
9 minute read
Aesthetic, Full-Contour Restoration Made with the New Double Screw Technique


Implant-supported maxillary complete rehabilitation with a zygomatic implant in bone loss
Article first published in Clinical Dentistry (2021): Restoring function and reinvigorating overall health. Clinical Dentistry, 1(8): pp 64-6.
Case made at Steger Dental Laboratory in Brunico (Italy) in collaboration with Dr. Andrea Tedesco, specialist in oral surgery and professor at The II Level University Master Course in zygomatic implantology at the University of Pisa.


INITIAL SITUATION
The patient was in good general health, was a heavy smoker, and reported two ineffective treatments caused by implant failures. Due to the pronounced partial edentulism, the patient underwent previous periodontal surgeries, and two left maxillary sinus lifts, both unsuccessful. Tooth migration caused by the severe periodontitis affected aesthetic as well as masticatory function, and the patient reported pain at the touch. The previous unsuccessful surgeries caused the patient psychological distress. The dental treatment described in this article aimed not only to restore the lost function and aesthetic but also to reinvigorate the patient’s emotional and social health.
The patient required complete maxillary and mandibular restorations, produced in a two-step treatment. The present case report describes the treatment carried out for the maxillary arch restoration only, for which a monolithic zirconia full arch was planned. For starters, the maxillary restoration was produced with consideration of the ideal vertical dimension. After a few wearing months, the restoration was used as a basis for the creation of the mandibular prosthesis so that the final result could reproduce a vertical dimension suitable for the patient. This decision permitted not only the finding of the best vertical dimension for the final restoration but also the reduction of stress on the patient, avoiding invasive surgery in both arches all at once.
1 2

3
Figures 1-3: Initial situation: severe periodontitis, tooth migration, and pain at the touch caused the patient psychological distress.





PLANNED TREATMENT AND AVAILABLE OPTIONS
After exhaustive anamnesis and diagnostic evaluation, the situation was clear: the Tc Cone Beam radiography revealed compromised dental elements and a severe left bone atrophy in the upper jaw, where two surgeries for sinus lifts had already been attempted in the past. The planned treatment consisted of complete tooth extraction and subsequent placement of traditional endosseous implants. A zygomatic implant was inserted in the area of the gingiva affected by severe atrophy and compromised by the previous implant failures. For the final restoration, monolithic zirconia was chosen. The choice was made considering the material’s excellent functional and aesthetic properties as well as the possibility to carry out the complete workflow digitally.
The data was then sent to the Steger Dental Laboratory in Brunico (Italy), where the dental technical team designed the required restoration according to a special protocol, including a new working technique, the Double Screw function. In the design software (Zirkonzahn.Modellier), a first set-up was made using the tooth sets available in the Heroes Collection virtual tooth library. The set-up revealed a strong divergence of the implants towards the vestibular area, which would affect the general aesthetic of the final restoration due to the well-visible screw channels in the anterior area.
The use of the Double Screw Metal technique permitted to strike a balance between function, stability, and aesthetics. Using standard working protocols would lead to making one of the following compromises: 1) Aesthetic compromise: vestibular screw channels would be kept and covered with composites, which would be visible on the final result. 2) Function compromise: tooth placement would be changed, moving the upper teeth forward.
In this way, screw channels would appear on the occlusal and palatal areas. However, the occlusion would be different from the patient’s natural one, which might cause musculoskeletal problems.
4
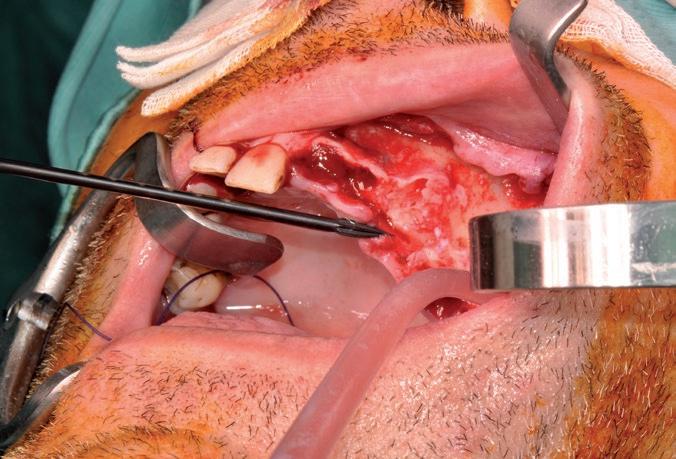
Figure 4: By means of a special surgical bone cutting bur, the dentist pierced the bone to place the zygomatic implant.
5
Figure 5: The final implant placement.
6
Figure 6: X-rays of the oral situation after implant placement. Nine implants were installed by the clinician; however, the patient rejected two implants.
7
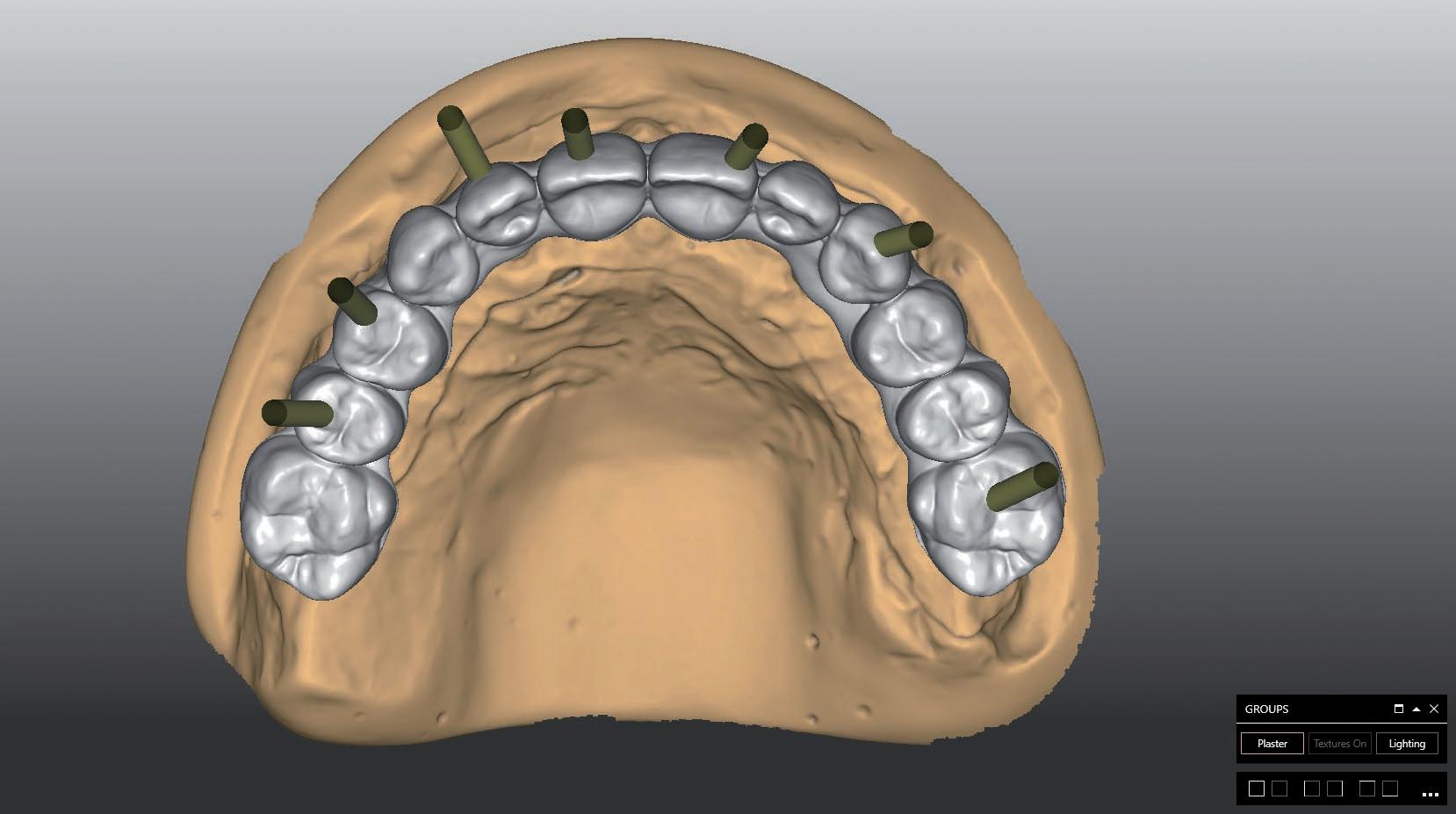
Figure 7: 3D view of the positions of the implants in the implant planning software.
8
9
Figures 8 & 9: The set-up revealed a strong divergence of the implants towards the vestibular area, which would affect the general aesthetic of the final restoration due to the well-visible screw channels in the anterior area.
10
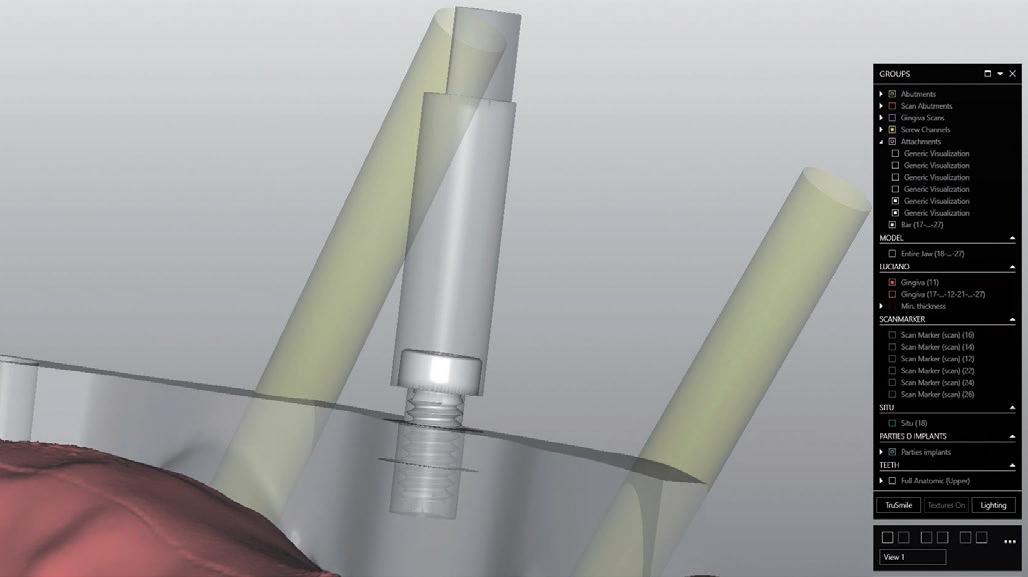
Figure 10: The two discs indicate the ideal screw insertion depth into the bar in order to avoid zirconia breakage and to find the optimal screw seat in the zirconia framework. Figure 11: The Double Screw channel (in grey) and the original channels (in yellow).

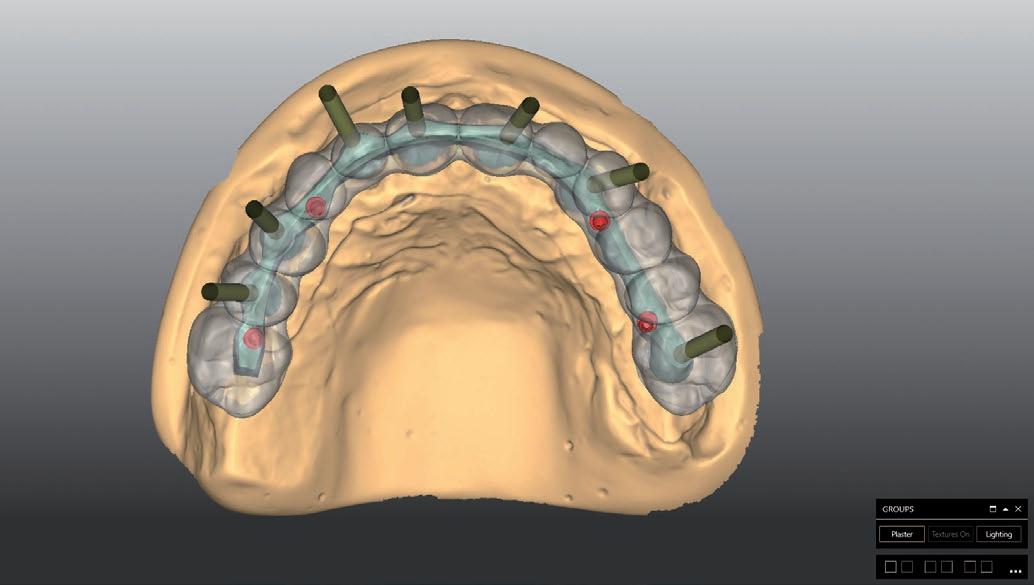
Figure 12: All screw channels (original ones in yellow, Double Screw channels in red). Figure 13: The restoration design with the Double Screw function.

11

12 13

2
The set-up revealed a strong divergence of the implants towards the vestibular area, which would affect the general aesthetic of the final restoration due to the well-visible screw channels in the anterior area. The use of the Double Screw Metal technique permitted to strike a balance between function, stability, and aesthetics without compromising on function or aesthetics.
RESTORATION DESIGN WITH THE DOUBLE SCREW TECHNIQUE
The Double Screw is a special technique that integrates additional screws in the bar design: the innovative concept dictates that the bar is screwed to the implants and the superstructure is screwed to the bar. This avoids non-aesthetic vestibular channels, especially in the anterior region and, at the same time, improves post-operative maintenance and hygiene. In the present case, the primary structure was designed with four additional screw channels to fix the bar to the implants. The software is provided with a new function specific to the Double Screw Metal technique, which permits the visualization of the screw positions as well as the generation of the screw threads within the bar design. The screws are already available in the software function, and the 3D rendering provides the optimal position of the screw channel in the primary structure, as well as the ideal fit of the screw head in the superstructure. The digital screws are provided with several discs indicating the ideal insertion depth to avoid any ruptures in the zirconia framework. The software function also permits the design of the channel thread.

MANUFACTURE AND FINALIZATION
After the design, the bar was milled in Zirkonzahn’s milling unit, and a special bur was used for milling the threaded channel (2G bur for titanium and CrCo). The bar was then digitized and used for the virtual design of the prototype based on the initial setup. The resin prototype was milled and worn by the patient for two months, during which the practitioner could evaluate aesthetics and function.
No adjustments were necessary for the design of the final restoration since the prototype met all functional and aesthetic requirements. The same design was then used to produce the final restoration in Prettau® 2 Dispersive® zirconia*. Prettau® 2 Dispersive® (Zirkonzahn)* is an innovative zirconia with a natural colour gradient already provided during the production phase, simulating the tooth natural shades from dentine to enamel. For this reason, characterization is greatly simplified since manual colouring is no longer required. In the present case, the restoration was customized with Colour Liquids (base colour for intensification of the cervical area; violet and blue for the incisal area) before sintering, and further embellished after sintering with ICE Stains 3D by Enrico Steger. Ceramics was applied only in the gingival areas.




CONCLUSIONS
This treatment showed how the new Double Screw technique permits the production of highly stable, bar-supported rehabilitations, even in complex cases with vestibular anterior implants, without compromising the full arch aesthetics. The final zirconia restoration completely met all practitioner and patient requirements. The success of the treatment results from the good communication between the dentist and dental technician, as well as from the mutual trust established between the two professional figures. In particular, this case report highlights the role of the dental laboratory, which extends beyond mere craftsmanship, providing the dentist with consultancy on the latest material innovations and techniques for improved aesthetics.


*The product’s field of application might vary depending on the country. Contact the product manufacturer for more information.

Stay up-to-date on new working techniques and take part in the wide range of online and face-to-face courses at the Zirkonzahn School – “Die Zirkonzahn Schule” – visit www.zirkonzahn-education.com.

For more information, please contact Elena Chudakova: +39 0474 066 649 (italian time zone), elena.chudakova@zirkonzahn.com, www.zirkonzahn.com.
14 15

Figures 14 & 15: The Double Screw function in the software permits the creation of the threads, which can be milled with high precision using special burs in Zirkonzahn’s milling units.
16 17 18
19 20
Figures 16-20: The natural gradient of Prettau® 2 Dispersive® zirconia* permits to simplify the characterization process since manual colouring is no longer required. In this case, for a more individual result, the restoration was coloured with Colour Liquids before sintering (17). After sintering (18), ICE Stains 3D by Enrico Steger were applied on the teeth to create an individual incisal effect and ceramics were layered only on the gingival area (19 & 20).
21
Figures 21 & 22: The Double Screw bar onto the implants.
22
23
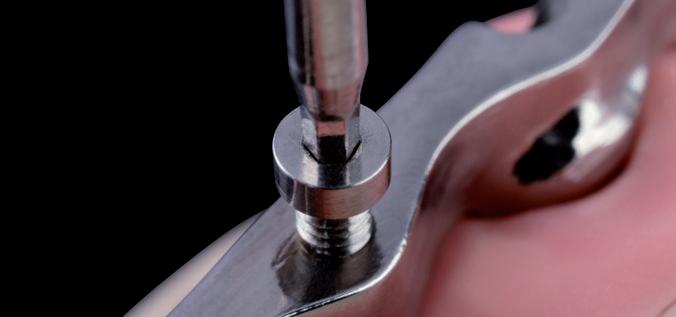
Figure 23: The secondary structure is screwed onto the four additional screw channels milled in the Double Screw bar.
24
Figure 24: Basal view of the final restoration. The bar was anodized in gold to increase the final restoration’s biocompatibility and aesthetic, reducing the grey scale value.
25
Figure 25: The final restoration in situ (note: the present article focuses on the manufacture of the maxillary restoration. The mandibular treatment was produced in a second step, in a shade matching with the colour of the zirconia restoration already in place).

Advice to smile about
The Scotiabank Healthcare+ Dentist Banking Program is designed to support you at every stage of your career. Our dedicated team of Healthcare Specialists offer tailored advice and banking solutions for your unique personal and dental practice financing needs.

