2020 - 2023


Following a series of successful workshops exploring the diaspora engagement in the Nursing Now global campaign, two Ugandan diaspora Nurses based in London formed an association, called Uganda Nurses and Midwives Association-UK (UNMAUK). It was launched at the back end of the second wave of the COVID-19 pandemic in July 2020 with five objectives:-
1. To provide a forum for networking professionally, sharing skills, exchanging ideas and views, and enhancing professional development;
2. To promote the health and well-being of members;
3. To provide a professional advocacy body to belong to;
4. Organise and deliver educational development meetings, training events, and courses for members and others;
5. Raise funds to support global health and social welfare initiatives.
This report provides a comprehensive report for the initial formation period covering June 2020 - September 2023.
We would like to thank our first inaugural Patrons,
• His Excellency Ambassador Julius Peter Moto, High Commissioner of Uganda to United Kingdom and Ambassador to Northern Ireland for his open door policy and leadership in enabling fruitful discussions and aligning our vision for the betterment of all.
• Ms Nancy Jirira, whose vast experience and knowledge of central governance ensured that in formulating our association, the objectives remain focused and centered on the issues we face as migrant professionals.
Our Leaders,
• Ms Felicia Kwaku OBE, Chair, Chief Nursing Officer Black Minority Ethnic Strategic Advisory Group (CNO BME SAG), whose guidance, leadership and support ensured that our concerns are tabled and presented well to our senior nurse leaders in the country.
• Dr Rose Clarke Nyanyonga PhD, for guidance and leadership in embedding the objectives to be adaptable and consistent. And, last but not least,
• Dr Joan Myers, OBE, for leadership, mentorship and advocacy for the BAME Nurses in the NHS workforce.
Anecdotal reports suggest that diaspora are all casual workers in their countries of residence. Amidst this analysis, the diaspora face several challenges and barriers in their countries of residence - from the consequences of migration to integration, social exclusion and racial discrimination. Despite these amounting barriers, the diaspora - whose economic remittances is well documented and recorded, include professionals in all industrial sectors from banking/finance to engineering.
From both personal and professional perspectives, there arose my ambition to pursue evidence that supports Tropical Health Education Trust (THET) s’ 2021 report – “experts in our midst”. The provision for an avenue and opportunity where the un-tapped knowledge and lived experiences of the diaspora can be utilized to support our growing and developing health care systems. Through active stakeholder engagement and collaboration, there was a realisation of this potential (Newland and Patrick, 2004). Therefore the formation of the association that inadvertently contributed to enhancing my leadership journey as an ambitious diaspora Ugandan Nurse, and together with Primrose, the initial phase has been focused on the strive and desire to evidence our full potential as stakeholders in contributing to alleviate human suffering while enhancing the health care systems.
Our initial strategic plan has been focused on embedding our vision, and mission through exploring how we grow and develop our objectives into tangible achievable activities. We have realised a lot of growth and also some gaps. Through the growth we have continued our mapping exercise, enhanced our stakeholder engagements, created and built our unique image - visibility these days is important.
I remain optimistic that UNMA-UK, together with the Diaspora Nursing and Midwifery consortium provide evidence to policy makers of the unwavering potential of the diaspora healthcare professionals who have successfully migrated and yet continue to forge ways to navigate through the systems, maintain strong links to their countries of birth/origin, integrate and contribute positively to the building and strengthening of healthcare systems for both countries of residence (host) and birth (origin).
Strength in Unity.
Elizabeth Pearson, @ezabe2 Lecturer in nursing Co-founder and Inaugural President UNMA-UK Founding Director, National Health Care Conferences (NHCC) Uganda.


One of my tasks as the High Commissioner of Uganda in London and Ambassador to Ireland was to work with Ugandans in diaspora.
I accomplished this by engaging the Ugandan potential leaders in London and Ireland. I encouraged them to work collectively and value the efforts of each other to promote their well-being while transferring knowledge and skills to Uganda.
I was particularly happy to meet with the current leaders of Ugandan UK nurses and midwives association. When Elizabeth Pearson came to my office in Trafalgar Square, we had a lot of discussions and ideas on how to move things forward. She went on to run training workshops in Uganda for Nurses and Midwives. Later on, working together with Ms Primrose Magala and a group of other Ugandans, they formed the current association. Ms Primrose Magala also paid several visits to my office in London and provided leadership in a number of eye camps in Uganda, including capacity building for ophthalmology nurses.
Had it not been for the adverse effects of COVID-19 that affected their work for the period of the lockdown - two years and half years - we would have achieved more progressive projects. However, not all is lost as I always say knowledge not shared is useless. The association has grown from strength to strength with membership standing at nearly four hundred members. I am optimistic that its expansion will have no limits.
As I step down as the Patron of the Association I have two pieces of advice for you.
First, you should be honest and transparent to members in all your strategic plans and communicate the outcomes of the same to members.
Secondly and equally important is that this association should remain apolitical; as you started.You should only work with both governments of Uganda and that of UK, so that not to patronise the objectives of the association.
I wish you the very best of luck in everything that you do. Continue to uphold the integrity of your values.
I thank you very much.
Ambassador Julius Peter Moto
High commissioner of Uganda to UK and Ambassador to Northern Ireland (2018-2022)
As of 2019, over 215 million people are reported to be living in host countries (Newland, and Patrick, 2004). Statistics indicate that 6% of them are doctors and 5% nurses. Referred to as diaspora - living and working in a country other than their birth country (country of residence), not their country of birth (country of origin). According to the 2011 census, over 60,000 people in the United Kingdom (UK) were born in Uganda. Anedoctal statistics indicate that when the second-generation Ugandans is included, the number of Ugandan descent in the UK is closer to 200,000 (Census, 2018).
The COVID-19 crisis rocked the world, the worst pandemic in more than a century. Over one hundred and twenty members of our small but growing community died due to the virus including some healthcare practitioners. We were limited on how to support our colleagues and the community members through the bereavement process – The practical repatriation process had major disruptions which through our cultural beliefs and norms had now been hindered due to the government directives on the Standard Operating Procedures (SOPs) for the lockdown.
According to the National Health Service (NHS) Workforce Race Equality Standard (WRES) report 2022, as of 31 March 2021, Out of the 1.27 million staff working in the NHS trusts in England, only 22.4% (309,532) were from a Black Asian and Minority Ethnic (BAME) background and of these only three hundred and fortyone were at the very senior management level. From the NHS One Nation One NHS report, over 800 registered healthcare professionals recorded Uganda as their country of birth. Anecdotal evidence suggests that over a quarter of these are running and coordinating initiatives and projects that impact the local and global community.
Despite these life threatening circumstances, many members were facing unfair discriminatory practice in the workplace. There were many incidents being reported were the provision for Personal Protective Equipment (PPE), was not being distributed equally, the deployment process was seemingly unfair to the BAME healthcare professionals (Chaudhury, et al 2020). Many were reporting being forced to work in the high risk areas unsupported. More about the wider Diaspora Nursing and Midwifery consortium can be found here https://www.england.nhs.uk/ nursingmidwifery/international-recruitment/.
Later on, the growing public concern about the vaccination hesitancy also raised more concerns.
Following discussions with various leaders, we realised the need and paramount opportunity to work collaboratively - bringing all the initiatives and projects under
one umbrella and support each other for a more sustainable effort. The association would place enhanced exposure and capacity to work with the local governments through delivery of micro and macro health and social care programs that strategically affect us as members of our BAME community. Identified as a BAME, the goal was to align the existing initiatives lead by all members under one umbrella organisation.
Most significantly, we realised the benefit to foster knowledge sharing in order to manage the disease pandemic through communication, learning, emotional and pastoral care in order to give the best of ourselves as frontline staff in the fight against the deadly disease. The ultimate goal was to ensure that we were well and healthy and that we would then give the best care to our patients and communities. This was aligned with the top three areas in the NHS that benefit from health researchquality improvement, patient safety and service design. The objectives set looked at how areas such as social factors affect the quality and outcomes of healthcare and provide initiates and solutions.
The United Kingdom (UK) NHS primary purpose is to deliver safe and effective care that improves healthcare outcomes for all. In other words, to provide a good experience for all (NHS constitution). When founded in 1948, it was a complex but unified organisation with a strategic plan to fund population-funded healthcare services centrally. Since then, with the increased ageing population, changes in population and structure, emerging new diseases, advancement in healthcare and changes in the prevalence and distribution of chronic conditions, it has and continues to face tremendous pressure.
Following a series of successful workshops exploring the diaspora engagement in the global Nursing Now campaign that was launched by Lord Nigel Crisp, (Co chair of the All-Party Parliamentary Group on Global Health, former Chief Executive Officer (CEO) of the NHS and Permanent Secretary at the Department of Health (DoH); Two nurses, Elizabeth Pearson and Primrose Magala, - who, after several engagements and managing different projects and initiatives in Uganda, realised the need to bring focus on supportive ways for the nurses and midwives here in the UK and globally.
As one of the Diaspora Health Organisations (DHO) the association strategically provided the social and professional value and would being a joined and more considerable impact advocating and providing culturally sensitive healthcare and, when needed, provide humanitarian aid to Uganda, our country of origin/birth. Uganda Nurses and Midwives Association-UK (UNMA-UK) and with five objectives:-
1. To provide a forum for networking professionally, sharing skills, exchanging ideas and views, and enhancing professional development;
2. To promote the health and well-being of members,
3. To provide a professional advocacy body to belong to,
4. Organise and deliver educational development meetings, training events, and courses for members and others.
5. Raise funds to support global health and social welfare initiatives.

Roughly a quarter of the over 1.27 million NHS employees are individuals of BAME background, as per the Office of National Statistics (ONS) statistics. In March 2019, NHS reported that 79.2% of its staff was White, and 20.7% identified as belonging to the BAME background. The data shows that 40% are medical doctors, and 20% are in the nursing workforce and, a larger population of BAME Health Care Professionals (HCP) employed in the medical sector than in other disciplines or managerial positions with just overall 7% of managers being BAME (Kline, 2014).
The percentage shows that those who reach the highest echelons of management (bands 8a to 9) who are not doctors or nurses are much lower. As a result, BAME HCPs are underrepresented groups who make up a disproportionate share of the NHS’s entry-level workforce. Nagpaul, (2020) and Archibong and Darr (2010) concluded that BAME HCPs hey are forced to toil in the shadow of the service’s pristine peaks because of a lack of opportunities for their advancement.
In addition, the Royal College of Nursing (RCN) quoted that in 2020, 24,142 registrants left the Nursing and Midwifery Council (NMC) register, compared to 26,863 in 2021 - an increase of 11.3%. These have been both directly and indirectly linked to this underrepresentation (Kline, 2014).
In 2016, Lord Philp Hunt commented on the underrepresentation of BAME executives on NHS Trust Boards and senior management positions in the NHS (The Guardian, August 21 2016). He concluded that this underrepresentation on executive boards has been linked to the persistence of severe service failure and inequality of provision with devastating individual and institutional consequences. Therefore the pandemic
disproportionately affected the members from the BAME background and this highlighted this gap even further. The vision of the association was created to bridge these gaps by working collaboratively with stakeholders to utilise our in-house resources and promote our well-being.

The vision is to unlock the professional know-how of our members, empower ourselves to develop beyond our limitations, and use the association to drive change within nursing and midwifery in the UK, Uganda and globally.
The motto for the association is “Strength in Unity”.
To develop a vibrant, supportive professional organization and network that prospers the welfare and advances of Ugandan nurses, midwives, students and associate nurses in the UK.


The association objectives and values relied on these themes:-
• Bridging the gap of inequalities for the BAME communities
• Inter-link with other diaspora and BAME communities and external stakeholders
• Build a Healthy Workforce - to promote Healthy Human resources
• Empower the diversity skill set within.
Promote professionalism, Health and Wellness, and Enterprise/Innovation.

• Provide and support Educational development
• Build a Professional network
• Promote health and wellbeing through creating affinity health promotion and prevention programs.
• Advocacy
• Support global health and social welfare initiatives.

The studies by Marangozov, et al, (2016) and Buchan, et al (2019) proved that the NHS, as the biggest employer of health care professionals in the UK, is institutionally racist, and many of the members have been and continue to be victims of this unprofessional behaviour, including harassment, victimisation and racial discrimination.
The criteria for membership encompass as many nursing workforce as possible.
The inclusion criteria for membership includes:-
1. Ugandan – affiliated by birth or heritage
2. Diaspora - working and or residing in the UK
3. Qualified Nurse/Midwife – trained in and/or outside the UK
4. Registered Nurse/Midwife – registered with the Nursing and Midwifery Council (NMC)
5. Student nurses/midwives – working towards qualification and/are preregistered with NMC
6. Associate nurses - working towards qualification and/ pre registered with NMC
7. Retired nurses/midwives (whom we refer to as our generals).
The benefits to members of joining the association are outlined as follows :-
1. Shared learning – Many BAME HCPs face many challenges when accessing Continued Professional Development (CPD) training from the workplace as evidenced by Likupe and Archibong, (2013). We are often marginalised and are not given priority.
2. Enhance team working skills - The association acts as an avenue/platform for practicing/enhancing teaching, writing, presenting, chairing skills.
3. A support network - The association mentors members and provides support for challenging situations faced by members.
4. Members also have access to colleagues who can help with revalidation in order to stay registered to practise in the UK.
5. Professional networking - Association membership also provides several networking opportunities.
6. Volunteering skills – Volunteering for special projects and allows you to make a real difference and give back to your profession.
7. Research – the association provides an avenue for members to participate and conduct various nurse-led research studies that is needed for policy formation and development.
8. Celebration – we take time to celebrate events and recognition of each other that reminds us why we became nurses in the first place.
The inaugural team aimed to operate sound governance, develop effective plans and activities in order to complete the formation phase that ensured the association can build resilience and sustainability in what would inevitably be very challenging years to come.
The inaugural team included:-
A. Two nominated Patrons
• His Excellency the High Commissioner of Uganda to the UK and Ambassador to Northern Ireland Mr Julius Peter Moto Ambassador. For his active engagement with diaspora community members, leadership and guidance - endeavours to actively listen and support the diaspora community.
• Ms Nancy Jirira, an NHS Nurse Manager, Health Visitor, Nurse Prescriber and Team Manager (Specialist Community Public Health Nurse) with extensive experience in local government and the experience of the progressive change of the NHS
B. Two executive co-founders
• Elizabeth Pearson. Having successfully and proudly runs a nurse-led initiative that aims to empowering Nurses/Midwives through provision of accessible and affordable CPD, fostering shared learning for Nurses and Midwives (www. nhccuganda.com).
• Primrose Magala. Having successfully and proudly runs a nurse-led initiative that focuses on alleviating the human suffering for neglect in the growing concern for eye health through eye camps and training (www.eyehealthafrica.org).
C. Eighteen nominated board members
• Secretary - Miriam Aligawesa, having successfully and proudly co-founded the Uganda Heath diaspora foundation.
• Other board members included - Rita Kyambadde, Haruna Nyanzi, Bridget Katungi, Gertrude Namwanje, Rita Kalema, Masembe Nkata, Richard Kasirye, Justine Nakimuli, Jona Robert Wanzala, Penni Wampamba, Jane M Acirocan, Teddy Matovu, Christine Kakai, Herbert Mwebe, Tim Mujerwa, Jean Bugonzi and Jacqueline Nsereko.
Shared learning webinar.

Association Core executive leaders in an engagement meeting with Patron Cllr Nancy Jirira and International Council of Nursing (ICN) Chief Executive Officer (CEO) Howard Catton, 2020.
One of the initial key goals was to develop an integrated mentoring program to support existing Health Care Professionals (HCPs) and prepare for the potential new International Recruited (IR) colleagues from Uganda to enable them and support them to adapt to the professional working life in the UK, manage re-registration processes and support the community to achieve their potential within the NHS.
The strategy was adapted into two phases - the formation and the consolidation phases - which would both cover a joint period of five years.
To provide a professional advocacy body, forum to belong to, to network professionally, share skills, exchange ideas, views, and enhance professional development
Mapping exercise
• Explore the members act the country
• Formulation of the team (initial interim committee until inaugural annual general meeting)
• Design activities for inclusion that enhances membership engagement
• Draft policies and guidelines for engagement
Completed July 2021 20 members elected through nominated
Raise funds to support global health and social welfare initiatives
To promote the health and well-being of members,
Organize and deliver educational development meetings, training events, and courses for members and others.
Organize and deliver educational development meetings, training events, and courses for members and others.
Shared knowledge activities with expertise, and skills
Concept note – draft and consultation completed
• Identify stakeholders Ongoing
• Registration to legalise our entity as a charitable organisation
Drafted Constitutionlegal binding governance document
• Enhance visibility Social media platformsPlatforms created Twitter, Website, Facebook
• Hardship support to identified causes Ongoing review
Enhances membership engagement
• Launch regional clusters to decentralise management
• Enhance activities for the involvement of members
Four regional clusters recognised and launched London Oxford Liverpool Northampton
Annual free Community health promotion event
• Aligning with strategic stakeholders Ongoing
• Support members
Mentorship program for shared support and learning based on nursing practice and nursing leadership. Mentors’ forum Mentees
Establish sustainable resources and funding to achieve our objectives
Strengthen the collaborations and partnerships with stakeholders like CNO, FNF, HEE, NHSI, Commonwealth Federation, and BAME diaspora consortium
External health and social care organisations
Shared learning including diaspora medical camp
Completed
Twenty four months after the official launch, the strategic activities for 2021 were aimed at strengthening the membership through the mapping exercise and enhance visibility through supporting member engagement activities. These were identified as key to improve the essential advocacy of the members including joint formation of the diaspora consortium of Nursing and Midwifery organisations.
Community Outreach Support to enhance integration through focus groups from the lived experiences.
The organisation members offered pastoral support to their peers during the pandemic and hosted a Virtual Vigil/Lumbe that brought the Uganda diaspora community together including our various community leaders like His Highness/ Owekitibwa Mr Ronald Lutaaya from the Buganda kingdom, and from religious leaders including Sheikh Kalantini. This was important because the SOPs hindered our ability to offer cultural bereavement support and the organisation was promoting and adapting to the new virtual ways of working and supporting members.
Nearly two hundred community members joined the virtual vigil, offered words of comfort and encouragement. They also offered financial contribution to the families who were experiencing hardship. Together the community members supported each other.

To strengthen our community in terms of personal and professional development, the association is working closely with one of the organisations run by one of our members, National Health Care Conferences (NHCC) Uganda, and others to provide education programmes for developing fundamental nursing principles in line with the policies and protocols of the NMC code, including the structured clinical examinations (OSCE). Other areas to offer support include communication and nursing skills, primarily due to cultural differences and language barriers, and interview techniques.
Through the financial hardship initiative, members offered incredible support for a couple of one-off contributions to the beneficiaries—a baby and a young adult both in Uganda. For the former - safe monitoring and safeguarding due to neglect and for the later - physiotherapy following caesarean section operation. We carried out a one-ff successful fundraising campaign.

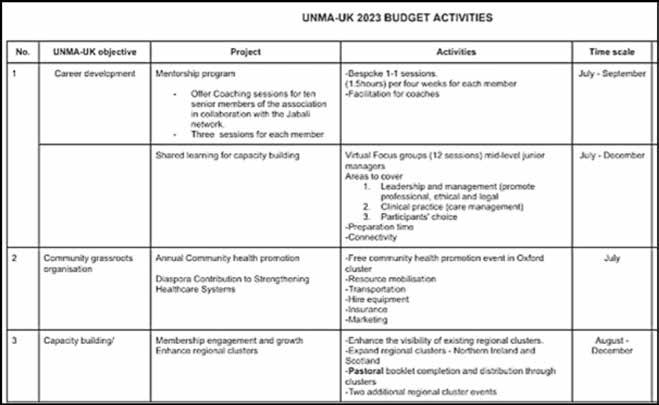
Nurses and midwives are leaders at every level and throughout their careers. One of the key strategic policy recommendations of the WHO for 2021-2025 is an investment in leadership skills development for nurses and midwives (WHO, 2021). Whilst nurses and midwives comprise the largest section of the health workforce in Uganda, there have been limited opportunities for their leadership development. The association leadership has been keen on external stakeholder collaborative work with the aim to deliver the objectives of the association each year through the formation and consolidation process. Some of the proposals include the following.
in partnership with Florence Nightingale Foundation (FNF), Health Education England (HEE), Royal Academy of Dramatic Art (RADA) – The proposal is aimed to enhance, support and development of Ugandan Nursing and Midwifery leaders. The project is aimed to:-
• Demonstrate enhanced awareness of how personality preferences influence personal effectiveness and performance in teams
• Identify and critically appraise opportunities to influence through personal and collective authority
• Develop strategies to express self in a manner which communicates presence, enables influence and has impact
• Explore personal and collective resilience and develop tools for staying effective under pressure
• Formulate and put into practice plans which contribute to improved outcomes for patients and staff underpinned by evidence and quality improvement methodology

Investing in this nurse mentoring project is an opportunity to raise the profile of the expertise of NHS diaspora nurses and will ensure that nurses in the NHS will benefit from these cross-cultural learning experiences.This will leverage the unique expertise of diaspora nurses to share experiences with Ugandan counterparts and it presents an opportunity for the members to share clinical expertise and identify ways the two different healthcare systems can learn from each other. Several engagement meetings have been held with all parties and we are awaiting for the outcome of the funding application.
- As a member of the diaspora consortium, that aims to work in partnership especially as rooted in our local communities - having an expert perspective on the needs of our local members and how best to provide services that meet our needs hence to raise advocacy for all BAME healthcare workforce collectively. Indeed, we recognise that as well as sub-contracting, forming a consortium is another way in which smaller organisations like ours can get involved in the delivery of public sector contracts.

- Strengthening BAME leadership capacity. Over the years, a reported mention of customary practice exists in the NHS, perpetuating an unwritten workplace culture instrumental in promoting inequalities among the BAME HCPs as per the recent 2020 Workforce Race Equality Standard (WRES) report and, only 7% of the are managers are reported to be from the BAME groups. Nurses must have opportunities to develop leadership potential and participate in decision-making forums because the leadership is required at all levels of nursing and midwifery, - from the national government to the bedside. Efforts to protect the quality, expand access, and improve outcomes will succeed with capable nursing and midwifery leaders.
Jabali network has a strong track record of developing nursing and midwifery leaders combined with the experience and knowledge of governance capable of improving patient and service outcomes. Members who will benefit from the initiative have been identified and the second stage of the engagement process has been delayed due to internal leadership and management issues that have to be resolved.

The activities for 2022 included a build up on the mapping exercise and exploring varied membership engagement activities.
Proactive engagement in the community
Most information and studies surrounding diaspora contribution empathise with the diaspora’s contribution regarding remittances to their countries of origin. Still, anecdotal evidence and lived experiences indicate that significantly diaspora present as a unique asset for their countries of origin as active networkers and mediators in this globalised and transitionally connected world.

Despite the overwhelming contributions, the current literature on diaspora engagement with the health systems is limited. Further and more formal assessments of these engagement activities and initiatives are now paramount to understanding and ultimately optimising diasporas’ efforts to improve the quality of the health systems.
The Annual free community health promotion events are designed to engage with the community as contributors and partners to build the healthier nation. As diaspora nurses, we are culturally aware and have a strong understanding of global health and health systems issues in different settings. Being listening attentively in order to understand people and their needs and having a non-judgemental approach to learning and development. Through these, we have selected engagement activities that align with our objectives that will provide exemplars of our contribution and enhance our research practice. They are specific to our goals, measurable as we evaluate their effectiveness, achievable as we have all the key persons, realistic to our ability to deliver and will be completed promptly.
Clusters - to enhance membership engagement and decentralise pastoral care through regional clusters.The 4 initial clusters were launched and led by the following members.
London – Primrose Magala
Liverpool – Justine Nakimuli
Northampton – Joe Lutwama and Oxford – Tim Mugerwa.
The benefits:-
• Increased transparency and accountability: Greater transparency in resource allocation, co-leadership, and operational performance leads to greater responsibility.
• Engagement with national and local networks: Having a single person to call within the region speeds up the process of communication and coordination of activities;
• Inclusion of affected communities: Tools and services developed through the cluster Approach ensure that those who know the most appropriate solutions to their regional problems are engaged in formulating the response, listening to diverse perspectives and be flexible with decision making;
• More effective advocacy: Where the Clusters, singly or collectively, speak with one voice on issues of common concern, including those affecting groups who are generally not heard; encouraging thought diversity and inclusion in the team
• Joint strategic and operational planning: The formal coordination process within and between Clusters enhances efficiency while improving effectiveness to deliver our objective.
With the mapping exercise enhanced through the first year of launching, we realised the need to focus on knowledge sharing for career advance webinars and seminars enhancing shared learning between colleagues here in the UK and from those in Uganda and beyond. Training and development for shared learning is extending in partnership with NHCC Uganda to enhance capacity building in two areas :- (i) leadership and management (to promote professionalism, ethical and legal practice), and (ii) clinical practice (care management). On average, there has been an increase on members attendance of the webinars held virtually. From twenty fifty members in 2020 to nearly seventy members this year.
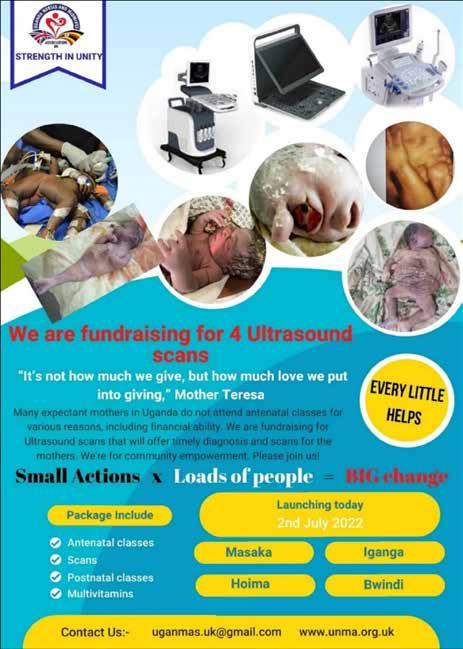
Inline with our objective to offer humanitarian aid in support of our social responsibility to positively impact participants’ perspectives and improve service delivery while using fewer resources, the association embarked on the project to focus on maternal health and services because there is a prevalence of high maternal mortality rates persist in Uganda due to an overall low use of contraceptives, limited capacity of health facilities to manage abortion/miscarriage complications, poor quality of healthcare services, limited access to healthcare services, cultural barriers in seeking access healthcare services, mistreatment of mothers by medical personnel, limited reproductive health literacy, reliance on traditional medicine by mothers, malaria and prevalence of HIV/AIDS among pregnant women.
According to the World Health Organization (WHO) (2019), approximately 830 women die daily from preventable causes associated with pregnancy and childbirth. In 2017, the Maternal Mortality Ratio (MMR) in developing countries like Uganda was found to be 462 per 100,000 live births whereas the MMR for high income countries was 11 per 100,000 livebirths (WHO, 2019), a stark 451 difference.
Complications (such as high blood pressure, gestational diabetes, anaemia, infections, breech position) during pregnancy and following childbirth remain a common cause of maternal mortality. Almost all of these complications develop during pregnancy (Atuhaire & Kaberuka, 2016). In Uganda, haemorrhage (42%), prolonged labour (22%) and unsafe abortion (11%) are the major causes for maternal mortality (Böhret, 2018).
Many expectant mothers in Uganda do not attend antenatal classes for various reasons, including the financial ability. We are fundraising for Ultrasound scans that will offer timely diagnosis and scans for the mothers including pre and post natal care services through our community midwives initiate.
IR remains a controversial area with multiple perspectives which could positively and negatively impact healthcare planning and delivery. However, with the global Health Human Resources (HHR) comprising of 59.2 million health workers, the World Health Organization (WHO) still estimates a deficit of approximately 2.4 million physicians, nurses, and midwives along with a need for an additional 2 million pharmacists and paramedical professionals and thus established a global code of practice to address this growing crisis (DoH, 2004).
The nursing workforce shortage continues to be a growing challenge globally, and in the UK, the government recognised the need to increase the number of registered nurses in the NHS by 50,000 by 2024-25. UNMA-UK, as a key stakeholder, is keen to explore the opportunity for our unemployed colleagues in Uganda. Soon after the launch of the Health and Care Visa in August 2020; that gives fast-track visas to all health workers from anywhere in the world to come to Britain, (https://www. gov.uk/government/news/government-launches-health-and-care-visa-to-ensure-ukhealth-and-care-services-have-access-to-the-best-global-talent), the President of the association drafted a proposal on capacity building and mutual benefit of the healthcare workforce in order to meet the demands of the Universal shortage. According to the Uganda Health Labor Market Analysis, (2019) the total number of registered health workers in Uganda has since increased exponentially from 45,598 in 2008 to 118,236 in 2020, of which 64% are nurses and midwives. The Uganda Nursing and Midwifery Council (UNMC), records the total number of nurses on the register was 74,873, of which 48,610 (65%) had active practising licence in 2020. UNMC estimates that over 5,097 more nurses are produced each year without new employment in the public sector.
Although the NMC registration is increasing slowly, with 1% growth mainly from international nurses, the NHS long-term plan has expanded IR significantly over the next few years to fill this gap. therefore, attracting international nurses is a critical strategy to fill the shortage. Of the 64% of the nurses and midwives on the UNMC register, 80% are enrolled nurses and midwives. The proposal would allow the educational capacity of the cadre level of the nurses (enrolled, diploma, degree and masters degree level) that will improve the country’s capacity and mutual benefit to both healthcare systems.
Benefits include but are not limited to:-
I. Experience and knowledge transfer - peer-to-peer support
II. Economy remittance – boost economy /income for both individual and country
III. Develop global health partnerships
IV. Mutual benefits both personal and professional
V. Empowering and improving skills of leaders
VI. Utilising retired leaders and their legacies constructively
VII. Capacity building for exiting staff to enhance the profession and retention rates
VIII. Creating a conducive, attractive professional for the next generation
As a key stakeholder, the association President has taken a lead role in the initial discussion and presentation of the project.
Stakeholder engagements
1. There have been several engagements between the two health systems as required from WHO ethical recruitment code.This is particularly important in building professional working relationship for the build up for mutual agreement. Mutual benefit was embedded and for as many stakeholders as possible. Eight high level stakeholder meetings with the proposed partners including the lead team from Department of Health and Social Care (DHSC) in the UK, Uganda technical team and UNMA-UK have been conducted successfully.
2. An initial request or appeal to the UK government must be sought.Through the office of the Permanent Secretary Ministry of Health, this has now been completed in February 2023. The technical team has been guided through the indications on plans to support the potential candidates to prepare and complete the mandatory process and tests.
3. Political leadership team engagement- in order for the memorandum of understanding can be achieved, UNMA-UK President requested the Minister of Trade and Envoy to UK and Uganda. His Lordship Dollar Popat was requested to support the political leadership to agree with the proposal and support the team’s efforts. To date, this has been achieved, and the technical team is concluding the details of the implementation plan upon which the agreement will be signed.
The Proposed Technical Management Team Included:-
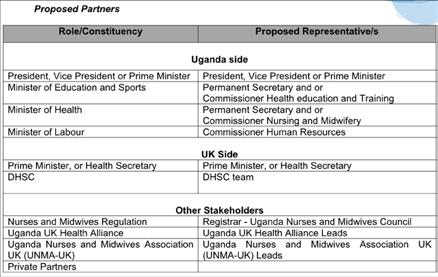

With His Lordship Dollar Popat, Honourable Permanent Secretary Ministry of Health Dr Diane Atwine, Former Speaker of Parliament Ms Rebecca Kadaga, Charles Ayume, Deputy Ambassador Mr Mugerwa, Co-founder and President UNMA-UK Elizabeth Pearson, Cofounder and Vice President Primrose Magala and many delegates. April 2022

Commissioner for Nursing and Midwifery, Ministry of Health Uganda Ms Agnes Chandia, Dr Joan Myers OBE, Tim Mugerwa and co-founder and President UNMA-UK Elizabeth Pearson, Feb 2023

With Honourable Minister of Gender Labour and Social Development, Amongi Betty Akena, Deputy Ambassador Mr Mugerwa, Co-founder and President UNMA-UK Elizabeth Pearson and members of the nurses association. September 2023
4. Requirements - Some key areas that require efforts for the agreement include:- equity training providers including International English Language Testing System (IELTS) language proficiency, training and education support in the nursing clinical mandatory skills.
• English language/ ILETS – identified as the first inhibition, we have challenged this on the policy level, and now there are various ways to qualify this requirement. The association has collaborated with a reputable organisation that is working with our nurses and helping them prepare for the test with higher chances of passing the first time and they are.
• Interview skills through our mentorship program - We offer and organise meetings and webinars to support colleagues using virtual platforms. These are interactive and offer one-to-one service when required. this includes CV writing and completing personal statements. The association agreed with signposting the key stakeholders in identifying areas of concern and involvement. Through informative online webinars, any misconceptions and misguided information about the project continue to be tackled by sharing lived experiences.
• Training and development for short recap training courses in nursing mandatory skills for the competence development and skills.


Some of the volunteering team members at our inaugural annual FREE community health promotion event July 2022,

Guests at the 2nd Anniversary celebration in London
2023/24 is our consolidation stage were the second phase of formation process takes place for any organisation to thrive. There is a need to embed sustainability of the activities and, therefore, the membership structure.
In this stage, there is need to review the structures and formulate the organisation culture and procedures. With more than 480 members reached through the varied activities that have enhanced membership growth including the 20 executive members

• The membership is diverse, ranging from students, newly qualified Senior Nurses and Midwives and some retired generals. Members with varied experiences, including managers, aspiring leaders, and academic and project managers in global health initiatives. The design of activities will vary from each stage in order to be inclusive and promote the diversity in Nursing.
The membership WhatsApp messenger group, which is a closed social platform is used for shared learning and support. It remains an active and vibrant platform with over three hundred members discussing issues that may arise in the local news and how this affects our practice, and any matters arising in the work place. It is a free supportive space.
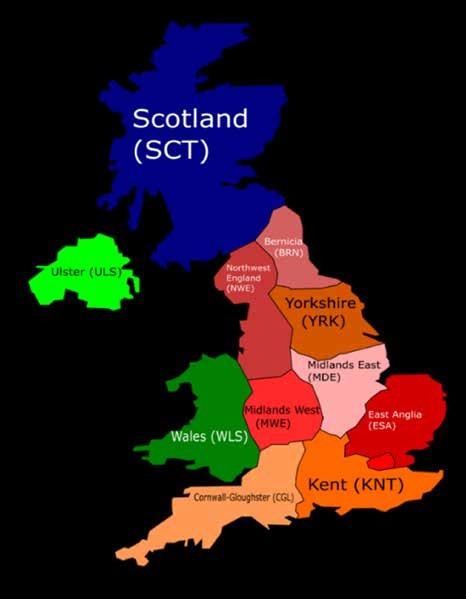
• To enhance membership engagement the structure of the association has been reviewed. The regional clusters are soon to be increased from four to six with an additional Scotland, and Northern Ireland. Experienced members will rotate as moderators in the joint interactive sessions.
Workplace integration is highly related strategy to increase retention rates reasonably and can be used by the NHS to decrease shortages and improve work experiences for BAME HCPs. Jabali network has a strong track record of developing nursing and midwifery leaders combined with the experience and knowledge of governance capable of improving patient and service outcomes. Through the partnership with the UNMA-UK, we will support the linking of qualified Ugandan diaspora clinical leaders in the NHS and social sector to advance into managerial positions.

To strengthen the governance of the association plans are underway to increase members participation in decision making, be conscious oriented equitable and inclusive in order to maintain transparency and accountability. A strategic consultant has reviewed the association governance structure. Good governance includes identifying a vision, developing a strategy, selecting and supporting a leadership to deliver that strategy, assurance that progress is being made. Membership is required to participate in this process in the consolidation phase.
There is significant variation in the extent to which research activities and engagement is embed across the NHS.
The association is keen to explore suggestions from members on bespoke research proposals that are unique and beneficial to our community members and the general public.
When faced with challenges and limitations, the leadership must know that the activities make a difference and explore means to make them sustainable.

• Vaccination drive for BME healthcare workers
The association also has proved that it can provide a strategic base for other healthcare departments to engage with the grassroots workers and delivery services as an accessible venue like the Covid champion drive. Our first promotion video of the vaccines for health care professionals was wifely received and successful.
• Stakeholders engagement
The association has continued developing active partnerships with other diaspora communities throughout the year. This includes the newly formed BME N&M Consortium, which is congratulated on getting the nurses’ voices recognised at the national level.
There are several external engagements that are being embedded in the phase for continuity of the activities.
• Shared learning
We are also pleased to continue developing learning opportunities such as the monthly webinars and delivery of community outreach. Therefore, we look forward to continuing to take our skills and services beyond the confines of the association.

Co-founder and Inaugural Vice President UNMA-UK Primrose Magala, made history of becoming the first-ever Ugandan to be awarded The Freedom of the City of London by the Master of The Worshipful Company of Spectacle Makers, on Thursday 14th September 2023.
There association has mainly utilised one stream of financial income from the Chief Nursing Officer (CNO); small grants project that Florence Nightingale Foundation (FNF) has been managing.
The funds have been used to complete the foundation stage of the association implementation and growth of membership. Reports have periodically been submitted to FNF as required. We were extremely pleased to have been awarded these small grant funds. The initial funds were used to launch and complete the first phase of the association and initial consolidation phase.Through initiatives such as the mentorship program, the mentors facilitated the support sessions for professional nursing development by exploring individual mentees’ strengths and weaknesses. This has proved to be very useful for both the mentors and mentees.
The association has encountered a few challenges as a growing organisation.
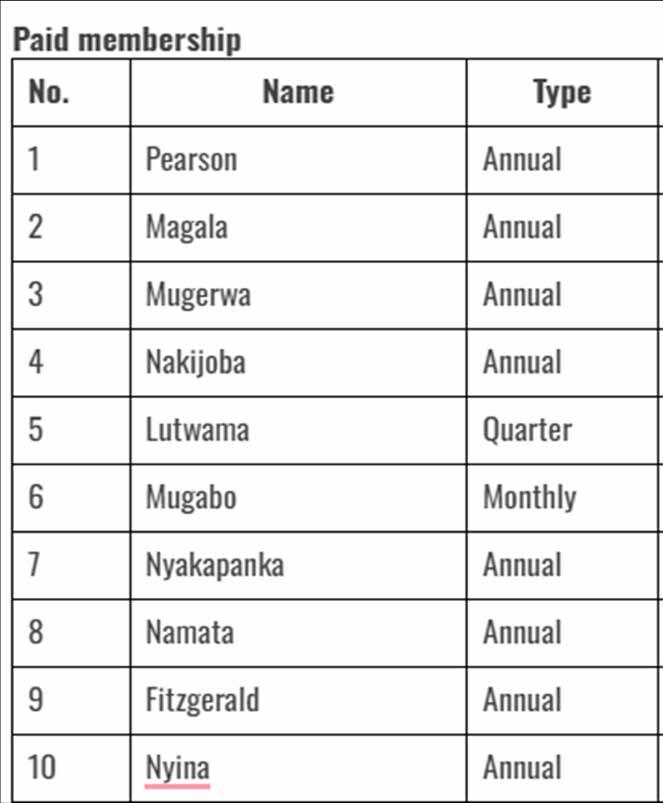
Membership registration and understanding - As a volunteer grassroot organization, which relies on voluntary income, we note with concern the low membership number. Given the benefits of the association, it is important for all members to actively be involved in the association activities in order to gain the full benefits. For sustainability, although the varied activities have enhanced membership involvement and engagement, this has not translated to formal registration as paid membership.
As of March 2023, only ten members had fully obliged to the registration as paid members. The benefits for membership will be continually reviewed to continue defining the benefits of the association to the Individual, Organisation and wider profession through the consolidated process.

Teamwork – The association formation phase has been successful with a number of achievements including enhanced stakeholder engagement, varied activities to promote membership engagement however, the team has gone through some challenges including inability to cohesively work together. Most of the initiatives, project implementations and management have been solely left to the President Elizabeth, to initiate, coordinate and deliver. Although attempts to use delegation tools have been utilized, three need to be a re-boast team spirit that brings together all members to participate and support in the delivery of the initiatives and projects. The value of the association to members is evident and needs to be continually emphasised. The benefits of teamworking clearly needs to be highlighted to bring to focus the supportive and corporative joint efforts.
Registration – One of the initial items identified in the formation phase was the importance for the association to register its legal structure as a charitable organisation. However to the nature of the main beneficiaries the application was rejected. It is imperative that the objectives of the association are reviewed in order to meet the criteria of the charitable status.
Understanding Governance - Governance is the process of making and enforcing decisions within an organization or society. It is the process of interactions through the laws, social norms, power (social and political) or language as structured in communication of an organized society over a social system (family, social group, formal or informal organization, a territory under a jurisdiction or across territories). Good governance adds value. It is lean, transparent and ethical. Good governance enables organisations to build a sustainable, better future for all. The lack of understanding of members’ obligations and rights, as well as the callous attitude has lead to barriers to good governance.
The ten principal themes that illuminate the different aspects of good governance include:-
• Clarity of purpose, roles and behaviours –‘what is the point of this organisation?’ The purpose of the organisation, and the vision set by those that govern it to support the achievement of that purpose, is the starting point for any system of good governance.
• Application of principles – The principles driving an organisation must be of fundamental value, understood by all users and reflect the organisation’s purpose
• Effective external and internal relationships - issues with communication between those who run the organisation and members
• Transparency and public reporting – Openness builds confidence and early disclosure supports early improvement. A mature organisation will have empowered staff who welcome comments, who apologise when things go wrong and respect users’ expectations that things will be put right.
With the strong exemplary leadership of the association, the formation phase has been successfully completed. The visibility of the Ugandan Nurses in the UK has gained a lot of traction and will continue to work together with the stakeholders.
The next consolidation stage is where the association is going through many formalities, adapting our policies, understanding our unique position and identifying our bespoke organisation culture. The acquisition of knowledge and skills, comes independence and conflict.
It is therefore important to engage in the consolidation process with passion and awareness of these facts as we continue to enhance the objectives, and enable organisation growth.
The rotation of activities to all regional clusters as hosts for the activities such as the anniversary celebrations, annual Free Health Promotion events and pastoral workshops, will enable the continued membership engagement.
Archibong, U. and A. Darr., (2010) The Involvement of Black and Minority Ethnic Staff in NHS Disciplinary Proceedings. ed. C. f. I. a. Diversity. Bradford: University of Bradford.
Archibong, U.E., Eshareturi, C., Mcintosh, B., & Kline, R., (2019) Black and Minority Ethnic: Disproportionality in disciplinary proceedings – Recommendations.
Atuhaire, R., & Kaberuka, W. (2016). Factors contributing to maternal mortality in Uganda. African Journal of Economic Review, 4(2). Retrieved from https://www.ajol.info/index.php/ajer/article/ view/136040
Beech, J., Bottery, S., Charlesworth, A., Evans, H., Gershlick, B., Hemmings, N., Imison, C., Kahtan, P., McKenna, H., Murray, R., & Palmer, B., (2019) Closing the gap: Key areas for action on the health and care workforce. Nuffield Trust, The King’s Fund, Health Foundation. www.nuffieldtrust.org. uk/research/ closing-the-gap-key-areas-for-action-on-the-health-and-care-workforce [Accessed 5 September 2022].
Böhret, I. (2018). Maternal Mortality in Uganda. https://doi.org/10.13140/RG.2.2.16930.07361
Buchan, J., Charlesworth, A., Gershlick, B., & Seccombe, I., (2019) A critical moment: NHS staffing trends, retention and attrition. The Health Foundation. www.health.org.uk/publications/reports/acritical-moment [Accessed 20 August 2022].
Buchan, J., Gershlick, B., Charlesworth, A. and Seccombe, I., (2019) Falling short: the NHS workforce challenge London: The health foundation.
Chaudhry, F.B., Raza, S., Raja, K.Z., and Ahmad, U., (2020) COVID-19 and BAME health care staff: Wrong place at the wrong time. J Glob Health.10(2):020358. doi:10.7189/jogh.10.020358 [Accessed 7 August 2022].
Coker, N., (2001) Racism in Medicine: An agenda for change. London: Kings Fund.
Dayan, M., Fahy, N., Hervey, T., McCarey, M., Jarman., H., and Greer, S., (2020) Understanding the impact of Brexit on health in the UK [Research report]. Nuffield Trust.
Department of Health, (2013) The NHS Constitution for England. ed. D. o. Health. London: Department of Health.
Dolton, P., Nguyen, D., Castellanos, M. and Rolfe, H., (2018) BREXIT and the Health & Social Care Workforce in the UK. Report to the Cavendish Coalition, NIESR (forthcoming).
Ford, M., (2020) BME nurses “feel targeted” to work on Covid-19 wards. Nursing Times.
Kline, R., (2014) The snowy white peaks of the NHS: a survey of discrimination in governance and leadership and the potential impact on patient care in London and England. Available at: https:// www.england.nhs.uk/wpcontent/uploads/2014/08/edc7-0514.pdf [Accessed 01 January 2022].
Likupe, G. and Archibong, U., (2013) Black African nurses’ experiences of equality, racism, and discrimination in the National Health Service. Journal of Psychological Issues in Organizational Culture, 3(S1), pp.227-246.
Likupe, G., (2015) Experiences of African nurses and the perception of their managers in the NHS. Journal of nursing management, 23(2), pp.231-241.
Marangozov, R., Williams, M. and Bevan, S., (2016) Beyond Brexit: Assessing key risks to the nursing workforce in England. Institute for Employment Studies. Retrieved from https://www. employmentstudies. co. uk/resource/beyond-brexitassessing-key-risks-nursing-workforce-england.
Nagpaul, C., (2020) The disproportionate impact of covid-19 on ethnic minority healthcare workers. The BMJ opinion. https://blogs.bmj.com/bmj/2020/04/20/chaand-nagpaul-the disproportionateimpact-of-covid-19-on-ethnic-minority-healthcare-workers/ [Accessed 9 October 2022].
National Audit Office. (2020) The NHS nursing workforce. National Audit Office. https://www.nao. org.uk/reports/nhs-nursing-workforce/ [Accessed July 26 2022].
Newland, K. and Patrick, E., (2004) Beyond remittances: the role of Diaspora in poverty reduction in their countries of origin, a scoping study by the Migration Policy Institute for the Department of International Development. Migration Policy Institute.
NHS Digital, (2021) NHS Workforce Statistics https://digital.nhs.uk/data-and information/ publications/statistical/nhs-workforce-statistics [Accessed 10 March 2022].
Office for National Statistics (ONS): Coronavirus (COVID-19) related deaths by ethnic group, England and Wales: 2 March 2020 to 10 April 2020, 7 May 2020 https://www.gov.uk/government/ publications/ons-coronavirus-covid-19-related-deaths-by-ethnic-group-england-and-wales-2march-2020-to-10-april-2020-7-may-2020 [Accessed 4 May 2022].
Tropical Health and Education Trust (THET) (2021) Partnership for global health; Experts in our midst Recognising the contribution NHS diaspora staff make to global health, August 2021 report.
Truth, A.U., (2013) No health without a workforce. World Health Organisation (WHO) Report, pp.1-104.
Wojczewski, S., Poppe, A., Hoffmann, K., Peersman, W., Nkomazana, O., Pentz, S. and Kutalek, R., (2015) Diaspora engagement of African migrant health workers–examples from five destination countries. Global health action, 8(1), p.29210.
World Health Organisation/Organization for Economic Cooperation and Development (WHO/ OECD), (2010) International migration of health workers. Improving international cooperation to address the global health workforce crisis. Paris: OECD. https://www.who.int/europe/aboutus/partnerships/partners/organisation-for-economic-co-operation-and-development-(oecd) [Accessed 9 July 2022].
These are initiatives/projects and or businesses organised and run by members and collaborative partners of the association and have supported various activities during this period.






Some of the webinars organised and facilitated by UNMA-UK members

Co-founder and Inaugural President, Elizabeth Pearson at International Council of Nursing, July 2023 Montreal, Cananda.

UNMA-UK Core leadership team, organising committee and diaspora leaders at the 3rd Anniversary celebration, July 2023 with Patron, Ms Nancy Jirira; Dr Joan Myers, OBE; Lord Mayor of Oxford; CNO Oxford; and our Guest of Honour Marjorie Neasham Glasgow BEM, His Majesty’s Lord-Lieutenant of Oxfordshire
Chief Guests of the 3rd Anniversary celebration, July 2023.

Some members at the Annual community promotion event in Oxford, May 2023.

Some of the webinars organised and facilitated by UNMA-UK members

Some of the webinars organised and facilitated by UNMA-UK members

Some of the webinars organised and facilitated by UNMA-UK members


Some of the webinars organised and facilitated by UNMA-UK members

and Inaugural


For the next generation ....

Co-founder Elizabeth Pearson meets the then Prince and now His Majesty King Charles III at Buckingham Palace for the commonwealth, June 2021

Members attending a meeting, 2021