
6 minute read
The Rise of OCT to Detect and Treat Glaucoma Earlier

BY SUSAN CHORTKOFF, MD
Like many of you, I am a clinician seeing many new and established glaucoma patients to diagnose disease so that treatment can be initiated and detect progression so that treatment can be advanced to prevent functional impairment.
The diagnosis of glaucoma is not based on a pathognomonic test or symptom but a compendium of tests and observations. These include history, assessment of risk factors, findings of intraocular pressure, corneal thickness, gonioscopic findings, optic nerve features, nerve fiber layer defects and hemorrhages, and testing that includes perimetry and imaging. Historically, optic nerve photographs served to document glaucomatous features and their change over time.1
Testing Improvements
Over the last 20 years, objective imaging and measurements of ocular structures have dramatically improved our ability to assess structural changes in glaucoma. While many other technologies have contributed to the development of imaging as a key determinant in diagnosing glaucoma and glaucomatous progression, optical coherence tomography (OCT) has risen to the forefront. It has brought us the ability to examine structural changes within the optic nerve head, the nerve fiber, and macular ganglion cell layers. This technology has given us unprecedented ability to detect early glaucoma development and progression even if we don’t fully understand the underlying pathogenesis of these changes. However imperfect, never before have we been able to correlate so closely the structural and functional relationships that result in glaucomatous damage.
Finding theFix in Visual Loss Indicators
We know that the presence of visual field loss on initial evaluation is highly associated with the development of blindness.2,3 Macular ganglion cell and circumpapillary retinal nerve fiber layer thickness (RNFL) measurements are mutually predictive of visual field progression and are relevant to facilitating early detection of disease deterioration.4 And while it has yet to be proven that detecting and treating early progressive glaucomatous change results in functional benefits to patients or prevents blindness,5-7 it allows us to discuss with patients the expanding surgical and non-surgical treatment options for their care while balancing potential risk and burden of treatment and its impact on quality of life.8 Using complementary diagnostic techniques to “find” patients with rapid rates of progression can help us determine those in which a more aggressive “fix” is warranted to prevent blindness.5
Comparing OCT Platforms, Combining Strategies
Over 100 companies offer OCT technology. Our glaucoma service primarily uses the Heidelberg Engineering imaging platform, which, along with the Glaucoma Premium Edition Software, allows measurement of progressive change in the circumpapillary RNFL, optic nerve structure, and ganglion cell layer. It is important to recognize that while diagnostic abilities of most OCT platforms are comparable, data is not transferrable 9-11 and that when we change technologies, our ability to measure progression is interrupted until we obtain new baselines.
In addition, we must carefully analyze results to identify potential pitfalls in diagnosis and progression analysis. Artifacts from segmentation error, inadequate image acquisition, poor signal strength (dry eye, cataract, nystagmus, strabismus), and coexisting ocular pathologies (myopia, peripapillary atrophy, epiretinal membranes, vitreous traction, and macular degeneration) may confound our ability to measure and follow one or another area of the pathways involved in glaucoma.
The disease stage may also influence which testing modalities offer the most reliable and accurate assessment of progression. For example, progressive structural loss in the peripapillary region predicts future functional losses at earlier stages of disease, whereas visual fields and measurement may better evaluate increased disease severity in the ganglion cell layer within the macula.
In all cases, visual field testing continues to be paramount in evaluating glaucoma, and metrics that combine testing strategies in glaucoma are being designed to achieve greater power than each test can alone.
Case Study in Structure-Function
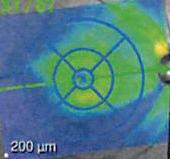
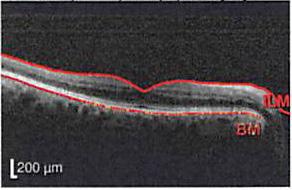
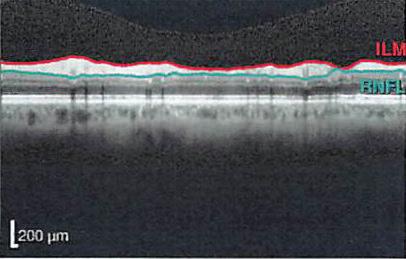
We followed a 71-year-old woman with ocular hypertension for eight years without progression until December 2019. At that time, we noted significant thinning (-57um inferior temporal and -8um global) on OCT RNFL imaging of the right eye, along with a corresponding large area of arcuate thinning on the macular thickness map change report. Treatment of intraocular pressures had been initiated before these changes and escalated after these changes occurred. Although initially, progression continued in the inferior RNFL and macular region, OCT measurements have now stabilized. (See figures below.) Visual field testing five months prior to these findings was completely normal in the involved eye, with only very subtle changes on visual field testing first being noted six months after OCT progression was first noted, with definitive progression in the superior paracentral field lagging until May 2021.

Baseline OD: 10/17/2018
Follow Up OD: 2/22/2022
Baseline OD: 10/17/2018

Follow Up OD: 2/22/2022

Baseline OD 12/2/2019
Follow Up OD: 2/2/2022

Dr. Chortkoff specializes in the management and treatment of glaucoma as well as comprehensive ophthalmology. She is a member of the American Glaucoma Society and the American Academy of Ophthalmology.
REFERENCES
1. Yuksel Elgin C, Chen D, Al-Aswad LA. Ophthalmic imaging for the diagnosis and monitoring of glaucoma: A review. Clin Exp Ophthalmology. 2022;50(2):183-97.
2 . Chen PP. Blindness in patients with treated open-angle glaucoma. Ophthalmology. 2003;110(4):726-33.
3 . Hattenhauer MG, Johnson DH, Ing HH, Herman DC, Hodge DO, Yawn BP, et al. The probability of blindness from open-angle glaucoma. Ophthalmology. 1998;105(11):2099-104.
4 . Hou HW, Lin C, Leung CK. Integrating Macular Ganglion Cell Inner Plexiform Layer and Parapapillary Retinal Nerve Fiber Layer Measurements to Detect Glaucoma Progression. Ophthalmology. 2018;125(6):822-31.
5 . Johnson DH. Progress in glaucoma: early detection, new treatments, less blindness. Ophthalmology. 110. United States2003. p. 1271-2.
6. Yu M, Lin C, Weinreb RN, Lai G, Chiu V, Leung CK. Risk of Visual Field Progression in Glaucoma Patients with Progressive Retinal Nerve Fiber Layer Thinning: A 5-Year Prospective Study. Ophthalmology. 2016;123(6):1201-10.
7. Miki A, Medeiros FA, Weinreb RN, Jain S, He F, Sharpsten L, et al. Rates of retinal nerve fiber layer thinning in glaucoma suspect eyes. Ophthalmology. 2014;121(7):1350-8.
8. Gracitelli CP, Abe RY, Tatham AJ, Rosen PN, Zangwill LM, Boer ER, et al. Association between progressive retinal nerve fiber layer loss and longitudinal change in quality of life in glaucoma. JAMA Ophthalmology. 2015;133(4):384-90.
9 . Lee ES, Kang SY, Choi EH, Kim JH, Kim NR, Seong GJ, et al. Comparisons of nerve fiber layer thickness measurements between Stratus, Cirrus, and RTVue OCTs in healthy and glaucomatous eyes. Optom Vis Sci. 2011;88(6):751-8.
10. Kanamori A, Nakamura M, Tomioka M, Kawaka Y, Yamada Y, Negi A. Agreement among three types of spectral-domain optical coherent tomography instruments in measuring parapapillary retinal nerve fibre layer thickness. Br J Ophthalmology. 2012;96(6):832-7.
11. Koh KM, Jin S, Hwang YH. Cirrus high-definition optical coherence tomography versus spectral optical coherence tomography/scanning laser ophthalmoscopy in the diagnosis of glaucoma. Curr Eye Res. 2014;39(1):62-8.
F INANCIAL DISCLOSURE
Dr. Chortkoff has no financial interest in any of the products mentioned in this article.








