Bringing the community together to solve Indiana's opioid crisis
TEAM A
OPIOID CRISIS
Team A Credits
Coach:
Youngbok Hong, Herron School of Research Team: Kimberly Gottschild, Herron School of Ar t and Design
Robin Brunk, Stephanie Baranko, Nursing - IE-I Nursing - IE-I
Jason King, Nursing - IE-III
Amanda Carmack, Nursing - IE-III
Leah Scalf, Nursing - IE-III
Mohammad Aref, Ravinderjit Singh, Medicine
Sarah’s Story
One patient feels stuck with her pain management options
Sarah, a wife, mother, and dental hygienist in her late thirties, once believed that yoga could cure everything, and didn’t understand why doctors didn’t just prescribe the practice to their patients. It was an unfortunate accident while practicing yoga itself that changed her mind.
“It was a Sunday morning, and I was just exploring my balance and decided I was going to try a forearm stand. It’s a big backbend and I didn’t realize that I didn’t have the flexibility, I basically I fell on my head,” she explains.
Sarah felt an electric-like shock go down her arm, and about an hour later realized she needed to head to the ER, where she discovered that she had suffered a fracture in her neck.
“They said it should heal on it’s own, that it’s a stable fracture. I was evaluated for surgery and was told I didn’t need it.”
In the ER she was given morphine, which didn’t help very much to address the pain, and she was prescribed Vicodin upon release.
But over the course of the next week, Sarah felt an immense pain go down her arm, and the Vicodin was not helping. “I had to call
the people at the trauma center to explain this isn’t working, I need something else,” she recalls.
And immediately she was treated like she was drug seeking.
“I’m very conscious of the perception of people that need or take opiate pain relievers. I have to prepare myself and what I say in my appointments. I do not know how to convey it without being questioned or mistrusted. You have to be honest, but you also have to think of ways to explain it so you can get across that you don’t just want to get high,” she explains.
The extreme pain, she found out, stemmed from a nerve that was being compressed by the fracture. When the bone broke the nerve had been traumatized, and the surgeon she visited said she needed surgery to fuse the vertebrae to relieve pressure on the nerve. She went forward with the surgery, yet the outcome was not as hoped. The pain still remains.
“I had nerve damage from the surgery. Because it’s damaged I have constant muscle spasms and its very painful. The muscle in my neck didn’t heal well because the nerves aren’t healthy. It’s a vicious cycle,” Sarah explains.
The surgeon could only provide her with short term post-operative pain relief. And with changing CDC prescribing guidelines for opioids, many doctors are no longer open to prescribing them at all. When her health insurance changed and she needed a new primary care physician, she was told upfront by her new doctor, upon reviewing her medical history, “We don’t prescribe controlled substances.”
At that point she knew she needed a pain specialist.
“And that’s a whole other thing,” Sarah continues, “because do they specialize in pain? No. They specialize in liability. I’m just there for them to see me and test my urine and know that I’m okay.”
“I don’t think the nurse practitioner I see there has been trained in the injuries or trauma I’ve had or even treatment options. I feel very much like trying different things, but I’m not allowed to go to different doctors. I’m kinda stuck.”
Sarah has done a lot of research on her own and prior to the pain clinic tried multiple other options such as massage, acupuncture, steroid injections, and other medications, but none of them have worked. Botox injections seemed like a good option for her, but health insurance won’t cover it and the two thousand dollar price tag is steep.
Sarah feels frustration over her experience as a patient. Having seen multiple types of doctors during her journey, she has most often felt rushed to tell her same story.
“I didn’t ever really feel like there was a real dialogue that felt effective or problem solving. It always felt like ‘Let’s fix this as soon as we can and get on to the next patient.’ I never felt like there was a true investment in my outcome,” she explains.
“I don’t feel like they understand how much my life has been affected and how it affects every aspect of my life like job, friendships, marriage – everything.”
If Sarah could change anything about her experience as a patient, she wishes she could see a doctor who knew her whole story and can be considerate of the whole picture when evaluating her condition. She’d also rather not to spend time going to a doctor, paying for the officevisit, and waiting to see a doctor once a month.
“At this point,” Sarah says, “I just want to get to a point of treating what I can and that involves treating the pain and living my life the best that I can.”
“I just want off this medication, I want to go back to my natural way of living, and I initially truly believed that would be the outcome. That’s why I had the surgery.”
But now, as her surgeon told her, she is going to have this pain the rest of her life. And treating the pain with an opioid is her only option.
The Patient Experience
Developing an understanding the magnitude of the opioid epidemic in Indiana.
The Patient Experience
Exploring Indiana’s opioid crisis from a human perspective
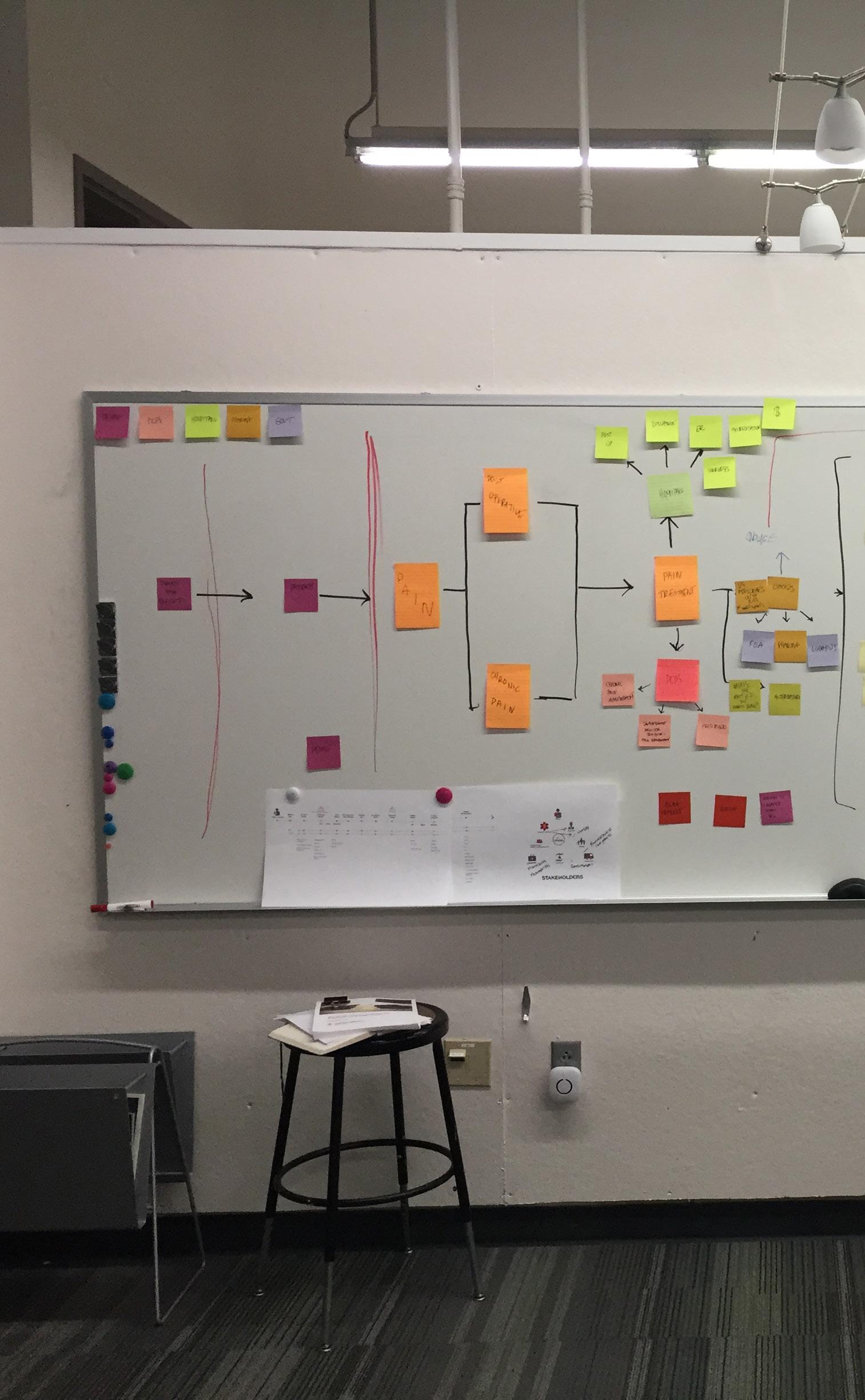
Developing a System Map
Gaining an overall understanding of the opioid epidemic facing Indiana required viewing the crisis from a “5,000” foot perspective. Analyzing the epidemic from afar allowed the research team to see the “forest in spite of the trees” and understand the stakeholders involved and affected, how they are related to each other, and the consequences they experience. At the center of the epidemic, the system map reveals, are non-terminal patients experiencing chronic or post-operative pain.
To the research team, the “Alternatives” touchpoint within the system map proved to be a bright spot among the many opioid related causes and effects that comprise the epidemic. Why not research this gap and explore ways to minimize the effects of the opioid epidemic?
The research team could further identify touchpoints within the “Alternatives” category: Prevention, which encompassed alternative pain management, provider education on pain, and an exit plan for those living with addiction and limiting access to street drugs.
Within these touchpoints, four research areas were defined: educating prescribers, exploring alternative pain management options, minimizing opioid prescriptions, and researching exit plans for those addicted to opioids or taking them for chronic pain.
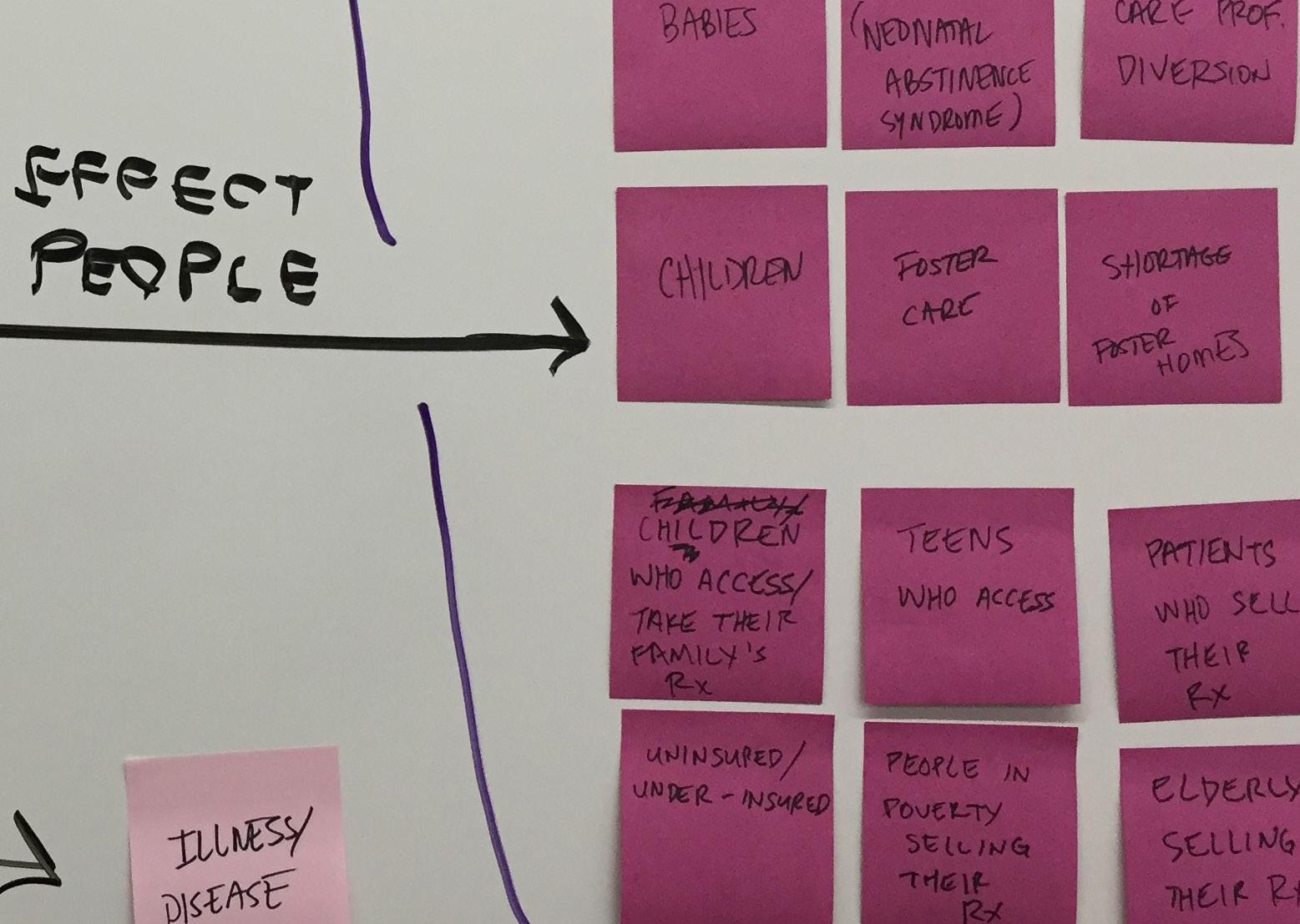
The opioid epidemic has had a devastating effect on the people of Indiana.
Kim explores the multiplem systemic effects of the opioid epidemic.
A
System
Map:
A System Map: Understanding the Opioid Epidemic in Indiana
Understanding the
Indiana
Government/Community Data
Pharmacy Education Initiative
Evidence Based Programs
The Patient Experience
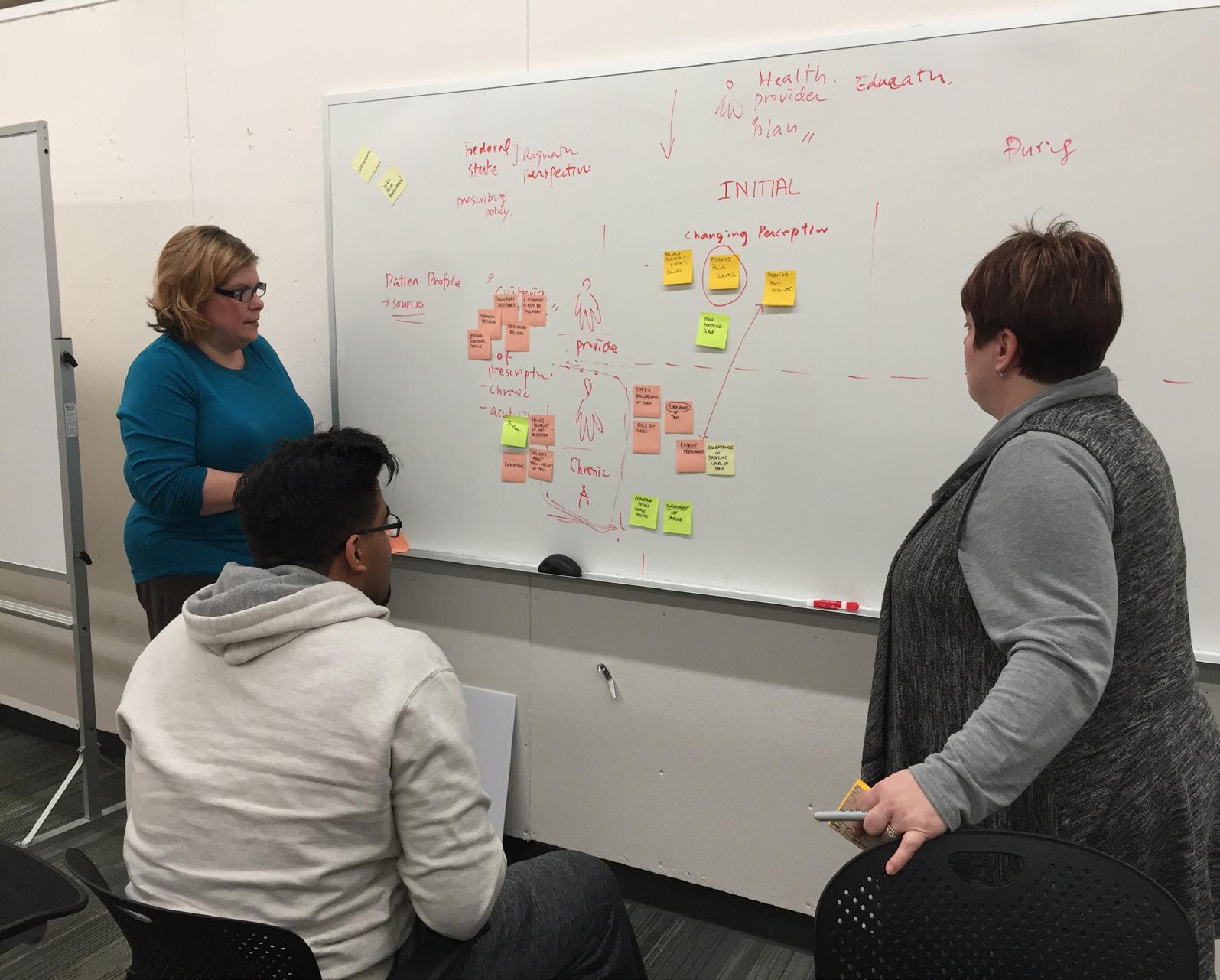
The patient journey mapping process revealed several key touchpoints and opportunities in the chronic pain patient’s journey.
Leah, Amanda, and Rav discuss the culture’s perception of pain as it relates to the patient experience.
Developing a Patient Journey Map
While the System Map is based on rich data gleaned from extensive literature review and an expert panel interview that provided information regarding several aspects of the opioid epidemic on an overarching societal level, the Patient Journey Map shifts focus to a more human centered perspective, analyzing the patient experience.
More specifically, the Patient Journey Map explores the opioid epidemic from “2,500” feet, taking a closer look at patient touchpoints before, during, and after opioid treatment. What do patients like Sarah experience before, during, and after pain treatment? Where are potential opportunities for solutions to support patients in their pain management journey?
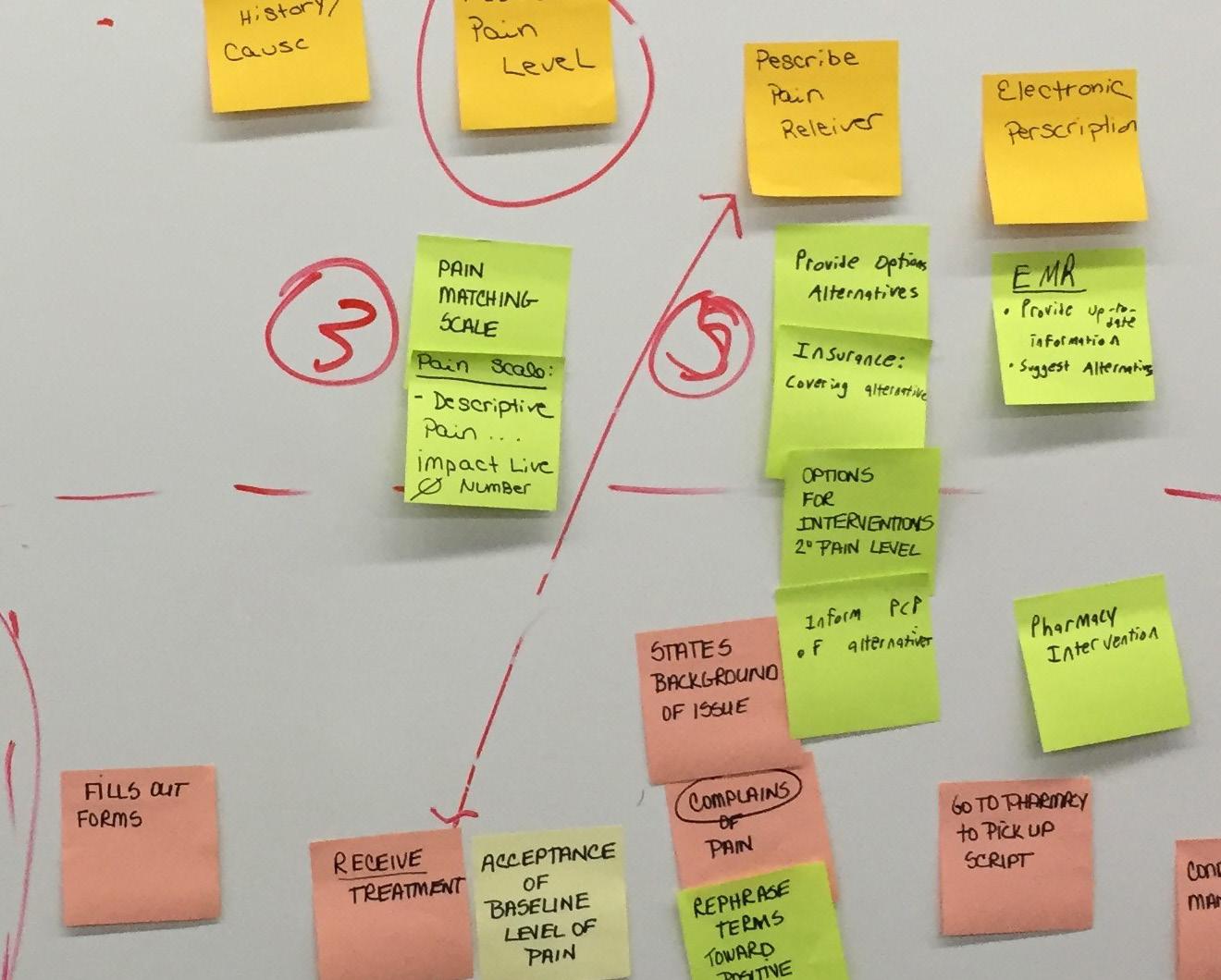
Synthesizing previously defined research areas while incorporating Sarah’s Story revealed several areas of insights such as the American concept and perception of pain in comparison to countries not currently experiencing an opioid crisis, how pain is expressed in American culture, the need for counseling when patients experience pain, life quality issues when pan is experienced, incentives for doctors to prescribe opioids, financial pressures American doctors face, pharmaceutical company influence, and how to support patients who feel stuck in their circumstances.
Ultimately, the Patient Journey Map demonstrates that patients like Sarah experience difficulty in accurately expressing the pain they experience, face stigma when expressing pain, may benefit from counseling when pain levels reduce a patient’s quality of life, and must often advocate for themselves when desiring alternatives or an exit plan.
A System Map:
A Patient/Provider Journey Map:
Understanding the Opioid Epidemic from a Human Perspective Provider Chronic Pain Patient
Before Treatment
Regulatory Pressures
Financial Pressure
Incentives
Pharma Marketing Impact
Minimize Incentives
Spiritual/Emotional Fatigue
Patient Profile Expectations
Beliefs About Pain/ Pain Relief
Trust/Distrust of HCP System
Pre-existing Beliefs Fear
Reciprocal Process
Defining the Problem
Defining the Problem
Reframing problems into opportunities
After developing the Patient Journey Map, the research team identified a recurring theme within the patient experience: empowerment. This led to a preliminary problem statement.
How might we empower patients through engagement before, after treatment?
empower through education and before, during, and
Framing the Solution
Discovering possibilities and turning them into tangible solutions
The team researched and then collaborated remotely via Google Docs and Zoom to frame solutions. The team ideated ways to 1. educate providers on pain management alternatives, 2. provide alternative treatment options, 3. reframe the cultural perception of pain, and 4. provide new vocabulary for the expression of pain before, during, and after treatment.
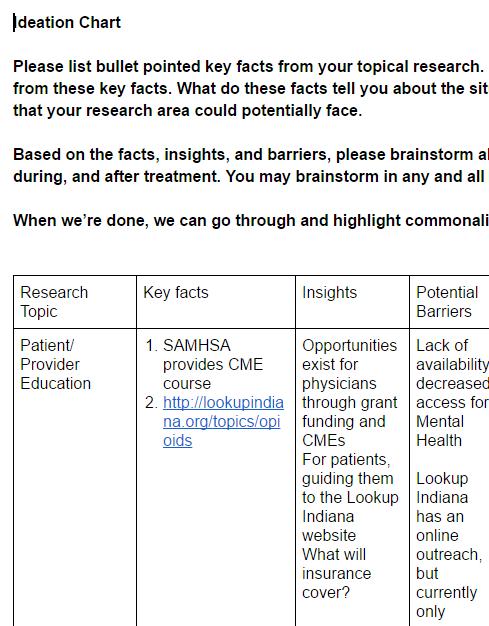
Multiple potential, data-based solutions for developing an empowering patient pain management experience were generated. These ideations comprise the Ideation Map found on pages 20-23.
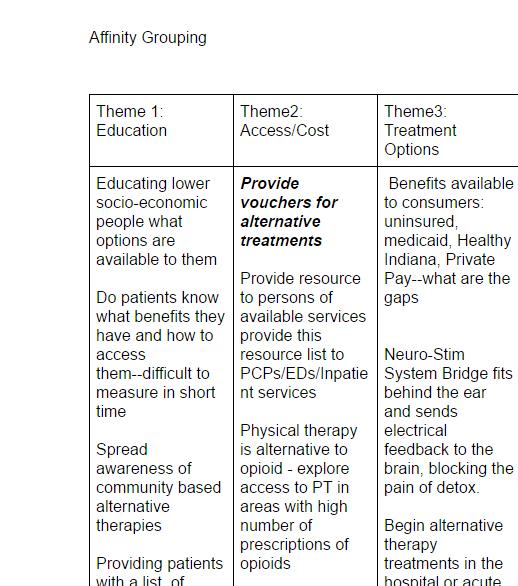
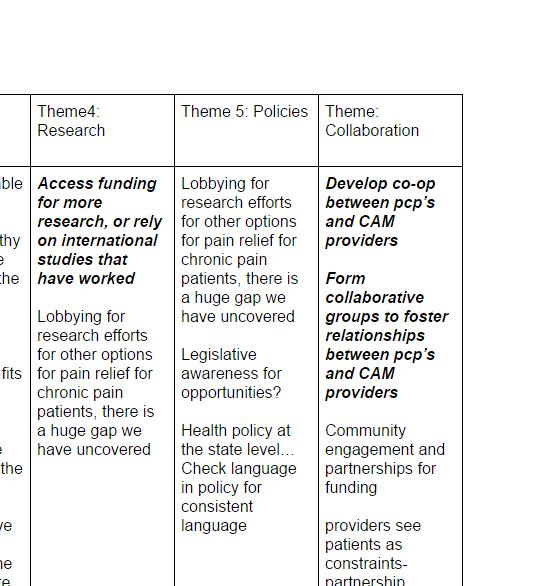
The research team then arranged the generated solution ideas in an affinity diagram (see pages 24- 25) to explore recurring patterns within the ideas. Six dominant solution categories were identified: education, access to and cost of alternative pain treatments, alternative treatment options, research on alternative treatments, health policy, and collaboration among stakeholders.
Collaborating online, the research team generated multiple ways to empower patients.
An Ideation Map:
Framing solutions to address the opioid epidemic
Research Topic Insights
Rephrasing Language
Key Facts
Empowerment is both a process and an outcome.
Rephrasing to strengths based language can increase empowerment in patients
Include patient as partner in pain management plan.
Barriers
Framing the Solution Passive Time to Tendency providers as required and Health Check consistent
Culture of Pain
The use of a self-reporting pain assessment is an effective tool for evaluating pain intensity but patient education about pain management is needed.
Various types of Pain scales http://onlinelibrary.wiley.com/doi/10.1002/ acr.20543/full
A chronic pain scale is available http://www.spineuniversity.com/chronic_ pain_grade_questionnaire_combines_with_ international_classification_of_functioning_ disability
A descriptive pain scale is available https://www.esahq.org/~/media/ESA/Files/ ClinicalTrialNetwork/PLATA/Docs/04A% 20Appendix4APLATAManuscript%20sfMG PQ%20v10%2025FEB2013.ashx
There are no pain scales available that offer pain descriptions and therapeutic alternatives for pain management.
The Ideation Map enabled the team to synthesize research and document data-driven solutions.
The use of a pain scale is vital for communication between patient and provider, but currently there does not appear to be any options that paint the whole picture (descriptive vs quantitative, listing alternative therapies) Lack physicians need pain use alternatives.
How Might We Empower Patients?
Barriers After Treatment Before Treatment During Treatment
Passive recipients.
Time Requires culture change to adapt new language.
Tendency of Healthcare providers see patients as constraints- partnership required investment of time and emotions
Health policy at the state levell
Check language in policy for consistent language
patient there does that
Lack of buy in from physicians regarding the need for an alternative pain scale and also the use of therapeutic alternatives.
system i.e. patient is referred to as partner in treatment.
Make patient aware of Language used as stated previously- seen as passive.
Change to provide patient positive view prior to entering healthcare resources that are available to them to empower them in their care
Create a values based culture through new language that values both patient and pcp
Develop new ways to express pain, which could change pain perspective and experience
Provide materials with new phrases for patients, helping guide them through their options in a way that made address fear that they are experiencing Approach that opioid addiction is a disease process rather than a disorder.
Need better pain scale that allows for patients being able to convey their current state.
Take the fear out of pain, comfort and encourage
Maintain empowering language (i.e. partner in care).
Ensure that everyone on healthcare team is on board with rephrasing( i.e.patient as partner in care) Make sure that all healthcare providers a re aware of resources available.
Change words like ‘complains’ and ‘claims’ to states or says
Use language that relieves fear in patients in materials
Use visuals and graphics to help patients express and understand in new ways - graphics are often more powerful than words and could provide new insight and understanding
Continue to maintain rephrasing toward strength based languageseeing patient as continuing partner in care I
nvite patients to be members or participants in family/patient councils to relay experiences and input on solutions
Provide patients a binder with before, during, and after treatment options in a way that is empowering and relieves fear
Use of pain scale such as chronic pain scale in acute setting with alternatives to opioids for differing pain levels.
Normalize idea that pain can also be a normal part of a healing process to restore function,
Take stigma out of experiencing pain, allow it to be acknowledged and expressed And/or helping patients understand that they will experience pain and use step treatment for freaking with acute pain
Make restoring function priority over reducing pain
Use of pain scale with alternatives for patients to use at home to alleviate/reduce pain to manageable level.
Education that pain may not be completely eliminated, but made manageable.
Often not covered by insurance, so not recommended or prescribed, example list from aetna: http://www.aetna.com/cpb/medical/ data/300_399/0388.html
Doctors are not always aware or taught of alternatives
PBM’s often determine which drugs are available at pharmacies for less, and are paid rebates by pharma and insurance alike
Alternative health insurance coverage, http://www.mygreensurance.com/home
Patients must often self-advocate to receive alternative treatment
CAM therapies don’t have the testing budgets that pharma does
Purdue Pharma paid Merck Medco rebates to be available without prior authorization and with low copayments
Opportunities exist for physicians through grant funding and CMEs For patients, guiding them to the Lookup Indiana website What will insurance cover? Lack access Lookup outreach, available
Perceived by insurance companies to be unreliable
No EBR to support alternative therapies and modalities thus not a covered benefit
Time factor? Trust? Don’t “believe in?”
It’s technically a whole other medical degree, ND, NMD, DO
This potentially prevents alternatives from being prescribed or readily available
A movement is growing to circumvent the traditional system
This could be draining for people who are already suffering
Insurance companies and PBMs require more evidence, but CAM will always lag behind
Financially burdened, patients would probably opt for the low co-pay option rather than CAM
How Might We Empower Patients?
Barriers Before Treatment During Treatment
Lack of availability/decreased access for Mental Health
Lookup Indiana has an online outreach, but currently only available in Northeast Indiana
Insurance companies, out of pocket cost to patient
Lack of communication between conventional and CAM providers
Difficult to adapt curriculum
PBM decision makers, health insurance companies
Accessibility, grassroots, not enough buy in? not covered through work?
Time, energy, money
Money, time,
Corruption, money creates illusion of preference
Provide resource to persons of available services provide this resource list to PCPs/EDs/Inpatient services
Understand what insurance will cover... What if they don't have insurance?
Providing patients with a list of options.
Clearly Explain course of opioid addiction as a side effect to every patient prescribed opioids
Empower pcp’s to suggest or prescribe alternative modalities
Lobbying for research efforts for other pain relief options for chronic pain patients, there is a huge gap
Provide vouchers for alternative treatments
Develop co-op between pcp’s and CAM providers
Access funding for more research, or rely on international studies that have worked
Need to look at the issue of access.
Meet with patients to reinforce alternative treatments to opioids and go over/ provide resource lists
Provide options of viable exit plans
Provide counseling options.
After Treatment
Provide information for patients on how to discontinue opioid use
Develop guidelines for pcps to provide patients for discontinuing opioids
Follow up with patients post treatment to prevent relapse
Provide counseling options.
Neuro-Stim System Bridge fits behind the ear and sends electrical feedback to the brain, blocking the pain of detox.
Rehabilitation versus incarceration
Spread awareness of community based alternative therapies
Begin alternative therapy treatments in the hospital or acute setting ?ED? for patients to experience effectiveness
Insurance companies could spend same money on CAM as they do prescriptions
Physical therapy is alternative to opioid - explore access to PT in areas with high number of prescriptions of opioids
Community engagement and partnerships for funding
Legislative awareness for opportunities
Go back to CAM modalities used before the 90’s.
Framing the Solution
Collaborating remotely via Google Docs, the team identified six dominant solution categories and grouped potential solutions to narrow down options.
Affinity diagram analysis revealed that empowering the patient alone is not enough to address the epidemic. Empowering patients is going to require the involvement of all stakeholders. If the entire community is affected by the epidemic, it’s also going to take an entire community to band together to support those living with pain. A systemic problem requires a systemic solution, the realization of which led the research to the final problem statement development:
How might we create a community space for stakeholders in order to support and empower patients?
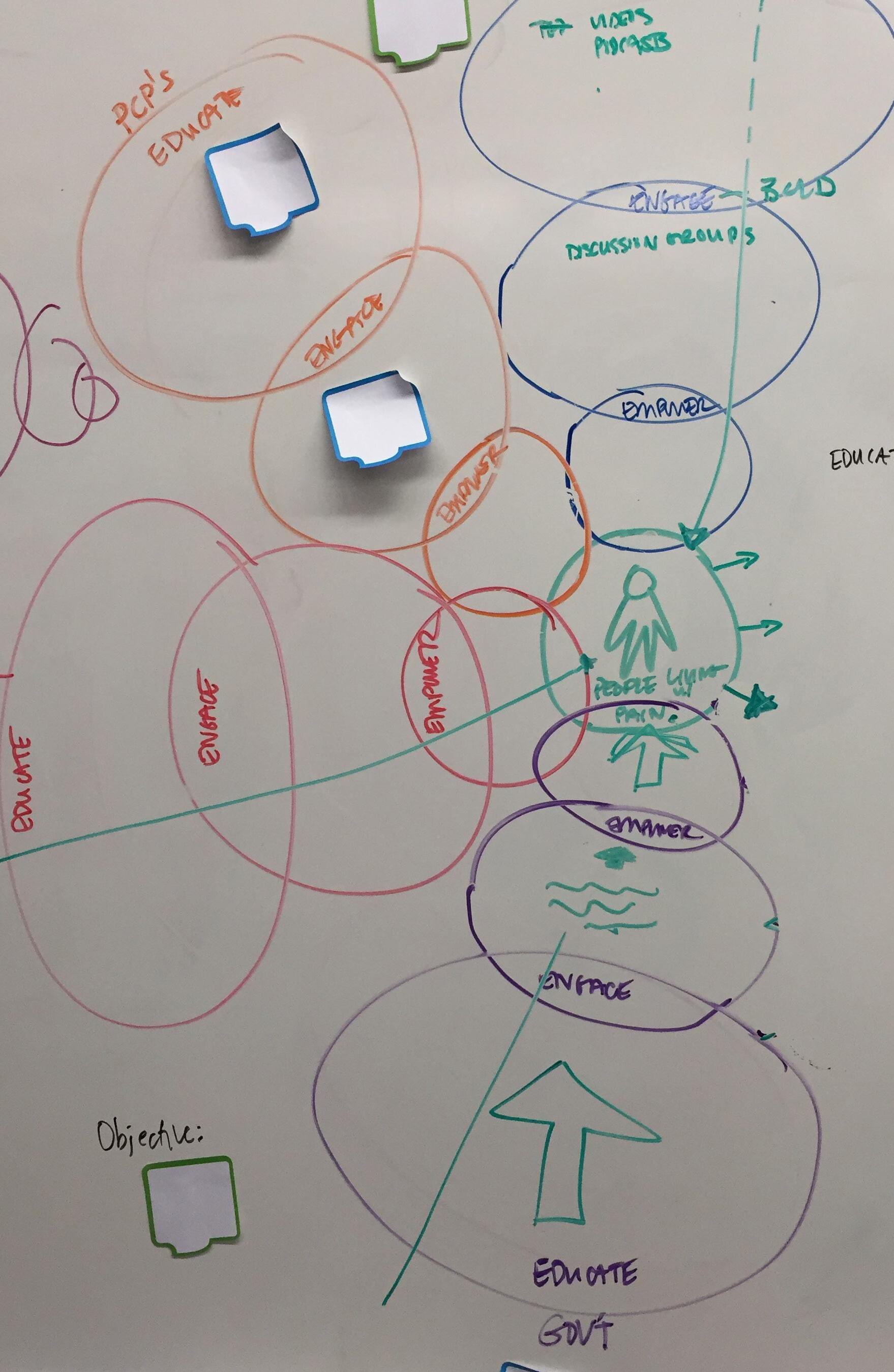
The research team ideated ways to bring stakeholders together, and decided to develop an online community that would educate, engage, and empower stakeholders so that they could, in turn, support and empower patients.
Visualizing solutions on the whiteboard helped the team make sense of their redefined problem space.
A Concept Map:
A Concept Map: Bringing Stakeholders
EMPOWER
ENGAGE Resources Toolkit Connections
The research team ideated ways to bring stakeholders together, and decided to develop an online community that would educate, engage, and empower stakeholders so that they could, in turn, support and empower patients. But:
How would an online community work?
The team developed a methodical tool for online community engagement, framing stakeholder opportunities through a “top-down, bottom-up” model. Moving website visitors from knowing to doing, the community would engage stakeholders in learning opportunities such as educational readings or videos, ways to engage and connect with content and community through online support groups or phone consultations, and opportunities to live out and experience what they have learned via apps or engagement in currently existing resources linked to the website, for example. The online community would serve as a vehicle to unite and draw attention to already existing organizations working to address the opioid crisis.
A Content Development Map:
Developing a methodical tool for online community development
A Content Development Map:
Developing a methodical tool for online community engagement
A Content Development Template per Stakeholder
Objective: Specific to each stakeholder
Educate
Read-Write
Learn
Resources:
• Readings • Learing Modules
Tookit:
Printable Resources
Apps
Links to Resources
Example Content Model: People Living With Pain
Objective: People living with pain will be empowered to manage their pain
Educate Learn
Culture of Pain Perception of Pain Alternatives Self-empowerment and Expression Opioid Risks
Read-Write Learners Visual Learners
• Readings
• Learing Modules
Auditory Learners
Kinesthetic Learners
• Videos • Podcasts
Empower
Tookit:
Printable Resources: Sliding Pain Scale Care Binder
Links: Telemedicine
CAM Resources Community Resources Mountainside Dixon Chiropractic
Books: Designing Your Life
Apps: SuperBetter
• Learning Apps
• Games
Mentors Facebook Groups
Discussion Boards Collaborative Groups
A Content Development Map (Cont’d):
Developing a methodical tool for online community development
A Content Development Map (Cont’d):
Developing a methodical tool for online community engagement
Example Content Model: Primary Care Physicians
Objective: PCP’s will be educated on best practices
Educate Learn
Read-Write
Empower
Apply
Resources: Federal Opioid Treatment Standards INSPECT ICAADA
• Readings
• Learing Modules MAT (Medication Assisted Treatment) Training
• Videos • Podcasts
• Learning Apps
Printable Resources
Tookit: opioidmanager.com POIT
Apps: PAIN Map POIT
Links to Resources
• Discussion Boards Collaborative Groups Networks Network with CAM providers Facebook Groups
Example Content Model: Community Members
Objective: Community members at-large will be educated and encouraged to get involved
Educate Learn
Risks of sharing prescription drugs
Pain management options The consequqnces of the epidemic
Read-Write Learners Visual Learners
• Readings
Dreamland
• Learing Modules
Auditory Learners
• Videos • Podcasts
Kinesthetic Learners
Empower
Apply
Tookit:
Volunteer Resources: Overdose-lifeline.org Centerstone.org Volunteerhq.org Eskenazi Health
Links: Community Resources
Books: Apps:
• Learning Apps
• Games
Facebook Groups
Become a Mentor
Discussion Boards Collaborative Groups
The research team works together to develop a strategic plan.
Project Outcomes
Developing a strategic plan for implementation
The research team developed a strategic planning outline for online community development.
Ideally, an online community of stakeholders would be created with the stakeholders themselves. Stakeholder input would create meaningful content and ensure a valuable and engaging user experience.
Among those stakholders, currently existing organizations and resources adressing the opioid crisis in Indiana, such as addiction treatment centers, would be invited to be an integral part of the community development. Incorporating organizations and non-profits already working to support people affected by the opioid epidemic would unite and bring attention to all the good work being done. Uniting currently existing organizations within the community would not only be built-in PR for the community, but would strengthen collective efforts to minimize the opioid epidemic and its consequences in Indiana.
Grant funding would need to be secured to hire professionals for web development, public relations, and website hosting. Ongoing website management would require funding, as well.
Robin concentrates on developing the team’s strategic plan.
A Strategic Planning Map:
I. Proposed Online Community Development
1.Stakeholder input: Volunteer stakeholders will participate in design sessions to decide what content is necessary and valuable
Journey Development 1.Stakeholder involvement
2.Expert input: Content area experts will engage in design sessions to develop appropriate content
II. Implementation
a. Substance Abuse Prevention and Treatment Block Grant (SABG) through the Substance Abuse and Mental Health Services Administration (SAMHSA)
ii.Project is in alignment with SAMHSA’s six strategic dimensions of recovery
A professional web development team be required
professional web development team will required Prototyping
1. Stakeholder focus groups: Stakeholders will engage in website prototyping sessions
2.Continued development
Evaluating and Selecting
1. Stakeholder focus groups will evaluate and select prototyp for implementation
Conclusions
Ultimately, an online community engages real people. People are at the heart of the opioid epidemic and the heart of the solution. No one stakeholder group, no one person, can go this alone.
Patients expriencing pain, like Sarah, deserve options, resources, empathy, understanding, and support.
The research team sincerely hopes that through coming together Indiana can create a better tomorrow for its people. Together, we can improve quality of care and life for our residents, our families, and our friends.
References
Cramer, M. E., & Wendl, M. J. (2015). Children’s Agricultural Safety Network: Evaluating Organizational Effectiveness and Impacts. Journal Of Agro medicine, 20(2), 105-115. doi:10.1080/1059924X.2015.1010067
Duwve, J., MD, MPH, Hancock, S., MPH, Collier, C., & Halverson, P., Dr.PH. (2016). Report on the toll of opioid use in Indiana and Marion county. (pp. 1-168, Rep.). Indianapolis, IN: Richard M. Fairbanks School of Public Health.
Indiana State Department of Health. (2016). 2016 Indiana special emphasis report: Drug overdose deaths. Retrieved from http://www.in.gov/isdh/files/2016%20ser%20.pdf
National Council on Alcoholism and Drug Dependence, Inc. (2017). Drug Overdose: A medical emergency. Retrieved February 19, 2017, from https://www.ncadd.org/get-help/get-immediate-help/drug-overdose-emergency
Pew Research Center. (2017). 13% of Americans don’t use the internet. Who are they? Retrieved from http://www.pewresearch.org/fact-tank/2016/09/07/some-americans-dontuse-the- internet- who-are-they/
Volkow, N. D., & McLellan, A. T. (2016, March 31). Opioid abuse in chronic pain: Misconceptions and mitigation strategies. The New England Journal of Medicine, 1253-1263. http://dx.doi.org/10.1056/NEJMra1507771
National Institute on Drug Abuse. Medication-Assisted Treatment for Opioid Addiction in Opioid Treatment Programs: Treatment Improvement Protocol (TIP) Series, No. 43. Center for Substance Abuse Treatment. Rockville (MD): Substance Abuse and Mental Health Services Administration (US); 2005. Report No.: (SMA) 12-4214.Retrieved on February 26, 2016 https://www.ncbi.nlm.nih.gov/books/NBK64164/
Nora D. Volkow, M.D., Thomas R. Frieden, M.D., M.P.H., Pamela S. Hyde, J.D., and Stephen S. Cha, M.D. Medication-Assisted Therapies — Tackling the Opioid-Overdose Epidemic. N Engl J Med 2014; 370:20632066May 29, 2014DOI: 10.1056/NEJMp1402780 retrieved from http://www.nejm.org/doi/full/10.1056/NEJMp1402780#ref3 https://www.icaada.org/credentials/mats
Substance Abuse and Mental Health Services Administration (2017) Opioid Use Disorder. Retrieved February 22, 2017, from https://www.samhsa.gov/disorders/substance-use#opioid-use-disorder
Substance Abuse and Mental Health Services Administration. (2016). Substance abuse and mental health block grants. Retrieved February 23, 2017, from https://www.samhsa.gov/grants/block-grants
Brooks, M. (2016, February 4). FDA unveils sweeping changes to opioid policies. Retrieved January 26, 2017, from http://www.medscape.com
Electronic Prescriptions for Controlled Substances Clarification, Department of Justice. § 21 CFR Parts 1300, 1304, 1306, and 1311 (2011)
Emergency Rule, Title 844 Medical Licensing Board of Indiana. §§ Section 1-Section 12 (Medical Licensing Board of Indiana 2013).
Prescription Drug Abuse Task Force. (2014). The Opioid Epidemic and the new Indiana Medical Licensing Board Opioid Laws [PowerPoint slides].
U.S. Department of Justice - Drug Enforcement Administration. (2013). National drug threat assessment summary (DEA-NWW-DIR-017-13). Washington, DC: U.S. Government Printing Office.
The authors and designers of this work grant limited permission to produce derivative works from the ideas and designs contained in this book for use only in nonprofit, educational, and community outreach settings. Commercial production of works based in whole or in part upon the ideas and designs contained in this book are strictly forbidden without the prior written permission of the copyright owners.
Scanning, uploading, and/or distribution of this book, or any designs or photographs contained herein, in whole or in part (whether re-drawn, re-photographed, or otherwise altered) via the Internet, CD, DVD, E-zine, photocopied handouts, or any other means (whether offered for free or for a fee) is permissible only within non profit, educational, or community outreach settings. Reproduction for commercial purposes without the expressed written permission from the copyright owners is illegal and punishable by law.
The copyright owners and publisher of this book appreciate your honesty and integrity and ask that you do not participate in or encourage piracy of copyrighted material.