Detailed Project Report

1
Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
Detailed Project Report
2
ESTABLISHMENT OF SUB CENTRE AT YEROOR DETAILED PROJECT REPORT SUBMITTED TO GOVERNMENT OF KERALA PREPARED BY RESUL POOKUTTY FOUNDATION DECEMBER 2020
Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
Table of Contents
Particulars Page No. Declaration 6 Acknowledgement 7
1. Salient Features 8 2. Executive Summary 11
3. Project In Detail
3.1 Introduction 16 3.2 Project Background 20 3.3 Project Objective 30 3.4 Project Methodology 31 3.5 Scope of Work 32 3.6 Overview of the Project Area 34 3.7 Project Concept in Nutshell 43 3.8 Need for the Project 3.8.1 Existing Situation Analysis 45 3.8.2 Requirement /Demand Analysis 46 3.9 Environmental & Sustainability Aspects 50
4. Site
Tests 4.1 Land Survey 51 4.2 Market Survey 54 4.3 Topography Survey 119 4.4 Facility Survey 120 4.5 Geotechnical Survey 129 4.6 Pollution Test 129 4.7 Water Quality Test 129 4.8 Noise Test 129
Surveys, Investigations &
5. Project Design & Project Components
Report
3
Detailed Project
Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
5.1 Functional Design of the Project 130 5.2 Value Engineering 146 5.3 Engineering Design 151 5.4 Power Supply & Distribution 157 5.5 HVAC 161 5.6 Fire Fighting 164 5.7 Plumbing & Storm Water Management 166 5.8 Rain Water Harvesting 173 5.9 Landscaping 173
Particulars
Sub Centre – Yeroor Grama Panchayath
Page No.
5.10 Internet Facility 174
5.11 Security System 175
5.12 Audio Visual System 175 5.13 Cabling and Switching 175 5.14 Office Automation 176 5.15 EPABX System 176 5.16 Nurse/Doctor Calling System 176 5.17 Waste Management Facilities 178 5.18 Statutory Clearances and Approvals 180
6. Quantity & Cost Estimates
6.1 BOQ & Cost Estimates – Buildings and Civil Works 182 6.2 BOQ & Cost Estimates – Power Supply & Distribution 192
6.3 BOQ & Cost Estimates – HVAC 204 6.4 BOQ & Cost Estimates – Plumbing & Storm Water Management 207
6.5 BOQ & Cost Estimates – Fire Fighting 214 6.6 BOQ & Cost Estimates – Low Voltage Systems 214
6.7 BOQ & Cost Estimates – Waste Management Facilities 223 6.8 BOQ & Cost Estimates – Furniture & Fixtures 223 6.9 BOQ & Cost Estimates – Medical Equipment 224 6.10 Projections of Preliminary Expenses, PMC Charges & Contingencies 228 6.11 Analysis of Rates 229 6.12 Summary of Cost Estimates 229
8. Operations & Management
Resul Pookutty Foundation
Detailed Project Report
4
7. Project Management 7.1 Project Management Organisation & Quality Management 231 7.2 Contract Management Strategy 233 7.3 Project Implementation Schedule 234 7.4 Commissioning of Project 235
8.1 Hospital Management Plan 235 8.2 Service Offerings 239 8.3 Operations and Upkeep 240 8.4 Waste Management 241 8.5 Public Relations 241 8.6 Pharmacy Operations 242 8.7 Drug Situations 243
Particulars
Project
Sub Centre – Yeroor Grama Panchayath
Page No.
8.8 Manpower Matrix 245
9. Project Impact Assessment
9.1 Benefits envisaged from the Project 245
9.2 Projections of Patient Inflow 251
9.3 Cost Benefit Analysis 252
10. Financial Analysis
10.1 Summary of Project Cost 254
10.2 Monthly Cash flow Requirement 254
10.3 Revenue Estimates 256
10.4 Estimates of Recurring Expenses 256
10.5 Sources of Funds 257
11. Conclusion
258
Annexures 258
Annexure – 1 – Topography Report
Annexure – 2 – Soil Test Report
Annexure – 3 – Water Test Report
Annexure – 4 – Pollution Test Report
Annexure – 5 – Detailed Drawings
Glossary
Resul Pookutty Foundation
5
Detailed
Report
DECLARATION
This is to certify that this Detailed Project Report for establishing a Sub-Centre at Yeroor, Anchal Block Panchayath has been prepared after validating the need for such an infrastructure at the proposed location. A market study has been commissioned to understand market demand and to assess the infrastructure gap in the project location. The project has been designed and proposed as per the IPHS standards for Sub-Centre released by Ministry of Health & Family Welfare, Govt. of India. Rates prescribed in Delhi Schedule of Rates (DSR) 2018 has been factored wherever applicable and the best market rates are taken where DSR is not applicable in finalising the outlay for the project. The project has been designed and proposed in strict compliance with all government laws applicable.
6
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
*
* * *
ACKNOWLEDGEMENT
We hereby acknowledge our sincere gratitude towards organisations and individuals who supported us in the selection of this project and successful completion of the Detailed Project Report. We place on record our gratitude to officials of Govt. of Kerala, Department of Health & Family Welfare, National Health Mission, Aardram etc. The wholehearted support of elected representatives and officials of Anchal Block Panchayath and Yeroor Grama Panchayath for the project has been very helpful and requires a special mention. We do place our sincere thanks to everyone contributed in the preparation of this DPR including the sectoral experts, technical agencies and consultants who provided their expertise in the Project.
7
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
1. Salient Features
Sl. No. Particulars
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Description
Detailed Project Report for establishing a Sub Centre at Yeroor Grama Panchayath and maintaining the facility for a period of 2 years 2 Details about the Project Location i. District Kollam ii. Taluk Anchal iii. Panchayath Yeroor iv. Assembly Constituency Punaloor 3 Implementing Agency Resul Pookutty Foundation (RPF) 4 DPR prepared by Resul Pookutty Foundation (RPF) 5 Project Outlay INR 293.64 Lakhs 6 Budget To be funded by Resul Pookutty Foundation. No Govt. Budget required for the project, other than the land. 7 Administrative Sanction 8 Nature of the Project New building the infrastructure required for establishing a Type A Sub-centre with all modern facilities 9 Present Status of Existing Buildings if any Existing building is 20 yrs. old and not suitable to step up the operations the Sub Centre as per the IPHS standards 10 Need for the Project Existing facilities in public health infrastructure are not suitable for the effective delivery of Healthcare services. No facility of e-health services existing in the project location. 11 Details of proposed building A modern two storied Pre-engineered building is proposed i. Number of blocks proposed 1 ii. Number of storeys of building 2 iii. Total area of each block Total area is 6000 Sq.ft iv. Other details of building 13 Details of Investigations/Surveys conducted
1 Title of the Project
Resul Pookutty Foundation
Topography Survey Soil Test Water Quality Test Pollution Test Reconnaissance Survey Facility Survey
8
14 Total estimated cost with item wise cost break up and details of Schedule of Rates
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Project Component
INR Lakhs
BUILDING & CIVIL WORKS 122.20
ELECTRICAL 14.03 AIRCONDITIONING 4.39
LOW VOLTAGE SYSTEM 12.87 PLUMBING 17.07
FIRE & SAFETY 0.16 FURNITURE 3.86 WASTE MANAGEMENT 2.50
MEDICAL EQUIPMENTS 13.64
PRELIMINARY EXPENDITURE 15.97
CONTINGENCY 24.60
PMC 18.50
TOTAL 249.80
The estimates are taken with DSR 2018 and competitive quotations wherever applicable. Apart from the Cost of establishment an additional provision of Rs.43.82 Lakhs also provided for the maintenance of the facility and Public Relation of the project for a period of 2 years 15
Whether detailed estimate attached? Detailed Estimates and BOQ are included in section 6 of the DPR 16
Whether technical specifications of the medical equipment attached, if any?
The Specifications and other details are given in section 5 of the project 17
Since the project is to construct the facility and transfer to Govt. of Kerala, no revenue projections are applicable. 18
19
Details of revenue streams
Details of Cost Benefit Analysis
Details of project management organisation strategy
The project expects a considerable savings in terms of healthcare spend by the public with improve usage of Public health facilities than the private healthcare facilities
RPF will be putting a Project Management Organisation for the professional Project Management and implementation of the project. The details of PMC are given in Section 7.1
Resul Pookutty Foundation
9
20
21
Details of contract management strategy
Details of Project Implementation Schedule (PIS)
22
Details of statutory clearances
23 Quality control infrastructure and mechanism
24 Operations & Maintenance (O&M) arrangements of the project after completion
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
E-Tendering process will be used for the award of the contact. Details given vide section 7.2
The Project is planned to complete with 8 months from the date of sanction. The detailed Project Implementation Schedule is given vide section 7.3
Building Permit to be obtained from the LSGI Licence Operate also shall be taken
Standards of IPHS is followed in the design and construction of the project
Once the project is completed, the facility will be transferred to Govt. of Kerala for operation. However it is proposed that RPF will take care of the buildings and facilities for a period of 2 years from the date of commissioning
25 Details of attached drawings Details are given in Section 11
26 Other attachments Survey/Study reports
Resul Pookutty Foundation
10
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
2. Executive Summary
India is country with mixed healthcare system where Public & Private Health Service providers playing a major role in the delivery of healthcare. Private healthcare institutions has also played a major role in building a healthy community but the access to these private healthcare services for poor and rural public are restricted/limited mainly due the cost and affordability. For the Rural patients, accessibility is also a major issue since most of these private hospitals are located in urban areas.
The recent Covid-19 pandemic has proved the need for robust public health institutions with adequate infrastructure and modern facilities for quick response and effective solutions. Kerala got a typical situation in terms of usage of public health infrastructure. The underutilization mainly comes from the quality perception by the public influenced by their exposure to private healthcare services. The public sector is unable to meet the demands for health care and the people of Kerala have responded to these inadequacies by increasing private sector use. The burgeoning private sector raises household health care expenditures, making health a commodity purchased by ‘ability to pay.’ Many public facilities remain underutilized.
Kerala has made significant strides in public health through investing in infrastructure, decentralized governance, and community engagement. Kerala is working towards making health care accessible, affordable, and responsive to an increasing burden of noncommunicable diseases. Currently the public health outlook of Govt. is shifting from curative models to preventive and promotive healthcare services. In order improve the public confidence on the Public Health Institutions, serious investment in terms of Infrastructure, technology and professionalism is highly essential.
By recognising the need and importance of the case, Resul Pookutty Foundation (RPF), a Notfor-Profit Organisation started by Resul Pookutty, international Celebrity sound designer and an Oscar Award winner came forward with a novel project to upgrade the Healthcare Delivery Network and to equip the same with modern healthcare technology solutions.
11
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
RPF has chosen Anchal Block Panchayat, Kollam District as the project area for the proposed intervention. RPF intends to fund this project and dedicate this to his hometown as he firmly believes that ``everything starts with Good health”.
The proposal for the upgradation of Healthcare Delivery System Anchal Block Panchayat comprises of re-building of the following institutions
• Community Health Centre (CHC)
• 5 Public Health Centres (PHC)
• 28 Sub Centres (SC)
• Implementation of E-health facilities across this network
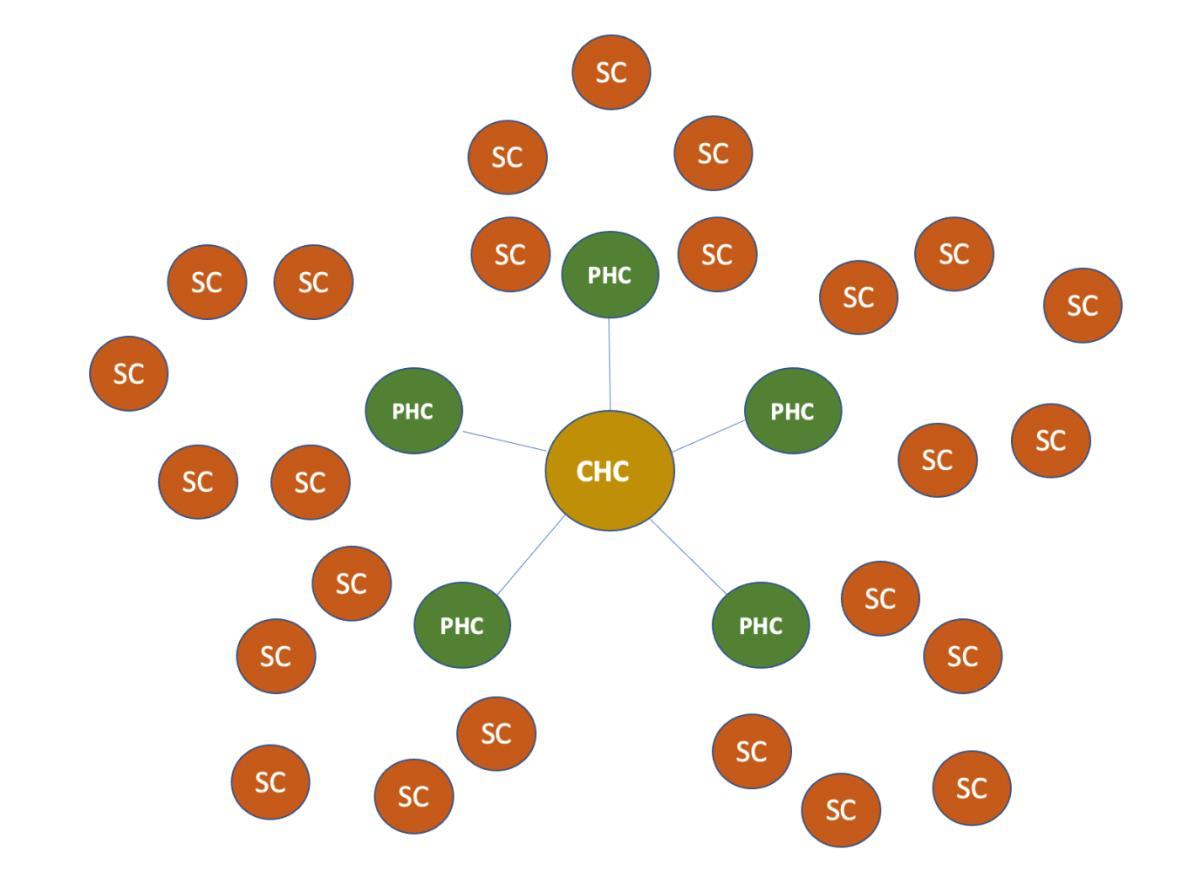
The conceptual framework of the three-tier Healthcare delivery model is given below:
Resul Pookutty Foundation
12
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
The CHC will be established in Anchal and PHCs will be established in Anchal, Yeroor, Edamulakkal, Karavaloor and Alayamon. 28 sub centres will be created under the PHCs as feeder clinics.
The E Health network will enable seamless connection of all the Sub Centres with PHCs and PHCs are in turn connected to the respective CHC. The E Health facilities in Sub Centre, PHCs and CHC will help to keep pace with the advances in medical knowledge, diagnostic procedures, storage and retrieval of information.
It is proposed to establish one Sub Centre as a Pilot Project for this master plan. The current proposal as per this DPR presents the detailed plans and estimates of the Sub Centre to be established at Yeroor.
The land for the project has been allotted by Govt. of Kerala for the construction of Sub Centre. Detailed evaluation of the site with all required studies and surveys performed for the planning of the facility. A detailed market study also performed to assess and validate the need for this project.
After considering multiple options from a value engineering standpoint, a two-storiedengineered building of 6000 sq.ft Is proposed for the Sub Centre. The building will be constructed with a modern outlook and world class design. The building will house all required facilities as
• Rooms for Doctors, JPHN, Asha Workers, Immunization
• Dedicated rooms for caregiving, feeding, immunization
• Provision for Pharmacy, Training Hall, Yoga Rooms
• E-Health Facilities
• Staff Quarters for Doctors and healthcare professionals
• General Facilities including air condition, solar power, surveillance systems etc. at par with any other private hospitals/clinics
The proposed Sub Centre has been envisioned and planned with the standards laid down in the IPHS standards released by Ministry of Health & Family Welfare, Govt. of India. The Sub Centre will be delivering the all required health services as mentioned in the IPHS standards except Intra-natal services. E-health services will be in addition to what is mandated through IPHS standards.
Resul Pookutty Foundation
13
Sub Centre – Yeroor Grama Panchayath
A total budget outlay of INR 368.44 lakhs has been provided in the budget for the project which includes the Cost of Construction, Furnishing of Sub Centre, Repairs & Maintenance for 2 years and Public Relation for a period of 2 years. The breakup of the project cost is given below: Sl. No Component INR Lakhs
Apart from the land which is provided by the Govt. of Kerala, 100% funding required for the project will be funded by Resul Pookutty Foundation from its internal resources/reserve earmarked for the project.
The cost of construction has been arrived with a detailed estimating process. The detailed BOQs are developed for each project component and rates are taken either from Delhi Schedule of Rates (DSR) or through competitive quotations. Provisions for Project Management charges and project contingencies also been factored in the estimation process to avail professional project management services and to fund for price variance or quantity variance during the construction.
Resul Pookutty Foundation
Detailed Project Report
14
3
1 Cost to Establish the Facility 231.30 2 R&M of Facility 17.10
PR Expenses 26.74 4 Project Management Cost 18.50 Grand Total 293.64
Sub Centre – Yeroor Grama Panchayath
The abstract of the cost of establishing the facility are given below: Sl. No Project Component INR Lakhs I BUILDING & CIVIL WORKS 1,22,19,885 II ELECTRICAL 14,03,182 III AIRCONDITIONING 4,39,800 IV LOW VOLTAGE SYSTEM 12,87,340 V PLUMBING 17,07,481 VI FIRE & SAFETY 15,999 VII FURNITURE 3,86,400 VIII MEDICAL EQUIPMENTS 13,63,500 IX WASTE MANAGEMENT 2,50,000 X PRELIMINARY EXPENDITURE 15,96,624 XI CONTINGENCY 24,60,313 XII PMC 18,50,441 TOTAL 2,49,80,965
The proposed project is expected to complete within a period of 8 months and will be handed over to Govt. of Kerala for staffing and operation. Even after the handing over, RPF will continue to support the project for period of two year by taking care of the maintenance & upkeep of the facility. By recognizing the need of building public confidence on this project, RPF will coordinate and fund Public Relation activities for a period of 2 years with a goal to achieve improved usage pattern and adoption by public.
It is aimed to create a new benchmark for rural public health institutions with this project. It is expected that a minimum of 5000 people in Yeoor Grama Panchayat will get benefited from this project.
Resul Pookutty Foundation
Detailed Project Report
15
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
The expected benefits from this project are as under
• Better access to health care for the rural and poor population
• Reduction in healthcare spending by the public
• Effective promotion preventive and promotive healthcare and wellness
• Improved usage of public health facilities
• Faster promotion of e-health facilities
• Better work environment for the healthcare workers
The details of different aspects of the project are presented in this DPR in the following sections.
3. Project in Detail
3.1 Introduction
India has a mixed health-care system, inclusive of public and private health-care service providers. However, most of the private health-care providers are concentrated in urban India, providing secondary and tertiary care health-care services. The public health-care infrastructure in rural areas has been developed as a three-tier system based on the population norms and it is managed by the government. The three-tier system includes: (1) Sub-centres (SC); (2) Primary Health Centres (PHC); (3) Community Health Centres (CHC). But the infrastructure facilities of health centres in rural areas are having its different problems affecting the quality of the healthcare provided.
The COVID-19 pandemic has proven the importance of Public Health Systems in the country. It played a significant role in the COVID-19 response by differentiating patients with respiratory symptoms from those with COVID-19, making an early diagnosis, helping vulnerable people cope with their anxiety about the virus, and reducing the demand for hospital services.
Active surveillance, setting up of district control rooms for monitoring, capacity-building of frontline health workers, risk communication and strong community engagement, and addressing the psychosocial needs of the vulnerable population are some of the key strategic interventions implemented by the public health system that kept the disease in control.
Resul Pookutty Foundation
16
Sub
Detailed Project Report
Centre – Yeroor Grama Panchayath
Public health systems are still of great importance after the COVID. Constant action is needed from the part of the public health systems to raise awareness about COVID in the general population and to prevent the population from other diseases.
Public – Private Partnership (CSR) models will certainly facilitate introduction and faster adoption of technology and creation of facilities in global standard and outlook for the public health delivery. Resul Pookutty Foundation is proposing to partner with Govt. of Kerala in the upgradation of Three-tier public health infrastructure in Anchal Block Panchayat.
The proposed initiative by Resul Pookutty Foundation (RPF) intends to comprehensively undertake the development of the Sub Centre, Public Health Centres (PHCs) and upgrade the Community Health Centre (CHC) in Anchal and maintain these for 2 years before it is handed over to the government. The project shall be a pilot model for development of sub-centres, PHC and CHC in Kerala which may set a new trend of comprehensive rural health management program.
Resul Pookutty Foundation’s vision is to transform Kerala’s current public healthcare system with the adoption of Digital Health Technology. The project can enhance the longevity and wellbeing of people by improving disease management. The use of technology can predict or detect illness earlier and prevent the lifestyle diseases with right interventions. The mission is to provide the Government of Kerala with the clinical study points which will help the government in making intelligent decisions to qualify and quantify the unmet health care needs. This also helps doctors in reducing their workload and enhancing their productivity. Evidence based primary screening technologies will identify the patients who are in the need of doctor’s consultation with simple screening test carried out by trained nurses. Thus, by identifying and averting population from potential lifestyle diseases and epidemics their quality of life can be improved. The project would address current health issues with proprietary lifestyle disease solutions. It would help the general public in increasing their knowledge and understanding how to minimize healthcare challenges and to improve the quality of life.
Resul Pookutty Foundation
17
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Foundation’s objectives include:
➢ Provide health care that is quality oriented and sensitive to the needs of the people.
➢ Achieve and maintain an acceptable standard of quality of care.
➢ Make the services more responsive and sensitive to the needs of the people of Kerala starting from grass root level that is from Sub-Centre itself, where the cases can be easily referred to the PHCs, CHCs, Taluk, District, General hospitals, etc.
The proposed project intends to offer services that help:
➢ Early identification of lifestyle related diseases of high risk individuals.
➢ Facilitate disease prevention with non-medical interventions like diet, exercise and change in unhealthy habit advice.
➢ Prioritize consolidated patients records and streamline management of chronic cases
➢ Manage population health in a cost effective and time efficient way without compromising the compliance of healthcare delivery.
THE PROJECT PROPOSAL
The proposal intends to develop the public healthcare infrastructure in Anchal Block, involving PHCs and Sub Centres in a structured and uniform manner, rendering them the capability to handle public healthcare needs for the next few decades, considering the trend in the increase in population.
The task involves the following:
➢ Facility planning for Sub-centre, PHC and CHCs.
➢ Infrastructure development for all the Sub-centre, PHC and CHC in the Block
➢ Providing an integrated solution connecting the Sub-centre to PHC and CHC.
The comprehensive proposal will include:
➢ Development of Infrastructure for all the Sub centres in Anchal Block which includes 28 Sub Centres, 5 Public Health Centres and up-gradation of the Community Health Centre in Anchal to a 100 bed hospital. The size of the units are proposed considering the trend in the growth of population and the expected demand in Healthcare delivery.
➢ Delivery of Medical Devices wherever applicable
Resul Pookutty Foundation
18
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
➢ Provision of an Integrated Software solution with IoT (Internet of Things) devices connecting the entire cycle of the Health care delivery system till the Hospital.
➢ Maintenance of the Units for 2 years.
Sub-Centre Model:
In the healthcare delivery setup, a Sub-Health Centre (Sub-centre) is the most peripheral and first point of contact between the primary health care system and the community. Ideally one Sub-centre caters to a population of around 5000 people. A Sub-centre provides interface with the community at the grass-root level, providing all the primary health care services and focuses on outreach services, prevalent diseases, tuberculosis, leprosy, Non-communicable diseases, nutrition, water, sanitation and epidemics. The facility for conducting delivery will also be available at most of the Sub-centres. Each Sub centre will be digitally connected with respective PHC and will be fully equipped to launch the e-Health program. The proposed sub centre will be designed by considering all the clinical requirements and logistic arrangement of the sub centre staff.
The additional services at the Sub centres shall include:
• Annual Basic Health Screening: Individual registers using Aadhar or Voter’s ID at the nearest empanelled Sub-Centres (Asha Workers will be trained).
• Complete Electronic Health Recording taken by Asha Workers
• All Individual Medical Records stored in SaaS Cloud Service.
• Data will be stored at represented government agency.
• Patients will be referred to PHC or Taluk based on their medical conditions.
• AI engine helps Nurses/Asha workers to advice patients to seek medical advice immediately based on the Predictive scores.
This DPR is presenting the detailed plan for establishing the pilot unit under the proposed development plans in Anchal Block Panchayat with a Sub Centre at Yeroor Grama Panchayat.
19
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
3.2 Project Background
India has a mixed health-care system, inclusive of public and private health-care service providers. However, most of the private health-care providers are concentrated in urban India, providing secondary and tertiary care health-care services. The participation of private health care service providers in rural areas is very low in many parts of India. Hence the role of Government in rural health systems is an important one.
Public health institutions have an important role to play in monitoring and evaluating health care of people in a particular area, especially in rural areas. Health Centres serve as a first port of call to a qualified doctor in the public health sector in rural areas providing a range of curative, promotive and preventive health care. A PHC providing 24-hour services and with appropriate linkages, plays an important role in increasing institutional deliveries thereby helping to reduce maternal mortality and infant mortality.
Majority of the population in rural India are financially not stable. They depend on public health institutions for the health services. Access to health care facilities is significantly urban biased.
Another point is that, the backward groups in our country need special attention as they not only suffer from unequal and lower access but also produce the worst health outcomes in the country. This is primarily because these groups have been traditionally excluded and discriminated, and therefore suffer from high incidences of poverty and low levels of education among other disadvantages, which have made their access to public health care tougher. Hence the public health care system is required to ensure better care and treatment for these marginalized communities.
India is a middle-income South Asian country with a population of over 1.3 8 billion. In India, healthcare is managed at the state-level. Over the last six decades, the Indian states have had varying levels of success in health outcomes. Notably, Kerala, a southwestern state of 33.3 million people has consistently been a prominent outlier with better health outcomes in a number of areas compared to most states in India. In 2011, Kerala attained the highest Human Development Index of all Indian states based on its performance in key measures:
Resul Pookutty Foundation
20
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
• Lower infant mortality rate of 12 per 1,000 live births in Kerala vs. 40 per 1,000 live births in India;
• Lower maternal mortality ratio of 66 per 1,00,000 live births in Kerala vs. 178 per 1,00,000 live births in India;
• Higher literacy among both males at 96% in Kerala vs. 82% in India and females with 92% in Kerala vs. 65% in India.
The health gains made in Kerala can be attributed to several factors, including strong emphasis from the state government on public health and primary health care (PHC), health infrastructure, decentralized governance, financial planning, girls’ education, community participation and a willingness to improve systems in response to identified gaps.
Kerala invested in infrastructure to create a multi-layered health system designed to provide first-contact access for basic services at the community level and expanded integrated primary health care coverage to achieve access to a range of preventive and curative services. Additionally, Kerala rapidly expanded the number of medical facilities, hospital beds, and doctors. From 1960 to 2010, the number of doctors increased from 1200 to 36,000, and the number of primary health care facilities increased from 369 to 1356 between 1960 and 2004. This increase in the number of PHC and doctors allowed for the provision of the right care in the right place, reduced the costs of patient care, and lowered the burden on secondary and tertiary care facilities. Despite this investment in expanded infrastructure, by the early 1980s there were reports of reduced access to medicine, lab supplies, and adequate sanitation (including drinking water and latrines) in public health centres in Kerala. In 1982, the National Health Policy, recognizing the limited resources in the public sector across all Indian states, encouraged nationwide policies that favoured privatized health care. Over the next 15 years, while public governmental institutions in India increased the number of beds by 5%, the private sector across the country expanded to manage 80% of ambulatory care and 60% of inpatient care. As the private health sector grew in Kerala, many residents sought care in these new locations. However, private health care was significantly more expensive and often
Resul Pookutty Foundation
21
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
unaffordable, with the poor spending up to 40% of their income on out-of-pocket payments to access care.
In 1996, recognizing the eroding trust in the public system, Kerala underwent a major overhaul when the state government implemented the People’s Campaign for Decentralized Planning movement. Within the campaign, a three-tier system of self-governance was established, comprising 950 Panchayats. The current PHC system consists of sub-centres, primary health centres that support five to six sub-centres and serve a village, and community health centres. The sub-centres serve the smallest population and do not have inpatient capacity, while PHC facilities serve about 26,000 citizens and provide maternity services and limited inpatient services, and CHCs provide care to approximately 2,30,000 individuals. Under the new system, the PHC centres and their referring sub-centres were brought under the jurisdiction of LSGs Institutions in order to engage more closely with the community to identify and implement effective changes to respond to local health needs and encourage the use of PHC centres and sub-centres as the first point of care. Communities were brought together to determine which health topics were important and needed attention, with selected topics ranging from strengthening PHC facilities to improving water and sanitation safety. This decentralization resulted in physicians and community members working together and many facilities undergoing significant renovations to address community priorities. As another component of the new system, individuals, especially in lower socioeconomic groups, were encouraged to utilize public health centres. Particularly in villages with strong panchayat governance, there have been improvements in access to medications and health outcomes, as well as increased patient utilization of care at PHC centres.
Since the 1970s, the Indian state of Kerala has been internationally praised for its health achievements despite its economic backwardness. The ‘Kerala Model for Development’ is often referred to as an example for other countries to follow. These achievements are said to be based on the good performance of its health sector as well as its non-health sector. Kerala provides an example of an approach that can provide vastly improved health at a rapid rate. Overall, Kerala has maintained low infant and maternal mortality rates, and higher literacy rates, when compared to the national average. Kerala has also continued to innovate to meet the needs of more vulnerable populations including establishing a Weekly Iron and
Resul Pookutty Foundation
22
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Folic acid Supplementation (WIFS) Program and Adolescent Friendly Health Clinics (AFHCs) to benefit adolescent health.
Kerala is also forward thinking in its health policy planning. The proportion of the population made up of adults over the age of 60 is expected to double by 2050, and Kerala is already developing geriatric care wards and geriatric friendly facilities in preparation. The state is also a leader in palliative care with its own Pain and Palliative Care policy (2008), which focuses on community-based home care initiatives. Kerala’s palliative care network contains over 60 units and serves more than 12 million individuals. In addition, Kerala is investing in health information systems to compile household level data designed to help with population health management and surveillance of communicable diseases.
Despite these health improvements, Kerala’s PHC system has recently faced a number of challenges:
• The epidemiological transition towards chronic disease;
• Erosion of public health funding and
• The continued presence of private health care at much higher cost has pushed the health system to its limits.
The rise of non-communicable diseases in the state has challenged the healthcare system. Kerala has a high prevalence of diabetes 14.80 percent of its population between the ages of 15 and 64 years is diabetic, compared with only 8 percent in India overall. Furthermore, the prevalence of many NCD risk factors in the state is estimated to be very high; a 2010 study found that 42 percent of adult males smoked and that 40 percent of the adult population ate diets low in fruits and vegetables, while 25 percent were overweight. The public sector is unable to meet the demands for health care and the people of Kerala have responded to these inadequacies by increasing private sector use. This trend is not something to welcome. The burgeoning private sector raises household health care expenditures, making health a commodity purchased by ‘ability to pay.’ Many public facilities remain underutilized. Lack of regulations over the private sector does not guarantee the quality of care.
Resul Pookutty Foundation
23
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Overall, Kerala has made significant strides through investing in infrastructure, decentralized governance, and community engagement. Though many challenges remain, it is working towards making health care accessible, affordable, and responsive to an increasing burden of non-communicable diseases.
The public health-care infrastructure in rural areas has been developed as a three-tier system based on the population norms and described below:
Sub - Centres (SC)
A sub-Centre (SC) is established in a plain area with a population of 5000 people and in hilly/difficult to reach/tribal areas with a population of 3000, and it is the most peripheral and first contact point between the primary health-care system and the community. Each SC is required to be staffed by at least one auxiliary nurse midwife (ANM)/female health worker and one male health worker (for details see recommended staffing structure under the Indian Public Health Standards (IPHS)). Under the National Rural Health Mission (NRHM), there is a provision for one additional ANM on a contract basis. SCs are assigned tasks relating to interpersonal communication in order to bring about behavioural change and provide services in relation to maternal and child health, family welfare, nutrition, immunization, diarrhoea control and control of communicable diseases programs. The Ministry of Health & Family Welfare has provided 100% central assistance to all the SCs in the country since April 2002 in the form of salaries, rent and contingencies in addition to drugs and equipment.
Primary Health Centres (PHC)
A primary health Centre (PHC) is established in a plain area with a population of 30,000 people and in hilly/difficult to reach/tribal areas with a population of 20,000, and is the first contact point between the village community and the medical officer. PHCs were envisaged to provide integrated curative and preventive health care to the rural population with emphasis on the preventive and promotive aspects of health care. The PHCs are established and maintained by the State Governments under the Minimum Needs Program (MNP)/Basic Minimum Services (BMS) Program. As per minimum requirement, a PHC is to be staffed by a medical officer supported by 14 paramedical and other staff. Under NRHM, there is a
Resul Pookutty Foundation
24
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
provision for two additional staff nurses at PHCs on a contract basis. It acts as a referral unit for 5-6 SCs and has 4-6 beds for in-patients. The activities of PHCs involve health-care promotion and curative services.
Community Health Centres (CHC)
Community health Centres (CHCs) are established and maintained by the State Government under the MNP/BMS program in an area with a population of 1,20,000 people and in hilly/difficult to reach/tribal areas with a population of 80,000. As per minimum norms, a CHC is required to be staffed by four medical specialists that is, surgeon, physician, Gynaecologist/obstetrician and Paediatrician supported by 21 paramedical and other staff. It has 30 beds with an operating theatre, X-ray, labour room and laboratory facilities. It serves as a referral Centre for PHCs within the block and also provides facilities for obstetric care and specialist consultations.
National Rural Health Mission (NRHM): Strengthening of Rural Public Health System
NRHM, launched in 2005, was a watershed for the health sector in India. With its core focus to reduce maternal and child mortality, it aimed at increased public expenditure on health care, decreased inequity, decentralization and community participation in operationalization of health-care facilities based on IPHS norms. It was also an articulation of the commitment of the government to raise public spending on health from 0.9% to 2-3% of GDP.
Seeking to improve access of rural people, especially poor women and children, to equitable, affordable, accountable and effective primary health care, NRHM (2005-2012) aimed to provide effective health care to the rural population throughout the country with special focus on 18 states having weak public health indicators and/or weak infrastructure. Within the mission there are high-focused and low-focused states and districts based on the status of infant and maternal mortality rates, and these states are provided additional support, both financially and technically. Gradually it has emerged as a major financing and health sector reform strategy to strengthen the state health systems.
Resul Pookutty Foundation
25
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Major initiatives have been undertaken under NRHM for architectural correction of the rural health system in terms of availability of human resources, program management, physical infrastructure, community participation, financing health care and use of information technology.
Resul Pookutty Foundation & Its response to this Scenario
Considering the abovementioned situations and the recognising the need for upgradation of Public Health infrastructure in Kerala, Resul Pookutty Foundation came forward with a novel project to upgrade the Healthcare Delivery Network and to equip the same with modern healthcare technology solutions.
Resul Pookutty Foundation(RPF), is a Non- profit Organization started by Resul Pookutty, international Celebrity sound designer and an Oscar Award winner. Being Kerala’s pride and born in Vilakkupara, near Anchal about 40 km from Kollam, Kerala, India, Resul’s main interest is in the development of his home town. He envisages providing a model health care set -up in Anchal district which could be developed and followed in other districts. RPF intends to fund this project and dedicate this to his hometown as he firmly believes that ``everything starts with Good health”. The objective of RPF is to pursue projects with social causes which can contribute to society on a larger scale.
Resul Pookutty Foundation
26
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
The organisation structure of RPF is given below:
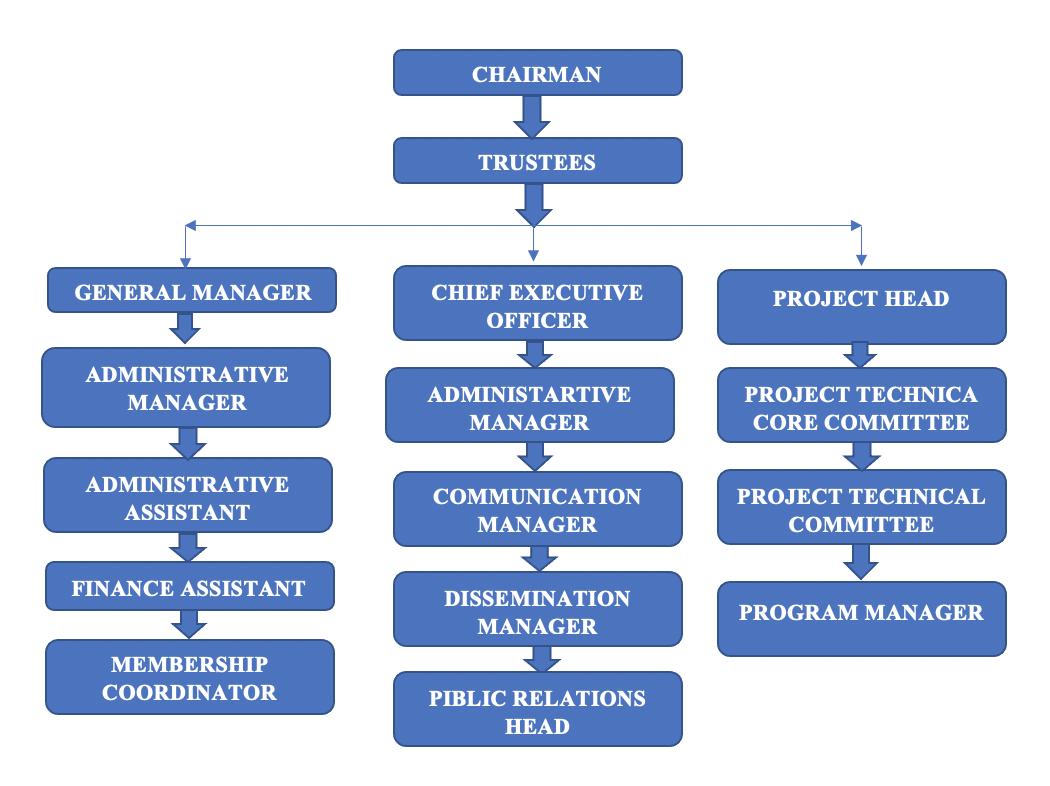
The report intends to develop a Health district of Anchal, under the Sponsorship of Resul Pookutty Foundation as a whole which includes the Sub-Centres, Public Health Centres and Conversion of the Community Health Centre to a 100 Bedded hospital. The passion originates for RPF since Anchal is the birthplace of Resul Pookutty.
The Project is proposed to be funded by Resul Pookutty Foundation.
Resul Pookutty Foundation’s vision is to Transform Kerala’s current Healthcare state with adoption of Digital Health Technology. In Resul’s Foundation, we can further enhance longevity by improving disease management. The use of technology can predict and detect illness earlier and prevent lifestyle diseases with right interventions. The Foundation's objective is to provide health care that is quality oriented and sensitive to the needs of the people to achieve and maintain an acceptable standard of quality of care. To make the services more responsive and sensitive to the needs of the people of Kerala starting from
Resul Pookutty Foundation
27
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
grass root level that is from Sub-Centre itself, where the cases can be easily referred to the PHCs, CHCs, Taluk, District, General hospitals etc.
RPF has integrated services that include collection of data, analysis, development, research, review and recommendations. The mission is to provide the Government with the clinical study points which will help the government in making intelligent decisions to qualify and quantify the unmet health care needs. This also helps doctors in reducing their workload and enhancing their Productivity. Evidence based primary screening technologies will identify the patients who are in the need of doctor’s consultation with simple screening tests carried out by trained nurses. Thus identifying and averting population from potential lifestyle disease epidemics and improving their quality of life improves. We address current Health issues with proprietary lifestyle disease solutions. We help the general public in increasing their knowledge and understanding how to minimize healthcare challenges and improve the quality of life.
The proposal intends to offer services that help:
• Early identification of lifestyle related diseases of high risk individuals
• Facilitate disease prevention with non-medical interventions like diet, exercise and change in unhealthy habit advice.
• Prioritize consolidated patients records and streamline management of chronic cases
• Manage population health in a cost effective and time efficient way without compromising the compliance of healthcare delivery.
RPF brings caregivers to remotely located rural clinics/sub-centres via telemedicine/virtual consultation. Provide vital statistics to doctors remotely with IoT enabled devices. Provide high quality medical care in rural healthcare setup. No highly trained medical staff are required. Preventive screening and risk stratification helps in mapping the public disease trend so that the policy makers can make the right decision on time to curb the problems at nascent stage.
28
Resul Pookutty Foundation
Sub Centre
Detailed Project Report
– Yeroor Grama Panchayath
The proposal intends to develop the infrastructure in Anchal and its surrounding PHCs and Sub Centres in a structured and uniform manner with capability to handle for the next few decades considering the trend in the increase in the population.
This includes the following:
• Facility planning for Sub-centre, PHC and CHCs
• Infrastructure development for all the Sub-centre, PHC and CHC in the district
• Providing an integrated solution connecting the Sub-centre to PHC and CHC.
The facility plan is designed based on the consideration of population as mentioned in each area.
Sub-Centre Model:
A Sub-Centre provides interface with the community at the grass-root level, providing all the primary health care services and focus on outreach services, prevalent diseases, tuberculosis, leprosy, Non-communicable diseases, nutrition, water, sanitation and epidemics. The facilities for conducting delivery are also available at most of the sub-Centres.
Each sub Centre will be digitally connected with respective PHC & fully equipped to launch the-Health program. The proposed sub Centre is designed by considering all the clinical requirements & logistic arrangement of the sub Centre staff Is made, Basic Model in Sub Centre will include the following:
1. Reception Area 2. Doctor’s room 3. Ante Natal Area 4. E- Heath room 5. Injection/ Emergency care Area
6. Conference room for Education of Preventive Health
Resul Pookutty Foundation
29
3.3 Project Objective
A Detailed Project Report (DPR) is a final, detailed appraisal report on the project and a blue print for its execution and eventual operation. It provide details of the basic programme the roles and responsibilities, all the activities to be carried out and the resources required and possible risk with recommended measure to counter them. The objectives of this Detailed Project Report are as follows.
• This DPR is a document created for Planning, Decision Making, approval of the public health infrastructure project proposed by Resul Pookutty Foundation (RPF)
• To assess and appraise the feasibility of the Public Health Infrastructure Project. Thus the DPR is intended to facilitate the decision making on the project.
• To create a Blueprint of the project for its design and execution along with its budget requirement for the project.
• Evaluate different options for the project in achieving the project objective and selection of the right model to be proposed for approval.
• To finalize the Design the specifications and details of facilities to be established in the project.
• To ascertain the budget requirement for the execution of the project and for the ongoing maintenance of the facilities.
Resul Pookutty Foundation
30
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
7. Staff
8. Pharmacy
9. JHN
10. Care-Giving
11. Store
12. Asha
13. Feeding
14. Patient
Accommodation
room
and JDHN room
Room
room
Worker room
Area
Waiting Area
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
• To assess the resource and funds requirement in the different stages in the lifecycle of the project.
• To establish a timeline to complete the project and to set a clear milestone chart for the project.
• To finalize the Project Management methodology, Contract Management Methodology and Quality management options for the project.
• To plan the cashflow requirement for the project and matching the same with the timeline of the project.
• To perform a detailed cost benefit analysis for the proposed project and provide necessary recommendations in this regard.
• To assess the risk factors for the project and explore the mitigation options.
• This DPR will also provide clarity on the roles of RPF, Govt. of Kerala and other stakeholders of the Project during the project execution and ongoing operations.
• To evaluate the social impact of the project and prove recommendation for the approval of the project.
3.4 Project Methodology
The DPR has prepared in consultations with different stakeholders at multiple levels. Resul Pookutty Foundation has selected this project for implementation based on the evaluation of existing facilities of the Primary Public Healthcare Institutions in Kerala. Multiple rounds of facility surveys has been performed to assess the need in terms of infrastructure development. Consultations with public health experts and interactions with the users of public healthcare facilities provided insights for the model to be developed as a sustainable solution to the existing infrastructure gaps. A detailed market study has been commissioned with experts in the field to validate the need and requirement of the project. The modern facilities such as e-health and tele-medicine aspects has been included in the DPR based on the recommendation from experts of health-tech.
Resul Pookutty Foundation
31
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
The following stakeholder groups have been consulted for the DPR preparation at different stages
• Govt. of Kerala Officials
• NHM Officials
• Public Health Experts
• Healthcare Professionals
• Health-Tech Experts
• Elected Representatives and Panchayath Raj Institutions
• Users of Public Health Facilities
• Technical Experts from different fields
The land for the project has been allotted by the Govt. of Kerala. Different types of site evaluation studies have been conducted to design the facility in the allotted land. Topography Survey, Geo Technical Examination, Pollution Test, Noise Test etc. has been performed for the site during the preparation of DPR. A detailed facility survey also has been performed as per the format and guidelines given in IPHS standards released by Ministry of Health and Family Welfare Govt. of India. Financial Professionals have also been consulted on the funding and cashflow management of the project.
The facility has been conceived and designed as per the IPHS standards and upgradations has been provided wherever required. The project concept has been presented with a high level technical committee formed by Resul Pookutty Foundation and the detailed workings and costing has been prepared based on their recommendations and approval.
3.5 Scope of Work
This Detailed Project Report has been prepared to achieve the specific target of establishing a Sub Centre with Yeroor Grama Panchayath as per the guidelines of IPHS standards of Ministry of Health and Family Welfare, Govt. of India. RPF has taken up a project of augmenting and modernizing public healthcare facilities at Anchal Block Panchayath. This DPR has been prepared to draw out the plans to establish a Sub Centre at Yeroor Grama Panchayath within the land provided by Govt. of Kerala.
Resul Pookutty Foundation
32
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
The following aspects have been covered in the DPR for the establishment of Sub Centre at Yeroor:
Sub Centre Building with Pre-Engineered Structure
Power Supply and Distribution Details
HVAC Details
Fire Fighting System
Water Supply System and Storm Water Management
Parking Facilities
Rain Water Harvesting
Landscaping
Waste Management Facilities
Furniture & Fixtures
Medical Equipment and Accessories
Telecommunication / IT
Internet facility
Security systems
Audio visual system
Low Voltage Systems
Office Automation
EPABX System
Nurse calling system
Doctor calling system
Statutory Clearances
This project envisage a turn-key completion of the project and handing over of the facility to the Department of Health and Family Welfare, Govt. of Kerala for operation. The scope of the project also includes the funding of repairs and maintenance of the facility by RPF for a period of two-years from the date of commissioning.
Resul Pookutty Foundation
33
3.6 Overview of the Project Area
About Kerala – An Overview
India is a middle-income South Asian country with a population of over 1.3 8 billion. In India, healthcare is managed at the state-level. Over the last six decades, the Indian states have had varying levels of success in health outcomes. Notably, Kerala, a southwestern state of 33.3 million people has consistently been a prominent outlier with better health outcomes in a number of areas compared to most states in India.
Kerala is situated in the southwestern end of the Indian subcontinent. Kerala has a long history of art and cultural heritage and foreign trade with other countries. The state with the highest literacy rate in India, is noted for its achievements in education, health, gender equality, social justice, law and order. In addition to these, the state has the lowest infant mortality rate in the country.
Kerala lies between the Arabian Sea in the West and the Western Ghats (Sahyadris) in the East with an area of 38863 sq km. It is one of the five states in the linguistic-cultural area known as South India. The neighbouring states of Kerala are Tamil Nadu and Karnataka. Mayyazhi (Mahe / Mahe) is a part of Pondicherry (Puducherry) and lies within Kerala. Though the Lakshadweeps in the Arabian Sea is part of the Union Territories, it has a close alliance with the linguistic and cultural heritage of Kerala.
Before the independence of India, Kerala was one of the princely states in India. Later on 1 July 1949, the princely states of Travancore and Cochin united to form the Travancore-Cochin State. Later, the Malabar region (formerly part of Madras state) was added to the TravancoreCochin State. The state was formed on 1 November 1956. The state of Kerala is divided into 14 revenue districts. The Kerala map is given below.
34
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
Achievements of Kerala in Health Sector
Kerala’s achievements in terms of some of the basic indicators of human development and health are well known and have been much commended upon. The State has a population of 31.84 million as per 2001 census. There has been a reduction in the decadal growth rate from 14.32 (1981-91) to 9.47 (1991-2001). Birth rate of 15, death rate of 6.4 and infant mortality rate of 12 (SRS 2006) is the lowest in the country. Institutional delivery rate is almost 100 %. Sex ratio is 1058 female per thousand men. Female literacy rate of 86.87% is the highest in the country. The total fertility rate is 1.93 (NFHS 3).

In 2011, Kerala attained the highest Human Development Index of all Indian states based on its performance in key measures:
• Lower infant mortality rate of 12 per 1,000 live births in Kerala vs. 40 per 1,000 live births in India;
• Lower maternal mortality ratio of 66 per 1,00,000 live births in Kerala vs. 178 per 1,00,000 live births in India;
• Higher literacy among both males at 96% in Kerala vs. 82% in India and females with 92% in Kerala vs. 65% in India.
Report
35
Detailed Project
Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
The health gains made in Kerala can be attributed to several factors, including strong emphasis from the state government on public health and Primary Health Care (PHC), health infrastructure, decentralized governance, financial planning, girls’ education, community participation and a willingness to improve systems in response to identified gaps.
When it established statehood, the area that made up Kerala already had a long history of health-focused policies; for example, vaccinations were made mandatory for certain segments of the community including public workers and students as early as 1879.
Once it achieved statehood, Kerala invested in infrastructure to create a multi-layered health system designed to provide first-contact access for basic services at the community level and expanded integrated primary health care coverage to achieve access to a range of preventive and curative services.
Additionally, Kerala rapidly expanded the number of medical facilities, hospital beds, and doctors. From 1960 to 2010, the number of doctors increased from 1200 to 36,000, and the number of primary health care facilities increased from 369 to 1356 between 1960 and 2004. This increase in the number of PHC and doctors allowed for the provision of the right care in the right place, reduced the costs of patient care, and lowered the burden on secondary and tertiary care facilities. Additional public health and social development initiatives that began soon after Kerala was made a state such as a push for safe drinking water in the state’s capital, Trivandrum, and primary education for men and women aided in creating the environment for a strong and effective primary care system.
Resul Pookutty Foundation
36
Kollam District – A Brief Overview

Kollam (erstwhile Quilon) is a southern district of Kerala, located 70 km north of the state’s capital Thiruvananthapuram. It is flanked by the Arabian Sea on the west, Tamil Nadu on the east, Alappuzha and Pathanamthitta districts on the north and Thiruvananthapuram district on the south. Housing a population of over 2.6 million, Kollam is one of the more densely populated districts of India. The headquarters of the district administration is centred at Kollam City, the district’s capital. Administratively, the district is composed of two revenue divisions viz. Kollam and Punalur with three taluks each under them.
Like the rest of Kerala, Kollam is climatically temperate with generally sunny weather peaking in heat during April-May. The monsoon falls from June to September. The soil is varyingly loamy, laterite and forest at the coastal regions, mainland and the forest areas respectively.
The heartland of Kollam is naturally veined by the Ashtamudi Lake, a massive, multi-branched water body, which is also a popular boating attraction for tourists. This and the Kollam canal cutting through the city give Kollam a place of prominence in the waterway systems of the country. A number of islands of varying sizes beautifully spot the vast expanse of the lake. The city is graced by beaches where people go to spend quiet evenings. Kollam also has a
Resul Pookutty Foundation
37
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
considerably large forest cover on its eastern side making home for several eco-tourism projects like Shenduruni, Thenmala, Palaruvi etc.
Kollam City boasts of a long history of political, commercial and cultural importance having found mention in several ancient travellers’ accounts. With a varied colonial past under the Portuguese, the Dutch and the British, Kollam has locations of historical importance like the Thangasseri light house, the St. Thomas Fort and cemetery built by the Portuguese, Thevally Palace, Cheenakkottaram etc. Besides, it also is the site of several old buildings constructed by the Travancore kings (its rulers during the pre-Independence times) in a variety of architectural styles, where many government offices still function.
Kollam has been the centre of the cashew industry in Kerala from the time of the Portuguese in 16th c. Having hundreds of working cashew factories in the district, Kollam still continues to be the largest processed cashew exporter in India. Neendakara and Thangasseri, the two fishing harbours and ports in Kollam, support a thriving marine industry providing a variety of employment and livelihood to people in large numbers.
Kollam's healthcare sector is considered as one of the most developed in the state of Kerala. There were hospitals giving free allopathy treatment (Dharmasupathris) in Quilon since ME 995. The Metropolitan Area of Kollam has 3 Medical Colleges and a good number of multispeciality and super-speciality hospitals. At present, the healthcare industry is witnessing stiff competition among these hospitals.
The Kollam district is divided into 11 Blocks, 69 Panchayats, 1 Corporation and Municipalities.
38
Resul Pookutty Foundation
Sub Centre – Yeroor Grama Panchayath
Demography Profile
CENSUS OF INDIA-2011 KERALA, Kollam District Population (provisional)
Demographic Label Value
Population 26,29,703
Child Population of age 0-6 2,38,062
Literate 22,42,757 Literacy rate 94.09 %
Gender ratio 1113 female: 1000 male
Source: https://kollam.nic.in/about-district/
Project Location – Anchal Block
Resul Pookutty Foundation
Report
39
Detailed Project
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
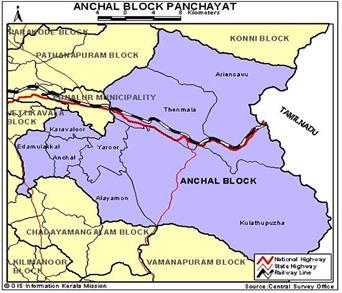
Anchal Block Panchayat is located in Pathanapuram taluk, Kollam district in the Indian state of Kerala. Anchal block includes Anchal, Kulathupuzha, Erur, Alayaman, Idamulaikkal, Karavalur, Thenmala and Aryankavu gram panchayats. Anchal block panchayat covers an area of 95.076 sq. Km and is spread over Anchal, Kulathupuzha, Thinkalkarikam, Channapetta, Erur, Ayiranalloor, Alayaman, Arakkal, Idamulakkal, Karavalur, Idaman, Thenmala, Piravanoor and Aryankavu villages.
The cashew sector is at the forefront of the industry in this block. There are nine cashew factories operating here. Traditional industries and brick industry using forest resources such as bamboo and bamboo are present in all the villages in this block.
In the past, Anchal and the surrounding villages were under the jurisdiction of Kottarakkara Elayidathuswaroopam. Geographically, Anchal block panchayat is situated in the hilly areas of Kerala. The main types of soils found here are sandy loam, riverine loam, loamy loam, forest soil, silt and sandy loam. The block has 14 villages and there are a total 58718 homes in this block.
General Information
Resul Pookutty Foundation
40
Block
Area
Number of divisions 15 Population 2,10,648 Men 1,03,795 Women 1,06,853
District Kollam
Anchal
95.076
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Population density 222
Female to male ratio 1,029
Total literacy 89.11
Literacy (men) 92.76 Literacy (women) 85.6
Source: Census Data 2001
Yeroor Grama Panchayat
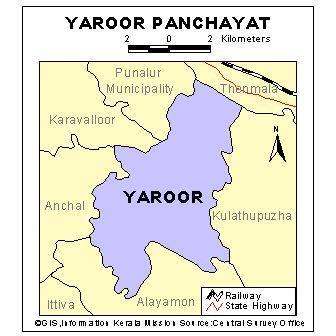
Yeroor Grama Panchayat is a hill station in Anchal block, one of the thirteen block panchayats of Kollam district panchayat in the Indian state of Kerala. The panchayat is located 16 km southeast of Punalur Municipality and 4 km east of Anchal town. The total area of the panchayat is 44.79 sq. Km.
Resul Pookutty Foundation
41
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
The history of Yeroor village dates back to centuries. Legend has it that the village got its name from the fact that it is home to a large number of cattle. As the name suggests, agriculture and animal husbandry were the main occupations of the villagers. Yeroor Panchayat is located on the western side of Kulathupuzha Panchayat, kissing the western slopes of the Western Ghats. Anchal and Karavalur panchayats in the west of Yeroor panchayat share borders with Thenmala panchayat in the north, Punalur municipality and Ayalamon panchayat in the south. It is not known whether any significant development took place in this densely forested and underdeveloped village in the old days when the people of Venattarachar and later the kings of Travancore ruled. The village had trade links with the surrounding areas of Tamil Nadu centuries ago. Yeroor panchayat was born in the first panchayat election held in 1953. The first Yeroor Panchayat covered the entire area of present day Thenmala Panchayat, Kulathupuzha Panchayat and Yeroor Panchayat. Yeroor panchayat has been divided several times to give birth to nearby panchayats. Thus the whole of the vast, scenic and fertile eastern and northern part of the Sahyas was given way to the new Yeroor panchayat to the south of the Kallada River, leaving the birth of three new panchayats. General Information
Resul Pookutty Foundation
42
District Kollam Block Anchal Area 44.79 sq. Km. Number of wards 19 Population 32,723 Men 16,147
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Women 16,576
Population density 731
Female to male ratio 1,027
Total literacy 90.11
Literacy (Men) 93.94
Literacy (Women) 86.42
Source: Census data 2001
The proposed Sub Centre will be established in the land provided by the Govt of Kerala.
3.7 Project Concept in Nutshell
This project envisage to establish a Sub Centre in Yeroor Grama Panchayat, as a pilot unit for the Health Delivery Upgradation Project proposed for Anchal Block Panchayat by Resul Pookutty Foundation. The master plan of the Health Delivery project proposed by RPF envisions complete upgradation of Public health infrastructure in Anchal Block Panchayat with the following activities.
• Development of Infrastructure for all the Sub centers in Anchal area which includes 28 Sub centers,
• 5 Public Health Centers and upgrade of the Community Health center in Anchal to a hospital.
• The size of the units are proposed considering the trend in the growth of population and expected demand in Healthcare delivery
• Delivery of Medical Devices wherever applicable
Resul Pookutty Foundation
43
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
• Provision of an Integrated Software solution with IoT devices connect the entire cycle of the Healthcare delivery system till the Hospital
• Maintenance of the Unit for 2 years
In the healthcare delivery setup, a Sub-Health Centre (Sub-center) is the most peripheral and first point of contact between the primary health care system and the community. Ideally one Sub-center caters to a population of around 5000 people. A Sub-center provides interface with the community at the grass-root level, providing all the primary health care services and focus on outreach services, prevalent diseases, tuberculosis, leprosy, Non-communicable diseases, nutrition, water, sanitation and epidemics. The facility for conducting delivery is also available at most of the sub-centers.
A 6000 sq ft building with two floors is proposed with the following facilities is proposed to be established as the Sub Centre at Yeroor. The facilities provided at the Yeroor Sub Centre are as follows
• Ground Floor o Doctor Room o Asha Health Worker Room
Feeding Room
Care Giving Room
Immunization Room
JPHN Rooms
E-health Room o Toilets including Disabled friendly toilets • First Floor o Staff Quarters o Conference Halls
Yoga Rooms
Health Inspector Rooms
IT Room
Dining Area
Resul Pookutty Foundation
44
o
o
o
o
o
o
o
o
o
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
• General Amenities
o Rain Water Harvesting
o Security System with CCTV Surveillance
o Audio Visual Systems with facilities for Video Conferencing
o Internet and Communication Systems
o Office Automation
o Doctor /Nurse Calling Systems
o Air Conditioning
o Parking Facilities
o Gate & Compound Walls
The building is proposed to be constructed as a pre-engineered steel structural building for faster completion, lesser maintenance and standardization across the other buildings in the project. A modern design has been taken to provide a global outlook for the building.
The e-health facility will be a major highlight of the Sub Centre. Each sub center will be digitally connected with respective PHC & fully equipped to launch the e-Health program.
3.8 Need for the Project
3.8.1 Existing Situation Analysis
Existing Public and Private Sector Healthcare Facilities in the Project Area
There are no private hospitals or dispensaries in the panchayat. Hospital facilities are available only in the urban centres of Punalur and Anchal. Yeroor Panchayat has one PHC and six sub centres. Public Health Centre at Bharathipuram is the only available medical treatment facility in Yeroor panchayat. Neither private hospitals nor private clinics are available within the geographical area of Yeroor Gram Panchayat. There is an AYUSH dispensary under Oil Palm India estate. Private hospitals and clinics are available only at Anchal area which is somewhat 10 Kilometers away from Yeroor Panchayat.
Resul Pookutty Foundation
45
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
For major ailment and delivery cases people of this area are entirely depended on Punalur Taluk Hospital. In short, currently in a geographical area of radius 10 Kilo meter no medical treatment facility is available, except Public Health Centre at Yeroor.
Condition of Existing Public Healthcare Facilities and their Usage Pattern by the Public Public Health Centre at Bharathipuram is the only available medical treatment facility in Yeroor panchayat and it is functioning with one doctor from 9am to 2pm, with limited space and minimum facilities. Presently people from all the 19 wards of the Yeroor Gram panchayat and some wards of Kulathupuzha Gram panchayat are making use of the service of the PHC.
Every day the PHC is over crowded with patients and as a result the doctor and other health professionals are not in a position to give proper care and attention to the patients. Even though Main Sub Centre is mainly intended for the benefit of the people of ward X and ward XI, people from other wards of Yeroor panchayat also make use of the sub centre for antenatal care, Immunisation Programme and Non Communicable Diseases (NCD) clinics.
3.8.2 Requirement /Demand Analysis
It is a cherished desire of respondents. In the study, most of the respondents (95%) indicated that the facilities for more diagnosing/ testing at Main Sub Centre are very essential because now people are depending on two private laboratories and they are charging high for such services.
Resul Pookutty Foundation
46
Detailed
Yeroor Grama Panchayath
Table-18
Need of the facilities for more diagnosing testing at Main Health Sub Centre
Response Frequency Percentage
Essential 38 95
Not essential 2 5 No Response -Total 40 100
Moreover, they said that they are more worried about the quality of the testing and accuracy of the results obtained from the private labs.
The illness can be reduced to the minimum level by conducting periodical medical check-ups. It will help to find the probability of illness in advance. Prevention of illness is better than cure therefore it is essential that the community should be provided with facilities for more diagnosing/ testing at the Sub Centre.
Respondents were asked to reveal their reactions to creation of community health status database at the Main Sub Centre and its online use for the subsequent treatment of the patients.
While 10% of the respondents reported high possibility of objection, ninety percent respondents reported that they did not have any objection.
Resul Pookutty Foundation
47
Project Report Sub Centre –
Table-19
Detailed Project Report Sub
Centre – Yeroor Grama Panchayath
Objection about the creation of community health database at Sub Centre and its online use for the subsequent treatment of the patients
Response Frequency Percentage
Objection 4 10
No Objection 36 90
No Response -Total 40 100
A fairly good percent of them said that availability of such a comprehensive database about the health status of the community members at Sub Centre would be an advantage for their future treatment. However, some of them pointed out that the database should be updated regularly and some mechanism should be developed to ensure that the data manipulation do not occur at any level.
The responses indicate that there is scope for the creation of community health database at the Sub Centre and its online use for the subsequent treatment of the patients, but its maintenance, updating and data security are the major challenges which will arise in future. The data manipulation can be reduced to a minimum level, if necessary preventive measures are taken.
Respondents are generally interested in making use of the services for tele-medicine and other virtual consultations with doctors (Table 20).
More than ninety percent of the respondents expressed their interest in making use of the services for tele-medicine and other virtual consultations with doctors if it is available through the Main Sub centre. Only 7.5% of the respondents were of the opinion that they are not interested in making use of the services.
48
Resul Pookutty Foundation
Yeroor Grama Panchayath
Table-20
Interest in making use of the services for tele-medicine and other virtual consultations with doctors
Response Frequency Percentage
Interested 37 92.5 Not Interested 3 7.5 No Response -Total 40 100
The responses show that majority of the respondents are happy with the innovative telemedicine and other modern practices like virtual consultation with doctors.
Need for reconstruction of the Yeroor Main Health Sub Centre
Respondents were asked to comment on the need for reconstruction of the Yeroor Main Sub Centre. While 40% of the respondents reported that new building with adequate facilities is very essential 60% of them were of the opinion that it is essential. Nobody who participated in the study mentioned that the reconstruction is not required.
Resul Pookutty Foundation
49
Detailed Project Report Sub Centre –
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Table-21
Need for the reconstruction of the Yeroor Main Health Sub Centre
Response Frequency Percentage
Very essential 16 40
Essential 34 60
Not required 0 0
Total 40 100
These responses give an impression that community members are strongly in favour of the reconstruction of the Yeroor Main Sub Centre and they are expecting a fully equipped and functional health sub centre with adequate infrastructure.
3.9 Environmental & Sustainability Aspects
Building is designed in an environment friendly and resource efficient manner. The building is designed with the intention to protect the health of the occupants, improve employee productivity, Conservation of Energy, water and resources, better indoor environment and reducing overall impact to the environment.
Following aspects has been introduced in the building as a part of green and sustainable design.
• Solar power system – It is a renewable energy, where PV cells are used to generate electricity from sunlight.
• HVAC system – We have selected advanced refrigerants available in the current market which can reduce the environmental impact and global warming.
• Smart Appliances – Energy Star rated appliances would be selected to reduce the overall power consumption in this project.
• Water Conservation – Water conservation is made happened using low water consuming fixtures and usage of rainwater by storing it in a rainwater storage tank.
Resul Pookutty Foundation
50
4. Site Surveys, Investigations & Tests 4.1 Land Survey
Details of location
o Taluk: PUNALUR
o Village: YEROOR
o Local Body: YERROR PANCHAYATH
o Topography: The site is spanning 120.8 m at North – South direction and 35.7 m at East – West direction. The site is sloping approx. 9 m towards the entry and approx. 6 m towards the rear. The contours are close together so steep slope.
o Direction route from major location (Town): Route from Anchal towards East to Kulathupuzha SH59 at 9.4 kms. Is the site.
o Distance from nearest bus stop and Name of Bus Stop: Maravanchira Bus stop –300m
o Bus routes passing through the bus stop: Anchal – Kulathupuzha
o Distance to nearest Auto/Taxi stand: 300m from nearest auto stand
o Distance to nearest CHC/PHC: 11 km – CHC Anchal
o Distance to nearest hospitals (Govt:/Pvt): At 8.3 kms. We have a private hospital St. Joseph’s mission Hospital.
o Nearest major hospital/ medical college: Govt: Taluk Head Quarters Hospital, Panamkuttymala, Punalur is at 19.5 kms. Govt. Medical College Parippally is at 37 kms.
• SITE
o Survey No.: 759/14
o Site Area: 95.710 cents / 3873.383 sq.m.
o Access (Width & Nature): The access road is bituminous with a width of 5 m.
o Topography with contours: Sloped topography with highest contour at 101.00 and lowest at 91.00.
o Nature of soil: Hill soil, Laterite soil
o Existing Flora: Tectona grandis - Teak, Terminalia catappa – Badam tree, Mangifera indica – Mango tree, Artocarpus heterophyllus – Jackfruit tree, Bambusoideae - Bamboo, Anacardium occidentale – Cashew tree.
Resul Pookutty Foundation
51
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
o Compound wall & gate: Compound wall is random rubble and brick construction. Plastered both sides. Gate is not provided.
o Elevation from High flood level: 48 m. MSL
o Nearest building number: 801/10, 794/10
o Nearest KSEB post number: AOL/AK/346/A1
o Google Map Coordinates: 8.9287590, 76.9830970
• BUILDING (if existing)
o Plinth Area: Lab & Office - 144.9267 sq.m. PHC - 225.1677 sq.m.
Pharmacy - 57.0317 sq.m. Main Sub center - 74.4923 sq.m.
Ladies Waiting Room - 47.9252 sq.m. Total Area - 549.5436 sq.m.
o Plinth Level: Highest Plinth level marked is 100.498 and the Lowest Plinth level marked is 96.652
• AVAILABILITY OF UTILITIES (including nearest access point)
o Power (HT/LT): SINGLE PHASE
o Water source (Natural/Public): NATURAL - WELL
o Public drain: At the entrance of the site beside SH59 o Telephone: BSNL o Internet (Coaxial/OFC): BSNL (COAXIAL)
o Mobile network coverage, strength and providers: BSNL, VI, AIRTEL JIO
• 50-meter radius o Livestock farm: NIL o Open well: NIL o Pond: NIL o Stagnant pool: NIL
Resul Pookutty Foundation
52
o Garbage dump: NIL
o Polluting industry: NIL
LAND SURVEY DETAILS
Resul Pookutty Foundation
Project Report
Panchayath 53
Detailed
Sub Centre – Yeroor Grama
4.2 Market Survey
MARKET STUDY METHODOLOGY
Assignment
The client proposes to establish a Public Health Sub Centre at Yeroor Panchayat in Anchal Block. As part of the feasibility study, the client has requested us to undertake a market study to establish the need for the sub centre and the rationale for the proposed services including Digital Health and health Management System.
Background:
As per the TOR, the client proposes a project to upgrade the primary healthcare facilities in Anchal Block Panchayath and the proposed project is meant to create a benchmark for primary healthcare facilities in the state. The project envisages construction of 28 Sub Centres and 5 PHCs and a Community Health Centre in line with the NRHM policy, involving advanced facilities and modern telemedicine infrastructure. The project sponsor shall construct the building, equipping the facilities and maintain the facility for a period of 2 years.
As a pilot project, a Public Health Sub Centre will be established at Yeroor Panchayat.
Objectives of the Study
The broad objective of the market research study was to understand the health care needs of the public in the specified geographical area, to identify the facilities required and the specific services to be provided while designing the project and to establish the rationale behind this project.
Specific Objectives
For the study the following specific objectives were set:
a. Understand the basic demographic profile, public health indices and socio economic conditions of the project area.
b. Map the existing public and private sector healthcare facilities in the project area
54
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
c. Assess the condition of existing public healthcare facilities and its usage pattern by the public and also the typical cases where public healthcare facilities are being used frequently.
d. Ascertain the case load in area for the existing institutions.
e. Identify the factors that influence the public confidence in the Govt. healthcare facilities.
f. Get the opinion of doctors and other health care professionals regarding the facilities to be created and the services to be offered.
g. Get the responses of the key stakeholders – the public- about the kind of services to be offered such as tele-medicine.
h. Understand the Key Success Factors and Key Risks for the project propose5
Research Methodology
Both secondary and primary data have been collected for the study. Secondary data were obtained from published reports of Central and State governments. A comprehensive review of the health care situation in the country and the state was done using secondary data.
For primary data, qualitative and quantitative surveys were conducted among three categories of respondents:
1. Doctors and other health care professionals
2. Officials in LSGI, government and elected representatives
3. Target beneficiaries (public) in the specified area of the panchayat
Qualitative studies
Qualitative studies were held with a total of 15 respondents from the first two categories. A total of 15 respondents were involved.
Focus Group discussion was held with health professionals, including the doctor at the PSC and other health professionals drawn from the study area. Semi-structured interviews were held with other categories of respondents.
Experienced researchers organised the Group Discussion and conducted the interviews.
55
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Market Survey
A market survey was conducted among target beneficiaries (public) in the specified area of the panchayat. A sample survey was conducted drawing 40 respondents from the two wards of Yeroor Panchayat, which are the core areas of services of the Yeroor Main Sub Centre, located at the vicinity of the PHC.
Data analysis
The data has been analysed using simple statistical techniques.
DETAILS OF THE PROJECT AREA
Yeroor Panchayat
Yeroor Panchayat is part of the Anchal Block in Kollam District in Kerala State. The geographical location of the area is on the foot hills of the Western Ghats, over 700 feet above the sea level.

This is perhaps among the earliest human settlements in Kerala and farming and cattle breeding, metallurgy and handicrafts have a long tradition here. The populations mainly consists of agricultural and plantation labourers and some Sri Lankan refugees. Until the land reforms in Kerala in the 1970s much of the agricultural land was owned by few land lords.
Yeroor is an agriculture area where more than sixty percent of the people are engaged in agriculture and allied sectors like poultry farming, pig farming, cattle rearing, etc. Three major estates namely, Oil Palm India Ltd, Rehabilitation Plantation Ltd and Farming Corporation and several rubber estates are located in this Panchayat.
Resul Pookutty Foundation
56
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
The demographic profile of Yeroor Panchayat is as follows:
Land Area: 44.79 Sq. Kilo Meter
Number of wards: 19
Population: 33929 Density of population: 758.36
No of House Holds: 8729
Population of the Project Area
The proposed project is targeted mainly at two wards of the Yeroor panchayatBharathipuram and Pathadi. Details of the project are discussed here. Data provided in Table1 gives a picture of the population of Bharathipuram. This ward has a population of 2320. Of the total population, 53% is women and 47% is men.
Table 1
Population of Bharathipuram (ward X)
Male Percentage Female Percentage Total 1085 47 1235 53 2320
Table2 indicates the population status of Pathadi. Population of this ward is 3270. Of the total population, 56% is women and 44% men.
Table 2
Population of Pathadi (ward XI)
Male Percentage Female Percentage Total 1450 44 1820 56 3270
Resul Pookutty Foundation
57
Economic Status of the People of Bharathipuram
Data in Table 3 shows that about half of the families in Bharathipuram ward belongs to the BPL and below BPL categories (50%).
Table 3
Economic Status of the Houses of Bharathipuram (ward X)
SNo. Economic Status Number of Houses Percentage Cumulative Percentage
1
>BPL 67 9.6 9.6 2 BPL 280 40.2 49.8 3 APL 125 17.9 67.7 4 APL> 225 32.3 100 Total 697 100
Economic Status of the People of Pathadi
Data furnished in the Table 4 reveals that 44% of the families in the Pathadi area belongs to the BPL and below BPL categories.
Table 4
Economic Status of the Houses of Pathadi (ward XI)
SNo. Economic Status Number of Families Percentage
Cumulative Percentage
>BPL 60 7 7 2 BPL 320 37 44 3 APL 212 25 69 4 APL> 262 31 100
1
Total 854 100
58
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Existing Public and Private Sector Healthcare Facilities in the Project Area
Health care facilities in Yeroor Panchayat
There are no private hospital or dispensaries in the panchayat. Hospital facilities are available only in the urban centres of Punalur and Anchal.
Yeroor Panchayat has one PHC and six sub centres. Public Health Centre at Bharathipuram is the only available medical treatment facility in Yeroor panchayat. Neither private hospitals nor private clinics are available within the geographical area of Yeroor Gram Panchayat. There is an AYUSH dispensary under Oil Palm India estate. Private hospitals and clinics are available only at Anchal area which is somewhat 10 Kilo meters away from Yeroor Panchayat. For major ailment and delivery cases people of this area are entirely depended on Punalur Taluk Hospital. In short, currently in a geographical area of radius 10 Kilo meter no medical treatment facility is available, except Public Health Centre at Yeroor.
Condition of Existing Public Healthcare Facilities and their Usage Pattern by the Public
Public Health Centre at Bharathipuram is the only available medical treatment facility in Yeroor panchayat and it is functioning with one doctor from 9am to 2pm, with limited space and minimum facilities. Presently people from all the 19 wards of the Yeroor Gram panchayat and some wards of Kulathupuzha Gram panchayat are making use of the service of the PHC.
Case Load in Area for the Existing Institutions
Every day the PHC is over crowded with patients and as a result the doctor and other health professionals are not in a position to give proper care and attention to the patients. Even though Main Sub Centre is mainly intended for the benefit of the people of ward X and ward XI, people from other wards of Yeroor panchayat also make use of the sub centre for antenatal care, Immunisation Programme and Non Communicable Diseases (NCD) clinics.
Resul Pookutty Foundation
59
SUB CENTRE - PROCESS FLOW CHART
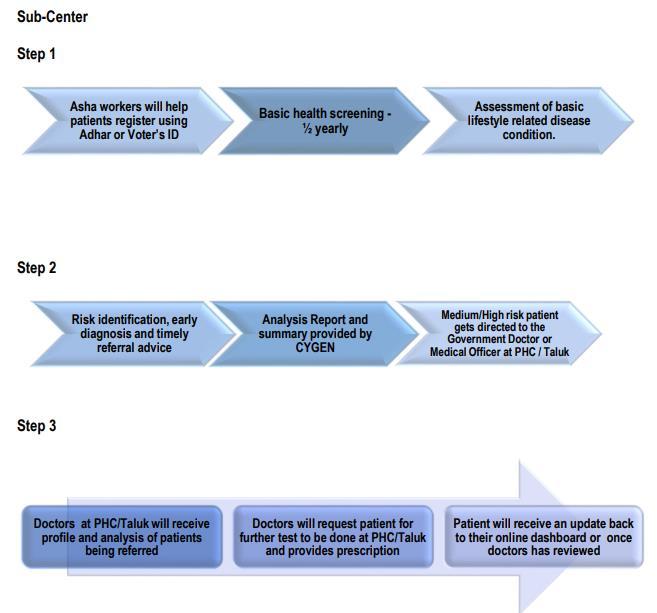
PUBLIC HEALTH CARE SITUATION IN INDIA AND KERALA
HEALTH CARE SITUATION IN INDIA
This section analyses the public health care situation in India, with special emphasis to the situation in Kerala.
Health Index – India & Kerala
India has made significant progress in the health sector in recent decades as a result of the rapid economic growth in the country. In the last few decades, millions of Indians were lifted out of poverty. Health system and health outcomes have also significantly improved. Despite the remarkable progress, health remains a critical area that needs improvement. When benchmarked against countries with similar levels of economic development, India is lagging on some critical health indicators. Moreover, there are huge disparities across States and Union Territories (UTs). The health outcomes of some States are comparable to that of some
60
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
upper middle-income countries and high income countries; for example, Neonatal Mortality Rate (NMR) in Kerala is similar to that of Brazil or Argentina.
The second round of Health Index (referred to as Health Index-2018) examined the overall performance and incremental improvement in the States and UTs for the period 2015-16 (Base Year) to 2017-18 (Reference Year), i.e., a two-year period. (Healthy States Progressive India - Report on the Ranks of States and Union Territories, NITI Aayog, Ministry of Health & Family Welfare, June 2019)
Health Index is a composite score incorporating 23 indicators covering key aspects of health sector performance. The indicators, methodology and categorization of States and UTs in the Health Index-2018 are consistent with the 2017 round with a total of 23 indicators grouped into domains of Health Outcomes, Governance and Information, and Key Inputs/Processes.
Overall performance
Kerala leads in the national Health Index. In the Reference Year (2017-18), the average composite Health Index score among the Larger States in India was 53.22, compared to the Base Year (2015-16) average of 52.59. There was a wide disparity of Health Index score across States, ranging from 28.61 in Uttar Pradesh to 74.01 in Kerala. There is no indication that the gap between poorest performing State and best-performing State is narrowing. Figure.1 displays the composite Health Index scores for Base and Reference Years for the Larger States and ranks the States based on their overall performance.
61
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Figure 1. Larger States Overall Performance – Composite index score & Rank
Source: Healthy States Progressive India - Report on the Ranks of States and Union Territories, NITI Aayog, Ministry of Health & Family Welfare, June 2019
Correlation between Health Index Scores and Economic Development
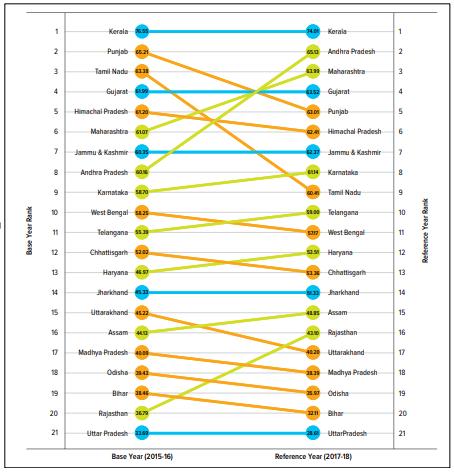
There was a general positive correlation between the Health Index scores and the economic development levels of States and UTs as measured by per capita Net State Domestic Product (NSDP) (Figure. 2).
Resul Pookutty Foundation
62
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Kerala does not rank high in per capita Net State Domestic Product. However, the state has performed well in the health Index. Few other states also have similar experience. Some States with relative low level of economic development performed well in the Health Index, such as Jammu and Kashmir, Manipur, Mizoram, Andhra Pradesh, and Punjab. On the other hand, some States and UTs with relative high level of economic development did not perform as well in Health Index score, such as Goa, Delhi and Sikkim.
Figure 2 .Composite Index Score & Per Capita Net State Domestic Product (NSDP) in 2016-17
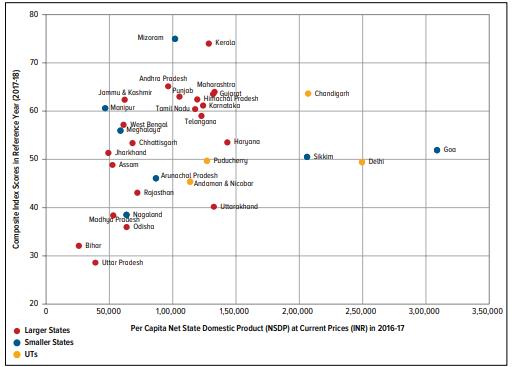
Source: Healthy States Progressive India - Report on the Ranks of States and Union Territories, NITI Aayog, Ministry of Health & Family Welfare, June 2019
Government hospitals and Beds in Rural and urban India and Kerala
As reported in the National Health Profile -2018, the country had a total of 23582 government hospitals with 710761 beds. This included 19810 government hospitals with 279588 beds in the rural sector and 3772 hospitals with 431173 beds in the urban sector (Table. 1)
63
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Kerala had a total of 1280 Government hospitals with 38004 beds at the end of 2017. This was inclusive of 981 government hospitals in the rural sector with 16865 beds and 299 hospitals with 21139 beds in the urban sector. It is pertinent to note that the number of hospital beds are more in the urban areas than in rural areas.
Table .1
Source: National Health Profile 2018, Central Bureau of Health Intelligence
Number of Sub Centres, PHC and CHCs in India & Kerala
Table. 2 provides details about the number of Community Health Centres, public health Centres and health Sub centres in the States and Union Territories in f India. The country had 5624 CHCs, 25650 PHCs and 156231 Sub Centres as at the end of 2017.
Resul Pookutty Foundation
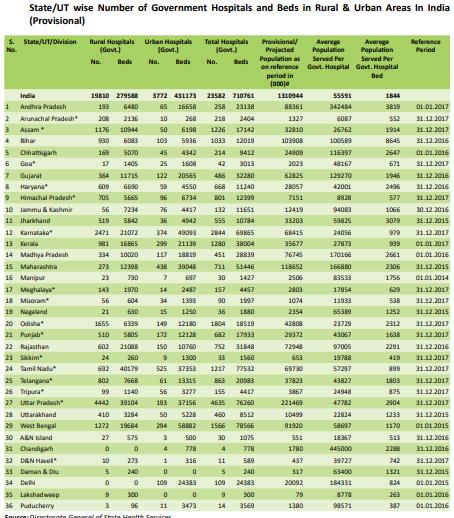
64
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
The Kerala State had 5380 Sub Centres, 849 PHCs and 232 CHCs. This indicates that the state has approximately 5 Sub Centres per Panchayat. The number of PHCs are less than the number of Panchayats and almost 20 % of the Panchayats do not have any PHCs. The number of CHCs are also far inadequate.
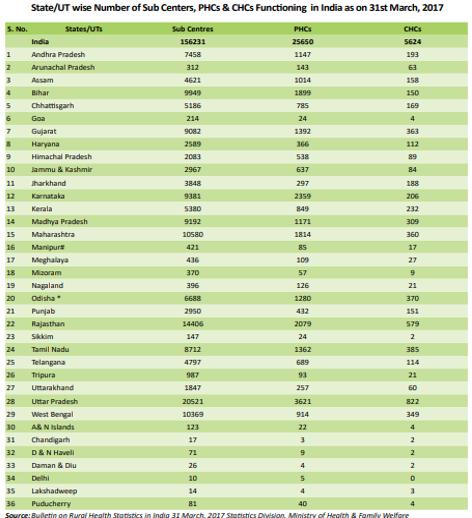
Table. 2
Source: National Health Profile 2018, Central Bureau of Health Intelligence
Health Financing in India
Health financing systems are critical for reaching universal health coverage. Developments in key health financing areas will determine whether health services exist and are available for everyone and whether people can afford to use health services when they need them. Health Finance indicators provide an understanding of patterns of investments, expenditure, sources
Resul Pookutty Foundation
65
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
of funding and proportion of allocation vis-à-vis other total allocations. It also provides an important tool to understand health outcomes in relation to the expenditure. Compared to countries that have either Universal Health Coverage or moving towards it, India’s per capita public spending on health is low.
Public Expenditure on Health in India
Trends in public expenditure on health in India is given in Table. 3.
➢ Total public expenditure on health for the year 2015-16 stood at Rs 1.4 lakh crores.
➢ Per capita public expenditure on health in nominal terms has gone up from Rs 621 in 2009-10 to Rs 1112 in 2015-16.
➢ Public expenditure on health as a percentage of GDP was 1.02% in 2015-16. There is no significant change in expenditure since 2009-10.
Table. 3
Trends in Public Expenditure on Health in India
Source: National Health Profile 2018, Central Bureau of Health Intelligence
Public Expenditure on health – International Comparison
India’s public expenditure on health as a percentage of GDP is one of the lowest in the world.
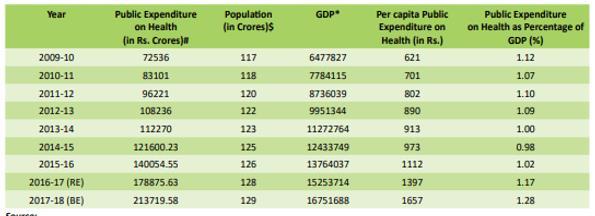
Public Expenditure on health as a percentage of GDP across World Bank Income groups is given in Figure. 3. Figure. 3
Public Expenditure on health as a percentage of GDP across World Bank Income groups -2015
66
Resul Pookutty Foundation
Detailed Project Report
Source: National Health Profile 2018, Central Bureau of Health Intelligence
Public expenditure on health as a percentage of GDP is 5.2% among the High Income countries, 3.8 % among the Upper Middle Income countries, 2.5 % among the Lower Middle Income countries and 1.4 % among the Low Income countries. India’s Public health expenditure less than that of the low income country groups – hardly around 1 %.
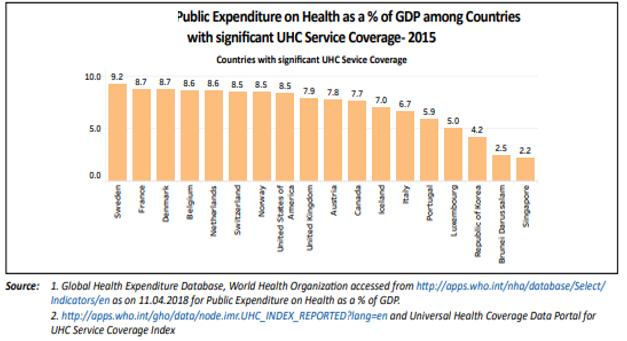
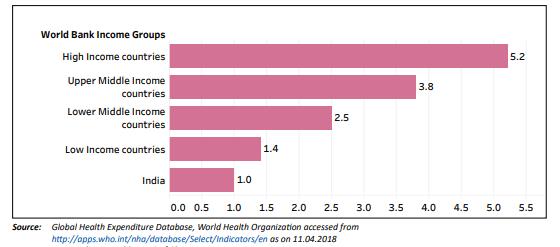
In comparison, some of the developed countries have considerably more spending on public health as per cent of their GDPs (Figure. 4). While the US spends 8.5 % of the GDP, some of the European countries spend even more - Sweden 9.2%, France 8.7 %, Denmark 8.7%, and Belgium 8.6 %.
Figure.4
Source: National Health Profile 2018, Central Bureau of Health Intelligence
67
Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Even some of India’s neighbouring developing countries spend considerably more share of the GDP to public health care (Figure. 5)
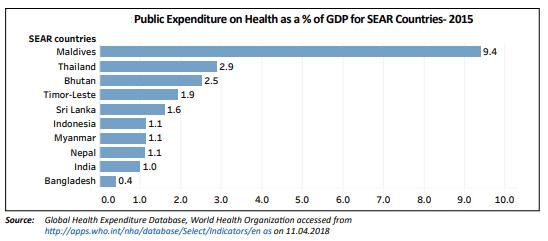
Figure. 5
Source: National Health Profile 2018, Central Bureau of Health Intelligence Maldives is perhaps an exception with 9.4 % of their GDP spend on public health. While Thailand spends 2.9%, Sri Lanka spends 1.6%.
Centre-State share in total public expenditure on health
➢ According to the National Health Profile 2018, Central Bureau of Health Intelligence, the Centre-State share in total public expenditure on health was 31:69 in 2015-16.
➢ Total public expenditure on health in 2015-16 was Rs 140,054 crores, with Medical and Public Health comprising the major share (78.7%). The share of Family Welfare was 12.6%. Urban and rural health services constituted 71% of the public expenditure on medical and public health in 2015-16.
Public Expenditure on health by States, including Kerala
Public Expenditure on health by states varies considerably among the Indian states (Table. 4)
Among the major states, health expenditure as a percent of State GDP is highest in Jammu & Kashmir (2.46%), followed by Himachal Pradesh (1.68 %)and Goa (1.34 %).
68
Resul Pookutty Foundation
Table. 4
Public Expenditure on health by components across states, 2015-16 (Actuals in Rs. Crores)
Source: National Health Profile 2018, Central Bureau of Health Intelligence
In Kerala the public expenditure on health is relatively low; it is only 0.93%. The total state expenditure was Rs. 5207 crores in 2017. As percentage of total state expenditure, expenditure on health was 5.85%.
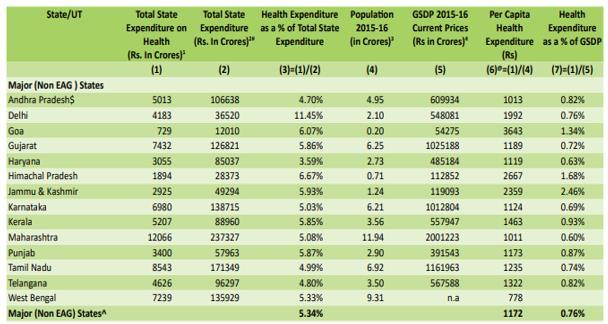
Per capita public health expenditure is also rather low in Kerala – Rs. 1463, while in Goa it was Rs. 3643, in Himachal Pradesh Rs.2667 and in Jammu & Kashmir Rs.2359.
Health Expenditure by Families
Based on Health Survey (71st round) conducted by NSSO, average medical expenditure incurred during stay at hospital from Jan 2013 - Jun 2014 was Rs. 14,935 for rural and Rs. 24,436 for urban in India
Average total medical expenditure per child birth as in patient over last 365 days (survey conducted from Jan to Jun 2014) in a public hospital in rural area is Rs. 1,587 and in urban area is Rs. 2,117.
69
Detailed Project Report Sub Centre –
Yeroor Grama Panchayath
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Health Insurance
Around 43 crore individuals were covered under any health insurance in the year 2016-17. This amounts to 34% of the total population of India. 79% of them were covered by public insurance companies.
Overall, 80% of all persons covered with insurance fall under Government sponsored schemes.
Source of financing hospitalisation
Details of the major sources of finance for hospitalisation expenditure are furnished in Table. 5. Table. 5
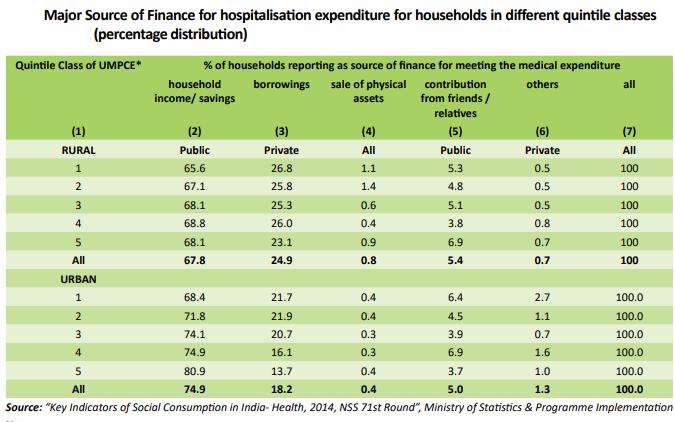
Source: National Health Profile 2018, Central Bureau of Health Intelligence House hold savings form the major source of finance for over two third of the households, followed by borrowing as reported by around 25 % of the families. Contribution by friends, relatives and others form another important source.
HEALTH CARE SITUATION IN KERALA
Health Situation in Kerala - Analysis based on NSS 71st Round (January – June 2014)
Data for this part of the analysis have been drawn from the ‘Report on Health in Kerala NSS 71st Round - January – June 2014’. The report is based on information collected through NSS Schedule 25.0 (Social Consumption: Health), conducted in the 71st round during January -
70
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
June 2014 from 2544 households (1264 in rural and 1280 in urban) in 318 sample First Stage Units spread over the State.
Morbidity and Hospitalisation
Morbidity is very high in Kerala, compared to other states. In India about 9% of rural population and 12% of urban population reported ailment during a 15 day reference period, a period of 15 days prior the household survey.
A comparison of morbidity in India and Kerala (number per 1000 Ailing Persons) during previous 15 days are given in Table. 6
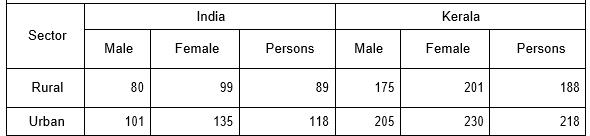
Table. 6 Proportion (per 1000) of ailing persons (PAP) during last 15 days: India, Kerala
Data reveals that in Kerala about 19% of rural population and 22% of urban population reported ailment during a 15 day reference period. Proportion (no. per 1000) of ailing person (PAP) was highest for the age group of 60 & above (505 in rural, 533 in urban), followed by that among children below 14 years (110 in rural, 120 in urban).
Morbidity Rates
Table. 7 gives the survey estimates on the morbidity rate. For the purpose of the survey, Proportion of Ailing Persons (PAP) was measured as the number of living persons reporting ailment (per 1000 persons) during 15-day reference period for different gender in rural and urban sector.
71
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Table. 7 Proportion (Per 1000) of Ailing Persons during Last 15 Days for Different Age Group Separately For Gender: Rural, Urban
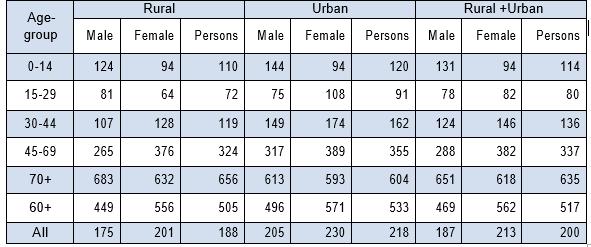
The morbidity rate shows a difference of 30 points between the rural and urban areas. For the age group 0-14 a gender difference in PAP seems to more for male than female in both rural and urban areas while the difference in urban males was higher (50 points). In rest of the age group PAP is more for females. The difference in PAP between the female and male populations was around 25 points in rural and urban Kerala. The normal pregnancy and childbirth related events were not treated as ailment in the survey; only the complications of pregnancy/child birth were considered as ailments.
Treatment of Ailments
Persons who were ailing had different types of treatment available such as Allopathy, Ayurveda, Homoeopathy, etc. In some cases no medical care was taken for their ailments. Table.8 gives the percentage distribution of spells of ailments by different types of treatments.
Resul Pookutty Foundation
72
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Table. 8 Per 1000 distribution of spells of ailments treated (through different types of treatment) during last 15 days for each quintile class of UMPCE
For 90% in both the urban and rural sectors, treatment was in Allopathy. Around 5 percent depends on ISM (Ayurveda, Yoga or Naturopathy Unani, Siddha and homoeopathy).
Around 3 percent depends on Homoeopathy both in rural and urban areas. The users of Yoga & naturopathy and others were negligible in figures. Around 3 percent did not take any treatment in rural sector.
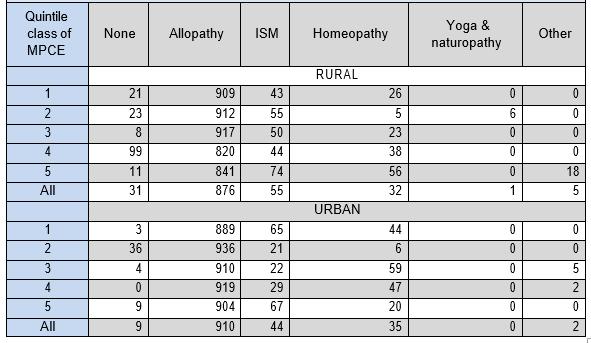
Private vs. Government sector
Data on the type of hospitals used by the sick are furnished in Table. 9.
Around 37% hospitalisation took place in public hospital, and 63% in private hospital in both rural and urban area.
Resul Pookutty Foundation
73
Table.9
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Per thousanddistributionof spellsofailmenttreatedonmedicaladviceoverlevels ofcare for each gender.
Private institutions remained the main provider of inpatient health care in both rural and urban areas. Private Doctors were the most important single source of treatment in both the sectors. Private health care institutions accounted for around 62% of the treatments in the state with 59 percent in rural and 65 percent in urban areas and the sector consist of private doctors, nursing homes, private hospitals, charitable institutions, etc.
Among the hospitalised cases 8.8 percent were below 4 years age group. It is also remarkable that among the youngest age group (0-4) rate of hospitalisation is higher in male than female. The use of Allopathy was most prevalent (98%) in treating the hospitalised cases of ailments, irrespective of gender.
Treatment Cost
Data on the cost of hospitalised treatment including medical and nonmedical expenses are presented in Table. 10.
Resul Pookutty Foundation
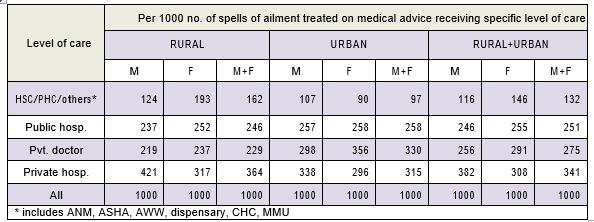
74
Table.10 10
The rural population spent, on an average, Rs.14001 for a hospitalised treatment and Rs.18324 for that in urban sector.
The average total medical expenditure for non-hospitalised (outpatient) treatment per ailing person for different classes are furnished in Table. 11.
Table.11
Average total medical expenditure for non-hospitalised treatment per ailing person for each quintile class.
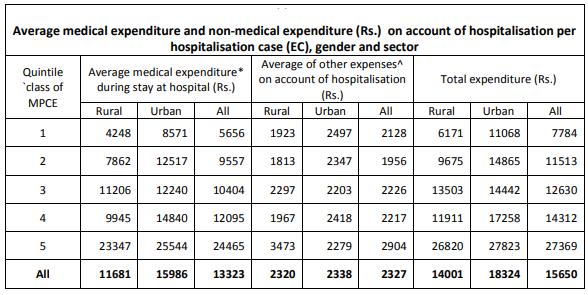
For people in the lowest class the average medical expenditure each time they have an ailment is Rs. 304 in the rural area and Rs. 371 in the urban area. Among the highest 20% category the expenditure is Rs. 629 in the rural area and Rs. 604 in the urban area.
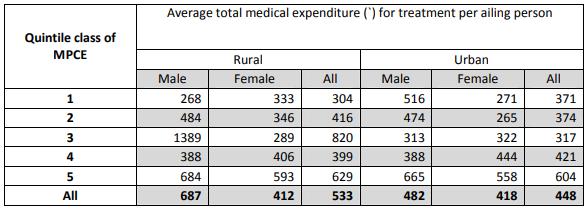 Resul Pookutty Foundation
Resul Pookutty Foundation
75
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Source of Finance
The NSS study has also noted that as high as 97% of rural population and 95% of urban population were still not covered under any scheme of health expenditure support such as insurance.
Major source of finance for hospitalisation expenditure for households in the state is Household Income / Savings (73 percent).
Contribution for hospitalisation expenditure for households from Friends and Relatives in rural area was 6.1 percent and for urban area it was 4.6 percent.
Childbirth and Maternity Care Services
In NSS 71st round survey detailed information was collected on childbirth, giving special emphasis on institutional child birth. The major findings of the study on Childbirth and Maternity Care Services are summarised here.
➢ Among women in the age-group 15-49 years, about 8% in the rural areas and 7% in the urban areas were reported as pregnant during the 365 days preceding the date of survey.
➢ Of all pregnancies reported to the survey, around 80 percent in rural areas and 82 percent in urban areas were completed within the year.
➢ In terms of these pregnancy outcomes, percentage of still birth was about 1% in rural and nil in urban areas while the same for abortion was 3% in rural and 5% in urban areas.
➢ In 99.6 percent of the cases the child births were in hospitals. In the rural areas, about 0.4% of the childbirths were at home or any other place.
➢ About 31% of childbirths took place in public hospitals and 68% in private hospitals.
➢ Lower the economic quintile class (20 % of the population) the higher the proportion of institutional childbirths that take place in public hospitals as compared to private hospitals. Free bed was utilized for 90% of childbirths at public hospitals.
➢ In the highest quintile class, 90 percent of childbirth took place in private hospitals.
➢ Contrary to public hospital scenario, in private hospitals, 98% childbirth took place in paying.
Resul Pookutty Foundation
76
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
➢ In rural areas around 7 days stay in public hospital and 6 days stay in private hospital were reported for institutional childbirth. In urban sector these were reported as 8 days and 6 days respectively.
➢ An average of Rs. 2057 was spent per childbirth in public hospitals and Rs. 20737 in private hospitals, which is around 10 times more than that of the government institutions.
➢ In the rural areas about 99.8 per cent of pregnant women took some pre-natal care, where as in urban area corresponding figure was 97.8 per cent.
➢ About 90.4 per cent of pregnant women took some post-natal care, where as in urban area corresponding figures was 94.5 per cent.
Status of the Aged Persons (60 and above)
The major findings of the NSS survey pertaining to the status of the aged persons are summarised here:
➢ India has around 1038 lakhs elderly persons (8.6% of the population comprising 60 plus population, Census 2011) and Kerala has 41.93 lakhs elderly persons (12.55% of the population comprises 60 plus population, Census 2011). An overwhelming majority of the elderly live in rural areas and there is an increasing proportion of oldoldest age category with feminization of ageing being more pronounced at this age.
➢ The extended family system remains the dominant form of family in Kerala. In such a system, most of the aged, particularly those who have lost their spouses, depend on their children for maintenance.
➢ The 2014 NSS survey in Kerala revealed that around 26% of the aged in rural and 31% in urban were not depended on others for their day-to-day needs.
➢ The dependence was very high for elderly females. Among them, about 85 per cent aged women in rural and 80% women in urban were economically dependent either partially or fully.
➢ Most of the economically dependent aged persons- 89% in rural and 85% in urban depend on their children for financial support and a sizable proportion (6% in rural and 8% in urban) on their spouses.
➢ About 97 per cent of the aged had at least one surviving child.
Resul Pookutty Foundation
77
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
➢ Around 53 per cent in rural and 47 per cent in urban were living with their spouses and other members.
➢ About 4.5% of the aged both in rural and urban (in which 7 percent were women) stayed alone.
➢ Among the aged persons about 2 per cent of were confined to their home and 4 per cent were confined to bed.
➢ Only 2% aged with chronic ailment felt as being in a better state of health as compared to the previous year. About 32% among them felt that their health situation was in a worse state compared to the previous year.
LIFESTYLE DISEASES IN KERALA
The prevalence of Life Style diseases is a major problem in Kerala, as indicated earlier. This section analyses the major findings of some studies on the critical diseases affecting people in the state based on several studies.
In Kerala, the prevalence of lifestyle diseases like diabetes, heart disease, high blood pressure and obesity is high and it results in very high mortality and morbidity from malignant heart disease.
The prevalence of risk factors is high even in rural Kerala: diabetes 20%, high blood pressure 42%, high cholesterol (>200mg/dl) 72%, smoking (42% in men) and obesity (body mass index >25) 40%, physical inactivity 41%, unhealthy alcohol consumption 13%.
Diabetes
Kerala is known as diabetes capital of India as prevalence of diabetes is high i.e. 20% which is double the national average of 8%. As compared, the prevalence in Thiruvananthapuram was 17%, in Hyderabad & New Delhi 15%, in Nagpur 4% and in Dibrugarh 3%.
Only 40% of people with diabetes had adequate control of blood sugar. Among those with diagnosed diabetes, 17% received no treatment, 15% were on diet alone, and 68% were on medications.
In Kerala, as compared to urban dwellers people from rural Kerala, paradoxically having higher rates of diabetes. In one large study the prevalence of diabetes was 19% in rural men and 22% in rural women compared to 12% in urban men and 17% in urban women.
Resul Pookutty Foundation
78
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Coronary Artery Disease
In Kerala 14% of all deaths are caused by coronary heart disease (CHD/CAD). In Kerala mortality rates for CAD (coronary artery disease), per 100,000 are 382 for men and 128 for women which is actually 3 to 6 times higher than Japanese and rural Chinese and also higher than other industrialized countries.
In the 1960s and 70s, heart attack in the very young i.e. before the age of 40 was very uncommon in Kerala. Heart attack rate among men in this age group increased 40-fold by 1990 with at least 20% heart attacks occurring before age 40 and 50% before age 50
Approximately 60% of CAD deaths in men and 40% of CAD deaths in women occur before the age of 65 years that is at very young age as CAD in Kerala is premature and malignant. Cardiovascular disease is the foremost killer of people with diabetes. 80% of diabetic patients die from heart disease.
Cancer
As per cancer registry data, in Kerala there are 974 female cancer and 913 male cancer patients per million. In one year, Kerala has roughly 35,000 new cancer cases occurs. Breast cancer is the most common malignancy among the women in Kerala; about 30 to 35% is accounted by breast cancer.
According to the data available with the Thiruvananthapuram Cancer Registry, the prevalence rate in rural areas is 19.8 per 100,000, while in the urban areas, it is 30.5 per 100,000 people.
CHAPTER SUMMARY ON PUBLIC HEALTH CARE SITUATION
Health Index
Despite the remarkable progress, health remains a critical area that needs improvement. When benchmarked against countries with similar levels of economic development, India is lagging on some critical health indicators.
The second round of Health Index (referred to as Health Index-2018) examined the overall performance and incremental improvement in the States and UTs for the period 2015-16 (Base Year) to 2017-18 (Reference Year), i.e., a two-year period
Kerala leads in the national Health Index. In the Reference Year (2017-18), the average composite Health Index score among the Larger States in India was 53.22, compared to the
Resul
Pookutty
Foundation
79
Sub
Detailed Project Report
Centre – Yeroor Grama Panchayath
Base Year (2015-16) average of 52.59. There was a wide disparity of Health Index score across States, ranging from 28.61 in Uttar Pradesh to 74.01 in Kerala
Health infrastructure
As reported in the National Health Profile -2018, the country had a total of 23582 government hospitals with 710761 beds. This included 19810 government hospitals with 279588 beds in the rural sector and 3772 hospitals with 431173 beds in the urban sector (Table. 1)
Kerala had a total of 1280 Government hospitals with 38004 beds at the end of 2017. This was inclusive of 981 government hospitals in the rural sector with 16865 beds and 299 hospitals with 21139 beds in the urban sector. The country had 5624 CHCs, 25650 PHCs and 156231 Sub Centres as at the end of 2017. The Kerala State had 5380 Sub Centres, 849 PHCs and 232 CHCs. This indicates that the state has approximately 5 Sub Centres per Panchayat. The number of PHCs are less than the number of Panchayats and almost 20 % of the Panchayats do not have any PHCs. The number of CHCs are also far inadequate.
Health Financing in India
Compared to countries that have either Universal Health Coverage or moving towards it, India’s per capita public spending on health is low.
➢ Total public expenditure on health for the year 2015-16 stood at Rs 1.4 lakh crores.
➢ Per capita public expenditure on health in nominal terms has gone up from Rs 621 in 2009-10 to Rs 1112 in 2015-16.
➢ Public expenditure on health as a percentage of GDP was 1.02% in 2015-16. There is no significant change in expenditure since 2009-10.
➢ Public expenditure on health as a percentage of GDP is 5.2% among the High Income countries, 3.8 % among the Upper Middle Income countries, 2.5 % among the Lower Middle Income countries and 1.4 % among the Low Income countries. India’s Public health expenditure less than that of the low income country groups – hardly around 1%.
Resul Pookutty Foundation
80
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
In comparison, some of the developed countries have considerably more spending on public health as per cent of their GDPs (Figure. 4). While the US spends 8.5 % of the GDP, some of the European countries spend even more - Sweden 9.2%, France 8.7 %, Denmark 8.7%, and Belgium 8.6 %.
Centre-State share in expenditure on health
According to the National Health Profile 2018, Central Bureau of Health Intelligence, the Centre-State share in total public expenditure on health was 31:69 in 2015-16. Total public expenditure on health in 2015-16 was Rs 140,054 crores, with Medical and Public Health comprising the major share (78.7%)
Among the major states, health expenditure as a percent of State GDP is highest in Jammu & Kashmir (2.46%), followed by Himachal Pradesh (1.68 %)and Goa (1.34 %).
In Kerala the public expenditure on health is relatively low; it is only 0.93%. The total state expenditure was Rs. 5207 crores in 2017. As percentage of total state expenditure, expenditure on health was 5.85%.
Per capita public health expenditure is also rather low in Kerala – Rs. 1463, while in Goa it was Rs. 3643, in Himachal Pradesh Rs.2667 and in Jammu & Kashmir Rs.2359.
Health Expenditure by Families
Based on Health Survey (71st round) conducted by NSSO, average medical expenditure incurred during stay at hospital from Jan 2013 - Jun 2014 was Rs. 14,935 for rural and Rs. 24,436 for urban in India
Around 43 crore individuals were covered under any health insurance in the year 2016-17. This amounts to 34% of the total population of India. 79% of them were covered by public insurance companies. Overall, 80% of all persons covered with insurance fall under Government sponsored schemes.
House hold savings form the major source of finance for over two third of the households, followed by borrowing as reported by around 25 % of the families. Contribution by friends, relatives and others form another important source.
Resul Pookutty Foundation
81
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
HEALTH CARE SITUATION IN KERALA
Data for this part of the analysis have been drawn from the ‘Report on Health in Kerala NSS 71st Round - January – June 2014’.
Morbidity and Hospitalisation
Morbidity is very high in Kerala, compared to other states. In India about 9% of rural population and 12% of urban population reported ailment during a 15 day reference period, a period of 15 days prior the household survey.
Data reveals that in Kerala about 19% of rural population and 22% of urban population reported ailment during a 15 day reference period.
For 90% in both the urban and rural sectors, treatment was in Allopathy. Around 5 percent depends on ISM (Ayurveda, Yoga or Naturopathy Unani, Siddha and homoeopathy).
Around 37% hospitalisation took place in public hospital, and 63% in private hospital in both rural and urban area.
The rural population spent, on an average, Rs.14001 for a hospitalised treatment and Rs.18324 for that in urban sector.
The average total medical expenditure for non-hospitalised (outpatient) treatment per ailing person for different classes
For people in the lowest class the average medical expenditure each time they have an ailment is Rs. 304 in the rural area and Rs. 371 in the urban area. Among the highest 20% category the expenditure is Rs. 629 in the rural area and Rs. 604 in the urban area.
Childbirth and Maternity Care Services
➢ In 99.6 percent of the cases the child births were in hospitals. In the rural areas, about 0.4% of the childbirths were at home or any other place.
➢ About 31% of childbirths took place in public hospitals and 68% in private hospitals.
➢ Lower the economic quintile class (20 % of the population) the higher the proportion of institutional childbirths that take place in public hospitals as compared to private hospitals. Free bed was utilized for 90% of childbirths at public hospitals.
➢ Contrary to public hospital scenario, in private hospitals, 98% childbirth took place in paying.
82
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
➢ An average of Rs. 2057 was spent per childbirth in public hospitals and Rs. 20737 in private hospitals, which is around 10 times more than that of the government institutions
➢ In the rural areas about 99.8 per cent of pregnant women took some pre-natal care, where as in urban area corresponding figure was 97.8 per cent.
➢ About 90.4 per cent of pregnant women took some post-natal care, where as in urban area corresponding figures was 94.5 per cent.
Status of the Aged Persons (60 and above)
➢ India has around 1038 lakhs elderly persons (8.6% of the population comprising 60 plus population, Census 2011) and Kerala has 41.93 lakhs elderly persons (12.55% of the population comprises 60 plus population, Census 2011). An overwhelming majority of the elderly live in rural areas and there is an increasing proportion of oldoldest age category with feminization of ageing being more pronounced at this age.
➢ The 2014 NSS survey in Kerala revealed that around 26% of the aged in rural and 31% in urban were not depended on others for their day-to-day needs.
➢ The dependence was very high for elderly females. Among them, about 85 per cent aged women in rural and 80% women in urban were economically dependent either partially or fully.
➢ Most of the economically dependent aged persons- 89% in rural and 85% in urban depend on their children for financial support and a sizable proportion (6% in rural and 8% in urban) on their spouses.
➢ Among the aged persons about 2 per cent of were confined to their home and 4 per cent were confined to bed.
LIFE STYLE DISEASES IN KERALA
In Kerala, the prevalence of lifestyle diseases like diabetes, heart disease, high blood pressure and obesity is high and it results in very high mortality and morbidity from malignant heart disease.
The prevalence of risk factors is high even in rural Kerala: diabetes 20%, high blood pressure 42%, high cholesterol (>200mg/dl) 72%, smoking (42% in men) and obesity (body mass index >25) 40%, physical inactivity 41%, unhealthy alcohol consumption 13%.
Resul Pookutty Foundation
83
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Kerala is known as diabetes capital of India as prevalence of diabetes is high i.e. 20% which is double the national average of 8%.
In Kerala 14% of all deaths are caused by coronary heart disease (CHD/CAD)and the mortality rates for CAD (coronary artery disease) per 100,000 are 382 for men and 128 for women which is actually 3 to 6 times higher than Japanese, Chinese and other industrialized countries. Cancer
As per cancer registry data, in Kerala there are 974 female and 913 male cancer patients per million. In one year, Kerala has roughly 35,000 new cancer cases occurs. The prevalence rate for cancer in rural Kerala is 19.8 per 100,000, while in the urban areas, it is 30.5 per 100,000 people.
MARKET SURVEY REPORT: ANALYSIS OF THE RESPONSES OF THE GENERAL PUBLIC MARKET SURVEY
A market survey was conducted among people in Bharathipuram (ward X) and Pathadi (ward XI) wards of Yeroor Gram Panchayat of Anchal block. The people of the two wards are the prime beneficiaries of services offered at the Main Sub centre at Yeroor. But people from other wards of the panchayat also make use of the service of the Sub Centre because of its vicinity to the Public Health Centre. Hence few members from the other wards were also included. The purpose of the study was to understand the health care needs of the public in the geographical area, to identify the facilities required and the specific services to be provided while designing the project as well as to establish the rationale behind this project. Forty community members were selected at random for the study and interviews were held with the respondents using a pre-tested research schedule. Analyse the data collected from the respondents through the sample survey among the general public is presented in this sections.
Resul Pookutty Foundation
84
Age of the Respondents
People of all age groups were included in the survey. About one- third of the respondents who participated in the study were in the age group of 31-40 years and thirty percent in the age group of 41-50 years. Of the remaining, 22.5%, 12.5% and 5% were from the age groups of 20-30 years, 51-60 years and 61-70 years, respectively.
Table-1
Age of the Respondents
Age(Years)
Frequency Percentage 20-30 9 22.5 31- 40 12 30 41- 50 12 30 51- 60 5 12.5 61-70 2 5
Total 40 100
Gender of the Respondents
Fifty-five percent of the respondents participated in the study were females and the remaining were male members.
Table-2
Gender of the Respondents
Gender Frequency Percentage Male 18 45 Female 22 55 Total 40 100
Socio-economic Background of the Respondents
In order to understand the socio economic background of the respondents, they were asked to indicate the colour / category of their ration cards. A ration card is issued by the state government based on the family’s economic status. In Kerala ration cards are issued in four colours: Yellow Card, Pink Card, Blue Card, and White Card.
Detailed Project Report
85
Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Yellow cards are issued to the poorest of the poor. They are beneficiaries of the Anthodia Anna Yolanda (AAY) scheme of the Central Government. The category includes the landless labourers, marginal farmers, artisans, craftsmen, widows, sick persons, illiterates and disabled adults with no means of subsistence.
Pink cards are issued to the Below Poverty Line (BPL) category. This category has priority for food subsidy. Their family annual income is less than Rs. 25000. Blue Cards are issued to people in the Above Poverty Line (APL) category and they have no Priority for subsidised food. Their family income is up to Rs. 100,000 annually. White Colour cards are issued to people in the category above APL; they have no priority for food subsidy and they have annual income above Rs. 100000.
The survey respondents were asked to indicate the colour of the ration cards in order to identify their socio-economic category.
The survey indicates that 45% of the respondents belong to the BPL and below BPL categories. Table 3 reveals that 42.5% of the respondents belong to Below Poverty Line and 40 % belongs to Above Poverty Line categories. The respondents belonging to below BPL and above APL category are 2.5% and 15%, respectively.
Table-3 Ration
Resul Pookutty Foundation
86
Card
Ration Card Category Number of Families Percentage Cumulative Percentage
BPL 1 2.5 2.5 BPL 17 42.5 45 APL 16 40 85 APL> 6 15 100 Total 40 100
Category of the Respondents
<
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
The fact that 45 % of the respondents in a random selection belongs to BPL and below categories indicates that the people of the area are economically backward.
Availability of sufficient medical treatment facilities in Yeroor Panchayat
There is high degree of dissatisfaction among the respondents in respect of availability of sufficient medical treatment facilities in Yeroor Panchayat, as 90% of the respondents reported dissatisfaction with the medical treatment facilities that are made available to them. Only ten percent of the respondents opined that sufficient medical treatment facilities are available in Yeroor Panchayat. According to some respondents, for major ailment and delivery cases they are entirely depending Punalur Taluk Hospital. They added that currently in a geographical area of radius 10 Kilo meter no medical treatment facility is available except the Public Health Centre at Yeroor.
Table-4
Availability of sufficient medical treatment facilities in Yeroor Panchayat
Response
Frequency Percentage
Available 4 10 Not Available 36 90 No Response -Total 40 100
The data shows that availability of sufficient medical treatment facilities at Yeroor panchayat is an urgent need of the community not only to provide better treatment to their ailments and delivery needs but also to develop a healthy society in the near future.
Availability of sufficient Government medical treatment facilities in Yeroor Panchayat
The level of satisfaction of the respondents regarding the availability of government medical treatment facilities in Yeroor panchayat is very low, as revealed by their responses (Table 5). Eighty percent of the respondents have reported that the government medical treatment
Resul Pookutty Foundation
87
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
facilities available in Yeroor panchayat are insufficient. Only one-fifth of the respondents stated that sufficient medical treatment facilities are available there. Some respondents stated that the Public Health Centre is the only available medical treatment facility in Yeroor panchayat and it is functioning with one doctor from 9am to 2pm, with limited space and minimum facilities. They added that every day the PHC is over crowded with patients and as a result the doctor and other health professionals are not in a position to give proper care and attention to the patients.
Table-5
Availability of sufficient Government medical treatment facilities in Yeroor Panchayat
Response
Frequency Percentage
Available 8 20 Not Available 32 80 No ResponseTotal 40 100
The above responses give an impression that the available government medical treatment facilities in Yeroor Panchayat is insufficient both in terms quantity and quality.
Availability of sufficient Private Hospitals in Yeroor Panchayat
The respondents’ opinion presented in Table 6 exhibit a clear picture for the availability of Private Hospitals in Yeroor Panchayat.
Resul Pookutty Foundation
88
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Table-6
Availability of sufficient Private Hospitals in Yeroor Panchayat
Response
Frequency Percentage
Available 0 0 Not Available 40 100 No Response -Total 40 100
All of them stated that no private hospital is available within the geographical area of Yeroor Gram Panchayat. Private hospitals are available only at Anchal area which is somewhat 10 Kilo meters away from Yeroor Panchayat.
Availability of sufficient Private Clinics in Yeroor Panchayat
It is pertinent to note that the availability of private clinics in Yeroor Panchayat is similar to that of the availability of private hospitals. All of the respondents said that no private clinic is available in the Yeroor Gram Panchayat. All of them expressed their negative feelings in this regard.
Table-7
Availability of sufficient Private Clinics in Yeroor Panchayat
Response
Frequency Percentage
Available 0 0 Not Available 40 100 No Response -Total 40 100
Availability of sufficient Private Testing labs in Yeroor Panchayat
With regard to the availability of sufficient private testing labs in Yeroor Panchayat, 75% of the respondents reported that sufficient number of private testing labs are not available in Yeroor Panchayat while 25% said it is available. According to them, 2 private clinical laboratories are available in this panchayat with limited facilities.
Resul Pookutty Foundation
89
Table-8
Availability of sufficient Private Testing labs in Yeroor Panchayat
Response
Frequency Percentage
Available 10 25 Not Available 30 75 No ResponseTotal 40 100
Some of them added that as a part of PHC a testing lab has been started recently but it has very limited facility in terms of equipment and manpower and they are doing the testing manually. The lab offers limited number of testing like Sugar level, cholesterol level, kidney function, creatine level, pregnancy test and malaria test. The responses indicate that non-availability of well-functioning testing labs in government sector together with insufficient number of private labs with limited facilities has worsened the situation very much and this turn adversely affect the early detection of ailments.
Awareness about the Main Health Sub centre functioning in the premises of the PHC at Yeroor When asked about their awareness of the Main Health Sub centre functioning in the premises of the PHC at Yeroor, all of the respondents said that they are aware of it. But majority of them pointed out that the Main Health Sub centre does not have any name board or sign board. So some of them think that it is a part of Public Health Centre at Yeroor.
Table-9
Awareness about the Health Sub centre functioning in the premises of the PHC at Yeroor
Response
Frequency Percentage
Aware 40 100 Not Aware 0No Response -Total 40 100
90
Detailed Project Report Sub Centre –
Yeroor Grama Panchayath
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Analysis of the responses reveal that even though the Sub Centre is working there independently, it has not succeeded in creating its own identity among the community members. A new building with name board and having adequate physical amenities and manpower will create a positive impression about the Sub Centre among the people and it would motivate them to make use of the services effectively.
Use of the health care services provided at the Main Sub centre by the respondents
A sizable portion of the respondents (70%) stated that they have made use of the health care services provided at the Sub Centre. Thirty percent responded that they have not used the health care service available at the Main Sub centre. They also added that they are not fully aware of the health care services provided at the Main Sub centre.
Table-10
Use of the health care services provided at the Sub centre by the respondents Response
Frequency Percentage
Made use of the health care services 28 70
Not used the health care services 12 30 No Response -
Total 40 100
The analysis in Table 10 shows that majority of the respondents have utilised the services of the Sub Centre. This interest noticed among the community members should be encouraged and strengthened by offering quality services and adding new and innovative medical care support at Sub Centre level.
Resul Pookutty Foundation
91
Detailed Project Report
Sub Centre – Yeroor Grama
Panchayath
Efficiency and usefulness of the health care services which are being provided by the Main Sub centre to ordinary people
Respondents were asked rate the quality of services provided at the main Sub Centre. A total of 70% respondents stated that efficiency and usefulness of the health care services which are being provided by the Main Sub Centre to ordinary people are ‘reasonably good.’ Nobody who participated in the study stated that the services they received from the Sub Centre was very good.
Thirty per cent differed from the rest and said that the health care services received from Sub Centre was not effective.
Table-11
Efficiency and usefulness of the health care services which are being provided by the Sub centre
Response Frequency Percentage Very good 0 0 Reasonably Good 28 70 Not Effective 12 30 No Response -Total 40 100
Adequacy of the space currently available at the Yeroor Main Health Sub Centre
Currently the Sub Centre is functioning in limited space, having one room for the staff and one hall for medical examination and all other purposes. With regard to the adequacy of the space currently available at the Yeroor Main Health Sub Centre, while 25% of the respondents said that the Sub Centre has adequate space, 75% disagree with them and said that the available space is inadequate.
Table-12
Adequacy of the space currently available at the Yeroor Main Sub Centre
Response
Frequency Percentage
Adequate Space is available 10 25 Available space is inadequate 30 75 No Response -Total 40 100
Resul Pookutty Foundation
92
Detailed Project Report
Sub Centre – Yeroor Grama
Panchayath
Majority of the respondents are much worried about the inadequate space available at Sub Centre. Some respondents openly said that they are not interested to come there to take immunisation for their kids because of the non-availability of convenient space for feeding their babies.
Data analysis in Table 12 shows that it is very essential to ensure that adequate space is available to the Yeroor Main Sub Centre in order to effectively discharge their duties and responsibilities in relation to public health care. Further, people come to the Sub Centre for various types of medical care support and they need adequate space to sit; otherwise it would demotivate them to come there and make use of the available services.
Sufficiency of the available amenities / facilities at Main Sub Centre
Respondents were asked to indicate the adequacy of equipment and other facilities at the sub centre.
Sufficiency of the available Medical equipment at Main Health Sub Centre
Respondents have some serious concerns about the availability of medical equipment at Main Sub Centre. Forty-five percent of the respondents said that medical equipment are sufficient. However, the majority stated that the Sub Centre do not have sufficient medical equipment.
Table-13
Sufficiency of the available Medical equipment at Main Health Sub Centre
Response Frequency Percentage Sufficient 18 45 Insufficient 22 55 No Response -Total 40 100
The analysis of the response reveals that immediate attention and corrective measures are required to strengthen the availability of medical equipment at the Sub Centre which will help to minimise the apprehensions to some extent.
Resul Pookutty Foundation
93
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Sufficiency of the Beds at Main Health Sub Centre
There is high degree of dissatisfaction among the respondents in respect of the availability of beds at Main Health Sub Centre. According to them currently as part of the Sub Centre no such facility is available to the community. All of the respondents opined that beds at Main Sub Centre are insufficient.
Table-14
Sufficiency of the Beds at Main Health Sub Centre
Response
Frequency Percentage
Sufficient 0 0
Insufficient 40 100
No Response -Total 40 100
All respondents emphasised that some rooms and beds should be made available as a part of Sub Centre. Lack of satisfaction among the respondents is truly an obstacle in making use of the available services at the Sub Centre.
Sufficiency of the Furniture at Main Health Sub Centre
The study revealed that the respondents are generally dissatisfied with the availability of the Furniture at Main Sub Centre.
Table-15
Sufficiency of the Furniture at Main Health Sub Centre
Response
Frequency Percentage
Sufficient 14 32.5
Insufficient 27 67.5
No Response - -
Total 40 100
More than two-third of the respondents complained that Main Health Sub Centre does not have sufficient furniture. Some of them are fed up with the inadequacy of furniture at the Sub Centre.
Resul Pookutty Foundation
94
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
The above analysis reveal that the available amenities / facilities at Main Sub Centre is meagre and this not only adversely affect their efficiency and functioning but also reduces the quality of services offered there. Appropriate action is needed to minimise the issues, retain their effectiveness and improve the quality of services.
Better facilities at the Sub Centre will provide community members with greater motivation to make use of the health care services and thereby improve the health status of the community.
For what kind of services do people go to the Main Health Sub Centre?
The community members’ responses presented in Table 16 exhibit a clear picture for the kind of services for which people go to the Main Sub Centre.
Table-16
For what kind of services do people go to the Main Health Sub Centre
Response Frequency Percentage
Immunisation 22 55 Pre-natal & post-natal check-up 10 25 Life style disease tests 7 17.5 First aid 1 2.5 No ResponseTotal 40 100
As many as fifty-five percent of the respondents opined that they go to the Main Health Sub Centre for immunisation. Twenty-five percent reported that they are making use of the Prenatal & post-natal check-up service of the Sub Centre. Of the remaining, 17.5% of the respondents go for life style disease tests. Only one person responded that he has gone there for first aid facility.
The responses revealed that the major services presently offered by the Sub Centre such as immunisation, Pre-natal & post-natal check-up and life style disease tests have reasonably good acceptance among the community but the Sub Centre needs to offer more services to cater to other health care needs of community members, especially for the aged, differentially abled and adolescent groups. Presently, the Sub Centre is offering very minimum programmes for these groups. So they are dissatisfied with the service of Sub Centre.
Resul Pookutty Foundation
95
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
It was learned that due to lack of facilities like computer and internet connection at Sub Centre, staff members after their daily field work are spending more of their time in PHC and CHC for their documentation, communication and other office related activities. As a result, community members are not in a position to come to the Sub Centre on a regular basis and make use of the expertise and service of the Junior Public Health Nurse and Junior Health Inspector.
Additional Health care and related services expected by the respondents from the Main Health Sub Centre
About one-fourth of the respondents pointed out that Medicine distribution for NonCommunicable Diseases is an additional service that they expected from the sub centre, which is currently done at the PHC and it is creating a lot of inconvenience to them.
Table-17
Additional Health care and related services expected by the respondents from the Main Health Sub Centre
Response
❖ Frequency Percentage
Medical camps 15 14.7 Medicine distribution for Non Communicable Disease 25 24.5 Palliative care support 5 4.9 Health education 10 9.8 IEC (Information Education & Communication) Support 10 9.8 Periodic clinics (gynaecology, paediatrics, skin, cancer etc.) 12 11.8 Testing Labs 25 24.5 Total 102 100
❖ Multiple responses
Another 25% of the respondents said that testing lab facility is the service that they expect from sub centre. About 15% of the respondents stated that they expected periodic medical camps in collaboration with government and non-government organisations. Periodic clinics related to gynaecology, paediatrics, skin, cancer, etc. would be a welcome addition (11.8%). Health education (9.8%), IEC (Information Education & Communication) Support (9.8%) and
Resul Pookutty Foundation
96
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Palliative care support (4.9%) are the other services that respondents expect from the Sub Centre.
Need for facilities for more diagnosing/ testing at Main Health Sub Centre
It is a cherished desire of respondents. In the study, most of the respondents (95%) indicated that the facilities for more diagnosing/ testing at Main Sub Centre are very essential because now people are depending on two private laboratories and they are charging high for such services.
Table-18
Need of the facilities for more diagnosing testing at Main Health Sub Centre
Response Frequency Percentage
Essential 38 95 Not essential 2 5 No Response -Total 40 100
Moreover, they said that they are more worried about the quality of the testing and accuracy of the results obtained from the private labs.
The illness can be reduced to the minimum level by conducting periodical medical check-ups. It will help to find the probability of illness in advance. Prevention of illness is better than cure therefore it is essential that the community should be provided with facilities for more diagnosing/ testing at the Sub Centre.
Possibility for objection about the creation of community health status database at Main Sub Centre and its online use for the subsequent treatment of the patients
Respondents were asked to reveal their reactions to creation of community health status database at the Main Sub Centre and its online use for the subsequent treatment of the patients.
While 10% of the respondents reported high possibility of objection, ninety percent respondents reported that they did not have any objection.
Resul Pookutty Foundation
97
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Table-19
Objection about the creation of community health database at Sub Centre and its online use for the subsequent treatment of the patients
Response Frequency Percentage
Objection 4 10 No Objection 36 90 No Response -Total 40 100
A fairly good percent of them said that availability of such a comprehensive database about the health status of the community members at Sub Centre would be an advantage for their future treatment. However, some of them pointed out that the database should be updated regularly and some mechanism should be developed to ensure that the data manipulation do not occur at any level.
The responses indicate that there is scope for the creation of community health database at the Sub Centre and its online use for the subsequent treatment of the patients, but its maintenance, updating and data security are the major challenges which will arise in future. The data manipulation can be reduced to a minimum level, if necessary preventive measures are taken.
Interest in making use of the services for tele-medicine and other virtual consultations with doctors if it is available through the Main Health Sub centre Respondents are generally interested in making use of the services for tele-medicine and other virtual consultations with doctors (Table 20).
More than ninety percent of the respondents expressed their interest in making use of the services for tele-medicine and other virtual consultations with doctors if it is available through the Main Sub centre. Only 7.5% of the respondents were of the opinion that they are not interested in making use of the services.
98
Resul Pookutty Foundation
Table-20
Interest in making use of the services for tele-medicine and other virtual consultations with doctors
Response Frequency Percentage
Interested 37 92.5 Not Interested 3 7.5 No Response -Total 40 100
The responses show that majority of the respondents are happy with the innovative telemedicine and other modern practices like virtual consultation with doctors.
Need for reconstruction of the Yeroor Main Health Sub Centre
Respondents were asked to comment on the need for reconstruction of the Yeroor Main Sub Centre. While 40% of the respondents reported that new building with adequate facilities is very essential 60% of them were of the opinion that it is essential. Nobody who participated in the study mentioned that the reconstruction is not required.
Table-21
Need for the reconstruction of the Yeroor Main Health Sub Centre
Response Frequency Percentage
Very essential 16 40 Essential 34 60 Not required 0 0 Total 40 100
These responses give an impression that community members are strongly in favour of the reconstruction of the Yeroor Main Sub Centre and they are expecting a fully equipped and functional health sub centre with adequate infrastructure.
Resul Pookutty Foundation
99
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Sub Centre – Yeroor Grama Panchayath
DEMAND ESTIMATE FOR THE PROPOSED SUB CENTRE AT YEROOR
Based on inputs from the health professionals working in the Main Sub Centre, patient inflow statistics have been worked out.
Patient inflow for the SC at Yeroor The average monthly patient inflow to the Main Sub Centre at present is as follows:
Projected Patient inflow for the proposed SC at Yeroor With improved facilities and services proposed for the Yeroor Main Sub Centre, the demand for the services are likely to increase substantially. Based on discussions with the health professionals at the Main Sub Centre and the PHC, the patient inflow for the proposed Sub Centre at Yeroor has been estimated as follows:
Detailed Project Report
100
Resul Pookutty Foundation
1.
2.
3.
4.
Total
Immunisation 90
NCD 175
Antenatal / postnatal services 30
IUCD 5
305
MONTHLY PATIENT INFLOW OF MAIN SUB CENTRE, YEROOR SNo Health Care Service Number of Beneficiaries Current Health Care Service Present Projected 1 Immunisation 90 150 2 Ante-natal / postnatal Care 30 40 3 Non Communicable Diseases Check up 175 250 4 IUCD 5 10 Sub Total 305 450 Additional Health Care Services Proposed 5 Lab Testing 150 6 Pharmacy with NCD/Palliative Care Medicine Distribution 300 7 Tele- Medicine 50 8 Health Clinics (Gynaecology, Paediatrics, Skin, Cancer etc.). Four Programmes in one month with 25 participants 100 9 Medical Camps (Eye, Skin, Cancer Detection, etc.). One Programme in one month 50 Total 305
PROPOSED
1100
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
MARKET STUDY: DISCUSSIONS WITH DOCTORS, HEALTH CARE PROFESSIONALS AND OTHER DEVELOPMENT ACTORS
1. INTRODUCTION
Detailed personal interviews and focus group discussions were held with 15 key actors consisting of Doctors, Public Relation officer, Elected Representatives, Officials, Health supervisors, Health Inspectors, Public Health Nurses and other health care professionals working in the Anchal community Health Centre, Yeroor Primary Health Centre and Yeroor Main Sub Centre, Yeroor Gram Panchayat, etc. regarding the services to be offered and the facilities to be created. The major findings of the interviews and focus group discussion are summarised below.
Weekly Antenatal care, Immunisation Programme for children up to the age group of 16 years and Non Communicable Diseases (NCD) clinic to check blood pressure and sugar levels on every Thursday are the popular services of the Main Sub Centre used by the community.
Presently the Yeroor Main Sub Centre is providing the following services to the community members.
• Antenatal care on every Monday.
• Immunisation Programme for children up to the age group of 16 years, on every Wednesday.
• Non Communicable Disease (NCD) clinic to check blood pressure and sugar level on every Thursday.
• Awareness generation orientation programmes in collaboration with Anganwadies which function under ICDS project.
• Regular House Visits, collection of health related data and providing follow up support to the needy.
2. OPINION ON ADDITIONAL SERVICES TO BE OFFERED IN THE SUB CENTRE
The additional services to be offered in the sub centre suggested by doctors, health care professionals and other development actors include the following:
Resul Pookutty Foundation
101
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
❖ Organise regular Medical camps like eye camp, skin camp, Non Communicable Disease identification camp, early cancer detection camp, etc.
❖ Organise monthly clinics related to gynaecology, cardiology, gastroenterology, geriatrics.
❖ Conduct adolescence clinics for both males and females to provide counselling, awareness generation and other support to reduce their mental stress with the support of clinical psychologists.
❖ Provide lab testing services and ECG facility to the community.
❖ Organise occasional health education orientation programmes on health and hygiene, epidemic/pandemic, sanitation, communicable and non-communicable diseases for parents and children.
❖ Develop electronic health programme i.e., create health related database of the community members and share the data through an online medium to doctors at PHC, CHC and other higher level hospitals and thereby help them to provide tele-medicine service in an efficient and speedy manner. (It was mentioned that Health department under Government of Kerala has already initiated similar steps to develop such an ehealth programme and more than 80% of the data collection has been completed in Kollam district.)
❖ Organise Life skill education/trainings for adolescent and youth groups in collaboration with other agencies.
❖ Conduct job oriented training and motivational support to differently abled persons in collaboration with government and non-government agencies working in this field to bring them back to normalcy.
❖ Provide Geriatric care and support in an efficient and time bound manner.
❖ Pharmacy support in sub centre will be beneficial to the community because it will not only reduce the work load of the pharmacy counter at the PHC but also improve the efficiency medicine distribution system. The non- availability of pharmacist will become a major constraint in implementing such a support.
Resul Pookutty Foundation
102
Yeroor Grama Panchayath
3. OPINION ON THE FACILITIES TO BE CREATED
According to doctors, health care professionals and other development actors, the following facilities are to be created in the sub centre to make it more functional and efficient in delivering the health care services to the community, especially the marginalised sections.
• Ante Natal Area
• Injection/Emergency Care Area
• Doctors Room
• JPHN AND JHI Room
• Asha Worker Room
• Multipurpose Conference Room for orientations, training programmes, workshops, Yoga and medical camps
• Store Room
• Feeding Area
• Patient waiting Area • E-Health Room • Pharmacy Room • IUCD Room • Toilets • Staff Accommodation • Facility for Waste Management • Play area for Kids
Resul Pookutty Foundation
103
Detailed Project Report Sub Centre –
Furniture ❖
❖
Equipment and
Incinerators
Water purifiers and other water supply facilities ❖ Recreational sets like Television, Music System, etc. ❖ Audio Visual equipment like LCD Projector, Video Camera ❖ Inverter ❖ Deep Freezer ❖ Playing sets for Kids ❖ Sports Kits ❖ Furniture such as tables, chairs, shelf, racks etc.
KEY SUCCESS FACTORS AND RISKS FACTORS
Key Success Factors
Discussions with experts indicate the following success factors for the project:
❖ High demand for medical care facility in the proposed area
❖ Lack of sufficient health care institutions in the proposed project area
❖ Inadequate infrastructure and other facilities in the existing PHC and Main Health Sub Centre
❖ Positive attitude of doctors and other health care professionals towards the proposed project
❖ Socio economic backwardness of the project area
❖ Positive attitude of community members
❖ Availability of land for construction and related activities
Key Risks Factors
Discussions have revealed some risk factors for the project:
❖ High maintenance cost
❖ Lack of manpower to offer additional health care services
❖ Chance for ineffective utilisation of the facilities created after the withdrawal of the project implementing agency
❖ Over burden on the part of Panchayati Raj Institutions to meet the operating expenses
The respondents stated that setting up of a full-fledged public health sub centre with modern facility will not only improve the efficiency of the delivery of the basic health care services to the marginalised communities but also will create a sustainable model which government and other agencies can replicate in other parts of the state and the country.
Resul Pookutty Foundation
104
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Sub Centre – Yeroor Grama Panchayath
SUMMARY OF FINDINGS OF THE MARKET STUDY
This section provides a summary of the findings of the data analysis provided in four chapters of the report:
1. Public Health Care Situation in India and Kerala
2. Health Care Situation in Kerala
3. Market Survey: Analysis of the Responses of the General Public
4. Study on Opinion of Doctors and Other Health Care Professionals
PUBLIC HEALTH CARE SITUATION IN INDIA AND KERALA
Health Index
Despite the remarkable progress, health remains a critical area that needs improvement. When benchmarked against countries with similar levels of economic development, India is lagging on some critical health indicators.
The second round of Health Index (referred to as Health Index-2018) examined the overall performance and incremental improvement in the States and UTs for the period 2015-16 (Base Year) to 2017-18 (Reference Year), i.e., a two-year period
Kerala leads in the national Health Index. In the Reference Year (2017-18), the average composite Health Index score among the Larger States in India was 53.22, compared to the Base Year (2015-16) average of 52.59. There was a wide disparity of Health Index score across States, ranging from 28.61 in Uttar Pradesh to 74.01 in Kerala
Health infrastructure
As reported in the National Health Profile -2018, the country had a total of 23582 government hospitals with 710761 beds. This included 19810 government hospitals with 279588 beds in the rural sector and 3772 hospitals with 431173 beds in the urban sector (Table. 1)
Kerala had a total of 1280 Government hospitals with 38004 beds at the end of 2017. This was inclusive of 981 government hospitals in the rural sector with 16865 beds and 299 hospitals with 21139 beds in the urban sector.
The country had 5624 CHCs, 25650 PHCs and 156231 Sub Centres as at the end of 2017. The Kerala State had 5380 Sub Centres, 849 PHCs and 232 CHCs. This indicates that the state has approximately 5 Sub Centres per Panchayat. The number of PHCs are less than the
Detailed Project Report
105
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
number of Panchayats and almost 20 % of the Panchayats do not have any PHCs. The number of CHCs are also far inadequate.
Health Financing in India
Compared to countries that have either Universal Health Coverage or moving towards it, India’s per capita public spending on health is low.
➢ Total public expenditure on health for the year 2015-16 stood at Rs 1.4 lakh crores.
➢ Per capita public expenditure on health in nominal terms has gone up from Rs 621 in 2009-10 to Rs 1112 in 2015-16.
➢ Public expenditure on health as a percentage of GDP was 1.02% in 2015-16. There is no significant change in expenditure since 2009-10.
➢ Public expenditure on health as a percentage of GDP is 5.2% among the High Income countries, 3.8 % among the Upper Middle Income countries, 2.5 % among the Lower Middle Income countries and 1.4 % among the Low Income countries. India’s Public health expenditure less than that of the low income country groups – hardly around 1 %.
In comparison, some of the developed countries have considerably more spending on public health as per cent of their GDPs. While the US spends 8.5 % of the GDP, some of the European countries spend even more - Sweden 9.2%, France 8.7 %, Denmark 8.7%, and Belgium 8.6 %.
Centre-State share in expenditure on health
According to the National Health Profile 2018, Central Bureau of Health Intelligence, the Centre-State share in total public expenditure on health was 31:69 in 2015-16.
Total public expenditure on health in 2015-16 was Rs 140,054 crores, with Medical and Public Health comprising the major share (78.7%)
Among the major states, health expenditure as a percent of State GDP is highest in Jammu & Kashmir (2.46%), followed by Himachal Pradesh (1.68 %)and Goa (1.34 %).
In Kerala the public expenditure on health is relatively low; it is only 0.93%. The total state expenditure was Rs. 5207 crores in 2017. As percentage of total state expenditure, expenditure on health was 5.85%.
Resul Pookutty Foundation
106
Detailed Project Report
Sub Centre – Yeroor Grama
Panchayath
Per capita public health expenditure is also rather low in Kerala – Rs. 1463, while in Goa it was Rs. 3643, in Himachal Pradesh Rs.2667 and in Jammu & Kashmir Rs.2359.
Health Expenditure by Families
Based on Health Survey (71st round) conducted by NSSO, average medical expenditure incurred during stay at hospital from Jan 2013 - Jun 2014 was Rs. 14,935 for rural and Rs. 24,436 for urban in India
Around 43 crore individuals were covered under any health insurance in the year 2016-17. This amounts to 34% of the total population of India. 79% of them were covered by public insurance companies.
Overall, 80% of all persons covered with insurance fall under Government sponsored schemes.
House hold savings form the major source of finance for over two third of the households, followed by borrowing as reported by around 25 % of the families. Contribution by friends, relatives and others form another important source.
HEALTH CARE SITUATION IN KERALA
Data for this part of the analysis have been drawn from the ‘Report on Health in Kerala NSS 71st Round - January – June 2014’.
Morbidity and Hospitalisation
Morbidity is very high in Kerala, compared to other states. In India about 9% of rural population and 12% of urban population reported ailment during a 15 day reference period, a period of 15 days prior the household survey.
Data reveals that in Kerala about 19% of rural population and 22% of urban population reported ailment during a 15 day reference period.
For 90% in both the urban and rural sectors, treatment was in Allopathy. Around 5 percent depends on ISM (Ayurveda, Yoga or Naturopathy Unani, Siddha and homoeopathy).
Around 37% hospitalisation took place in public hospital, and 63% in private hospital in both rural and urban area.
Resul Pookutty Foundation
107
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
The rural population spent, on an average, Rs.14001 for a hospitalised treatment and Rs.18324 for that in urban sector. The average total medical expenditure for non-hospitalised (outpatient) treatment per ailing person for different classes
For people in the lowest class the average medical expenditure each time they have an ailment is Rs. 304 in the rural area and Rs. 371 in the urban area. Among the highest 20% category the expenditure is Rs. 629 in the rural area and Rs. 604 in the urban area.
Childbirth and Maternity Care Services
➢ In 99.6 percent of the cases the child births were in hospitals. In the rural areas, about 0.4% of the childbirths were at home or any other place.
➢ About 31% of childbirths took place in public hospitals and 68% in private hospitals.
➢ Lower the economic quintile class (20 % of the population) the higher the proportion of institutional childbirths that take place in public hospitals as compared to private hospitals. Free bed was utilized for 90% of childbirths at public hospitals.
➢ Contrary to public hospital scenario, in private hospitals, 98% childbirth took place in paying.
➢ An average of Rs. 2057 was spent per childbirth in public hospitals and Rs. 20737 in private hospitals, which is around 10 times more than that of the government institutions
➢ In the rural areas about 99.8 per cent of pregnant women took some pre-natal care, where as in urban area corresponding figure was 97.8 per cent.
➢ About 90.4 per cent of pregnant women took some post-natal care, where as in urban area corresponding figures was 94.5 per cent.
Status of the Aged Persons (60 and above)
➢ India has around 1038 lakhs elderly persons (8.6% of the population comprising 60 plus population, Census 2011) and Kerala has 41.93 lakhs elderly persons (12.55% of the population comprises 60 plus population, Census 2011). An overwhelming majority of the elderly live in rural areas and there is an increasing proportion of oldoldest age category with feminization of ageing being more pronounced at this age.
Resul Pookutty Foundation
108
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
➢ The 2014 NSS survey in Kerala revealed that around 26% of the aged in rural and 31% in urban were not depended on others for their day-to-day needs.
➢ The dependence was very high for elderly females. Among them, about 85 per cent aged women in rural and 80% women in urban were economically dependent either partially or fully.
➢ Most of the economically dependent aged persons- 89% in rural and 85% in urban depend on their children for financial support and a sizable proportion (6% in rural and 8% in urban) on their spouses.
➢ Among the aged persons about 2 per cent of were confined to their home and 4 per cent were confined to bed.
LIFE STYLE DISEASES IN KERALA
In Kerala, the prevalence of lifestyle diseases like diabetes, heart disease, high blood pressure and obesity is high and it results in very high mortality and morbidity from malignant heart disease.
The prevalence of risk factors is high even in rural Kerala: diabetes 20%, high blood pressure 42%, high cholesterol (>200mg/dl) 72%, smoking (42% in men) and obesity (body mass index >25) 40%, physical inactivity 41%, unhealthy alcohol consumption 13%.
Kerala is known as diabetes capital of India as prevalence of diabetes is high i.e. 20% which is double the national average of 8%.
In Kerala 14% of all deaths are caused by coronary heart disease (CHD/CAD)and the mortality rates for CAD (coronary artery disease) per 100,000 are 382 for men and 128 for women which is actually 3 to 6 times higher than Japanese, Chinese and other industrialized countries.
Cancer
As per cancer registry data, in Kerala there are 974 female and 913 male cancer patients per million. In one year, Kerala has roughly 35,000 new cancer cases occurs. The prevalence rate for cancer in rural Kerala is 19.8 per 100,000, while in the urban areas, it is 30.5 per 100,000 people.
Resul Pookutty Foundation
109
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
MARKET SURVEY: ANALYSIS OF THE RESPONSES OF THE GENERAL PUBLIC
A market survey was conducted among people in Bharathipuram (ward X) and Pathadi (ward XI) wards of Yeroor Gram Panchayat who are the prime beneficiaries of services offered at the Main Sub centre at Yeroor. A random sample of 40 respondents of all age groups above 20 years including males and females were conducted. The objective of the study was to understand the health care needs of the public in the geographical area, to identify the facilities required and the specific services to be provided while designing the project as well as to establish the rationale behind this project.
Socio-economic Background
The survey indicates that 45% of the respondents belong to the BPL and below BPL categories. The fact that 45 % of the respondents in a random selection belongs to BPL and below categories indicates that the people of the area are economically backward.
Healthcare facilities in the Panchayat
There is high degree of dissatisfaction among the respondents (90%) regarding the availability of sufficient medical treatment facilities in Yeroor Panchayat. Regarding the availability of government medical facilities in Yeroor panchayat eighty percent of the respondents have reported high dissatisfaction. The Public Health Centre is the only available medical treatment facility in Yeroor panchayat and it is functioning with one doctor from 9am to 2pm, with limited space and minimum facilities. While almost 70 % of the people in Kerala reportedly depend on private health care facilities, it is surprising that there is no private hospital or clinic in the Yeroor panchayat. Private hospitals are available only at Anchal area which is 10 Kilo Meters away from Yeroor Panchayat or at Punalur, which is still farther. With regard to the availability private testing labs in Yeroor Panchayat, 75% of the respondents reported that sufficient number of private testing labs are not available in Yeroor Panchayat. Two private clinical laboratories are available in the panchayat with limited facilities. Some respondents pointed out that as a part of PHC a testing lab was started recently but it has very limited facility in terms of equipment and manpower and testing is done there manually.
110
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Using the Services of the Yeroor Main Sub Centre
All respondents are aware of Main Sub centre functioning in the premises of the PHC at Yeroor, although it does not even have a Name Board and some people think that it is part of the PHC. Most of the respondents reported that they have made use of the services of the Sub Centre. However, while rating the quality of services received from the Sub Centre, none of the respondents rated it as very good, but 70 % rated the services as ‘reasonably good.’
As many as fifty-five percent of the respondents have gone there for immunisation. Twentyfive percent reported that they are making use of the Pre-natal & post-natal check-up service of the Sub Centre. Of the remaining, 17.5% go there for life style disease tests. One person had gone there even for first aid facility.
Physical Facilities
A new building with adequate physical amenities and manpower will create a positive impression about the Sub Centre among the people and it would motivate them to make use of the services effectively.
With regard to the adequacy of the space currently available at the Yeroor Main Sub Centre, 75% of the respondents reported that the available space is inadequate. Majority of the respondents felt that the Sub Centre do not have sufficient medical equipment, furniture or bed. The responses reveal that immediate attention and corrective measures are required to increase the space availability and to strengthen the availability of medical equipment and other facilities at the Sub Centre and these would help to minimise the apprehensions to some extent.
New Services & Facilities
Another 25% of the respondents said that testing lab facility is the service that they expect from sub centre. About 15% of the respondents stated that they expected periodic medical camps in collaboration with government and non-government organisations. Periodic clinics related to gynaecology, paediatrics, skin, cancer, etc. would be a welcome addition (11.8%). Health education (9.8%), IEC (Information Education & Communication) Support (9.8%) and Palliative care support (4.9%) are the other services that respondents expect from the Sub Centre.
Resul Pookutty Foundation
111
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Most of the respondents (95%) indicated that the facilities for more diagnosing/ testing at Main Sub Centre are very essential because now people are depending on two private laboratories, where the test results are unreliable and the charges are very high.
Digital Data Base & Telemedicine
Respondents were asked to reveal their reactions to creating a community health status database at the Main Sub Centre and its online use for the subsequent treatment of the patients.
While 10% of the respondents were suspicious, ninety percent reported that they did not have any objection. Most of them said that availability of such a comprehensive database about the health status of the community members at Sub Centre would be an advantage for their future treatment.
The responses indicate that there is scope for the creation of community health database at the Sub Centre and its online use for the subsequent treatment of the patients. However, its maintenance, updating and data security are the major challenges which may arise in future.
The data manipulation can be reduced to a minimum level, if necessary preventive measures are taken.
More than ninety percent of the respondents expressed their interest in making use of the services for tele-medicine and other virtual consultations with doctors if they are available through the Main Sub centre.
Reconstruction of the Yeroor Main Sub Centre
Respondents were asked to comment on the need for reconstruction of the Yeroor Main Sub Centre. While 40% of the respondents reported that new building with adequate facilities is very essential 60% of them were of the opinion that it is essential. Nobody who participated in the study mentioned that the reconstruction is not required.
These responses give an impression that community members are strongly in favour of the reconstruction of the Yeroor Main Sub Centre and they are expecting a fully equipped and functional health sub centre with adequate infrastructure.
Resul Pookutty Foundation
112
4. STUDY ON OPINION OF DOCTORS AND OTHER HEALTH CARE PROFESSIONALS
Services to be offered
➢ Organise regular Medical camps like eye camp, skin camp, Non Communicable Disease identification camp, early cancer detection camp, etc.
➢ Organise monthly clinics related to gynaecology, cardiology, gastroenterology, geriatrics.
➢ Conduct adolescence clinics for both male and female to provide counselling, awareness generation and other support to reduce their mental stress and strain with the support of clinical psychologist
➢ Provide lab testing services and ECG facility to the community.
➢ Organise occasional health education orientation programmes on health and hygiene, epidemic/pandemic, sanitation, communicable and non-communicable diseases for parents and children.
➢ Develop electronic health programme i.e., create health related database of the community members and share the data through an online medium to doctors at PHC, CHC and other higher levels hospitals and thereby help them to provide tele-medicine service in an efficient and speedy manner.
➢ Organise Life skill education/trainings for adolescent and youth groups in collaboration with other agencies.
➢ Conduct job oriented training and motivational support to differently abled persons in collaboration with government and non-government agencies working in this field to bring them back to normalcy.
➢ Provide Geriatric care and support in an efficient and time bound manner.
➢ Pharmacy support in sub centre will be beneficial to the community because it will not only reduce the work load of the pharmacy counter at PHC but also improve the efficiency medicine distribution system. The non- availability of pharmacist will become a major constraint in implementing such a support.
Facilities to be created
According to doctors and other health care professionals the following facilities to be created in the sub centre to make it more functional and efficient in delivering the health care services to the community especially the marginalised sections.
Resul Pookutty Foundation
113
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
• Injection/Emergency Care Area
• Doctors Room
• JPHN AND JHI Room
• Asha Worker Room
• Multipurpose Conference Room for orientations, training programmes, workshops, Yoga and medical camps
• Store Room
• Feeding Area
• Patient waiting Area • E-Health Room • Pharmacy Room
Equipment and Furniture
Key Success Factors
Resul Pookutty Foundation
114
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
• IUCD Room
• Toilets • Staff Accommodation
• Facility for Waste Management
• Play area for Kids
Incinerators
Water purifiers
Recreational
Audio
Inverter
Deep Freezer
Playing
Sports Kits
Furniture
❖
❖
and other water supply facilities ❖
sets like Television, Music System etc. ❖
Visual equipment like LCD Projector, Video Camera ❖
❖
❖
sets for Kids ❖
❖
such as tables, chairs, shelf, racks etc.
➢ High demand for medical care facility in the proposed area ➢ Lack of sufficient health care institutions in the proposed project area
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
➢ Inadequate infrastructure and other facilities in the existing PHC and Main Health Sub Centre
➢ Positive attitude of doctors and other health care professionals towards the proposed project
➢ Socio economic backwardness of the project area
➢ Positive attitude of community members
➢ Availability of land for construction and related activities
Key Risks for the Project Proposed
➢ High maintenance cost
➢ Lack of manpower to offer additional health care services
➢ Chance for ineffective utilisation of the facilities created after the withdrawal of the project implementing agency
➢ Over burden on the part of Panchayati Raj Institutions to meet the operating expenses
CONCLUSIONS AND RECOMMENDATIONS
1. CONCLUSIONS OF THE STUDY
Despite the remarkable economic progress in India, the health sector remains an area of concern and when benchmarked against countries with similar levels of economic development, India is lagging on some critical health indicators. Public expenditure on health as a percentage of GDP is around 1%, compared to 8.5% in the US and more than that in several European countries.
Of course Kerala leads in the national Health Index. However, the public healthcare sector in the state is beset with several problems. In Kerala the public expenditure on health is relatively low; it is only 0.93%. Per capita public health expenditure is also rather low in Kerala – Rs. 1463, while in Goa it is Rs. 3643, in Himachal Pradesh Rs.2667 and in Jammu & Kashmir Rs.2359.
Morbidity is very high in Kerala, compared to other states. While the all India morbidity rate is 9% in rural areas and 12% among urban population, in Kerala morbidity affects 19% of rural population and 22% of urban population.
Resul Pookutty Foundation
115
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
The prevalence of lifestyle diseases like diabetes, heart disease, high blood pressure and obesity is high in Kerala, and it results in very high mortality and morbidity. The prevalence of risk factors is high even in rural Kerala: diabetes 20%, high blood pressure 42%, high cholesterol 72%, and obesity 40%, physical inactivity 41% and unhealthy alcohol consumption 13%.
Kerala is known as diabetes capital of India as prevalence of diabetes is high i.e. 20% which is double the national average of 8%.
In Kerala 14% of all deaths are caused by coronary heart disease and the mortality rates per 100,000 are 382 for men and 128 for women, which is actually 3 to 6 times higher than in Japan, China and other industrialized countries.
The prevalence rate for cancer in rural Kerala is 19.8 per 100,000, while in the urban areas, it is 30.5 per 100,000 people, much higher than the national average.
The rural population spent, on an average, Rs.14001 for a hospitalised treatment and Rs.18324 for that in urban sector.
Obviously the State government is not in a position to make considerable investment in health care infrastructure. A possible alternative would be health care infrastructure by NGOs and charitable organisations. Investments by such institutions were the real secret of the Kerala model development, at least in the health care sector.
The situation of the health care sector in the project area is very precarious. There are no private hospitals or dispensaries in the Yeroor panchayat. Public Health Centre at Bharathipuram is the only available medical treatment facility in Yeroor panchayat and it is functioning with one doctor from 9am to 2pm, with limited space and minimum facilities.
Presently people from all the 19 wards of the Yeroor Gram panchayat and some wards of Kulathupuzha Gram panchayat are making use of the service of the PHC.
Case load in the area for the existing institutions is quite high. For instance, the PHC is over crowded with patients and as a result the doctor and other health professionals are not in a position to give proper care and attention to the patients. The field survey indicates several limitations with respect to the facilities and services offered by the sub centres.
The study reveals that there is need for strengthening the public healthcare institutions in the Yeroor Panchayat. The Main Sub Centre is definitely a candidate who needs support.
Resul Pookutty Foundation
116
2. RECOMMENDATIONS FOR PROMOTION
A major risk factor in implementing the proposed project is public apathy towards government owned and managed health care institutions. This calls for confidence building measures to motivate the public to make effective use of the facilities created. Several measures have been suggested by experts as well as the public during the study, as indicated in the report.
Some of these could be adopted as promotional tools:
➢ Building and physical facilities with good ambiance that would attract children, adolescents and the old, besides the middle aged groups.
➢ Targeting specific healthcare programmes relevant to these specific groups. Segmentation, targeting and positioning strategies could be used effectively.
➢ Offer recreational programmes and opportunities for social interaction to different target groups – for example, the former for the young and the latter for the aged.
117
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
*****
MARKET SURVEY: YEROOR MAIN SUB CENTRE RESEARCH SCHEDULE
Name of Respondent ……………………………. Place ………………………. Phone ………………... Gender ……………. Age…………. Ration Card Category…………………….
1. Do you think there are sufficient medical treatment facilities in Yeroor Panchayat?
Yes [ ] No [ ]
2. In the Government sector, do you think there are sufficient medical treatment facilities in Yeroor Panchayat?
Yes [ ] No [ ]
3. In the private sector do you think there are sufficient medical treatment facilities in Yeroor Panchayat?
(a) Hospitals: Yes [ ] No [ ] (b) Clinics: Yes [ ] No [ ](c) Testing labs: Yes [ ] No [ ]
4. Are you aware of the Health Sub centre functioning in the premises of the PHC at Yeroor?
Yes [ ] No [ ]
5. Have you ever made use of the health care services provided at the Sub centre?
Yes [ ] No [ ]
6. Do you think this Sub Centre is providing useful health care services to ordinary people?
(a) Very good service [ ] (B) Reasonably Good service [ ] (c) Not Effective [ ]
7. Do you consider that the space currently available at the Yeroor Main Sub Centre is adequate?
Yes [ ] No [ ]
8. In your opinion, does this Sub Centre have sufficient amenities / facilities such as?
(a) Medical equipment: Yes [ ] No [ ] (b) Beds: Yes [ ] No [ ] (c) Furniture: Yes [ ] No [ ]
9. For what kind of services do people go to the Sub centre?
(a) Immunisation (b) [ ] Pre-natal & post-natal check-up[ ] (C) life style disease tests[ ]
10. Can you mention some of the additional services that this Sub centre could offer?
(1) ……………………………. (2) ……………………………. (3) ………………………………
11. Do you think facilities for more diagnosing testing would be appropriate?
Yes [ ] No [ ]
12. If the health related data collected through such tests and other means are documented and made available electronically for subsequent treatment of the patient, do you have any objection?
Yes [ ] No [ ]
13. If opportunities for tele-medicine and other virtual consultations with doctors are made available through the Sub centre, would you be interested in making use of the services?
Yes [ ] No [ ]
14. Do you consider the reconstruction of the Yeroor Main Sub Centre as essential?
(a) Very essential [ ] (b) Essential [ ](c) Not required [ ]
118 Resul
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Pookutty Foundation Appendix -1
*****
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
4.3 Topography Survey
A topographic survey gathers data about the natural and man-made features of the land, as well as its terrain. Permanent features such as buildings, fences, trees and streams accurately define the ground and its boundaries. Land contours and spot levels show the elevation of the terrain. This can often be related to national Ordnance Survey grid and datum information (often using GPS) and is surveyed by point. It is typically accepted that points are positioned in three dimensions which facilitates ground modelling and visualisations to be produced from the topographical survey Measurements for topographic surveys are done either with a surveying-quality GPS unit, or with an electronic EDM instrument.
A total station (TS) or total station theodolite (TST) is an electronic/optical instrument used for surveying and building construction. It is an electronic transit theodolite integrated with electronic distance measurement (EDM) to measure both vertical and horizontal angles and the slope distance from the instrument to a particular point, and an on-board computer to collect data and perform triangulation calculations.
In YEROOR the highest point of our site is 9 metres above the adjacent road. The entrance is at road level. And the rear side is 5 metres above the road. Existing structure plinth level has been marked. The flora and fauna of the site is also marked. The level of the public drain at the entrance is also marked. The TBM is marked at a level of 99.3 the road has a width of 16m. The Septic tank, Rainwater harvesting tank, Well, Incineration unit is marked
119
Resul Pookutty Foundation
4.4 Facility Survey
Report
120
Detailed Project
Sub Centre – Yeroor Grama Panchayath
Resul
Pookutty Foundation
StaffCategory InspectionNote Type
121
NearbymajorCities Supply/Generators Ceiling
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
122
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
storagesarefilled,disposalisarrangedbycalling thirdpartyagency Undergroundwellwaterisusedforwatersupply SiteSurveyNo. AvailabilityofInternetConnection
Resul Pookutty Foundation
123
SubcenterinlinewithvisionofAyushmanBharat.Thenewsubcenterisenvisagedtodeliverexpandedrange havededicatedroomsforJPHN,JHI,ASHAWORKER,DOCTORDIETICIAN.Thiscanverywellprotectthepatient Ownershipdocuments
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
124
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
andthesubcenterdifferententities.Thiswouldhelpinmanagingthecrowdin productiveway.
Resul Pookutty Foundation


125
SUBCENTER LADIESWAITINGROOM
Detailed Project Report Sub Centre –
Yeroor Grama Panchayath
Resul Pookutty Foundation
Project Report Sub
–
Panchayath 126 Resul Pookutty Foundation Flashlight/TorchBox-typepre-focused(4cell) Torch(ordinary) DressingDrumwithcover0.945litersstainlessstee Hemoglobinometer setSahlitypecomplete WeighingScale,Adult125kg/280lb WeighingScale,Infant(10Kg) WeighingScale,(baby)hangingtype,5kg SurgicalScissorsstraight140mm,ss SphygmomanometerAneroid300mmwithcuffIS:7652 Kelly’shemostatForcepsstraight140mmss VulsellumUterineForcepscurved25.5cm Cusco’s/GravesSpeculumvaginalbi-valvemedium Simsretractor/depressor SimsSpeculumvaginaldoubleendedISSMedium Cheatle’sForcep Icepackbox Spongeholder PlainForceps MEDICALEQUIPMENTSLIST
Detailed
Centre
Yeroor Grama
Project Report
Panchayath 127 Resul
25 Tooth
26 Needle
27 Suture
28 Suture
29 Kidney
30 Artery
31 Dressing
32 Cord
33 Clinical
34 Talquist
35 Stethoscope 1 36 Foetoscope 1 37 Hub Cutter and
38 Ambu
39 Suction Machine 40 Oxygen
41 Tracking Bag and
1 42 2 Measuring Tape 43 I/V Stand
Detailed
Sub Centre – Yeroor Grama
Pookutty Foundation
Forceps
Holder
needle straight
needle curved
tray
Forceps, straight, 160mm Stainless stee
Forceps (spring type), 160mm, stainless steel
cutting Scissors, Blunt, curved on flat, 160 mm ss
Thermometer oral & rectal
Hb scale
Needle Destroyer
Bag(Paediatric size) with Baby mask
Administration Equipment
Tickler Box (Immunization)
128
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Footstep Lamp Tubelights Mugs Saucepanwithlid Waterreceptacle Rubber/plasticshutting TalquistHbscale 23 Drumwithtapforstoringwater 24 Infantometer HOSPITALFURNITURELIST
Resul Pookutty Foundation
Project
4.5 Geotechnical Investigations
Soil investigation is performed at the Yeroor Main centre site to know the soil bearing capacity and arrive at the foundation requirement for the proposed G+1 building. The test was performed by an approved geotechnical engineer and the detailed report is generated, the same is attached in the Annexure for reference.
The test is conducted using a rotary power drilling machine. One bore hole is taken to a depth of 10m. SPT is conducted in regular intervals in bore hole. Soil is been lab tested and is observed that ordinary gravel is found up to 0.4m from the ground level. Loose lateritic clayey sand with pebbles are found up to 3m , then loose lateritic clayey silty sand was found up to 6m followed by dense weathered sand up to 9.8m. It is recommended to have an isolated foundation within 1.5m and 2m depth.
4.6 Pollution Test
Air quality test is performed using air sampling instruments of Envirotech Instruments. Sample is been tested to check Sulphur dioxide, Nitrogen dioxide, particulate matter less than 10 microns, particulate matter less than 2.5 microns and carbon monoxide levels. It is observed that all the parameters are well within the limits.
4.7 Water Quality Test
Water test is been performed with the objective of knowing the quality of water and making sure it is usable and is not harmful to human health. Water from the well at Yeroor Main centre is collected and tested for the parameters including PH, odour, colour, Turbidity,TDS, hardness, presence of chlorides, sulphates, iron, calcium ,magnesium and calcium carbonates. The concentration levels of all the above parameters items are within the range. Test is also made for finding any Ecoli / Coliform bacteria and the result is found to be absent and hence the water is safe for use.
4.8 Noise Test
Ambient Noise level is measured at the site using the sound level meter. Sound level is measured to be 50.1 dB (A) during the day time at 1m away from the main gate. This level is almost equivalent to the silent zone sound level.
Resul Pookutty Foundation
129
Detailed
Report Sub Centre – Yeroor Grama Panchayath
5. Project Design & Project Components
FUNCTIONAL DESIGN
According to IPHS the Sub-Centres is categorized into types - Type A and Type B. Categorization has taken into consideration various factors namely catchment area, health seeking behaviour, case load, location of other facilities like PHC/CHC/FRU/Hospitals in the vicinity of the Sub-centre. Here the Sub-Centre is Type A category it caters all recommended services. A typical layout plan for type A Subcentre with ANM residence having area of 85 square metres. The minimum covered area of a Sub-centre along with residential quarter for ANM will vary depending on land availability, type of Sub-centre and resources.
In view with the IPHS standards we have created a design with exploration of different aspects of the changing society and with additional services. The services offered in the Sub-Centre according to IPHS are:- Maternal Health, Child Health, Family Planning and Contraception, Safe Abortion Services (MTP), Curative Services, Adolescent Health Care, School Health Services, Control of Local Endemic Diseases, Disease Surveillance, Integrated Disease Surveillance Project (IDSP), Water and Sanitation, Outreach/Field Services, Communicable Disease Programme, Non-communicable Disease (NCD) Programmes, Promotion of Medicinal Herbs, Record of Vital Events. With respect to these services some additional modern utility services of E-health are proposed with space for pharmacy to promote Govt. owned pharmacies and Yoga to envisage the Ayushman Bharat program of Fit India.
The design for the peripheral contact is pivotal for the development of the health care system in our country. The physical and functional aspects of Sub-centre provide the design to be strong in modular and contemporary approach.
Modular Design: A design approach that subdivides a system into smaller parts called modules or skids that can be independently created and then used in different systems. The benefits are flexibility in design and reduction in costs. Examples of modular systems are modular buildings, solar panels, wind turbines and so on. Modular design combines the advantages of standardization with those of customization.
130
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Modularity means using the same module in multiple configurations enabling a large variety of designs without using many component types. This modularity brings several advantages such as reduced capital requirements and economies. Modularity is especially advantageous when the scale and scope of the project are relatively large. In such cases, it is a practical and economic option. Through modularity, you can achieve various designs, while achieving lowcost for development, as well as, cost saving in design and construction.
The new subcenter is envisaged to deliver expanded range of services that go beyond Maternal and child health care services to include care for non -communicable diseases and first level care for emergencies and trauma, including free essential drugs and diagnostic services.
Our moto is to create a quality experience in terms of service and infrastructure. The new building is proposed to have dedicated rooms for JPHN, JHI, ASHA WORKER, DOCTOR / DIETICIAN. This can very well protect the patient privacy and ensure the quality care is given to the patients.
The proposed Subcenter shall be equipped with high-speed internet and it is connected to the PHC. The dedicated room for E Health is planned which can be used for preventive screening for all the populations using innovative IOT devices. Electronic Health Records will enable the remote decision making based on clinical data collected. The Yoga Room is proposed for focusing on active preventive and promotive care with emphasis on wellness. This building also incorporates a two-bedroom accommodation for one staff. This with integrated services in the same layout for increasing the Quality for the User.
These services are made into MODULES and can be arranged in different orientation according to the site constraints. This helps in standardising the format for the Sub-Centre.
There are three modules in the ground floor and three in the first floor. These three modules can be arranged in different simulations to provide a better result while in different site conditions. This will help not to change the arrangement of the rooms in a particular module and will help to avail similar services in different simulations without changing the user
Resul Pookutty Foundation
131
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
experience. The Modular Design approach gives way to modular constructions and help in a sustainable development. These can be prefabricated and erected at site or pre-engineered and assembled at site. This will help reduce the use of natural resources. The construction process can be divided into phases for better efficiency of time and cost.
MODULE-1
This module consists of JPHN Room with Antenatal Clinic, Feeding Room and Public toiletFemale in the Ground Floor. Yoga Room, Conference Room and Staff toilet Male & Female in the First Floor


GROUND FLOOR
FIRST FLOOR
Resul Pookutty Foundation
132
Yeroor Grama Panchayath
MODULE 2
This module consists of Reception, Electrical Room, Janitors Store, Waiting Area for Antenatal Clinic, Asha worker Room, Caregiving Room with attached toilet in the Ground Floor. Dining Room, JHI Room, IT Room in the First Floor


GROUND FLOOR
FIRST FLOOR
Resul Pookutty Foundation
133
Detailed Project Report Sub Centre –
MODULE 3
This module consists of Pharmacy, Injection / Immunization room, E – Health room, Doctors / Dietician Room with attached toilet, disabled toilet, public toilet – Male in the Ground Floor. Staff quarters (2BHK) two-bedroom, hall, kitchen & toilet in the First Floor

GROUND FLOOR
Resul Pookutty Foundation
134
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
FIRST FLOOR MODULE ORIENTATION – 1



GROUND FLOOR
FIRST FLOOR
135
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
Sub Centre – Yeroor Grama Panchayath
MODULE ORIENTATION 2
GROUND FLOOR FIRST FLOOR
MODULE ORIENTATION 3
GROUND FLOOR FIRST FLOOR




Detailed Project Report
136
Resul Pookutty Foundation
MODULE ORIENTATION 4
GROUND FLOOR

FIRST FLOOR

Report
137
Detailed Project
Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
These modules can be arranged in different orientations according to the site conditions. It can be added into the PHC or can be built as a separate block. The design strategy gives a universal appeal and can be implemented in various topographies.
CONTEMPORARY ARCHITECTURE : CONTEMPORARY ARCHITECTURE is the architecture of the 21st century. The different styles and approaches have in common the use of very advanced technology and modern building materials, such as tube structures which allow construction of buildings that are taller, lighter and stronger than those in the 20th century, and the use of new techniques of computer-aided design, which allow buildings to be designed and modeled on computers in three dimensions, and constructed with more precision and speed.
Classicized ideas thrived on specific design elements. The have flourishes that are predictable and distinguishable while contemporary architecture is more flexible. Contemporary architects thrive on sophisticated and innovative ideas. They deviate from traditions and norms. To achieve this, they need contemporary materials to create these ideas. Contemporary architecture uses a vast range of building materials. These include concrete, glass, wood, and aluminum screens. These materials add contrast and homogeneity.
The Sense of Sustainability
The present is an era where global warming is a real issue. It is now essential to take specific measures to ensure nature is not compromised. For this reason, modern architects design buildings that are energy efficient. This is in part thanks to recycled materials for the construction process. This needs to include the use of solar panels for roofing purposes. Contemporary architecture relies on eco-friendly features. It embraces all types of innovations. These bring new meaning to modern building and construction. Moreover, it uses the latest technology and recyclable materials.
Area Calculation:
The areas are calculated using anthropometric and ergonomic data and the number of people using it. We have also incorporated the building furniture and equipment data while approaching the design.
Resul Pookutty Foundation
138
139
18 140 205 JPHNROOM GROUNDFLOOR (SQ.FT.) TOTALSQ.FT.) QUANTITY GROUNDFLOOR PHARMACY DOCTO'SDIETROOM
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
140
10 11 CARPETAREA 2315 130 FIRSTFLOOR 457 LIVINGDINING KITCHEN NO. QUANTITY AREA(SQ.FT.) TOTAL(SQ.FT.) FIRSTFLOOR ROOM 60 FIRSTFLOOR JHIROOM 60 TERRACEFLOORPLINTHAREA 375 CORRIDORSTAIR
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
SITE PLAN
141
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
The existing site plan is updated in the land survey. This is the proposed drawing. We have provided the Main Centre building near the entrance. The patients reaching to the site can avail the services of the Main Centre. This will disintegrate the population entering the site making it easy and viable for the patients. Since this building 5 meters above the Road level, it would be visible from any direction of the road
Resul Pookutty Foundation
GROUND FLOOR PLAN
142
INTERIOR GENERAL ARRANGEMENT PLANS
PERSPECTIVE VIEWS
FIRST FLOOR PLAN
FRONT ELEVATION (EAST)

Detailed Project Report
143
Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
NORTHEAST VIEW
Detailed Project Report

SOUTHEAST VIEW

144
Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
NORTHWEST TOP VIEW
SWOT ANALYSIS
STRENGTH
• Site is located adjacent to the state high way 56 Anchal-Kulathupuzha

• Walkable distance from the near bus stop
• Vehicle accessibility to the site is good
• Parking facility is available
• Connectivity to the Anchal CHC is good
WEAKNESS
• The altitude of the site 9 meter above the road level
• Access road inside the site is in poor condition
• The buildings are not barrier free
OPPORTUNITIES
• Site is near to the main state highway and easily accessible from all wards
• Due to the slopes the building allocation and orientation can be done according to the service provider
145
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
THREATS
• Since the site is near to the state highway and there is no provision of divider on the road accumulation of traffic problem during peak hours
5.2 Value Engineering
Concrete Structure
Concrete is the second most used material for construction after water in the world. Concrete structure can take compressive stresses very effectively but it cannot take tensile stresses. The reinforcement is given to concrete where the structure is under the tension load. Concrete is widely used in construction industry today because of its durability and compatibility. Concrete can be mould in any shape which make it a very useful.
RCC FRAMED STRUCTURE
Concrete structure can be made with many different ways. Some are given below:

Plain Cement Concrete
Plain cement concrete is a hardened mass obtained from a mixture of cement, sand, gravel, and water in definite proportion. The concrete structure made by using the plain cement concrete has good compressive strength but very little tensile strength, thus limiting its use in construction. Plain concrete is used where good compressive strength and weight are the main requirement and the tensile stresses are very low. For e.g.: In roads, concrete blocks for walls, etc.
146
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Reinforced cement concrete
Plain cement concrete has very low tensile strength. To improve the tensile strength of concrete some sort of reinforcement is needed which can take up the tensile stresses developed in the structure. The most common type of reinforcement is in the form of steel bars which are quite strong in tension. The reinforced concrete has innumerable uses in construction. For e.g.: in building, flyovers, water tanks, etc.
Prestress concrete
In ordinary reinforced cement concrete, compressive stresses are taken up by concrete and tensile stresses by steel alone. The concrete below the neutral axis is ignored since it is weak in tension. Although steel takes up the tensile stresses, the concrete in the tensile zone develops minute cracks. The load carrying capacity of such concrete sections can be increased if steel and concrete both are stressed before the application of external loads. This is the concept of prestress concrete. The prestressed concrete is used in the structures where tension develops or the structure is subjected to vibrations, impact and shock like girders, bridges, railway sleepers, electric poles, gravity dam, etc.
Advantages of concrete structure
• Ingredients used in concrete such as, cement, aggregates and water are readily available and cheap.
• Concrete assumes the shape of its mould and it can be poured and cast into any shape.
• Concrete when used along with reinforcement, is capable of taking bending and tension forces.
• The compressive strength of concrete is very high making it reliable to be used for
• Structures and components under compressive loads.
• The breakthrough in prestressed concrete applications enables reduced section sizes and reduction in self-weight.
• Due to massive nature, high unit weight and water tightness, concrete can be used for water retaining structures like Dams
Resul Pookutty Foundation
147
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Disadvantages of concrete structure
• Due to drying shrinkage and moisture expansion concrete may crack
• Therefore construction joints are provided to avoid these types of cracks
• Concrete is weak in tension.
• High Self weight of concrete is not always favourable for seismic prone structures.
• Sustained loads develop creep in structures.
• If salts are present in the concrete then it will result in the efflorescence in concrete structure
Steel structure
• The material steel, is an alloy of iron and carbon percentage (small percentage) and other elements e.g., silicon, phosphorous and sulphur in varying percentage. Depending upon the chemical’s composition, the different types of steel are classified as mild steel, medium carbon steel, high carbon steel, low alloy steel and high alloy steel. The mild steel, medium carbon steel and low alloy steel are generally used for steel structures.
Steel Truss Structures

The steel which is used for the manufacture of rolled steel structural, fastenings and other elements for use in structural steel works is called structural steel. Structural steel to be used for building purposes, has been standardized by Indian Standard Institution (I.S.I) I and specification of various qualities are contained in the following standards (as per I.S 800-1984)
IS: 226-1975 Structural steel (standard quality)
IS: 1977-1975 Structural steel (ordinary quality)
148
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
IS: 2062-1984 Weldable structural steel (Fusion welding)
IS: 961-1975 Structural steel (High tensile)
IS: 960-1977 weldable structural steel (medium and high strength quality)
Standard quality steel (mild steel)steel is the most commonly used steel for general construction purposes of buildings, railway bridges, transmission line towers, industrial structures etc.
Advantage of steel structure
Lightness: The steel structures are very light in comparison to other structures such as concrete structures
High strength and stiffness per weight: The steel is very stiff and they possess a high strength to weight ratio.
Ease of fabrication and mass production: It is easy to fabricate a steel structure so it is generally used for mass construction.
The steel members can be easily replaced, assembled and disassembled.
Fast and easy erection and installation: The steel structures can be erected very easily and faster than many other structures.
The steel structures can be used soon after their erection
No sudden failure: Steel being a ductile material does not have sudden failure, rather it gives clear indication by deflection before failure.
Formwork unneeded: Unlike concrete structures, the steel structure does not need any kind of formwork
Termite proof and rot proof: Unlike timber the steel doesn’t get corroded by the action of termite and it is pretty much resistance to rusting, If good quality steel is used.
Economy in transportation and handling: Because of being lightweight the steel structures are easy to transport and handling.
Resul Pookutty Foundation
149
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Disadvantages of steel structure
Susceptibility to corrosion: The steel members are prone to corrosion; therefore, they require some frequent treatment like painting and other methods for their protection.
High initial cost: The initial cost of steel structure is high.
Skilled labour: The steel structure requires skilled labour for their construction.
Point of difference
Concrete structure
Steel structure
Durability
Earthquake resistance
The concrete structure is more durable
The durability of steel structure is adversely affected by weather condition and rusting
The concrete structure is brittle so they are less earthquake resistance.
Steel Structure can withstand earthquake more effectively than concrete structure
Load carrying capacity
In the comparison to the steel the load carrying capacity of the concrete is low.
The load carrying capacity of steel structure is good
Scrap value
The scrap value of concrete is nil
The scrap value of steel is good
Self-weight
The self-weight of concrete is more
The steel is 60% lighter than the concrete
150
Resul Pookutty Foundation
Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
The foundation for the concrete structure should be strong because of the larger weight of concrete
The steel structure can be made with less expensive foundation
Construction time
The concrete structure generally needed 28 days before they are ready to use
The steel structure is fast in their erection and can be used soon after their erection
Labour
It requires less skilled labour
It requires more skilled labour Cost
The cost of construction is less
The cost of construction is more
Joining
The joints such as construction joint, expansion joint, contraction joint, etc are needed in concrete structure
The steel component is joined by using rivets, welding, nuts & bolts, etc. in steel structure
Steel buildings gives the leverage of time and cost other than the RCC buildings. Since we are using modular design and the project category comes under healthcare it would be easy for construction without disturbing the surroundings. It is more effective when different orientation happens across the site this keeps the budget stable as the module sizes are same.
5.3 Engineering Design
ENGINEERING DESIGN:
MODULAR CONSTRUCTION
There are many different ways to define the modular construction but one basic definition of modular construction can be given as follows: “Modular Construction is a preengineered process of making any structures or elements in a factory that is off-site and
151
Resul Pookutty Foundation
Sub Centre
Detailed Project Report
– Yeroor Grama
Panchayath
are delivered to the sites and assembled as large volumetric components or as substantial elements of any structures.”
It can also be defined as “A modular building is a pre-engineered structure that is flexible enough to satisfy virtually any requirement tougher than standard drywall construction, expandable, can be relocated and completely re-usable.”
With increasing industrialization to the building industry, steadily larger parts of buildings are made up of prefabricated components, delivered to the building site from the factories.
• Modular design, or "modularity in design", is a design approach that subdivides a system into smaller parts called modules or skids that can be independently created and then used in different systems.
WHY CHOOSE MODULAR CONSTRUCTION?
One of the major reason to adopt modular construction is that not only can one save up to 35% on the initial construction costs like labor and materials, but there are other benefits as well. Another major reason is about the quality as one can attain a suitable quality in the elements of any structures that are to be pre-fabricated or pre-cast in the construction factory. Modular construction takes most of the construction phase away from the building site. Quicker and efficient factory processes are replacing the slow, less productive site activities.
Sustainability in modular construction can be achieved through the factory production of the modular units for a modular construction project to complete with a good result, proper planning, coordination and communication must exist between various relevant parties involved from the early stage of the project.
The construction process can be divided into phases for better efficiency of time and cost.
PHASE 0
General material assembly
PHASE 1
Floor framing & decking
Int. /Ext. wall framing
‘Box’ mounted to chassis
Resul Pookutty Foundation
152
PHASE 2
Roof framing/mounting
Ceiling attached to ‘box’
Interior partition installation rough plumbing
PHASE 3
Sheetrock (walls)
Rough electrical (walls)
PHASE 4
Sheetrock (ceiling)
Batt/spray foam insulation
Rough electrical
PHASE 5
Exterior plywood sheathing
Rough opening cleanup
General interior cleanup
PHASE 6
Exterior plastic sheathing
Interior finish work (paint, trim)
PHASE 7
Finish plumbing
Finish electrical
Install flooring
PHASE 8
Install windows
Install siding
Weatherproof
Resul Pookutty Foundation
Detailed Project Report
153
Sub Centre – Yeroor Grama Panchayath
DRAWINGS FOR THE ENGINEERING MODEL STUDY
Yeroor Grama Panchayath
GROUND FLOOR PLAN
154
Detailed Project Report Sub Centre –
Resul Pookutty Foundation
FIRST FLOOR PLAN
EAST ELEVATION (FRONT)
155
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
NORTH ELEVATION (RIGHT)
SOUTH ELEVATION (LEFT)

WEST ELEVATION (REAR)
SECTION THROUGH THE STAIRS
156
Detailed Project Report Sub Centre –
Yeroor Grama Panchayath
Resul Pookutty Foundation
5.4 Power Supply & Distribution
Existing Power supply to existing subcentres are from the KSEB overhead lines. Connected load to all the existing subcentres are 3kW and is supplied with a single phase connection. Existing subcentres are all type a sub centres with minimum facilities and equipment’s. Hence the connected load remains within 3kW range.
Proposed sub centre in Yeroor Main Centre is 6000 sq.ft. Two storied building with more facilities is been incorporated compared to the existing subcentre. Facilities include, Airconditioned rooms, Internet, Public address system, security surveillance cameras etc. In addition more Medical equipment’s are added to cater the facility. Providing power to all of these medical equipment’s, lights and facilities the required connected load from KSEB is 30kW. Following table shows the power distribution and load details.
INVERTER/ UPS SYSTEM
Since power outages in the region are frequent due to various reasons like monsoon rains etc, it is essential to provide power backups. A 5 kVA UPS with battery backup is provided to serve this purpose. This UPS/Inverter facility will provide un-interrupted power to the facilities lights, fans and essential power supplies.
157
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
2
3
`4 Air-conditioners
5
Sl No. Description Consumption (kW) 1 Facility utilities like Lights fans and pumps 5.0
Computer and IT Services 3.0
Allowance for Apartment 3.0
15
Medical Equipment’s 4.0
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Specifications for some of the major components in Electrical part are listed below.
Main Switch Boards
All medium voltage switchboards shall be suitable for operation at three phase/three phase 4 wire, 415 volt, 50 Hz, neutral grounded system with a symmetrical short circuit level as BOQ. The switchboard, switchgear, control gear, busbar assemblies & associated equipment shall be certified for the category of duty specified. The main circuits shall have an insulation level of 1000V.
The Switch Boards shall comply with the latest edition with up to date amendments of relevant Indian Standards and Indian Electricity Rules and Regulations & IEC.
The switchboard shall have a rated withstand current of 65kA for 1 sec.
Wiring
All wiring for relays and meters and other associated equipment’s shall be with FRLS, 1050 class PVC insulated, stranded copper conductor wires. The wiring shall be colour coded and labelled with approved ferrules for identification. PVC ferrules yellow in colour, locked to avoid movement & with black engraved letters shall be provided at each end of all wires marked to correspond with equipment/circuit designation & termination numbers as specified / approved or as required.
A separate bunching & separate route shall be followed for AC& DC wiring. The minimum size of copper conductor control wires for switch-boards shall be 2.5 mm2.
Wiring shall be terminated through cage clamps or using crimping lugs where former not feasible, without joints or Tee on their run. Wiring shall be run on sides of panels, neatly bunched, secured without affecting equipment mounting.
Light Fittings
Fittings shall be designed for continuous trouble free operation under atmospheric conditions, reduction in lamp life or without deterioration of materials and internal wiring. Outdoor fittings shall be weather - proof and rain proof. All fitting shall be selected LED with Minimum power consumption as per government regulations.
Resul Pookutty Foundation
158
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Fittings shall be so designed as to facilitate easy maintenance including cleaning, replacement of lamps/starters etc. All fittings shall be supplied complete with lamps.
UPS System
UPS system shall be of 5kVA three phase UPS system, indoor (IP20) with surge protection system with 60 min backup battery, (SMF battery of reputed make), input pf>0.99, input current consumption, built in isolation transformers, with necessary battery circuit breaker., double conversion technology with input 415V, 50Hz three phase, output 415V, 50Hz three phase, SNMP card for network monitoring .It shall be 100% generator compatible, with efficiency > 94% and output power factor > 0.9 and including all accessories etc. as required. The system shall comply to IEC /EN 62040-1 and relevant IS standard. The acoustic noise of the system should be less than 58dB.The system shall comply with IEC /EN 62040-1, EN/IEC 62040-2, EN/IEC 62040-3 and relevant IS standard. The system shall be true online doubleconversion DSP based UPS system connected in parallel redundant load sharing configuration with each UPS unit having inbuilt parallel kit and also each UPS shall be with automatic & manual bypass switch capable of working in standalone configuration also. The system shall have IGBT rectifier and inverter. Rate shall inclusive of UPS DB Panel, UPS inverter, Batteries and connections
The work is required to be carried out in conformity with the Drawings and BOQ with specifications, which are for the purpose of guidance of the Contractor. The work should conform to established good Engineering practices, standards, codes and specifications.
ESTIMATE OF POWER SUPPLY AND DISTRIBUTION - Rs 14,03,182.
Resul Pookutty Foundation
159
GROUND FLOOR ELECTRICAL LAYOUT
FIRST FLOOR ELECTRICAL LAYOUT
160
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
ROOM DIET/DOCTOR
SINGLE LINE DIAGRAM
5.5 HVAC
Rooms for JPHN, JHI, IT, Care giving, Conference, Yoga Room, E Health room, Pharmacy and Doctor are provided with air-conditioning using split units. Toilets are ventilated using wall mounted or axial ducted exhaust fans. Outdoor units are conveniently located behind the building or at the top of the building, without harming the aesthetic appearance of the building.
DX Units
Wall mounted inverter split units of 1 and 1.5 TR capacities suitable to operate from 230+10%volt, 50Hz, single phase AC power supply is provided in the design. The outdoor unit are with air-cooled condenser with copper coil, fan, and fins with corrosion proof coating and with rotary compressor. Outdoor units shall be located at M.S. frame duly painted. The split unit shall be provided with green refrigerant gas like R32 or better and the unit shall be of minimum 3 star rating.
Report
161
Detailed Project
Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
FANS
Sub Centre is provided with 1200mm sweep ceiling fans in all the rooms for air movement. Toilet ventilation is provide using axial fans of wall mounted type and ducted ceiling suspended type. Electrical room and Janitor rooms are provided with industrial type wall mounted exhaust fans.
DUCTING
Rectangular ducts are used for ventilation along with axial ducted fans. Ducts shall be fabricated as per IS standards and is made of galvanised steel of Class 111 parameters which are confirming to IS 655-1963. Thickness of the duct shall not be less than 0.63mm. All ducts shall be supported from the ceiling with necessary GI rods an angles. Ducts in the roof would be provided with gooseneck and shall be provided with ss mesh to prevent any ingress of small insects.
ESTIMATE FOR HVAC SYSTEM - Rs 4, 39,800
162
Resul Pookutty Foundation
GROUND FLOOR HVAC SYSTEM
163
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
150X150 EXHAUSTDUCT EXF-4 SAC-GF-4 EXF-1 REFRIGERANTPIPESTO ROOF
FIRST FLOOR HVAC SYSTEM
TERRACE HVAC SYSTEM
5.6 Fire Fighting
As a minimum requirement for fire-fighting, the facility shall be provided with fire extinguishers. All the floors are provided with minimum one fire extinguisher at the nearest accessible location. Fire extinguisher provided is ABC dry powder of 6 Kg and shall be installed as indicated in the firefighting drawing.
ESTIMATE FOR FIRE FIGHTING SYSTEM - Rs 16,000
Resul Pookutty Foundation
Report
164
Detailed Project
Sub Centre – Yeroor Grama Panchayath
Yeroor Grama Panchayath
GROUND FLOOR FIRE FIGHTING SYSTEM
FIRST FLOOR FIRE FIGHTING SYSTEM
165
Detailed Project Report Sub Centre –
Resul Pookutty Foundation
5.7 Plumbing & Storm Water Management
The water supply, sanitary, drainage and storm water system is designed to provide enough water at the staff toilets, provide a healthy comfort stations and to conserve water utilising the storm water stored in the harvesting tank.
The water supply in the facility is provided from local well water. The water from the well would be pumped into the tank, from there it will be distributed using pipework to different locations.
Drainage system provided would be gravity type, which consists of a two pipe system. All the drainage lines would be finally connected to septic tank. The overflow water is allowed to soakaway in the soakaway pit. Disposal of sewerage is carried by authorised third party sewerage disposing tanker shall be called for collection and disposal. Storm water from the building would be collected in the rain water harvesting tanks as discussed in the earlier section of rain water harvesting.
Following are some of the main components of the system.
Water Supply Pipes.
All pipes for water supply within the building and tapings outside the building below ground or in wall chase, in shafts and terraces shall be CPVC pipes. The pipes with 50mm dia OD. Shall be SDR-11 Rating as per ASTM D-2846.
Drainage and Storm water pipes
All drainage pipes shall be conforming to uPVC IS 13592 Class B & 6kg/sqcm pipes for pipes below 75mm dia. All rain water and vent pipe shall be conforming to uPVC IS 13592 Class an including necessary fittings and accessories.
Sanitary Ware
Sanitary wares include European WC, Wash basins and Sinks. European WCs are floor mounted single piece white vitreous china water closet with seat and lid, 6 litre twin flush cistern & provided with S Trap. Wash basins are counter type wash basin, with 15 mm dia brass quarter turn CP basin pillar tap, 32 mm dia. brass CP waste coupling, 32 mm dia brass CP bottle trap with extension pipe. Sinks are Stainless steel wall mounted type wash basin, with 15 mm dia brass CP basin pillar tap, 32 mm dia. brass CP waste coupling, 32 mm dia brass CP bottle trap with extension pipe, stainless steel screws, 1no.15mm brass CP angle valve with 450 mm long metallic flexible tube, brass CP wall flanges.
Resul Pookutty Foundation
166
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Water Tank
A PVC water tank of 2000L capacity is provided at the upper roof of the building. This will ensure enough storage of water and availability of pressure at the user end.
ESTIMATE FOR PLUMBING & DRAINAGE SYSTEM - Rs 17,07,481. GROUNDFLOOR DRAINAGE SYSTEM
167
Resul Pookutty Foundation
FIRST FLOOR DRAINAGE SYSTEM
168
Detailed Project Report Sub Centre –
Yeroor Grama Panchayath
Resul Pookutty Foundation
FIRST FLOOR DRAINAGE SYSTEM
169
Detailed Project Report Sub Centre –
Yeroor Grama Panchayath
Resul Pookutty Foundation
110ØRWP OUTLETTYP.
SITE PLAN FOR DRAINAGE SYSTEM
170
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
LVL-2300 -800 LVL-4600 LVL LVL PEDESTRIAN BUILDING
GROUND FLOOR WATER SERVICE SYSTEM
171
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
32ØPipe 20Øtyp.
FIRST FLOOR WATER SERVICE SYSTEM
172
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
25ØPipeT/B 32ØPipe 32ØPipe
TERRACE WATER SERVICE SYSTEM
5.8 Rain Water Harvesting
As per KPBR requirement rainwater storage is considered in this building. An underground RCC storage tank is provided to store rainwater. Rainwater from the roof is collected via roof rainwater outlets/gutters and taken through down pipes to the storage tank. It is proposed to have a 15000 litre storage tank for the Yeroor sub-centre facility. An over flow pipe from the tank will be discharged to the nearby recharging pit.
5.9 Landscaping
Landscaping refers to any activity that modifies the visible features of an area of land, including: Living elements, such as flora or fauna; or what is commonly called gardening, the art and craft of growing plants with a goal of creating a beauty within the landscape.
• Planting beds (such as flower borders)
• Lawns.
• Shrubs.
• Flowering trees.
• Driveways.
• Walkways.
• Fences.
Project Report
Panchayath 173
Detailed
Sub Centre – Yeroor Grama
Resul Pookutty Foundation
40Ø 25ØPipe 25ØPipeT/B 25ØPipeT/B 50Ø
5.10 Internet Facility

The subcentre would be provided with highspeed internet. We have provided a service with100 Mbps uploading and downloading speed. Since the subcentre shall be properly networked with the PHCs and CHCs within the region we have considered in selecting a premium network package providing high speed internet services in the region.
BSNL connection would be provided internet and landline. Following service providers would be kept as an option and the selection of the same shall depend on the availability of their services within the region.
Panchayath 174 Resul
Detailed Project Report Sub Centre – Yeroor Grama
Pookutty Foundation
1. Jio
2. ACT
3. Airtel
5.11 Security System
Building would be under CCTV surveillance monitoring all the key points in the building and the plot. There would be CCTV cameras in the main entrance and exit areas, all views covering the building, main receptions and corridors. The system would consist of 5 internal cameras and 4 external cameras. Suitable recorders shall be provided as per the specifications given in BOQ. All visions would be recorded 24x7 and shall be stored in for a period of 30 days.
5.12 Audio Visual System
A power audio visual system will be provided within the facility with a combination of LED TV and speakers. A 32inch Smart LED TV would be placed at the doctor’s room and a 75 inch Smart LED TV in conference room. Doctor’s room TV shall use for remote doctor interface and video conferencing, while conference room TV would be used for presentations and video conferencing.
Public address system is provided in the building. Speakers would be placed all over the building at the receptions, corridors etc so that all the inmates are clearly audible to the sound from the speakers. The system would be used for providing background music and announcements. Also they would serve to provide any emergency messages and alarms to the occupants incise of scenarios like fire.
5.13 Cabling and Switching
Networking in the building is provided using for services like Internet, CCTV, TV and Audio systems. The entire networking cables along the building would be run through cable trays. All the telecommunication service would have their dedicated Rack and switching devices, preferable in the IT room or concealed in the ceiling. Following are the details of cable used in various low voltage systems
1. CCTV system uses CAT6A cables are for networking
2. Internet /LAN connections are provided using Cat 6A cables
3. Video connections for Smart TV is provided using Coaxial cables.
Resul Pookutty Foundation
175
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
4. Public Address system and speaker used bi-pair audio cables
5. Telecommunication cables are patch cables of 0.4mm diameter.
5.14 Office Automation
As part of office automation devices like printers, computers, copiers, scanners and telephones to staff rooms to enable communication, and improve office functionality. Printers and scanners would be provided at the doctor’s room and reception area. Telephone and Computers with Internet facility is provided at JHI, IT, E-health, Reception, JPHN and Doctor’s room.
5.15 EPABX System
Rooms for JPHN, JHI, Doctor, IT, Reception & E-Health room are connected together with Intercom telephone system. This is facilitated using an EPABX system which would automatically divert calls to the specified departments and can also manual operate by an attendant at the reception counter. Land line facility from BSNL would be provided to the subcentre. Facility would be provided with a 16 Line EPABX system. It adds the intercom facility within the organisation and can switch the external calls to the right extension. Initially the system would provide extension phones to 6 rooms as per the drawing, later extension can be added as per the requirement.
5.16 Nurse/Doctor Calling System
Nurse calling system enables a first level of attendance to the patients in case of emergency. Patients can use the nurse calling buttons placed near to the beds and crucial points, incise of emergency. This will create an alarm at the nurse station and the nurse can identify the room/bed number from which the alarm is coming and can respond to the case immediately. Once the patient is attended, alarm can be turned off by pressing the reset button provided at the bed unit. The design would provide nurse call system to 2 beds at the Care Giving Room. The doctor calling system is more or less similar to a queuing system, which helps to determine the order of patients as per the case of appointments. Doctors can call the patients as per the numbers provided during the appointment. This can reduce the prolonged waiting hours of some patients who are behind in numbers and can avoid the mis-concept of being handled inappropriately. Organising the OPD patients list in this manner helps to achieve a
176
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
systematic and genuine way in approaching the patients. The components of the system shall include the Token Issuer, Software for handling the queue for various services, Display of list on a LED TV currently serving for various services along with announcements.
Total ESTIMATE for Low voltage System - Rs 12,87,340
Resul Pookutty Foundation
GROUND FLOOR LOW VOLTAGE SYSTEM
177
FIRST FLOOR LOW VOLTAGE SYSTEM
5.17 Waste Management Facilities
Small-scale incinerators are a useful technology to combust household waste, medical waste, slaughter waste, etc. instead of discharging it in a landfill. Furthermore, heat and energy may be recovered and it helps to avoid open burning of municipal waste which creates much more harmful emissions and endanger human health and environment. Costs for these incinerators range from very high to low, but it is often possible to construct the incinerators by instructed community members and with local materials such as bricks and steel. The waste should be separated previously in order to retain organics or recyclable material before incineration. The ashes can contain toxic substances and heavy metals and should therefore, if possible, be disposed of safely Advantages
• No landfills required
• Substantial reduction of weight and volume of solid waste
• Breaks down chemical toxics and destroys pathogens (e.g. medical waste)
• There are many different products in all price ranges
Report
Panchayath 178
Detailed Project
Sub Centre – Yeroor Grama
Resul Pookutty Foundation
NETWORKRACK, SERVERRACK
Detailed Project Report
 Sub Centre – Yeroor Grama Panchayath
Sub Centre – Yeroor Grama Panchayath
Open dumps and poorly designed and managed landfills lead to (ground-) water pollution (landfill leachate) and contamination of sources. Small-scale incinerators can reduce the volume of non-recyclable wastes (e.g. household waste, medical waste, slaughter waste). Moreover, heat and energy may be recovered and it helps to avoid open burning of municipal waste, which creates much more harmful emissions and endangers human health and environment. Urban air pollution due to open incineration of municipal waste or incineration in systems without or with only poorly designed flue gas cleaning systems results in a serious health risk. Another big problem is uncontrolled landfill fires and open burning on the streets. Uncontrolled burning of waste is largely obsolete in developed countries, but continues to be practised in developing regions, causing the release of CO2 and other greenhouse gases. Some landfills in developing countries, such as the Smokey Mountain site in Manila, smoulder continuously another big problem is the “recycling” of e-waste in developing countries. This waste contains toxic chemicals such as lead or mercury. It is often burned to remove plastic and reclaim the valuable metals. .
179
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
The medical waste incinerator, which could be built in almost every developing country, is a simple two-chamber natural-draught incinerator designed to be operated at temperatures of 800°C and higher. The performance of the incinerator varies depending on the moisture content of the medical waste but a throughput of up to 15 kg/hour can be achieved. The incinerator has been designed so that it can be built on site, using standard building bricks or blocks and lined with refractory bricks. All the steel components, such as the loading door, the ash removal door and air inlet apertures can be made using basic workshop equipment. The two-chamber design helps to ensure that the combustion time is sufficient to destroy the products of combustion and minimise any harmful emissions.
D-20 Model (D-Type) = Rs. 2, 50,000/- (Electric Operated)
5.18 Statutory Clearances and Approvals
Land Title: Land titles are a way to ascertain an individual's ownership over a land parcel. Clear land titles are important to develop new infrastructure. Clear title ensures that the property is clear, marketable and it traces any charges or encumbrances created on the property and its present status.
Land Approval: Panchayats have the power to approve layouts and residential properties within the boundary of their village. The rural development and panchayats have been granted permission by the government to approve layouts/residential properties that are within one acre of land within the village boundaries.
Zonal Clearance: A Zoning Clearance is the procedure used by the local body or district body to verify that a proposed land use or structure is allowed in the applicable zoning district, and that the project complies with the development standards of this Zoning Code that apply to the use, consistent with the General Plan. After the land title & clearance, builder is required to take zoning approval from the local body / authority.
• The revenue department provides the ownership certificate for building permit under the provisions of Local Body Acts.
Resul Pookutty Foundation
180
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
• The state town planning checks regarding city development with the planning board and forwards the proposals to the various other concerned authorities in the city as required for issue of case specific approvals/ NOC before granting zoning approval.
Building Approval:
An approval from authority for sanction of building plans/ building permit under the provisions of Building Byelaws, Master plan and Local Body Acts. The Building approval comprises of the building plan and the layout approval for the construction of the building.
1) Building Plan:
• A builder should submit building plan before starting the construction activities. Building plans are a graphical representation of what a building will look like after construction.
• Building plan ensures that building complies with building laws.
• Once the building plan is approved, the builder should commence construction work within two years and there should be no deviation from the sanctioned plan.
2) Layout approval:
The builder has to get approval of layout plan from concerned authorities before starting construction of residential or commercial building.
• Approved Layout Plan is as per approved FAR (Floor Area Ratio) or FSI (Floor Space Index).
181
Resul Pookutty Foundation
6.
Quantity & Cost Estimates
6.1 BOQ & Cost Estimates – Buildings and Civil Works
ANNEXURE I
Civil - BOQ
Sl. No. Description
DEMOLITION
Demolishing brick work manually/ by mechanical means including stacking of serviceable material and disposal of unserviceable material within 50 metres lead as per direction of Engineer-in-charge.
In cement motar
Qty Unit Unit Rate Amount
1 Cost of 1.00 cum 51 cum 843 42556
Removing mortar from bricks and cleaning bricks including stacking within alead of 50 m (stacks of cleaned bricks shall be measured):
From brick work in cement mortar
2 Cost of 1000 Nos 25 Nos 2799 70665
Demolishing stone rubble masonry manually/ by mechanical means including stacking of serviceable material and disposal of unserviceable material within 50 metres lead as per direction of Engineer-in-charge : In cement motar
3 Cost of 1.00 cum 34 cum 1006 33892
Dismantling doors, windows and clerestory windows (steel or wood) shutter including chowkhats, architrave, holdfasts etc. complete and stacking within 50 metres lead : Of area 3 sq. metres and below
4 Cost of each 22 each 158 3473
Taking out doors, windows and clerestory window shutters (steel or wood) including stacking within 50 metres lead : Of area 3 sq. metres and below
5 Cost of each 22 each 61 1348
Dismantling wood work in frames, trusses, purlins and rafters up to 10 metres span and 5 metres height including stacking the material within 50 metres lead : Of sectional area 40 square centimetres and above
6 Cost of 1.00 cum 50 cum 1922 96123
Report
182
Detailed Project
Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
EARTH WORK
7 Surface dressing of the ground including removing vegetation and inequalities not exceeding 15 cm deep and disposal of rubbish, lead up to 50 m and lift up to 1.5 m.
8
1184 sqm 24 28830 Felling trees of the girth (measured at a height of 1 m above ground level), including cutting of trunks and branches, removing the roots and stacking of serviceable material and disposal of unserviceable material.
2.28.1 All kinds of soil
2.33.1 Beyond 30 cm girth upto and including 60 cm girth 5 each 381 1903
9 2.33.2 Beyond 60 cm girth upto and including 120 cm girth 3 each 1694 5083
Earth work in excavation by mechanical means (Hydraulic excavator)/manual means over areas (exceeding 30 cm in depth, 1.5 m in width as well as 10 sqm on plan) including getting out and disposal of excavated earth lead upto 50 m and lift upto 1.5 m, as directed by Engineerincharge.
10 Ordinary rock 280 cum 352 98598 Excavation work by mechanical means (Hydraulic excavator)/ manual means in foundation trenches or drains (not exceeding 1.5m in width or 10 sqm on plan), including dressing of sides and ramming of bottoms, lift upto 1.5 m, including getting out the excavated soil and disposal of surplus excavated soils as directed, within a lead of 50 m.
11 Ordinary rock 217 cum 448 97441 REINFORCED CEMENT CONCRETE CAST IN SITU FOUNDATION
FOOTING
CONCRETE WORK (foundation)
12 1:5:10 (1 cement : 5 coarse sand (zone-III): 10 graded stoneaggregate 40 mm nominal size) 15 cum 5520 81972
REINFORCED CEMENT CONCRETE FOUNDATION
FOOOTING
CAST IN SITU
Providing and laying in position specified grade of reinforced cement concrete, excluding the
183
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
13
cost of centering, shuttering, finishing and reinforcement - All work up to plinth level :
1:1.5:3 (1 cement : 1.5 coarse sand (zone-III): 3 graded stone aggregate 20 mm nominal size) 7 cum 7718 55031
FORM WORK
Centering and shuttering including strutting, propping etc. and removal of form for :
14
Foundations, footings, bases of columns, etc. for mass concrete 40 sqm 285 11269
COLUMN
Providing and laying in position specified grade of reinforced cement concrete, excluding the cost of centering, shuttering, finishing and reinforcement - All work up to plinth level :
15 1:1.5:3 (1 cement : 1.5 coarse sand (zone-III): 3 graded stone aggregate 20 mm nominal size) 2 cum 7718 15483
FORM WORK
Centering and shuttering including strutting, propping etc. and removal of form for :
16
Foundations, footings, bases of columns, etc. for mass concrete 30 sqm 285 8423
PLINTH BLEM CAST IN SITU
Providing and laying in position specified grade of reinforced cement concrete, excluding the cost of centering, shuttering, finishing and reinforcement - All work up to plinth level :
17
1:1.5:3 (1 cement : 1.5 coarse sand (zone-III): 3 graded stone aggregate 20 mm nominal size) 15 cum 7718 118861
FORM WORK
Centering and shuttering including strutting, propping etc. and removal of form for :
18
Foundations, footings, bases of columns, etc. for mass concrete 151 sqm 285 42937
STEEL WORK FOOTING
Steel reinforcement for R.C.C. work including straightening, cutting, bending, placing in position and binding all complete upto plinth level.
19
Thermo-Mechanically Treated bars of grade Fe500D or more. 452 kg 84 37715
COLUMN
Steel reinforcement for R.C.C. work including straightening, cutting, bending, placing in
184
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
position and binding all complete upto plinth level.
20
Thermo-Mechanically Treated bars of grade Fe500D or more. 322 kg 84 26911
PLINTH BEAM
Steel reinforcement for R.C.C. work including straightening, cutting, bending, placing in position and binding all complete upto plinth level.
21
22
Thermo-Mechanically Treated bars of grade Fe500D or more.
STRUCTURE ISMB 200
Structural steel work riveted, bolted or welded in built up sections, trusses and framed work, including cutting, hoisting, fixing in position and applying a priming coat of approved steel primer all complete.
WALL PANELLING
Providing and fixing Pre-laminated flat pressed 3 layer (medium density) particle board or graded wood particle board IS : 3087 marked, with one side decorative and other side balancing lamination Grade I, Type II exterior grade IS : 12823 marked, in shelves with screws and fittings wherever required, edges to be painted with polyurethane primer (fittings to be paid separately).
1406 kg 84 117376
11297 kg 102 1149470
23 25 mm thick 235 sqm 1548 363886
24 Supplying and installation of moisture resistant/fire resistant 6 mm thick Heavy duty fiber cement board (High pressure steam cured) conforming to IS 14862:2000 of category III type B as per standard sizes fixed with self-drilling / taping screws. Screws shall be of counter sunk rib head of 1.60mm to 4 mm thick of 8 to 10 gauge of length varying from 25 to 45 mm.
1757 sqm 869 1527097
Resul Pookutty Foundation
185
Sub Centre – Yeroor Grama Panchayath
25 Designing, providing, installing and fixing factory finished custom designed cold form Light Gauge
Steel Framed super structure comprising of steel wall panel, trusses, purlins etc manufactured out of minimum 0.75 mm thick steel sheet as per design requirements. The steel sheet shall be galvanized (AZ-150 gms Aluminium Zinc Alloy coated steel having minimum yield strength 300- 550 Mpa) conforming to AISI specifications and IBC 2009 for cold formed steel framing and construction and also as per IS: 875-1987, ISO 800-1984 and IS: 801- 1975. The wind load shall be as per provisions of IS 875 (part -III). LGSFS frame shall be designed as per IS: 801 using commercially available software such as Frame CAD Pro-11.7/ STAAD PRO-V8i/ArchitekV2.5.16/ Revit architecture-2011 or equivalent. Proper usage of Connection Accessories like Heavy Duty Tension Ties, Light Duty Hold-ons, Twist Straps (to connect truss with wall frames), Strong Tie, Tie Rod, H-Brackets, Boxing Sections, L-Shaped Angles for better structural stability. The framing section shall be cold form C-type having minimum web depth 89 mm x 39mm flange x 11mm lip in required length as per structural design requirement duly punched with dimple/slot at required locations as per approved drawings. The slots will be along centre line of webs and shall be spaced minimum 250mm away from both ends of the member. The frame can be supplied in panelized or knock down condition in specific dimensions and fastened with screws extending through the steel beyond by minimum of three exposed threads. All self drilling tapping screws for joining the members shall have a Type II coating in accordance with ASTM B633(13) or equivalent corrosion protection of gauge 10 & 12, TPI 16 & 8 oflength 20mm. The frames shall be fixed to RCC slab or Tie beam over Neoprene rubber using self expanding carbon steel anchor bolt of dia as per approved drawings. design subject to minimum 12mm diameter and 121mm length conforming to AISI 304 and 316 at 500mm c/c with minimum embedment of 100mm in RCC (RCC to be paid separately) and located not more than 300mm from corners or termination
186
Detailed Project Report
Resul Pookutty Foundation
kg 174 3307900
19000
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
of bottom tracks complete in all respects. The item also includes the submission of stability reports duly examined and issued by any NIT/IIT. The rate includes the concept design, detailed design, fabrication of sections, transportation, installation and all required fixing arrangement at site as described above.
GLAZING
25 Providing, assembling and supplying vision glass panels (IGUs) comprising of hermetically-sealed 6-12- 6 mm insulated glass (double glazed) vision panel units of size and shape as required and specified, comprising of an outer heat strengthened float glass 6mm thick, of approved colour and shade with reflective soft coating on surface # 2 of approved colour and shade, an inner Heat strengthned clear float glass 6mm thick, spacer tube 12mm wide, dessicants, including primary seal and secondary seal (structural silicone sealant) etc. all complete for the required performances, as per the Architectural drawings, as per the approved shop drawings, as specified and as directed by the Engineer-in Charge. The IGUs shall be assembled in the factory/ workshop of the glass processor. (Payment for fixing of IGU Panels in the curtain glazing is included in cost of item No.26.2) For payment, only the actual area of glass on face # 1 of the glass panels (excluding the areas of the grooves and weather silicone sealant) provided and fixed in position, shall be
3730 sqm. 150 559500
187
Resul Pookutty Foundation
Sub Centre – Yeroor Grama Panchayath
measured in sqm.(i) Coloured tinted float glass 6mm thick substrate with reflective soft coating on face # 2, + 12mm Airgap + 6mm Heat Strengthened clear Glass of approved make having properties as visible Light transmittance (VLT) of 25 to 35 %, Light reflection internal 10 to 15%, light reflection external 10 to 20 %, shading coefficient (0.25- 0.28) and U value of 3.0 to 3.3 W/m2 degree K etc. The properties of performance glass shall be decided by technical sanctioning authority as per the site requirement.
DECK ROOFING
Steel work in built up tubular (round, square or rectangular hollow tubes etc.) trusses etc., including cutting, hoisting, fixing in position and applying a priming coat of approved steel primer, including welding and bolted with special shaped washers etc. complete.
26 Hot finished seamless type tubes 898 kg 158 141356 Providing corrugated G.S. sheet roofing including vertical / curved surface fixed with polymer coated J or L hooks, bolts and nuts 8 mm diameter with bitumen and G.I. limpet washers or with G.I. limpet washers filled with white lead, including a coat of approved steel primer and two coats of approved paint on overlapping of sheets complete (up to any pitch in horizontal/ vertical or curved surfaces), excluding the cost of purlins, rafters and trusses and including cutting to size and shape wherever required.
27 1.00 mm thick with zinc coating not less than 275 gm/m² 524 sqm 1234 646193
Providing and laying cement concrete in retaining walls, return walls, walls (any thickness) including attached pilasters, columns, piers, abutments, pillars, posts, struts, buttresses, string or lacing courses, parapets, coping, bed blocks, anchor blocks, plain window sills, fillets, sunken floor etc., up to floor five level, excluding the cost of centering, shuttering and finishing:
Detailed Project Report
188
Resul Pookutty Foundation
28 1:3:6 (1 cement : 3 coarse sand (zone-III) : 6 graded stone aggregate 20 mm nominal size)
29
CERAMIC GLAZED FLOOR TILES
Providing and laying Ceramic glazed floor tiles of size 300x300 mm (thickness to be specified by the manufacturer) of 1st quality conforming to IS : 15622 of approved make in colours such as White, Ivory, Grey, Fume Red Brown, laid on 20 mm thick cement mortar 1:4 (1 Cement : 4 Coarse sand), Jointing with grey cement slurry @ 3.3 kg/sqm including pointing the joints with white cement and matching pigment etc.,complete.
PAINTING WORKS
30
Providing and applying white cement based putty of average thickness 1 mm, of approved brand and manufacturer, over the plastered wall surface to prepare the surface even and smooth complete.
Distempering with 1st quality acrylic distemper, having VOC (Volatile Organic Compound ) content less than 50 grams/ litre, of approved brand and manufacture, including applying additional coats wherever required, to achieve even shade and colour.
31 One coat
Wall painting with acrylic emulsion paint, having VOC (Volatile Organic Compound ) content less than 50 grams/ litre, of approved brand and manufacture, including applying additional coats wherever required, to achieve even shade and colour.
32 Two coats
Applying priming coats with primer of approved brand and manufacture, having low VOC (Volatile Organic Compound ) content.
33 With ready mixed red oxide zinc chromatic on steel / iron works having VOC content less than 250 grams/ litre
Painting with synthetic enamel paint, having VOC (Volatile Organic Compound) content less than 150 grams/ litre, of approved brand and manufacture, including applying additional coats wherever required to achieve even shade and colour.
34 Two coats
79 cum. 8025 629963
510 sqm 927 472385
1992 sqm 87 174001
1992 sqm 31 61553
1992 sqm 74 147209
524 sqm 33 17045
524 sqm 75 39274
189
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
35
36
37
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Providing and fixing aluminium work for doors, windows, ventilators and partitions with extruded built up standard tubular sections/ appropriate Z sections and other sections of approved make conforming to IS: 733 and IS: 1285, fixing with dash fasteners of required dia and size, including necessary filling up the gaps at junctions, i.e. at top, bottom and sides with required EPDM rubber/ neoprene gasket etc.
Aluminium sections shall be smooth, rust free, straight, mitred and jointed mechanically wherever required including cleat angle, Aluminium snap beading for glazing / paneling, C.P. brass / stainless steel screws, all complete as per architectural drawings and the directions of Engineer-in-charge. (Glazing, paneling and dash fasteners to be paid for separately) : For fixed portion
Polyester powder coated aluminium (minimum thickness of polyester powder coating 50 micron)
For shutters of doors, windows & ventilators including providing and fixing hinges/ pivots and making provision for fixing of fittings wherever required including the cost of EPDM rubber / neoprene gasket required (Fittings shall be paid for separately)
Polyester powder coated aluminium (minimum thickness of polyester powder coating 50 micron)
Providing and fixing 12 mm thick prelaminated particle board flat pressed three layer or graded wood particle board conforming to IS: 12823 Grade l Type ll, in panelling fixed in aluminum doors, windows shutters and partition frames with C.P. brass / stainless steel screws etc. complete as per architectural drawings and directions of engineer-in-charge.
Pre-laminated particle board with decorative lamination on both sides
Providing and fixing glazing in aluminium door, window, ventilator shutters and partitions etc. with EPDM rubber / neoprene gasket etc. complete as per the architectural drawings and the directions of engineer-in-charge . (Cost of aluminium snap beading shall be paid in basic item):
857 kg 392 335831
443 kg 452 200345
53 sqm 867 46016
190
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
38 With float glass panes of 8 mm thickness 79 sqm 1154 91043
GATE, FRONT ARCH, STAIRCASE & RAILING
Steel work welded in built up sections/ framed work, including cutting,hoisting, fixing in position and applying a priming coat of approved steel primer using structural steel etc. as required.
39 In stringers, treads, landings etc. of stair cases, including use of chequered plate wherever required, all complete
40 In gratings, frames, guard bar, ladder, railings, brackets, gates and similar works
41
Providing and fixing stainless steel ( Grade 304) railing made of Hollow tubes, channels, plates etc., including welding, grinding, buffing, polishing and making curvature (wherever required) and fitting the same with necessary stainless steel nuts and bolts complete, i/c fixing the railing with necessary accessories & stainless steel dash fasteners , stainless steel bolts etc., of required size, on the top of the floor or the side of waist slab with suitable arrangement as per approval of Engineer-incharge,(for payment purpose only weight of stainless steel members shall be considered excluding fixing accessories such as nuts, bolts, fasteners etc.).
SANDSTONE FLOORING (PEDESTRIAN, YARD)
40 mm thick fine dressed stone flooring over 20 mm (average) thick base of cement mortar 1:5 (1 cement : 5 coarse sand) with joints finishedflush.
42 Red sand stone
ROAD
Providing and applying tack coat using hot straight run bitumen of grade VG - 10, including heating the bitumen, spraying the bitumen with mechanically operated spray unit fitted on bitumen boiler, cleaning and preparing the existing road surface as per specifications :
43 On W.B.M. @ 0.75 Kg / sqm
946 kg 94 88569
2067 kg 131 270731
434 kg 575 249987
275 sqm 889 244630
305 sqm 36 11116 2 cm premix carpet surfacing with 1.8 cum and 0.90 cum of stone chippings of 13.2 mm size and 11.2 mm size respectively per 100 sqm and 52 kg and 56 kg of hot bitumen per cum of stone chippings of 13.2 mm and 11.2 mm size respectively, including a tack coat with hot straight run bitumen, including consolidation
191
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
with road roller of 6 to 9 tonne capacity etc. complete (tack coat to be paid for separately).
44 With paving Asphalt grade VG - 10 heated and then mixed with solvent at the rate of 70 grams per kg of asphalt
45 Brick work with common burnt clay machine moulded modular bricks of class designation 12.5 in exposed brick work including making horizontal and vertical grooves 10 mm wide 12 mm deep complete in cement mortar 1:6 (1 cement : 6 coarse sand).
46 SECURITY CABIN
305 sqm 140 42709
50 cum. 7424 371185
110 SQ.FT 1500 35000
TOTAL 1,22,19,885
6.2 BOQ & Cost Estimates – Power Supply & Distribution
ANNEXURE II
Electrical - BOQ
Sl. No. Description
The schedule of probable quantities may vary on the higher side or lower side. Hence, during material pocurement, the contractor shall workout the actual quantites based on the shop drawings issued for execution as per the project manager's/consultant direction. Material procurement list shall be given to the client by the contractor when intimated and the same shall not be delayed from the part of the contractor. The contractor should intimate the consultant & client regarding the progress of work and should submit weekly reports.
All equipments/ items supplied by the client shall be checked by the contractor for any damage or discrepancy. The same shall be done within the period of return claim for the client.
All bolts, nuts, ancors, supports, glands, clamps and all such consumables & meters required for testing, reading equipments, testing apparatus etc required for installation, getting initial & final approvals, making necessary changes in drawing as intimated by statutory authorities and
Qty Unit Unit Rate Amount
192
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
commisioning of the entire installation after arranging inspection of the same shall be under the contractors scope and while quoting for labour rates prices shall be including all above mentioned.
All rates in this schedule shall be quoted by the contractor inclusive of GST, travel expenditures and all other expenses required for satisfactory completion of the work & all taxes as applicable. During claiming of each bill the contractor shall denote the taxes seperately.
WIRING
1 Point wiring in PVC conduit
Wiring for light point/ fan point/ exhaust fan point/ call bell point with 1.5 sq.mm FRLS PVC insulated copper conductor single core cable in surface / recessed medium class PVC conduit, with modular switch, modular plate, suitable GI box and earthing the point with 1.5 sq.mm FRLS PVC insulated copper conductor single core cable etc. as required.(Point to be considered inclusive of switch, coverplate and baseplate, suitable size GI box, PVC conduit and all accesoires required for complete installation etc)
1.1 One light point controlled by one way switch
Supply,Installation, testing and commisioning 91 Point 1471 133861
1.2 Loop Wiring
Supply,Installation, testing and commisioning 22 Point 589 12958
2 Wiring for circuit/sub main:
Wiring for circuit/ submain wiring along with earth wire with the following sizes of FRLS PVC insulated copper conductor, single core cable in surface/ recessed medium class PVC conduit including conduit and all acessories as required for complete installation and instructed by engineer in charge/consultant.
2.1 2x 1.5 sq.mm + 1x1.5sqmm earth wire
Supply,Installation, testing and commisioning 1380 Metre 159 219420
2.2 2x 2.5 sq.mm + 1x2.5sqmm earth wire
2.3
Supply,Installation, testing and commisioning 185 Metre 194 35890
2x 4 sq.mm + 1x4sqmm earth wire
Supply,Installation, testing and commisioning 135 Metre 238 32130
3 6A plug points
Supplying and fixing three module GI box with three modular plate and cover in front on surface or in recess, including providing and fixing 3 pin 5/6
193
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
amps modular socket outlet and 5/6 amps modular switch, connection etc. as required.
Supply, Installation, testing and commisioning 52 Each 248 12896
4 16A plug points
Supplying and fixing four module GI box with four module modular plate and cover in front on surface or in recess, including providing and fixing 6 pin 5/6 & 15/16 amps modular socket outlet and 15/16 amps modular switch, connection etc. as required.
Supply, Installation, testing and commisioning 12 Each 346 4152
5 20A plug points
Supplying and fixing four module GI box with four module modular plate and cover in front on surface or in recess, including providing and fixing 3 pin 20 amps modular socket outlet and 32 amps modular switch, connection etc. as required.
Supply, Installation, testing and commisioning 10 Each 465 4650
6 FAN REGULATOR
Supplying and fixing stepped type electronic fan regulator on the existing modular plate switch box including connections but excluding modular plate etc. as required.
Supply, Installation, testing and commisioning 19 Each 409 7771
7
CEILING ROSE
Supply and fixing 3 pin, 6A ceiling rose on the existing junction box / wooden block including connection etc as required.
Supply, Installation, testing and commisioning 35 Each 65 2275
8 PVC conduit:
Supplying and fixing of following sizes of PVC conduit along with accessories in surface/recess including cutting the wall and making good the same in case of recessed conduit as required.
8.1 20mm
Supply, Installation, testing and commisioning 570 Metre 81 46170
8.2 25mm
Supply, Installation, testing and commisioning 1018 Metre 98 99764
8.3 32mm
Supply, Installation, testing and commissioning 60 Metre 126 7560
9 Wiring for Staircase Light Point
194
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Wiring for stair case light points with UPS powered 1.5 q.mm FRLS PVC insulated copper conductor single core cable in surface / recessed medium class PVC conduit and all acessories required for complete installation etc , with 1 way modular switch, modular plate, suitable GI box medium class PVC conduit and all acessories required etc and earthing the point with 1.5 sq.mm FRLS PVC insulated copper conductor single core cable etc as required and instructed by engineer in charge/consultant. (*Note - Staircase light point shall be controlled by a single switch located inside fire control room/security room in ground floor as per latest fire norms. (Point to be considered inclusive of switch, coverplate and baseplate, suitable size GI box, PVC conduit and all accesoires required for complete installation etc)
9.1 One light point controlled by one way switch ( Terrace)
Supply, Installation, testing and commisioning 1.00 Point 844 844
9.2 Loop wiring for Light point
Supply, Installation, testing and commisioning 4.00 Point 285 1140
10 PVC FLEXIBLE CONDUIT
10.1
Supply and clamping the following size of corrugated pvc fiexible conduit with necessary locking ring and check nut at termination pointed using suitable size GI/painted MS saddles spacing not exceeding 60 cms on surface including making good the damages, colour washing etc.as required 20mm dia
Supply, Installation, testing and commisioning 92 m 42 3864
11 BLANKING PLATE
Supplying and fixing modular blanking plate on the existing modular plate & switch box excluding modular plate as required.
Supply, Installation, testing and commisioning 52 Each 34 1768
12
12.1
LIGHT FIXTURES
Supply, installation, testing and commissioning of Linear basic all purpose surface/ wall mounted 20W LED batten with polycarbonate housing & integrated electronic driver with all accessories required for complete installation ( Havells make Lumiline/ Equivalent)
Supply, Installation, testing and commisioning 18 Each 2118 38124
12.2 Supply, installation testing & commisioning of LED Recessed slim panel luminare of square profile of
195
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
15W, RoHS compliant, with surge protection of 2.5kV, SMD light source with 1500Lm rated luminous flux, CRI>80, and efficacy 95-100 Lm/Watt with minmium 40000 hours burning life, IP 40, with aluminium body and PC diffuser, with white light suitable for hospital application, including driver and all accesories as required for complete installation, as instructed by engineer in charge and making good any damages made during installation (Luker LED - LNPS30 or equivalent)
Supply, Installation, testing and commisioning 46 Each 650 29900
12.3 Supply, installation testing & commisioning of linear & compact surface and wall mounted LED batten with polycarbonate housing & integrated,with size in mm (LxWxH) 597x25x41 suitable to use as mirror light with all accessories as required. (Havells LHEXBQP7IN1W009 or equivalent)
Supply, Installation, testing and commisioning 2 Each 500 1000
12.4 Supply, installation, testing and commissioning of 1x12W LED type surface/wall mounted luminare as bulk head with optal diffuser and all accessories, Supply, Installation, testing and commisioning 8 Each 1356 10848
12.5 Supply, installation, testing and commissioning of surface mounted circular LED Downlighter with a nominal system lumen output of 2000 lumens and a minimum system efficacy of 111 lm/W. Luminaire wattage should not exceed 18W. The luminaire should have a color temperature of 6500K and CRI>80. Diffuser material should be of PolyCarbonate. Driver of the luminaire shall have THD<10% and PF > 0.9. Luminaire height should not be more than 26mm. The driver shall comply to IEC 62384 , IEC 61347-2-13, IEC 61547, EMICISPR15 standards including all accessories as required for complete installation . (Philips Make Sleek Surface "SM251C LED20S 6500 PSU WH" or equivalent)
Supply, Installation, testing and commisioning 60 Each 750 45000
12.6 Supply, installation, testing and commissioning of Ceiling suspended/ wall mounted type Fire Exit indicator LED Lights Supply, Installation, testing and commisioning 5 Each 2200 11000
12.7 Supply, installation, testing and commissioning of Cool white LED lights,36W , IP65 waterproof for building sign board Supply, Installation, testing and commisioning 4 Each 1950 7800
196
Resul Pookutty Foundation
13
TPN MCB DISTRIBUTION BOARD
Supplying and fixing following ways, horizontal type three pole and neutral, sheet steel, MCB distribution board(IP 43) with metal door, 415 volts, on surface/ recess, complete with tinned copper bus bar, neutral bubar, earth bar, din bar, detachable gland plate, interconnections, phosphatised and powder painted including earthing etc. as required Including providing all necessary connections and making good the damages etc as required.
13.1 4 way (4 + 8), Double door TPN
Supply, Installation, testing and commisioning 1 Each 9111 9111
13.2 8 way (8 + 16), Double door TPN for Ground and First Floor
Supply, Installation, testing and commisioning 2 Each 11066 22132
13.3 Main panel TPN Double door for 63 Incomer and MCB/Isolators with bus bar connections and accessories
Supply, Installation, testing and commisioning 1 Each 15000 15000
14 MCB
'C' Curve, MCB:
Supply, fixing, testing and commisioning of 6 amps to 32 amps rating, 240 and 415 Volts, 'C' curve, miniature circuit breaker suitable for heavy currents in normal working of following poles in the existing MCB DB/VDB complete with connections, testing and commissioning etc. as required.
14.1 Single pole Supply, Installation, testing and commisioning 60 Each 268 16080
15 RCBO
Supplying, fixing, testing and commissioning following double pole, 240 volts, residual current circuit breaker with overload protection (RCBO) of the following rating and sensitivity current in the existing MCB SPN horizontal DB complete with connections, etc. as required and instructed by engineer in charge/consultant..
15.1 20A 30mA TPN RCBO
Supply, Installation, testing and commisioning 1 Each 4550 4550
15.2 40A 30mA TPN RCBO
Supply, Installation, testing and commisioning 2 Each 5254 10508
16 Isolator With Enclosure
197
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
Detailed Project Report
Supply and fixing of FP CRCA sheet steel powder coated enclosure on surface/recess along with following Amps, 415V, FP isolators confirming to IEC 60947-3 complete with all accesories, connections, testing and commissioning etc as required and as instructed by engineer in charge also making good any damages made during installation.
20A FP Isolator with enclosure
Supply, Installation, testing and commisioning 1 Each 750 750 40A FP Isolator with enclosure
Supply, Installation, testing and commisioning 2 Each 946 1892 63A FP Isolator with enclosure
Supply, Installation, testing and commisioning 1 Each 948 948
17 LT CABLE SUPPLY & LAYING
Supply, laying / clamping, testing and commisioning of the following XLPE insulated PVC sheathed armoured heavy duty power cable conductor of best conductivity aluminium 1.1kV grade strictly conforming to IS:1554 (Part-I) 1964 of the following sizes in cable trench/cable tray /wall using factory made heavy gauge GI/painted MS clamps. Space between clamps not exceeding 60cms amd making good the damages colour washing etc as required and as instructed by engineer in charge.
17.1 4cx35sq.mm AYFY Cable (clamped with 1mm thick saddle)
Supply, Installation, testing and commisioning 150 m 715 107250
18 END TERMINATION
Supply and making end termination with brass compression gland, earth clip and aluminum lugs/ Cu lugs for following size of XLPE insulated and PVC sheathed aluminum/copper conductor cable of 1.1kV Grade as reqiured.
18.1 4x25sq.mm A2XFY Cable (clamped with 1mm thick saddle)
Supply, Installation, testing and commisioning 2 Each 400 800
18.2 4x4sq.mm A2XFY Cable (clamped with 1mm thick saddle)
Supply, Installation, testing and commisioning 4 Each 250 1000
19 UPS SYSTEM
198
Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Installation, testing, and commissioning of 5kVA three phase UPS system, indoor (IP20) with surge protection system with 60 min backup battery, 6 nos 150 AH, (SMF battery of reputed make), having redundancy, input pf>0.99, input current consumption, built in isolation transformers, with necessary battery circuit breaker., double conversion technology with input 415V, 50Hz three phase, output 415V, 50Hz three phase, SNMP card for network monitoring .It shall be 100% generator compatabile, with efficiency > 94% and output power factor > 0.9 and including all accessories etc as required.The system shall comply to IEC /EN 62040-1 and relevant IS standard.The acoustic noise of the system should be less than 58dB.The system shall comply to IEC /EN 62040-1, EN/IEC 62040-2, EN/IEC 62040-3 and relevant IS standard. The system shall be true online double - conversion DSP based UPS system connected in parallel redundant load sharing configuration with each UPS unit having inbuilt parallel kit and also each UPS shall be with automatic & manual bypass switch capable of working in standalone configuration also. The system shall have IGBT rectifier and inverter. Rate shall inclusive of UPS DB Panel, UPS inverter, Batteries and connections Supply, Installation, testing and commisioning 1 Each 155000 155000 20 UPS
PANEL
Fabrication, supply, erection, testing and commissioning of cubicle type, dust and vermin proof, floor mounted, front operated type tested MV panel board made out of 16 SWG thick CRCA sheet fully compartmentalised complete with hinged and earthed front doors with name plate, danger notice board, heavy duty rubber gaskets, removable gland plates made out of 3mm thick sheet steel including all components as shown in the schematic drawing. All opening parts of the panel shall be sealable. Providing all connections and interconnections as required and providing all assecories as required for complete installation as instructed by engineer in charge/consultant.This panel should include pluggable type surge arrester in suitable enclosure Class B+C/ Class 1+2 as per IEC 61643 (IP 20) with potential free contact, thermal dis connector & provision for inbuilt for defective arresters between Line - Neutral and
Resul Pookutty Foundation
199
Neutral – Earth, one number arrester Spark Gap type to connect between Neutral and Earth of following ratings including base element & pluggable arresters. Nominal voltage - 230V 50Hz, type single MOV with built in thermal fuse and cooling gel(L to N) & spark gap encapsulated / non exhausting (N to E) . Lightning Impulse Current –37.5 kA (10/350µ sec) for Line to Neutral & 50 kA(10/350µ sec) for Neutral to Earth,Nominal discharge current-90 kA (8/20µ sec) for Line to Neutral & 50 kA(8/20µ sec) for Neutral to Earth, max discharge current 150 kA (8/20µ sec) for Line to Neutral & 100 kA(8/20µ sec) for Neutral to Earth. Voltage protection level 1500V (L to N) & 1500V (N to E). Operating temp -40º to +80ºC. Response time <25 nano sec (L to N), < 100 nano sec (N to E) DIN rail mounting type etc complete with back up HRC fuse as required and as directed.. Multi function digital LED meters with accuracy class 1, with necessary CT and accessories for measuring Voltage, current, kWh, KW, frequency, KVA, kVAr - 1 Set RYB phase indicating LED lamps with control fuses and switches - 1 set. Class B+C/ Class 1+2 Surge arrestor with necessary HRC fuse protection UPS Panel shall power lights and fans Outgoing 40A TP MCB- 3 Nos
Supply,Installation, testing and commisioning 1 Each 17500 17500
21 CABLE TRAY
Fabrication, supply and erection of vertical and horizontal type ladder cable trays and cable supports fabricated out of MS angles (ISA) and MS flats with sufficient width and spacing between successive cross members and supported at adequate spacing. The cable trays and supports shall be painted with two coats of Zinc Chromate primer and two coats of enamel paint. The design/routing of cable trays and its details shall be given for approval to site engineer in charge/consultant before execution.
Supply,Installation, testing and commisioning200x75 160 m 550 88000
22 Supply & fixing Laminated drawings of electrical lay out, schematic drawing etc on good frame work.
1 set 2800 2800
200
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
23 LIGHTNING & EARTHING PROTECTION
23.1 Supply, installation and tesing of 4 meter air terminal with accessories, providing and fixing air terminals as per IEC -62305 part-3 16mm rod tapered to 10 mm aluminium rod 4 meter rod: Meets the technical specification according to DIN EN 50164-2 (VDE 0815 part 202). Meets the requirement of VDE0185/305(IEC 62305) 101 VL 4000: semi-hard (E-AlMgSiO5 corresponds to DIN 48801) Suitable for high wind load. System consist of Fang Fix with base and clamp on the top air terminal is erected. Fang fix clamp made of cable bracket, lightning tested for 100 KA 10/350 micro sec waveform. 2 nos of 16 KG stone of 365 mm diameter, high level of stability. Quick and easy mounting of interception rod using anchors.Concrete, frost-resistant, can be stacked, including all accesories as required for complete installation as instructed by engineer in charge. Supply,Installation, testing and commisioning 1 SET 8000 8000
23.2 Supply and installation of 8mm solid aluminium round conductor: For concrete building Meets the technical specification according to DIN EN 50164-2 (VDE 0815 part 202). Meets the requirement of VDE0185/305(IEC 62305) RD 8/ALU: semi-hard (EAlMgSiO5 corresponds to DIN 48801) With 50 sq.mm cross sectional area. Polyamide Conductor holder:With M8 female thread or diameter 7mm, M8 Screw to connect the conductor holder. Weather and temperature resistant from -35 to +90 degree Celsius tested. Conductor holder @ 1 meter distance, including all accesories as required for complete installation as instructed by engineer in charge.
a) Vertical run- Down conductor
23.2. 1 Supply,Installation, testing and commisioning 40 m 387 15480
b) Horizontal run-Parapet application
23.2. 2 Supply,Installation, testing and commisioning 72 m 357 25704
23.3 Supply and fixing of cross connector/T connector: to route vertical down conductor /mesh formation made of stainless steel/hot dipped galvanised iron with necessary screws etc as required. Installed with 4 hexagonal bolts M8*25 with M8 hexagonal nuts and all accesories as required for complete installation
201
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Supply,Installation, testing and commisioning 24 Each 308 7392
23.4 Supply and fixing of expansion piece with connector: For equalising temperature related length changes. Necessary on conductors length over 20 meters. For round conductor Rd 8/ALU. Connector: For T cross and parallel connectors. Quick installation using hexagonal bolt M10X30 high-grade hot dip galvanised. Conforms to the requirements according to DIN VDE 0185-305 (IEC 62305) and all accesories as required for complete installation
Supply,Installation, testing and commisioning 6 Each 621 3726
23.5 Supply and Fixing Equipotential bonding rail for Lightning Arrestor applications(Test Joint). Equipotential bonding rail for equipotential bonding according to DIN VDE 0100-410/540 and lightning protection equipotetial bonding according to DIN VDE 0185-305. Base plate and cover hood from polystyrene. Colour: Black, UV resistant. Can be used outdoor also. Screw and crossbar made of VA. Capable of carring lightning current 100KA (10/350). Connection options: 7 x single or multicore conductors to 25mm square or fine core conductors to 16mm square. 1 x round cable Rd 810. 1 x flat strip to FL 30 or round cable RD 8-10 including corrosion tapes and all accesories as required for complete installation as instructed by engineer in charge.
Supply,Installation, testing and commisioning 3 Each 758 2274
23.6 Supply and laying hot dip Galvanised Steel Flat having 70 microns zinc 30X3 mm thick from earth electrode directly in ground as required. Hot Dip GI strip, corrosion resistant. Cross sectional area of 90mm square According to DIN EN 50164-2 (VDE 0185 part 202) Meets the requirement of VDE0185/305(IEC 62305) Zinc coating: 500 g/m square (70 micron coating) Should be tested and use exclusively for lightning protection earthing system and ring equipotential bonding including cross connectors and all accesories as required for complete installation as instructed by engineer in charge.
Supply,Installation, testing and commisioning 20 m 850 17000
202
Resul Pookutty Foundation
23.7 Supply, installation and testing of maintenance free Earthing system as per IS 2309 ,IEC 62305 part3, IEC 60364, IEC 62561 part 2, IS 3043, UL 467 & UL 96 standards. Earthing System comprises of molecularly bonded copper of 99.9% purity on low carbon steel of 3m length (1m (219 20 CU) x 3 nos), having a diameter of 20mm with copper coating thickness of 250 microns with self-coupling bore and peg arrangement (without the need for external coupler) with fault current withstand capability of 20 KA rms value for 1 second and I peak of 50 KA. For obtaining desired length, the number of rods shall be increased and is provided with Universal Clamp (2730 20 VA) made of SS 304 for clamping the cable/flat conductor to the rod. Impact point (219 20 IP) on the bottom rod for easy insertion. Earth enhancing mineral compound (ECS PB 12.5) is used for improving the soil conductivity. Earth enhancing mineral compound shall be so designed and constructed that in normal use their performance is reliable and without danger to persons and the surroundings. The material shall be mineral inert to sub soil and shall not pollute the environment. It shall provide a stable environment in terms of physical and chemical properties and exhibit low resistivity. It shall not be corrosive to the earth electrode itself. The material should have a resistivity less than 0.2 Ohm meter. It should be free from hazardous substances The mineral compound is required to have minimum 12.5 Kg of the total composite. Polypropylene & Polyethylene (UFE)Earth electrode inspection chamber with heavy duty cover should be used to cover the Earth Rod. The dimension shall be 170mmx 170mmx 190mm with a weight bearing capacity of 5KN, including all accesories as required for complete installation as instructed by engineer in charge. (Minimum 2 earth pits shall be provided. No of earth pits shall be increased till overall earth resistance of the system is less than 10ohms as per site conditions and soil resistivity)
Supply,Installation, testing and commisioning 3 SET 16500 49500
203
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
24 PREPARATION OF ALL DRAWINGS
Sub Centre – Yeroor Grama Panchayath
Preparation of all drawings (shop drawings for approval from client/consultant, all inspectorate and local authority approval drawings & final Asbuilt drawings after handing over), submitting and getting approval from Electrical Inspectorate, submitting of Completion certificates and arranging inspection, getting sanctions and energisation certificates, test reports, manuals, technical details,preperation of as-built drawings, obtaining as-built/GA drawings of all equipments from concerned and also obtaining all necessary sanctions from relevant regulatory boards, obtaining power allocation & power connection etc. for commissioning including commisiong of the whole installation in the premises. All statutory payments will be reimbursed on production of the original receipts.
1 LS 50000 50000
TOTAL 14,03,182
6.3 BOQ & Cost Estimates – HVAC
ANNEXURE III
Airconditioning - BOQ
Sl. No. Description
1 SPLIT UNIT
Supply, Installation, testing & commissioning of Wall mounted inverter split units of following capacity suitable to operate from 230+10%volt,50Hz,single phase AC power supply with air-cooled condenser with copper coil,fan,fins with corrosion proof coating and with rotary compressor.Necessary wirings from the power source to outdoor unit and indoor unit shall be included. M.S.frame duly painted to locate Outdoor Unit. Refrigerant shall be a Green Gas, R32 or better.
1.1 1.0 TR 3 Each 24000 72000
1.2 1.5 TR 6 Each 28000 168000
2 PIPING
2.1
Supply, Installation and testing of Refrigerant copper pipe , liquid and gas line insulated with 19mm thk. closedcell Nitrile Rubber insulation,interconnecting control cabling
Detailed Project Report
204
Resul Pookutty Foundation
Qty Unit Unit Rate Amount
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
between indoor/outdoor unit, and shall be provided with necessary support for indoor and outdoor units,complete in all respects for unit capacities:
Copper Refrigerant pipe for Liquid line
90 Metre 500 45000
Copper Refrgerant pipe for gas line 90 Metre 500 45000
3 FAN FIXTURES
3.1 Supplying, installation, testing and commisioning of ceiling fan of 1200mm sweep, including the down rod of standard length (upto 30 cm.) of (havels make, ES 50 White or CG make, Riveria or equivalent) including all accessories as required for complete installation.
3.2 Supplying, installation, testing and commisioning of wall mounted fan of 600mm sweep, including the Wall mounting bracket with provision for speed regulator of (havels make or CG make or equivalent) including all accessories as required for complete installation.
3.3 Supplying, installation, testing and commisioning of Ducted ceiling suspended type exhaust fan of 250mm sweep in the existing opening, including making good the damage, connection, testing, commissioning etc. as required, including all accessories as rquired for complete installation incluidng shutter etc complete as required.(Havells, Ventil Air DX White or equivalent) and all accessories as required for complete installation.
3.4 Supplying, installation, testing and commisioning of Ducted ceiling suspended type exhaust fan of 200mm sweep in the existing opening, including making good the damage, connection, testing, commissioning etc. as required, including all accessories as rquired for complete installation incluidng shutter etc complete as required.(Havells, Ventil Air DX White or equivalent) and all accessories as required for complete installation.
3.5 Supplying, installation, testing and commisioning of exhaust fan of 200mm sweep in the existing opening, including making good the damage, connection, testing, commissioning etc. as required, including all accessories as rquired for complete installation incluidng shutter etc complete as required.(Havells, Ventil Air DX
18 Each 1375 24750
1 Each 9500 9500
3 Each 4500 13500
1 Each 6500 6500
1 Each 2500 2500
205
Resul Pookutty Foundation
Detailed Project Report
White or equivalent) and all accessories as required for complete installation.
3.6 Supplying, installation, testing and commisioning of exhaust fan of 150mm sweep in the existing opening, including making good the damage, connection, testing, commissioning etc. as required, including all accessories as rquired for complete installation incluidng shutter etc complete as required.(Havells, Ventil Air DX White or equivalent) and all accessories as required for complete installation.
3.7 Supplying, installation, testing and commisioning of exhaust fan of 250mm sweep industrial type in the existing opening, including making good the damage, connection, testing, commissioning etc. as required, including all accessories as rquired for complete installation incluidng shutter etc complete as required.(Havells, Ventil Air DX White or equivalent) and all accessories as required for complete installation.
4 DUCTING
4.1 Supplying, installation, and testing of ducting connected to the fans. Ducts shall be fabricated out of galvanised steel of Class 111 parameters which are confirming to IS 655-1963. Thickness of the duct shall not be less than 0.63mm. All ducts shall be supported from the ceiling with necessary rod an angles. Ducts shall be provided with ss mesh at the roof and shall be with goose neck.
4.2 Supplying, installation, of powder coat Exhaust diffuser of 100 dia neck size for the toilet exhaust system
3 Each 800 2400
2 Each 3500 7000
45 Metre 620 27900
7 Each 2250 15750
TOTAL 4,39,800
206
Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
6.4 BOQ & Cost Estimates – Plumbing & Storm Water Management
ANNEXURE V
Plumbing - BOQ
Sl. No. Description
FLOOR MOUNTED EUROPEAN WC
1 Providing and fixing floor mounted single piece/double piece white vitreous china water closet (European type) with seat and lid, 6 litre twin flush cistern & provided with S Trap, CP angle valves, mosquito proof coupling of approved municipal design complete, including painting of fittings and brackets, cutting and making good the walls and floors wherever required :, or equalent specification.
WASH BASIN WITH FAUCET
2 Supplying and fixing 630 X 450mm or nearest size white glazed earthenware counter type wash basin, with 15 mm dia brass quarter turn CP basin pillar tap, 32 mm dia. brass CP waste coupling, 32 mm dia brass CP bottle trap with extension pipe, stainless steel screws, 1no.15mm brass CP angle valve with 450 mm long metallic flexible tube, brass CP wall flanges, 40 X 32 mm PVC reducer to connect the extension pipe from bottle to the PVC waste pipe, all of approved make etc., complete including cutting and making good the walls., or equalent specification.
3 Supplying and fixing 630 X 450mm or nearest size Stainless steel wall mounted type wash basin , with 15 mm dia brass CP basin pillar tap, 32 mm dia. brass CP waste coupling, 32 mm dia brass CP bottle trap with extension pipe, stainless steel screws, 1no.15mm brass CP angle valve with 450 mm long metallic flexible tube, brass CP wall flanges, 40 X 32 mm PVC reducer to connect the extension pipe from bottle to the PVC waste pipe, all of approved make etc., complete including cutting and making good the walls., or equalent specification.
URINALS
Qty Unit Unit Rate Amount
10 each 6914 69140
16 each 3680 58880
2 each 4343 8686
207
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
4 White vitrous flat back lipped Urinal of size 440x265x335mm/nearest size with automatic flushing cistern running on DC/AC, MS brackets, standard size flush pipe with required length with standard spreader and fittings, bottle trap, screws, washers, etc. as applicable and complete including breaking and making good the wall and floor as per Architectural drawings and relevant Standards., or equalent specification.
5 White vitrous china urinal Partition wall with anchor fasteners, C.P brass bolts, screws, washers, etc. as applicable and complete including breaking and making good the wall and floor as per Architectural drawings and relevant Standards., or equalent specification.
SINK WITH COCK
6 Supplying and fixing 550 X 450mm or nearest size Stainless Steel Kitchen Sink, with 15 mm dia brass CP basin pillar tap, 32 mm dia. brass CP waste coupling, 32 mm dia brass CP bottle trap with extension pipe, stainless steel screws, 1no.15mm brass CP angle valve with 450 mm long metallic flexible tube, brass CP wall flanges, 40 X 32 mm PVC reducer to connect the extension pipe from bottle to the PVC waste pipe, all of approved make etc., complete including cutting and making good the walls., or equalent specification.
7 Supply and fixing 600X450X200mm or nearest size white vitreous china laboratory sink with C.I. brackets, C.P. brass chain with rubber plug, 40 mm C.P brass waste and 40mm C.P. brass trap with necessary C.P. brass unions complete, including painting of fittings and brackets, cutting and making good the wall wherever required :, or equalent specification.
SHOWER
8 Shower System unit comprising of single lever shower diverter/mixer with upper trim, bath spout, casted type multi-flow shower head with wall/ceiliing flange and necessary fittings and complete including breaking and making good the wall and floor as per Architectural drawings and relevant standards., or equalent specification.
TOILET ACCESSORIES
Detailed Project Report
2 each 4869 9738
1 each 1400 1400
1 each 4850 4850
1 each 3162 3162
1 each 5350 5350
208
Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
9 C.P Health faucet with holder, one meter long flexible pipe, angle valve with wall flange and complete including breaking and making good the wall and floor as per Architectural drawings and relevant standards., or equalent specification.
10 Supply, installation and commissioning charges for Soap Tray/dish including, accessories, bolts/screws, washers, etc. as applicable, complete including making good the wall as per Architectural drawings and as relevant standards., or equalent specification
11 Supply, installation and commissioning charges for Towel Rail including, accessories, bolts/screws, washers, etc. as applicable, complete including making good the wall as per Architectural drawings and as relevant standards., or equalent specification.
12 Supply and installation of stainless steel grab bars for disable toilet including, accessories, bolts/screws, washers, etc. as applicable, complete including making good the wall as per Architectural drawings and as relevant standards., or equalent specification.
WATER SUPPLY PIPES
13 Supply, installation, testing & commissioning of CPVC water supply system pipe work including solvent welded/threaded fittings(tees, elbows, unions, reducers, coupling, etc.), GI "U" bolts, GI slotted rails, rail legs, accessories, etc. for supply riser, distribution risers, ring mains, suspended pipes, etc. with pipes and fittings as per uPVC schedule-40/80 suitable for working pressure of 20bars all in accordance with drawings and relevant standards.
Pipe supporting/ Clamping details:- For vertical shaft piping, pipes shall be clamped/supported by using 8mm GI "U" bolts to heavy duty GI slotted (2.5mm) rails& rail legs. For suspended piping, pipes shall be clamped/supported by using 8mm GI "U" bolts to heavy duty GI slotted rails(2.5mm) & slotted rails shall be suspended using 10mm threaded road, 10mm angle fastner, nuts & washers to the slab., or equalent specification. Cold water Pipeworks inside the toilets shall be concealed lines.
Detailed Project Report
10 each 1338 13380
1 each 849 849
1 each 849 849
2 each 499 998
209
Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
13.1 20 mm dia 226 RM 404 91304
13.2 25 mm dia 76 RM 474 36024
13.3 32 mm dia 80 RM 525 42000
13.4 40 mm dia 15 RM 546 8190
13.5 50 mm dia 9 RM 778 7002 PUMPS
14 Supply, installation, testing & commissioning of Water lifting pump, with pumps (2 nos on a 1duty + 1 standby basis) with control panel, automatic changeover switch, with all necessary valves, flexible connections, pressure gauges, strainers, supports, fixings and fittings electrical/ control panels, power and control cabling , cable trays, automatic level controller, etc. as specified and as shown on drawings and complying to relevant standards., or equalent specification.
14.1 Duty conditions:-1.5 LPS @ 25 M Head (One Duty + One standby) 1 set 55000 55000 VALVES
15 Supply, installation, testing and commissioning of fullway lever operated brass valves with brass body with necessary MTA fittings with all supports, flanges, fixings and fittings all as specified and as shown on drawings and complying to relevant standards, or equalent specification.
15.1 25 mm dia lever operated Ball Valve 6 each 1720 10320
15.2 32 mm dia lever operated Ball Valve 3 each 3130 9390
15.3 40 mm dia lever operated Ball Valve 3 each 4000 12000
15.4 50 mm dia lever operated Ball Valve 1 each 4980 4980
15.5 Allowance for Water meter and Valves package 1 each 9600 9600
DRAINAGE PIPING
16 Supply, installation, testing and commissioning of SWR pipes conforming to PVC IS 13592 Class B for 75mm dia and above, & 6kg/sqcm pipes for pipes below 75mm dia and uPVC IS 13592 Class A pipes for rain water & vent piping including necessary fittings and accessories clamped in position & jointing with O-rings, supports, brackets,etc. for above the ground installation(shafts/suspended) all in accordance with the drawings and specification. Pipe supporting/ Clamping details:- For vertical shaft piping, pipes shall be clamped/supported by using 8mm GI "U" bolts to heavy duty GI slotted
Resul Pookutty Foundation
210
(2.5mm) rails& rail legs. For suspended piping, pipes shall be clamped/supported by using 8mm GI "U" bolts to heavy duty GI slotted rails(2.5mm) & slotted rails shall be suspended using 10mm threaded road, 10mm angle fastener, nuts & washers to the slab., or equalent specification.
16.1 40 mm dia 62 RM 355 22010
16.2 50 mm dia 8 RM 410 3280
16.3 75 mm dia 130 RM 610 79300
16.4 110 mm dia 184 RM 865 159160
17 Supply, installation, testing and commissioning of concealed drainage system (condensate drain from indoor units to nearest drain point) PVC pipes confirming to IS 13592 Class B including necessary fittings, accessories, supports, brackets, etc including cutting the wall /slabs/surface and making good the wall after installation all in accordance with the drawings and relevant standards., or equalent specification.
17.1 25 mm dia 72 RM 1720 123840
18 Supply, installation, testing and commissioning of SWR PVC pipes conforming to IS 4985 class3(6kg/sqcm) including necessary fittings, excavation, connection to manholes, bedding the pipe in constant intrevels, back filling, removing the surplus etc. as per IS:1742-1983 and testing the lines to required hydraustatis pressure for below ground(seware) installation all in accordance with the drawings and relevant standards., or equalent specification.
18.1 110 mm dia 25 RM 782 19550
18.2 160 mm dia 140 RM 1295 181300
DRAINAGE FITTING
19 Supply, Installation, testing and commissioning of drainage fixtures and accessories including cutting and making good the wall/slab all in accordance with the drawings and relevant standards., or equalent specification.
19.1 uPVC deep seal multiple floor Trap with SS304 grade lockable type anticockroach floor drain. 14 nos 850 11900
19.2 110mm dia outlet rain water outlet costructed with CI body, aluminium ring and grade and SS304 grade screws
6 nos 1200 7200
211
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
19.3 S.S. frame square or round floor clean out with rubber seal and flat cover & screw for following pipe sizes
110 mm 1 nos 900 900
19.4 PVC clean out with accessories for following pipe sizes
110 mm 2 nos 350 700
MANHOLES
20 Supply, constructing sewer manholes 90x80 with 20cm thick brick walls in cement mortar 1:6, plastering inside & outside with cement mortar 1:3, 12mm thick with neat cement flushing coat and foundation concrete 20cm thick and forming channels with cement concrete 1:3:6 using 40mm broken stone, providing collars around pipes with cement concrete 1:2:4 using 20mm broken stone, corbels at top courses on two sides and R.C.C slab of 15cm thick with cement concrete 1:2:4 using 20cm broken stone and necessary reinforcement and providing necessary provision for fixing hinged type ductile iron manhole cover, its frame and C.I step as per relevant standards and specifications, or equalent specification.
20.1 60X60cm internal diamention & .9m average depth manholes with hinged type manhole covers(medium duty) & frames confirming to relevant IS standerds
GULLY TRAP
21 Supply, installation, testing and commissioning of PVC gully trap of size 160X110mm embedded in PCC of 1:4:8 using 20mm broken stone, all the above encased in a 115mm thick chamber of size 300X300 constructed using brick with cement mortar 1:3, 100mm thick cement concrete of 1:4;8 using 40mm broken stones, plastering inside, outside & exposed surfaces with cement mortar 1:3, 12mm thick and finished with a floating coat of neat cement. Providing and fixing hinged type ductile iron manhole cover & frame of size 300X300 in PCC of 1:2:4 using 20mm broken stones including two coat of black bitumastic painting of cover & frame as per relevant standards and specifications, or equalent specification.
MANHOLE COVER
17 nos 18422 313174
7 nos 2650 18550
212
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
22 Supply and fixing of CI manhole frame and cover of lockable type ( Double Sealed ) over openings of underground sump, overhead tank, rain water Sump, soak pits., or equalent specification.
22.2 600 x 600 mm size - Medium Duty cover ( Testing Load 2.5 to 10 Ton )
23
EARTHWORK RELATED TO PLUMBING
Construction of RCC Septic tank and Soakaway pit.Earthwork in excavation for chambers, septic tanks, soak pits etc., including all lifts in both wet and dry condition, bailing out water, shoring, stacking/disposal of surplus and un serviceable soil within a lead of 100m & spreading in layers and as per direction of Engineer. In all soils including soft rock/disintegrated rock and hard rock. The excavated earth which is to be used for back filling shall also be disposed and stacked separately at locations indicated by the Engineer within a lead of 100M. Back filling(with available earth) with mechanical compaction to achieve dry density in all positions required by the engineer with available earth from spoil heaps at all heights /depths including transporting, depositing, compacting, dressing, trimming etc., complete as desired in layers not exceeding 150mm including watering, consolidating by mechanical means instructions of the engineer. For depth up to 2.0m. , or equalent specification.
RAINWATER COLLECTION TANK
24 Construction of under ground RCC/PVC rain water collection tank with the provision of overflow pipe connecting to the nearest recharging point. Work shall all civili works including excavation, construction of tank, backfilling to complete the works. Capacity of the tank shall be 15 Cu.m
PVC TANK FOR WATER
25 Supply Installation and Testing of PVC Tanks of 2000 L capacity for daily water storage in the upper roof.
17 nos 4525 76925
1 65000 65000
1 150000 150000
1 11600 11600
TOTAL 17,07,481
213
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
ANNEXURE VI
FIRE EXTINGUISHER
1 Supply and fixing of 6 Kg ABC Dry Powder (Stored Pressure) Type Fire Extinguisher. Pressurized with dry nitrogen gas at 15 bar. Design, construction and testing as per IS 2171-1999 external epoxy powder coating with PO Red Shade No. 538 of IS 5, Supplied with standard accessories. Supply & Installation 4 no’s 3,999 15,996 TOTAL 15,996
ANNEXURE
Detailed Project Report
214
Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
6.5 BOQ & Cost Estimates – Fire Fighting
Fire & Safety - BOQ
Sl. No. Description Qty Unit Unit Rate Amount
6.6 BOQ & Cost Estimates – Low Voltage Systems
IV Low Voltage System - BOQ Sl. No. Description Qty Unit Unit Rate Amount
1 INTERNET, SERVERS AND NETWORK 1.1 ServerDell PowerEdge T30 Server, Intel Xeon E3-1225 v5 with 16GB RAM and 1TB SATA Hard Disk or Equivalent 1 LS 55000 55000 1.2 Netgear ReadyNAS 214 RN21400-100INS 4-Bay Diskless Network Attached Storage for Personal Cloud 1 LS 33200 33200 1.3 Cisco SG250-10P Smart Switch | 10 Ports Gigabit Ethernet (GbE) Ports 2 nos 24000 48000 1.4 Patch Panel,12Port,Cat6a,UTP,90 degree 1U of an EIA-standard 19-inch rack , Mounting hardware for wall-mount,Heavy-duty 14 ga cold-rolled steel construction,a tray at the rear of the panel.12PORT CAT6A Patch Panel Shielded Rackmount Loaded 568A/568B 2 nos 7500 15000
1.5 Keystone,Cat6A UTP,Black,Toolless Type RJ45 Jack Housing: ABS + PC, UL 94-V0 Contact Bracket: PC, UL 94-V2, transparent Color 6 nos 220 1320
Sub Centre – Yeroor Grama Panchayath
RJ45 Contact Material: Phosphor Bronze with Nickel Plating Finish: White
1.6 Faceplate,Single Port,Modular Straight Shutter(2-Piece) Width - 25mm Depth - 21mm Height - 50mm Back-box Depth - Minimum 15mm recommended Material - Polycarbonate/ABS thermoplastic resin, with grade UL94 V0 at 1.5mm flame retardency
Finish - High gloss
IDC Labels - Individual colour coded to T568B
IDC Blocks - 4 way industry standard IDC blocks Conforms to - ANSI/TIA-568-C Category 6 Specification
1.7 Patch Cord,Cat6A,UTP,24awg,Grey,LSZH ,2m
Conductor Metal: Bare Copper - Type: CAT6A 4-Pair S/FTP - Conductor: 26 AWG Stranded Bare Copper - Connectors: RJ45 - Wiring Standard: 568B
- OD: 6.0 ± 0.3 mm (.24in ± .01in)
- Contact Plating: 50 micron Gold-Plated
- Jacket Material: PVC
• Color Code: Gray
• Conductor: 23 AWG(0.574 ±0.007mm), Multicores (Solid)
• Insulation Material: Foam-PE, OD: 1.30 ±0.10mm, Average Thickness: 0.23 mm
• Jacket Material: LSZH (IEC 60332-1)
Average Thickness: 0.55mm nominal
1.80 Solid cable,Cat6A UTP,4pa r,23awg,Frpvc,305m,Grey PVC Jacket
Braided around all cable pairs Foil shielded cable pairs Wire insulation 26 AWG stranded copper conductors
6 nos 80 480
6 nos 420 2520
300 m 40 12000
Detailed Project Report
215
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
19 Legrand Valrack 18U/600W/600D integrated side panel Loading capacity 1670 lbs 19" Sever/ Networking Rack Cabinet (600*800*18U)
Material SPCC cold rolled steel 23.62(W) x 31.5(D) x 49(H) inch Internal depth 31 inches mounting profile 2.0mm,mounting angle 1.5mm, others 1.2mm Degree of protection
IP20 Degreasing, pickling, phosphoric, powder coated Universal Rack Accessories Sidewalls, Split rear doors
Baying Kits, toolless Shelves, casters, Bolt Down Kits, Cable Management Power Strips –vertical or Rackmount, Enclosure Monitoring System Toolless Blanking Panels, Fans
2 COMPUTERS AND PRINTERS
2.1 Desktop 8th Generation Intel® Core™ i5 processor 1 TB 7200 rpm SATA 8 GB DDR4-2400 SDRAM (1 x 8 GB)
Intel® HD Graphics 630
1 nos 21000 21000
5 nos 48000 240000
2.2 15-cc130tx 2017 15.6-inch Laptop (Core i5/8GB/1TB/Windows 10/2GB Graphics), 1 nos 85000 85000
2.3 Print Method:
On-demand inkjet (Piezoelectric)
Maximum Print Resolution: 5760 x 1440 dpi (with Variable-Sized Droplet Technology)
Minimum Ink Droplet Volume: 1.5 pl
Automatic Duplex Printing: No
Control Panel: 2.7” TFT Colour LCD Epson-L850-Photo-All-in-One-Ink-Tank-Printer
2.4 LED Display: 21” TFT LED
Active Area: 376 (H) x 301 (V) mm
Screen Resolution: 1280 x 1024 Display colour: 16.7M
Contrast Ratio: 1000:1 Brightness: 225 nits
Response Time: 14ms
Viewing Angle: 178° (H) x 178°(V) , Height: 1320mm Width: 525mm Body Depth: 182mm
3 SOFTWARES
2 nos 18000 36000
5 nos 15000 75000
216
Resul Pookutty Foundation
3.1
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Allowance for Hospital Management softwares like Services Management Patient Management OPD Management
IPD Management etc
4 TELEPHONE
4.1
EPABX controller with16 line extension and Operator console of ✓ 6 lines Tiltable graphical display monochrome, backlit ✓ Hands- Free (Full Duplex) ✓ Optical call alert ✓ 8 fixed function keys ✓ 6 freely programmable touch sensor keys ✓ Control Keys +/- ✓ 5 way Navigator ✓ Head set Jack ✓ USB port ✓ Wall Mountable
1 LS 125000 125000
1 nos 40000 40000
4.2
Extension phone sets Phone The Cisco phone 8845 offers a 5-in. high-resolution (800 x 480) widescreen VGA backlit color display. Localized language support, including right-to-left onscreen text, meets the needs of global users.
4.3 PatchPanel 19" 1U 24 ports RJ-45 signs 4 y 5 with RJ21 end24 x RJ45 ports wired to single RJ21 female
• Premium black brushed aluminium panel supplied with matching cage nut set
• Labelling and cable retention facility
• Fully enclosed to protect PCB
• Suitable for use with Cisco VG224 Voice Gateway
• 2 x RJ21 female and 4 x RJ21 (Cat 5e) versions also available
• Compatible RJ21 cables also available in a variety of lengths
4.4 Patch cable 0.4 mm diameter (nom.) & 0.5 mm diameter (nom.) High density polyethylene,Insulation Thickness (Average) 0.17 mm ,0.20 mm
4.5
Standard Wall Mount Rack / Cabinet / Enclosure – 4U, 19″ (W600 x D450 x H501mm)
SWM6409. Compliance: Comply with ANSI/ EIA RS-310-D, DIN414197 part 1, IEC297-2, DIN41494 part 7, GB/T3047.2-92 standard.
Universal Rack Accessories Sidewalls, Split rear doors Baying Kits, toolless Shelves, casters, Bolt Down Kits, Cable Management Power Strips –vertical or Rackmount, Enclosure Monitoring System Toolless Blanking Panels, Fans
Resul Pookutty Foundation
6 nos 1500 9000
1 nos 9000 9000
750 m 20 15000
1 nos 7500 7500
217
5 CCTV
5.1
2 Megapixel CMOS Vandal-proof Network
Dome Camera ,1/2.8" Progressive Scan CMOS,1920 x 1080 ,Local storage: Built-in Micro SD/SDHC/SDXC card slot, up to 128 GB.
NAS (Support NFS,SMB/CIFS),ONVIF, PSIA, CGI, ISAPI
5 nos 5300 26500
5.2
2 Megapixel CMOS Vandal-proof Network
Bullet Camera ,1/2.8" Progressive Scan CMOS,1920 x 1080 ,Local storage: Built-in Micro SD/SDHC/SDXC card slot, up to 128 GB.
NAS (Support NFS,SMB/CIFS),ONVIF, PSIA, CGI, ISAPI
4 nos 5500 22000
5.3
NVR Ip Video Inputs : 12 channel
1-ch, resolution: 1920 × 1080P /60Hz, 1600 × 1200 /60Hz, 1280 × 1024 /60Hz, 1280 × 720 /60Hz, 1024 × 768 /60Hz
4 SATA interfaces for 2 HDDs + 1 DVD-R/W (default), or 4HDDs
Up to 6TB capacity for each HDD
1 nos 12000 12000
5.4
Cisco SG350 28P -K9 28 Port Gigabit PoE (Power Over) Switch 8 x 10Base-T/100Base-TX - RJ-45 - PoE; 1 x console - 9 pin D-Sub (DB-9) - management;2 x 10Base-T/100BaseTX/1000Base-T - RJ-45 / SFP (combo)
Ports : 12-port Gigabit + 2 x combo Gigabit SFP
5.5 Patch Panel,12Port,Cat6a,UTP,90 degree 1U of an EIA-standard 19-inch rack , Mounting hardware for wall-mount,Heavy-duty 14 ga cold-rolled steel construction,a tray at the rear of the panel.24PORT CAT6A Patch Panel
5.6
Shielded Rackmount Loaded 568A/568B
Keystone,Cat6A UTP,Black,Toolless Type RJ45
Jack Housing: ABS + PC, UL 94-V0
Contact Bracket: PC, UL 94-V2, transparent Color
RJ45 Contact Material: Phosphor Bronze with Nickel Plating
Finish: 50 Micro-inch Gold Plated
1 nos 24000 24000
1 nos 7500 7500
12 nos 80 960
218
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
Sub Centre – Yeroor Grama Panchayath
5.7
Faceplate,Single Port,Mudu lar Straight Shutter(2-Piece) Width - 25mm Depth - 21mm Height - 50mm Back-box Depth - Minimum 15mm recommended
Material - Polycarbonate/ABS thermoplastic resin, with grade UL94 V0 at 1.5mm flame retardency
Finish - High gloss
IDC Labels - Individual colour coded to T568B
IDC Blocks - 4 way industry standard IDC blocks Conforms to - ANSI/TIA-568-C Category 6 Specification
5.9 Patch Cord,Cat6A,UTP,24awg,Grey,LSZH ,2m
Conductor Metal: Bare Copper - Type: CAT6A 4-Pair S/FTP
- Conductor: 26 AWG Stranded Bare Copper - Connectors: RJ45
- Wiring Standard: 568B - OD: 6.0 ± 0.3 mm (.24in ± .01in)
- Contact Plating: 50 micron Gold-Plated
- Jacket Material: PVC
• Color Code: Gray
• Conductor: 23 AWG(0.574 ±0.007mm), Multicores (Solid)
• Insulation Material: Foam-PE, OD: 1.30 ±0.10mm, Average Thickness: 0.23 mm
• Jacket Material: LSZH (IEC 60332-1) Average Thickness: 0.55mm nominal
5.10 Standard Wall Mount Rack / Cabinet / Enclosure – 2U, . Compliance: Comply with ANSI/ EIA RS-310-D, DIN414197 part 1, IEC2972, DIN41494 part 7, GB/T3047.2-92 standard.
Universal Rack Accessories Sidewalls, Split rear doors Baying Kits, toolless Shelves, casters, Bolt Down Kits, Cable Management Power Strips –vertical or Rackmount, Enclosure Monitoring System Toolless Blanking Panels, Fans
5.11 cat 6a UTP cabling and connectivity components support 10 Gigabit , STP cabling systems are a viable alternative for running 10 Gig over copper
12 nos 80 960
12 nos 200 2400
1 No. 2500 2500
480 m 60 28800
Standard Model Numbers :ST6000VX0001- 6TB HDD 1 No. 17000 17000 6
5.12
PUBLIC ADDRESS SYSTEM
Detailed Project Report
219
Resul Pookutty Foundation
6.1 Call Station - 2 x status LEDs
• PTT key
• 2 x zone selection keys
• 2 x zone selection LEDs
• DIP switches
6.2
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
1 No. 12000 12000
6.3
• Rotary volume control Modern two-zone call station for the PLE series Selectable gain Speech filter and limiter Output level control
Loop-through option for up to 8 call stationsAHUJA (CCS-2200) COUNTER
COMMUNICATION SYSTEM
Mixer Amplifier- 2 microphone/line inputs, plus 2 music source inputs
100 V and telephone input with priority & VOX Announcement only output, 3-wire volume overrideVoice-activated emergency override Wide range of power (30, 60 and 120 Watts)
Power Amplifier-120 and 240 W power amplifier in a compact housing
1 V line level balanced input 70 V, 100 V and 4 ohm outputs 100 V input for slave operation on 100 V speaker line
Temperature-controlled forced front to back ventilation (directly stackable)
24 VDC backup power with built in charger
6.4 Loud Speaker - High output true compression driver for wide dispersion and superior coverage control out to 10 kHz
Long throw 8-inch (200 mm) woofer housed in a large vented 14 gauge steel enclosure for extended LF performance down to 40 Hz 200 watt power handling provides for 114 dB maximum SPL
Front baffle transformer tap adjustment switch Includes tile rails and “C” mounting ring
6.6 High end digital cable - high performance standard and bi-wire speaker cables
7 TELEVISION AND DVD
7.1
SMART TV- Display Type: LED, Screen Size:55 inches,Connectivity: HDMI,USB ,Resolution: 1366x768
Wallmountable -Samsung 138 cm (55 inches)
4K Ultra HD Smart LED TV UA55TU8000KXXL
Resul Pookutty Foundation
1 No. 22000 22000
1 no. 28000 28000
5 nos 2100 10500
170 m 120 20400
1 Nos 70000 70000
220
7.2
SMART TV- Display Type: LED, Screen Size:32 inches,Connectivity: HDMI,USB ,Resolution: 1366x768
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
1 No. 20000 20000
Wallmountable -Samsung 80 cm (32 Inches) Wondertainment Series HD Ready LED Smart TV UA32T4340AKXXL
7.3 Upscales DVDs to near-HD quality on HDTVs that offer 1080p resolution (requires HDMI cable, sold separately)
7.4 Active optical cable locates an ultra-HD 4K x 2K 60Hz 4:4:4 HDMI display up to 100 meters (328 feet) from a video source. High speed and long distance transmission by optical system up to 100 meters
7.5 Standard Wall Mount Rack / Cabinet / Enclosure – 2U, 40x40x15 cm Compliance: Comply with ANSI/ EIA RS-310-D, DIN414197 part 1, IEC297-2, DIN41494 part 7, GB/T3047.292 standard. Universal Rack Accessories Sidewalls, Split rear doors Baying Kits, toolless Shelves, casters, Bolt Down Kits, Cable Management Power Strips – vertical or Rackmount, Enclosure Monitoring System Toolless Blanking Panels, Fans
7.6 White board in Conference room Wall mounted Type 6 ft x 4 ft for writing .
8 QUEUE MANAGEMENT SYSTEM
8.1 QUEUE management software shall provide with the options to select the type of service to select.Once the service type is selected, the system will calculate the number of persons waiting in the queue and their expected service time and will generate a token.The customer service officer will get the list of pending customers waiting in their group at his workstation with the description. They will pick the customer in a predefined order and as soon as they serve the current customer, the system will display and announce with voice prompt the token number of next customer who is supposed to be served. The center supervisor will be able to monitor the queue status from his/ her desktop online. The management will get the data and summary of
1 No. 8500 8500
155 No. 60 9300
1 No. 2500 2500
1 No. 4500 4500
1 LS 60000 60000
221
Resul Pookutty Foundation
information about the number of customers and service matrix, time, and other special reports. The components of the system shall include the Token Issuer, Software for handling the queue for various services, Diplay of list on a LED TV currently serving for various services along with announcements. Scope of the contractor shall include supply, installation, testing and commissioning of the complete system
9 Nurse Calling System
Supply, Installation, Testing and commissioning of Nurse call system including, Nurse station control unit, bedside call button and reset button and toilet button, with all necessary wiring and accessories to complete the system.
9.1 LCD console (Master unit)
-The LCD console must be a self-contained small-sized unit. On the console, LCD display with easy-to-read 5 lines / 80 letters backlight.
-The system shall display the called room number / bed number with the beep sound/alerting call.
-In the console, up to 4 incoming calls may be displayed individually.The console can be mounted on a desk or wall.You need to use a modular quick disconnect connector for the console. You must be able to remove and replace the console without turning off.
-In the idle state, the time shall displayed on the console. The time shall be The time format and time display must be consistent throughout the system.
Calling unit and Reset facility shal be provided at the Bed unit(2 Nos) and Toilet pull chord shall be provided(1 No.) in the care giving room
1 LS 45000 45000
TOTAL 12,87,340
222
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
Detailed Project Report Sub Centre – Yeroor Grama Panchayath 223 Resul Pookutty Foundation 6.7 BOQ & Cost Estimates – Waste Management Facilities ANNEXURE IX Waste Management - BOQ Sl. No. Description Qty Unit Unit Rate Amount 1 Medical Waste Incinerator D-20 Model - D-Type- Electric Operated 1 Nos
TOTAL 250,000 6.8 BOQ & Cost Estimates – Furniture & Fixtures
VII Furniture - BOQ Sl. No. Description Qty Unit Unit Rate Amount 1 ASHA ROOM 1.1 Chair 4 Nos 2100
1.2 Work Table 4 Nos
1.3 Storage Cabinet 4 Nos
2 CONFERENCE ROOM 2.1 White board 1 Nos 500.00
2.2 Work Table 1 Nos
2.3 Executive Chairs 2 Nos 6,500.00
2.4 Chair 4 Nos
2.5 Yoga Mat 10 Nos
3 DINING AREA 3.1 Dining Table 1 Nos 6,000.00 6000 3.2 Chair 5 Nos 2100
3.3 Microwave Oven 1 Nos 5,000.00 5000 4 DOCTORS ROOM 4.1 Chair 3 Nos 2100
4.2 Work Table 1 Nos
5 FEEDING ROOM
250000 250000
ANNEXURE
8400
4900 19600
11000 44000
500
4900 4900
13000
2100 8400
500.00 5000
10500
6300
4900 4900
Sub Centre – Yeroor Grama Panchayath
5.1 Wall mounted nappy changing table 1 Nos 4000 4000
5.2 Chair 2 Nos 2100 4200
6 INJECTION ROOM
6.1 Chair 3 Nos 2100 6300 6.2 Work Table 1 Nos 4900 4900
7 IT ROOM
7.1 Chair 1 Nos 2100 2100 7.2 Work Table 1 Nos 4900 4900
8 JHI ROOM
8.1 Chair 3 Nos 2100 6300 8.2 Work Table 1 Nos 4900 4900
9 JPHN ROOM
9.1 Chair 3 Nos 2100 6300 9.2 Work Table 1 Nos 4900 4900
10 PHARMACY
10.1 Chair 1 Nos 2100 2100 10.2 Work Table 1 Nos 4900 4900 10.3 Pharmacy Rack 140 Nos 1000 140000 10.4 Bins 12 Nos 500 6000 11 RECEPTION 11.1 Reception table 1 Nos 20000 20000 11.2 Tall Chair 1 Nos 2100 2100 11.3 Q Manager 4 Nos 6500 26000 TOTAL 3,86,400
Resul Pookutty Foundation
Detailed Project Report
224
6.9 BOQ & Cost Estimates – Medical Equipment ANNEXURE VIII Medical Equipment- BOQ Sl. No. Description Qty Unit Unit Rate Amount 1 CARE GIVING ROOM
Patient bed with mattress & side table
1.1
2 45000 90000
Sub Centre – Yeroor Grama Panchayath
1.2 Wall mounted spot light 2 4500 9000 1.3 Instrument Trolley 1 15000 15000 1.4 Clinical Ear Thermometer 1 1500 1500 1.5 IV Stand with wheels 2 1500 3000 1.6 Sphygmomanometer Aneroid 300 mm with cuff 1 2500 2500 1.7 Stethoscope 1 1500 1500 1.8 Sponge holder 1 1000 1000 1.9 Forceps 1 800 800 1.10 Nebuliser 1 3500 3500 1.11 Steam Inhaler 1 800 800
2 DOCTOR
ROOM
2.1 Instrument Trolley 1 15000 15000 2.2 Kidney Tray Big 1 1000 1000 2.3 Kidney Tray Small 1 800 800 2.4 Torch 1 400 400 2.5 Weighing Scale-Adult/Paediatric 1 1500 1500 2.6 Weighing Scale-Infant 1 5500 5500 2.7 Tray Instrument/Dressing with cover 1 2500 2500 2.8 Sphygmomanometer Aneroid 300 mm with cuff 1 2500 2500 2.9 Stethoscope 1 1500 1500 2.10 Clinical Ear Thermometer 1 1500 1500 2.11 Stature Meter for Adult 1 500 500 2.12 X-ray view box (LED) 1 15000 15000 2.13 Foetal Doppler 1 8500 8500 2.14 Scissors surgical straight 140mm 1 1500 1500
Resul Pookutty Foundation
Detailed Project Report
225
Sub Centre – Yeroor Grama Panchayath
2.15 Sponge holder 1 1000 1000 2.16 Forceps 1 800 800
4 INJECTION ROOM
4.1 Examination Couch with underneath storage & integrated foot stool 1 45000 45000 4.2 Instrument Trolley 1 15000 15000 4.3 Kidney Tray Big 1 1000 1000 4.4 Kidney Tray Small 1 800 800 4.5 Torch 1 400 400 4.6 Jar Dressing with Cover 1 2500 2500 4.7 Instrument Steriliser 1 8500 8500 4.8 Weighing Scale-Adult/Paediatric 1 1500 1500 4.9 Weighing Scale-Infant 1 5500 5500 4.10 Tray Instrument/Dressing with cover 1 2500 2500 4.11 Sphygmomanometer Aneroid 300 mm with cuff 1 2500 2500 4.12 Stethoscope 1 1500 1500 4.13 Clinical Ear Thermometer 1 1500 1500 4.14 Stature Meter for Adult 1 500 500 4.15 Vaccine Carrier box 1 2500 2500 4.16 Sponge holder 1 1000 1000 4.17 Forceps 1 800 800 4.18 Needle Destroyer 1 3000 3000
5 JHI ROOM
5.1 Sphygmomanometer Aneroid 300 mm with cuff 1 2500 2500 5.2 Stethoscope 1 1500 1500
6 JPHN ROOM
6.1 Examination Couch with underneath storage & integrated foot stool 1 45000 45000
Resul Pookutty Foundation
Detailed Project Report
226
Report
227
Detailed Project
Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation 6.2 Instrument Trolley 1 15000 15000 6.3 Kidney Tray Big 2 1000 2000 6.4 Kidney Tray Small 2 800 1600 6.5 Torch 1 400 400 6.6 Instrument Steriliser 1 8500 8500 6.7 Weighing Scale-Adult/Paediatric 1 1500 1500 6.8 Weighing Scale-Infant 1 5500 5500 6.9 Tray Instrument/Dressing with cover 1 2500 2500 6.10 Sphygmomanometer Aneroid 300 mm with cuff 1 2500 2500 6.11 Stethoscope 1 1500 1500 6.12 Clinical Ear Thermometer 1 1500 1500 6.13 Stature Meter for Adult 1 500 500 6.14 Mobile LED Examination Light 1 25000 25000 6.15 Scissors surgical straight 140mm 2 1500 3000 6.16 Sponge holder 2 1000 2000 6.17 Forceps 2 800 1600 6.18 Jar Dressing with Cover 1 2500 2500 6.19 Single basin with movable stand 1 2500 2500 6.20 Forceps sterilizer 2 1200 2400 6.21 SIMS Uterine Depressor/Retractor 2 1200 2400 6.22 Forceps haemostat straight Kelly 140mm 2 800 1600 6.23 Forceps uterine vulsellum curved 25.5 cm 2 1400 2800 6.24 Speculum vaginal bi-valve Cusco's/Graves medium 2 1400 2800 6.25 Speculum vaginal double ended Sims ISS Medium 2 1400 2800
Detailed Project Report Sub Centre – Yeroor Grama Panchayath 228 Resul Pookutty Foundation 6.26 Scissors, cord cutting 2 800 1600 6.27 Forceps, utility sterilising, cheattle, 11 ½” 2 1000 2000 6.28 Sound uterine (Simpson), calibrated in cm, 12 ½” 2 1200 2400 7 PHARMACY 7.1 Pharmacy Refrigerator 1 50000 50000 8 E-HEALTH 8.1 Examination Couch with underneath storage & integrated foot stool Medical 1 45000 45000 8.2 Instrument Trolley Medical 1 15000 15000 8.3 E Health System Medical 1 600000 600000 8.4 E Health System Implementation, Training, Medical 1 50000 50000 8.5 E Health System Software, Analytics & Cloud Services per year Medical 1 170000 170000 13,63,500.00 6.10 Projections of Preliminary Expenses ANNEXURE X Preliminary Expenditure Sl. No. Description Period Amount 1 Consulting fee for MEP Engineer, Architect, Draftsman and Civil Engineer 01-07-2020 to 30-11-2020 887224 2 Transportation Expense of Cochin, Kollam & Trivandrum 13-07-2020 to 10-11-2020 186500 3 Site Visit Expense 17-07-2020 to 04-12-2020 45000 4 DPR Costing for Subcentre 21-08-2020 to 10-12-2020 80000 5 DPR Costing for PHC 21-08-2020 to 10-12-2020 145000 6 Topography survey 13-09-2020 to 07-10-2020 6550 7 Water, Air, Noise Test 02-12-2020 to 08-12-2020 14210 8 Soil Investigation 02-12-2020 to 08-12-2020 32140 9 Market Research 02-12-2020 to 08-12-2020 125000 10 Miscellaneous Expenses 01-07-2020 to 30-11-2020 75000 TOTAL 15,96,624
6.11 Analysis of Rates
The detailed cost estimates have been prepared based on the Bill of Quantity (BOQ) arrived through the technical design and the rates taken from multiple sources. Rates have been taken from Delhi Schedule of Rates (DSR) 2018 wherever possible. Competitive quotes have been taken to ascertain the rates to be factored in the DPR, wherever DSR rates are not available or found inadequate. A standard 10% provision has been created on the overall project cost to accommodate the quantity variance and rate variance factors. Preliminary expenses has been estimated based on the quotes from service providers. A provision of 5% Project Management Charges also included in the costing with an estimate from renowned PMC companies.
6.12 Summary of Cost Estimates
By summarizing project component-wise BOQ and Estimates, a total cost of INR 293.64 Lakhs is estimated for establishing the Sub Centre at Yeroor. The project component-wise estimates are given below.
Resul Pookutty Foundation
229
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
I BUILDING & CIVIL WORKS
II ELECTRICAL
III AIRCONDITIONING
IV LOW VOLTAGE SYSTEM
V PLUMBING 17,07,481 VI FIRE & SAFETY 15,999 VII FURNITURE 3,86,400 VIII MEDICAL EQUIPMENTS 13,63,500 IX WASTE MANAGEMENT 2,50,000 X PRELIMINARY EXPENDITURE 15,96,624 XI CONTINGENCY 24,60,313 XII Project Management Cost 18,50,441 TOTAL 2,49,80,965
Sl. No Project Component INR Lakhs
1,22,19,885
14,03,182
4,39,800
12,87,340
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
The proposed total outlay will be funded by Resul Pookutty Foundation. In the event of any escalation to this cost beyond the estimates due to price hike/inflation, the same also will be funded by RPF. Apart from the Capital Expenditure, RPF will also be funding the Repairs and Maintenance of the facility, Coordinating and funding for the Public Relation of the Sub Centre for a period of 2 years. The recurring cost proposed to be incurred during the first two years of operation including the project management fee are estimated as under.
YEROOR SUB CENTRE - MAINTENANCE & PUBLIC RELEATION COST
Sl. No. Particulars Year 1 Year 2 Total
1 Repairs & Maintenance of the Facility 813,629 894,992 1,708,622 2 Public Relation Expenses 500,000 500,000 10,00,000 Media Cost 500,000 400,000 900,000 Creative Agency Fees 240,000 264,000 504,000 Event Management 150,000 120,000 270,000 3 Project Management Cost 925,220 925,220 1850441 Total Operating Cost funded by RPF 31,28,849 31,04,212 62,33,061
Considering the Capital Investment and Recurring Cost to be incurred by RPF, the total Project Cost for Resul Pookutty Foundation is estimated as below. The cost of operation by the Govt. is not factored here as the same has to be funded from Govt. Plan budget.
YEROOR SUB CENTRE - APPLICATION OF FUNDS
Sl. No Application Funding During Project Year 1 Year 2 1 Cost to Establish the Facility 23,130,524 2 R&M of Facility 813,629 894,992 3 PR Expenses 13,37,000 13,37,000 4 Project Management Cost 925220 925220 23,130,524 30,75,849 30,79,849 Grand Total 29,363,585
Resul Pookutty Foundation
230
INR INR INR
INR
7. Project Management
7.1 Project Management Organisation & Quality Management
RPF will be deploying a robust Project Management Methodology to ensure efficiency and effectiveness of the project execution. RPF’s project management methodology will ensure professionalism in planning, control and coordination of the project from conception to completion. It will work towards the goals in terms of utility, function, quality, time and cost, and the establishment of relationships between resources. The project management wing of RPF will be in charge of the overall planning, coordination and control of a project from inception to completion aimed at producing a functionally and financially viable project that will be completed on time within authorized cost and to the required quality standards.
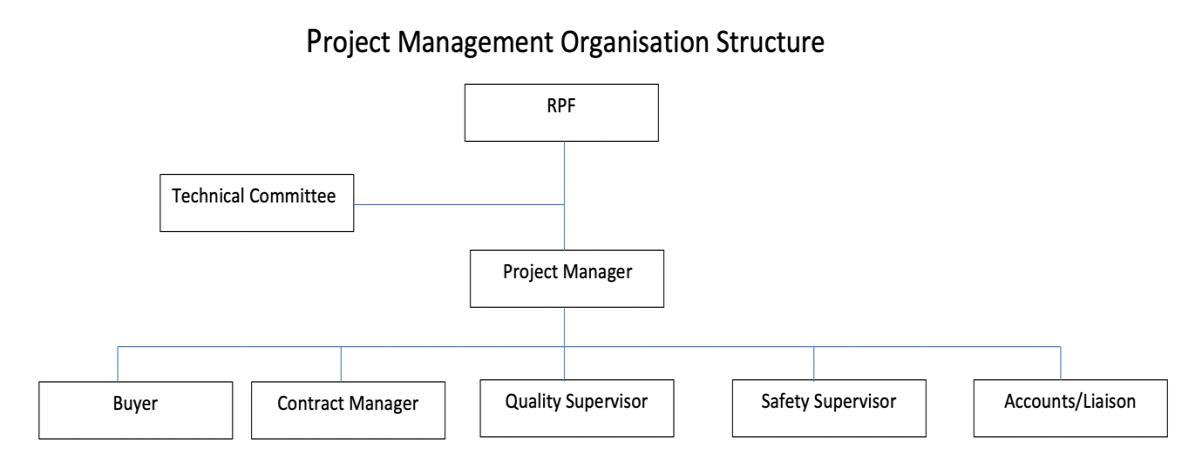
The PMC division of RPF will be the agency coordinating and communicating with different agencies and stakeholders in the project during the lifecycle of the project. The functions of PMC division shall include designing a master project plan, preparation of RFQ, managing the contractor appointment process, monitoring the construction progress and ensuring construction quality and documentation of the project. The PMC division shall also ensure the compliance with different laws and regulations applicable to the project at different phases of construction and commissioning.
The structure of the PMC division of RPF is given below.
231
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
A Technical Committee will formed with experts in the field of construction and healthcare infrastructure as an advisory team for the project management division. The committee will review the project in a structured manner with focus on time, cost and quality. The Technical committee will be setting and approving standards for the materials and construction quality.
Project Manager will be the head of the PMC division of the company and be responsible for the steady progression of the project from its beginning to its completion as per the Scope, Cost and Time parameters agreed upon in the project plan.
Buyer in the PMC team shall be responsible for coordinating with the construction team and ensuring smooth supply of materials at the required timelines and as per the planned budget. Contract Manger will be in charge of the liaison and coordination with multiple contractors in the project. Contract Manger shall be coordinating for the periodic measurement of the work progress and initiation of bills for payment. The Quality supervisor will be communicating the quality standards to the concerned operations team and shall be supervising the quality on a regular online basis. Safety supervisor shall be responsible for the aspects of Health, Safety and Environment (HSE) in the project. Suitable Standard Operating Procedures on HSE shall be implemented in the project during the entire lifecycle of the project. Accounts/ Liaison team shall be handling the functions of administration, public relation and Human Resources and accounting activities connected with this project.
The PMC division will be powered with a suitable Project Management Software like Primavera or MS Projects for the efficient and automated project management. Project management software can easily compare between the planned progress of construction work and actual progress of construction in the project. Its functions include collecting, recording, monitoring, controlling and reporting information concerning project performance. Controlling and monitoring can be done through the software and the causes of delays can be find out and plan for remedial solutions. The software will facilitate seamless planning and monitoring of the project and proper documentation. It will also be used in version management of drawings and designs used during the construction phase. A suitable technology platform also will be used to manage the project communication and collaboration. These technology solutions will reduce the use of hard copy printouts and documentations to a considerable extent.
Resul Pookutty Foundation
232
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Quality management of the entire project shall be managed through the PMC software and SOPs issued for the purpose. RPF will be coming out with a Quality Manual with the details of established quality standards for performance and procedures. The Quality Manual is designed to reduce the incidence of problems related to quality and result in implementation, where necessary, of corrective actions and modification of work procedures, where necessary, to reduce the incidence of future problems. The Quality Manual will comprise of RPFs policies on Assignment of Responsibilities, Training and Development, Quality Control Review, Quality Assurance Audits, Work Process Analysis and Documentation.
The finalised and approved Standard Operating Procedures and specifications shall be made available for all concerned stakeholders of the project. The results of the QC interventions in the project, including test results shall be documented in the PMC software as proposed in the SOP. All bills of construction and supply shall be passed only with the concurrence of the Quality Supervisor. Apart from the Quality Assurance, the QC team will also ensure reduction in wastage and loss prevention in the project.
The guidelines mentioned in the Indian Public Health Standards (IPHS) for Sub-Centres released by Ministry of Health and Family Welfare shall be followed for the entire project.
7.2 Contract Management Strategy
The contract of the project execution shall be entrusted with contractors with credible track record, technical expertise and a strong financial position. The method of contract shall be decided by the technical committee of RPF. Bids for contract will be issued based on a RPQ prepared on approval of the DPR and a two packet bid system will be adopted for the project.
Financial bid will be opened only for those technical bids are shortlisted in the preliminary stage. A matrix for the evaluation of technical bid shall be finalised and the technical committee of RPF shall be deciding on the finalisation of the shortlisted technical bids. RPF will be adopting e-tendering platform of Govt. of Kerala (Subject to permission from Govt of Kerala) or similar platforms for ensuring maximum transparency in the process. The tender shall be advertised through popular newspapers on release to invite good contractors for the project. Standard Operating Procedures of Kerala State Public Works Department (PWD) shall be followed in the award and management of the contract. Procurement of Medical
Resul Pookutty Foundation
233
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Equipment’s shall be done following using the guidelines of Kerala Medical Service Corporation Limited and under their supervision. Conditions of Bank Guarantee as Performance Guarantee shall be incorporate for major contractors to ensure their commitment on the project and quality of construction.
Certain unique solutions for E-health will be considered based on the requirement of a eHealth platform which may be interlinked across the sub enters, PHC and CHC
7.3 Project Implementation Schedule
234
Resul Pookutty Foundation
101112131415 EngineeringDesign CivillWorks BuidlingConstruction PowerSupply&Distribution HVAC FireFighting Plumbing&StormWaterManagement Parking SewageTreatmentPlant SolarPowerSystem RainWaterHarvesting Landscaping InternetFacility SecuritySystem AudioVisualSystem CablingandSwitching OfficeAutomation EPABXSystem Nurse/DoctorCallingSystem WasteManagementFacilities Furniture&Fixtures StatutoryClearancesandApprovals ProjectImplementationScheduleSubCentreYeroor ProjectDurationinMonths
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
7.4 Commissioning of Project
As per the plan, the Sub-Centre will be constructed and furnished with all required furniture & medical equipment’s required for the smooth operation. Once the facilities as per the plan are ready, testing and calibration of all equipment’s shall be done to ensure proper functioning and utility as per the plans. The facilities of E-health rooms shall be tested with mock and trial sessions with the experts in the field. Proper training shall be provided to the staff members deputed by Department of Health for the continued operations of the project.
A complete set of drawings and other specific details required for the future upkeep and maintenance of the facility shall be documented in a suitable Building Information Management System and the same shall be shared with the Govt. All statutory approvals and permissions to operate shall be obtained prior to the commissioning of the project. Registration for medical waste collection by IMAGE also will be completed before commissioning of the Project.
Even after commissioning of the project, RPF will continue to take care of the periodic maintenance and upkeep of the facility for a period of 2 years.
8. Operations & Management
8.1 Hospital Management Plan Hospital Management Committee
As per the proposed plan, Resul Pookutty Foundation will be constructing the building and furnishing the building with all necessary furniture and medical equipment’s. The SCs and PHCs under this project shall be equipped with the modern facilities for e-health and telemedicine using teleconferencing and IOT Devices. As per the plan, once the hospital is ready for commissioning, the entire facility will be transferred to the Govt. of Kerala for operations. It is also proposed that Resul Pookutty Foundation will continue to coordinate and fund for the maintenance and upkeep of the facility for a period of two years from the date of dedication of facility to the nation.
Resul Pookutty Foundation
235
Once it is transferred to the Govt., it will be staffed and operated by Department of Health and Family Welfare, Govt. of Kerala under the schemes and programs applicable to PHCs and FHCs. As per the current policy the public Healthcare institutions are managed by the Hospital Management Committee.
It is proposed that this facility also shall be managed as per the guidelines given in GO (MS) No. 79/2007/LSGD. As per the GO the following will be structure of the Hospital Management Committee.
About the Hospital Management Committee & Composition
The Government have decided to constitute Hospital Management Committees for hospitals and dispensaries transferred to local government from the three streams - Allopathy, Ayurveda and Homeopathy. These Hospital Management Committees stipulated in the Kerala Panchayat Raj Act and Kerala Municipality Act would be constituted by the local government concerned and the existing Hospital Development Committees would stand dissolved from the date of registration of the new Hospital Management Committees and all the assets would be transferred to the Hospital Management Committee from that date. The Management Committee from that date. The Management Committee may start functioning forthwith with the ex-officio members.
The composition of the Hospital Management Committee would be as follows:
1. The elected head of the Local Self Government – Chairperson.
2. Chairperson of the Standing Committee in charge of public health in the Local Government – Vice Chairperson.
3. Members of the Standing Committee in charge of public health in the Local Government not exceeding five including two women – Members.
4. The elected member of the Local Government representing the area where the health institution is situated – Member.
236
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
5. Engineers of LSGD, Kerala State Electricity Board and Kerala Water Authority having jurisdiction over the area in which the health institution is situated – Member.
6. Three persons to be nominated by the Local Government having knowledge and interest in the activities of the health institution who are willing to do voluntary social service and residing in the area of the LSGI.
7. One representative each of the political parties having representation in the Assembly from the respective districts or in the respective three-tier Local Government where the health institution is situated.
8. Medical Officer in charge of the medical institution - Member, Secretary and Convener.
It is proposed that a representative of Resul Pookutty Foundation shall be part of this HMC.
The term of the Management Committee shall be coterminous with that of the elected Local Government.
The management committee shall be registered as a charitable society.
Responsibilities of the Management Committee
1. It shall be the duty of the management committee to give suggestions the Local Government and the Officers concerned to make effective, the working of the Health Institution concerned as part of the performance of the duties in respect of the public health vested in the Local Government under the Act.
2. The Management Committee shall have supervisory power over the construction works, maintenance of the buildings, vehicles and equipment, water supply, supply of electricity, sanitation, providing amenities to the patients coming for medical treatment, maternity and child care, field level health activities etc. in the Health Institution.
3. The Management Committee shall ensure compliance to minimum standards of facilities; hospital care and treatment protocols prescribed from time to time.
4. The Management Committee shall periodically review Citizens Charter of Health Institution and give suggestions to Local Governments for revision.
Resul Pookutty Foundation
237
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
5. The Management Committee shall identify problems faced by patients and citizens in the Health Institutions.
6. The Management Committee shall acquire instruments, equipment, drugs, consumables, furniture, etc., through purchase, donation or any other appropriate means.
7. The Management Committee shall institute an internal grievance redressal mechanism in the Health Institution.
8. The Management Committee shall exercise vigil to prevent malpractices in the functioning of Health Institutions.
9. The Management Committee shall ensure transparency and accountability in the functioning of the Health Institution.
10. The Management Committee shall encourage people’s participation in the functioning of the Health Institution.
11. The Management Committee shall ensure transparency in the management of funds.
12. The Management Committee shall organize outreach service, health camps.
13. The Management Committee shall facilitate scientific management of hospital waste and biomedical waste.
14. The Management Committee shall review the functioning of the Health Institution.
15. The Management Committee may cause to run canteen/fair price medical store in the institution premises.
16. The Secretary shall, if demanded by the management committee, be bound to give for inspection, any document in connection with the working of the Health Institution, kept under his custody. Provided that the Management Committee shall not have the power to demand for or to inspect any document in respect of the medical treatment of a patient or to issue directions to any Officer in respect of the treatment.
17. The Management Committee shall constitute a fund by collecting donations from the public and utilize the same for improving infrastructural facilities or standards of services delivered by the institution. Receipt shall be issued for the amount collected under Sub-rule (4) and the Secretary shall keep a written account in respect of the income and expenditure.
18. The Management Committee shall facilitate social audit of the Health Institution.
238
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Other Matters
The decision of the subjects discussed in the meeting of the Management Committee shall be taken on the basis of the option of the majority of the members present in the meeting and the Convener shall send the decision to the Local Government for information and action thereon.
There shall be Bank Account for the Management Committee which shall be opened in the nationalized bank having the Health Institution in its service area. The account shall be in the joint name of the Chairman and the Secretary and shall be operated jointly.
The Management Committee shall cause regular accounts to be maintained of all its funds and the transaction thereof.
The Accounts of the Management Committee shall be annually audited by a Chartered Accountant or any qualified person appointed by government.
8.2 Service Offerings
Following are the list of services to be provided in a Sub-Centre
● Maternal and Child Health
● Intra-natal care
● Postnatal care
● Child Health Essential
● Immunization Services: Full Immunization of all infants and children against vaccine
Indian Public Health Standards (IPHS) Guidelines for Sub-Centres 9 preventable diseases as per guidelines of Government of India
● Family Planning and Contraception
● Safe Abortion Services (MTP)
● Curative Services
● Adolescent Health Care
● School Health Services
● Control of Local Endemic Diseases
● Disease Surveillance, Integrated Disease Surveillance Project (IDSP)
Resul Pookutty Foundation
239
● Water and Sanitation
● Outreach/Field Services
● Coordination and Monitoring
● National Health Programs.
● Promotion of Medical Herbs
● Record of Vital Events
Extra services proposed 1. E-health 2. Dietician 3. Pharmacy 4. Yoga Room 5. Care Giving Room
8.3 Operations & Upkeep
Upkeep and maintenance of public infrastructure has to be taken up with equal importance of building the same. It is even more important when it comes to the case of Healthcare infrastructure. By recognizing this need, RPF is proposing to undertake the Upkeep, Repair and Maintenance of the building and facilities for a period of two years including AMC of medical equipment’s. This will set a standard practice and benchmarks for upkeep and housekeeping of the facility.
RPF provisioned as sum of Rs. 43.82 lakhs for the Upkeep, Repairs & Maintenance for a period of two years. The year-wise breakup is given below.
Year Amt. INR Year 1 21,91,311 Year 2 21,91,311 Total 43,82,622
It is expected that the expenditure will be funded by Govt. directly or through other CSR funding after 2 years on a sustainable manner.
Resul Pookutty Foundation
240
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
8.4 Waste Management
Detailed Project Report Sub Centre
– Yeroor Grama Panchayath
The Sub Centre will be following directions of the Kerala Pollution Control Board for the management of the waste generated at the facility. An incinerator of suitable capacity has been proposed to be established at the Sub Centre to burn the waste which are permitted for incineration as per the PCB norms.
Bio Medical waste generated shall be sorted at the origin itself and will be disposed through IMAGE, Palakkad. IMAGE (Indian Medical Association Goes Eco-friendly) the biomedical waste treatment and disposal project of the Indian Medical Association. IMAGE, a state-ofthe art Common Biomedical Waste Treatment and Disposal Facility at Palakkad and it was commissioned on 14th December 2003. IMAGE was conceived and launched to support healthcare providers to overcome the challenges posed by the responsibilities laid down in the Biomedical Waste (Management and Handling) Rules 1998.
8.5 Public Relations
The public health usage scenario in Kerala is quite different from the rest of the country. The low usage of public health infrastructure is not only owing to the lack of facilities, but also due to the poor perception about the quality of services. The project proposed by Resul Pookutty Foundation is not just a project with some infrastructure, rather it is envisaged to create world class facilities in the public health infrastructure space. The proposal is to create a network of Sub-Centers, PHCs and CHC within Anchal Block Panchayath Area. A sea change in a small area is planned to augment the image of public health infra and to boost the confidence among the patients and stakeholders.
In order to promote the facilities to the general public, RPF has planned a series of Public Relation (PR) activities during the first two years within the project area. The PR activities has been designed based on the findings about the public perception on existing facilities and their preferences. Following PR Activities are proposed for the project.
• PR Articles about the facility and e-health program to be published to through different offline and online medium. The strategy is to project this as a trendsetter replicable model for rest of the country to follow in terms of public health infrastructure.
241
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
• Invite the best brains in the field of medicine and healthcare for talks through video conferencing mode and facilitate their services to the patients through e-health mode.
• Series of Health Seminars and webinars with luminaries from the field of medicine, health and wellness
• Regular Yoga Sessions and open the Yoga room for public. The Sub Centre will be converted as a wellness and activity center for every people in the project area who want to lead a healthy lifestyle. The idea is to build a community around the Subcenter.
• School Outreach programs and invite students to the facility for seminars
• Social Media Content Marketing and active presence in social media for announcements of programs and events.
• Promote Blogs and advocacy campaigns by opinion makers in social media
• Creating a video on facility which can go viral
• Inviting delegates and international missions from all over the world to study about this initiative and project this as a replicable model.
All these activities will be synchronized for the entire network of SCs, PHCs in the Project area. It is considered that an intense PR campaign for a period of two years will help to gain the momentum for the project and the public confidence will achieve a sustainable level.
By recognizing the need for gaining public confidence for the success of this project, Resul Pookutty Foundation will steer the promotion and public relation activities for the Sub-center. The budget requirement for the PR activities shall be funded by RPF for a period of two years.
8.6 Pharmacy Operations
There is no pharmacy according to IPHS in subcentres. We are providing a pharmacy space in our building. This to be consulted with govt. for running Karunya medical shops which is under the Kerala State Medical Services Corporation Ltd (KSMSCL).
Resul Pookutty Foundation
242
Detailed Project Report Sub
243
Drugs
1. Oral
2. Iron
3. Folic
Tablets IP 4. Iron
5. Trimethoprim
6. GV Crystals (Methylrosanilinium
7. Zinc
Dispersible
8. Iron & Folic Acid Syrup
per standards provided) 9. Water – Miscible Vitamin Concentrate IP (Vitamin
Syrup) 10. Methylergometrine Tablets IP 11. Paracetamol Tablets IP 12. Methylergometrine Injection IP 13. Albendazole Tablets IP 14. Dicyclomine Tablets IP 15. Chloramphenicol
IP 16. Povidone
USP 17. Cotton Bandage 18. Absorbent Cotton IP 19. Inj. Gentamycin 20. Inj. Magnesium Sulphate 21. Inj. Oxytocin Cap. 22. Ampicillin Tab. 23. Metronidazole Tab. 24. Misoprostol 200 mg 25. . BCG, DPT, OPV, Measles, TT, Hepatitis B, JE 26. any other vaccines as per Immunization Schedule and campaign vaccines
any) 27. Syrup Cotrimoxazole 28. Tab. Cotrimoxazole
adults) 29. Syrup Paracetamol 30. Tab. Albendazole 400 mg
Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation 8.7 Drug Situations Suggested List of
as per IPHS standard:
Rehydration Salts IP
& Folic Acid Tablets (IFA) – large (as per the standards provided)
Acid
& Folic Acid Tablets (IFA) – small (as per the standards provided)
& Sulphamethoxazole Tablets IP (Paediatric)
Chloride BP)
Sulphate
Tablets USP
(as
A
Eye Ointment
Iodine Ointment
(if
80+400 mg (for
Project Report
244
31. Adhesive
32. Savlon
33. Betadine
34. Clove
35. Gum
36.
37.
38.
39.
40.
41.
42. Condoms
43. Oral
3.
44. Emergency contraceptive
45. Disposable
46. Tab.
47. Tab.
48. Tab
49. Syrup
50. ORS Packets 51. Tab.
52. Tab.
53. Povidone
tube 54. GV Paint 55. Cotton Absorbent roll of
gms 56. Bandages,
57. Tab. Chloroquine 58. Condoms 59. Oral Contraceptive Pills 60. Emergency Contraceptive Pills
Detailed
Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
tape (leucoplast & Micropore)
solution (Anti-septic Solution)
solution (Povidone Iodine solution 5%)
oil
paints
Tab. and syrup Chloroquine for treatment of P. vivax and A.C.T Blister pack for treatment of P.F. cases.
Tab. Primaquine (2.5 mg and 7.5 mg).
Tab. DEC (Di Ethyl Carbamazine – only in filaria endemic areas)
Anti-leprosy drugs (MDT Blister Packs) for patients under treatment.
Rapid Diagnostic Kits for Malaria under National Vector Borne Disease Control Programme.
Anti-tuberculosis drugs as supplied under RNTCP (only in DOT centres).
(Nirodh)
pills
Copper – T (380-A)
pills
Delivery Kit for Clean deliveries at Home
Iron
Folic Acid
Punarvadu Mandur (ISM Preparation of Iron)
Iron
Paracetamol
Dicyclomine
Iodine Ointment 5%
500
4cmx4meters
8.8 Manpower Matrix
Type of sub centre Sub - centre B (MCH Sub - centre)
Staff Essential Desirable
ANM/Health Worker (Female) 2
Health Worker (Male) 2
Staff Nurse (or ANM, if Staff Nurse is not available) 1** Safai-Karamchari* 1 (Full time)
9.0 Project Impact Assessment
9.1 Benefits envisaged from the Project
The proposed project of upgradation of Healthcare Delivery systems is aimed at creating far reaching impacts and positive changes in the Public Health Systems of the country. Following are the expected benefits from the project for different stakeholders.
• Create a Benchmark facility and thereby enhance the minimum standards for public health infrastructure.
• Provide a world class facility to the patients which is at par of better than private healthcare infrastructure and thereby instill confidence among the public to use the Govt. facilities for treatments.
• Facilitate the focus shift from curative models to preventive and promotive models of healthcare
• Promote the multi-tier system of Healthcare Delivery for better adoption
• Facilitate savings in healthcare costs for the public by adoption of this facility.
• Promotion of healthcare schemes and programs Govt. like Ayushman Bharat, Janani Suraksha Yojana, Janani Shishu Suraksha Karyakram.
Report
Panchayath 245
Detailed Project
Sub Centre – Yeroor Grama
Resul Pookutty Foundation
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
• Effective facilitation of National Health Communicable Disease Programs and NonCommunicable Disease programs.
• Uphold acceptable quality of healthcare services and educate the public about the same through Citizen Charters.
• Improved awareness among the public on disease prevention, healthy lifestyle and wellness practices through seminars, webinars and community outreach programs.
• Achieve better community involvement of through the facilities such as Yoga Centers and seminar halls
• Introduce advanced technology solutions for healthcare and facilitate faster and efficient technology adoption for healthcare.
• Create a better work environment for the doctors and healthcare workers and attract more talent to the public health activities
• Create a model for Corporate Social Responsibility (CSR) projects which can be adopted by companies which are mandated for CSR spending as per the Companies Act.
• Improve community involvement in the promotion of public health services
• Promote Govt. of Kerala’s Campaign – “Our Health, Our Responsibility”
• Conduct effective IEC/BCC Activities and achieve huge beneficiary improvement in the following 100 areas proposed by Department of Health, Govt. of Kerala ✓ Population enumeration to happen in all operational Health and wellness centres ✓ Population based screening
Health promotion and NCD awareness activities
Promotion of physical activities
Diet modification
Other lifestyle modifications
Defaulter tracking and ensuring treatment ✓ Support groups for physical activity promotion, rehabilitation( counselling) ✓ Creating spaces for physical activity, Yoga, sports and outdoor games, exercise etc in association with LSGD/other agencies
Resul Pookutty Foundation
246
✓
✓
✓
✓
✓
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
✓ School and workplace interventions ( nurses outreach)Screening for mental illness using screening questionnaires as per “sampoornamanasikarogyam”/ “AASWAS”/ “Ammamanasu” guidelines and referral
✓ Ensuring treatment compliance and follow up of patients with mental disorders.
✓ Defaulter tracking
✓ Facilitate access to support groups.
✓ Vulnerability mapping, identification, mobilisation, treatment compliance follow up and referral of COPD/Asthma cases to FHC
✓ Tobacco cessation activities and COTPA
✓ IEC/BCC activities at community and schools level for primary and secondary prevention
✓ Identify and inform symptomatic cases to nearest health worker and facilitate medical care
✓ Active case search/ survey during an outbreak.
✓ Suchitwa mapping and hot spots identification
✓ Linkage with WHSNC, LSG, other line departments, NGOs and Harithakeralammission to address social determinants of health.
✓ Awareness on airborne infections, cough hygiene and hand washing, need for isolation.
✓ Immunisation
✓ High risk screening,
✓ Sanitary survey of drinking water sources and ensuring chlorination
✓ Periodic water quality monitoring.
✓ Maintaining ORS Depot
✓ Activities in connection with enforcement of public health and food safety laws
✓ Integrated Vector Management activities
✓ Migrant screening
✓ Active blood smear collection for detection of Malaria &Filaria.
✓ Mass and contact survey of malaria cases.
✓ Morbidity management of lymphatic filariasis
✓ MDA -TAS activities
Resul Pookutty Foundation
247
Sub Centre – Yeroor Grama Panchayath
✓ Doxy prophylaxis for high risk groups (handling domestic animals, fishing, farming etc)
Rodent control activities ✓ Identification, mobilisation and screening of individuals with hypo/erythematous patches and other symptoms suggestive of leprosy ( Aswamedham )
Periodic screening of school children and migrants
Mobilisation of close contacts of leprosy patients for screening
Ensuring treatment compliance in leprosy
Vulnerable population mapping
Identification of cases with cough more than two weeks/weight loss/ prolonged unexplained fever and referral to FHC for Sputum AFB
Identify and train DOTS provider
Promote HIV and diabetes screening in TB cases
Ensure treatment compliance, identify adverse drug reactions and refer in TB treatment
Identifying high risk pregnancies and follow up
Planning and implementation of activities at community level
Premarital counselling of eligible couples and Support for planning of pregnancy
Pre-conception supply of folic acid to prevent NTD
Early detection, registration of pregnancy and issuing of ID number and MCP Card
Antenatal check-up including screening of Hypertension, Diabetes, Anaemia etc
Immunization for pregnant woman-TD
IFA and Calcium supplementation
Transport entitlements
Follow-up of Gestational Diabetes Mellitus and Pregnancy Induced Hypertension.
Registration in RCH portal and MCP card. ✓ Initiation and management of ARI/Diarrhoea and other common illnesses and referral ✓ Screening, referral (DIEC/FHC) and follow up/tracking for disabilities, developmental delays and behavioural abnormalities. ✓ Ensuring full immunization coverage
Vitamin A supplementation
Resul Pookutty Foundation
Detailed Project Report
248
✓
✓
✓
✓
✓
✓
✓
✓
✓
✓
✓
✓
✓
✓
✓
✓
✓
✓
✓
✓
✓
Sub Centre – Yeroor Grama Panchayath
✓
Reporting of Adverse Events
✓ Following Immunization (AEFI)
✓ Follow up to ensure prophylactic and therapeutic compliance of IFA/WIFS
✓ Regular Post- partum care visits
✓ Home based new-born care through 7 visits in case of home delivery and 6 visits in case of institutional delivery
✓ Educating mother and family on new born danger signals.
✓ Identification and care of high risk new-born - low birth weight, preterm and sick new-born (with referral as required)
✓ Counselling and support for early and exclusive breast feeding complimentary feeding practices
✓
Identification of congenital anomalies and appropriate referral to DEIC/FHC
✓ Mobilization and follow up for immunization services
✓ Reporting of neonatal death
✓ Awareness about programs like Hridyam, New born screening (SalabhamJatakseva), SruthiTarangam, RBSK, Arogyakiranam and follow-up of beneficiaries
✓
✓
✓
✓
✓
✓
Growth Monitoring, IYCF and food supplementation linked to ICDS
Identification of acute malnutrition referral and follow up care for SAM
Prevention of Anaemia - Iron supplementation and Deworming
Prevention of Diarrhoea/ ARI
Promotion of Home Available Fluids (HAF) and ORS
Pre-school and School level Child Health activities - Biannual screening, School health records, Eye care, De-worming etc
✓
Screening of children as per national and state programs to cover 4’D’s Viz. Defect at birth, Deficiencies, Diseases, Development delay including disability (RBSK and Arogyakiranam)
✓
Awareness creation on proper use of electronic gadgets like mobile phone, tab, TV etc
✓
Promotion of physical activity and healthy food habits like reduced salt and sugar intake and increasing consumption of fruits and vegetables
✓ Adolescent Health
Resul Pookutty Foundation
Detailed Project Report
249
Sub Centre – Yeroor Grama Panchayath
✓ Awareness creation, Counselling and follow up on:
✓ Improving nutrition
✓ Sexual and reproductive health
✓ Prevention of substance misuse (Vimukthi program)
✓ Healthy life style promotion
✓ prevention of Anaemia
✓ Provision of IFA under National Program
✓ Identification of eligible couples for temporary and permanent methods
✓ Follow up of contraceptive users
✓ Counselling and facilitation of safe abortion services
✓ Follow up for any complication after abortion and appropriate referral if needed
✓ Awareness creation and referral services for infertility
✓ Identification and referral of visual impairment or defects in general population.
✓ Identification and referral of cases for cataract surgery
✓ Promoting annual retinopathy screening for all diabetic and hypertensive patients.
✓ Screening for common oral diseases/conditions and referral with special emphasis on geriatrics and palliative care patients.
✓ Screening for oral cancer and premalignant conditions in high risk individuals and referral
✓ Tobacco cessation activities and COTPA and IEC/BCC activities at community and schools level for primary and secondary prevention
✓ Identification of high-risk groups like persons living alone, widows, persons with co morbid conditions, addictions, bed ridden patients etc
Resul Pookutty Foundation
Detailed Project Report
250
9.2
Projections of Patient Inflow
DEMAND ESTIMATE FOR THE PROPOSED SUB CENTRE AT YEROOR
Based on inputs from the health professionals working in the Main Sub Centre, patient inflow statistics have been worked out.
Patient inflow for the SC at Yeroor
The average monthly patient inflow to the Main Sub Centre at present is as follows: 1. Immunisation 90
Projected Patient inflow for the proposed SC at Yeroor
With improved facilities and services proposed for the Yeroor Main Sub Centre, the demand for the services are likely to increase substantially. Based on discussions with the health professionals at the Main Sub Centre and the PHC, the patient inflow for the proposed Sub Centre at Yeroor has been estimated as follows:
251
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
2. NCD 175 3. Antenatal / postnatal services 30 4. IUCD 5 Total 305
PROPOSED
Sub Centre – Yeroor Grama Panchayath
INFLOW OF MAIN SUB CENTRE,
Testing 150
Pharmacy with NCD/Palliative Care Medicine Distribution 300
Tele- Medicine 50
Health Clinics (Gynaecology, Paediatrics, Skin, Cancer etc.). Four Programmes in one month with 25 participants
100 9 Medical Camps (Eye, Skin, Cancer Detection, etc.). One Programme in one month 50 Total 305 1100
9.3 Cost Benefit Analysis
A positive Cost Benefit Ratio is an indicator for the evaluation of any infrastructure project, especially a project with considerable social benefits. The factors to be included in the cost benefit analysis for this project are given below.
Costs
• Cost of Construction and Setting up the Centre
• Recurring expenses for the operation of the facility
• Manpower cost to operate the facility
• Utilities and consumables etc.
Detailed Project Report
252
Resul Pookutty Foundation
2
3
5
MONTHLY PATIENT
YEROOR SNo Health Care Service Number of Beneficiaries Current Health Care Service Present Projected 1 Immunisation 90 150
Ante-natal / postnatal Care 30 40
Non Communicable Diseases Check up 175 250 4 IUCD 5 10 Sub Total 305 450 Additional Health Care Services Proposed
Lab
6
7
8
Detailed Project Report
Sub Centre – Yeroor Grama Panchayath
Benefits
• As this being a Govt. owned and operated facility to be operated as per the policies and schemes of Central & State Governments, no direct revenue for the project is considered.
• Considering the objective of the project, the major benefit to be factored shall be the cost savings by the users in terms healthcare costs in comparison with their spending requirement in private hospitals
• With the modern outlook of the Sub Centre and the advanced facilities of E-health and telemedicine, the usage pattern also will certainly go up.
• There will be many benefits which cannot be converted to monetary terms for the computation of Cost Benefit Ratio.
The summary of the Cost Benefit Analysis performed for the project indicates a strong positive Cost Benefit Ratio. The proposed facility is expected to serve around 6000 people residing in the project area. The details of the Cost Benefit Analysis calculated with the projections of Cost & Benefit for a period 20 years is given below.
Particulars
Rs. Lakhs
Total Costs 2,647.73
Present Value of Cost 1,336.43
Total Benefits 4,030.05
Present Value of Benefits 1,737.73
Net Present Value 401.30
Cost Benefit Ratio 1.30
The project returns a positive Net Present Value of Rs.401.30 lakhs and a positive Cost Benefit Ratio of 1.30. This indicates the economic and social viability of the project.
253
Resul Pookutty Foundation
10. Financial Analysis
10.1
Summary of Project Cost
Summary of Project Cost INR
CIVIL 1,22,19,885 ELECTRICAL 14,03,182 AIRCONDITIONING 4,39,800 LOW VOLTAGE SYSTEM 12,87,340 PLUMBING 17,07,481 FIRE & SAFETY 15,999 FURNITURE 3,86,400 MEDICAL EQUIPMENTS 13,63,500 WASTE MANAGEMENT BOQ 2,50,000 PRELIMINARY EXPENDITURE 15,96,624 CONTIGENCY 24,60,313 PMC 18,50,442 TOTAL INR 2,49,80,966
10.2 Monthly Cashflow Requirement
The overall project of Yeroor Sub Centre is expected to be completed within a period of 8 months from the date of approval of the project. It is expected that the project will begin during the month of January 2020. The monthly consolidated cashflow requirements are given below
Resul Pookutty Foundation
Report
254
Detailed Project
Sub Centre – Yeroor Grama Panchayath
0 1000000 2000000 3000000 4000000 5000000 6000000 7000000
2384729 2642401 3224326 3565034 3785060 3289745 6089670
Jan-21 Feb-21 Mar-21 Apr-21 May-21 Jun-21 Jul-21 Aug-21 Series 1
Detailed Project Report
255
Project Component Project
Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation The project component-wise monthly cashflow is given below Monthly Cashflow Requirement Against - Implementation Schedule Total Amount
Duration in Months 1 2 3 4 5 6 7 8 12219885 Civil Works 0 1115592 743728 0 0 0 0 0 1403182 Power Supply & Distribution 0 0 0 0 0 0 0 1403182 439800 HVAC 0 0 0 0 0 0 439800 0 15999 Fire Fighting 0 0 0 0 0 0 15996 0 250000 Waste Management 250000 1707481 Plumbing & Storm Water Management 0 212207 212207 212207 448827 424413 212207 85413 1363500 Medical Equipment’s 0 0 0 0 0 0 818100 545400 1287340 Low Voltage Systems 0 0 0 0 0 0 0 1287340 386400 Furniture & Fixtures 0 0 0 0 0 0 0 386400 1596624 Preliminary Exp 800000 796624 2460313 Contingencies 219842 142299 191217 260196 309330 404166 361786 571777 1850441 Project Management Charges 500000 200000 200000 200000 20000 250441 300000 24980965 Total 1384729 1642401 4524326 5321034 3572759 3517735 5333632 7759029 The project also envisages an ongoing support to the facility in-terms of Repairs & Maintenance of the Facility and Public Relation Campaigns for a period of two years from the date of commissioning. The cashflow requirement during the period are as under. Year Amt. INR Year 1 31,28,849 Year 2 31,04,212 Total 62,33,061 RPF will disburse the funds as against the monthly requirement planned and as per the progress of the project.
10.3 Revenue Estimates
This being a Govt facility for public healthcare, factoring of revenue from operations to ascertain the feasibility of the project is not tenable. The entire cost of building and equipping the Sub Centre and the recurring cost towards repairs & maintenance and expenses towards Public Relations will be funded by Resul Pookutty Foundation through its internal sources. RPF is not intending to generate any revenue from this project.
However the following facilities created in the Sub Centre can be leased out by the Govt for specified activities on a rental basis. Such revenue can be used appropriately by the Govt.
• Rental of Pharmacy Space to Govt Sponsored Pharmacies
• Yoga Centre Rental
10.4 Estimates of Recurring Expenses
The recurring cost proposed to be incurred during the first two years of operation including the project management fee are estimated as under.
YEROOR SUB CENTRE - MAINTENANCE & PUBLIC RELEATION COST
Resul Pookutty Foundation
256
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
INR INR INR Sl. No. Particulars Year 1 Year 2 Total 1 Repairs &
of the Facility
2 Public
Expenses
Cost
Creative Agency Fees
3 Project
Maintenance
813,629 894,992 1,708,622
Relation
500,000 500,000 10,00,000 Media
500,000 400,000 900,000
240,000 264,000 504,000 Event Management 150,000 120,000 270,000
Management Cost 925,220 925,220 1850441 Total Operating Cost funded by RPF 31,28,849 31,04,212 62,33,061
10.5 Sources of Funds
This is a fully funded project sponsored by Resul Pookutty Foundation, a Non-Governmental Organisation committed for the development of Public Health Delivery systems in the state. The Application of Funds towards the construction and furnishing of the Sub Centre and for the maintenance of the facility for a period of two years will be fully funded by RPF, the sponsor of the Project. The sponsor will also coordinate and fund for the public relation activities of the Sub Centre for a period of 2 years to promote the facility and gain a greater public acceptance and usage.
RPF will be funding these projects from their internal funds earmarked for the developmental purpose.
The detailed statement on Source & Application of Funds are given below:
Resul Pookutty Foundation
257
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
YEROOR SUB CENTRE - APPLICATION OF FUNDS INR Sl. No Application Funding During Project Year 1 Year 2 1 Cost to Establish the Facility 23,130,524 2 R&M of Facility 813,629 894,992 3 PR Expenses 13,37,000 13,37,000 4 Project Management Cost 925220 925220 23,130,524 30,75,849 30,79,849 Grand Total 29,363,585 YEROOR SUB CENTRE - SOURCE OF FUNDS Sl. No Application Funding During Project Year 1 Year 2 1 Resul Pookutty Foundation 100% 29,363,585 1,46,81,793 1,46,81,793 Grand Total 29,363,585 1,46,81,793 1,46,81,793
11. Conclusion
This DPR showcases the detailed plans of an ambitious project presented by Resul Pookutty Foundation (RPF) to Govt. of Kerala to upgrade the Healthcare Delivery Systems of the state. This DPR presents the detailed needs analysis, plan description, budgeting and impact assessment of the project. The pilot project presented herein is part of a master plan developed by RPF for the comprehensive development of Public Health Institutions in Anchal Block Panchayat. The economic and technical feasibility of the project has been confirmed through different types of studies, surveys and a detailed Market Research.
The benefits envisaged from the project will certainly outweigh the investment required for the project. On successful implementation of this Pilot project, RPF will be launching the master plan after incorporating lessons learned from the Pilot project.
The DPR presents the detailed estimates, designs, drawings, specifications and project cost analysis.
RPF is very happy is presenting this project before the Department of Health and Family Welfare, Govt. of Kerala for approval.
Annexures
Annexure
Annexure
Annexure
Annexure
Annexure
258
Detailed Project Report Sub Centre – Yeroor Grama Panchayath
Resul Pookutty Foundation
– 1 – Topography Report
2
–
– Soil Test Report
– 3 – Water Test Report
– 3 – Pollution Test Report
– 4 – Detailed Drawings

