
5 minute read
Breast Implant Update


What to know about breast implants
By Dr Tim Cooper, Plastic Surgeon, Nedlands
Women with breast implants are increasingly concerned about the risk of developing cancer or implant-related illness. They may be experiencing breast pain or other unexplained symptoms and access information online and in the media.
There is considerable confusion as to the difference between BIA ALCL (Breast implant associated anaplastic large cell lymphoma), breast cancer, and BII (breast implant related illness). Many women with implants may well be concerned about a silent rupture.
BIA ALCL is a rare form of nonHodgkin’s Lymphoma, first classified as a distinct clinical entity by the WHO in 2016. It typically presents as an unexplained swelling of one or both breasts 5-10 years post implantation. ALCL has never been reported in smooth implants and appears related to more textured implants.
The more coarse, or macrotextured, implants have an incidence as high as one in 2000 breast augmentations, whereas the micro-textured products (all listed on TGA implant hub) have an
incidence of 1 in 80,000. This needs to be put in the context of the high lifetime risk of developing breast cancer.
Tissue expanders and anatomically shaped implants only come as textured products. Textured implants are often preferred as they have a lower risk of capsular
contracture and are positionally more secure.
The TGA and the FDA have withdrawn macro-textured implants from the market. Allergan, one of the implants most commonly involved with ALCL, voluntarily withdrew its product. The TGA has mandated implant manufacturers report any episodes of ALCL but has not recommended that all textured implants be removed in the absence of ALCL diagnosis. Gathering information regarding breast implants has been advanced by the ABDR (Australian Breast Device Registry) for all implantrelated surgery.
ALCL is diagnosed by cell cytology and immunohistochemistry of seroma fluid from US-guided aspiration.
Evidence supports the development of a low-grade infection with the formation of a bacterial biofilm attached to the textured surface of the implant in someone who is immunologically compromised. Recommendations have been made to minimise bacterial contamination in implant surgery.
Beechboro Family Practice
High patient volume at busy centre

• Full time/part time position available • Large and modern practice • Collegial environment


• Excellent CDM and treatment room nurse support • This position would ideally suit a female GP
BACK TO CONTENTS Key messages
Cancer associated with implants is rare and treatable Implant-related illness is not clearly defined. Empathy is key Rupture is detected on US and warrants removal.
The majority of these tumours are fluid, not solid. Hence mammography, MRI and /or PET CT are reserved for investigating diagnosed ALCL. Once diagnosed, patients should jointly be under the care of a plastic surgeon and a haematologist with a special interest in ALCL.
Typical treatment involves entire removal of the implant and capsule. Adjuvant therapy is rarely required. The majority of patients suffer no long term effects. However, there have been three reported ALCL fatalities in Australia in the past decade.
Breast implant illness (BII) Increasing numbers of women with breast implants self-identify and present with various systemic symptoms (e.g. fatigue chest pain, brain fog, rash, anxiety) believing these to be related to their breast implants.
There is no medically accepted diagnostic testing for BII. The potential link between silicone breast implants and autoimmune disease has been extensively studied for over two decades

with no causal link found. Medical grade silicone is an entirely inert substance created by hydroxylating silica to form polymethoxylsiloxane. with all traces of antioxidants, dyes and plasticers being removed.
Many concerned patients present with multiple tests organised by their naturopath and much information about their condition and how to manage it. This includes further lab testing, request for samples and instructions on ‘en bloc’ capsulectomy to remove all traces of silicone.
My approach is empathetic despite the lack of scientific evidence. If they wish to proceed with removal, then I will do so. If they are uncertain, I will perform an US to exclude a rupture. Anecdotally, many of these patients get better and remain grateful following explant surgery. The majority of implant ruptures are silent (clinically undetectable), but may be accompanied by a shape or consistency change, capsular contracture or axillary lymphadenopathy. Implants should not be considered lifetime devices nor be routinely changed at 10 years (where rupture rate should be less than 10%).
An US is recommended if rupture is suspected. MRI is only necessary in equivocal circumstances. Rupture is not a medical emergency and many patients will have had the rupture for some time. However, there remains a significant degree of patient anxiety with confirmed rupture.
Author competing interests - nil



Envision. At the forefront of imaging technology.
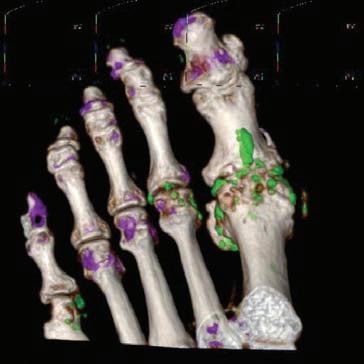
Dual Energy CT exploits the unique X-ray absorption properties of uric acid crystals and accurately diagnoses gout (green) in acute, chronic, or subclinical scenarios.
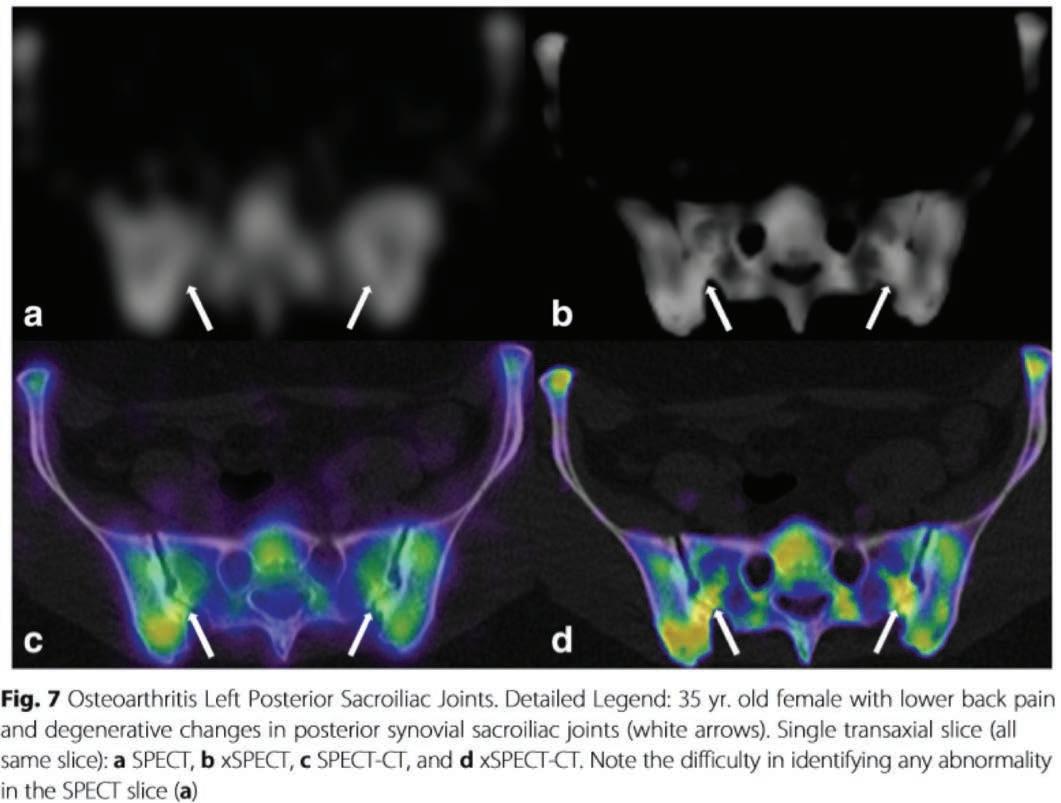
xSPECT-CT bone scans. Osteoarthritis Left Posterior Sacroiliac Joints. Detailed Legend: 35yr old female with lower back pain and degenerative changes in posterior synovial sacroiliac joints (white arrows). Single transaxial slice (all same slice): a SPECT, b xSPECT, c SPECT-CT, and d xSPECT-CT. Note the difficulty in identifying any abnormality in the SPECT slice on image a.
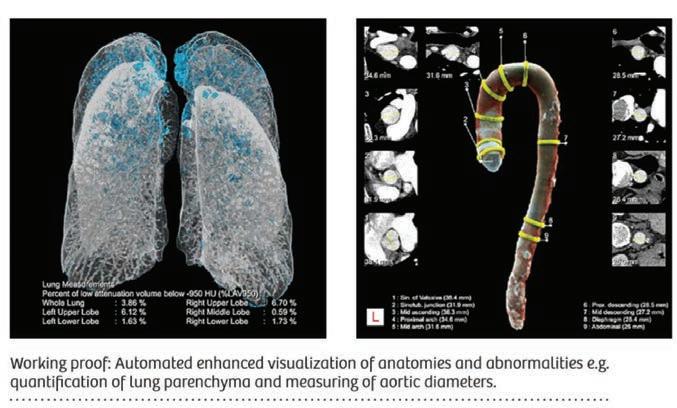
AI augmented CT imaging* Automated enhanced visualization of anatomy and abnormalities e.g. quantification of lung parenchyma and measuring of aortic diameters.
* with permission from Siemens Healthineers








