
17th May 2023 Poster Competition Group D QI in Progress


Weight of workplace violence in ED: (1)
§ 72% verbal violence
§ 18% physical violence
§ >50% instigated by family members
§ 27% instigated by patients
North Middlesex Hospital(3)

§ >180,000 patients attend ED per year
§ Serves a population >90 nationalities
§ Deprivation is common; with 1 in 5 children living in poverty
§ Rising local rates of youth violence
Interventions suggested in previous QI project:
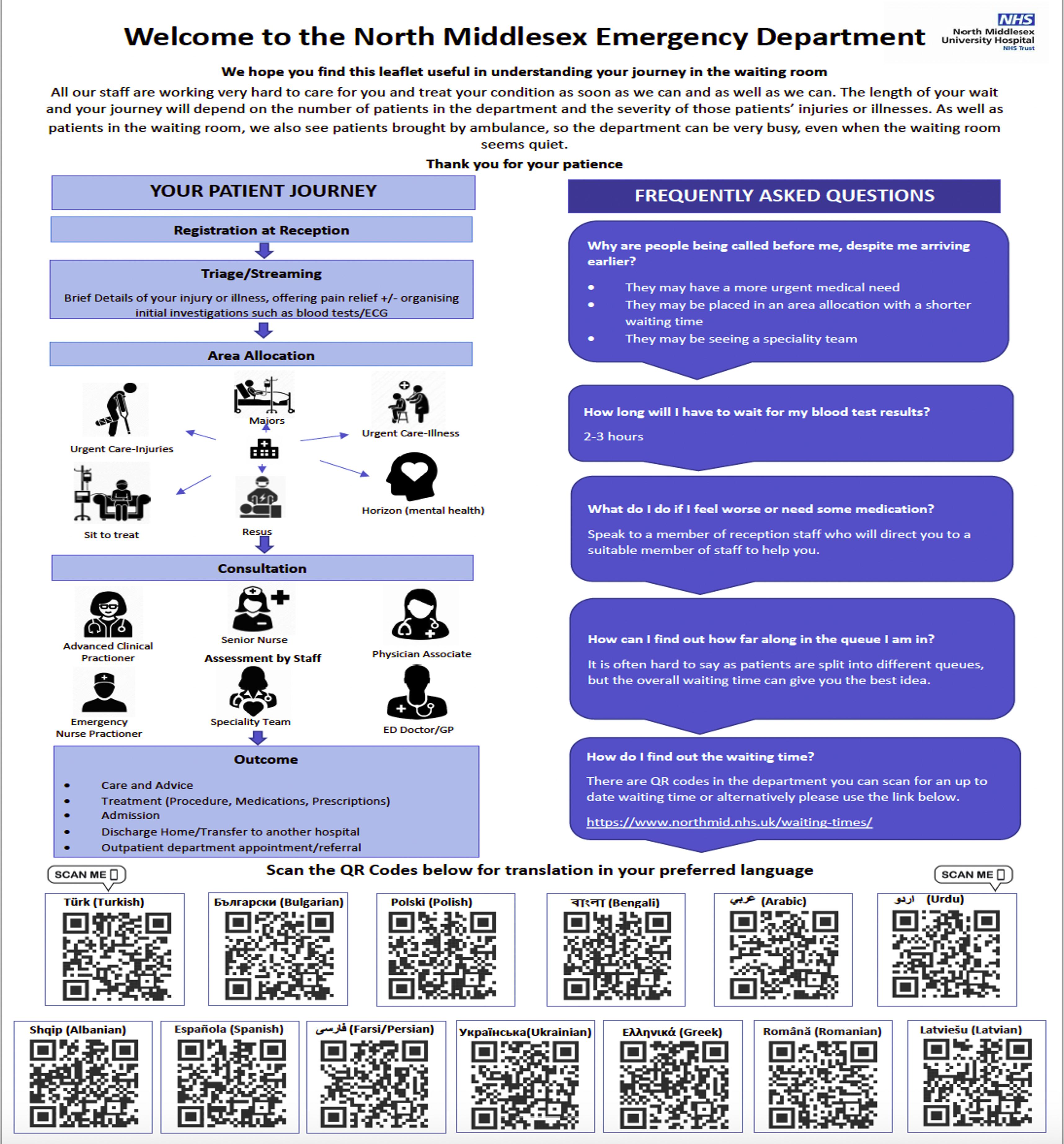
1) Information on current waiting times to be communicated to patients waiting in the ED
2) Artwork describing the triage process
3) Providing information in multiple languages
4) Structural adjustments to the main waiting area
5) Information on levels of violence and aggression toward NHS workers
Aims of our QIP:
Physical and mental impact of workplace violence on doctors and nurses: (2)
§ decreased job satisfaction (54%)
§ feeling scared (37%)
§ loss of sleep in (29% )
§ missing work due to violent incidences (6%)
All of the above can impact work productivity and patient care
What we have done:
§ Asked patients their perspectives on their experiences in ED
§ Involved nursing and reception staff in designing the information poster to ensure that adequate information is portrayed
1) To collect patient views on waiting times and understand the patient journey
2) To implement changes to the patient experience with a view to reducing the incidence of aggression towards staff in our department
3) Create a poster of the patient journey

4) Develop artwork with sixth form students
1) 'Mentimeter’ questionnaire developed for patients in the ED waiting room
2) Sixth form students engaged to create posters about violence and aggression; we worked in partnership with a local state school with a high deprivation index with students of diverse backgrounds who wanted to become healthcare workers in the future

3) Stakeholders involved: patients, reception staff, students, security team, governance team, violence and aggression trust group
4) Translated the poster into different languages with help from our staff group

5) Posters displayed in the ED reception area
6) Live waiting time screen under development

• A framework for developing, testing and implementing changes leading to improvement
• The fishbone diagram identifies possible causes for an effect or problem

• These helped us to structure brainstorming sessions and sort ideas into useful categories
§ We learnt that 2/3 of patients know where to find the updated ED waiting time
§ However, almost 50% of patients are not aware of which queue they are in and how long they will be in it
§ Clinicians need to better communicate this to their patients


We hope to:
1) Repeat the patient mentimeter questionnaire to compare results postintervention
2) Re-review statistics on violence and aggression after our changes have been implemented
3) Continue to engage with community representatives, security teams, trust violence and aggression group and local police
Authors: Dr Sally-Ann Ofori, Kaushiki Bakaya, Audrey Ward, Fatima Yaqub and Dr Natalia Barry* *North Middlesex University Hospital NHS Trust , Sterling Way, London, N18 1QX natalia.barry@nhs.netA lack of formal weekday morning medical SHO handover posed a risk to patient safety through crash bleeps being left unattended.
• 4% of SHOs felt there was an effective handover
• 85% had found a crash bleep unattended
• 56% had witnessed a crash call on an unattended bleep
• 17% of crash bleep tests were responded to
Aims
To introduce a new handover system to improve patient safety and doctors’ satisfaction over 6 months, aiming for:

• 80% of crash bleep tests to be answered
Over 3 PDSA cycles, we developed an SOP for a new formal morning medical crash bleep handover. Surveys were conducted amongst SHOs at baseline (n=27), cycle 2 (n=17), and cycle 3 (n=18). PDSA cycles below:
• 83% felt the handover improved patient safety

• 78% felt it made it made bleep handover quicker and easier
• 67% felt it was an effective handover
To develop formal crash bleep handover
Pilot handover process (May 2022)
Bleep test response rate data collected (June 2022)

Suggested edits made to handover process
To assess the sustainability of the handover model
Daily staffing emails sent to SHOs and RMOs (July 2022)
SHOs resurveyed (July 2022)
Handover process relayed to new starters at induction
To assess the effect of medical registrar presence
Medical registrar presence mandated (Aug 2022)
Improved junior perception
Unattended bleeps
The proportion of SHOs reporting seeing unattended bleeps decreased from 85% to 28%, and witnessed crash alerts on unattended bleeps decreased from 56% to 17%.
4% 59% 67% 0 10 20 30 40 50 60 70 80 Baseline Cycle 2 Cycle 3 SHOs who feel handover is effective (%) Perceived Effectiveness of Handover 85% 29% 28% 56% 6% 17% 0 10 20 30 40 50 60 70 80 90 Baseline Cycle 2 Cycle 3
% medical SHOs reporting finding an unattended crash bleep % medical SHOs reporting witnessing a crash alert on an unattended crash bleep
Response rate to switchboard crash bleep test calls increased from 17% over 1 week at baseline to 52% over 1 week in cycle 1.
A1 portrait
59.4cm x 84.1cm
23.39 inches x 33.11 inches
To size your poster correctly Go to Design in Bar above Go to Slide Size
• Page set up
• Custom
• Pick portrait orientation
• Key dimensions into Width and Height
59.4cm x 84.1cm
1. NAME YOUR FILE AS FOLLOWS: Insert your poster reference number and your first and last name into the filename when you save your poster PDF file: #posternumber_Firstname_Lastname_A1_PosterPDF_2023
2. WHEN COMPLETED UPLOAD YOUR POSTER HERE: https://www.dropbox.com/request/xQ6H2cPt2uer6CqAPIk8

• Our practice prescribes more high dose opioids and gabapentoids than national average1
• Limited evidence of benefit in chronic pain2,3
• Risk of harm increases with co-prescription50% increase in opioid related death when co-prescribed with gapapentinoids4
Aims
• Intervention: Increasing patient access to support from mental health and wellbeing coach. Educating patients about nonpharmacological ways to manage pain (e.g. exercise, mindfulness)


• Inclusion: Patients co-prescribed opioids and gabapentinoids. Selected a group of patients who’d already been invited by text (depression +/- chronic back pain +/- BMI >32)
• Exclusion: Undergoing treatment for cancer
• Reduction in number of patients coprescribed opioids and gabapentinoids (baseline=42, cycle 1=25, cycle2=20)
• Letters are an efficient method to contact patients and provide information

• Phone calls most effective way to engage patients in accessing support
• De-prescribing in chronic pain requires careful planning and collaboration with patient
• Next steps: wellbeing coach to book patients in with usual GP for de-prescribing consultation
Background and Aims:
The effectiveness of comprehensive medication reviews within the primary care setting is directly correlated with enhanced patient safety and improved clinical outcomes (1, 2). Structured medication reviews involve a thorough review of a patient’s medication and take into consideration all aspects of health, whilst weighing up risks vs benefits. Prescribing initially occurs in the primary care setting and therefore timely review of medications will reduce adverse side effects and ultimately reduce hospital admissions.

• The primary aim was to reduce medication errors for patients at risk of harm in a single GP surgery over 4 months by performing structured medication reviews.

• The secondary aim was to provide recommendations for safe drug prescribing and monitoring.
• A computer programmed search (SystemOne) was conducted on the electronic patient notes to identify patients at risk of harm.
• The definition of ‘patients at risk of harm’ was set out by Arden's (3) .
• A total of 107 patients were included.
• Patients receiving end of life care were excluded from the search.
• Data was collected over a 4 month period.
• PDSA methodology was used.



• Understand scope of issue.
• Aims and interventions discussed.
• Initial computer search run to identify patients at risk of harm due to medication errors.
•
Patients defined as at risk of harm due to medication errors:

• ≥ 65: NSAID and no gastroprotective.
• ≥ 18: history of peptic ulceration and NSAID.
• ≥ 18: history of peptic ulceration and anti-platelet.
• ≥ 18: anticoagulant and NSAID within 28 days of each other.
• ≥ 18: anticoagulant and anti-platelet within 28 days of each other.
• ≥ 18: aspirin and another type of anti-platelet within 28 days of each other.
• ≥ 18: history of unresolved heart failure diagnosis and NSAID.
• ≥ 18: eGFR of less than 45ml per minute and NSAID .
• ≥ 18: unresolved asthma diagnosis and non-selective beta-blocker.
Data analysed using the following parameters:
• Number of medication errors
• Specific medication error
•
•
SMR complete > Computer Search Re-run = 80% reduction in patients at risk of harm due to medication errors within a single GP surgery over 4 months.
Recommendations:
• Medication reviews should be performed early.
• Annual review of bloods should be performed in patients at risk of harm.
• Caution should be taken when prescribing an aspirin and anti-platelet together.
• Risk assessments should be performed to determine whether gastroprotection is required.
• Specialist input, patient history and patient choice play a crucial role in determining medication regimes.
• Date of medication error
• Date rectified
• Intervention
Computer search re-run:
• 80% reduction in patients at risk of harm due to medication errors.
• Recommendations made to the practice healthcare and prescribing teams.
• Plan for further PDSA cycles.
Structured Medication Reviews revealed:
• 17% of patients defined as at risk of harm had more than one medication error.
• The most common specific medication error was those who were prescribed both an aspirin and another type of anti-platelet within 28 days of each other.
• The most common intervention following the SMR was no intervention (Figure 1.).
• The reasons for no intervention are shown in figure 2.
• A comprehensive structured medication review by healthcare professionals can reduce the number of patients at risk of harm due to medication errors.
• The specific type of intervention should be tailored to each patient depending on patient choice, clinical history and also specialist medical input.
• Structured medication reviews are a sustainable, quick and effective method within the GP setting to reduce adverse side effects, enhance patient safety and improve clinical outcomes


Since introducing electronic notes to Stroke Rehabilitation Unit (SRU), neurological examinations on admissions have been poorly documented and inconsistent. Documenting a good quality neurological examination is useful for rehabilitation as it allows monitoring of function recovery. It is also crucial for patient safety to differentiate new and old symptoms in case of deterioration like further stroke events. The main issues as of January 2023 was admission documentation rarely contained all components of the neurological examination (power, sensation, tone, reflexes, coordination, cranial nerves). Additionally muscle power was not routinely quantified using the gold-standard MRC scale of power1 to assess individual muscle groups. Finally there was an overall lack of consistency between clinicians despite National Clinical Guidance for Stroke2 stating the need for “common, agreed terminology and set of data collection measures, assessments and documentation”

• Introduce an online clerking proforma with a particular focus on neurological examination. It should help clinicians perform a structured and standardised neuro exam and upload detailed documentation of it on electronic patient records. This proforma should be comprehensive and accessible and needs to be completed within 24h of admission to SRU
• Spread awareness regarding the importance of including as many components as possible of a full neurological examination, and encourage the documentation of MRC scale of power grading to quantify power in individual muscle groups. A standard for power documentation was set: power should be documented when using the proforma, using the MRC scale for at least 3 separate muscle groups per limb
The proforma was designed based on the previously-used paper proforma for admission clerking. It was then printed off and trialled by a clinician for an admission. Gaps in knowledge and poor confidence in neurological examination appeared to be a barrier to filling out the proforma correctly. Over the next 2 weeks, 4 clinicians admitted 7 patients using the proforma. Each clinician was contacted to feedback on their user experience, further improving the content and wording. The proforma was then added to the electronic records system. This was paired with neurological examination teaching for all clinical staff to improve skills, knowledge and confidence in using the proforma. Two sessions were offered, on cranial nerves and limb exam. These were interactive, practical teaching sessions repeated weekly.
References 1) Compston A. By Michael O'Brien for the Guarantors of Brain. Saunders Elsevier; 2010. Aids to the investigation of peripheral nerve

The biggest success of the interventions is the outstanding levels of compliance with the proforma (Figure 3). A contributing factors of this success was likely the regular departmental meetings as well as using the teaching sessions to reiterate the importance of using the proforma. The SRU clinical team is relatively small which made it easier to reach out to staff and address personal concerns. The teaching sessions were well received. They were repeated weekly to boost attendance, and 80% of targeted staff attended these sessions. While the “confidence scores” suggest a positive outcome (Figure 4), this is quite subjective. The positive impact may be more meaningfully assessed on re-evaluation in October 2023. Results from February-April 2023 suggest a positive effect on documenting muscle power (Figure 1), but the effect on including all key parts of the neurological examination are minimal or unclear as of yet (Figure 2). This study looks at clerking documentation rather than assessment quality, and addressing knowledge gaps is as important as convincing staff to document their findings. Time constraints might encourage a focus on positive findings. Further work could stress the importance of documenting each neurological examination component and reinforce skills required for ‘difficult’ components like reflexes or cranial nerves.



Regular weight measurements are a simple cost-effective intervention that can improve patient care and management.
We designed a QIP to review local adherence to national and international weight measurement guidelines and develop strategies to overcome barriers to regular patient weighing.
1. Assess the frequency of weight measurements in an inpatient acute ward

2. Develop strategies to improve frequency of weight measurements.
PDSA methodology was followed and eligible patients who met criteria for at least once weekly weight measurements (as per guidance from European Society of cardiology1, British society of Gastroenterology decompensated care bundle2, and NICE nutritional support for adults3) were included. The study was conducted over 7 months period and intervention was done in the form of educational focus groups and poster on the ward.












• Are inpatients having weight measured?
• Retrospective study of all patients over 30 days period.
• How often were weight measurements done compared to guidance?
• Targeted teaching to medical and nursing teams
• Check if intervention had any difference
• Retrospective review of newly admitted patients over 45 days
• Compare data from PDSA1 and PDSA2 cycle.
• Focus on improving frequency of weight measurement.
Eligible patients that had at least one weight measurement improved from 17/21(81%) in PDSA cycle 1 to 33/35 (94%) in PDSA cycle 2. However, the frequency of weight measurements was suboptimal. Mean weight measurements across both cycles were once weekly. Despite national guidance, only 5/17 (29%) in PDSA cycle 1 and 5/33 (15%) in PDSA cycle 2 had the appropriate frequency of weight measurements per week.
- We were successfully able to improve the likelihood of a patient having weight measurements done in their inpatient stay.
- Collaborative work between medical, nursing and allied health professionals was integral to our success.

- In future PDSA cycles, we will aim to increase the frequency of weight measurements through bedside charts and improved accessibility to patient weighing scales.


Delay of medications is recognised to be the leading cause of medication related mortality
In particular, delay of time critical medications such as antibiotics, anti-epileptics and hypoglycaemic agents have the propensity to delay recovery, increase hospital stay and lead to loss of symptom control
Each PDSA cycle showed an improvement, with cycle 1,2,3 showing 38%, 57% and 68% of patients were prescribed medications on time respectively.
Anti-epileptics
Anticoagulants
Antimicrobials
Antipsychotics
Insulin and other hypoglycaemic medications
Parkinson’s medication
Corticosteroids
Immunosuppressant medications*
1. Investigate the causes of delay of TCM at the time of medical admission.

2. 95% of all patients should have their TCM prescribed in a time-sensitive (less than 2 hour from time due) manner in the first 24 hours.
We investigated delay of TCM in the first 24 hours of admission Admission was defined by the point at which patient was clerked by the medical team. Delay was defined by a delay of > 2 hours
Data was collected on:
• Time of medical clerking
• Time of TCM prescription (either on paper chart or EPMA)
• Medicines reconciliation list of medication and including dose and time which it is due
• Time of transfer to the ward from ED
INTERVENTION 1: Poster
INTERVENTION 2: Acute medical team teaching
INTERVENTION 3: Medical induction
The project highlighted key systemic issues that led to delays:
• Lack of access to GP records to check regular medication
• Differing prescribing systems in ED vs the wards

• Admin systems creating delay in admission of patient onto electronic prescribing system
Optimising digital systems can help reduce harm caused by medication delay However, education can help bridge the gap to some degree prior to larger systemic problems are addressed
Suggestions for future work:
• Incorporate TCM prompts in medical clerking proforma
• Access to NHS spine for all doctors to get accurate lists of patient’s medications
• Reduce delays in online prescribing by enabling medical staff to admit patients to wards/AAU
The project highlighted key systemic issues that led to delays: • Lack of access to GP records to check regular medication • Differing prescribing systems in ED vs the wards • Admin systems creating delay in admission of patient onto electronic prescribing system

Drug level monitoring is the sampling of patient blood at specific times in order to measure certain drug levels to ensure drug dosing is therapeutic and not toxic The use of drugs requiring monitoring is increased in the intensive care setting, owing to the higher acuity of patient and the drugs required to treat them. The most common group of drugs which require monitoring is antimicrobials, which are used at ten times the rate of other wards (Dulhunty et al, 2011).
Inaccurate drug level monitoring was identified by the Intensive Care Unit (ICU) Multidisciplinary Team (MDT) at Hillingdon Hospital as being a patient safety issue, alongside having many other negative consequences (see figure, right) The main issue was the timing of drug level samples, requested by the medics and performed by the nursing staff
To improve the proportion of drug levels that are taken at the correct time in Hillingdon Hospital ICU.
Incorrectly timed drug levels Incorrectly adjusted doses Negative consequences
- Toxic drug levels
- Increased drug interactions
- Increased adverse effects
- Treatment failure through subtherapeutic dosing
- Wasted time
- Wasted resources
- Environmental cost

- Drug-specific issues
i.e. antimicrobial resistance due to subtherapeutic levels
A list of the most commonly monitored ICU drugs was established within the ICU MDT Two plan-do-study-act (PDSA) cycles were then undertaken between January 2022 and July 2022 – the first establishing a baseline proportion of drug levels which were taken at the correct time; and the second delivering an intervention aimed at improving this proportion
- Educational poster for ICU staff, distributed to each bed space Poster detailed timing of drug level, target levels, and when to give the drug after the level This was created in collaboration with the nursing staff, ICU lead pharmacist, and ICU lead consultant.
- Email distributed to nursing staff to inform them of the scale of the problem and explain the plan
- Discussion with nursing staff and junior medical staff to increase awareness of the educational poster.
Within PDSA cycle 1, between 31st Jan 2022 -10th Feb 2022, 20 drug levels were taken from 7 different patients. 2/20 (10%) were taken within the pre-established correct times.
Following the interventions in PDSA cycle 2, between 26th May 2022 – 4th July 2022, 26 drug levels were taken from 10 different patients. 21/26 (80.8%) were taken within the correct time period.
A clear improvement was demonstrated in the sampling of drug levels within the correct times following the introduction of the educational poster and promotion of the poster via email and discussion within the ICU MDT. This likely will have reduced risk to patients of having their drug dose altered incorrectly, exposing them to subtherapeutic or toxic drug levels. It would have also reduced the number of wasted drug level samples thus saving money, time, and reducing waste.
Limitations of the study included lack of assessment of whether patients’ drug doses were altered secondary to incorrectly timed samples and furthermore, whether the patient’s next drug level was outside of the therapeutic range. The sample sizes of the data were relatively small and the data collection periods also differed in length – the initial data collection period was cut short in view of the obvious need for improvement.
- Re-assessment of improvement at 12 months to see if the improvement has been sustained. The development of regular formal teaching for ICU staff regarding drug level monitoring could potentially help sustain the improvement.
- Nursing staff frequently mentioned that they were unsure whether they had to wait to give drug following drug level sampling. This could be assessed as drug administration delays would also impact on therapeutic levels.
An accurate and thorough examination is essential in confidently making neurological diagnoses. Too often the equipment required to complete an examination is not readily available and time is lost tracking down the required pieces, or an abridged examination is performed.
- To identify if staff have difficulties in finding appropriate equipment for neurological examination
- To establish funding for a novel mobile neurostand with all routinely used examination equipment available

- To liaise with medical engineering to create a reproducible stand suitable for ward environments
- To implement the neurostand on neuroscience wards with opportunity to create further iterations
- We performed an experiment to identify how much routine examination equipment could be found on 6 inpatient wards (Neurology, Stroke, 2 Neurosurgery and 2 AMU wards), Figure 1

- Clinicians were surveyed on ease of access to examination equipment, Figure 2, 3
After review of the data, a funding request was made for a bespoke mobile stand to act as a central location for all equipment
- The required equipment for a stand was identified and ordered through procurement
- Together with medical engineering, a prototype stand was made, Image 1
- A survey was sent to gather feedback on the neurostand, Figure 4
Sharps bin Tongue depressors 3m Snellen chart
Pen torches Antiseptic wipes Alcohol gel
Image 1
Multiple stakeholders had input into the creation of this stand, and will contribute towards addressing future issues such as:
- Making the stand easy to clean effectively
Summary
Stakeholders
Clinicians Medical engineering Procurement Infection control
- Choosing equipment which is durable and appropriate
- Ensuring ease of procuring parts for future stands
- Appreciating individual ward differences in location/design of stand
- Continual maintenance and replenishing of consumable items
- We have created a bespoke solution for a clinical issue on our neuroscience wards
- There is opportunity to create more stands and further refine the work







