5 minute read
Improving Quality of Vision and Life in a Patient with Aniridia-Associated Glaucoma


BY CRAIG J. CHAYA, MD
Anna, an 11-year-old with aniridia, was referred to the glaucoma service for poorly controlled intraocular pressure (IOP) despite maximal medical therapy. Her aniridia was familial, with her father having the same condition. Her best-corrected visual acuity was 20/250 in both eyes, and her IOP was 39 mmHg in the right eye and 28 mmHg in the left eye on Latanoprost, Brimonidine, and Dorzolamide/Timolol. She had moderate-to-severe light sensitivity at a baseline that had worsened over the last year. Because of her nystagmus, she had difficulties performing visual fields or optical coherence tomography (OCT) scans.
Treatment Plan
We performed an examination under anesthesia, which revealed peripheral iris stumps with evidence of progressive angle closure. Fortunately, her optic nerves appeared healthy, with no significant cupping in either eye. In addition, her corneas were clear without evidence of significant limbal stem cell deficiency. However, she had moderate cortical cataracts in both eyes.
We considered addressing the cataract and glaucoma separately or simultaneously. After discussing several options with Anna and her family, we planned to address the glaucoma first. We chose the XEN Gel Stent procedure because of her early age, difficulty managing a trabeculectomy in the setting of nystagmus, and the need for substantial IOP lowering.
In early 2020, she underwent a XEN Gel stent augmented with mitomycin C and Ologen collagen matrix. She recovered well from the surgery and had excellent IOP reduction in both eyes.
The next phase of her therapy focused on improving her vision. Anna’s cataracts had progressed. We considered the option of simultaneous cataract surgery and placement of an iris prosthesis to reduce glare and improve the quality of her vision. Anna was excited about this option and submitted a picture of an iris with her desired color, which was used as a template to custom-make her prostheses. In 2021, Anna underwent successful cataract surgery, with an IOL and iris prosthesis in each eye (Figures 1-3).

James Gilman, CRA, FOPS, project administrator of Moran’s Ophthalmic Imaging, scans the patient’s eyes following her iris prosthesis surgery.
About Aniridia
Aniridia is a condition with near-total or total absence of iris tissue. The condition can be inherited or acquired in cases of severe penetrating injury or during complicated anterior segment surgery. Inherited cases are bilateral and arise from defects in the PAX6 gene that is responsible for normal ocular development. This may result not only in aniridia but also in abnormalities of the cornea (limbal stem cell deficiency), fovea (hypoplasia), optic nerve (hypoplasia), and lens (cataracts). Sporadic aniridia may also be associated with non-ocular abnormalities such as a renal tumor known as a nephroblastoma (Wilms’ tumor). The condition requires vigilant screening.
In 2016, the FDA approved the XEN 45 Gel Stent as the first subconjunctival soft implant for refractory glaucoma. It is composed of pliable gelatin that allows it to conform to the contours of the eye. Its internal lumen is 45 microns in diameter and 6 mm in length. Although not wellstudied in children, the implantation of the XEN 45 Gel Stent is less invasive than traditional glaucoma surgery. In addition, the first FDA-approved silicone iris prosthesis, the CUSTOM FLEX ARTIFICIALIRIS, became available to treat all types of aniridia in 2018. The CUSTOM FLEX is color-matched to the unaffected iris or can be made to a patient’s desired color. In a study of aniridic patients (Reference 1) over 95% reported an improvement in glare and photophobia. In addition, there were no major adverse events or increases in post-operative complications.
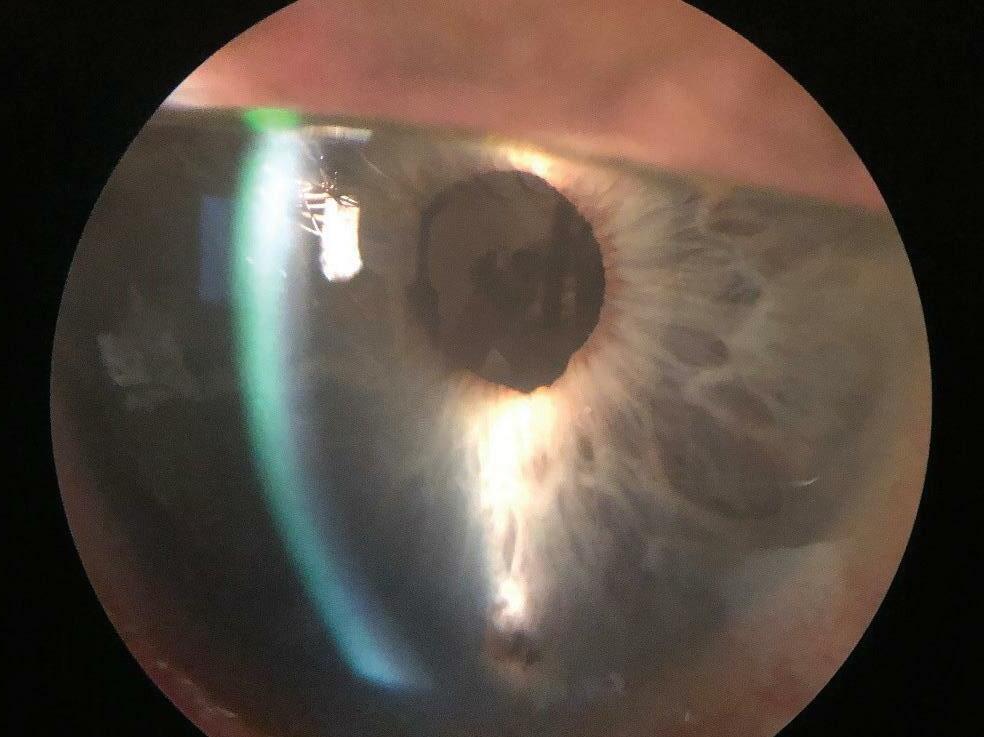
Figure 1

The patient’s right eye before iris prosthesis surgery.

The patient’s right eye before after iris prosthesis surgery.
Figure 2

The patient’s left eye before iris prosthesis surgery.

The patient’s left eye after iris prosthesis surgery.
Figure 3

The patient picked the color for the custom-made iris prosthesis in each of her eyes.
Case Discussion
Anna’s case illustrates the complexity of caring for aniridic patients who may be suffering from multiple issues like glaucoma, cataracts, and glare simultaneously.
For Anna, a staged approach was critical. First, we needed to manage her glaucoma to mitigate irreversible optic nerve damage. Then, we needed to remove her cataracts and place an iris prosthesis in the capsular bag to complete her anterior segment reconstruction. Placing both her IOL and iris prosthesis in the capsular bag would reduce the risk of long-term corneal decompensation.
Her specific vision goals and timely technology anchored our approach.

Dr. Chaya specializes in anterior segment ophthalmology and surgery, focusing on the medical and surgical management of routine/ complex cataracts and glaucoma. He serves as medical director of Moran’s Global Ophthalmology Division.
REFERENCE
1. Figueiredo GB, Snyder ME. Long-term follow-up of a custom-made prosthetic iris device in patients with congenital aniridia. J Cataract Refract Surg. 2020 Jun;46(6):879-887.
F INANCIAL DISCLOSURE
Dr. Chaya has served as a consultant and received research funding from AbbVie, the maker of the XEN 45 Gel Stent. He has nothing to disclose regarding HumanOptics, maker of the CUSTOMFLEX ARTIFICIAL IRIS prosthesis.