11 minute read
PREGNANCY IN FOOTBALL, A BLANKET BAN?


FEATURE / EVA FERRER MD
Introduction
Advertisement
Given that some national guidelines advise pregnant women to avoid football while pregnant1,5 it may be easy to ignore this topic and avoid any discussion, giving it a blanket ban. However, as with most things in life, it is not always clear cut and as something we will feasibly encounter working in women’s football, we should seek to understand the landscape better.
State of the Art
Professionalism of the women’s game is growing rapidly and research into specific health and performance issues for the players is accelerating. We need to be up to date with the latest literature and open to changing developments in all areas, including pregnancy and the postpartum period.
The main question I will address in this article is; ‘how can pregnancy and postpartum period, be managed for a football player?’
Despite a growing amount of research literature in women’s football, not many studies on pregnancy in postpartum in sport have been published 2,7 and even less, on football players. Given such a lack, it is no surprise that there are no globally accepted, scientifically validated recommendations or approach to managing a pregnant/postpartum athlete, regardless if in football or other sports. Research is therefore clearly urgently needed looking into health issues related to pregnancy and football, and how to manage each individual situation. Nevertheless, while there is limited research, this is something that we as practitioners can and likely will come across and must deal with.
What Should We Consider For The Pregnant Footballer?
Contraindications and health benefits
We need to remember that in the absence of contraindications (Figure 1 and 2) being an active mum is associated with multiple health positive effects 1,2,3 that can range from physical benefits such as decrease risk of pre-eclampsia 18,19 or urinary incontinence to mental health benefits such improving depressionrelated symptoms.
*Reproduced by permission of
Anatomic, metabolic and physiological changes and adaptations
For the athlete healthcare professional, our interest should be specially focused on the physiological and anatomical changes that occur during pregnancy6. These must be considered when designing the physical activity program10. Each woman and each pregnancy can and most likely will be different.
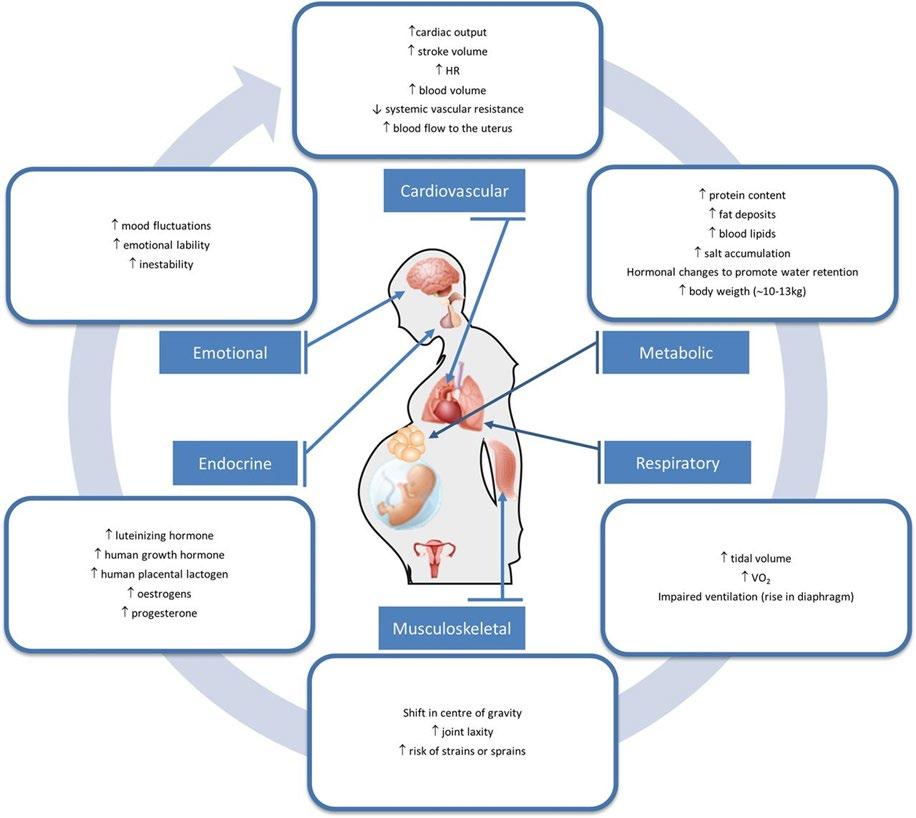
Maternal physiological adaptations to pregnancy have to be considered by modifying exercise routines and/or activity patterns. Changes in normal metabolic processes exist to accommodate the needs of the developing foetus (Figure
3). Pregnancy entails great changes in maternal hemodynamics, such as increase in blood volume, heart rate, and stroke volume, and a decrease in systemic vascular resistance4. The respiratory system can undergo changes due to anatomical and functional alterations2 Regarding hormones during pregnancy progesterone, relaxin and oestradiol are responsible for softening pelvic ligaments for childbirth9,21. Oestradiol affects the structure of bone, muscle, tendon and ligaments. Bone and muscle receive positive feedback improving its function while in tendons and ligaments oestrogens decreases stiffness that affects directly the risk of injury and the level of performance20
The anatomical changes that occur during the pregnancy period have an impact on how women’s ability to perform physical activity, exercise or sport. Changes in trunk mobility and motion control due to increased mass and dimensions, may reduce the functional range of motion of the trunk segments14 Due to the need to accommodate the growing foetus, the uterus expands and lumbar lordosis progresses displacing the centre of gravidity. This fact will change all the possibility of maintaining previous balance, which will be now poorer, and will need adaptations to compensate it. Wider stance and changing the step length will be a mechanical adaptation to occur in a progressive way14 The hip, related to the expansion of the uterus and the widening of the pubic symphysis will increase its flexion angle. However, not only does the pelvic area go through changes, the joints do too. Ligamentous laxity can affect stability of all weight-bearing joints from the pelvis to the feet15. The knees will increase their flexion but will reduce the extension, which will be responsible for biomechanical changes when walking or running. The decrease of ankle dorsiflexion and plantar flexion can also be an issue for a correct ability to move. As pregnancy progresses the body adapts to the changes previously mentioned and in each trimester several outcomes have a higher probability of existing. Some of the highlights are as follows:
First trimester
While exercising, average core body temperature increases by 1.5ºC after 30 min. At what level of exercise and what environmental temperature and humidity the upper limit for maternal core temperature is exceeded is still being studied. There is given evidence that during organogenesis, maternal hyperthermia above 39ºC may be teratogenic11. Caution should be taken to keep core temperature < 39ºC12, the hypothesised teratogenic threshold during pregnancy, while exercising.
Second and third trimester
Studies regarding this period are somehow controversial. Foetal growth restriction (FGR) and insufficient gestational-weightgain are possible negative outcomes that can overcome during this pregnancy period when exercising at levels significantly above recommendations7,17
Some authors suggest that practicing exercise at high-intensity may cause alterations in foetal heart rate (FHR)17 but other publications indicate that vigorous intensity exercise completed into the third trimester appears to be safe for most healthy pregnancies. Due to these dual results, professionals recommend avoiding exercising at a perceived exertion relative to ≥90% maximum heart rate13
Athletes can also experience major symptoms that can limit the possibility to practice. Nausea and vomiting has prevalence rates of between 50% and 80% in early pregnancy3 Fatigue can also be an issue22 as it decreases capacity for physical work.
In general population the prevalence rate of pregnancy-related low back pain (LBP) is estimated to be about 50% during pregnancy while elite athletes experienced a lower prevalence of pregnancy induced LBP compared with non-elite athletes23 probably associated with stronger abdominal musculature. Urinary incontinence is caused by the increase of pressure, pelvic floor distensibility and the bladder volume4
Sport can aggravate the symptoms of incontinence, which can have an average incidence around 26%.
Screening, Exercising & Monitoring
Once the player knows she is pregnant, she is surrounded by doubts around what she can/cannot, should/should not do. The first step to take, should be to collect all the information regarding this pregnancy and previous one(s) (if applicable). To facilitate the process of medical screening1, a useful and accessible tool is the Get
Active Questionnaire for Pregnancy (GAQ-P) (https://csep.ca/2021/05/27/getactive-questionnaire-for-pregnancy/)24 that provides a checklist format of contraindications (both absolute and relative) to maternal exercise. Other specific issues that could be asked for are related to history of eating disorders, previous menstrual function and pelvic floor health. Once cleared and if needed double-checked with the health care professional in charge of the players pregnancy, an individualized program should be established.
Recommendations based on the current medical guidance, are that pregnant players should not continue playing football beyond the first trimester. In the second trimester foetus moves higher and is unprotected by the pelvis, increasing the risk of damage26

Monitoring the player’s activity is a measure that will give the health practitioner information, on any change that could compromise the athlete and the foetus health. At the same time by tracking the different variables it will be easier to individualize and progress the fitness program.
Studies show that transient foetal bradycardia can exist when pregnant elite athletes exercise above 90% of the maximal maternal heart rate; therefore, the pregnant women should avoid exercising over ≥90% MHR27. Borg scale can also be used as a monitoring method but it does not correlate strongly with heart rate, if used it should stay between 12-14 if moderate exercise is targeted28. During exercise in normal pregnant subjects, there are diminished responses for every respiratory function, reflecting a decrease in pulmonary reserve and inability to exercise anaerobically.16
Considering the aforementioned physiological and anatomical changes of pregnancy, the recommendations for a healthy pregnancy program should follow, from week 1 to week 34 focus in physical condition and strength while from week 35 to delivery mobility, meditation, physical conditioning and strength are the main areas to focus on. Bear in mind, that during the 2nd and 3rd trimester when a pregnant woman is in a supine position the gravid uterus compresses the inferior vena cava, leading to decreased venous central ruturn and can cause a hypotension supine syndrome that usually occurs within 3–10 minutes after lying down.1
Due to the high incidence of urinary incontinence and pelvic floor dysfunction in late pregnancy and the postpartum period24, it is important to include pelvic floor exercise. These should be performed with “Exhale on exertion” to avoid increasing the intraabdominal pressure, when working.
Monitoring should not be limited to the player’s physical condition, mental health and nutritional needs should be followed up too. As mentioned previously, pregnant woman can experience physiological distress, to manage this situation, mental health must be followed as some athletes may feel anxiety regarding returning to a competitive level following childbirth7 On the other hand, ensuring maintenance of hydration and fuelling is also particularly important when practicing physical activity during pregnancy. A good balance between exercise and energy intake is basic for the foetus and the mother’s good health. Gestational Weight Gain (GWG) is an indicator for sufficient energy intake for foetal growth and development24
Postpartum Period And Return To Play (RTP)
After delivery return to play should not be rushed, the possible program to follow should be adapted to the different phases, depending on the individual rehabilitation needs. If pregnancy, labour, and birth has been uncomplicated and the new-mother feels capable while staying in the hospital, she can start rehabilitation focusing in pelvic floor exercises.
Once at home and during the initial postpartum period the clinical guidelines recommend women to gradually return to low-impact exercise, as 12 weeks are required
Figure 4: A proactive and individualised management will help to achieve a secure elite return to play. Although there is little evidence amongst elite athletes, it has even been postulated that some pregnancy-induced physiological changes may enhance exercise potential (30).
For The Musculoskeletal Soft Tissues To Heal24
Different authors divide the athlete RTP period in several phases. Donelly and colleagues29 propose the 6 Rs framework, ensuring that all aspects of perinatal athlete performance are considered, these 6 “R” are Ready (1-6 weeks), Review (8-12 weeks), Restore (12-16 weeks), Recondition (+16 weeks), Return and Refine. While Jackson et al24 gives a novel integrative concept to return elite female athletes dividing the post-partum period in “active recovery” focusing in low impact exercises and improving pelvic floor, “training” with increase in load and progressive exposure to impact and finally “performance” with sport specific exercises.
Healthcare professionals need to supervise closely the player’s physical and mental progress and follow some of the issues that are known to be important concerns that can impact on performance7,24,29, summarized in figure 4.
- Lack of sleep
- Pelvic floor disfunction
- Breast feeding
- Mental health
- Altered energy balance
- Increased joint laxity
Conclusions
A multidisciplinary physiological, physical and mental approach is needed to provide the player security and stability during the entire pregnancy and postpartum period. Even though more and more researchers are focusing on this female vital stage, more research is required to advance knowledge and understanding of pregnant and postpartum elite athletes, especially in football.

Take-home messages:
- The player needs to continue being active to achieve a healthy pregnancy, for her and her baby.
- Football is a contact sport and that’s an important fact that limits the player to continue playing.
- It is essential to be aware of the changes the players body will suffer.
- Throughout pregnancy individual adaptation will be needed, be cautious but not scared.
- Keep in mind that pregnancy does not finish after 9 months, a post-delivery period exists and that includes return to play.
- A multidisciplinary physiological, physical and mental approach is needed.
References
1. Mottola MF, Davenport MH, Ruchat S-M, et al. 2019 Canadian guideline for physical activity throughout pregnancy Br J Sports Med 2018;52:1339–1346.
2. Wieloch N, Klostermann A, Kimmich N, et al. Sport and exercise recommendations for pregnant athletes: a systematic scoping review. BMJ Open Sport & Exercise Medicine 2022
3. Bø K, Artal R, Barakat R, et al. Br J Sports Med 2016;50:1297–1305.
4. Barakat R, Perales M, Garatachea N, et al. Exercise during pregnancy. A narrative review asking: what do we know? British Journal of Sports Medicine 2015;49:1377-1381.
5. Artal R, O’Toole M.Guidelines of the American College of Obstetricians and Gynecologists for exercise during pregnancy and the postpartum period BJSM 2003;37:6-12.
6. Solli GS, Sandbakk Øyvind. Training characteristics during pregnancy and postpartum in the world’s most successful cross country skier. Front Physiol 2018 ;9:595.
7. L’Heveder, A.; Chan, M.; Mitra, A.; Kasaven, L.; Saso, S.; Prior, T.; Pollock, N.; Dooley, M.; Joash, K.; Jones, B.P. Sports Obstetrics: Implications of Pregnancy in Elite Sportswomen, a Narrative Review. J. Clin. Med. 2022, 11, 497
8. Soma-Pillay, P.; Nelson-Piercy, C.; Tolppanen, H.; Mebazaa, A. Physiological changes in pregnancy. Cardiovasc. J. Afr. 2016, 27, 89–94
9. Chidi-Ogbolu, N.; Baar, K. Effect of Estrogen on Musculoskeletal Performance and Injury Risk. Front. Physiol. 2019, 9, 1834.
10. A Bump in the Road? The BASES Expert Statement on Pregnant and Postnatal Athletes. The Sport and Exercise Scientist, Issue 74, Winter 2022.
11. Davenport, M.H.; Yoo, C.; Mottola, M.F.; Poitras, V.J.; Garcia, A.J.; Gray, C.; Barrowman, N.; Davies, G.A.; Kathol, A.; Skow, R.J.; et al. Effects of prenatal exercise on incidence of congenital anomalies and hyperthermia: A systematic review and meta-analysis. Br. J. Sports Med. 2019, 53, 116–123.
12. Ravanelli, N.; Casasola, W.; English, T.; Edwards, K.; Jay, O. Heat stress and fetal risk. Environmental limits for exercise and passive heat stress during pregnancy: A systematic review with best evidence synthesis. Br. J. Sports Med. 2019, 53, 799–805.
13. Beetham, K.S.; Giles, C.; Noetel, M.; Clifton, V.; Jones, J.C.; Naughton, G. The effects of vigorous intensity exercise in the third trimester of pregnancy: A systematic review and meta-analysis. BMC Pregnancy Childbirth. 2019, 19, 281.
14. Gilleard W, Crosbie J, Smith R. Effect of pregnancy on trunk range of motion when sitting and standing. Acta Obstet Gynecol Scand. 2002 Nov;81(11):1011-20
15. Ritchie, J Orthopedic Considerations During Pregnancy. Clinical Obstetrics and Gynecology 46(2):p 456-466, June 2003.
16. Artal,R , Wiswell, R, Romem, Y,Dorey F. Pulmonary responses to exercise in pregnancy, American Journal of Obstetrics and Gynecology,154 (2),1986, 378-383,
17. Salvesen KÅ, Hem E, Sundgot-Borgen J. Fetal wellbeing may be compromised during strenuous exercise among pregnant elite athletes. Br J Sports Med. 2012 Mar;46(4):279-83.
18. Brown, W.J.; Hayman, M.; Haakstad, L.A.H.; Lamerton, T.; Mena, G.P.; Green, A.; Keating, S.E.; Gomes, G.A.O.; Coombes, J.S.; Mielke, G.I. Australian guidelines for physical activity in pregnancy and postpartum. J. Sci. Med. Sport 2022, 25, 511–519.
19. Genest,D, Falcao,S , Gutkowska J, Lavoie J. Impact of exercise training on preeclampsia: potential preventive mechanisms. Hypertension. 2012 Nov;60(5):1104-9
20. Kumar P, Magon N. Hormones in pregnancy. Niger Med J. 2012 Oct;53(4):179-83.
21. Waugh, C, Scott, A. Case Studies in Physiology: Adaptation of load-bearing tendons during pregnancy May2022 Journal of Applied Physiology 2022 132:5, 1280-1289
22. Pugh LC. Childbirth and the measurement of fatigue. J Nurs Meas 1993;1:57–66.
23. Wowdzia JB, McHugh TL, Thornton J, Sivak A, Mottola MF, Davenport MH. Elite Athletes and Pregnancy Outcomes: A Systematic Review and Meta-analysis. Med Sci Sports Exerc. 2021 Mar 1;53(3):534-542
24. Jackson, T; Bostock, E; Hassan, A; Greeves, J; Sale,C Elliott-Sale, K1. The Legacy of Pregnancy: Elite Athletes and Women in Arduous Occupations. Exercise and Sport Sciences Reviews 50(1):p 14-24, January 2022.
25. James, M; Moore, I; Donnelly, Gráinne M., Brockwell, E Perkins, J; Coltman, C. Running During Pregnancy and Postpartum, Part A: Why Do Women Stop Running During Pregnancy and Not Return to Running in the Postpartum Period?. Journal of Women’s Health Physical Therapy 46(3):p 111-123, July/September 2022.
26. Torede, M. Guidelines for safe participation con contact and collision sports. Participation of the pregnant athlete in contact and collision sports
27. Beetham, K.S., Giles, C., Noetel, M. et al. The effects of vigorous intensity exercise in the third trimester of pregnancy: a systematic review and meta-analysis. BMC Pregnancy Childbirth 19, 281 (2019)
28. DA Silva DF, Mohammad S, Hutchinson KA, Adamo KB. Cross-Validation of Ratings of Perceived Exertion Derived from Heart Rate Target Ranges Recommended for Pregnant Women. Int J Exerc Sci. 2020 Sep 1;13(3):1340-1351.
29. Donnelly GM, Moore IS, Brockwell E, et al. Reframing return-to-sport postpartum: the 6 Rs framework British Journal of Sports Medicine 2022;56:244-245.
30. Kimber ML, Meyer S, McHugh TL, Thornton J, Khurana R, Sivak A, Davenport MH. Health Outcomes after Pregnancy in Elite Athletes: A Systematic Review and Meta-analysis. Med Sci Sports Exerc. 2021 Aug 1;53(8):1739-1747








