis notauniversal,homogeneous,coherent,andconsistentincorporationofthecrucialconceptofexclusionandexemptionrecommendedbyICRPintonationalregulations.
Legislativeandregulatoryauthoritiesshouldexercise someeffortstowarddefiningthescopeofradiationprotectioncontrolmeasuresthroughlegislationandregulations. Forthispurpose,theycouldusethewell-establishedand universallyacceptedradiationprotectionprinciplesofjustificationandoptimization.
Someradiationexposuresituationsmaybeconsidered for exclusionbythelegislationbecausetheirregulatorycontrolisdeemedtobeunamenableorunjustified.Newprudent legislationcouldthendevelopunambiguous exclusion criteriafordefiningthescopeofradiationprotectionlegislationbyusingtheoldlegislativeprincipleof deminimisnon curatlex.Iflegislationwithexclusioncriteriawereclearlyestablished,itwouldallowtacklingsomecontroversialissues ofspecificexposuresituations,suchasexposuretocosmic raysatgroundlevelandothernaturaloccurrences.
Inaddition,regulatorsmay exemptradiationlow-level exposuresituationsfromregulatorycontrolonthebasisthat deregulationistheoptimumprotectionoption(deminimis noncuratprætor).Suchactionwouldprovidethegeneral publicagreatservice.Thisguidancewouldprovidethebasis forrecognizingthat,inmanycases,exemptionsprovidethe optimalsolution.Thiswouldresolvetheproblemsofregulatinglow-energyornon-penetratingradiation,somenaturally occurringradioactivesubstances,lowlevelsofradioactivity inconsumergoods,andlow-levelradioactiveresidues.
Thus,theconceptsof exclusionand exemptionshould becomemodernparallelstotheancientlegalprinciplesof deminimisnoncuratlex and deminimisnoncuratprætor, respectively,whichoriginatedinRomanlawtwomillennia agoandsincethenhavegovernedthelegalproblemofregulatingtrifles:namely,regulatingwhatisinconsequential,
unfeasible,unimportant,orirrelevantfromthepointofview eitherofthelegislatorortheregulator(trifleinthissenseis notnecessarilyasynonymoftrivial).The deminimisnon curatlex principleaddressesthesituationsthatthelawshould (orshouldnot)takeaccountof,orcover.The deminimisnon curatprætor principleaddressesthesituations,amongthose coveredbythelaw,thatcanbefreedbytheregulatorfrom someorallregulatorycontrols.
SOCIALCONSEQUENCESOFRADIATIONFEAR
Beingfearfulofsomethingsisbothunderstandable andharmless doingnodamagetothegeneralpublic.Beingafraidofthedarkorbeingfearfulofsnakesmayimpact thelifestyleofanindividual,butithasnoimpactonothers. Butbeingafraidoflow-levelradiation,wherethereisno justificationforsuchfear,doescausedamagetosociety. Followingarejustafewexampleswheresuchunfounded fearoflow-levelradiationhasresultedinconsequences quitedetrimentaltomodernlife.
TheThreeMilenuclearaccident
Thisaccident,whichoccurredon28March1979near Harrisburg,PA,resultedinapartialcoremeltdownanda hugeeconomicloss(Rosztoczy2019).However,theradioactivesubstancesreleasedintotheatmospherewereminiscule,andthetheoreticallycalculatedradiationdoseswere lowerthanthenaturalbackgrounddosesincurredbyanairlinepassengerflyingfromLosAngelestoNewYork.Yet thesensationalnegativepublicityandfeargeneratedbythis eventresultedinalargesocialimpactonthepopulationand, moreover,inamajorhaltinthelicensingandconstruction ofplannednuclearreactorexpansions especiallyinthe UnitedStates.Anexponentialnumberofnewlicensingregulationsandbureaucraticpaperworkwasgenerated,drivingupthe costofnewplantstothepointofeconomicunacceptability.
TheChernobylnuclearaccident
Thisaccident,whichoccurredon26April1986in Ukraine(thenpartoftheformerSovietUnion),wasundoubtedlytheworstnuclearaccidenttoeveroccurintheworld. Therewasaworldwidereactionfollowingtheaccident, mainlytriggeredbythefearofradiation.Manypublishedarticles,evenbyrenownedacademies,containedpredictionsof ahumancatastropheassigningmillionsofvictimstotheaccident.However,thefactuallyobservedhealtheffectsattributabletoradiationexposurefromtheaccidenthavebeen assessedtobe muchlowerbytheinternationalscientific community(IAEA1996b;Gonzalez1996).
UNSCEARreportedthefollowingradiation-relatedconsequencesfromtheChernobylaccident(UNSCEAR2008a):
• 134plantstaffandemergencyworkers,manyofwhomalso incurredskininjuriesduetobetairradiation,receivedhigh dosesofradiationthatresultedinacuteradiationsyndrome.
• Thehighradiationdosesprovedfatalfor28ofthese people.
• 19survivorshavesincedied(followingthereportingof 2008),buttheirdeathshavebeenforvariousreasons andusuallynotassociatedwithradiationexposure.
• Severalhundredthousandpeoplewereinvolvedinrecoveryoperations,butthereisnoevidenceofhealtheffectsthatcanbeattributedtoradiationexposure,with theexceptionofasubstantialnumberofthyroidcancers attributedtodrinkinguncontrolledmilkcontaminated with 131I.Nopromptcountermeasuresweretaken,which resultedin15fatalities(uptotheyear2005)amongchildren,whoaremuchmoresusceptibletothyroidcancer thanadults.
• Unsurprisingly,theInternationalConferenceon Chernobyl:LookingBacktoGoForward (IAEA2005)concludedthat “Themajorityofworkerswhoparticipated inthecleanupefforts,themanythousandsofpersons evacuatedduringtheearlydaysfollowingtheaccident, andallthosewhocontinuedtoliveincontaminatedareas receivedradiationdosesfromChernobyl-releasedradionuclidesthatwererelativelylowandunlikelytoleadto widespreadandserioushealtheffects.” Thedosesto theseindividualsarecomparabletothosecausedbynaturallyoccurringradionuclidesthatproducearangeof backgroundlevelsroutinelyexperiencedbyeveryone ontheplanet.
Somenotableregionsofhighbackgroundradiationexistinseveralcountriesthatarecausedbyhigherconcentrationsofnaturalradionuclidesinbeachsandsorinsoilor water.TheChernobylexposuresarenotunlikethesenaturallyoccurringareasthatarenotassociatedwithdiscernible radiationhealtheffects.
Buttherewasalsoasocialtragedy mainlycausedby thefearoftheradiationfalloutfromtheunshieldedaccident (itshouldberecalledthatChernobyldidnothaveanycontainmenttomitigatetheconsequencesoftheaccident,instark contrasttothestandardsinnuclearreactorsworldwide).Such radiationawayfromtheimmediatesiteoftheplant,though low,wasmeasurablethroughoutmostofthenorthernregions oftheworld.Asaresult,peoplereactedwithunderstandable fear.Forinstance,themediahysteriainlargepartsofwestern Europeledtoanestimatedadditional40,000abortionsamong marriedwomenduringthepost-Chernobylmonths,allof whichweretheresultoffear(IAEA1996c).Theradiation levelswereneverhighenoughtojustifyevenoneofthose abortions.Somefoodsupplies,manyonlyshowingamodest presenceofradioactivesubstances,wereoftenabandoned, andevendrinkingwaterwassometimeslabeledhazardous forthelocalcitizenry,basedsimplyonfear.
Theinternationalconferencesumminguptheconsequencesoftheaccident(IAEA1996b)includedapopulation
www.health-physics.com
surveyonnon-radiationrelatedsymptomscarriedoutin areasdirectlyaffectedbytheaccidentvs.thoseareasnotdirectlyaffected.Thepopulationsinbothareassufferedabout thesamefearofradiation.Theseresultsshowedthatthefear ofradiationisnotdirectlyrelatedtowhetherpeoplearelivinginareasaffectedornot.
UNSCEARreportedthosepsychologicaltraumasand otherrelatedeffectsattributabletothefearofradiation,indicatingthat “TheChernobylaccidentisknowntohavehad majoreffectsthatarenotrelatedtotheradiationdose.They includeeffectsbroughtonbyanxiety…anddistress…and areessentiallyunrelatedtoanyactualradiationexposure” (UNSCEAR2008b).
Tragically,themostundesirableconsequenceofthehorrificaccidentatChernobylwasthefearofradiationrather thantheaccidentitself.
TheFukushimanuclearaccident
TheFukushimaaccident,occurringon11March2011 inJapan,wastriggeredbyanextremelylargeearthquakeunderthePacificOcean,whichcausedatsunami-generated wallofwater.Thetsunamiinundationhighapproached 33mandtherunuphighwasupto39m,killingtensofthousandsofpeople(IAEA2015a).TheFukushimaDaiichisite consistedofsixnuclearpowerplants.Atthetimeoftheaccident,Units1,2,and3wereoperating,butUnits4,5,and6 wereinplannedshutdown.Theearthquakedestroyedmost electricpowerlinesintheregion,andthethreeoperating plantslosttheirbackuppowersupplieswhentheensuing floodswipedouttheinternalelectricalsupply,includingtheir standbydieselgenerators.Theresultinglossofcoolingtothe threeoperatingreactorsledtocoremeltdownsandasizable releaseofradioactivematerialsintotheatmosphere,resulting indepositsonlandandintheocean.
Authoritiesmandatedtheevacuationandresettlement ofsomethousandsofresidentsandimposedarelocation ofthemfor,insomecases,severalyears.Theresultwasseriousdetrimentaleffectstothosepeople,includingthedeath ofsomeofthemostvulnerable.ButNONEoftheseimpacts weretheresultofradiationexposure.Theradiationlevels werejusttoosmall.
TheassessmentoftheFukushimaaccidentundertaken bytheIAEArevealedthat “dosesincurredbymembersofthe publicwerelowandgenerallycomparablewiththerangeof effectivedosesincurredduetogloballevelsofnaturalbackgroundradiation.” Unsurprisingly,itconcludedthat “noearly radiation-inducedhealtheffectswereobservedamongworkers ormembersofthepublicthatcouldbeattributedtotheaccident.” ThisconclusionagreedwiththeUNSCEARassessmentthat “nodiscernibleincreasedincidenceof radiation-relatedhealtheffectsisexpectedamongexposedmembersofthepublicandtheirdescendants” (IAEA2015b).
UNSCEARestimatedthat “Themostimportanthealth effect[fromtheaccident]isonmentalandsocialwellbeing,relatedtotheenormousimpactoftheearthquake, tsunamiandnuclearaccident,andthefearandstigmarelatedtotheperceivedriskofexposuretoionizingradiation” (UNSCEAR2014).Similarconclusionsandlessonswere reportedbyanICRPTaskGroup(Gonzalezetal.2013). Again,thefearofradiationhasbeenamajorculpritin theFukushimaconsequences.
Globalnuclearpoweradvances
Theadventofnuclearpower,startingwiththefirstemploymentofcommercialnuclearpowerinthe1960s,now providesapproximately10%oftheworld’selectricity.Itis generallyrecognizedbyresponsiblelong-termplannersthat theglobalneedsforelectricitywillcontinuetoclimb especiallyasthepushfortheelectrificationofthetransportationindustrymatures.Butthefearof “anythingnuclear” isimpedingthesociallicensingofnuclearprograms mainlybecauseoffearofradiation.
Nuclearwastecleanup
Oneoftheissuesthatconcernsmanyabouttheacceptabilityofnuclearpoweristhequestionofwhattodowith theso-called “nuclearwaste;” namely,radioactiveusednuclearfuelremovedfromthereactoronceitsusefullifetime togeneratepowerisover.First,weneedtorecognizethat about96%ofthis “waste” isnotwasteatall.Itcanbeconvertedtousefulnuclearfuelsinceitiscomprisedmostlyof uraniumorplutonium.Manycountrieshavedeclaredthat thisisnota “waste” butratheran “asset” tobepreserved. Unfortunately,thecurrentregulationsforthedesignof anundergroundnuclearwasterepositoryintheUnited Statesrequiretheradiationlevelatthesurfaceofsucharepositorytobelessthan0.15mSvy 1 forthefirst10,000y afterrepositoryclosure,whichisabout20timeslessthan naturalbackground.Thisabsurdrestriction,basedonthe unnecessaryfearengenderedbyradiation,makesitalmost impossibletodesignandbuildanuclearwasterepository. Myriadofbenefitsfromradiationasaby-productof nuclearenergy
Anotherfactorgenerallyunknowntothegeneralpublic relatestothemyriadofservicesandproductsthatradiation technologyhasprovidedtomodernlife.Anearlybookaddressingthistopic(Waltar2004)summarizedtheenormous contributionsthatradiationtechnologyisalreadyprovidinginthefieldsofmedicine,agriculture,modernindustry, transportation,spaceexploration,combatingterrorismand crime,artsandsciences,andenvironmentalprotection.This workhasbeenexpandedconsiderablyanddocumentedin therecentElsevierencyclopediaonnuclearenergy (Greenspan2021),whichcontains26chaptersintheSectiontitled “TheMedical,Agricultural,andIndustrialApplicationsofNuclearTechnology.” Thissectionisfocusedon
thesehighlybeneficialcontributionstoourglobalsociety.Already,thevalueofthesecontributionswellexceedsthatof thecommercialnuclearpowerindustry bothintermsof jobsandtheeconomy.Yettherearestillpeoplewhowill notsubmittoacomputerizedtomography(CT)scanbecause ofradiationfear,eventhoughthescienceclearlyshowsthat thebenefitsfaroutweightherisks(McCollough2018). Thereappearstobenoendinsightforthefurtheradvancementofsuchradiationtechnologies,butonlyiftheunsubstantiatedfearoflow-levelradiationcanbecurbed.
CONCLUSION
Thisarticlehasdescribedviewsonthehealtheffectsattributabletoradiationexposuresituationsinvolvinglowdose,lowdose-rate,andlowdose-ratechanges,takinginto considerationtheprincipalscientificprofessionsstudying thistopic;namely,radiationpathology,radiationepidemiology,radiationbiology,andradiationprotection.Itsgoalhas beentopresentanoverviewofthescientificevidence gainedoverthepasthalfcenturythatprovidessufficientassurancethatthereisnovalidreasontofearlowlevelsof radiationexposure.
Thecurrentapproachthatismostusedtoguideregulatorsinprotectingthegeneralpublicfromradiationexposure isreferredtoasLinearNo-Threshold(LNT).Itiscurrently deeplyembeddedintheinternationalradiationregulatory system,yetitisunderstoodverydifferentlybythevarious professionsinvolved,someasapremise,someasahypothesis, andsomeasapracticalmodel.Asaresult,theappropriateness ofhowitisusedishighlydebated.BecauseLNThasbeenunderstoodbymanyasimplyingthatradiationatanylevel,even downtozero,canpotentiallybeinterpretedtobeakillerof peopleandpotentiallymanypeopleoverspaceandtimeifthey areexposedtoeveninfinitelysmalllevelsofradiation,itis nowonderthatmanymembersofthepublicandtheir policy-makersarestillfearfuloftheword “radiation.”
Mostpolicymakerswillagreethatendeavorsinvolvingradiationhavemajorbenefits(e.g.,medical,agricultural,andindustrialapplications)iftheirradiationexposure canbeproperlyharnessed,butitcanbeharmfulifuncontrolled.Thereissolidagreementamongthefullradiation healthcommunitythatunrestrictedradiationexposureat highlevelsisdangerousforindividualsandclearlyshould beprevented.Thereisalsosolidagreementthatexposure atmediumlevelscanincreasethenormalincidenceof healtheffectsassociatedwithradiation(suchasmalignancies,whichcannotbeattributedindividuallybutonlycollectively)andshouldalsobelimited.
Butregardinglowlevelradiation,theconundrumis thattheeffects,eitherdetrimentalorbeneficial,ifany,are fromtheclinicalperspective verysmallanddifficulttobe evidenced.Anyradiationhealtheffectsatlowdose,ifthey
existatall,arealmostalwaysdwarfedbyothertoxinsthat welivewitheveryday,suchasthenaturalbodilyburning ofoxygensoessentialtolife.
AnerredinterpretationoftheLNTradiationprotection modelfeedsdirectlyintopublicfears.Unfortunately,such unsubstantiatedfearisnotwithoutconsequences.Suchfear hasalreadycauseddetrimentaleffectsonfrightenedpeople. Moreover,itisseriouslyrestrictingtheuseofradiationtechnologyinthefieldsofmedicine,agriculture,modernindustry,andenergy.Withtheever-growingneedtoliftbillionsof ourfellowcitizensoutofpovertyandprovidethemwith readyaccesstotheadvancesnecessarytoexperiencea higherqualityoflife,theunsubstantiatedfearofradiation isbecomingamatterofsevereethicalconsideration.
Enormousprogresscanandshouldbemadebyencouragingradiationregulatorybodiestorecognizetheshortcomingsofthepresentlyinterpretedandappliedregulation oflow-doseradiationexposuresituationsandtheneedtorevisitit allowingthemtotakeintoaccountthefactthatradiationdamage(ifany)atlowlevelsisessentiallyinsignificant.Themostsignificantcontributionofsuchregulatory agencieswouldbetoemploytheirworkinamannerclearly demonstratingtoacautiousandsuspectingpublicthatlow levelsofradiationaresimplynottobefeared.Welivein anatmosphereofsuchradiationeverydayofourlivesand shouldnotbealarmedwhensmallamountsofadditionalradiationexposure,usuallysimilartothevariationsinbackground naturalexposure,areintroducedintoourenvironment.
Inconclusion,thereisaclearscientificbasisforremovingtheunnecessaryanddebilitatingfearoflow-level radiation.Oncethisconclusionisacceptedbyapresently confusedpublic,enormousprogressinharnessingradiation processescanbeachievedtobringintobeingthebenefits desiredbyourgrowingglobalhumanity.
REFERENCES
AndererJ,GonzálezAJ.Radiationversusradiation:nuclearenergyinperspective acomparativeanalysisofradiationin thelivingenvironment.IAEABulletin2/1989;1989.
BrehwensK,StaafE,HaghdoostS,GonzálezAJ,WojcikA.Cytogeneticdamageincellsexposedtoionizingradiationunder conditionsofachangingdoserate.RadiatRes173:283–289; 2010.DOI:0033-7587/10.
BrooksAL,MorganWF,FeinendegenLE.2015HealthPhysics Societysymposium,13–14July2015,Healthrisksfromlow dosesandlowdose-ratesofionizingradiation.HealthPhys 110:241–248;2016.
BrooksAL,ConcaJ,GlinesWM,WaltarAE.Howthescienceof radiationbiologycanhelpreducethecripplingfearoflowlevelradiation.HealthPhys125(5):407–424;2023.
CalabreseEJ,DhawanG.Howradiotherapywashistoricallyused totreatpneumonia:coulditbeusefultoday?YaleJBiolMed 86:555–570;2013.
CalabreseEJ.Thelinearno-threshold(LNT)doseresponse model:acomprehensiveassessmentofitshistoricalandscientificfoundations.Chemico-BiologInteract301:6–25;2019.
CalabreseEJ.HowdidHermannMullerpublishapaperabsent anydatainthejournalScience?Ethicalquestionsandimplications ofMuller’sNobelprize.Chemico-BiologInteract368: 110204;2022.
CalabreseEJ,GiordanoJ.EthicalissuesintheUS1956National AcademyofSciencesBEARIgeneticspanelreporttothepublic.HealthPhys123:387–391;2022.
CardarelliJ,HamrickB,SowersD,BurkB.Thehistoryofthelinearno-thresholdmodelandrecommendationsforapathforward.HealthPhys124:131–135;2023.
ClarkeRH,ValentinJ.ThehistoryofICRPandtheevolutionofits policies.Baltimore:ElsevierLtd.;ICRPPublication109;2008. EuropeanCommission.Principlesandmethodsforestablishing concentrationsandquantities(exemptionvalues)belowwhich reportingisnotrequiredintheEuropeandirective.Radiation Protection65;XI-028/93-EN;1993.CommissionoftheEuropean Communities;RadiationProtectionDivision;CentreWagner. L-2920LUXEMBOURG.
FeinendegenLE,PollycoveM,NeumannRD.Low-dosecancer riskmodelingmustrecognizeup-regulationofprotection. Dose-Response8(2):228–252;2010.
FeinendegenLE,BrooksAL,MorganWF.Finaldiscussions,summaryandrecommendations.HealthPhys100:342–343;2011.
FeinendegenLE,CuttlerJM.Biologicaleffectsfromlowdoses anddoseratesofionizingradiation:scienceintheserviceof protectinghumans,asynopsis.HealthPhys114:623–626;2018. FeinendegenLE.Conferencesummary.HealthPhys118:322–326; 2020.
GonzálezAJ.Chernobyl tenyearsafter:globalexpertsclarify thefactsaboutthe1986accidentanditseffects.IAEABulletin 3/1996;1996.
GonzálezAJ.Thedebateonthehealtheffectsattributabletolow radiationexposure.PierceLawReview1:39–67;2002.
GonzalezAJ.Theethicalbasisoftheinternationalprinciplesofradiationprotection.RadioprotecciónXIX:35–47;2011a(in Spanish).
GonzalezAJ.Epistemologyontheattributionofradiationrisks andeffectstolowradiationdoseexposuresituations.IntJ LowRadiat8:172–219;2011b.
GonzalezAJ,AkashiM,BoiceJDJr,ChinoM,HommaT, IshigureN,KaiM,KusumiS,LeeJK,MenzelHG,NiwaO, SakaiK,WeissW,YamashiyaS,YonekuraY.Radiological protectionissuesarisingduringandaftertheFukushimanuclearreactoraccident.JRadiolProtect33:497–571;2013.
GonzálezAJ.Clarifyingtheparadigmonradiationeffects& safetymanagement:UNSCEAR reportonattributionofeffectsandinferenceofrisks.NuclEngTechnol46:467 – 474; 2014a.
GonzálezAJ.Clarifyingtheparadigmforprotectionagainstlow radiationdoses:retrospectiveattributionofeffectsvis-à-vis prospectiveinferenceofrisk.Australasia31:2–12;2014b.
GonzálezAJ.Keynoteaddress:imputabilityofhealtheffectsto low-doseradiationexposuresituations.Nuclearlawinprogress DerechoNuclearenEvolución.In:ManóvilRM,ed.ProceedingsoftheXXIAIDN/INLACongreso;PalacioSanMartín, CiudadAutónomadeBuenosAires,RepúblicaArgentina, 20
23October2014.2014c:69–76.
GonzálezAJ.Dealingwiththeaftermathofanuclearaccident: challenges,lessonslearned,solutions.In:InternationalConferenceonGlobalEmergencyPreparednessandResponse. Vienna:IAEA;2015.Availableathttps://www.oecd-nea-org/ jcms/pl_29289/nea-workshop-on-stakeholder-involvementrisk-communication.Accessedon16May2023.
GonzalezAJ.Thedoseanddose-rateefficiencyfactor(DDRF): unneeded,controversialandepistemologicallyquestionable.
Медицинскаярадиологияирадиационнаябезопасность (MedicalRadiologyandRadiationSafety)62:13–26;2017.
GonzálezAJ.Theconceptofradiationrisk.Preparedattherequest oftheNEA(OECD)'sCommitteeonRadiologicalProtection andPublicHealth.Presentedatthe2ndNEAWorkshopon StakeholderInvolvement:RiskCommunication;Sessionon “RiskCommunication:WhatandWhy;” attheOECDConferenceCentre,Paris,France,24–26September2019(withthetitle:Communicatingtheconceptofradiationrisk:thechallenge ofseparatingfactsfromconjectures,attributionfrominference).2019.Availableonlineathttps://www.oecd-nea.org/ jcms/pl_29289/nea-workshop-on-stakeholder-involvementrisk-communication.Accessedon18May2023.
GonzálezAJ.Emergingchallengesfortheinternationalsystemof quantitiesandunitsforradiationprotection.In:15thInternationalCongressoftheInternationalRadiationProtectionAssociation.EnhancedTopicSession-ET2-UnitsandMeasurement Quantities:ImplicationsofrecommendationsbyICRPand ICRU.2021.Proceedingsofthe15thInternationalCongress oftheInternationalRadiationProtectionAssociation.Seoul, SouthKorea:COEX;18–22January2021.Availableonlineat https://irpa.net/page.asp?id=54839.Accessedon18May2023.
GonzalezAJ.Legalimputationofradiationharmtoradiationexposuresituations.In:Nuclearlaw:theglobaldebate.New York:Springer;2022;141–159.
GreenspanE.Encyclopediaof nuclearenergy.Amsterdam: Elsevier;2021.
HealthPhysics.ProceedingsoftheJointAmericanNuclear SocietyandHealthPhysicsSocietyConference:applicabilityofradiation-responsemodelstolow-doseprotection standards,1–3October2018,Pasco,Washington.HealthPhys 118(3);2020.
InternationalAtomicEnergyAgency.Basicsafetystandardsfor radiationprotection,SafetySeries9.Vienna:International AtomicEnergyAgency;1962.
InternationalAtomicEnergyAgency.Internationalbasicsafety standardsforprotectionagainstionizingradiationandforthe safetyofradiationsources.Vienna:InternationalAtomicEnergyAgency;1996a.
InternationalAtomicEnergyAgency.OnedecadeafterChernobyl:summinguptheconsequencesoftheaccident.In:ProceedingsoftheInternationalConferenceonOneDecadeafter Chernobyl:SummingUptheConsequencesoftheAccident, jointlysponsoredbytheEuropeanCommission,International AtomicEnergyAgency,WorldHealthOrganization,in co-operationwiththeUnitedNations(DepartmentofHumanitarianAffairs).Vienna:IAEA;1996b.
InternationalAtomicEnergyAgency.OnedecadeafterChernobyl: summinguptheconsequencesoftheaccident.In:Proceedings ofanInternationalConferencejointlysponsoredbytheEuropean Commission,InternationalAtomicEnergyAgency,World HealthOrganization,inco-operationwiththeUnitedNations (DepartmentofHumanitarianAffairs.Vienna:IAEA;1996c; 283–318.
InternationalAtomicEnergyAgency.Internationalconferenceon Chernobyl:lookingbacktogoforward.In:Proceedingsofan InternationalConferenceonChernobyl:LookingBacktogo Forward,organizedbytheInternationalAtomicEnergy AgencyonbehalfoftheChernobylForumandheldinVienna, 6–7September2005.Vienna:IAEA;2005;189.
InternationalAtomicEnergyAgency.Fundamentalsafetyprinciples:safetyfundamentals.In:IAEAsafetystandardsseries. Vienna:IAEA;2006.
InternationalAtomicEnergyAgency.IAEAsafetyglossary: terminologyusedinnuclearsafetyandradiationprotection. Vienna:IAEA;2007.
www.health-physics.com
InternationalAtomicEnergyAgency.Radiationprotectionand safetyofradiationsources:internationalbasicsafetystandards. Vienna:IAEA;2014.
InternationalAtomicEnergyAgency.TheFukushimaDaiichiaccident.Vienna:IAEA;STI/PUB/1710¦978-92-0-107015-9; 2015a.
InternationalAtomicEnergyAgency.TheFukushimaDaiichiaccident.Reportbythedirectorgeneral;59IAEAGeneralConference:ReportGC(59)/14.Vienna:IAEA;2015b.
InternationalAtomicEnergyAgency.Attributionofradiation healtheffectsandinferenceofradiationrisks:consideration forapplicationoftheIAEA.Vienna:IAEA;SafetyStandards Series[IAEApreprint];2022a.
InternationalAtomicEnergyAgency.Legalimputationofradiationharmtoradiationexposuresituations(byGonzález,AJ). NuclearLaw:Chapter7.Vienna:IAEA;2022b.
InternationalCommissiononRadiologicalProtection.Problems involvedindevelopinganindexofharm.Oxford:Pergamon Press;ICRPPublication27;1977.
InternationalCommissiononRadiologicalProtection.1990recommendationsoftheInternationalCommissiononRadiologicalProtection.Oxford:PergamonPress;ICRPPublication 60;1991.
InternationalCommissiononRadiologicalProtection.Genetic susceptibilitytocancer.Oxford:PergamonPress;ICRPPublication79;1998.
InternationalCommissiononRadiologicalProtection.Low-dose extrapolationofradiation-relatedcancerrisk.Oxford:Pergamon Press;ICRPPublication99;2005.
InternationalCommissiononRadiologicalProtection.The2007 recommendationsoftheInternationalCommissiononRadiologicalProtection.Oxford:PergamonPress;ICRPPublication 103;2007a.
InternationalCommissiononRadiologicalProtection.Scopeof radiologicalprotectioncontrolmeasures.Oxford:Pergamon Press;ICRPPublication104;2007b.
InternationalCommissiononRadiologicalProtection.Stemcell biologywithrespecttocarcinogenesisaspectsofradiological protection.Oxford:PergamonPress;ICRPPublication131, Ann.ICRP44(3/4);2015.
InternationalCommissiononRadiologicalProtection.Ethical foundationsofthesystemofradiologicalprotection.Oxford: PergamonPress;ICRPPublication138;2018.
InternationalLabourOrganization.ConventiononemploymentInjurybenefits.InternationalLabourOrganization1964[Schedule Iamendedin1980](No.121)];1980.
InternationalLabourOrganization.Approachestoattributionof detrimentalhealtheffectstooccupationalionizingradiation exposureandtheirapplicationincompensationprogrammes forcancer.JointlypublishedbytheInternationalLabourOrganization,theInternationalAtomicEnergyAgencyandthe WorldHealthOrganization.PublicationILO-OSH73.Geneva, Austria:ILO;2010.
KudoS,NishideA,FurutaH,IshizawaN,SaigusaS.Ariskcomparisonbetweenlifestyle,socioeconomicstatus,andradiation: acohortstudyofcancermortalityamongJapanesenuclear workers(J-EPISODE).HealthPhys122:469–479;2022. LindellB.Thehistoryofradiationprotection.RadiatProtect Dosim68:83–95;1996.
LinsleyGS,GonzalezAJ.Exemptionfromregulatorycontrol:an internationalconsensus asummaryofessentialfeaturesand concepts.IAEABulletin3/1988;1988.
LiuX,LiuZ,WangD,HanY,HuS,XieY,LiuY,ZhuM,Guan H,GuY,ZhouPK.Effectsoflowdoseradiationonimmune cellssubsetsandcytokinesinmice.ToxicolRes(Camb)9: 249–262;2020.DOI:10.1093/toxres/tfaa017.
McColloughC.Benefitsofthelowdosesofradiationdeliveredin medicalimaging.In:ANS/HPSconferenceonApplicabilityof Radiation-ResponseModelstoLowDoseProtectionStandards.HealthPhys118(3):187–188;2018.
NationalAcademiesofScience,Engineering,Medicine.Leveragingadvancesinmodernsciencetorevitalizelow-doseradiation researchintheUnitedStates.Washington,DC:NationalAcademiesPress;2022.Availableonlineathttps://doi/org/10. 17226/26434.Accessedon18May2023.
PontificalAcademyofSciences.Biologicalimplicationsofoptimizationinradiationprocedures.Documenta14Conclusions (English,ItalianandFrenchtexts).HolySee;1983.
RosztoczyZR.RootcausesoftheThreeMileIslandaccident.NuclearNews(March):29–32;2019.
UnitedNations.Effectsofatomicradiation.NewYork:United Nations;UNGeneralAssemblyResolution913(X);1955.
UnitedNations.Officialrecordsofthegeneralassembly,sixty-seventh session,agendaitem50Resolution67/112 “Effectsofatomic radiation” adoptedbytheGeneralAssemblyon18December 2012[onthereportoftheSpecialPoliticalandDecolonization Committee(FourthCommittee)(A/67/421)].NewYork:United Nations;2012.
UnitedNations.UNSCEAR2013reporttotheGeneralAssembly withScientificAnnexes;VolumeI;ScientificAnnexA.New York:UnitedNations;2014.
UnitedNationsEnvironmentalProgram.Radiationeffectsand sources.Whatisradiation?Whatdoesradiationdotous?Where doesradiationcomefrom?UnitedNationsEnvironmentProgramme.Nairobi:Kenya;JobNo.:DEW/1937/NA;2016.
UnitedNationsScientificCommitteeontheEffectsofAtomicRadiation.1972reporttothegeneralassembly;Vol.II:scientific annexF:Effectsofradiationontheimmuneresponse.New York:UnitedNations;1972.
UnitedNationsScientificCommitteeontheEffectsofAtomicRadiation.2001reporttothegeneralassembly:Hereditaryeffects ofradiation.NewYork:UnitedNations;2001.
UnitedNationsScientificCommitteeontheEffectsofAtomicRadiation.2006reporttothegeneralassembly Effectsofionizingradiations;scientificannexA:epidemiologicalstudiesof radiationandcancerandscientificannexB:epidemiological evaluationofcardiovasculardiseaseandothernon-cancerdiseasesfollowingradiationexposure.NewYork:UnitedNations; 2006a.
UnitedNationsScientificCommitteeontheEffectsofAtomicRadiation.2006reporttothegeneralassembly;Vol.II:scientific annexC:non-targetedanddelayedeffectsofexposureto ionizingradiation.NewYork:UnitedNations;2006b.
UnitedNationsScientificCommitteeontheEffectsofAtomicRadiation.Reportofthefifty-fourthsession(29May-2June 2006)tothesixty-firstsessionoftheGeneralAssembly.OfficialRecordsSupplementNo.46(A/61/46)paraph31andseq. 2006.NewYork:UnitedNations;2006c.
UnitedNationsScientificCommitteeontheEffectsofAtomicRadiation.2008reporttotheGeneralAssembly;VolII:scientific annexD:healtheffectsduetoradiationfromtheChernobyl accident.NewYork:UnitedNations;2008a.
UnitedNationsScientificCommitteeontheEffectsofAtomicRadiation.ReportoftheUnitedNationsscientificcommitteeon theeffectsofatomicradiationtotheGeneralAssembly adoptedattheCommittee’s56th session(10–18July2008). NewYork:UnitedNations;2008b.
UnitedNationsScientificCommitteeontheEffectsofAtomicRadiation.UNSCEARreporttotheGeneralAssembly(A/63/46) Volume1,AnnexD:Healtheffectsduetoradiationfromthe Chernobylaccident.NewYork:UnitedNations;2008c.
www.health-physics.com
UnitedNationsScientificCommitteeontheEffectsofAtomicRadiation.2012reporttotheGeneralAssembly;VolI:scientific annexA:attributinghealtheffectstoionizingradiationexposureandinferringrisks.NewYork:UnitedNations;2012a.
UnitedNationsScientificCommitteeontheEffectsofAtomicRadiation.ReportoftheUnitedNationsScientificCommitteeon theEffectsofAtomicRadiation;fifty-ninthsession(21–25 May2012)tothesixty-seventhsessionoftheGeneralAssembly.OfficialRecordsSupplementNo.46.Paragraph25(e). NewYork:UnitedNations;2012b.
UnitedNationsScientificCommitteeontheEffectsofAtomicRadiation.2013reporttotheGeneralAssembly:sources,effects andrisksofionizingradiation;Vol.I:scientificannexA:levels andeffectsofradiationexposureduetothenuclearaccidentafterthe2011greatEast-Japanearthquakeandtsunami.New York:UnitedNations;2014.
UnitedNationsScientificCommitteeontheEffectsofAtomicRadiation.2017reporttotheGeneralAssembly;Vol.I:scientific annexB:Epidemiologicalstudiesofcancerriskduetolowdose-rateradiationfromenvironmentalsources.NewYork: UnitedNations;2017a.
UnitedNationsScientificCommitteeontheEffectsofAtomicRadiation.2017reporttotheGeneralAssembly;Vol.I:scientific annexA:principlesandcriteriaforensuringthequalityofthe Committee'sreviewsofepidemiologicalstudiesofradiation exposure.NewYork:UnitedNations;2017b.
UnitedNationsScientificCommitteeontheEffectsofAtomicRadiation.2019reporttotheGeneralAssembly;Vol.I:scientific
annexA:fvaluationofselectedhealtheffectsandinferenceof riskduetoradiationexposure.NewYork:UnitedNations;2019.
UnitedNationsScientificCommitteeontheEffectsofAtomicRadiation.2020/2021reporttotheGeneralAssemblywithScientificAnnexes;Vol.III;annexC:biologicalmechanismsrelevantfortheinferenceofcancerrisksfromlow-doseandlowdose-rateradiation.NewYork:UnitedNations;2021.
WaltarAE.Radiationandmodernlife:fulfillingMarieCurie’s dream.Amherst,NY:PrometheusBooks;2004.
WaltarAE,FeinendegenLE.Thedoublethreshold:consequences foridentifyinglow-doseradiationeffects.Dose-Response18(3): 1559325820949729;2020.
WielandP,GonzálezAJ.Protectionagainstexposuretolow-dose radiation:anevolvingparadigmsustainingregulatorydecisions.In:ScientificConferenceon “ApplicabilityofRadiation Response-ModelstoLowDoseProtectionStandards,” CosponsoredbytheAmericanNuclearSocietyandHealth PhysicsSociety.2018.HealthPhys118(3):240–241;2020. WorldCommissionontheEthicsofScientificKnowledgeand Technology.Theprecautionaryprinciple.Paris:UnitedNations Educational,ScientificandCulturalOrganization(SHS-2005/ WS/21cld/d20151);2005.
YablokovAV,NesterenkoVB,NesterenkoAV,Sherman-Nevinger JD.Chernobyl:consequencesofthecatastropheforpeopleand theenvironment.AnnalsNewYorkAcadSci1181:1–327;2009.