3 3 www.yourexpertwitness.co.uk
& EXPLOSIVES
INVESTIGATION





4 4 www.yourexpertwitness.co.uk 25 21 18 contents IN THIS ISSUE 2YWS Copyright Your Expert Witness. All rights reserved. No part of this publication may be copied, reproduced or transmitted in any form without prior permission of Your Expert Witness. Views expressed in this magazine are not necessarily those of the publisher. Printed in the UK by The Magazine Printing Company Plc www.magprint.co.uk Your Expert Witness Suite 2, 61 Lower Hillgate, Stockport SK1 3AW Advertising: 0161 710 3880 Editorial: 0161 710 3881 Subscriptions: 0161 710 2240 E-mail: ian@dmmonline.co.uk 7 Opening Statement NEWS 9 Ombudsman reveals human rights abuses 9 Experts gather to hear from their own experts 9 New Year’s resolution: get some CPD in! 11 Law Society attacks Raab’s criminal legal aid stance 11 Experts’ body comments on favourable outcomes
13 Aggressive experts – what’s the problem? FORENSIC ACCOUNTANCY 15 Money laundering: HMRC reveals extent of non-compliance 15 Crime Agency wins first no-name recovery ruling 17 My expert predictions for 2023 – the ‘Year of the Water Rabbit’
18 Investigating gas explosions: an expert describes his experience 19 2022: a year of successes for forensics practice FIRE
20 The cost-of-living crisis may lead to an increase in home fires TRANSLATION
INTERPRETATION 21 Professional accreditation body seeks assessors 21 Controversial language company sold to US giant 23 Being an expert: the other 25% LEGAL
25 Report sheds light on construction adjudication 26 Councils to get new powers to tackle ‘land banking’ A to Z WEBSITE GUIDE 26 Our A to Z guide to the websites of some of the country’s leading expert witnesses. EXPERT CLASSIFIED 62 Expert Witness classified listings 67 Medico-legal classified listings
VIEWPOINT
EXPLOSIONS
&
ISSUES IN CONSTRUCTION
PSYCHIATRIC & PSYCHOLOGICAL ISSUES




5 5 www.yourexpertwitness.co.uk 53 MEDICAL ISSUES 40 www.yourexpertwitness.co.uk 29 Medical Notes NEWS 31 Healthcare system is ‘gridlocked’, CQC finds 33 Doctors’ indemnity body calls for more women expert witnesses 35 NHS Resolution: it’s about more than just compensation 37 False claimant ordered to repay compensation PHYSIOTHERAPY 38 Hydrotherapy within expert physiotherapy reports – is it a justifiable cost? DIABETES 39 Diabetic foot ulcers: why do they happen and how are they treated? NOISE INDUCED HEARING LOSS 40 New noise level guidelines come too late for many sufferers OBSTETRICS & GYNAECOLOGY 41 Maternal mortality report prompts outcry from all sides ORTHOPAEDICS 43 Surgeon carried on working despite warning signs 43 First astronaut with a disability is orthopaedic registrar 45 Latest knee replacement recall sparks media storm DENTISTRY & MAXILLOFACIAL SURGERY 47 Dentists call for ban on ‘misleading’ cereal ads 50 The medicolegal challenges of facial trauma PLASTIC, RECONSTRUCTIVE & HAND SURGERY 51 Surgeons’ leader addresses breast implant illness 53 Will we always have to live with scars? OPHTHALMOLOGY & OPTOMETRY 55 Eye care profession calls for image standardisation 55 Safety alert issued for ophthalmic pellets 56 Why would you join in chambers with other experts? 57 Head injury and concussion: where are we now?
59 New blood test could diagnose myocarditis 59 Heart failure is on the increase among the young
CARDIOLOGY
61 Psychiatrists attack ‘hidden’ mental health waiting lists 61 Rise in primary school referrals ‘worrying’, says DECP 61 Psychologists criticise changes to Online Safety Bill 57


6 6 www.yourexpertwitness.co.uk
Opening Statement
[
WE HAVE BEEN HEARING a lot recently of expert witnesses being censured by judges for failing to properly adhere to the principle of not favouring one party or the other. So it was heartening to find the Expert Witness Institute reporting on a case where a judge praised the approach of an expert in the face of accusations of favouring the party who instructed them. We hope there will be more such instances to report in the future.
• Not all is so rosy in the garden, however, and there are still instances where an expert has fallen short of what is desired. Our regular contributor Chris Makin revisits one case where the expert witness for one of the parties delivered his evidence in such an obtuse way that the judge had to require him to set it down in writing.
• The delivery of evidence is just one element of an expert’s work, of course. From first approach by an instructing solicitor to the trial itself, there is a complex relationship between expert and client. How that relationship can be made as issue-free as possible is addressed by another regular contributor, Hayley Cowle of Translate Hive.
• Taking a case to court is these days becoming less of a given that in the past, thanks to the increase in the use of alternative dispute resolution, such as adjudication. How that particular form of ADR is shaping up in the construction industry has been the subject of a study by academics at King’s College London.
The great majority of parties adhered to the adjudication: indeed, a quarter of respondents to the survey had never experienced an adjudicated case going to court and nearly half said it only happened in 5% of cases.
• The construction industry is not entirely peopled by paragons of virtue, however. Levelling-up Minister Michael Gove has his sights on the housing industry. Among other reforms, local authorities will have the power to refuse planning applications on land that has previously had planning approved but no homes built.
• Other aspects of local authorities’ activities have come in for criticism by the sectors’ Ombudsman in a report on the treatment meted out to people by the authorities. The Ombudsman cites numerous cases where such treatment has amounted to a denial of human rights, primarily the right to a private life.

• A right we cherish in this country is the right to a fair trial, and that right is under threat by the government’s response to the Bellamy Review of Criminal Legal Aid, according to the Law Society. The government’s refusal to implement Lord Bellamy’s recommendations on funding will, the society believes, lead to an acceleration in the exodus from legal aid work of legal firms and practitioners.
• Looking to the future is the norm for publications at this time of year, so Fiona Hotston Moore’s predictions for the Year of the Water Rabbit is highly topical. She anticipates a rise in fraud cases, as well as insolvencies and insurance claims related to the COVID pandemic. More recent financial pressures could prompt a rise in matrimonial and family cases.
More alarmingly, the fire specialist at Strange Strange and Gardner sees the pressure to save money leading to a spate of fires – both from heaters, stoves and candles and from using tumble dryers at night. There is a known risk from the appliances and to have them operating while asleep is a risk.
• On the other hand, looking back on the past 12 months is the subject of an entertaining column by Dr John Douse, whose remit includes toxicology cases and dealing with explosives. q
Ian Wild
Ian Wild, Director of Business Development Your Expert Witness
7 7 www.yourexpertwitness.co.uk

8 8 www.yourexpertwitness.co.uk
Ombudsman reveals human rights abuses
[
A NEW REPORT shares how people’s basic human rights have been infringed when receiving public services in England.
Equal Justice, the new report by the Local Government and Social Care Ombudsman, explores a catalogue of cases where people have not been treated fairly and suggests how things should be put right.
Cases cited in the report include a man with a learning disability who was regularly given sedatives by care home staff over a seven-month period, impacting on his right to a private life. In another case a council denied a homeless family the right to enjoy a family life and home when it failed to
identify that the property they were living in was overcrowded; and in a further case a council’s interference in a family custody dispute impacted on the father’s right to a family and private life.
Michael King, the Local Government and Social Care Ombudsman, said: “People all too often think of ‘Human Rights’ with capital letters and in grand terms, but the basic expectations of how anyone should be treated – with fairness, respect and dignity – are just as applicable for people in their everyday lives as they are when major international events occur.
“We all have a right to expect these basic
standards when we use public services. I want to raise people’s awareness about those rights, so people can more easily recognise when their basic rights and freedoms have been neglected. And I urge councils to take a rights-based mindset when developing their services and making day-today decisions on how they are delivered.”
Most of the cases cited in the report involved the ‘Right to Private Life’, particularly in relation to people in receipt of adult care services, but other cases involved councils failing to provide education for children, or where adults were unfairly deprived of their liberty. q
Experts gather to hear from their own experts
[ BOND SOLON have published a report on their recent Expert Witness Conference. The training organisation’s Meera Shah offered her thoughts on the day.
“Mark Solon opened the conference with a short introduction followed by our renowned keynote speakers: The Lord Chief Justice, The Right Honourable The Lord Burnett of Maldon and a Court of Appeal judge, and The Right Honourable Lady Justice Carr DBE.
“The Lord Chief Justice was unable to be there in person, but he very kindly addressed the conference by way of a pre-recorded Q&A with Mark Solon. Many experts appreciated learning about the digital/paperless ‘movement’ that has been taking place across the court system. It was also encouraging to hear how much both speakers value expert witnesses during court hearings, with Lady Justice Carr opening with the following phrase: ‘Experts have never been more needed or played a more crucial role’.”
A number of presentations led up to the Annual Legal Update – a thorough analysis of the new cases and changes to law and
New Year’s resolution: get some CPD in!

procedure over the past year. Issues regarding how experts can protect themselves against litigation led up to lunch.
After lunch various parallel sessions were on offer on the following topics: medico-legal, family, commercial and criminal.
Meera Shah explained: “Unsurprisingly, the medico-legal session was the most popular, but we’ve had some excellent feedback on the other sessions too. I had the pleasure of sitting in on the family session with Elissa Da Costa-Waldman and Andrew Shaw and found that many of the learnings on duty and conduct could apply to experts across the board.”
A duo of presentations by IT expert Mark Cunningham-Dickie and construction disputes expert Mark Mills were followed by a debate between Amanda Pinto KC and Faisal Osman on whether evidence in person is always better than online.
At the end of proceedings the Bond Solon team joined the experts at Church House in toasting the conference with a drinks reception and a presentation for some of the new Cardiff University and Aberdeen University Expert Witness Certificate holders.
“So now that the biggest event in the Bond Solon 2022 calendar is behind us,” Meera Shah concluded, “plans for the 2023 Expert Witness Conference are already underway. Over 80 experts have already secured their place for next year’s event on 3 November 2023 and the conference working group is in hive mind mode, working on another informative and insightful programme.
“The Bond Solon team can’t wait to host you at Church House, Westminster, and virtually on Swapcard next year.” q
AS WELL AS HAVING the relevant qualifications and experience in their professional field, for expert witnesses it’s now regarded as essential to undertake recognised expert witness training.
[
Probably the UK’s leading provider of expert witness training and CPD is Bond Solon, offering courses covering all the core areas of expert witness work. Training is delivered through a mixture of live courses, webinars and e-learning.
That’s in addition to university certificates for expert witnesses that are widely regarded as the gold standard by instructing parties and the courts. The Cardiff University Bond Solon (CUBS) Expert Witness Certificate is for those practising in the English and Welsh jurisdiction and the University of Aberdeen Bond Solon (UABS) Expert Witness Certificate caters for those operating in Scotland.
With 2022 coming to a close, now is a great time to plan ahead and look at your expert witness training and CPD requirements for next year. Bond Solon have a wide range of courses and events to suit all expert witness training and CPD requirements, beginning as early as 9 January with the virtual course on Excellence in Report Writing.
For more information on courses and events visit the website at www.bondsolon.com/expert-witness/courses q
9 9 www.yourexpertwitness.co.uk

10 10 www.yourexpertwitness.co.uk
Law Society attacks Raab’s criminal legal aid stance
[ DOMINIC RAAB has completely rejected the advice of the government’s own independent review of the crisis in the criminal justice system by imposing a real-terms cut on legal aid rates. That was the opinion of the Law Society in response to the publication of the government’s final response to Lord Bellamy’s Independent Review of Criminal Legal Aid.
The review sought to solve the crisis in the financial viability of criminal legal aid work, but the government’s actions will make the on-going crisis worse, the Law Society said, adding that it is
Experts’ body comments on favourable outcomes
[ THE EXPERT WITNESS INSTITUTE (EWI) has been assiduous in publishing instances where expert witnesses have been taken to task by judges for failing in their duty of impartiality. So it was with a certain glee that they reported a case where the opposite was true and an expert was exonerated by a judge in the face of criticism.
“We have often drawn attention to cases in which claims regarding experts’ unreliability were supported,” the institute’s Wiebke Morgan wrote, “so we feel it is important to highlight that you should be aware such claims could be raised against you, and we are pleased to show that in an overall very interesting case, the judge rejected the defendant’s submission which seriously attacked the expert’s credibility, claiming they were an unsatisfactory expert witness, more inclined to argue their clients’ case than to assist the court, and that the expert was not a witness on whose evidence the court could safely rely.
“They said that the expert’s evidence was shown in crossexamination to be unsupported, speculative and in many cases positively misleading. The judge, however, did not accept that the expert was an unreliable witness.”
In his judgement on a case in the Business and Property Court on 29 November, Mr Justice Jacobs said after dealing with criticism of the witness, a Dr Bennett: “Accordingly, I do not accept that Dr Bennett is an unreliable witness. On the contrary, and as will be apparent from my detailed discussion of her evidence below, I consider that she was impressive, and indeed more impressive than Dr Nicola. I certainly have more confidence in her views than the contrary views expressed by Dr Nicola.”
The EWI also commented on an appeal arguing that a single joint expert should have been male: an appeal that was thrown out. The appeal was against a case management order in private law proceedings under the Children Act 1989 relating to a boy, now aged 8.
“The order under appeal permitted the parties to instruct a named independent social worker to carry out an assessment to assist the court to determine issues relating to child arrangements and education. The expert named in the order is a woman. The appellant father proposed that the assessment should be carried out by a male social worker. He asserted that the order permitting the instruction of a female social worker was an infringement of his human rights. The appeal was rejected.”
The case follows the EWI’s commitment to the pledge to support Equal Representation For Expert Witnesses – as reported in the last issue of Your Expert Witness q
‘extremely concerned that for many of our members there could be no viable future in criminal defence practice’.
“It is a tragedy for the British justice system that years of political neglect have forced us unavoidably to this conclusion,” the society said in a statement.
Its president Lubna Shuja added: “Dominic Raab has made the wrong decision in not implementing the immediate 15% criminal legal aid rate rise for solicitors. The independent review recommended this a year ago as a bare minimum to prevent the criminal defence sector from collapsing. Instead, he is imposing a real-terms cut on fees that have been frozen since the 1990s.”
The statement pointed to the numbers of duty solicitors and criminal legal aid firms that are continuing to fall at an alarming rate – with several police station schemes on the verge of collapse.
“Access to justice – including the fundamental right to representation at the police station – is in serious peril and the government is ignoring the threat.”
Analysis by the society suggests that the number of duty solicitors will decrease by another 19% by 2025 – 687 fewer duty solicitors –and the number of firms doing criminal legal aid work will decrease by 16% – 150 fewer firms – by 2025, leaving many people without access to a lawyer when they desperately need one.
“Until the government chooses to address the collapse of the criminal justice system, victims will continue to be let down and talk of being tough on crime will be nothing but hot air,” the statement said. “The Independent Review of Criminal Legal Aid was the last hope that the Ministry of Justice would take the crisis seriously and that there could be a viable future in criminal defence practice for our members. Instead Raab has thrown down a gauntlet to the profession.” q
11 11 www.yourexpertwitness.co.uk

12 12 www.yourexpertwitness.co.uk
Aggressive experts –what’s the problem?
By CHRIS MAKIN chartered accountant, accredited civil mediator and accredited expert determiner

[ I’VE BEEN READING again the case of Siegel v Pummell [2015]
EWHC 195 (QB). The facts are simple. Mr Siegel was injured in a motor accident and Mr Pummell (think about it!) admitted liability. There was a trial on quantum and Mr Siegel succeeded in securing a reasonable amount, but he claimed his costs on the indemnity basis for these reasons:
• The defendant’s expert neuropsychiatrist had made personal and
• combative attacks on the claimant’s expert psychologist
• The defendant’s expert had not cooperated in the joint statement
• process
• The defendant’s expert gave his written evidence, and his oral • evidence at trial, in such a confusing way that the judge had to • ask him, in the course of his evidence, to summarise it in a written • document. This meant that one of the claimant’s experts had to • be recalled.
Rudeness is one thing, but I find the third reason particularly disturbing. If the expert’s evidence is so obtuse that a judge has to tell him to write it out in simple English, he has failed. CPR says at 35.3(1) that ‘it is the duty of the expert to help the court on matters within their expertise’. Is a medical expert helping the court if they wrap up their evidence in so much medical jargon that neither the judge, nor the jury in a criminal case, can tell what they are talking about? I don’t think so!
We professionals who have bothered to train in the second profession, that of being an expert, know full well that we must address our evidence and opinions to the ‘informed layman’, whether judge or jury.
Reading on, the judge was very critical of the way the defence expert had given his evidence. Extracts from the judgment:
About Chris Makin
[CHRIS MAKIN was one of the first 30 or so chartered accountants to become an Accredited Forensic Accountant and Expert Witness –see www.icaew.com/about-icaew/find-a-chartered-accountant/find-anaccredited-forensic-expert
He is also an accredited civil and commercial mediator and an accredited expert determiner. Over the last 30 years he has given expert evidence at least 100 times and worked on a vast range of cases.

For CV, war stories and much more go to the website at www.chrismakin.co.uk – now with videos! q
“His evidence was combative and dismissive of that of other medical professionals who were not specialists in the same field as himself.”
“It was apparent during the trial that there was a degree of animus between the parties’ experts.”
The judge found that the expert was entitled to raise certain points, though preferably in a less unpleasant way.
Turning to the joint statement process, he found that the experts ‘were incapable of approaching the exercise in anything like the cooperative spirit which it requires’.
As I say, the claimant asked for his costs on the indemnity basis. The judge found that, although undesirable, the expert’s behaviour did not fall so far short of acceptable that this request should be granted.
But his approach on the third matter was different. He noted that: “The fact that the court was obliged to ask Professor Trimble, in the middle of his evidence, to provide a written statement as to what exactly his evidence was and the basis upon which he was saying it… did arise from serious shortcomings in the way in which he approached the giving of his evidence.”
Frankly, I am staggered that an expert should have to be asked to set out what he was talking about. The watchword must be KISS (Keep It Simple, Stupid). There are lessons here for experts which are so self-evident that I will not set them out. But there are lessons for instructing solicitors, too, because once your expert is let loose in the witness box you have no control over them, and they can so easily wreck your case.
You can solve the problem at an earlier stage. If, on first meeting or at conference with counsel, the expert is so preoccupied with demonstrating his intellectual superiority that you can’t tell what he is talking about, he is not doing his job, and he won’t in the witness box. So if you can, change your expert. If you can’t, do your best to train him to get off his high horse. And don’t use him again.
This need for simplicity was illustrated well in a VAT fraud trial where I was an expert at Wood Green Crown Court many years ago. Prosecuting counsel took ages to examine the inspectors from Customs, and constantly asked the judge to accept additional documents to be put in the trial bundle, which was already about ten full volumes. The judge had to be helped to insert the extra pages in the right places, and eventually one ringbinder sprang open and scattered the contents all over his bench. The judge expressed dissatisfaction (and how!) and said he would adjourn early for lunch. When he came back, he wanted the whole case summarised on one sheet of A4.
And so it came about. The case was very simple: a family of Turkish Cypriots has ice cream vans in tourist spots all over London, and the issue was whether they were each separate businesses under the VAT threshold, or a combined business where VAT arrears would have amounted to about £½ million. The prosecution still got their conviction, but the trial was much shortened.
So remember, KISS. If your chosen expert doesn’t work that way, don’t use them. And, a fortiori, if your expert is bad tempered or tries to lord it over the ‘enemy’, don’t use them, either. Bad manners and arrogance won’t help your case. q
13 13 www.yourexpertwitness.co.uk
14 14 www.yourexpertwitness.co.uk
Money laundering: HMRC reveals extent of non-compliance
[DOZENS OF ESTATE AGENTS have been fined more than £500,000 for breaching anti-money laundering requirements, HMRC has revealed.
HMRC named the 68 estate agents that have been fined a total of £519,645 for not complying with rules designed to stop criminals laundering money from illegal activity. The fines followed the first prosecution of an estate agent for trading despite not registering with HMRC to ensure compliance with money laundering regulations.
Nick Sharp, HMRC’s deputy director of economic crime, said: “We are determined to create a level playing field for businesses who play by the rules. That means taking action against the minority of businesses who fail to fulfil their legal responsibilities under the money laundering regulations.
“Money laundering is not a victimless crime. Our regulations are there to protect businesses from those criminals who would prey on their services to wash their dirty money. Serious and organised crime costs the UK billions of pounds every year and our anti-money laundering
Crime Agency wins first no-name recovery ruling
[THE NATIONAL CRIME AGENCY (NCA) has obtained a ruling from the High Court that allows Barclays to hand over criminal funds to the NCA in a first-of-its-kind civil recovery case. The money –amounting to over £50m – was identified by the bank in a number of accounts and transferred to secure holding accounts.
The civil recovery order means that, for the first time, legal powers were used to recover the proceeds of crime where the account holders were not named in the court action.
Adrian Searle, director of the National Economic Crime Centre (NECC) in the NCA, said: “Identifying and recovering funds and assets linked to criminal activity is a priority for the NCA. This High Court ruling is a great example of how the public and private sector can work together to recover proceeds of crime. The proactive identification of these funds by Barclays was the reason we could take this action. The money will be credited to the public purse and a portion used to fund a range of work including programmes designed to prevent fraud and protect potential victims.
“The NECC will continue to work with the financial and regulated sectors to identify and recover illicit finance, using all the tools at our disposal.”
A Barclays spokesperson said: “We are vigilant in rooting out and identifying any criminal activity. We welcome the High Court’s ruling, which enables the funds to be transferred to the NCA to support further their efforts in stopping scams and economic crime.” q
supervision is a vital tool in combatting that.”
Estate agents form the largest type of businesses found by HMRC not to be complying with anti-money laundering regulations. It has published the full list of businesses not complying on GOV.UK: 175 businesses received penalties totalling £2,180,708. The total represents a large increase from the previous list, published in May, which saw 147 businesses – including 41 estate agents – receive penalties totalling almost £800,000.
HMRC is currently investigating a number of other cases of businesses failing to register while trading, which could lead to prison sentences of up two years and an unlimited fine. q
15 15 www.yourexpertwitness.co.uk
My expert predictions for 2023 –the ‘Year of the Water Rabbit’
Forensic accountant and accredited expert witness Fiona Hotston Moore of FRP Advisory gives her predictions on the outlook for experts in 2023.


[2023 IS THE YEAR of the Water Rabbit. According to the Chinese horoscope, those born in the Year of the Rabbit are vigilant, witty, quick-minded and ingenious. Vigilance, quick-thinking and dexterity are all important skills for an expert witness; thus the Rabbits amongst us should be well equipped in what looks like being another volatile year.
In light of events which have unfolded over the last two years, it is perhaps foolish to try and predict what will unfold in 2023. However, as expert witnesses, our work follows from recent events and I will endeavour to give my predictions on which type of cases we will be providing expert opinion on in 2023.
Cases of fraud and false accounting
A forensic accountant will typically talk about the fraud triangle. This is the concept that there are three components which together lead to fraudulent behaviour. These are motive/pressure to commit fraud, opportunity to commit the act and rationalisation of the action.
Unfortunately, in times of financial pressure for individuals and businesses, there is inevitably an increased pressure to commit fraud, either to obtain funds for personal needs or to misrepresent the business’ financial position. At the same time, those managing the business or charity may be underresourced and less likely to spot the warnings signs. Therefore I expect to see a raft of such claims throughout 2023 and beyond.
Commercial disputes
Commercial disputes, including those arising from breach or termination of contract, typically increase in a volatile economy. In recent times businesses have faced huge inflationary pressures, supply chain issues and labour shortages. Businesses may seek to escape what has become an unprofitable arrangement or be unable to fulfil their commitments. As experts, we will be instructed to assess the commercial losses arising from contractual breaches.
Disputes arising post company sales
Both 2021 and 2022 have been buoyant times for business sales and many of these deals will have reflected recent positive trading results. The deals may include deferred or contingent consideration. The trading performance since the deal may have deteriorated and in such situations the buyer may look to recover part of the consideration paid or to avoid paying deferred consideration.
Disputes arising out of SPAs (sales and purchase agreements), including warranty claims, are already hitting our desks and I would expect these to continue in 2023.
Matrimonial, family and shareholder disputes
In times of financial pressure, we typically see an increase in family disputes and disputes between shareholders. These cases include divorces, probate disputes, partnership disputes and claims of unfair prejudice. As forensic accountants we will be instructed to value family businesses in order to assist the lawyers and courts attempting an equitable distribution of assets. In 2023 we may also be instructed to revisit our earlier opinions on business valuations in light of a deterioration in financial results and the economic outlook.
Insolvency and business failures
In cases where a business has ceased trading and creditors may not be paid in full, we are often instructed to undertake an investigation into the conduct of the directors and to identify matters such as sales at under value, defrauding creditors and misfeasance. We will assist the insolvency practitioner in taking any appropriate action to recover assets.
Professional negligence
As forensic accountants, we are instructed to consider whether the conduct of an accountant or tax adviser met the standard of a ‘reasonably competent’ professional. We are also instructed to consider the quantum of financial loss in claims against professionals in a range of sectors including medical, legal, financial services and construction.
Over the last decade clients have been more willing to pursue claims against those who were once their ‘trusted advisers’ and I expect this trend to continue.
Insurance claims
As forensic accountants we are already dealing with insurance claims arising from losses incurred during the pandemic. In the first instance legal counsel will need to determine if the loss is covered by any insurance and if so, we may be instructed to give an expert view on the quantum of any loss allowing for any reasonable mitigation.
Court delays
More generally we have experienced delays in instructions and hearings due to court backlogs. There have also been hiatuses arising from the sanctions on Russia. Unfortunately, I expect court delays and sanctions will continue and inevitably clients, lawyers and experts will have to manage cases with extended periods of inactivity and inevitable inefficiencies.
To conclude, experts will need to continue demonstrating vigilance, flexibility and dexterity in what looks likely to be another volatile year. q
17 17 www.yourexpertwitness.co.uk
Investigating gas explosions: an expert describes her experience
[
A NUMBER OF GAS EXPLOSIONS over the past few years have resulted in over 170 injuries and a dozen deaths. Those explosions come from a variety of sources, including fuel piped directly to a property or delivered in bulk transport, and fuel stored on a property.
Gas fuel systems can exasperate a building fire as the initial fuel source for the fire when it escapes from piping, storage or appliances; as the initial ignition source because of its low ignition energy; or by being both the fuel and the ignition source. Gas can also be a contributing factor that influences the fire growth rate and spread when the fuel system is attacked by a fire.
Understanding the role played by gas in fires and explosions requires careful consideration from an expert. Rose Campbell, risk analyst and expert services manager with CEERISK Consulting Ltd, has investigated many incidents where gas played a key role in the inception of a fire or explosion and the extent of the damage.
In her experience, investigation of gas fires and explosions requires careful analysis of all factors. Depending on the extent of the damage, which can be made worse by the presence of gas, that can be particularly tricky.

Rose Campbell explained: “A good place to start is looking at the compliance of all aspects of working fuel
gas systems to ensure they comply with local codes and standards. That also includes review of the design, manufacturing specification, construction, installation and other various components.
“The source of any gas leak must be determined as well. Leaks can occur from many areas, including pipe junctions, unlit pilot lights or burners, uncapped outlets, malfunctioning appliances and malfunctioning controls. The failure of gas regulators is also a contributing factor to gas leaks, as internal faults can cause the regulators to fail to reduce pressure to acceptable levels.
“One of the most common sources of gas leaks is corrosion, caused by rusting metal pipes or electrolysis between similar metals, metal and water, and metal and soil. Corrosion accounts for about 30% of known gas leaks.
“Other sources of gas escape include physical damage, which can occur during installation or as a result of impact during construction works, such as is the case when underground pipes are pierced during investigation.” q
• Rose Campbell is risk analyst and expert services manager with CEERISK Consulting Ltd, specialists in supporting experts investigating major incidents including gas explosions and building fires.

18 18 www.yourexpertwitness.co.uk
2022: a year of successes for forensics practice
Dr John Douse of OGT Forensic Ltd looks back at a year to remember in the fields of toxicology and explosives
[IN 2022 we continued to be instructed at the highest level and the pandemic years have provided us with our most successful achievements to date – despite the extreme circumstances.
Toxicological highlights have included instruction in a number of high-quantum criminal, commercial and family law cases involving:
• Carbon monoxide in an aircraft
• mid-air collision

• Arsenic contamination of a family residence
• Flunitrazepam – a case against The Sun newspaper
• Ricin and plant toxins
• Fatal hydrogen sulphide drain emission
• An accusation of international assassination with hydrogen cyanide
• Mustard and nerve chemical agents
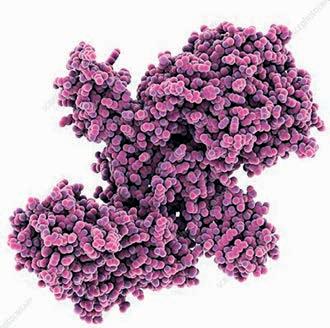
• A potential nine-figure quantum botulinum toxin case
• Correctly championing the Watson’s Total Body Water ethanol back
• calculation method
Plus, there have been a number of other fascinating instructions, such as cocaine in hair washout during professed abstinence, and cases where we have been able to rapidly assist the court.
Explosive highlights have included the salvage of the hazardous materials carrier MS Bow Diamond , which involved 500 tonnes of spilt TNT and RDX with the potential to repeat the Beirut Incident, absolving an explosives firm from both a potential eight-figure quantum fine and also the need to relocate abroad, successfully resolving a fiendishly difficult fireworks accident case involving a hypervelocity projectile discharged into spectators, a video about the explosive TATP and a World War II bomb explosion (pictured above).
A range of other complex explosive cases involved improvised propellant rocket motors, explosives manufacture, unofficial instruction manuals and a case which revealed copious nine-year-old deposits of liquid nitroglycerine on laboratory glassware at a defence inspection. We are privileged to be able to continue our fascinating forensic scientific odyssey.

Our approach to casework is the result of 36 years of forensic and 43 years of scientific (exOxford) expertise, experience of over 380 cases and painstaking investigational technique, which involves leaving no scientific or circumstantial evidential detail unconsidered.
If you feel that such an approach may be able to assist your client’s case – large or small, legal aid or private – contact us for a free initial consultation. q
The structure of the 145 kDa botulinum toxin A1 molecule, reported to be the most toxic substance known. It is used in medicine for therapeutic purposes and also for cosmetic aesthetic enhancement treatments, in low sub-nanogram doses.
19 19 www.yourexpertwitness.co.uk
• Dr John Douse BA MA DPhil (Oxford) is a Fellow of the Royal Society of Chemistry, Fellow of the Forensic Science Society (now the Chartered Society Of Forensic Scientists), Fellow of the Chromatographic Society, Member of the Expert Witness Institute and Member of the Institute of Explosives Engineers.
The pictures above show a World War II bomb, unearthed in an orchard having lain undisturbed and unnoticed for nearly 70 years, which was exploded. The thermal image is of the explosion after a few hundredths of a second.
The cost-of-living crisis may lead to an increase in home fires
 By Anthony Murray, Fire Investigation Specialist at Strange Strange & Gardner
By Anthony Murray, Fire Investigation Specialist at Strange Strange & Gardner
[
THE RISING COST OF LIVING has placed significant pressure on consumers to find affordable ways to heat and light their homes. Over the past few weeks, there have been reports of an increase in the use of portable heaters, electric blankets, wood-burning stoves and candles in homes – often as cost-saving measures. As a result, there is an increased risk of a fire.
Consumers are likely to try and save money by using high-energy white goods such as tumble dryers during the night, in order to take advantage of cheaper electricity in off-peak hours. There is still a risk of a fire when using such devices and it is likely people will have less time to respond, should one occur, due to them being asleep. As a result, the risk of accidental house fires will increase.


Strange Strange & Gardner will investigate a fire, determine the cause and advise if it may have been caused by defective equipment. We are well placed to assist in dealing with the aftermath of what is likely to have been a traumatic event. q
20 20 www.yourexpertwitness.co.uk
Professional accreditation body seeks assessors
[ CIOL QUALIFICATIONS (CIOLQ) has recently issued a call for suitably qualified and experienced individuals to join its database of assessment associates in a number of languages.
CIOLQ is an awarding organisation and the associated educational charity of the Chartered Institute of Linguists. It offers professional qualifications in interpreting and translation which are recognised both nationally and internationally by the professions, business and public services.
It assesses candidates in a wide range of languages against the Common European Framework of Reference for Languages (CEFR) scales C1 (Upper-Intermediate) and C2 (Advanced).
The timings and volume of assessments vary, but it regularly tests large cohorts in European and world languages approximately six times a year. It has an extensive database of freelance assessment associates (AAs), who are linguists from a variety of backgrounds and devote time to assessment commissions, showing dedication to their profession and personal development.
Assessing is both varied and incredibly rewarding. It can, however, be challenging but AAs frequently talk about the skills and knowledge they gain while doing that type of work, which can open up new opportunities and further career progress.
Because of the importance of the assessments, applicants should be committed to attending training and standardisation sessions if and when required and also be available for assessment windows.
Applicants, who are engaged on a freelance basis, should be native speakers of the language they are assessing and should also possess an excellent command of English. They should be educated to degree level or higher. q
Controversial language company sold to US giant
[
ON 11 NOVEMBER Capita Plc announced the sale of Capita Translation and Interpreting (Capita TI) to LanguageLine for an undisclosed amount. Capita TI’s employees and senior management will stay with the business as ownership transfers to LanguageLine, according to the announcement on the Capita website. Based in California, LanguageLine is part of French call centre giant Teleperformance.
For many years UK-based Capita TI managed one of the world’s largest language service contracts with the UK Ministry of Justice. That contract spawned a multitude of stories of mismanagement in the courts’ interpreter services. In 2015 Capita TI was ordered to pay £16,000 in costs after interpreters failed to appear on time or at all on seven occasions during one adoption case.
Jonathan Lewis, CEO of parent company Capita plc, said: “The sale marks another positive step, as we continue to simplify and strengthen Capita. We will continue to execute on our plan at Capita to materially reduce debt through the disposal of non-core businesses.”
According to language industry intelligence website SLATOR: “A multibillion-dollar outsourcing company, Capita Plc had reportedly been trying to sell off Capita TI since early 2020. At the time, Capita plc had earmarked for sale nine non-core businesses housed under ‘Specialist Services’, which included Capita TI. The asking price for all nine at the time was said to be at least £200m.
“However, Covid intervened and Capita put the planned sale on hold. The sale of Capita TI is a standalone transaction and financial details were not shared.”
Capita TI’s revenues had remained roughly flat since 2017 following its exit from the Ministry of Justice contract – albeit contributing as a standout performer among Capita’s Specialist Services from 2019 to 2020. q

21 21 www.yourexpertwitness.co.uk

Being an expert: the other 25%
by Hayley Cowle of Translate Hive
[ EXPERTS, by their very nature, should know what they’re doing; but what about the surrounding support, the experience the solicitor receives from instruction to report?
Here, we examine the importance of the organisation that precedes an expert performing their role – whether examination or reporting –together with the input during and after their involvement: the report ‘aftermath’. They are all administrative roles essential to the success of an expert witness.
Having spent many decades dealing with expert witnesses we have found that success depends on three aspects: the initial instruction, the expert themselves and the reporting.

Arguably, the expert witness report itself – the product – is the most important aspect to get right, but for efficiency, and thus profitability and to ensure repeat business, the ‘other 25%’ is important to get right.
The instruction
The ability to instruct an expert swiftly and easily, preferably in one go, is imperative to providing a great initial customer experience. I recall some experts providing an Excel spreadsheet with a huge table of questions, the majority of which were irrelevant to the case in question. Tabbing through jumped illogically from question to answer space. Those were then emailed back and we never really knew whether they’d received them or not…for days: the experience was pretty poor.
With so many great customer experiences to be found online we thought we could take inspiration and do better. We developed a one-touch ability for a solicitor or client to instruct directly from their case management system (CMS), saving them considerable time. Creating automations to ensure we had the salient details and nothing surplus and then linking smartly to a client’s CMS systems such as Proclaim or any system that accepts APIs – that is, most built in the past few years – we made the experience as easy as ordering an Uber!
The system allows solicitors to see pretty much what we see: the status of their instruction, handlers, costs, ETA for the report, management information etc; pretty much anything they need to know.
As any expert witness will tell you, there are often idiosyncrasies with cases, so it is imperative to have human input. The expert is expensive and is best placed doing his specialist work; it would be frivolous to have them answering non-expertise or administrative questions. That’s where a well-trained support team comes into play. They should be empowered to deal with enquiries, quotes and common queries raised. They should be able to estimate roughly how long a report is expected to take or cost, so they can be a proactive help to the client, ushering them through the process.
The reporting aftermath
Once the expert has compiled their report, we’ve often seen it sent directly – which can lead to silly errors. A mix of autonomous software and humans can be used to quality assure the report, ensure that it is billed accurately and is sent to the correct people.
In some cases the primary data will be delivered direct to a client’s CMS via API connections, saving time and ensuring 100% accuracy. That also assists with some queries and supplemental questions; and often gives the client the ability to pay online.
Again, a well-trained support team is imperative to field minor queries from the expert and deal with any administration queries. They should have clear and honest communication with the expert and it helps greatly when they have a decent understanding of the expert’s subject.
The support team should be able to organise joint reports with other experts and liaise with solicitors or barristers to book the expert into various court hearings, including the terms required.
Above all they should provide an excellent customer experience for the expert’s clients, while fully supporting the expert’s requirements.
Summing up
To some degree the roles surrounding the expert witness have an element of business development. They have the ability in some cases to upsell products, and certainly to ensure the customer experience meets (or hopefully exceeds) their expectations. Solidifying the client-expert relationship gives both parties additional confidence in the supply chain.
The expert is entirely responsible for the content of their report, including their various obligations under the Civil Procedure Rules and to the court; however, it is the way the case is dealt with from cradle to grave, the supportive administration that enhances the client’s experience, thus increasing the likelihood of future instructions. The expert’s report is of primary importance, but great customer service is the icing on the cake. q
23 23 www.yourexpertwitness.co.uk

24 24 www.yourexpertwitness.co.uk
Report sheds light on construction adjudication


[
A NEW REPORT from researchers at King’s College London (KCL) has provided a snapshot of the UK's construction adjudication infrastructure. It found the system for construction adjudication to be ‘robust and resilient’, while noting concerns over bias and a lack of diversity in key roles.
The report, 2022 Construction Adjudication in the United Kingdom: Tracing trends and guiding reform, provides the broadest and deepest empirical analysis of UK construction adjudication to date. Co-authored by Professor Renato Nazzini and Aleksander Kalisz of KCL’s Centre of Construction Law and Dispute Resolution (CCLDR), it looks at the experience of construction adjudication in the UK from the perspective of users and key organisations, and provides an analysis of vital empirical data on key aspects of adjudication.
Professor Nazzini commented: “This report provides a comprehensive account of the state of play regarding adjudication in the United Kingdom. Our objective has been to gather and analyse reliable data that can inform practice and guide legal developments and reforms. Our analysis shows that adjudication is fit for purpose but there are also areas for potential improvement, for example when it comes to the disclosure of conflicts of interests, the diversity of adjudicators and so-called ‘smash and grab’ adjudications.”
The report analyses data drawn from two questionnaires: one addressed to adjudicator nominating bodies (ANBs) and the second addressed to individuals involved with statutory adjudication. Ten ANBs replied to the first questionnaire and 257 individuals replied to the second.
Statutory adjudication was introduced in the UK in 1998 and the report finds that referrals have steadily increased, reaching an all-time high in the year to April 2021. That suggests, the authors argue, that Brexit and the COVID-19 pandemic have not significantly affected the upward trend in adjudication referrals.
The authors found that:
• Parties predominantly comply with adjudicators’ decisions: 25% of questionnaire respondents said that they have never experienced an adjudicated dispute being referred to litigation or arbitration and 42% of respondents replied that this occurs in less than 5% of cases.

• Nearly half (40%) of respondents suspected that on at least one occasion the adjudicator was biased toward one of the parties. The main cause of the suspicion of bias was the adjudicator’s relationship with the parties or party representatives.
• Few British ANBs publish the composition of their adjudicator panels online. Among the eight that do, women account for only 7.88% of listed adjudicators. There is no data on the representation of people with other protected characteristics.
• Over half (58%) of respondents felt that adjudicators' decisions should not be published; however, 30% replied that they should be published with redactions, following the model adopted in Singapore.
In his Foreword to the report, Lord Justice Coulson wrote: “I enthusiastically commend this report to anyone involved or interested in construction adjudication. I suspect that its publication will come to be seen as a seminal moment in the story of this unique dispute resolution process.”
The report is the first output of a three-year CCLDR research project, produced with the support of The Adjudication Society. q
25 25 www.yourexpertwitness.co.uk
Councils to get new powers to tackle ‘land banking’
[ COUNCILS MAY BE GIVEN further powers to tackle slow build-out by developers by applying financial penalties. The measure is being considered by the government in addition to the changes to planning regulations introduced in the Levelling Up and Regeneration Bill.
Those changes, designed to prevent developers ‘land banking’, mean that developers will have to report annually to councils on their progress and councils will have new powers to block planning proposals from builders who have failed to deliver on the same land.
Housing targets remain an important part of the planning system and the government will consult on how these can better take account of local density.
The Secretary of State for Levelling Up, Housing and Communities, Michael Gove, has also written to the Competition and Markets Authority to ask it to carry out a market study on housebuilding.
Mr Gove said: “We have an urgent need in this country to build more homes so that everyone - whether they aspire to home ownership or not - can have a high-quality, affordable place to live. But our planning system is not working as it should.
“If we are to deliver the new homes this country needs, new development must have the support of local communities. That requires people to know it will be beautiful, accompanied by the right infrastructure, approved democratically, that it will enhance the environment and create proper neighbourhoods.
“These principles have always been key to our reforms and we are now going further by strengthening our commitment to build the right homes in the right places and put local people at the heart of decision-making.” q
Welcome to our A to Z guide of the websites of some of the Expert Witness field’s leading players.

If you are one of our many online readers simply click on any of the web addresses listed below and you will be automatically directed to that particular website.
To get your website listed on this page just give us a call on 0161 710 3880 or email ian@dmmonline.co.uk
Translations and Interpreting for the Legal Profession since 1997. Specialists in Personal Injury and Clinical Negligence. www.abc-translations.co.uk
Salam Alaswad LLM PGDip BSc
• Financial derivatives • Contracts for Difference (CFD) • Forex fraud • Financial crimes • Pre-action assessment • Charts and diagrams for complex cases www.fxandcfd.com/expert-witness
Dr Paul Baskerville MA DM FRCS
Expert witness instructions in cases relating to all aspects of vascular disease. Can act on behalf of claimant, defendant or as Single Joint Expert. www.baskervilleclinic.com
CEERISK Consulting Ltd

Expert witness services in engineering
• infrastructure • construction • oil & gas • petrochemicals
• power & energy • mining • insurance • technology • telecomms www.ceerisk.com
Professor Frank Chinegwundoh MBE

Consultant Urological Surgeon specialising in Personal Injury and Medical Negligence cases on behalf of either claimant or defendant or as a Single Joint Expert. www.urologyconsultant.co.uk

Clarke Gammon
Chartered Surveyors with experience in All Aspects of Property • Residential property values
• Asset valuations • Land values and more www.clarkegammon.co.uk

D & HB Associates Ltd

Experts in Road Traffic Offences • Accident investigation and reconstruction • Tachograph analysis • Stolen vehicle examination and identification • Statement Taking www.dandhb.com
Dr Lars Davidsson MRCPsych MEWI
Consultant Psychiatrist and Accredited Mediator Reports within most areas of general adult psychiatry. Specialist in PTSD, anxiety disorders & mood disorders. www.angloeuropeanclinic.co.uk
Chris Dawson MS FRCS LLDip
Consultant Urologist with over 18 years experience of medico legal report writing and expert witness work in personal injury and clinical negligence cases. www.chrisdawson.org.uk



26 26 www.yourexpertwitness.co.uk
FHDI - Kathryn Thorndycraft-Pope
Laird Assessors
Martyn
Slyper Consultancy

Expert Witness in Assistive Technology
Personal Injury • Clinical Negligence • Industrial Injury E: ms@martynslyperconsultancy.co.uk www.martynslyperconsultancy.co.uk
Professor Christopher Raine MBE
Specialist in paediatric and adult otology
Mr Sameer Singh MBBS BSc FRCS Orth Consultant Orthopaedic Surgeon

All aspects of trauma – soft tissue and bone injuries

Upper and lower limb disorders and injuries • Whiplash injuries • Performs claimant and defence cases Clinic locations – London, Milton Keynes and Bedford

Dr Elizabeth J. Soilleux MA MB BChir PhD FRCPath PGDipMedEd
Expert Witness Pathologist with a particular interest in haematopathology. Short reports on specimens, full court compliant reports and expert biopsy reporting. www.expertwitnesspathologist.co.uk

Mr Bernard Speculand MDS FDS FFD FRACDS (OMS)
Consultant Oral and Maxillofacial Surgeon. Personal injury and clinical negligence cases for claimant, defendant and as Single Joint Expert. Special interest is TMJ Surgery.

Yvette Young (Secretary) T: 0121 605 1884 E: info@medsecadmin.co.uk www.birminghamtmj.co.uk

Target Psychology Ltd

Myles J O Taylor BA(Oxon) PhD FRCOG Expert witness specialising in: • General obstetrics & gynaecology









including twin to twin transfusion syndrome, intrapartum care and general gynaecology. www.mylestaylor.co.uk
Vincent Theobald-Vega Health and Safety expert

27 27
www.yourexpertwitness.co.uk
•
Examining documents & handwriting • to determine authenticity • to expose forgery
to reveal aspects of origin. Electro Static Detection Apparatus and Mi-Scope used. www.forensichandwriting.co.uk
Kulvinder Lall Consultant Cardiothoracic Surgeon Instructions taken in cases relating to cardiac and thoracic surgery, including aspects relating to surgical care and those following trauma to the structures of the chest. www.kulvinderlall.com
FIC Steel
international arbitration
cross-examination
in complex
• Pricing •
•
of
accounting
litigation support: • Fraud • Money laundering •
•
•
specialises
Duty
&
Dental Reports on the instruction of solicitors. www.dentolegal.com Haydn Jones MEng DipLaw FIET Data Technologist & Digital Regulation Expert • Injunctive relief • Money laundering • Digital currency theft • Counter funding of terrorism haydn@blockchainhub.com www.FCIR.co.uk Forensic Collision Investigation & Reconstruction Ltd Specialists in the analysis of road traffic collisions • Collision Reconstruction • Expert Witness • Vehicle Examinations www.kimhakin.com
Consultant Ophthalmic Surgeon and Expert Witness on ophthalmological matters
•
Civil Mediator •
The UK’s leading independent automotive expert witness firm supporting claimant, defendant and criminal solicitors. From instruction to court. www.laird-assessors.com Mr Roger Emmott CEng BSc(Hons) MSc/MBA MA FCMI
and iron ore expert with
and
experience
disputes
Contractual matters
Valuations T: 07974 351704 E: roger@rogeremmottassociates.com www.rogeremmottassociates.com DRC Forensics Limited EDRC Forensics Limited offers the complete range
forensic
&
Partnership disputes
Loss of profit
Professional negligence www.drcforensics.co.uk DentoLegal Ltd – Gary M Simon DentoLegal
in the preparation of evidencebased Breach of
& Causation and Condition
Prognosis
Mr Kim Hakin FRCS FRCOphth
Mr Chris Makin • Chartered Accountant
Accredited
Accredited Expert Determiner www.chrismakin.co.uk
• Medical negligence • Personal injury cases involving noise induced hearing loss. www.profchrisraine.co.uk www.orthopaedicexpertwitness.net
•
•
•
•
•
•
•
•
Public & Private Law Proceedings
Pre-Proceedings
Immigration Proceedings
Criminal Proceedings
Court of Protection Proceedings
Personal Injury and Clinical Negligence www.targetpsychology.co.uk
•
•
•
•
Asbestos management & removal
Construction design and management
Laboratories
Biological & chemical safety and much more. www.safety4hed.co.uk
•
–
Fetal Medicine • Multiple pregnancy
•

MEDICAL NOTES

[
LOOKING BACK on the past 12 months is a less-than-encouraging exercise when it comes to the world of the medical expert witness. Looking back over the year, the CQC – the medical profession’s regulatory body – describes the health and social care sector as ‘gridlocked’. The process of people being ‘stuck’ in hospitals because the social care sector is full, leading to people being ‘stuck’ in ambulances, leading to those ambulances not being able to attend emergencies, is described by the CQC’s chief executive.
• The almost-unimaginable lengths of waiting times for treatment of mental illness has also found its way onto the headlines. The Royal College of Psychiatrists has described the figures as a ‘hidden waiting list’, with three quarters of people on it resorting to emergency or crisis line numbers. It has a number of horror stories, one of which we hear about.
• A retrospective of maternal and neo-natal deaths has also been published. While there has been a slight improvement in the disparity between white patients and their black or Asian counterparts in rates of mortality, the gap between affluent and poor areas has widened. Both doctors and nurses in the sector are understandably outraged.
• The dire consequences of the NHS’s gridlock can only result in an increase in claims for negligence – whether that negligence can be seen to lie with the practitioner or systemic failures. While a number of high-profile cases find their way onto the pages of publications such as this and into the courts, a large number of cases where less-than-perfect care was received are dealt with by NHS Resolution via ADR and, as often as not, by a simple apology.
• Where there has been negligence, as well as redress by the trust in question, we rely on the profession’s own regulators to take action. The GMC is facing questions regarding one surgeon who has been allowed to continue to practise despite it being alerted to shortcomings as long ago as 2016.
• The other side of the coin has also come to light with the prosecution of a claimant for lying about the disabilities he suffered following surgery. He had claimed over half-a-million pounds for injuries which the judge described as ‘wholly false’.
• Unusually, this time of year has seen the four-yearly jamboree that is the FIFA World Cup. In England’s first match, against Iran, the Iranian goalkeeper was allowed to play on after a serious head injury – in the face of now-accepted practice and sporting guidelines. Former players of a number of sports are seeking redress for concussion injuries. Our contributor Mike Potts looks at the state of knowledge on the issue.
• Many head injuries result from and in facial trauma. Whether the trauma results from an assault, a fall, a motoring accident or even a game of football, the effects can be hidden. That is why great care must be taken in assessing the extent of injury caused by a facial trauma, as described by oral and maxillofacial surgeon Mr Zaid Sadiq.
• The result of many injuries is scarring, which can lead to severe psychiatric problems. While for most sufferers the effects are manageable, for some scarring leads to severe disability and even breathing problems. While there is redress for some whose scarring was the fault of someone else’s action, there is hope that the process of scarring may be halted or even prevented in the future. A forward-looking charity is investigating the possibilities.
• We cannot end the year more joyfully than by adding our congratulations to those of the British Orthopaedic Association in offering good wishes to John McFall, the first person with a disability to train as an astronaut at the European Space Agency. q
29 29 www.yourexpertwitness.co.uk

30 30 www.yourexpertwitness.co.uk
Healthcare system is ‘gridlocked’, CQC finds
[THE CARE QUALITY COMMISSION’S annual assessment of the state of health and social care in England, published in October, is that the health and care system is gridlocked and unable to operate effectively. That conclusion is based on CQC’s inspection activity, information received from the public and those who deliver care, alongside other evidence.
Most people are still receiving good care when they can access it: too often, however, people are not able to access the care they need. Capacity in adult social care has reduced and unmet need has increased. Only two in five people are able to leave hospital when they are ready to do so, contributing to record-breaking waits in emergency departments following a decision to admit, and dangerous ambulance handover delays.
As part of the assessment – which included a series of co-ordinated inspections across the urgent and emergency care pathway in 10 Integrated Care Systems (ICSs) – CQC convened a group of 250 health and care leaders. They described the system they work in as ‘in crisis’ and shared their fears that the risk of people coming to harm represents a worrying new status quo.
Health and care staff want to provide good, safe care but are struggling to do so in a gridlocked system, the CQC says. That is reflected in growing public dissatisfaction with health and care services – which is mirrored in staff dissatisfaction. More staff than ever before are leaving health and social care and providers are finding it increasingly challenging to recruit, resulting in alarmingly high vacancy rates which have a direct impact on people’s care.
Without action now, staff retention will continue to decline across health and care, increasing pressure across the system and leading to worse outcomes for people. Services will be further stretched and people will be at greater risk of harm as staff try to deal with the consequences of a lack of access to community services, including adult social care.

In this year’s report CQC also highlights its concerns about specific service areas: in particular, maternity services and those that care for people with a learning disability and autistic people – areas where inspections continue to find issues with culture, leadership and a lack of genuine engagement with people who use services.
CQC’s chief executive Ian Trenholm commented: “The health and care system is gridlocked and unable to operate effectively. This means that people are stuck – stuck in hospital because there isn’t the social care support in place for them to leave, stuck in emergency departments waiting for a hospital bed to get the treatment they need and stuck waiting for ambulances that don’t arrive because those same ambulances are stuck outside hospitals waiting to transfer patients.
“There’s lots of great care out there – from the GP practice in Manchester carrying out ward rounds in care homes to the new initiatives introduced by a hospital in Newcastle-upon-Tyne which have improved
people’s access to and experience of cancer treatments, to the ICS in Cornwall using inclusive technology to help give people more control of the services they use.
“However, the fact is that it’s hard for health and care staff to deliver good care in a gridlocked system. There are no quick fixes, but there are steps to be taken now on planning, investment and workforce that will help to avoid continuing deterioration in people’s access to and experience of care.”
Kate Terroni, chief inspector of adult social care and integrated care, and interim chief operating officer, added: “Through our inspection activity we see much good and outstanding care – as well as issues with culture and leadership which can lead to increased risk for people, as we’ve highlighted in maternity services and services for people with learning disabilities and autistic people.
“However, through our work on local areas and systems and our oversight of the whole health and care system, we also see increasingly clearly how a lack of investment in one part of the system has consequences for the whole, and the impact this has on whether people get good care.” q
31 31 www.yourexpertwitness.co.uk
32 32 www.yourexpertwitness.co.uk
Doctors’ indemnity body calls for more women expert witnesses
[THE Medical Protection Society (MPS) is calling on more women doctors in active practice to put themselves forward for expert witness work. Data from the General Medical Council (GMC) show that 86% of the experts instructed in fitness to practise cases are men –only 11% are women.
The figures, obtained by MPS through an FOI request to the GMC, follow the launch of MPS's report Getting it right when things go wrong: the role of the medical expert, which highlighted the shortage of appropriately qualified doctors willing to undertake expert work and the need for the pool to be more diverse to reflect the medical workforce.
MPS fears the low proportion of women on the GMC's list of expert witnesses is indicative of the wider medical expert community and says barriers preventing women from taking up the role need to be broken down.
Dr Lucy Hanington, medicolegal consultant at MPS, explained: "Medical expert opinion plays a critical role in a range of criminal, civil, coronial and GMC processes. Such opinion can determine, for example, whether or not the Crown Prosecution Service pursues a conviction for gross negligence manslaughter
following an incident or error that leads to the death of a patient. In the Family Courts, medical opinion is relied upon in relation to decisions where the lives and wellbeing of children are at stake.

“Many bodies, including courts and regulators, are reporting difficulties in finding appropriately qualified doctors to undertake expert witness work. This is concerning in itself, but data showing that only a fraction of GMC experts are women confirms our fear that the expert pool is lacking in diversity as well as in size. There is, though, no single, centralised register of accredited expert witnesses to ascertain the complete picture.
“Medical expert witnesses provide a lens through which the courts and regulators glimpse what is going on in the real world of contemporary medical practice and they therefore influence society’s perception of the cultural norms and standards in medicine. Because of this influence it is important that the pool experts are drawn from is diverse and representative of the profession.
“We know there is concern that women and ethnic minorities are underrepresented in senior leadership positions. Diversifying the
expert witness pool is part of a wider jigsaw in addressing this and we need to break down the barriers preventing women from considering the work.”
She pointed to one common misperception – that an elite few undertake the work at the end of their careers. In fact, the majority of consultants and GPs should have the requisite knowledge to provide opinion in their field of expertise after an initial period in post, and should feel confident in doing so.
“We recognise there are practical difficulties in combining the demands of the court with those of busy clinical practice and family life,” she conceded, “however a lot of expert work can now be completed remotely.
“NHS employers and private healthcare providers should encourage expert witness training and recognise the gains associated with expert witness work forming an integral part of a doctor’s skillset.
“The work requires regular updating of knowledge and clear communication skills, as well as the ability to analyse complex information and come to a conclusion. Encouraging doctors to diversify their role may also improve job satisfaction and prevent burnout.” q
33 33 www.yourexpertwitness.co.uk


34 34 www.yourexpertwitness.co.uk
NHS Resolution: it’s about more than just compensation
[
ONE OF THE LARGEST datasets of healthcare related compensation claims in the world is held by NHS Resolution.
Formerly known as the NHS Litigation Authority, NHS Resolution sees it as its duty to use the information responsibly to drive positive change for patients and staff, outlined in its remit under the National Health Service Litigation Authority (Arrangements for the Existing Liabilities Scheme) Directions 2019.
A key aspect of its three-year strategy is to proactively encourage shared analysis of the information it holds across national bodies, clinical colleagues, academics and other researchers, in a consistent way that helps others to combine its data and insights.
Clinical fellowships
NHS Resolution employs a number of clinical fellows: healthcare professionals with an interest in research who dedicate time to analyse trends in the claims data. They produce a number of academic reports – also known as thematic reviews – including:
• A thematic review of clinical negligence claims in patients with diabetes and lower limb complications, identifying several key time points during the patient journey where intervention could improve care quality.
• Emergency department compensation claims that look at high-value and fatality-related
claims over £1m, missed fractures and hospitalacquired pressure ulcers and falls in emergency departments.
• Analysis of the data from the first year of an indemnity scheme for general practice, identifying that quicker and more accurate diagnosis and improved prescribing processes could result in better patient outcomes.
As its clinical fellows come from a variety of clinical backgrounds, NHS Resolution can ensure a structured and clearly articulated approach as to how it undertakes research and ensure they have the tools they need to progress their reports and analysis in a consistent and robust fashion.
Attending writers’ retreats at the London Southbank University with facilitation from Staffordshire University on how to write reports, what to include in their contents and how to make strong recommendations is another way the organisation supports and develops its clinical fellows.
Clinical coding
Delivering a range of technological improvements through its Core Systems Programme, which looks at the systems used to support business delivery, is another key element of the three-year strategy. One example is the delivery of flexible, configurable data tools that can respond to changes rapidly and easily.
One aim is to maximise the clinical information that can be extracted from its Claims Management System to support thematic reviews and learning from harm.
This clinical coding workstream – working with an IT department who are undertaking a programme within NHS Resolution to enhance technology capability – looks at the Claims Management System to extract a set of categories in a subject area that shows their similar characteristics and how they are related to one another (ontology) over hierarchical relationships among concepts (taxonomy).
Immersive learning
Another way NHS Resolution works with academic partners is through designing and developing engaging educational modules. One example is a maternity module, which includes three case stories, currently in development alongside partners Staffordshire University and Health Education England.
Benefits of academic partnerships
Academic partners provide the direction, education and training to allow NHS Resolution to process information in an effective and prescriptive way, such as prioritisation and implementation of recommendations and guidance, so that it’s available to healthcare professionals at the point of care. q
35 35 www.yourexpertwitness.co.uk
36 36 www.yourexpertwitness.co.uk
False claimant ordered to repay compensation
[
A MAN FROM ROSS-ON-WYE was fundamentally dishonest about his injuries in his attempt to claim more than half-a-million pounds in compensation from Wye Valley NHS Trust, a judge has ruled.
Sean Murphy brought a claim against the trust, alleging breach of duty in surgical repair of a left biceps tendon rupture in March 2017. He claimed that the injury permanently damaged his left arm, rendering him unable to return to work as a builder, and that he could not return to playing rugby, attend the gym or enjoy fully engaging with his young family as he had before the injury.
Mr Murphy, 37, sought damages in excess of £580,000 for his injuries, including for alleged lost earnings until retirement, and care and assistance until the age of 70.
Wye Valley NHS Trust had admitted that surgery on 31 March 2017 was not performed to an acceptable standard, and that Mr Murphy had suffered injury as a consequence. The trust apologised for that failure, and interim payments for Mr Murphy’s damages and costs were paid to his solicitors at the time.

Following the trust’s admission, NHS Resolution subsequently determined that Mr Murphy was exaggerating his injuries. Investigations showed that he was, in fact, able to work, play rugby and go to the gym.
At the trial at the Royal Courts of Justice on 11 and 12 October, the Deputy High Court Judge Mr Healy-Pratt found the evidence
obtained and disclosed of the claimant playing rugby, weightlifting and working was ‘unambiguous and damning’ and his assertions that he could not do any of those things were ‘wholly false’. The judge assessed that, if the claim had been honestly presented, it would have been worth no more than 0.85% of the total claimed. He concluded that the damages claim actually presented was ‘fraudulent on a massive scale’. Accordingly, he dismissed the claim on grounds of fundamental dishonesty.
Mr Murphy was ordered to repay the interim payments for damages of £40,000 and legal costs of £10,000 that had been paid on behalf of the trust, within 30 days. The court also awarded the trust its legal costs for the action, to be assessed on the indemnity basis.
Helen Vernon, chief executive of NHS Resolution, said: “This was a blatant attempt to obtain compensation from the NHS by dishonest means. While we will continue to compensate genuine claimants fairly, we will not hesitate to take firm action where there is fraud and exaggeration.”
Wye Valley NHS Trust’s managing director Jane Ives said fraud took money away from providing services for all.
“The NHS is for everyone,” she said, “and this kind of fraudulent behaviour means there is less money to spend providing the care and treatment that people need. This trust will not hesitate in taking action against anyone making fraudulent claims.” q
37 37 www.yourexpertwitness.co.uk
Working with water: hydrotherapy within expert physiotherapy reports
– is it a justifiable cost?
[HYDROTHERAPY can be a contentious issue within specialist neurological physiotherapy expert reports, because of the significant costs associated with installation and maintenance of a pool.
There are key differences between aqua therapy, hydrotherapy and water-based exercise:
• Aqua therapy is used by suitably qualified physiotherapists employing the therapeutic properties of water in treatment programmes to help maximise a person’s function. The term has now been adopted by the Aquatic Therapy Association of Chartered Physiotherapists to highlight the distinction from hydrotherapy.

• Hydrotherapy is water-based therapy carried out by non-specialist therapists such as support workers, carers and family members, who may not have extensive knowledge about the therapeutic properties of water.
• Water-based exercise includes swimming, aqua aerobics or following an exercise programme in the pool – with or without care support – for cardiovascular, mental health and
By Tanya Owen
a myriad of other exercise-related benefits.
It is rare that any of the above will replace land-based exercise, but for some claimants they can be an important part of therapy, rehabilitation and long-term health and wellbeing, including promoting confidence in water following injury.
While aqua therapy requires warmer pools, and some claimants need warmer water in the longer term, it does not automatically follow that a claimant will need a swimming pool at home. Alternative options for the expert witness to consider include local hydrotherapy centres, warmer pools at private health clubs and spa/plunge pools.
Not every pool has fully-accessible changing rooms, hoist facilities, chair or step entry to the pool. However, that is changing, with many local pools expanding their facilities.
In addition to considerations of access, the physiotherapy expert witness will consider how the claimant presents, their symptoms, their requirement for support, suitable alternatives, their subjective account of the benefits, frequency
of use and any track record of engagement with hydrotherapy provision, as evidenced in the records available. The admissibility is ultimately a matter for the court and there remains a mix of case law regarding recoverability.
Sometimes what a claimant needs or wants in the longer term is access to water sports and leisure activities. Formal therapy goes on the back burner in favour of disabled surfing, scuba diving and sailing – and rightly so; life is to be lived. Unfortunately, those are rarely represented within expert physiotherapy reports, but they really should be, as they are integral to the principle of reasonable restitution. q
• Tanya Owen MSc Global Health and Development BSc (Hons) Physiotherapy is a private neurological physiotherapist with Neuro Physio Works Ltd and an expert witness with Somek and Associates. She qualified as a physiotherapist in 1999 and specialises in neurology, spinal cord injury, cauda equina syndrome, brain injury, cerebral palsy and stroke.
38 38 www.yourexpertwitness.co.uk
Diabetic foot ulcers: why do they happen and how are they treated?
In his second article on issues surrounding diabetes, Dr Bobby Huda, consultant in diabetes and metabolism at St Bartholomew’s and Royal London Hospitals, discusses a common complication of diabetes

[DIABETIC FOOT ULCERATION affects between 1-2% of people with diabetes each year and is estimated to take up 1% of the total NHS budget. The lifetime risk of developing a diabetic foot ulcer can be between 10-25%.
An ulceration is defined as a break in the skin. People with diabetes are more likely to have peripheral nerve damage (neuropathy) due to longstanding diabetes and/or peripheral vascular disease. Both complications affect the feet disproportionately due to the relative distance from the heart and spinal cord.
Diabetic neuropathy
This is defined as the presence of symptoms and/or signs of peripheral nerve dysfunction in people with diabetes after the exclusion of other causes. Other less common causes of peripheral neuropathy include vitamin B12 deficiency, thyroid dysfunction, infections, HIV and trauma.
The person with diabetes may experience numbness or pain in the feet. Pain is typically stabbing, burning, worse at night and is usually bilateral. The distribution of neuropathy is usually in a ‘glove and stocking’ fashion, with the feet being affected primarily. Less common are damage to specific nerves or nerve roots (entrapment neuropathies, mononeuritis multiplex). However, many people with diabetic neuropathy can have no symptoms at all. Early neuropathy can be identified at the diabetes annual review, where the feet are tested for sensation with a 10g monofilament for light touch and vibration with a tuning fork.
Peripheral arterial disease
Peripheral arterial disease (PAD) is defined as atherosclerotic occlusive disease of the lower extremities. It is associated with an increased risk of lower extremity amputation and cardiovascular, cerebrovascular and renovascular disease. Prevalence in people with diabetes ranges between 20-30% but is higher in the presence of a foot ulcer. The presence of PAD is detected by symptoms (intermittent claudication or rest pain) or signs (absent foot pulses, pallor).
Foot ulcers
People with a significant foot ulcer invariably have neuropathy and around 50% will have PAD. Ulcers can lead to infection very rapidly, particularly with poor glucose control. Ulcer healing is predicted by a number of factors, including control of infection, optimising blood supply and pressure offloading. Optimising those factors needs careful coordination within a diabetes foot multidisciplinary team. This traditionally includes a diabetologist, a vascular surgeon, an orthopaedic surgeon, podiatrist, microbiologist, and an orthotics specialist, with support from diabetes/vascular specialist nurses.
Care is delivered within a diabetes foot MDT clinic, which is podiatry led but with ready access to the MDT. Most diabetes foot ulcers can be managed with regular outpatient appointments and often ulcer healing can take several months. Admission to hospital is indicated in the presence of significant cellulitis, ischaemia, likely presence of osteomyelitis (bone infection), pain and signs of systemic sepsis or hyperglycaemia.
Risk of foot ulceration
The presence of neuropathy, ischaemia, poor glucose control and abnormal foot pressures can all lead to increased risk of foot ulceration. The presence of risk factors should be identified in the diabetes annual review, which usually takes place within primary care. Foot examination is one of the eight care processes that is measured in the National Diabetes Audit and GP practices are often incentivised to ensure that is carried out. Identification of risks should lead to basic footcare advice and either signposting or onward referral to a community podiatry team.
Previous foot ulceration, callus build up, abnormal foot architecture, for example in the case of Charcot’s neuroarthropathy – which will be covered in detail in a future issue – can significantly increase the chance of foot ulceration, and referral to orthotics for custom-made, pressure offloading footwear is often needed.
Possible issues with care
People with diabetes foot ulceration often have poor engagement with healthcare professionals, regularly missing appointments to optimise glucose control and identify complications. There is also an increased prevalence of mental health disorders, including depression. They often self-neglect and seek help late when developing foot ulceration.
Primary care and emergency department healthcare professionals, being non-specialists, are often slow to pick up on the significance of a diabetes foot ulcer and treatment with antibiotics, offloading and referral to a diabetes foot clinic can all be delayed. This is crucial, as a person with poor glucose control, neuropathy and ischaemia, if untreated can progress from a superficial ulceration to a major amputation – above knee or below knee – within a week.
Prognosis
The prognosis for people with diabetes foot ulceration is extremely poor. The risks of amputation are high and can vary between 12% and 87% depending on the degree of ulceration at presentation. Scoring systems such as Wagner or SINBAD can be useful in objectively predicting risk. Mortality is also high and up to 50% at five years after an amputation, which is a worse survival rate than many cancers.
Medico-legal aspects
Claims are often made around failure to identify significant diabetes foot ulceration and delay in onward referral to specialists: NICE guidelines (NG19) recommend referral within 24 hours. Hence, claims tend to centre around primary care or emergency departments.
Inappropriate footwear, particularly if mandated by the nature of work, can also give rise to claims if ulceration follows. As people with diabetes foot ulcers invariably have poor glucose control and are often poor engagers, defence will often focus on the inevitability of foot ulceration and amputation regardless of the incident episode. q
• To contact Dr Huda call 020 3594 6058 / 07919 924925, email bobby.huda1@nhs.net alternatively visit londondiabetes.com or clevelandcliniclondon.uk
39 39 www.yourexpertwitness.co.uk
New noise level guidelines come too late for many sufferers
[
EARLIER IN 2022 new guidelines were adopted by the Association of British Insurers and the Industrial Disease Claims Working Party for diagnosing and quantifying noise-induced hearing loss (NIHL) caused by the working environment.
One of the leading claims firms in the area explained: “Previously, a claimant had to prove that they had lifetime noise exposure level of at least 100dB. To reach this, a person would have to have worked in noise levels of 90dB for around 10 years. Now, for example, a person would only have to work in noise levels of 90dB for one year.
“Previously, anything under 85dB Lep,d was disregarded, as it was seen to be too low to cause any noise damage. The new guidelines recommend removing the lower action level, thus leaving all noise exposure as having the potential to contribute to a person’s hearing loss.”
The new guidelines were produced following a study by Professor Brian C J Moore, Mr David A Lowe and Mr Graham Cox to diagnose and quantify noise-induced hearing loss – the so-called MLC guidelines. The guidelines suggest substantial amendments to the existing guidance.
The Royal National Institute for Deaf People (RNID) says: “Exposure to loud noise is the second biggest cause of hearing loss. You might not notice the effects of noise-induced hearing loss until years after you were first exposed to loud noise.”
The RNID identifies the cause of noise-induced hearing loss as being around very loud noises for a long time. That could include:
• Being in a noisy workplace
• Listening to loud music
• Loud bursts of sound, like gunshot or explosions.
“If you have hearing loss caused by exposure to noise,” the RNID says, “you will experience a dip in your hearing in the high frequencies. This means you won’t be able to hear highpitched sounds as well as sounds at lower pitches. If the noise exposure carries on, this dip will spread and affect both lower and high frequencies.”

Some people experience tinnitus as the first sign that their hearing has been damaged by noise. Tinnitus is the sensation of hearing a ‘ringing’ or similar sound which has no external cause for the noise. It can be as little as a distraction or as serious as a debilitating illness.
In some cases NIHL can be caused by noise in the workplace. In those cases there may be a case for seeking compensation for an industrial injury. The construction industry is an example. Ironically, steps taken to avert other injuries, such as the warning sirens of reversing vehicles, may exacerbate the problem.
A British company, Brigade Electronics, is actively developing multifrequency warning signs for vehicles that lower the decibel count and so help to reduce exposure to damaging levels.
For many, though, the damage is done way before the effects become apparent and is irreversible. q
40 40 www.yourexpertwitness.co.uk
Maternal mortality report prompts outcry from all sides
[
NOVEMBER SAW THE PUBLICATION of the MBRRACE-UK Saving Lives, Improving Mothers’ Care 2022 report, which looks into the care of women who died during or up to one year after pregnancy between 2018 and 2020 in the UK.
MBRRACE-UK is a collaboration appointed by the Healthcare Quality Improvement Partnership to run the national Maternal, Newborn and Infant Clinical Outcome Review Programme which continues the national programme of work conducting surveillance and investigating the causes of maternal deaths, stillbirths and infant deaths.
The latest report shows stark and widening inequalities linked to poverty and disadvantage. It highlights the fact that women living in the most deprived areas are more than twice as likely to die than those in the most affluent parts of the country. Ethnicity-linked disparities remain stark, but they have narrowed since the previous report.
Reporting on the findings, the charity Birth Companions said: “One in five (20%) of the women who died had involvement from social services, a marker of high levels of vulnerability and trauma. More than one in ten (11%) were recorded as experiencing ‘severe and multiple disadvantage’ based on available data on issues such as a
mental health diagnosis, substance use and domestic abuse. This is, as the report states, ‘known to be an underestimate… due to poor data collection on these and other factors’.”
The leading direct cause of death is suicide, which has risen three-fold since 2017-19 among women who are pregnant or within six weeks of a pregnancy ending. Severe mental health issues were a factor in 40% of the deaths between six weeks and a year after pregnancy.
Speaking for the Royal College of Obstetricians and Gynaecologists, its president-elect Dr Ranee Thakar said: “The results of today’s report are worrying, especially the increase in maternal deaths and the increasing impact mental ill health has on mortality rates: 86% of women died in the postnatal period. The report highlights that actions to improve outcomes need to be focused on postnatal care and holistic support in the first year after birth, as well as during pregnancy.
“It is also clear from the report that disparities in society have a clear impact on the likelihood of mortality, with those from more deprived areas being twice as likely to die as women in the wealthiest areas, and only a small decrease in the higher risk of maternal mortality for black and Asian women compared with their white counterparts.”
According to the Royal College of Midwives (RCM), the ‘statistically significant’ increase in maternal deaths is a tragic indication of a lack of government investment in maternity services.
Gill Walton, chief executive of the RCM, said: “Any rise in maternal deaths, however small, is deeply worrying and we are moving backward not forward. Governments must focus efforts on the crucial areas where women are being let down and not getting the care they deserve and should expect.
“They cannot expect services to keep robbing Peter to pay Paul. This is having disastrous consequences for women and families and is impacting staff. We have overstretched midwives and maternity services that have been trying to do too much, with too little, for far too long. This should be a time of great joy for women and families, but tragically for some, it is a time of heartbreak. For all of us, women and their needs should come first and be right at the heart of everything we do.
Dr Ranee Thakar added: “Recognising inequalities is a first step to understanding and challenging the social, economic and political contexts that inform the way we all live our lives and the health choices we make, and we continue to call on the UK Government to commit to a time-specific target to reduce maternal inequities to drive urgent innovation, improvement and investment.” q
41 41 www.yourexpertwitness.co.uk
Surgeon carried on working despite warning signs
[
UP TO 600 NHS patients may need to be recalled in relation to treatment provided by an orthopaedic surgeon who has been operating at an NHS hospital in Walsall and a private hospital in Birmingham.
Concerns have arisen in relation to shoulder surgeries conducted by Mr Mian Munawar Shah, in particular Latarjet procedures and shoulder joint replacements (arthroplasty). The Latarjet procedure (pictured) –also known as the Latarjet-Bristow procedure – is a surgical procedure used to treat recurrent shoulder dislocations, typically caused by bone loss or a fracture of the glenoid.

The recall of patients is at the recommendation of the Royal College of Surgeons.
First astronaut with a disability is orthopaedic registrar
[THE BRITISH ORTHOPAEDIC ASSOCIATION has congratulated John McFall on his selection as the world’s first person with a disability to undergo astronaut training with the European Space Agency.
John had his right leg amputated following a motorcycle accident in 2000 and following that obtained a BSc and MSc in Sports and Exercise Science in South Wales, with a particular interest in biomechanics and gait analysis. John learned to run again using a prosthetic knee and competed at the Paralympic Games in Beijing 2008, winning a bronze medal in the 100 metres.

He then studied medicine, graduating from Cardiff University School of Medicine in 2014. He is currently a trauma and orthopaedic registrar in the Wessex Deanery and lives with his wife and three children in the north east of Hampshire.
John has said he hopes to inspire others and show that “science is for everyone... and potentially space is for everyone”. q
According to solicitors Bolt Burden Kemp LLP: “The BBC has reported that there have been 21 medical negligence claims relating to Mr Shah’s surgery between 2010 and 2018. Some of these concern significant deterioration in the patient’s condition post-op. It is not clear if complaints pre-date this. The NHS Trust responsible for Walsall Manor Hospital contacted the Royal College of Surgeons in 2020 and their review of his work may be what has prompted the intervention of the Medical Practitioners Tribunal Service and the GMC. It is not clear why there was such a delay in investigating Mr Shah’s conduct and/or work.”
The BBC quoted one patient who alerted the GMC to Mr Shah’s work in 2016. She said: “I tried to stop him because I knew that I wasn't the first and I wouldn't be the last. I tried to get something done so others didn't have their lives ruined.”
The partner of another patient said: “We've had to fight and demand every step of the way and I'm still not sure we've been told what's happened – we've still not had any proper explanation.” q
43 43 www.yourexpertwitness.co.uk

44 44 www.yourexpertwitness.co.uk
Latest knee replacement recall sparks media storm
[
THE LATEST MEDIA FRENZY regarding joint replacements was sparked in October when US supplier Zimmer Biomet issued a product recall for some variants of its NexGen range of knee replacements.
The national press reported that up to 10,000 of the recalled products had been implanted in UK patients and lawyers Leigh Day reported that the MHRA had confirmed that they are ‘investigating concerns raised about the performance of the NexGen knee replacement components’.
The products concerned were voluntarily recalled after concerns that the components were failing at an unacceptably high rate. The NexGen is the second most commonly used brand of knee replacement used in the UK, and is frequently recommended by NHS surgeons carrying out knee replacements.
Leigh Day warns that: “Patients who have been implanted with faulty knee replacements may have to undergo revision surgery to replace the faulty components with new ones. Patient outcomes from revision surgeries are typically worse than
for primary knee replacements, and patients can be left with life-long consequences such as ongoing pain, weakness in the joint, instability and loss of mobility.”
Michelle Victor, product liability partner at the firm, said: “This knee replacement product was very widely used and trusted by many patients and surgeons, with tens of thousands of people in the UK having been implanted with it. The reports of failure rates above 15% are deeply concerning for patients, and should prompt the MHRA to carry out a thorough assessment of whether the NexGen is safe to be used in the UK.
“If you are concerned about the performance of your NexGen knee replacement you should contact your orthopaedic surgeon to investigate. For those whose NexGen knee replacements have already failed, it may be possible to bring legal action.”
The British Orthopaedic Association issued a statement to provide information to patients who may be concerned.
The statement says: “The concerns
were identified by the National Joint Registry (NJR) as part of their routine monitoring of implants. The NJR is the largest orthopaedic registry in the world and routinely collects data on hip, knee, ankle, elbow and shoulder joint replacement surgery and monitors the performance of all joint replacement implants.

“If you are worried about your knee replacement with new pain, swelling or limping you should contact your orthopaedic surgeon to discuss. If you do not know what type of knee replacement you have, the NJR have offered a service so you can find out.
“The alert relates to the NexGen Stemmed Option Tibial Component used with either the LPS Flex or LPS Flex GSF Femoral Components. National Joint Registry data suggests that tibial component loosening is a key cause of increased revision surgery. The recommendation is to monitor patients who have had these devices, for any new pain, inability to bear weight, swelling or instability of the knee.” q
45 45 www.yourexpertwitness.co.uk

Dentists call for ban on ‘misleading’ cereal ads

[
THE BRITISH DENTAL ASSOCIATION (BDA) has called on government to stamp out what it describes as misleading marketing claims by children’s food manufacturers, revealed in damning new research from campaigning body Action on Sugar.
The latest findings show that some breakfast foods aimed at toddlers contain up to four teaspoons of sugar per serving. Over three quarters of products claim to have ‘no added sugars’ or ‘only naturally occurring sugars’, despite many containing sugars from fruit juices, concentrates and purees – all of which are harmful to dental health, the BDA says.
Government guidance states that no added sugars, including those from processed fruit, should be consumed by children up to two years old.
In a statement the dentists’ organisation says: “It's an all-too-familiar approach from industry. Earlier this year our study of 109 baby pouches aimed at children under the age of 12 months found over a quarter contained more sugar by volume than Coca Cola, with parents of infants as young as four months being marketed pouches that contain the equivalent of up to 150% of the sugar levels of the soft drink.
“We want to see sweeping action on food marketing and labelling, including the complete removal of misleading nutrition and health claims on baby and toddler food and drink products. Together with the publication of
the long overdue commercial baby food and drink guidelines, we can ensure dedicated baby aisles in supermarkets are a ‘safe space’ for parents.”
BDA chair Eddie Crouch commented: “The food industry is walking parents down the garden path, pushing sugar-laden products as healthy options. Claims of ‘no added sugar’ are utterly meaningless when toddlers are receiving four teaspoons over breakfast. Tooth decay is the number one reason for hospital admission among young children, and ministers can't remain bystanders. Action here is a prerequisite if we're ever going to turn the tables on wholly preventable diseases.”
In 2017, the Sugar Reduction Programme was introduced, with a 20% reduction in sugar levels in certain key contributors to children’s sugar intake expected by 2020. The final report has now been published, showing a small reduction in sugar content across the board.
Action on Sugar commented: “Despite a disappointing headline figure, there are examples of product categories that have seen significant reductions in sugar content, showing the potential for the food industry to reduce sugar levels in their products.
“However, what is most clear from this, is that a voluntary programme is not an effective way to get the widespread and consistent reductions in sugar content that we need.” q
47 47 www.yourexpertwitness.co.uk

The medicolegal challenges of facial trauma
By Mr Zaid Sadiq, Oral and Maxillofacial (Head and Neck) Surgeon
[
FACIAL TRAUMA can be a major cause of morbidity, particularly in young adults. This is because the head and neck region contains the major sensory and functional organs. A major component of the morbidity is changes to facial appearance which can lead to detrimental physiological, aesthetic and psychological effects.
Although facial trauma alone is rarely life-threatening, some of the complications associated with it, such as massive bleeding, undiagnosed cervical spine injury and brain injury, can lead to the death of the patient. Other complications may cause irreversible damage unless they are treated rapidly.
The treatment goals in facial trauma are to restore functionality, minimise scarring and avoid further injury to the structures of the head and face. Although the oral maxillofacial surgeon plays a pivotal role in the treatment of facial trauma, a multidisciplinary approach is often required to achieve the best outcome for the patient. It is therefore important that consultation with other specialists is undertaken as early as possible.
As with all traumatic injuries, the first steps are to ensure a safe airway and control bleeding. Airway obstruction associated with facial trauma usually occurs because of an inhaled foreign body, excessive bleeding or a displaced fracture compromising breathing. However, in some cases, soft tissue damage can lead to swelling at a later stage that is severe enough to obstruct the airway.
Once the patient has been stabilised, a thorough head to toe survey should be carried out and any findings accurately documented. This must include examination for potential involvement of the brain or cervical spine. These types of injuries are present in a significant number of patients with complex facial trauma caused by high energy insults, particularly where there are fractures to the anterior skull base or frontal sinuses.
To prevent irreversible neurologic injury, it is safer to assume that spinal cord injury has occurred until it has been definitely ruled out. Leaks of cerebrospinal fluid are also serious, as they carry an increased risk of meningitis developing in the patient, but identifying them is complicated by the fact that presentation can sometimes be delayed.
Around a quarter of orbital fractures are associated with injuries to the eye. Therefore, patients should be evaluated for injuries that may lead to sight loss and should be managed to reduce the risk of this possibility. Double vision, which may be caused by inflammation or oedema, is common after eye injuries and is normally only temporary. These cases need to be evaluated to identify trapped soft tissue or displaced bone fragments. Lower lid malposition is also a frequent complication and can lead to significant morbidity. Avoiding it requires specialist surgical input to appropriately repair the soft tissues.
Fractures in the facial area are very common, with breaks of the nasal bone occurring most frequently. However, these fractures can be missed due to masking by swelling or the lack of appropriate assessment. Delayed treatment of nasal bone fractures can cause permanent changes in appearance and breathing difficulties, and surgical repair can become more challenging.
Cheek bone fractures can significantly affect the appearance of the face, causing obvious facial asymmetry. Inadequate reduction can result in flattening of the cheek and increased facial width. Furthermore, malformation of the eye socket may lead to displacement of the eyeball. Delayed repair is complicated and increases the chance of poor long term cosmesis.
Fractures of the mandible, or jaw bone, are present in up to 70% of incidents of facial trauma. The jaw is particularly prone to injury due to its prominence. Typically, the jaw will break in two places: at the point of impact and also in the location directly opposite this site. As well as potentially disrupting the patient’s airway, a broken jaw can lead to difficulties in speaking and eating. Missing, cracked or chipped teeth are also common and may require restorative dental work.
The aims of mandibular fracture repair are to restore the pre-trauma function, including the facial symmetry and dental alignment. Misalignment of the teeth, nerve injury and abnormal bone healing are well recognised complications of mandibular trauma and are often the result of the injury or inadequately treated fractures.
The constant functional demand on the mandible during talking and eating can compromise healing, as excessive stresses across the fracture and the fixation plates holding the reduced fracture can lead to fixation failure. This leads to further instability and non-union of the fracture may potentially be the ultimate outcome.
Facial trauma can be very challenging to manage successfully. Complications are common and, in serious cases, long-term post-trauma complications, such as scarring, can almost be viewed as inevitable. Early identification and appropriate initial treatment, along with careful post-operative monitoring and re-evaluation, are vital in obtaining the best functional and aesthetic outcomes. q
• Mr Zaid Sadiq is an Oral and Maxillofacial (Head and Neck) Surgeon based at Queen Victoria Hospital in West Sussex. He is dual qualified in both medicine and dentistry and accepts both adult and paediatric medico legal instructions. He has a keen interest in head and neck cancer, trauma surgery, reconstructive surgery, facial fractures and tissue engineering. He is available on a weekly basis for consultations in London. Read his full biography and download his CV at www.medicolegal-partners.com/sadiq


50 50 www.yourexpertwitness.co.uk
Surgeons’ leader addresses breast implant illness
[
IN OCTOBER the president of the British Association of Aesthetic Plastic Surgeons (BAAPS), Mr Marc Pacifico, issued a statement on the phenomenon known as breast implant illness, or BII: an umbrella term used by some women who have breast implants to describe a wide array of systemic symptoms experienced by them, that is symptoms affecting their whole body rather than a single body part. The symptoms frequently include tiredness, joint ache, brain fog, memory loss and headaches, but many other symptoms have also been described.

Mr Pacifico said: “The World Health Organisation does not recognise BII as a medical diagnosis as it has not fulfilled the criteria to be classified as a disease. No scientific link between breast implants and these symptoms has yet been identified; however, many women who identify as having these symptoms experience varying degrees of relief after their implants are removed.”
He noted that a huge amount of research has been done on the subject; most notably, in the past few months three high-level and welldesigned research studies have been published on the topic. Those studies investigated three specific areas that women who identified as having symptoms associated with their breast implants have described as being important, and possibly the root cause of their symptoms.
He summed up the three areas as:
• Whether the technique in which the breast
• implant capsule (surrounding scar tissue)
• was removed made a difference to the
• relief of their symptoms: there is a strong
• drive to get surgeons to remove the
• implant totally within the surrounding
• capsule, referred to colloquially as ‘en bloc’,
• as opposed to other safer techniques with
• lower morbidity for patients
• Whether there were any underlying
• bacteria or other infections identified that
• might be contributing to their symptoms
• Whether any heavy metals could be
• identified in the patients that might explain
• their symptoms: heavy metal poisoning is
• often blamed for breast implant illness.
The findings from the three studies, he noted, were that there was no difference in relief of symptoms between different capsule removal techniques – ie ‘en bloc’ removal made no difference to symptom relief when compared with other techniques; there were no infectious causes identified and the only variations in heavy metal detection – that were all well below potential toxicological and even acceptable exposure levels – could be explained by being higher in women who had tattoos, were smokers and had dietary habits that increased heavy metal intake: that is, there was no evidence of heavy metal poisoning.
The statement continued: “The symptoms experienced by these women are very real, but we have no medical explanation for the cause of these symptoms, and their symptoms have not been scientifically linked to their implants. It is always hard to prove a negative, but it is likely that some women who identify as having these symptoms have other reasons for them.
“My main advice is that firstly, if you have implants and experience any symptoms – such as tiredness, joint ache, brain fog, memory loss etc – please do not first assume they are related to your implants. It is crucial that you see your GP to exclude other medical causes, that could range from medical diseases, infections, menopausal reasons or a host of other reasons that need to be excluded first.
“Secondly, if undergoing implant checks, ensure that you are seeing an appropriately qualified surgeon on the GMC specialist register in either plastic surgery or general surgery with a special interest in breast surgery.
“Finally, you should be aware that there is no scientific evidence to support the benefit of undergoing the riskier so-called ‘en-bloc’ capsulectomy compared to other capsulectomy techniques when it comes to relieving systemic symptoms thought to be linked to breast implants or BII. This should not be presented to you as the only possible solution to your symptoms.” q
51 51 www.yourexpertwitness.co.uk
52 52 www.yourexpertwitness.co.uk
Will we always have to live with scars?

[
THE ISSUE of the psychological effects of scarring has come into the public consciousness over recent years – partially as the result of horrific scarring caused in a rash of acid attacks some years ago. For some people the result of a scar can be lifelong loss of confidence and in some cases even physical disability. The Scar Free Foundation – a medical charity that aims to eliminate scarring by understanding how scars form – says: “For some people, the impact of their scarring is life-long. Scars can affect appearance, the way people are able to use their bodies and also emotional wellbeing and self-esteem.”
The charity describes a scar as: “…a mark left on the skin after a wound or injury has healed. When the human body suffers an injury, a biological process to repair the wound is triggered. Scarring itself is the production of excessive amounts of connective tissue produced as the body reacts and repairs the wound. Our body’s priority is very much on fast wound closure rather than restoring the injured area to how it was previously. This imperfect process results in the creation of a scar.”
It continues: “We still have much to learn about wound healing and the way scars form. Improving our knowledge of the cellular processes of wound healing, and how a person’s genes can affect this process, will mean that in the future we will be able to intervene in the healing process to stop scars forming in the first place.”
In the meantime, while scars continue to cause physical and psychological distress, ways need to be explored to help victims deal with the effects. That can include compensation where the injury can be proved to have been caused by either negligence or malice. The causes are manifold, ranging from road accidents and accidents at work to assaults and even dog bites. Medical negligence is a further cause, whether that is by causing the injury itself or failure to take adequate steps to prevent excessive scarring.
Facial scarring gives cause to high levels of compensation – perversely, higher in women than in men and higher for young people than older, as it is thought they have to live the consequences for longer. Ultimately, of course, the aim is to eliminate scarring, which is the aim of the Scar Free Foundation.
As Professor Janet Lord, principal investigator at the Scar Free Foundation Centre for Conflict Wound Research in Birmingham says: “Scar free healing within a generation…that’s what we’re about. Trying to understand the scarring process and, in doing so, prevent it.” q
53 53 www.yourexpertwitness.co.uk
54 54 www.yourexpertwitness.co.uk
Eye care profession calls for image standardisation
[
THE DEMAND for eye care services is predicted to increase by 40% over the next 20 years. Currently, primary eye care delivers over 22 million sight tests a year and nearly 10% of all patients attending a hospital out-patient department go to the eye clinic.
In order to transform efficiency, accessibility and the timely care of patients and cope with that increase, the College of Optometrists and other eye care organisations, including the Royal College of Ophthalmologists, the Primary Eye Care Information and IT Committee and the Optical Suppliers Association, have called for the standardisation of digital imaging.
The college says that standardisation of imaging will allow a seamless interface with technology for joined-up patient care and the use of artificial intelligence that is ultimately effective in preventing avoidable sight loss.
The College of Optometrists said in a statement: “Being able to share a patient’s record and diagnostic images digitally across systems and between eye care centres in primary and secondary care will increase the ability to make swift and efficient diagnosis and treatment decisions.
“Clinicians and healthcare professionals, patient groups and the manufacturing industry have come together and agreed that developing a set of standards will drive interoperability of digital systems and diagnostic analysis by end-users to deliver efficient and high-quality patient care.”
To improve interoperability of digital imaging and patient care, the college has developed a set of actions that can guide the development of digital imaging standards.
Safety alert issued for ophthalmic pellets
[ THE Royal College of Ophthalmologists (RCOphth) has issued a safety alert following reports of Mydriasert ophthalmic pellets being left in situ after cataract surgery.
The alert states: “Recent evaluation of the data from the National Reporting and Learning System has shown a significant number of reports to the system related to the use of the Mydriasert ophthalmic pellet for pupil dilation. This includes reports of the Mydriasert pellet being left in situ post-surgery and the Mydriasert pellet not being found during post-operative checks.
“Whilst the harm to the patient is low, it is still possible that patients who had the Mydriasert pellet left in situ post-surgery will suffer from red eye and potential infection. We recommend that departments evaluate their standard operating procedures for the usage of the Mydriasert pellets.”
This review, the RCOphth says, should ensure that a member of the theatre team has the designated role of removing the Mydriasert pellet. It should also decide on the location the Mydriasert pellet is removed – in the anaesthetic room or theatre – and state a method of recording the removal of the Mydriasert pellet as part of the operative report.
The college says it has worked with manufacturers Théa Pharmaceuticals to develop an infographic which can be used in hospital departments. q
The college said: “This is an initiative that will only succeed if it is broad and inclusive, involving primary and secondary eye care, industry, policymakers, health service commissioners, patients and providers, making use of the expertise available to improve the interoperability of eye care imaging and significantly improve eye care for our patients.”
In primary care, imaging is increasingly offered in addition to sight tests so changes can be assessed, monitored over time and shared with secondary care. In ophthalmology, a huge number of digital images have to be analysed, repeated and shared with other professionals across hospital eye units, community practices and primary care optometrists.
Time and resources are wasted and a patient’s health diagnosis is often delayed – which can lead to avoidable loss of sight. More visits to eye units also cause stress and anxiety for the patient and contributes to waiting time delays.

The college uses ‘Julia’s story’ to illustrate common issues with clinical image sharing. The eponymous Julia has to have separate scans made for assessment of an abnormality found by her optometrist each time she attends hospital, resulting in time lost and resources wasted. Even the original scan taken by her optometrist cannot be read by the hospital ophthalmologist.
With consistent and effective imaging standards in place, Julia’s story could be transformed to one where each service and team – across primary, secondary care and other healthcare specialties – can see every eye scan and monitor how the abnormality is developing. q
55 55 www.yourexpertwitness.co.uk
Why would you join in chambers with other experts?
By Mr Kashif Qureshi BSc MB BS FRCOphth consultant ophthalmic surgeon

WHEN ASKED to write an article to answer that question it’s worth considering the definition of an expert witness: “A person whose level of specialised knowledge or skill in a particular field qualifies them to present their opinion about the facts of a case during legal proceedings.”
[
I have been a qualified doctor for 23 years now, working mostly in the NHS. During that time I have had the privilege to see some examples of the best care possible provided for patients. Unfortunately, I have also witnessed some examples of significant patient harm caused by negligence.
Consequently, I decided four years ago to become an expert witness, whereby I could draw on my specialised knowledge to give an expert opinion regarding cases of medical negligence. I was very fortunate to be approached by a very highly regarded organisation, Eye-Law Chambers, that has the collective experience of some of the best and most experienced ophthalmologists and optometrists in the UK.
Working as an expert witness enables me to help patients get an expert opinion regarding issues that have affected their lives. That expert opinion must be impartial, honest and within the scope of expertise of the witness and must never stray into becoming an advocate. Working as an expert witness also enables me to be a better clinician, providing better care for patients and enabling me to learn from the cases we encounter.
Even in a speciality field within medicine such as ophthalmology, there are many niche areas which need a range of expertise to manage diseases affecting each structure. Having detailed speciality-specific knowledge about all areas of the eye is exceedingly difficult if not impossible. It is, therefore, particularly important to work alongside other complementary specialists, who can cover their specific areas so that patients get the best possible service.
Working within a group of expert witnesses we can serve patients and their legal representatives better by ensuring that we provide expertise within the scope of our practice. It is notable that all the experts in Eye-Law Chambers are in active, current clinical practice and are not doing medicolegal work in retirement.
Having access to fellow experts can also provide different opinions regarding a case from differing perspectives. That may be important to identify an aspect of a case that may not be initially obvious. Some may view working with a collective as a disadvantage, as it may reduce the independence of an expert; however, in practice the opposite seems to be true.
In an organisation such as chambers there is also administrative support which provides a connection with the instructing lawyers and the clients. This support reduces the time wasted on administrative tasks, which benefits the patient and their legal representatives by enabling more timely delivery of expert witness reports. Additionally, where there is more than one expert in a particular field, the clients are better served by having cases dealt with in a timelier fashion.
I have found working in chambers a great experience and have benefited from the reduced administrative burden, while also having new colleagues for support and mutual help. The model should be more widely used. q
56 56 www.yourexpertwitness.co.uk
• For further information visit www.eyelawchambers.com
Head injury and concussion: where are we now?
By Mr M J POTTS, consultant neuro-ophthalmologist

[ THE AWARENESS OF CONCUSSION has come a long way in the past decade. We are much better at recognising it, we have some tools for measuring it and we are more aware of its potential for long-term damage and injury. Preventing it is more difficult and we are developing guidelines in sport and other fields to recognise and manage it, so as to prevent long-term damage.
Some people are more susceptible to it and genetics and long-term research may help explain that. We recognise that unconsciousness is not obligatory for its occurrence: merely a marker of potential risk.
There are many definitions of concussion, but largely a direct or indirect blow to the head results in initial temporary loss of orientation – only 25% may have actual loss of consciousness – with disturbed vision and balance. Concussion only becomes obvious after 10 minutes, which is why players leave the field for a ‘HIA’ (head injury assessment). If concussion is confirmed by HIA then individual and personalised guidelines come into play for management and return to activities.

Long term and/or recurrent concussion results in loss of function in four domains: cognition, physical malaise and headaches, sleep changes and mood changes.
The visual system remains a highly sensitive system with which to detect concussion. Why? Well, because over half the brain pathways are directly or indirectly connected to the visual system. Over three quarters (80%) of patients have visual or vestibulo-ocular symptoms. Eye movements are affected in a high proportion (30% to 60%) and there may be complaints of blurred vision, double vision and photophobia.
Vestibular and vestibulo-ocular systems are also commonly affected. Most symptoms resolve in one to three weeks with rest, but some will persist – with disabling symptoms. A second concussion during the early recovery is very bad, especially in the first 10 days.
Testing for concussion has evolved. Early tests of rapid number naming were 86% sensitive and 90% specific; they have evolved to rapid word and picture naming (Maddocks questions). Immediate examination of vision and eye movements is still often used in the field.
We have developed better more sensitive HIA tests both at the scene and in the immediate post-injury examination. There are now national and sports-specific guidelines for the management and return to activity in place.
Long-term recurrent episodes result in chronic traumatic encephalopathy (CTE) and boxers have been shown to have reduced retinal nerve fibre layer thickness, although it is not seen after one concussion.
We have some treatment options, largely around preventing recurrence and especially early after the first injury. Vitamin B complexes may help. Guidelines for the safe return to activities are in place for both amateur and professional sports. We are now aware that three or more concussions is very ill advised and may be career ending.
New detection techniques, including gumshield accelerometers and saliva or blood-based shock proteins are being trialled.
Medico-legally, there are more cases being pursued due to the increased awareness and assessment. However, it is recognised that there are some challenging issues there. Most of the assessment techniques are subjective tests, making them vulnerable to bias and variable reproduceability.
Individual susceptibility to concussion is a factor we do not fully understand, although it will probably have a genetic component. It has been long known and recognised that the motivation to recover from concussion is another factor affecting long-term outcomes.
How and why Valentino Rossi was able to crash at such high speeds over such a long period with such a high risk of concussion, and yet be able to jump back on his bike with ‘rubber like’ enthusiasm, is amazing. Unfortunately, Marc Marquez – a much younger fellow Moto GP rider – has been less fortunate and has recently succumbed to recurrent double vision as a complication of his numerous crashes.
The final problem for medico-legal aspects of concussion comes in proving causation. Many of the 1960s and 1970s football and rugby players now affected by chronic traumatic encephalopathy who are considering claims for concussion after-effects also drank prodigiously and smoked heavily, making the assessment of causation problematic. Assessment and guidelines were not in place then, either.
No doubt ‘concussion’ will continue to evolve and we will begin to have some more answers to these complex questions, and especially to the genetic predisposition components. q
57 57 www.yourexpertwitness.co.uk
58 58 www.yourexpertwitness.co.uk
New blood test could diagnose myocarditis
[THE FIRST BLOOD TEST to diagnose inflammation of the heart muscle, known as myocarditis, could be in use in as little as a year following the discovery of a molecular signal in the blood by researchers at Queen Mary University of London. The research, funded by the British Heart Foundation (BHF) and led by Professor Federica Marelli-Berg, offers hope of a quick and cheap way of diagnosing the condition.
Myocarditis is a difficult condition to diagnose. Symptoms include a temperature, fatigue, chest pain and shortness of breath, which can all be easily mistaken for other conditions. The gold standard method for diagnosis currently is a

Heart failure is on the increase among the young
heart biopsy: an expensive, invasive and risky procedure which can sometimes still miss signs of the condition. The charity Myocarditis UK estimates that one young person dies suddenly every week in the UK due to previously undiagnosed myocarditis.
The latest research found that the presence of T cells – a type of white blood cell – expressing a molecule called cMet in the blood strongly indicates that a person has myocarditis. They say that cMet-expressing T cell levels could be detected through a routine blood test that could cost less than £50, with results available within hours.
The researchers hope that this finding will improve diagnosis of myocarditis and help people to get the treatment they need earlier, reducing the risk that they will develop life-threatening complications such as abnormal heart rhythms or heart failure.
In the study researchers compared blood samples from several groups of patients, including 34 people with a final diagnosis of myocarditis. It showed that patients with myocarditis had significantly increased levels of T cells with cMet on their surface compared to other groups, including heart attack patients and those with no medical condition.

The findings add to the evidence that myocarditis is an autoimmune condition. The team found that cMet-expressing T cells become activated by molecules expressed by heart cells, producing an immune reaction against these cells that leads to inflammation of the heart muscle.
The researchers also discovered that, in mice, T cells with the cMet molecule seemed to have a role in driving the development of the condition. Blocking cMet with a widely available drug reduced the severity of their myocarditis.
The team will investigate the findings further in future studies and hope it will help them to develop the first targeted treatment for myocarditis.
Professor Federica Marelli-Berg, BHF Professor of Cardiovascular Immunology at Barts and the London, Queen Mary University, London, commented: “Early intervention is crucial when treating myocarditis as, in some cases, it can be only a matter of weeks between the onset of symptoms and development of heart failure. But without a diagnosis doctors can’t offer their patients the right treatment.
[
A RISING INCIDENCE of heart failure has been identified among young people. It follows a recent French study that identified 1,486,877 patients who were hospitalised for heart failure between 2013 and 2018. Of those patients, 70,075 (5%) were between the ages of 18 and 50.
However, the data showed that, while the year-on-year incidence of heart failure in the general population decreased, when broken down by age group there was a significant increase in heart failure in young adults, particularly males aged 36-50 years.
The type of heart failure tended to be of ischaemic aetiology, and a corresponding increase in the traditional risk factors for ischaemic heart disease was noted. Those young patients had higher rates of obesity, hypertension, diabetes or dyslipidaemia, with higher smoking rates.
Up to 30% of young adults (aged 18-50) were re-hospitalised during the study, and about 10% died in hospital from any cause within the first two years after index hospitalisation, suggesting a poor prognosis. Being in the younger age bracket did not confer a survival advantage.
Reporting on the research for the British Cardiovascular Society, Dr Megha Agarwal said: “This is worrying data and we need to become better in the prevention of heart failure by modification of risk factors.” q
“We think that this test for myocarditis could be a simple addition to the routine blood tests ordered in doctors’ surgeries. When viewed in combination with symptoms, the results could allow GPs to easily determine whether their patients have myocarditis.
“While we still need to confirm these findings in a larger study, we’re hopeful that it won’t be long until this blood test is in regular use.” q
59 59 www.yourexpertwitness.co.uk

60 60 www.yourexpertwitness.co.uk
Psychiatrists attack ‘hidden’ mental health waiting lists
[ NEARLY A QUARTER of mental health patients (23%) wait more than 12 weeks to start treatment, due to lack of consultant psychiatrists. That was according to research released by the Royal College of Psychiatrists (RCPsych) for World Mental Health Day on 10 October.
A Savanta ComRes poll of 535 British adults diagnosed with a mental illness – including eating disorders, addiction, bipolar disorder, anxiety and depression –revealed what the RCPsych described as the damaging consequences of ‘hidden waiting lists’ on the lives of patients. Over two fifths (43%) say that the wait between initial referral and second appointment – the point when treatment usually starts – has caused their mental health to worsen.
More than three quarters (78%) of those on that hidden waiting list reported that they were forced to resort to emergency services or a crisis line in the absence of mental health support – including 12% going to A&E, 7% ringing 999, 16% contacting 111 and 27% turning to a crisis
line. Waits can be longer than six months for 12% of cases, while 6% of patients wait for more than a year.
Patients whose mental health deteriorated say that it has led to financial problems such as debt and struggles with work resulting in job loss, as well as relationship difficulties including divorce and family breakdown.
Long waits for NHS mental health treatment are largely down to an insufficient mental health workforce, particularly when it comes to psychiatrists. There is currently just one consultant psychiatrist per 12,567 people in England. The Royal College of Psychiatrists is calling for a year-on-year increase of medical school places – from 7,000 to 15,000 by 2028/29 – and a fullyfunded workforce strategy.
Dr Kate Lovett, presidential lead for recruitment at the Royal College of Psychiatrists, said: “We cannot sit idly by and watch the most vulnerable people in our society end up in crisis. Not only do spiralling mental health waiting times wreak havoc on patients’ lives, but they also leave NHS
Rise in primary school referrals ‘worrying’, says DECP
[THE Division of Educational and Child Psychology (DECP) of the British Psychological Society says that a reported rise in the number of primary school children being referred to ‘alternative provision’ is worrying, and reiterates the need to increase the number of educational psychologists to ensure access for all children.
The research from Ofsted found that a lack of access to specialist help means more primary school children with additional needs are being referred to alternative provision (AP), with around 7,000 primary-age children in England currently known to be in AP.
The DECP says it has long been concerned with the issue of school exclusions and their long-lasting impact on children and young people’s outcomes, and the lack of access to educational psychologist services for all children across the education system. The rise in children being placed into AP highlights the need for schools and staff to have ready access to educational psychologists who can provide evidence-based interventions and support, the DECP says.
Professor Olympia Palikara and Dr Victoria Lewis, co-chairs of the DECP, said in a joint statement: “We know that exclusion is damaging not only to children and young people’s outcomes, but also on school environments and society more widely. This rise in primary school children being placed in AP is worrying, and shows the reality of the current state of our education system and the lack of support available for children and education staff.
“Educational staff need the support of expert professionals, which could allow more mainstream schools to support pupils with additional needs at an earlier stage, thereby avoiding an AP referral or any other type of exclusion.
“AP should only ever be used as a last resort and as part of a graduated and temporary approach, where children and young people should have access to an educational psychologist as part of a supportive process which facilitates their movement back into mainstream. The exclusion figures are indicative of the challenges facing children and staff within the education system; it is important that the government use its upcoming response to the SEND review to ensure there are sufficient specialist professionals to help children.” q
services with the impossible task of tackling rising demand.
“If we don’t train more doctors by increasing medical school places, waits will keep getting longer – especially in underfunded specialties like psychiatry.
“Government needs to take responsibility for the fact that without decisive action on workforce, it’s denying patients timely access to lifesaving treatment.”
The RCPsych quotes one 45-year-old patient from South London, who has been in and out of hospital 20 times over a decade with addiction and other mental health crises: “I dropped out of university and moved back home when my mental health worsened, and I had to wait six to seven months to be referred to a community team. The only other way to get help was to present to A&E, which was a traumatic experience – having to be reassessed and readmitted again and again.
“What I experienced after I was discharged only made things worse. There is no help when you are discharged, and I found myself in this revolving door for 10 years.” q
Psychologists criticise changes to Online Safety Bill
[
THE BRITISH PSYCHOLOGICAL SOCIETY (BPS) has said it is ‘deeply concerned’ by news from the government that it will remove from the Online Safety Bill the responsibility on technology firms to protect people from ‘legal but harmful’ content.
Those sections of the proposed Bill had faced criticism from free speech campaigners, including former minister David Davis.
In a statement the BPS said: “The BPS has consistently called for tech firms to be responsible for protecting children and adults from content that is deemed ‘legal but harmful’, warning that there is clear psychological evidence that the internet can distort, normalise, glorify and by extension encourage behaviours that compromise the safety of its users and those around them.”
Psychological research has demonstrated a link between exposure to content depicting risky behaviours – such as drug use, excessive alcohol use, disordered eating and self-harm –and violence to others.
BPS chief executive Sarb Bajwa commented: “This move by the government is hugely disappointing and increases the dangers that both vulnerable children and adults face online. We are very concerned that, if this Bill passes in its current form, both children and adults could be left exposed to incredibly harmful content which we know can have an impact on people’s behaviour in the ‘real world’, as we have seen in some of the tragic cases of young people taking their own lives after viewing harmful content online.
“We do not believe that adjusting algorithms and shifting the responsibility away from the tech companies and onto the individual is the solution we need to keep everyone safe.”
61 61 www.yourexpertwitness.co.uk
q








62 62 www.yourexpertwitness.co.uk ACCOUNTANCY
CONSULTANTS
ANTIQUES SURVEYORS
AGRICULTURAL & HORTICULTURAL
ARTS &








63 63 www.yourexpertwitness.co.uk COLLISION INVESTIGATION & RECONSTRUCTION BETTING & GAMING BUILDING, PROPERTY & CONSTRUCTION









64 64 www.yourexpertwitness.co.uk
ENERGY CONSULTANTS ENVIRONMENTAL HYGIENE FINANCIAL SERVICES ERGONOMICS DIGITAL TECHNOLOGY
COMPUTER & MOBILE FORENSICS CRIMINOLOGY DIAMOND & JEWELLERY VALUERS







65 65 www.yourexpertwitness.co.uk
FORENSIC SERVICES INSURANCE MECHANICAL & PROCESS ENGINEERING POLICE CUSTODY
GEOTECHNICAL CONSULTANTS







66 66 www.yourexpertwitness.co.uk
WOOD & TIMBER
TREE CONSULTANTS STEEL & IRON ORE
TRANSLATING & INTERPRETING





67 67 www.yourexpertwitness.co.uk
ACCIDENT & EMERGENCY MEDICINE DENTAL & ORTHODONTIC EXPERTS CARDIOLOGISTS & CARDIOTHORACIC SURGEONS
MEDICO-LEGAL EXPERTS
ANAESTHESIA
GENERAL SURGEONS





68 68 www.yourexpertwitness.co.uk
ENT CONSULTANTS GASTROINTESTINAL & COLORECTAL SURGEONS
ENDOCRINOLOGY
GERIATRICIANS




HAEMATOLOGY



69 69 www.yourexpertwitness.co.uk
LIVER SURGEONS
NEONATAL
& HEPATOLOGISTS MICROPIGMENTATION MEDICAL NEGLIGENCE
MEDICINE NEUROPSYCHOLOGISTS
NEUROSURGEONS

OBSTETRICS & GYNAECOLOGY





70 70 www.yourexpertwitness.co.uk NURSING & REHABILITATION CONSULTANTS








71 71 www.yourexpertwitness.co.uk OCCUPATIONAL MEDICINE & THERAPY ORAL & MAXILLOFACIAL SURGEONS ORTHOPAEDIC SURGEONS OPHTHALMIC SURGEONS ONCOLOGISTS
PAIN

PATHOLOGY
PHARMACOLOGY


PHYSICIANS





72 72 www.yourexpertwitness.co.uk
MEDICINE
OSTEOPATHS
PSYCHOLOGISTS








73 73 www.yourexpertwitness.co.uk
PLASTIC & HAND SURGEONS
PSYCHIATRISTS
SPEECH & LANGUAGE THERAPY


TOXICOLOGY


74 74 www.yourexpertwitness.co.uk
REHABILITATION
UROLOGICAL SURGEONS







75 75 www.yourexpertwitness.co.uk
TRICHOLOGY
VASCULAR SURGEONS