“Women with breast cancer deserve the choice to make more informed decisions on their treatment and their outcomes.”
Dan Forche, President and CEO, PreludeDx Page 05
“For breast surgery decision-making, shared decision-making is critical.”
Judy C. Boughey, M.D., President, American Society of Breast Surgeons Page 18 In partnership with:
The actress talks about her battle with breast cancer
Read more on Page 14
OLIVIA MUNN
Saving Lives Takes More Than a Month
By the time you’re done reading this, another woman in the United States will be diagnosed with breast cancer. It happens every 2 minutes.
While advancements in breast cancer care have resulted in a 43% decrease in breast cancer death rates in the last three decades, diagnoses are on the rise — especially in younger women. Despite patients having a greater variety of treatment options than ever before, still, every 12 minutes, a woman dies from the disease in the United States.
One-third of breast cancer deaths in the United States could be prevented if everyone had the same access to high-quality care and modern treatments. Factors that may seem so simple to some — like transportation, childcare, food, housing, and navigating our complex health system — often stand in the way of more than 14,000 lives saved each year.
These barriers are just one example of why breast cancer education is so important outside the pink walls of October.
Achieving health equity
Advocates and healthcare professionals alike must identify the barriers in our patient care
system to ensure everyone benefits from advancements — not just those with good health insurance and access to academic medical centers.
For example, patient navigators have been game-changers for the breast cancer community. These professionals provide patients with education and access to resources that address social determinants of health. They empower patients to make more informed decisions.
Of course, it’s also so important that the navigation workforce continues to train more culturally responsive navigators as the demand for the profession grows to meet patient needs, especially as Black women in the United States are still 40% more likely to die of breast cancer than white women. Hispanic and Latina women are also more likely to be diagnosed with breast cancer at a later stage than white women.
Innovative medicine shouldn’t be a privilege
As one of today’s greatest advances, precision medicine is a privilege — but we need it to be the
standard. While it’s exciting to see innovations in breast cancer technology and research unfold, the most rewarding outcome is witnessing how they save lives. We must focus on the person first, not just their breast cancer. Previous medical histories and social determinants of health are crucial factors in a person’s breast cancer experience.
Similarly, with the increasing use of artificial intelligence (AI), we must also ensure the utilization of AI doesn’t inadvertently deepen disparities or create additional barriers to high-quality care due to increased costs, limited availability, lack of regulation and standardization, or a design that doesn’t help all people.
The old proverb still rings true: with great power comes great responsibility.
Power and responsibility
Despite all the advances in technology and research, early detection is still key for increased survival rates, which means the yearly mammogram remains the gold standard. What’s important for women of all ages, even
far before 40, is to know your normal. Depending on your family history and unique health background, you may benefit from mammograms earlier. Much like we saw Olivia Munn bravely do last year, knowing your risk and advocating for yourself can truly save your life.
We now have both the power and responsibility to help create a world without breast cancer, and it’s a mission that we at Susan G. Komen take to heart every day — but we can’t do it alone.
While October raises awareness about breast cancer, we must honor and address the unique experiences of women every day with purpose and determination. Only then can we truly end this disease.
Publisher Shannon Ruggiero Managing Director Gretchen Pancak Production Manager
WRITTEN BY Paula Schneider President & CEO, Susan G. Komen Foundation
A Personalized Treatment Tool
Available to Patients With Stage I-IIIA HR+ HER2- Breast Cancer
If you’ve been diagnosed with invasive breast cancer, determining your treatment plan might be the most important decision you make.
The Oncotype DX Breast Recurrence Score® test, which has been used by over 1.5 million patients, indicates the likelihood of your cancer recurring based on the biology of your tumor.1,2,3,4 It is also the only test that can predict whether you will benefit from chemotherapy.5,6
This test is for patients who have recently been diagnosed with node-negative or node-positive HR+ and HER2- invasive breast cancer.
The Oncotype DX Breast Recurrence Score® test uses tissue from your most recent biopsy or surgical excision (lumpectomy or mastectomy). The sample is then sent to a lab, where it’s analyzed to gather details on its potential behavior. This genomic test analyzes your tumor tissue for 16 cancer-related genes plus 5 reference genes to assess how your tumor might respond to treatment. This information is different from the typical insights gleaned from a genetic test, which aims to determine a person’s inherited cancer risk.
Ultimately, the test results help inform whether adding chemotherapy to your hormone therapy may help to reduce your risk of recurrence.
Insights gained
When the test is complete, your doctor will receive the results, and then they will review them with you at an upcoming appointment. The test will provide the following insights:
• The Recurrence Score® result, which will be provided as a number between 0 and 100. A low number means a lower risk that the cancer may return. For these women, it’s less likely that chemotherapy will be beneficial. However, a low score isn’t a guarantee that breast cancer won’t recur. On the other hand, a high Recurrence Score result suggests a higher risk that the cancer will come back — and a potential greater benefit from chemotherapy.
• Group Average Absolute Chemotherapy (CT) Benefit, a percentage that indicates the likelihood that chemotherapy will lower the chances of breast cancer recurring when paired with hormonal therapy. This number is based on data from other patients with similar recurrence scores to yours.2,3,4,5,6
More than 17,000 patients have been studied for the link between the Recurrence Score result and chemotherapy benefit.1,2,7,8 This includes patients:
• With node-negative early-stage breast cancer
• With node-positive early-stage breast cancer
• With varying racial and ethnic minority backgrounds9
Most commercial insurance plans and Medicare cover the Oncotype DX Breast Recurrence Score® test, and patients with Medicaid also have the test at their disposal. Talk to your doctor to see if the Oncotype DX Breast Recurrence Score test could enable better informed care for your invasive breast cancer.
Written By Melinda Carter
REFERENCES
Paik et al. N Engl J Med. 2004;351:2817-2826.
2 Dowsett et al. J Clin Oncol. 2010;28:1829-1834.
3 Kalinsky et al. N Engl J Med. 2021;385:2336-2347.
4 Sparano et al. N Engl J Med. 2018;379:111-121.
5 Albain et al. Lancet Ocol. 2010;11(1):55-65.
6 Paik et al. J Clin Oncol. 2006;24(23):3726-3734.
7 Kalinsky et al. N Engl J Med. 2021;385(25):2336-2347.
8 Sparano et al. N Engl J Med. 2018;379(2):111-121.
• Distant Recurrence Risk, which is a percentage that suggests the risk of breast cancer showing up in another part of the body if you are treated with endocrine therapy alone.
9 Abdou et al. Race and Clinical Outcomes in the RxPONDER Trial: A Clinical Trial Rx for Positive Node, Endocrine Responsive Breast Cancer (SWOG S1007). San Antonio Breast Cancer Symposium. December 2022.
The information provided is not clinical, diagnostic, or treatment advice. You should consult with a qualified healthcare provider about any questions you may have regarding a medical condition or treatment. Never disregard professional medical advice or delay in seeking it because of something you have read in this article.
For more information on Oncotype Dx Breast Recurrence Score Test, scan the QR code:
Demystifying DCIS: Treatment Choices and Patient Empowerment
DCIS, an early and preinvasive stage of breast cancer, often raises challenging questions regarding its diagnosis, treatment, and patient understanding.
Assistant Professor, Department of Breast Radiation Oncology, MD Anderson Cancer Center
What is ductal carcinoma in situ (DCIS), and how does it differ from other types of breast cancer in terms of diagnosis and treatment?
DCIS is a precancer. DCIS in and of itself has never killed a single woman in the United States. DCIS is a screening disease that typically presents as little calcifications that are trapped in the ducts of the breast. It is truly the earliest stage that we can put a stage on for breast cancer — Stage 0. “Pre-invasive breast cancer” is a contradiction that is confusing to a lot of people. In reality, we actually treat it very similarly to invasive breast cancer and potentially actually overtreat a lot of DCIS.
What are the key factors that doctors will consider when determining the course of
treatment for a patient with DCIS?
A lot of things factor into it, including the size and the grade of the DCIS that was found in the body. We typically do a biopsy first to give us an idea. “Is this high-risk or low-risk DCIS?” “Is it a large size?”
Usually, the first step is a surgical excision, so a lumpectomy or mastectomy. Mastectomies are typically only reserved for when you know there’s an extensive amount of DCIS to the point where we can’t preserve a natural-appearing breast.
People who are younger and healthier may have a preference to be more aggressive. I think that may be one of the flaws of our current paradigm, which is very patient-empowered decision-making. Sometimes we’re not necessarily giving patients the right information so they can make the best decisions for themselves — for example, what mastectomies can look like for patients, what their outcomes
may be, and what the complication rates may be. There is, unfortunately, this alarming trend of younger patients choosing bilateral mastectomies for something like DCIS, which, again, has never killed a single person in the United States.
Sometimes we’re not necessarily giving patients the right information so they can make the best decisions for themselves.
Are there any advancements that are helping clinicians figure out the appropriate way to treat this?
There are a lot of different tools now available, and many techniques have greatly improved.
Get informed to make the right post-surgical treatment plan for you. Ask your doctor:
“What is the risk my DCIS will come back? And what personalized treatment plan is right for me and my DCIS?” ?
There is also a clinical trial to see if we can just watch DCIS through active monitoring, which would be a huge shift in terms of how we consider DCIS.
How can patients with DCIS be more involved in their treatment decisions and feel more empowered during the process?
It’s perfectly fine and reasonable to seek a second opinion if you don’t feel comfortable with the options that are presented to you. One of the benefits of having a pre-invasive disease is that you have a little bit of time to seek a second opinion, especially if you’re going to make a large decision like a big surgery. I think feeling empowered is really making sure you can sit with the decision that you’ve made. Everything has risks and benefits, so make sure you know what all the options are. I also think it’s helpful to talk to other people who’ve been through the same process. There are people who regretted choosing more aggressive treatments because they experienced complications, but then you also have people who are so happy with their decisions.
Empowering Physicians and Patients with DCISionRT® Precision Diagnostic Testing for Ductal Carcinoma in Situ
Each year, more than 56,500 women are diagnosed with ductal carcinoma in situ (DCIS), a non-invasive type of breast cancer commonly referred to as Stage 0 breast cancer.
Awoman with DCIS is typically treated with breast conserving surgery, or lumpectomy, where the surgeon removes the tumor while leaving the majority of the breast intact. Radiation therapy (RT) is used in most patients to reduce the chance that DCIS will recur or progress to invasive cancer.
The challenge here is that not every woman with DCIS will benefit from radiation. While more than 70% of women get radiation treatment for DCIS today, randomized studies have shown that only about 15% will actually benefit from the therapy. Until now, there hasn’t been a test or combined clinical factors that could truly assess a woman’s benefit of radiation. And what woman would want to go through the time, energy and potential side effects of radiation treatment if she didn’t really need it?
Enabling better-informed treatment decisions
PreludeDx™ is changing the way physicians and patients approach DCIS treatment decisions with DCISionRT®, the only test on the market that predicts a woman’s benefit of radiation therapy in DCIS breast cancer.
Results from the 7-gene DCISionRT biosignature test are categorized as low, elevated, or residual risk, and provide a clear, easy-to-interpret risk assessment, facilitating shared decision-making between patients and their physician care teams.
“Breast surgeons and radiation oncologists are using DCISionRT results to guide treatment decisions,” said Dan Forche, president and CEO of PreludeDx. “They trust our company because we provide them with critical information they need to optimize treatment, and personalize the results according to each patient’s unique tumor biology.”
“DCISionRT is great news for patients,” said Dr. Chirag Shah, co-director of the Comprehensive Breast Program at Cleveland Clinic and director of breast radiation oncology. “In the era of personalized medicine, DCISionRT gives me the opportunity to talk to patients about what their disease is saying, and how to best tailor their treatment, based upon their individual risk and personal preferences.”
Empowering patients
This information is truly empowering for our patients. Earlier this year, Hannah Storm, award-winning sports journalist, shared the story about her breast DCIS and how DCISionRT impacted her care.
“The DCISionRT test was the bedrock of my treatment plan,” she said. “The low-risk result indicated that radiation would likely not benefit me based on my tumor biology, and that my lumpectomy alone would be enough. This gave me tremendous confidence. I was able to put my breast cancer recurrence fears behind me, knowing that taking medication for a few years, alongside regular checkups and testing, was my path forward toward continued good health.”
DCISionRT is, indeed, a gamechanger. PreludeDx reports that over 32,000 patients have had the test to date. The test has been ordered by over 2,200 breast cancer physicians and by top academics in over 80% of major U.S. cancer centers nationwide.
“Now we just need to ensure that every patient has access to this critical test,” Forche said. “Women with breast cancer deserve the choice to make more informed decisions on their treatment and their outcomes.”
Just ask LeeAnne L., a DCIS patient whose treatment plan was transformed because of DCISionRT. “I was able to get my test results back a week before my scheduled mastectomy,” she said. “My score came back at the lowest possible risk and showed no personal benefit from radiation. I was so relieved, I was able to have breast conserving surgery and avoid both mastectomy AND radiation. I can’t imagine where I would be right now if I hadn’t had this test.”
If you’ve been diagnosed with DCIS, ask your doctor about DCISionRT and how its personalized results can help you make a better treatment decision. Visit us at preludedx. com or call 888.211.DCIS (3247) for more information.
Written by Jessica Levco, Healthcare Journalist, on behalf
of PreludeDx
INTERVIEW WITH Dan Forche President and CEO, PreludeDx
INTERVIEW WITH Dr. Chirag Shah Co-Director Comprehensive Breast Program, Cleveland Clinic
Award-winning sports journalist Hannah Storm was able to make an informed treatment plan for her breast DCIS after receiving a low-risk result from the DCISionRT test. | Photo courtesy of Hannah Storm
Age 25
Have a breast cancer risk assessment with your healthcare provider.
Breast Cancer Screening Guidelines at Every Age
Early screening and detection are key to reducing mortality rates for women with breast cancer. This is when you should begin screening.
In the United States, breast cancer remains the most common cancer in women and the second most common cause of cancer death in women. According to the National Breast Cancer Institute, approximately 310,720 new breast cancer cases were diagnosed, and 42,250 people died from breast cancer in 2024.
Early detection with screening mammograms remains the most widely studied and definitively proven method to decrease the risk of dying from breast cancer. Yearly screening mammograms reduce the risk by up to 40%. Plus, when breast cancers are diagnosed early by screening, they are less likely to require aggressive surgeries and chemotherapy than when breast cancers are detected clinically (i.e., by feeling a breast lump or other symptoms).
Perhaps just as important is that women should undergo a cancer risk assessment. This assessment determines whether someone has a higher-than-average risk of developing breast cancer in their lifetime. Individuals with an elevated breast cancer risk may benefit from more intensive screening options and/or strategies to decrease their risk.
Written by the Society of Breast Imaging
This recommendation is especially important for African American and Ashkenazi Jewish women since they are at higher risk of developing breast cancer at a younger age than non-Jewish white women.
Following a risk assessment, some women may have a higher-than-average risk of developing breast cancer, especially if they inherited a genetic mutation or underwent cancer treatment involving radiation therapy to the chest at a young age. These higher-risk women should have a yearly breast MRI screening starting at age 25-30. A breast MRI has a higher chance of finding breast cancer earlier than mammograms in this population. Start yearly mammogram screenings at age 30 in addition to breast MRIs.
See your healthcare provider if you have any new or unexplained breast problems that do not resolve on their own. Your healthcare provider may order a breast ultrasound to evaluate the problem. A diagnostic mammogram, breast MRI, or biopsy may also be indicated, depending on your symptoms.
Age 40
Have a breast cancer risk assessment with your healthcare provider, if not done already.
All women should start undergoing screening mammography once a year. Women who are at higher-than-average risk should continue yearly mammograms. Yearly mammograms find cancers earlier and reduce the risk of dying from breast cancer compared to mammograms performed every other year. For women at higher-than-average risk of developing breast cancer, continue to undergo a yearly breast MRI screening in addition to yearly mammograms.
Age 70 and over
Have a breast cancer risk assessment with your healthcare provider, if not done already.
All women should have screening mammograms once a year and continue for as long as they are in good health. Screening mammograms continue to reduce the risk of dying from breast cancer in the elderly population, and decrease the need for aggressive surgeries and chemotherapy.
All women should have a cancer risk assessment at age 25. If found to be at a higher-than-average risk for breast cancer, these women may start intensive breast cancer screening. At age 40, average-risk women should start yearly screening mammograms and continue for as long as they are in good health. This screening strategy provides the most life-saving benefit for breast cancer early detection. Also, new breast symptoms should be brought to the attention of a healthcare provider as soon as possible for evaluation.
Emerging Imaging Technology Could Reduce Negative Exams and Biopsies for Patients
Nearly half of patients screened for breast cancer need two follow-up diagnostic exams. About 20% have three follow-up appointments, and about 10% have four. Meanwhile, 1 in 10 women who undergo these exams receive a biopsy, an often uncomfortable and stressful procedure that involves removing a small piece of breast tissue for testing.
The thing is, 75% of those women who go on to get that biopsy end up having a benign mass. This begs the question: What if there was a way to avoid that hassle and detect breast cancer in a faster and possibly more cost-effective way?
There is — and interest and adoption of this procedure has been growing in recent years.
Opto-acoustic imaging — sometimes abbreviated as OA — is a diagnostic procedure that has been proven to reduce the number of false positives from a worrisome screening mammogram or palpable mass, as well as unneeded biopsies by about 75%, according to multiple studies.1,2 Other research suggests it could save patients money as well.3
“Opto-acoustic breast ultrasound gives us the opportunity to make a much better decision about marginal lesions than we could ever get before,” said Michael Linver, M.D., a breast imaging specialist, clinical professor of radiology at the University of New Mexico School of Medicine, and adjunct professor of radiology at George Washington University School of Medicine.
“Up to now, regardless of imaging modality, many lesions imaged diagnostically were placed in the BI-RADS 3 (probably benign) category,” Dr. Linver added. “Often this was because the radiologists thought the lesions were benign but weren’t sure, so they made patients come back in six months to check again.”
About opto-acoustic imaging
OA takes place after manual inspection of a noncalcified mass in the breast or a suspicious mammogram. Its technology combines conventional grayscale sonograms, which illustrate the location, size, and shape of a lesion, and bright laser-light images, which show functional information about the blood supply and structure at the cellular level in and around the lesion.
Ultimately, results from OA/US answer that key question for patients: “Do I need a biopsy to determine if I have breast cancer?”
“In my opinion,” Dr. Linver said, “avoiding those unnecessary callbacks (for diagnostic tests and biopsies) is really the greatest gift optoacoustic imaging offers to those who use it.”
Although OA was introduced in the 2000s, Dr. Linver said its technology has “matured dramatically” in the past five years.
Real-life results
A manufacturer of OA imaging, Seno Medical, offers an OA imaging product called Imagio® that the U.S. Food and Drug Administration approved as the first opto-acoustic system for U.S. markets in 2021. It comes with an artificial intelligence tool called SenoGram® that helps radiologists interpret the results.
“This is game-changing for breast cancer imaging in that we get functional information — that we would normally get from advanced imaging — but with ultrasound,” said Basak Dogan, M.D., University Texas Southwestern’s
director of Breast Imaging Research.
That functional information is empowering physicians to better understand their patients’ tumors and make better-informed decisions about their care.
“OA imaging allows us to have a physiologic window on those lesions so that we might be able to downgrade those lesions,” explained Steven E. Harms, M.D., professor of radiology at the University of Arkansas for Medical Sciences. “In other words rather than resort to biopsy we can resort to follow up with imaging or maybe even classify to benign all together and go back to standard screening.”
Research backs up that sentiment, finding that OA imaging improves the quality of life in patients and lowers healthcare costs.3
B. Bersu Ozcan, M.D., lead author of the research, summed up the system simply: “Opto-acoustic imaging is fast, simple, and can dramatically improve diagnostics.”
Written by Melinda Carter
REFERENCES
1 Ghannam S, et al. Exploring the Utility of Optoacoustic Imaging in Differentiation of Benign and Malignant Breast Masses: Gen2 Study. Academic Radiology, 2024 October.
2 CONFIDENCE Registry Study (Netherlands). ClinicalTrials. Go NCT05084729.
3 Ozcan, BB, et al. Supplemental optoacoustic imaging of breastmasses: a costeffectiveness analysis. Acad Radiol 31(1):121–130.1.
Photo courtesy of Seno Medical
How Do I Know If I Am “High Risk?”
Most patients who develop breast cancer do not have any risk factors other than being a woman and getting older.
Some women are at high risk because of a known disease-causing mutation, most commonly in BRCA1 or BRCA2. Such mutations are more common in women of Ashkenazi Jewish descent and Black women. Prior radiation therapy to the chest before age 30, and at least eight years earlier, also creates a high risk for breast cancer, as does a personal history of breast cancer. Women at high risk are recommended to have annual screening with MRI and to add mammography after age 30.
Combinations of other risk factors may also put a woman at high risk. Factors to be considered include:
• Family history of breast cancer, especially if diagnosis was before age 50 or in multiple relatives on the same side of the family
• Prior breast biopsies, especially atypical biopsies
• High body mass index (BMI over 25) after menopause
• Combination estrogen and progesterone hormone supplements
• Dense breasts (heterogeneously dense or extremely dense) on a mammogram report.
Formal risk assessment should be done by age 25 and then every few years if new family history or other risks develop. A lifetime risk of 20% or more is considered “high risk.” Over 20% of women in their 40s are at high risk, but fewer than 1% of women in their 70s are at high risk, and screening MRI is not usually recommended beyond age 70.
WRITTEN BY Wendie Berg, M.D., Ph.D. FACR, Chief Scientific Advisor, DenseBreast-info.org; Professor of Radiology, University of Pittsburgh School of Medicine
Everything You Need to Know About Dense Breasts
You may be hearing a lot about “dense breasts” right now. That’s because on Sept. 10, an FDA requirement went into effect, which states that, after a mammogram, patients must be informed whether or not they have dense breasts.
Patients will also be informed that dense tissue makes it harder to find breast cancer on a mammogram, raises their risk of developing breast cancer, and that other imaging tests after a mammogram can help find cancers. Get educated.
Facts to know:
• Dense breast tissue is normal and common. 40% of women aged 40 and over have dense breasts.
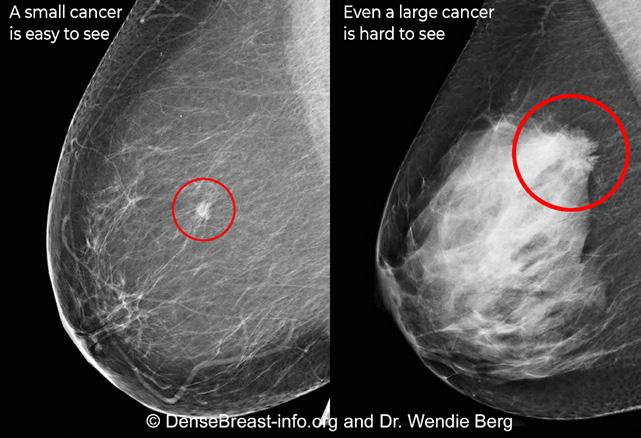
• Dense breast tissue increases risk. Cancer is four to six times more likely to develop in women with extremely dense breasts than in women with the least dense breasts.
• Dense breast tissue hides cancers. Though mammograms find some cancers not seen on other screening tests, in extremely dense breasts, mammograms will miss about 40% of cancers.
• In dense breasts, after a mammogram, other screening tests, such as ultrasound or especially breast MRI, substantially increase detection of early-stage breast cancers.
Can I tell if I have dense breasts by the way my breasts look or feel?
No. Breast density refers to the tissue composition of your breasts and is determined by the doctor that reviews your mammogram.
How do I know if I have dense breasts?
When you have your mammogram, your breast density is rated as one of four categories:
Early detection matters. Be an informed self-advocate and ask the question: “Is my mammogram enough?” Visit DenseBreast-info.org to learn more.
• Fatty
• Scattered areas of fibroglandular density
• Heterogeneously dense
• Extremely dense
Breasts that are heterogeneously or extremely dense are considered “dense” breasts.
How does dense tissue affect my mammogram?
Dense breast tissue is white on a mammogram and fatty tissue appears dark gray (see image). Unfortunately, cancers also display as white on a mammogram. If there is a lot of dense tissue on a mammogram, a cancer can be “hidden” among the dense tissue. This is true even if the mammogram is done with 3D/tomosynthesis.
For women with dense breasts, a “normal,” “negative,” or “benign” mammogram does not necessarily mean cancer is not present. No matter how recent your last mammogram, a lump or any changes in your breast should be brought to the attention of your health provider.
What about insurance coverage for additional testing?
Generally, if your health provider feels additional testing is medically necessary, it will be covered, though copay and deductibles may apply. Currently, 34 states have passed insurance laws to cover some level of additional testing after a mammogram. However, state laws vary and coverage is not assured. To address state-by-state law variations, a federal insurance bill, the Find It Early Act, was introduced by Reps. DeLauro (D) and Fitzpatrick (R), and Sens. Klobuchar (D) and Marshall (R). The bill would help address insurance barriers to testing needed to find cancer at the earliest stage possible. Learn more at FindItEarlyAct.org.
WRITTEN BY JoAnn Pushkin Executive Director, DenseBreast-info.org
Do You Have Dense Breasts? Here’s What You Need to Know
Have you recently received a letter from your doctor’s office about your breast density? You might be wondering what it’s all about.
Thanks to a new requirement from the U.S. Food and Drug Administration (FDA), doctors must inform patients about their breast density after their annual mammogram.1 If this letter has raised some questions for you, here is some information that might help.
What does it mean to have dense breasts?
Having dense breasts increases a person’s risk of developing breast cancer, and it can also make it more challenging for radiologists to detect cancer on a traditional mammogram.2 This is because dense breast tissue appears white on a mammogram — the same color as cancer — making it difficult to identify.
Nearly 50% of women have dense breasts, making it a common breast cancer risk factor.3,4 If this information is new to you, you’re not alone. A recent study found most women were unaware that breast density increases their breast cancer risk more than family history or being overweight.5
For dense breasts, think 3D Not only is mammography the most effective tool we have to detect breast cancer early, but it’s also used by radiologists to determine if your breasts are dense.6 When you book your annual mammogram, keep in mind that not all mammograms are created equally. Be sure to ask for the Hologic 3D™ Mammogram
that’s FDA-approved as superior for women with dense breasts compared to traditional 2D mammography.7,8*
Part of the 3Dimensions™ Mammography System, the Hologic 3D™ Mammogram is more accurate than traditional 2D mammograms for women with a variety of breast densities, detecting 20%-65% more invasive breast cancers.8* That means earlier detection for many women.7-12*
Not your mom’s mammogram
Fear of pain or discomfort is one of the primary reasons women skip or delay a recommended screening.13 Thankfully, today’s mammograms are different.
The Hologic 3D™ Mammogram is clinically proven to be more comfortable thanks to its innovative SmartCurve® system, a curved compression paddle that is designed to respond to the shape of your breasts.14** Plus, scans can last as little as 3.7 seconds on the 3Dimensions™ Mammography System.15 That’s quicker than any other exam.
I have dense breasts. What’s next?
Your doctor may recommend supplemental imaging to complement your annual mammogram. These additional breast exams may include diagnostic ultrasound, breast magnetic resonance imaging (MRI), or contrast-enhanced mammography (CEM).
CEM is a type of mammogram
that uses a special dye and X-rays to create detailed images of breast tissue. It has been available for nearly a decade but is now receiving increased attention due to growing evidence supporting its advantages.
While CEM and breast MRI are both powerful tools for detecting breast cancer, MRI can be inaccessible to many women, particularly those residing in rural areas or who suffer from claustrophobia.16,17 CEM is a comparatively more accessible, comfortable, faster, and less expensive option, making it a promising alternative for enhancing breast cancer detection.18-20
Take action for your health Knowledge is power. By
understanding your breast density, you can make informed decisions about your health. Take action today by scheduling your annual exam and asking for a 3D™ Mammogram.
Written by Hologic
*Compared to 2D mammography alone. ** Compared to mammography systems without the SmartCurve® system.
To learn more, visit hologic.com/ BustTheMyth Scan the QR code to access a complete list of corresponding references.
Photo courtesy of Hologic
Early Breast Cancer and the Risk of Recurrence
Breast cancer is the most common cancer among women, and although the majority are diagnosed with early-stage disease, some will experience a recurrence.
The term “early breast cancer” can include a variety of presentations at diagnosis, although it is often referring primarily to patients with with Stage 1 or Stage 2 breast cancer, based on the American Joint Committee on Cancer (AJCC) staging guidelines, which were last published in 2016 and updates are underway.1
While breast cancer staging was previously based solely on tumor size, axillary nodal status, and distant metastasis (also referred to as “TNM staging” or “anatomic staging”), it now includes additional prognostic markers, such as the hormone receptors (estrogen and progesterone receptors, ER/PR), human-epidermal-growth-factor-receptor-2 (HER2), histologic tumor grade, and genomic profiles. Thus, the latest stage groups are collectively termed “prognostic stages.”
Given the changes in systemic therapies over the years, the latest AJCC staging guidelines
reflect contemporary treatment strategies for patients with breast cancer, which are increasingly guided by tumor biology, in addition to the extent of the disease. Furthermore, these updates in staging further refined prognostic estimates for the assigned stage groups, and a recent study noted that more than 35% of patients had a change in their stage based on these guidelines.2
In a large validation study of 50,000 patients in the California Cancer Registry, the 5-year disease-specific survival was noted to be 97-99% for patients with Stage 1 disease and 93-94% for those with Stage 2 breast cancer, thus demonstrating excellent outcomes for the vast majority of patients with early-stage breast cancer.3
Determining the risk of recurrence Importantly, there are several prognostic assays based on gene expression that are
currently being used in clinical practice to help determine the risk of recurrence and potential benefit of adjuvant systemic therapy (such as chemotherapy), although only one of them is included in the AJCC staging guidelines. The National Comprehensive Cancer Network (NCCN) highlights five specific assays (Breast Cancer Index, EndoPredict, Mammaprint, Oncotype Dx, and Prosigna) that provide prognostic information and are based on high-level evidence and/or uniform NCCN consensus (≥85% support of the NCCN panel).4
These assays are most commonly performed on tissue removed during surgery but may also be performed on needle biopsy specimens. These test results help doctors and patients develop personalized treatment strategies based on the identified level of recurrence risk.
However, given the low risk of mortality with early-stage breast cancer, the latest guidelines from the NCCN recommend a history and physical exam every 3-12 months for the first five years after a breast cancer diagnosis, then annually thereafter. If a patient has breast-conserving surgery, annual mammography is recommended to assess for local-regional recurrences, although no routine breast imaging is indicated following mastectomy.
Given the low risk of distant metastasis and lack of improved outcomes with regular systemic screening, routine laboratory or imaging studies for distant metastases screening are not currently recommended in the absence of clinical signs and/or symptoms of recurrence.4
REFERENCES
1. AJCC Cancer Staging Manual (ed 8th). New York, NY, Springer International Publishing, 2016.
2. Plichta JK, Ren Y, Thomas SM, et al. Implications for Breast Cancer Restaging Based on the 8th Edition AJCC Staging Manual. Ann Surg, 2018.
3. Weiss A, Chavez-MacGregor M, Lichtensztajn DY, et al. Validation Study of the American Joint Committee on Cancer Eighth Edition Prognostic Stage Compared With the Anatomic Stage in Breast Cancer. JAMA Oncol 4:203-209, 2018.
4. Gradishar WJ, Moran MS, Abraham J, et al. Breast Cancer, Version 1.2024, NCCN Clinical Practice Guidelines in Oncology. Online, National Comprehensive Cancer Network, 2024
WRITTEN BY
Jennifer K. Plichta, M.D., M.S., FACS, CGRA President, National Consortium of Breast Centers
WRITTEN BY
Kristie A. Bobolis, M.D.,BHCN, CGRA President, National Consortium of Breast Centers Certification Board
Could Breast Cancer Come Back After an Early Diagnosis? What
You Need to Know
You may have rung the proverbial bell that announces the end of chemo or completed rounds of radiotherapy. You’re now declared “cancer free.” It’s normal to feel mixed emotions and have questions.
For many people with early breast cancer (eBC), remission doesn’t mean everything goes back to normal. There are scars from several surgeries, side effects from initial treatments, and the question: “What if it comes back?” This concern is valid, as 1 out of 3 people diagnosed stage 2 or 3 HR+, HER2- eBC will see their cancer come back within 20 years.
These statistics may seem daunting, but don’t be discouraged. Breast cancer is one of the most studied cancers, with research-backed strategies to help reduce recurrence risk. The more we know, the more we can do to help beat the odds.
The emotional impact of a breast cancer diagnosis can be profound. Kristin Juszczyk, NFL- wife turned fashion designer, shares her personal experience with the disease: “As a daughter of someone who experienced the devastating impact of breast cancer and witnessed recurrence first-hand, I feel inspired to help spread the word,” Juszczyk reflected. “I was so young when my mom was diagnosed with breast cancer. What’s missing from the conversation is knowing that for many people, cancer does come back, as was the case for my mom. So, I’m passionate about educating others and encouraging everyone to have these tough conversations.”
Understanding the risk of cancer coming back
The odds of cancer returning, known as risk of recurrence, depends on several factors, including tumor type, stage, and size; lymph node involvement; gene activity; age at diagnosis; and lifestyle.
While there are many factors at play, certain tests can help your care team understand your risk by scoring it.
“Understanding your diagnosis and working closely with your healthcare team is essential for managing the risk of cancer returning and keeping up with medical advances,” said Jean Sachs, CEO at Living Beyond Breast Cancer. “Having a strong relationship with your healthcare providers and sharing decision-making will help ensure treatment changes are tailored to your individual needs.”
Taking control
Knowing the factors that increase the risk of recurrence and taking action can not only help you beat the odds of recurrence, but also give you a sense of empowerment. Healthy lifestyle choices like regular physical activity, a balanced diet, and reducing alcohol and tobacco use are key.
Breast cancer can return to the breast or chest wall, but it often comes back as metastatic disease, meaning it has spread to other parts of the body like the bones, liver, or brain. This is why even if you’re “done” with active treatment, it’s crucial to have a long-term plan, which includes discussing adjuvant or maintenance therapy (treatments to help lower the risk of recurrence), and lifestyle changes with your doctor.
Adjuvant
therapy and its role in a holistic treatment
plan
In addition to adopting and maintaining healthy habits, adjuvant therapy can be crucial for patients with stage 2 or 3 HR+, HER2- eBC. This
type of therapy, which usually involves endocrine or hormonal treatment, can help reduce the risk of cancer coming back. However, some patients might need more than just standard adjuvant therapy to manage their risk.
It’s important to work with your healthcare team before and after treatment to create a personalized plan tailored to your risk levels and treatment goals.
Let’s help beat the odds, together
Breast cancer care is constantly evolving with new research and treatments leading to better outcomes. Staying on top of routine screenings, understanding the risk of recurrence, making healthy lifestyle choices, and following a holistic treatment plan by a healthcare team are essential steps after an eBC diagnosis.
Written by Novartis
For more information, visit UnderstandEBCRisk.com and sign up for exclusive resources to help navigate survivorship with your healthcare team.
INTERVIEW WITH Kristin Juszczyk Founder, Designs by Kristin 11/24 FA-11304578
Knowledge is Power: How a Genetic Test Changed Mathew Knowles’ Life
Mathew Knowles learned he has a BRCA2 gene mutation, so he’s at a higher risk of getting certain cancers. Armed with that knowledge, he has made significant life changes and prioritized his health.
Most know Mathew Knowles as a music executive and the father of music icon Beyoncé and singer Solange. But some don’t know he’s also a breast cancer survivor.
At 67, he woke up to dots of blood on the bed sheets. After a career selling medical equipment, he knew this could be a sign of something more serious.
“I wanted to find out immediately what was going on,” Knowles said. “I wanted to have a mammogram and get to the core of what the problem was.”
He went to his doctor for a mammogram and learned he had Stage 1A breast cancer.
“I was encouraged that it was Stage 1,” Knowles said. “I wanted to take care of it and move on with my life.”
He had a mastectomy to remove one of his breasts, allowing him to be cancer-free for the last five years. But during the mastectomy, his doctors also ran a genetic test. The results showed Knowles had a BRCA2 gene mutation, which changed his life.
An altered outlook Knowles’ family has a long history of cancer. Breast cancer was prevalent on his mother’s side of the family, and prostate cancer was evident on his father’s.
But Knowles never thought about how that history could affect his own health. After the genetic test, he learned a BRCA mutation means he’s predisposed to certain cancers, including breast, prostate, and melanoma. It also means he could have been eligible for certain targeted treatments for his type of cancer.
Knowles said he wishes he had known that information before his mastectomy because he and his doctor could have made a more informed decision about his treatment path. He said he might’ve had the other breast removed, too.
Instead, he is focusing on the future by prioritizing his health. He changed his diet, lost weight, and started exercising more. Knowles is now proactively going to the doctor for regular check-ups and screenings.
“Every year, I get a mammogram,” Knowles said. “And every year, I get a prostate exam. Annually, I get a pancreatic MRI. You add all of that together [and it’s] one day out of a year.”
The genetic test also altered the way he moves about the world.
“For the first time, I started to view life differently,” Knowles said. “I never really had a deep appreciation for nature, but I’m now looking at things I never looked at before [like] sunsets, the ocean, the flowers, and things I just took for granted. I think once you go through any type of disease, you are just grateful when you hopefully make it to the other end of that.”
Making informed decisions
Knowles said he wants to empower people by getting them the knowledge they need.
For instance, many men don’t even know they can develop breast cancer. While it’s rare, 2,790 men will be diagnosed with the disease in the United States this year and 530 men will die from it, according to the American Cancer Society.
People also need to know their family history, and Knowles says the best way to do that is to get genetic testing. Knowles, who partnered with AstraZeneca on its BeBRCAware campaign, has now made it his mission to get the word out about genetic testing so everyone can make informed decisions about their health, cancer risks, and care.
“Knowledge is power, and the more information you have about your health, the more informed your decision-making can be,” Knowles said.
Written by Frank James
Matthew Knowles | Keer Orr and Veronica Hill for Point & Click Photography
Not an actual patient.
The Power of Personalized Breast Cancer Care
It’s a sobering statistic: 1 in 8 women in the United States will be diagnosed with breast cancer during her lifetime.1
Breast cancer remains both the most common cancer in women and one of the leading causes of cancer-related deaths worldwide.1,2
But amid these alarming statistics, there’s also reason for hope: Breast cancer care is undergoing a significant transformation.
Last year, AstraZeneca received FDA approval for a breast cancer therapy, offering a critical new option for eligible patients.
“By leveraging our growing understanding of breast cancer biology, we aim to transform the lives of those living with this disease,” said Mohit Manrao, SVP, head of U.S. oncology at AstraZeneca. “Genetic testing and targeted therapies are key components of this journey, offering hope and new possibilities for those affected by breast cancer.”
“Outsmarting” breast cancer
Targeted therapy focuses on specific areas or substances in cancer cells that help them to survive and grow.3,4 The problem is that cancer cells are constantly evolving; patients who initially respond to targeted therapies may eventually develop resistance, causing the treatment to stop working.5
Fortunately, as understanding of cancer biology deepens, new treatments are targeting specific genetic mutations that may offer more time and increased quality of life for patients.6
A new treatment roadmap: genetic testing and biomarker testing
BRCA1 and BRCA2 genes play a role in protecting the body against certain types of cancers.7 While everyone has these genes, some people are born
with alterations to these genes or they develop them later in life. People with BRCA alterations are more likely to develop certain cancers, such as breast, ovarian, and prostate cancers.7
Genetic testing looks for inherited gene alterations passed down through families, helping people to understand their risk of these cancers. Genetic testing can take place whether or not someone is diagnosed with cancer.7
On the other hand, biomarker testing takes place after cancer diagnosis and examines specific genes, proteins, and other substances to provide key information about a patient’s cancer.8
Results from genetic and biomarker testing can offer healthcare providers insight into which therapies will be most appropriate for a patient’s condition.8 By helping to tailor treatment to the specific makeup of a tumor, this information helps ensure that patients receive therapies targeted to their specific type of cancer.8
New guidelines for genetic testing
The benefits of genetic testing are so compelling that it’s becoming the standard of care for certain types of cancers. In fact, The American Society of Clinical Oncology (ASCO) and The Society of Surgical Oncology (SSO) now recommend that everyone under 65 diagnosed with breast cancer should be offered BRCA1 and BRCA2 genetic testing.9 This shift highlights the critical importance of understanding your genetic makeup to inform treatment decisions.
The power of becoming BRCAware “Beyond offering more personalized treatment
plans, genetic testing can also reveal inherited mutations that increase the risk of cancer, allowing for early intervention,” said Aliya Omer, vice president, U.S. franchise head, breast cancer at AstraZeneca.8 “We encourage anyone interested in learning more to visit bebrcaware.com. It offers lots of useful information on breast cancer, as well as resources, support, and education, and information on genetic counseling.
“Breast cancer can be scary, but there is power in understanding your risk and knowing your options.”
Moving closer to a cure
With over 8,000 dedicated employees working together with community and industry partners, AstraZeneca is bringing transformative medicines to breast cancer patients. “Our mission is to offer a potential cure for an increasing proportion of the millions of people worldwide living with cancer,” Manrao said. “With every advancement, we move closer to our goal of transforming cancer treatment and improving patients’ lives.”
Written by AstraZeneca
REFERENCES
1. American Cancer Society. Key Statistics for Breast Cancer. Accessed November 8, 2024. https://www.cancer.org/cancer/types/breast-cancer/about/howcommon-is-breast-cancer.html.
2. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CACancerJClin.2024; 74(3): 229-263. doi:10.3322/caac.21834.
3. American Cancer Society. Targeted Therapy. Accessed November 8, 2024. https://www.cancer.org/cancer/managing-cancer/treatment-types/targetedtherapy.html.
4. American Cancer Society. How Targeted Therapies Are Used to Treat Cancer. Accessed November 8, 2024. https://www.cancer.org/cancer/managing-cancer/ treatment-types/targeted-therapy/what-is.html.
5. National Cancer Institute. Why Do Cancer Treatments Stop Working? Overcoming Treatment Resistance. Accessed November 8, 2024. https://www. cancer.gov/about-cancer/treatment/research/drug-combo-resistance.
6. Jallah JK, Dweh TJ, Anjankar A, Palma O. A Review of the Advancements in Targeted Therapies for Breast Cancer. Cureus.2023;15(10):e47847. doi:10.7759/ cureus.47847.
7. National Cancer Institute. BRCA Gene Changes: Cancer Risk and Genetic Testing. Accessed November 8, 2024. https://www.cancer.gov/about-cancer/ causes-prevention/genetics/brca-fact-sheet.
8. National Cancer Institute. Biomarker Testing for Cancer Treatment. Accessed November 8, 2024. https://www.cancer.gov/about-cancer/treatment/types/ biomarker-testing-cancer-treatment.
9. Bedrosian I, Somerfield MR, Achatz MI, et al. Germline Testing in Patients With Breast Cancer: ASCO–Society of Surgical Oncology Guideline. JClinOncol. 2024;42(5):584-604. doi:10.1200/JCO.23.02225.
To access breast cancer resources and support, visit bebrcaware.com
Finding Strength: Clea Shearer Discusses Life After Breast Cancer
Clea Shearer, co-founder of The Home Edit, shares how communication and selfadvocacy have become tools in her fight against breast cancer.
What unexpected challenges have you encountered after treatment?
I simply don’t have the same energy that I used to have, and that can be frustrating. However, I’ve learned to give myself some grace and not allow that to be a blockade. The mental piece is also taxing because I wake up every day with the mindset of fighting to keep cancer from coming back. It can be overwhelming at times, but I feel empowered to proactively do everything I can to prevent recurrence.
What has helped you cope with the difficulties of going through breast cancer?
I am a big communicator, so simply talking to people helps me. One of the reasons I decided to document my journey publicly was to give people a forum to openly discuss with me and each other. I hoped that by creating a community, we would all feel less alone, less afraid, and more supported.
What advice would you give someone going through a similar situation?
My biggest advice is to always advocate for your health. Whether that means scheduling mammograms, speaking up about the care you’re receiving, or going to your doctor with questions and concerns. No one is going to do that hard work for you.
INTERVIEW WITH
Clea Shearer Co-Founder, The Home Edit
Olivia Munn on Dealing With Breast Cancer as a New Mom
Diagnosed with luminal B breast cancer in April 2023, TV and film actress Olivia Munn shared what it’s been like navigating the diagnosis while raising a son (Malcom, 3 years old) and daughter (Méi June, 3 months old).
Could you walk us through your story of how you were diagnosed with breast cancer, and what your healthcare experience has been like since?
In the winter of 2023 after a clear mammogram test and genetic test results showing I had 0% chance of having any genetic cancers, my OB-GYN had me take the Tyrer-Cuzick lifetime risk assessment test. After receiving a score of 37.3% (anything above 20% is high risk), she sent me to get a breast MRI. After that MRI, an ultrasound, and multiple biopsies, I was diagnosed with bilateral breast cancer. I have undergone five surgeries in the past year and a half: nipple delay, lymph node dissection, double mastectomy, reconstructive surgery, a partial hysterectomy (I had my fallopian tubes and uterus removed), and an oophorectomy.
What was the most challenging part of treatment for you?
Although the surgeries were difficult, I think the medication I have to take for five years to suppress my hormone production has been the most taxing on me. The side effects range from debilitating exhaustion to full body aches. Compounded with having a baby (and now a toddler and newborn) at home, I’ve felt defeated at times and have struggled with my mental health. But I’m working through it with my oncologist and beginning to see some positive changes.
What part of treatment did you feel the least prepared for?
I wasn’t prepared for how hard it would be emotionally. When I learned of my diagnosis, I didn’t cry or shut down — I became very focused on learning everything I could and taking on each surgery and every new detail that emerged with a clear mind. I couldn’t let
fear seep in, although it was always there just beneath the surface.
What were some unexpected challenges of having breast cancer?
Everything about having cancer is unexpected, from the moment you get the diagnosis. It’s not something you can really prepare for. The biggest challenge for me has been finding a way to put myself and my treatment first at times. It feels like never ending doctor appointments and blood tests and medication, and I just want to pretend like I don’t need it and instead hang out with my babies and husband. But I don’t have that option, so I keep pushing forward.
As a breast cancer survivor, how has your healthcare routine changed?
Stress creates cortisol, which is a stress hormone. My cancer feeds on hormones, so I have really made a concerted effort to eliminate as much stress as possible. If I find myself in a stressful situation or dynamic, I’ll ask myself if staying in it would be worth my cancer coming back. The answer is always no.
What advice do you have for young women and other moms dealing with a breast cancer diagnosis?
There’s a beautiful sisterhood of women who have gone through breast cancer, and we are all here for each other. We lift each other up when we feel down and celebrate every milestone, no matter how small.
To any moms battling breast cancer, please give yourselves a lot of grace to be tired and lie in bed. Break the “No TV” rule and let your kids climb in bed with you and watch a movie. They’ll love being so close to you and there’s truly nothing better than snuggling your babies so tightly you can feel their little breaths on you.
Olivia Munn with husband John Mulaney and daughter Méi June. Photo courtesy of Olivia Munn
SUPPORT BEYOND MEASURE, FOR A LIFE BEYOND CANCER.
COMPREHENSIVE SUPPORT FOR BREAST CANCER PATIENTS AND THEIR FAMILIES.
United Breast Cancer Foundation is a leading nonprofit dedicated to making a positive difference in the lives of those affected by breast cancer. With a proven track record of excellence, UBCF offers a range of lifesupporting programs for women, men, and families across the nation.
Your generous contribution will enable UBCF to continue its vital work of providing hope and support to breast cancer patients and their families. By investing in us, you are investing in the future of countless individuals and making a tangible difference in the fight against breast cancer.
Fund early detection
Cover treatment costs
Improve quality of life
Support children of patients
Get Better Breast Reconstruction Results by Consulting a Plastic Surgeon Early
A breast reconstruction journey comes with a plethora of options. The ultimate outcome is determined by a patient’s personalized path based on three features — their breast cancer treatment plan, body type, and aesthetic goals.
Aboard-certified plastic surgeon is your most qualified guide to navigating the options for breast reconstruction and arriving at the best result.
Importance of introducing a plastic surgeon early
A crucial step to getting the best outcome is placing a plastic surgeon on your care team shortly after a cancer diagnosis. Early collaboration with a board-certified plastic surgeon who is a member of the American Society of Plastic Surgeons (ASPS) will allow you to understand and evaluate your available options based on your specific situation. A plastic surgeon will explain what is physically achievable while supporting your mental well-being.
“This is a very stressful time,” said Ron Israeli, M.D., a plastic surgeon specializing in breast reconstruction. “A plastic surgeon can help patients navigate the decision-making and allow them to understand there is light at
the end of the tunnel because someone will help them achieve their aesthetic goals.”
Restoring sensation
Patients initially will experience numbness in their reconstructed breast(s) because nerves must be cut and removed during mastectomy.
“When nothing is done to repair the nerves, communication between the brain and the chest gets disrupted, diminishing the ability for nerves to function normally,” said Jonathan Bank, M.D., FACS, a plastic surgeon and breast microsurgery expert. “This can lead to partial or complete numbness that may be permanent.”
Yet, plastic surgeons are critical to regaining breast sensation after mastectomy because they can reconnect tiny nerves in the chest with a graft, allowing them to regenerate and heal over time.
“Through advanced breast reconstruction techniques, plastic surgeons can help restore the important function of sensation,” Dr. Bank said. “Studies show that regaining sensation
can provide a variety of benefits for patients, including improved physical safety, emotional well-being, and overall quality of life.”
Nerves regrow as the patient’s body heals. The amount of breast sensation regained may vary and can take up to two years to return. It’s important to discuss what’s possible with your plastic surgeon when deciding on your reconstructive options.
It may take several procedures
Reconstruction often involves multiple procedures performed in stages. Even patients who choose to combine reconstruction with their mastectomy should consider revisions to achieve the best outcome. Again, working with a plastic surgeon will help refine your results.
“Almost always, there’s an advantage to being open to having additional procedures to achieve the best outcome,” Dr. Israeli said. “A second procedure may be minor, such as a skin adjustment or grafting fat from elsewhere to soften the breast.”
Making reconstruction affordable
Breast cancer can come with a hefty mental, emotional, and physical cost, but the actual price of the reconstruction of your choice is likely affordable. The federal 1998 Women’s Health and Cancer Rights Act requires group health insurance plans to cover reconstructive surgery, regardless of the number of revisions.
“This is a decision to be made by the patient and their doctor, not the insurance company,” Dr. Israeli said. “Breast reconstruction can help many women achieve a sense of wholeness, making a big difference in their lives.”
Expert guidance
Breast cancer is not a journey anyone would choose, but getting a board-certified plastic surgeon who is an ASPS member on your care team early as your guide will allow you to personalize your reconstruction and improve your outcome.
Written by The American Society of Plastic Surgeons (ASPS)
Restoring Sensation, Renewing Hope: A Solution for Women After Mastectomy
Breast cancer is more than a diagnosis — it’s a journey that profoundly reshapes bodies, identities, and lives. And while the visible changes are well-known, there’s a hidden side to mastectomy that often goes unspoken: the lasting numbness that can follow.
Even after reconstruction, women can experience partial to complete chest numbness, creating a permanent barrier to feeling whole again. Nearly 80% of women report numbness, pain, or a combination of both following mastectomy.1 It’s important to understand why it happens.
Understanding the loss of sensation
Sensory nerves run throughout our bodies. They function like electrical wires, helping us to interact and experience the world around us. Nerves allow you to feel temperature, pressure, touch, and even pain — everything from a cozy blanket to the touch of a loved one — and they keep you safe by helping you feel if something is too hot or sharp and at risk of hurting you.
During mastectomy, nerves running through the breast are cut and removed with the breast tissue. Once cut, nerves can no longer send signals. No signals mean no sensation. Think of how it feels when your mouth is numbed at the dentist. Numbness in your chest may be similar.
The loss of sensation can be devasting in countless unexpected ways, especially since touch is such an important part of our everyday lives. Without intervention, this lack of feeling can be permanent, even after breast reconstruction.
A path to restoration: the solution of Resensation
Thankfully, you might not have to accept numbness as your new norm. Resensation is a surgical technique that reconnects nerves cut during a mastectomy. It can help women reclaim the sense of touch, restoring not only sensation but also the connection, comfort, and confidence that go along with it.
During breast reconstruction, a trained plastic surgeon reconnects nerves cut during a mastectomy with a nerve allograft. Over time, the nerves can regenerate and gradually restore sensation. Many patients notice the signs of sensation beginning to return within several months after surgery, with feeling continuing to improve for up to two years.2
Patients who have had Resensation often describe it as a renewal. For Jessica D., a nurse and breast cancer survivor who chose to undergo the Resensation procedure, this return of feeling became central to moving forward: “Getting back sensation made me feel whole again — like I could finally put cancer behind me. After the shock of a cancer diagnosis, patients are often overwhelmed by the decisions they need to make in a short time,” Jessica explained. “While survival is the immediate priority, long-term side effects, like loss of sensation, which get less attention, can be equally devastating.”
For women like Jessica, the journey to healing isn’t just physical; it’s about reclaiming a level of normalcy and feeling like yourself again.
Know your options
Thisinformation,including illustrations, is noncommercial, providedforeducational purposesonlyanddoesnot constitute medical advice or substituteforprofessional medical advice. The level of sensationrestoredfollowing use of the Resensation techniquemayvaryand cannotbeguaranteed,due touniqueanatomyandother considerations.Pleaseconsultyour surgeonformoredetailedinformation.
REFERENCES
1 https://pubmed.ncbi.nlm.nih.gov/34841183/
2 https://insights.ovid.com/pubmed?pmid=11994590
If you or someone you love is considering breast reconstruction after mastectomy, know that numbness doesn’t have to be the “new normal.” Options like Resensation can offer the possibility of regaining sensation, empowering women to move forward with a renewed connection to their bodies.
Written by Resensation brought to you by Axogen
Explore your options at Resensation.com to learn more about this procedure and find a trained surgeon near you.
Detect Early, Save Lives:
The Importance of Breast Cancer Screening
Removing barriers to breast cancer screening leads to the best health outcomes.
It is well-documented that early detection of breast cancer saves lives. Over 95% of women who receive an early diagnosis can see high rates of survival with treatment. However, due to a range of factors, breast cancer mortality doesn’t impact all communities in the same way. If you are at higher risk, you may need to begin screening at a younger age. Some factors that can determine your risk include a family history or carrying a genetic mutation, such as BRCA-1. If you are part of a high-risk group, we recommend getting a breast cancer risk assessment at age 25 to develop a personalized screening plan. Brem Foundation to Defeat Breast Cancer developed a patient-facing risk quiz, CheckMate, that provides participants with a personalized risk list along with conversation starters for an upcoming medical visit.
An estimated 28 million women of recommended screening age have not had a mammogram in the last year, with cost as a driving factor. This data highlights the need for programs like Brem’s Wheels for Women and B-Fund, which break down barriers to care by covering costs and providing free resources. No woman should ever have to choose between her health and her financial security.
WRITTEN BY Clare Dougherty CEO, Brem Foundation to Defeat Breast Cancer
The Importance of Shared Decision-Making in Breast Cancer Surgery and Treatment
Shared decision-making empowers both patients and providers, ensuring informed breast cancer surgery choices through open dialogue in treatment planning.
Judy C. Boughey, M.D. President, American Society of Breast Surgeons
Can you explain what shared decisionmaking means in the context of breast cancer surgery and why it’s so important for both patients and providers?
Shared decision-making is the collaborative process where the patient and their healthcare providers work together to make decisions for the patient’s care. When you think about a lot of aspects of medicine, in particular surgery, there’s often one clear best recommendation, but I think what is unique about breast surgery is that there are often many options that the patient can have that have a similar cancer outcome. For breast surgery decision-making, shared decision-making is critical.
If a patient comes in with a devastating diagnosis and there’s really only one operation for them, that’s a pretty straightforward conversation. When the patient comes in with a breast cancer diagnosis, there are often at least two options for them — and within those two options, multiple additional options. It really comes down to a shared discussion between the patient and the physician.
This shared decision-making is a backand-forth discussion between the patient and the provider to discuss the pros and cons of each approach. It’s important for the physician team to listen to the priorities of the patient. For most patients, the first priority is to, of course, get rid of the cancer and treat it appropriately, but what are the other priorities? Is it the time away from work? Is it maintaining their own breast? Is it symmetry? Is it finances? Is it fear of radiation? Hearing all the aspects that are
concerning to the patient is important so that the patient and the physician can come up with a treatment that is the most appropriate for them, together.
Can you talk a little bit more about treating breast cancer from a surgical standpoint?
The first key decision that many patients have is breast-conserving surgery versus a full mastectomy. Patients who have extremely large tumors may not be a candidate for breast-conserving surgery, but for many patients these days, we detect the tumor earlier and they are a candidate for either breast conservation or mastectomy. So, is the patient interested in breast conservation? Is the patient interested in mastectomy?
Neoadjuvant systemic therapy can take the form of chemotherapy (used for most estrogen receptor negative breast cancer or HER2 positive breast cancer) delivered for three to six months before surgery. For patients with estrogen-responsive breast cancer, we can treat with endocrine therapy, an oral medication they can take for four to six months prior to surgery. Both of these approaches can shrink the tumor prior to surgery and potentially make patients candidates for breast conservation. Also, oncoplastic surgery — removal of the tumor with advancement of the adjacent tissue to restore the shape of the breast — enables removal of larger tumors and still conserves the breast.
Breast conservation surgery is usually followed by radiation, whereas a mastectomy may not always be followed with radiation, depending on the size of the tumor and whether the lymph nodes are involved or not.
There are so many different options, and it’s really important for the patient to hear the pros and cons of each approach when they come in.
INTERVIEW WITH
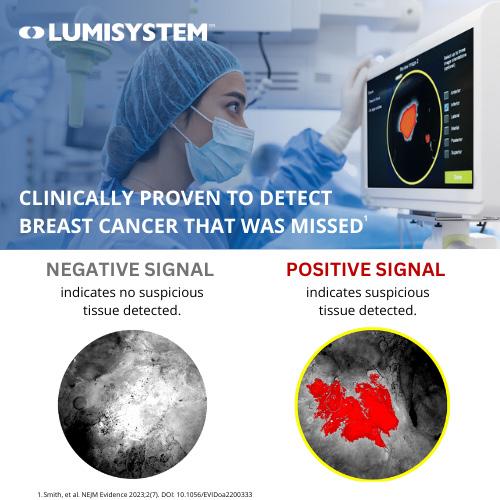
New Imaging Technology Could Result in Better Outcomes for Breast Cancer Patients
One in eight U.S. women will be diagnosed with breast cancer during their lifetime, and many of these patients will undergo a lumpectomy — a surgery to remove the tumor while preserving healthy breast tissue.
Despite advancements, up to 36% of patients require a second lumpectomy because cancer may have gone undetected. Newer surgical imaging technologies like LumiSystem™ represent a promising solution.
LumiSystem is the combination of two recently FDA-approved products: LUMISIGHT™ (pegulicianine), an optical imaging agent that fluoresces at sites of suspected cancerous tissue, and Lumicell™ Direct Visualization System (DVS), an imaging device that provides fluorescence guidance, enabling surgeons to do real-time scanning of the breast cavity during lumpectomy to detect and resect residual cancer.
Results from the LumiSystem clinical study showed that 10% (35 of 357) of women had improved surgical outcomes when using LumiSystem as a part of their lumpectomy procedure. (Of the 35 patients with improved surgical outcomes, LumiSystem detected and guided the removal of cancer that would have been missed otherwise in 27 patients. Nine patients experienced a conversion from
positive to negative margins. One patient experienced both benefits.) The study also showed that LumiSystem offers 84% diagnostic accuracy based on true positive and true negative images detected.
By integrating this technology into the procedure after the main specimen is removed, surgeons can make more informed decisions about additional tissue resection during surgery, offering patients a path toward improved surgical outcomes.
“During initial lumpectomy surgeries, surgeons still struggle to identify and remove all of the tumor,” said Barbara Smith, M.D., Ph.D., director of the Breast Program at Massachusetts General Hospital, professor of surgery at Harvard Medical School, and an investigator in the LumiSystem clinical study. “With LumiSystem, we now have a technology that is clinically proven to achieve a more complete cancer resection during lumpectomy, which could help some patients avoid a second surgery.”
References on file. MKT00314rA
Written by Lumicell
What is LUMISIGHT (pegulicianine) and Lumicell DVS?
To learn more about advances in breast cancer surgery, visit www.LumiSystem.com
IMPORTANT SAFETY INFORMATION
• LUMISIGHT (pegulicianine), an optical imaging agent, and Lumicell DVS, a fluorescence imaging device, are used in adults with breast cancer to help detect any remaining cancerous tissue at the surgical site following removal of the primary specimen during a lumpectomy procedure.
What is the most important information I should know about LUMISIGHT?
• Hypersensitivity Reactions: LUMISIGHT may cause serious hypersensitivity reactions, including anaphylaxis. Anaphylaxis has occurred in 4/726 (0.6%) of patients in clinical studies. Tell your doctor if you have any history of hypersensitivity reactions to pegulicianine or to contrast media or products containing polyethylene glycol (PEG). Your healthcare provider should have emergency resuscitation drugs, equipment, and trained personnel available during the use of LUMISIGHT. Healthcare providers should monitor all patients for hypersensitivity reactions and if one is suspected, immediately discontinue the injection and initiate appropriate therapy.
• The most common side effects (≥1%) include hypersensitivity and an abnormal color in urine.
What additional important information should I know about LUMISIGHT and Lumicell DVS?
• Adjunctive Use: Lumicell DVS is for use as part of the lumpectomy procedure and is not a replacement for the standard of care procedures and pathology.
• Risk of Misdiagnosis: The absence of a signal in surgery does not rule out cancer. Additionally, a positive signal may be seen in non-cancerous tissue.
• Interference from Dyes Used for Sentinel Lymph Node Mapping: Your healthcare provider should avoid use of dyes before imaging the lumpectomy cavity in patients who have received LUMISIGHT.
• Other Risks: Using the Lumicell DVS handheld probe may cause tissue damage or infection.
You are encouraged to report negative side effects of prescription drugs to the FDA. Visit MedWatch or call 1-800-FDA-1088. Please see the LUMISIGHT Prescribing Information, including Boxed Warning, and Lumicell DVS Instructions for Use. For complete product information visit www.LumiSystem.com.
Rx only
CANCER’S TRYING TO TAKE HER BREAST.
LET’S Help MAKE DAMN SURE IT DOESN’T TAKE HER
HOME.
®
No woman undergoing breast cancer treatment should ever have to choose between getting medical care or paying the mortgage. Sadly, treatment costs, coupled with income loss, force this decision. Pink Fund provides up to $3,000 over 3 months to help with housing, transportation, utilities and insurance. Donate at PinkFund.org to give Real Help for the Other Part Of The Fight®.