13 minute read
The lungs


The bronchial veins drain on the right to the azygos system and on the left to the hemiazygos system.
Advertisement
Radiological features
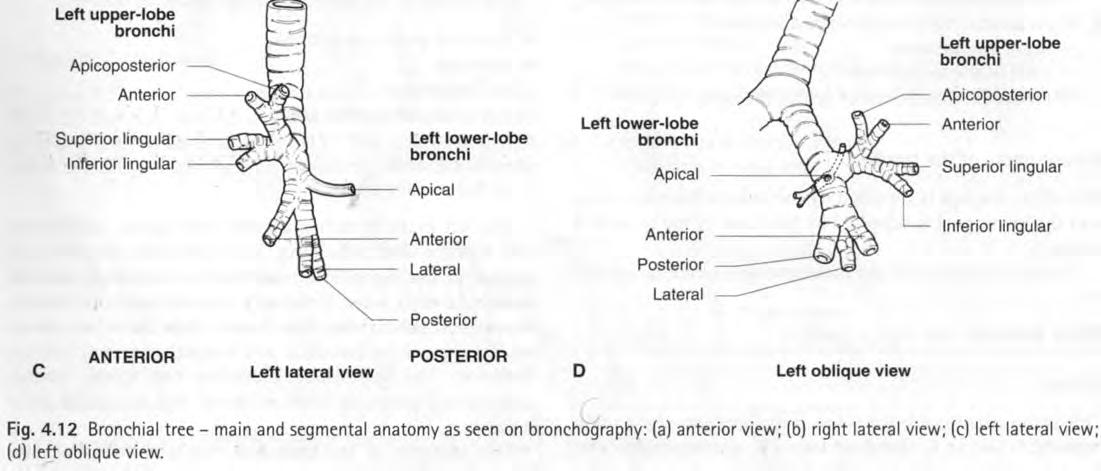
The radiological features of the trachea and bronchi are discussed in the following section on the lungs (see p. 122). THE LUNGS (Fig. 4. 13) The lungs are described as having costal, mediastinal, apical and diaphragmatic surfaces. The right lung has three lobes and the left has two, w i th the lingula of the left upper lobe corresponding to the right middle lobe.
One terminal bronchiole w i th lung tissue forms an acinus which, together w i th vessels, lymphatics and nerves,
forms the primary lobule. Three to five primary lobules form a secondary lobule.
Interlobar fissures (see Fig. 4. 8) The depth of fissures varies from a superficial slit to complete separation of lobes.
The oblique (major) fissure This is similar in both right and left lungs. It extends from T4/T5 posteriorly to the diaphragm anteroinferiorly. The left major fissure is more vertically orientated than the right. The fissures do not follow a straight plane from top to bottom but are undulating in their course. The medial aspect of each fissure passes through the hilum. The lateral aspect of each fissure is anterior to the medial aspect at the level of the hila and below. Above the hila, the relationship changes and the lateral aspect of the fissure is more posterior than the medial.
The transverse (minor) fissure This separates the upper and middle lobes of the right lung. It runs horizontally from the hilum to the anterior and lateral surfaces of the right lung at the level of the fourth costal cartilage. Its posterior limit is the right oblique fissure, which it meets at the level of the sixth rib in the midaxillary line. It is anatomically complete in only one-third of subjects and is absent in 10%.
Accessory fissures
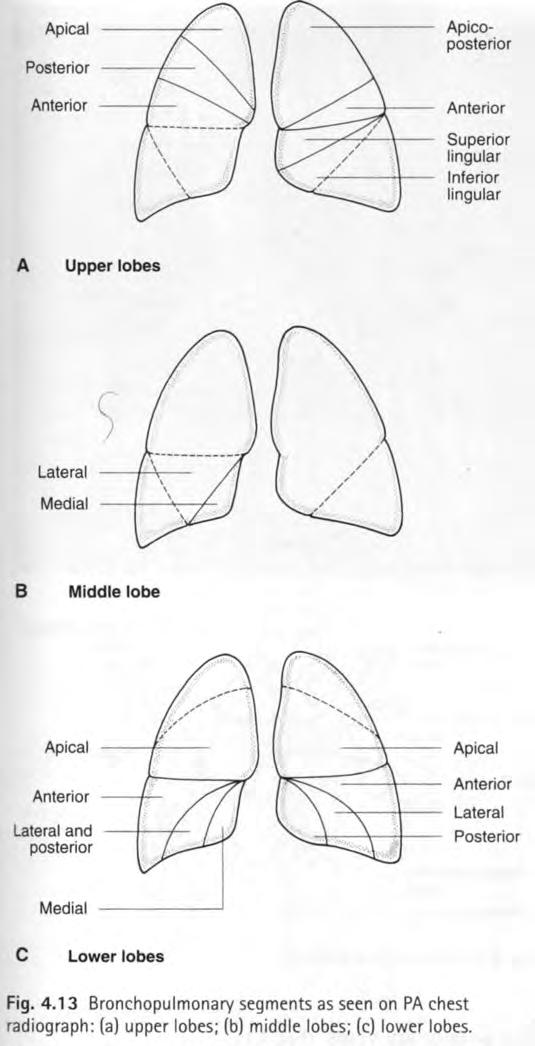
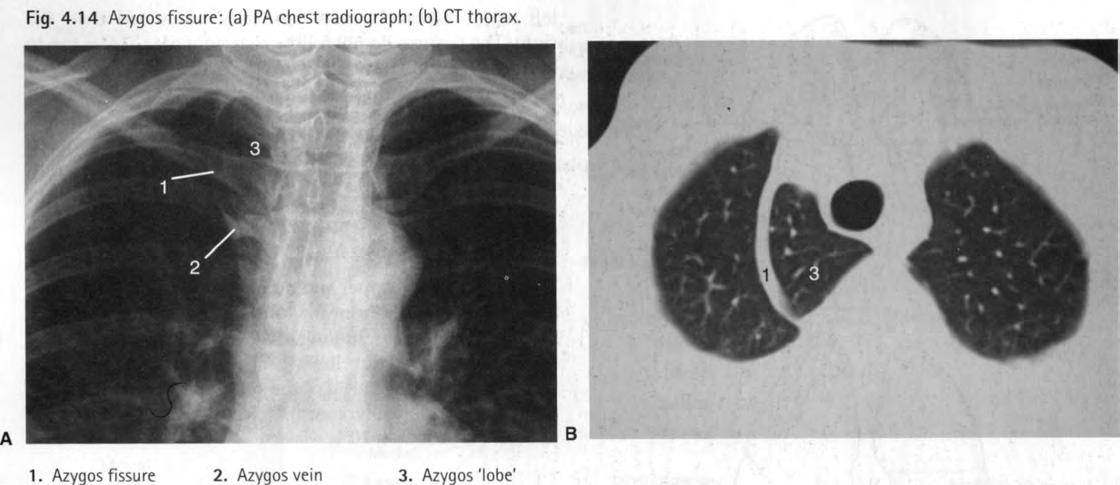
The azygos fissure (Fig. 4. 14) This is in fact a downward invagination of the azygos vein through the apical portion of the right upper lobe. It therefore has four pleural layers - two visceral and two parietal. The term 'azygos lobe' is inappropriate as there is no corresponding change in lobar architecture.
The superior accessory fissure This separates the apical segment of the right lower lobe from other basal segments. It lies parallel and inferior to the transverse fissure and passes posteriorly from the right oblique fissure to the posterior surface of the lung.
The inferior accessory fissure This separates the medial basal from other right lowerlobe segments. Called Twining's line, it is seen in 30-50% of postmortem examinations but in only 8% of PA chest radiographs.
Left transverse fissure This is found in 18% of postmortem specimens but is rarely seen on chest radiographs.
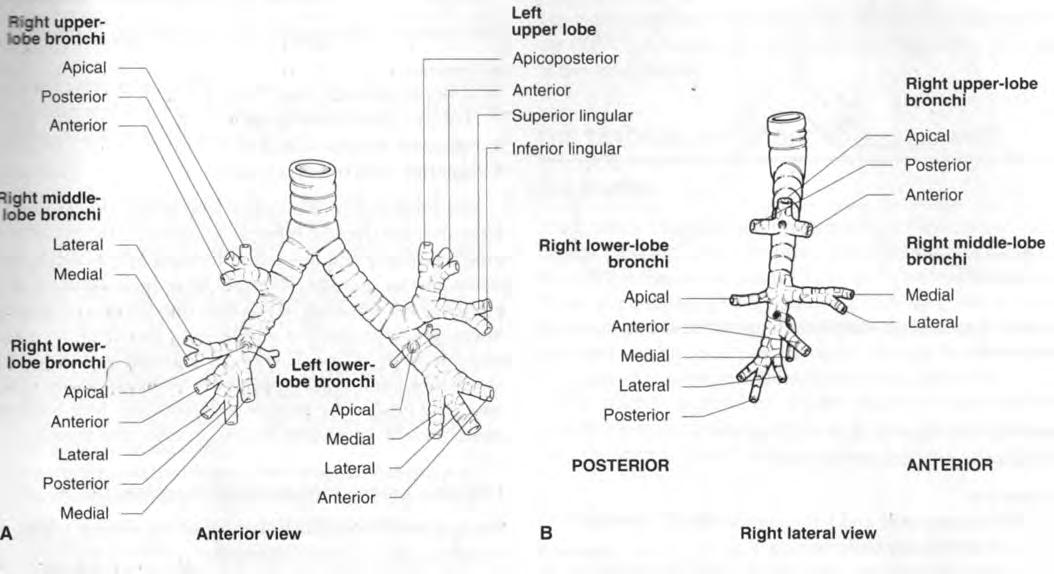
Bronchopulmonary segments (see Figs 4. 12 and 4. 13) Each lobe is subdivided into several bronchopulmonary segments, each of which is supplied by a segmental bronchus, artery and vein. Each segment takes its title from that of its supplying bronchus.
The anatomy of segmental bronchi is subject to variation, the most common being the origin of apical segmental bronchi, especially the right, from the trachea.
There is very little connection between segments except via: • The pores of Kohn: openings in the alveolar walls connecting adjacent alveolar lumens; and • The canals of Lambert: connections between terminal bronchioles and adjacent alveoli.
These allow gas and fluid transfer between segments but not between lobes. Ventilation of a segment is therefore possible when its segmental bronchus is occluded. This is called collateral air drift.
The pulmonary artery (Fig. 4. 15; see also Fig. 4. 44) (see also section on the great vessels) The pulmonary trunk leaves the fibrous pericardium and bifurcates almost at once in the concavity of the aortic arch anterior to the left main bronchus.
The right pulmonary artery is longer than the left. It passes across the midline below the carina and comes to lie anterior to the right main bronchus. It bifurcates while still in the hilum of the right lung. An artery for the right upper lobe passes anterior to the right upper-lobe bronchus. The interlobar artery to the right middle and lower lobes passes w i th the bronchus intermedius.
The left pulmonary artery spirals over the superior aspect of the left main bronchus to reach its posterior surface. It is attached to the concavity of the aortic arch by the ligamentum arteriosum.
The pulmonary arteries further subdivide into segmental arteries that travel w i th the segmental bronchi, for the most part on their posterolateral surface. The pulmonary arteries supply only the alveoli (cf. the bronchial arteries, which supply the bronchi). The pulmonary veins (Fig. 4. 16) These do not follow the bronchial pattern but tend to run in intersegmental septa. Two veins pass to each hilum - from lung tissue above and below each oblique fissure. These enter the mediastinum slightly below and anterior to the pulmonary arteries. On the right side the veins from the lobes may remain separate, so that three veins leave the right lung and enter the left atrium. On the left side the two pulmonary veins may unite and enter the left atrium as a single vessel.

The bronchial arteries
The bronchial arteries supply the bronchi, the visceral pleura and the connective tissue of the lungs. They arise

Fig. 4. 16 Pulmonary veins: DSA of pulmonary veins draining into left atrium. This angiogram was achieved by passing a venous catheter from the right atrium through a 'probe-patent' foramen ovale into the left atrium.
1. Right upper pulmonary vein 2. Left upper pulmonary vein 3. Catheter 4. Right inferior pulmonary vein 5. Left inferior pulmonary vein G. Left atrium
from the thoracic aorta in 90% of subjects, at T5 or T6 vertebral level in 80% of cases.
There are usually one right and two left bronchial arteries. The left bronchial artery arises at upper border of T5 and the lower arises from the aorta just below the left main bronchus. When a second bronchial artery occurs on the right side it often arises from the third intercostal artery.
Bronchial arteries may also arise from the subclavian artery or from its internal thoracic branch.
Tissues supplied by bronchial arteries drain to pulmonary veins or bronchial veins.
Bronchial veins
Bronchial veins form two distinct systems. The deep veins form a network of veins around the pulmonary interstitium and communicate freely w i th the pulmonary veins. They also form a bronchial vein trunk that drains to the pulmonary system. The superficial bronchial veins drain to the azygos vein on the right side and to the accessory hemiazygos vein on the left side.
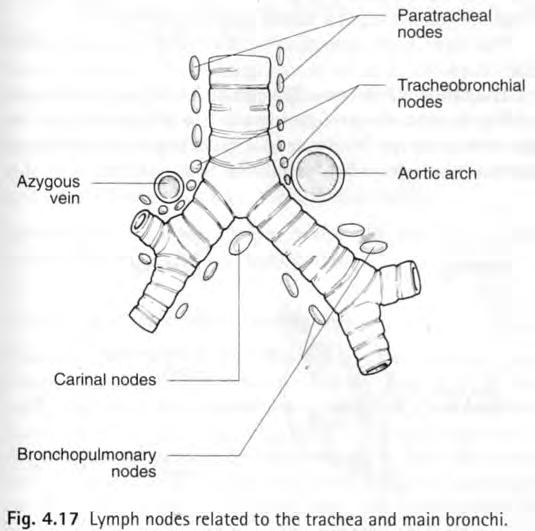
Lymphatics (Fig. 4. 17) Mediastinal lymph nodes that drain the lung are named according to their position: • Pulmonary nodes within the lung substance; • Bronchopulmonary nodes at the hilum; • Carinal nodes below the hilum; • Tracheobronchial nodes above the tracheobronchial junction; and • Right and left paratracheal nodes on either side of the trachea.
The lymph vessels of the lung are in superficial and deep plexuses. The superficial plexus beneath the pleura drains around the surface of the lungs and the margins of the
fissures to converge at the hila and the bronchopulmonary nodes. The deep channels drain w i th the pulmonary vessels towards the hila. There are few connections between the superficial and deep plexuses except at the hila. The bronchopulmonary nodes drain to the tracheobronchial nodes and the paratracheal nodes and thence to the bronchomediastinal trunks.
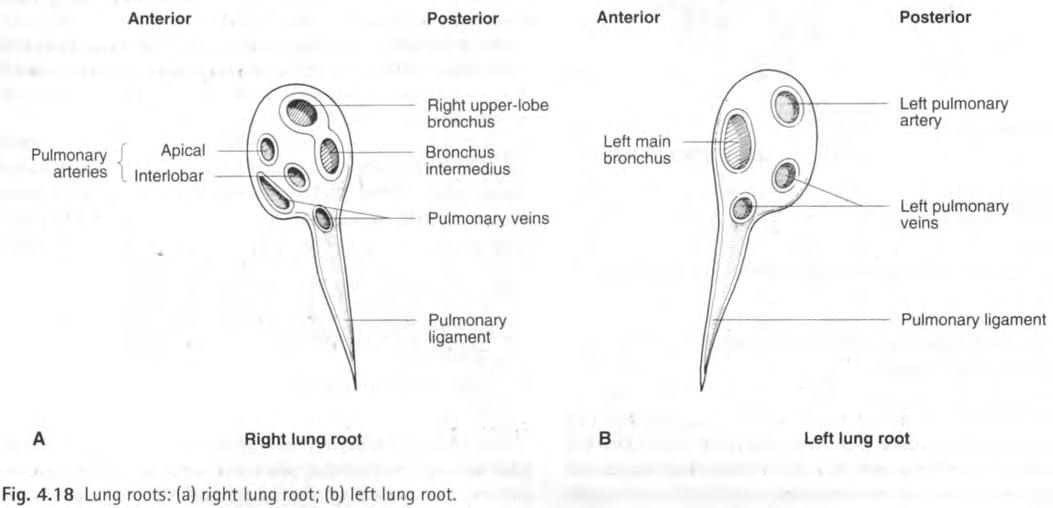
Lung roots (Fig. 4. 18) The roots of the lungs are formed by the structures that enter and emerge at the hila. They lie at vertebral levels T5-T7. The right lung root lies below the arch of the azygos vein and posterior to the superior vena cava and the right atrium. The left lung root lies below the arch of the aorta and anterior to the descending aorta.
Radiological features of the lung and bronchial tree
PA chest radiograph (see Fig. 4. 6) Fissures Fissures are only seen if tangential to the beam, and because of curvatures in three dimensions they are seldom seen in their entire length. The transverse fissure of the right lung is seen in 80% of dissection specimens but only 50% of chest radiographs. The azygos fissure, although found in 1% of postmortem subjects, is seen in 0. 4% of radiographs w i th the 'teardrop' shadow of the azygos vein in its lower end. The superior accessory fissure is seen in 5% of chest radiographs and, when present, is at a lower level than the transverse fissure. The inferior accessory fissure is seen in 8% of chest X-rays (CXR), 20% of high-resolution CT scans and 30-50% of anatomical specimens. The left transverse fissure is seen in less than 2% of CXR, 9% of high-resolution CT scans and 18% of anatomical specimens. Trachea The trachea is seen as a midline translucency w i th a slight inclination to the right in its lower half. Its lumen is 1. 5-2 cm in diameter.
The right paratracheal stripe (normally < 3 mm) is formed by the right wall of the trachea and the pleura, outlined on both sides by air. The left side of the trachea is not seen separately from the mediastinal shadows.
A smooth indentation on the trachea is commonly seen just above the bifurcation on the left side. This is caused by the arch of the aorta.
Gross AP or side-to-side (usually to the right side, owing to the aortic arch) displacement may be normal in a child, especially on an expiratory radiograph. Bronchi The bronchi contribute very little to the lung markings seen on plain films. The proximal bronchi may, however, be seen if outlined by the lungs.
On the frontal chest radiograph the posterior segmental bronchi of the left upper lobe and those of the apical segments of both lower lobes are often seen end-on. Their corresponding pulmonary arteries may be seen accompanying the bronchi as circular densities of about the same size. The right pair is higher than the left as the upper-lobe bronchus comes off at a higher level on the right.
The right main bronchus is orientated more vertically than the left.
The bronchus intermedius can be identified to the right of the cardiac shadow and medial to the density of the interlobar artery. The lower-lobe bronchus on the left is not normally seen, as it lies behind the heart shadow.
Bronchopulmonary segments These are depicted in
Figure 4. 13.
Pulmonary vasculature The vessels account for most of the lung markings.
The pulmonary trunk forms part of the left border of the heart. The interlobar artery is seen lateral to the bronchus intermedius on the right. This should not measure more than 16 mm midway down its visible length.
Bronchi and arteries are seen together radiating out from the hila. Pulmonary veins enter the mediastinum lower than the arteries as they converge toward the posterior aspect of the left atrium. This means that: • In the upper zone the veins are inferolateral to the arteries; and • In the lower zone the veins are almost horizontal and the arteries almost vertical.
The inferior pulmonary veins drain anteriorly and superiorly from the lung bases to the left atrium. Owing to their more horizontal course, if seen end-on on the chest film they may simulate a pulmonary mass.
The hilar point is where the upper-lobe vein crosses the descending pulmonary artery. The right hilar point is projected over the sixth posterior interspace and is 1 cm lower than the left.
The hilar angle is the angle between the vessels at the hilar point - normally 120°. Situs inversus The identification of situs inversus (see Fig. 4. 11) is helped by the appearance of the main bronchi on high-voltage chest radiographs or tomography. The morphological right lung, whether on the right or the left side of the thorax, is trilobed, has a short main bronchus, and has its bronchus above its pulmonary artery. Lymphatics Normal lymph nodes do not form discernible densities on plain radiographs.
Lateral chest radiograph (see Fig. 4. 7) Fissures The left oblique fissure is more vertical and reaches the diaphragm more posteriorly than that on the right. The left oblique fissure is at an angle of 60° to the horizontal, and the right at an angle of 50°. The anterior ends of the oblique fissures are 2-3 cm behind the anterior chest wall. Occasionally the upper end of the oblique fissure may reach T3. As the fissures are undulating, they may appear to be doubled in parts and are often not seen in entirety. For the same reason the posterior part of the transverse fissure may occasionally seem to cross the right oblique fissure. Where there is a superior accessory fissure, this extends posteriorly from the oblique fissure. Trachea On a lateral chest radiograph (see Fig. 4. 7) the trachea is seen to enter the thorax midway between the sternum and the vertebrae. Owing to some posterior inclination it ends closer to the vertebrae.
The posterior paratracheal stripe is formed by the posterior wall of the trachea and the pleura and is visible if the lung passes behind the trachea.
The tracheo-oesophageal stripe is formed by the posterior wall of the trachea and the anterior wall of the oesophagus. It is visible if there is air in the oesophagus. Bronchi On a lateral chest radiograph (see Fig. 4. 7) the left main bronchus, being more horizontal, is seen as a circular structure. The right main bronchus is more vertical and is therefore tubular on this view. The left pulmonary artery is seen as a comma-shaped density passing backwards over the left main bronchus.
The posterior wall of the right main bronchus and its division into upper-lobe bronchus and bronchus intermedius are often visible as a thin stripe as they are in contact w i th the lung. On the left side, however, the pulmonary artery and its branches are posterior to the bronchus and thus obscure the view of its posterior wall.
The upper-lobe bronchi may be seen as two rounded radiolucencies projected over the lower end of the trachea, w i th the right being 1-2 cm higher than the left. The right upper-lobe bronchus is seen about half the time and the left in about 75% of cases. The left has more sharply defined margins as the pulmonary artery lies superiorly and the superior pulmonary vein lies inferiorly
The lower-lobe bronchi may be seen running in an inferoposterior course in many cases. The left lower-lobe bronchus is the more posterior and has a curved configuration in its anterior aspect, merging w i th the orifice of the upper-lobe bronchus. Vasculature The pulmonary arteries may be seen at the hilum forming a conglomerate density w i th the pulmonary veins. The right pulmonary artery is seen end-on and is oval in appearance. The left pulmonary artery is commashaped as it arches over the left main bronchus. They may each measure up to 3 cm in diameter.
The confluence of the pulmonary veins is seen below the oval density of the right pulmonary artery on the lateral film. The superior veins are more anterior than the inferior pulmonary veins.
Pulmonary angiography A catheter is inserted via the femoral vein to the inferior vena cava (IVC), right heart and pulmonary trunk. The pulmonary trunk inclines posteriorly as it leaves the heart and is best seen when the beam is angled at 45° to the anterior chest wall. The pulmonary arteries and branches are seen as described above. Pulmonary veins are seen in the venous phase.
Bronchial angiography This is used in the diagnosis and embolic treatment of haemoptysis. The bronchial arteries are catheterized from








