
1 august 24,2022 j our nale TheExplanationAndTheSolution Crucial Trends ToKnow About Critical Access Hospitals Guidance FromCMS Addressing Contested DRGDocumentation TheEnd Of COVID PHE? What IsDRG Downgrade?


On August 18, 2022, CMSpublished a blog that offers guidance in preparing for the eventual end of the COVID 19 Public Health Emergency (PHE): https://www.cms.gov/blog/creating roadmap end covid 19 public health emergency
By watching data during the pandemic, CMShas assessed how ending flexibilities will impact patient care While it will be necessary to end many flexibilities to ensure quality and safety, continuing other flexibilities has proven beneficial and will continue after the PHEends. Through its "roadmap," which will be updated as changes occur, CMSoffers guidance for health care providers and facilities to transition to pre-pandemic operations following the end of the PHE. The detailed COVID 19 Emergency document outlines each 1135(b) waiver, provides examples of the waiver use, and states each waiver's fate at the conclusion of the PHE.
2 PARA Weekly eJournal: August 24, 2022
CMSrecognizes that health care providers have relied heavily on 1135(b) and emergency waivers that allowed continued health care throughout the PHE HHSSecretary Becerra will provide 60 days of advanced written notice before ending the PHE, which will term many of those waivers
CMSOFFERSGUIDANCETO PREPAREFORTHEEND OFCOVID 19 PHE
The current PHEis extended to October 13, 2022, which is now less than 60 days, indicating providers will see at least one more extension


19 emergency declaration waivers
https://www cms gov/files/document/covid
CMSOFFERSGUIDANCETO PREPAREFORTHEEND OFCOVID 19 PHE
1. CMSis determining which blanket waivers provide the flexibilities still needed
CMSwill implement three concurrent phases to prepare Hospitals, CAHs, ASCs and CMHCs for the end of the PHE
CMSprovides examples of flexibilities granted during the PHEto these providers. CMSassures they are actively monitoring each of the waivers and will update the document below to assist Hospitals, CAHS, ASCs and CMHCs with preparing for operations at the end of the PHE: https://www cms gov/files/document/hospitals and cahs ascs and cmhcs cms flexibilities fight covid 19 pdf
2 In the event of a future public health emergency, CMSis assessing which flexibilities were most successful 3 CMSis collaborating with the healthcare industry and partners to ensure preparedness in the event of another public health emergency
3 PARA Weekly eJournal: August 24, 2022



Highlights of the comprehensive CMSFlexibilities for Hospitals, CAHs, ASCs and CMHCs include: COVID 19 vaccines? CMSwill continue paying for the vaccines through the end of the calendar year in which the PHEis ended Then they will shift the coverage under Medicare Part B preventative services CMS Hospit als w it hout Walls? the flexibility that allowed hospitals (including CAHs) to provide services outside hospital departments will end with the PHE, and the CoPof CFR parts 482 and 485 will be enforced. Termination of remote hospital-only outpatient therapy (PT/OT/SLP) and education services provided in the patient's home will occur at the end of the PHE - Crit ical Access Hospit als? at the end of the PHE, CMSwill resume the requirement that limits the length of stay to 96 hours and the number of beds to 25 - C9803 Specim en Collect ion for COVID-19? the payment for this service will be packaged into the COVID 19 test after the PHEends Rem ot e Behavioral Healt h Services by clinical staff of the hospital ? the continuation of these services remains in question but are proposed in the 2023 OPPS/ASCrule, still in comment period, to remain
CMSstates the outcome of several flexibilities will be determined in the final 2023 OPPS/ASCand the Physician Fee Schedules, which are in comment period
CMSOFFERSGUIDANCETO PREPAREFORTHEEND OFCOVID 19 PHE
4 PARA Weekly eJournal: August 24, 2022

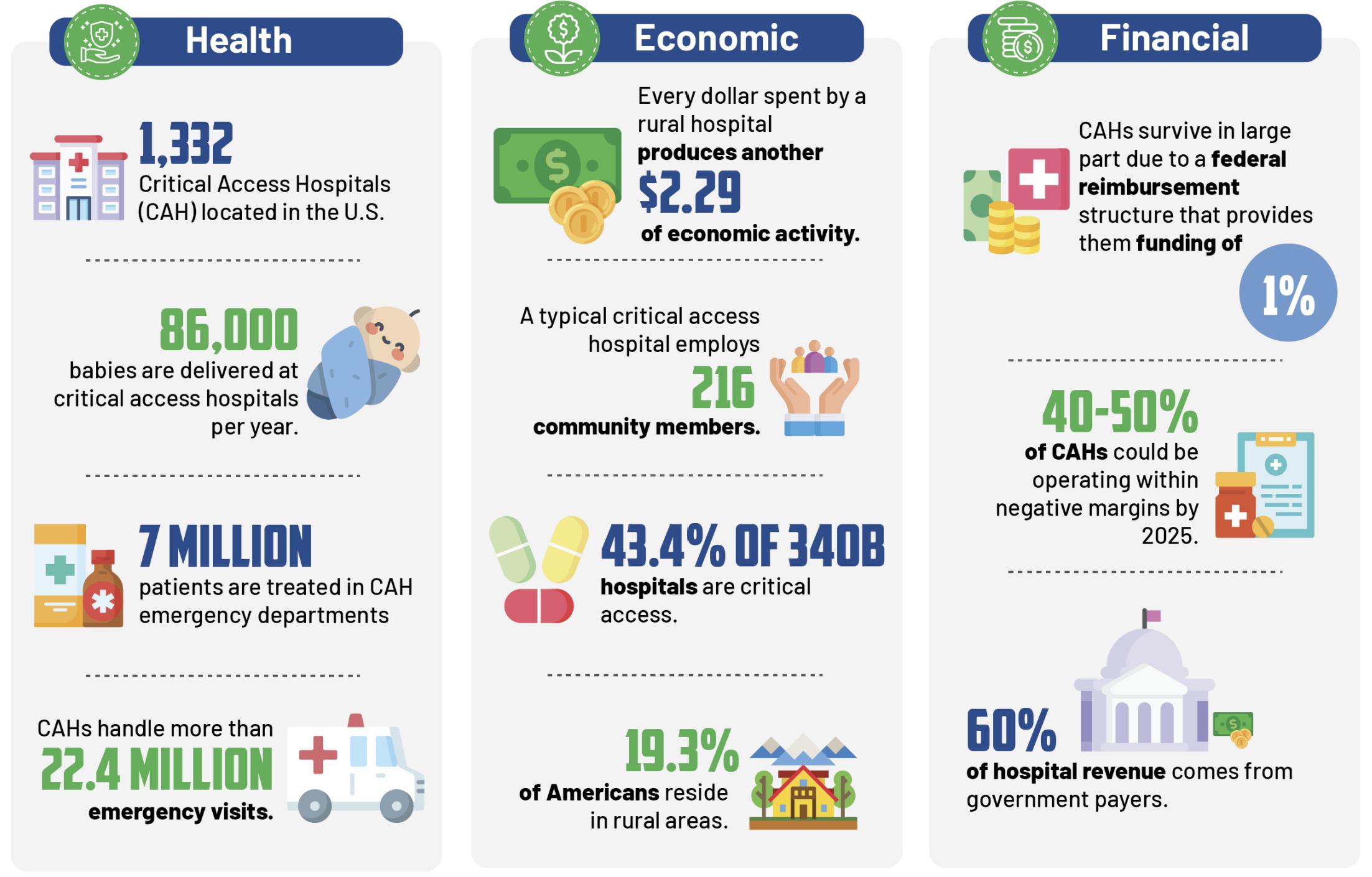
Despiteoperatingastheprincipal healthcareoptionfor millionsof patients,manyCritical AccessHospitals(CAH)aremost vulnerableof closingtheir doorsduetoseveral challengesthat makerevenuecycle management difficult. These challenges are often the result of low operating margins, difficult patient populations, and staffing shortages. Our experience has taught us that no two hospitals?revenue cycles are the same. What makes revenue cycle management more difficult in the rural hospital setting?And how can these organizations overcome key operational challenges originating from their unique position? Crucial trends that are affecting Critical Access Hospitals right now
CRUCIAL TRENDSAFFECTINGCRITICAL ACCESSHOSPITALS RIGHTNOW
5 PARA Weekly eJournal: August 24, 2022
Patient characteristics heavily influence hospital revenue cycles Residents in rural regions are more likely to experience socioeconomic and clinical challenges, resulting in higher costs than their non rural contemporaries do. As a result, hospitals have trouble negotiating with private payers and do not have the same leverage as facilities in densely populated regions to negotiate higher claim reimbursement rates. Another challenge CAHs face is working with a limited budget for healthcare technology investments. Like other industries, healthcare is adopting technology to improve quality, productivity, and maximize revenue Implementing technology can streamline the process allowing for optimal patient focused operations leading to full value recognition for the services provided. Due to tighter operating margins, CAHs may not have the means to implement and upgrade their technology like their larger competitors do We usually find that CAHs that manage their revenue cycle in house often operate with a limited staff wearing multiple hats.

6 PARA Weekly eJournal: August 24, 2022 It is imperative to your bottom line to employ a staff that is multi talented and can manage several mission-critical tasks covering multiple disciplines. However, limited access to talent in a low population area often means less qualified candidates, more open positions, and an overworked staff This can lead to burn out of existing staff and create turnover Crit ical Access Hospit als provide essent ial m edical care t o rural com m unit ies across t he count ry. CRUCIAL TRENDSAFFECTINGCRITICAL ACCESSHOSPITALS RIGHTNOW
It is also imperative for them to highlight and address chronic under performance or inconsistent performance within your organization to eliminate the issue Hospitals must carefully manage their vendor(s) and hold them accountable with performance metrics Given the unprecedented financial pressures and need to recover every dollar, we are connecting with revenue cycle leaders to offer a complimentary review of areas that are often overlooked
CAHs experiencing these challenges have benefited from a full or partial outsource of their revenue cycle
Please go to Aergo com to learn more about our services and schedule a consultation
Outsourcing can expand your talent pool, allow access to complementary technology that can integrate with your current system, and assist with maximizing reimbursements.
Out sourcing As A Solut ion
Denial and Accounts Receivable experts often have vast payer experience due to the fact that they deal with various payers across multiple services lines. Often these subject matter experts can articulate industry expertise, act as a payer liaison, and share payer experiences
All vendors are not the same, so you want to make sure you consider firms that have experience in working with CAHs or hospitals that work in a similar capacity with documented success. It is important that this firm is current with payer practices and policy changes.
Aergo Solutions has developed a strong track record of getting more revenue from hidden opportunities within Accounts Receivable, Denials, and DRG issues
7 PARA Weekly eJournal: August 24, 2022
CRUCIAL TRENDSAFFECTINGCRITICAL ACCESSHOSPITALS RIGHTNOW

8 PARA Weekly eJournal: August 24, 2022
NAVIGATINGTHENO SURPRISESACTMAZE
- The Trump Administration first introduced legislation requiring hospitals to publish their pricing effective January 1, 2021 The No Surprises Act of January 1, 2022 protecting insured patients from balanced billing in cases of emergency or when required to use out of network care at an in network facility - Current requirements for providers to deliver a Notice and Consent (NAC) form for insured patients who choose to continue with out of network care in an out of network facility - Current requirements for providers to produce a Good Faith Estimate for uninsured patients
Hist ory of t he No Surprises Act
These included:
Effective January 1 of 2023, the latest installment of No Surprises Act stipulates that affiliated co-providers will become responsible for producing their own Good Faith Estimates (GFEs). These affiliated co providers, such as anesthesiologists and pathologists, practice in hospitals but handle their own billing. In 2023, the convening provider who schedules the surgery or appointment must take the GFEs produced by affiliated co providers and their own GFEand combine them into a consolidated Good Faith Estimate These Good Faith Estimates will be required for both uninsured and insured patients. These upcoming changes will mark the most recent phase of a series of regulations designed to increase transparency in the healthcare industry
The Solut ion ParaRev offers software seamlessly that creates customized GFEs, and an application for convening and affiliated co providers to collectively produce a consolidated Good Faith Estimate
Regulations call for the creation of NACs and GFEs for all patients, both insured and uninsured
What does t his m ean?
NAVIGATINGTHENO SURPRISESACTMAZE
Like all group projects, the shared creation of consolidated GFEs (and NACs) between convening providers and affiliated co providers will require extensive communication, cooperation, and flexibility.Without an established and shared document management system that records a paper trail of requests and fulfillments, providers face the logistical nightmare of trying to coordinate and produce an already complex and now consolidated regulatory document.
Since the inception of pricing transparency regulations in 2020, affiliated co-providers have faced no regulatory scrutiny. All compliance responsibilities have fallen upon convening providers. As a result, the legal requirements of the No Surprises Act are not even on the radar of most affiliated co-providers.
Combined with years of disregard to impending NSA regulations, affiliated co providers risk finding themselves swamped by compliance catch up work
Come
By providing a central location for the upload of these documents, PARA?s application manages and simplifies the logistics and communication between busy and understaffed healthcare providers, helping all parties to comply with 2023 NSA regulations and avoid fines
The Issue of addressing t he 2023 No Surprises Act
January 1, 2023, all the responsibilities required of convening providers will be extended to affiliated co providers, making them equal partners in compliance 2023 regulations stipulate that GFEs must be produced for all patients, regardless of insurance status
9 PARA Weekly eJournal: August 24, 2022
TheRegulation RequiresFocusand Expertise
Even for providers familiar with GFEand NACproduction, the pure increase in quantity of GFEs and NACs needing to be produced is sure to overwhelm their systems
Affiliated Co-ProvidersareUnaware
TheQuantityof Workisa LogisticNightmare
For the few who are aware, a series of delays and leniency from CMShas given the impression that enforcement will never come This attitude leaves affiliated providers inexperienced and unprepared to face impending 2023 regulations
CMSis incredibly particular about not just what information providers must supply, but how it is presented The complex and convoluted regulations are constantly changing and evolving as interpretations differ and legal questions arise Healthcare providers truly require a dedicated team with the regulatory expertise to ensure that they remain in compliance Unfortunately, many providers lack the bandwidth and resources to dedicate a team solely to CMScompliance
Diagnosis related groups, often known as DRGs, are payment classifications for patients with a similar condition Usually, patients with the same classification are expected to utilize similar resources while hospitalized. Payer and audit firms downgrade a DRG by contesting the diagnosis code(s) documented in the patient?s medical records Historically, downgrades have occurred because coding validation has been so infrequently done However, over the last few years downgrades have become a growing problem across most payers utilizing DRG reimbursement methodologies. It?s concerning that DRG downgrades are now almost always about the clinical relevance of the diagnosis
10 PARA Weekly eJournal: August 24, 2022 What Is ADRGDowngr ade?
Over 50% of t he dow ngrades are post -pay audit s on zero balance account s oft en going back one t o w o years. These audit s follow a pat h t hat differs from t radit ional appeals.
t
DRGDOWNGRADES: IDENTIFYINGAND COMBATINGHIDDEN DENIALS

11 PARA Weekly eJournal: August 24, 2022 DRGDOWNGRADES: IDENTIFYINGAND COMBATINGHIDDEN DENIALS

Most payers send a letter to notify the hospital of a downgrade, and in most cases, will only accept appeal documentation sent by certified mail Appeal
Typically, downgrades resulting from post pay audits allow for a 60 day pre recoupment and an additional 60-180 day post-recoupment.
Payer Audit Triggers
DRGDOWNGRADES: IDENTIFYINGAND COMBATINGHIDDEN DENIALS
Sepsis - Pneumonia Kidney/UTI Sepsis DXcodes continue to prompt most DRG downgrades Additionally, DXcodes that are unspecified? such as ?unspecified sepsis?and ?unspecified pneumonia?or ?acute?on chronic conditions? are triggers HIM representatives often attempt to appeal these denials from a coding perspective. Clinician appeals are often required when HIM is unsuccessful. Clinicians certified in coding have the highest success rate, since downgrades for clinical validation require both medical necessity and coding review
Sepsis is a severe illness caused by the body?s response to infection. Sepsis progresses when the chemicals in the immune system release into the bloodstream to fight an infection, causing inflammation throughout the entire body Severe cases of sepsis can lead to septic shock, which can turn into a life-threatening medical emergency. According to our data, about 75% of the DRG downgrades we see are for sepsis, and there is little sign of those denial rates slowing down.
The best way to avoid these denials is to make sure that all relevant criteria are present from the beginning of treatment, but also that the treatment plan is consistently and accurately documented, as this diagnosis is vulnerable to DRG downgrades
12 PARA Weekly eJournal: August 24, 2022
The difference between Sepsis 2 vs. Sepsis 3 Sepsis 2 is defined as two or more SIRScriteria and infection on the same day Sepsis 3 is defined as an increase in SOFA score of two or more in conjunction with an infection.
Timely Filing guidelines may differ , depending on the DRG Downgrade
Diagnosis codes tied to the following DRGs frequently prompt audit review:
The Grow t h Of Sepsis Denials
Although it may seem intimidating or unnecessary to recruit outside assistance in handling these stubborn denials, it can alleviate stress on your in-house billing team, in addition to recovering millions of dollars in owed revenue.
13 PARA Weekly eJournal: August 24, 2022
How AI Program s Im pact Denials
The primary goal should be to quantify the problem by getting the billing department, case management, and HIM teams together Analysis must be performed to determine what is getting downgraded and if preventative measures in coding/or physician documentation can be put into place
It is imperative to track and identify problem payers and audit firms It is likely that some payers and audit firms are being unreasonable and/or aggressive in denying payment at the originally billed DRG.
There may also be language within the hospital's managed care contracts that could prevent or limit this behavior Each patient is different, and the treating physician is best suited to determine the appropriate level of care. The fact that downgrades often occur in the complete absence of a medical record proves that the pages and audit firms rely on their algorithms and statistics without any clinical considerations.
DRGDOWNGRADES: IDENTIFYINGAND COMBATINGHIDDEN DENIALS
The best way to achieve this goal: Develop a denial task force, including RCM experts - Create clear guidelines for physicians to produce precise clinical documentation Make sure the denial team has full access to the patient?s documentation
Due to the use of AI programs and technology the number of DRG downgrades and other unpaid claims can become overwhelming for hospitals' billing and coding departments
Hospitals are becoming inundated with so many DRG downgrades that handling them can become overwhelming for HIM and coding departments With staffing shortages becoming a reality for some organizations, it is essential to create a denial task force. Depending on the size of the hospital this team should consist of PFS, HIM, Case Management, and an outside agency, depending on the volume.
Creat ing An Int ernal Process

14 PARA Weekly eJournal: August 24, 2022 DRG Dow ngrade Sam ple Case St udy: $59,788 Appeal Overt urned About t he Pat ient : Patient is a 61 year old female with past medical history significant for Cholangiocarcinoma, Congestive Heart Failure, Pulmonary Nodule, admitted from 12/1/2020 ? 12/4/2020 for diagnoses including acute hypoxic respiratory failure secondary to hemothorax Principal Diagnosis: J95 71 Accidental Puncture and Laceration of a Respiratory System Organ of Structure During a Respiratory System Procedure. Secondary Diagnosis: J96.01 Acute Respiratory Failure with Hypoxia DRG Billed: 951 4 Moderately Extensive Procedure Unrelated to Principal Diagnosis ? Severity 4 - DRG Approved: 951-3 Moderately Extensive Procedure Unrelated to Principal diagnosis ? Severity 3 DXin Question: J9601 Acute Respiratory Failure with Hypoxia Review er Rat ionale: The hospital correspondence was reviewed and the submitted documentation from the medical record was examined The DRG of 951 4, as originally submitted by the hospital, was correct The audit finding has been overturned, and no further hospital action is needed. DRGDOWNGRADES: IDENTIFYINGAND COMBATINGHIDDEN DENIALS
15 PARA Weekly eJournal: August 24, 2022 This is it .Par aRev hascompl et ely updat edit s Compr ehensive COVID-19Guide.TheGuidecontains detail edinfor mat ionabout bil l ingandcoding,t est ingandot her guidancer el at edt oCOVID-19. It's online. You can download it by clicking the image to the right, or by clicking the URL here: https://apps.parahcfs.com/para/ Documents/ 2022%20Comprehensive% 20Covid-19%20Guide pdf COMPLETELY UPDATED: COMPREHENSIVECOVID 19 GUIDE


16 PARA Weekly eJournal: August 24, 2022 MLN CONNECTS PARA invit es you t o check out t he m lnconnect s page available from t he Cent ers For Medicare and Medicaid (CMS) It 's chock full of new s and inform at ion, t raining opport unit ies, event s and m ore! Each w eek PARA w ill bring you t he lat est new s and links t o available resources Click each link for t he PDF! Thursday, August 18, 2022 New s CMSDiscontinuing the Use of Certificates of Medical Necessity and Durable Medical Equipment Information Forms to Increase Efficiency and Reduce Burden for Clinicians, DMESuppliers, and Beneficiaries Quality Payment Program: Comment on Proposed Changes by September 6 - Skilled Nursing Facilities: Participate in Interoperability Survey Home Health: Revised Guide to Help Desks Claim s, Pricers, & Codes Claim Status Category and Claim Status Codes Update Event s Home Health OASIS EVirtual Workshops ? September 13 & 14 MLN Mat t ers® Art icles - International Classification of Diseases, 10th Revision (ICD-10) and Other Coding Revisions to National Coverage Determinations (NCDs) ? January 2023 Update International Classification of Diseases, 10th Revision (ICD 10) and Other Coding Revisions to National Coverage Determinations (NCDs) ? January 2023 Update ? 2 of 2 Quarterly Update for Clinical Laboratory Fee Schedule (CLFS) and Laboratory Services Subject to Reasonable Charge Payment Update to Hospice Payment Rates, Hospice Cap, Hospice Wage Index, and Hospice Pricer for FY 2023 Remittance Advice Remark Code (RARC), Claims Adjustment Reason Code (CARC), Medicare Remit Easy Print (MREP) and PCPrint Update ? Revised

17 PARA Weekly eJournal: August 24, 2022 MLN CONNECTS PARA invit es you t o check out t he m lnconnect s page available from t he Cent ers For Medicare and Medicaid (CMS) It 's chock full of new s and inform at ion, t raining opport unit ies, event s and m ore! Each w eek PARA w ill bring you t he lat est new s and links t o available resources Click each link for t he PDF! Thursday, August 18, 2022 New s Creating a Roadmap for the End of the COVID 19 Public Health Emergency Health Care System Resiliency (PDF) Preparing the Health Care System for Operation After the Public Health Emergency: Secretary of Health and Human Services (HHS) Xavier Becerra extended the existing COVID 19 public health emergency (PHE) through October 15, 2022 ? and has committed to providing states, health care providers, and other stakeholders a 60-day notice before ending the PHE.

18 PARA Weekly eJournal: August 24, 2022 Therew ereTEN new or revised Transmittalsreleased thisw eek. To go to thefull Transmittal document simply click on thescreen shot or thelink. 10 t r ans mit t al s

19 PARA Weekly eJournal: August 24, 2022 TRANSMITTAL R11570SS

20 PARA Weekly eJournal: August 24, 2022 TRANSMITTAL R11568OTN

21 PARA Weekly eJournal: August 24, 2022 TRANSMITTAL R11569OTN

22 PARA Weekly eJournal: August 24, 2022 TRANSMITTAL R11567CP

23 PARA Weekly eJournal: August 24, 2022 TRANSMITTAL R11561CP

24 PARA Weekly eJournal: August 24, 2022 TRANSMITTAL R11558CP

25 PARA Weekly eJournal: August 24, 2022 TRANSMITTAL R11566CP

26 PARA Weekly eJournal: August 24, 2022 TRANSMITTAL R11565CP

27 PARA Weekly eJournal: August 24, 2022 TRANSMITTAL R11564CP
28 PARA Weekly eJournal: August 24, 2022 TRANSMITTAL R11557MSP
29 PARA Weekly eJournal: August 24, 2022 0 m edl ear ns Therew ereNOnew or revised MedLearnsreleased thisw eek. To go to thefull Transmittal document simply click on thescreen shot or thelink.

30 PARA Weekly eJournal: August 24, 2022 MEDLEARN MM12765
31 PARA Weekly eJournal: August 24, 2022 MEDLEARN MM12870

32 PARA Weekly eJournal: August 24, 2022 MEDLEARN MM12274
best
33 PARA Weekly eJournal: August 24, 2022
you
legal/regulatorylandscapethisinformation
for instructional
thisdocument maybereproduced
ParaRev.
applied. You expresslyaccept and agree to
document isconfidential and proprietaryto
recording and broadcasting, or
disclaimsanyresponsibilityfor anydirect
FORYOURINFORMATION
As always, we
We
you
ParaRev?s
your
Theprecedingmaterialsare purposesonly. Theinformation ispresented "as-is"and to the of knowledgeisaccurate at thetime of distribution. However, dueto theever changing issubject to modification, asstatutes/laws/regulationsor other isintended to constitute, or should berelied on as, legal advice ParaRev expressly or consequential damagesrelated in anywayto anythingcontained on an ?as-is?basisand should beindependentlyverified beforebeing thisabsoluteand unqualified of liability.Theinformation in this ParaRev and isintended onlyfor thenamed recipient. No part of or without expresspermission. Permission to reproduce or includingpresenting, photocopying, byanyinformation retrieval system must be obtained in writingfrom Request for permission should be directed to sales@pararevenue.com. ParaRev is excited to announce we have joined industry leader CorroHealt h to enhance the reach of our offerings! ParaRev services lines are additive in nature strengthening CorroHealt h?s impact to clients?revenue cycle. In addition, you now have access to a robust set of mid cycle tools and solutions from CorroHealt h that complement ParaRev offerings In terms of the impact you?ll see, there will be no change to the management or services we provide The shared passion, philosophy and cultures of our organizations makes this exciting news for our team and you, our clients While can review the CorroHealt h site HERE, we can coordinate a deeper dive into any of these solutions Simply let us know and we?ll set up a meeting to connect. are available to answer any questions you may have regarding this news thank for continued partnership
disclaimer
distributed
transmit in anyform or byanymeanselectronicor mechanical,
updatesbecomeavailable. Nothingherein constitutes,
storageand
in thematerials, which areprovided

