9 minute read
Comparison of Glycemic Control


Comparison of Glycemic Control in Adult Direct Primary Care Patients with Type 2 Diabetes Mellitus Before and After Implementation of Pharmacy-Based Services
By: Dr. Madison Treadway, Dr. Dustin Wilson, and Dr. Stephen Fuller
Advertisement
Introduction
Many Americans struggle to afford healthcare costs and lack regular access to quality healthcare. These issues have been a major focus of legislation such as the Affordable Care Act. The Direct Primary Care (DPC) model sets out to overcome these obstacles while also improving patient and provider satisfaction.1-3 DPC, also known as “membership medicine,” is a practice model that charges patients a recurring fee for healthcare services which, in turn, eliminates the need for insurance billing.1 Instead of the traditional fee-for-service practice model, DPC memberships typically include evaluations, check-ups, basic medical services, and even laboratory work, depending on the contract.1,2
With the DPC model, patient interaction and the health needs of the patient become the focus instead of insurance coding and billing. While the removal of insurance billing frees up the provider to spend more time with the patient, the patient is also able to benefit from the removal of potential financial barriers to routine healthcare.1 In a survey of more than 200 DPC physicians, 98% reported improved patient satisfaction, 81% reported lower out-of-pocket costs for primary care services, and 68% reported an increase in patient compliance with preventative care guidelines.3
The utilization of pharmacists in the primary care setting is well-established. In a systematic review and meta-analysis of 38 studies, pharmacist interventions varying from medication reviews, education, adherence assessment, lifestyle counseling, and/ or physical assessments had a positive impact on cardiovascular and diabetes-related outcomes.4 However, the utilization of pharmacists specifically within a DPC clinic has not been studied.
Access Healthcare, located in Apex, North Carolina, is one of the first DPC clinics which was established in 2002 and now serves over 300 patients under one physician. This clinic utilizes the DPC model where patients pay a monthly membership fee to obtain urgent care and chronic care visits, basic primary care services, and laboratory services. Pharmacy services were integrated into the services available through the DPC membership in June 2021, and about 100 patients are currently being followed by pharmacy services. Since the utilization of pharmacists within a DPC setting has not been specifically evaluated, this study sought to describe type 2 diabetes mellitus (T2DM) care indices following the integration of pharmacy services into this interdisciplinary DPC team.
Methods
This was a single-site, descriptive, pre-post, quality improvement study reviewed and exempted by the Campbell University Institutional Review Board. The primary objective of this study was to describe the change in hemoglobin A1c (HgbA1c) before and at least 3 months after the initial pharmacist intervention in adults with
T2DM at a DPC clinic. Secondary objectives were to describe the percentage of patients achieving a HgbA1c < 7%, the number of antidiabetic medications (see Appendix A) prescribed per patient, and the frequency of hypoglycemia episodes (defined as patient-reported blood glucose < 70mg/dL over the last 30 days) before pharmacist intervention and at least 3 months after the initial visit.
Patients at least 18 years of age receiving care at Access Healthcare with an active diagnosis of T2DM who were seen by pharmacy services from June 1, 2021, to February 22, 2022, were included in this study. Patients receiving diabetes mellitus management from an outside provider or endocrinologist were excluded. Patients were identified by data query through the electronic health record (EHR) at Access Healthcare (Practice Fusion©). Patient data were collected from the EHR and compiled and stored in a de-identified, password-protected Microsoft Excel Spreadsheet file by the primary investigator.
The pharmacy services included an initial face-to-face visit lasting 1-1.5 hours with the pharmacy team that consisted of the clinical pharmacist or pharmacy resident with or without student pharmacists. The initial visit included disease state education, diet and exercise education, medication reconciliation, self-monitoring blood glucose (SMBG) assessment, therapy adjustments, and medication counseling. Patients then received 30-minute faceto-face follow-up visits with the The primary endpoints included mean HgbA1c before pharmacist intervention and at least 3 months after pharmacist intervention. Secondary endpoints included the percentage of patients achieving a HgbA1c < 7%, the mean number of antidiabetic medications prescribed per patient, and the mean number of reported hypoglycemic episodes before pharmacist intervention and after at least 3 months. Additionally, the mean number of down titrations of antidiabetic medications after pharmacist intervention was included as a secondary endpoint. A down titration was defined as medication discontinuation or dose reduction. The primary endpoint and secondary endpoints were analyzed using descriptive statistics. Each patient served as their own control.
Results
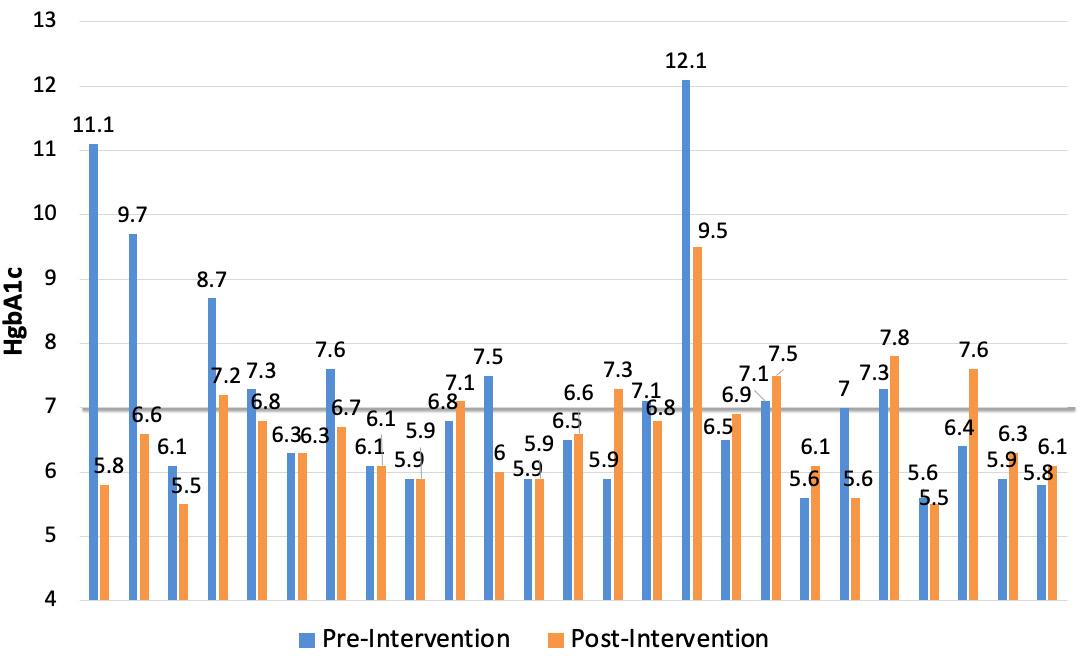
Seventy-seven subjects were screened, and twenty-five met the inclusion criteria. Of the twenty-five included in the study, the mean age was 67.6 ± 9.4 years, and 80% were male. Key characteristics of the patients at baseline are found in Table 1. The mean HgbA1c was 7.1% (95% CI, 6.5%-7.8%) and 6.6% (95% CI, 6.3%-7.0%) pre- and post-intervention, respectively (see Table 2). Figure 1 illustrates the HgbA1c for each individual patient pre-and post-intervention.
The percentage of patients with a HgbA1c < 7% were 56% and 76% in the pre-and post-intervention periods, respectively. The mean number of antidiabetic medications per person was 2.3 (95% CI, 1.8-2.8) vs. 2.2 (95% CI, 1.8-2.6), and the number of hypoglycemic episodes per person was 0.5 (95% CI, -0.4-1.5) vs. no hypoglycemic episodes, respectively. Additionally, 0.5 (95% CI, 0.2-0.8) down titrations of antidiabetic medications per person were observed.
Discussion
In this small quality improvement study, we observed trends towards a modest decrease in HgbA1c with no hypoglycemic episodes among adults with T2DM following initiation of pharmacy-based services into a DPC clinic. Large variations in the magnitude of HgbA1c changes were observed among the subjects. Compared to a systematic review and meta-analysis of 38 studies evaluating pharmacist integration into primary care practices, our study did not have as large of a decrease in HgbA1c.4 In this meta-analysis, HgbA1c reductions ranged from -0.70% to -1.30%, with a mean reduction of -0.88%.4 Pharmacist interventions provided, such as medication reviews, education, adherence assessment, lifestyle counseling, and/or physical assessments, were similar to the interventions provided by this DPC pharmacy team.4 However, many of the studies targeted uncontrolled populations. In contrast, our study included all patients at this DPC clinic with an active T2DM diagnosis regardless of the level of control.4
with a HgbA1c < 7% increased from 56% pre-intervention to 76% post-intervention. Achieving a HgbA1c goal of < 7% can provide positive long-term benefits, as we saw in clinical trials such as the Diabetes Control and Complications Trial (DCCT).5,6 This study compared an intensive goal of 7% to the standard goal of 9%, which showed that better glycemic control was associated with 50-76% reductions in diabetes-related microvascular complications, including retinopathy, neuropathy, and diabetic kidney disease.5 Among the six individuals in our study with a HgbA1c > 7% post-intervention, two were nonadherent to their medications, one had frequent hypoglycemic events prior to pharmacist intervention, and two had large HgbA1c reductions of at least -1.5%. Given that this study only evaluated the first HgbA1c after pharmacist intervention, it is possible that this metric could improve after longer follow-up with pharmacy service.
Before pharmacist intervention, 44% of patients were on at least 3 antidiabetic medications. The mean number of antidiabetic medications per person was similar after pharmacist intervention with 2.3 (95% CI, 1.8-2.8) pre-intervention versus 2.2 (95% CI, 1.8-2.6) post-intervention. While reducing the number of unnecessary medications has the potential to reduce polypharmacy and the risk of adverse events in an overtreated population, we found this particular metric was not useful since our cohort was not characterized as an undertreated or overtreated population at baseline. There are several limitations to this study worth noting. First, this study has limited external generalizability, given the findings are specific to a single site. The small sample size prohibited meaningful hypothesis testing for differences. This study had a short duration of follow-up by only observing the first HgbA1c at least 3 months after pharmacist intervention. Lastly, there were several pre-intervention HgbA1c outliers (such as 12.1%, 11.1%, and 9.7%) that impacted both the degree of change possible and the likelihood of meeting the categorical cutoff of HgbA1c < 7%.
Conclusion
A trend toward a decrease in the HgbA1c without an increase in hypoglycemic events was observed after the initiation of pharmacy-based services among adult patients with T2DM at a DPC clinic. Though this was a small quality improvement study, the results of this study introduce the potential positive impact the integration of pharmacy-based services into this unique practice model can have on diabetes mellitus care indices among adults with T2DM. However, this needs to be confirmed in larger, controlled studies. In addition, future studies should assess the impact on other chronic disease states (i.e., hypertension, hyperlipidemia, and obesity).
Authors: Madison T. Treadway, PharmD, was a PGY2 Ambulatory Care Pharmacy Resident at Campbell University College of Pharmacy & Health Sciences (CPHS) and Access Healthcare in Apex, NC. ma.treadway@wingate. edu. Dustin Wilson, PharmD, BCPS,is an Associate Professor at CPHS and a Clinical Pharmacist at Duke University Hospital. Stephen Fuller, PharmD, BCACP, CPP, is a Vice-Chair and Professor at CPHS and a Clinical Pharmacist at Access Healthcare.
References: 1. Direct Primary Care [Internet].
American Academy of Family
Physicians. AAFP; 2019 [cited 2021Aug16]. Available from: https://www.aafp.org/about/policies/all/direct-primary-care.html 2. Cole ES. Direct primary care: applying theory to potential changes in delivery and outcomes.
J Am Board Fam Med. 2018 Jul-
Aug;31(4):605-611. doi: 10.3122/ jabfm.2018.04.170214. 3. Grzeskowiak D, Huth E. Direct primary care: evaluating a new model of delivery and financing [Internet]. The Society of Actuaries. SOA; 2020 [cited 2021Aug16]. Available from: https://www.soa.org/globalassets/assets/files/resources/ research-report/2020/direct-primary-care-eval-model.pdf 4. Tan EC, Stewart K, Elliott RA,
George J. Pharmacist services provided in general practice clinics: a systematic review and meta-analysis. Res Social
Adm Pharm. 2014;10(4):608622. doi:10.1016/j.sapharm.2013.08.006 5. Diabetes Control and Complications Trial Research Group, Nathan
DM, Genuth S, et al. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus.
N Engl J Med. 1993;329(14):977986. doi:10.1056/
NEJM199309303291401 6. American Diabetes Association
Professional Practice Committee,
Draznin B, Aroda VR, et al. 6. Glycemic targets: standards of medical care in diabetes-2022. Diabetes
Care. 2022;45(Suppl 1):S83-S96. doi:10.2337/dc22-S006
• Sulfonylureas
• Meglitinides
• Biguanides
• Alpha-glucosidase inhibitors
• Thiazolidinediones
• Dipeptidyl peptidase-4 inhibitors
• Glucagon-Like Peptide-1 receptor agonists
• Insulin
• Amylin
Table 1. Demographic Characteristics*
Table 1. Demographic Characteristics* Characteristic Age – years Male – n (%) Race – n (%) White Black Hispanic Asian Insurance status – n (%) Commercial insurance Medicare No insurance
*Data are mean (± standard deviation) or n (%)
N = 25 67.6 ± 9.4 20 (80%)
16 (64%) 3 (12%) 3 (12%) 3 (12%)
5 (20%) 14 (56%) 6 (24%)
Table 2. Diabetes Mellitus Indices Before and After Pharmacist Intervention*
Table 2. Diabetes Mellitus Indices Before and After Pharmacist Intervention*
Pre-Intervention Post-Intervention
HgbA1c – %
7.1 (6.5 to 7.8) 6.6 (6.3 to 7.0) Change in HgbA1c – % – -0.5 (-1.1 to 0.8) No. of antidiabetic medications 2.3 (1.8 to 2.8) 2.2 (1.8 to 2.6) No. of down titrations – 0.5 (0.2 to 0.8) No. of hypoglycemic events 0.5 (-0.4 to 1.5) 0 HgbA1c < 7% – n (%) 14 (56%) 19 (76%)