
12 minute read
Chronic pain


Clients Who Don’t Get Better The Complex Conundrum of Chronic Pain
Persistent central sensitisation is a feature of many chronic conditions such as low back pain
Advertisement
Being a massage therapist is not always an easy business. Massage therapists, more than any other manual therapy profession, are constantly faced with the issue of chronic pain- that is, pain that persists long beyond the usual healing time for an injury. We are often the last point of call for clients who have run the usual gamut of the medical equivalent of the butcher, the baker and the candlestick maker (GP, NHS physio, chiropractor, osteopath). Those clients eventually turn to massage, way down the line, often after months or years of dealing with constant daily pain.
T
hose of you who are regular readers of my articles will know that there are many great soft tissue techniques that have proven effective in reducing chronic musculo-skeletal pain. The bread and butter techniques of an advanced clinical massage therapist are a creative combination of fascial work, precise trigger point therapy, acupressure and stretching. Using an amalgamation of these techniques within a treatment can often get a reduction of pain quickly and easily with common conditions such as back pain, rotator cuff issues, headaches, sporting injuries and RSI.
As a rule of thumb (what other rules could we possibly have as manual therapists!) we look at treating the condition once a week for up to 6 weeks with an expectation that we will be achieving a substantial reduction in pain by week 3. Without a doubt this works for most of the people most of the time.
Sounds great right?
Yet sometimes people just don’t get better. Clients with exactly the same condition, treated in exactly the same way, can have entirely different outcomes.
Why? Frustrating yet fascinating, this riddle turns us back to the drawing board to understand what could possibly be going on in the complex mystery of pain that just doesn’t go away.
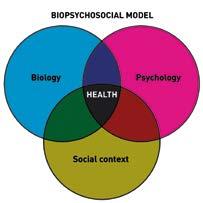
Fig. 1: The biopsychosocial model of pain posits that chronic pain is influenced heavily by both psychoclogical and social factors
The issue is not always in the tissues
Consider these 2 cases that I treated a few years ago:
Anna: Aged 25, developed pain in her right forearm. Working as a marine biologist she was fit and healthy, her job involved a great deal of physical activity and she had no significant emotional stresses. She presented as cheerful and positive about my ability to help her pain.
Martha: Aged 60, developed a similar pain in her right forearm. She was tearful and stressed. Her office job was really getting too much and she felt overwhelmed by the day to day demands. She would love to retire but was worried about the financial implications.
Who do you think got better first? Yes of course you’re right – Anna was pain free within a miraculous single treatment (wish all my clients were like that!) whereas Martha (treated with the same techniques) was still in pain several sessions later. She subsequently made the decision to retire and is finally living an idyllic pain free life!
Herein lies the dilemma of the working massage therapist – the “issue is not always in the tissues!” People are unique individuals and their own complex psychological make up, attitudes and personal history can affect the outcome of our treatments considerably. Our ability to help people out of pain is influenced by a complex array of factors including: • Current emotional state of the client • Age • Past history of issues such as anxiety, depression or experience of trauma • Client’s belief in your ability to help their pain • Attitudes to health – does the client see themselves as generally well or healthy • Beliefs about the current pain issue and its consequences– does the client believe this is a condition that will affect them for long term? Or do they see it as a short term, easily resolvable issue? • Their sense of control over the pain condition – do they feel helpless and at the mercy of experts or do they believe they can make a difference themselves
Interestingly, even sociological factors can also play a part in our experience of pain. For example, one study of those suffering from long- term whiplash pain discovered that poor recovery was associated with factors such as: • Being female • Larger number of dependents, • Married status, • Not being employed full time, low income • Low education • Lawyer involvement!
Clearly working with pain conditions is not a straightforward issue. Pain is not just about whether there are injuries or restrictions within the soft tissue and joint structures of the body but is highly coloured by our attitudes, beliefs and expectations.
This model of pain is known as the “biopsychosocial model” (FIG 1). In the biopsychosocial model the experience of pain is believed to be a combination of biological, psychological and social factors. Understanding the biopsychosocial model is vital for massage therapists – pain is NOT just due to structural factors such as misaligned vertebrae, tipped pelvises or differentials in leg length but is much more complex.
The issues in the tissues versus the pain in the brain
So if the pain condition is not always coming from damage to the tissues, what exactly is going on? In his likable and readable books and talks on pain biology, neuroscientist Lorrimer Moseley (Google him- he’s great!) summarises prevalent research that shows how chronic pain is a perception of the brain rather than always being an accurate representation of what is happening at the tissue level. Thus, the sensation of pain can be mediated by a variety of factors including emotional state, previous experience, expectations and sense of control over the pain condition.
This phenomenon is known as sensitisation. This is a neurological process by which the central nervous system can “change, distort or amplify the experience of pain”. In other words the brain can act like a faulty stereo speaker that at whim can turn up the volume of the pain or significantly change the sensation. (FIG 2) Under normal circumstances, for example after injury, sensitisation is a good thing, causing the injured area to feel hypersensitive to touch or movement thus protecting the tissues from further damage. Usually this pain and sensitisation will diminish as the person heals and the pain response will return to normal levels.
Fig. 2: The brain can act almost like a faulty stereo speaker that can “turn up” or “turn down” the volume of pain sensations
However for some people, persistent central sensitisation can be maintained long after tissue healing has taken place. In other words the client is in (real) pain even though there is no longer any injury or damage. This persistent pain sensitisation has been shown to be a feature in many of the client conditions that are staples of the massage therapist’s clinic – for example chronic low back pain, TMJ, headaches and long term neck pain (main image). It seems that some of the factors mentioned above (previous experience, attitudes to health, emotional state etc) can have a significant influence on whether the client develops this persistent pain sensitisation response.
Understanding the role of the central nervous system in persistent pain sensitisation is very different from dismissing pain as being “in the head” or “psychosomatic”. These kind of beliefs are unhelpful to the client and will not solve the problem. The pain is very real and not imaginary, it’s just that the CNS has amplified the normal signals.
Pain sensitisation is the reason why, in my 2 clients above, Anna was so much easier to treat than Martha. For Anna, the issues were very much in the tissues, meaning a speedy recovery following treatment. However for Martha, her feelings around her job, current anxiety and lack of sense of control contributed to a persistent pain sensitisation response. Good bodywork alone was not the answer – effective treatment needed to also factor in the effect of the “pain in the brain”.
The treatment sandwich approach – intervening in psychology rather than physiology
So as bodywork therapists how are we expected to deal with these amplifying and distorting effects of the central nervous system? Surely we deal with bodies not the mind? Right?
Wrong. Every time you interact with a client you are interrelating with their personal psychology and belief system. Whether you realise it or not your attitudes will have a direct effect on whether the person gets better.
Significantly, your client’s healing process depends not just on the hands- on techniques used but also the quality and content of the practitioner- client interaction. (FIG 3)
As a massage therapist you have 2 significant opportunities to interact and connect verbally with your client – the first is during the client consultation at the beginning of the treatment; the second is at the end where feedback and self -care suggestions can be given. I call this the “treatment sandwich” – manual techniques are
Fig. 3: Your client’s healing process depends not just on the hands-on techniques used but also the quality and content of the practitionerclient interaction. slotted in between the beginnings and endings of slices of verbal clienttherapist interaction.
The importance of these verbal components in enhancing client recovery from pain conditions cannot be over-emphasised. The consultation aspect of the treatment enables the practitioner to assess the role of potential perpetuating and aggravating factors in the client’s pain condition, provide support and reassurance, and where appropriate reflect information back to the client to assist them to make informed choices.
Similarly, the self -care suggestions form an important part of the healing process as they are handing responsibility back to the client to take control of their health. As a mental health professional for many years I was well aware of the crucial concept of “empowerment “ in recovery and working with many pain conditions is no exception. Helping the client to feel that there is something they can do for themselves to decrease their pain is often the key to recovery.

Practical suggestions for client self care and education
Although the issue of chronic pain is complex there are some simple ways that you can help your client without taking on the role of counselor:
• Emotion: Research has shown that increasing psychological well -being causes an associated decrease in pain. It is definitely a skill to be able to identify within your consultation if psychological factors may be a significant contributor to the pain condition, without making the time into a counseling session! Questions such as “Was there anything else going on for you when the pain started” can be very revealing as can asking the client to rate their current stress levels on a scale of 1-10. Be prepared to probe a little without being intrusive; always remain open minded and non judgmental.
Fig. 4a & 4b: Movement is an effective way of decreasing chronic pain. Encourage your clients to engage in activities they enjoy – dancing is just as good as yoga! If you feel psychological factors may be playing a part, your recommendations may vary from suggesting talk therapy (CBT is particularly helpful for chronic pain) to suggesting the client might need to take more time for themselves or call their friends more.

• Physical Activity: Movement is good! And most of us don’t do enough of it. Activities such as walking can not only increase well- being but have also been shown to decrease chronic low back pain. Encourage your clients to return to the activities they enjoy or to walk to work rather than driving. (FIG 4A and 4B)
Using Pacing and gradual exposure
One of the challenges around recovery for clients in pain is determining how to advise them on exercise, movement and the challenge of returning to both necessary and enjoyable activities. All too often clients in pain fall into some level of inactivity due to their pain levels.
Clients’ attitudes often fall into the categories of “boom and bust” (push through the pain then drop with exhaustion) or “avoidant” (avoiding potentially painful activities altogether).
A more sensible approach involves gradually increasing the level of the activity in question. Movement is important in recovery from chronic pain and it is important your client is encouraged to gradually return to the activities they enjoy. 1. Decide with your client which activities they want or need to work on (cycling, walking, tennis, playing with kids, dancing) 2. Determine their baseline - this is the amount of activity the client can do without pain flaring up. (Might only be 3 minutes cycling
on a flat surface but thats a good start) 3. Encourage a planned progression of the chosen activity - the client does a little more than they did yesterday but not much more (i.e.: 4 minutes cycling the next day) 4. If the pain flares up return to the previous baseline for a while
• Catastrophising: The client’s experience of pain can be dramatically influenced by their anxieties and beliefs about their condition – this tendency is known in psychology as catastrophising (FIG 5). Unfortunately the medical profession sometimes doesn’t help with this tendency – a friend of mine who went to the GP with a simple back pain was referred to the disabled hydrotherapy group! She was convinced she was going to be in pain for the rest of her life whereas in actuality the pain was likely to be a simple soft tissue injury. Explaining to your clients about the concept of pain sensitisation helps them to understand that there may be other reasons for their pain other than tissue or structural damage. This in itself can be profoundly empowering and help them to make the necessary lifestyle changes to make a difference.
Fig. 5: The client’s experience of pain can be dramatically influenced by their anxieties and beliefs about their condition. This tendency is known in psychology as catastrophising
RACHEL FAIRWEATHER
Rachel is author of the best selling book for passionate massage therapists – ‘Massage Fusion: The Jing Method for the treatment of chronic pain”. She is also the dynamic co-founder and Director of Jing Advanced Massage Training (www.jingmassage.com), a company providing degree level, hands-on and online training for all who are passionate about massage. Come and take part in one of our fun and informative short CPD courses to check out the Jing vibe for yourself!
Rachel has over 25 years experience in the industry working as an advanced therapist and trainer, first in New York and now throughout the UK. Due to her extensive experience, undeniable passion and intense dedication, Rachel is a sought after international guest lecturer, writes regularly for professional trade magazines, and has twice received awards for outstanding achievement in her field. Rachel holds a degree in Psychology, a Postgraduate Diploma in Social Work, an AOS in Massage Therapy and is a New York licensed massage therapist.








