“A plant-based diet can help with bowel regularity, and in turn relieve common digestive symptoms, such as constipation and bloating.”
Dr. Megan Rossi, Founder, The Gut Health Doctor Page 08
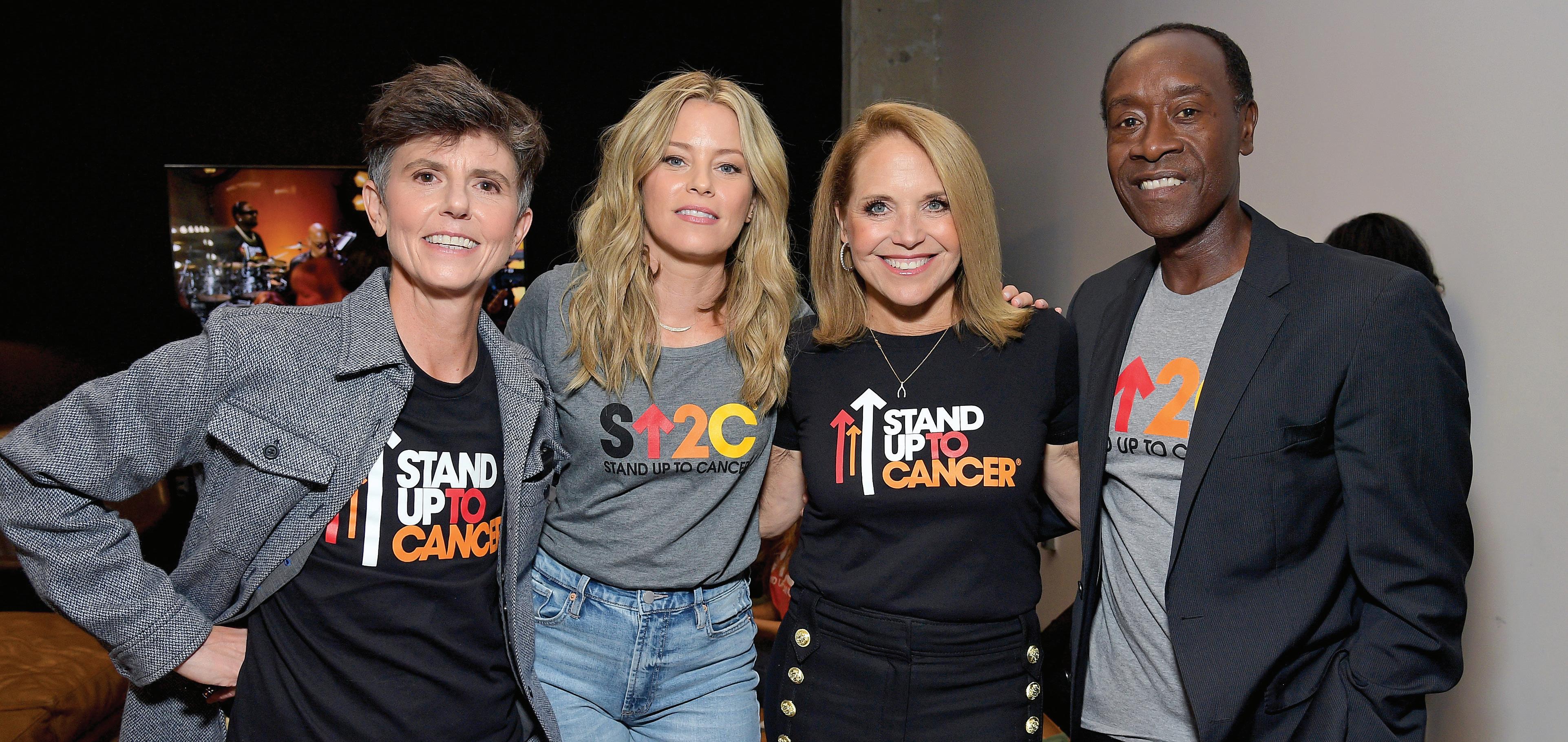
The legendary journalist talks about her battle with cancer and advocating for others
Read more on Page 16
“AI-powered tools have shown great promise in detecting GI diseases early ... through enhanced image recognition during colonoscopies.”
J. Casey Chapman, Chief Medical Officer, GI Alliance
Page 20
KATIE COURIC
Innovating Personalized GI Care: What It Means for You
In gastroenterology, innovations are making it possible for doctors to deliver bespoke care, which tailors treatments based on individual needs rather than a one-sizefits-all model.
The goal is simple: to provide the best care possible, using the latest technologies and practices that fit your unique situation. Personalized care can also mean more accurate diagnoses, better outcomes, and treatments that fit seamlessly into your life.
The need for better GI care
Did you know that between 60 and 70 million adults in the United States suffer from digestive (GI) issues? Conditions like heartburn, bloating, and more serious diseases like colorectal cancer can greatly affect your quality of life. Research shows that 40% of people with GI conditions avoid normal activities like exercising or spending time with family. This is a problem because many GI conditions can be improved, or even prevented, with early diagnosis and proper care.
Unfortunately, many people wait too long to discuss their symptoms with a doctor. One-third of patients with GI problems don’t mention their symptoms unless their doctor asks. This delay can make it harder to treat conditions like colorectal cancer, where early detection is critical.
Even when you’re ready to seek help, getting an appointment can sometimes be difficult. This is why improving access to care, reducing costs, and making sure your experience as a patient is as comfortable as possible are top priorities in healthcare today.
New innovations making a difference
Exciting new technologies are making personalized care easier and more effective than ever. Below are a few ways healthcare is improving for people like you:
1. Early detection of esophageal cancer
Esophageal cancer is often diagnosed late, making it harder to treat. However, a pre-cancer condition called Barrett’s esophagus can be detected earlier with new, less invasive
screening methods. Traditionally, doctors used endoscopy (inserting a camera down your throat) to look for signs of Barrett’s esophagus. Now, a simpler option exists: swallowing a small balloon device that collects cells from your esophagus. This innovation could make it easier and faster to catch this serious condition early.
2. At-home colon cancer screening
Colon cancer is another GI condition where early detection can save lives. However, many people avoid getting screened due to the inconvenience of scheduling a colonoscopy or concerns about bowel preparation. New at-home tests allow you to check for colon cancer from the comfort of your home.
Recently, a blood test for colon cancer detection was approved. These non-invasive tests can help increase screening rates and catch cancer earlier, but patients need to remain informed regarding the accuracy of these at-home tests compared to a colonoscopy.
Regardless of the screening method, doctors are innovating in colonoscopy
procedures using AI to make colon cancer prevention even more accurate and effective.
3. AI and machine learning (ML)
AI and ML are making significant contributions to GI care, particularly in detecting GI cancers. These technologies analyze images from procedures like colonoscopies to help doctors identify precancerous polyps more accurately. AI scans every frame of a video during a colonoscopy, allowing doctors to catch even the smallest abnormalities.
4. Microbiome analysis
Your gut is home to trillions of tiny organisms that play a big role in your overall health. An imbalance in these organisms (called your microbiome) can lead to GI issues. Doctors can now analyze your microbiome to understand which bacteria are causing problems, and recommend personalized diets or probiotics to restore balance and improve your health.
The future of GI care is personal
The future of gastroenterology is exciting. Not only are we moving toward more personalized care, but we are also improving how and where you receive treatment. Though challenges remain, such as insurance and regulatory hurdles, the GI care of the future will be more personal, more precise, and more focused on what works best for you.
To Supplement or Not to Supplement? That Is the Question
Are you confused about which supplements are science-backed and worth your time?
Dr. Megan Rossi, founder of The Gut Health Doctor, is here to cut through the noise.
While it’s exciting to see the growing awareness of gut health, it’s also frustrating to watch companies hop on the trend with misleading products that lack scientific backing. The truth is, feeling and looking your best doesn’t need to be complicated or expensive. For most people, optimal gut health cannot be achieved with supplements alone, but instead requires a plant-rich, diverse diet that acts as a natural fertilizer for your “good” gut bacteria, helping them thrive. That being said, certain supplements can play a supporting role in specific health needs. Here’s what the science says:
Probiotics
There is strong evidence to support a number of condition-specific probiotics that can help manage specific symptoms or conditions. However, here is the thing: You need to take the right strain (i.e., type of bacteria), at the right time (e.g., if you need to go on antibiotics), and you need to take it in the right way (i.e., for the right length of time and dose).
For example, research has shown that if you need to take antibiotics, then taking the probiotic Lactobacillus rhamnosus GG throughout and for a week afterward significantly reduces your risk of antibiotic-associated diarrhea, which affects as many as one-third of patients. There are also several other evidence-backed probiotics available for female health, infant colic, and cold and flu, to name a few.
Psyllium husk
For those struggling with bowel irregularities, psyllium husk is a simple, evidence-based supplement that can help manage both constipation and diarrhea. Research, including studies from King’s College London, shows psyllium is unique because gut bacteria don’t digest it like most fibers. Instead, it absorbs water, helping soften hard stools or thicken loose ones. Psyllium can also alleviate other symptoms, like incomplete evacuation — the feeling that your bowels aren’t fully emptied. Start with half a tablespoon (around 3g) daily, and gradually increase to a maximum of 3 tablespoons per day, ensuring you add an extra 150ml of water per tablespoon to support psyllium’s role.
Vitamin D
Vitamin D is another supplement worth considering not just for your immune health (as commonly
advertised) but your gut health, too — particularly during the darker months. In places like the United States, United Kingdom, and Canada, limited sunlight in the autumn and winter makes it challenging to maintain adequate levels. Vitamin D3 (cholecalciferol) is the most effective form for raising your levels according to a review of 20 studies (compared to vitamin D2, often found in plant foods like mushrooms). Also, vitamin D is fat-soluble, meaning it’s best taken with a meal that includes healthy fats to aid absorption. Think oily fish (like salmon or mackerel), extra virgin olive oil, avocado, nuts, seeds, or full-fat yogurt.
As a general rule, aim to meet your nutritional needs through a diverse, plant-rich diet (think 30 plant points per week), fermented foods, and oily fish before turning to supplements. If you have specific health concerns or suspect you might need supplementation, consult a healthcare professional or registered dietitian who can provide personalized, science-backed advice tailored to your needs.
Written by Megan Rossi, Ph.D., RD, APD, Founder, The Gut Health Doctor (@theguthealthdoctor)
Beyond Regularity: Digestive Health and Fiber
Discover how fiber can transform your health. In this Q&A, Susan Bowerman, a registered dietitian and Herbalife Advisory Board chairperson, breaks down the different types of fiber, their role in weight management, and their overall benefits for health and wellness.
Are all fibers the same?
There are two broad classes of fiber: soluble and insoluble. Soluble fibers, found in foods like oats and beans, thicken in liquid, promoting fullness. Insoluble fibers, present in vegetables and whole grains, add bulk and help with regularity.
How does fiber support weight management?
High-fiber foods take longer to digest and are more filling. They have fewer calories per bite than low-fiber foods and help regulate blood sugar, which may reduce snacking.
How does fiber affect other aspects of health?
Fiber helps regulate blood sugar, reduces the absorption of fat and cholesterol, and supports the growth of good bacteria in the gut. These are some of the reasons why fiber is important in the diet.
How much fiber is recommended per day? In the United States, more than 90% of women and 97% of men do not meet recommended intakes for dietary fiber. For adults consuming 2,000 calories per day, the current Dietary Guidelines for Americans (available at dietaryguidelines.gov) recommend up to 28 grams of fiber.
Megan Rossi | Photo by Ashton Leach
INTERVIEW WITH
Susan Bowerman, M.S., RD, CSSD, CSOWM, FAND Senior Director, Worldwide Nutrition Education and Training, Herbalife; Chair, Herbalife Dietetic Advisory Board and Outer Nutrition Advisory Board
Science-Backed Wellness: Starting With the Gut
Sometimes called “the second brain,” gut health is crucial to overall health and wellness, and the right nutrition philosophy is the secret to both.
People around the world are seeking healthier lives. Increasingly, that means navigating an explosion of misinformation while seeking a balanced, holistic approach to overall health.
That holistic approach begins with the brain-gut connection. “Your brain is the control center of your body — and in a way, the gut is a ‘second brain,’” noted Luigi Gratton, M.D., M.P.H., vice president, office of health and wellness at Herbalife and chair of the Herbalife Nutrition Advisory Board. “How do we make sure your gut is healthy? By consuming nutrients that support the growth of beneficial bacteria.”
The brain-gut connection
The constant, bidirectional communication between the brain and the gut influences all aspects of our health. Our mental and emotional health can impact our gut (like when your appetite vanishes when you become anxious), and gut health can, in turn, impact physical, mental, and emotional health. Keeping the gut healthy is the key to overall, holistic health.
Filling the nutrient gap
Ironically, a major obstacle to a healthier gut is the food we eat. Modern diets are deficient in crucial nutrients like potassium, magnesium, and vitamin D. One way to address this is by adding
these nutrients to products we consume, something Herbalife does as a matter of course. For example, Herbalife’s hydration product, CR7 Drive (developed with Herbalife-sponsored athlete Cristiano Ronaldo) contains a healthy dose of magnesium.
Another factor is what’s called the “microbiome,” microbes that form part of the immune system in your gut. Supporting the microbiome can involve consuming probiotics that encourage the growth of healthy gut bacteria, prebiotics that feed those bacteria, and eating lots of fruits and vegetables. “It’s almost like tending a garden,” Dr. Gratton noted, “eliminating harmful bacteria while nurturing beneficial bacteria through proper nutrition.”
Supplements can support a healthier gut, and their benefits are maximized when paired with healthy lifestyle choices — like getting enough exercise and sleep. The manufacturing process also plays a vital role in their effectiveness. Many probiotics, for example, are actually destroyed by our stomach acids before they can take effect. Herbalife has Simply Probiotic which is formulated with a powerful GanedenBC30®* strain that survives the gastric journey to get to where it counts.
A legacy of health and wellness
Herbalife has been committed to enhancing health and wellness for nearly 45 years and has a robust, holistic
Nutrition Philosophy built on six pillars, which when combined have shown to impact overall health and wellness.
“The first pillar is protein, which is important for gut and microbiome health,” Dr. Gratton explained. “Next is healthy carbohydrates like fiber, which are essential for regularity and digestive health. Our third pillar is healthy fats — the typical American diet is often high in omega 6 fats while being low in omega 3 fats. To correct this imbalance, we recommend consuming dietary fats in the right amounts. Fourth, the vitamins and minerals essential for all our bodily functions. The fifth pillar is proper hydration. Finally, our sixth pillar is what we call phytonutrients: Plant-based nutrients that support the body. The Herbalife Nutrition Philosophy is our core belief that with balanced nutrition, a healthy and active lifestyle, and a personalized plan, you can live your best life.”
Seed to Feed commitment
It’s not just about which supplements you take — it’s about ensuring they meet high quality standards. Herbalife’s dedication to quality is exemplified by its Seed to Feed process, a rigorous quality-control system that ensures that ingredient quality, manufacturing, and testing meet stringent standards. Herbalife performs multiple rounds of internal testing on its ingredients to verify their identity, ensure they meet potency standards, and confirm they
To learn more about Herbalife’s Nutrition Philosophy and wellness community, visit www.Herbalife.com
HERBALIFE NUTRITION PHILOSOPHY’S SIX HEALTH
PROTEIN Gut integrity CARBOHYDRATES SUCH AS FIBER
Digestion elimination
HEALTHY FATS (OMEGA 3S)
Balance of fats, including Omega 3 and Omega 6
VITAMINS & MINERALS
Essential for energy, immunity, and overall health
are free from contaminants that could impact their safety or effectiveness.
For example, Herbalife sources the majority of its tea from dedicated fields in China. Herbalife not only tracks its tea from planting to cultivation, they process it using water extraction, instead of the alcohol-based process that is used by some companies, resulting in a much cleaner tea.
Community and evidence
A final obstacle to holistic health is the explosion of nutrition and health misinformation, especially online. Herbalife combats misinformation through the community it has built and its commitment to science-backed products.
“Our network of independent distributors is our unique strength and differentiation,” Dr. Gratton said. “They operate like a public health initiative, grounded in evidence-based nutrition and supported by our advisory board of over 100 experts, including physicians, dietitians, and sports scientists who help train and educate our distributors.”
Herbalife stands firm in its commitment to science-backed solutions as opposed to momentary trends. “Our philosophy is built on a foundation of scientific evidence,” said Dr. Gratton. “We prioritize evidence-based nutrition to ensure our products effectively support health and well-being.”
Written by Jeff Somers
PILLARS
HYDRATION
Affects processes in the body like digestion, joint and brain functions, and skin health
PHYTONUTRIENTS (PLANT-BASED NUTRIENTS) Support overall body function
INTERVIEW WITH Luigi Gratton, M.D., M.P.H. Vice President, Office of Health and Wellness, Herbalife
Gut Instinct: Katie Couric’s Tips for Better Overall Health
Katie Couric (@katiecouric) is an award-winning journalist and #1 New York Times bestselling author of her memoir, “Going There.” In 2017, she founded Katie Couric Media, which has developed a number of media projects, including a daily newsletter, “Wake-Up Call”; a podcast, “Next Question”; digital video series; and several documentaries. You can find it all at katiecouric.com. Here, she shares her tips for how to eat better, get more active, and do a host of things to help you look, feel, and be healthier.
How have the dietary choices you’ve made impacted your digestive health and overall quality of life?
I try to eat foods that are high in nutrients and fiber. I’ve become a kale junkie and love to make what I call my “kitchen sink” salad, full of high-protein foods like garbanzo beans, eggs, and feta cheese, along with every veggie you can think of. I also need calcium to stave off bone loss as I age. Red meat is a treat for me, and I try to stay away from processed foods in general.
How do we shift the conversation from “diet culture” to healthy, long-lasting nutritional choices?
I think we are witnessing that now. Many people I know are focused on overall health and not necessarily
weight loss. Being strong is the new skinny!
As the new year approaches, what tools can people use to take a healthy, holistic approach to improving their diet?
I think drinking a ton of water (half your weight in ounces) and really focusing on fiber and protein is the way to go. I think avoiding anything in a wrapper or bag is a good policy if you can do it. And of course, exercising. I think staying active is not only good for your body, but it also puts you in a mindset to eat healthy.
Is there anything else you’d like to share with our readers?
Whether you’re talking cancer, heart
I think drinking a ton of water (half your weight in ounces) and really focusing on fiber and protein is the way to go.
disease, or a host of other diseases, lifestyle choices can have a huge impact. These things don’t necessarily inoculate you against disease — sometimes it’s a genetic issue and even the healthiest lifestyle can’t protect you — but you are ahead of the game if you do these things.
I also think taking a break from social media is part of a healthy lifestyle. Go for a walk, get off your phone, leave it at home when you meet a friend if you can. We are all addicted to our digital devices and it’s not good for your body, soul, or mind!
For more insights from Katie Couric, subscribe to her “Wake-Up Call” daily newsletter and “Next Question” podcast.
(From left to right) Tig Notaro, Elizabeth Banks, Katie Couric, and Don Cheadle | Photo courtesy of Stand Up To Cancer
Dr. Megan Rossi Teaches You How to Eat More Plants
Dr. Megan Rossi, author of “How to Eat More Plants,” debunks common healthy-eating myths and shares her tips for sticking to a plant-based diet.
What are common misconceptions about a plant-based diet?
1. That a plant-based diet means plants only. By definition, plant-based means just that — the base of your diet is plants, and then whatever you choose to add to that base is completely up to you. In “How to Eat More Plants,” I talk about the spectrum of a plant-based diet. On one end, you have veganism, and at the other end is flexitarianism. In terms of health, wherever you sit along that spectrum doesn’t necessarily matter, as long as the greatest proportion of your diet comes from plants, you’re following a plant-based diet, and you’re doing the best by your gut and overall health.
2. That a plant-based diet automatically means it’s healthy. There is a world of difference between the nutrition found in ultra-processed foods and that found in whole plants. It’s the latter that has been associated with optimal health, and it’s what I recommend as the focus of any plant-based diet.
3. If you have a sensitive gut, you can’t commit to a plant-based diet. Plant-based eating can absolutely
be for everyone. Even if you struggle with a sensitive gut, the trick is to slowly increase the variety and number of plants into your diet over several months.
How can a plant-based diet positively impact the digestive system?
Plants are not only full of dietary fiber — they also contain a range of plant chemicals, including polyphenols, which we know feed our “good” gut bacteria and support the right balance of bacteria in your gut. This, in turn, has been shown to support the strength of your gut lining (as the bacteria produce beneficial chemicals known as short chain fatty acids, which fuel our gut lining). A plant-based diet can also help with bowel regularity, and in turn relieve common digestive symptoms, such as constipation and bloating.
Why is a healthy diet beneficial for various conditions?
We’ve known for a long time that enjoying a plant-based diet is linked with lower risk of a range of chronic conditions, including heart disease, type 2 diabetes, and more. However, it’s only been more recently
where we’ve uncovered more of the mechanisms (i.e., how the diet has these health associations). A lot of this benefit comes down to the fact that plants feed our gut bacteria, and it’s these bacteria that play an active role in protecting our bodies from various conditions.
For example, research has shown that our gut microbiota can help regulate our appetite and blood sugar levels, which play an important role in conditions like type 2 diabetes. Our bacteria are also thought to play a role in a range of autoimmune conditions, and studies have shown that nourishing our bacteria can even help manage mental health conditions, such as depression. I cover how the gut influences various organs and functions — including the gut:skin, gut:hormone, gut:brain, and gut:immune connections — in an entire chapter within “How to Eat More Plants.”
If someone is experiencing digestive concerns, what are some things they should talk to their doctor about?
If you’re experiencing ongoing digestive issues, your first port of call should be to go and see your physician to rule out organic conditions, such as
inflammatory bowel disease, celiac disease, and colon cancer, which can be masked by digestive symptoms. When going to see your physician, to ensure you make the most of your time together, I would recommend you take a summary of your symptom history, such as when your symptoms started, how often they present, whether they are linked with your diet or stress levels, etc.
What is a cost-effective way to improve digestive health?
Increase the diversity of plants in your diet. This doesn’t just mean buying fresh fruit and vegetables from your local deli, but increasing your “super six,” also known as wholegrains, fruits, vegetables, legumes, nuts and seeds, and herbs and spices. This can be as simple and cost-effective as bulking out meals with saltfree canned legumes, such as chickpeas or lentils, or even buying frozen fruit and vegetables. It’s much more economical and still great for the gut!
I also recommend buying fruit and vegetables that are in season. It’s much cheaper, often more nutritious, and it’s a great way to try new plants that you haven’t tried before.
Megan Rossi | Photo by Ashton Leach
New Treatment Guidelines for Barrett’s Esophagus Patients Are Released
If you’re living with Barrett’s esophagus, a precursor to esophageal cancer, you have a lot of healthcare choices to make.
New clinical practice guidelines may make some of those choices easier when made with your healthcare team.
Published in the journal Gastroenterology, the “Clinical Practice Guideline on Endoscopic Eradication Therapy of Barrett’s Esophagus and Related Neoplasia” has updated evidence-based guidance for Barrett’s esophagus patients. The American Gastroenterological Association (AGA) authored the revised guidelines.
A primer on Barrett’s esophagus Barrett’s esophagus happens when prolonged acid reflux damages the protective lining of the esophagus, causing it to redden and thicken. The esophagus is a swallowing tube that links the mouth and the stomach. Consistent irritation can cause tissue damage and changes to the esophagus on a cellular level.
Clinically speaking, this damage can make the lining of the esophagus look more like the lining of the intestines. This is called intestinal metaplasia, where tissue in one part of the body replaces itself with tissue found elsewhere biologically. Though the risk is minimal, metaplasia can increase the risk for cancer.
Metaplasia can progress to dysplasia, which indicates the presence of precancerous cells that can be reversible. Dysplasia is considered low-grade or highgrade, depending on the degree of cellular change.
The latest guidelines for Barrett’s esophagus patients address an array of concerns for this population. Among them is how to consider the option of undergoing endoscopic eradication therapy for potential esophageal cancer risk reduction.
Endoscopic eradication therapy consists of minimally invasive procedures, such as endoscopic mucosal
resection (EMR) or endoscopic submucosal dissection (ESD), followed by ablation (burning or freezing) techniques.
Key guideline takeaways Here’s what patients with Barrett’s esophagus need to know about the guidelines:
• For patients with low-grade dysplasia, it may be appropriate to either remove or monitor the cells. This is a decision doctors and patients should make together after discussing the risks and benefits of treatment. “While the benefit is clear for patients with high-grade dysplasia, we suggest considering endoscopic eradication therapy for patients with low-grade dysplasia after clearly discussing the risks and benefits of endoscopic therapy,” said guideline author Dr. Tarek Sawas. “A patient-centered approach ensures that treatment decision is made collaboratively, taking into account both the medical evidence and the patient’s preferences and values. Surveillance is a reasonable option for patients who place a higher value on harms and a lower value on the uncertain benefits regarding reduction of esophageal cancer mortality.”
• For patients with high-grade dysplasia, AGA recommends endoscopic therapy to remove the abnormal precancerous cells.
• Most patients undergoing endoscopic eradication can be safely treated with EMR, which has a lower risk of adverse events. Patients who undergo ESD can face an increased risk of strictures and perforation. AGA recommends reserving ESD primarily for lesions suspected of harboring cancers invading more deeply into the wall of the esophagus, or those who have failed EMR.
• Patients with Barrett’s esophagus (dysplasia or early cancer) should be treated and monitored by expert endoscopists and pathologists who have experience in Barrett’s neoplasia (or irreversible abnormal cell growth that leads to cancer).
The importance of the doctor-patient conversation
Another guideline author, Dr. Joel Rubenstein, emphasizes that the decision to get endoscopic eradication therapy comes down to an individual’s preferences and comfort level, as well as their doctor’s recommendations.
“We (healthcare providers) need to have a conversation with patients in clinic prior to when they show up in the endoscopy unit on a gurney,” Dr. Rubenstein said. “Patients need to be fully aware of the risks and benefits, both in the short term but also in the long run, to decide which treatment approach is best for them. This decision often comes down to personal factors and values.”
What’s more, when patients are in touch with their healthcare providers, they can take steps to better prevent or manage Barrett’s esophagus, and thereby lower their risk for dysplasia and esophageal cancer.
Another takeaway from the new guidelines is that tobacco use and obesity are risk factors for esophageal adenocarcinoma. Therefore, losing weight and quitting smoking can improve clinical outcomes.
A final takeaway from the guidelines is that patients should be aware of how best to manage acid reflux, which can cause that initial damage to the esophagus. The guidelines note that an optimal treatment plan is one that is well-rounded, including both medication and lifestyle changes.
Written By Melinda Carter
A Game-Changing Test in the Fight Against Esophageal Cancer
Castle Biosciences’ TissueCypher® test can offer patients with Barrett’s esophagus a clearer picture of their risk of developing esophageal cancer.
EINTERVIEW WITH
Cadman Leggett, M.D. Gastroenterologist, Mayo Clinic
sophageal cancer is a killer. It’s the eighth most common form of cancer worldwide and the sixth leading cause of cancer death. The five-year survival rate is around 20%.
One reason for those grim numbers is that most esophageal cancers are diagnosed too late. The first symptom many patients develop is difficulty swallowing, and at that stage the tumor is not easily treatable in most cases.
“That’s essentially what happened to my father,” said Cadman Leggett, M.D., an expert in esophageal diseases and gastroenterologist with the Mayo Clinic. “My dad was in his early 50s when he developed esophageal cancer. He underwent chemotherapy, radiation therapy, and surgery, but unfortunately those measures were not enough to cure his disease. This is the reason why I decided to dedicate my career to fighting esophageal cancer.”
The tragedy of esophageal cancer is that it can be a very treatable disease if it’s caught early. Many people first develop a condition called Barrett’s esophagus (“BE” or “Barrett’s”), which is the only known precursor condition to esophageal cancer. A small percentage of patients with this condition may progress to cancer. However, if patients with BE at the highest risk for developing cancer are identified and treated early, they can often avoid esophageal cancer entirely.
INTERVIEW WITH
Emmanuel Gorospe, M.D., M.P.H. Gastroenterology
Medical Director, Castle Biosciences
As a physician scientist who has dedicated his career to the care of patients with BE and esophageal cancer, Dr. Leggett notes that today’s minimally invasive treatment for BE through endoscopy is highly effective in preventing advanced esophageal cancer. However, Dr. Leggett emphasized the importance of identifying patients at risk of progression and acting within the window of opportunity.
Barrett’s esophagus
BE is increasingly prevalent around the world. “A normal esophagus has a type of lining that is very similar to our skin,” Dr. Leggett explained. “With BE, that lining is injured by chronic reflux — basically, acid. The lining heals but is replaced by a type of lining that looks more like the lining found in your stomach, but with a distinct composition of cells.”
While BE is not itself malignant, it can progress to cancer over time. The term “dysplasia” is used to describe specific, pre-cancerous changes in the Barrett’s tissue — if there are no signs of these dysplastic changes, the condition is described as non-dysplastic BE (NDBE). Most people with Barrett’s are non-dysplastic. But in a subset of NDBE patients, BE can become dysplastic and may eventually become esophageal adenocarcinoma, an invasive form of esophageal cancer.
That makes screening for BE crucial. “If a patient has experienced chronic reflux symptoms at any point in their life, they should talk to their healthcare provider about being screened for BE,” Dr. Leggett said.
However, relying on chronic reflux (heartburn) symptoms in conjunction with other risk factors (like being older, being obese, or being a smoker) to trigger BE screenings is not completely effective. It’s possible to have BE and not know it because one can still have Barrett’s but not manifest any heartburn symptoms. That’s why everyone with any history of reflux should discuss screening with their healthcare provider regardless of whether they are currently experiencing heartburn.
“BE can be a silent disease that may go on for years and put people at risk for cancer progression,” explained Emmanuel Gorospe, M.D., M.P.H., gastroenterology medical director at Castle Biosciences.
Dr. Gorospe calls BE a “paradox” because the treatments available to remove precancerous cells are usually incredibly effective — the biggest challenge arises in finding the highest-risk patients to apply them to.
Risk and limitation
Patients with BE are diagnosed and monitored through a procedure called endoscopy. “We use a flexible tube with a camera,” Dr. Leggett explained. “We examine the esophagus, the stomach, and the small bowel and focus on the Barrett’s segment. We target subtle abnormalities — in texture and vasculature — and obtain a tissue biopsy or perform a technique called resection. A high-quality endoscopic examination is extremely important in detecting these subtle areas of dysplasia.”
Those biopsies (esophageal tissue samples) are sent to a pathology lab where a pathologist will confirm whether BE is present and assign it one
of four grades: non-dysplastic (NDBE), indefinite for dysplasia, low-grade dysplasia, or high-grade dysplasia. The patient’s gastroenterologist will use the pathology grade to determine the patient’s risk of progression and discuss next steps, which may include routine surveillance or discussion of BE treatment with endoscopic eradication therapy (EET).
“There are limitations in using dysplasia as a marker for risk,” Dr. Leggett noted. “We are only sampling a very small percentage of the esophagus — less than 5% — so it is prone to sampling error, and there is a chance of missing dysplasia. In addition, there can be a lot of discrepancy in the interpretation by the pathologist.”
In other words, all physicians have a margin for error when it comes to spotting existing dysplasia—and even if they do believe that they have spotted dysplasia, the pathologist receiving the resulting tissue samples may disagree
“But the question is, will it get cloudy tonight? Or tomorrow morning?” Biopsies provide a snapshot of what the patient’s cells look like at a single point in time. But a pathology lab’s traditional analysis of those “snapshots” provides little information about the risk of future disease progression. That is a critical detail needed to prevent cancer, and physicians are often left to make educated guesses about when to schedule the next surveillance endoscopy. They can be cautious and schedule surveillance every year (with added costs), or they can schedule the next follow-up in three years, guessing that the BE won’t progress before then.
This is the game that TissueCypher is changing. Rather than have physicians make educated guesses about an individual patient’s risk of progression, this AI-driven test looks more deeply at the biopsies to predict the patient’s specific risk over the next five years.
inform the patient of their individual risk,” Dr. Leggett said. “When I get a TissueCypher test and it’s a low-risk score, then the patient often feels reassured. Or, if it’s an intermediate or highrisk score, it can empower the patient to be proactive about their own care.”
The larger medical community is recognizing that changes are needed in our approach to BE and esophageal cancer risk. The American Gastroenterological Association recently published clinical practice guidelines related to the use of EET in the treatment of patients with BE. The guidelines recognize that a subset of patients with NDBE may have a higher risk of developing esophageal cancer than traditionally assumed — and specifically acknowledged the potential benefit that tests like TissueCypher can have in identifying these patients.
or provide a subjective diagnosis.
Once someone is diagnosed with BE, performing surveillance of the BE tissue for signs of progression can be yet another challenge. Current guidelines outline disease management and treatment recommendations for patients with Barrett’s according to population-based risk data. As an example, the guidelines recommend that patients with non-dysplastic Barrett’s be rechecked for signs of dysplasia every three to five years. We know, however, that some patients will progress faster than expected, which is virtually impossible for physicians to predict without additional information. Castle Biosciences, however, has introduced a “game-changer” to the process: TissueCypher.
A fuller picture
“When you take a biopsy, it’s like looking up in the sky and seeing that it’s all clear at that moment,” Dr. Gorospe said.
“The TissueCypher test works by identifying nine biomarkers and the structure of the tissue,” Dr. Gorospe explained. “It looks at those together to produce a risk class for each patient — either low, intermediate, or high — as well as a score; a numerical figure that has a corresponding probability of cancer progression.”
The process looks beyond the visual clues traditionally used by pathologists and delves into the “unseen world” of molecular changes — changes that are impossible for the human eye to detect. TissueCypher employs a validated, AI-driven algorithm that removes human subjectivity from the analysis.
Human cells are incredibly complex; there are millions of data points in a typical tissue sample, well beyond the capability of humans to analyze efficiently. The AI platform used in TissueCypher was trained by analyzing these data points in both patients who progressed to cancer as well as those who didn’t progress. That resulted in identifying a “signature” that was consistent with progression. The intensity of that signature in a sample can be translated into a risk score.
“TissueCypher allows you to better
Both Dr. Gorospe and Dr. Legget believe TissueCypher is a “game changer.” “Having an objective, personalized, and evidence-based prognostic test for BE can certainly change the way we care for patients,” Dr. Leggett said.
“Today’s biggest challenge in preventing esophageal cancer is not the availability of treatment, it’s the ability to identify patients at risk,” Dr. Gorospe said. “Using TissueCypher on a patient’s endoscopic biopsy tissue can enable clinicians and patients to have a more personalized discussion about therapy or surveillance aligned to the patient’s individual risk of developing cancer.”
Written by Jeff Somers
To learn more, scan here:
What Is Exocrine Pancreatic Insufficiency? Basics to Know
The pancreas is a key organ for digestion. When the pancreas is functioning properly, it makes enzymes that create a chemical reaction in the body that break down food and allow for nutrients in food to be absorbed.
But in the case of exocrine pancreatic insufficiency (EPI), this process is disrupted, leaving patients at risk for malnutrition. While symptoms of EPI can be confused with those of other digestive issues, greater awareness of this health issue can help affected individuals get a diagnosis and necessary treatment more quickly.
Causes of EPI
The main cause of EPI is damage to the pancreas. This can happen for multiple reasons, including:
• Chronic pancreatitis
• Recurrent acute pancreatitis
• Cystic fibrosis
• Pancreatic cancer
Extra-pancreatic causes, such as surgery of the digestive tract, can also cause EPI. Examples are procedures that remove some or all of the pancreas, and surgery of the stomach or intestines, as this disrupts the normal process of digestion required for pancreatic enzymes to work most effectively.
Symptoms of EPI
EPI signs vary by individual and can depend on the underlying cause of EPI. Sometimes, EPI symptoms may go unnoticed until nutrient deficiencies and their corresponding complications develop.
Some potential symptoms of EPI include: diarrhea, abnormal stool (may appear greasy, oily, or foul-smelling), gas and bloating, abdominal pain, and unexplained weight loss.
Nutrient deficiencies that commonly show up include those of fat-soluble vitamins A, D, E, and K. EPI can cause maldigestive symptoms that overlap with other common digestive issues, including: irritable bowel syndrome, inflammatory bowel diseases, such as Crohn’s; Celiac disease; small intestinal bacterial overgrowth; and diabetes.
Although less common, the following conditions
also share symptoms with EPI: bile acid diarrhea, giardiasis and other infectious diseases, and disaccharidase deficiencies.
Diagnosing EPI
There is no single test that can diagnose EPI. EPI diagnosis requires a combination of symptoms and/ or abnormal testing. The testing used when EPI is suspected depends on the individual.
The following tests can be used to diagnose EPI:
• Fecal elastase test, which can detect the concentration of an enzyme called elastase that is released by the pancreas. This test must be done on solid stool and is only accurate when the diagnosis of EPI is highly suspected.
• Fecal fat test, which can determine whether there is excess fat in stool (a sign of EPI) and other conditions known as “steatorrhea”
• Secretin stimulation test (or pancreatic function test), which gauges whether the pancreas is responding normally to secretin, a hormone the body releases after eating that causes the pancreas to produce digestive enzymes
• Cross-sectional imaging, which may be ordered to determine if symptoms of steatorrhea are related to pancreatic disease or extra-pancreatic disease
How EPI is treated
Treatment for EPI can include pancreatic enzyme replacement therapy (PERT), which requires a person to take pancreatic enzymes whenever eating. PERT can be effective in improving the consistency and frequency of stool, and protecting one from nutritional symptoms; however, other changes may be required, including:
• Diet changes, as working with a registered dietician can be beneficial
• Staying in close contact with doctors to let them know whether side effects are happening so PERT can be adjusted or other conditions evaluated
In some cases, PERT may not address all nutrient deficiencies, and in these cases, taking supplements to replete deficiencies may be appropriate. It’s important to discuss this with a doctor before introducing a new vitamin or supplement to the diet.
Complications of untreated EPI
Nutrient deficiencies on their own are a complication, but leaving EPI untreated can also lead to:
• Skeletal issues, such as bone fractures and osteoporosis
• Muscle problems, such as muscle loss (called sarcopenia)
• Surgical complications
• Dangerous weight loss
• Reduced quality of life
• Increased risk of premature death
These are just some of the reasons recognizing the symptoms of EPI, and then getting a timely diagnosis and proper treatment, are so crucial.
WRITTEN BY Yasmin G. HernandezBarco, M.D. Expert, American Gastroenterological Association (AGA); and Gastroenterologist, Massachusetts General Hospital
Understanding EPI: An Often Misdiagnosed, Yet Treatable, GI Issue
Gastrointestinal (GI) health is essential for overall well-being. However, up to 70 million Americans experience digestive diseases of the GI tract, including problems with digestion and nutrient absorption. While these conditions can be chronic, many are treatable. That’s a relief for patients who are struggling with symptoms ranging from constipation and bloating to stomach pain and diarrhea.
Many factors have been impacting the increase in GI health issues.
People with diabetes may also have an increased chance of GI issues, including gastroparesis and Crohn’s Disease.
Gastroparesis is when the stomach has difficulty emptying. Often, high blood sugar damages the stomach nerves in the digestive tract. Research links Crohn’s disease, a type of inflammatory bowel disease, with an increased risk of type 2 diabetes.
Understanding EPI and its impact on health
Another GI issue affects the pancreas, the organ that’s important for digestion. If the pancreas gets inflamed or swollen, a person may experience gas, bloating, diarrhea, and other GI issues. Every year, pancreatitis affects 87,000 people in the United States.
Exocrine pancreatic insufficiency (EPI) is a condition in which the pancreas cannot produce enough enzymes to digest food properly. The body needs these enzymes — lipase, protease, and amylase — to absorb essential nutrients. Without those nutrients, one may experience GI symptoms like bloating, greasy stools, diarrhea, and unintentional weight loss. EPI has a significant impact on patients’ quality of life, but it’s often misunderstood and misdiagnosed.
EPI can develop suddenly or over time, and its symptoms can be mild or severe. Diagnosing EPI can be challenging because it shares many of the same symptoms as other GI conditions.
Dr. Cynthia Rudert, a board-certified gastroenterologist, explains that EPI is often confused with conditions like irritable bowel syndrome (IBS), making it one of the most misdiagnosed issues in gastroenterology. “Patients come in with gas, bloating, and even undigested food in their stool, and they’re often told they have IBS,” Dr. Rudert said. “But when we dig deeper, many are found to have EPI, which requires a completely different treatment approach.”
The condition doesn’t discriminate by age or body type. Dr. Rudert recalls treating patients as young as four and as old as 94, highlighting that “you don’t have to be thin to be malnourished.”
She advises patients to talk to their doctor about their symptoms and let the doctor know if they see undigested food in their stool, since that could be a sign of EPI.
Undiagnosed or untreated EPI could result in muscle loss since the patient isn’t absorbing the necessary nutrients. Fortunately, advancements in EPI diagnosis and treatment, such as pancreatic enzyme replacement therapy (PERT), offer new hope for patients. We’ll explain more about this treatment below.
The role of GLP-1 medications in GI health Glucagon-like peptide-1 (GLP-1) receptor agonists are another factor impacting GI health.
These are a class of medications frequently prescribed for managing diabetes, obesity, and weight- related health conditions. Medications like semaglutide, liraglutide, and dulaglutide work by mimicking a hormone that helps the body regulate blood sugar, appetite, and digestion.
The weight loss drugs are growing in popularity. Currently, 1.7% of Americans have been prescribed a GLP-1 — a 40% increase over the past five years.
“These treatments are going to enable people to be healthier and have less heart disease, fewer strokes, less fatty liver, and perhaps even lower rates of alcoholism and substance abuse,” said Dr. Anthony Auriemma, medical director at Ascension Weight Loss Solutions.
Dr. Auriemma, an expert in his field, has treated thousands of patients with GLP-1 medicine since the drugs were introduced nearly 20
years ago. He says modern GLP-1 drugs are more targeted and potent than their predecessors.
While GLP-1 medications are widely regarded as effective, they can sometimes cause gastrointestinal side effects, such as nausea, vomiting, diarrhea, abdominal pain, or constipation. In rare cases, more complex GI conditions, including EPI, can arise, particularly in patients with a history of pancreatitis or pancreatic conditions.
Dr. Auriemma says doctors work to create individualized care plans for their patients. He encourages patients to talk with their doctors about their care and to monitor themselves for any ongoing GI symptoms, noting that early identification of underlying issues can improve patient outcomes.
“EPI treatment is life-changing for many patients,” said Dr. Rudert, who shares the story of a 94- year-old man who had been misdiagnosed by top doctors for years. Once correctly diagnosed with EPI and getting started on enzymes, his condition improved dramatically. “You can turn somebody’s life around,” she added.
When to talk to your doctor
Patients experiencing persistent GI symptoms, including those on GLP-1 therapy, should talk with their doctor about their digestive health. It’s important for patients to track how they feel and to log their symptoms, such as greasy stools, bloating, or unexplained weight loss, all of which may signal an underlying condition like EPI. Early diagnosis and treatment are crucial to managing symptoms and preventing long-term complications.
EPI treatment is life-changing for many patients. You can turn somebody’s life around.
Treating EPI
Patients may not know that there are effective FDA-approved treatments that may help them manage their EPI. Pancreatic enzyme replacement therapy (PERT) is the standard treatment for patients diagnosed with the condition. The prescription enzymes are taken at every meal and during snacks. They help break down food so the body can absorb necessary nutrients effectively, alleviating symptoms and preventing complications like malnutrition.
“Your health is unique, and your treatment should be too,” Dr. Auriemma said. Working with a knowledgeable provider ensures symptoms are managed effectively, whether through dietary adjustments, PERT, or supplemental vitamins, such as A, D, E, and K, which are often deficient in EPI patients.
Patients may benefit from nutritional advice from a doctor or a dietician. Many GI health issues can be improved by drinking water, avoiding alcohol, avoiding processed foods, and eating a low-fat, protein-rich diet. Eating small meals throughout the day rather than a few large meals may also help make digestion more comfortable.
Take control of your digestive health
If you’re experiencing any of the symptoms of EPI, speak to a GI specialist or ask your doctor for a referral. Patients shouldn’t let undiagnosed GI conditions hold them back. With advancements in diagnostic tools and effective treatments, relief is within reach. By understanding the signs of EPI and taking proactive steps to address them, patients can regain control of their health and live their lives to the fullest.
Liver Disease Affects More Than 100 Million Americans —
Most Are Unaware
Unlike your heart and lungs, you cannot feel your liver working; however, it is just as essential to your life.
Your liver performs more than 500 vital functions a day, including filtering toxins from your blood, managing blood clotting, making bile to digest fat, storing sugar for energy, making protein for blood plasma, and helping with digestion.
Many of the liver’s functions are related to your metabolism. These metabolic functions allow you to convert food to energy, break down food into the basic nutrients your body needs, and eliminate waste. When the liver is unable to perform those functions properly, it can lead to liver failure and the need for a lifesaving liver transplant.
Liver disease affects all ages, genders, races, and ethnicities, and it can be caused by various factors, such as genetics, lifestyle, and exposure to common toxins and chemicals. Many of these liver diseases have few to no symptoms, so it is important to understand your risk and talk to your doctor about liver disease prevention and early detection.
A growing epidemic
The rise in obesity and diabetes in the United States is fueling a little-understood yet life-threatening disease known as metabolic dysfunction-associated steatotic liver disease (MASLD), formerly
nonalcoholic fatty liver disease.
MASLD is a medical condition in which there is an excessive buildup (approximately 5-10% of the liver’s total weight) of fat around the liver. Left untreated, MASLD can progress to an advanced stage of disease known as metabolic dysfunction-associated steatohepatitis (MASH), which can lead to cirrhosis, liver failure, and the need for a lifesaving liver transplant. In fact, MASH is now one of the leading causes of liver transplantation in the United States.
Did you know:
• MASLD affects 80-100 million Americans
• Obesity is one of the leading causes of MASLD
• More than 2 in 5 American adults have obesity
• MASLD is found in 75% of overweight people and 90% of those considered obese
• MASLD is the most common form of pediatric liver disease
Are you at risk?
When diagnosed early, many people can slow their disease progression and, in some cases, reverse it. The liver is the only solid organ in your body that can regenerate or repair itself after injury, so it is important to talk to your doctor about any risk factors you may
have, as many of the tests that indicate liver disease are not considered routine. People who are most at risk for developing MASLD/MASH include those who: are 40-60 years old, are female, are overweight or obese, have diabetes, have high triglycerides, and/or have high cholesterol.
Minimizing your risk
Everything you eat, breathe, and touch is processed through your liver, so ensuring good liver health is critical. You can take steps to minimize your risk by following these simple tips:
• Maintain a healthy weight
• Eat a healthy diet
• Exercise regularly
• Limit alcohol intake
• Only take medications as prescribed
To learn more about liver disease, prevention, and early detection, head to liverfoundation.org. To find out if you’re at risk for MASLD/MASH, visit thinkliverthinklife.org/quiz to take our short liver health quiz, which is also available in Spanish.
Written by American Liver Foundation
Katie Couric Is Pushing for Progress in Cancer Detection
Spurred by her own cancer journey, Katie Couric has amplified her advocacy efforts, turning personal challenges into widespread awareness and legislative action.
How have your personal experiences with cancer changed the way you now advocate for your and others’ health?
My experiences with cancer, both as a caregiver and as a patient and survivor, have made me acutely aware of the importance of being proactive about one’s health. After losing my husband, Jay Monahan, to colorectal cancer at age 42 and my sister, Emily, to pancreatic cancer at 54, I became a strong advocate for early screening and detection.
My own breast cancer diagnosis in 2022 further reinforced the importance of my advocacy. I was six months late for my annual mammogram when I was diagnosed, and since that experience, I have become even more vocal about the necessity of timely cancer screenings. My breast cancer diagnosis revealed I have dense breast tissue, a factor that increases the risk of breast cancer and can require additional screenings to properly detect the disease. I’m a big supporter of more comprehensive testing for women with dense breasts, and I was so happy the FDA announced new regulations in 2023 requiring mammogram providers to inform patients about the density of their breasts. I also helped introduce legislation called the Find It Early Act in Congress. This bill would ensure all health insurance plans cover additional screening for women with dense breasts, like ultrasounds and MRIs, with no cost sharing. Overall, I encourage people to be their own advocates and be proactive about their health. Know your family history, find a doctor who takes your concerns seriously, and seek second opinions if you feel you need more information.
Are there any misconceptions about colon cancer screening that you’d like to debunk?
One of the big misconceptions about colorectal cancer is that it’s an old man’s disease. That’s simply untrue. Women are diagnosed as often as men, and there’s been an alarming increase in colon cancer cases among both men and women under the age of 50. Also, I think many people think that if they don’t have a family history, they’re immune from getting this disease, but I always say that no family history is no guarantee. In fact, 75% of colon cancer cases involve people with no family history.
Finally, I think a lot of people are unaware that the screening age for a baseline colonoscopy has been lowered to 45. That happened in 2021, but I think we need to ensure people are aware of that change. There are several screening techniques that can be discussed with your doctor.
What can healthcare providers do to increase the rate of early diagnosis of colon cancer?
It’s critical for all healthcare providers to encourage patients to get screened for colon cancer. They should always get a family history as well. For example, my daughters will need to be screened when they turn 31 because the first-line relative of a colon cancer patient needs to be screened 10 years before that person was diagnosed. I’m a big fan of genetic testing, too, because it can help guide what you’re getting screened for and when.
As a co-founder of Stand Up To Cancer, what are the cancer research developments you’re most excited about right now?
I’m really excited about all the new developments
in cancer research today and think there are a lot of promising breakthroughs coming in the near future. For example, researchers have been able to build on the success of the mRNA vaccine for COVID and are now conducting clinical trials using this technology to develop personalized cancer vaccines.
Immunotherapies, including CAR-T cell therapy, have seen significant improvements and can, in some cases, replace standard treatments. Progress in early-stage detection methods, including non-invasive blood tests, will lead to cancers being found earlier, and new technologies, such as large language models and AI will help improve all of these approaches — especially early detection and diagnostic accuracy — making new treatments more precise and personalized.
Jimmy Smits and Katie Couric at a Stand Up To Cancer Event | Photo courtesy of Stand Up To Cancer
Advanced Prevention: How the GI Genius™ Module Can Enhance Polyp Detection During Colonoscopies
Don’t underestimate the importance of your colon: It’s an essential organ that eliminates waste and harbors trillions of bacteria — the good kind that shield your gut and generate substances to maintain a healthy microbiome. The latter, in turn, helps to safeguard your body from infections and may even contribute to reducing the risk of colorectal cancer.
Yet, according to the World Health Organization, “colorectal cancer is the third most common cancer worldwide, accounting for approximately 10% of all cancer cases and is the second leading cause of cancer-related deaths worldwide.” Still, the American Cancer Society points out that there’s a 91% five-year relative survival rate if the disease is caught in a localized stage — meaning it hasn’t spread “outside of the colon or rectum.”
Harish K. Gagneja, M.D. — chief medical officer at Austin Gastroenterology and the vice chair of the Board of Governors at the American College of Gastroenterology — stresses how prevention is key when it comes to preserving a colon that functions properly. And what’s the best way to practice such prevention and detect precancerous lesions called polyps? Quite simply: a reliable colonoscopy.
For many physicians, colonoscopies are more than just a screening-method. “I’m in the business of preventing colorectal cancer,” Dr. Gagneja emphasized.
However, as a procedure, a colonoscopy can have its challenges.
An intelligent colonoscopy module
“Colorectal cancer is, in many ways, a tragedy we know how to prevent,” said Ha Hong, the chief AI officer at Medtronic’s endoscopy division. “But, without the right tools, some early signs can be missed.”
Enter the GI GeniusTM intelligent endoscopy module,
Medtronic’s AI-fueled technology for colonoscopies.
“This tool represents an incredible potential for technology to enhance a doctor’s ability to save lives,” Hong explained. “It isn’t just ‘smart tech’ — it’s designed to amplify human capability, helping doctors to better catch polyps [small growths in the colon] before they have the chance to turn into something much worse. The potential here isn’t incremental improvement — it’s a new level of detection that could mean the difference between a routine procedure and a lifesaving one.”
A 2023 study out of Northwestern University found that doctors using the GI Genius module have been detecting polyps at a 13% higher rate than those who are not using the tech. Furthermore, another study (published in the journal Gastroenterology) reported that AI can “detect colorectal polyps that have been missed due to perceptual pitfalls,” with a 50% reduction in miss-rate.
Currently, more than 3 million people worldwide are benefiting annually from a GI Genius colonoscopy. Think of it as a super-sharp-eyed second observer assisting your physician in finding suspected polyps, while automating quality metrics.
Dr. Gagneja has fully iintegrated the GI Genius module into his colonoscopy procedures, and added that he’s “interested in incorporating any new technology in [his] day-to-day practice that improves the outcome for [his] patients.”
His experience has shown that this neoteric technology has readily
bolstered his ability to identify problematic issues in the colon. He also mentioned how easy it is to use: “There’s no steep learning-curve — it’s really a plug-andplay kind of technology. It is like having a third eye working for you.”
Alleviating AI fears
AI is now seemingly saturating all aspects of our lives, and it’s understandable to feel wary about some of its applications. But both Medtronic and the physicians who are using the GI Genius module underline how the technology isn’t there to replace doctors doing colonoscopies. Rather, it’s an extra tool to boost accuracy and efficacy by directing their attention to areas they may have missed — and hence guide them toward more informed decision-making and potentially better health outcomes.
“AI in healthcare may sound new and futuristic, but the motivation behind it is simple: to make healthcare safer and more accurate for patients,” Hong said. “Patients are still getting the human touch, but with a GI Genius colonoscopy, they’re also getting the added benefits of technology that’s acting like a digital safety net.”
In the end, the doctor still has the final say. This new tech can empower them (rather than compete with their skills). Or, as Dr. Gagneja pithily puts it:
“Gastroenterologists who are not using AI in the future will be replaced by gastroenterologists who are indeed making use of advances in AI.”
Written by Omar Sommereyns
Dr. Gagneja is a consultant for Medtronic.
INTERVIEW WITH Ha Hong Chief AI Officer, Endoscopy Division, Medtronic
INTERVIEW WITH Harish K. Gagneja, M.D. Chief Medical Officer, Austin Gastroenterology
Photo courtesy of Medtronic
More Pleasant Colon Cancer Screening? A New Blood Test Makes It Possible
50 million Americans due for colon cancer screening avoid it because they consider traditional tests so unpleasant. But this screening can now be as simple as a blood test.
If you’re overdue for your colon cancer screening, you’re not alone. Even though colon cancer is highly treatable when it’s found early, 1 in 3 adults eligible for screening in the United States don’t complete this critical step, often because they see the available options as unpleasant, inconvenient, or uncomfortable. If you can relate, there’s a new option that might change your mind: a blood test recently approved by the U.S. Food and Drug Administration (FDA) to screen for colon cancer.
Why early detection is so important
Getting regular health screenings is crucial to find disease early, especially as you age. This is particularly true for colon cancer. If the disease is caught in its early stages, before symptoms develop, the five-year survival rate is an impressive 91%. Despite this, colorectal cancer (affecting the colon or rectum) remains the second leading cause of
cancer-related deaths in the United States.
One of the main reasons: 3 out of 4 individuals who die from colon cancer are not up to date with screening. If you aren’t screened in a timely manner, colon cancer may not be found until symptoms develop, in later stages, when survival rates can plummet as low as 13%.
The problem with the “ick” factor
Current guidelines recommend that individuals at average risk for colon cancer (who have no personal or family history of colon cancer or related diseases) begin screening at age 45. So, given the importance of early detection, why are millions of eligible Americans still avoiding colon cancer screening? Simply put, many people find the traditional options — colonoscopy and stool-based tests — unpleasant or inconvenient.
While the tests are accurate, some
complete them. The screening rate for colon cancer in the United States is stagnant at about 59%, which falls well below the National Colorectal Cancer Roundtable’s goal of 80% for eligible individuals.
Shield works by detecting colon cancer signals in the bloodstream from DNA shed by tumors.
people just don’t want to deal with the special diets, colon cleanouts, discomfort, and extra time off work associated with colonoscopy or the “ick” factor of handling stool. In fact, studies show that only 28-71% of patients who are prescribed these screening methods
Colon cancer screening is only effective if you complete the test. With 53,000 Americans expected to die from colon cancer in 2024, we need another option for the millions who are avoiding screening.
A more pleasant screening option
The good news is that the FDA approved a new screening option earlier this year that could be more appealing for many people. With Shield™, a blood test for screening adults age 45 and older at average risk for colon cancer, the process is as simple as getting a blood draw during any healthcare visit. The convenience and the more pleasant nature of the test appear to make a difference: One
study showed that more than 90% of people who were given a prescription for the test completed it.
Shield works by detecting colon cancer signals in the bloodstream from DNA shed by tumors. After a simple blood draw, your screening results — and the peace of mind of knowing your status — are available in approximately two weeks. (If the test is positive, you’ll need to have a colonoscopy to confirm whether you have cancer.)
The FDA approval of the test was based on results from the ECLIPSE study, published in The New England Journal of Medicine. One of the largest cancer screening studies of its kind, enrolling more than 20,000 people, ECLIPSE showed that Shield has 83% sensitivity, which means the test accurately identifies 83% of individuals with colorectal cancer. This performance is within range of other non-invasive screening methods recommended in current screening guidelines, in which overall sensitivity ranges from 74-92%.
Making screening a no-brainer
Many people today make it a priority to take care of their health — eating well, exercising, and seeing a healthcare provider for annual check-ups. But when it comes to colon cancer screening, they’re just not as proactive as they would ordinarily be — often to their own detriment.
Dennis B., a 55-year-old attorney, was diagnosed with a benign brain tumor in 2018, so his doctor ran a battery of screening tests. He mentioned screening for colon cancer to Dennis for the first time and recommended a colonoscopy. Dennis agreed to schedule it.
However, despite his best intentions, Dennis didn’t follow through with scheduling his colonoscopy. And for several years after that, he also didn’t complete the paperwork required to receive an at-home stool-based screening test.
When Dennis saw his doctor recently — still holding out on screening — his doctor told him that he now had a different screening option for him; one that could be done conveniently and required no special preparation, diet
options to improve access
This blood test is a much more pleasant way to screen, and the convenience of it makes getting screened pretty much a no-brainer.
changes, sedation, or stool collection.
It was the Shield blood test. Dennis was intrigued by this new option for screening and agreed to try it. Fortunately, the results came back normal.
He later commented, “Most people in my situation know we’re supposed to get screened for colon cancer, but it’s hard to find the time to schedule it if you have a busy life and a demanding job. I realized I had taken quite a risk by waiting so long to screen. This blood test is a much more pleasant way to screen, and the convenience of it makes getting screened pretty much a no-brainer.”
In addition to the simplicity of it, screening with a blood draw during a routine healthcare checkup can be much easier for many people who don’t have good access to healthcare facilities or transportation, or don’t have flexibility in their job schedule or paid time off. Indeed, studies show that when healthcare providers offer different screening options, it can boost the number of people getting tested, which in turn could potentially reduce colon cancer deaths because patients can get earlier treatment.
The Shield test is already covered by Medicare, so if you have Medicare Part B, you’ll have no out-of-pocket cost. If you have a Medicare Advantage plan, you may have a copay. Coverage by commercial insurance plans typically depends on the test being included in screening guidelines established by the American Cancer Society and the U.S. Preventive Services Task Force (USPSTF). Preventive healthcare services recommended by the USPSTF are covered by insurers with a $0 out-ofpocket cost for patients. (The USPSTF colon cancer screening guidelines have not been updated since 2021.) This would make the test more affordable and accessible for the millions of individuals looking for an alternative screening option.
Take action now to protect your health Don’t let the inconvenience or the “ick” factor of traditional colon cancer screening tests stop you from taking care of your health. Early detection can save your life, and now the Shield blood test makes screening more pleasant and more convenient than ever before.
If you’re 45 or older, at average risk, and are due for colon cancer screening, talk to your healthcare provider about what screening option makes the most sense for you, or visit ShieldCancerScreen.com for more information.
References are available upon request; please email press@guardanthealth.com.
To learn more, visit ShieldCancerScreen.com
More
WRITTEN BY Craig Eagle, M.D. Chief Medical Officer, Guardant Health
How AI Is Impacting GI Care — and Improving Patient Outcomes
Our panel of experts talked about the growing use of artificial intelligence in GI care, particularly during colonoscopies, and what this means for the diagnosis and treatment of colorectal cancer and other GI disorders.
Austin Lee Chiang, M.D., M.P.H. Chief Medical Officer, Medtronic Endoscopy
What are the newest, most impactful advancements in the GI care space today?
Austin Lee Chiang: The field of gastroenterology is experiencing a significant transformation driven by innovation. One of the most impactful advancements is the integration of artificial intelligence (AI) in colonoscopy procedures, specifically technologies like GI Genius. As the first FDA-cleared, AI-assisted colonoscopy device, GI Genius enhances a physician’s ability to detect colorectal cancer and precancerous lesions in real time, which is critical for improving early detection and prevention.
Beyond AI, advances in therapeutic endoscopy and minimally invasive techniques are allowing us to treat more conditions without the need for traditional surgery. Additionally, innovations in diagnostic tools, such as capsule endoscopy and molecular testing, are making it easier to uncover underlying GI disorders early and tailor treatment to individual patient needs. Advances in drug development targeting gut hormones have also brought about medications like GLP-1 agonists, which have led to significant weight loss outcomes that have been widely publicized.
Jonathan Ng: AI is transforming the healthcare industry. In recent years, the U.S. Food and Drug Administration authorized over 900 AI devices that have demonstrated a positive impact on patient care.
In the colorectal cancer screening space, AI is now helping physicians better identify problem areas during screening colonoscopies before they worsen or progress into cancer.
During a colonoscopy, advanced AI
technology like Iterative Health’s SKOUT can serve as an extra set of eyes trained to recognize the most frequently overlooked abnormalities during a traditional colonoscopy — subtle, flat lesions often referred to as “sessile” polyps.
In addition to the benefits for patients, AI polyp detection technology has also evolved to play an important role in combating physician burnout, which nearly 50% of providers face today.
A common concern with early versions of AI for polyp detection was that frequent false alerts made the procedure taxing for physicians, causing them to lose trust in technology and tune it out entirely. Today, AI algorithms like those powering SKOUT have been significantly fine-tuned to maximize the detection of what’s clinically meaningful while minimizing false alerts.
Physicians performing colonoscopies with SKOUT have shared that they not only provide higher-quality exams, but also feel less exhausted after a long day of procedures when they have AI as an extra set of eyes.
J. Casey Chapman: The field of GI medicine is in a bit of a Renaissance period in many ways. There have been many advancements in just the past few years. Medical therapies for diseases like inflammatory bowel disease, which includes both ulcerative colitis and Crohn’s disease, have made great strides, being able to document clinical improvement and, most importantly, actual healing of the affected segment(s) of the GI tract. These medications have paved the way for what is now called “treat to target,” with the target being the absence of inflammation, focusing beyond symptom control.
Jonathan Ng, M.B.B.S. Founder & CEO, Iterative Health
GI Alliance Research sites, located throughout the country, have been fortunate to be on the forefront of these medical advancements, and being able to offer them to our patients with chronic disease. It’s a very exciting time as we have seen with many new recent treatments, but we will be seeing many more on the short-term horizon. Other impactful advancements include new personalized or bespoke ways to diagnose and monitor certain populations. For example, we now have tests that can help us detect who may be at higher risk for esophageal cancer, allowing those patients to be seen and evaluated sooner.
Another prime example of impactful innovation is the recent collaboration between GI Alliance and Medtronic, which introduces the GI Genius™ system. This AI-powered device aids in detecting colorectal polyps during colonoscopy, significantly improving early detection rates of colorectal cancer. By offering this advanced technology, GI Alliance physicians are enhancing patient care by increasing the likelihood of identifying precancerous polyps early, which leads to timely interventions and better outcomes. Using GI Genius can reduce the risk of missed polyps, giving patients a higher level of confidence in their screenings, ultimately lowering the incidence of colorectal cancer.
How does utilizing AI in GI care impact patient outcomes?
ALC: AI, particularly in the form of computer-aided polyp detection tools like GI Genius, acts as a powerful assistant to GI specialists. It works by highlighting areas of the colon that may contain polyps, ensuring we don’t miss
J. Casey Chapman, M.D. Chief Medical Officer, GI Alliance
abnormalities during a colonoscopy — a challenge even for experienced physicians.
Studies show that technologies like GI Genius can improve the adenoma detection rate, which is directly linked to better patient outcomes, including reduced colorectal cancer rates. Importantly, GI Genius has also been shown to reduce the adenoma miss rate by up to 50%, providing an even stronger layer of support during screenings. By enabling us to detect and remove more precancerous polyps, AI improves early detection, helps prevent cancer, and ultimately leads to better survival rates for patients.
JN: One in 24 Americans is diagnosed with colorectal cancer in their lifetime, and colonoscopy is the gold standard of prevention and early detection. When caught early, colorectal cancer has a 90% survival rate, and AI is an exciting new tool supporting physicians in providing the most advanced screenings for their patients.
A large U.S. clinical trial of more than 1,300 patients, which used Iterative Health’s SKOUT technology, found that even for highly experienced physicians, adding AI technology boosted detection of precancerous lesions without increasing the removal of benign tissue.
JCC: AI-powered tools have shown great promise in detecting GI diseases early, such as colorectal cancer and colon polyps, through enhanced image recognition during colonoscopies. The early detection of polyps is key to preventing colorectal cancer. Machine learning algorithms can analyze endoscopic images with high accuracy,
identifying abnormalities that may be missed by the human eye. This has real potential to improve early detection, which is crucial for conditions like colorectal cancer, thereby reducing mortality rates.
By automating certain tasks, such as clinical documentation, AI allows healthcare providers to focus more on the patient interaction and critical clinical decision-making. This improved efficiency can reduce waiting times, lead to better patient satisfaction, improve outcomes, and decrease provider burnout.
How can GI specialists stay connected and share information in order to uplevel the industry as a whole?
ALC: Collaboration within the GI industry is critical to driving progress and improving care for patients. By partnering through professional societies, attending conferences, and participating in research initiatives, GI specialists can share best practices and stay informed about the latest advancements.
Collaboration also extends to working
with organizations like the Colorectal Cancer Alliance and FightCRC, who have partnered with us to educate the public about colorectal cancer prevention and innovative tools like GI Genius. These partnerships strengthen our collective ability to innovate and deliver better patient outcomes.
As a practicing GI, I’m also passionate about the power of social media to foster collaboration, educate, and dispel misconceptions about GI care. Platforms like Instagram, Twitter, and LinkedIn allow us to connect with both peers and patients, share knowledge, and promote preventive measures like colorectal cancer screening. Social media is a critical tool to reach wider audiences, demystify GI health, and build a more informed and empowered community.
JN: A direct line of communication between the users and developers of technology is critical for advancing GI care. Meaningful, frequent collaboration with physicians allows us to better understand clinical needs and to
relentlessly innovate GI technology like SKOUT.
Most recently, close consultation with a panel of more than 20 expert GI physicians enabled Iterative Health to boost SKOUT’s ability to detect clinically significant polyps by over 40% at double the speed, in just 6 months. These interactions help ensure innovations in GI technology are grounded in practical, clinical expertise.
JCC: With the rapid advancement in medical technology, it is more important than ever to share information on the latest advancements, research, and clinical practices. Some ways to accomplish this are through GI professional societies like the American College of Gastroenterology, American Gastroenterological Association, and the American Society of Gastrointestinal Endoscopy (ASGE). These provide GI physicians a platform to exchange insights, discuss challenges, and, most importantly, learn about new data and treatments.
More inward-facing ways to stay
abreast include collaborative research initiatives, allowing physicians to stay engaged with the latest innovations while contributing to advancements in the field. Virtual learning has also become a necessity, enabling the dissemination of knowledge in a more real-time manner by building virtual education universities that allow access to up-todate information on a large scale.
Last, but certainly not least, is mentorship and training, utilizing experienced GI specialists to mentor younger professionals, answering questions not only about the science but also the business practice of medicine, an area not covered in medical school or post-graduate medical training.
At GI Alliance, we really try to foster this culture of collaboration by not only participating in these societies but also hosting our own educational initiatives, research programs, and mentorship opportunities, which empowers our specialists to remain leaders in the field of gastroenterology while enhancing patient care nationwide.
Don’t Miss Out on Life’s Greatest Moments
Colorectal cancer is among the most detectable and treatable cancers, and regular screenings can significantly reduce risk.
At Olympus, we aim to help reduce the societal burden of colorectal cancer. Through colonoscopy screenings, physicians use Olympus technologies and tools to identify and remove the abnormalities that can lead to cancer.
Our vision is to build and deploy an Intelligent Endoscopy Ecosystem that connects our industry-leading hardware, consumables, and service with cloud-based AI solutions and data that work together, supporting physicians by improving efficiency and enabling them to focus on what matters most, their patients.
The Value of Colonoscopy Screening
As a practicing gastroenterologist, my colleagues and I spend much of our professional careers dedicated to the screening, surveillance, and treatment of colorectal cancer and precursor lesions called adenomas. Around 1.9 million colorectal cancer cases are diagnosed worldwide every year. Without early diagnosis, nearly half of those cases will be fatal.ii
The good news is that colorectal cancer and adenomas are highly treatable and curable when detected at early stages. Patients have options when it comes to effectively screening for colon cancer. Options include non-invasive stool tests, which can be taken at home, and direct visualization tests, the most accurate of which is colonoscopy. Although some newer blood tests are also available, longer-term data on their effectiveness is unknown, and the blood tests do not replace colonoscopy.
The U.S. Preventive Services Task Force recommends that adults ages 45 to 75 at average risk be screened for colorectal cancer.iii Exams should be performed earlier in the presence of family history or medical conditions. Ask your healthcare provider for more information if you have questions about your individual risk. You can also visit colonoscopytoday.com to learn more and find a doctor for colonoscopy screening.
Why do we perform colonoscopies?
Colonoscopies are performed to visually inspect the walls of the colon for several abnormalities that could be a healthcare concern for patients now or in the future. One of the most common
findings during screening colonoscopy is an adenoma.
An adenoma is a growth of abnormal tissue on the surface of the colon that may have the potential to transform into colon cancer over many years. Adenomas usually have no symptoms.
When gastroenterologists perform colonoscopy in practice, we are trained to be able to see and remove adenomas, which are then sent to the lab for analysis by our pathologist colleagues. Usually referred to as colon polyps, these adenomas are common, especially as you get older. Over 1 in 3 adults have adenomas.iv When found at early stages, they are easily removed. An endoscopist’s ability to find polyps during colonoscopy is known as their Adenoma Detection Rate, or ADR — a measurement of how often the endoscopist detects adenomas during procedures. This is an important number as research has shown that for every 1% increase in ADR, the risk of a fatal cancer developing between screening colonoscopies decreases by 3-5%.v
Medical technology development has been integral to the improvement of colonoscopy over the years. In fact, the field of gastroenterology is inextricably linked to these technological advancements.
Olympus, a leading medical technology company and a pioneer in gastrointestinal endoscopy, is committed to making screening more accessible and effective. Innovations in endoscopy, such as high-definition endoscopes, special tools we use for therapies and enhanced imaging capabilities, have rapidly advanced the field of endoscopy. These innovations have occurred in partnership with clinicians, as our scientific knowledge continues to grow.
An intelligent horizon
As we look to the future of GI endoscopy, I am filled with hope for how we all can positively impact patients in the communities they live in. The ultimate vision is an Intelligent Endoscopy Ecosystem — one that connects innovation, expertise, and AI decision support systems to allow more time for physicians to concentrate on our primary objective: taking care of our patients.
REFERENCES
Colorectal Cancer. World Health Organization. https://www.who.int/news-room/fact-sheets/ detail/colorectal-cancer. July 11, 2023.
ii Screening and Surveillance for Colorectal Cancer Expanded Information. FASCRS.org. https:// fascrs.org/patients/diseases-and-conditions/a-z. Accessed Nov. 25, 2024.
iii U.S. Preventive Services Task Force, “Final Recommendation Statement, Colorectal Cancer: Screening.” May 18, 2021.
iv Patient Education: Colon Polyps. https://www.uptodate.com/contents/colon-polyps-beyond-the-basics/print. Accessed November 22, 2024. Corley, D.A., Jensen, C.D., Marks, A.R., Zhao, W.K., Lee, J.K., Doubeni, C.A., Zauber, A.G., de Boer, J., Fireman, B.H., Schottinger, J.E. and Quinn, V.P., 2014. Adenoma detection rate and risk of colorectal cancer and death. New England journal of medicine, 370(14), pp.1298-1306.
WRITTEN BY Dr. Craig Munroe Gastroenterologist and Global Lead, Medical Affairs, GI Endo Therapy, Olympus
Scan here to learn more:
Black Americans Are at Greater Risk for Colorectal Cancer
Colorectal cancer is the third most common cancer among men and women in the Black community.
In the United States, Black Americans tend to experience earlier onset and worse disease outcomes, and they have the second-highest incidence and mortality rates of colorectal cancer. They are 15% more likely to develop the disease and 35% more likely to die from it than nonHispanic white Americans. Rates of early-onset colorectal cancer in the Black community are also increasing. Screening is the number one way to prevent colorectal cancer or find it early when it is highly treatable. Colorectal cancer has about a 90% survival rate with early detection and treatment. That’s why it’s critical for Black Americans to know colorectal cancer risk factors, symptoms, and screening options.
What to know
A prominent risk factor for colorectal cancer is being a Black American. As noted above, Black people have a higher incidence rate of the disease. Other risk factors include a family history of colorectal cancer; certain inherited genetic syndromes like Lynch syndrome; chronic inflammatory bowel diseases, such as ulcerative colitis or Crohn’s disease; and type 2 diabetes.
Symptoms to look for include a change in bowel habits, rectal bleeding, abdominal discomfort, weakness and/or fatigue, and unexplained weight loss. There are a variety of screening options, including colonoscopies and at-home screening tests, depending on your individual risk factors.
The Colorectal Cancer Alliance offers a free,
Believe
easy quiz that provides a screening recommendation based on personal risk factors at quiz.getscreened.org. You can print the results and share them with your doctor.
The Colorectal Cancer Alliance works to empower people to better navigate colorectal cancer outcomes in their lives and communities. This includes ongoing local and national efforts to increase awareness among young Black people who might not know their risk factors, and providing resources and screening assistance aimed at early detection. We offer certified care navigators and financial assistance for non-medical expenses related to colorectal cancer screening and treatment. Visit colorectalcancer.org/health-equity to learn more about the Alliance’s Health Equity initiatives and impact.
the Hype: Rapper Chuck D Says Colorectal Cancer Screenings Save Lives
As a member of the rap group Public Enemy, Carlton Ridenhour (AKA Chuck D) has never been afraid to take a stand for what he believes in. Now a collaborating artist with Hip Hop Public Health, which has partnered with Stand Up To Cancer, Chuck D is urging people to get screened for colorectal cancer.
What inspired you to start raising awareness about colorectal cancer?
We’ve all lost someone, and in a lot of situations, there were things that could have been done to keep them healthier and on this Earth longer. Sometimes it’s something as basic as getting check-ups.
I learned from Hip Hop Public Health that Black people tend to get diagnosed with colorectal cancer after it’s already progressed, and that leads to higher death rates — higher than any other racial or ethnic group in the United States.
Why is it important to encourage all people over 45, but especially people of color, to get screened for colorectal cancer?
There’s long been distrust with doctors and
people in public administration because they’ve ignored us for so long, and as a result there’s a tendency to not go to the doctor. At the same time, there’s an over-trust in the things we consume blindly that are slowly killing us. So, there’s a lot to overcome, but the work Hip Hop Public Health does is a good way to get in there and change things up.
Is there anything you’d like to say to our readers to encourage them to get screened?
If you’re 45, or if you’re younger and have a family history of colorectal cancer, get screened. Period. You should get screened even if you don’t have any symptoms.
WRITTEN BY
Angele Russell
Senior Director of Health Equity, Colorectal Cancer Alliance
Chuck D | Photo courtesy of Travis Shinn
Putting Yourself First: Early Detection For Colon Cancer Matters
A colon cancer screening test shipped to your home could help detect cancer early.
Leigh Anne has lived a life showing up for others. As a mom, wife, and teacher, she has dedicated her time to caring for and helping those around her. Because of this, she, like many, put off having a colonoscopy. There were too many other things to worry about. After seeing her mom battle breast cancer, Leigh Anne knew about cancer, but colorectal cancer wasn’t top of mind. She saw her doctor regularly and every visit he would mention that she was overdue for a colonoscopy.
Colorectal cancer is the third most diagnosed cancer and the second leading cause of cancer deaths in the United States.1 Even as colorectal cancer deaths are increasing in people younger than 50 years old, more than 60 million Americans are not up to date with colorectal cancer screenings.2
“After having the same discussion year after year with my doctor, he mentioned that there are these Cologuard® box tests for colorectal cancer screening,” Leigh Anne said. “I was so fearful of anesthesia and having a colonoscopy, that I made a deal with my doctor. If the Cologuard test was positive, I would promise to get a colonoscopy.”
Within two weeks, Leigh Anne received her results. The Cologuard test was positive.
“My husband drove me, and I went in for my colonoscopy,” Leigh Anne said. “I woke up and was brought out to where he was and I asked, ‘I have cancer, don’t I?’ and he said, ‘Yes, you do.’”
Leigh Anne’s world was turned upside down, but she knew she needed to be authentic and model strength, resilience and hope — for the high school students she teaches and for her family. She made her lesson plans for when she would be gone and scheduled her surgery.
An early catch
After the surgery was complete, Leigh Anne received a call from her surgeon. Her cancer was stage 1, her margins were clear, and she would need no radiation or chemotherapy. Her cancer was caught early.
A non-invasive, easy-to-use test, like the Cologuard test, is a simple and effective way to screen for colorectal cancer. In a recent study, when Cologuard tests detected cancer, an estimated 80% were early-stage and precancerous cases, meaning they would be easier to treat or even prevent when they were detected. 3,4*
“Early detection is the most important predictor of colorectal cancer survival5,” said Dr. Folasade May, gastroenterologist and director of quality in digestive diseases at UCLA Health. “Now the American Cancer Society encourages people at average risk for colorectal cancer — meaning anyone who isn’t high risk — start routine screening at age 45.6 Cologuard is an effective, easy to use option to screen.” †
Leigh Anne learned that the best way to show up for others is showing up for herself and that includes prioritizing her health and screening. This past year, she celebrated 10 years of marriage — just one of the many milestones she’s been able to be a part of since surviving cancer. She has also seen one daughter get married, two become engaged, and is now a grandmother to three grandchildren. In part, she thanks early detection for giving her the chance to celebrate each of these moments.
In the past 10 years, the equivalent of one Cologuard test was completed every 20 seconds.7* It’s FDA approved and convenient – delivered right to your door, with no preparation, no time off and no changes to your diet or medication required.8 Cologuard detects 92% of colon cancers, even in early stages. It’s also covered by Medicare and most other major insurers, meaning more than 94% of people pay nothing.9 If you do need a follow-up colonoscopy, there is no cost sharing applied.10,11
“Now my adventures can continue,” Leigh Anne said. “This is part of my story and if I can make a difference in someone else’s story and help them screen and potentially catch cancer early, I want to do that too.”
Written by Laura Anderson, Exact Sciences
The Cologuard test is intended to screen adults 45 years of age and older who are at average risk for colorectal cancer by detecting certain DNA markers and blood in the stool. Do not use if you have had adenomas, have inflammatory bowel disease and certain hereditary syndromes, or a personal or family history of colorectal cancer. The Cologuard test is not a replacement for colonoscopy in high risk patients. Cologuard performance in adults ages 45-49 is estimated based on a large clinical study of patients 50 and older. Cologuard performance in repeat testing has not been evaluated.
The Cologuard test result should be interpreted with caution. A positive test result does not confirm the presence of cancer. Patients with a positive test result should be referred for colonoscopy. A negative test result does not confirm the
REFERENCES
* Estimates are based on modeling projections using performance data from the pivotal DeeP-C study. †Dr. Folasade May has provided consulting services for Exact Sciences. They have not been compensated for any media work.
1 American Cancer Society. Colorectal Cancer Facts & Figures 2023-2025. Atlanta: American Cancer Society; 2023.
2 Ebner DW, Kisiel JB, Fendrick AM, et al. Estimated average-risk colorectal cancer screening-eligible population in the US. JAMA Netw Open. 2024;7(3):e245537.CDC
3 Imperiale TF, Ransohoff DF, Itzkowitz SH, et al. Multitarget stool DNA testing for colorectal-cancer screening. N Engl J Med. 2014;370(14):1287-1297
4 Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024.CA Cancer J Clin. 2024;74:12-49. 2 Itzkowitz SH. Incremental advances in excremental cancer detection tests. J Natl Cancer Inst. 2009;101(18):1225-1227. doi:10.1093/jnci/djp273
5 National Cancer Institute. Cancer stat facts: colorectal cancer. Accessed October 7, 2022. https://seer. cancer.gov/statfacts/html/colorect.html
6 ACS. Guideline for Colorectal Cancer Screening. Accessed March 6, 2024. Updated January 29, 2024. https://www.cancer.org/cancer/types/colon-rectal-cancer/detection-diagnosis-staging/acs-recommendations.html
7 Estes C, Dehghani M, Ozbay A, et al. Clinical, social and economic impacts of colorectal cancer screening with the multi-target stool-DNA test: 10-year experience – a simulated study. MedRxiv.org https://doi. org/10.1101/2024.08.07.24311643
9 Exact Sciences estimate based on historical patient billing. Rate of coverage varies by state and region. Exceptions for coverage may apply; only your patients’ insurers can confirm how Cologuard would be covered. 10 CMS. FAQs about Affordable Care Act implementation part 51, Families First Coronavirus Response Act and Coronavirus Aid, Relief, and Economic Security Act implementation. Centers for Medicare & Medicaid Services. January 10, 2022. Accessed January 25, 2024. https://www.cms.gov/CCIIO/Resources/FactSheets-and-FAQs/Downloads/FAQs-Part-51.pdf
11 CMS. Calendar year (CY) 2023 Medicare physician fee schedule final rule. Centers for Medicare & Medicaid Services. November 1, 2022. Accessed January 25, 2024. https://www.cms.gov/newsroom/fact-sheets/ calendar-year-cy-2023-medicare-physician-fee-schedule-final-rule
To learn more about the Cologuard’s testing kit, visit Cologuard.com
absence of cancer. Patients with a negative test result should discuss with their doctor when they need to be tested again. False positives and false negative results can occur. In a clinical study, 13% of people without cancer received a positive result (false positive) and 8% of people with cancer received a negative result (false negative). Rx only.
This story reflects on an individual’s experience. Not every person will have the same treatment, experience, outcome, or result. The Cologuard test is prescribed by your health care provider. Talk to your health care provider about available screening options and whether the Cologuard test may be right for you. There are potential risks associated with the Cologuard test and it may not be appropriate for all patients. For more information about the risks, talk to your health care provider or visit www.cologuard.com for more information.
Leigh Anne | Photo courtesy of Exact Sciences
ABOUT THE COLOGUARD TEST
How an Early Colonoscopy Greatly Improved One Woman’s Cancer Prognosis
Advocating for herself and her own health led Brooks Bell to seek an early colonoscopy, which led to a colon cancer diagnosis. Now cancer-free for five years, she partnered with the Colorectal Cancer Alliance on Lead From Behind to encourage others to get screened as soon as they’re able.
In 2018, Brooks Bell felt she was in her prime. She was 38, married to her longtime partner, happily living in North Carolina, and maintaining a healthy lifestyle. Bell was also running a digital analytics agency she founded in her 20s and leading a team of 50 employees. Everything changed when she was at a business conference and noticed blood in her stool. She immediately hopped on a telehealth call from her hotel room. The doctor told her she was young; it was nothing to worry about.
After two months of having bloody stool, Bell knew something was wrong. She went to a gastroenterologist and had a colonoscopy.
“I had to advocate for myself,” Bell said. “I was bleeding inside. That cannot be a sign of good health.”
That colonoscopy revealed that Bell had Stage III colon cancer. She had an 87% chance of survival.
“I was pretty lucky, even though it was Stage III,” Bell said. “I still had pretty good odds of survival. If the tumor had a chance to go even a millimeter deeper into my colon wall, my odds of survival would have dropped 10 points.”
Cancer treatment
For the next six months, Bell underwent treatment, which included surgery that took out some of her colon and three months of intensive chemotherapy. Her treatment plan took six months in total.
She was then declared cancer-free, but that didn’t mean she was in the clear. There was a chance the cancer would return in the next two years.
“I was deeply anxious,” Bell said. “I had nightmares. I felt like I had to do everything I could to reduce my chance of recurrence.”
She threw herself into high-intensity exercise and learned to cook most of her meals to feel some sense of control. Bell ended up training for and competing in a triathlon. It’s now been over five years, and she’s still cancer-free.
An advocate for early colonoscopies Bell’s cancer journey inspired her to create Lead From Behind in partnership with the Colorectal Cancer Alliance, the nation’s leading nonprofit organization dedicated to ending colorectal
cancer. Lead From Behind aims to raise awareness about the importance of colonoscopies and early screening. She wants everyone to get checked as soon as they turn 45 — the age some insurances cover the procedure.
“Colonoscopies actually prevent colon cancer,” Bell said. “The procedure doesn’t just diagnose the cancer early on, it can also prevent it.”
Bell explained that before a cancerous tumor forms in the colon, it’s a polyp. Colonoscopies can spot and remove the polyp during the procedure, eliminating the possibility of it becoming cancer.
Bell said she knows many people are scared of getting the life-saving procedure, but she calls it a “spa day.”
“It’s no longer your grandfather’s colonoscopy,” she said. “It doesn’t
hurt. You’re actually asleep for only 25 minutes, and it will be the best nap, the best sleep you’ve ever had. It’s not like you’re getting a big scary surgery.” If you’re under 45 years old, Bell said talking is the most important thing you can do. Talk to your family members to make sure they’re getting tested and learn if there is any history of colon cancer in the family. And talk to your doctor.
“Don’t be afraid to talk about your poop with your doctor,” Bell said. “If you have something weird going on down there, you need to bring it up.”
Written by Frank James
Interview with Brooks Bell, Founder, Lead From Behind
Brooks Bell (left) and her husband, Jesse Lipson Photo courtesy of Brooks Bell
Time for your colonoscopy
ARE YOU 45 YEARS OF AGE OR OLDER?
Time for your colonoscopy
If
If not removed, polyps may become cancerous over time
If not removed, polyps may become cancerous over time
More than 90% of polyps can be found by a colonoscopy
More than 90% of polyps can be found by a colonoscopy
More than 90% of polyps can be found by a colonoscopy
Time for your colonoscopy
A colonoscopy is a common, painless procedure during which your healthcare provider uses a camera to look inside your rectum and entire colon for small growths called polyps.
A colonoscopy is a common, painless procedure during which your healthcare provider uses a camera to look inside your rectum and entire colon for small growths called polyps.
A colonoscopy is a common, painless procedure during which your healthcare provider uses a camera to look inside your rectum and entire colon for small growths called polyps.
PLENVU® requires less overall liquid to drink vs standard bowel preps
PLENVU®
A camera used by healthcare providers to look for small growths called polyps
For your colonoscopy prep, is designed with you in mind
Note: It is important to drink sufficient clear liquids before, during, and after the
INDICATION
IMPORTANT SAFETY INFORMATION
PLENVU® requires less overall liquid to drink vs standard bowel preps
PLENVU® (polyethylene glycol 3350, sodium ascorbate, sodium sulfate, ascorbic acid, sodium chloride, and potassium chloride for oral solution) is a prescription medication used by adults to clean the colon before a colonoscopy.
PLENVU® requires less overall liquid to drink vs standard bowel preps
PLENVU® 32 oz medicine
camera used by healthcare providers to look for small growths called polyps
• Do not take PLENVU® if you have a blockage in your intestine (bowel obstruction), an opening in the wall of your stomach or intestine (bowel perforation), problems with food or fluid emptying from your stomach (gastric retention), a problem with food moving too slowly through your intestines (ileus), a very dilated large intestine, or an allergy to any of the ingredients in PLENVU®.
Note: It is important to drink sufficient clear liquids before, during, and after the use of PLENVU®.
Note: It is important to drink sufficient clear liquids before, during, and after the use of PLENVU®.
INDICATION
INDICATION
PLENVU® 32 oz medicine PLUS AT LEAST 32 OZ ADDITIONAL CLEAR LIQUIDS vs 128 oz medicine ADDITIONAL CLEAR LIQUIDS MAY BE
Scan for helpful resources < ASK YOUR DOCTOR ABOUT PLENVU®
PLENVU®
dry mouth, urinating less often than normal; headache, or feel faint, weak, or lightheaded, especially when you stand up.
• PLENVU® can cause ulcers of the bowel or bowel problems (ischemic colitis). Tell your healthcare provider right away if you have severe stomach-area (abdomen) pain or rectal bleeding.
• PLENVU® can cause serious allergic reactions that may include skin rash, itching, raised red patches on your skin (hives); swelling of the face, lips, tongue, and throat; and kidney problems.
PLUS AT LEAST 32 OZ ADDITIONAL CLEAR LIQUIDS vs 128 oz medicine ADDITIONAL CLEAR LIQUIDS MAY BE CONSUMED
• PLENVU® and other bowel preparations can cause serious side effects including loss of body fluid (dehydration) and changes in blood salts (electrolytes) in your blood. These changes can cause abnormal heartbeats that may result in death, seizures (even if you have never had a seizure), or kidney problems. Your chance of having fluid loss and changes in body salts with PLENVU® is higher if you have heart problems, kidney problems, or take water pills, high blood pressure medicine, or non-steroidal anti-inflammatory drugs (NSAIDS).
• The most common side effects in patients taking PLENVU® were nausea, vomiting, dehydration, and stomach pain or discomfort.
• Your healthcare provider may do blood tests after you take PLENVU® to check your blood for changes. Tell your healthcare provider right away if you have any symptoms of too much fluid loss (dehydration) including vomiting, dizziness, heart problems, kidney problems, seizures,
PLENVU® (polyethylene glycol 3350, sodium ascorbate, sodium sulfate, ascorbic acid, sodium chloride, and potassium chloride for oral solution) is a prescription medication used by adults to clean the colon before a colonoscopy.
IMPORTANT SAFETY INFORMATION
IMPORTANT SAFETY INFORMATION
• Do not take PLENVU® if you have a blockage in your intestine (bowel obstruction), an opening in the wall of your stomach or intestine (bowel perforation), problems with food or fluid emptying from your stomach (gastric retention), a problem with food moving too slowly through your intestines (ileus), a very dilated large intestine, or an allergy to any of the ingredients in PLENVU®.
PLENVU® (polyethylene glycol 3350, sodium ascorbate, sodium sulfate, ascorbic acid, sodium chloride, and potassium chloride for oral solution) is a prescription medication used by adults to clean the colon before a colonoscopy.
ASK YOUR DOCTOR ABOUT PLENVU®
Tell your healthcare provider about all of your medical conditions and medicines you take, including prescription, nonprescription medicines, vitamins, and herbal supplements before you take PLENVU®.
4-LiterPrep
• PLENVU® and other bowel preparations can cause serious side effects including loss of body fluid (dehydration) and changes in blood salts (electrolytes) in your blood. These changes can cause abnormal heartbeats that may result in death, seizures (even if you have never had a seizure), or kidney problems. Your chance of having fluid loss and changes in body salts with PLENVU® is higher if you have heart problems, kidney problems, or take water pills, high blood pressure medicine, or non-steroidal anti-inflammatory drugs (NSAIDS).
resources ASK YOUR DOCTOR ABOUT PLENVU®
• Your healthcare provider may do blood tests after you take PLENVU® to check your blood for changes. Tell your healthcare provider right away if you have any symptoms of too much fluid loss (dehydration) including vomiting, dizziness, heart problems, kidney problems, seizures,
• Your healthcare provider may do blood tests after you take PLENVU® to check your blood for changes. Tell your healthcare provider right away if you have any symptoms of too much fluid loss (dehydration) including vomiting, dizziness, heart problems, kidney problems, seizures,
These are not all the possible side effects of PLENVU®. Ask your healthcare provider for more information.
Scan for helpful resources <
for
You are encouraged to report negative side effects of prescription drugs to the FDA. Visit www.fda.gov/medwatch or call 1-800-FDA-1088
For product information, adverse event reports, and product complaint reports, please contact Salix Product Information Call Center: Phone: 1-800-321-4576 or Fax: 1-510-595-818
dry mouth, urinating less often than normal; headache, or feel faint, weak, or lightheaded, especially when you stand up.
dry mouth, urinating less often than normal; headache, or feel faint, weak, or lightheaded, especially when you stand up.
Please see adjacent Brief Summary.
• PLENVU® can cause ulcers of the bowel or bowel problems (ischemic colitis). Tell your healthcare provider right away if you have severe stomach-area (abdomen) pain or rectal bleeding.
• PLENVU® can cause ulcers of the bowel or bowel problems (ischemic colitis). Tell your healthcare provider right away if you have severe stomach-area (abdomen) pain or rectal bleeding.
• Do not take PLENVU® if you have a blockage in your intestine (bowel obstruction), an opening in the wall of your stomach or intestine (bowel perforation), problems with food or fluid emptying from your stomach (gastric retention), a problem with food moving too slowly through your intestines (ileus), a very dilated large intestine, or an allergy to any of the ingredients in PLENVU®.
• PLENVU® and other bowel preparations can cause serious side effects including loss of body fluid (dehydration) and changes in blood salts (electrolytes) in your blood. These changes can cause abnormal heartbeats that may result in death, seizures (even if you have never had a seizure), or kidney problems. Your chance of having fluid loss and changes in body salts with PLENVU® is higher if you have heart problems, kidney problems, or take water pills, high blood pressure medicine, or non-steroidal anti-inflammatory drugs (NSAIDS).
• PLENVU® can cause serious allergic reactions that may include skin rash, itching, raised red patches on your skin (hives); swelling of the face, lips, tongue, and throat; and kidney problems.
• PLENVU® can cause serious allergic reactions that may include skin rash, itching, raised red patches on your skin (hives); swelling of the face, lips, tongue, and throat; and kidney problems.
• The most common side effects in patients taking PLENVU® were nausea, vomiting, dehydration, and stomach pain or discomfort.
• The most common side effects in patients taking PLENVU® were nausea, vomiting, dehydration, and stomach pain or discomfort.
• Tell your healthcare provider about all of your medical conditions and medicines you take, including prescription, nonprescription medicines, vitamins, and herbal supplements before you take PLENVU®.
• Tell your healthcare provider about all of your medical conditions and medicines you take, including prescription, nonprescription medicines, vitamins, and herbal supplements before you take PLENVU®.
These are not all the possible side effects of PLENVU®. Ask your healthcare provider for more information.
These are not all the possible side effects of PLENVU®. Ask your healthcare provider for more information.
You are encouraged to report negative side effects of prescription drugs to the FDA. Visit www.fda.gov/medwatch or call 1-800-FDA-1088.
You are encouraged to report negative side effects of prescription drugs to the FDA. Visit www.fda.gov/medwatch or call 1-800-FDA-1088.
For product information, adverse event reports, and product complaint reports, please contact Salix Product Information Call Center: Phone: 1-800-321-4576 or Fax: 1-510-595-818
For product information, adverse event reports, and product complaint reports, please contact Salix Product Information Call Center: Phone: 1-800-321-4576 or Fax: 1-510-595-818
Please see adjacent Brief Summary.
Please see adjacent Brief Summary.
A
IMPORTANT FACTS ABOUT PLENVU®
(plen-vu)
(polyethylene glycol 3350, sodium ascorbate, sodium sulfate, ascorbic acid, sodium chloride and potassium chloride for oral solution)
The risk information provided here is not comprehensive. To learn more, talk to your doctor about PLENVU®. Please see full Prescribing Information at www.myplenvu.com
What is the most important information I should know about PLENVU? PLENVU and other bowel preparations can cause serious side effects, including:
• Serious loss of body fluid (dehydration) and changes in blood salts (electrolytes) in your blood. These changes can cause: abnormal heartbeats that can cause death. seizures. This can happen even if you have never had a seizure. kidney problems.
Your chance of having fluid loss and changes in body salts with PLENVU is higher if you:
• have heart problems • have kidney problems.
• take water pills (diuretics), high blood pressure medicine or non-steroidal anti-inflammatory drugs (NSAIDs).
Tell your healthcare provider right away if you have any of these symptoms of serious loss of body fluid (dehydration) while taking PLENVU:
• vomiting • urinating less often than normal • dizziness • headache
See “What are the possible side effects of PLENVU?” for more information about side effects. What is PLENVU?
PLENVU is a prescription medicine used by adults to clean the colon before a colonoscopy. PLENVU cleans your colon by causing you to have diarrhea (loose stools). Cleaning your colon helps your healthcare provider see the inside of your colon more clearly during your colonoscopy. It is not known if PLENVU is safe and effective in children.
Do not take PLENVU if your healthcare provider has told you that you have:
• a blockage in your intestine (bowel obstruction).
• an opening in the wall of your stomach or intestine (bowel perforation).
• problems with food and fluid emptying from your stomach (gastric retention).
• a problem with food moving too slowly through your intestines (ileus).
• a very dilated intestine (toxic megacolon).
• an allergy to any of the ingredients in PLENVU. See the end of this Medication Guide for a complete list of ingredients in PLENVU.
Before taking PLENVU, tell your healthcare provider about all of your medical conditions, including if you:
• have problems with serious loss of body fluid (dehydration) and changes in blood salts (electrolytes).
• have heart problems.
• have seizures or take medicines for seizures.
• have kidney problems or take medicines for kidney problems.
• have stomach or bowel problems, including ulcerative colitis.
• have problems with swallowing, gastric reflux or if you inhale food or fluid into your lungs when eating or drinking (aspirate).
• have a condition called glucose-6-phosphate dehydrogenase (G6PD) deficiencythat destroys red blood cells.
• are withdrawing from drinking alcohol.
• have phenylketonuria (PKU). PLENVU contains phenylalanine.
• are allergic to any of the ingredients in PLENVU.
• are pregnant or plan to become pregnant. It is not known if PLENVU will harm your unborn baby. Talk to your healthcare provider if you are pregnant.
• are breastfeeding or plan to breastfeed. It is not known if PLENVU passes into your breast milk. You and your healthcare provider should decide if you will take PLENVU while breastfeeding.
Tell your healthcare provider about all the medicines you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements.
PLENVU may affect how other medicines work.
If you need to take any other medicines by mouth, take those medicines at least 1 hour before starting each dose of PLENVU.
Especially tell your healthcare provider if you take:
• medicines to treat a blood salt (electrolyte) imbalance.
• medicines for blood pressure or heart problems.
• medicines for seizures (antiepileptics).
• medicines for kidney problems.
• water pills (diuretics).
• non-steroidal anti-inflammatory drugs (NSAIDs).
• laxatives. Do not take other laxatives while taking PLENVU.
• medicines for depression or other mental health problems.
• starch based thickeners. For patients who have trouble swallowing, do not mix PLENVU with starch-based thickeners
Ask your healthcare provider or pharmacist for a list of these medicines if you are not sure if you are taking any of the medicines listed above.
Know the medicines you take. Keep a list of them to show your healthcare provider and pharmacist when you get a new medicine.
What are the possible side effects of PLENVU?
PLENVU can cause serious side effects including:
• Changes in certain blood tests. Your healthcare provider may do blood tests after you take PLENVU to check your blood for changes. Tell your healthcare provider if you have any symptoms of too much fluid loss, including: vomiting ‒ heart problems ‒ seizures dizziness ‒ kidney problems ‒ dry mouth feel faint, weak or lightheaded especially when you stand up (orthostatic hypotension)
• Ulcers of the bowel or bowel problems (ischemic colitis): Tell your healthcare provider right away if you have severe stomach-area (abdomen) pain or rectal bleeding.
• Serious allergic reactions. Symptoms of a serious allergic reaction may include: skin rash raised red patches on your skin (hives) kidney problems itching swelling of the face, lips, tongue and throat
The most common side effects of PLENVU include:
nausea • vomiting • dehydration • stomach pain or discomfort
These are not all the possible side effects of PLENVU.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
General information about the safe and effective use of PLENVU.
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use PLENVU for a condition for which it was not prescribed. Do not give PLENVU to other people, even if they are going to have the same procedure you are. It may harm them. You can ask your pharmacist or healthcare provider for information that is written for health professionals.
Distributed by: Salix Pharmaceuticals, a division of Bausch Health US, LLC Bridgewater, NJ 08807 USA
Manufactured by: Norgine Limited, 7 Tir-y-berth Industrial Estate New Road, Tir-y-berth, Hengoed, CF82 8SJ United Kingdom (GBR)
The Laboratory’s Role in Transforming Cancer Care
Pathologists and medical laboratory scientists play a unique but essential role in diagnosing and treating cancer.
Receiving a cancer diagnosis is scary. It can feel like there are an endless number of unknowns, from the general question of “how bad is it?” to what your treatment and care will look like to what your life will look like as a survivor.
A cancer diagnosis 10 or 20 years ago left a lot of these questions unanswered, but advancements in cancer screening, diagnosis, and treatment have been able to drastically transform unknowns into knowns. The medical laboratory is central to providing those answers. Pathologists and medical laboratory scientists play a unique but essential role in cancer care — we are the ones who run the tests that screen and detect the indicators of cancer. We are the ones who confirm the diagnosis with your primary care physician, who collaborate with your oncologist to establish the right
course of treatment at the right time that is right for you.
To ensure patients are receiving the highest quality care, the pathology and medical laboratory science community continually works toward advancing diagnostics in four main areas.
Screening
You’ve probably heard of molecular diagnostics, or molecular testing, which is the process of analyzing the genome for biological markers that may indicate a medical issue. Molecular testing has become an essential part of practice in pathology and laboratory medicine, and in some cases it has paved the way for new screening approaches, such as for human papillomavirus or colon cancer. These advancements are available now, but they’re also paving the way for future screening tests for 20-50 different types of cancers using samples of blood
or stool, which can mean earlier detection and treatment for patients.
Diagnosis
Along with molecular testing, genetic sequencing — and direct sequencing of tumor variants — is quickly becoming the standard of care for patients with a new cancer diagnosis. Your tumor variant may mean a different prognosis or a different sensitivity to a potential treatment. These new tests enable us to diagnose cancer on a more personalized level.
Treatment
Prognostic testing — performing a test specifically to determine if a patient can receive a certain drug — has been a mainstay in cancer treatment, but in the past five years, its use has revolutionized cancer care. Pairing prognostic testing with specific cancer therapies can better target a patient’s tumors and potentially provide a better outcome.
Post-treatment surveillance
Once a course of cancer treatment is completed, patients continue to be monitored to determine if the treatment was successful. The laboratory has helped advance this standard of care, using high-sensitivity molecular testing that pushes the boundaries of the limits of detection. This can help determine if the cancer has returned or spread. The technologies used for screening, testing, and treating cancer are evolving rapidly, but the laboratory remains the central core of each new test. The screening, testing, and diagnosing we do as caregivers is essential both for patients and for the transformation of cancer care now and in the future.
Written by Kimberly W. Sanford, M.D., MASCP, MT(ASCP), Former President, American Society for Clinical Pathology
A Novel Treatment for Metastatic Colorectal Cancer Patients Changes the Game
For people living with metastatic colorectal cancer, a novel therapy offers favorable outcomes after they’ve finished chemotherapy.
Colorectal cancer (CRC) is one of the most common forms of cancer — and the second-deadliest. About 50% of CRC patients will progress to metastatic CRC (mCRC), meaning the cancer has spread to other organs. And with that progression comes a grim prognosis: The fiveyear survival rate with mCRC is just around 15%.
Most mCRC patients are treated with chemotherapy (often combined with other non-chemotherapeutic options). But the effectiveness of these treatments is limited.
“Current therapies are not adequate,” explained Dr. Ardaman Shergill, medical oncologist and assistant professor of medicine at the University of Chicago Medicine. “After first- and second-line chemotherapy, for most patients, the prognosis with later lines of therapy is less than a year, so there is a significant need for effective and generally tolerable treatment options for refractory disease.”
The need
The declining effectiveness of treatment is a significant challenge for people living with mCRC. Thihan Padukkavidana, Ph.D., Senior Scientific Director of Medical Affairs at Takeda Oncology, says “When patients with metastatic disease progress after initial chemotherapy interventions, having an effective therapy is key. In addition, because outcomes can be quite poor, impacting patients’ quality of life is absolutely important.”
Traditional mCRC treatments carry severe side effects and other impacts to daily activities. Chemotherapy is broad and can impact healthy cells alongside cancer cells, resulting in a range of side effects. And travel to cancer
centers for IV treatments can take a physical, mental, and financial toll on patients.
Researchers have been trying to find innovative options. “We haven’t really had a new molecule in this space in over a decade,” Dr. Padukkavidana noted. “There have been over 70 trials explored and terminated since 2010.”
But a recently approved novel treatment offers some hope for post-chemotherapy mCRC patients: FRUZAQLA® (fruquintinib).
The innovation
FRUZAQLA is not chemotherapy. It is a targeted therapy that affects vascular endothelial growth factor (VEGF) receptors, which are used by the body to generate blood vessels. Cancer uses this mechanism to stimulate blood vessel growth so it can grow. FRUZAQLA inhibits this process, slowing down cancer growth.
“FRUZAQLA is a unique VEGF inhibitor which shuts down all 3 of the VEGF receptor targets with limited off-target inhibition,” noted Dr. Padukkavidana.
FRUZAQLA offers several important benefits:
• It’s convenient to take. FRUZAQLA is a once-daily oral pill, without any food restrictions. Patients can take the medicine from anywhere.
• Effective: Studies (takeda.info/ FruzaqlaResults) have demonstrated that FRUZAQLA is effective. Specifically, in a clinical study, people with mCRC lived a median of 7.4 months with FRUZAQLA +
Best Supportive Care vs 4.8 months with placebo (sugar pill) + Best Supportive Care. While people taking FRUZAQLA can potentially experience a range of side effects including fatigue, rashes, and hypertension, these can usually be mitigated by adjusting the dosage.
Advocacy
It’s crucial that patients educate and advocate for themselves. “There are a few therapies out there in this setting, and they all have different side effects,” Dr. Padukkavidana said. “You have to advocate for the appropriate therapies that are effective while maintaining quality of life.”
To assist people living with CRC, Takeda Oncology offers Here2Assist, a comprehensive patient support program offering help with access to medications, financial support, and other helpful resources. Takeda Oncology has also created two doctor discussion guides for patients looking for helpful topics to bring up at their doctor visits—one that focuses on starting FRUZAQLA treatment, available at takeda. info/FruzaqlaGuide, and one that is for patients still evaluating their mCRC treatment options, available at takeda.info/mCRCGuide.
Dr. Padukkavidana adds a final plea — get a colonoscopy if you’re over the age of 45.
“Screening procedures like colonoscopies are incredibly important,” he said. “Life is precious. The test can identify the disease early so you can prevent it from progressing.”
To access Here2Assist, visit fruzaqla.com/ financial-support
To access FRUZAQLA patient resources, visit fruzaqla.com/ patient-resources
INTERVIEW WITH Dr. Ardaman Shergill Medical Oncologist, University of Chicago Medicine
INTERVIEW WITH Thihan Padukkavidana, Ph.D. Senior Scientific Director of Medical Affairs, Takeda Oncology
Photo credit: Tall Paul / Paul Olkowsk
What is FRUZAQLA?
FRUZAQLA is a prescription medicine used to treat adults with colon or rectal cancer that has spread to other parts of the body (metastatic colorectal cancer [mCRC]) and who have received previous treatment with certain anti-cancer medicines. It is not known if FRUZAQLA is safe and effective in children.
FRUZAQLA may cause serious side effects, including:
• High blood pressure (hypertension). High blood pressure is common with FRUZAQLA and can also be severe. Your healthcare provider will check your blood pressure before starting treatment with FRUZAQLA,1 time every week for the first month of treatment, and then at least 1 time a month or more often if needed during treatment. Your healthcare provider may prescribe medicine to treat your high blood pressure if needed. Tell your healthcare provider if you get any of the following symptoms of hypertension during treatment:
o severe headache o lightheadedness or dizziness
o confusion o changes in vision
o chest pain o trouble breathing
o nosebleeds o vomiting
• Severe bleeding (hemorrhage). FRUZAQLA can cause bleeding that can be serious and may lead to death. Tell your healthcare provider if you get any of the following symptoms of bleeding during treatment:
o unusual, severe, or bleeding that will not stop
o bruising o lightheadedness
o vomiting blood or your vomit looks like coffee grinds
o blood in the stool or black stool that looks like tar
o blood in the urine or urine that looks red, pink, or brown
o coughing up blood or blood clots
o menstrual bleeding that is heavier than normal
o unusual vaginal bleeding o nose bleeds that happen often
• Infections. FRUZAQLA can increase the risk of infections, including serious infections that can lead to death. The most common infections with FRUZAQLA happened in the urinary tract, nose or throat, and lungs. Tell your healthcare provider if you get any of the following symptoms of infection during treatment:
o fever
o severe cough with or without an increase in mucus (sputum) production
o severe sore throat
o trouble breathing
o burning or pain when you urinate
o redness, swelling or pain in any part of the body
• A tear in your stomach or intestinal wall (gastrointestinal perforation). FRUZAQLA can cause gastrointestinal perforation that can be serious and may lead to death. Tell your healthcare provider right away if you get any of the following symptoms of gastrointestinal perforation during treatment:
o severe stomach (abdominal) pain or stomach pain that does not go away
o vomiting or vomiting blood
o blood in the stool or black stool that looks like tar
o fever or chills
o nausea
• Liver problems. Increased liver enzymes in your blood are common with FRUZAQLA and can also be severe and may lead to death. Your healthcare provider will do blood tests before and during treatment with FRUZAQLA to check for liver problems. Tell your healthcare provider if you get any of the following symptoms of liver problems during treatment:
o yellowing of your skin or the white part of your eyes
o dark-colored (tea-colored) urine
o pain in your right upper stomach-area (abdomen)
o loss of appetite
o nausea or vomiting
o bleeding or bruising
• Protein in your urine (proteinuria). Protein in your urine is common with FRUZAQLA and can also be severe. Your healthcare provider will check your urine for protein before starting and during treatment with FRUZAQLA. Tell your healthcare provider if you have to urinate more than usual, or if you get swelling of your face, hands, arms, legs, or feet during treatment.
• Hand-foot skin reactions (Palmar-Plantar Erythrodysesthesia [PPE]). Hand-foot skin reactions are common with FRUZAQLA and can also be severe. Tell your healthcare provider if you get a severe rash or redness, pain, blisters, bleeding, or swelling on the palms of your hands or soles of your feet during treatment.
• Posterior Reversible Encephalopathy Syndrome (PRES). PRES is a serious condition that can happen in your brain during treatment with FRUZAQLA. Tell your healthcare provider right away if you get any of the following symptoms during treatment:
o headache o seizures
o confusion o changes in vision
o problems thinking
• Wound healing problems. Wounds may not heal properly during treatment with FRUZAQLA. Tell your healthcare provider if you plan to have any surgery before starting FRUZAQLA or during treatment.
o You should stop taking FRUZAQLA at least 2 weeks before planned surgery.
o Your healthcare provider will tell you when you may start taking FRUZAQLA again after surgery.
• Blood clots in your blood vessels (arteries). FRUZAQLA can cause blood clots or blockage in your blood vessels that may lead to heart attack, stroke, or death. Get medical help right away if you get any of the following symptoms during treatment:
o severe chest pain or pressure
o pain in your arms, legs, back, neck or jaw
o shortness of breath
o numbness or weakness of your face, arm, or leg, especially on one side of your body
o feeling lightheaded or faint
o sweating more than usual
o sudden confusion, trouble talking or understanding things
o trouble walking
o sudden severe headache
o sudden vision changes in one or both eyes
o dizziness, or loss of balance or coordination
• Allergic reactions to FD&C Yellow No. 5 and FD&C Yellow No. 6. FRUZAQLA 1 mg capsules contain the inactive ingredients FD&C Yellow No. 5 (tartrazine) and FD&C Yellow No. 6 (sunset yellow FCF). FD&C Yellow No. 5 (tartrazine) can cause allergic-type reactions (including bronchial asthma) in certain people, especially people who also have an allergy to aspirin. FD&C Yellow No. 6 (sunset yellow FCF) can also cause allergic reactions. Tell your healthcare provider if you get hives, rash, or trouble breathing during treatment with FRUZAQLA.
The most common side effects of FRUZAQLA include:
• voice changes or hoarseness
• stomach-area (abdominal) pain
• diarrhea
• weakness, lack of strength and energy, and feeling very tired or sleepy (asthenia)
These are not all of the possible side effects of FRUZAQLA. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
Before taking FRUZAQLA, tell your healthcare provider about all of your medical conditions, including if you:
• have high blood pressure
• have bleeding problems
• have an infection
• have liver or kidney problems
• plan to have surgery or have had recent surgery. You should stop taking FRUZAQLA at least 2 weeks before your planned surgery. Your healthcare provider will tell you when you can start FRUZAQLA again after your surgery
• have recently had a blood clot, stroke, or heart attack
• are allergic to FD&C Yellow No. 5 (tartrazine) or FD&C Yellow No. 6 (sunset yellow FCF).
• are pregnant or plan to become pregnant. FRUZAQLA can harm your unborn baby. You should not become pregnant during treatment with FRUZAQLA.
Females who can become pregnant:
o Your healthcare provider will do a pregnancy test before you start treatment with FRUZAQLA.
o Use effective birth control (contraception) during treatment and for 2 weeks after your last dose of FRUZAQLA.
o Tell your healthcare provider right away if you become pregnant during treatment with FRUZAQLA.
Males with female partners who can become pregnant:
o Use effective birth control during treatment and for 2 weeks after your last dose of FRUZAQLA.
o Tell your healthcare provider right away if your partner becomes pregnant during your treatment with FRUZAQLA.
• are breastfeeding or plan to breastfeed. It is not known if FRUZAQLA passes into your breast milk. Do not breastfeed during treatment and for 2 weeks after your last dose of FRUZAQLA.
Tell your healthcare provider about all the medicines you take, including prescription and overthe-counter medicines, vitamins, and herbal supplements. FRUZAQLA may affect the way other medicines work, and other medicines may affect how FRUZAQLA works.
Especially tell your healthcare provider if you take blood thinners (anticoagulants).
Know the medicines you take. Keep a list of your medicines to show to your healthcare provider and pharmacist when you get a new medicine.
Take FRUZAQLA exactly as your healthcare provider tells you. Do not change your dose or stop taking FRUZAQLA unless your healthcare provider tells you to.
If you miss a dose of FRUZAQLA, you can take the missed dose within 12 hours on the same day. If more than 12 hours have passed, take your regularly scheduled dose the next day at the usual time. Do not take 2 doses at the same time to make up for the missed dose.
Do not take another dose if you vomit after taking FRUZAQLA. Take your regularly scheduled dose the next day at the usual time.
The risk information provided here is not comprehensive. To learn more, talk about FRUZAQLA with your healthcare provider or pharmacist. The FDA-approved full Prescribing Information including patient information can be found at www.fruzaqla.com or call 1-844-217-6468.
US-FRZ-0300 11/24
It’s here!
Ask your doctor about Shield, the more pleasant way to screen.
Shield is Medicare covered.
Visit www.shieldcancerscreen.com to learn more
Important Product Information
Intended Use
The Shield™ test is a qualitative, in vitro diagnostic test intended to detect colorectal cancer derived alterations in cell-free DNA from blood collected in the Guardant Shield Blood Collection Kit.
Shield is indicated for colorectal cancer screening in individuals at average risk for the disease, age 45 years or older. Patients with a positive result should be followed by colonoscopy. Shield is not a replacement for diagnostic colonoscopy or for surveillance colonoscopy in high-risk individuals. This test is performed at Guardant Health, Inc.
Precaution: Based on data from clinical studies, Shield has limited detection (55%-65%) of Stage I colorectal cancer and does not detect 87% of precancerous lesions. One out of 10 patients with a negative Shield result may have a precancer that would have been detected by a screening colonoscopy. Shield demonstrated high detection of Stage II, III, and IV colorectal cancer.
Limitations and Other Important Information: The Shield test is not indicated for patients that have personal history of colorectal cancer, adenomas, or other related cancers; or those who had a positive result on another colorectal cancer screening method within the last six months, have been diagnosed with a condition associated with high risk for colorectal cancer such as Inflammatory Bowel Disease (IBD), chronic ulcerative colitis (CUC), Crohnʼs disease; or who have a family history of colorectal cancer, or certain hereditary syndromes. Providers should discuss the most appropriate screening test to use with patients depending on their medical history and individual circumstances. Shield may produce a false negative or false positive result. A false negative result may occur when the Shield test does not detect a colorectal tumor signal while a colonoscopy identifies a colorectal cancer. A negative result does not guarantee the absence of colorectal cancer or advanced adenoma, and patients should continue participating in colorectal cancer screening programs at the appropriate guidelinerecommended intervals. A false positive result may occur when the Shield test generates a positive result while a colonoscopy will not find colorectal cancer or advanced adenoma. Please visit ShieldCancerScreen.com for complete product information about the Shield test including full safety information.