
5 minute read
Incidental findings on cardiac CTs


By Dr Scott Claxton, Respiratory Physician, Joondalup
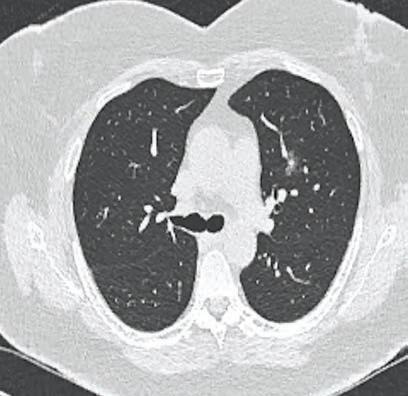
Jennifer is 63 and complained of chest pain. She has a family history of ischaemic heart disease and a history of intermittent smoking for a few years. A CT calcium score didn’t show any coronary artery calcification but an incidental ground-glass nodule was seen in her left upper lobe (Fig 1). This was followed up over a twoyear period when it showed the development of a solid component (Fig 2).She was referred for resection and pathology identified an adenocarcinoma.
CT-based investigation for diagnosing coronary artery disease and assessment of cardiac risk is increasing. As a result, coincidental imaging of the lung fields is also increasing. This has led to increased identification of clinically silent but not necessarily clinically irrelevant, non-cardiac abnormalities.
These can comprise findings in the chest wall, breasts, skeleton, lung, pulmonary vasculature, mediastinum and non-coronary vasculature. Some will be clearly significant requiring prompt assessment. For others, the shortand long-term risk is not so clear and follow-up probably with further imaging will be required. Even in health, the respiratory continued from Page 39 Every consultation is the chance to ask, “how are things going for you, really?” Remembering to check in on a person especially if they live alone, have little social support, have lost their job or are finding the ongoing situation increasingly difficult to manage. Doctors can provide accurate and trustworthy information to combat the hype, misinformation and conspiracy theories and reaffirm the positive aspect of healthy lifestyle choices.
Fig 1.
system is exposed to numerous, potentially irritating or noxious challenges. Respiratory infection is common and over time these can lead to abnormalities in lung tissue that may be identifiable radiologically. With normal ageing comes changes in lung function and histology, a loss of elastic recoil, increased collagen deposition, loss of small airway supports. In addition, other more well-defined factors can impact on lung structure and function (cigarette smoke, pollution, asbestos etc.). While sometimes these may cause symptoms and be recognised, Use a brief questionnaire (e.g. Short Warwick-Edinburgh Mental Wellbeing Scale) and or subjective wellbeing questionnaire as a form of rapid assessment of mental wellbeing. Evaluate wellbeing on the basis of how people feel and function on a personal and social level, and how they evaluate their lives as a whole. Provide additional ongoing support via telehealth. This facilitates tracking patient progress, especially for those previously diagnosed with complex or severe mental health other times they may be early stage disease or entirely benign. Incidental imaging of the lung fields brings them to attention. In turn the lung abnormality will need to be assessed on its own merits.
Cardiac disease and respiratory disease share risk factors (smoking, increased age) and so abnormality in both is to be expected. Non-cardiac (and for the purposes of this discussion – pulmonary) incidental findings on cardiac CTs are generally grouped as either significant or non-significant. The former can include lung nodules and masses, pulmonary emboli, aortic abnormalities, breast masses, pleural masses and effusions. Non-significant, or perhaps better referred to as less immediately significant, findings include emphysematous change, small (<6mm nodules), pleural thickening, interstitial lung abnormalities. In one large study of 2050 scans, 5% had significant, non-cardiac findings. The most common were lung nodule (<3cm) or lung mass (>3cm). In a patient with a history of cigarette smoke exposure there is the concern that these lesions may
Rethinking mental health in COVID-19
represent early malignancy. For challenges or considered vulnerable to poorer mental health. Making mental wellbeing part of a regular health check has the potential to reduce the prevalence of mood disorders in our community. Now that would be something to celebrate.
Author competing interests - nil
Key messages
The lungs are exposed to challenges and assaults, which can leave their mark. With the growing use of cardiac CT, these findings will be more frequent. The specific nature of the findings will determine the need and extent of follow-up.
large masses, further investigation (e.g. biopsy) may be indicated. For smaller nodules, further CT followup may be required. The specific program of follow-up varies depending on the nature of the nodule (ground glass, semi-solid, solid) and the risk of underlying malignancy (age, smoking history, nodule size, number of nodules, past history of malignancy). Data from lung cancer screening programs and other cohort studies has allowed the development of follow-up algorithms for pulmonary nodules dependent on the risk of malignancy (e.g. Fleischner
Fig 2.
Society). These aim for a balance between accurate and timely detection of malignancy and limiting radiation exposure by repeat scanning. Other incidental pulmonary findings such as bronchial wall thickening, emphysema and fibrosis may represent age-related changes. This may include exposure to environmental pollution (i.e. urban compared to rural living) or be related to previous cigarette or other (e.g. occupational) exposures. Often these abnormalities may be asymptomatic, or the symptoms accepted as part of growing older. Initial clinical assessment and lung function testing may be indicated. Follow-up assessment either radiological or physiological (lung function) may be required to identify progression or development of disease especially with interstitial lung abnormalities. The timing of this is less clear than with nodules but may not need to be any more frequent than annually. Assessment of the potential cause is necessary. A history of occupational or environmental exposure (e.g. asbestos) may help with planning of follow-up. Prior imaging is always useful.
– References available on request Author competing interests – nil
At SKG Radiology, we know your patient’s welfare, as well as your own, is very important to you. We recognise the continuing need to provide the same great quality service across our practice, so we
are bulk-billing all out-patient Medicare rebateable services*,
during this time of crisis.
* Some exceptions do apply.
When you depend on the right result, the choice is clear, SKG Radiology.

Genea Hollywood Fertility provides a comprehensive individualised range of fertility treatments for Western Australians.
Our specialist team has up to 30 years’ experience in fertility treatments.

Our patients have access to Genea’s world leading science.
All patients have individualised assessment and treatment
Genetic testing is available where needed
Our treatment charges are transparent
Our clinicians, scientists and support staff are committed to achieving successful outcomes.
Dr Simon Turner MBBS, FRANZCOG, FRCOG Prof Lincoln Brett BMedSc, BSc (Hon, MBBS, FRANZCOG Dr Julia Barton MBBS, FRANZCOG, FRCOG Dr Michael Allen MBBS (UWA), FRANZCOG, MRMed Dr Joo P. Teoh FRANZCOG, MRCP (Ire), MRCOG, MBBCh, Msc (Lon), MD (Glasgow) Subspecialty Repromed (UK)
Genea Hollywood Fertility means high success rates, understanding staff and individual care.
Genea Hollywood Fertility








