Hearing Practitioner Australia October/ November 2024
It’s official, Specsavers has been named one of the Best Workplaces in Australia for the second year in a row by Great Place to Work®, the global authority on workplace culture. What makes us the best? It’s our commitment to our peoplemaking sure we are a place where everyone feels welcomed, valued and proud to belong. Where our people can come to work and make a difference every day. Find out more about what makes us one of the best at audiology-anz.com.au/
FIRST AUSTRALIAN CHILD TO RECEIVE GENE THERAPY FOR DEAFNESS IN PIONEERING TRIAL; TWO MORE WAITING
the hearing nerve.
Prof Birman, a Clinical Professor at Sydney University and Macquarie University, delivered the intra-cochlear injection of the therapy called SENS-501 and reported initial positive safety results for the patient.
“I am very excited to participate in this groundbreaking gene therapy trial that may have the potential to transform the lives of the babies carrying the OTOF gene mutation,” she said.
“The surgery was well tolerated by the patient and no safety signals were reported. From early observations, changes in the child’s behaviour and vocalisations were noted.
“I am grateful to the family of the first patient to receive the gene therapy for placing their trust
in this innovative approach and potentially paving the way for the use of gene therapies in the aid of hearing loss. I am looking forward to following the progress of the first patient in the follow-up period and further recruitment of patients in (the) Audiogene (trial) assessing SENS-501 efficacy.”
The infant is one of, if not the, first
NEW INDEPENDENT CONDUCT AND COMPLAINTS BODY LAUNCHED FOR HEARING PRACTITIONERS
A new independent organisation to promote ethical hearing service practice and handle complaints against audiologists and audiometrists is in force from 1 October 2024.
The Hearing Professional Conduct and Complaints Body Ltd (HPCCB) is the culmination of years of work and replaces the previous AudA and ACAud Inc. HAASA Ethics Review Committees (ERCs).
“It will also handle complaints regarding the provision of hearing services by audiologists and audiometrists who are members and/or clinically certified by the Australian College of Audiology (ACAud) Inc. HAASA and Audiology Australia (AudA),” she said.
“Since the first joint Ethics Review Committees in 2018, AudA and ACAud Inc. HAASA have been committed to creating a single independent entity for the handling of complaints.
“The establishment of the HPCCB is the culmination of years of work between the professional bodies and ERCs to determine the best
model for the separate entity.”
Hewat said the independent body would further increase the consistency of the management and investigation of breaches of the Code of Conduct and the provision of ethical and professional guidance.
The Code of Conduct for audiologists and audiometrists sets the professional and ethical standards that members and/or clinically certified audiologists and audiometrists must meet.
Former ERCs chairperson and now HPCCB chairperson, Ms Claire Hewat, said the new body would promote ethical hearing service practice to audiologists, audiometrists, members of the public and others. continued page 8
Members of Audiology Australia (AudA) and the Australian College of Audiology (ACAud) Inc. HAASA must display, or make available, a summary of the Code of Conduct
in the world to receive this gene therapy from French biotechnology company Sensorion. At least seven other children from China, the UK and the US have received gene therapy from other companies for the same type of deafness with a conference told earlier this year that they had hearing restored, "marking a new era in deafness treatment".
“Currently in the pre-clinical research phase, this gene therapy program represents significant hope for families affected by this rare form of genetic deafness,” Sensorion said, adding it had “the potential to dramatically improve the quality of life of patients with genetic deafness.”
Sensorion said SENS-501 (OTOF-GT) was developed to treat
The Passe & Williams Foundation has funded $85 million of ENT research and clinical practice in Australia and New Zealand over three decades including the EarGenie to improve paediatric hearing tests. page 38
Sydney ENT surgeon Professor Catherine Birman OAM performed the procedure. Image: Royal Prince Alfred Hospital.
Image: Bionics Institute.
Nothing is smaller. Nothing sounds better.
INTRODUCING
The world’s smallest custom rechargeable hearing aid.
Personalised craftsmanship and industry-best sound in the smallest hearing aids possible.
Virtually invisible Transparent sound Custom fit for you
When size matters, why fit anything else?
Explore Signature Series:
IN THIS ISSUE
15
Hearing aids like a brain Patients and practitioners give their verdict on Starkey’s Genesis AI hearing aids.
18
21
Diversifying your practice
Cerumen removal and paediatric audiology are two ways audiologists can extend their services to better serve their communities, while also doubling as excellent practice building initiatives.
In this issue we talk to audiologists in practices across the country about why they started ear wax removal and what it brings to their clinics.
If Mr Sam Mitchell’s business in Perth is anything to go by, there is a major unmet need. He runs two clinics devoted solely to cerumen removal and they’re open seven days a week to keep up with demand.
Triumph of the human spirit Melbourne audiologist Yazdaneh Galt headed to The Oscars to see her story told in film.
He's among a host of audiologists who believe there should be Medicare and health insurance rebates for audiologists who perform the procedure, saying this would free up ENTs, enable patients to be seen in a timely manner and save patients money.
They argue audiologists should make cerumen removal 'their domain', given they are trained in ear pathology and look into ears day in, day out.
Audiologists offering cerumen removal discuss how they have made it work for their practice.
29
An inspiration
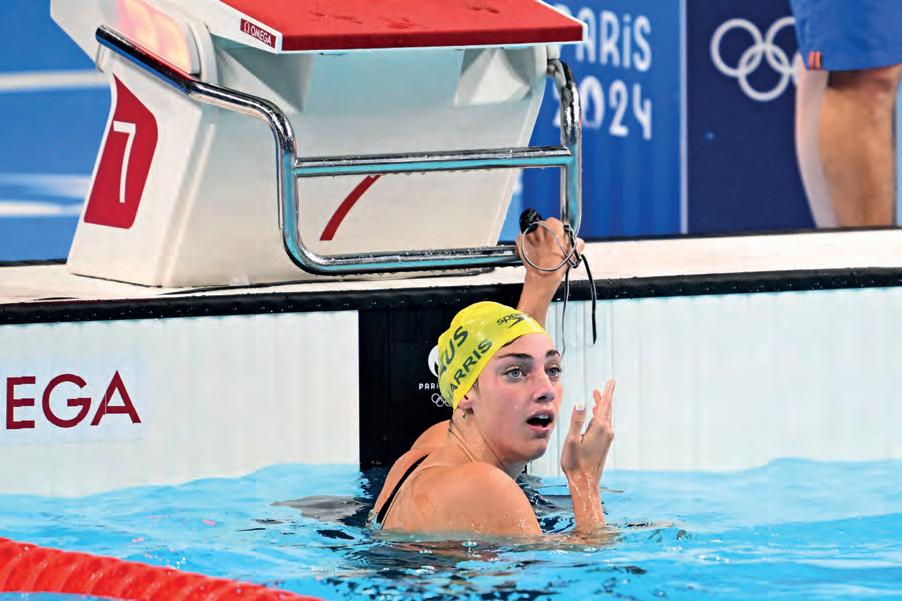
Hearing-impaired Olympic medallist Meg Harris took Paris by storm in the pool.
Audiology Australia has been lobbying for Medicare rebates for audiologists to perform cerumen removal for some time and says it will continue to do so.
Caring for children is another way audiologists can expand their practice and better meet the needs of their community. We talk to three paediatric audiologists in community and hospital settings and discover the exciting new EarGenie diagnostic headband which aims to be in practices within two years.
This edition, we continue to find inspirational people in the hearing field such as Melbourne audiologist Yazdaneh Galt. As a young mother who escaped domestic violence, she lived with her children in a women’s refuge several years after arriving from Iran. Her remarkable story has been transformed by her daughter into an award-winning film nominated for an Oscar and now streaming.
We were also delighted to tell the inspirational story of champion hearing-impaired swimmer Meg Harris after returning from the Paris Olympics with gold and silver.
There’s also a round-up of OMOZ 2024, an informative piece on skin cancers on ears and an explainer on dementia and hearing loss with three leading Australian experts who put the evidence into perspective.
HELEN CARTER Editor
Just as HPA went to print, the FEDERAL GOVERNMENT announced thousands of students studying health professions, including audiology, will receive a mental health boost via a new $6.7 million psychological distress training initiative. Australian-based global health promotion leader, Mental Health First Aid International (MHFAI), has created a new online Health Professional education program, with course material designed specifically for health professionals. Students studying audiology at six of Australia’s seven universities that offer audiology are eligible for the free
OFF THE BEATEN TRACK
UPFRONT STAT
Weird
Curtin University researchers have used state-of-the-art imaging to shed light on the hearing sensitivity of Australian’s fairy penguins and the danger of marine noise pollution. Supported by the WA Marine Science Institution’s Westport program, the study is the first to detail how they perceive sound in air and under water.
Wonderful
The first hearing-impaired Miss South Africa Mia Le Roux hopes to be a voice for inclusion. “We all have situations where we maybe feel we don’t belong, we might feel excluded, but we need to learn to have space for everyone,” she told SABC News Wits University Centre for Deaf Studies Associate Professor Claudine Storbeck said it was a wonderful opportunity to show that people are not disabled because they are Deaf.
Wacky
Barely audible to human ears, healthy soils produce a cacophony of sounds like an underground rave concert of bubble pops and clicks. Recordings by Flinders University microbial ecologist Dr Jake Robinson found tiny living animals create sounds as they move and interact with their environment. With 75% of the world’s soils degraded, underground species face a dire future without restoration but eco-acoustics is emerging as a tool to detect and monitor soil biodiversity and investigate ecosystems where almost 60% of the Earth’s species live.
online element of the training. IN OTHER NEWS, Macquarie University has officially welcomed its first World Health Organization (WHO) Collaborating Centre; the Macquarie University HEAR Centre in ear and hearing care. Directed by the university’s Professor of Audiology Catherine McMahon, the HEAR Centre is achieving its vision to be a world-leading research centre in hearing health through its new standing as a WHO Collaborating Centre. These centres are institutions that form an international collaborative network carrying out activities to support WHO programs. Among 80 people who attended the launch on 27 August were Dr Shelly Chadha, WHO technical lead (ear and hearing care) and Dr Huong Tran,
Skin cancers
About 10% of skin cancers occur on the outer ear and can progress into cancers in the ear. Page 32.
WHAT'S ON
THIS MONTH
AUDIOLOGY AUSTRALIA ONLINE CONFERENCE
24 - 25 October
Running over two half days, the live stream will be available to AudA members and non-members, as well as audiology students from AudA accredited universities. audiology.asn.au
director, Programmes for Disease Control, WHO Western Pacific. FINALLY, researchers have confirmed dizziness as an independent predicting factor for falls in older people for the first time, adding that a common cause is benign positional vertigo (BPV) where crystals in the inner ear’s balance system become dislodged. They said dizziness was not just a normal part of ageing but caused by specific diagnoses with various treatments and cures. Other common causes were orthostatic hypotension and vestibular migraine. Their meta-analysis found a conclusive link between older adults experiencing dizziness and a dramatically elevated risk of falling. The review of 29 studies and 103,000 participants was published in Age and Ageing NEXT MONTH COCHLEAR IMPLANTS FOR ADULTS
The Audiology Australia-endorsed event, The Continuum of Care: Perspectives on cochlear implants for adults, is taking place in Rockhampton, Queensland. portal.audiology.asn.au
The
THERAPY AIMS TO RESTORE NORMAL HEARING PROCESS
continued from page 3
congenital deafness linked to mutations in the OTOF gene which plays a key role in the transmission of auditory signals between the hair cells of the inner ear and the auditory nerve.
“Its aim is to restore hearing by introducing a functional copy of the OTOF gene directly into hair cells via viral vector technology,” it added. “By replacing the defective gene, this therapy aims to restore the normal process of converting sound into electrical signals, enabling patients to regain their hearing ability.”
Prof Birman injected the therapy into the round window in the inner ear under general anaesthetic using a system developed in partnership with the company EVEON, so the injected dose could be measured precisely and the inner ear structures preserved.
Partner company, The Institut Pasteur, said a gene could only enter inner ear cells if transported by a viral vector capable of crossing the cell membrane.
The adeno-associated virus (AAV) delivered the gene but as the gene was so big, it was divided into two DNA fragments each transported by an AAV, which were then assembled inside the inner ear cells.
Sensorion said its phase 1/2 clinical trial called Audiogene aimed to evaluate safety, tolerability and efficacy of the treatment in infants aged six to 31 months at the time of injection.
It said initial safety data indicated no serious or adverse events were detected after administration.
“The medical condition of the child (upper respiratory infection unrelated to SENS-501 injection) at the time of efficacy assessment (ABR month one) did not allow to get reliable hearing sensitivity,” Sensorion said.
“By targetting the early years of life, when auditory system plasticity is optimal, the therapy seeks to maximise the chances for children with pre-lingual hearing loss to acquire normal speech and language.”
TWO OTHER PATIENTS
Sensorion said two additional patients had been screened. It anticipated completion of the first cohort of three patients and publication of initial efficacy data by the end of 2024. Recruitment completion of the second cohort of three patients is planned by June 2025.
The study involves two cohorts of two doses, followed by an expansion cohort at the selected dose. While safety will be the primary endpoint for the dose escalation cohort, auditory brainstem response will be the primary efficacy endpoint of the dose expansion cohort.
Audiogene will also assess clinical safety, performance and usability of the administration device system.
Sensorion CEO, Ms Nawal Ouzren, said: “Sensorion is making tremendous progress across its hearing care franchise of innovative therapies for the restoration, prevention and treatment of hearing loss disorders. Notably, we have made significant advances in our gene
At least 80 Aust kids have OTOF gene mutations
At least 80 Australian children have been found to have OTOF gene mutations for auditory neuropathy, according to paediatrician and clinician/ scientist Associate Professor Valerie Sung from the Murdoch Children’s Research Institute. She said they were among 1,200 children on the Australian National Child Hearing Health Outcomes Registry (ANCHOR) to have gene testing. She is project lead of ANCHOR. A/Prof Sung revealed the information in a presentation to Canadian researchers on 23 September.
therapy clinical trial, Audiogene, for the restoration of hearing in very young patients born with severe to profound hearing loss caused by mutations in the gene encoding for otoferlin.
“This program received regulatory approval in January 2024, and we are today confident that we will have treated the first cohort of patients by year end 2024, with one patient already injected and two additional patients already screened. I am very thankful to the parents of these patients for their trust and to the study investigators participating in this study for their dedication.”
EXISTING COMPLAINTS WILL TRANSFER TO NEW BODY
continued from page 3
and inform clients of how they can make a complaint.
“Furthermore, the establishment of the HPCCB as a separate entity to AudA and ACAud Inc. HAASA reinforces the independence of the complaints handling process from the hearing professional bodies,” she added.
“It will also provide some administrative process improvements, as all matters will now be handled by the same body.
“Otherwise, the powers and approaches of the HPCCB in providing support and guidance and handling complaints will be identical to those under the ERCs.”
Hewat said that if practitioners had a
current matter open under the Ethics Review Committees there was nothing they needed to do.
“Your matter will be transferred over and handled from 1 October 2024 by the HPCCB,” she said.
The body operates according to its Constitution, the Complaints Management and Resolution Procedure By-law and related policies and guidelines.
Ms Sandra South continues with the organisation as its ethics officer.
Board members are chairperson Ms Claire Hewat, AudA nominees Ms Alison Jackson and Mr Bill Raymond, AcAud Inc. HAASA nominees Mr Dean Moore,
The therapy was developed under the RHU AUDINNOVE consortium comprising Sensorion, the Necker Enfants Malades Hospital, the Institut Pasteur, and the Fondation pour l’Audition. Ms Sharon Oliphant-King and Mr William Olayos, and community members Ms Helen Mikolaj and Mr Tim Benson.
Apart from the Code of Conduct, the new website also features details of how to make a complaint, sanctioned members and information for the public.
Additionally it has a section on guidance for practitioners which provides answers and guidance in response to some of the frequently asked questions asked by audiologists and audiometrists such as ‘Can I use testimonials?’ The body said it welcomed suggestions for new guidance topics.
The Australasian College of Audiometry (AuCA) has expanded to New Zealand marking the beginning of an exciting new chapter for the college. AuCA’s general manager Ms Heather Joseph said the NZ launch occurred at a New Zealand Audiological Society conference in August 2024 in Ōtautahi, Christchurch. “As an independently owned college offering a Diploma in Audiometry, we are keen to open the door for more individuals to enter the hearing industry and qualify to work as audiometrists, meeting the community’s needs,” she said. “With AuCA now offering face-to-face, in-person workshops in Auckland and multiple cities in Australia coupled with flexible, on-line learning and workshops, there is real opportunity for clinical administrative staff and assistants to upskill into a career as an audiometrist.”
COCHLEAR ANNIVERSARY
The Royal Prince Alfred Hospital in Sydney has celebrated 40 years since NSW’s first cochlear implant was implanted in Ms Sue Walters in 1984. She was also the world’s first person with a cochlear implant to make a phone call. Pioneering surgeon, Professor Bill Gibson AO, performed the surgery. Walters, who is president of CICADA, Prof Gibson, recipients, families and past and present colleagues celebrated at a commemorative event at the hospital on 16 August. They included cochlear implant biomedical engineer Dr Halit Sanli and Professor Diana Horvath AO, CEO at the hospital when the first cochlear implant was performed. Walters has since become an advocate and is president of CICADA charity and volunteer organisation dedicated to supporting hearing-impaired Australians who use cochlear implants.
DRUG TRIALS
A novel drug delivery system may prevent hearing damage during cancer treatment by transporting medications to the inner ear which protect it during chemotherapy. The chemotherapy drug cisplatin is a lifesaver for many with cancer but often causes hearing loss. University of Oklahoma researchers created a system that transports medications to the inner ear where they stand guard as cisplatin approaches. The medications block calcium, which damages the inner ear hair cells, or are antioxidants which protect hair cells and maintain the delicate homeostasis of the inner ear. The hydrogel drug delivery system is injected into the ear as a liquid and turns into a gel. Inside are nanoparticles that carry medications and slowly release them. Meanwhile scientists from Hannover Medical School Germany have developed drug-eluting implants they hope can treat idiopathic sudden sensorineural hearing loss. The elastic implant impregnated with the steroid dexamethasone delivers the drug into the inner ear.
STEROIDS NEEDED WITHIN A WEEK OF SUDDEN HEARING LOSS
People with sudden hearing loss who receive steroids within seven days are five times more likely to fully recover their hearing than those not given steroids, a new study shows.
It identified factors that predict full hearing recovery after a sudden drop in hearing, with the strongest predictor being steroid treatment within a week of sudden hearing decline. Clinician scientists from University College London Hospitals (UCLH) collaborated with 240 junior doctors and undertook the largest study of adults who were seen with sudden hearing loss across 76 hospitals in England and Wales.
Analysis found patients who received treatment within seven days were five times more likely to fully recover their hearing compared to those who were not given steroids, even after accounting for all other patient and hearing loss factors. Findings were reported on 5 September 2024 in JAMA Otolaryngology Head & Neck Surgery Alarmingly about 40% of the patients missed out on receiving treatment within this critical window. The team at the National Institute for Health and Care Research
UCLH Biomedical Research Centre found that only about 60 per cent of the patients were treated in the timeframe.
As a result, researchers developed an online tool based on data from the SeaSHeL (Sudden onset Sensorineural Hearing Loss) study that can predict the chance of full hearing recovery in adults presenting with the condition.
The Seashel recovery calculator, freely available online to clinicians, estimates the chance of full recovery based on key patient and disease factors; age, heart disease, dizziness, severity of hearing loss and whether steroid treatment has been given.
FDA APPROVES AIRPODS PRO2 AS HEARING AIDS AND HEARING TESTS
Apple has launched its new AirPods Pro 2, claiming the software-based earbuds can be used as a clinical-grade over-the-counter hearing aid for adults with perceived mild to moderate hearing loss.
On 12 September 2024, America’s Food and Drug Administration (FDA) authorised Apple’s Hearing Aid Feature (HAF) as the first over-the-counter (OTC) hearing aid software device.
Dr Michelle Tarver, acting director of the FDA’s Center for Devices and Radiological Health said: “Today’s marketing authorisation of an over-the-counter hearing aid software on a widely used consumer audio product is another step that advances availability, accessibility and acceptability of hearing support for adults with perceived mild to moderate hearing loss.”
Apple said, at the US launch on 9 September 2024, that it was providing the world’s first all-in-one hearing health experience featuring a clinically validated Hearing Test Feature, and a clinical OTC
Hearing Aid Feature.
“A personalised hearing profile from the Hearing Test seamlessly transforms AirPods Pro into a clinical-grade hearing aid. The AirPods use the results of your hearing test to make adjustments that help you hear voices and sounds around you,” Apple said. It said the HAF helped make access to hearing assistance easier than ever by boosting voices, media and phone calls so they were easier to hear.
It was intended for people aged 18 years or older with ‘perceived mild to moderate hearing loss’, Apple added, stating the capability was “clinically validated in a controlled, randomised study that evaluated the perceived benefit of the feature and its custom settings compared to an audiologist-assisted setup.”
Users can also set up the HAF with an audiogram created by a hearing health professional. The Hearing Test was developed using real world data and is based on pure-tone audiometry.
See a doctor or get to hospital for steroid treatment within a week of sudden hearing loss for the best chance of recovery. Image: The Little Hut/ stock.adobe.com.
Apple’s AirPods Pro2 can be used as hearing aids. Image: Apple.
WARNING ON BUTTON BATTERIES
Button batteries, which are used i n some hearing aids, can cause devastating injuries and death by their ingestion or insertion into the ear or nose, Australian researchers have found.
Showing members how to access
AUDIOLOGY AUSTRALIA SIMPLIFIES CPD PROCESS
Audiology Australia (AudA) has introduced changes to CPD requirements for members which simplify the professional development process by only having two categories and include a CPD dashboard to help members keep tally.
of eight CPD points in category one and a minimum of four points in category two. The remaining eight points can be gained across either CPD category as suited to individual professional development goals.
More information is available by downloading Audiology Australia’s CPD Handbook from its website.
batteries can be deadly if swallowed or inserted in the ear or nose. Image: suconeko. comugi/stock.adobe.com.
The batteries power household items including remote controls, watches, toys and some hearing aids. The study examined injuries from battery ingestion in children and found a combination of young age, button battery size and delayed diagnosis created a ‘perfect storm’ that increased the chance of severe injuries and death.
Their review of 217 studies included 439 children worldwide who had swallowed or inserted the batteries into the nose or ear and was published in the World Journal of Paediatrics on 22 August 2024.
It found the group most at risk for severe injury or death were children younger than two who swallowed a battery 20mm in diameter or more. These are small enough to be easily swallowed but not small enough to reliably pass through a child’s oesophagus. Smaller batteries can also cause injury and long-term complications.
The review found 26% of injuries from swallowing batteries were burns to the oesophagus and 23% were extremely severe injuries which included the battery burning a hole through the oesophagus into the trachea.
Audiology Australia
From 1 July 2024, members still need to earn a minimum 20 continuing professional development (CPD) points, but the process is easier with just two categories. Category one is development through listening to others and guided participation in activities. Category two is development through self-guided activities.
Minimum CPD requirements are also now in effect. Audiologists must earn a minimum
Audiologists can gain CPD by attending the 2025 Audiology Australia Conference in Adelaide from April 1-4, through live webinars, endorsed events or via more than 140 AudA online learning recordings available free for members at a time that suits them.
Members can also earn a point when completing a quiz after reading the organisation’s magazine. People can plan their CPD by searching the events calendar and online learning library. Tracking points is also easier with the new CPD dashboard accessed through the member hub which enables practitioners to see how they are performing against their requirements. Other new benefits this year include free confidential phone (1300 720 004) and email support for HR and employee relations advice.
PLAN TO BRING LENIRE FOR TINNITUS TO AUSTRALIA
Children who did not have the button battery removed within six hours were almost eight times more likely to die.
The most common initial symptoms of button battery swallowing were choking, difficulty feeding, coughing and, over time, vomiting and drooling.
Researchers called for industry to redesign button batteries as current standards only focus on child resistant packaging and product compartments.
CPD. Image: Supplied by Audiology Australia from Event Photos Australia. The device delivers mild pulses to the tongue’s surface.
Image: Eoin Holland for Neuromod Devices.
Neuromod Devices is planning to make its Lenire device available in Australia and would partner with audiologists and ENTs experienced in treating tinnitus, the company has confirmed.
The device sits in the mouth delivering mild pulses to the surface of the tongue to reduce symptoms and is accessed from healthcare professionals including audiologists and ENT surgeons. It soothes tinnitus by pairing tongue and sound stimulation to help people pay less attention to tinnitus in a type of dual mode stimulation called bimodal neuromodulation.
Mr Joe Roche, Neuromod Device’s head of communications, said the company was ‘aware of the high demand in Australia for Lenire.’ “We intend to make Lenire available in Australia in the near future to the nearly five million Australians living with tinnitus,” he told Hearing Practitioner Australia.
“Neuromod partners with audiologists, ENT surgeons and healthcare professionals with experience treating tinnitus patients. As tinnitus is a subjective condition that manifests in different ways on a per patient basis, extensive experience in treating tinnitus patients is essential.
“Lenire receives a high volume of inquiry from hearing care practitioners and people living with tinnitus in Australia. This is unsurprising as recent data suggests that an estimated 17% – 20% of Australians live with some form of tinnitus.”
Neuromod claimed it had clinically proven safety, efficacy and tolerability of the device through three clinical trials involving more than 600 tinnitus patients and real-world evidence. It claimed 91% of compliant patients in its second largest trial reported that symptoms had reduced from moderate to mild and continued to do so for at least a year after treatment.
Button
MEDCHEM SUPPORTS SNHL THERAPY
AUDIOLOGY-LED CLINICS VIABLE POST GROMMET SURGERY
Audiology-led follow-up clinics for post-grommet insertion are “a viable option” for most children who have the surgery, a Perth study shows.
The study in 93 children found the clinics provided “efficient, high-quality care” with three-quarters of paediatric patients not requiring ENT input or review postoperatively.
MedChem Australia will support an Ear Science Institute Australia (ESIA) project researching novel small molecules for the treatment of sensorineural hearing loss (SNHL).
Ear Science’s Hearing Therapeutics team said there were no pharmacological or cellular treatments available for SNHL. Its pilot project aims to repair and regenerate inner ear tissue using cellular and pharmacological treatments.
MedChem Australia announced on 1 August 2024 that it had selected the ESIA project in the first round of portfolio and pilot projects on drug discovery programs it would support with medicinal chemistry and pharmacokinetics expertise.
“I am very privileged to lead this ground-breaking research program and collaborate with MedChem teams at Monash University and the Walter and Eliza Hall Institute (WEHI) to develop a new therapeutic intervention for hearing loss,” Adjunct Associate Professor Elaine Wong from ESIA said.
Project leads are A/Prof Wong and Professor Marcus Atlas from Ear Science in collaboration with Dr Victor Chuang, Honorary Fellow at Ear Science, and Professor Lee Yong Lim and Associate Professor Connie Locher from the University of Western Australia. MedChem Australia director Professor Brendon Monahan said the project aligned with its goal to facilitate translation of cutting-edge research into tangible advancements in drug discovery.
MedChem Australia is a partnership between Monash University, WEHI, The University of Sydney and Therapeutic Innovation Australia, with support from the federal government’s Medical Research Future Fund.
Researchers said, in the August edition of the International Journal of Paediatric Otorhinolaryngology, that results added to the body of evidence that the clinics were feasible and supported a shift towards more interdisciplinary models of care, which could address challenges faced by ENT services.
They said the novel approach could alleviate demands on ENT services and improve clinical outcomes for affected children. Researchers said otitis media (OM) had a high prevalence in childhood and grommet insertion was the most common surgical treatment for OM. In tertiary hospitals in Australia, OM was also one of the most common reasons for paediatric surgery.
“The public health system in Australia
faces considerable strains, including high demand for ear, nose and throat specialists,” they wrote. “Extending the scope of practice for audiologists to manage post-operative care for children receiving grommets has the potential to alleviate this burden.”
In the study, audiologists reviewed children at six weeks and 10 months post-operatively, escalating care to an ENT specialist if abnormalities were observed. Children with normal hearing and patent grommets were reviewed and discharged by the audiologist. At six weeks, 72/93 (77 %) presented with in-situ grommets and normal hearing, while 21/93 (22 %) were escalated for immediate ENT care. At the 10-month review, 54/72 (75 %) were discharged without further ENT intervention, and 18/72 (25 %) required additional ENT investigation.
“This model allows an extended scope (ES) audiologist to offer assessment, diagnosis and recommendation for children with semi-urgent ear health issues, holding the potential to expedite clinical services and improve the efficiency and satisfaction of healthcare delivery in children with OM,” researchers said.
$75 MILLION NEXTSENSE CENTRE TO HELP 10,000 FAMILIES A YEAR
The new $75 million NextSense centre for innovation aims to support ongoing research, education and treatment to enhance the lives of people with hearing and vision loss nationwide.
The state-of-the-art custom-built facility will deliver best-in-class services and be a home for sharing research and practical knowledge across Australia and the world as well as train the next generation of professionals.
The centre will be the focal point for
NextSense national operations and will also house allied health, disability and cochlear implant services for children and adults, a school and preschool.
Located in Sydney’s Macquarie University precinct, it will bring the organisation closer to its key partners, Macquarie University Hearing, Cochlear and Hearing Australia. It will also support more adults with hearing loss as by 2050, more than six million Australians will have hearing loss, NextSense said. Despite being the largest group affected by hearing loss, adult awareness of health and social impacts was low, chief executive Mr Chris Rehn said.
Officially opening the centre in August 2024, Australian Prime Minister Mr Anthony Albanese said: “We invested in this centre because it’s helping Australians with hearing or vision impairment lead full lives. From teachers in the school to cochlear implant specialists, the workers at Macquarie Park represent the possibility of a better future for many Australians.
The study found most patients did not need ENT input post grommet surgery. Image: romaset/ stock.adobe.com.
Australian Prime Minister Anthony Albanese opening the NextSense innovation centre. Image: NextSense.
Adjunct A/Prof Elaine Wong and Prof Marcus Atlas from ESIA will lead the project. Image: Ear Science Institute of Australia.
HEARING LOSS 'EQUAL BIGGEST MODIFIABLE RISK FACTOR' FOR DEMENTIA AT POPULATION LEVEL
Hearing impairment is equal top of the list of modifiable risk factors associated with the greatest proportion of people developing dementia globally, the 2024 Lancet Commission on dementia claims.
Based on latest evidence, nearly half of dementia cases worldwide could be prevented or delayed by tackling 14 modifiable risk factors, the new report said. Risk factors associated with the greatest proportion of people developing dementia were hearing impairment and high cholesterol in midlife, each responsible for 7% of cases globally.
The third Lancet Commission on dementia prevention, intervention and care was presented at the Alzheimer’s Association International Conference in America on 31 July 2024 and published in The Lancet
Researchers said risk modification affected the population and did not guarantee that any individual would avoid dementia. However, “evidence is increasing and is now stronger than before that tackling the many risk factors for dementia reduces the risk of developing dementia,” they said.
“The evidence that treating hearing loss decreases the risk of dementia is also now stronger than when our previous
Commission report was published four years ago,” they said.
“Use of hearing aids appears to be particularly effective in people with hearing loss and additional risk factors for dementia.
“The observational evidence of the benefits of hearing aids for dementia risk is increasing. Even if only the studies with long follow-up are considered, to reduce the chance of reverse causality, the evidence on hearing aids reducing dementia risk is consistent and supportive.
“Since the last Commission, a systematic review and meta-analysis of eight cohort studies with 126,903 participants, followed up for two to
Hearing loss is responsible for 7% of dementia cases globally. Image: Антон Сальников/stock.adobe. com.
25 years, reported that people with hearing loss who used hearing aids had a significantly lower risk of cognitive decline and dementia than those who did not use assistive devices,” they said.
In another cohort of 2,114 people older than 50 with self-reported hearing loss including 1,154 with mild cognitive impairment, hearing aid wearers were at significantly lower risk of developing all-cause dementia than those not using hearing aids.
“As severity of hearing loss increases, dementia risk increases: all four studies that investigated dose–response between hearing and dementia risk reported that every 10 dB decrease in hearing ability increased dementia risk,” they said. “The magnitude of this risk increase varied between studies, from a 4% increase to a 24% increase in dementia risk per 10 dB decrease in hearing ability.”
The Commission was authored by 27 dementia experts including Professor David Ames from the National Ageing Research Institute and The University of Melbourne Academic Unit for Psychiatry of Old Age.
NOTE: Turn to page 34 to hear what Australian experts have to say.
STRATEGIES FOR SUCCESS REVEALED AT HBA SEMINAR
Attendees at a Hearing Business Alliance seminar on strategies for business success gained valuable insight into the business side of the hearing industry nationally and globally.
Ms Jane MacDonald, HBA chief executive officer, said feedback was positive from the 26 people representing 21 independent audiology businesses who attended the event on 31 July 2024 at Mercure Perth.
National Acoustic Laboratories director Dr Brent Edwards gave an update on global industry trends enhancing audiology practice and Dr Bec Bennett, NAL senior research audiologist, spoke about enhancing audiology practice and navigating the digital frontier.
Ms Clare Hewat, independent chair of The Ethics Review Committees for Audiology Australia and AcAUD inc
HAASA, discussed changes to the committee. Ms Stacey Tonkin, Aon partnership and growth manager, health and professionals, updated on industry insurance mitigation risk while HBA business manager Mr Stephen Logan discussed changes in Australia’s hearing industry in Australia.
MacDonald presented findings from the recent Hearing Services Program survey on proposed changes to the HSP Schedule of Service Items and Fees, and updates on compliance reminders were also presented. Assistant secretary in the Department of Health and Aged Care with responsibility for the HSP, Mr Chris Carlile, also gave an HSP update.
Delegates heard about HBA’s partnership with American audiologist Dr Cliff Olson and his HearingUp network to “promote audiologists and audiometrists who adhere to a measured
standard of excellent client care.”
Independent small business owners of audiology or audiometry practices in Australia who are members of HBA can join and more than 35 have joined so far.
“It’s a one-stop site to help (consumers) find an independent hearing care professional whose clinic follows comprehensive best practices,” HBA said.
Attendees at the HBA seminar in Perth in July. Image: HBA.
CLINICAL TRIAL COMPLETED FOR MÉNIÈRE’S DISEASE DRUG
A phase three clinical trial of a novel anti-in flammatory drug for Ménière’s disease has been completed, its developer Sound Pharmaceuticals has announced.
Ebselen aims to improve hearing loss, tinnitus and dizziness in Ménière’s disease. Image: 9nong/stock. adobe.com.
The American biotechnology company said SPI-1005 taken twice dally as an oral capsule, contains ebselen, a new chemical entity, which aims to improve hearing loss, tinnitus and/or dizziness in Ménière’s patients.
It said ebselen had shown safety and efficacy in three different forms of acquired sensorineural hearing loss in adults. This included loud sound exposure or acute noise-induced hearing loss, Ménière’s disease, and antibiotic or aminoglycoside-induced ototoxicity.
No significant drug interactions had been observed across multiple study populations, it added.
Phase 1b and 2b trials enrolled more than 165 patients. The StopMD-3 study randomised 221 patients from 11 centres in the US to 800mg ebselen a day for 28 days or matching placebo treatment followed for 84 days; 201 patients continued treatment for six to 12 months.
Lead investigator and chair of Otolaryngology-HNS at the Medical University of South Carolina, Professor Paul Lambert, said: “To our knowledge, this phase three study is the longest continuous treatment trial to improve hearing loss/tinnitus in patients living with Meniere’s disease.”
Dr Jonathan Kil, Sound Pharmaceuticals’ co-founder and CEO, said it was a pivotal trial. Sound Pharmaceuticals stated that ebselen was a selenorganic compound that mimics and induces glutathione peroxidase (GPx) activity and reduces neuroinflammation across the central and peripheral nervous system.
GPx activity was critical to several cell types and tissues including in the inner ear and prefrontal cortex of the brain and was often reduced during exposures to environmental insults or aging, it added.
The company said loss of GPx activity had been shown to result in sensorineural hearing loss in multiple animal models.
ASPIRIN DOES NOT SLOW HEARING LOSS; AUS STUDY
They hoped aspirin might delay hearing loss through anti-inflammatory effects. Image: Victor Moussa.stock.adobe. com.
Taking low-dose aspirin daily does not slow the progression of age-related hearing loss in healthy older adults, according to new Australian-led research.
The researchers had hoped aspirin might help delay hearing loss through its blood circulation and anti-inflammatory effects. But their trial of 279 healthy community-dwelling people aged 70 years or older found 100mg aspirin a day was no better than placebo for slowing age-related hearing loss.
However, they said more investigation was warranted on whether a longer follow-up or the use of a more powerful anti-inflammatory agent might prove beneficial. The complex relationship between aspirin, inflammation, and hearing loss warranted continued investigation to elucidate potential mechanisms and clinical implications, they said.
“Aspirin use did not affect the age-related decline in hearing threshold or in binaural speech perception threshold compared with placebo over a follow-up period of three years,” the researchers wrote in JAMA Network Open on 25 July 2024.
They included University of Melbourne Professor Gary Rance and Macquarie University Professor Harvey Dillon.
The ASPREE-Hearing (Aspirin in Hearing, Retinal Vessels Imaging and Neurocognition in Older Generations) substudy was embedded within the parent ASPREE (Aspirin in Reducing
Events in the Elderly) clinical trial.
ASPREE was a double-blinded, randomised placebo-controlled trial that aimed to assess the effect of low-dose aspirin on disability-free survival in 19,114 relatively healthy people aged 70 years or older.
Newly recruited Australian ASPREE participants excluding those with bilateral cochlear implants and implanted hearing aids were invited to participate in the ASPREE-Hearing substudy.
The researchers said age-related hearing loss occurred because of cochlear degeneration and may be further exacerbated by inflammation and microvascular changes, as observed in animal models.
The rationale for studying the effect of aspirin was based on its potential to affect key aspects of the pathology of age-related hearing loss. There was evidence that degenerative changes affecting microcirculation of the cochlea may be important in the development of age-related hearing loss.
Aspirin, through its ability to prevent platelet aggregation and clumping, and to maintain blood circulation through aging capillaries provided a rationale to explore its action in delaying progress of hearing loss.
Another potentially useful property was anti-inflammatory actions as chronic low-grade inflammation had been implicated in age-related hearing loss, they added.
SUCCESSFUL FIRST TRIAL OF MÉNIÈRE’S GEL STEROID SHOT
The formulation provides continous diffusion across the membrane and into the cochlea. Image: Spiral Therapeutics.
An effective treatment for Ménière’s disease appears a step closer after a world first initial clinical trial in Australia of a gel steroid injection reported ‘significant reductions in vertigo frequency and severity’, an otolaryngology conference has heard. US-based hearing therapeutics start up, Spiral Therapeutics, announced the successful completion of the phase 1b/2a clinical trial which tested safety, side effects and best dose of the new treatment SPT-2101 (6% dexamethasone).
The long-acting steroid is injected during surgery in a crosslinking gel formulation into the round window membrane of the ear. The platform ensures targeted, sustained drug release over two months directly to the cochlea. Results were presented at the American
Academy of Otolaryngology Annual Meeting 2024 in Miami on 28 September 2024.
“Data review of 21 patients showed a significant reduction in vertigo frequency and severity,” Perth surgeon Dr Jafri Kuthubutheen said. “The study recruited 21 patients across sites in Perth, Melbourne and Sydney.”
Dr Kuthubutheen was the first in the world to perform the procedure.
“The treatment with SPT-2101 showed superior vertigo management compared to the control group, with a statistically significant difference (p< 0.05)," he said.
“Additionally, non-responders in the placebo group who crossed over to receive SPT-210 demonstrated a dramatic reduction in definitive vertigo days (DVDs) at month three (78.7%).”
SA hearing aid like a brain
Starkey launched its Genesis AI hearing aids in Australia earlier this year. Described as the biggest leap forward in hearing technology, they work like the human brain and employ artificial intelligence to improve the user experience.
outh Australian audiometrist Mr Dean Laird has been fitting hearing aids for 34 years and rates the latest technology from manufacturer Starkey – the Genesis AI hearing aid – as one of the top devices he has fitted.
“It’s been a revelation in terms of client acceptance,” he says. “The AI component works well and feedback is very positive, from people who have previously had different hearing aid brands and Starkey products.
“They’re saying they’ve noticed a big improvement in overall clarity and hearing speech in noise as it’s easier to understand. Also streaming and connectivity work well so it’s seamless.”
Starkey spent five years developing the technology built around a powerful processor designed to “work like the human brain” by using artificial intelligence (AI) to analyse and automatically optimise sound. The processor is reportedly the industry’s most advanced processor technology, operating up to four times faster than predecessors with six times more transistors to create better sound quality.
“The goal of Genesis AI is to mimic how a healthy auditory system works all the way up to the brain,” Starkey explains. “To achieve this, we developed a new approach called Neuro Sound Technology designed to mimic the cerebral cortex of the brain.”
This gives the hearing aid the ability to process sound the way a normal auditory system does, automatically filling in the “gaps” produced from years of hearing loss. The resulting true-to-life sound makes it easier for wearers to distinguish words and speech more intuitively and naturally, hear soft sounds without distracting noise, and reduce the effort it takes to listen and hear, Starkey says.
Sound is natural, not mechanical
Laird owns My Hearing Centre independent clinics operating from eight sites near Adelaide. He received Genesis AI hearing aids in January 2024 and has fitted a broad spectrum of patients. Many are first-time hearing aid users but also others who have upgraded from older technology due to trouble hearing speech in background noise.
He says it’s clear that Starkey has made a conscious effort around listener comfort. Feedback from clients indicates the sound quality is natural, not mechanical.
“The biggest benefits are hearing in noise and not having to readjust
ABOVE, L to R: The Genesis AI Starlink and charger; The stylish and compact Macro_mRIC R wireless Genesis AI hearing aid.
anything because the AI automatically makes more than 80 million adjustments an hour to suit the environment,” he says.
“They’re definitely worth their price,” he says. “Other benefits clients like include excellent length of charge – the longest in the industry to the best of my knowledge, lasting around 50 hours – and compact size including the RIC rechargeable which is one of the industry’s smallest for its battery life.”
Another industry-first feature that enhances speech clarity is Edge Mode+. This continuously scans, adapts and optimises hearing as the
Starkey’s Genesis AI range is designed to be compact, discreet and improve clarity and speech in noise.
Images: Starkey.
Image: Starkey.
from A Better Ear.
Great feedback from patient survey
user changes environments or as each environment changes. The user can turn on Edge Mode+ if they decide they need to hear speech more clearly in certain situations, such as noisy gatherings, busy restaurants or
“The Edge Mode+ analyses the environment in real time and prioritises speech over noise using AI to optimise sound quality on demand for clearer speech and to improve listening comfort in noise,” Laird explains.
He also likes the way the CROS system works as the CROS battery can get through the day without losing charge.
“They can get wet within reason as Starkey has designed them to be waterproof to a metre and sweatproof so they won’t stop working when exercising or playing sport,” he adds. “They suit people of all ages and lifestyles and there’s a choice of rechargeable behind the ear or receiver in ear hearing aids without losing any ability or technical specifications.”
Positive feedback included patients making comments such as “not so many arguments,” “very impressive battery life,” “not as shrill, sharp, or annoying,” and “better separation of sounds; could tell the difference between trucks and buses near home, feeling more confident and safer.”
One participant, Jacqui, said that after just 14 days, the results exceeded all expectations. “The clarity of sounds is extraordinary,” she said. “Even in noisy environments, I can hear conversations clearly, and background noises no longer compete with speech.”
She noted a remarkable difference compared to her previous hearing aids. “My partner has noticed a big difference in what I am hearing as well. It would be very difficult for me to go back to my original hearing aids after wearing these,” she shared.
Jacqui also highlighted the benefits of switching from traditional batteries to a rechargeable model. “I’m more comfortable with the safety and convenience of rechargeable aids, especially with my little grandchildren around," she said.
“The change has been quite extraordinary for me. I have always felt burdened by wearing my hearing aids but knew I needed to for my health, social and safety needs. But I am happy to wear these all day; they have made a huge difference to my quality of life.”
The pilot program is ongoing.
Fall detection alert sensors
Another innovative feature is fall detection alert capability.
“This is important for patients and their families,” Laird says. “If you fall, there are sensors built into the hearing aids, like Apple has on its watches, that automatically notify your relative and tell them your location even if you’re unconscious which could potentially save lives.”
Clients set up the alert through the MyStarkey phone app and the hearing aids send a phone text to selected contacts such as immediate relatives should a fall be detected.
One of Laird’s patients, retired civil engineer Mr Deric Oehlers, was diagnosed with hearing loss about six years ago. “I was missing out on conversations in a crowd and had the TV on very loud which was uncomfortable for others so I decided to get hearing aids,” he says.
“They helped when watching TV or talking one-on-one but were not ideal for hearing in crowds such as at the bowls club when there were a lot of people talking. You just get to the stage you don’t bother trying to listen because it’s very difficult to hear.”
But a newsletter from My Hearing advertising that Genesis AI enhanced speech in noise prompted Oehlers to seek the hearing aids from Laird.
“I didn’t want any other hearing aid because I thought I’d be back to square one," Oehlers says."I probably wouldn’t have gone back if it wasn't for Genesis AI but I thought they were worth trying.”
Oehlers trialled the hearing aids for a month and noticed they helped in noisy environments such as restaurants and sitting around the table with friends at the bowls club. Five months later and Oehlers says they were worth the investment. “The Edge Mode+ definitely works as it enhances
Image: Starkey.
Image: Starkey.
The Genesis AI Starlink charger.
The Genesis AI mRIC.
“Our all-new, powerful processor was designed to work like the human brain, leveraging the neuroscience of the ear-brain connection and information processing to create better sound quality, pushing energy-efficient artificial intelligence to its limits, analysing and automatically optimising sound over 80 million times an hour.”
Wearers don’t need to adjust the hearing aid as the inbuilt AI automatically makes adjustments, according to the wearer’s environment.
“Genesis AI is completely reimagined from the inside out; it’s the only hearing technology system to feature an all-new processor, all-new sound, all-new industrial design, all-new fitting software and all-new patient experience,” Starkey says.
Bhowmik says the improved performance is unmatched in the industry and battery life is doubled.
Its sensor technology promotes a safer, healthier life by recognising if the user is moving or sitting and providing better situational awareness, Starkey adds. Once the hearing aids sense the wearer is moving, they instantly adjust microphones to ensure the person receives the best sound from every direction. This provides greater hearing, no matter the situation or action, and greater awareness and safety in surroundings.
“The biggest benefits are hearing in noise and not having to readjust anything because the AI automatically makes more than 80 million adjustments an hour to suit the environment.”
Dean Laird My Hearing Centre, South Australia
Dr Judy Grobstein, regional director of education and audiology for Starkey APAC, says the Genesis AI is “a game changer for hearing health and ultimately improves health, wellness and quality of life”.
Starkey president and CEO Mr Brandon Sawalich says the company is leading the hearing industry not just with incremental improvements but breakthrough benefits.
Starkey says it designed Genesis AI with ‘friendly AI’ – artificial intelligence that has a beneficial effect – to enhance hearing, quality of life and help hearing aid wearers perceive and understand the world around them more easily in a way that feels natural and seamless.
Wearers can connect the hearing aids to the MyStarkey app to remind them to put their devices on as the hearing aids can sense if they are being worn or not. A self-check feature also ensures they’re in working order and providing maximum benefits.
The multi-purpose device also incorporates health and wellness features including the first to integrate sensors, track and encourage social engagement and count steps. Like a personal fitness tracker, its health monitoring and fitness features can sense when the user is doing physical activities. Pairing the hearing aids with the MyStarkey app also enables wearers to track progress and set goals.
“Our significant breakthroughs in hearing health innovation offer infinite benefits to patients and hearing care professionals alike but most importantly empower all those experiencing hearing loss,” he adds.
Laird says the Genesis AI is easy to fit and software is straightforward and user friendly.
Hearing aids have improved dramatically since the chunky beige devices he adjusted with screwdrivers in the early days.
“There were a lot of behind the ear devices and I even fitted some of the old body aids with a cord and transistor radio-like transmitter,” he recalls.
“It’s incredible how far we’ve come now.
"As Starkey is at the forefront of AI with the Edge Mode+ I would agree that Starkey is revolutionising hearing technology.”
For more information about Genesis AI hearing aids and the technology behind them, see starkeypro.com.au
Image: Starkey.
Starkey says it has reinvented the hearing aid with Genesis AI to provide the best hearing experience for hearing aid wearers.
A triumph of the human spirit
The powerful story of Melbourne audiologist YAZDANEH AMIRYAZDANI GALT has made it onto the silver screen and was nominated for an Oscar at the 2024 Academy Awards. HPA goes behind the scenes to meet the courageous woman who inspired the award-winning movie Shayda which is now streaming.
In 1995, young Iranian mother Yazdaneh Amiryazdani fled a violent marriage with her two young children to live in a Brisbane women’s refuge in search of a better life. Her daughter Noora Niasari, only five at the time, grew up to be a filmmaker and has turned her mother’s inspirational story into an award-winning movie.
Yazdaneh’s courage, resilience and hard work have transformed her from a struggling single mum to a celebrated audiologist who owns an independent practice, ACE Audiology Melbourne in Bulleen and Ivanhoe. Her success is a testament to her strength of character and the support she acknowledges receiving from many in her adopted country, Australia.
“When I watched the film, I was struck by how distant I felt from that version of myself. It was an emotional revelation—this is how far I’ve come. The past is always with you, but you move beyond it. I’ve managed to leave it behind, and
that feels like a victory,” she reflects.
Arriving in Australia in 1991 from Iran with her children, Noora and Ali, and her then-husband – whom she had married in an arranged union at just 17 – Yazdaneh endured years of abuse and domestic violence, far more harrowing than depicted in the film, before escaping to the refuge.
The refuge’s head, Ms Deirdre Doherty (portrayed as Joyce in the movie), offered them protection and support, and the bond with her remains strong.
“We still keep in touch with Deirdre; we’re very close friends,” Yazdaneh shares. “She attended the movie premieres and events, including the Sundance Film Festival in America. For me, she was not just a role model but a beacon of feminist advocacy. Her life’s work has been a testament to her unwavering dedication to women’s rights.
“Deirdre's relentless commitment to advocating for women’s rights and her profound influence on so many lives truly define her legacy. So, obviously for her, this was a proud moment. She and Leigh Purcell, the actor who played her in the film, met at several of the premieres, have a striking resemblance and even sound alike.”
The film does take creative liberties to enhance its cinematic appeal, Yazdaneh says. For instance, the movie features only one child, and Yazdaneh was portrayed as a nurse, whereas in reality, she pursued psychology at the University of Queensland for a year (1993-1994).
After separating from her husband, Yazdaneh and her children spent seven months in the refuge. She later secured permanent residency and returned to university in 1998 to continue her Bachelor of Psychology.
“I completed my degree in 2000 but I realised that my own trauma made it challenging for me to handle others’ problems as a psychologist,” she recalls.
“I discussed this with one of my lecturers, Professor Doug Maher, who suggested audiology as a potential path.”
To explore this new direction, she volunteered at an audiology practice.
“I approached audiologist Ms Joyce McIntyre, manager of the Neurosensory Unit in Brisbane, to gain hands-on experience in audiology and offered to assist at the front desk,” Yazdaneh recalls. “She kindly agreed, allowing me to observe various aspects of the field. After three months, I was certain this was my career path. Her encouragement and support, including a letter of recommendation, were instrumental in my acceptance into Macquarie University in Sydney.”
In November 2002, just before graduating, Yazdaneh already had a job lined up with National Hearing Centres (now Amplifon). She moved to Melbourne six years later, where she and fellow audiologist, Mr Jonathan Galt later married. Yazdaneh opened clinics in Bulleen and Ivanhoe, with a new state-of-the-art facility recently established in Bulleen.
Meanwhile, Noora, having made a name for herself in short films and documentaries, was determined that her debut feature film would be about
Images: Yazdaneh Galt.
Yazdaneh Galt and her daughter Noora Niasari in front of a poster of their movie, Shayda
Yazdaneh with staff, family and friends at the opening of a new premises for ACE Audiology by Bulleen MP Matthew Guy, standing next to Yazdaneh.
"When I watched the film, I was struck by how distant I felt from that version of myself. It was an emotional revelation; this is how far I’ve come. The past is always with you but you move beyond it. I've left it behind and that feels like a victory."
Yazdaneh Galt ACE Audiology, Melbourne
Though Yazdaneh is deeply proud of her daughter’s work, she admits: “At times, it felt strange to see my life portrayed as entertainment. It can be painful when people ask questions like, ‘Why didn’t you leave earlier?’ People survive as best as they can and leave when it’s safe.”
Noora described the experience to The New Arab as “an incredibly healing and cathartic process, even through a fictionalised lens.”
The family has flourished in Australia. Alongside Noora’s successful film-making career, Ali worked as an audiologist before studying medicine and is about to start a medical intern position.
Yazdaneh remains profoundly grateful to those who supported her during her darkest times, including solicitor Ms Stephanie Tonkin. “I feel incredibly fortunate to have encountered such pivotal individuals during one of the most challenging periods of my life,” she says. “Stephanie was a beacon of hope, whose unwavering bravery and dedication not only guided me toward freedom but also made the journey to rebuilding my life significantly easier.
“Her presence was a true stroke of luck and I am deeply thankful for the extraordinary people who stepped in to help me when I needed it most.”
Tonkin will undertake the Great Ocean Walk from November 12-15 to raise funds for the Women’s Legal Service Queensland, which she co-founded.
Yazdaneh adds: “As a survivor of domestic violence, I understand the immense courage it takes to seek help and the strength required to rebuild. The ‘Walk for Change’ is more than just a journey; it’s a tribute to every woman who has bravely taken steps towards safety and freedom. I invite everyone to support this vital cause and help ensure no woman faces this struggle alone.”
The walk will honour the brave women who seek help to escape domestic and family violence. Over four days, the team aims to raise $25,000 by walking 40 kilometres to commemorate the 40th anniversary of the Women’s Legal Service Queensland. Yazdaneh says donations can be made to womens-legal-service-queensland.grassrootz.com/
ABOVE, L to R: Yazdaneh in 1993 with her children Ali and Noora; Yazdaneh and Jonathan Galt with Noora and Ali.
ABOVE: At the AACTA awards, Shayda ’s actors and executive producers including Cate Blanchett (fifth from left), with Yazdaneh (far right), and the women’s refuge head, Deirdre Doherty (next to her).
Making cerumen removal work for your practice
Cerumen removal is taking off in Australia with audiology at the forefront. As more practitioners train in ear wax removal and clinics offer the service, it's not only providing a short-term revenue boost, but is another way of spreading key health messages and seeing more clients for future hearing needs.
Perth audiologist Mr Sam Mitchell took a risk to open a full-time cerumen removal business. He now runs two clinics which are open seven days a week to cater for demand.
Mitchell opened Clear Ears Perth in 2022 after seeing patients in hospitals who had waited years for an ear wax clean from overworked ENT surgeons.
Previously, for seven years he worked in independent audiology clinics mainly focusing on adult rehabilitation. That was until 2020 when he began working in major public hospitals in Perth, gaining experience in hearing implants and conducting assessments for ENT clinics.
“I had some experience with micro-suction but I routinely used curettage in adult rehabilitation. It was a skill I was confident I could do and felt there was limited access to this service in Perth,” he says.
“I noticed patients who had been waiting several years to be seen by an ENT and who would have benefitted from simple cerumen removal in a community setting, while helping to relieve some pressure on ENT clinics. I started cerumen removal as a side hustle and was surprised by the demand and overwhelmed by the appreciation for the service being available.
“It was difficult to leave my hospital job as I enjoyed the hearing implant work and had worked hard to secure a full-time contract. I had to choose between a secure public service job and pursuing Clear Ears Perth full time. It was a risk and also scary at the time as my wife had just given birth to our third daughter.”
Mitchell started seeing patients after hours and on weekends at one of his clinics in Balcatta and did home visits. He hired staff and was managing the clinic while still working at the hospitals. “Once I found a suitable space I opened the second clinic in a suburb that people south of the river could access easier as patients were travelling a long way to Balcatta in the north so it made sense,” he recalls.
He realised there was demand for weekend treatments from people working during the week and had staff who were studying or working in other jobs who wanted weekend work. He now employs six audiologists across both clinics.
“When your ear is blocked with ear wax, it’s distressing and you want it resolved ASAP," MItchell says. "This can happen over the weekend but having the service accessible every day can prevent blocked ears becoming infected and avoids these patients going to the emergency department.”
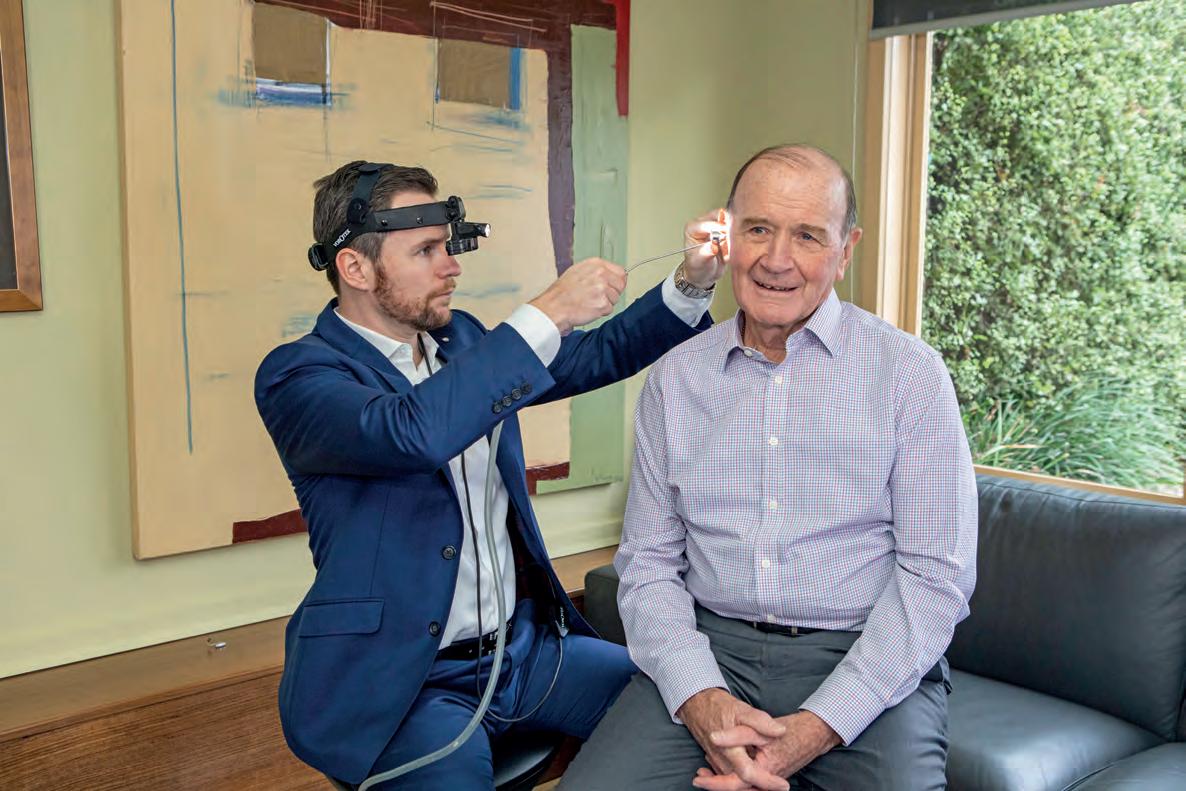
Microsuction the ‘gold standard’
Equipment includes a converged binocular optical system which is like looking through a microscope. However, it’s worn on the head, allowing depth perception and both eyes to clearly see deep into the ear. Being head-worn allows the audiologist to be mobile, instead of having to
Perth audiologist Sam Mitchell uses microsuction to remove cerumen.
Showing a patient problematic ear wax.
Images:
Sam Mitchell.
"I saw how busy the ENTs were and thought if simple cerumen removal cases could be seen in the community, it might help relieve some pressure from the ENT clinics."
Sam Mitchell Clear Ears Perth
constantly adjust the position of a microscope.
“Micro-suction is more comfortable for the patient compared to curette, forceps or ear hook. The ear canal is very sensitive, especially the deeper you get and micro-suction can be used without having to touch the canal wall,” Mitchell explains.
“Each case is different but generally micro-suction is safer and the best tolerated method; manual cerumen removal using micro-suction is the gold standard compared to ear irrigation which carries more risks.”
The business extended to paediatrics due to demand from parents asking about the safest way to remove ear wax for their children.
“We had limited the age to eight years and over but are now seeing four-year-olds. There was demand and as all clinicians are highly experienced in the procedure, we thought it was our duty of care to offer the service,” Mitchell says.
“Like any other skill, the more exposure to different cases and the more you carry out the procedure, the better you will get at it. It’s important you’re not complacent when doing cerumen removal as consequences of it being done incorrectly are much greater than when doing a hearing test or hearing aid fitting. Always err on the side of caution.”
Mitchell says GPs are offering micro-suction but irrigation is still commonplace. “The UK and New Zealand are ahead of Australia in this space and ear irrigation hasn’t been used for several years.
"I think most audiologists who are doing cerumen removal are mainly using it as a complementary service alongside fitting hearing aids,” he says.
“Along with ENTs, audiologists are best suited to this work and that’s why I decided to only hire audiologists. However, in my experience there have been many audiologists who realise they are not suited to the role as it requires dexterity and patience to become proficient in the skill and it’s not easy for everyone to pick up.”
Between them, his staff have done every course on cerumen removal
offered through CPD and are looking at overseas training to continue to improve services and knowledge. “There needs to be a more advanced course on cerumen removal in Australia as some of the current courses I feel are substandard and only provide the basics,” he adds.
Blogs on his website educate the public. “We have a duty of care to provide this information which can prevent people from doing things that could damage their ear health. They shouldn’t need to pay for this advice," he says.
Elsewhere, in Adelaide, audiologist Ms Alicia Littledyke from Hearing SA achieved cerumen removal certification while working at Bloom Hearing and is now offering the service at Hearing SA.
“It’s maybe 30% of our business at two Hearing SA clinics. On my busiest day I treated seven people for ear wax,” she says.
“Wax removals are straightforward, simple and with the right maintenance, can be done without a lot of follow-up. Removing wax that was impacting hearing aids and offering the service to people outside our client base is popular and allows us to build another side of the business.
“Cerumen removal wasn’t something that was taught in the standard audiology course. When I went to university 12 years ago, we were told audiologists don’t touch ear wax – that’s something you leave for GPs and ENTs – so it’s changed over the past 10 years.
“Not only has there been more demand – I think more people understand wax and the impact it can have.”
Littledyke says GPs have been confident to perform cerumen removal, but she’s been told by many that syringing or water flushing – which can lead to burst ear-drums or infection – was one of the biggest causes of malpractice complaints. Many have stopped for insurance purposes, she adds.
“Trying to get into an ENT is difficult in terms of waiting times, more steps, referrals and costs,” she says. “Audiologists are saying to GPs and ENTs we’re here to bridge the gap and we are specialists in ears. We look at them all day, every day, can be trained and have the right equipment to offer that service and take pressure off doctors and surgeons.”
Increased air travel
Littledyke is increasingly seeing younger people coming in for cerumen removal and more musicians. While wearing earbuds, in-ear monitors and headphones can compact ear wax, she believes extra demand relates more to increased understanding. But she also believes a big factor is more air travel which can make pressure in the ears uncomfortable.
“Especially if going overseas or on longer flights, having a big build-up of wax with additional air pressure can cause a lot of discomfort,” she adds.
“Swimming is another factor as swimming softens wax. Wax might have been building up for ages but then instantaneously something happens and being able to offer a service where people can be seen within a short period and receive instant relief is great.”
Dry vacuum micro-suction has been passed down from ENTs, and learning to perform wax removal with this is a big part of training programs, she adds.
“It’s generally very safe and effective with minimal risks because it’s a dry procedure. We’re not putting any water in the ear so if they’re at risk of infections or they’ve had previous damage, we’re not putting them at further risk. It’s gentle and is done within 30 minutes.”
Micro-suction machines cost about $2,000 to $2,500, and other accessories include probes to get into ear canals of different shapes and sizes, she adds.
Several universities and companies offer training courses including theory and practical components. Audiology associations sometimes offer cerumen workshops at conferences which she says are always popular.
“It’s an evolving skill that many clients can benefit from and audiologists can add to their scope-of-practice, starting with removing wax for patients with hearing aids to ensure they have maximum hearing, and then adding it as a service for any patient,” she says.
Hearing SA sees both types from age 16 up. “We have a mix of regular
Sam Mitchell’s business extended to paediatrics after demand from parents seeking safe ways to remove ear wax for their children.
Images: Sam Mitchell.
Images: Sam Mitchell.
Knox Audiology also expanding
As chief operating officer of Knox Audiology – with four Melbourne clinics –Ms Jane Louey says cerumen removal is performed by a single audiologist at its Wantirna clinic, comprising 3% of appointments this year.
In July the rest of the team received training including audiologist Ms Vanessa Zhang, and the business started advertising the service more. It uses micro-suction and curettage and is receiving referrals from GPs.
“You can build that relationship from a gentle approach of looking at wax and Social media including video posts of ear wax removal have also contributed
education particularly if there’s a fungal infection or redness. This educates on preventing re-infection.
A new portable magnified vision system used overseas enables wider scope and videos what is happening during the procedure, enabling patients to watch on a live monitor. It also enlarges the view for audiologists.
Littledyke discusses management options with patients including softening options from pharmacies, and stocks several sprays. Some need regular maintenance treatments every six to 12 months. She sets them up to use a spray weekly or monthly to soften wax and move it down the ear canal, instead of allowing it to dry out and build up, leading to blocked ears.
She encourages other practices to initiate cerumen removal but recommends a certification course.
“When you first start it can be quite scary to work the equipment, making sure you’re doing it in a safe and pain-free way and avoiding risk,” she says. “Do practise sessions on staff or relatives to build skills. Be informed of options and share the word with GPs and pharmacists so they can refer patients to you.
“We are in a shopping centre and have a good relationship with our pharmacists; we send them people and they send us people. If GPs know it’s for an ear health problem, and they’re booked out, they send the patient to us. We have a sign out the front about wax removal and on quiet days advertise walk-ins; it’s an easy way to fill gaps.”
From a work satisfaction perspective, cerumen removal breaks up the day by providing a change to hearing testing and hearing aid fitting.
“If you’ve had a few long in-depth, complex appointments, this is quite a light session, a nice appointment where you get a nice win resolved quickly,” Littledyke adds.
Complex or risky case are, of course, referred to an ENT surgeon. She says the next step is more portable equipment to serve patients who cannot travel to a clinic. “There needs to be more services though, more audiologists offering it,” Littledyke adds.
“I recommend wax removal because it can affect hearing test results. If a person comes in with hearing loss but they have an ear full of wax we can fix the issue almost immediately if it’s a wax issue,” Zhang says. “I’ve seen audiologists who haven’t done a cerumen course refer to another audiologist or GP so that’s another reason audiologists should train in wax removal as they can then do a hearing test straight away.
“Wax naturally migrates out of the ear by itself but when there’s obstacles like a hearing aid, it can stop halfway as hearing aids can make it harder for wax to naturally come out. Genetics and some foods may affect wax, so promoting a heathy, well-balanced diet can help maintain appropriate ear wax production.”
The Global Ear Clean Spray Sales Market Report 2024 says the market is witnessing significant growth, driven by rising awareness of ear hygiene and increasing incidence of ear-related conditions. Cerumen removal services will only grow in Australia and audiologists are the ideal profession to seize the opportunity.
Senior audiologist from Hearing SA Alicia Littledyke.
Alicia Littledyke performing cerumen removal.
Vanessa Zhang from Knox Audiology.
Image: Hearing SA. Image: Hearing SA.
Image: Vanessa Zhang.
Audiologists call for Medicare and health insurance rebates for cerumen removal
Several audiologists who practise cerumen removal believe Medicare and health insurance rebates should apply for patients who seek ear wax removal from audiologists.
Audiology Australia (AudA) has advocated actively in this space and continues to push for audiologists to have rebates for cerumen removal. “It is something we support and will continue to raise with government as appropriate,” AudA says.
Audiologist Mr Sam Mitchell, owner of Clear Ears Perth, said he believed the government should extend the Medicare rebate from GPs to audiologists and health insurance should come to the party and allow members to claim.
“It’s disappointing the government is not acknowledging the positive impact community-based cerumen removal can have on people’s ear health,” he says. “With a Medicare rebate it would allow wax removal to be more affordable and increase accessibility.”
One of Australia’s first adopters of microsuction, Mr Keith Chittleborough from Melbourne’s Earman Audiology, told HPA : “Given that cerumen removal is not a patient priority for ENTs, shifting the burden of expert wax removal from ENTs to specialist audiologists through a change in Medicare funding pathways could be advantageous to ENTs, audiologists, and patients.”
Mitchell also believes the Medicare rebate should extend to nurses and further extend for GPs. In 2020, Medicare removed the rebate for GPs for removal of uncomplicated wax in the absence of other ear disorders, only allowing it if a GP considered it medically necessary.
“It’s gone backwards as the MBS rebate only applies to GPs if
However, he believes GPs should refer to audiologists. “Audiologists need to provide more services beyond hearing aid fittings and sales to change the perception of audiology with other professions and the wider community,” he adds.
Chief operating officer of Knox Audiology in Melbourne, audiologist Ms Jane Louey says: “The first question often asked by patients when enquiring about wax removal is, ‘Do I get anything back from Medicare? Medicare rebates would make the service more accessible and could make it more appealing for GPs to refer to audiologists, especially GPs who would prefer not to do cerumen removal given the option.”
Hearing SA senior audiologist, Ms Alicia Littledyke, also backs Medicare rebates and adds: “Some private health insurance companies offer rebates for an audio consult. Our clinic is working with funds to determine if educating clients, checking their ear health and doing wax removal qualifies as an audio consult.”
Chittleborough, a trainer for Ear Health Courses and contractor to ENT practices, recommends a high gold-standard of medical microscope and an ENT chair, digital otoscopy shared with the patient pre- and post-service, wax removal via all methods (microsuction, curette and, when indicated, indirect water) and the audiologist having thorough knowledge of complicating pathologies.
He suggests 30 minutes dedicated time and a $150 charge. “As audiologists we should not underestimate the value of our expertise,” he says. “An ENT may have a set $230 consult fee ($85 Medicare rebate) plus ear toilet $145 (with $106 rebate using item 41647 when cerumen removal with operating microscope or endoscope is clinically necessary) leaving the patient a minimum $185 out of pocket plus long wait times.”
Chittleborough said, in an AudA blog, earlier this year: “I don’t go six months without treating a patient whose sudden sensorineural hearing loss was sat on by a GP, who gave drops for ear wax or a nasal spray, and who didn’t see an audiologist for weeks or months later when the theorised critical window for treatment via oral corticosteroids, or trans-tympanic membrane injection, was lost.
“Ten years ago, virtually no audiology practice was doing microsuction earwax removal. I’d like to see the word 'audiologist' become synonymous with ear expertise; all performing wax removal and first point-of-call when a patient thinks ‘what’s up with
“I’d like to see a referral funding pathway shakeup, with tweaks like the capacity for audiologists to refer directly to ENTs and Medicare rebates for diagnostic audiology without the redundant
Chittleborough said in the blog that nurses were creating businesses for ear cleaning. “Shouldn’t this be the domain of audiologists? What’s the point of our expensive Masters degree with pathology modules if we refer patients to others, sometimes risking potential dangers of syringing, to manage
Mitchell says: “Along with ENTs, audiologists are best suited to this work and that’s why I decided to only hire audiologists at our clinics,” adding there needs to be a more advanced course in Australia.
Image: Keith Chittleborough.
Helping children and growing your practice
At least five million children aged under 18 live in Australia. Providing hearing care to those children who need it not only helps them and their families but can boost the performance of audiology businesses.
Hearing Australia is the nation’s largest provider of government-funded hearing services for children, providing hearing aids to those with permanent or long-term hearing loss, and caring for youngsters with cochlear implants. But independent audiologists also have a valuable role in the paediatric service landscape.
In fact, it’s an area private clinics are increasingly playing in: helping them become a go-to hearing professional in their communities while bringing a new dimension to their workday and a differentiating factor to their business.
About 300 babies are born in Australia every year with hearing loss, and two in every 1000 school-age children have hearing impairment.
Hearing Australia is funded by the Australian Government’s Hearing Services Program (HSP) to provide hearing services and devices to young Australians. Children with diagnosed hearing loss or a likelihood of needing hearing aids can receive ongoing services through the HSP, provided they meet eligibility requirements.
The organisation says it cares for about 14,000 children up to age 12 who use a hearing aid or cochlear implant and in 2022, its practitioners fitted more than 2,100 children from birth to age 12 with their first hearing aids. Each year 2,600 young Australians receive their first hearing aids before age 18.
For private hearing practitioners, detection and intervention for hearing loss is not the only way to be involved with care of children. Otitis media, auditory processing disorder (APD) and cerumen removal are other services they can
successfully provide to this patient cohort.
Hearing screening at schools is another avenue to extend services to children by detecting cases that might have slipped through the net. Educating teachers what to look out for is also a valuable community service audiologists can provide and raises awareness of the clinic’s name in the wider community.
Knox Audiology – a shining example
Knox Audiology in Melbourne has provided paediatric services for about 30 years. Nearly half its patients are children, says chief operating officer, audiologist Ms Jane Louey.
“Paediatric cases make up approximately 40% of our caseload on average across all four clinics,” she says. “Each clinic is different based on demographics. For example, our Doreen clinic has a higher percentage of paediatric cases based on its location in the northern growth corridor which is a popular region for young families.
“This has remained constant during the seven years I’ve worked here. Changing from bulk billing to a private billing model probably offset any increase in demand that may have occurred over the past few years.”
The business provides neonatal assessments for newborns needing follow-up assessment after hearing screening in hospital who are not referred through the Victorian Infant Hearing Screening Program.
Audiologist Vanessa Zhang from Knox Audiology performing paediatric hearing testing.
Image: Knox Audiology.
Knox Audiology Wantirna does non-invasive testing ideally while the baby is resting or asleep, measuring their hearing ability with auditory brain stem response (ABR) tests and auditory steady-state response (ASSR).
Auditory processing consultations, assessments and therapy for children with APD is another service offered.
Diagnosis and referral for otitis media treatment also occurs. When middle ear complications arise, the team works with five ENT surgeons who support Knox Audiology as well as other referring ENT specialists in the local area. This includes monitoring hearing levels to assess whether treatment with antibiotics or grommet surgery has been effective and hearing is restored.
Early career audiologist Ms Vanessa Zhang has worked at the business since graduating from The University of Melbourne in 2022. She says the course covered a fair amount of paediatric audiology and in the short time she has practised, she’s noticed more independent clinics are taking it up.
“It’s important to offer paediatric audiology because hearing impairment affects children’s learning, speech and language development and their global development, health and wellbeing,” she says.
“If anything is concerning such as an ear infection or long term cold or flu that’s caused a bit of blockage in the ear, nose and throat area, that can impact on how they’re learning. It’s important to have services like this in the suburbs where people live.”
Other benefits of seeing children include building a relationship with their parents and entire family who may then return for hearing issues.
“We’ve had a couple of cases where it was initially the child who was the patient and while I was presenting tones and sounds, the parents or grandparents noticed they didn’t hear them,” she recalls. “I suggested it might be a good idea for them to think about a hearing assessment and they’ve been followed up with hearing tests and are being monitored.
“School and kindergarten teachers seem more aware of conditions such as APD now and often suggest to parents that children are assessed.”
Pre-covid, the clinic's audiologists often did screening at primary schools and kindergartens and hearing education for teachers, she says. The clinic hopes to do more hearing education for teachers in the future.
The practice also posts blogs on its website about hearing issues from newborns to teens as part of its community education. “If a parent has a child with hearing concerns, having something that’s easy to read, instead of medical jargon, is best,” Zhang says.
“We mainly focus on diagnostic hearing assessments for children
(rebatable through Medicare with a GP referral) and babies referred for further assessment after newborn hearing screening. We refer children needing hearing aids to Hearing Australia and do a lot of APD diagnosis and therapy, offering auditory processing assessments for children aged from six years up.”
APD testing and therapy
The clinic offers nine different tests for APD depending on the child’s age and attention. If the diagnostic assessment is long, audiologists split consultations and continue later that day or on another day. Initial treatment of in-person therapy extends to using iPad apps for brain training video games that can be done several times a week at home.
Knox Audiology audiologists have undergone training with the Auditory Processing Institute to enable diagnosis and treatment.
Assistive listening devices such as wireless technology and FM systems for children struggling to hear in class are also provided. These wireless amplification systems ensure the teacher’s voice is picked up by a small microphone worn by the teacher and transferred directly to the child so they can hear clearly and understand accordingly, or via a speaker which benefits the whole classroom.
“The teacher’s voice is streamed directly into the child’s earpiece to reduce background noise and distraction,” Zhang adds. “We allow the child to trial the system in class first before deciding.”
National Disability Insurance Scheme (NDIS) funding can sometimes be used for APD assessment and therapy, and assistive listening devices at school, but this depends on circumstances, she adds.
Otitis media and grommets
“We do a lot of middle ear testing and tympanometry to tell us what’s happening with the eardrum and if there’s congestion or fluid buildup consistent with otitis media,” Zhang says. “If we see a child maybe twice and both times there’s fluid and congestion, we recommend they return to their GP for an ENT referral.
“Pre-grommet testing helps medical professionals decide whether the child could benefit from grommets or whether otitis media can just naturally resolve. Post surgery, we do checkups every six months until the grommet comes out and after that regular checkups to monitor hearing and the middle ear in case fluid returns.”
Paediatric audiologist
Tamara Veselinović performing otoscopy.
Image: The Kids Research Institute Australia.
Competency standards and certification
In March 2022 Audiology Australia (AudA) published Paediatric Competency Standards for Audiologists available for download. They describe minimum knowledge, skills and attributes required of audiologists to provide paediatric services at an advanced level. They can be used by an individual audiologist to guide professional development, clinical team leaders to assess competency of staff members and for certification.
AudA says standards are important to support delivery of consistent, high-quality care and offer clarity and guidance to paediatric audiologists, their clients and families.
They provide a framework for care and are quality assurance.
The organisation led the project for the Hearing Health Sector Alliance in a process supported and guided by the Paediatric Competency Standards Working Group. There was sector-wide consultation, input from focus groups and 72 audiologists with an interest or experience in paediatric audiology from around Australia and overseas.
AudA also developed voluntary certification to provide its accredited audiologists with the chance to apply for recognition as a paediatric audiologist at an advanced skill level. A paediatric certification framework outlines the process to apply for certification and ongoing PD requirements to maintain certification. Application for certification is assessed against the standards. See audiology.asn.au
Gold standard tests for subjective audiometry including VRA, play audiometry, speech audiometry and pure tone audiometry are done. APD screening and assessments provide additional information for children whose listening difficulties cannot be explained by audiometry alone.
Zhang says paediatric cases provide variety. “It breaks up the day, I enjoy it as it’s rewarding to see parents’ faces before and after treatment seeing their child can hear better.”
Working with children can be challenging though and practitioners must be patient and resilient, she cautions. “Even though you have high standards and try to get every single result and threshold, it’s OK to sometimes take a step back and say, you may not get it all this time because the child’s unwell or won’t sleep. It’s OK to get it next time.”
The room also requires a different configuration for paediatric testing of young children, she adds. Children aged over seven can have the same set-up as adults but younger children, aged three or four, need a small table to play with cards, toys and pegboards so they can hold on to something, rest their elbows and focus.
From around age three, children can wear headphones and have hearing assessed with play audiometry which teaches response to a test tone by putting a peg into a board. For those aged one or two, the room must be calibrated to where they’re sitting, on their parents’ lap, for example. Visual reinforcement audiometry featuring a puppet is used to gauge hearing.
so and presenting a tonal or click stimulus.
Hospital care
Ms Tamara Veselinović is a paediatric audiologist who works at Perth Children’s Hospital and the Djaalinj Waakinj Centre for Ear and Hearing Health, a centre which improves access to ear care for Aboriginal children in the metropolitan area.
She is also a PhD student with the Ear Health team at The Kids Research Institute Australia (formerly known as Telethon Kids Institute) and the University of Western Australia where she is an adjunct clinical lecturer.
Working in a research setting, with Aboriginal families and with a multi-disciplinary team in hospital, she had to learn extra skills.
“ The patients aren’t just ours, we’re trying to make a plan for them, so we work with Aboriginal Health Workers, ENT surgeons and speech pathologists to devise a plan for the child’s developmental needs as well,” Veselinović says.
“In the hospital we see any child referred, which can include referrals from GPs, ENTs and speech pathologists in the community, as well as general paediatrics, rehabilitation, neurology and oncology departments in the hospital. As there are many reasons a child may be born with or acquire ear and hearing problems, there is wide case variety within the paediatric audiology setting.
“We see children referred for syndromes, those with genetic risks of developing hearing loss and children who fail their newborn hearing test but then pass who we monitor to ensure it isn’t something that we didn’t pick up.”
The hospital audiologists monitor children with certain viral infections early in life such as meningitis as they potentially could develop permanent hearing loss. Additionally, they monitor children who sustain injuries, specifically head injuries, head knocks or concussion which can damage the cochlea.
“We also seen children with tinnitus, which is often challenging as it is difficult to explain to a child why they have ringing in their ears but when you do you can ease those nerves in the parents as well as the child,” she adds.
“We work closely with the ENT department as we’re next to each other so we bounce cases off each other to figure out the best plans.”
The cartoon character Bluey is a popular aid on an iPad as a visual reinforcer during paediatric hearing tests.
Paediatric audiologist Tamara Veselinović in the Perth Children’s Hospital audiology department.
Image: Perth Children’s Hospital.
ABOVE, L to R: Knox Audiology chief operating officer Jane Louey and audiologist Vanessa Zhang. Image: Knox Audiology. Image: Knox Audiology.
A baby wearing the
“I love the work. It’s complementary to my personality and it's fast paced; you have to think quickly because if you lose the attention of a child, you’re not going to get anything,” Veselinović says.
“It’s challenging but equally rewarding; you get the opportunity to work with different disciplines and learn from each other, which maybe isn’t always the case working independently in adult audiology practice.
“You don’t always get a ‘thank you’ from the patient – they might be screaming and crying but the hospital is associated sometimes with bad things so we have lots of toys and our clinic is colourful. Every audiology booth is a different theme and colour and the kids enjoy that.
“While alot of the basic equipment is the same as in independent audiology clinics, we also have more advanced and comprehensive pieces at the hospital to perform diagnostic testing. For example, we do electrophysiological testing of the Auditory Brainstem Response in infants and balance testing using vestibular testing equipment.”
Encouraging more into paediatrics
Veselinović personally believes that every audiologist should be equipped clinically to see children.
“We have that skillset but it’s whether you enjoy paediatrics because it can be challenging,” she adds. “We probably need more paediatric audiologists.
“In WA, most paediatric audiology is done in the public healthcare system although there are a few private paediatric audiologists with their own clinics
but compared to private adult clinics, there’s a huge difference.”
The Perth Children's Hospital audiologists work closely with Hearing Australia and refer children with hearing loss to the organisation for hearing aids and cochlear implants.
Veselinović believes that in future, the scope of practice will extend more for paediatric audiologists to manage grommet cases post-surgery because of the volume of cases,
“Having audiologists manage grommet cases post-surgery will alleviate the burden on the public health care system because it will free up time for surgeons to do surgery," she says. "Audiologists have enough experience and are well trained to know when the patient’s’ ears are good and when they need to see a doctor.”
Research she was recently involved in found that 75% of children who were followed up by an audiology-led clinic did not need an ENT to review them post grommet surgery.
Only 25% had to be escalated for an ENT to check.
“In paediatric audiology, we still have quite a few challenges and barriers because we work with a diverse range of kids, particularly in hospital settings, kids who are difficult to test so if we find better ways to do that, that would be amazing,” she says.
“When babies have to be tested, if they have severe, profound hearing loss, they have to be asleep and for other tests they need to be quiet but kids often cry so we have logistical behavioural things that we need to consider.
“Sometimes it makes it difficult to get results. You have to be extremely patient but we’re constrained with our time because we have patients booked in. If you don’t get anything, you bring them back in and sometimes the journey is very long to get a confirmed diagnosis because we have a small child who doesn’t want to be there.”
EarGenie aims to revolutionise assessments
This is where Professor Colette McKay, the Bionics Institute’s principal scientist and leader of its translational hearing program, comes in. Prof McKay is developing better paediatric hearing tests and innovative ways to fast-track early intervention for babies, infants and young children with hearing loss.
The EarGenie® system, developed by her team and NIRGenie, a spin-off company funded by the Bionics Institute and The University of Melbourne, could revolutionise hearing assessments for these youngsters.
Prof McKay hopes it will gain FDA approval in the next two years and be available in audiology practices soon after.
She says it may eventually allow audiologists to tune hearing aids and cochlear implants accurately from the start, allowing babies, infants and young children to hear vital sounds giving them the best start in life.
The non-invasive and harmless brain imaging system for detecting auditory responses uses light – a technique called functional near-infrared spectroscopy (fNIRS) – to measure the brain’s response to sounds.
It started as a research ‘bonnet’ with lots of cables connected to computers and has developed into a prototype headband containing light sources and detectors.
The Velcro headband wraps around the child’s head and connects to a laptop via Bluetooth. When the brain responds to a sound, there is a change in oxygen level in the brain detected by EarGenie.
These changes indicate whether the child has heard the sound and if they can differentiate between different sounds, known as discrimination.
“It’s similar to the blood pulse oximeter clipped on your finger in hospital to measure oxygen levels but this is like a pulse oximeter for the head,” Prof McKay says. “When a child hears a sound or distinguishes between two sounds, that oxygen level changes, and we can detect that in the signal.”
NOTE: Read more about the EarGenie and how it is the first clinical test of speech sound discrimination on page 38.
Image: The Bionics Institute.
ABOVE, L to R: The EarGenie bonnet has now been developed into a headband; Prof Colette McKay from the Bionics Institute.
EarGenie research ‘bonnet’ used in Prof Colette McKay's work.
Image: The Bionics Institute.
Image: The Bionics Institute.
An inspiration on the world stage
Australian swimmer MEG HARRIS, who also happens to be hearing impaired, was the second fastest woman in the pool at the 2024 Paris Olympics, winning individual silver in the 50 metres freestyle, plus team gold and silver medals. She speaks to HPA about the barriers she’s overcome to becoming an elite athlete.
Meg Harris has a message for children with hearing loss; you don’t have to do this alone. If you have a goal, there are people who will help you get to where you want to go.
Harris, 22, is the epitome of this message, having been diagnosed with moderate hearing loss in both ears from nerve damage at age six but going on to become a world record holder, multi Olympic and Commonwealth Games medallist, world champion and a recipient of the Order of Australia Medal (OAM).
Her many achievements stem from hard work, persistence and skill but she humbly credits much of her success to the support she has had.
“I would love to believe I am a role model to kids and athletes out there,” she says. “However, I don’t believe it’s an individual achievement. I wouldn’t be where I am without so many people in my life.
“My message to children who have a hearing impairment is you don’t have to do this alone. If you have a goal or anything you want to achieve, there are people out there who will help you get to where you want to go.
“It may be your parents, a teacher, someone you meet along the way; there will always be people who will help you on your journey not just in sport but life. Use it.”
Harris stunned the swimming world – and even herself if you saw the television footage – with a silver medal in the women’s 50m freestyle at the Paris Olympic Games. She touched the wall with a personal best time of 23.97 seconds to snatch silver behind world record holder,
Sweden’s Sarah Sjoestroem.
It was Harris’s first individual Olympic medal and followed a back-to-back (with the Tokyo Olympics) gold medal-winning 4x100m women’s freestyle relay, and silver in the 4x100 women’s medley relay.
Tokyo in 2020 was her Olympic debut where at age 19 she claimed her first gold in the 4x100m women’s freestyle relay and a bronze in the 4x200.
At the 2022 World Championships, she nabbed a gold in the women’s 4x100 freestyle relay, a bronze in the 50m women’s freestyle and a silver in the mixed medley 50m relay.
Commonwealth Games medals include a silver in 2022 in the 50m women’s freestyle and mixed 4x100m freestyle relay followed by gold and a world record in the 2023 World Championships for the 4x100 women’s freestyle relay.
Harris was one of seven Deaf or hearing-impaired athletes at the Paris Olympic Games including fellow Aussie, Matildas goalkeeper Mackenzie Arnold, now an ambassador for Audika.
British swimmer Suzanna Hext also took part in the 2024 Paralympics wearing her cochlear implant thanks to a rule change in 2023 enabling her to wear the implant while racing. And this year is the 100th anniversary of the Deaflympics, which will be in Tokyo in November 2025. These are a
ABOVE: Meg Harris proudly displaying her first individual Olympic medal, silver from the 50m freestyle at the Paris Olympic Games.
Image: Delly Carr/Swimming Australia.
"It may be your parents, a teacher, someone you meet along the way; there will always be people who will help you on your journey not just in sport but life. Use it."
Meg Harris Australian swimmer
Deaf version of the Olympic Games solely for hearing impaired people run by the International Committee of Sports for the Deaf.
Harris applauds all this representation.
“The fact that it is being acknowledged and shown to young kids that anything is possible and it’s not something that you have to be ashamed of goes a long way,” she says.
She has accepted her hearing impairment now but that wasn’t always the case at primary school when she went for six years without wearing her hearing aids consistently.
“It’s unsure whether I was born with hearing loss or developed it through a virus when I was young. I was diagnosed through a school test in grade one,” she recalls. “I was fitted with hearing aids almost immediately.
"After finding out I went to Hearing Australia and they ran more tests just to confirm. However, I didn’t start wearing them consistently until I was around 12 – I wanted to fit in.”
Harris says she relies heavily on lip reading especially in loud situations which she picked up by habit. “Because of this I really struggled with meeting new people during the pandemic due to masks.”
Born in Wodonga, Victoria and raised in Mackay, Queensland, she has been swimming and lifesaving since age three and had her passion for swimming ignited at age five when her mother became a swim teacher.
She has been with Hearing Australia since diagnosis and the organisation has provided all her hearing aids which she says have been crucial in her personal and swimming journey. She can Bluetooth her hearing aids to her phone, receive her phone-calls through them and adjust their sound on her phone.
“I don’t use ear plugs or ear moulds when swimming as I need what hearing I have left in the pool and I can still hear in the water without my hearing aids. It’s natural to me because I haven’t known anything different.
“I didn’t realise how much I was missing out on until I started wearing hearing aids consistently in high school. They have also helped -when on swim camps and especially during media post racing, however in the pool I have never known the difference as I can’t wear them to swim.”
She doesn’t however believe being partially deaf has created barriers to her swimming.
“I wouldn’t say it’s created barriers although I do struggle sometimes when travelling using extra energy when in new situations trying to hear,” Harris says. “But I am lucky I have always been surrounded by people who have gone above and beyond to make sure I’m comfortable and am not missing out on anything.
“I can hear the starters gun in most situations as the crowd is quiet at this point. However, growing up I had to work on my reaction time as I was trying so hard to hear it, I was more focused on listening then getting off the block – it wasn’t one natural movement.
“The most challenging part for me is the whistle to get on the blocks and “take your marks” when the crowd is still making noise as sometimes it’s not as loud as the starter gun.”
She does better when she knows a person and how they talk, making it easier to lipread or make out what they’re saying. When it comes to her coach and team-mates talking, she doesn’t feel she’s missing out on much.
“My coach likes to use hand signals too. With media, I have so many people that have helped me, it ranges from answering the question for me if they can tell I’m struggling to hear without making a big deal or bringing my hearing aids to me post-race. I really am so lucky that I am surrounded by people who go above and beyond for me.”
Harris says she has had time to reflect on what an incredible experience the Olympic Games in Paris was.
“The races have sunk in and the success I had this year was not one I thought I was going to get out of this season. I could not be more proud and grateful for everyone around me.
“In terms of the Olympics experience as a whole, that will take a lot longer to sink in, just trying to comprehend the scale of how much impact the Olympics had on people and to be a part of that history and see the amount of support we had not only from our country but the world, it’s crazy and not something I could’ve ever imagined.”
Harris is also studying nursing, is cofounder of a clothing brand, a project32 (athlete development program) athlete and chief inspiration officer at Auswide Bank.
The Australian Olympic Committee paid tribute to her, saying: “Meg is partially deaf but, like Cindy-Lu Fitzpatrick before her, she continues to inspire young children to follow their dreams.”
Fitzpatrick, 59, now Cindy-Lu Bailey OAM, is a Deaf swimmer who represented Australia in the 1982 and 1986 Commonwealth Games and Deaflympics.
She is considered the most decorated woman in Deaflympics history with a record haul of 29 medals and is one of Australia’s greatest swimmers despite not being able to hear the starters gun.
Like Harris, she also received the Order of Australia Medal in 1985 for services to swimming.
Image: Meg Harris.
Image:
Delly Carr/Swimming
Australia.
Image: Delly Carr/Swimming Australia.
A picture of determination; Meg Harris diving into the pool at the Paris Olympics.
Harris stunned the swimming world, and herself, when she took silver in the 50m women’s freestyle.
Programs helping Deaf children
Both champions have no doubt inspired hearing-impaired children and now Deaf Children Australia (DCA) has stepped in to make it easier for coaches and clubs to assist Deaf and hard of hearing children. DCA, a not-for-profit organisation that champions the growth and social inclusion of Deaf and hard of hearing (DHH) children and young people, has launched two innovative programs to assist their participation.
DCA’s Blueprint, which launched in June 2024, aims to promote inclusion of DHH children and young people in mainstream recreational and sporting clubs.
This range of free resources supports clubs, groups and community organisations to feel empowered and confident to support DHH children. Funded through the Department of Social Services it provides coaches, teachers and parents information to assist inclusion in activities and ensure children's participation is as enjoyable as their hearing peers.
Resources include more than 100 sports-specific Auslan signs on video.
DCA project officer Ms Sanonu Robertson says 121 people registered for its launch webinars. They included coaches, club presidents and parents from a wide range of organisations ranging from tennis to martial arts, swimming, tae kwon do, dance, soccer, athletics, hockey, football, teeball, golf, judo, astronomy, coding, chess, circus, all abilities activities , basketball and kids pilates.
“More than 60 Blueprint toolkits are in circulation and we've received fantastic feedback from clubs about its practicality and application in various settings,” she says, adding a webinar will take place in November.
“We have also received insight from early educators and primary/ high school teachers who have expressed interest in the resources and feel they would be appropriate and relevant to a classroom setting.”
One little athletics committee member said it was the first time in nine years they had seen such professional, user friendly and well researched inclusion resources. A basketball coach added: “The kit is simple but effective. I love the visual resources to encourage inclusive communication. The highlight is the pocket reference – it’s handy, convenient and is exactly what it says it is – for your pocket.”
DCA’s Blueprint followed a DCA survey which found parents of DHH children were concerned about their children’s capacity to integrate into everyday sporting and recreational activities. Parents could see the benefit of their child being involved with sports, music and other recreational activities, providing a pathway to make friends.
A second survey found 77% of respondents revealed their communities had limited knowledge and skills to effectively communicate with a DHH child. This feedback prompted the DCA team to create the program to
confidence to include DHH children in everyday sports and activities.
Puggles Swim for children with hearing loss
A similar survey several years ago provided a glimpse into the struggles faced by families with DHH children when it came to swimming. Many parents expressed fears about their child’s safety in the water and others voiced frustration over a lack of inclusive swim programs.
As a result, DCA launched Puggles Swim in 2022, the nation’s first swim program tailored to the unique communication requirements of DHH children. It was the result of a collaboration with AUSTSWIM and Swim Coaches and Teachers Australia, leading swim course developers, instructors, and elite Deaf swimmers, to create an interactive online course. The Royal Life Saving Society – Australia has since endorsed it.
Profoundly Deaf competitive swimmer and cochlear implant wearer, Mr Nick Layton was part of the steering committee during Puggles’ development. A former ambassador of the program, he remains supportive of its initiatives. Layton won five medals at the World Deaf Swimming Championships in Argentina, his first international event.
“Puggles now has a nationwide footprint with more than 1,100 accredited swim teachers completing the course in 302 swim schools across the nation which are listed in our online map,” Robertson adds.
The program teaches swim teachers pivotal skills of Auslan sign language, Deaf awareness and includes waterproof flashcards with Auslan signs. Ms Carol Webb, the mother of a Puggles swimmer says: "This program is so important to give confidence to parents that their child can communicate and learn and be water safe.”
As DCA says, winning is taking part. But also, imagine how inspired those little Puggles would have been seeing Meg Harris on the Olympic podium.
Image: Deaf Children Australia.
Hearing impaired student EJ (right), having tennis lessons under direction of her coach who is signing.
A Puggles Swim instructor signing.
Image: Deaf Children Australia.
Skin cancers and conditions on the ears
Summer is approaching which is a good reminder for hearing practitioners to look out for suspicious lesions and spots in, on and around the ears to be referred to doctors.
HPA gleans some valuable insight from Darwin audiologist KERRY BELL and leading dermatologist DR STEPHEN SCHUMACK
Northern Territory audiologist Ms Kerry Bell is challenging audiologists to be on the lookout for skin cancers and melanomas on and around the ears. She says Australia has no national skin cancer screening program so the onus is on individuals monitoring their own skin – and ears are often overlooked when it comes to sun protection, hats and sunscreen.
“Audiologists are uniquely placed to fill this gap,” Bell told delegates in an informative session on skin cancers on the ears, other ear lesions and skin conditions at The Sound Exchange’24 Audiology Australia event in Melbourne earlier in 2024.
“We look at ears every day and see the direct population at higher risk for skin cancer and melanoma such as older people so it’s a good opportunity to check when we are doing otoscopy,” she told the event.
Around the pinna, she says squamous cell carcinomas (SCCs) and basal cell carcinomas (BCCs) commonly present as small lesions that don’t heal over time and may itch or bleed.
“About 10% of skin cancers occur on the outer ear and can progress into cancers in the ear.
ABOVE: Basal cell carcinoma (BCC) on an ear from over exposure to UVA, particularly sunlight, resulting in the need for an operation to remove it.
“It’s important to look all around the ear during otoscopy and ask patients how long suspicious spots have been there. We don’t need to be diagnosing but act as a screener. It’s more a matter of highlighting lesions to the patient and asking them to monitor them and see a GP for investigation.”
She says the pinna plays an important part in the auditory pathway and if a patient has the pinna removed in skin cancer surgery, it can affect sound localisation tasks and ability to impartially separate sound and noise. Custom device options such as hearing aids, bone conduction and middle ear implants, and cochlear implants can assist those with skin cancer of the ear, she adds.
Bell advises that if audiologists are unsure or concerned about any skin lesions or conditions they see on, in or near a patient’s ear, they should take clinical notes and always refer them to a GP or dermatologist.
A free dermatology website, dermnetnz.org, is a good resource to assist.
Dr Stephen Shumack from the Australasian College of Dermatologists did not speak at The Sound Exchange but has since given HPA an outline of what audiologists need to know and provided the below tips about skin conditions and cancers on or around the ears.
Skin conditions
Eczema is the most common inflammatory skin condition around the ears and favours other flexions too such as elbows and knees, along with eyelids, face and body. It can also exist in the ear canals and can blister and ooze. People with eczema can also develop red and scaly skin from secondary bacterial infection.
Patients can be advised to use soap-free cleansers such as QV, Cetaphil and Dermeze, topical steroid lotions/creams, and non-steroidal topical therapy on the ears, and to avoid irritants.
Seborrheic dermatitis is another form of eczema which can affect the ears, eyebrows, nasal folds and eyelids but is more pink than eczema and favours creases. Treatment is similar to eczema including 1% hydrocortisone cream twice daily for the face and over-the-counter antifungal shampoo such as Selsun Gold or Nizoral shampoo 3-5ml used twice weekly for a month and then weekly.
Psoriasis may occur in people with other conditions such as arthritis, Crohn’s disease, ulcerative colitis and coeliac disease. Plaques tend to be thick and scaly and removing triggers such as alcohol, smoking and extra weight can help. Topical therapy as used in eczema is helpful along with vitamin D analogues and 15 minutes a day of sun exposure.
People with comedonal acne should be advised to wear oil free cosmetics, use soap-free cleansers, and use OTC benzoyl peroxide topical lotion or cream.
Large brown or pink age spots (seborrhoeic keratoses) or barnacles can appear in older people, have a waxy appearance and are benign.
Chondrodermatitis nodularis helicis (CNH) affects the outer ear rim and involves inflammation and a small hard bump on the ear cartilage. These areas can be quite tender to the touch. They are often caused by pressure such as sleeping on one spot with headphones pressing on that spot. They can also be caused by heat or cold. They have a crust on top and are tender. and if they don’t resolve, referral to a GP or dermatologist is required.
Skin cancers
Basal cell carcinomas (BCC) are the most common type of skin cancer and the least concerning but must still be treated through excision. After years of sun exposure, BCCs can develop on the pinna.
Those at higher risk are older men, people who have had other non-melanoma skin cancers, have fair skin and light hair, are immunosuppressed, have had previous skin injury or have Gorlin syndrome. BCCs are generally slow growing and the least invasive skin cancer. They are nodular and include pearly nodules with blood vessels crossing the surface. They can be cut out and sent to a pathologist for confirmation of diagnosis.
Features include rolled edges and central ulceration, itchy bleeding sunspots and a BCC on the ear often appears as a crusty spot that will not heal. BCCs should be referred to a GP or a dermatologist for formal diagnosis and treatment.
Squamous cell carcinomas (SCCs) are tender, grow quickly and these patients should be referred to a GP or a dermatologist as soon as possible. SCCs can be painful and itchy, feature scaly red patches, open sores and rough, thickened or wart-like skin. Lymph nodes may be enlarged. People who have had a lot of sun exposure, a history of smoking or immunosup pression are at higher risk. Surgery and radiotherapy may be required. Actinic keratoses are rough, scaly patches on the skin that develop from years of sun exposure. They are often found on the face, lips, ears, forearms, scalp, neck or back of the hands. Those with fair skin who have had a lot of sun exposure, older people and the immunosuppressed are at higher risk. Actinic keratoses feature a red base with a small white crusty lesion and can be precancerous. They are generally not tender but if tender and thickened, they should be biopsied.
SCC in situ or Bowen’s disease in the superficial epidermis is a pre-invasive, very slow growing and very early form of SCC. It can be confused with psoriasis and appears in sun exposed areas. It is larger and thicker than actinic keratosis and should not be tender but if it becomes tender it requires biopsy. Those at higher risk of Bowen’s disease include people who have had a lot of sun exposure or ionising radiation exposure and the immunosuppressed. There is a 3-5% chance of it becoming invasive SCC. OTC urea or salicylic acid cream can help. Transplant patients may require excision.
Pigmented lesions
Naevus or moles are very common and generally round. People with lots of moles are at increased risk for melanoma and should be referred to a GP if there is a change in size or structure of a mole, if a new mole, different from the others, appears when they are over age 40 or it has ABCD characteristics (asymmetry, border irregularity, colour variation or a diameter over 6mm).
There have been many new therapies for melanomas including systemic treatments in recent years. Patients with a melanoma on their ear are generally older and might have had previous melanoma, BCC or SCC. Risk factors for melanoma include having many moles, fair skin, UV exposure, working outside or being immunosuppressed.
Melanomas are flat and while generally a brown or black raised lump with
"It’s important to look all around the ear during otoscopy and ask patients how long suspicious spots have been there. We don’t need to be diagnosing but act as a screener and ask them to see a GP for investigation."
Kerry Bell NT audiologist
dark, irregular colours and borders, they can also appear like a pinkish raised lump or mole that grows quickly. Some can lack pigment and have no colour. If changes occur such as sudden bleeding, there is a risk of metastases and death.
New systemic treatments can work wonders but have side-effects. If detected early, melanomas are very treatable with excision. Always refer to a GP or dermatologist for consideration of biopsy and excision.
Remind patients to wear sunscreen and a hat that covers their ears. If they have red, itchy, scaly, painful, bleeding, new, rapidly changing or failing to heal lesions, or a rash that is not improving with topical cream, refer them to a GP or a dermatologist.
About the authors
Audiologist Kerry Bell came to the NT on a university placement in 2009 and has worked in rehabilitation and diagnostics from outreach in Cape York, to private practice and humanitarian audiology in the Pacific. She works for NextSense supporting the Cochlear Implant and Implantable Devices Pp=rogram for Territorians and works as a lecturer and tutor for Charles Darwin University’s Master of Audiology program.
Dr Stephen Shumack OAM is a general clinical dermatologist, Clinical Associate Professor at the Sydney Medical School (Northern) of the University of Sydney and a senior staff specialist at the Royal North Shore Hospital of Sydney in St Leonards. He is the treasurer of the International League of Dermatological Societies, a past chairman of the board of the Skin and Cancer Foundation Australia, a former president of the Australasian College of Dermatologists and former editor in chief and now on the editorial board of the Australasian Journal of Dermatology. He has published and spoken widely on dermatological care including psoriasis, eczema and skin cancer diagnosis, management and research.
Image: Australasian College of Dermatologists.
Image: Dermatology11/Shutterstock.
Ulcerated nodular basal cell carcinoma (BCC).
Image: Prime Creaetive Media.
Dermatologist
Dr Stephen Schumack.
cognitive decline, and dementia Hearing loss,
The links between hearing impairment, cognitive decline and dementia are receiving much attention as studies point to an association. Other research is investigating whether hearing intervention can lower dementia risk or slow progression. What is the evidence and what does it mean for audiologists and patients?
The 2024 Lancet Commission on dementia ranked hearing loss as the equal highest modifiable risk factor for dementia at a population level, claiming 7% of dementia cases may be due to hearing loss.
While this latest summary adds to the evidence, Australian audiologists who are experts in the field say that although there is a link between hearing impairment and cognitive decline, it is not yet proven that hearing loss causes dementia – or that hearing intervention reduces risk or progression.
Audiologist Professor Julia Sarant is head of The University of Melbourne’s Hearing Loss and Cognition Program which she established in 2016 after becoming aware of ‘this significant health crisis, probably the biggest we’re going to have due to global population aging.’ “A couple of decades ago, only a few countries were aging globally and had significant aging populations. Now it’s the whole world,” she says.
“With aging comes hearing loss, so we have greater prevalence of older adults, hearing loss, and dementia and cognitive decline.”
She says there have been many studies in recent decades and growing awareness and evidence around an association between hearing loss and cognitive decline/dementia.
“When I started looking at it, there were a couple of good reviews which seemed to synthesise the evidence to suggest quite strongly that there was an association between hearing loss and cognitive decline,” Professor Sarant explains.
“I would describe it as an independent association between hearing loss and cognitive decline, and hearing loss and dementia, but not a causal link as there’s no evidence of a causal relationship – that hearing loss causes cognitive decline or dementia.”
The 2024 Lancet Commission states there are 14 modifiable risk factors for dementia and the more a person has, the higher their risk of dementia.
“Risk does not equal cause and just because you have a risk of something doesn’t mean you’re going to develop the condition,” Prof Sarant says. “It depends on genes too which can interact with exposure to risk factors.”
She says the commission has delivered more evidence as it is now based on six meta-analyses compared with three in 2020.
“They’ve doubled the evidence, so I guess that’s stronger evidence but is it definitive evidence, is it strong evidence? I don’t think it is, it doesn’t prove causality,” Prof Sarant says.
Randomised controlled trials (RCTs) cannot follow people for long enough to see if they develop significant cognitive decline and dementia, she says, adding the ACHIEVE study was only three years due to it being ethically unacceptable to deprive people with hearing disability of an intervention.
But she rejects that observational evidence, used in the commission, is not good enough. An RCT, for example, was not done to prove smoking causes lung cancer; instead, enough evidence was accumulated in high quality
"I would describe it as an independent association between hearing loss and cognitive decline, and hearing loss and dementia, but not a causal link as there’s no evidence that hearing loss causes cognitive decline or dementia."
Prof Julia Sarant University of Melbourne
Image: Julia Sarant.
The 2024 Lancet Commission on dementia estimated 7% of dementia cases worldwide at a population level may be associated with hearing loss.
observational studies to show that smoking causes lung cancer.
“We need high quality observational studies because they’re the only ones that can be long term, following people for at least a decade,” she says.
It also depends on populations studied as ACHIEVE found hearing aids did not reduce dementia risk but its ARIC sub-group of sicker, older people with many dementia risk factors showed hearing-aids slowed loss of thinking and memory abilities by 48%, she says.
‘Amazing results’ by treating hearing loss
Prof Sarant’s own studies to see if hearing intervention impacts cognitive outcomes in people wearing hearing aids or cochlear implants have had impressive results, finding no or reduced cognitive decline, and even significant improvement in those treated with cochlear implants.
However, she says this does not prove hearing intervention prevents or slows dementia, and as sample sizes were small, her team is recruiting larger samples with longer follow-up.
“We know there’s an association, with pretty strong evidence to suggest people with hearing loss decline faster, and that’s a dose response effect.
"Four studies show that for every 10dB of hearing loss, there’s a faster rate of cognitive decline,” she says.
“Our ENHANCE study showed a greater effect than the ARIC subgroup.
"Our group with hearing loss who had hearing aids were at much lesser risk of decline in terms of physical health and had fewer risk factors (than the ARIC group) but still we found a bigger impact of hearing intervention and saw no cognitive decline.
“We saw stability over three years. In our comparative group, a representative sample of the normal community of adults – about 50% who had no hearing loss and the rest with mainly very mild hearing loss – we saw
cochlear implants.
a greater rate of decline per year on three out of four tests compared to our intervention group with hearing loss. Results of our studies indicate that hearing intervention can stabilise cognitive function and perhaps delay the onset of cognitive impairment.”
Results she is submitting for journal publication show the cochlear implant study had “amazing results”. “We saw stability in three of five tests over four and a half years but significant improvement in working memory and executive function. It’s a much stronger result and fits nicely with theories of how hearing intervention could help.”
The comparative group did worse overall than the implanted group
Image:
Raths/stock.adobe.com.
Dementia is a significant health crisis due to global population aging.
Prof Julia Sarant’s studies found significant improvement in those treated with
even though cochlear implantees were more poorly educated, started off with lower cognitive scores, and had more mood disorders and cardiovascular disease.
Could hearing intervention help?
Prof Sarant says three hypotheses could explain how hearing aids and cochlear implants may assist cognitive health. The first is that reduced auditory stimulation causes degeneration in brain structure and function, for which there’s physiological evidence.
“The second is that reduced communication ability leads to reduced social interaction, which can lead to loneliness, isolation and mood conditions such as depression and anxiety, which are known risk factors for dementia,” she explains.
“The third is that processing a degraded auditory signal requires more cognitive resources and these are diverted from other cognitive functions which impairs those functions. A classic is working memory. Speech, perception and understanding is a cognitive task, so we need skills like working memory, inhibition and attention to take in information, make sense of it, and look for what words match with the stimulus.”
Supportive evidence includes imaging studies where areas of the brain light up when a person is processing speech, and studies which show other areas appear to be recruited for listening tasks. However, these theories need more investigation, she adds, because like cancer, there are multiple risk factors, different people have different combinations and factors can interact and be additive.
Head of Brain and Hearing at the Ear Science Institute Australia, Perth audiologist Associate Professor Dona Jayakody, is also studying the links and interventions, and was in the US for the 2024 Lancet Commission launch. She says commission experts advised more evidence was needed to confirm links as “we have evidence but it needs strengthening.”
followed for two years. The study has finished with results due soon.
“Regardless of the evidence related to hearing loss and dementia, treating hearing loss has positive health benefits including better quality of life, improved communication and improved mental distress and psychosocial well-being,” A/Prof Jayakody adds.
“There is strong evidence of an association between hearing loss and dementia but more evidence is needed to confirm if using hearing aids reduces dementia risk or slows progression,” she adds. “While a causal link has not been established between hearing loss and dementia, increasing severity of hearing loss has been associated with poorer cognitive function, which could indicate greater dementia risk.”
Contributing factors include the aging auditory system and the way it processes information, she adds. "In untreated hearing loss, people can feel lonely and isolated which can boost depression, anxiety and stress which are dementia risk factors," she says..
A/Prof Jayakody says the Lancet Commission reduced the percentage of dementia cases that could be due to hearing loss from 8% in 2020 to 7% in 2024 but it could only draw conclusions on published work so more research was needed to help them make better conclusions.
Around 2015 her team began investigating impacts of untreated hearing loss on older adults. The study in more than 400 people found untreated hearing loss increases risks of cognitive impairment, depression, anxiety, stress, social isolation, loneliness and physical frailty. The researchers then studied outcomes in those treated with hearing aids, cochlear implants and bone conduction implants.
“In cochlear implant recipients, we saw a significant improvement in executive functions and reaction time which are cognitive functions. We assumed this was because they had good speech scores after a year (of being implanted) and improved quality of life,” A/Prof Jayakody says. “The rate of cognitive decline in the hearing aid cohort was a bit less than those who didn’t receive a hearing aid.”
To further investigate, the team expanded to include geriatrician, psychiatry and imaging specialists. Their HearCog randomised controlled trial which began in 2020 includes 180 people aged over 70 years with hearing loss at risk of dementia who have never used hearing aids. One group received delayed hearing aid treatment and both groups were
Marker of dementia risk
More sceptical is director of the Centre for Hearing Research at the University of Queensland, audiologist Professor Piers Dawes, who believes hearing loss is a marker of dementia risk as it’s a marker of general frailty.
He says the 2024 Lancet Commission states treating hearing loss may reduce dementia cases by 7% at a population level but he stresses this does not apply to each individual; for example, hearing loss does not raise a person’s chance of dementia by 7%.
“The commission reported a relative risk (RR) of 1.4 at an individual level, meaning a 40% increased risk of dementia associated with hearing loss.
"But the risk of dementia at an individual level is still small overall," Prof Dawes says.
“The top personal risk factors for dementia in the report were depression
Researchers are investigating whether interventions including hearing aids and cochlear implants can reduce the risk of dementia or slow progression.
Image: Piers Dawes.
Prof Piers Dawes from the University of Queensland's Centre For Hearing Research.
social isolation and untreated vision loss; all were more of a risk individually for dementia than hearing impairment.
“The new Lancet Commission hasn’t really changed anything; we still haven’t got solid evidence that hearing loss causes dementia. There is evidence that hearing loss is a marker of risk for dementia but that is not to say that hearing loss causes dementia. Even the ACHIEVE study did not deliver definitive proof of benefit of hearing aids everyone was hoping for.
“The latest Commission report represents an enormous amount of work and deservedly receives widespread attention but it is not perfect when discussing hearing loss and hearing aids. Like Alice in Wonderland, we are in danger of going down a professional rabbit hole: the attention devoted to hearing loss and dementia has become a distraction from the evidence-based importance of healthy hearing for healthy ageing, an important social responsibility.”
He adds that all the evidence linking hearing loss to dementia risk is observational, saying we know hearing loss is associated with dementia risk but because two things are associated does not mean one causes the other.
“There are numerous reasons why hearing loss could be associated with dementia as almost all modifiable risk factors for dementia identified in the report are also risk factors for hearing loss. These include high cholesterol, traumatic brain injury, inactivity, diabetes, smoking, hypertension, obesity and excessive alcohol,” Prof Dawes says.
“It’s the same with studies looking at benefits of hearing aids for cognitive outcomes. Most are observational – comparing hearing aid users with non-users. When you see a difference it’s hard to say if it’s because of the hearing aids or some other difference between hearing aid wearers and non-users. Hearing aid users tend to be more well educated and affluent, and rates of use are much lower in ethnic minority groups.
“These social demographic factors are associated with health outcomes including dementia risk. Researchers try to measure and control for them statistically but there’s not a perfect control for these potential confounds so you can never be sure any apparent benefit of the hearing aid in these observational studies is due to hearing aids and not some confound.”
Prof Dawes says one RCT looked at whether hearing aids could reduce cognitive decline. “To avoid limitations of an observational study, you need a trial to randomly allocate people with hearing loss to a hearing aid intervention or a control condition to see if there is difference in cognitive
"There is strong evidence of an association between hearing loss and dementia but more evidence is needed to confirm if using hearing aids reduces dementia risk or slows progression."
decline over time,” he says. "Such trials are rare but an impressive recent trial was ACHIEVE."
The main finding of ACHIEVE was negative, he adds, as there was no effect of hearing aids in reducing cognitive decline. But the Lancet report does not discuss this main finding, he adds.
“It focuses instead on a post-hoc secondary analysis that shows a benefit of hearing aids in reducing cognitive decline in a subgroup of people described by ACHIEVE authors as a ‘high risk’ group. The Lancet report would have benefitted from more scrutiny of this secondary result because there are several reasons we suspect this result may be spurious (e.g. a small effect, unclear mechanism of effect and no dose-response effect of hearing loss)."
‘Inappropriate and unethical’ without convincing evidence
Prof Dawes says many in the audiology community 'share our concerns that we may be going down a professional rabbit hole.' "It’s an appealing idea that treating hearing loss would prevent dementia but one concern is that we’ve lost proper scientific objectivity about whether this is true or not.
“It is inappropriate and unethical to advocate addressing hearing loss in terms of dementia prevention on the grounds of relevance to the individual and lack of convincing evidence of benefit,”he says. "If there are benefits, they are not clinically relevant at an individual level."
Another concern is the dementia focus may turn people off acting on hearing impairment due to stigma, he says. Linking hearing loss to dementia may reinforce the stigma, denial and dis-engagement with hearing care that many people experience at hearing loss diagnosis.
Rather than ‘scare tactics’ around dementia risk, he says positive messaging by audiologists is preferable about well-proven benefits of hearing aids in improving communication and maintaining an active, socially engaged lifestyle.
“Hearing loss is a major public health problem and it’s important to address hearing loss in its own right but if people say hearing loss is important because it causes dementia, we risk agreeing with a common perception among policy makers, clinicians and the public that hearing loss is not that important,” Prof Dawes says.
Prof Sarant says audiologists can advise patients that some studies suggest hearing intervention may improve cognitive health but there are limitations to most and evidence is not strong of a causal link.
“Audiologists could discuss the topic in the context of healthy aging and use positive messaging. Fear-mongering will only make people anxious and increase stigma so hearing intervention should be supported and promoted for its multiple well- established benefits, and cognitive health may be one,” she says.
“There’s also a huge role for audiologists in working with people with cognitive impairment; they can refer people early to get the support they need and modify their clinical practice.” She is concerned some audiologists are doing cognitive screens and urges them to instead refer to a geriatrician, memory clinic, or psychologist trained in these procedures.
A/Prof Dona Jayakody Ear Science Institute Australia
Image: Dona Jayakody.
Image: adriaticfoto/Shutterstock.
Over the past 33 years, the Melbourne-based Passe & Williams Foundation has funded more than 400 research projects in Australia and New Zealand, donating $85 million and significantly impacting ENT research and clinical practice. Thousands of people have benefitted.
A legacy for good
Within days of birth, every newborn in Australia is offered free hearing screening, usually in hospital. The research which led to this critical test becoming universal was kick-started by the Passe & Williams Foundation.
The foundation’s CEO Dr Jeanette Pritchard says paediatric otolaryngologist Professor Harvey Coates AO and Dr Veronica Smyth each received initial funding to improve neonatal hearing screening, leading to a national framework for early detection.
Likewise, Video Head Impulse Test (v-HIT) technology, which is now the gold standard for assessing balance disorders, was also initially funded by the foundation, she adds. It granted funds to University of Sydney Professor Ian Curthoys, Professor Michael Halmagyi and Associate Professor Hamish MacDougall to develop the technology.
“These projects demonstrate the foundation’s impact on clinical practice and patient outcomes,” Dr Pritchard says. “The main goal of the research we fund is to benefit clinical practice and many projects have resulted in changes to the way practitioners do their work.
“It has improved outcomes for patients and may have saved lives. Our grants have also helped researchers pursue projects that might not have been funded otherwise.
“We look at what the potential impact might be for patients. About 35% of our funding or more than $30 million has been allocated to projects relating to otology, audiology or hearing-related research, something that an ENT practitioner would be treating and that could be surgical, allied health, biomedical, paramedical, anything in the ENT remit.”
Professor Coates from The University of WA and Dr Smyth from the University of Queensland’s Department of Audiology and Speech Pathology each received grants of $30,000 to investigate ways of improving detection of hearing impairment in newborns and infants, Dr Pritchard says.
“After that, state-based programs were implemented around neonatal hearing screening and then the national framework was established ensuring all neonates were screened,” she adds. “Our grants were small, but they were the trigger and Harvey often mentions that when he’s talking about the foundation.
“We granted $7 million to the University of Sydney team of Curthoys, Halmagyi and MacDougall who developed a methodology for neurologists
and ENT surgeons to measure semicircular ear canal dysfunction in patients with balance disorders.
“These tests are now the gold standard for neurology clinics around the world, enabling patients to be quickly and easily assessed, diagnosed and then treated.”
Dr Pritchard, who has a background as a scientific researcher in medical diagnostics, says these are just two examples of the important research funded by the foundation's grants, scholarships and fellowships.
Its board comprises ENT specialists, other medical specialists, academics and scientists. Grants also focus on involving clinical practitioners at an early stage which helps drive translatable research.
She says its unique focus on ENT sets it apart from other charitable organisations. It also supports career pathways for researchers, granting scholarships and fellowships and funding them from junior positions through to professorships.
“We’re told by people in our specialty and from other specialties that this is a game-changer,” she adds.
The foundation has funded more than 40 scholarships for ENT trainees training to become surgeons, enabling them to also study for their PhD during training.
“The main goal of the research we fund is to benefit clinical practice and improve outcomes for patients. More than $30 million has been allocated to otology, audiology or hearing-related research.”
Dr Jeanette Pritchard Passe & Williams Foundation
Above: The EarGenie headband to help diagnose hearing loss could be in audiology practices within a year or two. The Passe & Williams Foundation has contributed grants and fellowships to progress its development by Professor Colette McKay.
Image: The University of Melbourne.
Image: Passe & Williams Foundation .
small but really important project in Dubbo, Hear Our Heart Ear Bus, which runs off the smell of an oily rag,” Dr Pritchard says.
The bus provides free ear health education, targeted hearing testing and free access to ear specialists for children in Dubbo and districts. Audiology staff screen children’s hearing at school if a teacher or parent believe they may have hearing problems.
EarGenie to help babies with auditory neuropathy
Another innovation being brought to life partly due to Passe & Williams Foundation grants and fellowships is the EarGenie system, developed by Professor Colette McKay, the Bionics Institute’s principal scientist and leader of its translational hearing program in Melbourne.
She is developing better paediatric hearing tests and innovative ways to fast-track early intervention for youngsters with hearing loss.
The technology is a non-invasive, harmless brain imaging system for detecting auditory responses in babies, infants and young children. It uses light via functional near-infrared spectroscopy (fNIRS) to measure the brain’s response to sounds.
The tool, which started using a research 'bonnet' system with lots of cables, has developed into a prototype with a headband containing light sources and detectors that wrap around the child’s head. The headband connects to a laptop via Bluetooth. When the brain responds to a sound, there is a change in oxygen level in the brain detected by EarGenie.
These changes indicate whether the child has heard the sound and if they can differentiate between different sounds, known as discrimination.
“It’s similar to the blood pulse oximeter clipped on your finger in hospital to measure oxygen levels but this is like a pulse oximeter for the head,” Prof McKay says. “When a child hears a sound or distinguishes between two sounds, the oxygen level changes, and we can detect that in the signal.”
When screening babies with auditory neuropathy, it may appear they’re profoundly deaf, she says, but their hearing can range between normal and severely deaf because screening technology measures electrical responses of hearing nerves, which rely on synchrony in those nerves.
“With auditory neuropathy, synchrony is not there, so it looks like the nerves aren’t firing when they may be OK,” Prof McKay explains.
“When parents are told ‘your baby has this condition but you’ll have to wait until they’re older to know what they can hear, or whether a hearing aid will
Image: Passe & Williams Foundation.
Scientist Dr Erin Brazel in The University of Adelaide laboratory working on otitis media vaccines.
Image: The University of Adelaide.
Dubbo’s Hear Our Heart Ear Bus and its dedicated volunteers.
Origins of the Passe & Williams Foundation
In 1908 in Kenya a baby girl was born, Ms Barbara Slatter. Her legacy 126 years later is that thousands of people around Australia and the world have benefitted from research funded by the foundation she established to honour the memory of her two husbands.
The first of those men, South African-born Mr Edward Roland Garnett Passe (pronounced ‘pass’), moved with his Australian parents to Victoria in 1907. He graduated in dentistry from The University of Melbourne in 1926 and moved to England to study medicine at London Hospital, later becoming fascinated with otolaryngology.
Slatter, who had studied art in the UK, provided illustrations for his otolaryngology book The Singing Voice. Six years later they married and Passe joined the Royal Naval Volunteer Reserve, attaining rank of Surgeon Commander. The pair moved to Plymouth, where he served at the Royal Naval Hospital during WW2, and she was an air raid warden. Post-war Passe was a pioneer of the fenestration operation to treat otosclerosis deafness and was one of the first British surgeons to advocate sympathectomy to treat nerve deafness, tinnitus and Ménière’s disease. He died from haemoptysis aged 48.
Across the world, Mr Rodney Wellington Williams was born in New York in 1892 and after serving in the US Navy as a seaman during WW1, returned to a stockbroking firm where he rose to become floor partner in charge of trading at the New York Stock Exchange.
He met his second wife, Slatter, in Scotland and they married in 1968. When he died in 1984, at age 91, Williams left her a substantial bequest. During her marriage to Passe, she had learnt how difficult it was for a young surgeon to obtain specialist medical training in otolaryngology head and neck surgery (OHNS) so she decided to provide support to young ENT surgical trainees.
This was realised when Williams’ bequest enabled her to establish a trust in 1986 to support OHNS research and practice in Australia. The trust funds the foundation, which became operational in 1991 after her death. Thanks to wise investment and management, the estimated $38 million she left to the trust now sits at $108 million, and that is after $85 million has been donated.
*This historical information was provided by medical writer and historian Tina K. Allen.
help’, the baby misses out on critical early intervention because nobody knows what their functional hearing is.”
In some cases, these babies might wait years before appropriate intervention yet every week of delay in intervention means babies fall further behind in language development.
“Sometimes they’re two years old before a decision is made to do a cochlear implant if that’s the most appropriate action, or they’re 12 months of age before we can fit a hearing aid or know whether the aids are helping them develop language,” she says.
About 10% of babies with permanent hearing loss have auditory neuropathy.
“While other kids with other forms of deafness are getting cochlear implants and hearing aids early, this group is missing out. In just one EarGenie test, we play a series of sounds at different levels and can see which sounds the baby can hear.”
An elastic cap, similar to a swimming cap, was used to develop the
technology, but a prototype headband has now been developed for ease of use in clinics. “It’s easier for clinicians to put on as the cap was quite difficult to manage with lots of cables.
“The protoype is a headband that closes with Velcro fasteners. The lights and detectors in the headband talk to a computer using Bluetooth. The whole system currently consists of a laptop computer and the headband with embedded electronics.”
Initial trials showed fNIRS was 95% accurate at determining when babies heard sounds.
First clinical test of speech sound discrimination
“The other important thing that EarGenie can do,” Prof McKay says, “is to tell whether a baby, infant or child can discriminate between sounds.
“To develop language, you need to do more than just hear speech. You need to tell the difference between all the different speech sounds.
“We’ve developed the first clinical test of speech sound discrimination and that’s important for hearing-impaired babies, infants and young children because results will tell us, if they’ve got a hearing aid, whether it’s giving them the information they need to develop language.”
It also enables practitioners to see if the hearing aid has been programmed correctly, whether it's sufficient for the child or they need a cochlear implant.
“If the child’s profoundly deaf, then it’s a no brainer, they are referred for a cochlear implant. However, most children are not profoundly deaf – they have at least some hearing so always a hearing aid is trialled first,” she adds.
Currently the baby’s language development with their hearing aid is monitored and only when it’s clear they are falling behind are they referred for cochlear implantation.
“This is the wrong way around because you’re already waiting for the child to be delayed in language before you do something about it,” she explains. “If hearing aids are not providing them with discrimination between sounds they’re not going to develop language with the device, and they’re better off with a cochlear implant.”
Prof McKay says EarGenie could revolutionise hearing assessments for babies. She hopes it will be in audiology practices soon, after getting FDA approval, and says it may eventually allow audiologists to tune hearing aids and cochlear implants accurately from the start, allowing babies, infants and young children to hear vital sounds and give them the best start in life.
Her research team is recruiting paediatric audiologists and hearing-impaired infants from newborn to age two to evaluate the clinical value of EarGenie for the care of infants with hearing loss. Paediatric audiologists can be located anywhere nationwide for the trial, because their part is conducted online, but infants must be local to Melbourne to attend testing.
“We’ll provide results to two panels of audiologists, one that has standard audiological measurements the child has gone through and the other will have standard results plus the fNIRS results,” she says.
“We’re establishing how confident those audiologists are in deciding the next intervention steps for the baby. If the baby has a hearing aid, we might ask the audiologist if the child’s hearing aid is adequately programmed, for example.
“The prototype is clinician-friendly and operates automatically. It analyses the signal and automatically tells clinicians the confidence of whether the baby responded to the sound or distinguished sounds.”
In 2025, researchers will provide the EarGenie prototype to external clinics seeking feedback for the final design. The Bionics Institute and The University of Melbourne invested pre-seed funding to start a spin-off company (NIRGenie) to develop EarGenie but additional investment is being sought to advance commercialisation.
Audiologists and parents of hearing-impaired infants wanting to take part in the trial can email HearingStudy@bionicsinstitute.org.
ABOVE, L to R:, Rodney Williams, Barbara Slatter (Passe/Williams), Edward Garnett Passe.
Images: Passe & Williams Foundation.
Dr Brazel is also director of microbiology at GPN Vaccines and has been working for several years in partnership with the company to develop Gamma-PN.
“We have engineered this vaccine candidate targeting Streptococcus pneumoniae (Gamma-PN), taken it through preclinical development and manufacturing, and the vaccine is currently being evaluated in clinical trials.”
As this vaccine targets only one species of bacteria responsible for otitis media, they sought to develop vaccines to help target a broader range of bacteria that cause ear infections.
“Last year at The University of Adelaide, with funding from the National Industry PhD Program and GPN Vaccines, my team began a similar approach to create and test a range of other vaccines to expand this
the world that are prescribed for these common infections,” she adds.
“These infections in some instances can be incredibly difficult to treat and we urgently need new ways of dealing with them. Vaccines are one strategy that could help reduce incidence or severity of acute ear infections and hopefully also the need for antibiotics.
“The Passe & Williams Foundation has been incredibly important for advancing this research and I am very grateful. Since the award I have established and led the Molecular and Translational Microbiology Research Group, which is part of the Research Centre for Infectious Diseases at the University of Adelaide.
“This has allowed me to build my research team including supervising students focused on developing new approaches to treat and prevent bacterial infections. This fellowship allows me to focus my efforts on these new vaccines to give them the best chance to progress to the clinic where they can have a real impact.”
Scientist and EarGenie inventor, Professor Dr Colette McKay, from the Bionics Institute.
Image: The Bionics Institute.
Images: Passe & Williams Foundation.
Clinical Professor Harvey Coates whose newborn hearing screening research was funded by the foundation.
Improving children’s ear health
Researchers gathered at the OMOZ (Otitis Media Australia) 2024 conference in Newcastle to hear the latest research and brainstorm ideas for improving ear and hearing health for children. More than 300 people attended the conference which was a sold out success, writes SHARRON HALL.
BY SHARRON HALL, RESEARCH MANAGER, ABORIGINAL EAR HEALTH, HUNTER MEDICAL RESEARCH INSTITUTE.
Sixty per cent by 60 days of age. That is the proportion of Northern Territory Aboriginal babies who were found to carry bacterial strains in their nasal passages that can spread to the middle ear, causing otitis media (OM) and hearing loss in early childhood.
These alarming figures were brought to the attention of the medical community in 1994 when Professor Amanda Leach AM from Menzies School of Health Research published the results of her PhD thesis. It is now 30 years since that initial revelation. What has changed?
The message from researchers who gathered on Awabakal and Worimi lands at the 7th OMOZ conference in Newcastle, NSW, is that early onset and persistence of ear infections and hearing loss remain major health issues today, especially for Indigenous communities. Conference host, Professor Kelvin Kong AM, an ear, nose and throat (ENT) surgeon and proud Worimi man, calls hearing loss a developmental emergency that drives entrenched disadvantage.
The conference, which attracts an eclectic group of registrants, is the premier meeting for Indigenous Health Practitioners, community members, researchers, clinicians, paediatricians, surgeons, audiologists and allied health practitioners investigating and treating chronic ear disease in Australia. Normally held every two years since the inaugural meeting in 2010, the conference location moves to a different city each time.
From an attendance of 70 people in Darwin in 2010, the 2024 delegation has grown to approximately 320 people from all walks of life and many cities and towns across Australia. The
conference survived lockdown through being hosted online by a team of researchers at The Kids Research Institute (formerly Telethon Kids Institute) in Perth.
The 2024 meeting, at Newcastle City Hall, brought old and new friends together in a joyful union of Aboriginal and Torres Strait Islander and non-Aboriginal researchers committed to improving hearing health outcomes for all children.
Central to the purpose of the OMOZ conference is the importance of being inclusive and respectful of Aboriginal and Torres Strait Islander knowledge and culture. The meeting began on 27 August with a ‘Mob Only’ day for about 70 Aboriginal and Torres Strait Islander delegates to get to know one another. This informal discussion of health issues, work practices and other topics of importance aimed to achieve the
Delegates from the ‘Mob Only’ day at OMOZ 2024 at Newcastle City Hall, Australia’s first town hall to fly the Aboriginal flag.
Australia’s first Indigenous ENT surgeon and conference host, Professor Kelvin Kong, AM, opening the conference.
the Worimi Conservation Lands and Murrook Culture Centre, which is north of Newcastle.
The conference program from 28 to 30 August featured keynote speakers and workshops, before delegates attended sessions.
Challenges accessing ENT pathways
A familiar theme throughout many presentations centred on challenges parents and carers of children face in accessing a specialist ENT pathway when concerned about their children’s ear health, hearing loss, speech development, behaviour problems, poor school attendance and performance. According to research findings, the difficulties result from issues ranging from long wait times for appointments to clinicians’ uncertainty in detection, diagnosis and treatment of acute and chronic otitis media and needing to travel long distances to ENT service providers.
In the absence of early childhood screening programs, it is possible for hearing loss to go unnoticed in the developmental years.
Presenters found ear infections and hearing loss occur at increased rates in low socioeconomic urban communities, which often have higher populations of Indigenous Australians, as was seen in urban areas of NSW, WA and SA. In some studies, this can be correlated with crowded housing.
The OMOZ 2024 guest speaker, Dr Shelly Chadha, was the World Health Organization representative responsible for work undertaken by WHO to improve global outcomes on prevention of hearing loss. Trained in India as an ENT specialist, Dr Chadha spoke of the isolation and educational barriers experienced by those living with hearing loss.
She recalled her sadness, as a young medical resident, when asked to treat a girl who had attempted suicide because her ear infection in both ears meant she couldn’t go to school or make friends.
Hearing loss the tip of the iceberg
Dr Chadha likened the global extent of hearing loss to an iceberg, which can appear to be of a certain size on the ocean surface but is much greater in size underwater. She said one billion people were at risk of hearing loss worldwide and warned that, each year, the cost of not delivering adequate hearing health care adds up to one trillion dollars globally.
What can be done to achieve better outcomes in ear and hearing health? Researchers at the conference reported innovative ideas and
images: Hunter Medical Research
Delegates at the conference opening.
Jaimee Rich (left), research nurse, with Sammi Fatnowna, itinerant teacher and ear health educator.
Delegates had a blast sand boarding on sand dunes at Birubi Beach.
The smoking ceremony on Worimi land at Birubu Beach was another highlight.
“Hearing loss is a developmental emergency that drives entrenched disadvantage. The goal is for all Australian children, both Indigenous and non-Indigenous, to have the same chance of having healthy ears and normal hearing, no matter where they live in Australia.”
children. The beauty of investing in ear health training is that capacity to improve detection and diagnosis of ear or hearing problems can be built into many tiers of health service, from the local community health worker to the clinical practitioner or emergency doctor.
surgeon
Prof Kelvin Kong AM OMOZ 2024 host, ENT
Having a trained workforce on the ground in rural and remote regions means people living away from metropolitan areas receive culturally safe ear and hearing primary health care, reducing the need to travel big distances or wait so long for specialist appointments. The meeting discussed the many ways to reduce impediments and delays to ear and hearing health care access but there is so much work to be done.
Technological advances from using artificial intelligence algorithms for describing an image of the ear drum, to growing ear tissue cells artificially in a test tube, are promising new directions from data experts, audiologists and scientists worldwide.
Bacterial ‘slime’ hides from antibiotics
Australian researchers are among the leaders tracking the bacteria responsible for ear infections and conducting clinical trials of vaccines made available over the years. WA scientists have explored the mysterious properties of biofilm, the bacterial ‘slime’ that infections can create, demonstrating the intriguing way bacteria can ‘hide’ from effects of antibiotics. Researchers and remote communities of the NT have run trials of vaccines with potential to protect against some highly infectious strains of bacteria, such as the common Pneumococcal species and H. influenzae that can cause ear disease in children.
During the COVID-19 pandemic years, the increased use of telemedicine made a positive impact on improving access to specialist ENT care in several jurisdictions. For those with the skills to use a video-otoscope and tympanometer, which allows the capture of images and tests vibration of the ear drum, results can be transmitted electronically for viewing by an ENT specialist in a metropolitan centre. This strategy has improved opportunities for rural patients to be seen quickly and locally by a trained ear health care worker who can place them on their pathway to better hearing outcomes.
The OMOZ 2024 conference proved that ear and hearing health research has greatly strengthened in Australia but we are standing on the tip of the iceberg. Much more needs to be done and more support is needed from government, health services, policy makers and medical institutions to ensure our research findings translate into far greater awareness and effective practice.
For the conference host, Professor Kelvin Kong, the goal is for all Australian children, both Indigenous and non-Indigenous, to have the same chance of having healthy ears and normal hearing, no matter where they live in Australia.
Kassandra Waia from Menzies Research Institute.
Keynote speaker Professor Hasantha Gunasekera, a clinical academic pediatrician at The Children’s Hospital at Westmead and board member of the Academy of Child and Adolescent Health.
Dr Guy Cameron, ear health researcher at NSW Health and Indigenous imaging fellow (left) with delegate and speaker Mitchell Aafjes.
Hearing Practitioner Australia is the only dedicated business-to-business publication for the nation’s hearing industry. Established out of a desire for premium, local and independent content for audiologists, audiometrists, otolaryngologists/ENTs and other Australian hearing professionals, HPA brings industry-specific reporting and analysis, in addition to the latest in news, business, products, policy, and research, plus more.
AMPLIFICATION OPTIONS WHEN HEARING AIDS ARE NOT SUITABLE
A/PROF ALEXANDER SAXBY explains which groups may benefit from a bone anchored hearing implant, also referred to as a BAHI.
FOR THOSE IN WHOM HEARING AIDS ARE NOT SUITABLE, CONSIDER IF THEIR HEARING LOSS IS WITHIN THE FITTING CRITERIA FOR A BONE CONDUCTION HEARING IMPLANT AND OFFER A TRIAL USING A HEADBAND.
A/PROF ALEXANDER SAXBY
While traditional hearing aids are effective for most people with hearing loss, there is a subset for whom they are not suitable. These patients can sometimes benefit from implantable solutions which deliver acoustic stimulation in a novel way.
What conditions might render the ear canal unsuitable for conventional hearing aids?
• Recurrent or chronic infection
• wax impaction in extremely narrow canals
• bony exostoses with associated debris
• fi brosis of the tympanic membrane and deep canal (medial canal stenosis)
• congenitally absent ear canal (canal atresia)
• Wide meatoplasty and mastoid cavity after mastoidectomy. This article covers implantable solutions that bypass the ear canal, delivering the acoustic signal to the cochlear. One common device is a bone anchored hearing implant (BAHI) of which several different brands and models exist. Less commonly seen are middle ear implants which direct the vibrational sound signal through the ossicular chain or round window rather than via the skull bone. Both have advantages and disadvantages.
How do BAHIs attach?
Several different products are available that achieve vibration of the skull bone to deliver sound energy to the cochlea. Optimal placement is generally above and behind the auricle which achieves good bone vibration while placing the microphone in an ideal position. They can be placed onto the side of the head using a headband or adhesive patch.
This provides a useful trial of whether the device is adequate for audiological needs. This removable non-operative solution can be a more permanent solution for those too young for surgery, or in whom an operation is contraindicated. In most cases it precedes a more definitive operation in which a secure attachment is made to the bone. BAHIs are classified according to this bone attachment as active or passive.
Passive bone conduction implants
The vibrating component of the implant
ADVANTAGES Improved hearing quality
• Direct bone conduction bypasses middle ear issues
• Can provide clearer sound quality in conductive hearing loss
Comfortable and discreet
• No ear mold necessary
• Small discreet processor behind the ear
Durability
• Low maintenance option with good reliability
• Outer processor can be upgraded
DISADVANTAGES Surgical procedure required
• Generally minimally invasive day-surgery procedure but still carries risks of surgical complications
• Post-operative wound site complications
Cost and availability
• Devices are more expensive than traditional hearing aids but often covered by health insurance or available through government programs
Limited output
• Decibel output and candidacy criteria varies depending on device and brand
• Most devices require the bone threshold to be less than a moderate level but some super-powered devices can extend output to a moderate-severe level
Aesthetic concerns
• Metallic abutments, when used, can be less popular with patients, but magnet options are available
• Different brands vary on how far the device protrudes from the head; some are more discreet than others
is outside the body. Connection to the bone is directly via an abutment which is screwed into the skull bone or via a set of magnets (one under the skin and one attached to the processor) with the internal magnet firmly screwed to the skull bone.
Active bone conduction implants
• The vibrating component is implanted under the skin with a magnet/coil set up to communicate with an exterior processor which houses the battery and microphone.
• There is no attenuation of the signal by the skin so they tend to be more powerful.
• Acoustic feedback is practically eliminated due to lack of external moving parts.
• Placing the vibrational unit internally means the outer processor is smaller and more discreet.
Why not just use BAHIs on everyone?
Firstly, in most cases a conventional hearing aid works well and doesn’t require any operation. Secondly, BAHIs have a maximum output. For single-sided deafness candidates, they generally need to have near normal bone conduction thresholds in the contralateral ear for the device to be useful due to attenuation of the signal crossing over.
If used for conductive or mixed hearing loss ipsilaterally, bone conduction thresholds should ideally be less than
55dB but in some newer more powerful devices they can accommodate hearing loss in a higher range.
This leads to a subgroup of patients in whom conventional hearing aids are contraindicated but who have hearing loss beyond what a BAHI can deliver. This niche is where middle ear implants can be useful.
Middle ear implants
These implants have a vibrating component which is generally attached to the ossicular chain directly, to the short or long process of the incus. They can also be placed onto the round window membrane. Sound energy is more directly coupled to the cochlea so a stronger output can be achieved, in the moderate to severe range. If hearing loss is worse than that, and hearing aids are still contraindicated, patients become candidates for a cochlear implant.
There is nuance and complexity to all this, and exceptions occur. It is always appropriate in difficult cases where the conventional pathway to hearing aids does not seem in the patient’s best interests, to refer to an otologist who will explain alternative options, many of which can be managed by the referring audiologist post-surgery.
ABOUT THE AUTHOR: Associate Professor Alexander Saxby is a paediatric and adult ENT surgeon from Sydney who specialises in hearing implants.
Table 1: Advantages and disadvantages of BAHIs.
UPSKILLING RECEPTION STAFF TO AUDIOMETRISTS
In this two-part series, DR ANNE-MAREE DALEY discusses the importance of training and continuing education particularly upskilling reception staff to audiometrists.
UPSKILLING STAFF MEMBERS TO BECOME AUDIOMETRISTS CAN BE HIGHLY BENEFICIAL FOR BOTH THE BUSINESS AND THE INDIVIDUALS INVOLVED.
DR ANNE-MAREE DALEY
id you know that approximately 70% of people aged 70 and over experience significant hearing loss?
Additionally, one in six Australians suffer from some form of hearing loss.
Unfortunately, this number is projected to increase to one in four by 2050 due to the aging population and increased exposure to loud noise.
Sadly, many people with hearing loss go unmanaged, which can significantly impact an individual’s social, emotional, cognitive, and physical well-being.
Addressing hearing loss through early intervention, support systems, and technological solutions is essential to mitigate these effects and improve overall quality of life.
Hearing health practitioners are well equipped to treat and manage individuals with hearing loss; however, there is an existing shortage of hearing health practitioners, and this is expected to worsen as the prevalence of hearing loss in the population increases.
This shortage leads to longer waiting times for assessments and treatments, reduced quality of care, and limited access to services, especially in rural and remote areas. It is critical to address this shortage to ensure that people with hearing loss receive timely and effective care.
A potential solution involves providing additional training for reception staff in audiology clinics. Efforts should be made to expand training programs, enhance retention rates and utilise tele-audiology.
This series delves into the significance of upskilling reception staff to become audiometrists, enhancing their careers and the overall efficiency and success of audiology clinics.
UPSKILLING RECEPTION STAFF
Reception staff in audiology clinics often serve as clients’ first point of contact. They handle many tasks including, but not limited to, scheduling appointments, minor repairs and management of hearing devices, managing patient records and providing initial patient support and counselling. Their role is pivotal in ensuring smooth clinic operations and a positive patient experience. However, with additional training and education, these staff members
can take on the role of the audiometrist, increasing their value to the clinic and enhancing career prospects. Upskilling staff members to become audiometrists can be highly beneficial for the business and the individuals involved. Reception staff transitioning to audiometrists can offer more comprehensive and seamless patient care due to their familiarity with clinic operations and patient interactions, leading to a more empathetic patient experience.
THE BENEFITS OF UPSKILLING
By focusing on career advancement through upskilling, audiology businesses can create a win-win situation where both staff and business benefit.
1. Enhanced patient care: Reception staff transitioning to audiometrists can provide comprehensive care. Their familiarity with patient interactions and counselling ability, which they already practise within the business, can lead to a more seamless and empathetic patient experience.
2. Career advancement: Offering pathways for reception staff to upskill and become audiometrists provides staff with valuable career development opportunities. By acquiring new skills and qualifications, staff can move into a more specialised and higher-paying role, enhancing job satisfaction and company loyalty.
3. Increased job satisfaction: Offering employees the chance to advance in their careers significantly boosts their job satisfaction. These opportunities communicate a sense of appreciation and value, indicating that the employer is committed to their professional development.This fosters a greater sense of fulfillment among employees, leading to heightened motivation and engagement in the workplace.
4. Higher retention rates: Providing career advancement opportunities can also lead to higher staff retention rates. Employees are more likely to stay with a business that supports their growth and offers clear pathways for advancement. This reduces turnover and associated costs of recruiting and training new staff. It is also easier to upskill staff than recruit staff.
5. Reduced recruitment costs: Recruiting new staff involves significant costs including advertising, interviewing and onboarding. Alternatively, upskilling existing employees can be more cost-effective as it eliminates many of these expenses.
6. Enhanced revenue production: While training to become an audiometrist, reception staff can perform audiometric assessments, improving the clinic’s efficiency. This allows for better resource allocation and reduces the need to hire additional specialised staff. Also, existing staff already know the clinic’s operations, which can lead to increased revenue production, improving the business’s success.
7. Enhanced clinic reputation: A clinic that invests in the professional development of its staff often builds a strong reputation as an employer of choice. This can attract top talent and create a positive work environment, further contributing to the clinic’s success.
8. Investment in training: Training comes with a cost but the long-term advantages of cultivating employees who are in sync with the company’s unique requirements, values and culture can surpass the initial investment. In-house training guarantees that staff acquire the precise skills and knowledge necessary for their roles.
Note: Part two looks at pathways for upskilling and continuing education including the Australasian College of Audiometry’s (AuCA) audiometry certificate, diploma, occupational audiometry course, on-the-job training and mentorship.
ABOUT THE AUTHOR: Audiologist of 19 years Dr Anne-maree Daley is an educator with the Australasian College of Audiometry. She has published articles on hearing health in local newspapers and professional journals including co-authoring research in the Australian and New Zealand Journal of Audiology.
UPCOMING CHANGES TO THE NDIS LEGISLATION
KATY HEWITT helps allied health practitioners and NDIS providers streamline their administrative tasks so they can dedicate more time to patient care. She has some tips so audiologists and audiometrists are prepared for upcoming changes to the scheme.
FROM 3 OCTOBER 2024, A NEW DEFINITION OF NDIS SUPPORTS WILL COME INTO EFFECT, OUTLINING WHAT NDIS FUNDING CAN AND CANNOT BE USED FOR.
KATY HEWITT
As a hearing practitioner, staying on top of changes to the National Disability Insurance Scheme (NDIS) is crucial. From 3 October 2024, new reforms will begin rolling out, directly impacting how providers interact with the NDIS.
These changes will clarify funding, streamline processes, and affect the way services are delivered to participants. Whether you’re already registered or considering registration, these updates are important to understand.
WHAT’S CHANGING?
Several key areas of the NDIS will be impacted by these reforms, with three main updates that directly affect practitioners like you:
1. A new definition of NDIS supports
From 3 October 2024, a new definition of NDIS supports will come into effect, outlining what NDIS funding can and cannot be used for. This updated definition will be designed to make the rules clearer for both participants and providers. All hearing practitioners, whether delivering hearing tests, assessments or fitting hearing aids, will need to ensure that their services align with these changes.
It’s important to review the guidelines carefully to avoid providing services that fall outside of the NDIS funding rules. For example, the NDIS might impose
stricter limits on what’s classified as an essential audiology-related support.
In some special cases, participants may still request funding for supports that are not specifically listed as NDIS supports. This flexibility could allow you to provide additional services but the application process will be more structured. More details will be shared as this change approaches.
2. Budget and plan changes
One significant shift will be how participant plans and budgets are presented. From 3 October 2024, if a participant’s plan is reviewed, they’ll be given a total budget amount instead of a detailed breakdown of individual supports. This change will make it easier for participants to manage their NDIS funds but it also requires providers to adapt to this broader approach.
For hearing practitioners, this could mean a shift in how participants allocate their funding for services like hearing assessments, hearing aids or ongoing therapy. Participants will need to be cautious not to overspend in one area at the cost of others. While the changes offer participants more flexibility, they also carry the risk of misallocation, which might affect their ability to fund all necessary supports.
Initially, all plans reviewed after this date will be for 12 months. In the future, plans could extend beyond this, giving participants more long-term stability.
3.
Streamlining supports
As part of the updates, the NDIS will work to make the system more streamlined for both participants and providers. This includes simplifying access and planning processes, making it easier for participants to understand what services they can access. This will also involve clearer rules for registered providers, and all hearing practitioners will need to ensure they comply with the new requirements.
If you’re already a registered provider, now is a good time to audit your services and ensure they fit within the new guidelines.
For those looking to register with the
NDIS, be prepared for a more thorough and structured process, as changes to registration requirements will likely involve more detailed evaluations possibly including participant feedback.
WHAT YOU SHOULD DO NOW
The changes will kick in fully in October 2024. Here’s what you can do to make sure you are ready:
• S tay updated: Regularly check the NDIS website, ndis.gov.au and subscribe to the NDIS newsletter to stay informed about any new developments or further clarification.
• P repare your practice: Review your current service offerings and make sure they comply with the updated definitions of NDIS supports. Engage your clients early on, explaining any changes to how their NDIS funding will be structured and what it means for their hearing-related services.
• Engage with participants: Proactively communicate with your NDIS participants about the upcoming changes, especially regarding how the new total-budget approach will impact their ability to fund your services. Provide them with guidance on how to manage their funding responsibly.
• R eview your documentation: With stricter regulations coming into effect, it’s important to ensure that your documentation is thorough and up to date. Maintain detailed records of all services you provide to NDIS participants, as this will be crucial if you face an audit.
ABOUT THE AUTHOR: Katy Hewitt is a team leader at Allied Admin Partners, an Australian business providing online administration services for allied health professionals, along with a membership offering exclusive access to free resources and guides tailored for allied health professionals. Email info@alliedadminpartners. com.au, call 0402 651 747 or visit, www.alliedadminpartners.com.au/
BELOW: The NDIS funds several hearing supports if people are not eligible for the Hearing Services Program.
THE NEED FOR OVERSEAS AUDIOLOGY PROFESSIONALS
population, this demand is expected to rise significantly. Audiologists and audiometrists play a crucial role in diagnosing and managing conditions such as hearing loss, tinnitus, and balance disorders.
However, the current workforce is insufficient to meet the growing needs, particularly in regional areas where healthcare services are stretched thin. The shortage of qualified audiologists and audiometrists in these regions has led to increased waiting times and limited access to essential hearing health services.1 We must consider different ways to address this to ensure Australians can access timely hearing care.
Regional and remote areas of Australia face unique challenges in healthcare delivery. Due to the changing demands of a modern workforce looking increasingly for flexibility and urban living, these areas often struggle to attract and retain healthcare professionals such as GPs, nurses, optometrists and audiology professionals.
As a result, Australians are experiencing longer waiting times for audiology services and are burdened with travelling long distances to access care simply because of where they live.
Overseas-trained audiologists can help bridge the gap in service provision. Many countries have well-established audiology training programs that produce highly skilled professionals. By recruiting audiologists and audiometrists from
overseas, Australia can tap into a pool of highly qualified professionals who are ready to contribute to the healthcare system. These professionals bring diverse experiences and perspectives, enriching audiology in Australia.
BENEFITS
• Addressing workforce shortages. The most immediate benefit of recruiting overseas audiologists and audiometrists is addressing workforce shortages in regional areas. They can fill vacant positions, reducing waiting times and improving access to care in underserved regions.
• Enhancing service quality. Overseas audiologists and audiometrists often bring unique skills and knowledge from their training and practise in different healthcare systems. This diversity can enhance the quality of audiology services in Australia by introducing new ideas and approaches to client care.
• Cultural competence. Australia is a multicultural society and having audiologists and audiometrists from diverse backgrounds can improve cultural competence in healthcare delivery. Overseas professionals can better understand and address needs of clients from various cultural backgrounds, leading to more effective and personalised care.
• Professional development. Presence of these overseas practitioners can stimulate professional development among local practitioners. Exposure to different practices and perspectives encourages continuous learning and adaptation, fostering a culture of excellence in the audiology profession.
• Economic benefits. Recruiting overseas professionals can be equally as cost-effective as training new audiologists and audiometrists domestically, and can help to quickly address immediate workforce needs, ensuring that audiology services remain accessible and sustainable.
CHALLENGES AND SOLUTIONS
While benefits are clear, there are challenges including differences in training standards, regulatory requirements and potential language barriers. However, these can be mitigated through targeted support and integration programs.
accreditation. Implementing standardised assessment and accreditation processes ensures they meet Australian standards. Audiology Australia and the Australian College of Audiology (ACAud inc HAASA) have established pathways for overseas-trained professionals to gain recognition and accreditation. A recent ACAud announcement that simplifies the accreditation process for overseas audiologists is most welcome.
• Mentorship and support programs. Providing mentorship and support programs for overseas audiologists and audiometrists can help them adapt to the Australian healthcare system. These can include clinical supervision, professional development opportunities and peer support networks.
• Language and cultural training. Offering these programs can help overseas audiologists and audiometrists overcome communication barriers and better understand the cultural context of their patients. This training enhances their ability to provide effective and empathetic care.
If you're looking for an audiology professional to meet client demand for your business, it's worth exploring overseas-trained professionals to bring a range of opportunities to your practice.
Reference: 1. Audiology Australia 2023 Audiology Qualifications and Training
Name: Nick Taylor
Qualifications: Bachelor of Science, Audiology, University of Manchester, UK
Affiliations: Head of Professional Services and Product – Audiology, Specsavers
Australia and New Zealand
Location: Melbourne
Years in industry: 21
ABOVE: Qualified overseas practitioners can fill
in regional and remote areas.
“THE
CURRENT WORKFORCE IS
INSUFFICIENT TO MEET THE GROWING NEEDS, PARTICULARLY IN REGIONAL AREAS WHERE HEALTHCARE SERVICES ARE STRETCHED THIN."
There is a need for more overseas audiology professionals in Australia. Qualified international practitioners can help fill this gap. Nick Taylor.
Image:
Image: Specsavers.
gaps
People on the move
and patient care to this new chapter with a team who shares her commitment to innovation and patient-centred care.
also services regional visiting sites. Ward is training to see paediatric and complex needs cases in the future. She graduated with a Master of Clinical Audiology from The University of Melbourne in 2023.
Ms Tania Stern has started a new role as learning and organisational development business partner with Demant. She brings 22 years of audiological, sales and operations experience and will facilitate the leadership development curriculum and support PD and continuous learning of employees. After working as a paediatric audiologist at Australia Hearing, she started her career at Demant as a sales rep and product trainer for Oticon AU. She then worked in Switzerland for 12 years as a product development audiologist for Bernafon. Returning to Australia she started with Audika – Demant’s retail arm - as a clinical trainer then a group sales and business performance trainer.
Foundation of Western Australia. In this position, she is responsible for assessing and managing hearing disorders in children. A clinical audiologist with expertise in diagnostics and rehabilitation, she completed her studies at the University of Kelaniya in Sri Lanka. Ranasinghe has extensive experience in the field, having worked for four years as an audiologist at Medcon Hearing Care Centre in Sri Lanka. She then spent six years as a clinical audiologist at Vision Care Hearing Solutions in the Western Province. Additionally, she served as a visiting clinical audiologist at Lanka Medical Audio.
NEW PAEDIATRIC AUDIOLOGIST APPOINTED
Image: Alicia Littledyke.
Image: Ear Science Institute Australia.
Image: Tania Stern.
Image: Shashikala Ranasinghe.
EVENTS CALENDAR
To list an event in our calendar please email helen.carter@primecreative.com.au
OCTOBER 2024
INDEPENDENT AUDIOLOGISTS AUSTRALIA
Audiology for life seminar Melbourne, Australia 11 October independentaudiologists.net.au
ORL2024
NZ Society of Otolaryngology – Head and Neck Surgery annual scientific meeting Hamilton, New Zealand 15-18 October asohns.org.au
HEARING AID ACOUSTICIANS CONFERENCE
68th International Congress of Hearing Aid Acousticians EUHA Congress and Industry Exhibition Hannover, Germany 16-18 October euha.org/
AUDIOLOGY AUSTRALIA
Online Conference 24-25 October audiology.eventsair.com/audaonline24
HEARING IMPLANT COURSE
24th International Victorian Hearing Implant Surgical Course Melbourne, Australia 24-26 October asohns.org.au
3RD ARAB COCHLEAR IMPLANT CONFERENCE
Abu Dhabi, United Arab Emirates 24-26 October arabcic.com
DECEMBER 2024
NEXTSENSE
Day of learning for itinerant teachers of the Deaf Sydney, Australia 6 December Nextsense.org.au
FEBRUARY 2025
HEARING BUSINESS ALLIANCE
Annual seminar Melbourne, Australia 28 February - 2 March hearbusiness.com.au
MARCH 2025
ASOHNS 2025
Annual scientific meeting Sydney, Australia 28-30 March asohns.arinex.one/
APRIL 2025
AUDIOLOGY AUSTRALIA
2025 National Conference Adelaide, Australia 1-4 April audiology.asn.au
NextSense will run a day of learning for itinerant teachers of the Deaf at the Australian Hearing Hub, Macquarie University, NSW, on 6 December.
The 2025 Audiology Australia conference will be at the Adelaide Convention Centre from 1-4 April 2025.
The 3rd Arab Cochlear Implant conference will be in the United Arab Emirates from 24 to 26 October.