Publications Agreement No: 41203011 THE OFFICIAL PUBLICATION OF THE TORONTO PROFESSIONAL FIRE FIGHTERS’ ASSOCIATION VOLUME 16 | ISSUE 1 Demographics Issue














































The tension was high, and the membership was divided before the second and final special meeting to deal with the City of Toronto’s mandatory vaccination policy. To make matters worst, unlike the only other meeting call by the membership in the history of Local 3888, ours was online, a platform not yet perfected. As if there weren’t enough challenges. All bases, from legal counsel to a parliamentarian from the IAFF, were covered to ensure that over 750 people would receive fair, consistent, sound information.
My 24 years of experience would be tested tonight, and so would my composure because if yesterday’s meeting were a barometer, there would be fireworks. In my entire career, I have never seen anything so contentious. That includes the amalgama tion of 6 departments where I started my union career. Although many of us heard stories of families who have been torn apart over COVID, I never imagined that our Sisters and Brothers would show such hatred for one another. To be fair, that didn’t apply to most members. It was hard to be lieve that months before the announcement of the policy, those same members enjoyed a sacred bond, unlike most professions.
From the beginning, the Executive Board vowed to remain neutral, put our personal opinions aside, and not be swayed by any one or anything. Although many tried, from both sides of the battle lines. To the entire board’s credit, that theme was adhered to regardless of the political ramifications. The mandatory vaccination policy (MVP) was a legal issue and would be adjudicated through those proceedings. Regardless of individuals’ opinions, the goal was to approach each issue fairly and respectfully and to apply the same principles consistently. As always, we needed to represent all our members regardless of their position. Unfortunately, that would mean not making anyone happy. The first step was stopping the forum posts, a platform that could lead to more discipline and turmoil. Secondly, stay out of the media, considering the problematic City budget on the horizon. The perception of showing a break in the ranks would not be favourable. With the stage set, it was time to buckle up for a year-long rollercoaster ride of impos sible no-win situations created by COVID.
Late Friday evening on August 26, 2022, we received the final mandatory vaccination grievance award from Arbitrator Rogers, a
complex document of over 100-pages. The decision was not public, but within an hour, calls filled our voicemail from the media and members with enquiries. Like everything up to this point with the MVP, there were more questions than answers. Likewise, there were many things to digest and consider. Unfortunately, although comprehensive, Mr. Roger’s approach lacked step-by-step instruc tions on the implementation. Without those details, the City and the Association must decipher the arbitrator’s intentions and ne gotiate a settlement. In addition, the absence of a breakdown on how and when impacted members are reinstated meant information to the public would be limited. However, on a positive note, the resolve was consistent with all the legal advice provided to Local 3888 reported in both special meetings. In simplest terms, the arbitrator ruled that the policy was reasonable, but discipline and termination for our unvaccinated members were unreasonable.
By the time this article is received, there may be little relevance, but here is an attempt at “pulling back the curtains” and providing insight into how we got to where we are today.
When the City of Toronto introduced the mandatory vaccination policy (MPV), Local 3888 took a proactive approach. We immediately and formally put the City on notice for developing a policy without the involvement of Toronto Fire’s sole bargain ing agent. There were also many meetings to discuss education from a human relations perspective to avoid conflicts at work loca tions. However, the policy was often applied inconsistently and frequently altered, such as the movement of deadlines and changes in discipline. Furthermore, the requirement to get boosters and removing precautions such as distancing and mask-wearing raises questions about whether it applies today. However, from a Toronto Fire perspective, our measures at the pandemic’s peak were proven effective. A credit to the professional ism shown by our membership daily.
Next, we pooled our expertise and knowledge by bringing all City labour organizations together to share information and legal opinions and presented ourselves as a united front. It is important to note that we received several legal views. In addition, the TPFFA shared the cost for our opinion with the OPFFA because of the Provincial impact. We managed other expenses by sharing some of the arbitration costs with
Local 416 because we both used mutual counsel. Furthermore, your Association was able to cancel some arbitration dates due to the repetition of the City witness statements already presented in the Local 416 case for further savings. Nevertheless, although we filed the grievance later than Local 416 and started the expedited process later, we received our decision well in advance.
There were six arbitration dates (March 28, April 5, April 6, May 9, June 13, June 24, 2022) and the entire process from the filing of the grievance on October 6, 2021, to August 26, 2022, only took three hundred and twenty-four days to complete.
In total Local 3888 filed 106 grievances (many of which are in abeyance) related to the City Policy through the advice of legal counsel:
• A policy grievance.
• A grievance for termination of sick benefits for members impacted.
• A grievance for the denial of LTD benefits for members impacted. (successfully resolved)

• Several individual grievances are held in abeyance.
At the time of this article, I have no crystal ball to predict where we will be in terms of terminated members being reinstated and how it will affect everyone on individual bases. Furthermore, I can not comment on how many members may have chosen to move on or take another path. Finally, I don’t have the answers for those who do not want to work with someone who decided not to be vaccinated if that is a resolve. However, I will acknowledge that no matter the out come, some of you will not be happy, a real ization that never will change regarding this topic. Finally, I will say that your Association respects the professionalism of our members, and your Executive represented all of you well under impossible circumstances.
On September 13, 2022, the Principal Officers and I met with the City to officially discuss the next steps in the Rogers award. Our goal is to find closure to a dark chapter in the history of our union.
Kevin McCarthy, President Toronto Professional Fire Fighters’ Association I.A.F.F. LocalSavings of up to 30% on plans with unlimited data**
Big discounts on our most popular phones
**Beyond max. speed data, speeds are up to 512 Kbps

Get the same great prices for up to 5 friends or family members when you add them to your account3
Exclusive offers and everyday savings with Bell Advantages @ The Source™4
Current as of August 23, 2022. Available with compatible devices within network coverage areas available from Bell Mobility. Speed and signal strength may vary due to traffic, topography, environmental conditions and other factors, like Bell’s management of network resources, using methods which include Internet traffic management practices. See bell.ca/ITMP. Existing Bell customers who choose to switch to the Bell Exclusive Partner Program before the end of their contract are required to pay out their device balance and are subject to a $50 migration fee. 9-1-1 government monthly fee in AB.: $0.95, N.B.: $0.97, N.L.: $0.75, N.S.: $0.43, P.E.I.: $0.70, Qué.: $0.46, N.W.T.: $1.70. Sask.: $1.95. Bell remits required amount to government. Taxes extra. Other conditions apply. Subject to change without notice, not combinable with other offers. (1) Based on a third-party score (Global Wireless Solutions OneScore™) calculated using wireless network testing in Canada against other national wireless networks. See bell.ca/network (2) Offer ends December 31, 2022. You can continue to use data at these reduced speeds until your next monthly bill period. Only available in Canada. Not compatible with Roam Better Unlimited calling applies to calls made from Canada to a Canadian phone number or calls received while you are inside Canada. Sent texts include texts sent to a Canadian phone number while in Canada and exclude texts sent to a landline, to a U.S. or international phone number, premium texts (short codes), alerts, texts sent with a messaging application and roaming (international GSM texts). Received texts include texts received while in Canada and exclude roaming, premium texts (short codes), alerts or dial-up texts received from a messaging application. Out of bundle charges may apply. (3) Up to 5 friends or family members can be added to the primary subscriber’s account. (4) The Bell Advantages Program is available with select Bell consumer and small business services with accounts in good standing. The Bell Advantages Program and offers are subject to cancellation or change without notice. Registration is required and a Bell mobile phone number or Bell account number must be presented at time of purchase. Cannot be combined with any other offers. While supplies last. Taxes and Environmental Handling Fees are See thesource.ca/en ca/register/termsAndConditions to and

The IAFF holds a convention every two years. This is where direction is provided to the lead ership from the 330,000 members of the IAFF. The first convention took place in Washington, D.C., in 1918. This year, Ottawa was the host of the 56th Biennial Convention. In 2020, COVID-19 forced the convention, originally scheduled for Orlando, to move online. Canadian bor der restrictions were a significant con cern this year. There were concerns that american delegates would not attend. There were discussions about moving the convention to Las Vegas. Ultimately, after a survey went out to all affiliates, the decision was made to keep the con vention in Ottawa. This left the Ottawa local with only a short time to prepare. They did an excellent job.
IAFF President Ed Kelly chairs the convention. He was elected as our General President at the 2020 Virtual Convention. Each morning, he moder ated a round table discussion. Topics in cluded firefighting in the wildland-urban interface. It was very interesting to hear city firefighters talking about wildfires moving from the forests and brush into the interface where it starts to interact with homes. On another day, the dis cussion centred around the connection between sleep deprivation and cancer. Another round table focused on finan cial wellness, something that we are working with our Education Committee to bring to our members as well. A final panel discussion focused on behavioural health.
As the elected leaders of the TPFFA, it is our responsibility to speak for the 3,000 members of our association. Toronto is one of the largest locals in the IAFF, and as such, we get ten seats at convention. The number of seats a local gets at a convention is proportional to the size of their membership. There were close to 2,000 delegates present in Ottawa. Many alternates and guests also
attended. Most of the votes are done with the raising of hands. When a vote is close, the chair may do a standing vote to help determine the outcome. When things are too close to call, or by the re quest of the convention delegates, a roll call vote can take place. This is a rare oc currence, where each local, one by one, stands and provides their vote. A roll call vote can take hours. Once a roll call vote is called for, local affiliates have ten min utes to ensure that their delegates are present in the conference room. After ten minutes, the doors are tiled (locked), and no one can come or go until the vote is complete. Each delegate is responsible for a proportion of that locals’ vote. So, if you are missing someone, you lose their votes.
Tuesday at the convention is Per Capita Tuesday. This is when resolutions that have a cost assigned to them are dealt with. Going into this convention, our per capita was $15.68 per month, per active member, and $7.84 per retired active member. Each penny that per capita is increased provides approxi mately $35,000 to the IAFF. To figure out what that means to us, you need to multiply that by the number of members and then again by twelve months. On average, we have approximately 3,000 members at any time. Which means we pay the IAFF about $47,000 a month or $564,480/year.
In previous years, a resolution would be made to increase the per capita by the equivalent of the Consumer Price Index (CPI). At the 2020 convention, a resolu tion was passed to make this automatic, as it had never been voted down previ ously. This was capped at 3.5%. The CPI being added to our per capita this year did hit the max of 3.5% or 55 cents. That 55 cents adds more than $20,000 to our costs before any of the resolutions made it to the floor for debate.
Resolutions submitted by the IAFF executive board and local affiliates going
into this year’s convention had the poten tial to raise that per capita significantly. It was clear from conversations with other large locals that there was little appetite for such increases. Committees meet prior to the convention opening to discuss and debate the resolutions. This allows the opportunity for a resolution to be pulled or amended. Several reso lutions were modified or withdrawn at the committee stage to keep the costs to the locals down. By the end of business, delegates had adopted seven per capita resolutions, notably three cents for in creased cancer research. The three cents will allow the IAFF to fund research into cancers that specifically affect firefight ers. A total of 29.5 cents were added to properly fund the IAFF Foundation and the many services it provides. The 29 ½ cents is a significant amount of money. Yet, the explanation was sufficient to have most affiliates agree. One of the issues was that there was no dedicated funding for the IAFF memorial that takes place in Colorado Springs each year. Secondly, the Foundation had a high administration fee, which deters large donors from considering it for significant donations. By moving the admin costs to per capita, the percentage of donations dedicated to administration will drop sig nificantly. The expectation is that major donors, who would like to be associated with firefighters, will start to make their donations to our foundation. The funds raised are used for a variety of services for IAFF Members. Some of the most im portant are disaster relief grants, burn as sistance grants, survivor scholarships,

and behavioural health and wellness services through the IAFF Centre of Excellence. When all was said and done with per capita resolutions, 48.25 cents had been added through resolu tions. Ultimately, the final per capita is $16.73 per month, per active member, and $8.37 per active retiree. Each member in the active retiree category pays ½ per capita, and for that cost, we receive a ½ vote at the convention. Convention action will add approximately $37,000 to the TPFFA budget in our next fiscal year. I will be engaging the Finance Committee in discus sions to ensure that we can absorb this increase without a cor responding increase to your union dues.

There were many other resolutions presented that had no fi nancial impact. While I don’t have the space to discuss them all, one is worth mentioning. A resolution that we were excited to support ensures that the IAFF provides immigration assistance
to Canadian members who are hired to work in the offices in Washington. The need for this was seen most recently when our President Emeritus, Frank Ramagnano, was hired to work in the IAFF Washington office. The hurdles that he and others like him faced, were the impetus for this resolution.

Convention is a great opportunity to network and learn from our peers in the IAFF. For several members of your Executive
 James Reed, Secretary-Treasurer Toronto Professional Fire Fighters’ Association I.A.F.F. Local 3888
James Reed, Secretary-Treasurer Toronto Professional Fire Fighters’ Association I.A.F.F. Local 3888
July 1st, 2022 marked my one-year anniversary since I was voted in as Vice President of Local 3888. I remember the day like it was yesterday. I felt honoured and humbled by the fact that Local 3888 members entrusted me with the duties and responsibilities to move the Association toward a progressive and positive fu ture. I appreciated the trust and support back then, and I continue to appreciate each one of you as we continue to face challenges together.
The Executive Board has been a strong and dynamic team who have met many challenges head-on over the course of a year.
To provide an update, I will summar ize our accomplishments and what we continue to challenge on behalf of our members.
• Staff Shortages: We have started our third recruit class of 96 future firefighters.
• Call Backs: As of September 2021, call backs were arranged through a Memorandum of Agreement allowing trucks to remain in service.
As the Chair of the Government Relations Committee and past member, I under stand and recognize the importance of lobbying different levels of government on behalf of our profession. We had a strong and productive team travel to Ottawa for the Legislative Conference. Federally, we pushed for the Hero’s Fund. Provincially, we have many occupational diseases rec ognized as WSIB compensable, in addition to PTSI. On the municipal level, we were successful with a positive 2022 budget.
• 29th Legislative Conference – April 4 & 5, 2022 – Ottawa: I would like to thank the team of ten who travelled to Ottawa. The team from the Executive board was Ken Webb, Rob Kular, Ryan Morrison and Bill Morris. Members from the
floor included Tomas Girdauskas, Tori Goulart, James McCreight, James Wenger and Matthew Fabbro. The two lobbies for Legislative Conference involved private members bill C224, a framework to address occupational cancers for firefighters across Canada. This bill passed the second reading with full party approval, except for the Bloc Quebecois. The second lobby was an amendment to the criminal code to in clude firefighters and paramedics against assault while on duty.
For the upcoming municipal election this fall, we will be requesting volunteers to assist with campaigns. We would appre ciate your participation. For interested parties, please contact any of the Government Relations Committee members or members of the union executive board for details.
We once again look forward to working closely with our allies on council as we enter the upcoming budget. Our execu tive board will also be entering into an other bargaining session, as our collective agreement expires on December 31, 2023.
• Vaccination Policy: We finished our last arbitration date on June 24th, 2022. We await the arbitrator’s decision.

• 2021 Acting Captain’s Process: I was assigned as the Chair in December of 2021. As a committee, we addressed many flaws in the process. We are cur rently at a step two grievance, with an other meeting scheduled with TFS in the event we will need to move to step three. The committee is also looking to have a TOR (Terms of Reference) estab lished prior to any other promotional processes. This was never established, as outlined in the MOA and the Collective Agreement. The committee’s objective is to have rules established for all future
promotional processes i.e., provide ad equate training, a fair review process and officer development.
I would also like to take this opportun ity to recognize the hard work and dedica tion of the Ceremonial and Bereavement Committee and the Honour Guard, who play an important and compassionate role when dealing with the families who suffer the loss of their loved ones. You provide solace and support to the spouses and families during their moments of profound loss. Great job and thank you.
I am honoured to be working with and alongside our current executive board. The days are long and your commitment is unwavering toward the betterment of Local 3888 membership. You are appre ciated.
In closing, I would be remiss if I didn’t acknowledge the retirement of Neil McKinnon as Chair of the WSIB com mittee. I’ve had the sincere pleasure of working with Neil while he was on the executive board and as the WSIB Chair since 2008. I speak for many who will at test to Neil always being the person who answered his calls to provide sage advice and guidance, using his wealth of experi ence and expertise. Neil, I wish you the best of health and years of memorable moments with your wife Nancy, children, and grandchildren.
 Fraternally, John Maclachlan
John MacLachlan, Vice President Toronto Professional Fire Fighters’ Association I.A.F.F. Local 3888
Fraternally, John Maclachlan
John MacLachlan, Vice President Toronto Professional Fire Fighters’ Association I.A.F.F. Local 3888

If you have ever taken a stone and thrown it into a pond, you have seen the concentric circles that are rippling outward from the center where you threw the stone. Those ripples may not be the only effect that your throw might have had. It’s very possible that the sound of it going in may have scared a duck that was on the pond or the weight of it going down through the water disturbed fish that were swimming there. You are tied to all of that. You’re tied to the stone. You’re tied to the water. You’re tied to the ducks, and you’re tied to the fish, by the ripples. You have caused change through a single and simple act.


I get the honour of working with kids & youth in a mentorship program in the downtown core of Toronto. I get to see the amazing mentorship skills of our student leaders with younger students, and the lasting impact on their lives.
For example, during our summer camp, Toronto Fire had sent a fire truck and firefighters to hang out and play games with the kids. There was one child in particular who was really struggling with almost every game that was being played. The demeanor of the child was extremely hurt and didn’t want to try anymore games because they didn’t want to face anymore embarrassment.
One of our student leaders decided to become this child’s number one cheerleader and every opportunity they had to cheer this child on, they cheered like the Raptors had just won another NBA Championship. Quite quickly, all the firefighters started to cheer this child on just as exuberantly, and the demeanor of the child completely changed.
That child went on to graduate from high school and now is into his last year at the University of Toronto. He also is the new leader of the very same

summer camps that he attended as a child. He shared with me that the impact of the student leader, and all the firefighters cheering him on, inspired him and gave him a feeling of being safe in the neighbourhood, knowing that the firefighters are nearby.
The ripple effect you have as fire fighters goes so far beyond what you can even imagine. Every time you are at an event and the kids are crawling all over the fire trucks, they are inspired by you and they feel safe. Every time you rush into action, you are making a major difference in so many peoples’ lives, which leaves a lasting impact, generation to generation. If the situation that you are rushing towards is dark and feels hopeless, you are bringing hope and light into that situation by doing what you must do.
“The light shines in the darkness, and the darkness has not overcome it.”
– Apostle JohnIt’s an honour for us as the chaplaincy team to support all TFS personnel and their families. Let us be present in your crisis, whether to talk, listen, or pray as we walk through it together.
Thank You for the amazing ripple effect that inspires, encourages, and keeps our communities safe.
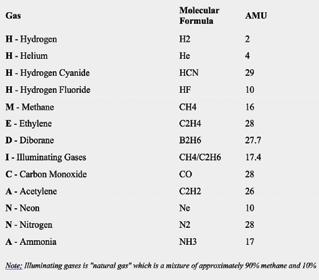
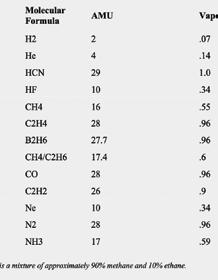
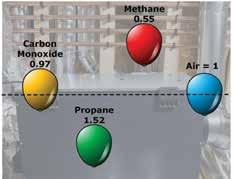
Why do we care which gases are lighter than air? Various reasons. Firstly, gases that are lighter than air are unique. Almost all gases are heavier than air. Furthermore, all vapours are heavier than air. Vapours are simply liquids under normal, ambient temperatures and pressures that have changed into a gaseous state. Liquids in vapour form are heavier than air because liquids generally have bigger and heavier molecules.
When gases are lighter than air, they will obviously present different problems for responders when dealing with an accidental release. This particular property can sometimes help us in dealing with an accidental release, and other times it may hurt us. When dealing with a release indoors, lighter than air gases will tend to collect in the ceiling space, making ventilation efforts rather difficult. However, this tendency is enviable when dealing with an outdoor release, as the gas will tend to float up and away and dissipate naturally, without human intervention.
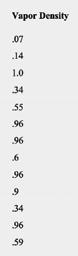
The physical property that we are discussing is referred to as “vapour density”, sometimes also referred to as “relative gas density”. Vapour density can be defined as the relative weight of a gas or vapour compared to air, which has an arbitrary value of 1.
Anything that has a vapour density of less than 1 is, therefore, lighter than air and will tend to rise. Gases with a vapour density greater than 1 will tend to sink. Vapour density is calculated by using the molecular weight of the given compound you happen to be dealing with. For example, methane with 1 atom of carbon and 4 atoms of hydrogen has a molecular weight of 16.04. Simply divide the molecular weight of methane (16.04) with the molecular weight of air (28.9), which gives you a vapour density value of 0.55. This value is less than 1, so we know that methane will rise in air.
Many of our fire ground decisions can be influenced by the vapour density of a given compound, including PPE decisions, hot and cold zone locations, instrument monitoring strategies and more.
In the early 1900s, a New York City fire officer developed an acronym for remembering the lighter than air gases, HA HA MICE
H- Hydrogen
A- Ammonia

H- Helium
A- Acetylene
M- Methane
I- Illuminating Gases (old term for natural gas)
C- Carbon Monoxide
E- Ethylene
This acronym was helpful and was used for many years. However, a new acronym needed to be developed as it became known that there were more than just 8 lighter than air gases.
Around 2001, a new acronym for remembering the lighter than air gases was created. This new acronym was 4H MEDIC ANNA and was developed by David Peterson, a well-known Hazmat Training Officer in Madison, Wisconsin. If you can simply remember the lighter than air gases, you know that all other gases and vapours you may encounter are heavier than air.
It’s important to keep in mind that vapour density is only a general concept and that on the fire ground, there are many other factors that can and will influence how a
particular gas will behave. Some of these environmental factors can include:
• air currents that can cause gases and vapours to form a mixture
• temperature, which can either cause gases and vapours to become more buoyant than expected or less so
• gases released from a container under pressure will initially be heavier than normal until they can be heated up by ambient temperatures and sunlight
• humidity will “weigh down” gases and vapours, meaning they will tend to be heavier than they otherwise would be
• dew point will also raise moisture levels in the air causing gases and vapours to again be much heavier than they normally would be
• aerosols, the presence of fine droplets, will also weigh down
Additionally, gases and vapours, when encountered in the field, will very rarely be present in their pure forms, as they are when lab tested. A rigid adherence to the numbers alone may not give responders a true indication of how a particular gas may behave in each situation. Responders must be thorough and attempt to determine if any of the aforementioned factors are at play.
I’ve always found acronyms helpful for remembering things. There are certainly enough of them in the fire service for various things. In this modern era of information being just a click away, the need for remembering things may not seem quite as important. However, acronyms can still be a time saver, even if it’s just a few precious seconds. If you can commit 4H MEDIC ANNA to memory, that’s great. If not, that’s okay too. It may assist you in the field sometime or even on a test in the fire service. Either way, why not try?
Stay safe!
One of the most famous tragedies involving a lighter than air gas is the Hindenburg disaster that occurred on May 06, 1937, in Lakehurst, New Jersey. The Hindenburg was an airship that originally was engineered to use the inert, lighter than air gas Helium. However, at the time, the U.S. barred the import of Helium, as they had dominated the Helium market. Consequently, the airship, which originated in Frankfurt, Germany had to be reengineered to use the extremely flammable Hydrogen as the lifting gas. Helium is approximately 1/8th the density of air, while hydrogen is approximately 1/16th the density of air, and more abundant.

During the attempted, “tethering” of the ship to the ground, a spark likely ignited some leaking hydrogen gas, resulting in the ship being consumed by flames in mere seconds. This disaster resulted in some 36 deaths and miraculously, had 62 survivors. Sadly, this incident was not the only accident involving Hydrogen as a lifting gas for airships, resulting in lives lost, but it’s the only one that was captured on film, with Herbert Morrison uttering the immortal words, “Oh the Humanity”.
This disaster quickly resulted in the end of an era regarding cross continental travel by airship. However, airships are in fact still in use today. It is quite commonplace to see the “Goodyear Blimp” at sporting events and they also have many other uses in industry, of course using the much safer Helium as a lifting gas.





As of June 2022
Quantity

















25 2019/20 /21 Pumper/ Rescues Spartan/ Dependable
6 2022 105' Quint Aerials Spartan/ Smeal
1 2020 135' (41 meter) Bronto Emergency One/Bronto
2 2021 Air/Light Trucks Freightliner/ Dependable
1 2020 Squad Spartan/ Dependable
20 2022 Pumper/ Rescues TBD
5 2022 100' Quint Aerials Emergency One
2 2022 Hybrid Pumpers
The REV Group
2 2021 HAZ MAT Trucks Spartan/ Dependable
1 2022 Fire Boat Metal Craft Marine Lt.
The first group of seventeen units are currently in production with two left to be delivered as of June 20, 2022. A further eight trucks are on order with a potential of five of these being delivered prior to year end.
These units are in production, with delivery beginning early 2023
This unit has been ordered, and is scheduled for delivery in the Fall of 2022.
These units have been delivered and are in the process of being placed in service.
This unit has been delivered and are in the process of being placed in service.
The document to purchase up to twenty Pumpers is out for bid now, with delivery anticipated late 2023
Units are approved and being ordered, delivery expected late 2023 or early 2024.
Units are approved and being ordered, delivery expected late 2023 or early 2024.
These two units are currently on order, with delivery likely not until early 2023
A replacement for the William Thornton is in production, with delivery scheduled for early 2023. This vessel is a 55' Firestorm, aluminum hull, twin engine, jet propulsion, with twin 3000USG per/min fire pumps.
Service
Carbon Monoxide 3,809 3,721 3,440 3,280 3,227 1.3%
CBRNE & Hazardous Materials 3,633 3,425 3,180 2,992 3,013 1.2%
Fires 170,274 182,322 179,535 159,183 132,457 51.6%
Medical 62,678 69,354 72,848 69,167 79,307 30.9%
Non Emergency 1,063 1,116 1,606 1,191 1,081 0.4%
Other Emergency Incidents 15,168 16,936 16,989 13,182 12,497 4.9%
Technical Rescue 8,888 10,357 9,764 7,710 8,420 3.3%
Vehicle Incident 18,348 18,457 19,743 16,169 16,933 6.6%
Total Unit Responses 283,861 305,688 307,105 272,874 256,935
Total Emergency Unit Responses 282,798 304,572 305,499 271,683 255,854
% Change
Total Emergency Incidents 4.3% 7.7% 0.3% -11.07% -5.8%
*
*
Station Sum of 10,499 9,077 8,771
2016 25067 P121 Spartan ERV
2016 25068 P132 Spartan ERV
2016 25069 P114 Spartan ERV
2016 25070 P233 Spartan ERV
2016 25071 P311 Spartan ERV
2017 25073 P142 Spartan ERV
2017 25074 P146 Spartan ERV
2017 25075 P221 Spartan ERV
2016 25076 P313 Spartan ERV
2017 25077 P344 Spartan ERV
2017 25078 P442 Spartan ERV
2017 25079 P145 Spartan ERV
2018 25083 P222 Spartan ERV
2018 25084 P226 Spartan ERV
2018 25082 P135 Spartan ERV
2018 25085 P343 Spartan ERV
2018 25080 P111 Spartan ERV
2018 25081 P232 Spartan ERV
2020 25086 P131 Spartan Dependable
2020 25087 P123 Spartan Dependable
2020 25088 P443 Spartan Dependable
2020 25089 P342 Spartan Dependable
2020 25090 P334 Spartan Dependable
2020 25091 P212 Spartan Dependable
2020 25092 P324 Spartan Dependable
2020 25093 P346 Spartan Dependable
2020 25094 P244 Spartan Dependable
2020 25095 P234 Spartan Dependable
2021 25098 P326 Spartan Dependable
2021 25100 P143 Spartan Dependable
2020 25097 P113 Spartan Dependable
RESCUES
2009 25026 25027 25028 25029
2009 25030 25031 Spartan 25036 Spartan 25039
2014 25064 R122 E-One E-One
2014 25065 R241 E-One E-One
2016 25072 R413 Spartan ERV 25095 R224 Spartan Dependable 25096 R112 Spartan
SQUADS
2009 28015 S313 Spartan Seagrave
2012 28016 S331 Spartan Dependable 28017 S143 Spartan Dependable 28018 S445 Spartan Dependable 28019 S232
1998 30017 DECON 234 GMC VAN
2005 30031 WT211 Freightliner Dependable 30032 HAZ332 Spartan Seagrave 30035 HMS332 Ford LCF DEL Unicel 30036 HAZ145 Spartan Dependable 30038 A/L 421 Freightliner Dependable 30039 A/L 231 Freightliner Dependable 30044 COM30 Freightliner 30061 MPV341 Ford F550 30062 P552 Ford F550 30065 TR235 Freightliner Dependable 30066 A/L 333 Freightliner Dependable 30067 A/L 111 Freightliner Dependable 30070 Rehab Freightlinter PK Vans 30073 HR332 Spartan Dependable 30072 HR114 Spartan Dependable 30076 HMS145 Isuzu NRR DEL Unicel 30080 FT121 Freightliner E-One 30082 COM10 International Harves 4300 30084 Support 7 Freightliner Bodies 30085 Box 12 Freightliner Bodies 27054 333 Mack/Bronto Lafleure/1200
 BY KEN DE JONG, TORONTO FIRE CAPTAIN, STATION 445 A
BY KEN DE JONG, TORONTO FIRE CAPTAIN, STATION 445 A
This is a series of Q&A articles on Toronto Fire related organizations that can get you more involved in the firefighting community. Some of the best people on the job give back to the fire service and their community in fun and exciting ways. If you find this organization interesting, consider reaching out to them for more information.

This interview is with the President of the Greater Toronto Multiple Alarm Association (GTMAA), Carolyn Wignall. On behalf of all the hungry and thirsty firefighters at multiple alarm fires – THANK YOU TO THE VOLUNTEERS! – for your dedication to (both) canteen trucks!

Ken: What does your organization do and what is its history?
CAROLYN: The Metro Toronto Multiple Alarm Association (MTMAA) was started in February 1975, by Gary Wignall. It started out as more of a social group of fourteen individuals who had a common interest in the fire service. The MTMAA took over the operation of the canteen , now called Support 7, from the Scarborough Fire Retirees as of May 9, 1977 after the Scarborough Council gave it their stamp of approval on the recommendation of Fire Chief Bill Wretham. They had run two ‘unofficial’ calls prior to that date in May.
We are a member group of the International Fire Buff Associates, which is made up of 60 similar groups or clubs around North America. We make a number of charitable donations throughout the year to Camp BUCKO, the Bruce Beauchamp Memorial Fund, TPFFCS Memorial Ride to Ottawa and Toronto Fire Fighters Toy Drive.
CAROLYN: Social media has been our biggest help in recruiting and giving us exposure into who we are and what we are all about. We are on Facebook, Twitter and Instagram and that is where a lot of our prospective members have heard about us. We have active fire service members, fire service retirees and those with a general interest in the fire service, whether it be rehab, fire apparatus, fire service history, photography, communications or just wanting to give back.
CAROLYN: Members are expected to attend our monthly business meetings and club events. There are numerous events that we do throughout the year like the St. Patrick’s Day Parade, Beaches Easter Parade, Toronto Fallen Firefighter Memorial, Ontario Fallen Firefighter Memorial, Fire Prevention events and any other activity Toronto Fire Services or L3888 need us to attend, in addition to fire incidents.
Photo by Larry Thorne Photo by Jeremy ReigberKen: What is your most epic event that you’ve done or you’ve been at?
CAROLYN: Probably the biggest event/fire incident that Support 7 has attended is the Mississauga train derailment in November 1979. Our members were on scene for eleven straight days, serving food and beverage to the emergency services personnel that responded.


Ken: Have you met anyone famous or done any other special events?
CAROLYN: Mostly local celebrities and politicians.
Ken: Is there any training involved?
CAROLYN: Yes, there is training involved. There are rules and procedures that we follow, especially when on a fire scene and when it comes to the operation of the canteen. We hold information sessions for prospective members prior to those individuals participating in club events or at fire scenes. We have a very good relationship with Toronto Fire Services and Local 3888, and we maintain our high level of service to the department and its firefighters.
Ken: Where and when do you meet for meetings and events?
CAROLYN: We hold our Business Meetings at the Local 3888 Union Office on the third Tuesday of each month, except for the summer months.
Ken: Are there any costs that are the responsibility of the members?
CAROLYN: There are yearly dues that our members pay, which includes a subscription to our club’s newsletter, the “Trumpet”. We also have an option for those that are not members of GTMAA to subscribe to our newsletter as well.
Ken: What would you say to someone out there thinking of joining the GTMAA?
CAROLYN: We would love to have you join our group. We have a great group of people that have a love for the fire service and giving back to firefighters…even at 3 a.m. at a 4th alarm fire!

CAROLYN: Come say hi the next time you see Support 7 and our members at a fire scene or TFS event. We would love to talk to you.

Carolyn Wignall, President
Phone: 416-231-3578
Email: gtmaa1975@gmail.com
Facebook: https://fb.com/gtmaa
Twitter: https://twitter.com/gtmaa
Instagram: https://instagram.com/gtmaa.sup7
Photo by Jeremy Reigber Photo by Jeremy Reigber Photo by Mykhail Baehr










We all know that the benefits of sleep far outweigh lack of sleep. We may think that we can manage our sleep depriva tion, though eventually, it catches up to us. Can you relate to being quiet, grumpy, short, and impatient? These behaviours do not leave us feeling good and are felt and flagged by those around us as well. More importantly, it’s the long-term effects of sleep deprivation that we need to be aware of and get a handle on, to be fit for duty and for the road ahead.
Sleep deprivation marks our mood, energy levels, cognitive function, and performance, short and long-term. Who has time for sleep during a busy shift and off-shift hours with a myriad of other to-do items to get done? Science tells us that generally,
 Lynn Sciberras
Lynn Sciberras
between 7 to 9 hours of REM (Rapid Eye Movement) quality sleep is ideal, and while we know this can be challenging, it can also be possible, if there is no sleep disorder. Not taking time to sleep in off time hours is detrimental to our health, so napping, scheduling a sleep pattern, or whatever works to get some Zzzz’s is essential.
Outlined on the next pages are several biological outcomes when it comes to sleep deprivation. Add to this the psychologic al outcomes like being unable to focus and problem solve…the list goes on. Read Michael Sehl’s article to find out how to make sleep one of your top five goals as a shift worker. Your life, and those around you depend on it.

Sleep can be one of the hardest things to fit into our busy lives. There are count less reasons why sleep may be disrupted, including kids, health, work, and fi nancial pressure. It is interconnected, interwoven, and sometimes even in com petition with many of the priorities and values pulling at us from every direction.
Sleep is silently connected to, and impacts, almost every aspect of our health. In fact, “long work hours and chronic sleep loss have been associated with adverse health consequences for most bodily systems.” (Elliott & Keuhl)
This article is not going to be a lecture on why you need sleep. We already know it’s important. This article has 3 goals:
1. To increase awareness of the long-term effects of sleep disruption/depriva tion and its strong connection to every aspect of our health and well-being.
2. To help you choose to re-prioritize where sleep stands in your busy life.
3. To explore ways we can manage sleep as shift workers.

“Chronically sleep deprived people frequently do not perceive their lack of sleep as a problem.” (Elliott & Keuhl) Being that it is a chronic issue, sleep deprivation just begins to feel like everyday life where we consistently walk the line of feeling partially asleep and partially awake. Culturally, exhaustion can even be praised as a status symbol.
“Chronic sleep loss also is associated with a general increase in health complaints and musculoskeletal problems, higher body weights, a greater risk of obstructive sleep apnea and height ened levels of cardiovascular disease and cancer.” (Elliott & Keuhl) These also happen to be the top health risks faced by firefighters.
“Chronic sleep loss can lead to feelings of depression, and the adverse effects on mood may be even greater than those on alertness and cognitive performance. Sleep has effects on brain receptors for serotonin and other neurotransmitters, which are related to mood and memory. Only a few days of sleep restric tion can alter these receptor levels, and a week of restorative sleep is required to reverse the changes. Sleep loss also leads to irritability, a sense of being ‘stressed’ and a reduced sense of well-being. (Elliott & Keuhl) Sleep deprivation leaves us less resilient, less psychologically hardy, and more vulnerable to poorer states of mental health.

Fatigue results in muscle fatigue, slowed reactions, poor judg ment, and reduced cognitive processing of information. Causes of fatigue can include lack of sleep, interrupted or poor quality of sleep (which denies opportunities for protracted deep sleep ing periods), disrupted circadian work and rest cycles, and ill nesses such as sleep apnea. (Elliott & Keuhl)

“Shift work sleep disorder is considered a specific diagnosis because of the frequency with which shift workers suffer from sleep disturbances and excessive sleepiness.” (Elliott & Keuhl)
“Short sleep duration, even after adjusting for other risk factors, increased the risk of coronary heart disease by 50 percent, and interestingly, long sleep duration (more than 9 hours a night) also increased that risk. Comparisons are difficult, but some have sug gested getting less than six hours of sleep per night increases heart disease risk comparable to that of smoking a pack of ciga rettes a day. The stages of deep sleep are times when the heart rate and blood pressure are lowered, and important bodily repair functions may occur. Disruption in that sequence may predispose to hypertension.” (Elliott & Keuhl)
Digestive enzymes are secreted in a cyclical fashion related to the normal daily rhythm, and the different daily patterns and unusual meal times of longer work hours and night shifts may disrupt that normal sleep physiology. These disruptions may explain the up to 6x increase in gastrointestinal disorders, such as peptic ulcers, in digestion, diarrhea and constipation, observed among those with sleep deprivation and night shift work.” (Elliott & Keuhl)
“Strong mounting evidence links sleep loss with obesity and the hormonal changes that result in weight gain.” Ghrelin is a hor mone produced by stomach cells that stimulates the appetite; its level usually increases before meals. The hormone leptin is pro duced by adipose tissue; leptin levels directly relate to the amount of body fat. Higher ghrelin levels stimulate appetite, as do low er levels of leptin. Studies indicate that shorter sleep duration in young, healthy adults is associated with a pattern of decreased leptin and increased ghrelin. There is a strong biological link be tween chronic sleep deprivation and weight gain. (Elliott & Keuhl)
“Weight gain and obesity are associated with development of type 2 diabetes. Short sleep durations more than double the risk of de veloping diabetes.” A study of Japanese workers found that shift workers had a much greater risk of developing diabetes, even when controlling for body weight. Diabetes also is a major risk factor for development of heart disease. (Elliott & Keuhl)
“Shift workers are at increased risk for obstructive sleep apnea (OSA). OSA is a common sleep disorder found in approximately five percent of the general population, but more than 10 percent of shift workers. OSA is associated with obesity, hypertension, diabetes and heart disease.” (Elliott & Keuhl)
Normal restorative sleep is needed for optimum functioning of the immune system; sleep deprivation increases susceptibility to infec tions. Inadequate rest lowers levels of immunoglobulins needed to fight infections and appears to increase levels of inflammatory markers in the blood that have been associated with an increased risk of cardiovascular disease. Sleep loss may activate inflammatory processes, thus explaining the association of sleep deprivation and cardiovascular morbidity. (Elliott & Keuhl)
Identifying a clear link between shift work and cancer is complicated by many other factors including exposure to carcinogens. Nonethe less, sufficient evidence exists such that in 2007, “the International Agency for Research on Cancer (IARC) classified shift work with cir cadian disruption (chrono disruption) as a probable human carcino gen.” (Holderbaum)
A U.S. study that has followed more than 80,000 female nurses (the largest group of U.S. shift workers) for more than 15 years found that nurses working a rotating night shift of at least three nights per month for 15 or more years had an increased risk of colorectal cancer. The risk of breast cancer is also increased among female night shift workers. It is speculated that a disruption of normal daily (circadian) fluctuations in hormone levels is the connection between work hours and malignancies in women. Gonadal hormone patterns among men also have a circadian rhythm, which could be impacted by long work hours and sleep deficits. Male employees with sleep and fatigue problems have shown lower testosterone levels than workers without those problems.” (Elliott & Keuhl)
At night, when most people sleep, the brain is getting rid of its waste, including amyloid-beta, which is a brain protein associat ed with Alzheimer’s disease. The brain only cleans itself of these wastes during sleep; long periods of being awake can lead to an excessive build-up of amyloid-beta.” (Peterson)
• Speak with your primary care physician about annual screening for sleep disorders.
• Regular exercise, including some high-intensity interval training (HIIT). Sleep deprivation has been linked to insulin resistance, which eventually leads to pre-diabetes. Exercise, such as HIIT, can help to improve insulin sensitivity and normalize hormone levels.
•Eat healthy fresh foods and try to reduce your intake of processed foods. For example, some research suggests broccoli sprouts may help clear amyloid beta plaques, reduce cancer risk, and even kill cancer cells.
•Take a daily nap. Naps can, in fact, make up for some of the sleep deprivation that comes with the job. Consider tools like ear plugs, an eye mask or room darkening blinds. Personally, I use Binaural beats theta-wave tracks and a sleep mask to help me doze off in the afternoon.
•Do not eat more than a small snack for about 2–3 hours before bed to give your body time to digest your last meal and to ensure you are metabolically prepped for sleep.
• Create a cool, dark sleep environment.
• Resist using your phone and other electronics before bed. Light suppresses melatonin, a hormone that influences circadian rhythms; blue light, such as that emitted by electronic devices, is especially harmful.

• Get 7–8 hours of sleep on your off days to help combat the nega tive effects of poor sleep on duty.
Are we shift workers doomed to poor sleep and ill health? NO!
We know sleep impacts several interconnected body systems. We also know sleep is remarkably curative and most certainly strengthens our overall resiliency to almost everything the job and life throws at us. Chronic loss of sleep leaves us more vulnerable. With this knowledge, we can choose to prioritize sleep just as we do other healthy habits like food choices and exercise.
Like many, I see and enjoy our schedule as a blessing and wouldn’t change it for the world. Evidence also points to the 24-hour being the best type of shift work, allowing for periods of recovery and rest between shifts, as well as a fairly consistent circadian rhythm, based on daytime wakefulness and nighttime rest.
It is my hope that this article exposes “the other silent killer” that is sleep deprivation/disruption. I wish you all a long and healthy life. May this information allow each of us to make even some small changes that support our sleep, recovery, the support systems we create, self-care, self-compassion, and overall well-being. Thank you and goodnight!

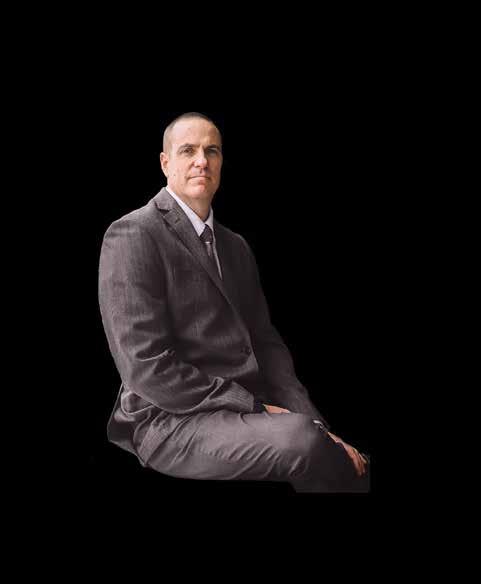
Rose Saunders-Wilson grew up in Milton, Ontario. In 1976, she volunteered at the local hospital as a ‘Candy Striper’. This continued in high school for her co-op placement. After hundreds of hours at the hospital, she was completely convinced that she would become a nurse. Unfortunately, in 1983, she contracted Guillain-Barre Syndrome. This was too much for Milton Hospital to deal with back then, so they sent her to Toronto General Hospital. Before becoming completely paralyzed and in the ICU for months on a respirator, she signed on to a study out of Washington D.C. to study this virus. The study assisted with major decisions on her treatment, as well as with her medications and blood
products. “Thank goodness for that, because this process involved six plasmapheresis procedures, and at that time, there was a tainted blood scandal with contaminated HIV+ blood.”
After months in hospital, she returned home to continue her recovery, where she then relearned how to sit, use her hands, and walk. “It was traumatic for sure. I missed entering college, and with wearing leg braces (foot drop splints), mobility was a bit of an issue!” Her recovery was nothing short of miraculous. “On my first visit back to Toronto General to visit my neurologist, I wore nice low heel shoes and a dress. She cried, and so did I. It was magical! It would be years before I would return to my dream of nursing. As it turned out, it took twelve years, almost to the month.”
In 1991, Rose was driving and saw a person lying on the sidewalk. She pulled over and ran to him. There was a pharmacy bag beside him so she flagged down a passing car and asked them to take the prescription to the pharmacy, to call 911, and also to return with some information about this man. Cell phones were rare back then.
He was wearing a medic alert bracelet that said he had epilepsy. A woman ran across the street and told Rose she had called 911. Rose had rolled the man into the recovery position and the woman said, “I’m so glad that someone from the ambulance was here.” Rose answered, “I’m not, but what a great idea!”
And so it began. At that time, Rose was a divorced, single mom, working as a waitress. She returned to adult learning to finish her advanced science courses, and she successfully challenged the entrance exam for Humber College’s Ambulance and Emergency Care (EMCA) program.
While taking the science courses, she also signed up for the Halton Hills Ambulance Volunteers. They put her through the Ministry of Health & Long-Term Care programs, to qualify her to work part-time on an ambulance.
In 1993, she started at Humber College’s EMCA Program and did her preceptorship/mentorship with Streetsville Ambulance (now called Region of Peel Paramedic Services).


While still in paramedic college, a job opportunity was posted for the City of York Fire Department. Rose and a few of her classmates applied for the positions.
During her college ride-out, she was hired as a Paramedic, as a part-time employee. Only part-time, because of her Ministry Certificate Qualification for EMCA was still pending. Rose says, “This was such a satisfying profession and I loved every moment of it. Dropping patients off at hospital emergency rooms and not learning their outcome most times was frustrating though. I wanted to know and do more!” After graduation, she enrolled in the Humber College Nursing program to fulfil this desire.
In 1995, near the end of her first year of the Nursing Program, Rose received a letter from the York Fire Department. They invited her to participate in the first phase of their testing, which was the written exam. The Head Nursing Instructor called Rose into her office, where some of the other senior instructors were present. They all agreed that this was an opportunity that should not be missed, so she accepted the invitation.


“The test write was very intimidating. At 31 years old, and looking at all my young male competitors, I was wondering what the heck I was thinking. Well, it turned out that I ROCKED the test and got a phone call congratulating me and inviting me to a physical assessment at York University. After I passed the physical, there was an interview. When I received my employment offer, I needed some time. Time to think about my future, my current situation, and this decision that would affect my daughter and myself. What is my “best” choice? I was working on an ambulance with one of my best “life” friends. She asked me to step out of the ambulance, and then she locked the door. She picked up the microphone and through the bumper mounted loud speaker, she yelled at me, YOU IDIOT! CALL TOMORROW AND TAKE THE DAMN JOB! June 5th, 1995 was my first day as a recruit firefighter at the City of York Fire Department.”
“Station 421 was such a thrill, with a Pumper, Aerial, Chief’s Car and Squad. The dinner table and station antics were all new to me. We trained on everything. For swift water rescue and ice water rescue we had to pass a swim test. This was done at the York Memorial Collegiate Institute pool. The task was to swim ten laps of the pool. The whistle blew and we all dove into our lane choosing front crawl, because it is a powerful stroke and will polish off these easy ten laps in less time. While pushing through the laps,
I could look down the lanes and see everyone else doing the front crawl. After five lengths, I was feeling like I might drown if I didn’t flip over and do an easier stroke. Gasping, while now doing the backstroke, almost every guy flipped over too. Afterwards, they said they weren’t going to flip over until I did!”
The opportunity to teach was offered by the medical section of the newly amalgamated TFS. Rose jumped in and began by recertifying defibrillation and first aid to on-duty staff. Firefighter Chris George, who also ran Humber College’s firefighting course, enjoyed her course so much that he offered her a teaching position at Humber. Rose found so many opportunities at Humber to use her recruitment skills to encourage these students to apply to TFS. She still gets reminders from TFS firefighters who learned from her at Humber. As an Acting Captain at Station 413, she met a firefighter who fondly remembered a lesson she taught at college regarding the role that hemoglobin played in carrying oxygen throughout the body. Rose says, “Teaching is such a privilege! I’ll never underestimate the importance of doing your best to help everyone understand and learn.”
From 1999 until 2002, Rose accepted a secondment into Recruitment and Outreach. After six months, the position was given the rank of Captain, and she competed successfully for this position. She felt it was an amazing opportunity.
Rose also joined a ‘speakership’ and mentorship program through ‘Women In Motion’. She was partnered with a young woman once a month at a brunch that also involved weekly follow-up phone calls and visits. “She was not looking to become a firefighter, so my goal was to network with powerful women at these events and partner her up with them. They could help her with all of the amazing contacts and the opportunities they had available to them.”
It was during this time that Rose also became part of the EAP program. This gave her the chance to give back within the fire service. Often, years after retiring, members would reach out to chat, or ask about how to move forward with a referral for one of the many services EAP has access to.


Rose also conducted speaking events with high school women, multiple times a year. Through this partnership, she ran one of the first live web high school broadcasts, with an online question and answer period.
Part of her outreach work was to find new locations where people may not see themselves as possibly becoming a firefighter. They could hear her story, and hear about Toronto Fire’s other amazing options beyond Operations, such as Fire Prevention, Communications, or Mechanical. Rose could show them that even with tough entry criteria, women have been showing up and doing well. “I am so proud of anyone who heard my words and came in for the challenge and made it happen.”
“In partnership with the Canadian Armed Forces, Toronto Police Services, Toronto Paramedic Services, Corrections Canada and Markham Fire, we hosted the largest uniformed job fair in Canadian history. It was magnificent! There were military vehicles and emergency service vehicles everywhere. The posters were plastered on billboards throughout the city. It was an amazing success!”
In 2012, Rose wrote for Training Captain, and in December of 2012, she went into the training division EMS section. It was short lived though. They had a reduction of staff in training and nine officers were returned to the sections they had come from. Last into the section - first out.
In 2013, she went to Station 424, Runnymede Hall. This was her first time to be stationed in a single vehicle hall. Her Captain was an amazing mentor and made sure to put her in the front seat as much as possible to prepare her for her fast approaching position of Acting Captain. This station was closed for operations staffing, so they were all transferred. She went to Station 411 for a few months until being designated
as an Acting Captain.
In 2014, Rose was promoted to Acting Captain at Station 413, with Scott McLaren as her Captain. You would be hard pressed to find a Captain as dedicated to the Honour Guard and to the dignity and honour of that position. He has encouraged others to join and share his passion. This station had just been reduced to a one-truck hall. She split her time as an Acting Captain between 413 and 411. Both stations have their share of high impact vehicle collisions, fires and medical calls. “These incidents stretch you. The crews you work with are your foundation and together you are a team.”
In 2019, Rose joined the Designated Officer program. “In the D.O. program, we would respond to on-duty incidents of all reported exposures to communicable disease, such as COVID. This office blew up when the pandemic hit Toronto. The Designated Officer team was learning as we moved forward. It was evolving with the virus and the conditions to which we were all exposed. There were hours of phone calls, and contact tracing reports.
This also led to the opportunity for Operations staff that have a medical professional background (Nursing/ Paramedic) to represent Toronto Fire Services as Vaccinators at mass immunization or mobile vaccination clinics. Using vans and support staff to do patient data entry, with Public Health preparing medications in shelters, drop in centres, soup kitchens and encampments throughout the city. Rose confesses, “My well known secret is that these mobile clinics were my greatest pleasure. Such amazing people, both those who work there and those who visit. They share everything. Their histories and their secrets.”
On May 12th, 2016, we lost TFS firefighter Sara Rosen. This tragic event affected Rose, as she saw this powerful, intelligent firefighting woman taken before her time. Her response was to work with other female fire fighters to ensure Sara was seen and represented. Cathy Smyth and husband Sean, Susie Opie, Stacy Hannah and Rose worked diligently to host the first ‘Sara’s Ride’. “Participating in the organization and hosting of this ride was so healing, and the turnout was phenomenal! Sara’s family attended and gave the participants their blessings. We needed this healing.”

Rose joined the Positive Space Committee in 2016, to try to step in wherever Sara had been working. They assisted with the Pride Parade and other Emergency Services Pride and LGBQ2+ activities.
In 2021, Rose became the Station 443 Captain. COVID continued, and she still spent hours at Vaccination Clinics and in the DOCC. She has fallen asleep at 0300 with her fingers on the keys of the computer she had been working at since 0630 the day before.
Then, an opportunity arose that Rose never knew she wanted. “I was eligible to write the District Chiefs Exam! During the Covid chaos that had become a constant in my life, I chose to write. It was the toughest promotional process of my career. First, we had to successfully complete the entire HAZ 1072 course. Then, along with many worthy candidates, we faced the written exam, and then the oral exams.”
“WHAT? I PASSED? Now I see my name on the Acting District Chief’s list.”
“I’m so blessed to have so much support. So many people went out of their way to listen to me practice my High Rise spiel for the oral portion of the test, and they encouraged me to study, when all I wanted to do was sleep.”
Rose would feel remiss if she did not mention the fine female firefighters and Captains that came before her. “These are strong, amazing leaders who paved the way for all of the opportunities I was able to compete for. To them, I am grateful. In life, sometimes you need to see one to be one, and lead by example.” Rose is an excellent example of continuing to demonstrate this example for future firefighters!
Rose states that she draws on the constant strength and support of her family at home. Her husband of 25 years Billy Wilson, her daughter Kayleen, and her son William provide this support for her.
“I feel extreme job satisfaction as I hit my 27th Anniversary on June 5th 2022. Who knows what tomorrow will bring, but thanks to some nurses, and a strong Paramedic sister back in 1995, I gave firefighting a shot!”
“BEST, DECISION, EVER!”






For the regular readers of Firewatch and, more particularly, of our retiree article, you have noticed that our content generally covers a pretty wide scope. Generally speaking, it’s because of our audience. Our audience is as wide ranging as you can get. Sometimes it is difficult to actually choose what our content will be. We try to be as timely as we can and include topical information based on the questions we get asked through our various social media platforms. It’s important for all of us to have established some kind of social media presence. For those who run in the other direction when it’s mentioned, please read on while we explain why. The time has come that our Pensions and Benefits have moved beyond the singular use of the telephone. Sure, you can still call in and ask questions, but, dealing with claims now requires at least an email address. In order for our 3888 Benefits staff to assist in a denial of service, you need to find the 3888 webpage and select the Concern button. It’s the only way to get into the queue and to ensure that you get a timely reply. Further, it’s better to have an electronic copy of the documents you will need to support your “Concern”. This all might appear daunting to those who are not a fan of the electronic age, but it’s really not. With some help, you will get your claim processing done more efficiently.
“Do you need a computer for this?” is a commonly asked question. No! All this can be done now using a smart phone or a tablet. Many of our members have migrated to a tablet, because of vision and dexterity issues, plus it’s easier to see pictures sent by family. None of this is complicated. The only things required are some familiarity with the endless menus and a bit of patience. Some RTFFA executives have met up with a few members at the union office (also a local Tim’s) and have provided some help. This is going to be an on-going process, so if you need help, just ask. Note! If you want your OAS/CPP to be “Directly Deposited”, you will need to login to the CRA page and follow the instructions! This also requires a social media presence.
Those who have recently attempted to get information from the city will have noticed that the process has changed. In the past, we used to be able to contact them by phone, or on the web, and chat with one of our designated contacts directly. Going forward, you will be re-directed to a group called “Team Central”. You will get a reply that looks like this:
“If you are a CURRENT/Former employee, please contact TEAM Central to make your request at 416-338-0016 or through a web form online at insideto.toronto.ca/teamcentral (if you’re on the City network) or www. toronto.ca/teamcentral (if you’re not on the City network).” Once you navigate the various menus, you should get what you’re looking for.
A few issues ago (Summer 2020), our article covered the information a member might need when considering retirement. It was designed to be a “Pre-Retirement Checklist”. The article centred on your 65th birthday and the significant issues that surround it. It covered the issues of Old Age Security (OAS) and Canada Pension Plan (CPP) very briefly. Your author is on that precipice and thought it pertinent to share some insight. One month after your 64th birthday, you should receive two ominous looking Canada Revenue Agency (CRA) envelopes. Don’t panic! They look like tax reassessment letters, but they are not. These are really important; you must read them carefully and keep them. If you are not financially literate and use a tax service or accountant, forward these letters to them when you get them.
Both of these forms contain personal information, so treat them with some care. Further, they will have your client numbers and CRA contact info. We will share a synopsis of both of these forms:
Old Age Security (OAS)
We are pleased to inform you that your Old Age Security Pension should start one month after you turn 65.
Your estimated pension is the current maximum Rate of “###.##” each month.
This amount is taxable and may increase based on inflation
Your pension is scheduled to start automatically based on the following information:
1. Your year and month of birth are 19##-##
2. You are a Canadian citizen or are a legal resident of Canada
3. You have lived in Canada for at least 40 years since the age of 18 Canada Pension Plan (CPP)
Your Pension at a glance – Is it time to apply
You are receiving this letter because you contributed to the Canada Pension Plan (CPP). You may qualify for the CPP retirement pension.
The CPP retirement pension is paid monthly and is taxable income. You can receive it even if you are still working.
Here is some important information about the CPP retirement pension
It includes a personalised estimate of your monthly pension.
When is the best time to start receiving your CPP retirement pension. It’s your choice! The longer you wait, the more money you will get each month. You can start any time after you turn 60. But there is no financial advantage to waiting past the age of 70.
The best age for you to start your pension depends on your own situation.
Your health, finances, and retirement plans all play a part in that decision. This is just a synopsis. Remember that the bridge ends ($1000+-) on your 65th birthday and some may opt to use OAS and CPP to replace it. These forms, in their entirety, will be shared on our Facebook page in the coming week, so those who wish can see what to expect.
In closing, as the summer season is upon us, I’m sure that most recognize our collective hesitation to jumping into an actual vacation. We’re all still working our way back into the world with apprehension while still watching and interpreting “the numbers”. Many of us have had and perhaps are facing Covid head on, and on a positive note, are weathering the illness with success due to our vaccination status. Take this opportunity to get away this summer. Take a breather, see new sights, get some air.
YOU WON’T REGRET IT! As always, we continue our collaboration with all the groups mentioned in our last article.
Our last word, again, goes out to you, all the members of our TFS Family. Runs are still occurring and fires are still being professionally extinguished. Applause all around!
The RTFFA will continue to keep all of you updated on our activities. We couldn’t make the spring meeting happen. We are now aiming to resume our membership meetings sometime in the fall, and we will keep you posted. Keep your fingers crossed! The Fall Meeting will include our General Elections!
Our membership drive is continuous; if you’re interested in becoming a member, feel free to contact us at active.retired@torontofirefighters.org. The dues ($25.00) are payable annually on the 1st of May.
Come join us, and remember to follow us on social media, we post every day:
On the Web - https://www.retiredtorontofirefighters.org/ On Facebook - https://www.facebook.com/TFSRetirees On Twitter - @TFSRetirees
Be well and stay safe.
President Alan Thomas - Secretary/Treasurer Chuck West - Alan Hall - Paul Halls - Ron Coates - Al FalknerThe following is a list of “life hacks” for the firehall which has made my career a little easier. It is by no means a complete list, as I am always learning and adding new ones.
When working at a new hall, on a callback or after being off for some time, do a circle check of the truck, opening and visually checking all cabinets. Don’t rely on the driver to tell you where everything is; make your own mental notes of where important or heavily used equipment are located, such as the medical gear, hi-rise equipment, and forcible entry tools.
BY TPFFA EDUCATION COMMITTEETalk to the other individual on the back and have a plan of who does what for common situations. For example, at a VSA, the senior individual starts doing compressions while the junior individual sets up defib pads. For first-in hi-rise alarms, discuss who carries what, and who will do elevator control. For car fires, perhaps the senior individual pulls the trash line and flakes it out while the junior individual dons their SCBA and takes over the nozzle. These quick conversations can help develop trust and improve efficiency.
Organize and be in control of your personal protective equipment at all times. This is very easy to do, and it starts with creating a home for your PPE. For example, I always keep my flash hood in my right coat pocket, gloves in my right pants pocket, eyewear protection around my waist, wedges in left pant pocket etc. This way, I don’t need to look for anything when I need it. I’ve noticed that the recruits at the Toronto Fire Academy all have an identical, neat and organized way of placing their PPE on the ground so that they can rapidly don it and easily see all their items.
Read and be aware of local news. This is good to do, especially if you are driving. Some halls have a local newspaper, which has news relevant to those who work in the area. For example, in the Beaches, we have the Beach Metro News (Ward 9 news). This can help drivers be aware of events or road closures.
Read one or two FCCs daily, and always stay up to date with new ones. This is especially important when studying for the promotional exam but knowing FCCs will also make you a better firefighter. Reading a few a day will make studying, when the time comes, more manageable, and will give you the ability to win debates and impress other firefighters by dropping sources.
Learn more about your area by sampling local cuisine. Toronto is a very diverse city with many places for takeout. Treat yourself sometimes and learn about your area. This will also improve mental health!
Organize your pump panel in a familiar way when driving. I am a visual person, so when driving, I always arrange the pump panel so that the discharges are pointing in the direction of the nozzle. That way I can quickly see a visual map of where discharges are located when lines are pulled off my truck by other firefighters. I was showed this simple hack early on by a senior firefighter. Just remember that some discharges lock when placed in the vertical position, so you will need to reposition them when operating them.

Avoid expressing your “views” at the workplace. Firehalls are dynamic places with people from all backgrounds and lifestyles. Perhaps, similar to family gatherings, it is usually not a great idea to share your controversial opinions or feelings on politics with your crew, as it can land you in “hot water” with them. Instead, keep the topics light and non-polarized, and save the arguing and name calling for the internet (but don’t cyberbully).
Place a dog water bowl outside of the hall and change the water daily. This will win you the respect and admiration of the public and give you opportunities to casually interact with them. You get bonus points if you keep dog treats on hand, but always ask permission before feeding another person’s dog a treat.
Consider exercising or doing mobility exercises at work. We are very lucky to have the ability to work out at work. Our health is our most important investment. If you don’t want to do a full workout, consider doing some stretching or mobility training for injury prevention. Focus on the three most commonly injured areas for firefighters: back, shoulders, and knees.
Develop and pursue hobbies outside of work. This is a wonderful job, but don’t let it become your personality. Have interests and things to do that are unrelated to firefighting. This will prevent you from becoming burned out, but also clear your mind and give you outlets for stress. These will be different for everyone, but my top five are boxing, running, sailing, drawing, and volunteering with animals.
The
November 17, 1991 Acting District Chief Brian G.H. Kirby
April 30, 2019
January 30, 2019
May 15, 2019
Captain Gordon W. Crawford
Firefighter William B. Gibson
Firefighter Edmond F. Lynch
September 12, 2019 District Chief Paul Dzuba
November 3, 2019 District Chief Herbert Hammond
November 24, 2019 District Chief James (Jim) Ritchie
December 20, 2019 District Chief Karl Dieter Bertram
June 26, 2019
January 16, 2020
February 21, 2020
Captain Gregory A. Simerson
District Chief Wayne Elford
Firefighter Roger Martin
April 25, 2020
Captain Victor Patrick Kelly
May 4, 2020 Firefighter Glenn Grieve
June 19, 2020
August 11, 2020
Firefighter James Duffney
Captain Gary Campbell
November 4, 2020 Firefighter Robert A. Chalmers
February 20, 2021 Acting Platoon Chief Glenn Sherwood
June 14, 2021
August 11, 2021
August 17, 2021
May 2, 2022
Harry Causer
Robert Burrows
David Conner
Donald Bruce
Frank William Lenard Merritt
Fraser Thomas
Stanley J. Barr
Ernie Thompson
Leonard Alfred Benstead
Ernie ‘Tanglefoot’ Alston
John Monroe Stevenson
Ronald D.
Fire Fighter William James Luscombe
Stanley Edward Arsenault
April 5,
April 7,
April 8,
April 11,
April 16,
April 18,
April 24,
April 24, 2022
April 28,
May 2,
May 3,
May 7,
May 8,
May 12,
Patrick Newman 20,
Ronald Callejas
Frank Edward Whitaker
Gary R. Magill
Evan Boyd Sherwood
Norman Joseph
James ‘Jimmy’ Ross Dale
John ‘Jack’ Henderson
Philip Currell
Colin Charles Clive
Charles Edward Sidney Hodges
William C. Wilson
Captain Johnnie Walker
Captain Daniel Thompson
Captain Martin Costoff
Firefighter Ted J. Szabunia
June 4, 2022
June 5, 2022
June 10, 2022
June 11, 2022
June 13, 2022
June 22, 2022
June 26, 2022
June 27, 2022
July 4, 2022
July 13, 2022
July 17, 2022
George Keith Milling July 31, 2022
Edward John Butler
Dennis Bugden
Stan McKelvey
July 31, 2022
August 7, 2022
August 29, 2022
They shall grow not old, as we that are left grow old; age shall not weary them, nor the years condemn. At the going down of the sun and in the morning, we will remember them.
Ted was born on December 25th, 1959 and was hired by the TFD at the age of 37, on August 22, 1997.
Brother Szabunia was a very proud fire fighter and proud to be of service to his community throughout the duration of his career. Records show Ted was stationed at 424 on P424 D platoon until 2014, then transferred to P233 D on April 21, 2014, thru to March 8, 2015. Effective on March 9th of that year, Ted was assigned to A215 A platoon, then transferred to D platoon on A215 January 25th, 2016. He found great joy in helping those around him and working with a team who he could connect with and rely on. Sadly, at the age of 62, we lost our brother to brain cancer on May 2, 2022. In honouring brother Szabunia’s wishes, we was be laid to rest in Peterborough for his LODD ceremony.
Brother Kelly was a proud fire fighter who was looked up to as an example from his peers. He was a member who exhibited great confidence and leadership. He was known to make those around him feel safe and comfortable. He was always willing to help and devote his time and efforts to the communities of Toronto.
He was a devoted women’s softball coach and honourable retired Captain of the Toronto Fire Department serving the public for 35 years were a few of his greatest achievements. Throughout the duration of his career, he devoted everything to being the best fire fighter that he could be.
In Honour of Toronto Fire Captain Victor Patrick Kelly, a Memorial Plaque will be hung at a TFS Station.
Fire Fighter Jayson Tibor Pal November 20, 1972 - June 11, 2022

Fire Fighter Traci Cairns May 26, 1969 – August 30, 2022

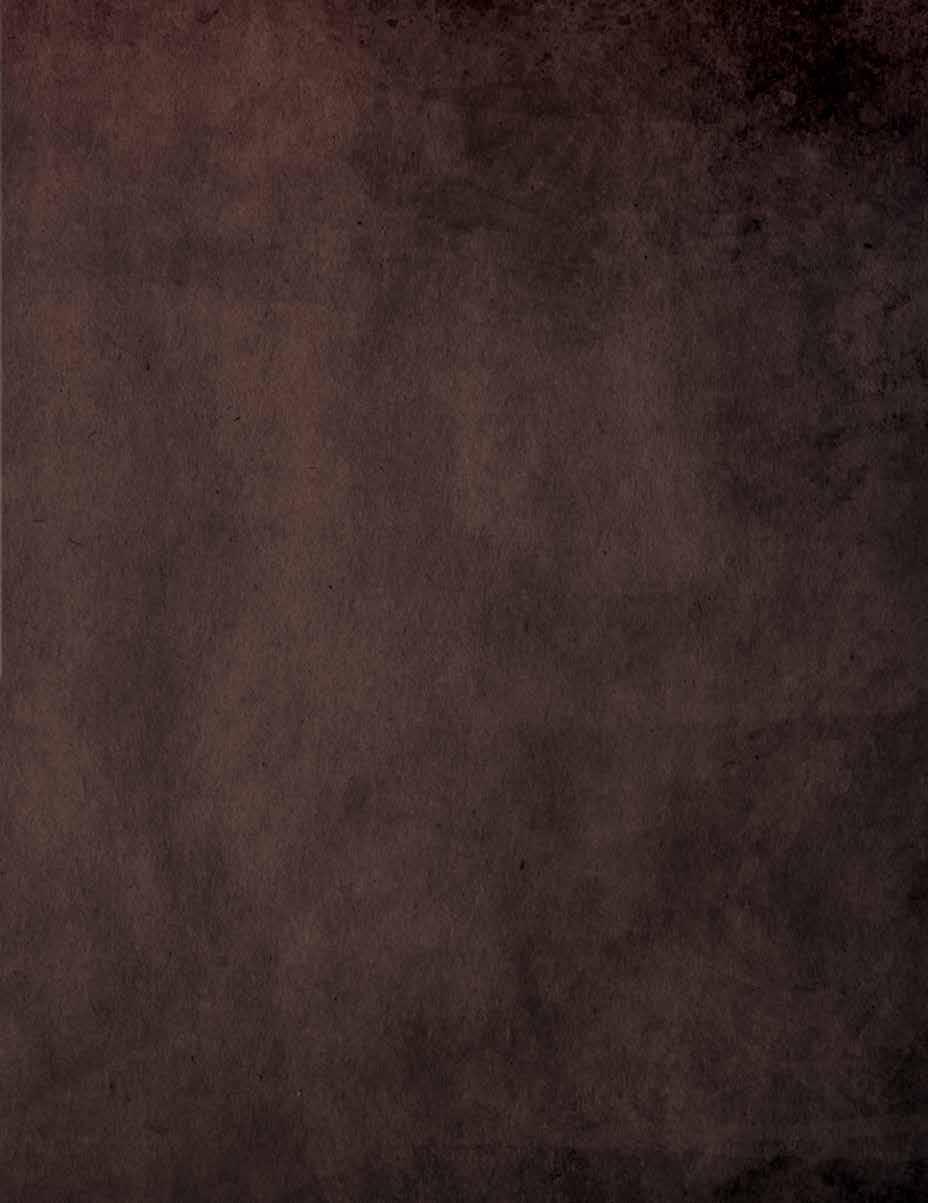 In Honour of Fire Fighter Ted Szabunia, a Memorial Plaque will be hung up at TFS Station 215.
Toronto Fire Captain Victor Patrick Kelly, peacefully passed away on Saturday, April 25, 2020 after a prolonged battle with Lung Cancer at Brampton Civic Hospital.
In Honour of Fire Fighter Ted Szabunia, a Memorial Plaque will be hung up at TFS Station 215.
Toronto Fire Captain Victor Patrick Kelly, peacefully passed away on Saturday, April 25, 2020 after a prolonged battle with Lung Cancer at Brampton Civic Hospital.
Be it through direct pressure, where you’re applying force directly to the injury, or indirect pressure, from occluding the artery above the injury. We do this with our hands and with tools, and we do this quickly and aggressively to save every drop of blood. If we do not act quickly, patients can die within 5 to 10 minutes.
Major hemorrhage is one of the leading causes of preventable death. These lessons were made clear in battlefield studies, but are now being highlighted in the public sector. This is why St. John Ambulance has added tourniquets to its basic first aid course. Sunnybrook has instituted a Stop the Bleed program, and there are now 2 tourniquets and 3 packs of hemostatic gauze in every fire truck within the City of Toronto.
Prior to joining the fire service, I served in the Canadian Forces as a Medical Technician for 12 years. I was selected to the Special Forces in 2014 and have been trusted with the honor of teaching tactical medicine all over the world. I made the transition to Toronto Fire Services in July 2021, and hit the trucks in late November as a probationary firefighter, into what was to be the fourthdeadliest year on record for Toronto. As of writing this article in mid-March, there have been 84 shootings in the city since the start of 2022.
I joined the Local 3888 EMS committee because I hoped to use my prior experience to help my fellow firefighters take some lessons learned from military medicine. The theory and skills are the same in the city as they are in the field, and the area where we can make the biggest difference in terms of preventable traumatic death, is with major hemorrhage control.
When losing significant blood volume, consider the components of blood and the impact it may have to any chance of recovery:
• Red blood cells carry oxygen to the tissues. Shock is a state of de-oxygenation in the body, so less red blood cells mean less oxygen, which means less perfusion to the brain.
• White blood cells fight the potential infection from the introduction of bacteria through the open wound.
• Platelets form the clots that close the wound, and medical research has shown us the first clot is the best clot.
• Plasma provides the volume that keeps the arteries full, which allows the heart to move fluid.
Though emergency responders focus on the A - B - Cs for all medical calls, the military has adapted its response for traumatic patients. The acronym that’s used within the Canadian Armed Forces is MARCHE, which was taken from the Tactical Combat Casualty Care. If we contrast AirwayBreathing - Circulation vs Massive Hemorrhage - Airway - Respirations – Circulation – Hypothermia/Head – EVAC/ Everything else, the only difference is the critical importance of immediate arterial hemorrhage control. The application of direct pressure and indirect pressure takes precedence over everything else. Just think of it as C – A – B.
Our ability to stop arterial bleeds is focused on two areas: axillary and inguinal, which means the limbs and where the limbs meet the body. Injuries that are in the head, torso, abdomen and pelvis limit our ability to apply pressure; you cannot place a tourniquet around someone’s chest, nor can you pack enough gauze in someone’s belly to apply enough pressure to occlude an internal bleed. Injuries in the arms and legs, and those in the shoulders, groin, buttocks and neck are much more manageable at our level. We treat those injuries with pressure.
The first steps in controlling a high volume/high flow bleed are the immediate recognition and application of direct pressure and/or indirect pressure.
Tourniquets work.
Packing can be effective. Pressure stops bleeds.
Using gloved hands, place as much weight as can be tolerated overtop the area and try to compress the severed arteries inside.
Sometimes feeling a pulsation can be difficult, but stemming the volume of blood buys a significant amount of time for the application of a tool. If direct pressure can’t be used, shift to indirect pressure by occluding the brachial or femoral artery by applying pressure in the regions where you would access those same pulses. Whoever is holding pressure should remain in place while the partner removes any barriers (like clothing) and gets the hemostatic gauze or tourniquet ready. Be sure to practice this in teams because applying a tourniquet by yourself is different than working around a partner. The person applying pressure only removes their hands when their partner is confident that the adjunct is in place properly and they do so slowly to ensure the intervention is effective. We do this as quickly and efficiently as we can.
One of the strengths we have as a fire service is our team based approach. Even if two firefighters move together to stop a major bleed, another member can simultaneously assess the airway and breathing. The bleed may be one of many critical problems and what we should strive for is concurrent competent care.
Without rehashing why the A - B - Cs (or A - R - Cs) are important, I want to take a moment to illustrate why the military has an “H” for Hypothermia. Simply - cold kills. Specifically in terms of blood loss, there is a mechanism known as the “Lethal Triad”, a cascading effect of Hypothermia, Acidosis & Coagulopathy (the ability to form clots). The concept is as follows:
1. The human body should be around 37 degrees Celsius. Blood is that temperature. When there is a loss of blood, that warm fluid and its nutrients are now not circulating in the body. Without it, the body becomes hypothermic.
2. The body forms clots most efficiently when it is in a state of homeostasis. When hypothermic, coagulopathy becomes compromised. When clots can’t be formed, the body will bleed more.
3. In addition to that, without the oxygen and nutrients in blood, the body becomes acidotic, another condition affecting homeostasis, which in turn affects clotting.
4. This means more bleeding.
5. This causes further hypothermia.
6. This causes further acidosis.
7. And so on, until death.
If wounded soldiers in 40 degree weather in Iraq can become hypothermic due to blood loss, so too can our patients here in Canada. Once you have concluded your critical interventions, your next focus needs to be warmth for the traumatic patient.
That means:
1. Get the patient off the ground if possible
2. Use the emergency blanket in our first aid bags
3. Offer to turn up the heat in the back of the ambulance
• Full amputations should always get a tourniquet. The initial reaction the body will have when a limb is severed is to have the arteries retract into the muscle and have the area compress them closed. This is why there may not be an initial presentation of large volumes of blood, but as the body relaxes (or is unable to maintain that compression), a large deluge is possible. In this aspect, it’s better to be proactive than reactive.
• Review “cavitation” in regards to bullet wounds. The space you’re packing into may be much larger than what you thought when looking at the size of the bullet hole. Remember that packing needs to be compressed in place for 3 minutes and then secured in place with a pressure dressing.
• Always look for an exit wound when applying a tourniquet or packing an injury. When in doubt, place a TQ “high and tight”.
• Remember that these interventions are painful to apply. Constantly recheck your tourniquets and packing to make sure they are still working. Patients that have a reduced level of consciousness, or that have been given medication, may try to remove it. Always recheck any intervention after moving the patient. Recheck does not mean tamper with: if it’s working, let it work!
One of the most important considerations that can be made in regards to the application of pressure is that it may not be 100% effective. Likely, if you’re only using manual pressure, and even after using a device, there could still be blood coming from below the tourniquet from the tissues or bone marrow, or there still could be blood soaking through the packing. What’s critical for us to remember as firefighters is through that pressure, we’re kinking the hose. EMS is on the way and there is a hospital within 10 minutes in any direction. If the best you can do is a 90% solution, that could still mean the difference between 50cc vs 500cc spilled on the floor. Hold it and keep it there. Get someone to put their hands on your hands if you get tired. Do whatever it takes. Given how quickly we respond to calls and our close proximity to trauma hospitals, the seemingly simple act of recognizing the bleed and holding pressure until help arrives might be the difference in saving a preventable traumatic death.


reaction after comprehensive clinical evaluation (Mendez 2021). The patient will know if they experience an Idiopathic Allergic/Anaphylactic response as this is a diagnosis after testing. Exercise Induced Anaphylaxis is rare. This type of anaphylaxis, with research, found that exercise is usually a cohort to a food born allergen. The individual food may not trigger an allergic response, but exercise afterward may lower the response threshold, reverse any built tolerances, and may increase the severity of the allergic response to anaphylaxis (Christensen et al 2019).
Anaphylactic events often bring forth treatment and assessment questions. These responses are low frequency but high acuity events, and with that, high stress. We, as firefighters, strive to successfully assess and treat patients, despite everchanging conditions. It is always good to refresh not only how we assess and treat patients, but why we utilize the tools we are given, and what these tools do. This article was created to assist firefighters and to increase our knowledge of epinephrine and our comfort level when responding to anaphylactic emergencies.
Anaphylaxis is defined as a severe, systemic, hypersensitive reaction that can be characterized by rapid onset of potentially life-threatening symptoms (Christensen et al 2019). The signs and symptoms of an anaphylactic event will range depending on the body system involved. The most common signs of anaphylaxis are angioedema (swelling), urticaria (hives), erythema (rash), and pruitus (itchiness) (Fischer et al 2018). Anaphylactic emergencies include vasodilation/ vasopermiability, which decreases blood pressure, respiratory issues of tracheal membrane swelling, and mucous production creating dyspnea (shortness of breath). In general, a patient will know the exposure that has caused the allergic reaction (i.e. insect bite, food allergen, etc.).
There are occasions where an anaphylactic reaction began due to exercise or with no known exposure. These are categorized as either an Exercise Induced Anaphylactic Reaction or an Idiopathic Anaphylactic Reaction. Idiopathic Anaphylactic Reactions are often physicians’ diagnoses when no other identifying allergens trigger a
Why is Epinephrine the drug of choice to combat an anaphylactic attack? It’s a naturally occurring hormone in the body. When administered to the body at different solutions and dosages, Epinephrine will implement certain hormonal reactions, which in turn, will create action in the bodies systems.
Specifically, epinephrine administration stimulates receptor sites. These receptors are known as B1, A1, and B2 adrenergic receptor sites (we will never need to memorize this)! The importance comes with what these receptors do when stimulated. Relaxation of the smooth muscle of the bronchial tree will decrease mucous production and tracheal swelling, to ease breathing (EMC 2022). Cardiac stimulation will increase heart rate and blood pressure. Contraction of the skeletal and vascular smooth muscle will also increase blood pressure and decrease the fluid moving from the blood vessels to interstitial spaces (space between the blood vessel and cell). Decreased interstitial fluid reduces swelling, hives, rash and other visible skin affects (EMC 2022). Everything an epinephrine dose does
STEVEN ROBBINS ACTING CAPTAIN, STATION 434-C DESIGNATED OFFICER, IMS ATI, EMS COMMITTEE MEMBERcounteracts what anaphylaxis is (swelling, low blood pressure, breathing issues etc.).
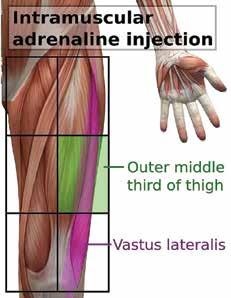
It is important to remember that these effects of epinephrine administration are rapid (5 minutes) but will only last 15-20 minutes (SWORP 2022). This is why any patient that receives an epinephrine dose (Epi Pen) must be transferred to paramedic care (Sunnybrook 2021).

Better understanding anaphylaxis and epinephrine can now assist us to understand the Toronto Fire Service (TFS) Medical Directive application of epinephrine for anaphylactic patients. TFS utilizes epinephrine solute of 1/1000 with an adult dose of 0.3mg and a dose of 0.15mg for patients under 20kg/44lbs (Sunnybrook 2021).
Exclusions/Contraindications - in a life-threatening anaphylactic event there are NO ABSOLUTE Contraindications. (Sunnybrook 2021)
One of the most important things a fire crew can do during a medical emergency is a thorough and methodical patient and scene assessment. Especially when administering a drug!
When assessing for anaphylaxis, look for the signs of hives, swelling and discolouration around the face. Assess the airway, look for swelling of the lips and tongue, listen (auscultate) for stridor (high pitch whistle/ squeak) in the upper airway or silence of air in the lower airways. Is the patient nauseated, vomiting, or experiencing stomach/gastric issues? Observe the overall total appearance of the patient; ask about the exposure, dizziness, light headedness (obtain and record a blood pressure), weakness, anxiety level, and the responsiveness of the patient. We have learned this assessment pneumonic as FAST.
• Face
• Airway
• Stomach
This can be incorporated into the primary assessment after always methodically performing a scene survey (EMCAP), the patient level of responsiveness (AVPU) and the critical assessment of airway, breathing, and circulation (ABCs). Note that a patient with a history of poorly controlled asthma may increase the severity of an anaphylactic response. Thorough patient investigation aids in obtaining this information.
Conditions
Over 50 % of Toronto Fire Services call volume is medical related. While anaphylaxis is less common overall, it is truly severe when encountered. Understanding what is happening to the body systems during anaphylaxis, and how epinephrine counters these responses, strengthens our knowledge base. This will then aid us with patient assessments, application of the anaphylaxis medical directive, and what firefighters should observe post administration. Knowledge creates confidence. Confidence in our knowledge/skills is observed with our abilities, and ability leads to better outcomes.
Take care and be safe.
In the exercise world, it is rare to be able to state anything definitively. The most we can say with authority is that everyone should exercise. Beyond that, nuance prevails. How, when, where or why you should exercise is entirely debatable.

Mobility work is no exception. When asked about any particular stretch, my first reaction is always to question why that stretch is being performed. Has a relevant limitation to joint range of motion been identified and, if so, has it been established that the specific muscle being stretched is the culprit? If not, then the stretch being performed is as likely to be a waste of time, as it is to be effective.
Don’t get me wrong. I am not anti-stretching. Appropriate mobility train ing can significantly affect joint range of motion and thereby determine the suitability of a particular exercise for the needs of a given individual. But mo bility training is not a panacea. Just because we perform stretches does not mean we will be protected from injury. In order to program mobility work effectively, we should have a system that tells us what needs to be stretched and (perhaps more importantly) what doesn’t.
Mobility screening is one way of accessing this kind of information. An appro priately designed and administered mobility screen can effectively rule out mobility issues at certain joints, while drawing attention to joints where mobility work might prove im pactful.

We can loosely define joint mobility as the degree to which two adjoining bones can move in relation to one another without being restricted by surrounding tissues. These sur rounding tissues include muscles, ligaments and tendons, but we should also recognize that joints can be restricted by the shapes of the bones themselves, and even by the positioning of those bones.
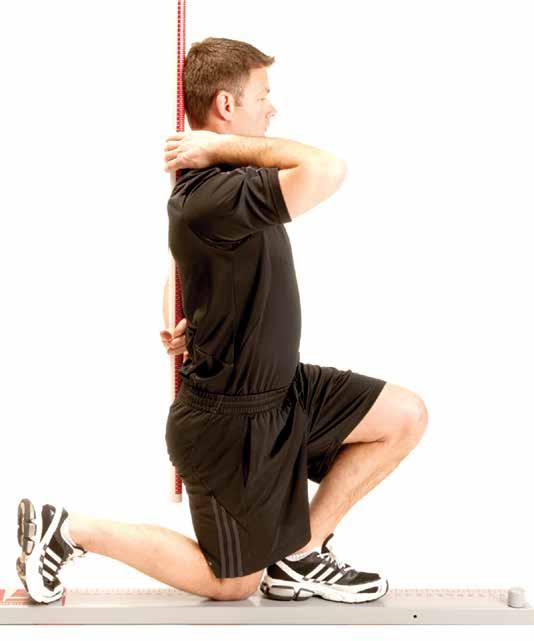
THE CASE FOR MOBILITY SCREENING “Cap, my back hurts when I squat. What stretches should I do?”
BY ALEX BOERSMA, TORONTO FIRE CAPTAIN, STATION 426-D fire fighter’s guide to health and nutrition Fit to SURVIVE like this easily rate as my most frequently asked. Inevitably, my reply will be less than satisfactory. It will usually consist of a shrugging motion accompanied by the age-old standby: “It depends.”
Active ROM describes the extent to which you can use your own muscles to move limbs around a joint. For ex ample, if you cannot lift your arm straight overhead with out compensating somewhere around the neck or back, you probably have some restriction in your active ROM. Active ROM requires not only adequate flexibility in the tissues around the joint, but also appropriate control and coordin ation of the muscles that move the limbs. In the case of not being able to lift your arm directly overhead, the problem may be that the tissues around the shoulder joint are resist ant to lengthening. But it could also be that the muscles that want to pull the arm down (the lats, for example) are overly active and preventing the muscles that want to lift the arm up (the deltoids) from doing their job effectively. In the latter case, stretching the lats will be unlikely to change the ROM of the shoulder joint.
Passive ROM, on the other hand, describes the extent to which an external force can move limbs around a joint. For example, even though you may not be able to lift your arm directly overhead by yourself, it is possible that I could place my hands on your arm and with mild pressure force your arm up overhead into the desired position. This would indi cate that even though you lacked active ROM, it was not the flexibility of the tissues that was the problem. Instead, the restricted ROM was probably due to impaired control and/ or coordination of the muscles involved.
Generally speaking, a lack of active ROM does not provide us with enough information to prescribe stretching protocols. A lack of passive ROM, on the other hand, indicates that joint movement is limited by the surrounding tissues and that there may be some benefit to stretching these tissues.
Restricted ROM around a joint will impact the way you move. Usually, there will be some kind of compensation in the joints above or below the restricted joint. For example, if your shoulder ROM is restricted but you need to lift your arms straight overhead, you will probably compensate by bending backwards excessively, potentially putting your lower back in a compromised position.
An appropriately designed and administered movement screen should be able to identify deficiencies in joint ROM and determine whether those deficiencies are due to active or passive limitations. In doing so, it may provide you with four important pieces of information:
1. What exercises to steer clear of.
2. What alternative exercises might be more beneficial.
3. What ranges of motion to use for a given exercise.
4. Whether a stretching protocol might be indicated, and if so, which tissues should be stretched?
As an example, let’s say you perform a movement screen and identify that you have restricted ROM at the shoulder joint. What might this tell you?
1. It may suggest that you steer clear of direct overhead pressing exercises such as seated military presses or push presses.
2. It may suggest that you instead perform vertical pressing exercises which do not go directly overhead, like incline seated presses or landmine presses.
3. It may suggest that if you do press directly overhead, you limit ROM in these exercises.

4. If the screen identifies a restriction in passive ROM at the shoulder, it may suggest that you try stretching some of the muscles that resist lifting the arm overhead (such as the lats, the teres muscles or the long head of the triceps).
Mobility screening, then, can be an invaluable tool, both for selecting appropriate exercises, as well as for determining if a particular stretching protocol is appropriate.
For a more in-depth article on mobility screening, please see: https://performanceredefined.ca/ wp-content/uploads/2019/07/ Mobility-Manual-Preview.pdf
Also, if you would be interested in participating in an in-person workshop on mobility screening through the TPFFA educational committee, please contact me at dynacore16@gmail.com.
There are two ways of looking at the range of motion (ROM) of a joint: active ROM and passive ROM.
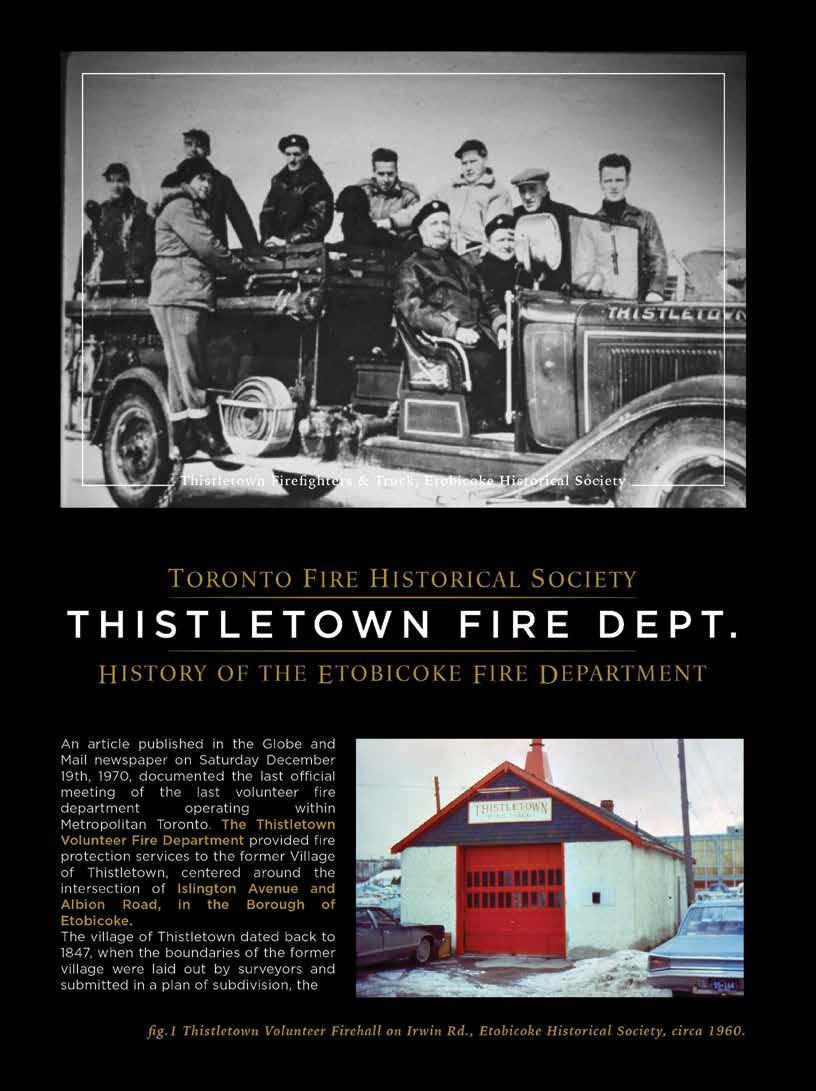
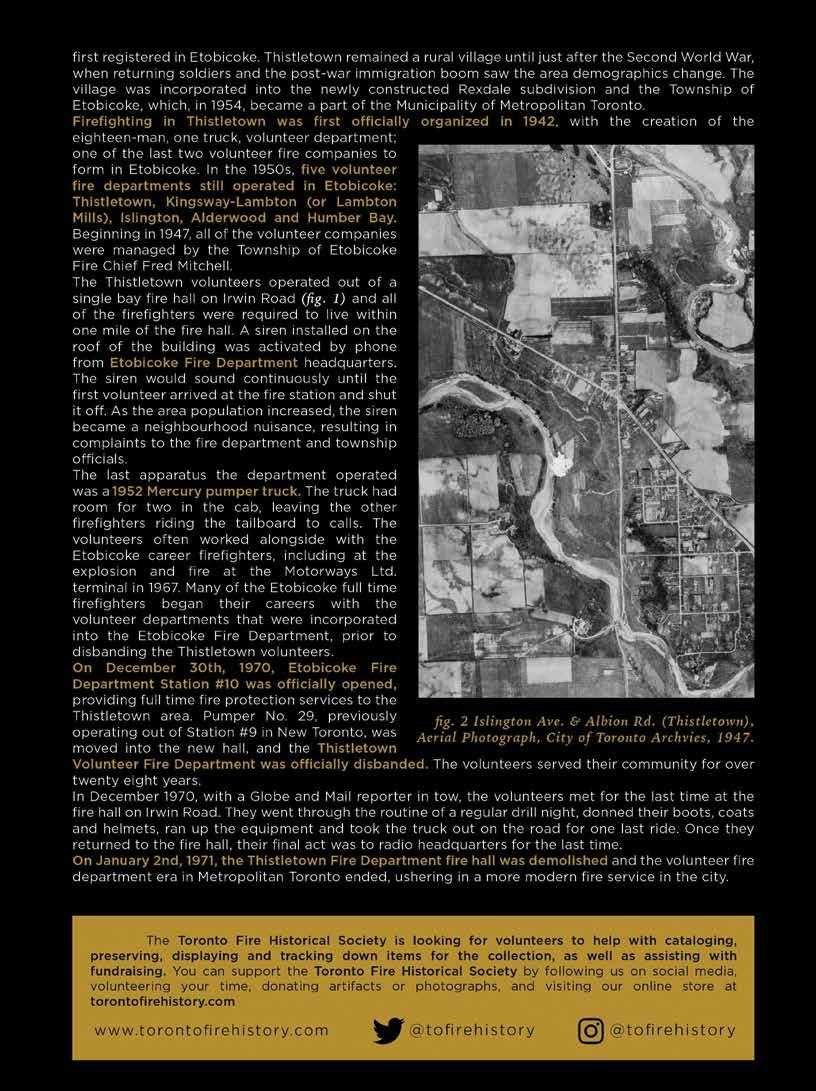
In a slow cooker or pot, place chicken breasts and pour over chicken stock to emerge chicken breasts, add 1 Cup of Franks Red Hot Sauce and 1/2 blocks of butter. Add salt, pepper, garlic powder and spices to taste (Italian spice mix works well here). Slow cook or simmer in a pot until chicken breasts begin to fall apart under gentle prodding with a fork. Stir occasionally to keep all chicken emersed in sauce. Once chicken begins to pull apart, remove the chicken breasts and place on plate or cutting board and pull using two dinner forks (save the broth used for cooking). Once pulled apart place pulled chicken back into broth and stir together.
While chicken is cooking, slice sweet potatoes in half lengthwise. Lightly oil cut side and salt, place cut side down on lined baking sheet. Oil skin side and lightly salt. Bake at 400 degrees for ~40 minutes or until potatoes are soft.
Slice bell peppers and sweet onion lengthwise and sauté in oil/butter, lightly season with salt and pepper.
Shred cheese.
Assemble by placing sweet potatoes on plate cut side up, cover with pulled chicken with broth, top with sautéed peppers/onions, shredded cheese, sour cream, cilantro and a squeeze of lime.
Enjoy.


 We are very happy to acknowledge the Landing Group of Restaurants for their continued support of Toronto Firefighters Charity. We hope that the check presentation below is the first of many in the future. Congratulations to Pumper 314, built in 1921 and located at 32 Grosvenor Street, Toronto.
We are very happy to acknowledge the Landing Group of Restaurants for their continued support of Toronto Firefighters Charity. We hope that the check presentation below is the first of many in the future. Congratulations to Pumper 314, built in 1921 and located at 32 Grosvenor Street, Toronto.