Medical record




























Assessment & Plan Time to Confront the Public Health Needs of Berks County






INSIDE:
































































Adolescent Mental Health: What Can We Do to






Address the Stress?


Update of Prostate Cancer










BCMS Bylaws Changes























SPRING 2023 BERKS COUNTY
Your Community Resource for What’s Happening in Healthcare
MEDICAL SOCIETY
Medical record
A Quarterly Publication
To provide news and opinion to support professional growth and personal connections within the Berks County Medical Society community.
Berks County Medical Society
MEDICAL RECORD
D. Michael Baxter, MD, Editor Editorial Board
D. Michael Baxter, MD
Lucy J. Cairns, MD
Shannon Marie Foster, MD, FACS
Raymond C. Truex, Jr., MD, FACS, FAANS

Jillian Ventuzelo, DO
T. J. Huckleberry, MPA
William Santoro, MD, FASAM, DABAM
Contents
Features
10
The Report from the Berks County Public Health Services Study: Where Do We Go from Here?
7 Guest Editorial: A Step Forward for Public Health
15 Adolescent Mental Health: What Can We Do to Address the Stress?
Berks County Medical Society Officers
Jillian Ventuzelo, DO President
William Santoro, MD President Elect
Kristen Sandel, MD Chair, Executive Council
Ankit Shah, MD Treasurer
Jin Xu, MD Secretary
Michael L. Haas, MD
Immediate Past President
T. J. Huckleberry, MPA Executive Director
Berks County Medical Society
Phone: 610.375.6555 | Fax: 610.375.6535
Email: info@berkscms.org www.berkscms.org
The opinions expressed in these pages are those of the individual authors and not necessarily those of the Berks County Medical Society. The ad material is for the information and consideration of the reader. It does not necessarily represent an endorsement or recommendation by the Berks County Medical Society.
Manuscripts offered for publication and other correspondence should be sent to 2669 Shillington Rd, Sinking Spring, PA 19608, Ste 501. The editorial board reserves the right to reject and/or alter submitted material before publication.
The Berks County Medical Record (ISSN #0736-7333) is published four times a year by the Berks County Medical Society, 2669 Shillington Rd, Sinking Spring, PA 19608, Ste 501. Subscription $50.00 per year. Periodicals postage paid at Reading, PA, and at additional mailing offices.
POSTMASTER: Please send address changes to the Berks County Medical Record, 2669 Shillington Rd, Sinking Spring, PA 19608, Ste 501.
SPRING 2023
18 Prostate Cancer: Current screening recommendations, diagnostic approaches, and management of localized disease
21 Reading Berks Science and Engineering Fair 2023: Berks County Medical Society Health and Science Awards
Berks County Medical Society BECOME A MEMBER TODAY! Go to our website at www.berkscms.org and click on “Join Now”

22 Disability Insurance Can be Key for Physicians
24 A Higher Purpose Close to Home: Free Clinic Opening a Reading Satellite
26 Music as a Relaxing Interlude to a Successful Medical Career: An Introduction to the Berks Sinfonietta Chamber Orchestra
34 Foundation Partners with WellSpan to bring BMWC Youth Summit to Fruition
in every issue
3 President’s Message
5 Resident Rounds
6 Student Vital Signs
8 Editor’s Notes
27 Compass Points
Content Submission: Medical Record magazine welcomes recommendations for editorial content focusing on medical practice and management issues, and health and wellness topics that impact our community. However, we only accept articles from members of the Berks County Medical Society. Submissions can be photo(s), opinion piece or article. Typed manuscripts should be submitted as Word documents (8.5 x 11) and photos should be high resolution (300dpi at 100% size used in publication). Email your submission to info@berkscms.org for review by the Editorial Board. Thank YOU!
Hoffmann Publishing Group, Inc., 2669 Shillington Road, #438, Sinking Spring, PA 19608 www.Hoffpubs.com
For Advertising Information & Opportunities Contact: Alicia Lee 610-685-0914 x210 Alicia@Hoffpubs.com Sherry Bolinger 717-979-2858 Sherry@Hoffpubs.com
BERKS COUNTY MEDICAL SOCIETY
William Santoro, MD FASAM, DABAM Chief, Section of Addiction Medicine, Reading Hospital/ Tower Health President

Dear BCMS Member,
When I was asked if I would be willing to serve as President of Berks County Medical Society, I did not realize that I would be serving during the 200th year of the society. Organized in 1824, the Berks County Medical Society was the first medical society in Pennsylvania outside of Philadelphia. Dr. Isaac Hiester was elected president by unanimous vote of the assembly. He remained president of the society for the next 24 years.
Today, 200 years later, I am humbled to follow in his footsteps and, frankly, thankful that my term will be significantly shorter than his. Serving as president of this renowned society during any year is both an honor and a privilege, however, to do so during such a milestone, in my mind, adds an extra layer of responsibility.
When I accepted the nomination and the dust settled, I was asked what I thought I would like my term to concentrate on. Those who know me, know that my chosen field within medicine has been Addiction. Those who know me also know that I enjoy running. Of course, everyone assumes that my term would be highlighted with an emphasis on Addiction and wellness. While this will likely be true, I am hoping to expand that vision further.
“May you live in interesting times,” an English expression that is claimed to be a translation of a traditional Chinese curse, comes to mind. While seemingly a blessing, the expression is wrapped in irony as life is typically better in “uninteresting times” of peace and tranquility than in “interesting times,” which are usually marred with trouble.
We are living in interesting times. I am not going to delineate the troubles that plague society today; that would be too easy, and the list would be too long. I would rather focus on the solutions. Problems are always easy to describe and lament. Solutions take thought and vision.
My goal is to demonstrate, by action, that especially today the Berks County Medical Society is a relevant and important organization. I hope to show it is a Society every member is proud to be a part of; a Society every member would question why any provider would choose to not be a member.

Being active in the Berks County Medical Society the past number of years, most recently the past two years as president elect, I have seen a slow, but steady, decrease in the number of members. Each year I asked myself, why? Each year I came up with a reason… or an excuse. That’s when I realized I was focusing on the problem, when I should be focusing on the solution. We have often heard it said the best way to solve a problem is to first understand the problem. While I usually agree with this philosophy, sometimes we need to take the advice of the military and understand an army that waits until it is perfectly well prepared will never deploy.
We live in the most advanced country in the history of the world and yet the healthcare we deliver often comes up short of countries less fortunate than ours. I believe it is time that we each take a good look at ourselves and ask how we can be part of the solution. Whether or not we believe healthcare should be a universal right is irrelevant. We must, as physicians, nurse practitioners, and physician assistants, always strive to deliver the highest quality care to every person. We need to recognize that we are a team, regardless of the background that brought us to this point… medical school, nursing school, or physician assistant school. We are a team regardless of our specialty… medical, surgical, or
continued on next page >
P resident ’ s M essage
SPRING 2023 | 3
Confidence for the long term.
President’s Message
continued from page 3
behavioral health. Collaboration, cooperation, and mutual respect are the qualities of which winning teams are made.


As we move through our 200th anniversary year we need to both look back over our history and look forward to our future. Doing this we will celebrate with multiple events. We anticipate having our annual Drug Take Back Day, the Installation of Officers, the Pat Sharma Scholarship Day, Early Career & All Members Day at the Reading Phillies, Legislative Day, and the House of Delegates.
When our society first came to being in 1824, all that Berks County had was a handful of individual practicing physicians. Berks County did not even have a hospital. Today we have five inpatient hospitals, multiple health systems, hundreds of medical offices, along with over 3,000 practicing physicians and direct care providers.
Our future is bright with our local Penn State connections and the Drexel University College of Medicine, a world-renowned medical school, training our society’s future physicians. Many of these students will go on to help fill the residencies of our local Health Systems. Many of those residents will go on to become practicing physicians in our communities. And many of those practicing physicians will become members and leaders of the Berks County Medical Society. I am hoping that the Society can celebrate
with events such as a Resident’s Day and a Medical Student’s Day. With the Drexel College of Medicine Tower Health Campus well now established, I think it is important to include the medical students in our upcoming plans and celebrations. I look forward to organizing events coordinated with the medical school and their students.
Looking to the future I think it is important for the Berks County Medical Society to advocate to our elected officials for a Berks County Department of Health. An independent Department of Health would help pave a course to improve the health of all Berks Countians. It could partner with the Berks County Medical Society, hospitals, and local providers to establish a communitybased health resource network that could assist residents impacted by any healthcare issue.
I hope each of us takes the time to appreciate the interesting times in which we live. Whether these interesting times are a blessing or a curse, I believe is truly up to us. What we pursue and how we respond will determine whether these interesting times in which we live are a blessing or a curse. It is important to mark, and celebrate milestones like our 200th Anniversary, which remind us who we are and who we may yet become.
4 | www.berkscms.org
Service, Performance.
• connorsinvestor.com
Integrity,
610-376-7418
Our long-term perspective and counseled insight provide the confidence investors need in today’s challenging environment. As a registered investment advisor, our fiduciary responsibility is only to you and the best interests of your investments.
Count on our qualified professionals for the trust, tenure and talent you can take confidence in—for the long term.
Resident Rounds
by Hannah Thompson Herring, DO
My name is Hannah Thompson Herring, and I am currently a second year Obstetrics and Gynecology resident at Tower Health/ Reading Hospital. I am so excited to be starting a new column, “Resident Rounds,” which will serve as an avenue to highlight day-to-day physician responsibilities and address common healthcare issues.
I am originally from Walkertown, NC – a small town in the Piedmont Triad. Although a true “Tarheel” at heart, I moved to Lynchburg, VA to attend undergraduate at Liberty University. While at LU, I received my Bachelor of Science in Biology and Chemistry and a Master of Science in Biomedical Sciences. I then attended Liberty University College of Osteopathic Medicine for medical school.
Throughout medical school I was captivated by the medical complexity and intricacies of all aspects of healthcare. Yet, I knew that I desired a surgical subspecialty, but also valued continuity of care and building lasting trusting relationships with patients throughout varied stages of life. During my last rotation of medical school, I finally was able to find a field that encompassed all the things that I desired in my medical career, OBGYN. Whether delivering babies
on labor and delivery, performing surgical procedures in the operating room, or counseling patients in the office, I enjoyed the variety as it allowed for new experiences and challenges and provided opportunities for continued professional growth and development.
After graduation, I plan to pursue private practice as a general obstetrician and gynecologist to provide up-to-date, comprehensive, and compassionate medical care to my patients. I also hope to continue to participate in resident and medical student education and provide evidencebased education on all aspects of women’s health to my patients.
Outside of the hospital, you can find me clipping in for a Peloton class or going for long walks around the Reading Museum. But my favorite way to spend my spare time and days off work is cuddled on the couch with my husband, 7-month-old son, and mini golden doodle.
Over the next few years, I hope you will read along as I share my personal experiences as a resident facing the challenges and opportunities of a long and fulfilling medical career.

SPRING 2023 | 5 M edical R eco R d F eatu R e
Student Vital Signs
 by John LeMoine, MS II Drexel
by John LeMoine, MS II Drexel
There exists a universal longing to contribute and make a difference in the lives of others. It is a grounding yet fulfilling sensation to see in someone’s eyes—whether it be a loved one, a friend, or a stranger in need—that you have established a connection and made their day better.
Contribution to others does not have to be grand; rather, it is often the small interventions that make the most difference. To quote Gandalf the Grey, it is the “everyday deeds of ordinary folk that keeps the darkness at bay. Simple acts of kindness and love.”
Every medical student and future physician is different, but I can confidently vouch that all my classmates at Drexel College of Medicine are eager to assist the public at this exciting turning point in our medical training.

After two years of in-classroom academic training, the inaugural class of roughly 40 students at the West Reading medical school campus have completed their Step 1 examination, which is the first of three boards exams required to become a fully licensed physician. With the passing of Step 1, students will be joining the abundant healthcare staff at Reading Hospital in May, where we will observe and assist doctors in various departments of the hospital. This process allows students not only to learn the practical side of
medicine, but also to explore the different specialities in medicine, in the hope of choosing our own careers in our fourth year.
Sure, we all enjoyed the first two years of school. We studied the intricacies of every disease-causing bacteria, virus, and fungus. We explored how every organ behaves normally, how they behave abnormally, and how to remedy the abnormal. But what most medical students long for the most is the opportunity to apply their knowledge and skills in a patient setting.
The goal of the patient-doctor conversation is to communicate ideas about health and disease in a way in which both parties, patient and physician, can understand each other’s perspective. However, medicine is a language in itself, which can make it difficult to comprehend. As medical students, one of our responsibilities is to spend extra time with patients, facilitating this comprehension. After all, accepting and understanding one’s own condition is an essential first step for a better prognosis.
In the near future, we are looking forward to connecting with patients of Berks County, listening to their concerns, and communicating in a way that is beneficial for all.
6 | www.berkscms.org
M edical R eco R d F eatu R e
University College of Medicine/Tower Health Campus
Guest Editorial: A Step Forward for Public Health
 by Kevin K. Murphy, President, and Monica Reyes, Vice President for Programs and Initiatives Berks County Community Foundation
by Kevin K. Murphy, President, and Monica Reyes, Vice President for Programs and Initiatives Berks County Community Foundation
In March, the Berks County Commissioners released a study exploring options for strengthening our local public health infrastructure. We commend them for their foresight on this issue. Now is the right time to ask how Berks County can ensure public health efforts are directed at the local level, and not subject to the whims or bureaucracy of federal and state health departments managed by people who don’t live here or have a pulse on our community.
The report released by the commissioners suggests adding key positions to oversee public health efforts and to ease the coordination of task forces that already exist around key issues like the opioid epidemic and gun violence. By directing these efforts at the county level, we can be sure any suggested interventions are tailored to the needs of Berks County’s rural, suburban, and urban residents.
While it’s easy to assume the need for more robust public health infrastructure arose as a result of the Covid-19 pandemic, the need was always there, just brought to light when the pandemic struck. Our local leaders – in our communities and our schools – sought answers from county officials, who in turn were forced to rely on often slow or contradictory state and federal responses. In the Pennsylvania counties with a stronger public health infrastructure, trustworthy information and guidance flowed faster and was tailored to local needs.
For nearly thirty years, the Community Foundation has managed charitable funds that provide grants for community health initiatives, most notably from the Community General Hospital Healthcare Fund and the Home Healthcare Foundation Fund. Through that work, we’ve seen the tireless efforts of our healthcare systems and nonprofits to fill the public health gap in our community. The time is now to support and enhance those efforts through the establishment of a public health infrastructure that serves all residents and allows our county to take the lead on both day-to-day public health issues and to be at the ready when another health emergency strikes. It’s the right time, and the right thing to do for Berks County.
F eatu R e
SPRING 2023 | 7
by D. Michael Baxter, MD, Editor

BERKS COUNTY PUBLIC HEALTH





The Centers for Disease Control and Prevention (CDC) reports that for the second year in a row life expectancy has declined in the United States even as it has increased for most other industrialized nations. While one would expect an impact from the devastating losses of the COVID-19 Pandemic (1,128,404 deaths as of mid-April 2023), this trend actually began much earlier, in 2010. Most alarmingly, all-cause mortality among children and adolescents (ages 1-19) has increased in recent years. The startling fact is that we are witnessing a most unusual demographic for our country—life expectancy for our current youth will be less than that of their parents.


Even though we have made remarkable progress in the care of premature newborns, treatments for childhood cancers and other diseases, the fact remains that mortality rates are rising for our children and youth. As one author in a recent Journal of the American Medical Association article states, “A nation that begins losing its most cherished population–its children–faces a crisis like no other.” (JAMA, March 28, 2023: Vol. 329 (12), 975-976). The causes of this tragic trend are what might be called “Social Disease Disorders”—homicides and suicides

8 | www.berkscms.org e dito R ’ s N otes
LET US BE YOUR GPS.

Our goal is to reduce stress, enabling you to feel reassured and in control through the transitions you experience on your journey. If you have questions about investment management, your plan for retirement, or a recent change in your financial picture, we are ready to help you transition well. www.domaniwealth.com


(primarily from guns), drug overdoses, and unintentional injuries (many due to automobile accidents).
In the Winter edition of the Medical Record, we addressed the topic of “Gun Violence” and the devastating effect the readily available supply of guns, including assault weapons, has on our society. In 2023, there have already been nearly 150 mass shootings in the US including one at a Christian elementary school in Nashville claiming the lives of 3 children and 3 adults, at a bank in Louisville, KY, which claimed the lives of 5 adults, and the death of 4 teenagers at a birthday party in Alabama. There is no end in sight to such violence which is often targeting our youth. In that same issue of the Medical Record, we also focused on the growing threat of lethal Fentanyl overdoses across our country, including here in Berks County.
In this Spring issue we continue to focus on topics which have a dramatic effect on health and the delivery of health care to our population. An article on “Adolescent Stress” describes how the COVID-19 Pandemic and associated isolation only made these
mental health problems worse for our youth and places them at increased risk for harm.
In addition, our cover story highlights findings from the recent Berks County Public Health Services Study report. Notably this extensive study describes increased health risks for our county residents and the need for additional health services. Perhaps the most vulnerable are the estimated 34,000 without health insurance. Thus, not coincidentally, this edition also describes the expansion of services of the Western Berks Free Medical Clinic into the city of Reading and appeals for volunteers to help address the health of this underserved population.
As we face these challenges, we are reminded that the Berks County Medical Society guiding Compass not only promotes Education, Professionalism and Congeniality among our members but also Advocacy to improve health and make this a better community for all.
SPRING 2023 | 9
Domani Wealth, LLC (“Domani”) is an SEC registered investment adviser with its principal place of business in Lancaster, Pennsylvania. Domani and its representatives may only transact business in states where they are appropriately notice-filed and registered, respectively, or exempt from such requirements. For information pertaining to the registration status of
please contact the SEC or
Domani,
the state
securities regulators for those states in which Domani maintains a notice-filing.
Thomas K. Williams, CFP®, CPA tom.williams@domaniwealth.com 610.927.4685
Michael J. Dinan CFP® michael.dinan@domaniwealth.com 610.927.4685
The Report from the Berks County Public Health Services Study: Where Do We Go from Here?
by D. Michael Baxter, MD,
Does Good Health Matter?
Of course it does, whether we take it for granted in our younger years, or we hold onto it tenaciously as we age, it remains all important. Many factors contribute to health including genetics, personal behaviors, and environmental risks. In addition, societal factors defined as Social Determinants of Health, those conditions where people are born, live, work, learn, play, worship, and age that affect a wide range of health and quality of life outcomes, can have a significant role in our health. We learned all too clearly during the recent COVID-19 pandemic that such factors can have a disproportionate effect on disease risk and death.
Health impacts communities as well. In general, the healthier the residents of a community, the more prosperous and economically stable that community will be. High quality health care institutions and ready access to affordable health care are important prerequisites for such communities as is a strong public health infrastructure, coordinating, guiding, and implementing proven strategies to promote wellness and fairness in the delivery of health care.
Purpose of the Berks County Study
In November of 2021, the Berks County Commissioners initiated an RFP (Request for Proposals) for consultants to conduct a “Study for the Delivery of Health and Public Health Services in Berks County.” Several highly qualified vendors responded. The contract for this study was awarded in May of 2022 to Health Management Associates, Inc., of Philadelphia, a national research
and consulting firm which specializes in publicly funded health and human services policy. This group was asked to address the following:
• Assess the health and public health services in Berks County to identify opportunities to ensure that all residents have resources and opportunities to pursue their highest level of health.
• Examine how the County coordinates and aligns crosssector action tied to public health that engages county residents, businesses, schools, community organizations, and government sectors.
• Ensure Berks County has community-informed information to assess how health care and public health services support county residents in improving health outcomes and health equity.

As the document states: This report aims to recommend steps for the County to be able to lead in public health emergencies as well as in preventing avoidable health conditions and closing health disparities.
On March 28th, 2023, the HMA team presented their findings and recommendations to the Berks County Commissioners. The full report in English and Spanish and a summary can be found at:
https://countyofberks.com/departments/commissioners/publichealth-services-study
This article presents a limited summary of their findings and recommendations.
10 | www.berkscms.org M edical R eco R d c ove R s to R y
FAAFP
Methodology Employed
The HMA consultants worked under the guidance of a fivemember team of County government officials and leaders of local community organizations. They reviewed and analyzed Pennsylvania state and Berks County statistics and health data and reviewed the Community Health Needs Assessment reports of both Reading Hospital/Tower Health and Penn State St. Joseph’s. They also compared Berks County health data to that of five adjacent counties (Chester, Lancaster, Lehigh, Montgomery, and York). In addition, they conducted focus groups with 81 members of the Berks Community including residents, front-line workers, and health program staff, while also interviewing key community leaders and health care stakeholders.
Key Findings and Comparisons
Table 1. Population Statistics (2020 US Census)
(all time since 2020)
Berks County in general compares favorably in leading causes of death except for a higher rate of stroke and COVID-19 deaths.
Berks residents self-report somewhat poorer on their health and a higher number of poor physical health days but compare favorably in regard to poor mental health days and low birthweight.
continued on next page >
The most notable differences in the demographic data were the number of Hispanic/Latino residents and fewer college graduates compared to both Pennsylvania and United States data.
Indicator Berks Pennsylvania United County States Asian 2% 4% 6% Black/African 8% 12% 14% American Hispanic/Latino 24% 8% 19% Multi-Racial 3% 2% 3% Other 1% 1% 2% White, Non-Hispanic 69% 75% 59% Median Household $69,272 $67,587 $69,021 income Percent in Poverty 13% 12% 12% Percent with Disability 10% 10% 9% (less than 65 years) Percent Under 18 years 22 % 21% 22% Percent Above 65 years 18% 19% 17% High School 88% 91% 89% Completion College Degree 26% 33% 34%
Indicator Berks Pennsylvania United County States Heart Disease 172.2 176.0 165.0 Cancer 156.9 161.0 152.5 Accidents 48.9 70.2 49.4 Stroke 46.5 36.5 37.6 Chronic Lower 33.9 37.1 40.9 Respiratory Disease Diabetes 19.3 21.0 21.5 Alzheimer’s 16.7 21.7 31.0 Kidney Disease 14.6 15.9 13.0 COVID 412.9 387.6 327.3
Table 2. Leading Causes of Death (rate per 100,000), 2017, National Center for Health Statistics
Indicator Berks Pennsylvania United County States Poor or Fair Health 20% 18% 17% Poor Physical 4.2 3.9 3.9 Health Days Poor Mental 4.6 4.6 4.5 Health Days Low Birthweight 8% 8% 8%
Table 3. Quality of life indicators. Berks County, 2022 (County Health Profiles)
SPRING 2023 | 11
The Report from the Berks County Public Health Services Study: Where Do We Go from Here?
continued from page 11
Berks County has a higher than the national average of adult smokers and slightly higher rates of adult obesity. In addition, Berks County has higher reported rates of STIs and a higher teen birth rate than Pennsylvania as a whole.
Berks County compares favorably with the US population for uninsured 8% vs 12%, however 8% of the 2020 census population of 429,342 leaves an estimated 34,350 local residents without health insurance. In addition, Berks County residents have access to fewer primary care physicians, dentists, and mental health providers than their Pennsylvania and US peers. Preventable hospital stays are also increased for local residents.
Leading Causes of Death
Heart disease (6)
COVID death (6) Stroke (6)
Chronic lower respiratory (6) Cancer (5)
Kidney disease (5)
Poor or fair health (6)
(4)
(4)
(1)
Health Rankings
Poor physical health days (6)
Premature death (5)
Low birthweight (5)
Physical inactivity (6)
Teen births (6)
Poor mental health days (4)
Health Factors and Behaviors
Adult smokers (5)
Adult obesity (5)
Sexually transmitted infection (5)
Primary Care Physician (6)
Food environment index (4)
Excessive drinking (4)
Access to exercise ops (3)
% Uninsured (4)
Healthcare/Clinical Care Access
Dentist (5) Mental Health Provider (5) Preventable Hospital Stays (6) Mammography Screening (5) Flu Vaccination (6)
12 | www.berkscms.org
Indicator Berks Pennsylvania United County States Adult smokers 19% 18% 16% Adult obesity 34% 33% 32% Food environment 8.7 8.4 7.8 indes (10=best access to healthy food) Physical inactivity 28% 25% 26% Access to exercise opportunities 79% 78% 80% Excessive drinking 19% 20% 20% Sexually transmitted infections (rate per 100,000) 535.9 481.9 551.0 Teen births (rate per 100,00) 20 15 19
Table 4. Health Factors and Behaviors, 2020
Indicator Berks Pennsylvania United County States Percent Uninsured 8% 7% 11% Primary Care 1,590:1 1,220:1 1,310:1 Physicians (ratio) Dentists 1,770:1 1,410:1 1,310:1 Mental Health 640:1 420:1 350:1 Providers Preventable Hospital 4,221 3,966 3,767 Stays Mammography 45% 47% 43% Screening Flu Vaccinations 55% 54% 48%
Table 5. Health care/Clinical Care Access, 2020
Domain Lowest outcomes Middle performing Best outcomes (Berks 5 or
(Berks 3 or 4) (Berks 1 or 2)
Table 6. Summary of Health, Mortality, and Access (per capita) Rankings, County Comparison
6)
Diabetes
Alzheimer’s
Accidents
One of the most revealing pieces of the report compared Berks County health data to that of five of our adjacent counties (Chester, Lancaster, Lehigh, Montgomery, and York). As Table 6 shows, with 1 ranked highest and 6 lowest, Berks County ranked 5th or 6th in most categories, 4th in a few and only 1st in the reported cases of Alzheimer’s Disease.
Other interesting data showed that while the city of Reading does have significant health issues, particularly in the conditions of smoking, asthma, and obesity, other areas of the county have higher rates of chronic heart disease and cancer. Also, it may be surprising to some that the city does not have the highest rate of uninsured but rather that distinction falls to the residents of the 19507-zip code in the western portion of Berks County.
In summation, the report states that when compared to state and national data, “Berks would appear to have a persistent pattern of poorer health behaviors and outcomes for most indicators.” In addition, the data indicates that poorer health outcomes are not confined to the city of Reading where, in fact, some indicators are more favorable, rather “public health is a countywide issue.”
Recommendations for Improving Public Health in Berks County
As the foundation for their formal recommendations, the HMA consultants established a set of “guiding principles” for establishing a Berks Public Health Model:
They based these on the recognition that health leaders and stakeholders in Berks County are committed to assuring the health of Berks County residents and an approach that:
• Coordinates public health services underway through government, health care, and other agencies.

• Provides one clear, trusted voice about public health threats, response, and concerns.
• Increases access to public health data for the public and key health partners.
• Identifies clear roles and responsibilities for public and private partners and reduces duplication of efforts.
• Improves the health of county populations that exhibit the greatest disparities.
• Ensures that prevention and wellness information and resources are accessible in both English and Spanish.
continued on next page >
As the premier Realtor in Berks County, Lisa Tiger uses her marketing, and extensive network to more quickly match buyers and sellers.
Lisa’s passion and tenacity combined with her sales and marketing skills have made her the most successful agent in Berks County. She would love to have the opportunity to share that success with you.
When you are ready to buy or sell, Team up with the Tiger!
Offers:
• Comprehensive outpatient evaluations conducted by a therapist trained in substance use disorders.
• A range of outpatient group counseling options for teens and adults.

• Individual counseling.
• Trauma Services.
• Critical support for family members.
• Specialized addiction program.
• Prevention and education programs.
• Recovery support for alumni.
SPRING 2023 | 13
WWW.CARON.ORG
Located in Wyomissing, Pennsylvania 845 North Park
Wyomissing, PA 19610 484-345-4670
CARON OUTPATIENT TREATMENT CENTER
Road
The Report from the Berks County Public Health Services Study: Where Do We Go from Here?
continued from page 13
Four Recommendations:
• Create a Berks County Health Director position to lead public health collective action and coordination and serve as a trusted communicator about public health information. The position would either be a county employee or an employee of a non-governmental agency, but in either case would report to the County Commissioners.
• Develop a new Berks County Public Health Advisory Panel to advise the Berks County Health Director and guide public health assessment, policy, and assurance activities. These will be uncompensated positions representing expertise in public and behavioral health.

• Support the establishment of a Healthy Berks Coalition to serve as a coordinating body for public health efforts in the county. The Public Health Director will coordinate or co-facilitate the Coalition’s activities. This coalition will include leadership from such organizations as the Berks Community Health Center, Tower Health/Reading Hospital, Penn State St. Joseph’s Hospital, United Way, the Hispanic Center, the Berks County Community Foundation, Co-County Wellness Services, Berks County mental and emergency services, schools, faith-based and other public and private organizations.
• Create a Berks County Health Analyst position to improve Berks County specific public health data completeness and accuracy and who will report to the Berks County Health Director. This position will: Identify data gaps, provide census tract/zip code level monitoring
of County residents’ health, support a strong response to pandemics or other public health emergencies and be a county employee or subcontractor.
Where Do We Go from Here?
This report is a detailed description of the status of the public health of Berks County and the challenges which lie before us. It is an excellent beginning, and our County Commissioners should be commended for initiating and funding this effort. There are important steps ahead and this study provides guidance. While the HMA consultants professed neutrality on the need and role for a County Department of Health, they did find considerable support for the concept among various county health leaders and constituent groups.
To be totally transparent, the Berks County Medical Society has officially called for the creation of a Berks County Department of Health in an editorial in the March 2021 winter edition of the Medical Record. However, the HMA consultants also identified concerns from others regarding the potential added costs and bureaucratic impediments of such an agency.
While that debate continues (including in the future pages of the Medical Record), this should not deter us. As the study demonstrates, we have significant health problems facing us in Berks County even when compared to our surrounding peer counties and these health concerns are indeed county wide. With the outline that this study provides, it is time to move forward to improve the health of everyone in Berks County and to meet whatever further challenges might lie ahead.
14 | www.berkscms.org
Being a huge extrovert trapped indoors took a toll on my mental strength and energy, and I slowly sunk into a depression. I didn’t recognize it at first. I felt broken. All the color and light spilled out of me, and I was a shadow of who I usually was. I lost passion for things I previously loved, stopped talking to close friends, then criticized myself for not being there for them, as I had made myself the therapist of the friend group while they were all struggling with their mental health too.
— Oluwakemi Ojikutu, 10th grade student, via email
Adolescent Mental Health: What Can We Do to Address the Stress?
by Steph Lee, MD, MPH, FAAP, Penn State St. Joseph’s Health Center
Poor mental health is a common theme I’ve seen as a pediatrician in downtown Reading. I’ve seen youth like Miss Ojikutu who started to struggle with their mental health for the first time, or others who were in therapy but whose mental health was worsening. It’s time we all come together and improve the health of our youth.
The mental health of adolescents has been deteriorating for the past decade – persistent feelings of sadness or hopelessness increased 40% between 2009-2019 for U.S. high school students. Since the pandemic, the situation has worsened – in 2021, more than 3 out of 10 high school students reported experiencing poor mental health during the COVID-19 pandemic. Nearly 60% of female students experienced persistent feelings of sadness or hopelessness, with Hispanic and multiracial students more likely than Asian, Black, and White students to have persistent feelings of sadness or hopelessness. And Black students were more likely than Asian, Hispanic, and White students to attempt suicide.
What I’ve seen with my patients mirrors what’s happening across the state of Pennsylvania. In the past year, about 120,000 youth (age 12-17) reported suffering at least one major depressive episode in the past year and over half, 55%, did not receive any sort of mental health treatment.

Adolescence is a critical time for youth to learn how to expand their social circles and establish identities outside of their family roles. Typical development for this age group was disrupted by the pandemic and preventive public health measures. These measures
continued on next page >
SPRING 2023 | 15
F eatu R e
Adolescent Mental Health: What Can We Do to Address the Stress?
continued from page 15
were necessary but have lasting effects that need to be addressed. One systematic review noted that during pandemics, stress, worry, and feelings of helplessness occurred in adolescents, as well as social and risky behavioral problems such as substance abuse, suicide, relationship problems, academic issues, and absenteeism from work.
What do adolescents think is causing poor mental health among their peers? Miss Ojikutu stated, “Many of the mental health issues that high school students battle come from us not knowing how to deal with our stress and anxiety. Whether it’s the constant horror of school shootings and gun violence, the overwhelming problems in the world, or even teenage drama, we don’t have time to actually process and deal with our emotions, and instead, have to push through and deal with our emotions as if nothing happened.”
It’s important for youth to have access to mental health professionals so they can learn how to process emotions in a healthy, safe way, without self-harm, and have an outlet for stressful situations that may need an outside perspective to resolve.
When it comes to the biggest investment in your lifetime, your experience is just as important as your agent’s. Over the last 40+ combined years in Berks real estate, the Eric Miller Team have delivered uncompromising honesty, integrity, attention, and tenacity, prioritizing their customers’ needs to give them the experience they deserve.


The Erics have mastered a blend of savvy negotiation, strategic problem-solving, and impactful marketing driven by a passion for their community. As Berks County natives, students, coaches, and playground leaders, the Erics know the area and market better than anyone. They join less than 0.5% of RE/MAX agents worldwide in the Circle of Legends, along with Hall of Fame and Lifetime Achievement status, and over $650 million sold.
You know the importance of trust and experience when it comes to making life-changing decisions. So do we.
Office: 610.670.2770
• Cell: 484.269.2394
EMiller@GoBerksCounty.com
BerksCountyUpscaleHomes.com
What can adults do to help youth get back to a healthy headspace?
• Get parents involved. A student in 12th grade, Danielle Radosh, suggested via email that parents be open to having discussions about mental health. “My generation is relatively comfortable discussing mental health issues. …However, it seems that sometimes parents are less comfortable talking about mental health and seeking treatment for their children. Some parents may be embarrassed or feel that they have failed.” Having open discussion about mental health normalizes it, just like other aspects of health.
• Encourage parents to give youth time to practice healthy coping skills. Miss Ojikutu shared how “I spent my summer mornings reading books, then the afternoons exercising, often by myself, focusing on myself, and refilling my happiness tank. I soon opened up to my friends again and set boundaries of how much of myself and my time I could give to them while still taking care of myself.”
• Talk to schools to see what’s available to improve. Recently, Governor Shapiro proposed a five-year $100 million block grant program for schools for mental health services for students and staff which could include school psychologists, counselors, or social workers. Research shows that the more students feel connected and supported at school, the less likely they are to have symptoms of depression or consider attempting suicide.
What can physicians do?
• Any specialty can send referrals and give information on local psychology resources.
• Make parents aware of the importance of taking care of mental health.
• Contact schools so they can also provide resources and follow up with parents on a more consistent basis.
With the right guidance from parents, schools, and mental health professionals, adolescents can learn to navigate their life again and overcome any mental health struggles.

16 | www.berkscms.org M edical R eco R d F eatu R e
“Eric is an efficient and courteous realtor who is attentive to each of his clients. His experience with and knowledge of our market are vital in helping sellers connect with appropriate buyers and in facilitating a smooth transaction for both parties. We couldn’t be happier with our choice of having him and his team represent us.” - Dr. Feaster



HoffmannPublishing.com • 610.685.0914 x201 Reach 75% of All Berks County Adults… Advertise in Berks 1st Magazine The Official Berks County Government Magazine Grow Your Business in Berks! Contact Tracy@Hoffpubs.com today for rates and advertising information. Reserve your space in the Summer/Fall 2023 issue by June 30, 2023. Published for the County of Berks, PA, Berks 1st is the County’s official full-color magazine, shar ing news about constituent services, events and timely and trending topics surrounding county services. Mailed by the County, Berks 1st is addressed directly to 87,646 residential addresses (60%
Spanish and English language digital versions will be available on the County’s website. Restoring Passenger Rail Service to Berks Connecting Berks to Broadband Celebrating 75 Years: Armed Forces Day Parade May 20, 2023 Rincón en Español Berks County, PA, Government News & Services Escaneé para leer! Scan to Read Online! SPRING 2023
to 70% of every household within many of the major regional municipalities), and into another 300 high-traffic locations.
Prostate Cancer: Current screening recommendations, diagnostic approaches, and management of localized disease
by Paulette C. Dreher, D.O., Center for Urologic Care of Berks County
Prostate cancer (PCa) remains the most commonly diagnosed cancer in men in the United States with more than an estimated 240,000 patients diagnosed with prostate cancer yearly.1 Greater than 60% of men are over the age of 60 with an average age of 67 years at the time of diagnosis. However, despite 1 out of 7 U.S. men being diagnosed with PCa, only 2.8% will have disease-related mortality. It is important to also consider individual risk estimation, as African American men have a 59% higher incidence than Caucasian men and carry a greater risk of more aggressive disease at diagnosis.
PSA & Prostate Cancer Screening
Prostate specific antigen (PSA) remains the mainstay of PCa screening. PSA was introduced in the late 1980s and subsequently contributed to a 70% increased incidence of PCa. However, PSA screening also resulted in a trend towards earlier diagnosis with 81% of patients presenting with localized disease as well as a decrease in PCa-related mortality of greater than 40%.2 PSA is a reproductive protein produced by the glandular tissue of the prostate with the goal of seminal fluid liquefaction. PSA is elevated in PCa due to the disruption of the glandular architecture, resulting in the loss of a basal cell layer and leeching of PSA. In fact, PCa cells typically make less PSA than normal prostate cells.
The accepted normal range of PSA remains 0-4ng/dl, but this value is also directly correlated with prostate size and can be adjusted for based on an accepted PSA density with less than 0.15 being favorable. Conversely, up to 15% of PCa may be diagnosed below the 4ng/dL threshold. False elevations of PSA can occur because of infection, inflammation, trauma and ejaculation. Thus, repeating a PSA after single elevation is an important part of prostate cancer screening and patient education and should be done under ideal conditions with 2-3 days of abstinence from activities that may spuriously increase PSA, such as bicycle riding, strenuous exercise, and sexual activity. Typically, 4-6 weeks is a sufficient time frame.
In 2012 the U.S. Preventative Task Force (USPTF) recommended against PSA screening with a moderate-high certainty that service benefit did not outweigh the harms and risks. This recommendation was applied to all men in the U.S. population regardless of age, race, and family history. As a result, there was a temporal increase in the stage of PCa diagnosis with many patients presenting with advanced disease.1
Current screening guideline recommendations consider patient age, life expectancy, and individualized risk based on family history {first degree relatives, multigenerational disease, family history of metastatic disease, or history of lethal adenocarcinomas (prostate, breast, ovarian, pancreatic)}, and race. Emphasis is placed on the importance of shared decision making between the patient and the physician.
The current American Urological Association (AUA) recommendations, which they acknowledge are based on low to moderate level evidence, are:
• Men <40 years should not be screened
• No routine screening in men 40-54 years at average risk
o Men 40-54 years at higher risk should be screened with PSA after shared decision-making conversation
• Men ages 55-69, recommended shared decision-making when deciding to undergo screening
• In men >70 years or any man with <10-15 years life expectancy PSA screening is not recommended
o Some men in excellent health 70+ may benefit from continued PCa screening
The guidelines also consider reducing the harms of screening. As such, a routine screening interval of two years or more may
18 | www.berkscms.org
M edical R eco R d F eatu R e
be preferred over annual screening with no decrease in associated disease-specific mortality, and even suggest that rescreening intervals can be individualized based on baseline PSA.3 The goals of screening are to identify high risk patients, to detect potentially lethal disease at an earlier stage, to decrease PCa-specific mortality and to decrease overall treatment burden.
Screening tests other than PSA, such as urinary and serum biomarkers, risk calculators and imaging, such as multiparametric MRI, are available and frequently utilized by urologists to help identify men at greater risk of harboring aggressive prostate cancer. As of yet, there is no conclusive data to suggest use of these secondary screening tools may reduce unnecessary biopsies while maintaining the ability to detect aggressive disease, but many urologists find them helpful in adjudicating elevated PSAs prior to biopsy.3
Role of MRI
Multiparametric MRI (mpMRI) imaging of the prostate allows for radiologists to evaluate and grade lesions identified within the prostate based on the Prostate Imaging Reporting and Data System (PIRADS). The goal of PIRADS is to delineate lesions suspicious for harboring clinically significant PCa. The guidelines state that the role of MRI (and other imaging modalities) is unproven in the primary screening process and as a result there is some variation of use amongst urologists.3 The PROMIS study concluded that using MRI to triage risk might allow 27% of patients to avoid a primary biopsy and result in the detection of 5% fewer clinically insignificant cancers. Additionally, data suggested that using mpMRI to direct subsequent TRUS biopsies would detect up to 18% more cases of clinically significant PCa.4 Similarly, the PRECISION trial found that clinically significant PCa was detected in 38% of mpMRI targeted biopsy patients vs. 26% of standard TRUS biopsy patients (p=0.005) and that fewer men undergoing mpMRI were diagnosed with clinically insignificant PCa.5
Prostate Biopsy
Given the current standard of care, prostate biopsy remains necessary for the diagnosis of PCa to be made although some centers are examining diagnosis directed by imaging alone. Transrectal
ultrasound guided (TRUS) prostate needle biopsy remains the most common approach to biopsy. Transperineal biopsy allows the needle to fire transcutaneous rather than transrectally and may minimize or eliminate post procedure sepsis, although perceived difficulty, lack of training, patient comfort, and barriers in efficiency have limited widespread adoption. Both transrectal and transperineal templates typically utilize 12 core samples. MRI-Ultrasound fusion biopsy uses software to combine imaging targets generated by the interpreting radiologist with live ultrasound and allows for the surgeon to target specific lesions (commonly those graded as PIRADS 4 and 5) within the prostate gland. Typically, patients undergoing targeted MRI fusion biopsy also receive a simultaneous standard template biopsy, although there is some debate regarding the omission of the standard template for these patients.
Management of localized prostate cancer
Upon receiving the diagnosis of prostate cancer, patients are riskstratified to guide management. Risk stratification may range from very low risk to very high risk and considers the Gleason score of the biopsy (histology), the volume of disease (number of positive cores and palpable nodules), and the PSA at diagnosis. Depending on risk stratification, management options may include active surveillance, radiation therapy, or surgery. Typically, other factors incorporated in treatment decisions include comorbidities, patient preferences, and life expectancy as commonly estimated using the Social Security Administration’s actuarial tables.
Active surveillance is considered for patients with very low risk, low risk, and favorable intermediate risk PCa. Active surveillance (AS) is a management strategy wherein men with known prostate cancer are serially monitored for disease progression with PSA (every 6-12 months), DRE (every 12 months), possible repeat biopsy (in 1-2 years or as dictated by changes in PSA, imaging or physical exam) and tissue-based genomic testing. The intent is that patients on AS may pursue definitive treatment should the clinical picture indicate disease stage, volume or grade progression, or per the patient’s preference.3 The decision to pursue AS involves shared decision making between patient and physician and considers the oncologic risks of disease progression, patient comorbidities, life expectancy and treatment harms.3 Active surveillance has been
continued on next page >
SPRING 2023 | 19
Prostate Cancer: Current screening recommendations, diagnostic approaches, and management of localized disease
continued from page 19
shown to be a safe and effective method of managing prostate cancer, and up to 2/3 of men on AS may avoid treatment altogether.
Surgical management offers a curative treatment for men with localized prostate cancer. Surgery consists of radical prostatectomy with or without pelvic lymph node dissection. Currently, laparoscopic robotic-assisted approach is the most common technique utilized in the United States. Robotic-assisted approaches may significantly decrease the morbidity of the procedure and allow for some patients to go home on the same day of their procedure. Surgery is appropriate for patients with clinically localized disease, no surgical contraindications, and with life expectancy greater than 10 years.
Radiation therapy also offers a potentially curative treatment for men with localized prostate cancer. The most common type of radiation therapy is external beam radiation (EBRT) that is delivered daily over the course of several weeks. Stereotactic body radiation (SBRT) is a higher dose of radiation over a shorter period that also may be offered to select patients. In patients with unfavorable intermediate, high risk, or very high-risk disease, additional imaging tests such as a bone scan, CT, MRI or PET scan are often warranted to ensure that the cancer has not yet spread, which may alter the treatment considerations. For patients with these risk stratifications, active surveillance is not an option due to high risk of progression and metastasis. In general, disease recurrence or progression is typically monitored using PSA surveillance.
However, in patients with significant comorbidities or decreased life expectancy the patient and physician may elect a watchful waiting or observation protocol, which typically involves waiting until a patient becomes symptomatic or PSA or imaging suggests imminent symptoms before pursuing palliative treatment. The goal of watchful waiting is to avoid the morbidity of treatment in patients for whom their life expectancy would preclude any benefit of treatment with curative intent.
There have been several landmark longitudinal trials performed to understand which patients may benefit most from definitive treatment. The PIVOT trial randomly assigned patients to surgery or observation and at 20 years of follow-up found no significant differences noted in death from prostate cancer (p=0.06) in patients undergoing surgery (7.4%) and watchful waiting (11.4%). Although notably surgery did reduce the risk of progression (40.9% vs 68.4%; HR 0.39, 95% CI 0.32-0.48) and treatment progression when compared to watchful waiting group (33% vs 59.7%, HR 0.45, 95% CI 0.36-0.56).5
The PROTECT trial examined 15-year outcomes in patients randomized to active surveillance, surgery and radiation. At 15 years there were no differences observed in PCa mortality across the groups (AS 3.1%, surgery 2.2%, radiation 2.9%, p=0.53).7 Not
surprisingly, more metastatic disease was observed in the surveillance group (9.4%) than the treatment groups (4.7% prostatectomy and 5.0% radiation), with no demonstrated impact on mortality.7 Of note, by 15 years 61.1% of AS patients had converted to treatment with curative intent at a median of about 8 years.
Trials such as PIVOT and PROTECT serve as the foundation for shared decision-making between physicians and patients regarding treatment decisions and inform the discussion regarding the heterogeneity in treatment approaches, which are highly patientspecific and goal-directed. They support the safety of AS in wellselected patients but confirm that ultimately some patients will be better suited for treatment.
When discussing prostate cancer screening, diagnosis, and treatment with patients, it is important to emphasize that each patient is managed based on unique individual criteria. PSA elevations are not specific for prostate cancer and the decision to biopsy involves discussion between the physician and patient. Additionally, it is valuable to counsel that prostate cancer comprises a spectrum of phenotypic severity, and while some men may be candidates for AS, others may receive greater benefit from treatment with curative intent. Thus, primary care physicians should feel comfortable initiating PCa screening with their patients, and as questions inevitably arise regarding who is most appropriate and for which approach, my colleagues and I are happy to be there to support and guide.
Citations:
1. Seigel et al. Cancer Statistics. 2013, 2021
2. Howlader N, Noone AM, Krapcho M, Miller D, Bishop K, Altekruse SF, Kosary CL, Yu M, Ruhl J, Tatalovich Z, Mariotto A, Lewis DR, Chen HS, Feuer EJ, Cronin KA (eds). SEER Cancer Statistics Review, 1975-2013, National Cancer Institute. Bethesda, MD, https://seer. cancer.gov/archive/csr/1975_2013/
3. Carter HB, Albertsen PC, Barry MJ et al: Early detection of prostate cancer: AUA Guideline. J Urol 2013; 190: 419.
4. PROMIS: Lancet.2017Feb25; 389 (10071):815-822; doi: 10.1016/ S0140(16)32401-1
5. Kasivisvanathan V, Rannikko AS, Borghi M, et al MRI-targeted or standard biopsy for prostate-cancer diagnosis. N Engl J Med 2018;378:1767-1777.PIVOT
6. Freddie C. Hamdy, Jenny L. Donovan, J. Athene Lane, et al. Fifteenyear outcomes after monitoring, surgery, or radiotherapy for prostate cancer. March 11, 2023
7. DOI: 10.1056/NEJMoa2214122
M edical R eco R d F eatu R e
20 | www.berkscms.org
2023 Reading Berks Science and Engineering Fair Berks County Medical Society Health and Science Awards
The Berks County Medical Society awarded our annual prizes for Health and Science projects in the 2023 Reading Berks Science and Engineering Fair at Albright College on March 14th.
Congratulations to the prize winners and a BIG note of appreciation for every student who entered a project. It was an enthusiastic and delightful event.
Senior Division
“Screening for Antibiotic Resistive Genes in Staphylococci Bacteriophagic DNA”
Abigail Weber—Conrad Weiser HS
“Visible Light and Its Influence on Embryonic Viability”
Matthew Ferenz—Daniel Boone HS
“White Light vs. Red Light for Activating Brain Protein”
Enrique Lopez—Governor Mifflin HS
Junior Division
“How Do You Combine Smells and Manipulatives to Relieve Stress and Anxiety?”
Emily Arnold—Conrad Weiser MS
SPRING 2023 | 21
M edical R eco R d F eatu R e
Disability Insurance Can be Key for Physicians
by Michael J. Dinan, CFP® , Partner | Senior Wealth Advisor, Domani Wealth

Long-term disability insurance isn’t front-of-mind for many of us, managing busy work lives, time with family, and other responsibilities.
Especially for physicians in prime earning years and relatively good health, disability insurance is certainly not pinging on any radar.
However, unfortunately accidents and illness do not discriminate. Thousands of people each year are unable to work due to an unexpected incident, whether recovering from major surgery or experiencing debilitating effects of a developing disease. Many of our members see these cases firsthand in their work. In fact, the U.S. Social Security Administration reports that more than 25 percent of people currently in their twenties will experience a debilitating illness or injury before their typical retirement age.
Being proactive about personal and household finances has always been wise; however, the global COVID-19 pandemic is perhaps a stark reminder to always be prepared for the unexpected. With that in mind, it may be beneficial to consider taking a closer look at your disability insurance options. Not only does this benefit offer income protection, it can also play into your overall financial planning strategy.
Disability Insurance: What You Need to Know
Disability insurance replaces a percentage of your income should you become unable to work because of an injury or prolonged illness. Many organizations offer short- and long-term disability plans as part of an employee benefits packages.
Causes of Long-Term Disability Claims
If you have healthy savings, short-term disability claims (such as pregnancy or a broken limb) might not affect your long-term financial health. However, longer-term claims could significantly impact your overall financial picture. Especially in a time when inflation continues to be of concern, and costs for just about everything seem out of hand, protecting your financial stability is paramount.
According to the Council for Disability Awareness, the most common causes of long-term disability in 2020 included:
• Musculoskeletal disorders (27.6%)
• Cancer (15%)
• Injury, such as fractures and sprains (12%)
• Mental health, such as depression (9.3%)
• Circulatory issues, such as heart attack or stroke (8.2%)
Disability Defined: Own Occupation vs. Any Occupation
One important distinction among disability insurance policies is how a disability is defined. Providers will typically offer either “own occupation” or “any occupation” coverage:
• Any Occupation: Provides coverage for when someone is unable to work in a job suitable for their education, experience, and age. This means if the insured person could find work elsewhere, even at a lower wage, the policy would not pay benefits. Typically, any-occupation policies cost less and, as such, are often the norm in group disability insurance plans (like your employer may offer you).
• Own occupation: Provides coverage for the insured person’s specific occupation at the time of the claim; this means if the person is unable to perform the duties of that position, their benefit claim would most likely be approved. Further, the person could still receive the long-term disability benefit even after finding employment in a completely different occupation.
Disability insurance can be a critical benefit of employment, particularly for a household’s primary earner. However, typical group policies have limitations that could adversely impact high-income earners.
22 | www.berkscms.org M edical R eco R d F eatu R e
ADVERTORIAL
Disability Insurance Considerations for Physicians
While you may have employer-provided group disability insurance and don’t think much about it, it’s good to learn exactly what’s covered if you are a major breadwinner in your household.
Group disability insurance often has a maximum coverage amount, which is a percentage of your income – 60 percent is typical. However, it’s important to note this is based on a salary and does not include bonuses, income from practice ownership, or other forms of pay. Also, there’s usually a monthly cap on payments, which means those in higher salary situations might suddenly find themselves compensated at a much lower percentage rate. Someone earning $250,000 per year might have a long-term disability insurance through their employer that caps a monthly payment of $5,000, which amounts to only 24 percent of their salary.
A mix of employer-paid and individual disability insurance policies may help maximize supplemental income should a long-term disability occur.
How Disability Insurance Fits into an Overall Financial Picture
Disability insurance can play a significant role in a financial plan. For example, if a professional is out of work due to a disability claim, they might not be able to contribute to a retirement or savings plan in the same way they had been. They also might not have access to other group benefits, such as health insurance for family members.
A disability claim may also increase the burden on family members, as they may have to step into a role with higher earnings potential while also helping to manage your care if you are disabled for a period of time.
Disability insurance can help mitigate risk, planning for potential income gaps to help maintain overall financial wellbeing. Someone on a long-term disability claim might need to dip into savings to cover everyday living expenses or needed care while out of work.
Finding the Right Disability Insurance Policy
As you learn more about the disability insurance your workplace provides, ask specifics about how much income would be replaced and what a claim might look like for your finances.
You can also consider:
• Own-occupation vs. all-occupation policy options
• Percentage of income replaced
• Cap on annual benefits
• Maximum length of benefit period
• Portability
• Taxes – properly structured benefits can be tax-free
To find supplemental insurance options, you can consider the following:
• Add additional disability insurance coverage through your employer’s group plan. You may be able to elect voluntary coverage, such as cost of living benefits, at an additional premium.
• Purchase your own policy: You can go to market and find a self-pay disability insurance plan that fits your needs, budget, and long-term goals. It’s important to note that individual policies need to go through the underwriting process – that is, your premium will depend on your health.
• Ask about executive disability carve-outs: Some employers participate in group disability insurance programs that have multiple layers of coverage. Executive disability carve-out offers a “guaranteed issue benefit” for high-income earners that might otherwise be capped out of income replacement.
• If you are a business owner at a practice, you can also look into a range of disability and income replacement insurance options through companies that specialize in business insurance.
None of us want to think about unexpectedly finding ourselves out of work for an extended period of time, especially during years we know we are supporting our family and earning for our futures. This generally means we don’t think about disability insurance. However, fully understanding how injury or illness would affect a physician’s income (and livelihood) in the short- and long-term can help you make better proactive decisions for you and your family.
Michael J. Dinan is a CFP® professional and trusted wealth advisor for individuals and families throughout Berks County. He creates financial plans fully focused on each person’s financial goals, which can include components addressing retirement, investment, estate, philanthropic, income tax, and insurance planning. He’s known for his caring nature and dedication to volunteering in the community.
Disclosure: Domani Wealth, LLC (“Domani”) is an SEC-registered investment adviser with offices in South Central Pennsylvania. Domani and its representatives may only transact business in states where they are appropriately notice-filed and registered, respectively, or exempt from such requirements. For information pertaining to the registration status of Domani, please contact the SEC or the state securities regulators for those states in which Domani maintains a notice-filing.

SPRING 20 23 | 23
A Higher Purpose Close to Home: Free Clinic Opening a Reading Satellite
by Wendie Waschitsch Past-President, Board of Directors, WBFMC
by St. Daniel’s Lutheran Church of free space, free utilities, and independence to address the growing health disparity crisis affecting Berks County’s medically underserved population.
Remember the idealism that sparked your decision to become a physician? You probably told anyone who asked that you wanted a career with a higher purpose... one that embraced a lifetime commitment to humanity through neverending learning, collaboration, and service to your patients, as well as to others who needed your talents the most.
Enter reality, and the demands of medical school, the manic grind of residency, and the stressful challenges of putting your talents, knowledge, and skills to work in your medical practice. Your role as trusted partner in advising, treating, and helping your patients through the most difficult times of their lives is personally fulfilling. But your 70-plus hour schedule often leaves little time for the lifework balance you envisioned, let alone gives you time to fulfill a higher purpose beyond your patient family.
Perhaps Western Berks Free Medical Clinic (WBFMC) can offer a close-to-home opportunity to revisit your idealism, help tackle the broader issues of health disparities facing our community, and only require a short commute and a few hours of your time.
Become a volunteer at a soon-to-open Reading site on Kenhorst Boulevard.
Our Mission

When Western Berks Free Medical Clinic opened its doors in 2002, its nonprofit mission was simple: provide free primary health care to friends and neighbors without health coverage no matter the reason. Its original location in Robesonia resulted from an offer
Eight years after the Clinic’s opening, this crisis was underscored when the City of Reading was named the poorest city in the country by the US Census Bureau. While no longer holding this ignominious distinction, Reading continues to experience poverty rates 128.9% and 142.15% higher than the country and state averages, respectively, and sadly claims an unemployment rate 22% higher than the national average. Three of every 10 city residents live at or below the poverty level, with that figure rising to 40% in nine metropolitan neighborhoods noted for their “extreme” poverty status.
Western Berks Free Medical Clinic’s all-volunteer medical team is responding this year, the 275th anniversary of the city’s incorporation, by opening a second, more accessible Reading site for uninsured individuals in need of primary health care.

Of all the forms of inequality, injustice in healthcare is the most shocking and inhumane.”
— Martin Luther King, Jr., 1966
M edical R eco R d F eatu R e 24 | www.berkscms.org
N A FC 2022 STANDAR D S
Julie Sheidy, RN; patient Fataw Osumanu; Nisha Busch, first year medical Student at Drexel University School of Medicine Tower Health Campus.
Retiring MDs or DOs: Apply for No-Cost Volunteer License
PA CME Requirements: 20 CME credits every 2 years
+ 2 CME credits in mandated child abuse recognition
+ 2 CME credits in pain management, addiction identification, or prescribing opioids
(NOTE: WBFMC volunteers do NOT prescribe opioids!)
Professional liability coverage paid by WBFMC in exchange for annual volunteer hour commitment
We are especially grateful to Dr. David O’Rourke who graciously donated office equipment for our new health center.

We Need You!
Volunteer opportunities exist for active or retired family practitioners, internists, gynecologists, hospitalists, emergency medicine physicians, and physicians in other specialties with a primary care focus. We also welcome active or retired CRNPs, as well as RNs and LPNs. In addition, non-clinical individuals with strong Spanish-English skills are encouraged to volunteer as interpreters.
You can choose to volunteer at either the new Reading or original Robesonia location, whichever is more convenient.
Physician Licensure Info: Both medical and osteopathic doctors with active licenses AND retiring physicians who select volunteer licensure within the Commonwealth of Pennsylvania are welcome to contact us for additional info, facility tour, and/or support in sharing the Clinic’s higher purpose.
Active Licensure Info: CME and medical liability requirements for physicians with active licensure do not change as a result of becoming a physician volunteer. It is important to note, however, that their current health system/employer usually extends its professional liability to include the volunteer experience.
Retired Licensure Info: Retired physicians who obtain volunteer licensure have much lower CME requirements and will be covered under Western Berks Free Medical Center’s policy in exchange for a minimum annual commitment of volunteer hours.
Federal Tort Claims Act: The Clinic is in the application process for deeming status under the Federal Tort Claims Act. Once approved, neither WBFMC nor individual providers acting in good faith will need separate professional liability coverage.
As volunteer staffing becomes available, the Reading site will mimic and grow the schedule, but focus on daytime appointments.
Service Extensions: Special collaborations enable WBFMC patients to receive diagnostic testing at no charge, to be assisted with opportunities to enroll in assistance programs if eligible, and to participate in advanced clinic services on a sliding-fee scale. A social determinants of health process helps patients address socioeconomic factors, such as housing, food insecurity, and safety, that also impact their health and well-being.
Volunteer Engagement: The Clinic’s medical staff is led by a volunteer medical director, with three volunteer physicians serving on its board of directors to assure provider input on operational and strategic issues. With the medical director, a part-time staff nurse works closely with volunteer nurses to assure consistency in supporting clinical and patient experience excellence.
Volunteers are encouraged to share suggestions for clinical or administrative improvement and are encouraged – but not required – to join any committee or task force that matches their interest.

One More Thing!
Current volunteers and staff are ready to answer your questions, provide tours, and even walk you through the application and/ or volunteer licensure process. Contact Greg Colahan, executive director, at execdir@wbfmc.net to get started.
Western Berks Free Medical Clinic

Robesonia Site: 480 Big Spring Road (inside St. Daniel’s Lutheran Church)
Reading Site: 615 Kenhorst Boulevard (inside Mary’s Shelter)
To apply or for info/tour, contact Greg Colahan at execdir@wbfmc.net.
Clinic Schedules: All patients are seen by appointment only. The Robesonia site offers weekly evening sessions for primary and chronic care, and a monthly evening clinic for women’s health care.
SPRING 2023 | 25
The following article is one in an occasional series of reflections by physicians on the hobbies and activities that provide personal balance in their demanding professional lives.
Music as a Relaxing Interlude to a Successful Medical Career An Introduction to the Berks Sinfonietta Chamber Orchestra
by Barton Smith, MD
Most of us take the 8th cranial nerve for granted, but for the composer or performer of music it is at the center of existence. The late Czech American composer, Karel Husa, while giving me a lesson on his Sonatina for Piano, expressed his palpable enthusiasm for all sound. Even with music easily accessible in all parts of our life, we often allow our other senses to put those sounds in the background. But bringing sound to the center of our focus through attentive listening, or by performing music ourselves, provides a satisfying contrast to the intense discipline required by the practice of Medicine.
Exposure to music at a very young age, encouragement (no pressure) from family to play (not perform), and the chance to participate with others in making music are the factors that led to music becoming an indispensable part of my life. Earning a bit of money playing in a dance studio and in a small band while in high school and college was a “bonus.” Performing music of great composers offers the satisfaction both of gaining insight into the art that is required for composing, and of approaching the perfection of the composer’s intention. Finally, volunteering for a musical group such as the one described next offers its own healthy diversion from the demands of our profession.
Great vocal, and instrumental, music, skillfully played, is readily available in Berks County. A welcome, and unique, addition to our musical scene occurred in 2014 when Dr. David McConnell, Kathleen Bahena, Andrew Cusano, and James Gilmer founded
the Berks Sinfonietta Chamber Orchestra. A primary aim was to provide orchestral employment for local professional musicians. Its inter-generational approach also created an environment in which skilled young musicians play alongside their mentors. It even provided the orchestral debut of an 80-year-old amateur pianist.
Another key part of the orchestra’s mission is, in the words of co-founder James Gilmer, repertoire that “spans many eras and will introduce local audiences to new and unfamiliar music.” The orchestra has made diversity a normal feature of its programming, striving to program music by female, non-white, and living composers. The program listing that shows all concerts played is available at www.berkssinfonietta. org; reading through it reveals a remarkable traversal of classical works ranging from CPE Bach in the eighteenth century to premiere performances of music by Berks County oboist and composer Jill Haley. The web site also provides links to many YouTube performances and educational videos. The Orchestra has observed every February as Black History Month, with concerts of music by Black composers, in collaboration with Lincoln University’s Concert Choir and the Albright College Chamber Ensemble. Major choral works such as Mozart’s “Requiem” and his “Mass in C Minor” were performed by the Sinfonietta and the Vox Philia choir, founded by Dr. McConnell in 2012. Finally, the Sinfonietta initiated “Music on the Mountain” at Hawk Mountain Sanctuary’s beautiful amphitheater in 2021. This year’s program
The Berks Sinfonietta Chamber Orchestra is a 501 (c) (3) organization. It welcomes the support of Berks physicians, their families, and their staffs at all levels. Attend the concerts and consider volunteering. You may request information at info@berkssinfonietta.org or from Board member, Dr. Barton Smith at ksmith3685@aol.com.
at Hawk Mountain is on Saturday afternoon June 10 and will feature Beethoven’s Third Symphony, the Eroica.
Berks County physicians have been deeply involved in its musical scene. The Reading Symphony Orchestra, started in 1913, has been supported by father and son surgeons Frank and William Runyeon, and by Sergio Proserpi and his wife Penny among many others. Dr. Benjamin Souders founded the Friends of Chamber Music in 1953, the program now led by his son Thomas, and in recent years others of the medical community including Neil Hoffman. As far as I know, the only Berks physician also a professional musician was the late Bob Mulligan, an outstanding trombonist and jazz arranger, and recipient of the Jazz Fest’s Frank Scott Medal. It would be wonderful to see our medical community support the Sinfonietta.
26 | www.berkscms.org
M edical R eco R d F eatu R e
BERKS COUNTY MEDICAL SOCIETY BYLAWS
T.J. Huckleberry, MPA Executive Director

Per our existing Bylaws, after our Executive Council unanimously approves any addendum or removal of text, that a copy of said changes be disseminated via our magazine for member review.

Overview of changes to Bylaws (2nd Consideration)
• Shifted our leadership structure from current Executive Council/ Administrative Committee Structure to a Board of Directors.
• Removed the position Chair of Executive Council and Secretary and transferring their duties to President and Executive Director.
• Removed antiquated language concerning penalties, disciplinary actions, and AMA mandates.
• Added sections outlining our endowment and Trust.
• Updated necessary pronouns.
• Updated language on criteria for meetings and committees.
Founded 1824 Incorporated 1904
As amended through February 2023
CHAPTER I – NAME

The name and title of this Society is Berks County Medical Society.
CHAPTER II – PURPOSES AND POWERS
SECTION 1. Purposes. The purposes of this
Society shall be to promote and protect the art and science of the practice of medicine for physicians of Berks County.
SECTION 2. Powers. This Society shall have all the powers usual and incident to organizations of like character which are permitted by the laws and customs of the Commonwealth of Pennsylvania and necessary or appropriate to the fulfillment of its purposes.
CHAPTER III – MEMBERSHIP
A. Active Member
1. Full Active. Persons who hold the degree of Doctor of Medicine or Osteopathy or the equivalent from a recognized accredited medical school, and who hold or are eligible to hold an unrestricted license to practice medicine and surgery in Pennsylvania, are eligible for active membership in this Society. Upon admission to membership, such members shall have the right to vote and hold office in this Society.
2. Residents and Fellows. Residents and fellows serving in residency or fellowship programs are eligible for active membership in this Society. Upon admission to membership, such members shall have the right to vote and hold office in this Society.
3. Students. Medical students enrolled in a medical school approved by this Society are eligible for active membership in this Society. They shall make application directly to this Society. Such students
are entitled to all rights and privileges of membership. Medical student active members shall pay such amount as is fixed each year by the Board of Directors.
B. Retired Member. A physician who is retired from the active practice of medicine, and currently resides in Pennsylvania or was previously active in the Society. A retired member may vote, hold office, and serve as a member of any workgroup or committee on the state and county levels.
C. Supporter Member. Any physician who is engaged in professional activities related to the active practice of medicine, but who is not engaged in active practice within the jurisdiction of a component medical society. A supporter member may not vote or hold office. A supporter member may serve as a member of any workgroup or committee on the state or county levels.
D. Administrative Member. An administrative member shall be:
1. A County Society Executive. A county society executive, who may or may not be a physician, shall be exempt from paying dues;
2. A Practice Administrator. Practice administrators from a practice with at least one physician member and a membership level of 50 percent or more, as of the current membership year, shall be exempt from paying dues. Practice administrator with less than 50 percent membership are not exempt from paying dues; or
continued on next page >
SPRING 2023 | 27
c o MP ass P oints
Berks County Medical Society Bylaws
continued from page 27
3. A Hospital Medical Staff Coordinator. Hospital medical staff coordinators must meet the State Society’s membership guidelines and are not exempt from paying dues. An administrative member may not vote or hold office but may serve as a non-voting member of any workgroup or committee provided that the percentage of administrative members does not exceed 25 percent.
4. Honorary Member. Physicians who are not residents of Pennsylvania, but are members of their own state or territorial medical association, may be elected to this category by the House of Delegates by a three-fourths vote at any annual meeting. The individual is not required to have an unlimited license to practice medicine and surgery in the Commonwealth of Pennsylvania. The honorary member is not required to pay any annual dues. No more than two honorary members may be elected in any one year to this category by the House of Delegates. An honorary member is not entitled to any of the rights and privileges of membership.
Requirement. An active or associate member of this Society, who is not a resident, must qualify for the American Medical Association’s Physician’s Recognition Award or its equivalent and must continue to qualify for such award in order to remain a member in good standing of the Pennsylvania Medical Society. The Board of Trustees of the Pennsylvania Medical Society shall have the power to waive such requirements, in keeping with approved procedures, for members requesting waivers.
fiscal year.
SECTION 4. Rights and Privileges of Members, Including Voting Rights. All members of this Society shall have all the rights and privileges of membership, except as otherwise provided in these bylaws. All members of this Society, and thereby members of the Pennsylvania Medical Society, in good standing shall have such rights and privileges as members thereof as may be granted to them from time to time under the bylaws of the Pennsylvania Medical Society. Members who are delinquent, as provided in SECTION 2 of Chapter IV, or under suspension shall not be eligible to vote, hold office, or take part in any scientific or business proceeding of the Society. Provided a member has full membership or proper membership in one county medical society in Pennsylvania, he/she may be eligible to hold affiliate membership in any other county medical society in the state.
SECTION 5. Continuing Medical Education
SECTION 6. Applications for Membership. A candidate for membership other than honorary shall make application in writing upon forms provided or approved by the Society. Applications shall be reviewed pursuant to guidelines of the Society to determine whether the applicant meets the qualifications for membership. New applications are forwarded to Pennsylvania Medical Society for verification of eligibility. PAMED will notify BCMS of the status of the candidate. If our county has no objections, the applicant will be accepted for membership. In case of a rejection, the reasons for rejection shall be set forth in writing. An applicant or any member of this Society dissatisfied with the decision may present the matter to the next regular meeting of the BCMS Board of Directors.
SECTION 7. Appeals from Rejections. Any physician who has been refused membership in this Society or has duly filed an application for membership which has neither been accepted nor rejected within six months after filing thereof, shall have such rights of appeal as may be provided by the bylaws of the Pennsylvania Medical Society.
SECTION 8. Applications by Transfer. A physician applying for membership as a transferee from any other county medical society shall submit an application as a new member and shall accompany his application with a transfer letter or card in lieu of any admission fee. The procedure for election to membership shall be the same as set forth in these bylaws. Annual dues shall be prorated making due allowance for dues previously paid by the transferring members during the
SECTION 9. Transfer Letters. A member in good standing, who is free from all indebtedness to this Society and against whom no charges are pending, wishing to withdraw from membership shall be granted a transfer card or letter. This document shall state the date the member associated himself with this Society, the date of issuance thereof and a statement that he is in good standing and that his dues are paid to a date specified. In addition, if the member is going to another county in Pennsylvania, the letter shall contain a recommendation that the member be admitted to membership in the other county medical society without the delay attendant upon ordinary applications for membership. Such card or letter shall be signed by the appropriate officer or officers of this Society.
SECTION 10. Suspension and Termination of Membership. Any member of this Society suspended from membership in the Pennsylvania Medical Society shall be automatically suspended from membership in this Society for a period corresponding to the State Society suspension. Any member of this Society, whose membership in the Pennsylvania Medical Society is terminated for any reason whatsoever, shall automatically cease to be a member of this Society upon the expiration of sixty days following the effective date of termination of membership in the State Society.
CHAPTER IV – DUES AND EXPENSES
SECTION 1. Annual Dues. The annual dues for Active members shall be as set forth by the membership at the annual meeting for the ensuing year. This Society may set its annual dues in accordance with these bylaws. However, the dues categories and the percentages of the full annual dues to be paid by each category must be in accord with the Pennsylvania Medical Society’s categories and percentages;
a) Active members unable to practice because of illness or disability shall pay no annual dues;
b) Active members shall pay no dues for the
28 | www.berkscms.org
period between the initial granting of a license to practice medicine or osteopathy in Pennsylvania and the end of the first full calendar year after the initial granting of the license, however, an Active member in first year of practice shall pay 25% of dues, in second year of practice shall pay 50% of dues, and third year of practice shall pay 75% of dues;
c) Honorary members shall pay no annual dues;
d) new members joining after November 1 of the assessment year shall pay no dues, provided that the annual dues for the relevant membership category is paid for the following year;
e) new members joining after July 1 of the assessment year, but before November 1, shall pay 50 percent of the annual dues for the physicians specific membership category;

f) Associate members shall pay 10% of annual dues;
g) reduced-income category is available for physicians earning less than $60,000 and dues will be set on a case-by-case basis; and h ) Administrator/Office Manager classification shall pay dues in compliance with Pennsylvania Medical Society’s dues structure. Notwithstanding the forgoing, the Board of Directors shall have the power at any time to excuse the payment of dues, or any part thereof, of any member of this Society under any circumstances in which it deems such action is justified.
SECTION 2. Delinquent Dues. A member whose annual dues are not paid prior to March 1 shall be delinquent and shall not be in good standing in this Society. No delinquent member shall be entitled to exercise any of the rights and privileges of membership in this Society during the period of his delinquency. The Secretary shall see that a notice is sent to each delinquent member within fifteen days after March 1, stating the amount then due, the fact that the member is delinquent and that unless such amount is paid within thirty days after the date thereof that the membership of such member will be terminated.
SECTION 3. Funds and Disbursements. All funds of the Society shall be deposited in a depository designated by the Board of Directors. Disbursements of the funds
Great care for your patient starts with a strong team.
Adam J. Altman, MD
Angela Au Barbera, MD
Helga S. Barrett, OD
Jennifer H. Cho, OD, FAAO
Christine Gieringer, OD
David S. Goldberg, MD, FAAP
Marion J. Haligowski III, OD
Dawn Hornberger, OD, MS
Y. Katherine Hu, MD, MS
Lucinda A. Kauffman, OD, FAAO
Christina M. Lippe, MD
Barry C. Malloy, MD
Michael A. Malstrom, MD
Mehul H. Nagarsheth, MD
Abhishek K. Nemani, MD
Tapan P. Patel, MD, PhD
Jonathan D. Primack, MD
Kevin J. Shah, MD
Michael Smith, MD
Anastasia Traband, MD
Monica Wang, OD
Denis Wenders, OD
Linda A. Whitaker, OD, MS
With 20+ eye care specialists, Eye Consultants of Pennsylvania is the leading eye care practice in the region. Our doctors are always available for consults and referrals on eye issues, and our entire practice is committed to cooperative management of your patient. That means that we communicate and consult 360°. We share information, and we provide direct cell numbers to our partner physicians. And ultimately, it means better care and outcomes for your patients.
For consultations and referrals, call 610-378-1344.
of the Society shall be made in such manner and upon such authority as shall be prescribed by resolution or resolutions of the Board of Directors.
SECTION 4. Fiscal Year. The fiscal year of this Society shall be January 1 and end on December 31.
SECTION 5. Required Signatures for Checks. All checks issued by this Society shall have the
signature of two of the following officers: the President, President-Elect, Treasurer, and the Executive Director.
CHAPTER V – FUNDS
SECTION 1. Special Funds- The Board of Directors may establish special funds for educational, scientific, charitable, benevolent, endowment, medical defense, or other continued on next page >
SPRING 2023 | 29 Offices in Wyomissing, Pottsville, Pottstown, Lebanon and Blandon EyeConsultantsOfPA.com Adult Strabismus | Cataract Surgery & Intraocular Lenses | Comprehensive Ophthalmology & Optometry | Contact Lenses Cornea and External Diseases | Cosmetic & Reconstructive Eyelid Surgery | Cosmetic Botox‑Latisse
Diabetic Eye Care Glaucoma | Laser Vision Correction (Including Bladeless LASIK) | Low Vision | Macular Degeneration
Neuro Ophthalmology Oculoplastics | Orthoptic Therapy | Pediatric Ophthalmology & Optometry | Vitreo – Retinal Surgery
|
|
Berks County Medical Society Bylaws
continued from page 29
purposes by resolution. These may be in the form of trusts or otherwise, with trustees or managers, and under terms determined by the Board.
SECTION 2. Deposit of Monies and Special Funds – The Executive Director shall deposit all monies of the Society received by the Society in the Pat Sharma Educational Fund as the treasurer shall direct in accordance with the duties of that office.
SECTION 3. Pat Sharma Educational Fund - Each year the Board of Directors may appropriate a sum of monies for all active, retired, and supporter members to be allocated to the Educational and Scientific Trust of the Berks County Medical Society. The Board of Directors set the sum aside in a special fund to be known as the Pat Sharma Educational Trust. The Educational Committee of the Board of Directors shall approve allocation of funds for Educational and Scholarship based on criteria established by The Pat Sharma Educational Trust. No such allocations may be made without the approval of a majority of the Board of Directors. The Board of Directors may establish further terms and conditions of the Pat Sharma Educational Trust, within the general terms and for the purposes herein established, as it shall deem necessary and desirable. Monies and special funds shall be disbursed by the treasurer in accordance with specific or general resolutions of the Board of Directors.
SECTION 4. The Endowment Fund – The Endowment Fund is funded by the net proceeds, after expenses and other associated disbursements, of the sale of Berks County Medical Society properties and assets. Each year the Board of Directors may appropriate a sum of monies for all Capitol needs and expenses related to the Society. No such allocations may be made without the approval of a majority of the Board of Directors. Monies and special funds shall be disbursed by the treasurer in accordance with specific or general resolutions of the Board of Directors.
CHAPTER VI – MEETINGS
SECTION 1. Annual Meetings. There shall be an annual meeting of this Society held at a time selected by the Board of Directors.
SECTION 2. Special Meetings. Special meetings of this Society may be held at any time upon the affirmative vote of two-thirds of the members of the Board of Directors.
SECTION 3. Time, Place, and Notice. The meetings of this Society shall be held at such time and place as shall be designated by the Board of Directors, and the Executive Director shall notify the membership of such meetings at least ten days in advance thereof.
SECTION 4. Procedure. Any business may be transacted at the Annual and regular meetings of the Society, but no business shall be transacted at any special meeting of the Society except as may be stated in the notice of the meeting. The American Institute of Parliamentarians Standard Code of Parliamentary Procedure shall govern the Order of Business and the proceedings at all meetings of this Society unless otherwise provided in these bylaws.
SECTION 5. Quorum. A quorum for the transaction of business at any Annual or Special meetings of this Society shall consist of at least 5% of the Active, and Resident members.
CHAPTER VII – NOMINATIONS AND ELECTIONS
SECTION 1. Nominating Committee and Nominations. The Nominating Committee shall be comprised of the Board of Directors, exclusive of the following incumbent Executive officers: President, President-Elect, and the Treasurer, and shall meet prior to the September Board of Directors Meeting. The Immediate Past President shall act as the Chair of this Committee. Five members of this Committee will comprise a quorum. It shall be the duty of the Nominating Committee to nominate one or more candidates for each of the offices to be filled
at the Annual Meeting and to report its nominations to the Board of Directors and to cause its report to be distributed to the entire membership of the Society promptly thereafter. Additional nominations may be made from the floor at the Annual Meeting.
SECTION 2. Elections. The election of the officers of the Society, such number of delegates and alternate delegates to the Pennsylvania Medical Society as to which this Society may be then entitled, and such members of the Board of Directors as are required to fill vacancies therein shall take place at the Annual Meeting. A majority vote of all Active and members present and voting shall be necessary to elect.
CHAPTER VIII – OFFICERS AND DUTIES
SECTION 1. Officers. The elected officers of this Society shall consist of a President, President-Elect, and Treasurer.
SECTION 2. Term of Office. The term of office of all officers of this Society shall be for a period of two years and until their successors are elected and assume office unless provided otherwise by these bylaws. Each such regular term shall commence following the annual meeting after taking the oath of office.
SECTION 3. President. The President shall preside at the meetings of the Society and perform such other duties as custom and parliamentary usage may require or as may be prescribed by these bylaws. He/She shall make a written report on his/her term as President, which shall be filed with the Executive Director of the Society and shall be delivered in person at the Annual Meeting.
SECTION 4. President-Elect. The PresidentElect should attend all meetings of the Board of Directors and should assist the President in the performance of his/her duties. The President-Elect will oversee membership recruitment and assist with member recommendations to the Board of Directors. Upon completion of his/her term as President-Elect he/she shall automatically succeed to the office of President after taking the oath of office.
30 | www.berkscms.org
SECTION 5. Successor to the President and President-Elect. If the office of President should become vacant, the President-Elect shall immediately become President and shall serve for the remainder of the term of his/her immediate predecessor. If a President-Elect succeeds to the presidency, he/she shall serve as President until the second Annual meeting of this Society following his/her accession as President-Elect. If the office of President-Elect becomes vacant the Board of Directors shall designate from among the Board of Directors one who shall act as President-Elect, until the next Annual Meeting of this Society, at which time the voting members shall elect an eligible person as President-Elect. If the offices of President and President-Elect should become vacant, the Board of Directors shall designate from among the Board of Directors one who shall act as President, one who shall act as President-Elect, each of whom shall so act until the next Annual Meeting of this Society, at which time the voting members shall elect an eligible person as President, an eligible person as President-Elect. Should the President, as determined by the Board of Directors, be incapacitated or unable to perform the duties of his office, the President-Elect shall act in his/her stead.
SECTION 6. Treasurer. The Treasurer shall have custody of all funds and securities of this Society and shall render full and accurate reports at the regular meetings of the Board of Directors and at such other times as may be directed by the Board of Directors or the membership. He/she shall keep full and accurate accounts in books of account belonging to the Society. The Treasurer shall be elected at the Annual Meeting for a term of two years. He/she may not serve more than two consecutive terms.
SECTION 7. Vacancies in Office. Vacancies in any office, other than that of President, President-Elect occurring between Annual Meetings of this Society, shall be filled by a majority vote of the Board of Directors, and the persons so elected to fill vacancies shall serve until the next ensuing January 1 and until their successors are elected and take office.
CHAPTER IX – DELEGATES AND ALTERNATES TO THE PENNSYLVANIA MEDICAL SOCIETY


SECTION 1. Number. This Society shall have such number of delegates and alternates to the Pennsylvania Medical Society as may be prescribed by the bylaws of said Society, who shall faithfully represent the members of this Society and the profession of this county in the House of Delegates of the Pennsylvania Medical Society and report thereon to this Society.
SECTION 2. Term of Office. The term of office of each delegate and alternate shall be for a period of a year and until his/her successor is elected and assumes office, except as otherwise herein provided. Each such regular term shall commence on January 1 and end on December 31. In the event that in any year the number of delegates and alternates to which the Society is entitled under the bylaws of the Pennsylvania Medical Society is greater than the number of delegates and alternates elected for that year at preceding Annual Meeting, the Board of Directors at the discretion of the Delegation Chair shall elect for a regular term such number of additional delegates and alternates to which this Society may be entitled. In the event that in any year the number of delegates and alternates to which this Society continued on next page >
SPRING 2023 | 31
Berks County Medical Society Bylaws
continued from page 31
is entitled is less than the number elected for that year at the preceding Annual Meeting, the Board of Directors shall determine, by any means in its discretion, the delegates and alternates whose terms of office are to terminate, and the terms of office of such persons shall thereupon be terminated.
SECTION 3. Alternate Delegates. In the event that any delegate determines that he will be unable to attend a forthcoming meeting of the House of Delegates of the Pennsylvania Medical Society, he should promptly so advise the Executive Director of this Society, who shall present the matter to the Board of Directors. The Board of Directors shall have the power to designate any one of the alternate delegates to substitute for such delegate at the forthcoming meeting of the House of Delegates, but if no such designation is made or can be made or if the alternate delegate so designated fails or is unable to attend the meeting of the House of Delegates, the alternate delegates attending the meeting shall be seated as determined by the Chairman of the delegation or in the absence of the Chairman, the President- Elect or in the absence of either, by the Credentials Committee.
CHAPTER X – Board of Directors
SECTION 1. Duties. There shall be a Board of Directors of the Society which shall have general supervision and management of the affairs and business of the Society and shall act for the Society in the intervals between meetings of the membership, except that it may not establish any policies or take any actions, inconsistent with prior actions of the membership of the Society. It shall have charge of the property and financial affairs of the Society and shall perform such other duties as prescribed by law covering directors of corporations or as may be expressly delegated to it by the membership. It may have such committees as it deems necessary properly to conduct its business. It shall exercise general supervision over the conduct of all committees and over all appointive officers, agents and employees, from whom it may require reports at least annually. It shall designate from time to time the officer
or officers to execute documents in the name and on behalf of the Society.
SECTION 2. Composition. The Board of Directors shall consist of the following members: President, President-Elect, Treasurer, Delegation Chair, Collegiality Chair, Education Chair, Advocacy Chair, Editor, Residency Chair, Medical Student Chair, Early Career Physician Chair, Past President, and three members-at-large. Three members-at-large shall be appointed by the President to serve a two-year term. A resident physician and Medical Student shall also be appointed by the President to a one-year term as a member-at-large. In addition, an Administrator/Office Manager Representative, and the President of the BCMS Alliance shall also serve on the Board of Directors; however, the Administrator/ Office Manager Representative and President of the BCMS Alliance are non-voting members of the Board of Directors.
SECTION 3. Election. The election shall take place at the Annual Meeting and a majority vote of Active and Associate members present and voting shall be necessary to elect.
SECTION 4. Meetings. A regular meeting shall be held on days and times fixed by the Board of Directors at its initial meeting of the fiscal year. The quorum for a meeting of the Board of Directors shall be not less than seven members.
SECTION 5. Vacancies. In the event of a vacancy in the Board of Directors, the remaining members of the Board of Directors shall fill the vacancy, and any person selected shall fill out the unexpired term of the director whom he/she succeeds.
CHAPTER XI – COMMITTEES
SECTION 1. Appointment and Tenure of Office of Chairs and Members. All appointments of chairperson and members of committees shall be made by the President except as otherwise provided in these bylaws. The term of office of all chairs and members of committees shall be for two years and shall commence on January 1, or as soon thereafter as appointed, and shall end on December 31.
SECTION 2. Sections. This Society shall have the following sections: Operations, Collegiality, Advocacy, Professionalism, and Education/Communication. Each Section shall regularly report to the Board of Directors. The Sections shall be as follows:
A. Operational Section. This Section shall consist of the following committees:
1. Nominating Committee. The Nominating Committee shall be composed, appointed, and have the functions as provided elsewhere in these bylaws.
2. Finance Committee. The Finance Committee shall be chaired by the Treasurer and shall oversee the budget, and Educational Trust.
3. Membership Committee. The Membership Committee shall be chaired by the President-Elect and will oversee the retention and recruitment of members.
4. Personnel Committee. The Personnel Committee shall consist of the President, President Elect and the Treasurer and will oversee all personnel matters.
B. Collegiality Section. The Collegiality Section will be chaired by a member appointed by the President and will oversee all social events.
C. Advocacy Section. The Advocacy Section will be chaired by a member appointed by the President and will oversee all programs advocating for physicians and for patients. This shall include the Society’s interaction with the PA Medical Society, Access To Care, and other related activities.
D. Education/ Communication Section. The Education/ Communication Section shall be chaired by a member of the Board of Directors and will oversee services related to Physician education and communication and annual scholarship selection process. This section may include but not be limited to Health Talk, the Medical Record, BCMS Website and the Memorial Lecture/Residents’ Day.
SECTION 3: Special Committees. The Society may have such special committees as the membership may from time to time
32 | www.berkscms.org
determine. Such committees are typically convened by either the President (or designee). Unless otherwise ordered by the membership, special committees shall consist of such number of members as the President shall determine.
CHAPTER XII – INDEMNIFICATION OF DIRECTORS AND OFFICERS
No director or officer of the Berks County Medical Society shall be personally liable for monetary damages for any act that is performed as a director or officer or any failure to act on behalf of the Society, unless:
1. the director has breached or failed to perform this duties in good faith in the manner he reasonably believes to be in the best interest of the Society, and with such care, including reasonable inquiry, skill and diligence, as a person with ordinary prudence would use under similar circumstances; and
2. the breach or failure to perform was a result of self-dealing, willful misconduct, or recklessness. The Society shall indemnify any director or officer of the Society for expenses incurred in the defense of claims made by the Society, whether brought by the Society itself or by a member on behalf of the Society, against a director or officer, provided that a court of lawful jurisdiction has not found the director’s or officer’s action or failure to take action to constitute a willful misconduct or recklessness. The Berks County Medical Society shall also have the authority to advance funds to any director or officer for the defense of the claims set forth in the bylaw above, provided that the director or officer deliver to the Society a written document agreeing to return the advanced funds in full if it is found by a court of lawful jurisdiction that the director’s or officer’s actions or failure to act constituted willful misconduct or recklessness.
CHAPTER XIII – PRINCIPLES OF MEDICAL ETHICS
Each member of this Society, by accepting membership herein, shall be deemed to have subscribed to the Principles of Medical Ethics of the American Medical Association.
CHAPTER XIV – SEAL
The Board of Directors shall have the authority to adopt a seal for this Society, and when so adopted, it shall be the official seal of the Society.
CHAPTER XV – AMENDMENTS
These bylaws may be amended at any regular meeting by a twothirds vote thereto, provided that such an amendment has been reviewed by the Bylaws Committee, approved by the Board of Directors, published, and acted upon at the next Annual Meeting. No amendment to these bylaws shall be valid or effective unless it is in accord with the bylaws of the Pennsylvania Medical Society. A copy of all amendments hereto shall be filed with the Executive Vice President of the Pennsylvania Medical Society.
Do you have patients with:
• Chronic Headaches
• Tinnitus
• Jaw Pain
• Insomnia
• Ear Pain without signs of infection

• Dizziness
• Clicking, popping, or grating in the jaw joint
• Limited jaw opening or locking
• Swallowing difficulty
• Snoring
• Pain when chewing
• Sleep issues
• Facial pain
• Neck pain or stiffness
• Tired jaws
• CPAP Intolerance
If so, they may be suffering from TMJ Dysfunction and/or Sleep Disordered Breathing, such as snoring and obstructive sleep apnea. We offer comprehensive diagnosis and treatment. Our many years of experience have resulted in a high rate of successful outcomes.


Our philosophy involves a conservative, non-surgical, non-pharmaceutical approach to management with an emphasis on multidisciplinary care.
DDS, MS
SPRING 2023 | 33
Tammy
Diplomate, American Board of Dental Sleep Medicine Fellow, American Academy of Craniofacial Pain 2433 Morgantown Road (Route 10) Suite 200, Reading, PA 19607 www.TMJSleepCenter.com • 610.796.2835
Balatgek,
Challenging Cases? We Can Help...
Foundation Partners with WellSpan to bring BMWC Youth Summit to Fruition
Changing the vernacular from “I want to be …” to “I am going to be …” is a first step on a journey of becoming a physician according to WellSpan Vice President and CMO, Women & Children, Carlos Roberts, MD, at a summit to guide and inspire diverse high school students toward a future profession in medicine.
The Foundation of the Pennsylvania Medical Society shared in an exciting partnership with WellSpan Health to bring a Black Men in White Coats Youth Summit to William Penn High School, York, in March.

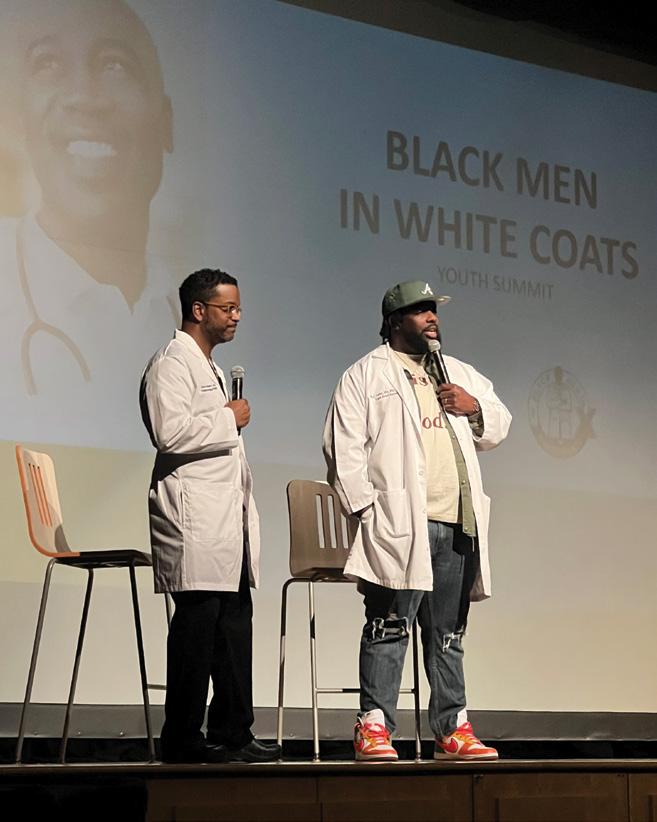
“It was an exceptional day. We filled a room with physicians and healthcare professionals from historically underrepresented groups so that students holding those same racial and ethnicity identities could be inspired to consider a career in medicine,” says Karla Tolan, manager, Diversity, Equity, and Inclusion for WellSpan Health. “More than 150 students, parents and caregivers, and 77 volunteers, participated in WellSpan’s inaugural event, a fantastic turnout for the first year!”
The genesis of the Black Men in White Coats campaign started in 2013 with the aim of increasing the number of black men pursuing careers in the medical industry. This initiative was founded by Dr. Dale Okorodudu in response to an AAMC report highlighting the decreasing number of black male applicants to medical school. The summits invite students, parents, educators, clinicians,
and community leaders together to “uplift our communities. The goal of the summits is to inspire our youth to consider careers in healthcare while laying the foundation for success via mentorship and networking,” according to its website.
The Foundation of the Pennsylvania Medical Society Executive Director Heather Wilson says that establishing a support system to strengthen the diversity of physicians is a goal of the non-profit’s scholarship programs. “We strive to gain more students who authentically look, speak, and understand the communities they will serve,” she says. In the last five years, the foundation added additional scholarships to advance the commitment to include more diverse cultural composition of the medical school student body.
“Registrants for the day-long healthcare career exploration program represented 50 different high schools and seven states –some rising early to travel together by bus to hear from WellSpan’s expert physicians and medical professionals, who live and work in the region and represent racially diverse identities and lived experiences, through keynote presentations, Q&A panels, and breakout sessions,” says Tolan. “One physician told us that the first time he saw another black doctor was in medical school, so this shortens that timeline exceptionally for many kids.”
Keynote speaker Russell Ledet, MD, PhD, MBA, Indiana University School of Medicine Triple Board Resident Pediatrics/ Psychiatry/Child Psychiatry, entered the stage with a white coat, basketball sneakers and a baseball hat. His indelible stage presence served to encourage students. He said that even though he came from humble beginnings, his hard work, mentorship, and passion launched him into a successful medical career. When he realized what he was capable of he pursued it. Currently he has eight letters behind his name emblazoned on his white coat.
Breakout session facilitator Raymond C. Truex, Jr., MD, FACS, FAANS, medical director, Physicians’ Health Program, Foundation
M edical R eco R d F eatu R e 34 | www.berkscms.org
Photos by Sela Fuhrman, WellSpan Health
TEACHERS LOVE TO TEACH AND STUDENTS LOVE TO LEARN
of the Pennsylvania Medical Society, volunteered to participate in breakout segments on bleeding control and mental health self-care, for practical student experiences during the day. “The students heard in the summit that the pursuit of medicine is challenging on all levels. Although they can achieve their goals, it is not without a great deal of discipline and hard work.”
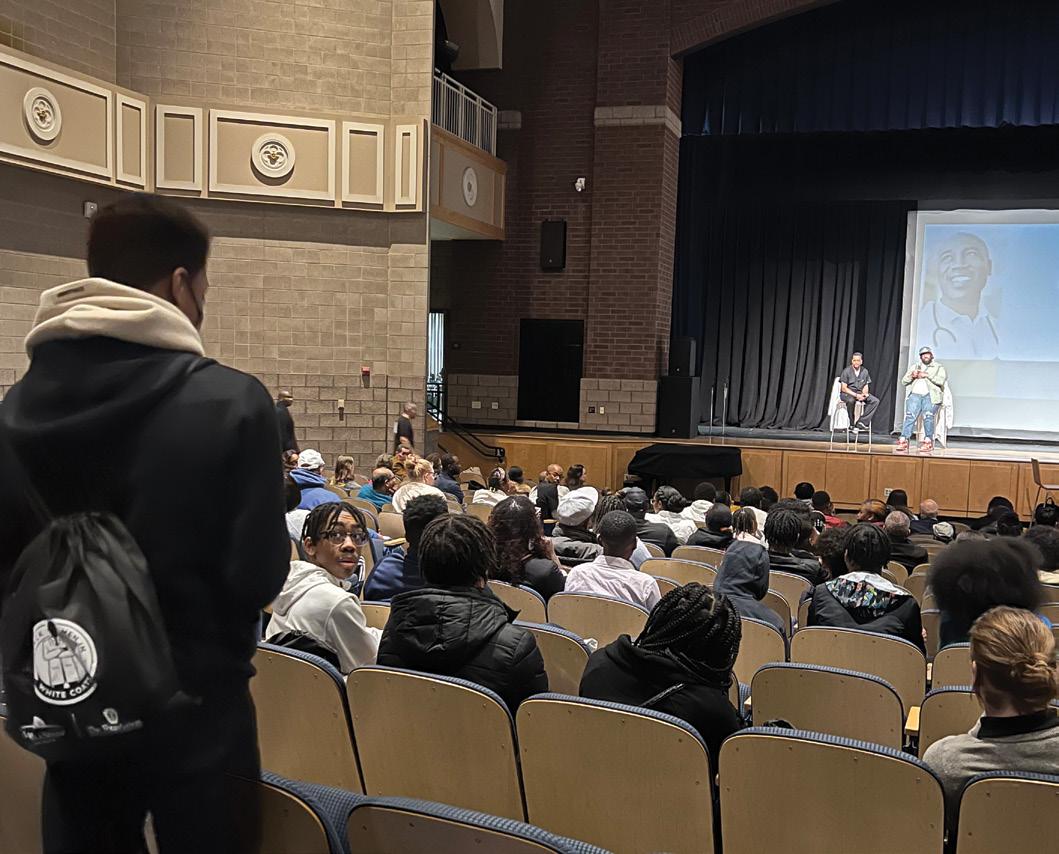
Dr. Truex says the students were counseled on the importance of caring for themselves and recognizing stress indicators in their friends and classmates. They learned about resources and how students can find help. “Medicine is a shared experience and mentors are here to help each and every one of these attendees,” he says.
Foundation Board Member Lynda Thomas-Mabine, MD, FCPP, Division Chief of Gynecology at Chestnut Hill Hospital and Section Chief for Robotic Surgery at Temple Health, travelled from Philadelphia accompanied by members of Medical Society of Eastern Pennsylvania to participate in this historic summit.
Dr. Thomas-Mabine said, “The successful event can be replicated in other areas to harness the momentum and provide shadowing opportunities. We have brought together these role models to mentor these bright students so that they can envision a successful career in medicine.”
Tolan agrees. “It was a great day that culminated in a call and response. The kids roared into the chant, ‘I can do anything! I can pursue anything!’”

The mission of the Foundation of the Pennsylvania Medical Society is to provide programs and services for individual physicians and others that improve the wellbeing of Pennsylvanians and sustain the future of medicine.

WWW.LANCASTERCOUNTRYDAY.ORG | 717-392-2916 AT LANCASTER COUNTRY DAY SCHOOL challenging academics are only the start of each student’s opportunities for personal discovery and growth. From preschool to 12th grade, LCDS students are able to develop established passions or try new activities in a supportive independent school environment.
SUMMER TOURS AVAILABLE! To book a tour, please contact the Admission Office at admissions@lancastercountryday.org or (717) 392-2916 x2228 SPRING 2023 | 35
WHERE
We are happy to make time for your patients
Eye Emergencies
Cataracts
Glaucoma
Diabetic Eye Exams
Macular Degeneration
Yes, we can see your patients same day for emergencies and often same week for consults.
At BERKS EYE PHYSICIANS AND SURGEONS, we are happy to offer state-of-the-art and efficient care. Our doctors provide appropriate diagnosis and treatment, and fast feedback to you. Whether your patient has a sudden change in vision, cataracts, diabetes impacting vision, or even has a family history of glaucoma or macular degeneration, we would be honored to monitor and react to issues related to your patient’s eye health.

610-372-0712 | berkseye.com | 1802 Paper Mill Road, Wyomissing, PA 19610 |
Left to Right: Domenic C. Izzo, Jr., MD, Benjamin Nicholas, MD, Francisco L. Tellez, MD, FACS, Kasey L. Pierson, MD, Peter D. Calder, MD, Guri Bronner, MD
