
33 minute read
Soft Tissue Release


Soft Tissue Release Trunk & Neck - part one
BY MARY SANDERSON
Advertisement
Extract from Soft Tissue Release - A Practical Handbook for Physical Therapists
Figure 1. The spine (lateral view).
The Spine
The spine (fig. 1) consists of 33 individual vertebrae: seven cervical, twelve thoracic, five lumbar, five sacral (fused) and four coccygeal (fused). Although only small movements occur between the vertebrae, the combined action of all of them facilitates good overall spinal mobility. Between the vertebrae are cartilaginous discs, which make up approximately onethird of the total height of the spine. The vertebral column is maintained in its upright posture by strong ligaments and muscles; it has three natural curves (four if the sacral curve is included), which together with the intervertebral discs are responsible for absorbing shock. Flexible, strong muscles will enhance the fluid content of the discs and allow efficient maintenance of the spinal curvature.
Most people will suffer backache at some point in their lives, although maintenance of correct posture can reduce the likelihood of injury problems. Good spinal posture places minimal strain on the muscles that maintain the body’s stance. If the body sways from its neutral position, the movement is counteracted by muscles which contract eccentrically. If an inefficient posture is continued, then adaptive responses lead to poor health of the muscles, muscle imbalance and dysfunction in the form of reduced muscle strength, loss of spinal mobility, nerve root irritation and pain generally.
Postural adaptation often develops over many years, and someone may not be aware of a problem until the tension and imbalance give rise to a traumatic injury, such as a prolapsed disc.
The position of the pelvis is affected by the abdominal muscles and spinal extensors as well as the hip flexors and extensors. An increase in the lumbar lordotic curve will result in tight hip flexors and back extensors, weak abdominal muscles and a tendency to compensatory thoracic kyphosis. The side flexors need to be evaluated with regard to lateral imbalance. Massage therapists must be systematic in treating the hips and antagonists with any presentation of back pain.
There are many different types of stress placed on posture, and the therapist needs to be aware if the subject suffers from any of these. There may be a structural problem, such as a leg length discrepancy. Occupational factors, for example driving for long hours or sitting behind a keyboard, may be involved. If sports are the cause, the problem could be repetitiveness, such as in long-distance cycling, or
Figure 2. Deep back muscles.
an overload of one side of the body, such as in golf or tennis. The root of the problem needs to be addressed and altered if possible. Maintenance massage of the back area is invaluable.
Correct posture is still not well understood by the general public so, following treatment, postural awareness should be discussed along with mobility, stretching and strengthening exercises.
When someone presents with any neurological deficit or acute symptoms, input from a medical practitioner is essential, and STR may not initially be appropriate where protective spasm and severe inflammation are present. Traumatic injuries sustained from heavy lifting or falling, and sciatic, disc and degenerative conditions, will benefit from having the soft tissues strong, supple and in balance; the timing of the introduction of STR should be carefully considered for maximum benefit. STR can help improve movement patterns and relieve nerve root irritation.
Spine Extension Major Muscles: Erector spinae (iliocostalis, longissimus, spinalis), quadratus lumborum, interspinales, multifidus, semispinalis and gluteus maximus (from a flexed position). The contraction of all three muscles on both sides of the erector spinae is the main contributor to extension of the back. The iliocostalis (lateral layer) has attachments that run the length of the spine. The longissimus (middle layer) and the spinalis (medial layer) attach to the skull and to the cervical and thoracic vertebrae. There are many complex muscle contractions that always occur, as the erector spinae also controls flexion of the spine and stabilises the non-weightbearing side, to prevent the pelvis from dropping, during side flexion. The erector spinae is also critical in maintaining the secondary curve.
The transversospinalis muscles are found deep to the erector spinae; in order, starting with the most superficial, these are the
MUSCLE
Thoracic
Spinalis Postural deviations of upper torso, particularly lateral flexion and minor posterior rotation. Restricted upper body movement, especially flexion and contralateral rotation at segmental levels. Scoliosis.
Longissimus thoracis Stiff thoracic region and reduced flexion in thoracic spine. Could contribute to overall reduction in lumbo-pelvic rhythm, with link to lumbar longissimus.
External intercostals Increased difficulty with inspiration and decreased ‘bucket handle’ rib motion.
EFFECTS OF MUSCLE RESTRICTIONS
Lumbar
Iliocostalis lumborum Increased lumbar lordosis when in neutral stance, with reduced contralateral side bending.
Longissimus thoracis Could impact on lumbo-pelvic rhythm and reduce ease of lumbar flexion.
Thoraco-lumbar
Multifidus Localised decreased contralateral lumbar side flexion and rotation. Reduction in lumbo-pelvic rhythm.
Quadratus lumborum Increased ipsilateral flexion in neutral position. Reduction in lumbo-pelvic rhythm. Changes in gait. Perception of short leg on tight side with supine leg-length assessment.
Internal obliques Limitations on contralateral posterior torso rotation and side flexion.
External obliques Reduction in ipsilateral posterior torso rotation.
Rectus abdominis Increased thoraco-lumbar flexion. Concomitant reduction in ease of inspiration and thoraco-lumbar extension.
Other
Latissimus dorsi Increased kyphotic posture.
Figure 3. Active STR to the erector spinae as the pelvis is posteriorly tilted. Figure 4. Active STR to the quadratus lumborum Figure 5. Active STR to the erector spinae in the thoracic region – a lock is attained and the subject arches their back.
semispinalis, multifidus, rotatores and interspinales. The deepest muscles cross only one or two vertebrae.
Spine Side Flexion Major Muscles: Quadratus lumborum, erector spinae, intertransversarii, obliques, rectus abdominis and multifidus. Side flexion is produced by the muscles on the side being flexed. When standing on one leg, the quadratus lumborum acts strongly on the non-weightbearing side to stop the pelvis from dropping. It also stabilises the twelfth rib during forced expiration, by fixing the origin of the diaphragm. When the quadratus lumborum muscles on both sides contract, they are responsible for lumbar spine extension and stability.
Spine Rotation Major Muscles: Obliques, multifidus, rotatores and semispinalis. During rotation to one side, contraction of the external oblique on the opposing side and contraction of the internal oblique on the same side occurs. The external oblique is the most superficial side muscle. Its upper origins on the anterior ribs interdigitate with serratus anterior and the lower origins with latissimus dorsi. The internal oblique lies below the external oblique and runs diagonally in the opposite direction above the transversus abdominis.
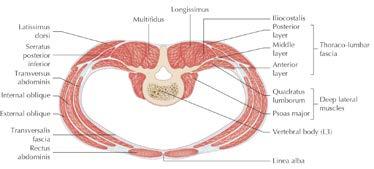
Fascia of the Trunk
The trunk, like the rest of the body, is covered with superficial and deep fascia. The deep fascia of the neck area is thick and strong, enveloping the muscles, and supports and connects the trunk to the muscles of the shoulder girdle and upper limb. There is a specialised deep layer of fascia in the lower back known as the thoraco-lumbar fascia. It consists of three layers located in the lower thoracic, the lumbar and the sacral regions. The posterior layer is superficial to the erector spinae, and the latissimus dorsi partially arises from it. The middle layer is situated between the erector spinae and the quadratus lumborum. The anterior and thinnest of the layers is located in front of the quadratus lumborum. All three layers converge at the lateral border of the erector spinae. This then extends to form an origin for the transversus abdominis and internal oblique.
MFR locks are very beneficial in ensuring that the muscle regains full separation. As many of the lower back muscles in particular are very strong, the quality of the lock is crucial for any release to occur.
The deep fascia of the abdomen is thin and elastic to allow expansion of the chest and abdomen. The lower abdomen is covered by the aponeurosis of the external oblique which merges at the linea alba with the external oblique of the other side.
Spine Extensors, Side Flexors and Rotators – Treatment With the subject in a side-lying position, make a secure reinforced lock just above the sacroiliac joint close to the spine; advise the subject how to perform a posterior tilt of the pelvis (fig. 3). The pressure should be directed slightly towards the head. The pelvic tilt provides a small stretch but the movement is controlled and precise.
Although trunk flexion can be used, the movement may prove too severe for a lock to be maintained. Apply locks and move up the whole of the lumbar area, then return and treat more laterally to the initial locks. Treat around the sacroiliac joint with two or three MFR locks and either a pelvic tilt or flexion of the spine or hip.
For the quadratus lumborum, use one thumb reinforced with the other (see fig. 4); take the depth of the erector spinae and drop in on the lateral border of the muscle, in between the rib cage and the pelvis. Maintain this pressure while the subject extends and adducts the hip and abducts the arm.
Treatment of the erector spinae can continue until you reach an area not affected by the stretch from the pelvic movement. This procedure is usually only beneficial around the lumbar area. For release in the erector spinae further up the back, it will be necessary to lock as the subject flexes the trunk; instruct the subject to arch the back or to push backwards into the lock (figs. 5 & 6).
The direction of pressure in this case should be towards the base of the trunk.
On occasion, weight-bearing STR may prove to be a useful technique. STR can be performed with the subject
Figure 6. Active STR to the erector spinae using an elbow. as the pelvis is posteriorly tilted.
Figure 7. STR to the erector spinae in a weightbearing position.as the pelvis is posteriorly tilted.
Figure 8. STR to the erector spinae as the subject arches into the ‘angry cat’ stretch.
Figure 9. STR to the erector spinae in seated. Figure 10. STR to the QL in seated.
standing and holding onto a wall or the couch for support or on all fours (fig. 7); apply an MFR lock and instruct the subject to flex or side flex the spine. Another useful position is with the subject on all fours; lock in on either side of the spine as the subject arches into the ‘angry cat’ stretch (fig. 8), and release the lock as the subject returns to neutral.
Seated STR also works well, even on the larger individual. Because the muscles are under tension it is advised to treat the top layer of the thoraco-lumbar fascia, rather than trying to delve into the extensors. Apply an MFR lock while securing the subject across the front of the hips, and instruct the subject to side flex or flex the spine (fig. 9); severe muscle shortening can be relieved because of the fascial release. By having the subject’s arm raised on the side being treated, the stretch on the latissimus dorsi may enhance the STR effect.
Also, with the subject seated, the quadratus lumborum can be targeted and the subject can side flex (see fig. 10).
For the thoracic region, working with rotation can prove to be valuable in restoring correct movement patterns. Use your elbow to gently engage the semispinalis thoracis, once the superficial shoulder girdle muscles have been released, and instruct the subject to rotate the spine to the same side for a stretch. Also, lock deep into the laminar groove to address the multifidus muscles; instruct the subject to rotate to the same side for a stretch.
Spine Flexion Major Muscles: Rectus abdominis, obliques, and psoas major/minor (when the insertions are fixed). Flexion occurs during concentric contraction of the muscles on both sides of the spine. The flexors also affect the position of the pelvis by modifying its tilt and subsequently the curvature of the lumbar spine. Attachments of the abdominal muscles to the pelvis, at the symphysis pubis, and muscles within the abdominal wall are all occasionally torn, with consequent fascial adherence.
Thickening of the fascia can occur with poor posture, leading to further postural imbalance and weakness. If the spine flexor muscles are weak, the pelvis drops, the hip flexors and spine extensors become hypertonic in relation to the spine flexors, and the lumbar curve tends towards lordosis.
Figure 11. Abdominal muscles.

Correct, isolated strengthening of the abdominal muscles is necessary to regain lost strength.
Spine Flexors and Rotators – Treatment With the subject in a supine position, treat the rectus abdominis: start from the origin on the pubis with an MFR lock, then instruct the subject to perform a very minimal side flexion. Progress to the outer borders of the muscle on one side, hooking under it while the subject side flexes. Angle the lock carefully near to the insertions to avoid bruising from the bone.
See the section on hip flexors for treatment of the psoas (page 44). The obliques may be treated in a similar fashion, by applying pressure as the subject side flexes. Alternatively, use a side-lying position, in which a trunk rotation can be used to provide adequate stretch for a release. Locks must be applied away from the movement, and pressure should be angled to produce a shallow MFR lock.
Treatment in a seated position is an excellent way to add in a greater range of movement when addressing the rectus abdominis or the oblique muscles. Use broad surface locks, such as the whole hand (fig. 13) or a soft fist (fig. 14), and instruct the subject to side flex to the opposite side. For release of the internal oblique muscle, lock and rotate to the opposite side for a stretch; for release of the external oblique, lock and rotate to the same side.
Compression of the Abdomen Major Muscles: Transversus abdominis, obliques and rectus abdominis. These muscles increase abdominal pressure and provide a muscular support for the pelvis, abdomen and viscera.
Respiration: Inspiration Major Muscles: Diaphragm, external intercostals, levatores costarum, serratus posterior and superior, pectoralis minor and SCM.
Respiration: Expiration Major Muscles: Transversus abdominis, subcostales, transversus thoracis, internal intercostals, obliques, latissimus dorsi and quadratus lumborum (fixes ribs).
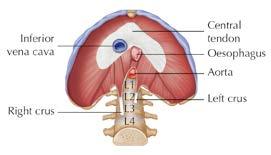
Diaphragm
The diaphragm (fig. 15) is a large sheet of dome-shaped fibrous muscle that separates the thoracic and abdominal cavities. As it contracts it is drawn downwards, and the subsequent change in pressure causes air at atmospheric pressure to enter the lungs. When it relaxes it returns to its initial position and air is expelled from the lungs.
During forced expiration, for example during moderate or heavy exercise, the expiratory muscles become involved in order to drive air out more quickly. Through their contraction, there is an increase in abdominal pressure that pushes the diaphragm up more quickly to expel air faster.
The transversus abdominis (the deepest of the abdominal muscles) is the most powerful expiratory muscle. The internal and external intercostal muscles criss-cross the ribs and are responsible for drawing the ribs together (for expiration) and apart (for inspiration) respectively.
Respiratory Muscles – Treatment
Treatment of the respiratory muscles can be beneficial for anyone. Postural deficiencies can affect respiratory patterns due to the diaphragm’s attachments on the rib cage and lumbar vertebrae, and equally the other way. STR will have a positive effect on asthma sufferers. Athletes will find it can improve their breathing techniques, as the chest adopts a new lightness and freedom.
Ensure that the subject is in a comfortable supine position with the knees and hips flexed. Gently curl your fingers behind and in front of the lower ribs (fig. 16) towards the anterior attachments of the diaphragm while the subject is slowly inhaling; hold

Figure 13. STR to the oblique muscles using the whole hand.

Figure 14 STR to the oblique muscles using a soft fist.
the position and allow inhalation to finish. Still maintaining the pressure, instruct the subject to exhale gently; after exhalation, release the pressure. For the intercostal muscles, a side-lying position is a good way of exposing the ribs. Lock in between the ribs (fig. 17), hold the pressure and instruct the subject to breathe in and to breathe out.The external intercostal muscles are the most superficial and are therefore more directly affected by this technique.

Figure 16. STR to the diaphragm
Originally published in 1998, Soft Tissue Release: A Practical Handbook for Physical Therapists was the first ever book to be written on soft tissue release and its reputation as one of the most highly respected textbooks on the subject is as strong today as it was then. Now in its fourth edition, this latest version contains the most up to date information on the role of fascia and even more comprehensive anatomical imagery to illustrate the theory and techniques involved.

Soft tissue release (STR) is an effective treatment approach designed to be easily integrated by any therapist working with pain, injury and movement dysfunction. Put simply, STR involves a ‘lock and stretch’ of tissue – but how exactly does it work, what is accepted as ‘best practice’ in terms of application, and how can it be used alongside other tools and techniques?
In this highly practical guide, Mary Sanderson shares a comprehensive range of techniques she has found to be the most beneficial during her own successful career as a physical therapist and lecturer. Detailed chapters present the prerequisite theory of how STR works, comprehensive advice on the treatment of over XX individual all of the main muscle groups and specific guidance on how to modify techniques across different settings.
Soft Tissue Release: A Practical Handbook for Physical Therapists is a complete reference guide for students embarking on clinical practice, therapists from all backgrounds wanting to understand more about pain management, or any individual wishing to harness the power of soft tissue release to treat their own pain.
MARY SANDERSON
Mary is a specialist in soft tissue therapy and has been a senior tutor for the London School of Sports Massage (LSSM) since 1994. She has run her own private practice in St Leonards on Sea, East Sussex, for over 25 years, treating a wide range of clients including elite sports people, musicians and performers. Mary also regularly presents on CPD programmes for manual therapists, personal trainers and coaches.

Is It Time to Review What We Say About Fascia & How We Think We Can Treat It?
BY RUTH DUNCAN
All of us were taught about the nervous system in our manual therapy training. But, often anatomy and physiology (A&P) were taught as stand alone systems where their integrated workings were either missed or lost. This, for many of us, resulted in an inadequate understanding of how systems influence each other in health and disease.
A&P helps us to assess risk, identify contraindications, understand pathologies and helps us build client rapport through knowledge. As some qualifications involve treating injuries (and pain), A&P is relevant to providing the best evidence informed practice (EIP), building an appreciation of tissue damage, repair and what we can do to assist recovery to promote a return to pain-free active lifestyle (or sport).
However EIP involves much more than A&P and some may argue that A&P is not even relevant to an EIP. However, EIP prompts us to become more discerning in our professional decisions including how we claim
our therapy works, often called the ‘mechanism of action’. EIP also promotes best practice where all therapists should reflect regularly on what they have been taught, how they practise and review any new evidence, science and guidance. As a result, we replace outdated practice with contemporary evidence continually providing the best care for our clients that we can.
Fascia is often heralded as ‘the missing link in traditional healthcare’ (Barnes 1990). Most fascial commentary begins with describing fascia as being previously thought of as a packing organ and continues with new evidence that supports its greater role and responsibilities in health and disease. There is no doubt that fascia research is amazing and has offered scientific explanations including the potential for fascia to be involved in the metastasis of cancer (Friedl and Alexander 2011), menopause symptoms (Fede et al. 2019), low back pain (Shilder et al. 2014) and myofascial pain syndromes including Fibromyalgia (Pratt 2021) and (Stecco et al. 2011). But, this doesn’t necessarily translate to how we can fix, stretch, release or resolve fascial dysfunction using fascia-oriented manual therapies such as Myofascial Release (MFR). Many studies researching fasciaoriented therapies report evidence of benefit, albeit low, compared to nonintervention such as fascia and headaches (Ajimsha 2011), low back pain (Wu 2021), temporomandibular pain (Kamir 2010), chronic musculoskeletal pain (Laimi 2018) and scar tissue therapy (de Valois 2021). However, many journal papers simply avoid mentioning the potential mechanism of action or state that how the intervention works remains unclear. Additionally, consideration for bias, variability and reliability requires critical evaluation in all journal studies.
For decades, we have discussed fascia as being a matrix which supports, separates and protects everything else. We have described it as the container of the mind and the keeper of trauma. We also have described how we can touch the intricate fascial web, following its spirals, twists and turns that influence its structure and, as a result, we can release the body’s stored physical and emotional traumas. For every Myofascial Therapist reading this, this will be something which you can identify with and appreciate what is being said as they have plausibility appearing to fit with what we believe we feel happening under our hands and what our clients experience. I remember attending the Fascia Research Congress (FRC) in 2009 in Amsterdam, Netherlands where Tom Myers was challenged by a presenter who suggested that deep fascial tension and fascial connections could not be described as trains or lines. Tom’s reply was simply that he knew what he felt under his hands. What we feel, what we interpret and what we intuit comes from experience and does play a part in EIP. However, despite clinical results, experience does not provide reliable scientific evidence but instead provides what is known as anecdotal evidence. Each one of us has our own style, belief and opinion that is reflected in our own treatment approach regardless of our training. While this offers diversity for the ever-increasing assortment of clients’ needs, the result is inconsistency potentially resulting in poor practice standards. Additionally, we can become very protective of our titles, who we trained with and preferred treatment approaches which can be considered as bias that also contradicts an EIP.
Dr Robert Schleip, a prominent fascial researcher, described fascia as the ‘Cinderella of orthopaedic tissues’ (Schleip et al. 2010) as the fascial tissues have finally come to the ball and been noticed by the medical and research community. He also presented a lecture at the 2012 FRC in Vancouver Canada titled ‘Alice in Wonderland: Getting Curiouser and Curiouser’ discussed by the Association of Massage Therapists Ltd in Australia in one of their magazine articles (Schleip 2014). The theme here is not Disney characters, although some critics may be quick to point this out which, in itself would be confirmation bias, but Dr Schleip is indicating that there is still the great unknown regarding fascia and how we may be able to treat it resulting in rabbit hole after rabbit hole.
Furthermore, due to fascia’s ability to morph and adapt to stimuli, statements like ‘fascia is alive’ (Schleip et al. 2022, p265) and comparisons with spiral energy and bird murmurations imply a somewhat mystical and magical quality to it. On one hand, this embraces holism, attracting a personality type who resonates with this style of language and, as such, becomes a meaningful component of their clinical results. Yet, on the other hand, arguably this places fasciaoriented therapies into pseudoscience and often leads to them being criticised by traditional healthcare professionals.
Is it time to take a serious look at current evidence and become more evidence informed, refining our terminology, language and explanations of the properties attributed to fascia?
As an MFR training provider, I have always made it a priority to apprise myself of current research and evidence, integrating it into all of our training programmes

so that our students not only have valuable practical skills but also have a fundamental theoretical framework helping them to evaluate, consider and reflect on treatment approaches.
Now into my 3rd decade of teaching MFR however, there is still the unanswered question of ‘what happens when we touch?’ Anecdotally, I know that MFR makes a difference not just to my clients but to the thousands of clients treated by the wealth of skilled therapists who have trained with me. Despite my experience, science hasn’t yet been able to identify exactly what makes MFR different to any other style of manual therapy (if indeed it is) and why it can have such a profound effect on our clients.
There are many models and hypotheses as to how MFR may mechanically work including piezoelectricity and the semi conductive nature of fascia (Oschman in Schleip at al. 2022 p188), thixotropy (Schleip 2003), viscoelasticity (Yahia 1993) and fluid dynamics (Meert in Schleip et al 2022, p294) and (Bordoni 2018). There are also many models regarding the structure of fascia including biotensegrity, chains, bags and lines. Yet, none of these models offer definitive answers on what we actually do to the fascia, if anything.
However, there is an ever growing body of evidence about touch, sensation and pain. The power of touch has been researched for decades with the most familiar researcher on touch being Tiffany Field from the Miami Touch Institute. Her research generally indicates that touch benefits wellness, reduces stress and improves relaxation and sleep. More recently, a complex interplay of biomechanical and neurophysiological mechanisms have been suggested as an appropriate and worthy concept as a potential mechanism of action for manual therapy including MFR (Bialosky et al. 2009) and (Bialosky et al. 2018). This correlates with the concept discussed by Dr Schleip for almost two decades and is a current and on-going area of fascia research (Schleip 2003). Fascia has been heralded as a sensory organ due to its high mechanosensitivity. According to Dr Helene Langevin ‘connective tissue functions as a bodywide mechanosensitive signaling network’ (Langevin 2005) and as a result, may influence the experience of pain (Langevin 2021) and (Shilder et al. 2014). This is because fascia is embedded with nerve receptors which discriminate pressures and loading as well as tissue chemical and temperature changes. All tissues have this capability, identifying changes to their structures, accommodating and adapting as necessary to maintain balance and harmony (allostasis).
But, how could the sensory nature of fascia help us to understand how we may be able to influence it?
You will have all heard about the 5 senses, taste, sight, hearing, smell and touch. You may have been taught about the integumentary system, that is the skin, hair, nails and exocrine glands. Mostly, you may have been taught about the skin as that’s what we physically touch in all manual therapy. You may have been taught that the skin is a sensory organ because it senses, or discriminates against, different types of touch. A long and light nurturing massage effleurage stroke is determined by different nerve receptors embedded in skin than those which determine cross-fibre friction and, the physiological changes as a result of those different styles of touch can be different too.
Most literature discusses the skin as being the largest sensory organ. However, fascial anatomy research is disputing this as it is now suggested that the fascial system contains approximately 250 million sensory nerve endings (Fede et al. 2022) and (Schleip 2022 p. 157) whereas the skin is said to have only 200 million nerve endings.
Considering this information, it is plausible that touch transmitted via the skin, including MFR, could stimulate millions of nerve endings, sending signals to the brain resulting in physiological changes that also rely on many different factors unique to each individual as suggested in the Bialosky et al. (2018) model. This is quite different to previous suggestions of a more mechanistic approach of tissue change by manipulation that I previously mentioned.
The nervous system is a 2-way street. When impulses are generated from the periphery, outside of the brain and spinal cord, such as in touch from manual therapy, they move along nerves as action potentials (electrical signals) towards the brain. This is called afferent signalling. Hence the term ‘affective touch’ as it has an affect on the body.
When impulses are generated from the brain and spinal cord and move out to the periphery along nerves, they have an effect on the body such as moving a joint. This is called efferent signalling. Simply put, affect is to influence change in the body and effect is a response due to change. If we have this 2-way street of both afferent and efferent processing, it can’t be done by the skin alone.
Every tissue type, organ, bone and vessel are innervated. Even nerves have their own nervous system, called nervi nervorum. This means that all information about your internal and external environment is sent to your brain via nerves. This obviously includes the fascial system and suggests that when the skin and all underlying structures feel pressure from manual therapy, they transmit this information via the nervous system to the brain resulting in a response or action some of which are experienced as feelings. These experienced feelings result in physiological changes involving hormones, neurotransmitters and cellular exchanges which reduce stress, modulate tissue tone and reduce the experience of pain amongst others.
In the second edition of Fascia: Tensional Network of the Human Body published in 2021, Dr Schleip validates these concepts with this quote stating :
‘However, today an increasing number of practitioners are basing their concepts to some extent on the mechanical sensory nature of the fascia and it’s assumed ability to respond to skilful stimulation of its various sensory receptors’ (p 158).
He also describes in many articles and books his own experience with providing fascia-oriented therapy to anaesthetised patients who had provided him permission for his nonempirical study. He had to concede that anaesthetised patients did not respond to his treatments in the same way as fully conscious patients did (Schleip 2022 p.157). This leads us to assume that the nervous system is likely to be a key player in manual therapy.
In addition, physiological changes are also derived from contextual meaning and play an important role in the Biopsychosocial approach within an EIP. You may have previously known contextual meaning as placebo but in fact, these are meaningful measures that ask your client what matters to them and not what’s the matter with them. For example, a client may want treatment from you as they believe in your capabilities as you helped their friend. It may matter that a client gets treatment from a specialist scar tissue or MFR therapist as they have read on social media that these treatments are the best for their pain. These beliefs can potentially enhance treatment outcomes. The question here is however, how much of our treatment outcomes are actually related to the belief that a therapy works versus the actual mechanical tissue changes by our chosen therapy?
There is no doubt that the science of touch and pain is vitally important. Yet, despite the value of the A&P of touch, most therapists are not taught enough detail about the nervous system or how psychosocial factors influence health to use them in their practice to their advantage. This potentially may be perpetuating the confusion and unsupported claims of how manual therapy works and what it can fix.
Additionally, touch means something different to everyone. It is not as simple as just the nervous system. It involves beliefs about what that touch may do as well as culture and previous experiences. It also

involves the trust and rapport between client and therapist, now called the therapeutic alliance, and it involves the entire contextual environment of the treatment session. All these components influence what your touch means to each individual client.
While it seems that we are closer than ever before to extrapolating a mechanism of action, it is still unclear if fascia-oriented therapies affect the body differently to any other manual therapy. Additionally, we have to accept that all manual therapies may have greater similarity than we would like to believe where no model or trademarked method, known as a modality empire, has superiority (Ingraham 2022). However, despite this, the therapeutic relationship involves many components such as client communication, psychosocial factors, self-efficacy, resilience and beliefs and should not solely rely on a mechanism of action thus moving from a ‘doing to’ relationship to a ‘being with’ relationship. As a result, it is becoming more evident that revision of both teaching and the practice of fascia-oriented therapies needs to be addressed as current evidence does not support many of the claims routinely used. Furthermore, the terms ‘fascia-focused’ and ‘fasciaoriented’ are somewhat obsolete. The only thing we definitely know that we can touch is the skin. While some research suggests that we can influence deeper structures such as the gliding mechanisms attributed to hyaluronan (Pratt 2021), further studies are required.
In our Certificate in Integrated Myofascial Therapy (CiMFT), I introduce mechanosensation and how touch discrimination can be used to offer insight into how MFR may affect the body via the nervous system. Not only that, by understanding the anatomy of fascia, its innervation and the importance of what touch means to your client, you are better equipped to choose appropriate MFR techniques to meet client needs resulting in more productive and client-focused treatment outcomes.
There is definitely an ‘out with the old and in with the new’ attitude across the profession especially regarding the mechanisms of action.
Question what you were taught. It’s perhaps time to reevaluate, revise and update.
References
Barnes, JF. (1990) Myofascial Release: The Search for Excellence. Malvern PA. Friedl, P., & Alexander, S. (2011). Cancer invasion and the microenvironment: plasticity and reciprocity. Cell, 147(5), 992–1009. https://doi.org/10.1016/j.cell.2011.11.016 Fede, C., Pirri, C., Fan, C., Albertin, G., Porzionato, A., Macchi, V., De Caro, R., & Stecco, C. (2019). Sensitivity of the fasciae to sex hormone levels: Modulation of collagen-I, collagen-III and fibrillin production. PloS one, 14(9), e0223195. https://doi.org/10.1371/journal.pone.0223195 Schilder, A., Hoheisel, U., Magerl, W., Benrath, J., Klein, T., & Treede, R. D. (2014). Sensory findings after stimulation of the thoracolumbar fascia with hypertonic saline suggest its contribution to low back pain. Pain, 155(2), 222–231. https://doi.org/10.1016/j.pain.2013.09.025 Pratt RL. Hyaluronan and the Fascial Frontier. International Journal of Molecular Sciences. 2021; 22(13):6845. https://doi.org/10.3390/ijms22136845 Stecco, C., Stern, R., Porzionato, A., Macchi, V., Masiero, S., Stecco, A., & De Caro, R. (2011). Hyaluronan within fascia in the etiology of myofascial pain. Surgical and radiologic anatomy : SRA, 33(10), 891–896. https:// doi.org/10.1007/s00276-011-0876-9 Schleip, R., Zorn, A. and Klingler, W. (2010) “Biomechanical properties of fascial tissues and their role as pain generators,” Journal of Musculoskeletal Pain, 18(4), pp. 393–395. doi: 10.3109/10582452.2010.502628. Available at https:// www.rolfing.berlin/wp-content/uploads/zPDF/ Schleip2010_JMusculoskPain_post-print.pdf
RUTH DUNCAN
Myofascial Release UK (MFR UK) teaches a variety of myofascial approaches including sustained myofascial techniques, compression and traction techniques, position of ease techniques, direct soft tissue mobilisation, rebounding, unwinding and fascial self-care and rehabilitation approaches. MFR UK also teaches fascial assessment, pelvic, sacrum and spinal evaluation and pelvic balancing techniques using pelvic positioning wedges in part 2 of the structural series. MFR UK welcomes those with a minimum of a level 3 handson qualification such as sports massage, holistic massage, Bowen, Shiatsu, Craniosacral therapy, Thai massage and similar. Also welcome are osteopaths, sports therapists, physiotherapists and chiropractors.
Further details can be found on www.myofascialrelease.co.uk Email: info@myofascialrelease.co.uk | Tel: 0333 006 4555
Schleip et al (2022) ‘Fascia: Tensional network of the the human body, 2nd eds. Elsevier Ltd, Poland. Schleip, R. (2014) A Journey in Fascia Wonderland with Robert Schleip: Bridging the Gap Between Clinicians and Scientists. Association of massage therapists ltd, pp. 6-9. Available at https://www. fasciaresearch.de/publications/AMT_2014Journal.pdf Schleip, R. (2003). Fascial plasticity - A new neurobiological explanation: Part 1 and Part 2. Journal of Bodywork and Movement Therapies. Available at https://functionalfascia. com/wp-content/uploads/2017/06/ Schleip-Fascial_Plasticity.pdf Yahia, L. H., Pigeon, P., & DesRosiers, E. A. (1993). Viscoelastic properties of the human lumbodorsal fascia. Journal of biomedical engineering, 15(5), 425–429. https://doi. org/10.1016/0141-5425(93)90081-9 Available at https://pubmed.ncbi.nlm.nih.gov/8231161/ Bordoni, B., Lintonbon, D., & Morabito, B. (2018). Meaning of the Solid and Liquid Fascia to Reconsider the Model of Biotensegrity. Cureus, 10(7), e2922. https://doi.org/10.7759/cureus.2922 Ajimsha M. S. (2011). Effectiveness of direct vs indirect technique myofascial release in the management of tension-type headache. Journal of bodywork and movement therapies, 15(4), 431–435. https://doi.org/10.1016/j.jbmt.2011.01.021 Wu, Z., Wang, Y., Ye, X., Chen, Z., Zhou, R., Ye, Z., Huang, J., Zhu, Y., Chen, G., & Xu, X. (2021). Myofascial Release for Chronic Low Back Pain: A Systematic Review and MetaAnalysis. Frontiers in medicine, 8, 697986. https://doi.org/10.3389/fmed.2021.697986 Kalamir, A., Pollard, H., Vitiello, A., & Bonello, R. (2010). Intra-oral myofascial therapy for chronic myogenous temporomandibular disorders: a randomized, controlled pilot study. The Journal of manual & manipulative therapy, 18(3), 139–146. https://doi.org/10.1179/106698110X12640740712374 Laimi, K., Mäkilä, A., Bärlund, E., Katajapuu, N., Oksanen, A., Seikkula, V., Karppinen, J., & Saltychev, M. (2018). Effectiveness of myofascial release in treatment of chronic musculoskeletal pain: a systematic review. Clinical rehabilitation, 32(4), 440–450. https://doi.org/10.1177/0269215517732820 de Valois B, Young T, Scarlett C, & Holly E. (2021). An evaluation of a ScarWork service for cancer survivors experiencing adverse effects of surgery and/or radiotherapy. European Journal of Integrative Medicine, 44. https:// doi.org/10.1016/j.eujim.2021.101327 Bialosky, J. E., Bishop, M. D., Price, D. D., Robinson, M. E., & George, S. Z. (2009). The mechanisms of manual therapy in the treatment of musculoskeletal pain: a comprehensive model. Manual therapy, 14(5), 531–538. https://doi.org/10.1016/j.math.2008.09.001 Bialosky, J. E., Beneciuk, J. M., Bishop, M. D., Coronado, R. A., Penza, C. W., Simon, C. B., & George, S. Z. (2018). Unraveling the Mechanisms of Manual Therapy: Modeling an Approach. The Journal of orthopaedic and sports physical therapy, 48(1), 8–18. https://www.jospt.org/doi/10.2519/jospt.2018.7476 Langevin H. M. (2006). Connective tissue: a bodywide signaling network?. Medical hypotheses, 66(6), 1074–1077. https://doi.org/10.1016/j.mehy.2005.12.032 Langevin H. M. (2021). Fascia Mobility, Proprioception, and Myofascial Pain. Life (Basel, Switzerland), 11(7), 668. https:// doi.org/10.3390/life11070668 Fede et al. (2022). Innervation of human superficial fascia. Frontiers in Neuroanatomy, vol. 16. Available at https://www.frontiersin. org/articles/10.3389/fnana.2022.981426/full Ingraham, P. (2022) Modality Empires: The trouble with the toxic tradition of ego-driven, trademarked treatment methods in massage therapy, chiropractic, and physiotherapy. PainScience Blog. Available at https://www. painscience.com/articles/modality-empires.php © Fascia Research Society. Photography by Thomas Stephan








