

1 FEBRUARY1,2023 j our nal e Regulatory Brief A CorroHealth Company Pacemaker Procedures IsWaitingOn NSA ReallyA GoodIdea? OPPSPayment Packaging

- December 2020 Congress passes No Surprise Act in the year-end omnibus spending bill
- January 1, 2022: It is illegal for providers to bill patients for more than the in-network cost-sharing
- January 1, 2023: CMSamends the Fee Guidance For the Independent Dispute Resolution Process
- January 1, 2023: HHSannounces it would not begin enforcement of the good faith estimate (GFE) requirement for uninsured and self-pay individuals However, the GFErequirement continues for facilities and providers (convening providers) that schedule a patient?s visit
- Health plans must treat out-of-network services as if they were in-network (except ground ambulance transport)
- The law created a new final-offer arbitration process to determine how much insurers must pay out-of-network providers
- Designed to increase patient choice beyond choosing their facility and principal physician

- Designed to fix a ?market failure?so that patients can understand associated ancillary charges, such as anesthesiologists, assistant surgeons and other providers
- Designed to remove the risk that patients will be surprised by large out-of-network bills, for example when receiving emergency care, elective procedures or being transported by air ambulance
- All out-of-network emergency facility and professional services
- Post-stabilization care at out-of-network facilities until such time that a patient can be safely transferred to a different facility
- Air ambulance transports
- Out-of-network services delivered at or ordered from an in-network facility
- Create Consumer Cost-Sharing: Holds consumers harmless by limiting their costs to in-network costs, including deductibles and out-of-pocket maximums
- Address Logical Care Settings:Emergency and post-stabilization care and non-emergency care in in-network facilities, fully insured and self-funded plans. Includes air ambulance services, but not ground ambulance services
- Establish a Path for Dispute Resolution:An independent dispute resolution process will trigger if parties do not reach a voluntary agreement in a 30-day negotiation period
- Set Enforcement at a State Level with Federal Backup: States have primary enforcement role. Federal enforcement will step in when states that lack authority or fail to substantially enforce the law. Federal enforcement uses civil monetary penalties
- Understand how the law applies in the states where the provider or facility renders services
- Identify, benchmark, and compare current payment trends for out-of-network claims.
- Fully understand the Dispute Resolution Process to determine when to initiate a dispute
- Audit previous claims to determine if balance billing occurred when prohibited
- Stay up to date on changes through participation in the PARA NSA Q&A bi-monthly webinars
Quest ion: We recent ly perform ed bot h a t em porary pacem aker and a perm anent pacem aker procedure during t he sam e out pat ient encount er (w it h a span of 2 days.) Medicare didn? t pay for t he t em porary pacem aker procedure. Can you offer guidance t o help us get paid for bot h procedures? An exam ple w ould be 33210, follow ed by 33208 on a subsequent day


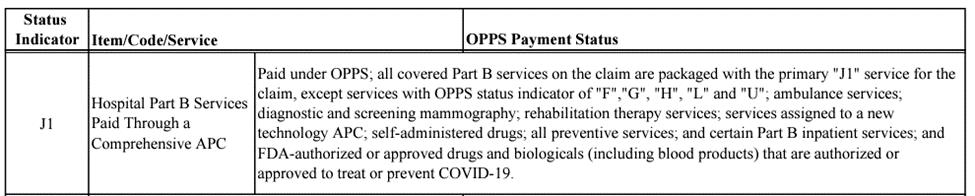
Answ er: Actually, under Medicare?s Outpatient Prospective Payment System (OPPS), the hospital was paid for both procedures, although only CPT 33208 carries the total reimbursement amount Medicare?s OPPSpayment system calculates reimbursement for a claim according to the ?Status Indicator?of the HCPCScodes reported on the same outpatient claim, regardless of the date of service Both HCPCS(33210 and 33208) are OPPSstatus J1 ? ?Hospital Part B Services Paid Through a Comprehensive APC?:
Under OPPS, only one Status J1 code will be paid, payment for all other lines will be ?packaged?to the primary (highest paying) J1 code on the same claim When CMSsets the rate of reimbursement for a ?comprehensive APC?, the rate-setting process takes into consideration costs reported from the entire body of claims submitted by facilities nationwide for the same procedure. Therefore, it?s not quite true that the hospital isn? t paid for the temporary pacemaker procedure, it?s just that its reimbursement is ?packaged?into the rate

paid on the primary code, which payment has already taken into account the typical costs for accompanying procedures ? including a temporary pacemaker procedure We found a claim that illustrates Medicare?s OPPSpayment for the services described within the Medicare claims database, using the PARA Dat a Edit or CMS tab:

Here?s an excerpt from the Medicare document that explains status indicator J1 (Addendum D1 of the OPPSFinal Rule) ? it explains that ?all covered Part B services on the claim are packaged with the primary ?J1?service for the claim? ?:
Here?s an excerpt from Medicare?s Integrated OCE(IOCE) CMSSpecifications V24.0, effective 1/1/2023, which explains how Comprehensive APCpayment is processed:
5.5 Com prehensive APC Processing
Effective 1/1/2015 (v16 0), certain high cost procedure codes which have an SI=J1 are paid an all-inclusive rate to include all services submitted on the claim, except, for services excluded by statute All allowed, adjunctive services submitted on the claim are packaged into the ?comprehensive?APCpayment rate (i e , the status indicator is changed to N) Multiple comprehensive procedures, if present on the claim in specified combinations, may be assigned to a higher-paying comprehensive APCrepresenting a complexity adjustment. Services that are excluded from the all-inclusive payment retain their standard APCand SI for standard processing.
C. If there are multiple comprehensive APCprocedures existing on the same claim from the different categories listed above, the comprehensive APCprocedures are packaged (SI = N) according to the hierarchy of services present; the procedure or service highest in the hierarchy is assigned the comprehensive APCfor the claim Additional processing conditions for each of the different categories is listed separately below
Outside of the ordinary APCreimbursement rate, there are only two ways that both procedures 33210 and 33208 reported on the same claim wilI qualify for additional reimbursement under OPPS? and that additional reimbursement would be paid on only the primary J1 code on the claim:
- Certain combinations of two or more HCPCSwith status J1 on the same claim will trigger a higher payment due to a ?complexity adjustment?? but that higher payment will be included in the amount paid on the primary code
- If a claim has an extraordinarily high amount of charges, the claim may become eligible for additional ?outlier?reimbursement ? but this claim did not meet outlier criteria
This case did not qualify for a complexity adjustment, nor were the total charges high enough to generate additional reimbursement under OPPSOutlier methodology
Com plexit y Adjust m ent - For certain combinations of J1 procedure reported on the same claim, OPPSprovides for additional payment on the primary code called a ?complexity adjustment.?CMSpublishes the list of code combinations that result in a complexity adjustment in Addendum Jof the OPPSFinal Rule.In the 2023 Addendum J, the combination of 33208 with 33210 does not qualify for a complexity adjustment.
Here?s an excerpt from Addendum Jindicating that the code pair 33208 with 33210 did not qualify for a complexity adjustment in 2023 (note there are several tabs in the workbook):

Out lier Adjust m ent ?Under OPPS, a claim paid by APCmay become eligible for additional reimbursement in the form of an outlier adjustment if two criteria are met:
- In 2023, the cost of the procedure, as measured by total covered charges x the facility?s ?Cost to Charge?ratio, must be more than $8,625 above the regular APCrate of reimbursement, and
- The facility?s cost must exceed 1.75 x the APCrate
Here?s an example of the OPPSoutlier calculation for a claim with very high charges:

On January 23, 2023, the Office of Management and Budget (OMB) approved three revised forms that are required by April 27, 2023. Those three revised forms are:
- Medicare Outpatient Observation Notice (CMS-10611)

- Important Message from Medicare (CMS-10065)

- Detailed Notice of Discharge (CMS-10066)
The revisions involved adding standardized nondiscrimination language required on forms and notices The original content and intent of the notices remain unchanged The new forms and instructions can be accessed in the PDE under t he Advisor tab

On January 26, 2023, the Federal Drug Administration (FDA) added AstraZenica?s Evusheld (tixagevimab and cilgavimab) to the list of drugs no longer authorized under an EUA in the United States. Previously Evusheld was approved as a pre-exposure option for individuals with moderate to severe immunocompromised systems or for whom COVID-19 vaccinations were not recommended The FDA states this monoclonal antibody therapy is ineffective with several omicron subvariants, includingBQ.1, BQ.1.1, BF.7, BF.11, BA.5.2.6, BA.4.6, BA.2.75.2, XBB, and XBB.1.5.1 .


The letter issued from the FDA to AstraZeneca is available through the following download: https://www fda gov/media/154704/download

Facilities seeking to recover underpayments made by Medicare due to unlawfully reduced OPPSreimbursement for drugs purchased under the Health Resource Service Agency?s 340B program between 2018 and September 28, 2022, will have to wait until this fall to learn exactly how and when CMSplans to remedy that financial shortfall
By some estimates, nearly $10 billion dollars of underpayments are at stake Drugs purchased under the 340B program are reported with modifier JG on outpatient facility claims
PARA Dat a Edit or users can identify 340B discounted payments from Medicare by searching the CMStab for outpatient claims reporting modifier JG:


CMSasserts that due to budget neutrality requirements, it is unable to immediately remit payment to correct years of prior claims processing. The agency has promised to publish a proposed remedy prior to the publication of the 2024 OPPSProposed Rule, which is typically released in early summer. The final decision on repayment methodology should be released in the fall of 2023, commensurate with the release of Medicare?s 2024 OPPSFinal Rule
Dissatisfied with the delay in resolution, the American Hospital Association filed a motion with the United States District Court for the District of Columbia to require immediate repayment to the affected providers, claiming that this was the only appropriate solution to resolve the underpayments That motion was denied on January 10, 2023 The court?s decision included the following key excerpts:
?Plaintiffs argue that the Supreme Court?s holding in Becerra ?dictates a single possible remedy?: ?repaying those hospitals that were unlawfully underpaid, from 2018 to the present, the difference between what they were paid and ASP plus 6%.?? And this Court has already identified several potential remedies that the parties previously put on the table ? Thus, the Court is puzzled by Plaintiffs?attempt to now characterize the remedial path as providing just one option, and it fails to see what exactly that option is.
?To the extent Plaintiffs seek an order commanding HHSto repay each underpaid claim to the penny, that cannot possibly be the only rational choice available to the agency.As Plaintiffs readily acknowledge, HHScould seek to implement a remedy such as a prospective one-time rate increase that avoids calculating individual claims ?
?Although the Court declines to retain jurisdiction, it expects that HHSwill act promptly to remediate its underpayments ?


The AHA issued a press release which reported the court decision at the following link: https://www.aha.org/news/headline/2023-01-10-district-court-remands-case-hhs-determineremedy-340b-underpayments



?The U S District Court for the District of Columbia today decided to allow the Department of Health and Human Services to propose an appropriate remedy for its past underpayments to hospitals participating in the 340B drug pricing program. ? In the outpatient prospective payment system final rule for calendar year 2023, the agency said it would defer any proposal of a remedy for CYs 2018-2021 until sometime before its CY2024 payment rule, and in subsequent legal filings, the agency stated that it intends to announce a final remedy before the 2024 OPPSrulemaking cycle is complete next fall.
?In a statement shared with the media today, AHA General Counsel Melinda Hatton said, ?For more than five years, the Department of Health and Human Services has unlawfully withheld vital funding from 340B hospitals that helps them provide a range of important benefits to their patients and communities.
"We are disappointed that the district court elected to extend this delay by remanding this case back to the department to determine the appropriate remedy. HHSrecently indicated that it expects to propose a remedy by April, and like the district court said in its opinion, the AHA ?expects that HHSwill act promptly to remediate its underpayments ?We look forward to continuing to work with the Administration to develop a plan to swiftly repay 340B hospitals, with interest, while ensuring the remainder of the hospital field is not penalized as they too continue to serve and care for their patients and communities.?
As a result of legal action taken by the AHA, the District Court previously ordered Medicare to stop applying the unlawful 340B discounts on claims processed on or after September 28, 2022. Medicare announced its compliance with that directive in its ?MLN Connects?edition dated October 13, 2022:

https://www.cms.gov/outreach-and-educationoutreachffsprovpartprogprovider-partnershipemail-archive/2022-10-13-mlnc# Toc116466499
Beginning January 1, 2018, Medicare reduced OPPSreimbursement for separately payable (Status K) drugs purchased under the 340B program at certain hospitals In 2018, CMSadjusted the reimbursement amount for 340B drugs at the average sales price (ASP) minus 28 5 percent, although certain hospitals were excepted from the payment adjustment policy.In 2019, CMS dropped the reduction to ASP minus 22.5%.
Drugs which were not acquired through the 340B program were paid under the OPPSat ASP+6 percent in both 2018 and 2019. Affected hospitals are required to append modifier ?JG?(Drug or biological acquired with 340B drug pricing program discount) to outpatient claims reporting payable drugs to facilitate the discounted rate of payment
In 2019, CMScalculated payments made on drug charges with the JG modifier appended at .775 of the ASP(in other words, ASP minus 22 5% )That rate is lower than standard OPPS methodology of 106%ASP(ASPplus 6% ) Therefore, for every $100 in allowable paid on lines reporting modifier JG in 2019, affected hospitals could recover an additional $36 77
On June 15, 2022, the Supreme Court of the United States (SCOTUS) issued a decision that Medicare improperly reduced OPPSreimbursement to certain hospitals which purchase drugs under HRSA?s 340B program in 2018 and 2019 The full text of the court?s decision is available at https://www supremecourt gov/opinions/21pdf/20-1114 09m1 pdf )

CMScontends that due to budget neutrality requirements, reversing the current payment policy could cause Medicare to fund the additional expense by cutting OPPSreimbursement in other areas, or even recouping other payments made under OPPSin the same years.
According to a study commissioned by the Federation of American Hospitals, even rural OPPS hospitals that were exempted from the 340(b) cuts could eventually be affected by the fallout: https://avalere.com/insights/opps-340b-policy-reversal-lowers-hospital-payment-and-increases-copays#
? nearly half (49 4%) of all OPPS340B hospitals would see a net payment decrease in total OPPSpayments under a policy reversal. This occurs because the corresponding budget neutrality payment reduction for all non-drug items and services would outweigh the drug payment increase. The aggregate beneficiary cost-sharing amount for separately payable drugs across all OPPS340B hospitals is estimated to increase by $472.8 million under a policy reversal Of note, the specific cost-sharing amount a beneficiary pays for a drug or a service under OPPSis capped at the amount of inpatient hospital deductible, which is $1,484 in 2021
The American Hospital Association published a Special Bulletin on June 15, 2022, stating that ?Now that the Supreme Court has ruled, we look forward to working with the Administration and the courts to develop a plan to reimburse 340B hospitals affected by these unlawful cuts while ensuring the remainder of the hospital field is not disadvantaged as they also continue to serve their communities.?
https://www.aha.org/system/files/media/file/2022/06/2022-0615-Special-Bulletin-340BSupreme-Court-Decision pdf

?[u]nder the text and structure of the statute,? the case was ?straightforward?as a matter of law: ?Because HHSdid not conduct a survey of hospitals? acquisition costs, HHS acted unlawfully by reducing the reimbursement rates for 340B hospitals ?
Meanwhile, in October of 2022, Medicare Administrative Contractor Novitas Solutions (Jurisdiction JH) offered to reprocess any discounted 340B payments made in calendar year 2022 at the full APC rate; however, no other MAChas followed this example, including Novitas Solutions in Jurisdiction JL.

The Jurisdiction JH MACoffer to reprocess 2022 claims is found at the link below: https://www novitas-solutions com/webcenter/portal/MedicareJH/pagebyid?contentId=00259704

Withtheintroductionof theNoSurprisesAct,PriceTransparencyfor theinsuredindividual has becomeconfusedwiththeGoodFaithEstimatefor theuninsuredindividual.
It?s important to understand the difference of an estimate generated for an individual under the Price Transparency law and an uninsured individual under the No Surprises Act Price Transparency Tool (PTT) The PTTis a patient-facing online tool meant to be used by patients who are shopping for services prior to scheduling. These individuals can be insured or uninsured
The desired service must be available as a shoppable service to generate an estimate with the PTT Although generating an estimate for services involves a variety of contractual discounts and health insurance plan information, the PARA Price Transparency Tool (PTT) allows the patient to determine their cost from the provider-based web portal


More information about the PARA PTTcan be found at this link:
PARA Price Tranparency Tool - Sept 2021 pdf (para-hcfs com)


When the patient is having trouble accessing or navigating the PTT, or the desired service is not a shoppable service, the Charge Quote tab of the PARA Data Editor (PDE) can be used by PDEUsers to generate a quote These quotes are not mandated by any laws, but the benefits of providing cost estimates prior to scheduled services include:

- Providing price transparency
- Providing estimates prior to service, avoiding unexpected financial liability
- Reducing Patient dissatisfaction directed at the provider
- Increasing self-pay collections while decreasing bad debt
The Charge Quote tool is available to PDEUsers under the Charge Quote tab
An instructional video on how to use the Charge Quote tool is available under the Advisor tab and can be found by keying ?Charge Quote?in the Summary field.
The No Surprises Act (NSA) requires that all healthcare providers and facilities who schedule services for uninsured individuals provide a Good Faith Estimate (GFE) which meets certain requirements. PARA and CorroHealth have developed tools which include all of the required data elements and disclaimers as outlined in the NSA These tools (PDENSA Tool and NSA Co-Provider Portal) are available to PARA clients who act as the convening provider or the co-provider to issue a compliant GFEto uninsured individuals.

The PDENSA tool is accessed by PDEUsers to issue the GFEto uninsured individuals who are scheduling a service or requesting the price of a service

The NSA Co-Provider Portal is accessed by Users who work in conjunction with the convening provider to issue a comprehensive GFEof all reasonably anticipated charges from all anticipated providers during the scheduled service. The Co-Provider Portal can also be used to issue a GFE directly to an uninsured individual when the co-provider is scheduling the service in their office/clinic and is now considered a convening provider who must furnish all the required GFE data elements
A demonstration of how these two platforms work together to create a GFEcan be viewed at this link: CorroHealth NSA Platform Overview Demonstration (vimeo.com)

In the 2023 OPPSFinal Rule, Medicare added nine codes to OPPSAddendum E, the ?Inpatient only?list. Medicare will not cover these services when billed on an outpatient claim except if the patient expires before admission to inpatient status or when the provider transfers the patient to another facility.
2023 Inpatient Only Procedures Addendum Emay be located by searching ?2023?in the Advisor tab of the PARA Dat a Edit or (PDE).

The nine newly added Inpatient Only HCPCSprocedures are identified with the letters ?NC?in the column labeled ?N?(Change Indicator) as shown below:

Medicare provides guidance on these exceptions in the Medicare Claims Processing Manual, Chapter 4 ?Part B Hospital, Paragraph 180.7 ? Inpatient-only Services:

https://www cms gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c04 pdf
?There are two exceptions to the policy of not paying for outpatient services furnished on the same day with an ?inpatient-only?service that would be paid under the OPPSif the inpatient service had not been furnished:
Except ion 1:If the ?inpatient-only?service is defined in CPT to be a ?separate procedure?and the other services billed with the ?inpatient-only?service contain a procedure that can be paid under the OPPSand that has an OPPSSI=Ton the same date as the ?inpatient-only? procedure or OPPSSI = J1 on the same claim as the ?inpatient-only?procedure, then the ?inpatient-only?service is denied but CMSmakes payment for the separate procedure and any remaining payable OPPSservices. The list of ?separate procedures?is available with the Integrated Outpatient Code Editor (I/OCE) documentation. See
http://www cms gov/Medicare/Coding/OutpatientCodeEdit/
Except ion 2:If an ?inpatient-only?service is furnished but the patient expires before inpatient admission or transfer to another hospital and the hospital reports the ?inpatient only?service with modifier ?CA?, then CMSmakes a single payment for all services reported on the claim, including the ?inpatient only?procedure, through one unit of APC5881, (Ancillary outpatient services when the patient dies.) Hospitals should report modifier CA on only one procedure.?
CMSsummarized the CY2023 Medicare Hospital Outpatient Prospective Payment System and Ambulatory Surgical Center Payment System Final Rule changes in its Newsroom Fact Sheet available through the following link:
https://www cms gov/newsroom/ fact-sheets/cy-2023-medicare-hospitaloutpatientprospective-payment-systemand-ambulatory-surgical-center-2

PARA invit es you t o check out t he m lnconnect s page available from t he Cent ers For Medicare and Medicaid (CMS). It 's chock full of new s and inform at ion, t raining opport unit ies, event s and m ore! Each w eek PARA w ill bring you t he lat est new s and links t o available resources. Click each link for t he PDF!

Thursday, January 26, 2023 New
- Medicare Enrollment in PECOS: Faster & Easier Application Process ? Coming Summer 2023
- Medicare Enrollment: Maintain the Same Owners in All Enrollment Records
- Hospitals: Revised Beneficiary Notices Required April 27
- Chiropractic Manipulative Treatment of the Spine: Comparative Billing Report in January
- Poverty: Help Reduce Disparities
MLN Mat t ers®Art icles
- Home Health Changes for Disaster Claims and Certain Adjustments
Therew ereNINEnew or revised Transmittalsreleased thisw eek.
To go to thefull Transmittal document simply click on thescreen shot or thelink.










Therew asONEnew or revised MedLearnsreleased thisw eek.
To go to thefull Transmittal document simply click on thescreen shot or thelink.


Theprecedingmaterialsare for instructional purposesonly. Theinformation ispresented "as-is"and to the best of ParaRev?s knowledgeisaccurate at thetime of distribution. However, dueto theever changing legal/regulatorylandscapethisinformation issubject to modification, asstatutes/laws/regulationsor other updatesbecomeavailable.
Nothingherein constitutes, isintended to constitute, or should berelied on as, legal advice ParaRev expressly disclaimsanyresponsibilityfor anydirect or consequential damagesrelated in anywayto anythingcontained in thematerials, which areprovided on an ?as-is?basisand should beindependentlyverified beforebeing applied.
You expresslyaccept and agree to thisabsoluteand unqualified disclaimer of liability.Theinformation in this document isconfidential and proprietaryto ParaRev and isintended onlyfor thenamed recipient. No part of thisdocument maybereproduced or distributed without expresspermission. Permission to reproduce or transmit in anyform or byanymeanselectronicor mechanical, includingpresenting, photocopying, recording and broadcasting, or byanyinformation storageand retrieval system must be obtained in writingfrom ParaRev. Request for permission should be directed to sales@pararevenue.com.
ParaRev is excited to announce we have joined industry leader CorroHealt h to enhance the reach of our offerings! ParaRev services lines are additive in nature strengthening CorroHealt h?s impact to clients?revenue cycle. In addition, you now have access to a robust set of mid-cycle tools and solutions from CorroHealt h that complement ParaRev offerings

In terms of the impact you?ll see, there will be no change to the management or services we provide The shared passion, philosophy and cultures of our organizations makes this exciting news for our team and you, our clients

While you can review the CorroHealt h site HERE, we can coordinate a deeper dive into any of these solutions Simply let us know and we?ll set up a meeting to connect.
As always, we are available to answer any questions you may have regarding this news We thank you for your continued partnership