Has the time come for audiologists to be regulated under Ahpra?
THE EYE AND EAR PRACTITIONER
Meet the Victorian independent practising as a dual audiologist and optometrist
HOLISTIC HEARING REHABILITATION
A deep dive into the 5-step plan setting the gold standard in hearing health
AUDIOLOGY STAKEHOLDERS DEBATE FUTURE WORKFORCE REGULATION AS DECISION LOOMS
Australia’s peak audiology bodies and stakeholders have differing opinions over regulation of practitioners as a report considering future options and a decision by health ministers looms.
Two accrediting bodies are aligned and want self-regulation for audiologists and audiometrists through mandatory membership via a practitioner professional body (PPB).
A third professional association, and a peak consumer voice, Deafness Forum Australia, which represents over four million people with hearing difficulties, balance or ear disorders, believe mandatory registration of audiologists and audiometrists under the Australian Health Practitioner Regulation Agency (Ahpra) is best for the industry and the public.
Ahpra registration is among seven options state and territory health ministers have put on the table as they
consult on the future of audiology regulation, with a final paper due in July 2024.
Four options in the Queensland Health Consultation Paper Audiology Decision RIS (regulatory impact statement) shortlisted for the sector and public to consider before consultations closed on 31 May were:
• The status quo – the current model of self-regulation (certification under the National Alliance of Self-Regulating Health Professionals – NASRHP).
• Regulation specific to audiologists who perform paediatric diagnostic and cochlear implant care services, under the National Registration and Accreditation Scheme (NRAS) .
• Jurisdictional registration requiring audiologists to register in their jurisdiction to practise.
• National registration of all
audiologists through the NRAS under Ahpra. To be registered with Ahpra, a profession must be assessed for eligibility into NRAS.
Independent Audiologists Australia (IAA), a professional association representing audiologists in private practice, strongly advocates for mandatory Ahpra registration for all audiologists and audiometrists, regardless of workplace or specialty.
The accrediting bodies, Audiology Australia (AudA), which
GEL STEROID SHOT SLASHES MÉNIÈRE'S VERTIGO IN WORLD FIRST AUSTRALIAN TRIAL
An injection of the steroid dexamethasone in a gel formulation into the ear has dramatically reduced the number of days Ménière's disease patients have vertigo in a world first early clinical trial in Australia.
Three months after treatment, 70% of patients were no longer having definitive vertigo days (DVDs) where attacks lasted 20 minutes or longer. The gel formulation and novel delivery method enabling sustained release is what makes the therapy unique, says its developer, US-based hearing therapeutics start-up, Spiral Therapeutics.
SPT-2101 is a sustained-release formulation containing 6% dexamethasone for treatment
of Ménière's, which affects 40,000 Australians.
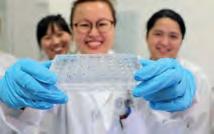
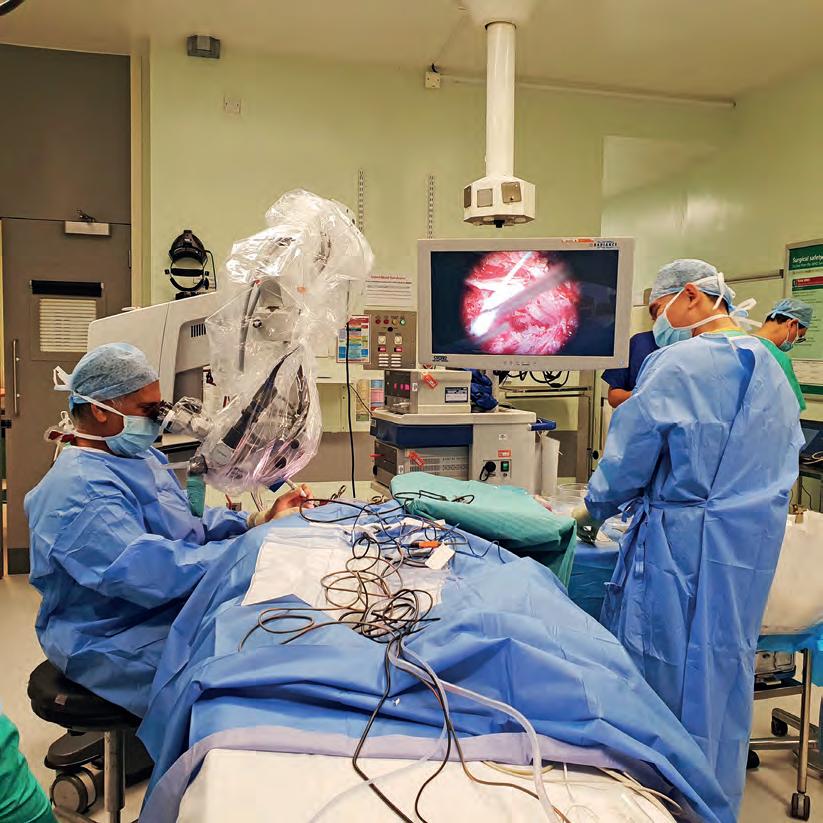
Lead investigator, Dr Jafri Kuthubutheen, an ENT, otology and skull base surgeon from Royal Perth Hospital, was the first to perform the novel surgical procedure on 10 patients in his tertiary care neurotology clinic.
“This is an important milestone in our journey to find better ways to treat Ménière's disease which affects so many of our patients,” he said. “I’m looking forward to what the future holds as we reimagine the way we treat inner ear disease.”
After receiving the formulation delivered precisely to the round window membrane, vertigo control
was measured with DVDs. The average number of DVDs was 7.6 during the baseline month dropping to 1.9 by month three. During the third month, 70% had zero DVDs.
“SPT-2101 delivery to the round window is safe and feasible, and controlled trials are warranted to formally assess efficacy,” researchers wrote online on 1 June 2024 in Otology & Neurotology
Sydney audiologist Dr Valerie Looi, the Australian clinical consultant to Spiral Therapeutics, told Hearing Practitioner Australia that a trial extension was about to finish recruitment at four Australian sites and the company was planning international phase III trials in 2025.
continued page 8
represents audiologists, and the Australian College of Audiology (ACAud) which represents audiologists and audiometrists, believe stronger regulation can be achieved through mandatory membership of audiologists and audiometrists to a PPB and an uplift of NASRHP’s regulatory powers.
All three professional bodies (AudA, ACAud and IAA) want audiology and audiometry to sit in the same regulatory environment.
NASRHP chair Ms Anita Hobson-Powell said the alliance needed legislative backing for formal recognition, which would strengthen it.
“Formal recognition of the NASRHP as the authoritative body entrusted to provide independent oversight to the self-regulating professions is needed
continued page 8
TAKING THE 'DIN' OUT OF DINNER
Adelaide audiologist Laura Drexler has created a website and app to help diners find quiet places to eat. The Ambient Menu highlights less noisy times and eateries for the hearing-impaired and those with normal hearing who prefer a peaceful meal experience. page 40
The National Scheme is governed by health law. Image: Jade/stock.adobe.com.
IN THIS ISSUE
Perfect alignment
Neelima Yadlapalli explains how she came to have her own stake in an audiology business in her 20s.
Your voice in Canberra
As the head of two major hearing industry organisations, audiologist Jane MacDonald wears many hats.
Hearing connections
Deep dive into current and future hearing aid tech improving the lives of those with hearing loss.
HERE TO SERVE THE HEARING INDUSTRY EDITORIAL
Welcome to the inaugural edition of Practitioner Australia (HPA) independent the nation’s thriving hearing industry.
After several months of planning, we’re excited to reach this milestone and be a voice for the entire industry, supporting and documenting the professional lives of audiologists, audiometrists, ENTs hearing health professionals in Australia.
HPA’s publisher, Prime Creative Media, established the masthead in April 2024 with the hearingpractitionernews.com.au website and social media channels, followed by a weekly e-newsletter. We’ve been excited by the excellent engagement so far – and now we have our first print edition, which will be published bi-monthly.
Sage advice
The lessons Dirk de Moore has for beginners and seasoned audiologists after 40 years practising.
The industry-dedicated editorial team consists of myself and managing editor Myles Hume who has edited HPA’s sister publication, Insight ophthalmic magazine, for five years. Between us, we have 37 years of health reporting experience. A major highlight has been immersing myself in the hearing industry, interviewing a variety of practitioners and attending our first industry conference, The Sound Exchange ’24 in Melbourne. There, we had the opportunity to share our vision with audiologists and industry suppliers who welcomed us with open arms. This is also evident through important partnerships we have formed with Audiology Australia, Hearing Business Alliance and the Australasian College of Audiometry.
I’ve been struck by the passion and enthusiasm of those I have interviewed, many of whom have a personal link to hearing loss. This edition is peppered with stories of people doing incredible things in practice, research and advocacy to help those one in six Australians with hearing issues. Regardless of your role in the industry, we’ve worked hard to ensure there’s content for you. The latest industry news, profiles on key decision makers and a deep dive into new hearing aid technology are included, but one I specifically urge you to read is Mr Daniel Pistritto’s Soapbox column on page 50. His heartfelt contribution, Life after deaf, encapsulates why hearing practitioners turn up for work each day – and why HPA is here to serve you.
HELEN CARTER Editor
Hearing Practitioner Australia is the only dedicated business-to-business publication for the nation’s hearing industry. Established out of a desire for premium, local and independent content for audiologists, audiometrists, otolaryngologists/ENTs and other Australian hearing professionals, HPA brings industry-specific reporting and analysis, in addition to the latest in news, business, products, policy, and research, plus more.
Just as HPA went to print, two bills passed in Maryland, USA, extending the SCOPEOF-PRACTICE for audiologists to include bloodwork and imaging. They clarified audiologists could “evaluate, diagnose, manage and treat auditory or vestibular conditions in the human ear”. From October 1, 2024, audiologists there can prescribe, dispense or externally fit a sound processor to an osseo-integrated device or cochlear implant. They can also order cultures and bloodwork testing related to auditory or vestibular conditions, in-office nonradiographic
OFF THE BEATEN TRACK
UPFRONT STAT
Weird
"Cheap wine" might have been a hit for Cold Chisel but it was not the case for Beethoven, according to US researchers who said consumption of cheap lead-based wine may have caused the composer's deafness through lead poisoning. They reported in Clinical Chemistry that DNA in two locks of his hair showed extremely high levels of lead, arsenic, and mercury.
Wonderful
British fashion retailer ASOS is being praised for using a model with a cochlear implant in some of its advertisements for earrings. The model, Natasha Ghouri, praised her modelling agency, M Models, for believing in her. Ghouri said it was her biggest achievement
Wacky
A Monash University-led team of palaeontologists has made a significant discovery in fossils that offers key information about the evolutionary shift from the jaw joint bones to those of the middle ear in early mammals. The findings, published in Nature, provide a clearer insight into the evolution of hearing in mammaliaforms. The fossils, from the Jurassic Period, are of two different species and show noticeable physical characteristics, suggesting a gradual change in the jaw joint's function towards specialising in hearing.
scanning or imaging of the external auditory canal and radiographic imaging related to auditory or vestibular conditions. IN OTHER NEWS, the official opening of Ear Science Institute Australia's first interstate Lions Hearing Clinic occurred in Neutral Bay, NSW. Ear Science CEO Professor Sandra Bellekom said research at Ear Science had had a national presence and impact for a long time and it was “a watershed moment to bring our clinical excellence to the east coast, providing patients in NSW clinical care led by science”. The NSW clinic joins 15 other Lions Hearing Clinics in Perth and WA. Ear Science board chairman Mr Rob Gordon, founding director Professor Marcus Atlas and local MP Ms Felicity Wilson also gave speeches.
FINALLY, a study in BMJ Public Health has found video gamers may be risking hearing loss and tinnitus. The global review of 14 studies of 54,000 adults and children found average sound levels often nearly exceeded or exceeded permissible sound exposure limits and risks grew the more time people spent gaming. Those who gamed regularly were more likely to experience tinnitus, measured high-frequency hearing loss and self-perceived difficulties hearing than those who never gamed. Study author, University of Pretoria audiology professor Dr De Wet Swanepoel said the study was “an eye-opener, highlighting the often-ignored issue of sound-induced hearing loss among the youth, particularly in relation to gaming”.
ENT patients
The Royal Victorian Eye and Ear Hospital sees more than 11,000 patients annually in its otology and cochlear implant specialist clinics. Page 18.
WHAT'S ON
THIS month
CERUMEN COURSES 14, 17, 22 JUNE
Ear Health Courses is running Cerumen Management 101 Courses on 14 June at Macquarie University, 17 June online and 22 June at The University of Melbourne. earhealthcourses.com.au
Complete calendar page 49.
NEXT month HBA SEMINAR 31 JULY
Hearing Business Alliance will run a one-day strategies for business success seminar at Mercure Perth. Proposed changes to the HSP will be discussed. hearbusiness.com.au
Each body has reinforced its stance in submissions to the consultation which the Queensland Department of Health has engaged Deloitte to do.
AudA CEO Ms Leanne Emerson said Deloitte had clarified that its scope for the review did not include audiometrists other than to consider impacts to audiometrists once a recommendation was made. The PPBs had strongly advocated for inclusion of audiometry and audiology through the review, she said.
The review followed incorrectly programmed cochlear implants received by children in Townsville and Adelaide.
Deafness Forum Australia said regulation was needed to prioritise safety as “the catalyst for considering regulation of the audiology profession was audiology failures in Townsville and Adelaide children’s hospitals, prompting millions in compensation to families and lost learning years for children” through wrongly programmed cochlear implants.
IAA said the only viable option was mandatory Ahpra registration of audiologists and audiometrists to protect the public, clearly define and regulate scope-of- practice, bolster professional standing, and avoid “increasing the complexity of the already fragmented regulatory landscape in our sphere”.
IAA president Dr Tegan Keogh said: “We support mandatory registration as the gold standard for safeguarding public interests, ensuring quality of service provision, and upholding professional recognition. IAA
cares about patient safety and the standing of audiologists in the community’s eyes, which is why we were the only professional body to submit a request for registration at the National Health Ministers Meeting.”
She said reasons IAA urged Ahpra registration were protection of title; quality and compliance; protections for the public; and health profession agreements with National Boards.
Meanwhile, Emerson said the most effective way to achieve professional regulation was through mandatory membership of audiologists and audiometrists to a PPB, supported through regulation changes to strengthen the powers of NASRHP, of which it is a member.
“Strengthening NASRHP’s powers would create title protection for audiologists, independent oversight of quality and complaints, and mandatory certifications for areas of audiology that pose additional risk (which could be done through AudA),” she said.
SCOPE-OF-PRACTICE IMPLICATIONS
There was also a risk that Ahpra registration could result in restrictions to current scopeof-practice such as full and expanded scope services, Emerson added. Ahpra registration would not address other issues that contributed to broader systemic failures in the specific cases, she said. Title protection, increased profile and improved access to referral and prescribing rights could be achieved outside the Ahpra model, she added.
However, Keogh said “the scope of practice could significantly increase
SERVICES POTENTIALLY OPENING ACCESS TO PRESCRIPTION RIGHTS.”
DR TEGAN KEOGH, IAA.
services offered by audiologists, potentially opening access to prescription rights (otitis externa, outer ear fungal infections or initial management of otitis media in children), and additional Medicare rebates for audiologists.
“The protective framework offered by Ahpra could allow an extended scope of practice for audiologists to perform these services, easing the high cost and burden of ENT wait lists. IAA will continue to advocate for audiologists in this space. The scopeof-practice is under review and IAA has provided a submission on this.”
The Australian College of Audiology incorporating the Hearing Aid Audiology Society of Australia (ACAud inc HAASA) said it remained committed to self-regulation and mandatory membership with a PPB.
ACAud chair Ms Marguerite Rushworth said: “ACAud remains committed to robust self-regulation. There are two professional bodies in Australia and they work to a consistent and agreed scope-of-practice with an effective external ethics review process to protect consumers.”
If regulation was introduced, it was imperative it included audiologists and audiometrists, Rushworth added.
About 800,000 practitioners from 15 health professions are regulated under NRAS and Ahpra. An Ahpra spokesman said although Ahpra made a submission, it was only a stakeholder as health ministers decide if other professions are to be regulated under the National Scheme.
Read more reaction from each of the organisations on page 10.
NOVEL 'MICS' DRUG DELIVERY IS POINT OF DIFFERENCE
continued from page 3
“The extension is a randomised placebo-controlled clinical trial being conducted in Perth, Sydney, Melbourne and Adelaide,” Dr Looi said, adding that it introduced a placebo-arm, allowing patients to later cross-over to receive the active drug if symptoms remained.
“Resuts are looking very promising. We’ve recruited 22 people – 10 in the initial study and 12 more in the placebo-arm extension. The study's likely to expand in 2025 so there's potential for greater involvement next year.”
In the initial trial, adults aged 18 to 85 years with unilateral definite Menière’s disease per Barany Society criteria received a single
injection under direct visualisation into the round window niche. Precise placement was achieved in all with in-office microendoscopy. Adverse events included one tympanic membrane perforation, which healed spontaneously after the study, and two cases of otitis media, which resolved with antibiotics.
Spiral said the landmark publication was a significant milestone in its journey to combat inner ear disorders via its novel minimally-invasive cochlear system (MICS) drug delivery platform. CEO and founder, Mr Hugo Peris, told HPA that injections of liquid steroid solution through the tympanic membrane were routinely used by clinicians off label
Dexamethasone in a gel formulation provides continuous drug diffusion across the membrane and into the cochlea. Image: Spiral Therapeutics.
for Menière's vertigo but Spiral believed " precise, long acting administration as opposed to blind, short-lasting delivery like the standard of care, is required for drugs to reach the inner ear and have an effect".
"We're demonstrating that a sustainedrelease formulation of dexamethasone, precisely-delivered at the round window membrane under visualisation, leads to significantly better management of vertigo in Ménière's patients," he said.
The formulation achieved weeks to months of residence in the middle ear and could be adapted to deliver drugs with anti-inflammatory, otoprotective and neuroprotective activity for balance disorders and hearing loss.
continued from page 8
Peak bodies and stakeholders debate
STRONGER SELF REGULATION THE PATH FORWARD, SAYS AUDIOLOGY AUSTRALIA
Audiology Australia (AudA) believes the most effective way to achieve professional regulation is through mandatory membership of all audiologists and audiometrists to a practitionerprofessional body (PPB).
t believes this should be supported through regulation changes to strengthen the powers of the National Alliance of Self-Regulating Health Professions (NASRHP), of which it is a member, to increase title protection and further strengthen independent oversight of quality and complaints, as well as mandatory certifications through Audiology Australia for areas of audiology that pose additional risk.
AudA said strengthening NASRHP’s powers could ensure safety and quality standards across self-regulating professions, leading towards advancing professionalism and safeguarding of health services.
“NASRHP oversees standards across 60,000 allied health professionals. It provides independent oversight of evidence-based minimum practice standards for health professions which meet requirements of membership. These align with Ahpra registration and standards, and both provide nationally consistent oversight of quality, including compliance with a code of conduct and consumer safety,” AudA CEO Ms Leanne Emerson said.
“‘Both regulatory systems work effectively to address scope-of-practice, competency
ACAUD INC HAASA CONFIDENT RIGOROUS SELF-REGULATION CAN BE ACHIEVED
The Australian College of Audiology incorporating the Hearing Aid Audiology Society of Australia (ACAud inc HAASA) said it remained committed to “robust self-regulation” and mandatory membership with a practitioner professional body (PPB.)
It believes this should be supported through regulation changes to strengthen the powers of the National Alliance of Self-Regulating Health Professions (NASRHP), of which it said it was in the process of becoming a member. The current structure of ACAud aligns with the requirements of NASRHP.
ACAud chair Ms Marguerite Rushworth emphasised that the primary objective should be the establishment of a regulatory framework designed to optimise the delivery of high quality audiological services. This framework should not only foster innovation within the field but also enhance accessibility for all individuals in need of these services.
She said that while the current consultation process was a step in the right direction, it had failed to consider several alternative options that could more comprehensively and effectively address these critical goals. By incorporating these overlooked options, a more robust and inclusive regulatory environment
standards, practitioner certification requirements and CPD, plus notifications or complaints. Neither provide industrial or business advice or a mandate on how an organisation or health service should conduct its operations. These gaps are important to consider.”’
AudA said the goal should be a regulatory environment that optimised delivery of high quality audiological services while promoting innovation and accessibility but there were options not included in the current consultation process that could comprehensively address this.
The organisation said it welcomed the opportunity to strengthen the profession and support professional regulation but there were positives and negatives to each model being considered. While regulation may support title protection and provide a clear pathway to address concerns and complaints about practising audiologists, AudA said it wouldn’t address a range of other issues that contributed to broader systemic failures in settings identified in the recent Queensland and South Australian inquiries. Equally, there was a risk that registration could result in restrictions to the current scope-of-practice for audiologists and audiometrists.
Findings from the inquiries suggested there was no evidence that regulatory models being considered would have changed outcomes for those affected or would offer protection against future issues, AudA said. Instead, the findings pointed to wider systemic failings across the health sector as contributing factors.
“It concerns us that this review may divert attention away from addressing the wider issues that have occurred across two public health systems,” Emerson added.
‘’Audiology Australia is not against the profession achieving registration and we continue to raise the issue with government whose response is that as a low-risk profession it doesn’t meet the criteria for registration.
“Some consequences come with registration that may not serve our members and advantages that regulation may offer including title protection, increased profile and improved access to referral and prescribing rights can be achieved outside the Ahpra model.”
AudA said striking a balance between regulation and flexibility was essential to support patient safety, high professional standards and advancement of the audiology sector.
could be achieved, ultimately benefitting both providers and recipients of audiological care, she added.
Rushworth said that if regulation was to be introduced, it was imperative that it included the entire sector – both audiologists and audiometrists.
“ACAud recognises the serious nature of the recent incidents in Queensland and South Australia and offers our deepest condolences to the families impacted,” she said.
“However, we believe that the current consultation might not address the root cause or prevent similar future incidents. It is important to note that the consultation paper seems to lack a complete understanding of the intricacies of our field, impacting the proposed measures’ potential effectiveness. Regulation would not have prevented the incidents from occurring and would not in the future.
“ACAud remains committed to robust self-regulation and working with peer organisations to strengthen the profession. The impact on the wider profession has not been considered.”
Rushworth said ACAud already enforced a comprehensive sector-wide Scope of Practice, Code of Conduct and Ethical Review Framework, along with the National Competency Standards, which collectively ensured the high standards of its members’ practise.
“Should regulation be introduced, it is imperative that it encompasses the entire sector, including both audiologists and audiometrists,” she said.
Rushworth said ACAud’s advocacy for mandatory membership with a practitioner professional body (PPB) underscored its belief in a unified approach to regulation.
“Given the size and specific risks associated with our sector, we are confident that it can be effectively managed through rigorous selfregulation,” she added.
“We are committed to collaborating with all stakeholders to ensure that any regulatory measures enhance the trust and quality of the hearing health care services we provide to the community.”
Image: Audiology Australia.
Audiology Australia CEO Leanne Emerson.
Image: Marguerite Rushworth.
Australian College of Audiology chair Marguerite Rushworth.
proposed regulation for audiologists
IAA SUPPORTS AHPRA REGISTRATION FOR AUDIOLOGISTS AND AUDIOMETRISTS
Independent Audiologists Australia (IAA) strongly believes in mandatory registration via the Australian Health Practitioner Regulation Agency (Ahpra) for audiologists and audiometrists, regardless of workplace, specialty or location as the only viable measure to provide consistent safeguards to patients at all stages of the lifespan – and to restore public confidence in audiology as a profession.
President Dr Tegan Keogh, PhD, said that for more than 15 years, IAA had lobbied and campaigned government for what it believes is an important step in quality assurance of the
“IAA cares about safeguards for patients and the standing of audiologists in the community which is why we were the only professional body to submit a request for registration at the National Health Ministers Meeting,” Keogh said.
"To our knowledge, no other professional body has made such a submission before.
“Regulation under Ahpra is not a new topic. In 2017 the parliamentary inquiry into hearing health recommended the Australian Government pursue registration of the hearing health sector under Ahpra. The events reported in 2023 in SA and Queensland have demonstrated the significant potential for life-altering risk to patients engaging with our sector and the shortcomings of self-regulation in managing this risk. Change is needed.
“IAA supports mandatory whole-of-sector
ALLIANCE OF SELF-REGULATING HEALTH PROFESSIONS SEEKS GREATER POWER
The National Alliance of Self-Regulating Health Professions (NASRHP) needs legislative backing for formal recognition, which will strengthen the body and enable better self-regulation of audiologists, the alliance believes.
Its chair Ms Anita Hobson-Powell said the current Scope of Practice Review had initiated discussions about the “regulation” of the health professions space. But she said the review lacked the recognition that self-regulation could be divided into two categories.
“Firstly, there are those who truly self-regulate, with individual professional bodies deciding how they will regulate their profession,” she said. “Secondly, there are professions falling under the NASRHP, operating to meet external standards for self-regulation.
“Formal recognition of the NASRHP as the authoritative body entrusted to provide independent oversight to the self-regulating professions is needed and must be in legislation.
“NASRHP can ensure safety and quality standards across self-regulating professions, leading towards advancing professionalism and safeguarding of health services.”
registration as the gold standard for safeguarding public interests, ensuring quality of service provision, and upholding professional recognition.”
She said there were four reasons why IAA continued to advocate for registration; protection of title; quality and compliance; protections for the public; and health profession agreements with the National Boards.
Keogh noted that titles of Ahpra-registered health professions were protected by law. If someone used a proteted title to describe their professional role, others could expect this person was appropriately trained and qualified in that profession, registered, and met safe and professional standards of practice, she said. They would have a clearly defined scope-of-practice for this title linked to their educational level and enforceable by law.
“Under the National Law, Ahpra works to make sure registered health practitioners meet the standards of their profession and takes action if it determines there is a risk posed to the public,” she said. “It’s a criminal offence for someone who isn’t a registered health practitioner to use a protected or specialist title. This isn't a function of NASRHP.”
Ahpra registration would mean legal protection of the title ‘audiologist’ and penalties for misuse including possible jail time. A national register of audiologists and audiometrists would allow the public to find accurate information about practitioners, and make informed choices about how they receive hearing and balance care, she added.
Ahpra advises the National Boards on registration standards, codes and guidelines for health practitioners. This ensures that only those with the necessary skills and qualifications to provide competent and ethical care are registered, Keogh said.
This would not restrict anyone from practising within their righful scope but would provide clear guidelines for the public about the expected scope for each profession and a transparent regulatory framework to allow audiologists to practise at the top of their scope, appropriate to their training. National Boards and Ahpra enforce the Health Practitioner Regulation National Law in each state and territory. By ensuring only suitably trained and qualified practitioners are registered, Ahpra upholds competent and ethical practice to protect public health and safety.
Hobson-Powell added that to ensure comprehensive oversight and standardisation “a legislative requirement mandatorily requiring all self-regulating health professional bodies to submit their regulatory frameworks for independent validation by NASRHP needs to be established”.
“Legislative mandates should unequivocally designate NASRHP as the equivalent to the Australian Health Practitioner Regulation Agency (Ahpra), establishing parity and credibility within the regulatory landscape,” she said.
In 2017, the national alliance emerged as a beacon of integrity, administering a robust quality standards framework for organisations within self-regulated health professions not covered by the National Registration and Accreditation Scheme (NRAS), Hobson-Powell said.
The Australian Department of Health and Aged Care provided seed funding, underscoring the need for an independent entity to uphold standards in self-regulated professions, she said. But since then, the government had not capitalised on its investment.
“NASRHP is ready to fill the gaps in self-regulation, it just needs legislative recognition to have the additional impact required for self-regulating professions,” she said.
NASRHP’s quality assurance system oversees about 60,000 allied health professionals dedicated to autonomous service delivery. More than 23,000 operate under self-regulation without the benefit of NASRHP’s regulatory oversight, she said.
In 2018 the Council of Australian Governments (COAG) stated that NRAS primarily served to shield the public from potential harm rather than to confer prestige or validate individual professions. Despite this, she said federal and state laws often referenced the Health Practitioner Regulation Law, which excluded two-thirds of the allied health workforce.
Image: IAA.
Independent Audiologists
Australia president Dr Tegan Keogh PhD.
Image: Anita Hobson-Powell.
National Alliance of Self-Regulating Health Professions chair Anita Hobson-Powell.
IN BRIEF
NASAL SPRAY
A nasal spray vaccine invented by researchers from Telethon Kids Institute and the University of Western Australia to prevent childhood ear infections is being produced for human trials planned for 2025. Lead inventor Associate Professor Lea-Ann Kirkham, a research microbiologist, has worked on the therapy for 10 years. She said it had been shown to work in the laboratory and work was now under way to start clinical trials. If successful, the spray could help prevent 700 million childhood ear infections globally a year, including severe infections that can lead to hearing loss. It could also slash millions of antibiotic prescriptions and surgeries to insert grommets. The therapy is for otitis media in young children, using ‘friendly bacteria’ to guard the ear from infection.
HEARING DONATION
BHP has donated $825,000 to Ear Science Institute Australia‘s philanthropic arm – the Gift of Hearing – to improve access to hearing services and treatment for First Nations people in WA. Collaborating with the community, Puntukurnu Aboriginal Medical Service (PAMS) and other stakeholders, BHP donated the funds to enhance the institute’s programs and improve the ear and hearing health outcomes of Aboriginal families in the East Pilbara region. “We are proud to partner with Ear Science to support the amazing work it does in the Pilbara, with a long-term vision to improve the ear health and quality-of-life for Indigenous peoples,” said Mr Meath Hammond, BHP head of corporate affairs.
APP-BASED DIAGNOSTICS
A smartphone app which uses artificial intelligence can accurately diagnose acute otitis media (AOM) by connecting to an otoscope, a study has found. The free iPhone app from the University of Pittsburgh assesses a short video of the patient’s eardrum captured by connecting an otoscope to a smartphone camera.
Senior author Dr Alejandro Hoberman, a paediatrics professor, said the automated classifier interpreted videos of the tympanic membrane to enhance accuracy in AOM diagnosis and assist treatment. He said study findings suggested it was “more accurate than many clinicians” and another benefit was that videos captured could be stored in a patient’s medical record and shared with other providers. Published in JAMA Pediatrics and using 1,151 videos of the tympanic membrane from 635 children at outpatient clinics, the study found sensitivity of 93.8% and specificity of 93.5%.
FED BUDGET: AUDIOLOGY MISSES OUT ON PLACEMENT PAYMENTS
Calls have been made for the Australian Government’s new weekly payments for some students doing practical placement to extend to audiology and speech pathology students.
From July 2025, the Commonwealth Prac Payment scheme will provide student teachers, nurses, midwives and social workers with a $320 weekly payment during their mandatory practical placements.
The new cost-of-living measure will be means-tested to target students who need it the most and will cover about 68,000 higher education and 5,000 VET students a year.
But Allied Health Professions Australia wants the measure expanded to cover allied health students including audiology and speech pathology students during their clinical and professional placements.
AHPA CEO Ms Bronwyn Morris-Donovan said “placement poverty” was real for many students of allied health disciplines where mandatory placements could be extensive.
“AHPA calls for an expansion of this ‘placement payment’ to ensure the supply of qualified allied health professionals matches demand for services and incentivises the
next generation of allied health professionals,” Morris-Donovan said. Meanwhile, audiology practices are among small businesses who can benefit from a one-year extension of the government’s $20,000 instant asset write-off scheme, announced in the Budget. The scheme was due to end on 30 June 2024.
“The Government is providing $290 million in cash flow support by extending the $20,000 instant asset write-off,” a statement said. “Small businesses with annual turnover of less than $10 million will be able to immediately deduct eligible assets costing less than $20,000 until 30 June 2025.”
MEDICARE CO-CLAIMING VICTORY FOR HEARING SECTOR
In a win for the audiology sector, the Medicare Benefits Schedule (MBS) brain stem evoked audiometry item can be co-claimed with vestibular assessment items from 1 July 2024.
The change will save patients money and make it easier for them to access the services. The Department of Health and Aged Care announced in May 2024 that co-claiming restrictions for the items would be removed and they could be claimed together “where clinically relevant for a patient’s circumstances”.
The changes are:
• Item 11300 (evoked audiometry) will be amended to remove co-claiming restrictions with vestibular assessment items 11340, 11341 and 11343.
• Items 11340, 11341 and 11343 will be amended to remove the co-claiming
restriction with item 11300.
Audiology Australia (AudA) said the outcome was a “major win for the audiology sector” and came after a long consultation with Audiology Australia’s policy and advocacy team, and government and key stakeholders in the hearing health sector including several AudA members
“For audiology clients, the changes will make accessing diagnostic audiology services easier and more affordable if a brain stem evoked audiometry and a vestibular assessment are required,” AudA said.
Independent Audiologists Australia (IAA) said it had lobbied persistently and worked hard to achieve the change and was pleased to see the department taking its feedback into consideration. "We’ll continue to advocate on behalf of members and their patients in this important area,” IAA said.
The change will save patients money and improve accessibility. Image: Robyn MackenzieShutterstock.com
‘Placement poverty' is a major issue for many allied health students. Image: Simone van den Berg/stock.adobe.com.
BIOBANK SET UP FOR GENETIC DEAFNESS THERAPIES
A biobank being established in Perth will be the first of its kind in Australia to store tissue related to genetic-associated hearing loss, aiming to advance genetic therapies for childhood and adult hearing loss.
The Australasian Hearing Registry and Biobank (AHRB) will be based at Ear Science Institute Australia and is a direct result of promising gene therapy trials overseas in deaf children, with the goal of having similar trials here.
“Recent breakthroughs in gene therapies have highlighted the potential success of new treatments, and it is with this understanding that Ear Science Institute Australia proposed the creation of the WA-based biobank,” a statement said.
“The gene therapy trials overseas have shown life changing results in children who could previously not hear and we anticipate the biobank catalysing more of this research in Australia.”
The biobank will allow increased access to genetic samples by linking to national and international registries through a network of clinicians, researchers, institutes and patients.
It will enable Ear Science to build research capacity that will lead to improvements in understanding genetic causes of hearing loss and help develop novel treatments including establishing personalised care.
A biobank is a facility that stores and manages biological samples donated from individuals for use in research, diagnostics, and treatment. Samples are typically linked to medical records or lifestyle information to provide researchers with comprehensive datasets for studying diseases, genetics and other aspects of human health and biology.
community is what Ear Science is known for,” she said. “Thanks to a $500,000 grant from the WA Government’s Future Health Research and Innovation (FHRI) Fund, we can truly tackle the cause and treatment of genetic hearing loss experienced by over 12 million children and adults worldwide.”
Adjunct Associate Professor Elaine Wong, head of Hearing Therapeutics at Ear Science Institute Australia added: “Pioneering gene therapy could restore hearing in patients with profound genetic hearing loss.
Biobanks play a crucial role in advancing medical research, personalised medicine and drug development by giving researchers access to large-scale, well characterised collections of biological materials.
Hearing loss affects one in six Australians and genetic disorders account for about 50% of these.
Ear Science CEO and audiologist, Adjunct Associate Professor Sandra Bellekom, said the institute was proud to lead Australia with the nation’s first hereditary hearing loss biobank. “The bringing together of researchers, hospitals, clinics and the
“The approach could help researchers develop therapies for other types of inherited hearing loss. About 155 genes have been identified to be associated with hearing loss, and two-thirds of childhood hearing loss has a genetic cause.”
The $1 million project is a collaborative project initiated by Ear Science founder Professor Marcus Atlas with Associate Professor Fred Chen and Dr Samuel McLenachan at Lions Eye Institute, Dr Stephen Rodrigues at Perth Children’s Hospital and Professor Nicholas Pachter at WA Health, as well as other partners in WA and collaborators across other states.
Adjunct A/Prof Elaine Wong. Image: Ear Science Institute Australia.
REPORT HIGHLIGHTS PROVIDER COMPLIANCE ISSUES
The latest Self-Assessment Report (SAT) has highlighted recurring compliance issues faced by service providers delivering the Hearing Services Program.
The Federal Government report, covering the period up to March 2024, included 333 service providers who were mandated to submit a SAT and revealed 97.6% of providers felt the SAT assisted them to comply with program requirements.
About 51.7% identified one or more issues requiring follow-up, including deficiencies in records management, completion of practitioner confirmations, disclosure of device supply arrangements, and incorrect practitioner listings.
The report also found that while 98.5% of providers have a written device supply arrangements disclosure, many reported they provide this to clients with other provider information “at the first appointment” or “on request” and, in some instances, provide this “verbally”.
“Please note that this disclosure must
List of approved membership categories by PPB
Audiology Australia
Australian College of Audiology
Hearing Aid Audiology Society of Australia
• Full accredited member or • Fellow accredited member or • Life accredited member
• Full/ordinary member or • Fellow member
• Full member or
• Fellow member
Source: Department of Health
format and be sent to a new provider in electronic format.
Finally, more than 25% of providers reported practitioner changes through the practitioner confirmation section of the SAT. Approximately 33% of these were outside the five working days required under the contract, with some up to five years old.
be provided to all clients in writing every time a device is discussed (before every fitting, refit, replacement, or spare device). This requirement applies even if a provider has no preferred supplier arrangements,” the report stated.
Additionally, some providers – including some storing all records electronically –reported printing and posting electronic records to a new provider.
The report stated all documents that are created electronically or are scanned into a provider’s system after completion by a client, must remain in electronic
Providers were reminded to “update the information held in the portal, including qualified practitioner information, within five working days of any change”.
Meanwhile, a notice issued by the Hearing Services Program, has reminded providers to ensure that only qualified practitioners (QPs) deliver or supervise services to program clients.
Providers are urged to ensure that QPs possess current financial membership in an approved category with a Practitioner Professional Body (PPB) at the time of service delivery. Failure to adhere to this requirement may result in reimbursement obligations for claims where the QP lacked current membership status.
MACQUARIE UNIVERSITY EXPERTS PROPOSE NEW THEORY ON HOW HUMANS HEAR
New brain research by a Macquarie University team has debunked a 75-year-old theory about how humans hear and how they determine where sounds are coming from.
It found a “sparse, energy efficient form of neural circuitry” performs this function.
The previous engineering-based theory was that each location in space was represented by a dedicated neuron in the brain whose sole function was to determine where a sound was coming from. This assumption has guided research and audio technologies for decades.
The new study found spatial hearing circuitry in humans is much simpler than first thought, and similar to what animals use for spatial listening.
It found that rather than having an array of neurons with each tuned to one place, human brains process sounds in the same way as many other mammals, using neural circuitry.
The paper’s senior author, Distinguished Professor David McAlpine, academic director of Macquarie University Hearing, explained findings and implications of the research paper, which was published in Current Biology on 7 May 2024, to the university’s magazine, The Lighthouse
“Just like other animals, we are using our ‘shallow brain’ to pick out very small snippets of sound, including speech, and use these snippets to tag the location and maybe even the identity of the source,” he said.
He said findings could lead to better voice recognition technology and more advanced hearing devices including hearing aids, cochlear implants and smartphones.
The goal for hearing aids and implants was to mimic human hearing and accurately locate the source of sounds but this remained elusive, he explained.
The current approach stems from a model developed by engineers in the 1940s to explain how humans locate a sound source based on differences of a few tenths of millionths of a second when the sound reaches each ear.
This model uses the theory that each location is represented by a dedicated neuron in the brain whose function is to determine where a sound is coming from.
In 2001, Prof McAlpine challenged this engineering model in Nature Neuroscience and although his theory was opposed, he continued to gather evidence to support it, showing that the existing model did not
Prof David McAlpine, Professor of Hearing, Language and the Brain, and Director of Hearing Research, Macquarie University Faculty of Human Sciences. Image: Chris Stacey/Macquarie University.
apply to species after species, including the prime animal for spatial listening, the barn owl. Proving it in humans was harder as it was more difficult to show the process in action in the human brain, he said.
“We like to think that our brains must be far more advanced than other animals in every way, but that is just hubris,” he said. “It was clear to me that this was a function that didn’t require an over-engineered brain because animals come in all shapes and sizes.
“It was always going to be the case that humans would use a similar neural system to other animals for spatial listening, one that had evolved to be energy-efficient and adaptable.”
COCHLEAR ACQUIRES OTICON MEDICAL BUSINESS
Cochlear Limited has acquired Oticon Medical cochlear implant business from Danish-headquartered hearing health company Demant.
An ASX announcement on 21 May 2024 said all required conditionality had been satisfied and Cochlear would support the hearing health outcomes of 20,000 people with Oticon Medical cochlear implants.
The statement said the acquired cochlear implant business would be integrated into Cochlear over the next few months. It said that following Demant’s decision to discontinue its efforts in hearing implants, Cochlear had acquired Demant’s cochlear implant business for a zero headline purchase price.
Cochlear’s CEO and president Mr Dig Howitt said: “We welcome Oticon Medical’s cochlear implant customers to Cochlear and remain committed to supporting the long-term hearing outcomes of these 20,000 patients.
“Customers are our priority as we work closely with Demant for a smooth transition.
“Driven by our mission to innovate and deliver a lifetime of hearing outcomes, we will seek to provide Oticon Medical’s cochlear implant customers continued support with a lifetime of hearing solutions.
“We will develop and commercialise next generation sound processors and services to enable the vast majority of customers to transition to Cochlear’s technology platform over time. We will also support customers with continued access to repairs and replacements of current Oticon Medical cochlear implant technology for as long as feasible.”
Cochlear said it expected to incur integration costs in the 2024 financial year of about $30 million pre-tax, primarily related to restructuring. This amount would be reported as a non-recurring significant item, with no impact on Cochlear’s 2024 financial year underlying net profit guidance of $385 million to $400 million. Earlier it was reported Oticon Medical was expected to add $75 million to $80 million to Cochlear's annual revenue.
SPECSAVERS AUDIOLOGY NETWORK SURPASSES 300
Specsavers has opened its 300th audiology store, in a milestone the company says signifies its commitment to making expert hearing solutions more accessible to communities nationwide.
Specsavers Leopold opened in Geelong, Victoria, in late February 2024 in time to offer free 15-minute hearing checks during Hearing Awareness Week.
Audiology professional Ms Lesley Thyssen said her team was excited to open its doors to the local community.
“We look forward to assisting people to connect and thrive through improved hearing health. The satisfaction we get when a customer has a dramatic improvement in their lives and ability to communicate is what I love most about my job," she said.
“There’s fantastic new technology which keeps getting better every day and it’s great to be able to help a large segment of the population.”
Specsavers managing director of audiology Australia and New Zealand, Mr
Tom Craw, said the new offering gave a more accessible solution to hearing loss by providing Specsavers’ well-known clear, low prices and expert service.
“The meaning of Hearing Awareness Week is to highlight the importance of adequate hearing care for all and we’re working to do just that by continuing to open stores in locations for our customers,” he said.
“Audiology is now available in 300 stores, so even more Australians can access quality hearing care at an affordable price.
Specsavers Audiology genuinely cares about its customers’ hearing health and access to fair and affordable hearing care.
‘‘Early detection can make a significant difference.”
Specsavers Audiology is accredited as a qualified hearing service provider by the Australian Government Hearing Services Program. It offers comprehensive hearing assessments for $49 and various hearing aids by leading manufacturers. A pair of hearing aids at Specsavers starts at $1,495.
HEARING AIDS WITH ARTIFICIAL INTELLIGENCE IMPROVE HEARING
Starkey Australia has launched on the national market a new hearing technology system using artificial intelligence to improve the experience of those with hearing loss.
The company says its Genesis AI system provides optimal hearing for any listening situation, enabling wearers to hear soft sounds and distinguish words and speech more naturally while significantly reducing their listening effort.
It says the hearing aids process sound the way a ‘normal’ auditory system does, filling in the gaps produced from years of hearing loss. Starkey says Genesis AI feature the industry’s smallest and most powerful processor that operates up to four times faster than predecessors with six times more transistors, to create better sound quality.
provide the best hearing experience for hearing aid wearers.
Starkey’s chief technology officer and executive vice president of engineering, Mr Achin Bhowmik explained: “By tapping into advanced technology, sensors, machine learning and artificial intelligence, Starkey Australia has reinvented the hearing aid to
“Our all-new, powerful processor was designed to work like the human brain, leveraging the neuroscience of the ear-brain connection and information processing to create better sound quality, pushing energy-efficient artificial intelligence to its limits, analysing and automatically optimising sound over 80 million times an hour.”
Specsavers managing director of audiology ANZ Tom Craw.
Genesis AI makes more than 80 million automatic adjustments an hour. Image: Starkey Australia.
Cochlear CEO and president Dig Howitt. Image: Hearing Australia.
PARTNERSHIP TO COMBAT HEARING LOSS
A new partnership between Ear Science Institute Australia (ESIA) and the National Acoustic Laboratories (NAL) will bring hearing researchers from across Australia together to improve treatments for people with hearing issues.
The partnership, announced 2 May 2024, represents a collaboration of nearly 100 years of combined expertise in research, innovation and hearing healthcare.
“This powerful partnership with the Ear Science Institute Australia brings together many of the brightest and most ambitious hearing researchers in Australia, all with the shared vision of having a significant impact on hearing healthcare to improve the lives of people with hearing difficulty everywhere,” said Dr Brent Edwards PhD, NAL director.
VIC STUDY MAY PAVE WAY FOR LOCAL GENE THERAPY
A Melbourne study is recruiting Australians with auditory neuropathy to undergo genetic testing which could lead to gene therapy in Australia for this and potentially other forms of hearing loss and deafness.
Based on reports from China, the US, and the UK, gene therapy in clinical trials has restored hearing in several children who were born with profound hearing loss due to variations in the otoferlin gene (OTOF) which produces the protein otoferlin, needed to allow inner hair cells in the ear to communicate with the hearing nerve (see page 24).
The Australian study is part of a five-year international study sponsored by US company Akouos Inc, a wholly owned subsidiary of Eli Lilly and Company, which sponsors one of the US trials. Principal investigator of the Australian study site, Associate Professor Valerie Sung, said the natural history study is in children and adults with the same form of auditory neuropathy deafness in both ears.
“Just over a dozen Victorian children have had the genetic test and many are still in progress but none have been positive for the variant. We’re recruiting anyone born after 1980 with auditory neuropathy in both ears, Australia wide.”
The study is a collaboration between the Murdoch Children’s Research Institute (MCRI), The Royal Children’s Hospital (RCH) and The University of Melbourne. A/Prof Sung is a consultant paediatrician at the hospital, Senior Research Fellow at the MCRI and Honorary Clinical Associate Professor in the university’s Department of Paediatrics.
“One in 10 children with permanent hearing loss have auditory neuropathy and there’s a genetic basis underlying moderate to profound hearing loss in more than half of deaf and hard of hearing children but we don’t know how often genetic variants cause auditory neuropathy,” she said.
NAL is a world-renowned hearing research organisation involved in evidence-based innovation to improve hearing health for more than 75 years. Funded by the Australian Government, it is based at the Australian Hearing Hub, Macquarie University, Sydney, and was the team behind the first hearing aid in Australia.
Ear Science Institute is a globally recognised for-purpose organisation in Perth and a centre of excellence that aligns hearing science, medicine, and clinical teams to develop innovative treatments for ear and hearing disorders, with the goal of eventually finding a cure for hearing loss.
“As we look towards the next era in hearing treatment, this meaningful partnership with National Acoustic Laboratories will bring new opportunities for knowledge sharing, leading to improved access, advanced solutions and better individual hearing care for people everywhere,” said Associate Professor Sandra Bellekom, Ear Science Institute CEO.
Dr David Sly, the institute’s chief operating officer, added: “One of the first endeavours as a team is to diagnose and treat people with hidden hearing loss, a frustrating condition where a person has trouble hearing but their tests show normal results. Sounds can be heard but conversations not understood.”
“Participants will learn whether they have a variation in the OTOF gene that could be an eligible target for gene therapy,” she told Hearing Practitioner Australia. “Our study is not linked to gene therapy trials but aims to understand what happens to hearing loss level, quality and function over time for people with OTOF-mediated auditory neuropathy.
A/Prof Sung said participants would first have a genetic counselling appointment via telehealth or in person at the hospital to determine whether genetic testing was the right choice for them and their family. A saliva testing kit could be posted and the sample returned by mail. There is no cost to patients, their insurance or their healthcare providers. Hearing practitioners can refer patients to the study via hearing.research@rch.org.au
HOPES DRUG CAN REDUCE LOSS OF RESIDUAL HEARING IN CI PATIENTS
A biotechnology company will trial giving its new investigational drug to cochlear implant recipients to see if it reduces loss of residual hearing during and after cochlear implantation (CI).
Sound Pharmaceuticals (SPI) is a private company focused on developing the first drug treatment for hearing loss and tinnitus in the US. It announced 22 May 2024 FDA notification that its Investigational New Drug Application (IND) may proceed involving SPI-1005 treatment (ebselen) and cochlear implantation.
Sound Pharmaceuticals said ebselen was a novel anti-inflammatory compound that mimics and induces the activity of Glutahione Peroxidase, an enzyme critical to hearing and balance.
“Ebselen has shown safety and
efficacy in three different forms of acquired sensorineural hearing loss in adult patients, including loud sound exposure or acute noise induced hearing loss, Meniere’s disease, and antibiotic or aminoglycoside induced ototoxicity,” SPI said.
“The goal of this phase 2 trial is to reduce the loss of residual hearing during and after CI.”
The trial will enrol 40 adult CI candidates scheduled to receive a cochlear implant who have residual low frequency hearing that is moderate to severely impaired and at risk of being lost after implantation. SPI is collaborating with MED-EL. The companies entered an exclusive worldwide collaborative agreement involving the use of SPI-1005 with cochlear implants.
A/Prof Valerie Sung from Murdoch Children’s Research Institute. Image: MCRI.
An anechoic chamber at the Australian Hearing Hub and National Acoustic Laboratories (NAL). Image: NAL.
The trial will enrol 40 adult CI candidates. Image: Peakstock/ stock.adobe.com.
The Australian College of Audiology (ACAud) and the Hearing Aid Audiology Society of Australia (HAASA) – two of Australia’s three professional accrediting bodies for hearing practitioners – are merging to form a stronger organisation for enhanced advocacy, member support and client services.
In what’s being described as a major boost for the future of audiometry nationwide, the organisations announced on 13 March 2024 they would amalgamate to become the Australian College of Audiology incorporating Hearing Aid Audiology Society of Australia.
ACAud incorporating HAASA will be the initial trading name but further name development and branding consultation will occur.
ACAud CEO Ms Jane Hedger, who has since left the role, told Hearing Practitioner Australia (HPA) that HAASA’s 130 audiometrist members were being moved into the ACAud database of 875, creating an organisation of 1,005 members.
She said three-quarters of ACAud members were audiometrists and the rest audiologists but in the real world, both professions worked side-by-side, so it made sense to have a professional body representing both.
“It’s about looking at the sector as a whole and how two smaller organisations can be stronger and create more advocacy for members and better services for clients,” Hedger said. “The sector needs to be advocated for and should be raising everyone up with the ultimate aim of clients receiving a better service closer to where they live.
“We all need to prepare for massive change
in healthcare and the hearing sector as technology and artificial intelligence shape the future, along with clinical shortages as the population ages.”
She continued: “The whole point of merging is to ensure we can continue to provide clients with safe, accessible and clinically appropriate services. There will be lots of challenges but with our combined membership, we can tackle them together.
“Another driver for coming together was that we can better advocate for both professions, particularly around greater inclusion of audiometrists.”
HAASA board director, NSW audiometrist Mr Chris Harrison, told HPA that feedback from the society’s members about the merger had been mostly positive.
“We see it as a positive for the industry – one voice for audiometrists means power behind our numbers, and it’s great for the future of audiometry as one voice empowers advocacy,” he said. “It’s been a long time coming and will strengthen the profession, for example when advocating for improved TAFE training, we can advocate for a plan nationwide.”
The merger would also minimise costs of having two bodies and boost continuing professional development as HAASA had led the way with two events annually, he said. The new board would also grow the education program, providing more opportunities for members and a richer variety of events.
A joint-statement on both websites said the organisations were excited about the move.
“This union represents a strong and strategic partnership to better serve and protect members, improve educational pathways, grow the workforce, and advocate for all hearing health clinicians,” it stated. “Both organisations have recognised the need for greater infrastructure and resources in the face of a rapidly changing sector.
“With a shared vision for empowering and acknowledging the important role that audiometrists and audiologists play, we embark on this journey together to ensure sustainable growth and robust advocacy for our valued members.”
Boards decided to merge ‘in members’ best interests.'
Both bodies notified members in emails and the website statement which included FAQs.
HAASA members were also advised at a continuing education program day on 15 March 2024.
While members were not consulted in the decision-making process, the boards “made the decision in the best interests of ensuring our members could be supported and protected into the future”, with benefits including a broader range of professional development opportunities, enhanced advocacy and a larger, more diverse network of professionals.
“We felt there was no benefit to be obtained in a protracted public discussion,’’ they stated. “Our boards have worked together to conduct this process with optimism for our shared future and the difference we can make for members and Australians living with hearing difficulties.”
ACAud and HAASA boards at a recent meeting. Image: ACAud.
Eye and Ear hospital’s $317 million redevelopment
The recently-completed revamp of Australia’s only eye, ear, nose, and throat hospital has delivered major upgrades to the 161-year-old facility.
The Royal Victorian Eye and Ear Hospital’s world class redevelopment of facilities for care, treatment and research has officially opened, with capacity to treat an additional 7,000 patients each year.
Ear and hearing care are an important part of what the hospital delivers, seeing more than 11,000 patients annually in its otology specialist clinics and cochlear implant specialist clinics.
Victorian Minister for Health and Health Infrastructure, Ms Mary-Anne Thomas, officiated at the opening on 23 April 2024 of the upgraded world class specialist health, research and education facility, unveiling a plaque commemorating the occasion.
“The Royal Victorian Eye and Ear Hospital has a long history of delivering world-renowned care, treatment and research – this redevelopment will help staff continue this groundbreaking work,” Thomas said.
“More Victorians will now be able to get the specialist eye and ear, nose and throat public health care they need with the hospital upgrade expanding its capacity to treat an additional 7,000 patients each year.”
The state-of-the-art upgrade boasts a new 13-cubicle 24-hour emergency department (ED), ED Short Stay Unit with four 24-hour beds, perioperative suite with eight upgraded operating theatres and 14 recovery spaces, as well as a further 37 same-day beds and 42 consulting rooms.
There is an additional inpatient ward with 24 beds, and a dedicated floor for clinics, offering more than 90 specialist services.
Improved teaching, training and research facilities are now on upper levels, with patient services located on the first three floors of the buildings to improve navigation across the hospital.
The redevelopment also delivered a new Central Sterile Services Department and a full upgrade of the hospital’s engineering infrastructure and central plant, making the hospital safer and more efficient.
Thomas revealed the Victorian Government invested $144.7 million toward the project, with the Commonwealth providing $100 million, and the hospital an additional $72.9 million.
More than 41,000 ENT presentations
The hospital provided more than 192,000 episodes of care in 2022-2023, which included over 136,000 specialist clinic appointments, 42,371 emergency attendances and more than 14,000 inpatient admissions.
More than 41,000 patients attended the hospital for ear, nose and
“Doctors from all over the world come to train at the hospital in ophthalmology and otolaryngology, to learn from leaders in the industry and colleagues, renowned here and internationally.”
A/Prof Penelope Allen Head of the Eye and Ear’s Vitreoretinal Surgical Unit.
throat conditions in 2022-2023 including 13,829 emergency department presentations, 1,789 inpatient admissions and 25,523 seen in specialist clinics. This included 5,370 patients at otology specialist clinics and 5,927 at cochlear implant specialist clinics.
The hospital’s CEO Mr Brendon Gardner said he looked forward to seeing the positive impact the redeveloped hospital would have on metropolitan, regional and rural patients.
“As Australia’s only eye, ear, nose, and throat hospital, today signifies a new chapter in our 161-year history,” he said. “As Victoria’s third oldest public hospital, our specialist knowledge and expertise position us well to continue to provide the best care for Victorians over the next 160 years and beyond.”
Established in 1863, The Eye and Ear was instrumental in developing the world-leading bionic ear, which later became the groundbreaking cochlear implant. It is Victoria’s leading provider of eye and ear health, integrating clinical care, research and education to optimise innovation and provide advanced treatments for vision and hearing loss.
“The Eye and Ear was built on three pillars; care, training and research,” said Associate Professor Penelope Allen, head of the Eye and Ear’s Vitreoretinal Surgical Unit.
“What is most profound to me is that we are all still upholding these principles today. Doctors from all over the world come to train at the hospital in ophthalmology and otolaryngology, to learn from leaders in the industry and colleagues, renowned here and internationally.”
The redevelopment supported 2,500 local jobs throughout the project.
Image: Leo Farrell.
Image: The Royal Victorian Eye and Ear Hospital.
The Eye and Ear’s rich history of saving and enhancing the lives of millions of patients is acknowledged and celebrated in the history wall in the main hospital foyer which was designed by Fitzroy-based designers Arterial.
At the official opening, director of surgical services Sinead Cucanic (from left), board of directors chair Dr Sherene Devanesen, ophthalmologist Dr Jaqueline Beltz, University of Melbourne Professor of Otolaryngology Stephen O’Leary, Health Minister Mary-Anne Thomas, CERA managing director Prof Keith Martin, and Eye and Ear CEO Brendon Gardner.
The perfect alignment
Melbourne audiologist NEELIMA YADLAPALLI shares why she chose Specsavers Audiology to take her career to new heights as a business partner and why it aligns with her ethics and ambitions.
Starting your own practice as a health professional while in your 20s would be daunting for many. But Melbourne audiologist, Ms Neelima Yadlapalli, has achieved this accomplishment by becoming a Specsavers audiology partner in two clinics, and all before her 30th birthday.
Yadlapalli says she never would have been able to afford to set up an independent practice at this age or had enough business acumen to deal with the practicalities of establishing and operating a business.
“At 29, I definitely would not have been able to afford to go into business by myself – it’s a huge outlay if you do it on your own,” she says. “The amount of work involved in doing your own marketing, financial planning and forward thinking, I would have struggled by myself.”
However, the financial and practical backing of Specsavers came to the rescue of the enthusiastic practitioner, helping her make a smooth transition to business owner. Today, she is a Specsavers audiology partner and director in two audiology practices based in northern Melbourne optometry stores at Preston and Northcote shopping centres.
“I love the autonomy and knowing that I’m working in a practice where I can provide the best value to my customers and see the benefit of good hearing in their lives. Specsavers just aligns with my ethics,” Yadlapalli says. “It’s so rewarding, and my husband who works in IT is jealous because I get to see first-hand the benefits of what I do every day.”
Yadlapalli’s pathway to the hearing industry began with a fascination for science, leading to majors in genetics and pharmacology at The University of Melbourne.
“I enjoyed science but wanted the people aspect,” she recalls. “I realised working in the lab was not for me and I was lucky to find audiology which encompassed everything that was interesting to me.”
After graduating in 2012, she worked for a corporate network in Frankston.
“I discovered the satisfaction of helping people hear better, conducting hearing tests and fitting hearing aids and I was humbled by the impact I could have on people’s quality-of-life,” she says.
She worked there until 2018 practising in the clinic one day a week to keep up her skills and working as a state trainer for Victoria and Tasmania, another role she found rewarding. This included training graduates and audiologists in various aspects of clinic life.
“It was dynamic, I had to be adaptable, and each day was different,” she recalls. “I enjoyed connecting with my peers, seeing them grow and upskill. It was a fantastic experience that allowed me to make a positive impact on others’ careers and patient care.”
Innovative approach
But after six years, she yearned to practise full time and, as luck would have it, this was around the same time as Specsavers Audiology was entering the Australian market (2017).
“That was where my true passion lay and I was really drawn to Specsavers – it had such an innovative approach and marketing strategies, and I knew they would disrupt our hearing aid industry,” Yadlapalli recalls. “My intuition told me Specsavers was poised to revolutionise the industry, and I wanted to align myself with a forward-thinking organisation.
“The prospect of owning my own clinic with the support and autonomy that Specsavers offered was a signature drawcard for me.”
As a director she bought shares in the business, which was not expensive as it was new.
“The process was quite straightforward. I came in and the clinics, the equipment, everything was set up for me. At both sites, I had a soundproof room including a soundproof booth for hearing tests and heavier doors to keep things quieter, and Specsavers paid for these.
“The set-up fees are taken out over a five-year loan from revenue
Images: Specsavers.
Neelima Yadlapalli says the biggest benefit of the partnership structure is the financial stability and reduced business risk.
“I love the autonomy and knowing that I’m working in a practice where I can provide the best value to my customers and see the benefit of good hearing in their lives. Specsavers just aligns with my ethics"
Neelima Yadlapalli Specsavers Audiology partner
generated which is negligible, about $1,500 a month, and spread out so you don’t notice it.
“But it didn’t take long, six to 12 months, before I started to make dividends. Although I was surprised at how quickly it happened, I also believed it would work. We’ve grown immensely in the past six years –about 30% last year – and I’m now looking at hiring another audiologist. This is a culmination of coming out of COVID, the good work I’ve been doing, word of mouth and Specsavers marketing.”
Financial stability, best outcomes, value and service
Yadlapalli says the biggest benefit of the partnership structure is the financial stability and reduced business risk. As an audiologist she was previously unaware of the costs involved in running a business.
“But the support and resources from Specsavers have not only opened my eyes to these costs but enabled me to manage them effectively,” she says.
“The other big advantage is having the backing of the major hearing aid brands and being able to provide them at a very reasonable cost compared to competitors. This has given me the confidence as an audiologist that I am fitting products which will give the best outcomes, value, and service for my patients because the buying power that Specsavers has means I can give a better hearing aid at a reduced price.”
Yadlapalli says one example is that while $10,000 might be charged by competitors for a top of the range hearing aid, she can provide the same device to patients from $3,500 or from $1,900 for Hearing Services Program funded customers.
“Because we provide this reduced price, most people are more
accepting of going for the top of the range model to meet their needs as they’re not as worried about the financial costs and they receive much better outcomes than if they had gone for a lower priced, lower-level hearing aid which they might have struggled with,” she adds.
People are starting to shop around now and they’re the ones who benefit most, she says.
Optometry benefits
A key feature of the Specsavers audiology model is the co-habitation with pre-existing optometry practices. Advantages of this include sharing rent and front-of-house staff costs but she says the greatest benefit is the optometry database which enables staff to suggest patients who might benefit from a hearing test.
“Optometry has such a large database and working in a trusted store with a vast customer database has been a game-changer. It’s enabled me to reach a broader patient base. Patients have also expressed their appreciation for the one-stop-shop experience, where they can address both their eye and ear concerns.”
Another benefit is the opportunity to not talk about ears the whole day. “It’s been nice to work alongside another profession.
‘‘A lot prefer back-to-back appointments for eyes and ears but sometimes if they are diabetic, for example, the eye appointment might go longer so they return another day for ears. Having both in one store, and often easy access in shopping centres where many of our stores are, means patients are already building rapport with the store so are comfortable to come back and see us for hearing.”
Her advice to graduates and established audiologists who might be considering Specsavers but feel nervous or unsure is to “come and speak to one of us to see if their values and views align with ours”.
“There’s so many of us running Specsavers businesses now, it’s not unchartered territory anymore,” she says. “It’s a great place to work and our stores are like a small business, owned and run by optical directors. There’s always someone in the business who oversees day-to-day activities and strives to do their best by customers and staff. It fosters a nice close working environment and we’re like little families in each store.”
Front-of-house staff upskill to assist audiology patients and help with bookings. In her clinics, the plan is to train them to do basic repairs of hearing aids so when she is not there at weekends they can assist patients. When optometry patients aged 50 and over come in, reception staff offer a hearing questionnaire and hearing screening on iPads while they are waiting. iPads have been a great tool to generate awareness, she says..
“Many patients say they’ve never had a hearing test before and had no idea where to go,” Yadlapalli explains.
While many come from the optometry database and iPad checks, a good proportion also come from marketing and word-of-mouth. The audiology business also refers patients to its optometry colleagues, with patients often saying while they are there, they may as well have their eyes examined too.
“In six years, there has been a lot of sharing of customers. I’m a big believer in treating each customer like gold and this has never led me astray. I never miss an opportunity to do my best which has helped my business.”
Neelima Yadlapalli with practice staff.
Why patients and practitioners are embracing Specsavers
When audiologist Mr Nick Taylor came from England to Australia to help establish Specsavers Audiology, he was confident the model would take off, based on success overseas. His predictions were correct –with both the Australian public embracing it and more than 300 audiology professionals joining the Specsavers brand as joint venture partners in its opening years.
“It’s been very successful; we’ve screened 3.3 million Australians over six and a half years, which is, I believe, the most hearing screenings anywhere in the world, something we’re very proud of,” Taylor says. “About 40% are found to have hearing loss.”
The model of incorporating audiology practices within Specsavers optometry stores has paid off with about 60% of audiology consults coming from in-store optometry patients aged 50 and over who do a three-minute hearing screen as part of their eye and ear health check before seeing the optometrist. If this indicates potential hearing issues, the customer is offered an appointment with an audiology professional to discuss their results and any further steps needed.
Taylor, chief audiology officer for Specsavers Australia New Zealand, says because of its optics business, about 6.5 million Australians come into Specsavers stores every couple of years, creating a stream of potential customers whose demographic fits the most common patient type requiring hearing care – those over 50 – and the adult demographic Specsavers focuses on.
“This allows us to access many people to promote hearing health,” he says.
“Because we have so many customers coming into our stores, we don’t have KPIs or sales targets for our partners. Instead, we base everything on the Specsavers’ key value of providing accessible and affordable health care to all.
‘‘Our clinicians not having corporate pressure as to why they didn’t make targets or sales is an important reason why many join Specsavers. H istory shows that this model works very well with many businesses becoming profitable within a few months of operation.”
Clinicians’ expertise is largely in clinical practice but to back this up, the company provides a full suite of operations support including looking after marketing, finance and procurement for all Specsavers Audiology businesses.
“As we’re the nation’s only franchise-based audiology business, we give clinicians the ability to own their own business with support of a fantastic, big, well-known brand that provides those other skills and expertise,” Taylor adds.
Apart from clinical education that Specsavers also offers – and buying power enabling reduced prices – it provides a mentoring program for early career audiology professionals to support them
through their career journey including the possibility of becoming future business owners.
Doing the right thing by customers
Taylor says the principle of doing the right thing by the customer is the tone optometrists and Specsavers founders Mr Doug Perkins and Dame Mary Perkins set when they founded the company 40 years ago. In addition to a passion to make eyecare more affordable, they wanted to include other healthcare services.
Audiology was a natural partner.
“Our customers choose Specsavers for our amazing value, professionalism, customer service, and of course, convenience. They don’t see Specsavers optometry and Specsavers audiology, they just come in and see Specsavers eyes and ears together,” Taylor explains.
The audiology business was launched 20 years ago in the UK and now operates across Australia, New Zealand, the UK and Northern Europe.
Taylor joined Specsavers UK business in 2012, where he headed audiology training and professional services.
“It appealed to me the way Specsavers operates, with millions who have hearing difficulties who can’t access hearing care, plans that Specsavers put in place to address that on a large scale was the biggest attraction.”
Invited to be part of the launch team for Australia and New Zealand in 2017, he has been head of audiology’s professional services and product ever since.
“Developments in hearing aid technology have been fabulous and part of my role is to make sure our partners have great products to offer customers,” he explains.
“We passionately believe in clear and transparent pricing. Prices are on our website and in our stores and we want people to shop around and do their research because we’re confident when they do, they’ll see the amazing value Specsavers offers. We also offer a wide variety of prices and technology levels.”
The goal is to have audiology in all its optometry stores – currently just under 400.
“Whether you’re a great audiologist or audiometrist, you can be a business owner or an employee in our audiology stores,” Taylor says. “We’re proud that Specsavers has been listed as a ‘great place to work’ for the past three years by Great Place to Work, a global authority on workplace culture, and in 2023 was named as one of Australia’s top 10 best workplaces. To be recognised as a company built on great people is fantastic.
“There’s nothing more important in a business than the people who work there and, as Richard Branson said, the way you treat your employees will be reflected in the way they treat their customers.”
Audiologist and optometrist Lachlan Smith performing a hearing test at his Camberwell junction practice, Smith Eye and Ear Solutions.
Eye and earpractitioner looking out for his patients
Practising two different health disciplines in his daily life makes LACHLAN SMITH’s career doubly interesting. He gives an insight into how this happened and why it works.
Dual qualifications in audiology and optometry not only make Mr Lachlan Smith unique in Australia but are a huge bonus for his patients.
The multi-skilled audiologist and optometrist estimates that one in four of his patients see him for both eye and ear conditions at his two Melbourne clinics. For elderly patients, particularly, the convenience of being able to see the same practitioner in the same clinic and often on the same day for vision and hearing problems, cannot be underestimated.
Hearing and vision work together and are processed by the brain to provide a total perception of the environment. Smith’s dual disciplines also work in synergy to provide comprehensive services through Smith Eye and Ear Solutions, located in Camberwell Junction and Moonee Ponds.
“Audiology and optometry complement each other,” he says. “It’s very convenient and some of the presentations go hand in hand. If you’re going to complement certain disciplines, this would be the way to do it.
“You don’t need a lot of physical space for audiology so that’s also beneficial.”
While some corporate networks are bringing audiology and optometry under the one roof, Smith says that, as far as he knows, he is the only practitioner in Australia who is qualified as and working as both an audiologist and an optometrist.
Often patients have been a loyal optometry patient, and have developed trust and rapport with him, making for a seamless transition to audiology client. The convenience of a one-stop-shop is valuable and sought after.
The same can be said for his Indigenous patients in remote north-west Queensland. Smith flies to Mornington Island every month to spend a week running eye and ear clinics. Patients include young children with otitis media that can interfere with learning, speech and socialisation, and older patients with hearing damaged from repeated ear infections when they were younger.
This remote work is funded by the Queensland Government which covers the cost of his visits.
Residents often need to travel distances for appointments so the convenience of having a health professional who can examine and treat eye and ear conditions simultaneously at one appointment is a rarity and a windfall for the area.
It’s also difficult for remote communities to attract health professionals, making the dual qualification a bonus.
Smith began the visits through Gidgee Healing, an Aboriginal Medical Centre based in Mount Isa, in 2020 and did them full time for about eight months including during the pandemic before continuing post-pandemic on a part-time basis.
“It’s hard to get patients to come in because of the lack of transport so when they do, if you offer both disciplines and follow-up on referrals, that’s where it’s most beneficial,” he explains. “Sometimes basic stuff is missed through administration errors or just not followed up, so it’s great to be able to pick that up.”
Grandfather’s war-related hearing loss
Smith became an audiologist first before becoming an optometrist. The journey started as a child due to his grandfather’s severe hearing loss triggered by noise exposure during the Second World War.
“It was back in the day when hearing aids weren’t much help,’’ he recalls. “I was around hearing loss a bit as my grandfather introduced me to it. I was looking for something a bit different for a career and had that exposure and it kind of fell into place.”
Smith graduated in audiology from the University of Queensland in 2011 and worked in Cairns for about 18 months for Amplifon before moving home to Melbourne.
In 2013 he opened an audiology clinic in his father Anthony Smith’s Moonee Ponds optometry practice. Smith believes this was Melbourne’s, and Australia’s, first clinic to combine the disciplines at a primary care level.
His father had bought the Moonee Ponds practice in 1996, and previously in 1979 a Camberwell optometry practice, founded by Mr Frank Slade in 1928.
“When I rented a room in Dad’s optometry clinic, Dad was cutting back towards retirement so only working part-time and I was working part-time in
Images: Lachlan Smith.
Providing a valuable service for the local children on a remote island.
audiology,” Smith recalls. During this time, he realised he wanted to also be an optometrist so began studying the qualification at Deakin University, and combined with audiology consulting, this was a hectic period.
“I was among the first to graduate from optometry at Deakin and also among the oldest,” he says. “I think the other graduates thought it was a bit peculiar that I was still studying and what-not being one of the oldest in the cohort.
“Dad came to me with the idea for the dual clinic as he knew Boots and Specsavers in the UK had successfully integrated both services into one business, so it was not completely unprecedented.
"Dad’s clinic was well-established and had a loyal patient base, so we thought it could work well.”
After his father retired, Smith bought the business and it remains a family affair with his optometrist sister, Mrs Hayley Stewart, also working part time in both practices. Their father also continues to do some work there too.
Medical, pathology, counselling and rehab
When asked which he enjoys the most, the answer is, not surprisingly, both. Like most optometrists nowadays, Smith is therapeutically endorsed, so he can diagnose, treat and help manage eye-related medical conditions including age-related macular degeneration (AMD), glaucoma and diabetic retinopathy.
Studies have coincidentally shown a strong association between hearing loss and age-related eye conditions such as cataracts and AMD, suggesting common risk factors for both.
“Although optometry and audiology do complement each other, they’re very different,” Smith explains. “There’s more of a medical and pathology base in optometry, whereas there’s more counselling, handholding, and rehabilitation in audiology, which means audiology consults generally take longer.
“In audiology you might see the same person four to six times (close together for example) whereas in optometry, you probably see them once then not again for a while.”
Advantages of two clinical offerings
As Mr Steven Ross, then business development manager of hearing care solutions company, Sonova, told a large optical event in the UK in 2018, optometry and audiology are a good fit.
“The reason optometry and audiology should meet is because they share the same customer base: 97% of over 65-year-olds need some form of vision correction; 73% of 70-year-olds need some form of hearing correction,” Ross told Optometry Today
“If you’ve already got the premises, you’ve got the front-of-house staff, you’ve already got the customers. One of the hard things is to get a
many people over 55 for both consultation types.
“If they’re having an optometry consult and it’s obvious they have a hearing problem, I mention I can do a hearing test, and alternatively if they’re asking leading questions about their eyes during an audiology consult, I suggest having an optometry consult,” he adds.
Other advantages of combining the two clinical offerings include sharing bookings systems, administration and costs.
Hearing aids are custom-made, so no extra storage or financial outlay is needed for stock. Audiology rooms don’t have to be soundproofed although they must be sound treated to an overall ISO calibration standard.
Smith does not find it difficult to swap hats.
“You get used to it and see patients in different rooms, each set up with different equipment," he says.
"It takes a lot of time, effort and money but once it’s set up, it works well."
L-R, a family affair, Hayley Stewart, her father Anthony Smith and brother Lachlan Smith all work in the same practices.
The children of Mornington Island also benefit from Lachlan Smith’s optometry services.
Addressing the root of genetic deafness
Gene therapy is the new frontier in medicine, and the hearing sector is at the forefront. Trials have begun for people born with certain types of deafness, and more are on the way, offering the potential for one-off treatments that can change lives.
In May 2024, a toddler from the UK who was born with profound genetic deafness made headlines around the world when news broke that a pioneering gene therapy had restored hearing in her treated ear. Doctors said the therapy resulted in “dramatically improved hearing to normal levels”.
The American conference where the results were reported also heard that gene therapy had restored hearing in other children in China and the US, marking “a new era in deafness treatment”.
Results from the various trials were released on 8 May 2024 at the 27th annual meeting of the American Society of Gene and Cell Therapy where French company Sensorion also announced it would begin trials of its gene therapy for deafness in 2024.
Six months after a single intracochlear injection delivered via a one-off infusion into British girl Opal Sandy’s right ear, her hearing had “improved close to normal hearing levels” in the treated ear, doctors said.
At 11 months of age, she was among the world’s youngest to receive the therapy after being born with auditory neuropathy due to a variation in the otoferlin gene (OTOF) which produces the protein otoferlin, needed to allow inner hair cells in the ear to communicate with the hearing nerve. Opal is taking part in the CHORD trial by Regeneron Pharmaceuticals which aims to determine if the investigational gene therapy DB-OTO can provide hearing for children born with this condition. Regeneron released
initial results at the American conference.
It said results showed “dramatically improved hearing to normal levels” in Opal and initial hearing improvements in another child aged four at a six-week assessment. The ongoing trial is enrolling children in the UK, US and Europe.
Clinicians said they noticed continuous improvement in Opal’s hearing in the weeks after treatment and at 24 weeks post-therapy confirmed close to normal hearing levels for soft sounds, such as whispering, in her treated ear. Now 18 months old, she can respond to her parents’ voices and say some words.
Spectacular results
Professor Manohar Bance, chief investigator of the British trial and ear surgeon at Cambridge University Hospitals NHS Foundation Trust, said in a statement: “These results are spectacular and better than I expected. Gene therapy has been the future in otology and audiology for many years and I’m so excited that it is now finally here. This is hopefully the start of a new era for gene therapies for the inner ear and many types of hearing loss.”
Opal received an infusion containing a harmless virus (AAV1) which delivered a working copy of the OTOF gene via injection in the cochlea of her right ear during surgery. In the same surgery, at Addenbrooke’s Hospital in Cambridge, a cochlear implant was fitted in her left ear.
Prof Bance explained the therapy helps hair cells regrow. He said children with a variation in the OTOF gene often passed newborn screening, as the hair cells were working, but not talking to the nerve. It meant this hearing loss was not commonly detected until children were two or three years of age – when a delay in speech was likely to be noticed.
He added: “We have a short time frame to intervene because of the rapid pace of brain development at this age. Delays in diagnosis can cause confusion for families as the many reasons for delayed speech and late intervention can impact a child’s development.
“More than 60 years after the cochlear implant was first invented –the standard of care treatment for patients with OTOF related hearing loss – this trial shows gene therapy could provide a future alternative. It marks a new era in the treatment for deafness. It also supports the development of other gene therapies that may make a difference in other genetic related hearing conditions, many of which are more common than auditory neuropathy.”
Opal’s mother Mrs Jo Sandy said: “When Opal could first hear us clapping unaided it was mind-blowing – we were so happy when the clinical team confirmed at 24 weeks that her hearing was also picking up softer sounds and speech. The phrase ‘near normal’ hearing was used and everyone was so excited that such amazing results had been achieved.”
speech sounds. It’s already making a difference to our day-to-day lives
British baby Opal with parents Jo and James Sandy.
Images: Cambridge University Hospitals NHS Trust.
Paediatrician Dr Richard Brown.
“These results are spectacular and better than I expected. This is hopefully the start of a new era for gene therapies for the inner ear and many types of hearing loss.”
Prof Manohar Bance Ear surgeon
like at bath-time or swimming when Opal can’t wear her cochlear implant. We feel so proud to have contributed to such pivotal findings, which will hopefully help other children and their families in the future.”
Dr Richard Brown, CUH consultant paediatrician and investigator on the CHORD trial added: “It is likely that in the long run such treatments require less follow up so may prove to be an attractive option, including within the developing world. Follow up appointments have shown effective results so far with no adverse reactions and it is exciting to see results to date.”
Follow up will continue for five years to show how patients adapt to understand speech.
Addressing root cause
Medical School, USA, concluded the therapy was safe and efficacious.
Otolaryngology Associate Professor Zheng-Yi Chen of Massachusetts Eye and Ear Infirmary and Harvard said FDA approval of the therapy could be three to five years away.
Clinical trial investigator, Dr Lawrence Lustig, chair of Columbia University’s Department of Otolaryngology – Head and Neck Surgery, presented results from the British children at the conference, saying the opportunity of providing the full complexity and spectrum of sound in children born with profound genetic deafness was a “phenomenon I did not expect to see in my lifetime”.
“These impressive results showcase the revolutionary promise of DB-OTO as a potential treatment for otoferlin-related deafness, and we are excited to see how this translates into an individual’s development, especially since early intervention is associated with better outcomes for speech development,” he said in a statement.
“We’re part of the beginning of a new era of gene therapy research that looks to create treatment options that address the root cause of profound genetic deafness.”
Regeneron said Opal had improvement of hearing to normal levels across key speech frequencies at 16 months of age at the 24-week assessment with an average 84 decibel improvement from baseline and one frequency measure reaching 10dB in hearing level per pure-tone average (PTA). Across all tested frequencies, an average 80dB improvement from baseline was observed. Auditory brainstem response (ABR) was positive, with best frequency reaching 45dB.
A second participant experienced consistent results to Opal at the six-week assessment including initial improvement of hearing with responses to loud sounds, which was observed across key speech frequencies, with an average 19dB improvement from baseline and one frequency measure reaching 80dB in hearing level per PTA.
Across all tested frequencies, an average 16dB improvement from baseline was observed. ABR was positive, with best frequency reaching 75dB.
Other trials
In a trial by Refreshgene Therapeutics, five of six children in China with autosomal recessive deafness 9 received AAV1-hOTOF gene therapy and showed "robust hearing improvement" over 26 weeks. Updated findings released at the conference by researchers from Fudan, China and Harvard
“This is truly remarkable. When we tell the story, even for our colleagues, it brings a tear to the eye,” Chen told the Harvard Gazette. “I’ve been working in this field for three decades, and I know how difficult it has been to come to this point.”
Akouos also shared data at the conference about its investigational gene therapy AK-OTOF-101 including that in October 2023, an American boy aged 11, born profoundly deaf in both ears with OTOF-mediated hearing loss had his hearing improved enough that he now has only mild to moderate hearing loss in the ear that was treated.
Caution urged
Like all therapies, however, gene therapy is not without risks, and has even been linked to deaths due to potential liver toxicity. America’s Mayo Clinic says a gene can’t easily be inserted directly into cells but is delivered using a carrier called a vector which is commonly a virus. This technique presents risk including unwanted immune system reactions which could cause a reaction that ranges from swelling to organ failure; targeting the wrong cells, risking damaging healthy cells; infection caused by the virus and disease; and the possibility of causing errors in genes which may lead to cancer.
A study in The Lancet in January 2024 on the gene therapy trial for deaf children in China said there were “no dose-limiting toxicity or serious adverse events reported”.
However, there were 48 adverse events – 46 (96%) were grade 1-2 (mild to moderate) while two (4%) were grade 3 (decreased neutrophil count in one participant).
Not everyone is happy with news of the promising results. The British Deaf Association said there must be a “detailed and comprehensive discussion of the implications of medical interventions such as gene therapy before this type of procedure is approved for widespread use”.
“Wherever deafness is concerned, the deaf community must be central in this conversation,” it said in a statement. “Deaf people are not sick or broken. We reject the medical model of deafness that reduces us to our disability. We are proud, healthy, active citizens who contribute to society and just happen to communicate in a different modality – using signed language rather than spoken.”
The surgical team performing Opal’s gene therapy transfer.
New horizons in hearing technology
Hearing aids help the hard of hearing connect with the world around them. We look at what technology is on the horizon to improve these connections, and even enhance sound for those with normal hearing.
Since 1898 hearing aids have transformed the silent world of the deaf and hard of hearing, improving communication and quality-of-life for millions of people. In recent years, they have metamorphosised from large, beige clunky devices into slim-lined and discreet high-tech aids hidden in the ear canal.
But what of the future? Are hearing aids poised for an artificial intelligence (AI) revolution, and will newer microchips responsible for sound processing enable hearing at normal or super-human levels? Here, three experts discuss some of the latest innovations and what is coming.
One of them is Dr Jorge Mejia. For 20 years, he has worked as a researcher at Australia’s National Acoustic Laboratories (NAL), developing algorithms for hearing aids and helping people navigate the complexity of hearing loss.
“Whatever we do, it needs to get to the clinicians and their clients, and change something fundamental in a positive way about how they live their lives,” he says. “The fact we have identified ways to improve people’s ability to communicate and make life easier, that is the reason we wake up and every day come to the office and do what we
do. Feedback from our clients is meaningful and important for us to continue to be motivated to achieve the things we need to.”
An electrical and computer engineer with a PhD in medical engineering science, Dr Mejia began his career working in satellite development in robotics. He then joined NAL, the research division of Hearing Australia based at the Australian Hearing Hub at Macquarie University, where he is head of the signal processing department.
“In the early days one of the problems was feedback cancellation (whistling) which remains a challenge today, but NAL gave me that challenge to look into and that’s how I became involved in hearing health,” he recalls. “That was in the early 2000s and since then I’ve been working at different stages of research from ideation to product development and commercialisation.
“One of the major initiatives in NAL in recent years has been the drive to enhance translational research and commercialisation.”
AI-driven technologies
The organisation is invested in exploring the integration of artificial intelligence (AI) applications in hearing health, with research focusing
on leveraging AI to enhance diagnostics, treatment, and rehabilitation for individuals with hearing impairment.
“We believe in harnessing the power of AI to revolutionise hearing healthcare, making it more accessible, personalised, and effective. The aim is to develop cutting-edge AI tools and technologies that can assist audiologists in providing better care and improving outcomes for patients,” Dr Mejia explains.
He says the whole industry has a significant emphasis on AI and it has already been used in different shapes and forms.
“There are many stages patients interact with clinicians, interact with technology, so most of the big manufacturers today have incorporated some form of AI into hearing aids to tap into this,” he says.
In the future, he predicts hearing aids will be characterised by continuous innovation and integration of AI-driven technologies.
“We envision hearing aids that are smaller, more discreet, and more powerful, with AI algorithms that can dynamically adapt to the user’s unique listening preferences and auditory needs,” he says.
“Another innovation we can expect to see more of in future hearing aid technology is user-intent sensors. This gives the client as accurate information as possible about the environment through the auditory system, including spatial awareness and natural hearing, without over-compressing or over-processing sound waves.”
Christo Fourie Gold Coast audiologist and founder of Value Hearing
self-managing the technology.
Industry experts say AI and machine learning (ML) will also enable more personalisation and situational awareness in hearing aids, requiring the consumer to do less manual adjustment. For example, AI will be able to track the direction a hearing aid wearer turns their head towards sound to maximise what they hear from that direction.
Dr Mejia says audiologists can best prepare for this future by staying informed of technological advancements, participating in professional development activities and collaborating with industry partners to ensure they can effectively incorporate innovations into clinical practice.
The AI-powered hearing aids which already exist have advanced features including ML-based sound processing, automatic environmental adaptation, and wireless connectivity, he explains. Some incorporate sensors for health monitoring and ML for adaptive sound processing while others have AI-driven features like binaural directionality for spatial awareness and environmental optimisers for real-time sound optimisation.
Another AI specific hearing aid launched in 2024 is the “biggest leap forward ever in hearing technology,” according to its manufacturer, with AI analysing and automatically optimising sound more than 80 million times an hour in this particular hearing aid. A processor designed to work like the human brain leverages the neuroscience of the ear-brain connection and information processing to create better sound quality, the manufacturer says, and it also incorporates health and wellness features, being the first to integrate sensors, track and encourage social engagement, and enable counting steps.
Another company says it has been using ML in its hearing aid technology for more than two decades. Its latest AI application uses an ML-model trained on thousands of real-world sound recordings tagged to indicate different environments. These hearing aids adapt automatically by selecting the best settings for every listening situation and zoom in on a single voice in a noisy environment.
AI advantages
Advantages of incorporating AI in hearing aids include that AI algorithms can adaptively adjust to various listening environments, optimising sound processing and improving understanding of speech in noisy situations, Dr Mejia says.
“Secondly, AI-powered features such as sound classification and noise reduction enhance user experience by reducing cognitive load and improving comfort,” he adds. “Additionally, AI enables advanced connectivity options, allowing for seamless integration with other smart devices such as phones, laptops and telehealth platforms. AI in hearing aids can improve clarity of speech and assist users in
“Thirdly, there are (phone) apps where you can query the app as to whether there’s a problem with your hearing aid or listening situation, and the app will tell you ways to fix the issue.”
Manufacturers are leveraging AI to do that on large language models but while these tools are out there, people cannot always take advantage of the technology. NAL is developing tools and solutions to support this ecosystem, from diagnostics to treatments.
“While AI is increasingly becoming a standard feature in hearing aids, we don’t foresee it ‘taking over’ entirely,” Dr Mejia adds. “Instead, AI technologies will likely be integrated into a range of hearing aid models and there will be different price points and user needs.
“While premium models may offer more sophisticated AI capabilities, basic functionalities will still be available in more affordable options. Ultimately, the goal is to ensure that all patients have access to AI-enhanced hearing solutions that deliver optimal performance and improve their quality of life.”
Dr Mejia reminds that the ecosystem is not only about technology but people and their social interactions with others. People come forward because of a hearing problem which might translate to, “I need a better job, I need to talk to my wife and understand her; she complains that sometimes I don’t get why she’s so angry. I want to hear my children or grandkids. Sometimes I don’t know what they’re talking about.”
“There are many things we need to understand and we’re at the early stages of tapping into the power of AI to do that.
“AI can play a significant role when you have a conversation with someone with a hearing impairment. That person, for example, might not hear the spoken emotions you express in your voice. AI can analyse this and the context. It could potentially, and this is not far in the future, give you an additional cue to help you realise that this communication is getting a bit heated, you need to alter the way you communicate because it’s going in a certain direction.”
Personalisation of technology
Hearing aid processors are also being trained to personalise the environment in the way the wearer wants to hear the sounds around them. Whether in a conversation, a restaurant, a quiet room, or watching TV, users previously adjusted settings on their device but now AI in hearing aids automatically does this as part of ML methodologies that analyse the environment and every change, every second, produce an analysis telling the hearing aids where you are and adjusting behind the scenes.
Instead of the patient focusing on adjusting settings, they can focus on the conversation or what is in front of them, freeing up more cognition and concentration.
“AI is taking away the complications and streamlining the process –that’s what we call personalisation of technology,” Dr Mejia explains.
Image: Christo Fourie.
To achieve this, hearing aids are linked to apps which, apart from remote hearing aid adjustment, can produce real-time monitoring of hearing health metrics, and access personalised rehabilitation exercises. Some aids and hearables track health data, similar to an Apple watch.
Advanced chip technology
Hearing aid chips are also becoming more complex as AI architecture is embedded into them and Dr Mejia thinks this will increase exponentially. While their tiny processors are remarkable in what they can do, AI often requires a lot more power than is currently possible.
“We are hitting some limitations in what we can do with hearing aid processors, what we can put into these microchips,” he says.
At the online Future of Hearing Healthcare Conference in May 2024, Dr Mejia discussed digital tools that enable patients to take greater control of their hearing health and participate more actively in their treatment journey.
He says NAL researchers are harnessing the power of AI to create tools for precise speech-in-noise assessments, enhancing the accessibility of hearing screening tools for adults and children. They’re using AI-powered assistive technologies to facilitate self-management
of hearing aid devices. One example uses a form of AI , a neural network, for more precise diagnosis of sensorineural hearing loss in any language.
User-intent sensors
“Another innovation hearing professionals can expect to see more of in future hearing aid technology is user-intent sensors,” says Gold Coast audiologist and founder of Value Hearing, Mr Christo Fourie. He believes the most impactful hearing aid in 2024 is the Oticon Intent because of its new chipset, the Sirius, which contains world first 4D user-intent sensors.
Fourie says this type of technology is about giving the client as accurate information as possible about the environment through the auditory system, including spatial awareness and natural hearing, without over-compressing or over-processing sound waves.
“It’s the first time it’s actually been in a hearing aid, processing the sound directly. With most other hearing aids, the AI is about adaptively changing the settings of the hearing aid based on the environment. This is the only hearing aid that has deep neural networks – a form of AI – on the chip in the hearing aid and that is an advanced, technically complicated process to achieve.”
A better chip increases the processing speed which means the accuracy of the sound coming into the ear is better. Things like distortion, or compression due to the limits of what the chip can process, are reduced and the amount of information coming in with a new chip is also improved, Fourie explains. The more powerful the chip, the more AI algorithms can be added.
“People are noticing the clarity and naturalness with the new chip because it’s all about reducing the listening effort by giving the brain all these subtle cues which are typically lost in processing,” he says. “The numbers we’re fitting are creeping up even though it’s more expensive.”
Bluetooth low energy audio is also coming to that chipset, he says.
‘Super abilities’ to communicate
According to Dr Mejia, hearing aids will be relevant for decades to come. “In fact, the idea that hearing aids are only for people with hearing problems is going to be less of a thing in the future.”
With the popularity of earbuds skyrocketing, hearables are the next big thing. The technology increases the chance for people with normal hearing to maximise this sense by interconnecting with other technologies.
One example is Auracast broadcast audio. It’s a new Bluetooth technology enabling people to focus in on a conversation in a noisy restaurant, a TV screen across a loud sports bar, hook directly into a public address system at an airport, or connect directly to a musician at a concert, blocking background noise. A small transmitter allows electronic devices to broadcast audio directly to the wearer.
While developed for those with normal hearing to target sound, the hearing impaired will also benefit. Several companies are using Auracast already in hearing aid devices and everyone in the industry is looking to adopt it, Dr Mejia says.
“Soon we are going to see this being more uniformly used because the potential to create the opportunity not just for hearing impaired people, although they would benefit a lot from this, but for all of us, is going to be immense,” he says.
“This integration of technology to our lifestyle will become more normalised and future technologies are going to create super abilities to communicate and remain connected. Language barriers will no longer be there. My normal ability to hear sounds may not be sufficient so this will enhance it.”
Image: NAL.
Dr Jorge Mejia from NAL in the anechoic chamber at the Australian Hearing Hub, Macquarie University.
Image: Andrew Bellavia.
“People say designing for accessibility is for everyone but this is the opposite – designing for everyone is designing for accessibility because the mass marketing possibilities of Auracast will drive more installations and that will benefit the hearing impaired.”
Andrew Bellavia
American thought leader in hearables and hearing health
Mr Andrew Bellavia, an American thought leader in hearables and hearing health and founder of Aurafuturity market and branding consultancy, spoke about Auracast at two conferences in May 2024: the Australian College of Audiology (ACAud) conference in Cairns and the Hearing Health and Technology Matters’ (HHTM) Future of Hearing Healthcare Virtual Conference. He is also co-host of HHTM’s This Week in Hearing podcast.
“Auracast is already in Australia – you can buy a Samsung TV that streams Auracast or if you have an older TV, you can put an Auracast streamer on it,” he told delegates. “You can share audio to multiple speakers, two people can watch a movie and both listen through headphones.
“Soon it will be in public spaces where people will get the most impact including hearing-impaired people. Multi-screen venues will be next because of the mass market potential. At a noisy sports bar you will be able to tune in to the audio on every screen.
“People say designing for accessibility is for everyone but this is the opposite – designing for everyone is designing for accessibility
because the mass marketing possibilities of Auracast will drive more installations and that will benefit the hearing impaired.”
Fourie believes Auracast will eventually replace telecoil because Auracast transmitters can be in any public setup and anyone with headphones, earbuds or hearing aids will be able to access nearby audio.
“Your partner might be using headphones and you might have hearing aids and you are watching the same movie but both can listen to the audio through different devices from that same transmitter, your tablet or phone. That will open up a whole lot of connectivity to people,” he explains.
“Auracast is a new protocol that creates a much more usable form that addresses most of the concerns we had with older Bluetooth technologies that weren’t designed for hearing aids and did not take hearing aids into account.”
Fourie reminds, however, not to underestimate the importance of a good fitting when it comes to hearing aids.
“There’s a lot of focus on products but I believe a poor product fitted with best practices can outperform a good product fitted poorly,” he says. “I think audiology worldwide has hurt itself by focusing on the product, rather than what audiologists can do because if we have a product we are comfortable with, knowing its ins and outs, understanding how it works for different clients, following best practices, we can make that work very well.”
Dr Mejia tends to agree. “Despite all the hype about AI creating automation, at the end of the day, human factors are still important. Audiologists around the world and clinicians play an important role in keeping people motivated, on the right pathways towards what they need to achieve.
“It’s not just about having a cool piece of technology in your ears. It’s also about understanding how the technology is impacting you and how to best use it.”
Experts remind not to underestimate the importance of a good fitting when it comes to hearing aids.
First hearing aid with new connectivity features
GN has just released Beltone Serene hearing aids which it says are the industry’s first hearing aids to connect to Bluetooth LE Audio and revolutionary new Auracast broadcast audio while also supporting existing connectivity options such as hands-free calls for iPhone, iPad and one-way Android streaming.
Gto have longer battery life in one charge,” Sabin told the Future of Hearing Healthcare 2023 virtual conference. “It offers better performing products, greater availability of Bluetooth hearing aids with new standardisation, multistream for binaural hearing aids, global interoperability and multi-language support between devices and Auracast broadcast audio.”
N says the Beltone Serene was specifically designed to assist hearing in even the noisiest of situations, allowing people to focus on what others are saying and hear with confidence in any setting.
“These weatherproof and sweatproof hearing aids are designed for everyday life and seamlessly connect to the wearer’s favourite devices,” GN says. “Beltone Serene offers a range of tiny and comfortable styles for mild to profound hearing loss, comprising the clearest streamed sound with the lowest latency and battery consumption for all-day streaming.”
Auracast broadcast audio, a new Bluetooth capability, is the next generation of assistive listening technology in hearing aids, everyday consumer audio devices and public spaces. It’s believed the technology will transform access to audio by enabling hearing-impaired people – and even the hearing-enabled – to share audio with family or friends listening at home to television or music from a smartphone, tablet or PC.
Importantly, in public spaces, it enables hearing aid users and those with normal hearing to connect directly to live audio in airports, train stations, theatres, bars, waiting rooms, stadiums, schools, conferences, lectures, and anywhere audio is broadcast.
Auracast creates new possibilities for streaming audio in public and private places and enhances the way people interact with others and the world around them. It’s predicted that by 2027, three billion Bluetooth LE Audio devices will be connected to Auracast.
Bluetooth Special Interest Group (SIG) explains that its Bluetooth LE Audio is the first new Bluetooth technology in two decades and until now there’s been no standardised Bluetooth protocol for hearing aid streaming. LC3 is the new standard codec for audio transmission for all products using Bluetooth LE Audio, developed with the consumer electronics industry and hearing aid manufacturers. It will result in significantly fewer compatibility limitations. When codecs were not optimised for hearing aids, hearing aid manufacturers developed and added their own proprietary protocols, leading to connection issues across different manufacturers, and consistent compatibility between hearing system firmware, smartphone operating systems and Bluetooth protocols could not be guaranteed.
Support the next 20 years of audio broadcasting
Mr Chuck Sabin, senior director of market development at Bluetooth SIG, says the new framework and flexible architecture of Bluetooth LE will support the next 20 years of audio innovation.
“Bluetooth LE enables higher sound quality at lower power enabling devices
GN offers an Auracast-supported TV-Streamer+ for clear TV audio streaming, with improved speech understanding compared to standard TV speakers, allowing people with Auracast-compatible smartphones, headphones, earbuds and hearing aids to tune in for shared listening.
GN philosophy is its ‘Organic Hearing’ approach that “sounds natural, feels natural and connects people naturally to the world”, and the company says 89% of users recommend Beltone Serene for hearing in noise.1
“With a 150% improvement in speech understanding in noise compared to legacy products,2 and industry-best access to surrounding sound (compared to other premium brands with 4-microphone binaural beamforming or advanced noise management3), Beltone Serene offers an outstanding listening experience that lets clients focus on what’s important to them,” GN says.
The Beltone Serene range offers – among other hearing aid models - the industry’s smallest rechargeable RIE4 with all-day power and latest sound technology for hearing in noise, and smallest wireless RIE CROS device.
Beltone Serene features include a ‘Hear in Noise’ program in the Beltone Hear Max app – empowering people to take control of their hearing aids directly from their smart devices.
Feedback management, low frequency boost, directionality, environment recognition and speech intelligibility in noise are among other features, in addition to TapControl on the ear or one hearing aid to answer calls, and new fitting options in the Beltone Solus Max fitting software to tailor onboarding and achieve best fit.
Sabin, from Bluetooth SIG, gave Mr Andrew Bellavia, an American thought leader in hearables and hearing health, a demonstration of Auracast at the EUHA congress in 2023.
Bellavia said, in a Hearing Health and Technology matters video at the congress, that Auracast has the potential to transmit to an unlimited number of devices in range. It would also change the way people interpreted the world as everyone, not just the hearing-impaired, could unmute what’s occurring around them.
“Users can connect to silent TVs everywhere, announcements at airports or train stations and hear better in noisy environments. The three uses are personal – with friends and family, in multichannel environments such as a sports bar, and single channel venues such as conferences,” he said.
NOTE: For more information about the Beltone portfolio, visit gnhearing.com
REFERENCES:
1. End-user NPS rating. Data on file (2023.)
2. 4.36 dB SNR improvement compared to legacy products. Jespersen & Groth (2022)
3. Compared to other premium brands with 4-microphone binaural beam.
4. Data on file, (2023).
GN says its Beltone Serene is the industry’s first hearing aid to connect to Bluetooth LE Audio and Auracast.
Wellbeing is crucial for hearing outcomes
Hearing loss can lead to isolation and loneliness from communication loss and disconnection. Holistic hearing rehabilitation is gaining traction as the ‘gold standard’ in hearing healthcare, integrating social and emotional wellbeing to improve outcomes. Attendees at The Sound Exchange ’24 were among the world’s first to experience hands-on learning of a 5-step plan to support implementation of this approach into clinical practice. Speakers included plan co-authors.
When it comes to tackling hearing loss, it is increasingly clear that rehabilitation is a team sport. Those supported through their hearing care journey by family or friends have been found to experience better results from devices including hearing aids than patients who are isolated and lack support.
Lead developer of the 5-step plan for holistic hearing rehabilitation, researcher and Audiology Australia (AudA) president Dr Barbra Timmer, who was in Melbourne for the Sound Exchange, said audiologists in her team wanted to drive change in thinking as most audiologists were still more likely to ask a patient about their hearing than how they were feeling. Outside Australia, the story is different with the importance of asking a patient not just about what they can hear but how they are coping socially and their emotional wellbeing becoming so well understood it is being written into clinical software.
In Germany these indicators are included in software used by audiologists to record improvements in hearing after hearing aids have been prescribed. Patients’ social and wellbeing needs and goals have been incorporated into management plans in the NHS in Wales and are embedded in CRM software across the UK to align supports to goals, and to measure that treatment outcomes meet patients’ needs.
Dr Timmer’s message to audiologists including in the packed room at The Sound Exchange ’24 is clear: “Don’t just ask ‘how’s your hearing?’ also ask, “how do you feel about your hearing?”
Before their hearing loss is addressed and treated, people often feel increasingly isolated, lonely, embarrassed, even ashamed because they
miss parts of the conversation, they can’t join in jokes, they don’t know the full story at home or work, and often find it easier to retreat and isolate, Dr Timmer said. Even at home, relatives can become angry and short with them due to having to constantly repeat themselves. Research showed it took on average seven years before hard of hearing patients asked for professional help yet they rarely discussed these feelings with their audiologist.
“Some patients who were surveyed said their audiologist never discussed feelings of isolation or asked about loneliness or how they were feeling emotionally,” Dr Timmer explained.
Social integration and support is key
A senior lecturer, scientist and research academic at The University of Queensland, Dr Timmer is helping spearhead change globally as the lead author of the 5-step plan for holistic hearing rehabilitation, a project she masterminded with several co-authors of the plan during the 2019 Phonak “Hearing well and being well – a strong scientific connection” conference in Frankfurt. The co-authhors agreed to team up to develop the model. Grounded in evidence-based research the resulting paper on their 5-step plan made a splash in the International Journal of Audiology as the most read paper of 2023.
Watching her talk at The Sound Exchange '24, her passion for driving the change is clear. Speaking at the AudA masterclass, Dr Timmer told the 100 delegates lack of social integration was a key factor in mortality and morbidity. She said recent studies had found this was the most important
Support from loved ones through the entire hearing health journey is vital for patients.
Image: Studio
predictor of mortality behind the number two risk factor, lack of social support. Loneliness and lack of support were more important risk factors for death and disease than obesity, smoking, diabetes, hypertension or any of the other well known risk factors, she added.
“Many people are not aware of this but we are starting to see research increasingly show this,” she told delegates. “This is why we want to make sure we practise the 5-step plan for holistic hearing rehabilitation. Look at the holistic and wellbeing needs of our patients. Everything is interconnected – cognitive, physical, social, emotional,” she told the audience.
“Audiologists are communication specialists. It’s important to involve family because the number two predictor of morbidity and mortality is lack of social contact. Once family know how to help, they’re willing to do it.”
Change the narrative
Although they may not discuss these topics with clients, Dr Timmer says audiologists do realise the importance of wellbeing in their clients and are starting to embrace methods to incorporate rehabilitation plans and measures into their practise. This is supported by the fact the top two downloaded papers in the International Journal of Audiology in 2023 were on wellbeing, including research by Dr Timmer and colleagues.
“Wellbeing is a hot topic – wellbeing of patients and clinicians too. There’s lots of interest and research,” she added. “The next five years I expect there will be an upswing in research and evidence on effects in audiology about generalised wellbeing. It will change the narrative in clinics - it won’t just be about hearing loss, it will be about wellbeing too.
“The 5-step plan says it is important we address a patient’s social and emotional wellbeing because in identifying this we feel we add value and we have better outcomes in hearing rehabilitation.”
And while hearing aids improve social and emotional wellbeing, there are other ways it can be improved too, she added.
Perception of hearing loss remains a challenge.
“There is still a lot of stigma associated with hearing loss. The University of Queensland touched on the topic in recently conducted research about how stigma impacts use and uptake of hearing aids in an international survey of over 300 Australians, Brits and Americans with hearing loss who were hearing aid wearers, non-users and past-users,” Dr Timmer said.
“One-third of those who were not wearing hearing-aids, and 8% who were, said they would never disclose their hearing loss in any situation. What can we do? Start talking about hearing loss to make people more comfortable about telling others about their hearing difficulties and help them realise the benefits of hearing rehabilitation. The research also showed that hearing aids were seen to be discreet, beneficial and high-tech, even by those not wearing them.”
The survey also asked 300 family members why their relatives were not using hearing aids.
“A common response was – ‘no-one has ever suggested using hearing aids’ which ties in with that figure of many waiting seven years before seeing us,” she said.
Although it was good to give people time and space to decide to seek help, leaving people without help for so long could mean deterioration in their social and emotional wellbeing.
The 5-step plan comprises:
• I dentifying the social and emotional wellbeing of the patient.
• Involving and inviting family members – (see tips box).
• Including social and emotional wellbeing goals in the management plan.
• Relating needs and goals to interventions such as hearing aids and communication strategies.
• Using counselling skills in the hearing loss rehabilitation process.
Another co-founder of the plan, The University of Queensland Executive Dean, Faculty of Health and Behavioural Sciences, audiologist Professor Louise Hickson PhD AM, expanded at Sound Exchange on the importance of including loved ones in the hearing health journey.
“Family-centred care is about including family members in all aspects of rehabilitation and is not limited to biological family but can be anyone who the client feels comfortable with – close friends or relatives can be included in the appointments virtually with platforms like Zoom. You can call them beforehand to offer to include them virtually,” she said.
“Why include family? Because family care, they will do what they can to help their relative or friend, and evidence is very strong that family involvement improves outcomes. If family is involved, the person with hearing loss is more likely to seek help so please engage with family. Think of the family as the client.
“Families help with decisions the patient makes including cost and style of devices and whether to get hearing aids now or later. Hearing aids are a major financial decision and families are an important part of this decision.”
Prof Hickson said wearers of hearing aids were more successful using
“Feeling less embarrassed or less fatigued by my hearing loss,’ or ‘being more connected with family and friends’ are great goals and can be achieved with a range of options from auditory and communication training, the use of hearing technologies, social prescribing and counselling. These goals are as important as those that address a change in hearing.”
Dr Barbra Timmer University of
Queensland
Dr Barbra Timmer at The Sound Exchange '24 masterclass.
Image: Audiology Australia, taken by Event Photos Australia.
Image: Audiology Australia.
them if they had support from the community around them.
“People whose partners have (untreated) hearing loss can experience third party disability because it can also limit them attending family gatherings and limit their social interactions too but rehabilitation can reduce this disability,” she added.
Involving family not only led to better clinical outcomes, but also improved outcomes for businesses because happy clients told others, Prof Hickson reminded delegates.
Unfortunately, research shows that only about 30% of adults attending audiology appointments in Australia bring a significant other, she said. The study found certain tips worked (see tip box) and increased in-person family attendance from 26% to 48%.
Dr Timmer advised creating an individual management plan and relating social and emotional needs and goals to audiology rehabilitation recommendation, such as hearing devices, communication and auditory training and social prescribing.
“Use counselling skills and technology to explore and monitor social and emotional wellbeing. You’re not just providing a path in audiology care but are providing added value to the therapeutic alliance with your patients. Monitor and document these new social and emotional goals regularly.”
She said holistic hearing care was the foundation of the audiology competency standards in Australia. Essential to this was addressing the social and emotional wellbeing of clients and The Sound Exchange stream taught how social and emotional wellbeing could be addressed in audiology appointments by using the plan.
“Some audiologists say they don’t have the time or a structured approach to this and I understand the time pressures on audiologists and the pressure to optimise their appointment times are very real but if we do not screen our clients’ social and emotional wellbeing, and make sure we address this during their hearing care journey, how do we know that we are adding real value to their hearing care?” Dr Timmer told Hearing Practitioner Australia (HPA).
“No client comes to us for hearing devices, they come to improve their communication, feel more connected to others, not be a burden on family, for a host of reasons which are all related to the impact from their hearing loss. Hearing devices are one tool in the range of services
Tips for staff include:
• Educate patients about why they should bring family.
• Invite the relative beforehand via phone, email or text to attend and be actively involved. An invitation is received better beforehand rather than as an afterthought on arrival and may reduce interjecting and interrupting if they have prepared questions. When invited beforehand, relatives feel they are valued.
• Ensure the relative does not sit in the waiting room during the consult but goes in.
• In the consult, the audiologist should ensure the relative has a chair at the same table to encourage involvement, rather than being in a corner.
• The audiologist should ask the patient to tell their hearing story then ask the relative for their view.
Source: Prof Louise Hickson.
we provide but if that is the only thing we provide, then we are too device-centric and are forgetting the comprehensive nature of the role of an audiologist.”
The 5-step plan has skills and techniques that audiologists can use for counselling and suggests questionnaires for social and emotional wellbeing and holistic hearing care, including resources to set rehabilitation goals or expected outcomes.
“These goals often relate to an improvement in speech understanding or audibility as a result of hearing devices. What the individual management plan tries to incorporate is a more holistic approach. This means discussing hearing goals and social and emotional goals,” Dr Timmer explained.
“Feeling less embarrassed or less fatigued by my hearing loss”, for example, or “being more connected with family and friends” are great goals and can be achieved with a range of options from auditory and communication training, the use of hearing technologies, social prescribing and counselling. These goals are as important as those that address a change in hearing.
“I’d love to see the plan profiled in the audiology university programs. All institutions teach the links between hearing and wellbeing and the core of person-centred care but perhaps the 5-step plan is a good model to bring these teachings together,” Dr Timmer told HPA
Some of the leaders of the holistic hearing rehabilitation masterclass, Dr Maren Stropahl (from left) Pauline Buchan, Zoe McNeice, Prof Louise Hickson, Dr Bec Bennett, Dr Jack Holman.
Image: Prime Creative Media.
An audiologist’s journey to a
cochlear implant
noticed that the left headphone was not working,” she recalls. “I thought ‘how annoying’ but with further investigation I realised the issue was that I had actually lost hearing in my left ear.”
‘My colleague diagnosed me’
Court was performing a lot of vestibular testing at the time, and as part of a large multidisciplinary team within a large teaching hospital, it was an ENT colleague who provided the official diagnosis.
The Ménière's started with classic low frequency hearing loss, aural fullness, tinnitus, and vertigo.
“My hearing loss and tinnitus would come and go but then it became permanent, and I experienced occasional episodes of vertigo and extreme nausea,” she recalls.
“For patients who were struggling with the same symptoms, I was able to reassure them that it would get better. Overall, it enhanced my perspective and ability to empathise with patients with tinnitus and vestibular conditions.”
Court says that as her hearing worsened, although maintaining a degree of hearing, her speech discrimination was affected, and she could not understand anything through her left ear. Socially and at work, hearing in background noise and in groups was more difficult.
“I am very pro-hearing aids and I tried about five different hearing aid devices over several years, but for me they weren’t able to offer significant benefit.”
Cochlear implant for single-sided deafness
In 2008, MED-EL Medical Electronics achieved its first cochlear implantation for single-sided deafness.
“I was following this research because I worked with cochlear implant patients and I knew if anything happened to my good ear, I’d have an implant in a heartbeat,” Court recalls. “I saw the outcomes firsthand; I knew what a great help they were and how quickly people could start hearing again.”
At this time, she was living in Bermuda with her Australian-born husband Michael delivering hearing services to the island’s population. After having two children there, her vestibular symptoms ceased, but she remained with both hearing loss and tinnitus.
HELEN COURT is an audiologist with Ménière's disease and a cochlear implant. She explains how her lived experience allows her to see things from both the practitioner and patient perspective.
There is no doubt in Ms Helen Court’s mind that hearing loss and having a cochlear implant have enhanced her work as an audiologist. Court was diagnosed with Ménière's disease at age 23 as she was embarking on a career in audiology. But instead of being pessimistic about the diagnosis, she continued her promising career trajectory and chose to use the experience to improve the lives of her patients.
“I wanted a career that involved helping people. At university, I went to a careers day and entered my details into a computer algorithm,” she recalls.
“It revealed my ideal careers were either an audiological scientist or a prison governor. In hindsight I would have been a fantastic prison governor but I looked into audiology and thought it sounded perfect for me.”
UK-born Court had no family history of hearing problems when she began studying a biology and physics degree, followed by a Master’s Degree in Audiology at The Institute of Sound and Vibration Research, University of Southampton which is world renowned for its audiological research.
After a gap year volunteering for a charity, she completed her Masters and began an internship at St George’s Hospital, a teaching hospital in London with a large audiology department.
“It was whilst performing a daily routine equipment check in clinic that I
“We moved to Australia in 2007 and I wanted to be the best mum I could, which meant being proactive with my health, and most importantly being able to hear the children from any location, so I decided to get a cochlear implant as soon as they were funded by private health insurance,” she says.
A fondness for all three excellent cochlear implant surgeons she worked with meant she drew lots to choose her surgeon, with Dr Chris Que Hee at St Andrew’s Hospital “drawing the short straw”, she recalls.
Switched
on her own implant
In 2014, she underwent cochlear implant surgery without trepidation as she knew she had everything to gain in terms of hearing.
“I was surprised to wake up feeling good, I was in no pain, and I was eager to find out what it sounded like,” Court said.
Back at work a week later, an excited Court switched on her own processor during her lunch break.
“Typically, patients visit their audiologist to have their implant activated, also known as a ‘switch on’, but being an audiology professional, I was able to perform this myself.
Images: MED-EL.
Helen Court’s cochlear implant is mostly obscured by her hair, with just the processor showing.
“During activations I had performed for my patients, I knew what to expect, but I was still surprised by some of the sounds, such as the noise the patient response button made, and the keyboard clicking.
“The other thing that amazed me was the silence; the implant had helped get rid of my tinnitus and for the first time in 20 years, I didn’t hear ringing in my ears – how incredible was that!”
Implant makes life more balanced
In terms of how the implant has changed Court’s life, she says she feels more balanced, and not in the vestibular sense of the word.
“Until you actually experience it, it’s hard to explain how you feel when you can only hear out of one ear,” she says. “You feel that sound is imbalanced, and for about 20 years I could not localise anything, which was really frustrating.”
Life with a cochlear implant and hearing with two ears again was great. However, eight years later, when having an MRI for a suspected tumour on her pituitary gland, the MRI scanner pulled the implant’s magnet out.
After that Court chose to replace her implant with a MED-EL cochlear implant, which was 3.0T MRI compatible, meaning it was safe for her to have unlimited MRIs. Another advantage was that it provided complete cochlear coverage, giving better access to hear low frequency sounds and improved sound localisation.
Court worked at a busy clinic on the Sunshine Coast for about 10 years, helping cochlear implant, hearing aid, vestibular and paediatric patients.
“WHEN I SEE PATIENTS IN THE CLINIC, THEY’RE OFTEN SURPRISED I HAVE AN IMPLANT MYSELF AS THE PROCESSOR IS UNDER MY HAIR AND NOT VISIBLE,” SHE SAYS. “PATIENTS LOVE THAT I’VE GOT A COCHLEAR IMPLANT AS THEY KNOW THAT I UNDERSTAND WHAT MAPPING IS LIKE AND WHAT IT’S LIKE TO HAVE SINGLE SIDED DEAFNESS."
After fitting many MED-EL patients, and feeling the call of a new intellectual challenge, an opportunity arose to join MED-EL.
Attends surgery to do testing
As a clinical specialist in the Queensland team, she supports implantees at all stages of their hearing journey including their decision to be considered as an implant candidate, choice of device, support after surgery and fitting of the processor. She supports and trains audiologists to program and manage implantable devices and provides surgical support through analysis of pre-operative scans to determine the size of the cochlear and obtain the optimal electrode array for each patient.
Court also attends surgeries to ensure correct functioning of the implant and performs objective measures of hearing thresholds through the implant, which can be used at switch on.
“When I see patients in the clinic, they’re often surprised I have an implant myself as the processor is under my hair and not visible,” she says. “Patients love that I’ve got a cochlear implant as they know that I understand what mapping is like and what it’s like to have single sided deafness.
“I’ve learnt so much from mapping myself and doing my own rehabilitation and that gives me a real insight into optimising the maps for patients with single-sided deafness.”
Court also volunteers with Hearpeers, a global community of mentors set up by MED-EL that provides free one-on-one support to hearing implant recipients and potential patients seeking information from others with lived experience.
Additionally, she is involved with CICADA Australia, a charity and volunteer organisation dedicated to supporting hearing impaired Australians who use cochlear implants or are considering one. She says while many babies and children benefit from cochlear implants, sadly many adults who would benefit keep struggling with hearing aids and don’t consider implantation.
“Audiology is part of my life, it’s who I am, and I feel it’s my mission, my calling to help people with a hearing loss,” she says.
Helen Court in surgery helping other cochlear implant patients by ensuring correct functioning of the implant.
Helen Court at the Australian College of Audiology congress in Cairns in May 2024.
Leading our hearing health heroes
LEANNE EMERSON is the new head of the nation’s largest accrediting body for audiologists, Audiology Australia. Here she discusses plans to grow the organisation, unite the industry and raise the public profile of hearing health.
After eight years she returned to clinical work as a counsellor at Alzheimer’s Australia for several years, before again stepping into management roles including acting CEO of the organisation’s Victorian body across two years
When the eight state and territory organisations merged into one national body to become Dementia Australia in 2017, Emerson moved to an executive role and overall, spent more than 20 years with the organisation. While passionate about the work, she wanted to move back to a CEO role in a for-purpose, not-for-profit space that could benefit from her management
“I was looking for a challenge where I thought my skills would bring something new to an organisation and help them achieve their objectives, and I wanted to do it in an area I believed I could bring the same level of passion,”
“There is an overlap between hearing loss and dementia, and personal alignment with my family’s hearing loss. Audiology Australia works from a set
Tasked with leading the nation’s peak professional accrediting body and its 3,600 audiologist members, Emerson started with Audiology Australia in
“I had come from a large aged-care and dementia world to a smaller but no less complex audiology world. The week I started we launched our new strategic plan, a new customer relationship management software system, had an annual general meeting and my first board meeting and most of that was on my first day!” she recalls. “It wasn’t a bad way to start because I had to ‘get down and dirty’ quickly and get across audiology, hearing health and how
From becoming managing director of an aged care facility at age 22, to working in dementia and aged care management for more than 20 years, Emerson’s career so far has been the perfect preparation to tackle the challenges ahead for audiology. She believes fresh eyes, along with a consumer perspective and wealth of management experience in patient care, will give her an advantage as she seeks to help unite a somewhat fragmented hearing industry.
Personal experience of hearing loss also brings another valuable outlook. Her mother was diagnosed with otosclerosis and significant hearing loss at age 17 and became deaf in one ear after surgery to rectify it in the 1960s severed a nerve.
“My siblings and I inherited the otosclerosis and while I have some hearing loss, it’s remained stable for the past ten years." Emerson says.
“Growing up I remember Mum really struggled with her hearing and there weren’t the supports or services available that there are now, so I have a perspective of what it’s like as a consumer and the impacts that not having hearing addressed adequately has on your life.”
Her mother was a nurse and so from age 15 Emerson worked part-time in an aged care facility while at school and later while studying psychology at university. After graduating, she applied for the aged care managerial job and says it was controversial in those days for a psychologist, rather than a nurse, to have this role. Over the next few years, she managed several facilities and believes a postgraduate degree in organisational psychology, covering organisational change management, building teams and healthy work cultures assisted greatly.
“For a small industry, there’s a lot going on and the industry punches above its weight in terms of the hearing health care it provides. Everyone I’ve met, including our members, I’m impressed with their passion and energy; everyone genuinely cares about being able to provide exceptional hearing services, everyone is looking to improve what they do, and they’re a tenacious group.”
Unifying the sector
On one hand, she says the industry is fragmented with different perspectives, agendas, and focus areas, and while it’s obvious that people are working hard and passionately towards better outcomes, “they’re not always doing it in a joined-up way”.
“The fact there are different drivers for each perspective of the four largest stakeholder groups – clinicians, industry, research and consumers – means we are not always as strategic as we could be,” she says.
“The challenge is to come together to keep our eye on the big picture. The Hearing Health Sector Alliance (HHSA) provides a vehicle to have a united voice, comprising groups with members from professional bodies, consumers, research and industry, headed by Jane MacDonald from Hearing Business Alliance. I sit on the executive of HHSA and see real opportunities for us to have significant impact across the sector.”
The alliance plays a fundamental role in addressing more than 140 recommendations of the Roadmap for Hearing Health, setting five priorities and a comprehensive action plan. Audiology Australia, as part of that group, has several objectives it wants to achieve in coming years.
Leanne Emerson at The Sound Exchange ’24 in Melbourne, May 2024.
Image: Hearing Practitioner Australia.
According to Emerson, HHSA is the ideal vehicle for a united voice to government.
‘‘At the end of the day, we’re all trying to ensure the patient/consumer gets the best hearing health care they can – that’s an easy focus to agree on,” she says.
Priorities and
goals
Emerson says her new direction is a more bold, assertive approach to addressing key issues for members. “Audiology Australia is a mature organisation that has a wealth of wisdom from more than 3,600 members to draw on, so we need to garner those perspectives and be responsible but also confident and bold in the way we represent them to government.”
She likes open, robust discussion with transparency and says people don’t have to agree all the time but there’s a need to understand different perspectives and look for the opportunities.
“A former colleague used to say there is wisdom in the dissent, and that has stuck with me because everyone has a voice; these only add value and heighten the quality of solutions we come up with,” Emerson adds.
The immediate future is flooded with reviews and a reform agenda, and the association will focus on advocating for “what we need in audiology throughout those reviews because they are a critical moment in the evolution of audiology," she says. These include a review into regulation of the industry.
The medium and longer-term focus is to ensure members feel heard and valued, and increasing the value proposition so they get what they need from their professional body.
A vital part is elevating the public profile to the broader community, so it understands more about the important work audiologists do.
“Everyone knows what a GP and a nurse do but I don’t know that everyone knows what an audiologist is or does,” Emerson explains. “We want a public awareness campaign – there have been several already including our recent substantial one – Audiologists. We Hear You!, and we’ll continue to campaign to ensure the profile of hearing health and the work of audiologists is elevated."
National campaign needed
“We need a national campaign to look at hearing loss risk reduction, and to demystify and destigmatise whatever it is holding back people from having their hearing checked and taking on board recommended devices or programs.
“It would help people understand more about the importance of hearing health and consequences to quality-of-life of not pursuing any concerns.”
One of HHSA’s aims is funding for such a campaign and the alliance will advocate to government for this, she reveals.
Delegates at Audiology
“We need a national campaign to look at hearing loss risk reduction, and to demystify and destigmatise whatever it is holding back people from having their hearing checked and taking on board recommended devices or programs.”
Leanne Emerson Audiology Australia
“This is the point, working in silos each part of the sector can do some promotion or advertising and people hear about a certain offer or company, but they’re not getting information about why hearing health is so important,” she says. “HHSA is well positioned to do that from a sector wide perspective in the interests of improving hearing health for Australians.”
Improving access to services for people from Aboriginal and Torres Strait Islander background is another of Audiology Australia's priorities. Building capability across the profession to ensure First Nations peoples have access to hearing health care in a culturally appropriate manner is part of the organisation’s Reflect Reconciliation Action Plan.
Securing audiologists and audiometrists in rural and remote areas is another item near the top of the Audiology Australia agenda.
Professionals are often unwilling to relocate to these areas and those in these regions work hard travelling to service their local populations.
“Many rural employers have trouble attracting staff and we need to look at solutions. I know of audiologists who regularly fly from Melbourne to Darwin to provide services in remote areas for example,” she says.
Screening of aged-care residents
A significant challenge though, she says, lies with elevating the profile of allied health more broadly and audiology specifically. At all levels - government, industries and community - allied health professions are too often an afterthought, she adds.
“The Royal Commission into Aged Care identified significant gaps in the provision of allied health services into aged care, for example, yet we have the lowest number of allied health services in aged care than ever before.
“We know that 73% of people over the age of 70 have moderate to severe hearing loss, yet there is no government funded program to routinely screen aged care residents.
“Audiologists have to work harder to have their voices heard through the busy reform agenda.
"There’s a lot of discussion which comes up around regulation, what it means, the options, the benefits, disadvantages, but fundamentally there are a few key changes we would like to see for the profession and at the top of that list, is protection of title.”
Other challenges include systemic issues including limits to prescribing and referral rights, which mean audiologists cannot go about their work in the most seamless way.
One example of referral rights for audiology – being assessed as part of a national scope-of-practice review – is that if audiologists need to perform diagnostic scans, they cannot refer directly for them. Instead, the patient needs to see a GP for a referral – an extra step the association argues is unnecessary.
There might be a lot on the ‘to do list’ in the world of hearing health but Emerson is up for the challenge and believes the future is bright if the sector can come together and put aside individual biases for the overall good of the community.
Australia’s biennial event
The Sound Exchange ’24 in Melbourne 2024.
A voice for independent audiology
Audiologist JANE MACDONALD wears two crucial hats in Australia’s hearing industry. She is head of the Hearing Business Alliance, the nation’s only business body representing small to medium independent audiology businesses. And she is chair of the Hearing Health Sector Alliance, comprising 16 organisations and representing consumers, professionals, research and industry. She discusses this important work.
When Mrs Jane MacDonald started in audiology 38 years ago, she never imagined she would be spearheading an organisation that is the business voice for Australia’s small to medium audiology practices. And the weight of the job isn’t lost on her.
As CEO of the Hearing Business Alliance (HBA), she liaises with members, stakeholders and regularly treks to Parliament House – or dials into Zoom meetings – to talk to politicians and health department officials advocating for one of the most crucial segments of the audiology market – independents.
“It’s busy in meetings but it’s not difficult doing these negotiations because I think of all the patients our members are helping and how important it is,” MacDonald says. “And for small to medium independent business owners, the loan is against the family home to set up and expand the business – no other audiology job has that. It's something I am acutely aware of as my mum had a small dress-making business when I was a child. It encountered hard times and we lost our family home as a result.”
HBA advocates for members, striving for fair and equal opportunities to all providers, and a level playing field when it comes to competition and providing a voice for small business.
The organisation formed in 2016 with 10 small independent audiology businesses, including the Mildura practice owned by herself and her husband Mr Don MacDonald. In under a decade, the alliance has skyrocketed 16 times its size.
‘’Representatives of hearing businesses from Victoria, Queensland and NSW met in Sydney because they recognised there was a missing seat at the table during important conversations with government and other stakeholders,” MacDonald recalls. “They thought small business should be represented at these meetings.
“At this gathering, the name and terms of membership were agreed including that HBA should be a business body and it’s the business that is the member, operating on a one business/one vote basis. Member businesses are owned by audiologists, audiometrists and others. We wanted to be a voice because we felt we had no voice.
“It is also to help government because sometimes government officials don’t realise the impact some decisions are having on smaller independents. It’s about bringing attention to the services that small independents provide, things the bigger providers normally don’t deliver such as paediatric audiology, diagnostic and vestibular audiology for people with balance problems and cochlear implant programming.”
More than 680 sites nationwide
In a market heavily influenced by corporate networks, including some from overseas, the alliance provides a united voice for local independent audiology clinics, helping them become better organised and stronger businesses.
“In 2024 HBA’s membership is approaching 160 businesses, delivering
audiology services at more than 680 sites across Australia, and employing over 450 audiologists and audiometrists,” MacDonald proudly reveals.
“Our membership represents more than half of the independent audiology businesses in the hearing sector in Australia.
“This is why my role has evolved into a full time position. The goal is to get everyone on board.”
HBA’s mission is to inspire and encourage hearing care businesses to reach their full potential by representing members to consumers, professionals, government and non-government bodies on hearing health consultations and developments.
It is committed to helping small business providers remain financially viable so they can continue to serve their hearing-impaired clients and local communities as it is difficult to compete on price with some of the corporate networks while promoting best audiological practice, MacDonald says.
“The collective voice adds volume to the message of small business. Collaboration amongst members provides support to each other and this is especially important when running a small business can feel lonely,” she explains.
Its enormous growth means she has reduced the amount of clinical practice she does to involvement with neonatal diagnostic audiology, a part of the profession she loves.
But there are no regrets because she feels her role can create a significant impact on the sector, and ultimately the public.
“I do this because after being an audiologist for 38 years and helping so many people with their hearing – and based in a relatively remote rural location – understanding the challenges for people with hearing and ear related conditions, how difficult it can be for them to access local services
Images: Jane MacDonald.
Jane MacDonald outside Parliament House in Canberra.
and affordable services, that’s really important to me,” she says.
“It’s also about helping other businesses like the one I own with my husband, and all our members, to continue to provide services to their clients in those communities. We have many rural members.
“My own little practice has grown so others are now doing that work. We employ 12 audiologists and 35 staff. There will soon be six clinics plus outreach services, so I know that that important clinical work is still happening, supporting the community.”
After graduating as an audiologist from The University of Melbourne, MacDonald worked in Melbourne before moving to the country Victorian town of Mildura in 1990. She was the only resident audiologist for a 400-kilometre radius.
She worked at Mildura Base Hospital and also did private work in her own business for six years. MacDonald moved to Scotland with her Scottish husband, married, had two children and lived and worked there for seven years before returning to Mildura in 2003.
During the past 21 years, along with her business development manager husband who is also an audiometrist, she expanded that one clinic, Country Hearing Care, to five in rural Victoria and NSW. The practices are in Mildura, Broken Hill, Swan Hill, Echuca and Eaglehawk, a suburb of Bendigo. A large clinic in Bendigo is under construction.
business viability.
“We are worried that changes could cause closures. Any reduction in business viability is always a concern.”
In 2018, MacDonald started working part-time with HBA, while still working a few days in the clinic. That changed in early 2023 after the growth in membership and increased advocacy necessitated working full-time.
Audiometrists, collaboration and HSP changes
The alliance also lobbies for business operations that impact audiometrists.
“Some health insurers cover services provided by an audiologist but not an audiometrist even though doing hearing tests and fitting hearing aids are within their scope-of-practice – and this is recognised by the Hearing Services Program,” MacDonald explains.
“Some practices only have audiometrists, especially in rural areas, where patients might have to drive long distances to see an audiologist. If there is a husband-and-wife team in a clinic and one is an audiologist while the other is an audiometrist, the client who sees the audiologist will get a rebate while the one who sees the audiometrist won’t. It’s crazy, and it’s something that we are working on.”
HBA provides business advice including seminars and collaborates with organisations advocating for the industry and the public including the Australian Small Business and Family Enterprise Ombudsman “because sometimes things happen that impact small business providers more than other providers”.
HBA works with Audiology Australia and the Australian College of Audiology and has a Memorandum of Understanding with both, collaborating on things that could impact audiology business.
Most HBA members are Hearing Services Program providers and the Department of Health and Aged Care recently surveyed stakeholders asking for responses to proposed changes to the program.
“The collective voice adds volume to the message of small business. Collaboration amongst members provides support to each other and this is especially important when running a small business can feel lonely.”
Jane MacDonald Hearing Business Alliance
One proposal is to reduce more than 50 HSP items to 10 which the government says would be to simplify the schedule and make it easier for providers and patients.
“There have been no costings for reducing schedule items for hearing aid fittings,” MacDonald says. “About 16 different fitting claim items would be replaced with one. We look forward to the department’s costings to see how this could be cost neutral as they are all different. We expressed concern about some other proposals too."
The alliance has invited Mr Chris Carlile, Department of Health and Aged Care assistant secretary of the Hearing Services Branch to provide an update at a business seminar in July.
Other work HBA has been involved in to improve practise and business includes a working group on tele-audiology and Department of Veterans Affairs collaborations.
“HBA members are a collaborative group and even though some are competing against each other, they are helpful. We have member-only Zoom meetings to discuss issues and members are supportive, and a member-only Facebook group where someone asks a question or raises an issue and others respond with helpful answers.”
Government seeks HBA and HHSA opinions
Constant lobbying is the HBA’s biggest achievement, she says.
“HBA has written many submissions in areas that impact our members’ businesses. There has been a lot of change in the hearing health sector and it is imperative that the voice of small business is heard,” MacDonald says.
She’s honoured to be Chair of the Hearing Health Sector Alliance (HHSA).
“HBA is proud to be a founding member of the HHSA and government now approaches the HHSA for information and feedback,” she adds. “HBA also provides feedback to MPs, the Hearing Services Program team, Practitioner Professional Bodies, universities delivering Masters of Clinical Audiology programs and others to provide perspective around business implications of service delivery."
HBA collaborates, through its membership on the HHSA, with the Hearing Care Industry Association (HCIA) – the business body representing larger hearing chains. HBA also sends information to new members, supporting them to set up a business, helping them write a business plan and get a contract to become a HSP provider.
With more than 240 years’ collective experience in the hearing sector, HBA’s executive and board directors are well placed to understand challenges and rewards of owning and running an audiology business.
The Hearing Business Alliance executive and board in February 2024.
Taking the din out of dinner
Adelaide audiologist LAURA DREXLER has created a website and app to help diners find quiet places to eat.
The Ambient Menu highlights quiet times and eateries for the hearing-impaired and those with normal hearing who prefer less noise while dining out. She believes it’s the first of its kind in Australia, and possibly the world.
While studying audiology, Mrs Laura Drexler turned her research project into a small business that is helping thousands of Australians with and without hearing loss have better experiences while eating out.
“In 2019, my student group and I were looking at the interaction between family dinners and hearing loss. Family dinners are good for mental health, social engagement and overall wellbeing but hearing loss can affect those things in a negative way,” she says.
“We were studying the link but instead people we interviewed spoke about noisy restaurants, how challenging that was for them, how isolated they felt and how at the end of the night, they were exhausted and started to withdraw. I thought, ‘surely there’s a website I can direct my future patients to to help them find a quieter place to eat’, but there wasn’t so I created one.”
She received grants from Onkaparinga Council, Business SA and the Deafness Foundation to help establish the website.
“The Ambient Menu is a web app that connects people who struggle to hear in background noise to an acoustically friendly restaurant. We act as a conduit to guide people to a restaurant where they can comfortably have a conversation and our mission is to take the ‘din’ out of dinner,” Drexler says.
“Diners leave reviews based on background noise, food and service because you don’t want to go somewhere that’s like a library or has terrible food or service. It’s all about finding the right place for you at the right time that suits your listening needs.”
In five years the Ambient Menu has amassed nearly 10,000 subscribers who log on to find good local eateries with matching ambience.
Restaurants can achieve a higher rating by meeting criteria during accreditation from Drexler and her husband Andy who have completed training in acoustics and as noise assessors. They personally visit to review
and provide an education pack with noise-reduction tips to restaurant owners. Diners search for their sound level – quiet, low, moderate or lively –and suburb.
The Ambient Menu lists more than 6,000 restaurants of which about 1,300 have been reviewed in South Australia and Queensland including the Sunshine Coast and about 100 in Brisbane. There are a handful in Victoria with plans to include more this year.
As the business launched in Adelaide during the COVID-19 pandemic, South Australian restrictions on dining made Drexler pivot to focus on Queensland where there were less restrictions, and she could visit friends.
She won the 2023 Flinders University Early Career Alumni Award because of how many people the business has helped, was selected as a South Australian Featured Woman to Watch 2024 and nominated for Community Leader of the Year and Emerging Business of the Year for the 2024 Small Business BEAM Awards.
“It’s a lot of work, especially since I also work as an audiologist and in ambulance patient transport, but it’s worth it when I get messages from people thanking me and saying how much it’s helped them as they can now enjoy dining out.”
Laura Drexler Audiologist, Ambient Menu creator
Images: Laura Drexler.
Audiologist Laura Drexler using her Ambient Menu app in a restaurant.
“It’s a lot of work, especially since I also work as an audiologist and in ambulance patient transport, but it’s worth it when I get messages from people thanking me and saying how much it’s helped them as they can now enjoy dining out,” Drexler says.
Paramedic work
The path to audiologist and business owner was an unusual one. At 19 she became a police officer but after five years swapped to being a paramedic. Her police officer firearms instructor husband developed very high frequency noise-induced hearing loss, tinnitus and vestibular issues. At one stage he was bedridden with vertigo and struggling.
“This piqued my interest in vertigo, and along with seeing ambulance patients with these issues, I took an interest in vestibular issues. My husband achieved tinnitus relief from seeing an audiologist who gave him counselling and strategies and both said I would make a good audiologist,” she recalls.
While working as a paramedic and with a young son, Drexler began her Masters of Audiology at Flinders University.
“Going back to uni in my 40s, being the oldest in my course, getting a massive HECS debt and going from being an experienced paramedic to a newbie was not a decision I took lightly but it was the right decision. I love my job, it’s challenging, rewarding and something different every day.”
After 20 years in the ambulance service, Drexler still works part-time in patient transfer to pay people who help with the Ambient Menu gig. Her main career is as an audiologist for Adelaide Audiology working for an ENT surgeon doing WorkCover and compensation claims. She also works in adult rehabilitation doing hearing loss assessments and at a private clinic on vestibular assessments. She has recently quit a fourth job, fitness instructing, due to her workload and is doing extra studies in acoustic consultancy.
Accreditation for quietness
To accredit restaurants as part of the initiative, Drexler or her husband attend a restaurant, speak to staff, find out what they have to offer, the quietest times, busiest times and quietest places to sit. Additionally, they evaluate acoustics.
Drexler has also recruited ‘Ear Buds’ – friends, audiologists and audiometrists - who find and review restaurants including speaking to owners and, with their permission, advertise their quieter and busier times. So far, they have done 128 reviews.
“The restaurants love it because they’re not getting noise complaints and because it helps attract customers to quieter nights,” she says.
Ambient Menu accreditation includes taking noise readings when calculating acoustic capacity – how many people can be there before it reaches a livelier level. To achieve this status, restaurants must meet quiet criteria for 80% of dining times. If this is achieved, they also receive an education pack advising how to speak to people who are hard of hearing.
“It gives tips like ‘don’t turn your back when speaking, have your face in the light, have large font menus, and don’t yell. We also provide a seating map showing quieter spots,” Drexler explains.
Restaurants that have been accredited are seeing peaks in numbers, she adds.
In 2023 Drexler did a presentation on 20 ways to find a quiet restaurant for the CICADA (Cochlear Implant Club and Advisory Association) Australia volunteer organisation to support cochlear implant patients and she is now on its committee due to her passion for helping people with hearing loss have better dining out experiences.
Tips include not going on the main strip where most restaurants are as they’re normally busy because they have high rent.
“Reasons some restaurants are louder include the louder the music is,
wheelchairs, with walkers or vestibular disorders.
Drexler’s goal is for Ambient Menu to be in every state in Australia and become a household name. She is always looking out for more audiologists and audiometrists to become Ear Buds and do detailed reviews.
Image: Flinders University.
Proudly showing her Ambient Menu banner.
A family affair. Laura Drexler with her husband Andy and son Michael, who help in the business, at Flinders University’s Early Career Alumni Award ceremony in 2023.
Sage advice from a 40-year veteran
This year marks four decades of practising for audiologist DIRK DE MOORE including 30 years in the rural Victorian city of Bendigo. He says being the first Australian audiologist to achieve an MBA has given him a slightly different view. He provides valuable advice for practitioners starting out and others more advanced.
When people google Bendigo Hearing Clinic and land on its website they are not greeted with photos of hearing aids or people having hearing tests. Instead, they see the owner Mr Dirk de Moore in his golfing gear with his golfclubs, and a large photo of his big-eared kelpie Nala at home in the garden.
The caption for de Moore's photo says he is “a golfing enthusiast, Blues (Carlton football club) supporter and your audiologist”.
Photos of happy patients pictured doing what they love also feature on the home page website gallery but still not a hearing aid in sight even though all wear hearing aids. There’s farmer Frank, a lamb producer and Collingwood Aussie Rules supporter; Ian, a pharmacist and winegrower pictured in his vineyard; motoring enthusiast and Geelong Cats supporter John; and bank manager and mum Maree.
Penny, a receptionist and horticulturalist, is holding secateurs in her garden while de Moore's mum Eileen, a retired music teacher and church organist, is also featured.
‘’There’s still stigma about hearing aids and it annoys me when you look at some audiology websites and I think they couldn’t have chosen a more unattractive photo of a hearing aid,” de Moore says. “Consumers don’t wake up and say, 'I think I might buy some hearing aids today'; there’s still a long lag time, about seven years before action.
“I know a lot about my patients, who they barrack for, what dogs they’ve got, what type of farm they have, their interests and so on. Our appointments are filled with chat and I think that patients enjoy that relationship.
“I would encourage audiologists, rather than using stock images on their websites, to show photos of real people enjoying doing what they love to
do, of course aided by better hearing.”
To further spread the hearing health message, de Moore has written 10 articles educating the public about hearing for a local magazine featuring his tagline ‘Life Amplified’.
After completing a science degree at the University of Melbourne, he went on to study audiology and graduated as an audiologist in 1983. He then spent his first 10 years working at what was then the largest employer, the National Acoustic Laboratory, now known as Hearing Australia. He worked with adults with severe to profound hearing problems before moving to manage one of the organisation’s major Melbourne clinics.
Simultaneously de Moore embarked on studying an MBA which involved taking a year off work to study full-time. “It was hard but I learned so much about marketing and strategy, and it made me question what I was really trying to achieve,” he recalls.
Work life balance
The idea of working in a rural hospital was appealing as he thought he could also start a private practice on the side so he took a role as senior audiologist at Bendigo hospital and moved to rural Victoria, a decision he has never regretted.
“I encourage people who want to start private practice to consider having some form of regular income or cash flow, and on the side to gradually open a private practice and develop it,” de Moore says. “There’s that classic thing you hear in business of being so busy that you can’t work on your business because you’re too busy working in your business. There are choices, options available in private practice but many don’t strategically think about them.
Audiologist and keen golfer Dirk de Moore balances life with work.
Images: Bendigo Hearing Clinic.
“You can live really well in a regional area, however, and I would encourage young audiologists to give it a go.”
The hospital work involved a lot of diagnostic work servicing the GP community but also included a large paediatric load, many children with middle ear infections, and auditory brainstem testing for suspected tumours. “There was a huge paediatric demand, and there still is in regional areas in hospitals. It was a great environment,” he recalls.
After working at the hospital for eight years, de Moore had built his private practice sufficiently to practise there full-time. He was the only audiologist in private practice in Bendigo, as others worked for the government’s Australian Hearing clinics.
Technology has had a huge impact on changing audiology over the 40 years he has practised. He has seen vast improvement in electronics, hearing aid sizes and aesthetics with more power, recharging abilities and Bluetooth connectivity that links to phones , as well as expanded scope-of-practice.
“There’s also a trend towards people embracing newer technology –baby boomers are very accepting of the technology as they need it to perform in the workforce and multifunctionality of devices increases acceptance,” he adds.
Tips for graduates and independents
When audiologists graduate these days, there’s a broad range of options for employment, de Moore says.
“Major retail outlets, private practice, research or working for a
“There’s that classic thing you hear in business of being so busy that you can’t work on your business because you’re too busy working in your business. There are choices, options available in private practice but many don’t strategically think about them.”
Dirk de Moore
manufacturer,” he says. “One thing I always told audiology students when I lectured for many years at The University of Melbourne was, ‘you might be just thinking about passing this course and getting a job but if I was your age I would consider working in Switzerland or maybe the US.' I know many people who’ve had successful international careers with overseas based hearing aid companies.
“Another tip I always give new graduates is talk to people who are more advanced in the profession than you because there’s a wealth of wisdom there,” he says.
“If you’re talking to people 20 to 30 years in, they’ve been where you are going so listening to them and taking their advice is sensible. Also try to move around in the first few years to get a broad base of experience and a feel for what you’re passionate about. Some people are just not cut out to be in private business.
“My main advice for independents in private practice is to be more strategic. Stand back and write out the things you can do in private practice such as the government work, NDIS, WorkSafe, wax removal, then decide what you do and don’t want to do. Obviously, you need to do things that will enable you to be profitable enough to stay in business but it’s interesting to think about what you are passionate about and what you enjoy most and try to choose those options.”
While 85% of his revenue comes from private hearing aid sales through a large private clientele, de Moore does a small amount of industrial screening, ear plugs and wax removal.
“I don’t do government work because I did that for 27 years. I’m 64 now and I want to play golf twice a week and work 20 to 22 hours and as long as I can maintain that and stay financially viable, it’s a great lifestyle and really good work life balance. I think I can continue working until I’m maybe 70 at this pace," he says.
“I love the work, I’m passionate about it. I have a great relationship with my patients and many of them I’ve looked after for 30 years because I’ve been in private practice in Bendigo for 30 years now.
"Finally, I feel very privileged to have worked for so long in this profession. Almost all audiologists I know are intelligent, ethical and highly professional people working to improve the quality of life of their fellow Australians.”
Lamb producer, Collingwood supporter and hearing aid wearer, Frank.
Receptionist, horticulturalist and hearing aid wearer, Penny.
Dirk de Moore has more time for his dog Nala due to his flexible lifestyle.
The heat was on at ACAud’s Cairns congress
The Australian College of Audiology’s national congress took place in Cairns and featured thought leaders, researchers and practitioners alongside some intriguing presentations.
More than 840 people travelled from around Australia and the world to attend the Australian College of Audiology’s National Congress ACAud 2024 in Cairns. The theme was ‘The heat is on – Sustaining audiology in a changing climate’.
The congress, at Cairns Convention Centre from May 8 to 10, aimed to help audiology practitioners learn how to navigate sweeping changes impacting the industry in a world that is experiencing profound shifts due to environmental, technological and societal changes.
ACAud said the field of audiology was not exempt from their impact and the program was designed to equip practitioners with the knowledge and skills needed to sustain audiology practice amidst change. Discussions ranged
Rushworth said attendees were treated to a series of insightful presentations by national and international speakers sparking rich discussions and invaluable networking opportunities.
Thought leaders, researchers and practitioners spanning various fields shared insights, strategies and best practices for navigating challenges ahead through plenary and keynote presentations, workshops and masterclasses.
The dedicated day of hands-on learning through interactive workshops provided participants with practical real-world experience, enhancing their professional skills and knowledge, Rushworth said.
“The congress posted a full trade show which was a standout feature showcasing the latest advancements in audiology technology,” she added. “Delegates had the unique opportunity to explore cutting edge innovations and interact with industry leaders.”
One presentation which made a lasting impression on delegates was the inspiring story of Ms Sophie Li who signs and uses cochlear implants. Li is the daughter of Australian ballet dancer Mary McKendry and Li Cunxin, the
world-famous ballet dancer whose autobiography made into a movie.
Rushworth said three unforgettable social events added to the excitement including a traditional smoking ceremony and a welcome cocktail function.
‘’The grand finale was a spectacular gala ball at Fogerty Park complete with a dazzling firework display and a mesmerising performance by a fire artist,” she said. “This stunning evening under the stars left a lasting impression on all who attended making the ACAud 2024 National Congress a standout event of the year.”
Keynote speakers included Professor Anu Sharma PhD, Professor Grant Searchfield and Mr Andrew Bellavia. Prof Sharma is associate chair in the Department of Speech, Language and Hearing Science and Fellow in the Institute of Cognitive Science and the Centre for Neuroscience at the University of Colorado, Boulder. Her research examines neuroplasticity in children and adults with hearing loss who receive hearing aids or cochlear implants.
Prof Searchfield is head of the University of Auckland’s audiology section and deputy director of the Eisdell Moore Centre for hearing and balance research. His research focus is cognitive processes involved in tinnitus perception and innovative technology for management of hearing loss and tinnitus. Bellavia from America is the founder of AuraFuturity hearing and hearables market and branding consultancy and co-host of This Week in Hearing podcast.
The congress was the last official event for former CEO Ms Jane Hedger whose last day with ACAud was on 10 May 2024. She started in her new role on 27 May as CEO of Volunteering Queensland.
Members of the Hearing Aid Audiology Society of Australia (HAASA), which has merged with ACAud, received up to 15.5 CPED points, ACAud members received up to 30 CPD points and Audiology Australia members received nine points.
Opposite top: The finale at the gala ball featured a mesmerising performance by a fire artist, in keeping with the congress theme, The heat is on.
Opposite bottom, left to right: The auditorium was packed for the plenary speakers; The Australian College of Audiology board.
Top, left to right: The gala ball was a big hit; Happy delegates and industry representatives at the trade expo.
Above, left to right: Getting hands-on with an interesting exhibit; Melbourne audiometrist Daniel Pistritto meets Mr Croc, another popular exhibit; Speakers were thanked for their high calibre presentations. Nicky Chong-White (from left), Andrew Bellavia, Jessica Vitkovic, Jaime Leigh, Prof Nerina Scarinci, Prof Anu Sharma, Dr Caitlin Barr, A/Prof Melanie Ferguson, Prof Julia Sarant.
Below: The sponsors preparing to try out their boomerangs. Phonak's Cameron Sinclair (from left), Dawn Rollings (Starkey), McCoy Harvey (Oticon), Brenton Comerford (Unitron) Brad McConville (Bernafon), Paul Jones (GN) and Nick Taylor (Specsavers).
Largest Sound Exchange in history
Australia’s biennial event is a highlight on the CPD calendar, and this year featured five masterclass streams across two days of hands-on learning, workshops, and panel sessions in Melbourne.
Audiologists from around Australia learned new skills to put into clinical practice at Audiology Australia’s biennial event, The Sound Exchange ’24 in Melbourne in May.
The Sound Exchange ‘24, the most sold-out iteration of the event in history, kicked off at the Pullman Melbourne Albert Park with optional pre-conference workshops on 26 May and ended on 28 May. An industry expo featuring 25 exhibitors was also the largest exhibition in the history of The Sound Exchange.
Audiology Australia (AudA) president Dr Barbra Timmer said that overall, more than 600 people attended including delegates, sponsors, exhibitors, speakers, manufacturers who set up work stations in the masterclass streams and audiologist student volunteers.
“The Sound Exchange is wonderful because it’s a series of masterclasses where delegates get to, as a team of audiologists, delve deep into topics,” she said. “The beauty of The Sound Exchange is that it provides hands-on, interactive clinical advice and tips that people can take back to their clinics and put into practise.”
Five masterclass streams of immersive two-day workshops, lectures and panel sessions aimed to equip attendees with new knowledge and skills. Dr Timmer said the topics were chosen after being identified as ‘hot topics’ from member feedback.
The masterclass themes were the management of chronic conductive hearing loss in adults; the 5-Step Plan for Holistic Hearing Rehabilitation; community paediatrics – behavioural assessment of children aged eight months to six years; vestibular boot camp; and cochlear implants, maximising auditory potential across the lifespan.
Attending her first AudA conference as its new CEO, Ms Leanne Emerson said it was a fantastic turnout.
“The Sound Exchange has a strong practical focus. Delegates participated in workshops rather than lectures and got to touch, feel, experience some of the skills that our presenters took them through so hopefully they went away with something practical they can take back to their businesses,” she said.
“Learning is done best where people have an experience of it.
"Immersive-style learning tends to ‘stick’ to be more enduring so that means participants go away with some concrete skills they can apply to their practise.
“We also had terrific support for the expo from companies and
manufacturers, providing important touchpoints on products and services. We are truly appreciative of their support and the support of our sponsors.”
At a welcome reception, Emerson announced that AudA’s national conference next year would be in Adelaide from 1-4 April 2025.
She also thanked staff, volunteers, stream leads and delegates for bringing the event together and thanked the event’s platinum sponsor Cochlear, gold partner Phonak and silver partners Starkey and Unitron.
Members of the Ethics Review Committee (ERC), which hear and investigate complaints for AudA and the Australian College of Audiology incorporating Hearing Aid Audiology Society of Australia, attended to increase awareness among practitioners of the important role the committee plays and how it can help manage complaints and concerns. The ERC has guidance and advice on its website to help clinicians resolve and understand issues including answers to questions they are often asked.
As it was National Reconciliation Week, AudA staff and volunteers wore T-shirts at the event featuring artwork from Indigenous artist Bitja (Dixon Patten) who AudA commissioned to create art for its Reflect Reconciliation Action Plan. The plan aims to elevate awareness about Aboriginal and Torres Strait Islander hearing health and improve access to culturally inclusive and appropriate hearing services.
Images: Prime Creative Media.
The 5-Step Plan for Holistic Hearing Rehabilitation session was a sell out as were other sessions.
Audiology
Delegates benefitted from interactive, hands-on workshops that challenged them to think about new insights they could take into their daily practise.
ANOTHER OPTION FOR THE HEARING HEALTH WORKFORCE
CHEDY KALACH explains why the hearing industry’s newest training organisation, the Australasian College of Audiometry, has launched and the role it will have in educating the future audiometry workforce.
SOME ARE ASKING IF THIS POTENTIAL INCREASE IN AUDIOMETRISTS WILL AFFECT AUDIOLOGISTS AND THE PUBLIC NEGATIVELY. THE ANSWER IS, “NO, AUDIOMETRISTS WILL NOT TAKE THE PLACE OF AUDIOLOGISTS.
CHEDY KALACH
You may have heard that there is another option for training in the hearing health sector.
Firstly, yes, a new 100% Australian independently owned small business has hit the audiological industry offering nationally recognised training for audiometry. The Australasian College of Audiometry (AuCA), a subsidiary of ACOD Pty Ltd (RTO Code: 45068), launched in January 2024 and aims to provide a high standard of education in audiometry.
AuCA maintains its independence and commitment to excellence and is not affiliated or in partnership with any other corporations thereby guaranteeing an unbiased educational experience for all its students.
AuCA undergoes regular audits by the Australian Skills Quality Authority (ASQA) and is an active member of the Independent Tertiary Education Council Australia (ITECA). Membership to ITECA is only available to high quality independently owned colleges. Launching this year means the course content is current and updated with the objective to help students become work-ready.
Secondly, some are asking if this potential increase in audiometrists will affect audiologists and the public negatively? The answer is: “No, audiometrists will not take the place of audiologists.”
The various universities that do a great
Government statistics show there is a shortage throughout Australia except for metropolitan Brisbane . Having audiometrists in a flexible college where they can study online at their own pace, from anywhere, will help fill the shortage, particularly in regional Australia, again to work alongside audiologists.
Would you rather a well-trained dental hygienist with great people skills who fits into your practice’s culture and work ethic or a dentist who has the technical skills but poor ‘soft skills'? Both can perform the same basic tasks but the experience with the hygienist will be more pleasant. Obviously, the hygienist has a limited scope-of-practice and will need to refer to the dentist for certain tasks. Similarly, a well-trained audiometrist will be an asset to your practice and profession. It’s all about the person and how they work within your practice.
Traditionally, the only option for training in audiometry was with TAFE in NSW. Now, AuCA gives another option with local face-to-face workshops (in many capital cities) and the customer service that can only be achieved by an agile family-owned business.
ACOD Pty Ltd was developed from frustrations within the vocational education sectors. The directors were continuously approached by various clients requesting a flexible agile course delivery and questions about why the course was being delivered a certain way. Working in the public system, they would receive responses such as "this is the product we are offering, so we can’t change it for them". In other words, they regularly saw students and employers not being offered a customised program for their needs.
Hence, the birth of ACOD in 2017 and the expansion of AuCA. AuCA’s main objective is to offer high level, affordable training, placing the student at the centre and regularly asking what would you want if you were the student or the employer? The directors are not and do not claim to be experts in the audiology profession but pride themselves on putting the customer first and have been in the vocational education sector for decades.
AuCA consists of a great team of audiologists who developed the materials and deliver a course focusing on the needs for future audiometrists. The audiologists have a vast range of experience from occupational noise to paediatric rehabilitation. They include relatively new audiologists and PhD audiologists. This ensures AuCA has knowledge of the profession that only comes from experience and modern trends within industry. All staff share the same student-centred passion for high quality work-ready graduates. In addition to our wonderful audiologists, AuCA has invested in an exceptional general manager to help lead the team and various projects, Ms Heather Joseph. She comes with experience from owning various businesses and has a graduate certificate in business management specialising in project relationship management.
It is commonly known – at least within the audiological profession – that hearing loss is one of the leading treatable risk factors for dementia. We know dementia in Australia is on the rise particularly with our aging population. Audiological services and the need for hearing healthcare professionals will soon be a huge growth industry. Furthermore, how can we increase the public perception of hearing loss and raise awareness without increasing the audiological market? We will need qualified audiometrists to help audiologists support this increased demand.
REFERENCES:
1. Data from Jobs and Skills Australia https://www. jobsandskills.gov.au/data/skills-shortages-analysis/ skills-priority-list?code=252711
2. Hearing Australia - https://www. hearing.com.au/news-and-articles/ the-link-between-hearing-loss-and-dementia/?gclid=CjwKCAjwxLKxBhA7EiwAXO0R0BcfhNqNCurvxR4NQPCV-n1hkjHoqGSP-ubIO5O7Z2nHSCGRlv0NwBoC2gsQAvD_BwE
ABOUT THE AUTHOR: Chedy Kalach is director of The Australasian College of Audiometry (AuCA), the hearing industry’s newest training organisation. The college was established by the founders of Australia’s largest trainer of optical dispensers, the Australasian College of Optical Dispensing (ACOD). Contact him via chedy.auca@edu.au.
BELOW: AuCA staff
(from left), audiologist
Annemaree Daley, education support leader
Jessica Wagenfeld, director Chedy Kalach, general manager
Heather Joseph and audiologist Lian Gijo.
CASE NOTES ARE EVERYTHING
WESLEY ONG is a tech-savvy Queensland audiologist who hosted a recent webinar sharing tips about clinical use of AI in audiology including outsourcing paperwork. He says AI medical scribes can dramatically reduce the amount of time spent on paperwork.
IT’S AMAZING TO THINK AN AI PLATFORM CAN LIVE IN THE MOMENT WITH YOU AND YOUR PATIENT DURING AN APPOINTMENT SO WHEN YOU ASK IT TO WRITE A REPORT, OR OUTLINE PLANS, IT CAN PRODUCE THAT WITH FLAWLESS MEMORY.
Over your career as an audiologist, how many technological breakthroughs have changed the way you perform your day-to-day clinical tasks?
I’ve been a clinician working in rehabilitation since 2010. Over the past 13 to 14 years of my audiological infancy, I’ve lived through: oving from using a pen to typing my clinical case notes.
• Programming hearing aids wirelessly.
• The introduction of telehealth and remote programming – something that was prophesised for years to change the way we deliver service.
Furthermore, many clinicians have been practising longer than I have been alive. They have seen many more changes, advancements and evolution within our industry. I will forever be hearing fables of the “trim pot”.
All these advancements have made our lives easier, faster or simpler in one way or another, ultimately impacting the outcomes of our clients. And although one single technology has not made a “quantum leap” in how we practise, each decade of the technology we use is remarkably different from the next. Yet from what I understand of our audiological heritage, some things remain surprisingly the same. We perform Hughson-Westlake procedure on a machine, program hearing aids, counsel patients and barely have enough time to do our notes.
Artificial intelligence is one of those buzz terms that has also been prophesised to change our lives. We are living in a pivotal moment in our society where this technology is being defined in how we use it now and into the future. And as this becomes reality, it is scary how powerful it really is. If you haven’t mucked around with ChatGPT yet, don’t worry, you will soon. In the not-too-distant past, “Googling” a simple daily life question seemed to be amusing – it is now common practice in our lives, across cultures and generations. You’re either an early adopter using AI now, or you’re going to be adopting it very soon. It will take conscious and deliberate effort to avoid it.
Like many of you, I pour my heart and energy into listening and engaging with my clients. However, while trying to listen and interact, my eyes are darting back and forth between my screen and my client’s eyes whilst my fingers are bashing my keyboard in a lunatic fashion. If I decide to do this at the end of the appointment, or at the end of the day, my memory only maintains so much. I only have enough time and energy to write down key notes and some items simply don’t make it onto the record at all. And what if my time and energy is so low that it doesn’t get done at all? Items forget to be actioned, key goals and important clinical knowledge vanishes and ultimately, the client is the one who suffers due to poor clinical practice. We can all agree that case notes are boring but case notes are everything.
There are various AI powered speech to text or medical scribes for healthcare professionals. Heidi Health is one. It is an Australian-built AI platform built by doctors for doctors and health professionals. I was sceptical about the ability of technology like this to streamline the patient journey. It was a Friday night as I lay in bed with the platform running on my phone. I convinced my wife to role-play the dialogue of a typical audiology appointment. What unfolded in front of my eyes took my breath away.
Every detail of case history, client goals and assessment presented in a concise, professional format with impeccable accuracy.
I took it to work on Monday and it delivered in the real world as well and saved hours each week on case notes, capturing more detail and accuracy than before. It’s scarily easy to use too by just hitting record.
It’s amazing to think an AI platform can live in the moment with you and your patient during an appointment so when you ask it to write a report, list COSI goals or outline future plans, it can produce that with flawless memory. You can build templates, get templates built for you on documents you’ve created previously while also meeting the Australian Privacy Principles and satisfying Hearing Services Program requirements.
There are only two things in my life that have changed something I do every day in such a profound way. The first is a bidet and the second is using an AI platform that takes clinical notes and arranges them for me.
ABOUT THE AUTHOR: Wesley Ong is a previous executive of Independent Audiologists Australia, previous president of EARS Incorporated and the director/founder of Fidelity Hearing Centre in Redland, Queensland. Ears Incorporated is an Australian, not-for-profit organisation focusing on increasing access to hearing care by training health workers and educators in developing countries.
ABOVE: The AI medical scribe allows the audiologist to remain fully engaged with the patient.
Image:
WESLEY ONG
Image: Wesley Ong
EVENTS CALENDAR
To list an event in our calender, email editor, helen.carter@primecreative.com.au
JUNE 2024
COCHLEAR AND AUDIOLOGY AUSTRALIA
Continuum of care perspectives on cochlear implants for adults CPD event 12 June – Shanikas Berwick, Australia 17 June – The Ville Resort, Townsville, Australia audiology.asn.au
EAR HEALTH COURSES
Cerumen management 101 14 June – Macquarie University 17 June – live online 22 June – University of Melbourne earhealthcourses.com.au
PARENT PARTNERSHIPS FOR DEAF CHILDREN
Promoting parent partnerships for children who are deaf or hard of hearing 6 June – Coaching families from diverse backgrounds Online
Nextsense.org.au
JULY 2024
HEARING BUSINESS ALLIANCE Strategies for business success seminar Perth, Australia 31 July hearbusiness.com.au
AUGUST 2024
OMOZ (OTITIS MEDIA AUSTRALIA) 2024
Newcastle, Australia 27-30 August Omoz.com.au
EAR HEALTH COURSE
Cerumen management 101 24 August Flinders University, Adelaide. earhealthcourses.com.au
PARENT PARTNERSHIPS FOR DEAF CHILDREN
Promoting parent partnerships for children who are deaf or hard of hearing 8 August – Bringing it all together Online Nextsense.org.au
SEPTEMBER 2024
36TH WCA WORLD CONGRESS OF AUDIOLOGY 19-22 September 2024 Paris, France wca2024paris.com
OCTOBER 2024
NEXTSENSE AUDIOLOGY MASTERCLASS
Vestibular function and balance performance in children with sensorineural hearing loss 23 October Online
Nextsense.org.au
DECEMBER 2024
NEXTSENSE
Day of learning for itinerant teachers of the deaf at the Australian Hearing Hub 6 December Macquarie University Nextsense.org.au
American audiologist Dr Cliff Olson will speak at Hearing Business Alliance’s one day seminar in Perth in July about a business opportunity for HBA members.
Image: Cliff Olson.
Image: Taras
OMOZ 2024 will be at Newcastle City Hall from 27-30 August.
Ear Health Courses will run cerumen management courses nationwide in June and August.
SOAPBOX
LIFE AFTER DEAF
The time has arrived for society to acknowledge the humanity and dignity of people with hearing loss.
Reflecting now, I ponder how many of my perceived 'behavioural issues' during high school stemmed from my struggle to hear adequately.
Later, when I began working, I did all I could to keep my hearing loss hidden including using a hearing aid disguised to look like glasses. I look back on the mistakes I made trying to hide my hearing difficulties and realise the only person I was fooling was myself.
a teenager and suffered total loss of hearing in my left ear as a young adult due to stapedectomy complications. My experiences and struggles with hearing loss led me to pursue a career as a hearing care professional and I now share my experiences through my personal blog 'Talking Hearing Loss' and on my LinkedIn profile. My mission is to break the stigma surrounding hearing loss and help those impacted by loss of hearing to find 'Life after Deaf'.
As an audiometrist who has traversed the labyrinth of life with hearing loss as my constant companion, I am compelled to illuminate the often-overlooked hurdles faced by individuals with auditory impairments. Living with hearing loss transcends difficulty in hearing; it entails manoeuvring through a world that frequently overlooks your needs and fails to grasp your experiences.
From tender years, I grappled with the barriers and misconceptions enveloping hearing loss. Mundane tasks such as deciphering conversations in bustling environments or tuning into television programs morphed into daunting challenges. Society's lack of awareness and empathy compounded these difficulties.
The dread of standing out as 'different' or becoming a target for ridicule in school compelled me to shun hearing aids. Growing up with a parent who lost their hearing during adolescence and was encouraged to conceal their impairment and hearing aids from society, I knew no alternative.
Despite remarkable technological strides, misconceptions and stigma continue to shroud hearing aids and cochlear implants. Many perceive them as emblems of frailty or senility rather than life-changing tools that enable us to fully engage with the world.
I, too, grappled with this perception. I loathed my hearing loss and detested the arduous endeavour of concealing my disability to blend in with societal norms. The fear of being perceived as feeble or equated with the elderly stifled my willingness to seek assistance. This stigma deters countless individuals from seeking the support they require, depriving them of the opportunity to reconnect with loved ones and pursue passions.
The pervasive lack of accessibility in our communities further isolates people with hearing loss. Public spaces often lack essential accommodations such as captioning or hearing loop systems, rendering it arduous for us to fully participate in social and cultural endeavours. Even basic communication poses a challenge when others are oblivious to effective communication strategies with individuals with hearing loss.
By the time I started work, my hearing had deteriorated to the point that I could not ignore it. Every day was a struggle, just trying to understand what was being said around me.
Often in meetings I would miss key things that were discussed so when I gave input or asked a question, I would be told that question had been asked, the issue had been covered or my question was irrelevant. I quickly learnt it was easier for me to keep quiet and not contribute. People interpreted this as me being introverted, anti-social and not having a good work attitude. It can be difficult to raise with your employer that you need special
accommodations but I felt they did not understand what hearing loss meant which made it harder to get the help I needed. My self-esteem dropped to an all-time low; I was constantly depressed at work and became irritable about the smallest things. My self-worth was so low I could see no way out.
The most profound obstacle is the emotional toll of feeling isolated and misunderstood. Envision continually advocating for your needs, explaining why you can't hear well, or enduring the exasperation of being sidelined in conversations. It’s a draining, disheartening, and profoundly unfair ordeal.
The time has arrived for society to acknowledge the humanity and dignity of people with hearing loss. We must endeavour for heightened empathy, comprehension, and inclusivity across all spheres of life. This necessitates acquainting ourselves with the intricacies of hearing loss, challenging stereotypes and fervently advocating for accessible environments and accommodations.
Let us shatter the silence enveloping hearing loss and amplify the voices of those who have languished in the margins for too long. By cultivating a culture of empathy and understanding, we can fashion a world where every individual, irrespective of their hearing ability, is esteemed, respected, and embraced.
Name: Daniel Pistritto
Affiliations: Connect Hearing, Carlton
Location: Melbourne, Australia
Years in industry: 10
“MANY PERCEIVE HEARING-AIDS AND COCHLEAR IMPLANTS AS EMBLEMS OF FRAILTY OR SENILITY, RATHER THAN LIFE-CHANGING TOOLS THAT ENABLE US TO FULLY ENGAGE WITH THE WORLD.”