READ MORE Fitting success: 98% of patients successfully fitted with two pairs of lenses or fewer1,2*
INJECTION WORRY FOR OPHTHALMIC SECTOR
A controversial policy shift may force some patients into abandoning eye treatments
INVESTING IN FUTURE OF NATIONAL WORKFORCE
Why buying 'Aussie-made' goes beyond just securing a good supply chain for eyecare
TYRANNY OF DISTANCE –A SORRY TALE
The dark truth for some patients living beyond Australia's biggest cities
AUSTRALIA’S LEADING OPHTHALMIC MAGAZINE SINCE 1975
If you want to work for a company that’s passionate about supporting our people to be the best they can be and building a culture where all team members can thrive and everyone feels welcome, valued and proud to belong, you’ll shine at Specsavers. spectrum-anz.com/careersat-specsavers/
INTRAVITREAL INJECTIONS IN HOSPITAL SETTING NO LONGER COVERED BY PRIVATE HEALTH
A controversial intravitreal injection (IVI) policy shift will force some patients into paying out-of-pocket costs they haven’t previously –prompting some to drop out of care altogether – while causing disruption to already-stretched ophthalmology clinics.
Macular Disease Foundation Australia (MDFA), the Australian Society of Ophthalmologists (ASO) and the nation’s largest private ophthalmology provider Vision Eye Institute (VEI) are concerned with the government decision that prevents macular disease patients from making private health claims for anti-VEGF injections performed in private hospitals and day surgeries.
Instead, these people will now need to have their injections performed in private ophthalmology clinics.
change could impact up to 12,200 macular disease patients.
Shutterstock.com & CStock/stock.adobe.com
The procedure can’t be claimed through private health in this setting, so an out-of-pocket cost will likely be required.
It will be the only option left because, as MDFA CEO Dr Kathy Chapman pointed out, “public hospital eye injection clinics and bulk billing private ophthalmology clinics
are either not available, or already at capacity”.
MDFA said the Federal Government confirmed the measure from 1 July 2025.
It estimates 12,200 patients will be affected amid a cost-of-living crisis.
But it also presents a challenge for ophthalmologists who are offering
OPHTHALMOLOGISTS AUSTRALIA’S TOP EARNERS
The average taxable income of Australian ophthalmologists increased almost 9% to $644,898 in the latest official tax data, outranking all other medical specialists and other high-powered careers to become the country’s highest earning profession.
Meanwhile, the average taxable income of optometrists dipped slightly to $102,773, according to new data from the Australian Tax Office (ATO) for the 2021-22 financial year. Optical dispensers and optical mechanics also reported a decrease, while practice managers and orthoptists enjoyed some modest increases.
Breaking down the data by profession and sex, Australia’s 424 male ophthalmologists were the
highest earning group. They had an average taxable income of $756,832 (median $532,388), which was around $50,000 (7.5%) more than the year prior. For the 184 female ophthalmologists, that number was $386,964 (median $252,347), around $40,000 (11.8%) more.
By being the highest-earning profession, ophthalmologists not only ranked higher than other doctors but also law and finance professionals. The second highest earning group (counting both male and female) were plastic and reconstructive surgeons at $608,669, with neurosurgeons knocked off their perch as the highest earning occupation in recent years. Meanwhile, the average taxable income across 5,021 Australian
optometrists was $102,773 (median $92,478). This was around $4,000 (3.7%) less than the year before.
Male optometrists earned $118,536 on average in the latest data, while females earned $92,476.
This was well above the average taxable income of all Australians, which increased from $68,289 to $72,327 in 2022-22, and the median from $50,980 to $53,041. However, the information is limited in nature; for example, it only includes data visible to the tax department and captures annual incomes of all part-time, casual and fulltime workers.
The data showed orthoptists had an average taxable income of $69,529 (median $ 64,834),
IVIs in hospital settings.
VEI CEO Ms Amanda Cranage said it was fortunate that her organisation’s national network could already offer in-clinic IVI services, but shifting the volume of patients from its day hospitals into its clinics “will not be without its challenges from an operational point of view”.
“For example, navigating the concerns of patients who have private health insurance but are no longer given a choice of where their procedure will be performed, as well as safeguarding patients from abandoning their treatment due to cost concerns,” she said.
The contentious measure stems from the Medicare Benefits Schedule (MBS) Ophthalmology Taskforce Review.
Dry eye insights
Optometrist Aidan Quinlan explains his own protocols for subclassifying dry eye, provides his own insights for accurate diagnosis and management, and highlights the benefits of preservative-free lubricating drops tailored to each patient’s symptoms. page 25
continued page 8
The
Images: Numstocker/
Image: Aidan Quinlan.
IN THIS ISSUE
Year in review
More market consolidation and workforce changes were key themes shaping the ophthalmic sector in 2024.
Catching up with Perri
Take a deep breath and dive into the busy world of optometrist, foodie and mother, Jess Perri.
PLAYING THE LONG GAME
There was one comment in a recent healthcare consumer report that shouldn’t scare eyecare professionals, but instead underline their priorities as they navigate a challenging economic environment.
It concerns loyalty – a lynchpin of successful optometry enterprises. For every lost patient, the cost to acquire new ones in their place can be immense. That means playing the long-game (for instance reglazing an existing frame for a budget-conscious customer) over short-term wins can pay huge dividends. Patients remember.
This mindset is crucial right now, if NAB bank’s Health Insights Report 2024-25 is anything to go by. A big shift noted in the report is “a new breed of healthcare consumer” who’s not only taking a more proactive approach to managing their health but showing less loyalty if they feel their needs aren’t being met.
34 Under the microscope
Adelaide congress told how RANZCO has never been under greater government scrutiny.
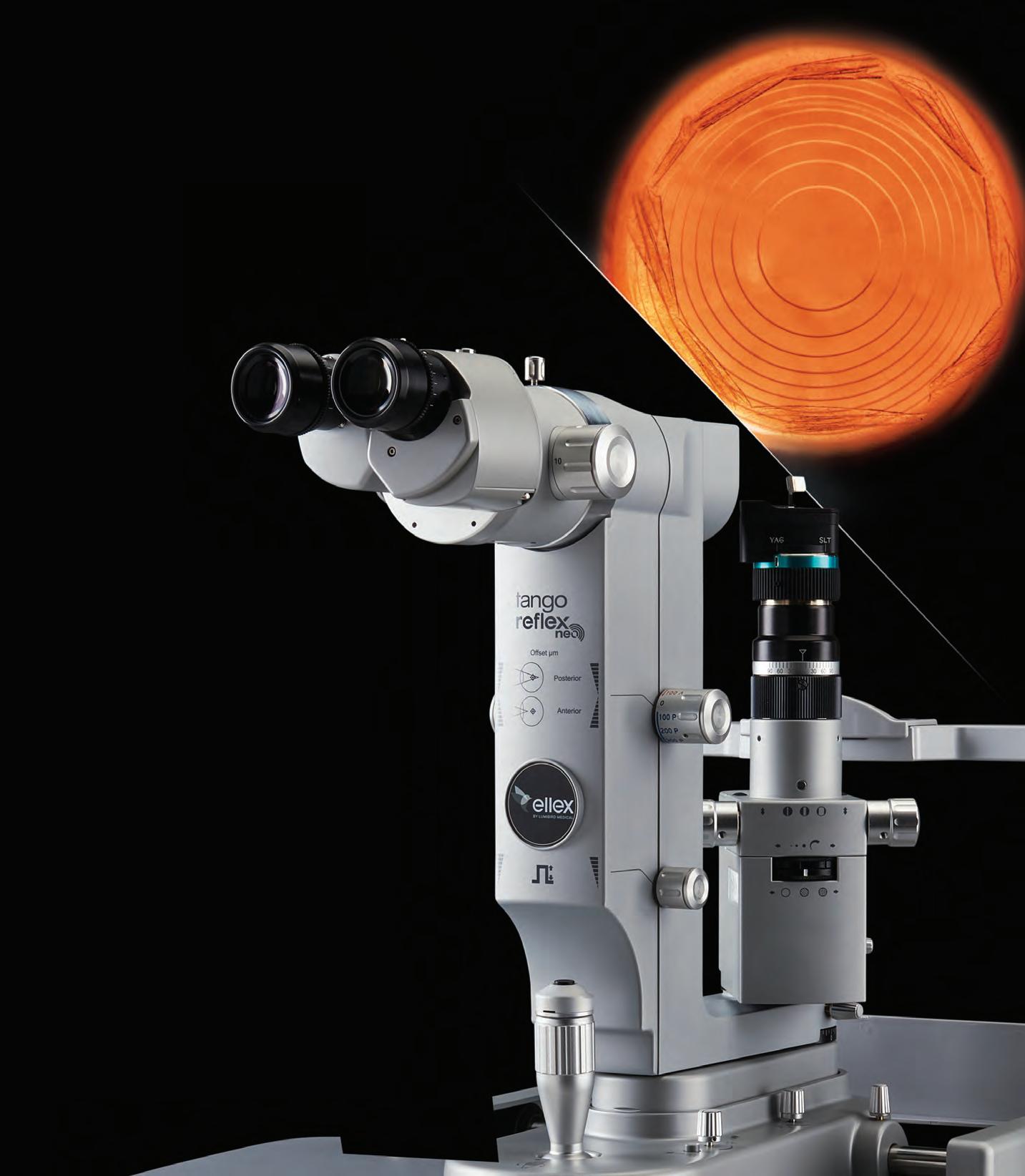
38 A laser-like focus
A South Australian firm is one of few globally with the technical ability to make ophthalmic lasers.
Around a third of dissatisfied patients switched health professionals in the past two to three years. While this number wasn’t as high for optometrists (6%) and specialists, including ophthalmologists (7%), two things need to be front of mind: personalisation and integrity.
These were central pillars in KPMG’s snapshot into the attributes Australian consumers value most when dealing with businesses. Teasing this out for optometry: practices are expected to understand their patients’ wants and needs, while instilling trust they’re doing the right thing by them.
This raises the chances of a word-of-mouth referral when expectations are met, and they’re also more likely to return themselves.
But how does one do business with a smile on their face while being challenged by high interest rates and more price-sensitive consumers?
Afterall, almost 40% of patients didn’t see their optometrist or specialist because they couldn’t afford it during the past year.
It shows that now is arguably a time to dig deep on two fronts: trimming fat within the business while adopting a patient-first mentality.
Whether it’s knowing patients by name, securing a fair deal on your lease, or figuring out how your practice is performing against key benchmarks like own-frame usage, second-pair sales and wage percentage, it’s vital to remember the details matter in times like this. From little things, big things really can grow.
MYLES HUME Editor
UPFRONT
Just as Insight went to print, the Federal Government's landmark scope-of-practice review was released.
The ‘Unleashing the Potential of our Health Workforce’ report was headed by Professor Mark Cormack and covered health professions working outside of hospital settings, including optometrists and orthoptists. The year-long review found virtually all the nation’s health professions are held back by restrictions and barriers unrelated to their skills, training and experience. The probe of national
WEIRD
India’s ruling BJP party has come under fire after reports patients in hospital for cataract surgery in Gujarat had been woken up and convinced to sign up as party members. The hospital vowed to investigate the matter, as did the BJP which condemned the ploy and said it “might be a conspiracy to defame the BJP”, the New Indian Express reported.
WONDERFUL
Lions Outback Vision has been announced the winner of the Western Australian Government’s Pilbara healthcare initiative, The Challenge. The group took the $5 million top prize with Australia’s first mobile retinal camera with fully integrated artificial intelligence, which screens for eye diseases like diabetic retinopathy. The technology helps diagnose sight-threatening disease on-the-spot, providing crucial early detection for individuals in remote areas.
WACKY
Rising Australian golfer Mr Jeffrey Guan suffered a career-threatening eye injury when he was hit by a golf ball. Golf Australia reported that the ball was struck by his pro-am playing partner in the NSW Open regional qualifier at Catalina Golf & Country Club on the NSW far south coast. He was seeking specialist treatment at the Sydney Eye Hospital.
health settings also highlighted a number of issues potentially holding back the ophthalmic sector, including practitioner title protection and the “unnecessarily complex” process to make reforms around issues like drug prescribing. Federal health minister Mr Mark Butler is now reviewing the report’s 18 recommendations. IN OTHER NEWS , older drivers may soon need eye tests from an optometrist or ophthalmologist before driving in South Australia, under a new plan to make roads safer. That is one of two key changes being discussed by a number of medical and road safety groups.
It’s hoped the recommendations would alleviate concerns for GPs who complete the assessments, especially in borderline cases. FINALLY, the Royal Australasian College of Surgeons, which counts ophthalmologists among its ranks, is implementing one of the most significant governance overhauls in its near 100-year history. After receiving overwhelming support from its membership, with 82.6% of votes in favour, the college has an updated constitution to strengthen financial and risk management as it “navigates the complexities of the modern governance environment”.
Health imbalance
People are waiting an average of 69 days for cataract surgery in Australian cities, with that nearly doubling in the outer regions (129 days) and very remote communities (114 days). Page 43
WHAT'S ON
THIS MONTH
ISOO 2024
3 – 7 December
The International Society of Ocular Oncology is heading to Goa, India, with sessions to focus on tumours of the eyelid, adnexa, ocular surface disease, uvea, retina and orbital issues. iapb.org
Published by:
Complete calendar page 56 insightnews.com.au
NEXT MONTH
SKI CONFERENCE
18 January
The next Ski Conferences for Eye Care Professionals is heading to Sun Peaks Ski Resort, Canada. Eyecare professionals, including orthoptists and optical dispensers, are invited for the event. skiconference.com.au
Finalised in 2020, it recommended reclassification of item 42738 into a Type C procedure that does not “normally need hospital treatment”.
In-hospital intravitreal injections should occur in fewer than 3% of patients, the taskforce said, but in reality occurs in 18%, and is increasing. The committee felt “this is largely unnecessary and may be due to financial incentives”.
“This recommendation focuses on reducing low-value care,” it said.
Chapman said MDFA was concerned that with many people already feeling the cost-of-living pinch, macular disease patients previously accessing IVIs through private health would now have another expense to add to their budget.
“Macular Disease Foundation Australia is concerned that this will force people to give up their treatment altogether because they will no longer be able to afford it.”
Decision may ‘compound’
issues
Dr Chapman said MDFA had previously said it would only support the reclassification of this MBS item if there had been a significant increase in the number of public outpatient clinics offering bulk-billed eye injections.
The organisation had several recommendations to improve adequate and equitable access, including an ophthalmology practice incentive to bulk bill IVIs for age pensioners with AMD.
“We know that the cost and affordability of treatment are still huge concerns for
many people living with macular disease, and there are still limited options to receive bulk-billed treatments,” she said.
Dr Chapman said MDFA had raised these concerns with the office of health minister Mr Mark Butler and would continue to.
“The Australian, state and territory governments must step up to improve access to eye injections,” she said.
“Our message for government is that investing in increased access to eye injection treatment for people with macular disease will not only save the sight of tens of thousands of people but will also save the government billions of dollars in the long term.”
Cranage said VEI recognised these barriers – cost being the most prohibitive – and in 2016 established its first purpose-built, low-cost IVI injection clinic in Boronia, Victoria. But it continued to offer various cost options to patients across all VEI clinics, including the day theatre setting or as an outpatient.
But she was concerned for patients currently receiving injections in theatre with no out-of-pocket cost. This would be alongside their private health insurance premium which she presumed wouldn’t decrease and may be unaffordable for some.
“We can only assume some patients will be forced to forego some injection appointments due to cost and access to affordable in-room injections. This will have a devastating impact on their sight and quality of life,” she said.
“Patient care is at the core of what we
“WE KNOW THAT THE COST AND AFFORDABILITY OF TREATMENT ARE STILL HUGE CONCERNS FOR MANY PEOPLE LIVING WITH MACULAR DISEASE.”
DR KATHY CHAPMAN, MDFA
do, and knowing this decision will impact thousands of patients’ access to the care they need is why we are committed to offering a range of cost options for injections across all VEI clinics.”
ASO president Dr Peter Sumich said the IVI situation was “a conundrum”. He called it a “Pandora's box” that was opened years ago when IVI was not a significant budget item, but was now best left to the business marketplace to sort out.
“It’s like a Rubik’s Cube being turned without a clear solution,” he said.
“To spell out the complexity: at present, in private settings, the Federal Government doesn’t have to fund the full IVI procedure but does fund the drug.
“In public hospitals, the state has to fund the drug but not the procedure. The insurers fund the procedure in private day surgeries, but not the drug, and this funding provides a welcome service to their policy-holders. Whilst the insurers resent the cost it does make their policy-holders happy.
“If private surgeries are not able to acquire funding then the cost may fall back on state governments who cannot even manage the small number of patients they service now.”
Alternately, he said it might fall to the Federal Government, which would be hit for the treatment, plus procedure, plus safety net.
“So in summary, it is convoluted, hard to explain simply, and a change in the system will probably hurt everyone, even the private insurers who will be assailed by their policy-holders who currently enjoy no gap funding,” he said.
INCOMES DIP FOR SOME WORKING IN OPHTHALMIC SECTOR
continued from page 3
a modest increase on $68,200 in the preceding 12 months. The profession is female dominated, with 919 women versus 129 men. Females earned $67,797 on average and men $81,870.
For optical dispensers, the average taxable income was $42,561 ($48,512 males and $40,944 for females), down from $45,000 (6.4%) the year prior. Optical mechanics earned $64,824 on average (males $65,865 and females $63,126), down from $66,600.
Health practice managers earned a healthy average taxable income of $83,205 (median $70,264), up 3% from
The ATO figures also revealed the average income of medical and pharmaceutical sales representatives, which was $124,903.
The 2021-22 data is the latest available.
The average optometry income was $102,773. Image: Mongkolchon Akesin/ Shutterstock.com.
Top 10 earning professions (men and women grouped together):
• Ophthalmologist - $644,898
• Plastic and reconstructive surgeon – $608,669
• Neurosurgeon – $593,221
• Otolaryngologist/ENT – $576,925
• Urologist – $543,818
• Cardiologist – $513,526
• Orthopaedic specialist – $504,563
• Vascular surgeon – $490,193
• Cardiothoracic surgeon – $473,371
• Judge – $459,843
Image:
OPTOMETRISTS RATE WELL IN AUSSIE CONSUMER SURVEY
Optometrists are a caring, empathetic bunch who are very good at listening to their patients and offer outstanding value for money.
Those are the key takeaways from the latest Health Insights Report 2024-25, commissioned by NAB bank, which surveyed 2,000 Australians in mid-2024 about the way they perceive and experience healthcare.
The 13th report covers a number of areas, including overall satisfaction with healthcare provided by all disciplines, value for money, communication and language used, ease of access, and the quality of the practice environment.
Mr John Avent, NAB’s Health and Medfin executive, said the survey showed that cost-of-living pressures might be beginning to impact health decisions.
“One in two Australians told us affordability was a key reason they had avoided seeing a health practitioner, like a GP or a dentist, in the past 12 months for a health concern – a trend that may risk delayed diagnosis and treatment,” he said.
He said the most important insight was the attitude of consumers, post-COVID.
“We’re seeing a new breed of healthcare
consumer who is not only taking a more proactive approach to managing their own health but showing less loyalty if they feel their needs aren’t being met. Around a third of patients switched a health professional in the past two to three years.”
In last year’s consumer snapshot, optometry scored the highest of all disciplines in terms of overall satisfaction. In the latest survey it lost that spot to vets.
But it was still rated near the top of all disciplines in most categories surveyed. GPs, pharmacies and dentists remain the most commonly visited or used health practitioners by Australians. In 2024, 71% of people had visited a GP in the past 12 months –albeit down from 73% in 2023 and 78% in 2022. Visits to optometrists fell slightly over the year (33% vs. 35%) but were still somewhat higher than in 2022 (28%).
When they did visit, patients found optometrists to be among the most caring and attentive of all healthcare practitioners. When asked if those professionals really listened to them, optometrists came out on top at 8.1 pts out of a possible 10, followed by pharmacists and vets (8.0 pts).
Consumers gave optometrists a thumbs up for value for money. Image: Syda Productions/stock. adobe.com
2024, the most common issue cited was affordability. Around four in 10 said that was the main barrier to visiting optometrists (39%). Lack of time was highlighted by 28% of those surveyed. The poll noted a large increase in the number who said optometrists (49%, up from 40%) cost more. This was particularly prevalent in rural towns.
Despite those concerns, with a score of eight out of 10, optometrists were second only to pharmacies (8.1 pts) for the value of care, advice or treatment provided, and around seven in 10 believed optometrists provided ‘excellent’ value.
IN BRIEF
MORE SLT EVIDENCE
A deeper analysis of the landmark Laser in Glaucoma and Ocular Hypertension (LiGHT) Trial – that ultimately recommended selective laser trabeculoplasty (SLT) as a first-line glaucoma intervention – has shown the disease progresses 29% slower in patients with this method compared with eye drops. “Selective laser trabeculoplasty should not only be considered an effective and safe alternative to medications as a first-line treatment for primary open-angle glaucoma but can also offer an advantage in reducing vision loss,” said lead researcher Dr Giovanni Montesano, of Moorfields Eye Hospital in London. The new study was presented on 20 October 2024 at AAO 2024, the 128th annual meeting of the American Academy of Ophthalmology.
ODMA-ACBO AGREEMENT
The Optical Distributors and Manufacturers Association (ODMA) has announced that the Australasian College of Behavioural Optometrists (ACBO) will be hosting its annual conference in conjunction with ODMAFair25. ACBO Connect 2025 will take place on Friday 27th and Saturday 28th June, 2025 at the International Convention Centre in Sydney. ODMA said the partnership “brings two of the most significant events in the optical industry together, offering an unmatched opportunity for optometrists, vision therapists, and industry professionals to enhance their learning, network with peers, and discover the latest innovations in the eyecare sector”.
SEEWAY LAUNCHES
Guide Dogs NSW/ACT has launched SeeWay, its new subsidiary brand and pilot program offering Australia’s first comprehensive network of support for people with low vision. A statement said SeeWay aimed to transform how eyecare professionals offered ongoing support to people experiencing permanent changes in vision due to conditions like genetic disorders, macular degeneration, glaucoma, or diabetes – conditions that often leave people feeling unsure of where to turn for practical resources and emotional support. “Many of these people do not qualify for formal disability funding, though they are in no less need of assistance in navigating daily life,” the release said. “SeeWay is designed to bridge this gap, offering a pathway for individuals to access the guidance and support they need earlier.”
REVIEW OF CERT IV IN OPTICAL DISPENSING UNDER WAY
Employers offered opinions in 12 meetings held across the country. Image: Image: Adrian Chinery/ Shutterstock.com.
A major review of the optical dispensing qualification, the first in a decade, is under way to bring the training course into line with contemporary industry practices.
As part of the measure, practice owners and employers of optical dispensers were invited to attend workshops around the country to have a say on updating the HLT47815 Certificate IV in Optical Dispensing qualification.
Directors at the Australasian College of Optical Dispensing (ACOD), with Optical Dispensers Australia (ODA) and other industry supporters, have pushed for the review “to ensure the sector remains vibrant, relevant and well-equipped to contribute effectively to Australia’s needs”.
According to ODA, it has been 10 years since the current optical dispensing qualification was last updated, leaving parts of the course “lagging behind when it comes to current industry advancements and technology”. This includes areas such as myopia management and the use of digital dispensing instruments.
Registered training organisations (RTOs) that deliver the Cert IV course, such as ACOD, must adhere to the training package
set by external parties, regardless of how long ago it was last updated.
“For optical dispensing, this includes teaching several core and elective units that have become outdated since the last update in 2015,” ODA said.
HumanAbility, a not-for-profit, industry-led Jobs and Skills Council funded by the Australian Government, is leading the review.
The organisation requested ODA, as a leading body representing the optical dispensing profession, to ask employers to participate in face-to-face or online workshops during November and December 2024 to build a picture of what the future optical dispensing qualification should look like.
With 12 physical meetings held in centres across the country and three online sessions, the aim of the workshops was to thoroughly understand the current and emerging needs within the sector.
The analysis and review will focus on updating qualifications to reflect current industry practices, improve career pathways, enhance the safety and quality of training to meet today’s industry requirements, and anticipate future challenges.
ALCON’S NEW CATARACT AND VITREORETINAL SYSTEMS ARRIVE
Alcon’s anticipated Unity surgical portfolio have now been included on the Australian Register of Therapeutic Goods (ARTG) and notified to the WAND database in New Zealand.
The company’s Unity Vitreoretinal Cataract System (VCS) and Unity Cataract System (CS) were unveiled at the RANZCO Congress in Adelaide.
Both are designed to deliver greater workflow efficiencies over Alcon’s current systems, Constellation Vision System for vitreoretinal and combined procedures, and Centurion Vision System with Active Sentry for cataract surgery.
Unity VCS is now Alcon’s most advanced vitreoretinal and cataract surgical innovation combined together in one platform, providing “surgeons and technicians the benefits of maximised operating room space with just one device”. And Unity CS is a standalone cataract system.
Alcon said the systems leverage a novel phacoemulsification modality to deliver up to two times faster nucleus removal with
40% less energy into the eye. In vitreoretinal advancements, the new technology offers cutting speeds of up to 30,000 cuts per minute. The platform offers surgical stability and efficiency with a unique proprietary fluidics system, says Alcon.
“We are excited to announce that our latest breakthrough technologies, Unity VCS and Unity CS, have received regulatory approval in Australia and New Zealand,” said Ms Penny Stewart, Alcon ANZ’s country manager and cluster franchise head of surgical.
“Unity VCS and Unity CS build on Alcon’s expertise in surgical equipment with pioneering innovations for vitreoretinal and cataract surgery – driving advancements from cutting speeds to fluidics management, to ergonomics and workflow. We are looking forward to continuing to gather real-world user experiences before we introduce these technologies in 2025.”
Alcon has tested the Unity systems during in wet lab sessions with more than 200 surgeons from 30-plus countries.
The new portfolio was released at November’s RANZCO Congress in Adelaide. Image: Konektus Photo/ Shutterstock.com.
Dry Eyes? Restore the tear film with every
blink® Intensive Tears
Long lasting relief from the feeling of dry, tired eyes. An advanced lubricating eye drop specially formulated to provide protection and comfort for the eyes that are dry, irritated or uncomfortable.
• With hyaluronic acid
• May be used with contact lenses
For more information contact your Bausch + Lomb
blink® Intensive Tears PLUS
A thicker, more viscous advanced lubricating eye drop formulation that adapts to your dry eye needs and provides long lasting relief.
• Specially formulated for enhanced ocular comfort
• Recommended for both day and night use
• With hyaluronic acid
• For Moderate to Severe Dry Eye
What 2024 had in store
Further consolidation of the national optometry market, controversy over medical workforce changes and an update on the world’s first whole-eye transplant were among the major headlines shaping the ophthalmic sector.
KEY BUSINESS HIGHLIGHTS
If there was a gong for the biggest and most frequent business news in 2024, it would have gone to EssilorLuxottica. One can feel the momentum building behind the world’s largest optical company, since the two giants joined forces in 2018.
Locally, the biggest news came in January with the acquisition of EyeQ Optometrists and its 25 practices. Founded in 2007, the Australian-owned, optometrist-led company has a nationwide presence, with the majority in New South Wales. After “regular approaches from interested parties” the founders decided the best fit was EssilorLuxottica which was attracted to “the complementary nature of its practice network” and will retain the EyeQ brand.
Globally, EssilorLuxottica acquired an 80% stake in Heidelberg Engineering, best known for its high-end OCT machines, which coincided with another thought-provoking deal – taking over the Supreme clothing brand for AU$2.2 billion.
The other big local acquisition of the year was George & Matilda (G&M) Eyecare’s deal with National Optical Care. Involving 26 practices, it’s the biggest in G&M’s eight-year history. But the network did several smaller acquisitions throughout the year, with 35 in total.
Owndays is one to watch too. The Japanese optical retailer – with more than 550 stores globally – moved the dial in Australia by opening two locations at Westfield Hurstville and Westfield Burwood. It now has four locations here.
Specsavers’ strong presence in Australia was confirmed in some impressive revenue figures. The Australian business contributed £874.5 million (AU$1.69 billion) to its global revenue of £4.01b (AU$7.74b) to February 2024. That’s 17.7% above the previous year and comfortably places Australia as Specsavers’ second biggest market.
The independent market also performed well in tough economic conditions. Eyecare Plus grew above 7% on average across its network and is expected to continue this momentum with initiatives like its new Entrepreneurs Club to really take root in 2025.
WORKFORCE ISSUES
Two issues dominated workforce issues this year: bolstering the volume of medical professionals in Australia, and remote optometry consultations. On the former, the Australian Health Practitioner Regulation Agency (Ahpra) has streamlined the registration process – as recommended in the ‘Kruk’ independent review – resulting in a surge of new international medical practitioners, with 1,205 more registered in the 2023-24 financial year than in the previous 12 months.
ABOVE, L to R: Co-presidents Dr Jacqueline Beltz and Prof Gerard Sutton at AUSCRS 2024 on Hamilton Island; Specsavers' reported a record 246-strong graduate cohort.
With ophthalmology to be targeted in 2025, the Australian Society of Ophthalmologists (ASO) fears the policy-shift will end up sidelining RANZCO and other medical colleges from the vetting process. And the Royal Australian College of GPs has put health ministers on notice, stating they bear all responsibility for anything that goes wrong with their “rushed process”.
Remote optometry took off in the Australian optometric landscape in 2024. OPSM began rolling this out where patients are taken through the consultation alongside a trained technician, while the optometrist beams in remotely from another part of Australia.
With Specsavers also developing its own model, it’s hoped this new approach – supported by high-tech systems – will improve eyecare access in hard-to-staff areas of the country while offering newfound workforce flexibility.
As Specsavers celebrated its biggest graduate cohort in 2024 with 246 joining the business, the national optometry workforce surpassed 7,000. A quarter of Australian optometrists are now also 29 years or under.
Contributing to this, 40 new optometrists entered the workforce as part of the inaugural graduate cohort from the University of Western Australia optometry school, with every student securing employment and 90% staying to work in WA.
ABOVE: Five Australians featured in The 2024 Power List (top left, clockwise): Prof Keith Martin, Prof David Mackey, Prof Robyn Guymer, Dr Ben LaHood and Prof Stephanie Watson.
JANUARY
KEY DECISIONS AND POLICIES
There were some noteworthy changes to Medicare from March 2024. One of the biggest was a new item for a third visual field test in a 12-month period for patients with a high risk of glaucoma progression.
Other changes related to contact lenses where the government agreed to combine 10921, 10922, 10923 and 10925 into a single item and reword the explanatory notes to remove the requirement to deliver the lens.
Also, for foreign body removal the descriptor was amended for 10944 to clarify the requirement for complete removal of the rust ring with a ferrous embedded foreign body, and to provide more clarity around when this item can be claimed.
Optometrists and ophthalmologists faced another Ahpra registration fee hike. Even though it was modest – optometrists will pay a $14 increase (4.1%) and ophthalmologists and other medical professionals $32 more (3.2%).
Amid an Ahpra crackdown on non-surgical cosmetic procedures, optometrists seeking to expand into “ocular aesthetics” – with things like intense pulsed light, bipolar radiofrequency and micro needling – were urged to consider implications around their professional indemnity insurance (PII) cover, and remain on top of proposed regulations determining how these can be marketed to the public.
Changes may be afoot for ophthalmologists over 70 as data revealed complaints jump significantly as doctors get older. The Medical Board of Australia wants to introduce general health checks with a GP for late career doctors in a bid to improve public safety.
The Labor Government’s election promise for 60-day scripts also became a reality for ophthalmic patients seeking dry eye and glaucoma medications in 2024.
PEOPLE AND LEADERSHIP
In one of Insight’s most-read stories of the year, five Australians made The Ophthalmologist magazine’s Power List. They were Melbourne’s Professor Keith Martin and Professor Robyn Guymer, Adelaide’s Dr Ben LaHood, Sydney’s Professor Stephanie Watson, and Western Australian Professor David Mackey.
The sector shone in both the Australia Day and King’s Birthday honours.
On Australia Day, Emeritus Professor Christian Lueck AM, retired Melbourne optometrist Mr Michael Aitken OAM, and Ms Sandra Knight OAM for her contributions to low vision, were recognised.
For Kings Birthday, six industry figures were acknowledged. They were: ophthalmologists Professor Glen Gole AM, Dr Diana Semmonds AM, Dr James Elder OAM, Northern Territory optometrist Ms Helen Summers OAM, and Ms Emma Elizabeth Stanford, a senior research fellow in Indigenous Eye Health Unit in Melbourne.
The Optometry Board of Australia appointed a new chair in Mr Stuart Aamodt, an independent optometrist from Perth.
CERA’s deputy director and head of ophthalmic neuroscience, Professor Peter van Wijngaarden, is now leading The Florey, the largest brain research centre in the Southern Hemisphere. He is continuing his association with CERA as an honorary researcher.
Prominent Australian optometry academic Professor Sharon Bentley, from Queensland University of Technology, was appointed the new dean of the University of California, Berkeley, optometry school.
There were some big movements in ophthalmology too. Dr Justin Sherwin became the new director of Peninsula Eye Centre, Mornington, previously operated by Dr Rick Wolfe for more than 35 years. Dr Loren Rose started at Sydney Eyecare Burwood as a director, and Dr Eve Hsing and Dr Delia Wang joined OKKO Eye Specialist Centre in Queensland.
Optical Dispensers Australia reshuffled its advisory board, with Tokai Optical Australia general manager Mr Justin Chiang and Opticare director Mr Michael Nasser joining Ms Jessica Kingsley – a technical sales and product application specialist at ZEISS Vision Care ANZ – and Will Street Eyecare (Bendigo, Victoria) optical dispenser-practice manager Ms Sarah Thompson.
MARCH
APRIL
AUGUST
OCTOBER
SEPTEMBER
NOVEMBER
Registration fee hike for eyecare professionals
RANZCO Congress took place in Adelaide with 2,222 attendees
Policy shift revealed affecting anti-VEGF injections in hospital settings
JUNE
George & Matilda acquires National Optical Care
Rayner unveils ‘world-first’ spiral IOL
EssilorLuxottica acquires EyeQ Optometrists.
National optometry workforce surpasses 7,000.
Robotic cataract surgery debuted at ASCRS
THERAPIES AND EQUIPMENT
Rayner’s new spiral intraocular lens (IOL) – a world-first design called Galaxy and Galaxy Toric – was one of the big product announcements for 2024. It has Therapeutic Goods Administration (TGA) approval and will be available through reimbursement soon.
The TGA also approved the evolution of two key products in the ophthalmic sector.
Eylea 8mg, a higher dose of aflibercept allowing for longer treatment intervals, was cleared for adults with neovascular aged-related macular degeneration (nAMD) and diabetic macular oedema (DME).
Glaukos’ new iStent infinite Trabecular Micro-Bypass System was approved too; the key upgrade being the inclusion of three stents – as opposed to two – preloaded into a newly designed auto-injection system offering unlimited delivery attempts.
Australian-based Eyerising International, whose repeated low-level red-light (RLRL) therapy was approved for myopia in 2023, addressed safety concerns about its device. The company responded to several “inaccuracies and misrepresentations” in a paper published in Ophthalmic & Physiological Optics (OPO) journal. In other news, the Tokyo Medical and Dental University (TMDU) introduced the company’s RLRL for its myopia patients.
It was hoped Australia would have its first-ever approved therapy for geographic atrophy in 2024, but this didn’t eventuate.
One of Australia’s foremost macular disease experts, Professor Robyn Guymer, said the biggest challenge for the two leading drugs has been obtaining market clearance in Europe. Despite them being approved in the US, one issue has been that the trials were not able to show a visual acuity benefit in the treatment group. But she questioned the emphasis on this when it’s all about how much longer central foveal vision can be saved. Plus, it’s common to have good visual acuity until very late in the disease.
It was also a big year for ophthalmic microscope innovations, with Bausch + Lomb installing its first Australian SeeLuma at Mater Private Hospital Redland in Brisbane under Dr Sunil Warrier, and ZEISS releasing its ARTEVO 850 3D visualisation system and ARTEVO 750 microscope.
Alcon released the 1.5 update for its NGENUITY 3D visualisation system, and at RANZCO unveiled its new UNITY Vitreoretinal Cataract System and UNITY Cataract System, to replace the Constellation Vision System and Centurion Vision System with Active Sentry, respectively.
KEY EVENTS AND TRADE SHOWS
O-SHOW24 was a success at Sydney’s Hordern Pavilion in May, concluding with close to 1,000 visitors over two days. Hot on the heels of the event, the Optical Distributors and Manufacturers Association (ODMA) announced
a shake-up of its events program with ODMAFair returning to Sydney in June 2025. The organisation is living up to its reputation as a leader in this space, creating new efficiencies across the sector by combining the event with the Australasian College of Behavioural Optometrists annual conference – ACBO Connect 2025 – and Optometry NSW/ACT’s Super Sunday clinical conference.
AUSCRS 2024 on Hamilton Island was a highlight, with the emergence of extended depth of focus (EDOF) IOLs taking centre stage at an event that was both fun and scientifically sound.
The Specsavers Clinical Conference – now in its 13th year – was a big hit too. This time it was on the Gold Coast with more than 400 optometrists attending in-person and another 450-plus watching online from around Australia and New Zealand.
As is tradition, the RANZCO Congress rounded out the year with some heavy hitting speakers from Australia and abroad. But it was outgoing president Dr Grant Raymond’s comments about the college’s future relevance that made everyone sit up and take note.
At the Adelaide meeting, he said the college had never been under greater government scrutiny, with its power to assess the suitability of specialist international medical graduates (SIMGs) and accredit public hospital training posts in jeopardy.
“Should SIMG assessment and hospital training post accreditation be taken away from colleges, RANZCO’s role will be substantively changed. RANZCO is somewhat a recipient of collateral damage from some problematic issues with other colleges,” he said.
RESEARCH AND BREAKTHROUGHS
The ophthalmic sector received an update on how the world’s first whole eye and facial transplant was progressing. After 18 months, the team of more than 140 surgeons reported no sign of rejection and some indication of retinal response to light stimuli.
The promise of CRISPR gene therapy took another encouraging stride after the landmark BRILLIANCE phase 1/2 trial demonstrated 11 out of 14 treated participants experienced some improvements in vision and quality-of-life measures. All were born with a form of Leber congenital amaurosis caused by mutations in the centrosomal protein 290 (CEP290) gene. The trial included the first patient to ever receive a CRISPR-based investigational medicine directly inside the body.
US cataract surgeon Dr David Chang debuted a novel robotic cataract surgery procedure on a porcine eye at the American Society of Cataract and Refractive Surgery (ASCRS) conference.
A deeper analysis of the well-known Age-Related Eye Diseases Studies (AREDS and AREDS2) revealed something important for eyecare professionals: that certain supplements can slow disease progression in geographic atrophy. Previously, AREDS2 supplements were known to slow intermediate to late AMD.
Locally, a study published in Public Health Research & Practice by UNSW researcher Dr Angelica Ly, found around a quarter of Australian eyecare patients are avoiding treatment due to cost reasons, pointing to the impact of declining Medicare rebates and a mismatch between subsidised care and practising patterns.
In significant local research grants, at least eight ophthalmic research projects were awarded as part of the National Health and Medical Research Council (NHMRC) program.
The big winners were Flinders University’s Professor Jamie Craig and Professor Justine Smith for their respective projects on:’Expanding the indications for polygenic risk testing in glaucoma’ ($2,476,520); and ‘Addressing the greatest unmet needs in uveitis’ ($2,953,040).
Associate Professor Andrew White, from the Centre for Vision Research at the Westmead Institute for Medical Research in NSW, received Glaucoma Australia’s 2024 Quinlivan research grant. He will use the funding to focus on the development of Irbesartan as a potential therapeutic agent for glaucoma.
OPSM began rolling out remote optometry.
Image: EssilorLuxottica.
Family and food are the key things that fuel optometrist JESS PERRI. But, as she tells Insight, her passion for diet and nutrition is also benefiting her wider family of patients.
Taking a breather with Jess Perri
Ms Jess Perri never had a chance.
Carried into the optometry business even before she was born as her mother worked through pregnancy, and then adopted by that family of patients who saw her as one of their own, a profession in eyecare was practically in her DNA.
But it was a dusty old university tome that sealed the deal.
“I think it was Wolff’s Anatomy of the Eye and Orbit, with graphic images of what I recall being bacterial keratitis, and this huge ulcer on the cornea,” she says.
“I remember showing my mum and being like, this is kind of gross, and this is kind of cool, which is probably not a common thing for a six-year-old.”
There’s little about the healthy, energetic 37-year-old’s life that could really be described as ‘common’.
Her roll-call of achievements and activities would have most collapsing into a couch and nursing a sleepy tea: busy optometrist, reality TV chef, avid pasta maker, teacher and company founder, passionate advocate for the role of nutrition in good health, distance runner.
Oh, and there’s two young children – seven-year-old Maya and Henry, who is four.
Family is at the heart of Perri’s story. It’s the focal point for so many of
her endeavours, whether that family is the one she shares a house with, the people with whom she shares her pasta-making skills, or the wider family whose vision she is entrusted with at Dr Optical in Glen Iris and clinics elsewhere in Victoria.
Family, food, and the guiding, inspirational arms of strong women.
All were delivered in large and lively helpings in her grandparents’ kitchens, where her two Nonnas taught an eager three-year-old Jessica how to make pasta, instilling the gift of good food for the family and beyond.
“A lot of my childhood, after school, on the weekends, school holidays, was spent cooking with my grandparents, and I learned a lot of the basic pasta shaping from when I was very young,” she recalls.
“I learned the Italian alphabet before I learned the English one.”
The lessons continued in her “second home” – her mother Ms Elena Perri’s optometry practice in Huntingdale, Melbourne, which opened in 1983.
She practically grew up watching her mum caring for an extended family of patients while running a successful practice and pioneering early skills in myopia management.
Her mother was the “pinnacle of a successful woman . . . the child of Italian migrants who not only went to university but then opened two practices”.
“So she was a driven, career-focused woman who really instilled the value of education in us,” Perri says.
If that path to optometry took familiar, familial steps, life beyond her University of Melbourne graduation in 2010 was a little more of a lottery.
“My boyfriend at the time, Jason Korman, who became my husband, put down my name and I won a green card,” she recalls. “So a few weeks after we got married, we packed up two suitcases and we just moved to New York.”
Perri couldn’t work as an optometrist so took a role as an assistant to a corneal specialist. And she dived even deeper into the world of food over the four years they spent in the US.
“I started cooking more, educating myself about food, doing
Image:
Jess
Perri.
Image: MasterChef Australia.
A young Jess Perri gets an early insight into the optometry business, at her mother’s practice.
“YOU CAN’T JUST LOOK AT DIABETIC RETINOPATHY AS AN ISOLATED CONDITION OF THE EYE. IT’S A CONDITION OF THE PERSON. SO THAT IS A BIG ELEMENT OF THE DISCUSSIONS I HAVE.”
cooking courses at the Institute of Culinary Education, and I created a food blog.”
It would become a passion that Perri would take to new heights when she became pregnant with daughter Maya and the family headed back to Australia.
If optometry was the road that Perri was always destined to head
down, food has always been another important destination on that journey and the fuel to sustain her. Perri regularly coaches others on how to make and shape pasta in her commercial kitchen at home – “When we built this house, I said to my husband, you can do everything else, do not touch the kitchen plan.”
That love of food and Italian legacy saw her compete on reality TV show Masterchef two years ago, and she now makes and markets her own pasta under the brand name Pretty Pasta.
There’s a website in the works, packaging is at the design stage, interviews to be conducted.
This and other experiences have taught her “that you can try new things at any age and nothing really limits you, other than your own ability to keep trying and keep going”.
It’s tempting to suggest that Perri, who regularly tells her husband “we’ll sleep when we’re dead” and who doesn’t have a great deal of downtime, might be spreading herself too thinly, like pasta rolled and pulled so tightly it might snap.
But she pushes on regardless because not only is the focus on food a passion and a business, it also became very personal when her father had a heart attack at the age of 53.
“It completely changed our lives as a family,” she says. “My father went from being an otherwise pretty fit and healthy guy to all of a sudden needing 20 different medications.
“So I went back and that’s when I studied nutrition and the purpose of that was really to help my dad.”
But she also saw the potential to help others – especially through diabetes management. When she returned to her studies in 2012, she undertook postgraduate studies in nutrition (diabetes management) at Deakin University.
Her passion – an intersection of nutrition and ocular health – has been taken into her work at Dr Optical, where she works with another optometrist and, in somewhat of a rarity in Australian optometry, an ophthalmologist on site, Dr Roland Bunting.
Patients frequently need help with macular degeneration, cataracts, and management of diabetic retinopathy, glaucoma and myopia.
“We’ve got all the bells and whistles.”
But just as important as the latest technology and techniques is the opportunity to talk with the patients.
Like mother, like daughter.
“My mum was invested in people and her patients beyond just, ‘I’m just going to give you glasses’. There was always a relationship there. And my mum was adored by her patients. I can’t think of any other word than that.
“So I took it upon myself to open up those conversations with patients about food and lifestyle.
“There are many studies which have shown that certain foods, certain vitamins, certain minerals are beneficial against, for example, macular degeneration.
“Diet and lifestyle are such huge components in diabetes management and diabetic retinopathy.”
It’s a whole-body issue.
“You can’t just look at diabetic retinopathy as an isolated condition of the eye. It’s a condition of the person. So that is a big element of the discussions I have.”
Perri talks with patients about stress relief as well. For her, that used to be about long-distance running, including marathons.
That has gone by the wayside of late, although she likes to sneak in a good “semi-long run” at the weekends.
Something’s got to give, right?
Especially when you’re feeding and building a family that will become a village of support and sustenance.
Because there’s only so many hours in a day, and sleep beckons.
Image: Dr Optical.
Food might be a passion but optometry is Jess Perri’s first love.
Pasta-making and shaping was learnt at a young age and Jess Perri now makes her own in a business venture called Pretty Pasta.
Image: Jess Perri.
Securing supply of goods and jobs
An Australian lens manufacturer says investing in locally made products is more than just securing a good supply chain. It’s also about securing the future of the country’s youth workforce.
Acountry full of warehouses but lacking the skilled young people making the products to fill them.
That’s Mr Adam Fletcher’s key concern and argument for promoting products branded with the “Australian-made” sticker – and the manufacturing that supports it. Fortunately, the CEO of Australia’s largest independent ophthalmic lens manufacturer has a blueprint that he hopes will enhance both the local optical and manufacturing industries.
“In a lot of industries, the products they make are becoming less and less manufactured here in Australia,” he says.
“Among our 53 staff we employ a lot of young people and we’re actually providing a future for them. So it is about the future and providing a craft, education, work skills, and having manufacturing here in Australia.”
CR Labs has long been a leader in the Australian optical manufacturing industry and today completes approximately 1,200 jobs a day. It is well-known for its innovative, high-quality lens production, original designs and customer service, and considers itself a pioneer in the Australian market, providing independents with the opportunity to shine with high quality of lenses suited to all frame types.
Among the major lens suppliers, it’s one of, if not the only, company that surfaces its lenses in Australia.
Fletcher’s company, launched in 1976 by his father, Mr Ray Geake, is planning for a self-sustaining future, with a succession plan that not only includes his own family – “I’ve got my son working in the business” – but also the development of an academy to teach young people the fundamentals of optics and even basic hand skills to work in manufacturing.
“We believe that the future of independent optometry lies in nurturing talent and empowering the next generation,” says Fletcher.
As part of that, CR Labs is developing educational initiatives to equip young minds with essential industry knowledge.
“Through hands-on training, workshops, and partnerships with educational institutions, we aim to foster a deeper understanding of
optics, lens technologies, and manufacturing processes, ensuring that the next wave of professionals is prepared to drive Australia’s optical industry forward. “Our investment in optometry professional services only reinforces our dedication to these educational initiatives for optometry and dispensing.”
Fletcher says this training and wider support for local manufacturing is vital in the face of well-documented supply chain issues, for the future workforce and the current retailers negotiating a tough, tricky economy.
A STEADY SUPPLY OF ISSUES
According to experts, those issues are likely to continue into 2025 and beyond.
Professor Vinh Thai, a supply chain expert from RMIT’s College of Business and Law, says 2024 has been another tough year for supply chains because of ongoing geopolitical risks, including Russia’s invasion of the Ukraine and the escalating war in the Middle East.
Also, “the high cost of fuel has made supply chains much more expensive and also fragile".
He expects that fragility to continue in 2025.
“Although supply chains in 2024 have been performing better than in 2023, there lies ahead a plethora of supply chain issues in 2025 as there has been, so far, no concrete sign that the current chaotic uncertainties will be eased soon.
“Hence, retailers need to constantly scan their supply chain environment and address issues as they arise early and proactively.”
For Fletcher, that mitigation of risk for retailers involves scanning for products made in Australia, and supporting local manufacturing.
That includes the eye care sector, in which CR Labs is the biggest manufacturer of surfaced – and glazed – lenses located in Australia.
His company services the independent practices exclusively, which are under pressure from a growing corporate share of the market.
Images: CR Labs.
As well as its work to manufacture products locally, CR Labs has set up its own testing facility.
“By keeping production local, we secure employment opportunities, strengthen the domestic optical industry, and continue to offer world-class products that benefit independent optometrists nationwide.”
Adam Fletcher CR Labs
“When I started working with dad, the market was 80% independent,” he says.
“We flash forward 35 years, and it’s much smaller now.”
Fletcher believes those independents benefit from a number of advantages in dealing with a local manufacturer.
“I think the greatest things that we offer are our quality, our service, and our speed,” he says.
“On average, our turnaround time is four days, so if you go into an optometrist on a Saturday, you can come back next Saturday and pick up your pair of glasses.”
That quicker turnaround means less time for a customer to have second thoughts. “You look at the market at the moment and people are probably a little bit shy on spending money, so that longer turnaround provides more time for buyer remorse.
“If the glasses are good quality and they are turned around quickly, the patient is then happy with the purchase and they have less time to think about it.”
The company has invested in its own testing facility as well, so lenses are no longer sent overseas for quality control.
That means CR Labs lenses are tested to Australian conditions and standards.
“Australia standards actually exceed the global standard in terms of what the expectation is, because Australia is one of the harshest environments in the world,” he says.
“You can’t just have it as a standard European standard, because our standards far exceed that, which means we can offer the best warranty for products.”
He also believes issues with global supply chains will likely push up the prices of products imported into Australia, including eyewear.
“The cost of goods, particularly freight coming into Australia, could rise significantly if tensions in the Middle East escalate, potentially impacting trade routes and global supply chains,” he says.
KEEPING IT IN THE FAMILY
But Fletcher acknowledges that his company is also vulnerable to the rising costs of overseas materials brought into Australia and used in making its lenses.
“Once upon a time, if you go back 20 years ago, we used to have local casting in Adelaide, but they no longer manufacture in Australia.”
But the company has adapted and mitigated the risk by warehousing product and softening the supply chain highs and lows.
There are other challenges for manufacturers in Australia, from rising operational costs and navigating supply chain disruptions to competing with lower-cost overseas production.
There is also the constant battle of regulation standards that must be met.
But Fletcher says CR Labs remains “committed to local manufacturing, ensuring high-quality, Australian-made products that meet the needs of independent optometrists.
“Our focus on innovation and advanced technologies, like the CR Tower and AustralisVR, reinforces our dedication to sustainable growth despite these pressures.”
What has helped the company handle the highs and lows for almost 50 years is supportive customers.
“We’re one of the oldest manufacturers in Australia, and the practices have remained extremely loyal through our journey.
“CR continues to have significant growth right across the country, particularly in New South Wales.”
In partnership with Safilo, those businesses and others get access to Carrera Authentic Lenses, for which CR Labs is the only authorised laboratory in the world.
“This exclusive partnership not only reinforces our global standing but also ensures the creation of more jobs here in Australia,” says Fletcher.
“By keeping production local, we secure employment opportunities, strengthen the domestic optical industry, and continue to offer world-class products that benefit independent optometrists nationwide.”
Those products provide a point-of-difference for many of those practices, helping them maintain a profile and market share in a competitive industry.
More importantly, it’s an investment in the future of not only the optometry industry and the workforce it will rely on, but also the goal of keeping Australia strong and self-reliant.
“When you look at the young people that are coming through, they’re our future,” says Fletcher.
“They’re the ones that we need to look after. And it’s not only from a manufacturing perspective, it’s also from a professional perspective as well, to be able to provide people with a choice, being able to provide people with some freedom.”
That’s important to Fletcher. His father brought him into the business as a full-time apprentice in Optical Surfacing and Fitting in 1989. He only intended to stay a year or two before moving on, but 35 years later he’s still there.
“It was the longest apprenticeship known to man.”
Now his son, Cooper, is involved. He’s training as an AR (Anti-Reflective) specialist.
“Here we go. Similar thing to me, and I thought ‘I know where this is going’.” Unlike the father, the son might only stay a year or two before moving on. Or maybe, like his dad, he’ll still be there after 35 years.
But that’s only going to happen if people continue to buy local, continue to support local manufacturing, continue to offer his son and many others the choice.
Image: CR Labs
CR Labs has been manufacturing in Australia since 1976 and is well-known for its innovative, high-quality lens production.
#Targets all layers of the tear film, suitable for evaporative, aqueous deficient & mixed dry eye
G&M plays a strong hand
After arguably the biggest 12 months in its eight-year history, George & Matilda Eyecare wants to carry that momentum into 2025. Insight hears from three independents who joined the network in the second half of 2024.
Others may be starting to eye the end of the year and a decent break, but there’s little rest at George & Matilda (G&M) Eyecare as it plans further expansion in the optometry industry.
The network has recently announced its latest acquisition – Lighthouse Optometrists in Ramsgate, NSW – bringing the number of partnerships in 2024 to 34.
The NSW move is hot on the heels of forays into Western Australia and Queensland, plus the acquisition of National Optical Care (NOC)’s 26-practice business in September, the largest in its eight year-history.
Optometrist Ms Gina Basily has spent 13 years in the industry and started Lighthouse Optometrists in 2018.
"I’ve always been passionate about both medicine and retail, and optometry brings them together in a way that allows me to deliver a holistic approach to patient care," she says.
our presence in WA,” he says. “This gives us the opportunity to provide better quality eyecare services to more Australian communities. We are excited for the strong pipeline of practices we have lined up to join us in 2025.”
Judging by reactions of the most recent acquisitions, there may be no shortage of options for Beer and his team.
Colleague Ms Kathryn Jorgensen, an optometrist at the West Specs Kalgoorlie practice, says she remains motivated by the work and the care provided to patients.
“I have been an optometrist for 37 years, and I chose this industry because I always wanted to work in a health-related field.
“I am proud of the quality eyecare and products we offer, and we strive to go above and beyond to help our patients.”
Her practice’s reputation is built on a foundation of exceptional service, personalised treatment plans and a commitment to community health. It is renowned for innovative programs, such as the ‘Come and See’ initiative, which has helped to provide life-changing vision care to thousands of people overseas.
“We’re thrilled to join the George & Matilda Eyecare family,” says Basily. “This partnership aligns perfectly with our vision of delivering the highest quality eyecare. By leveraging the resources and expertise of George & Matilda Eyecare, we can continue to grow and better serve our patients.”
Other practice owners have reached similar conclusions over the past couple of months.
The partnership with Basily’s practice follows G&M’s acquisition of three practices in Western Australia – Nedlands, Greenwood, and Kalgoorlie. That came just two weeks after it took on two Queensland practices, at Main Beach and Sanctuary Cove.
Mr Andrew Godfrey was the owner of the three WA practices.
Of the sale, he says: “I like to think of our working life as a train journey. For us, this is our stop.
"We had worked with George & Matilda before and were impressed with the systems and processes they have in place, knowing they can take care of our staff, patients, and practices."
For optometrists considering their future, Godfrey offers insightful advice: “It’s easy to keep doing what you’re doing, but it’s important to look at the landscape and decide whether your future is best served through change.
“As Kenny Rogers said, 'You’ve got to know when to hold ’em, know when to fold ’em.'”
The G&M network now has more than 120 locations that service 140 communities (when counting outreach work), and founder, CEO and managing director Mr Chris Beer acknowledges it is facing a massive integration task amid its most rapid growth period.
But he has hinted that it will look to make other acquisitions as he grows the network.
“With an ambition to grow the G&M community by up to 20 practices a year I am very happy to have welcomed 34 new businesses in 2024, including doubling
That would continue under the new G&M banner.
Ms Natalie Guillon, an optometrist at the Opticentre Nedlands practice, also emphasised the importance of patient-focused care, adding: “I love the variety that optometry offers, and I am passionate about providing thorough eye examinations.
“Our practice is known for our expertise in contact lenses.”
That, too, would continue in the new partnership. It’s a big part of G&M’s value proposition: partnering with independents woven into the fabric of their communities, not interfering with their clinical sovereignty, while fine-tuning the retail and dispensing side of the practice.
“By joining the George & Matilda Eyecare, these practices gain access to valuable resources, including marketing and operational support, business management tools, and professional development opportunities,” the company says.
Those tools also include platforms that power vital business functions such as product ordering, payroll, patient recalls and buying power. There’s also supply chain technology that allows visibility of every brand, every stock-keeping unit to different customer segments, age groups and demographic.
Practices would have access to those resources while maintaining their
“We are always continuing to learn from the practices that join our team as there are so many in the industry with strengths and passions that only make our community stronger.”
Chris Beer
George & Matilda Eyecare
Image: George & Matilda Eyecare.
ABOVE: Joanna Rogers (from left), Daniel Meoli, Maria Dhimitri, Merna Michael, and Gina Basily, from Lighthouse Optometrists in Ramsgate, NSW, have joined the G&M network.
Image: G&M Eyecare
“As the network continues to grow, patients can expect the same high standards of care, professionalism, and service that have become synonymous with George & Matilda Eyecare,” the company says.
‘NO COOKIE-CUTTER APPROACH’
It was a similar story when G&M acquired the two practices in Queensland.
The well-established practices at Main Beach and Sanctuary Cove were owned and operated by optometrist Mr Michael Jackson, who has 25 years’ experience in the industry.
He says joining G&M was a strategic decision driven by the changing optometry landscape.
“There’s a shift in the industry where younger optometrists are seeking more flexibility, particularly with part-time work and managing larger financial commitments,” he says.
“I realised that selling to a corporate model was inevitable to achieve my
personal goals, and George & Matilda was the perfect fit.
“They allow us to maintain our independent spirit while managing the increasing regulatory and financial pressures on practices. Having a larger entity to support us makes it more sustainable in the long term.”
His experience working with G&M has been positive.
Over the years, he has owned three practices, starting with Ballina before opening his practice in Sanctuary Cove 10 years ago and Main Beach four years later.
For G&M, one of the challenges has been creating platforms that cater for the many varied needs of practices within the network. So when independents like Lighthouse Optometrists, Main Beach, Sanctuary Cove and the three WA practices join, they’re able to plug into G&M’s sophistacted platforms while maintaing many of the quirks that help them differentiate.
Beer says there is no “cookie-cutter approach” to the model, despite what some in the industry might think. The fact every practice is unique is a double-edged sword: it makes G&M a highly attractive option for independents looking to sell, but is complex to execute.
That is, in part, because not one practice has the same supply chain or frames range.
Engaging with the different practices, finding out what worked and didn’t work, and what sold and didn’t sell, actually helped G&M to finetune its own business model, he says.
“Our team continues to focus on ensuring the practices that join the G&M team are integrated smoothly with no impact to their patient experience.
“We are always continuing to learn from the new practices that join our team as there are so many independent optometrists in the industry with strengths and passions that only make our community stronger as they share their experiences throughout G&M.”
It appears there are still many cards left to play.
PBS Information: Xalatan (latanoprost 0.005% eye drops, 2.5 mL) is listed on the PBS as antiglaucoma preparations and miotics.
Before prescribing please review Product Information available via www.aspenpharma.com.au/products or call 1300 659 646.
Minimum Product Information: XALATAN® (Latanoprost 50 µg/mL) Eye Drops. Indication: Reduction of intraocular pressure (IOP) in patients with open-angle glaucoma or ocular hypertension. Contraindications: Hypersensitivity to ingredients. Precautions: Change in eye colour due to increased iris pigmentation; heterochromia; eyelid skin darkening; reversible eyelash and vellus hair changes; macular oedema often associated with aphakia / pseudoaphakia; other types of glaucoma; contact lenses; severe or brittle asthma; herpetic keratitis; driving or using machines – transient blurry vision; elderly: no data; children: do not use, no data; lactation- metabolites present in breast milk, risk / benefit. Pregnancy: Category (B3) Interactions: other prostaglandins, thiomersal. See PI for details. Adverse Effects: Eye Disorders: blurred vision, burning, conjunctivitis, excessive tearing, eye pain, foreign body sensation, hyperaemia, iris hyperpigmentation, itching, punctate epithelial erosions, grittiness, stinging, eyelash and vellus hair changes, punctate keratitis, blepharitis, eyelid oedema, localised skin reaction on eyelids; Systemic: bronchitis, upper respiratory tract infection, eczema, rash, urinary tract disorder, abnormal liver function, myalgia, arthralgia, dizziness, headache, rash, chest pain, asthma, dyspnoea . See PI for details and other AEs. Dosage and Administration: One eye drop in the affected eye(s) once daily. Other eye drops should be administered at least 5 minutes apart.
References: 1. Clinical Practice Guide for the Diagnosis and Management of Open Angle Glaucoma. Optometry Australia 2020 2. Australian Commission on Safety and Quality in Healthcare Active Ingredient Prescribing Guide - list of medicines for brand consideration December 2022
If clinically necessary for the treatment of your patient, prescribe by brand and disallow brand substitution2
Jan Coetzee (left) and Michael Jackson, from Sanctuary Cove Optical, joined the G&M network in October.
Image: Sanctuary Cove Optical.
Enquiries: info@crlabs.au
Dry eye: assessments, management strategies laid out in two case reports
Optometrist AIDAN QUINLAN explains his own protocols for subclassifying dry eye, provides his own insights for accurate diagnosis and management, and highlights the benefits of preservative-free lubricating drops tailored to each patient’s symptoms.
ABOUT THE AUTHOR:
In the complicated and conflicting world of dry eye disease (DED), the Tear Film and Ocular Surface Society (TFOS) Dry Eye Workshop (DEWS) reports serve as a pillar for clinical decision making. The group’s updated, internationally-recognised definition of DED was established in 2017: “Dry eye is a multifactorial disease of the ocular surface characterised by a loss of homeostasis of the tear film, and accompanied by ocular symptoms, in which tear film instability and hyperosmolarity, ocular surface inflammation and damage, and neurosensory abnormalities play etiological roles.”1
Two important components of this definition stand out.
LEARNING OBJECTIVES:
At the completion of this article, the reader should improve their management of dry eye disease, including:
• Recognise the importance of personalised treatment strategies for DED patients, considering the complexity of disease subtypes and individual variations in symptoms and responses to treatment
• Evaluate the advantages of preservative-free eye drops in reducing adverse ocular surface effects and improving outcomes in patients with DED
• Understand how distinct subclassifications of DED necessitate different treatment approaches and the tailored use of aqueous-based versus lipid-based lubricating drops
First, the multifactorial aspect of DED demonstrates a complex disease with varying aetiologies. It also alludes to the multitude of treatment modalities available. And second: homeostasis; which is defined as “a self-regulating process by which biological systems maintain stability while adjusting to changing external conditions”.2 With dry eye, the loss of homeostasis implies that the body has lost the ability to maintain a state of equilibrium. This results in tear hyperosmolarity, instability of the tear film and resulting associated sequelae (increased osmolarity, inflammation, neuropathy and reduced function).
DRY EYE CATEGORIES
The consensus in dry eye research and clinical practice has been established around two key diagnostic labels: 1) Evaporative DED, which is excessive evaporation of the tear film due to meibomian gland dysfunction (MGD); and 2) aqueous deficient dry eye (ADDE), which is reduced tear
lacrimal gland production.
It’s generally accepted that rather than representing two separate categories, most patients suffer from a combination of both abnormal meibomian gland physiology which results in evaporative DED and tear underproduction which results in aqueous deficient DED.3
Estimates of overlap between the two groups span from 30% to 70%.3 One published research article found evaporative dry eye was three times more likely to be sub-classified compared to aqueous deficient dry eye. (Interestingly, over 30% of patients were found to have both types of DED).4
CASE REPORTS
Recognition of complexity is essential for management of DED. However, regardless of the underlying causes, appropriate daily lubricant eye drops play a critical role in managing dry eye symptoms and ocular health. The patients in the following case reports had different subclassifica-
Images:
Aidan Quinlan.
CLINICAL CPD HOURS
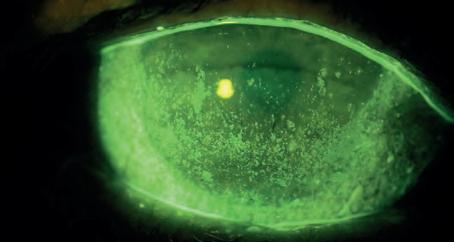
Figure 2: Diffuse inferior conjunctival and corneal SPK was seen with installation of sodium fluorescein diagnostic eye.
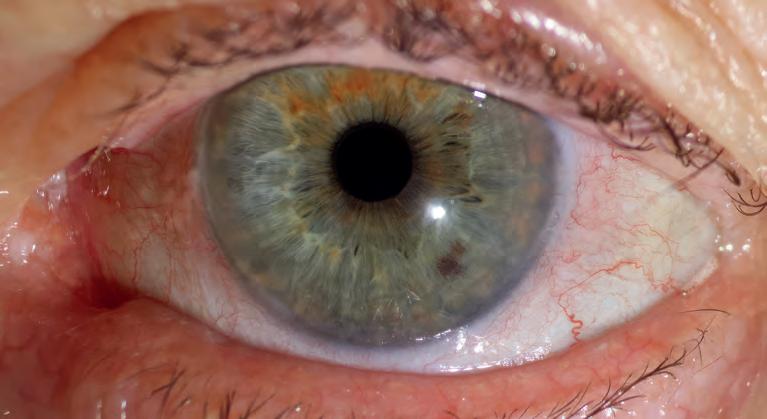
Figure 1: An overview photo of Mrs L shows diffuse conjunctival redness, lid margin telangiectasia and low TMH.
tions of DED, each necessitating a distinct treatment approach, each reliant on lubrication drops, but of different classes.
While the first patient benefits from using a watery, aqueous-based drop, the second requires an oil-based, lipid drop. Each type of drop is crucial in improving hydration, nourishing the ocular surface and mimicking the natural meibum to improve tear stability. As these case reports show, NovaTears, Hylo Fresh and Hylo Forte were essential in relieving symptoms and improving the quality of life for these patients.
CASE REPORT 1
Mrs L* is a retiree with a love of painting and a caregiver of her husband and disabled daughter. She is bothered by constantly dry, sore and irritable eyes which are worse while painting or reading. Mrs L has a prior diagnosis of Sjögren’s syndrome. Her McMonnies questionnaire gave a score of 24 (suggestive of dry eye), and her OSDI survey score was 63/100 (suggesting severe dry eye). Unaided vision was reasonable in each eye at 6/7.5+.
Our initial overview photos (Figures 1 and 2) show diffuse conjunctival redness, lid margin telangiectasia, and a low Tear Meniscus Height (TMH). Measurement of TMH with Medmont Meridia showed R 0.13 mm and L 0.13 mm below the value of <0.2 mm that could be indicative of dysfunction of the lacrimal gland.5
An additional phenol red thread test (PRTT) agreed with the above finding. TearLab osmolarity testing results were R 330 mosmol/L and L 340 mosmol/L – well above the threshold for abnormal at >308 mOsm/L.6 It is important to remember that the magnitude of tear osmolarity is significantly correlated with dry eye signs as measured by corneal staining, conjunctival staining, TBUT and Schirmer’s test.7 This relationship is well documented in this case.
Non-Invasive Tear-Break Up Time (NIBUT) showed an almost constant disruption of placido rings with NIBUT for three to four seconds on both eyes. Corneae showed significant superficial punctate
keratitis (SPK) and punctate epithelial erosions (PEE) staining with NaFl. It was largely distributed in the inferior half of cornea showing the impact of incomplete blinking habits and indicated possible nocturnal exposure during sleep.
With infrared meibography, Mrs L’s meibomian glands showed mild shortening and disorganisation. Meibum was flowing with mild cloudiness and thickness of deeper oils expressed with a two-pronged meibomian gland expressor. Several issues contributed to the patient’s ocular surface disease:
• Moderate aqueous deficient DED because of decreased lacrimal gland function from underlying Sjögren’s syndrome;
10 minutes followed by gentle digital massage to further improve meibum flow and gland function. VitA-POS ointment applied into the lower fornix before sleep was prescribed to protect the eye from probable nocturnal exposure. In addition, blink exercises were used to improve blink technique and ensure complete blinks.
• Finally, I prescribed a non-preserved lubricating drop in the form of Hylo-Fresh (containing sodium hyaluronate 1 mg/mL).
Hylo-Fresh, containing the active ingredient sodium hyaluronate 1 mg/mL, is a great option for patients with aqueous deficient dry eye. Sodium hyaluronate is used in artificial tear supplements to increase viscosity and provide enhanced lubrication effects to the ocular surface. Several research studies have demonstrated its ability to bind to ocular surface cells and promote wound healing.3
HyloFresh and its alternative HyloForte (with sodium hyaluronate 2 mg/mL, leading to increased viscosity) are both preservative- and phosphate-free. I will touch on the importance of this on the next page.
CASE REPORT 2
“A KEY ASPECT TO PRESCRIBING LUBRICATING DROPS IN THESE CASES – AND IN PART ALL DED CASES – IS CONSIDERING THE USE OF PRESERVATIVES.”
• Mild meibomian gland dysfunction (severe due to the poor meibum quality and degree of lid margin inflammation) with secondary evaporative DED;
It’s vital to hone in on each component of the patient’s ocular surface disease for best symptomatic and clinical improvement.
• In order to manage her aqueous deficient dry eye and to improve lubrication and hydration, I inserted short-duration punctal plugs to retain vital aqueous in the eye.
• We tackled her meibomian gland dysfunction with the use of an anti-inflammatory dose of oral azithromycin tablets (500 mg on the first day, then 250 mg once a day for four more days). Research suggests azithromycin had a better clinical response when treating meibomian gland dysfunction compared to oral doxycycline, with fewer side-effects and a shorter course.8 Mrs L was also encouraged to take omega-3 supplements as they help improve meibomian gland function and decrease ocular inflammation.
• A sustained heat was applied across the glands for
Mr M* is a keen surfer that has trouble with sore, stinging eyes throughout the day that was exasperated from salt water. He also has a scratchy lower lid with misdirected lashes and history of left inferior lid melanoma removal. Mr M was currently using hydrating lubricating tears which he picked up at the local pharmacy and has used hot compressions for several months. The results from his OSDI questionnaire showed gritty and painful eyes all the time over the last week.
TearLab chemistry testing showed osmolarities of right 320 mosmol/L and L 334 mosmol/L. An abnormal reading in terms of magnitude and >8 mOsm/L difference between the two eyes.6
My anterior health assessment and ocular surface workup showed several causes of Mr M symptoms. Mr M’s left lower lid showed moderate trichasis with three to four lashes touching the inferior bulbar conjunctiva and cornea. He has moderate inferior SPK associated with the lashes. Assessment of the meibomian glands showed minimal meibum expressibility even with firm pressure with forceps indication hyposecretory meibomian gland dysfunction.
A main cause of this condition was revealed with infrared meibography with the Medmont Merida. It showed frank atrophy of 60-70% of inferior meibomian glands due to chronic dysfunction and prior surgery of the inferior left lid.
Several components are involved in Mr M’s ocular surface disease and help us understand some of his prior troubles with different management:
Figure 3: An overview photo of Mr M shows mild conjunctival redness, lid margin telangiectasia with notching and misdirected inferior lashes.
• Moderate hyposecretory meibomian gland dysfunction with 50-60% atrophy of glands L>R. In turn, leading to moderate evaporative DED.
• Inferior trichiasis L>R causing irritation, scratchiness and SPK on inferior cornea.
• A small indication of potential nocturnal ocular surface exposure causing morning irritation and soreness.
I find in these cases the best option is to begin with patient education and improving patient understanding of the ocular disease conditions. It can be helpful to use grading scales to further improve patient awareness of limitations to different management.
In this case, Mr M was educated regarding his meibomian gland atrophy and inferior lid trichiasis. He was able to understand why the left eye was more symptomatic than the right eye and many months of hot compressions were rather unhelpful for his overall condition. Although, due to lower rates of atrophy of the right and superior glands, an anti-inflammatory dose of oral azithromycin tablets (500 mg on the first day, then 250 mg once a day for four more days) was still used to improve remaining gland function.
The troublesome inferior left lashes were removed with fine tweezers and Mr M was instructed to return once they regrow for removal. He was educated on the option of electrolysis, which is a safe and effective process that uses a high-frequency electric current to destroy the hair follicle. VitApos ointment applied into the lower fornix before sleep will improve symptoms of nocturnal exposure.
I prescribed NovaTears, an oil-containing lubricating eye drop with active ingredient perfluorohexyloctane 100% v/v to be used four times a day. The efficacy and safety of perfluorohexyloctane ophthalmic solution in patients with dry eye due to meibomian gland dysfunction was assessed in the GOBI study.9 NovaTears demonstrated statistically significant and clinically meaningful improvements in the signs and symptoms of DED. Several other studies have also shown improvements in tear stability, corneal staining, and OSDI scores with perfluorohexyloctane containing lubrication drops.10
A key aspect to prescribing lubricating drops in these cases – and in part all DED cases – is considering the use of preservatives. Several preservatives are used in ophthalmic preparations for DED, the most common and widely studied in benzalkonium chloride (BAK). BAK has been shown to cause disruption of tear stability, cellular damage of both the corneal and conjunctival epithelium, and induce inflammatory changes on the ocular surface.10
Other studies of symptomatic ocular surface disease where patients were switched from preserved to preservative-free treatments showed astounding results. Incidence of irritation, burning, dry eye and foreign body sensation, tearing and itching reduced by two-thirds, with the incidence of conjunctival hyperaemia, staining, and blepharitis
dropping by half.10 In some cases, patients can be apprehensive to switch to preservative-free topical lubricates due to preservative-free preparations being supplied in single-dose units leading to handling issues, increased cost and increased packing waste.
Products such as HyloFresh and HyloForte come in specialised multi-dose bottles which make preservative-free sterility possible. It is the unique COMOD multi-dose application system which adjusts airflow and prevents the solution from coming into contact at any time with the surrounding air eliminating the potential for contamination. It means that patients such as Mrs M can confidently use these drops frequently to nourish the ocular surface and improve symptoms without adverse effects of preservatives.
Mr M, on the other hand, is using a lubricating drop with a semifluorinated alkane medium which bacteria cannot live in. It means that preservative-free NovaTears is ideal for regular use. NovaTears is suitable for patients like Mr M where significant improvement in the underlying disease mechanism is not expected due to the dense atrophy of meibomian glands.
Patient education about the targeted use of drops such as NovaTears which stabilise their tear-film is helpful. In this case, I instructed Mr M to insert drops before going out for a surf, on cold mornings or prior to a walk in windy weather. It is important that patients know about the smaller volume drop of NovaTears and the ‘warm’ or ‘soft’ feel of the low-surface tension drop when it hits the eye – vastly different to the drops they may have previously been using.
An often complex and varied condition, DED can be tackled using a rational and well-reasoned series of assessments. Hopefully this article aids in making the diagnosis of your patient’s condition(s) more straight-forward, improves your management
discussions and leads to appropriate treatment and management strategies. In a quest for patient satisfaction and positive ocular health outcomes.
*Patient names changed for anonymity.
NOTE: The author received a monetary honorarium from AFT Pharmaceuticals for providing this article.
REFERENCES
1. J ennifer P Craig 1, Kelly K Nichols 2, Esen K Akpek et al. TFOS DEWS II Definition and Classification Report. Ocul Surf. 2017; 15 (3): 276-283. doi: 10.1016/j.jtos.2017.05.008.
2. B illman GE. Homeostasis: The Underappreciated and Far Too Often Ignored Central Organizing Principle of Physiology. Front Physiol. 2020 Mar 10; 11: 200. doi: 10.3389/fphys.2020.00200.
3. J ones L, Downie LE, Korb D, Benitez-Del-Castillo JM, Dana R, Deng SX, Dong PN, Geerling G, Hida RY, Liu Y, Seo KY, Tauber J, Wakamatsu TH, Xu J, Wolffsohn JS, Craig JP. TFOS DEWS II Management and Therapy Report. Ocul Surf. 2017; 15 (3): 575-628. doi: 10.1016/j.jtos.2017.05.006.
5. A rita, R., Itoh, K., Maeda, S., et al., Efficacy of diagnostic criteria for the differential diagnosis between obstructive meibomian gland dysfunction and aqueous deficiency dry eye. Jpn J Ophthalmol. 2010; 54 (5), 387–391 DOI: 10.1007/s10384-010-0858-1.
6. Wolffsohn JS, Arita R, Chalmers R, et al. TFOS DEWS II diagnostic methodology report. Ocul Surf. 2017; 15: 539–574.
7. G reiner JV, Ying GS, Pistilli M, Maguire MG, Asbell PA; Dry Eye Assessment and Management (DREAM) Study Research Group. Association of Tear Osmolarity with Signs and Symptoms of Dry Eye Disease in the Dry Eye Assessment and Management (DREAM) Study. Invest Ophthalmol Vis Sci. 2023; 64 (1) :5
8. K ashkouli, M.B., Fazel, A.J., Kiavash, V., et al, Oral azithromycin versus doxycycline in meibomian gland dysfunction: a randomised double-masked open-label clinical trial. Br J Ophthalmol. 2015; 99 (2): 199–204. DOI: doi.org/10.1136/bjophthalmol-2014-305410.
9. Tauber J, Berdy GJ, Wirta DL, et al, GOBI Study Group. NOV03 for Dry Eye Disease Associated with Meibomian Gland Dysfunction: Results of the Randomized Phase 3 GOBI Study. Ophthalmology. 2023; 130 (5): 516-524.
10. Walsh K, Jones L. The use of preservatives in dry eye drops. Clin Ophthalmol. 2019; 13: 1409-1425.
NOTE: Insight readers can scan the QR code or visit insightnews.com.au/cpd/ to access a link to this article to include in their own CPD log book.
Figure 4: Transillumination of Mr M’s left inferior lid shows a significant frank gland atrophy (seen as the absence of dark acini structures) and shortening of remaining glands.
ABOUT THE AUTHORS:
Playing it safe: integrating UV safety with myopia control
BSc (Med), MBBS, FRANZCO, GAICD, Eye & Laser Surgeons, Bondi Junction & Miranda Paediatric, Strabismus & Cataract surgery
With growing attention on outdoor time as a preventive measure for myopia control in children, a nuanced challenge emerges: balancing exposure to natural light with protection from harmful ultraviolet radiation. The authors offer guidance for eyecare professionals navigating this quandary.
WBSc (Hons) MBBS (Hons) FRANZCO PhD
Paediatric and general ophthalmic surgeon Clinical senior lecturer, Macquarie Medical School
Adjunct Associate Professor, University of Canberra Founding member of Myopia Australia
MBBS BscMed FRANZCO GradCert AGSM Director Eye Associates, Macquarie St Sydney Ophthalmologist and cataract surgeon Clinical Senior Lecturer University of Sydney
ith the rising concern of the myopic epidemic, there is an increased global awareness and push to encourage children to spend 14 to 17 hours a week in high-lux, UV-free outdoor light. This has been shown to offer a protective effect against axial length growth, and it’s a message that has quickly become a staple of our discussions with patients.
clinically-evident pingueculae or pterygium.1 It has been shown that pterygium is an indicator of UV exposure; patients with pterygium should, in fact, be screened for cutaneous melanoma as they have a 24% increased risk.5
Children have the least-naturally developed protection against UVR; 80% of UV eye exposure occurs before a child turns 18 years old.1 As eyecare professionals, we need to educate our patients about the importance of protecting their eyes from the complications of axial myopia as well as UV-related eye diseases. To do so, we need to understand how UVR reaches the eye and ensure that the sunglasses we are advocating our patients to wear provide maximum protection from UV radiation, while allowing in high lux light to protect from myopia.
UV-RELATED EYE DISEASES
In this article, however, we’ll discuss the flipside of this simple message. The sight-threatening complications of ultraviolet radiation (UVR) on the eye and adnexal structures, including: periorbital skin cancers, pterygia, pingueculae, ocular surface neoplasia, cataracts and macular degeneration. While it has been established that axial length growth occurs predominately in childhood, UV fluorescence photography has helped the scientific community to recognise that significant UV eye damage also occurs in these formative years.1 And just as frequently-sunburned skin can have serious consequences later in life, UVR-related eye diseases can result later in life for those who “sunburn” their eyes in childhood.
BSc (Med) Hons I, MBBS, MSc (Research), Eye & Laser Surgeons, Bondi Junction & Miranda Corneal, cataract & refractive surgeon
LEARNING OBJECTIVES:
At the completion of this article, the reader should be able to improve their myopia management, including:
• Assess the importance of sunglasses optimally designed for UVR protection
• Understand UVR’s correlation with both myopia prevention and increased risk of eye disease
• Advocate a balanced approach to UV protection and myopia prevention in eye care practices
UV fluorescence photography (UVFP), which can objectively quantify the degree of UV damage in childhood,1-3 has been used to demonstrate an inverse relationship between childhood UV exposure and myopia.4
UVFP analysis has shown that 30% of children aged 9-11 have UV damage to their eyes. By 12-15 years of age, 81% of children had UV damage detected, and most alarmingly, 29% had
Australia has some of the highest rates of UV-associated diseases in the world, in part due to our outdoor lifestyles and our climate. As our understanding of UV-related eye diseases has evolved over the last 50 years, we have learned how UV light damages the eye as well as the periorbital skin. Periorbital skin cancers account for 10%6 of all skin cancers of which more than half occur on the lower lid.7
Pingueculae and pterygia have an earlier onset than other UV-related eye diseases, with a peak prevalence between 20-40 years of age. To determine a person’s degree of UVR exposure
Around 80% of UV eye exposure occurs before a child turns 18, highlighting the importance of maximum protection sunglasses.
Image: Beamers.
Indonesia (11.0°)
simply considering where they live is inaccurate, as UVR levels depending on the latitude, altitude, sun elevation, cloud cover and ground reflection7 and can be skewed based on their occupation, participation in outdoor hobbies, activities and habitual use of UV protection, such as sunglasses and hats.
For example: pinguecula, the precursor to pterygia, varies from 11% in Southern India8 to 56% in Greenland.11 The wide variation of pterygium and pingueculae prevalence cannot be accounted for by the variations in latitude or altitude alone, just as the prevalence of skin cancer cannot be entirely explained by latitude or altitude.91
The prevalence of myopia has been tabulated against the prevalence of pterygium and pinguecula.
In several populations with a low prevalence of myopia, a high prevalence of pterygium was noted (Table 1). Similarly, this inverse relationship was evident when tabulating the prevalence of myopia against pinguecula (Table 2).
For example, in Shanghai, a high prevalence of pinguecula and low rates of myopia were documented. The very high myopia rate in South Korea at 70.6%10 inversely correlates with the 3.8% rate of pterygia.11 In Greenland, myopia prevalence was 14.1%,12 higher than expected compared to the pterygium prevalence of 8.6%.13 However, the high rate of myopia could be explained by the change in education policy, which made it compulsory for all Inuit children to start formal schooling. This
policy would increase the rates of myopia prior to causing a reduction in the prevalence of pterygium, which has a later onset. Data from Zhang et al.,14 summarised in Table 3, shows the correlation of axial lengths against pterygium.
THE DANGERS OF UVR
UVR penetrates the eye and is a risk factor for the development of anterior cortical and posterior subcapsular cataract.15 Studies suggest UVR is a risk factor for macular degeneration.16,17 Despite the UV protection afforded to the macula by UV absorption of an adult natural lens (REF), adults who worked outdoors have higher incidence of AMD and soft drusen.18 Furthermore, the amount of leisure time spent outdoors in summer was significantly associated with wet macular degeneration.25 Less well known is that an immature child’s lens only absorbs 90-95% of UVR, thus allowing significant amount of UVR to reach the macula. We suggest this as the pathogenesis for the inversely reducing rate of any age-related macular degeneration for each dioptre of increasing spherical equivalent of myopia noted in a Korean study.19
DISEASE PREVENTION
Studies confirm Australia’s high incidence of skin cancers from UVR exposure, particularly during childhood and adolescence,20,21 which has spurred numerous skin cancer prevention programs, promoting the use of sunblock, rashies and hats to protect the skin.22,23 But the eye and periorbital skin is still left unprotected. By age 70, two-thirds of Aussies have had treatment for at least one non-melanoma skin cancer.24 About 10% of all skin cancers occur in the periocular area. Furthermore, UVR eye diseases impact millions of Australians. Despite the large number of Aussies affected, the message about the importance of protecting the eye and periorbital skin with protective sunglasses is still not well known or understood, even though the need for UV skin protection is well understood.
Is prevention of eye diseases less important than the prevention of skin diseases?
Parents avoid applying sunblock to the periocular skin on their writhing children for fear of getting sunblock in their eyes, and they don’t insist on protective sunglasses, leaving both the periocular and ocular areas unprotected. The comment ‘my child won’t wear sunglasses or she doesn’t like them’ justifies why the eyes are unprotected. However, most children also dislike sunblock –which is essentially a thick paste smeared over their body, but their parents/teachers/adults insist that it is worn to reduce skin diseases. Furthermore, the different levels of UV skin protection offered by the various SPFs of sunblocks is understood. However, the UVR protection is less well classified or understood for the eye. Even in adults, the
Table 1. Correlation of pterygium prevalence with myopia prevalence.33
Table 2. Correlation between the prevalence of pinguecula and myopia.33
periorbital skin is most frequently left uncovered with sunblock in 14% of cases.25
When should we start protecting children?
As early as possible. It is known that exposure to UVR is cumulative and even short duration exposure can lead to long term eye health problems, many of which begin symptom free. Children receive approximately three times the annual adult dose of UVR, as they spend more time outside.
Eyecare professionals need to encourage our patients to understand the need to protect the eye from harmful UV rays. The message is clear: when a child is outside during daylight hours, their eyes should be protected from exposure to UVR. Eighty per cent of UV exposure occurs before a child turns 18 years old.26 The signs of UV damage to the anterior segment of the eye can be detected as early as nine years of age.1
IMPACT OF POORLY-DESIGNED SUNGLASSES
The tint of sunglass lenses reduce glare for the wearer and relax the squint reflex. This causes the palpebral aperture to widen, the brow to relax and the pupils to dilate.7 This widening paradoxically allows more UVR onto the periorbital skin, ocular surface and into the eye. Furthermore, as the sunglass lens is a smooth surface, the reflected UVR reaching the back surface of the lens from around the poor-fitting frame is reflected off the lens into the dilated pupil of the eye.7,27 UVR damages the skin due to the effects of direct rays of light. The eye, however, is damaged from direct, overhead and reflected rays of UVR. So it’s important to consider frame design in addition to lens quality when advocating the use of sunglasses. Unfortunately, as noted in Sliney et al,7 some sunglasses can actually increase UVR exposure to the eye.
SUNGLASSES WITH BEST PROTECTION
In a child’s eye, which normally has a larger pupil diameter than an adult eye, the UVR not only damages the anterior segment and periocular skin, but also can penetrate through the pupil and immature lens and onto the retina, and particular the macula.28 In addition to this, UVR is reflected from the ground, and surfaces around the wearer, and reflected off the back surface of the lenses and into the child’s anterior segment and through the pupil.29 The proportion of the direct, overhead and reflected light varies due to altitude, time of day, season and surfaces surrounding the child.
All sunglasses are not the same, and price is not an indication of the level of eye protection offered by a pair of sunglasses. Sunglasses designed to offer maximum protection should block all three pathways: direct, overhead and reflected UVR from reaching the eye and periodical skin. They should block reflected side light entering the eye from below and around the temporal and nasal sides of the lenses, with antireflective coating on the back/inner
Table 3. Axial length vs prevalence of pterygium.33
Study 1: Zhang, L.M., et al. Axial Length < 23mmAxial
A: Direct UV light – maximum entry in eye in the 2 hrs after sunrise and 2 hrs before sunset.
UV rays enter the eye from sunrise to sunset by combination of direct, reflected and overhead light.
B: Overhead UV light – maximum entry into eye between 12-2pm.
D: Blocking side light reduces UV entering eye by 18-25%28
C: Reflected light – enters the eye bouncing off the surfaces around us. Max time between 9am-12pm, 2-5pm.
Sunglasses should block these to offer maximum protection.
Figure 1. eye by a combination of overhead (B) and reflected light (C). Furthermore, the UVR that comes in around the arm of the sunglasses (D) bounces off the back surface of the lens into the dilated pupil as the dark lenses have disabled the squint reflex.33
side only (Figure 1).30 This prevents UVR reflected from the inner surface of the lens entering the eye. The further a lens sits in front of the eye the greater the irradiation to the eye and periorbital skin.31,32
Lens polarisation reduces reflected UVR reaching the eye through the lens. To maximally protect the eye and periorbital skin from UVR, polarisation should occur in the presence of wrap-around frame design.11 In addition to wraparound frame design, polarisation and anti-reflective properties, the lens material should block direct UV light and have absorption of up to 400 nanometres for maximum protection. Children’s sunglasses should be protective, comfortable to wear and meet the international safety standards.
Protection should be worn whenever the child is outside, from sunrise to sunset, 365 days of the year. Children need to be protected from an early age, as UV penetration into the eye is maximal in the first 10 years of life, when the eye has the least developed natural defences. This habit of eye protection needs to be encouraged throughout life. Wearing protective sunglasses should be part of the sun-protection campaign worldwide, as long-term eye and skin health are both essential, and in particular in Australia with our high rates of UVR diseases.
This push for UV protection is even more important as children are being encouraged to spend more time outside to reduce myopia progression. Myopia prevention and UV protection can occur simultaneously.
It is also important as eyecare professionals that in the future our patients don’t feel that their child’s UVR eye disease is due to our advice to keep their
children playing outdoors. The exposure for UVR eye diseases commonly occurs in childhood, but the diseases frequently manifest in adulthood, after cumulative damage has already occurred. In order to reduce the prevalence of these UVR related eye diseases, childhood UV exposure should be minimised.
Eyecare professionals are in the ideal position to lead the change in understanding and minimising the long-term impact of both myopia and UVR eye diseases, by educating patients, and encouraging the use of maximally protective sunglasses for children. We need to take a holistic approach to eyecare and diseases prevention, it is important to reduce the rates of axial myopia but equally we need to ensure that we don’t inadvertently increase the rates of UV related eye diseases.
NOTE: References will appear in the online version of this article.
Dr Shanel Sharma, Dr Alina Zeldovich and Dr Daya Sharma founded Beamers, which produces and sells sunglasses with Optoshield technology to address all three pathways of UVR reaching the eye and periorbital skin: www.beamers.com.au.
ODMA gears up for 2025 fair
Planning continues for the return of the popular trade fair in Sydney next year. Insight talks to the event's key organiser about what people can expect to see, what’s new and how the industry can benefit.
The future of the optometry industry sometimes keeps Ms Amanda Trotman up at night.
Other people might count sheep as they lay back and surrender to slumber, but it’s questions that often rumble around the head of the Optical Distributors and Manufacturer’s Association (ODMA) CEO.
She’s thinking about the increasing corporatisation of the industry and the many challenges and opportunities that go with running independent businesses in a tough economy.
“It’s about how I can help buck some of those trends? How do we ensure new and health fund clients are being referred to independent practices, not just to chains? How do I utilise a website that shows where independent practices are located? How do I get messaging out to consumers? How do I help independent practices partner with suppliers for mutual benefit? How does the optical industry embrace the latest technology confidently?”
Luckily for those independents and others, Trotman and her team are working to answer those questions, bringing experts, experienced speakers and industry representatives together for the ODMAFair25, running from 27 to 29 June. The popular event is returning to Sydney at the International Convention Centre (ICC).
One of those speakers is Mr Adam Spencer, who will kick off the event during a lively and entertaining breakfast and networking session.
A well-known and engaging speaker, with many years of experience in TV, radio and events, Spencer is particularly focused on the rise of artificial intelligence (AI) and Chat GPT, cyber security, and the future of work.
How to use technological advances for good and avoid potential risks can keep business owners awake at night, but Trotman hopes Spencer's presentation and others will help optometry practitioners sleep a little easier.
“We made the decision that it would be nice to have someone like Adam who has a broader perspective,” says Trotman. “Someone who was going to be inspirational and make us maybe think outside the box more.”
Other key speakers will include Provision’s Mr Mark Corduff and Mr Philip Rose of Eyecare Plus on How to Become a Practice Owner; Dr Soojin Nam and Ms Heidi Hunter, both independent practice owner-optometrists, on Establishing Your Practice Point of Difference; and 2022 International Optician of the Year Mr Grant Hannaford, of The Academy of Advanced Ophthalmic
Optics, dissecting Myopia Management for the Optical Dispenser
An opening breakfast event and keynote speaker are not the only innovations planned for next year's fair.
Trotman and her team recently announced new awards for the event, with fresh categories including Best Independent Practice of the Year, Best Independent Practice Window Dressing, Versatile Frame of the Year, and Top Customer Service Team.
Other awards include those for the best supplier and sales representative.
At the centre of the large exhibition space will be a Knowledge Centre.
That’s where the short but informative education sessions will be run.
“We have found in the past that it can be hard to run these sessions given the background noise, so we are going to do presentations with headsets here for the first time; people will be able to sit and listen to those sessions and not feel like they can’t concentrate,” says Trotman.
These will be in addition to the three education streams highlighted at the event, which will run in conference rooms outside the fair: business; practice management; and dispensing.
BACK TO THE FUTURE
Trotman says the fair is returning to Sydney, in part as a response to a number of calls from the industry. More details are yet to come about what will happen with O-SHOW, run in alternate years, and ODMA’s event presence in Melbourne.
Importantly, the venue in the Darling Harbour precinct will provide plenty of room for exhibitors keen on more space, as well as the Knowledge Centre and catering to support people at the event.
Some of that space will be used by Optometry NSW/ACT, which has joined forces with ODMA to have its Super Sunday clinical conference aligned with the trade fair and under the same roof.
Trotman is particularly excited about this collaboration – another example of listening to industry feedback.
“We’re very mindful that other associations and not-for-profit groups are all running events as important parts of their offering too, and the ODMAFair event is a chance for us to help others get some efficiencies from scale and save some costs whilst each event helps bolster attendance at the other's event.
“ODMA is very focused on the business and practical advice, and we wanted to put together a program for that and have that complement the other associations’ CPD focus,” she says.
“Other associations must deliver CPD sessions to members, whereas ODMA, with its strong trade industry focus, is very good at the business, practice management and dispensing focus. By collaborating on Super Sunday and also with ACBO for their annual conference, we are avoiding stepping on any toes, whilst being able to also incorporate a CPD element, so we just think this model we have initiated achieves the best of both worlds and ultimately increases return on investment for both practice attendees and exhibitors.”
She sees that collaboration and events like ODMAFair25 as vital as the industry, and independent practices in particular, face a number of challenges and opportunities.
“We’re seeing new offerings such as Optometrist Warehouse by Chemist Warehouse and some lens companies increasing consumer marketing budgets, and I think we’re going to see more brand awareness of the different lens options and benefits amongst consumers, and with all this I see a need for the independent practice messaging to gain cut-through with consumers.
Myopia management will be an even bigger focus in future, with messaging aimed at parents given the children’s high level of screen time.
“I’d love to start to see the messaging: you go to the dentist twice a year, why don’t you get your eyes checked regularly even if you do not need glasses currently.”
“I’d love to start to see the messaging: you go to the dentist twice a year, why don’t you get your eyes checked regularly even if you do not need glasses currently.”
Innovation and new technology will likely be hot topics at the fair too.
“AI and intelligent glasses, seeing how excited everyone is about their advancement, but now the question is turning to: ‘what does this mean for privacy? What does this mean for safety? And so we are hoping to find some speakers willing to have a good question and answer session on some of these topics that are still new and emerging and help us all get up to speed.”
Trotman doesn’t expect all those questions to find answers at this one event, but she believes the networking opportunity it presents, and the bringing together of so many optometrists, practice owners, suppliers and associated professionals in one place means a lot of progress will be made.
A UNIQUE OPPORTUNITY
It will also mean a great opportunity for suppliers too, despite the significant cost of attending and exhibiting for some.
“It’s not cheap to have a sales rep on the road, trying to cover practices across large areas, and often not able to show a full product range despite lugging around a lot of product," says Trotman.
“Rather than attending optical practices trying to get them to spend the required time to look at your products, and they’re rushed and they’re distracted, events offer a nice alternative where people that come to this event come to do business and focus on their business future away from their place of work. It’s a unique opportunity.
“People are going to go there to see certain suppliers, plus for sure something else will catch their eye, and that might never have happened, if they didn’t walk down an aisle.”
The impact is positive for everyone involved, she says.
“I’m still a very, very big advocate of live events.
“It’s such a unique opportunity, and you can’t put into words that when you’re there, the buzz, the positivity and the optimism at our events is inspiring.
"And it’s conducive to doing good business and fostering good business relationships,” she says.
At time of writing, three-quarters of the booths were already accounted for, and Trotman and her team were now looking wider than the traditional exhibitors, to those many other companies that support the optometry industry. “I’d like to get some of those miscellaneous services, whether that’s insurance, banking, fit-out companies.”
She is confident that the fair will be a success, but she does have one plea for those exhibiting and others considering it.
“We’d like to get exhibitors to do a better job of telling us what they’re going to have on their booths, so we can then help them market that better; tell us what’s newly released, what has not been seen in Australia before, about the new technology.”
If that can be done, and it helps people realise it is a must-attend event and it contributes to a great result, then Trotman believes ODMAFair25 will help build a better, stronger optometry industry.
“There’s room for both – the corporates and the independents – but we don’t want to get to a point where the independents feel that their only succession plan is selling to a corporate chain.
"So we are here to support those conversations with our program and speakers and networking opportunities and that is also why we work closely with the buying groups and their immense expertise.
“We hope to attract both experienced and young optometrists to the event, and some of our talks may inspire some to grow their business or set up a specialisation and for some to start their own practice down the track," she says.
Amanda Trotman ODMA
"And maybe, people who already have an optometry business can start thinking about their succession plan well in advance and bring on people that will buy into their business, which is a real positive for the continued strength of the independent sector.”
Fostering these connections and helping them grow will likely mean a more restful night’s sleep for all.
ABOVE, L to R: ODMAFair25 is a unique opportunity for suppliers to meet many of their customers in one place; the event will be held at the International Convention Centre in Sydney; Adam Spencer will be the opening speaker during a new breakfast event.
RANZCO roundup: 2024 congress highlights
The well-oiled machine that is the RANZCO Congress headed to Adelaide where ophthalmologists heard about the big issues the college is grappling with behind the scenes, as well as some positive news on the First Nations workforce front.
The RANZCO Plenary session at the college’s annual congress often acts as an excellent barometer for the health of ophthalmology in Australia.
The hour-long session is a moment for prominent RANZCO figures to update fellows on various workforce and eyecare accessibility issues across Australia, while also highlighting the college’s relevance in two spheres: the contemporary medical landscape and eyecare ecosystem.
But it’s on this final point that plenary chair Dr Grant Raymond, who ended his two-year RANZCO presidential term at the congress in Adelaide 1-4 November 2024, left fellows with plenty to ponder.
He said RANZCO and other specialist medical colleges had never been under greater government scrutiny. In the last 16 months alone, the college has made some 41 written responses.
“Some 14 important government reviews have been or are presently under way. This is a massive resourcing and financial impost on RANZCO. The price we are paying for having a seat at the table is very high,” said Dr Raymond who passed the presidential reins over to Professor Peter McCluskey with Dr Diana Conrad now vice president.
The two most pressing issues for RANZCO are the Kruk review and the National Health Practitioner Ombudsman Review – and Dr Raymond made RANZCO’s position clear on these two matters.
On the Kruk review, which is fast-tracking specialist international medical graduates (SIMGs) into Australia, he said doctors from certain countries will be entering the national health system through expedited Ahpra pathways –without college assessment. They would only be supervised for six months.
With ophthalmology expected to be involved in 2025, he said there is no individual assessment of experience, breadth of practice or recency of practice.
“RANZCO believes this approach, with limited assessment and oversight will produce patient safety and quality of practice issues, it will likely exacerbate issues with workforce maldistribution and worsen rural training options.
“What is needed is investment in public hospital regional and rural health services and increased regional and rural training posts. The band aid the government is proposing is nothing more than a temporary part-solution.”
He said RANZCO would “demonstrate good faith” by developing its own expedited pathway that would only be for SIMGs assessed as substantially comparable.
RANZCO’s present figures suggest 47% of English SIMG applicants when assessed individually are not considered substantially comparable with Australian-trained ophthalmologists.
On the National Health Practitioner Ombudsman – “the new cop on the block” – Dr Raymond said it was uncertain whether the Australian Medical Council will take control away from colleges for accrediting training posts in public hospitals.
“Should SIMG assessment and hospital training post accreditation be taken away from colleges, RANZCO’s role will be substantively changed. RANZCO is somewhat a recipient of collateral damage from some problematic issues with other colleges,” he said.
“Watch this space.”
Tasmania ophthalmologist Dr Kristin Bell, the RANZCO 'Vision 2030 and beyond' clinician lead, said a lot of these issues came down to poor governance over the years and a lack of accountability of state and federal governments.
It’s led to “huge gaps in service delivery” that’s “ad hoc” across Australia, disadvantaging regional and vulnerable Australians. Preventable blindness in these communities isn’t something that sat well with the college, she said.
“The consequences are coming home to roost for the governments of Australia, and hence this is probably the driver for the regulatory changes that [Dr Grant Raymond] has mentioned. Governments are getting a bit desperate. We’re running short on GPs, the workforce is in the wrong place and, not
Images: Prime Creative Media.
Dr Grant Raymond (from left) chairing the RANZCO Plenary alongside Dr Kristin Bell, Dr Justin Mora and Prof Nitin Verma.
Tim Jarvis, an environmental scientist, adventurer, author and film-maker, delivered a memorable keynote.
surprisingly, people are starting to notice.”
Fast-tracking overseas trained doctors into Australia was a knee jerk, band aid option that would not deliver a sustainable solution.
Instead, governments should be investing in public hospitals.
“They grow our workforce, and they also determine where our workforce into the future is distributed,” she said.
“We don’t know how all of these reviews of the regulatory environment are going to come home to roost, but we do know that they’re going to impact on how the specialist medical workforce is trained and assessed in Australia.
“The monopoly we have at the moment, on training the ophthalmologists of the future, we may not have that going forward. So everything’s up for grabs, and we really have to position ourselves to be part of the solution.”
BIG INROADS INTO FIRST NATIONS WORKFORCE
Meanwhile, Dr John Kennedy’s update on RANZCO’s philanthropic activities through the Australia and New Zealand Eye Foundation (ANZEF) came with a more upbeat tone.
Most encouraging is the pipeline of First Nations ophthalmologists for Australia and New Zealand.
Currently, there’s just one Indigenous ophthalmologist in Australia, Dr Kris Rallah-Baker – a major underrepresentation with 3% of the population Aboriginal or Torres Strait Islander. And in New Zealand – where 18% of the population are Maori – there’s just four Maori and two Pasifika ophthalmologists.
“The simple premise is that despite massive efforts over the years, Indigenous eye health remains in a less-than-ideal state. If there were more Indigenous ophthalmologists, then they may take the lead in addressing the problems in their communities, and ANZEF is actively promoting projects to increase the number of trainees."
A big part of this has been reducing financial barriers for First Nations trainees such as $30,000 towards the $50,000-$60,000 exam and administration costs over the five-year training program.
After beginning the program in 2022, by next year there will be 10 First Nations trainees in the program – evenly split across Australia and New Zealand.
“Our college leads the way among medical specialties,” Dr Kennedy noted.
“As well as supporting trainee eye registrars, we have a program to get Indigenous medical students switched on to a career in ophthalmology. There are currently two fourth-year medical students at UNSW completing an Indigenous Ophthalmology Award scholarship, and there’s a new Glaukos three-year grant for medical students in South Australia from Adelaide and Flinders universities.
“Currently, one way or another, we have more than 40 First Nations medical students and junior doctors engaged with ophthalmology as a potential career.”
Dr Kennedy also acknowledged an ANZEF-Alcon partnership worth $47,000 a year over three years for some 100 scholarships throughout Australia, New Zealand and the Pacific region.
HIGHLIGHTS FROM THE CONFERENCE AND TRADE FLOOR
The first full official day of the meeting started on an inspiring note with keynote speaker Tim Jarvis AM offering sage leadership advice he gleaned from retracing a miracle Antarctic expedition of Ernest Shackleton with the same equipment and clothing.
He expertly weaved in some key messages around climate change and sustainability – and gave the audience plenty to think about when it comes to medical waste.
“The carbon footprint of the medical industry in Australia is twice that of aviation, can you believe?”
He urged leaders to distinguish between their vision and mission.
“Shackleton didn’t use these words, but my take on it is that he said, ‘look, the mission is to cross Antarctica. Unfortunately, now it’s off with the loss of the ship. The new mission is to save ourselves. The good news is the vision is still very
GRADUATION AND AWARDS EVENING
• Thirty-three doctors admitted as fellows by the Vocational Training Program pathway
• Fiv e doctors admitted as fellows by the Specialist International Medical Graduate pathway
• Dr D avid Lubeck admitted as a fellows by the Ophthalmologist of Eminence pathway
Trainers of Excellence 2024
• Dr Alexandra Crawford – New Zealand
• Dr Anne Mala tt – Sydney Eye Hospital
• Dr B en LaHood – South Australia
• Dr Geo ffrey Chan – Western Australia
• Dr John Do wnie – Prince of Wales Hospital Prof Shuan Dai –Queensland
• Dr Szczepan Nowakowski – Victoria
• Dr Colin Thomps on – Regionally Enhanced Training Network
much intact. The vision was to do something at the limits of human endurance, return heroes or whatever it might have been. It’s very important to have a clear understanding of what the vision is. If all you’ve got is a mission, it makes it very difficult to change the way you do things.”
Among the major lectures, Professor Robyn Jamieson’s Ida Mann Lecture on the future of gene therapies and precision medicine was a highlight, as was Dr Rosa Braga-Mele’s cataract update that covered a tremendous amount of territory from exercises avoid musculoskeletal pain through to the latest phaco technology.
Flinders University’s Professor Justine Smith had a full house for her update on the “wide world of uveitis”. And Professor Stuart McGregor’s description of how an Australian team translated a polygenic risk score (saliva test) from the lab into commercial use through Seonix Bio offered a glimpse into how eyecare professionals may soon identify patients at risk of glaucoma and other diseases like keratoconus.
On the exhibition floor, the big talking points were Alcon’s new Unity Vitreoretinal Cataract System and UNITY Cataract System. They were contained in a closed off area with only selected ophthalmologists able to experience the technology that will effectively replace its Constellation Vision System and Centurion Vision System with Active Sentry, respectively.
ZEISS and Bausch + Lomb also made their presence felt with new surgical microscope technologies while Glaukos Corporation proudly showed off its new three-stent iStent infinite system for glaucoma.
And there was also plenty of interest in the new spiral intraocular lens (IOL) design from Rayner, Galaxy and Galaxy Toric.
The next RANZCO Congress is heading to Victoria 14-17 November 2025 at the Melbourne Convention and Exhibition Centre.
A feature of the congress is the networking that happens during session breaks.
Conference with twist doesn’t disappoint
Ophthalmology Updates! and its unique format is the ideal remedy to keep on top of an ophthalmic landscape being shaped advances in AI, geography atrophy and disease diagnosis, plus more.
Questions and dilemmas ophthalmologists will need to grapple with around artificial intelligence (AI) generated some of the liveliest debate at the recent Ophthalmology Updates! conference in Sydney.
So too did arguments over new versus legacy anti-VEGF injections for neovascular age-related macular degeneration (nAMD), two promising drugs for geographic atrophy (GA), and the potential of an Australiandeveloped saliva test for glaucoma.
Over a beautiful sunny weekend in Sydney 24-25 August, delegates from across Australia and New Zealand gathered at the iconic Fullerton Hotel for the annual conference.
It’s a key opportunity to brush up on common subspecialty topics and learn about frontier issues while also leaving plenty of room for debate between the audience and presenters.
In 2024, attendees were treated to a dash of Hollywood Pizzazz, as the “Cataract Coach”, Dr Uday Devgan, returned to Australia to share his wisdom. Known for his dedication to teaching, with daily surgical videos uploaded online, Dr Devgan took the audience through numerous common and uncommon scenarios in cataract surgery.
Posterior capsule tears, traumatic cataract, white cataract and surgery in the setting of poor zonular support were all covered using examples from Dr Devgan’s extensive library of videos, all freely available at cataractcoach.com.
AI continues to draw increasing interest in ophthalmology and was a key focus of the meeting.
Professor Pearse Keane, Professor of Artificial Intelligence at University College London, took delegates on a journey from the historical
development of AI to its current state-of-the-art, raising questions about the potential impact of the rapid advancement in this field on the practice of ophthalmology.
Community screening for common eye diseases, and accurate and efficient recruitment of patients to clinical trials are just a few areas that may benefit in coming years, he explained.
A panel discussion with Melbourne’s Professor Peter Van Wijngaarden delved into the many potential advantages, pitfalls and ethical issues in this area. How far do we trust AI in its current state? Who is responsible for errors made by AI? These are among many questions we will need to consider over time.
Prominent Australian glaucoma specialist Professor Jamie Craig shared interesting data from the PROGRESSA study. It revealed that glaucoma suspects with higher stiffness parameters and lower central corneal thickness are more likely to progress. Additionally, factors such as cardiovascular disease, low BMI (body mass index) and sleep apnoea may be linked to a greater risk of progression.
Prof Craig also detailed SightScore, a polygenic risk score for primary open angle glaucoma developed after years of research. This test, which analyses a saliva sample, is currently available to clinicians (although not subsidised). It has the potential to identify individuals at highest risk for glaucoma, enabling clinicians to prioritise and target screening and monitoring more efficiently.
Meanwhile, Associate Professor Rishi Gupta from Halifax, Nova Scotia, Canada provided insightful talks on the interpretation of pigment epithelial detachments and management of primary intraocular lymphoma. His vitreoretinal surgery session with cases of intraocular foreign bodies was a stark reminder of the importance of wearing safety eyewear.
Images: Ophthalmology Updates!
Prof Pearse Keane (left) and Prof Peter van Wijngaarden during the session on AI.
A/Prof Rishi Gupta during his retina update.
Dr Andrea Ang (from left), Dr Tayna Trinh and A/Prof Chameen Samarawickrama were among the delegates and speakers.
A/Prof Gupta put forth his best effort to win over the local audience as one half of two “great debates” with Associate Professor Hemal Mehta. These debates centred around: faricimab versus aflibercept for nAMD, and Syfovre versus Izervay for GA. In both cases audiences were reasonably divided.
Dr Andrea Ang, from the Lions Eye Institute, highlighted the lack of significant advancement in treating HSV keratitis since the Herpetic Eye Disease Study (HEDS) 30 years ago.
However, it remains a condition many clinicians find difficult to manage and her insights into use of steroids in HSV keratitis were valuable.
Many clinicians without expertise in cornea may have been wondering what in the world CAIRS was – and they were enlightened by Dr Ang’s clear summary of Corneal Allogenic Intrastromal Ring Segments for keratoconus.
Sydney-based Dr Loren Rose provided an update on ongoing advances with myopia management with particular relevance to optometrists.
Updates on the management of thyroid eye disease, choroidal haemangioma, and scleritis were provided by local specialists.
Dr Darshi Ramanathan, a neurologist with a special interest in MOG-Antibody Associated Disease (MOGAD), bridged the gap between neurologists and ophthalmologists to improve understanding of this increasingly diagnosed condition.
After launching eight years ago – and missing a couple of years due to COVID – Ophthalmology Updates! continues to be an innovative, collegial and highly educational event on the conference calendar.
For event convenor Professor Adrian Fung, the opportunity to ask questions is valued most by delegates, with more than 200 people attending in 2024.
“The field of ophthalmology – and the subspecialities within it – changes fast. Treatment options have changed since Ophthalmology Updates! first started in 2016,” Prof Fung said.
TARGETED ENERGY TO TREAT DRY EYES AND INFLAMMATION
“This event is an opportunity to learn from each other and share our real-world experiences. There is a lot of discussion on areas where there’s room for debate on the best way to manage patients.”
He said the conference model includes revision of a ‘common’ condition across a range of subspecialities, as well as exploration of a ‘frontier’ topic on a topical subject.
“With speakers presenting the newest data in their field, the event provides a yearly concentrated overview from experts on the latest diagnostic techniques and treatments across a range of subspecialties,” he said. Details for Ophthalmology Updates! 2025 will be announced soon.
Dr Uday Devgan, the ‘Cataract Coach, flew in from the US to deliver his session.
Ellex – the sum of its parts
Given the precision required for laser procedures, ophthalmologists expect the same from their manufacturer. But that’s easier said than done, as South Australian-based Ellex Medical can attest to, as one of few firms globally with the technical ability to make their entire units in-house.
In ophthalmology rooms and hospitals across the world are 38,300 medical instruments branding the Ellex name. Most are ophthalmic laser units; incredibly intricate, high precision pieces of kit the Australian business has built a reputation on for more than three decades.
Given that ophthalmologists are firing lasers into delicate ocular tissues for glaucoma, retinal conditions and posterior capsulotomies, it’s no surprise the expertise to build such instrumentation is limited to few manufacturers globally.
What many may not appreciate is the bulk of these units involve hundreds of components largely assembled by hand. But the other thing they may not realise is that 100% of Ellex Medical lasers are built in Mawson Lakes, a suburb 12km north of Adelaide’s centre, where it employs around 130 staff.
It’s part of the Technology Park precinct alongside more than 100 other like-minded companies in defence and aerospace, advanced electronics and IT. Some of them are global firms, and it would be fair to count Ellex among them.
The company is highly self-sufficient, machining many of its own parts and building the highly complex laser cavities at the heart of its instrumentation. It’s something it’s proud of given there’s limited companies globally with this technical know-how (more on this later).
Insight recently toured the headquarters of Ellex that lives on as an Australian success story, buoyed by the backing of its relatively new European parent company Lumibird.
Today, the company produces around 100 laser systems per month, with each individual unit taking three to four weeks to complete, on average. Around 95% are exported to international markets, Europe and Japan the largest.
It’s remarkable when you consider how it all began – back in the 1980s with
an Australian scientific laser company called Quentron.
It was a government grant that paved the way for Quentron to expand into ophthalmic lasers. The first of those was a YAG laser photodisruptor, a device that stood at the intersection of function, ergonomics and aesthetic design.
Later, Quentron was acquired by venture capitalists who rebranded as Laserex. At this vital juncture in 1990, a management buy-out saw Ellex emerge as an independent company with its ophthalmic laser technology.
There’s been many highlights along the way.
As it continued to produce proprietary lasers, Ellex also signed original equipment manufacturer (OEM) deals with companies like Alcon and Lumenis. In 2000, it entered the photocoagulator market with Laserex Integre, then expanded further in 2006 by acquiring ophthalmic ultrasound technology.
As the company grew, so did expectations by going public on the ASX in 2001. It outsized its premises multiple times, moving into Technology Park in 2017.
It also had forays into other areas such as its 2RT system for intermediate-stage disease, and minimally invasive glaucoma surgery (MIGS) with the iTrack canaloplasty. Both of these products would be separated from the business to form Nova Eye Medical in 2020.
That’s because Ellex – and its laser and ultrasound products – were acquired by Lumibird, a European technology company whose subsidiary, Quantel Medical, was competing with Ellex in the market.
The Lumibird Medical division now comprises three complementary divisions: Ellex (Australia), Quantel (France) and Optotek (Slovenia).
Ellex continues to flourish under the synergistic effect of joining a group with similar expertise. Together, the group has more than 200 patents and launches two to three new instruments a year. Ellex is a strong contributor with equipment like the Neo premium laser range (Ultra Q Reflex Neo, Tango Neo and Tango Reflex Neo) in 2022.
But what’s also pleasing for Ellex customers is they now have access to more technology. For instance, Ellex has divested its own ultrasound technology and now is supplying the superior ABSOLU system from Quantel. There’s also the PROcap (Premium Refractive Outcome Capsulotomy) YAG capsulotomy platform available in Ellex systems, and the ability to now reach customer bases it never envisaged such as in dry eye diagnosis (C.DIAG) and intense pulsed light treatment (C.STIM).
KEEPING IT IN-HOUSE
Ellex’s Technology Park site is how you’d expect – a factory with a real clinical edge. It’s spacious, highly organised and the production teams go about their work diligently. There’s half-built laser units, each clearly labelled with a model and serial number, and signs above some doors warning “laser firing” might be in session.
Each Ellex laser goes through a four-step process overseen by an expert workforce. It’s difficult enough manufacturing medical equipment, but even harder when it involves a laser.
As Ms Angela Standing, Ellex general manager, explains, this is why the process requires an incredible level of detail and tight control.
“A laser has an intricate optical path generating differing laser wavelengths that flow through to a delivery path to the end patient,” she says. “This involves fine alignment of many optical and mechanical elements and thorough calibration/testing at each process, including quality specifications at each stage of product realisation, to ensure end product requirements are met.”
But before they even begin assembly, they need to validate each part is manufactured as intended. It’s a big job when you consider more than 5,000 unique parts go into Ellex lasers, most of those produced internally.
The four key areas that go into manufacturing an Ellex laser are: optical assembly, mechanical assembly, the all-important laser cavity build, and integration.
The optical and mechanical assembly teams are responsible for crafting all optical and mechanical assemblies. Depending on the complexity
Images: Ellex.
involved, assemblies can take anywhere from a few minutes to several hours to complete.
“As an example, our Tango SLT laser has 40 sub-assemblies comprising more than 500 unique parts,” Standing says.
The company’s team of laser cavity builders is responsible for just that.
To understand why few companies possess this technical capability, Ellex says it comes down to the complicated nature of ophthalmic laser production. Given the wavelengths involved – and the need to ensure accuracy “within excruciatingly tight tolerances” – ophthalmic laser cavities are inherently complex to manufacture.
Further exemplifying this, all laser cavities have a mixture of optical, mechanical and electronic elements that are built as small sub-assemblies before being brought to life by being placed, aligned, calibrated and tested in the laser cavity housing. In the case of Ellex’s Yttrium Aluminum Garnett (YAG) laser cavity, the YAG crystal involved is doped with a rare-earth element – typically neodymium (Nd) – to create the laser active medium. The cavity ensures the light remains coherent and focussed.
Bringing together the various assemblies during the laser cavity build generally takes several days. Which is remarkable when you consider the cavity is not much larger than a tennis ball.
“The majority of our competitors outsource the manufacture of their laser cavities. In contrast, we have a strong IP platform and equally skilled manufacturing teams which enables us to conduct the manufacture of our laser cavities in-house,” Standing says.
It all occurs in a sealed off area, known as its Controlled Environment Room (CER). Air in this room is “scrubbed” by high velocity HEPA-filters to control airborne particles that also control temperature and humidity controls. All who enter must move through an “air shower” to minimise particulate matter, and wear clothing coverings.
“Any pollutants, such as dust, can lessen the product life of a laser which is heavily reliant on clean optical paths,” Standing says.
Use of specialised test equipment and software also take place in the CER. This is part of the laser cavity build test qualification process to ensure correct alignment, calibration and the relevant power specifications.
Once the laser cavity build is completed, the system is passed on to the integration team that brings everything together to create the finished product.
They follow a precise procedures and a commissioning book of detailed full system alignment and calibration specifications to ensure all Ellex systems meet quality requirements. From testing output power on power meters, electronic specifications on oscilloscopes, through to checking micron size laser beam parameters on a beam view camera, these are all vital steps to ensure the lasers work as intended the moment they’re unboxed by the ophthalmologist.
TOOLING ITS OWN PARTS
Another way Ellex has been able to keep its edge is through the Ellex Machine Shop (EMS), which it started in 2001.
Given the need for high-precision components, EMS is responsible for machining some components used in the sub-assemblies and system parts. Again, it’s all about achieving more consistency and quality control.
“The establishment of EMS has enabled a higher level of consistency and quality in system components than was previously possible with external suppliers, which is paramount in ensuring that the lasers produced deliver the intended treatment effect,” Standing says.
EMS also supplies to several other third-party customers. But equally, Ellex does outsource some components to some local, interstate and international suppliers. This includes the low-value, low-complexity components, as well as small number of highly specialised components, such as cable assemblies.
Thanks to Adelaide’s reputation as in defense technology, this proximity has given Ellex easy access to world-class laser and optical resources.
“Maintaining the SA-based manufacture of our products is also important from an IP standpoint,” Standing says.
“We hold several patents with respect to our laser cavity design, but it also enables us to closely align the activities of our engineering and manufacturing teams, which ensures improved efficiency across both teams and helps us maintain the highest standards of quality.”
A finished laser unit, which take three to four weeks to complete on average.
Ellex produces many of its own laser components in the Ellex Machine Shop.
Angela Standing is general manager of the Ellex business.
Scopes that make the surgeon shine
Two Australian ophthalmologists speak to Insight about why they are excited about the double-release of microscopy technology from ZEISS – even though they focus on entirely different segments of the eye.
Two instruments caused the most buzz on the ZEISS booth at the recent RANZCO Congress in Adelaide – and both for the same reason.
When most manufacturers pour their efforts into microscopy technology, it can take years to emerge with a single state-of-the-art system, but ZEISS has made a splash in the local market with two distinct microscopes under its ARTEVO product line.
Whether you’re an anterior or posterior segment surgeon, ophthalmologists are excited about the potential of this technology to bring a new edge to their surgical work.
After releasing what it describes as the industry’s first digital microscope (the ARTVEO 800 in 2019), the ARTEVO 850 is the company’s latest innovation in heads-up 3D visualisation surgery, something that has been popular in the vitreoretinal space.
Meanwhile, the ARTEVO 750 is its latest microscope targeted mainly at cataract surgeons, building on the success of its LUMERA technology that has long been a standard-bearer in operating theatres across the country.
Intraoperative OCT (iOCT) is a key feature in both technologies, along with a host of other innovations that vitreoretinal surgeon Professor Andrew Chang and cataract surgeon Dr Georgia Cleary had first access to in Australia.
IN THE VITREORETINAL SURGEON’S HANDS
In the weeks leading into the RANZCO Congress, ZEISS put the ARTEVO 850 into the hands of Prof Chang, head of ophthalmology at the Sydney Eye Hospital and medical director of Sydney Retina Clinic.
He was impressed on several fronts. Not only does the heads-up display promote better posture, but he can perform retinal surgery with a magnified stereo view, wearing 3D glasses that bring all-important depth perception to his work. In fact, surgeons can boost this by 60% using the new Smart DoF function.
An improvement ZEISS has made for the ARTEVO 850 is true colour representation, with more than 1 billion colours used to represent the surgical field in natural colours. This is thanks to a high dynamic range (HDR) monitor and two 4K three-chip cameras, projecting the surgical image in high fidelity on a 55-inch screen.
With the surgery easily viewable to everyone in the operating room, Prof Chang says theatre support staff can more readily respond to the surgeon’s needs and trainee doctors can learn more effectively.
“The surgeons can also move from anterior to posterior segment very easily on the ARTEVO 850,” Prof Chang says, referencing the AutoAdjust function that automatically changes the settings when switching between the two.
“The other advantage is the Hybrid Viewing System, allowing you to wear the stereo glasses to view the magnified image in stereo on the screen, and still maintaining the ability look down the oculars of the operating microscope
to perform certain parts of the surgery.”
With advances in technology, Prof Chang observed that “latency” issues on the heads-up display are greatly reduced. In earlier versions of these microscopes, he says surgeons had to adapt to a slight lag, but ZEISS had overcome this with improved computing power and technology.
Speaking at a ZEISS-hosted breakfast at the RANZCO Congress, Prof Chang walked through recent surgeries using the ARTEVO 850 where, in many cases, iOCT was crucial to macular surgery. For example, showing the fine layers of the neural macular and confirming successful removal of retinal membranes just several microns thick.
“Amazingly, the iOCT just passes through [vitreous] fluid, and even though we have stained the membrane blue, the OCT still shows you the precise neural structure. It’s reached a point where iOCT images are virtually as good whilst in surgery as those we obtain in the clinic.
“The other benefit of the ARTEVO 850 is the ability to change the colour of illumination, for example enhancing the colour blue can help to better visualise retinal membranes.”
Here, he’s referring to the Digital Color Assistant function to accentuate anatomical details.
Prof Chang highlighted a diabetic patient who, despite previous laser, suddenly lost vision and could only see hand movements. He had a diabetic tractional retinal detachment and vitreous haemorrhage, making it difficult to visualise the macula.
“But when I positioned the iOCT over it, you can see the traction bands and where they are attached, showing where to dissect tissue and target precisely where the traction is located. The macula might be covered with blood, but the iOCT shows that the macula is spared so this patient should recover vision after surgery.”
He expects the ARTEVO 850 to shine in other areas, such as gene therapies administered by subretinal injection, as well as tPA injections for submacular haemorrhage.
“When we match the intraoperative image with the pre-op scan, this is super quick, much faster than the previous model. Together, these improvements all shave time off each case.”
Dr Georgia Cleary Melbourne ophthalmologist
Image: ZEISS.
The ARTEVO 850 is ZEISS’ latest innovation in 3D visualisation ophthalmic surgery.
Image: Georgia Cleary.
iOCT is crucial to ensuring the surgeon is accessing the precise retinal layer.
But its capabilities go beyond vitreoretinal surgery, with other ophthalmic subspecialists able to benefit.
“Our anterior segment colleagues find the iOCT very useful when performing DSEK as they can ensure that the graft is in place. Glaucoma surgeons benefit from the high digital magnification when they precisely place their stents,” he says.
“It’s a game-changer for posterior segment work, but the ARTEVO 850 is excellent for anterior segment surgery as well. This technologic platform allows us to work from front to back of the eyes seamlessly, safely and effectively.”
CATARACT SURGEON ‘SHAVING TIME OFF EACH CASE’
Across the various Melbourne surgical facilities Dr Clearly performs ophthalmic surgery in, she’s had access to a ZEISS OPMI LUMERA 700. It’s been a workhorse microscope over the years; one she describes as the industry standard – up until this point.
But she’s somewhat disappointed to go back to her old microscope after trialling the ZEISS technology poised to supersede it, the ARTEVO 750.
She spoke to Insight following two cataract lists at Cabrini Brighton with the new microscope, where she was struck by several improvements around patient safety, pre- and intra-operative surgical efficiency, and the upgrade to the CALLISTO eye 5.0 system that acts as the surgeon’s “intuitive cockpit” alongside the microscope.
She’s also excited about the potential of greater visualisation in her corneal transplant work. This is on top of all the other hallmarks of ZEISS microscopy such as reliability, image quality and digital integration with instrumentation, such as the IOLMaster 700 biometer, used in the work-up phase.
Among the new features, ZEISS is promoting the RGB LED illumination function (also available on the ARTEVO 850) that allows ophthalmologists to select different light colour temperatures according to their preferences. A mix of red, green and blue LEDs generate different light color temperatures, from cold to warm.
There’s also AdVision, a system that overlays surgery data into the eyepiece at a 40% higher resolution and high contrast. The surgeon can select from a wide range of cataract assistance functions, phaco parameters or iOCT.
“It was very customisable; for example, we played with the capsulorrhexis overlay and I found I liked a yellow circle that wasn’t bold, so that it didn’t interfere with the task at hand,” Dr Cleary, who’s also head of the Surgical Ophthalmology Unit at the Royal Victorian Eye and Ear Hospital, says.
“But additionally, there’s lots of useful content that one can see in this heads-up display. It included patient details, the intended toric axis, whether the recording is on or off, and the colour temperature in use. This data is located peripherally in the digital overlay, which is great because it doesn’t distract you while operating.
“But even just having the patient’s name and details in there is a constant reminder that we have the correct patient in front of us at all times.”
In fact, Dr Cleary says there are other ARTEVO 750 features that enhance patient safety, largely thanks to graphical interface improvements ZEISS has made to CALLISTO eye.
Integrating the microscope with this system gives surgeons like Dr Cleary a centralised point of control. It might sound simple, but an example of this is the new patient summary page. When the theatre team take their ‘time out’ prior to each case, it allows them to easily confirm what’s on the operating table aligns with the surgical plan.
“It’s all presented on a nice layout and now there’s a diagram that shows us the toric alignment which was not present on the previous iteration. It’s excellent for patient safety; this page didn’t exist to the same degree in the previous model.”
She’s also noticed much speedier patient data upload into the microscope,
creating new efficiencies for theatre staff, and fewer steps.
Digital toric alignment is a key application of CALLISTO eye in the cataract surgery workflow. This requires the microscope to match an intraoperative image of the eye with a pre-operative scleral image obtained on the IOLMaster 700.
“The other big thing: when we match the intraoperative image with the pre-op scan, this is super quick, much faster than the previous model.
“Together, these improvements all shave time off each case.”
Dr Cleary says ophthalmologists make the common mistake of associating CALLISTO with markerless toric alignment only. But in reality it can perform other tasks such as sizing of the capsulorrhexis or pinpointing the incision placement.
In the latest update, these cataract assistance functions can be completely surgeon-controlled with a push of a button on either the foot control panel or handgrips.
During her first surgical lists with the ARTEVO 750, Dr Cleary briefly used the iOCT function that she expects will reap benefits in corneal transplant work too.
“The iOCT image was definitely enhanced from the previous Rescan, and also captured images and zipped to the correct focal plane incredibly quickly,” she says.
“Previously, the ambient lighting of the operating theatre could make it difficult to see the image on the screen clearly, but this was much sharper and offered greater contrast.”
ABOVE: Prof Andrew Chang taking advantage of the Hybrid Viewing System on the ARTEVO 850, allowing him to view the magnified image in stereo on the screen while maintaining the ability to look down the microscope’s oculars.
Image: Andrew Chang.
Image: ZEISS.
Out of sight, out of mind
Insight regularly publishes inspiring stories of charitable work and outreach programs. The eyecare sector is a generous one, but is that work masking a darker inconvenient truth for Australians living in the nation’s regional, rural and remote areas?
The Tyranny of Distance sounds like an epic novel, a tale of high-seas adventure and thrilling journeys to exotic locations on the other side of the world.
But sadly, for many Australians it is a term denoting something rather more dystopian: a desperate thriller in which health outcomes are uncertain, the danger is very real, and the threats grow the further you move from the relative safety of the nation’s main centres.
Poor health outcomes and even higher mortality rates are a fact, not a fiction, for many.
The shocking tale is outlined in the numbers.
According to the Australian Institute of Health and Welfare (AIHW), more than 7 million people (29% of the population) live in regional and rural Australia.
Those people face challenges accessing health care, including eye health services, which can lead to higher levels of chronic disease and injury, and shorter lives.
The statistics make it clear: the further you are away from the main centres, the shorter your life is likely to be.
In AIHW 2021 data, age-standardised mortality rates increased as remoteness increased for males and females.
Compared with all of Australia:
• People living in inner or outer regional areas had a mortality rate 1.1 times as high.
• People living in remote areas had a mortality rate 1.2 times as high.
• People living in very remote areas had a mortality rate 1.5 times as high.
It’s a similar story in eye health.
Writ large early in RANZCO’s Vision for Australia’s Eye Healthcare to 2030 and Beyond is one simple statement: “Timely access to eye healthcare prevents more than 80% of permanent visual impairment and blindness.”
But further reading reveals that access is neither timely nor effective, especially in Australia’s smaller, more distant communities.
People in the cities may grumble about wait times at their local hospital, but they appear to be the lucky ones.
Recent data shows people waiting an average 69 days for cataract surgery in the city, with that nearly doubling in the outer regions (129 days) and very remote communities (114 days).
Some areas have practically no access to ophthalmology services, according to RANZCO.
“Approximately 30% of the entire population and more than 60% of the
Aboriginal and Torres Strait Islander population, which is more regionally based, have no or very limited access to publicly funded outpatient services in the area they live,” it said in its report.
“Some inner urban, many outer urban, and most regional Local Health Networks (LHNs) do not fund public ophthalmology outpatient services at all. These services represent 80% of ophthalmic healthcare delivery.”
RANZCO outlines a number of reasons for this failure, including a lack of an over-arching plan for national service delivery and poor funding of the LHNs.
“The chronic lack of investment in public ophthalmology services across Australia . . . has driven a substantial and increasing imbalance in the ophthalmology workforce between the public and private sectors.”
That means almost 90% of the work ophthalmologists do is in the private sector and often beyond the financial grasp of many who rely on public services.
The picture is not much better in the optometry sector.
In a recent global survey, Australia was one of just 46% of nations to meet the mark on the recommended optometry ratio: one professional for every 10,000 citizens.
But it appears Australia’s commendable ratio of 1:3,897 is heavily focused on the main streets and thriving malls of its bigger cities, rather than the quieter roads of its regional, rural and remote centres.
Government figures from 2019 show that the ratio of optometrists for every
“Many Australians, predominantly in regional and rural areas, are not able to access timely, preventative eyecare within their communities, simply because there is no optometrist available. In 20 years, 2 million Australians will need eye tests but will not be able to access them.”
Dr Ben Ashby Specsavers
Image: totajla/shutterstock.com.
ABOVE: Statistics show that the further you are away from Australia’s metropolitan centres, the more likely you are to have poor health outcomes.
Image: Specsavers.
100,000 people was 20.7 in metropolitan centres, above the 19.1 average for all Australia.
That actually increased to 22.7 in its larger rural centres, but it was downhill from there: 18.3 in regional centres, 17.6 in medium rural towns, 3.7 in small rural towns, and 8.5 in remote communities.
While some reports have tipped an oversupply of optometrists, one major study commissioned by Specsavers suggested a developing deficit over the next 20 years, with its impacts hitting hardest in the regions and beyond.
The 2023 analysis by Deloitte Access Economics forecasts a shortage of 1,102 full-time equivalent optometrists in 2042, with more than 800 of those in the regions.
Concerned about this inequitable access to eye care, the company offers optometrists significant packages and support for those willing to relocate and practice outside of the big cities.
And like a number of eyecare providers, Specsavers is also trialling the use of technology to support remote optometry work in which a patient can be assessed within their own community by an optometrist who is located many miles away.
That might be part of a future solution, but let’s first get a better understanding of the present threat to eye health and its impact on vulnerable communities.
ROAD BLOCKS AND BLIND SPOTS IN THE REGIONS
There is more than a hint of resignation in Dr Andrew McAllister’s voice.
It was there in a recent RANZCO podcast on the health of regional ophthalmology and it’s there now as he speaks with Insight
It’s a resignation borne of frustration from constantly butting heads with bureaucracy in a vain attempt to bring accessible eye health services to his region.
Dr McAllister is an ophthalmologist and retinal subspecialist with his own practice in Toowoomba, a Queensland city with a population of about 170,000 serving the large catchment of Darling Downs, with close to 300,000 people. Despite that size, the region has no public ophthalmic services, with patients without private cover needing to travel more than one and a half hours from Toowoomba to Brisbane for care, and a great deal more if they live further out.
In 2022-23, the Queensland Government spent $84.24 million through the Patient Travel Subsidy Scheme (PTSS) to support people needing to travel for
specialist public healthcare, including ophthalmology. The subsidy covers part of their travel and accommodation costs.
Patients driving past one of the six private ophthalmologists in Toowoomba and continuing down the Warrego Highway to Brisbane cost taxpayers just under $6.8m that year.
And the figure is set to rise after the government this year committed to covering the entire accommodation cost of a patient’s first four days, at a commitment of $70.3m over the next four years. That means the annual cost of the PTSS is likely to go beyond $100m.
That still leaves many patients with much to pay from their own pockets, with some needing to stay a week and more in Brisbane, meaning obvious financial impacts through loss of income and other costs, including food and hospital parking, which can be $100 a day.
None of that makes sense to Dr McAllister and others, who have spent a great deal of their own time caring for those communities missing out, and bashing against those bureaucratic brick walls, from every conceivable angle.
“The patients don't need to go to Brisbane for emergency surgery,” says Dr McAllister. “Having the specialist skills that I've got as a retinal surgeon means that we can definitely treat patients locally.”
For those specialists, the tyranny of distance is the defeat of logic and common sense. And the silence from those entrusted with ensuring public access to healthcare.
It all comes at great cost to “marginalised” regional and remote communities.
“These people living in rural areas, they don’t always seek care because of difficulty in transport, distance of travel, and quite often you'll see some chronic diseases that haven't been treated as well as they should have,” he says.
Motivated by his father, a long-serving GP in the region, and ophthalmology mentor Dr Bill Glasson, Dr McAllister applied for a public ophthalmology role when he first moved back to Toowoomba in 2019.
But in a sign of what was to come over the next five years, “the role was rescinded due to a lack of funding”. That left him with no other option than to move into private practice.
It has been a similar refrain for every idea put forward by Dr McAllister and his colleagues over those years. Even when they have offered their services for free.
“I've offered to see patients in my rooms and set up everything myself, and
Patients needing specialist treatment in Queensland are often transported to Brisbane, despite the long distances and great expense involved.
because I've got my own practice and the expense associated with that, I was quite happy to start a clinic for the public hospital based in my private rooms initially, until I had something set up.”
The answer back from Queensland’s public health executives has always been a polite thanks, but no thanks: there is money to transport and house patients from the deepest parts of this large region but none to set up or subsidise public services closer to home.
That is unlikely to change, even when the region gets a new hospital –expected to be some time in the next decade.
When locals pushed for ophthalmic services in that plan, the answer was the same as that given to Dr McAllister’s petition of the state government in 2023: there is no money to fund public ophthalmology in Toowoomba or in other equally struggling regional centres.
If the government is relying on private practice and the generosity of industry outreach and charity to pick up the slack, Dr McAllister says that too is starting to look shaky.
Among Toowoomba’s ophthalmology community is at least one practitioner well into his 70s.
And as is the case in other regions, recruitment is tough.
“I've been advertising for ophthalmologists for at least the last 18 months; it's been extremely hard,” says Dr McAllister.
“We've had no interest from locally trained ophthalmologists to settle here in Toowoomba.”
There has been some interest overseas but, ironically, given the paucity of public services, the area does not qualify as a “region of need”, meaning applications for registration are not supported.
It would be understandable if Dr McAllister suffered a little 'PTSS-D'. It appears he and many others have been left to carry the burden of not only filling the many gaps in available care but also planning for ophthalmology’s uncertain future in his region.
“The system is really kind of failing the area,” he laments.
But as well as the resignation in his voice, there remains some resilience.
“I guess I've got to a point where we've looked at multiple ways to try and get around on this, and you know, there's no point whingeing and banging your head,” he says.
“You take things in your own hands and come up with a solution that you know is going to be beneficial for the local population, even when the health department isn't that interested.
“Until there is a genuine interest from the public hospital and from the politicians that look after this area, it's really just up to us as individuals to start making changes.”
SHOULD’VE GONE TO THE REGIONS…
On the surface, optometry looks pretty healthy in Australia.
The country is comfortably meeting the recommended international ratio of professionals to patients, and there appears to be no shortage of practices and practitioners.
But even at Specsavers, the nation’s largest provider of eyecare with almost
“It's left up to the Local Hospital Networks to decide what service they'll deliver, and at times they just entirely withdraw services because they don't have to provide them.”
400 locations across all states and territories, there are troubling clouds on the horizon.
Like other businesses and industries, it is struggling to find optometrists and eyecare professionals willing to stray too far beyond the bright lights of Australia’s biggest centres.
Dr Ben Ashby, the company’s director of clinical services for ANZ, says 40% of its Australian locations have an unfilled optometry vacancy over the course of the year, with more than 60% of those outside the major cities.
That’s despite Specsavers promoting the benefits of regional communities, offering support to relocate, and other inducements, including regular trips home and extra leave.
“Many Australians, predominantly in regional and rural areas, are not able to access timely, preventative eyecare within their communities, simply because there is no optometrist available,” he says.
“In 20 years, 2 million Australians will need eye tests but will not be able to access them.”
To help fix that, Specsavers has been trialling a remote model of care in several Victoria, Tasmania and NSW regional locations.
As part of that trial, nearly 500 people have visited a clinical practice where a technician supports an optometrist working from an off-site location.
Communicating via live video-conferencing, the optometrist and technician organise OCT, tonometer and autorefractor tests, ask basic questions of the patient and then review the clinical results.
Dr Ashby says the pilot has shown that remote eyecare detects eye conditions at rates equal to traditional in-person eye consultations.
Despite that success, he says it is not a replacement for in-person eyecare in regional areas but rather “a viable solution to help bridge the gap in underserviced areas . . . so patients do not have long wait times and experience unnecessary barriers to routine care simply because of where they live”.
The company has identified more than 100 locations that could use the remote eyecare model, but it is not funded by Medicare, meaning the service would not be financially viable.
“Without Medicare funding, the financial cost to roll this out would not be sustainable,” says Dr Ashby.
The company has joined others in the industry, including Optometry Australia, in calling on the Federal Government to include this model in the MBS so that people living in regional and remote areas can have access to the service.
GOVERNMENTS STATE AND FEDERAL ROOT OF THE PROBLEM
Dr Kristin Bell RANZCO
Specsavers and Optometry Australia are not alone in prodding the states and Commonwealth to step in and step up to deliver timely and effective eyecare in regional, rural and remote areas.
A failure in leadership by those in charge of healthcare in Australia is
Specsavers has been trialling remote optometry work for communities where it is struggling to recruit optometrists.
Image: Specsavers.
Image: Kristin Bell.
probably the main complaint for Dr Kristin Bell. This has resulted in a lack of governance and poor accountability over the equitable funding and delivery of healthcare.
“I think you can point to one particular group, and that's the health ministers and the health secretaries of Australia,” says the Hobart ophthalmologist, who is also RANZCO’s Vision 2030 and beyond clinical lead, regional education chair and lead of its regionally enhanced training network.
She sees public ophthalmology as a struggling tree tended by an indifferent gardener.
That lack of leadership and attention has undermined all that might have given it life. Not just the tree but the roots that support its weight, the branches that dictate the health and effectiveness of its reach, and the workforce needed to ensure all are healthy and sustainable.
The 2020-25 National Health Reform Agreement was supposed to be that core document from which other branches of state and federal government would ensure the healthy spread of equitable funding and services, including ophthalmology, into and across all of Australia.
But that has not happened, says Dr Bell.
“There is simply no governance or checks and balances to make sure that they're actually doing that in regional areas,” she says.
That lack of a plan and the accountability that might have gone with it has allowed state and regional health powerbrokers to turn inward, centralise funding and delivery, and practically ignore the regions.
“It's left up to the Local Hospital Network (LHNs) to decide what service they'll deliver,” says Dr Bell. “And at times they just entirely withdraw services because they don't have to provide them.”
A recent report commissioned by the National Rural Health Alliance estimated each person in rural Australia was missing out on $850 in healthcare funding each year – about $6.5b annually.
No plan, no accountability, and no collection of data to help officials better understand the impact of that deficit.
“They're not including waitlists for outpatient services, so how can you actually see if services like ophthalmology are equitably delivered?”
It’s tempting to suggest that it’s the sector itself and private individuals that have had to step in to the vacuum left by this indifferent government gardener. That the tree would indeed wither and maybe die without that effort.
Dr Bell doesn’t agree.
“I think we are just making sure we're not part of the problem, and we really
Dr Andrew McAllister has offered to take on public patients in his Toowoomba practice, but instead must watch them transported to Brisbane, costing many millions of dollars.
want to be part of the solution,” she says. “We're all doing our bit, running collaborative workshops with Optometry Australia, Orthoptics Australia, a number of the NGOs, GPs and non-ophthalmic specialists.
“We're doing all the things we can do on our side. And then on top of that, we are using our voice to advocate as much as we can, and we partner with others as well to try and amplify that voice.”
THE GOVERNMENTS RESPOND
The Commonwealth and the state governments insist they are listening.
Queensland Health says it is committed to providing high-quality eyecare to all Queenslanders.
A spokesperson said that, in the 2023-24 financial year, it had performed more than 13,000 elective ophthalmology surgeries, effectively managing the waitlist, despite a 3% increase in demand.
“As a largely decentralised state, we do face unique challenges in delivering healthcare,” they said. “To ensure equitable access to eye care,especially in rural and remote areas, we deploy visiting ophthalmologists to provide essential services in regions like Thursday Island and Weipa.
“We are also actively working with tertiary education providers to increase the number of medical student placements.”
The spokesperson also said the Surgery Connect pathway had allowed public patients to access care in private hospitals, with 5,188 ophthalmology patients benefitting In 2023-24, in regions such as Cairns, Mackay, Townsville, and the Sunshine Coast.
The national Department of Health and Aged Care said it funded a number of eyecare outreach programs for indigenous communities in regional, rural and remote areas.
It was also spending $3.2m in the second nationwide survey of eye and ear health, as part of its commitments to United Nations goals towards eradicating avoidable blindness.
It was also working to implement priority actions under the National Strategic Action Plan for Macular Disease, with a focus on at-risk populations.
Regarding workforce issues for all medical specialists, the government had invested $708.6m over four years through its Specialist Training Program, “to extend vocational training for specialist registrars into settings outside traditional metropolitan teaching hospitals”.
And it was financially supporting organisations like RANZCO to increase ophthalmology training in regional, rural and remote areas.
Image: Toowoomba Retina & Eye Specialists.
Meet Dirk den Dulk
B.Opt, Cert OcTher, Cert in Practical Vision Therapy
Dirk den Dulk graduated from UNSW in 1979. Over his stellar career, he has owned 30 practices and has mentored students who now also work at George & Matilda Eyecare. His passion for optometry has not waned, with Dirk working part time at both our Albion Park and Balgownie practices, while also working 1 day at Illawarra Vision Therapy and volunteering as a Clinical Supervisor at Deakin University.
Dirk joined G&M almost 5 years ago. “I’m 110% happy! I’m the most relaxed I have ever been. I don’t have to worry about the backend, I get to focus on what I love which is looking after patients and in particular, paediatric optometry. With G&M’s model, you’re a partner, not an employee. You get to have a say, people listen, and you get good support. I would have joined G&M Eyecare sooner if only I knew about it earlier. My advice to anyone looking for balance in life or looking for a retirement plan, is ‘don’t wait!’”
“Being an optometrist is the most satisfying profession. Joining George & Matilda Eyecare has given me balance, so I can also enjoy a family life and be hands on with my grandchildren”
Let’s Connect Contact Cassie Gersbach, General Manager of Partnerships at cassie.gersbach@georgeandmatilda.com.au
Stepping up for patients with low vision
Specsavers has worked with Vision Australia to redesign the referral process for patients with low vision, providing an early opportunity to connect them with support and maintain their independence.
For Mr Chris Papatheodorou, a system change has prompted a big improvement in the way his team cares for patients with low vision and blindness when they visit the busy Specsavers Ringwood store in Victoria.
Today, he can register them with Vision Australia’s patient support service through the click of a button. This is because the process has now been integrated with the Oculo e-referral platform commonly used among Australian optometrists and ophthalmologists.
The change is part of Specsavers Ringwood’s broader involvement in a pilot between Specsavers and Vision Australia that commenced a little over a year ago. Store optometry director Papatheodorou says it has made the low-vision patient submission process much quicker.
“It’s a much-improved system compared to the former web-form process,” he says. “Referring patients via Oculo facilitates the missing inter-professional relationship between optometrists and Vision Australia’s client wellbeing team.”
When announcing the initiative in September 2023, Specsavers said the partnership emerged from a realisation that its optometrists could be further supporting patients with low vision. With optometrists so focused on detecting eye conditions early, there was often a reliance on ophthalmology colleagues to step in when patients experience low vision or blindness.
“However, thanks to organisations like Vision Australia, patients can receive services and support to power their independence – and it doesn’t have to be as a last resort,” says ANZ clinical services director Dr Ben Ashby.
“It is simply unfair that not all relevant patients have the opportunity to receive the extension of care that Vision Australia offers, so we’re doing all we can to make it easier for optometrists to refer their appropriate patients to Vision Australia when the timing is right.”
SPECSAVERS-VISION AUSTRALIA PILOT
Since late 2023, Specsavers and Vision Australia have been working together on “a holistic approach” to caring for people with low vision and blindness, thought to impact more than 450,000 Australians.
With this number predicted to grow to more than one million in 2050, Dr Ashby explains that as trusted and accessible frontline eye health professionals, optometrists have a role to play in improving their patients’ quality of life by referring them to an appropriate low-vision organisation.
“We’re proud to provide our customers with an exceptional level of clinical care. Through regular eye health checks and with our advanced OCT technology used in every eye exam, our optometrists do a great job of detecting changes in vision earlier than ever before. We want to make sure patients continue receiving care and support after they leave a Specsavers practice. And that’s where our partnership with Vision Australia comes in,” he says.
Patients with a visual acuity <6/12 with both eyes open and/or a visual field of ≤30 degrees meet the criteria for Vision Australia’s range of services. This includes connecting with trained support personnel, orientation and mobility
training, adaptive technology training, and support for family members and carers.
However, the organisation says it takes an average of five years for people to seek further support.
Vision Australia’s general manager of client services and transformation Ms Tania Hobson says this is partially driven by fear of confronting their eye condition but more so not knowing where to go or even that the support exists.
“We want to make sure health professionals know they can direct patients to Vision Australia for both support services as well as assistive technology that will help them to continue to live independently,” she says.
The pilot program with Specsavers is designed to uncover the barriers optometrists may face when connecting patients with support organisations, streamline the registration process, and increase referral rates to align with the assumed prevalence of low vision in the community.
STREAMLINED PATIENT SUBMISSION PROCESSES
In May 2024, Vision Australia accepted feedback from the Specsavers pilot that the existing patient registration process could be simplified.
So, the organisation made its support centres in Kooyong and Dandenong in Melbourne, along with Robina on the Gold Coast, available on the iCare Oculo platform to receive patient referrals.
This platform, originally developed in Australia and sold to Finnish company iCare in 2021, is designed to share clinical correspondence securely and instantly between healthcare professionals. It’s widely used by Australian optometrists and ophthalmologists.
All other Vision Australia centres are planned to be live on Oculo before the end of this year, allowing all optometry professionals to then refer directly to them.
Vision Australia reports to have already seen the impact of this adjustment,
Images: Specsavers.
Chris Papatheodorou, optometry director at Specsavers Ringwood.
Vision Australia’s Debbie Locke visiting the Specsavers team at Keysborough, Victoria.
"What many optometrists may not know is that their patients could be eligible for government funding that covers vital lifestyle aids that help them function day-to-day.”
Tania Hobson Vision Australia
with an increase of new patient submissions since the Melbourne and Gold Coast locations were added to Oculo.
As an extension of the pilot, Vision Australia representatives have visited selected Specsavers practices for face-to-face education and engagement sessions to better understand and address the barriers to optometry referrals.
Hobson says the small-group sessions have been a great way to explain the support on offer at a granular level, answer questions, and build mutual trust between the organisation and Specsavers practices.
“We know that optometrists genuinely care about their patients and want to be sure that they’re putting them in touch with an organisation that will give them the very best support and services after they leave the test room. By building these local relationships, I believe we’re starting to comprehend and overcome these barriers,” she says.
While many people have a general idea of what Vision Australia offers, Hobson says real-life examples of how different aids and technology are used can put it into perspective for patients and optometrists.
“Practical solutions, such as improved lighting along driveways or bigger, bolder and brighter settings on technology, can enhance daily living and help people who struggle to see,” she says. “And what many optometrists may not know is that their patients could be eligible for government funding that covers vital lifestyle aids that help them function day-to-day.”
COMPASSION FOR LOW-VISION PATIENTS
According to Vision Australia, empathising with the complex needs of low-vision patients is essential for eye health professionals. And referrals to support organisations often hinge on an optometrist’s perception of how their patient may benefit; however, seeing things through a patient’s eyes can be challenging.
“We know that vision loss is the least relatable condition, and we often don’t stop to consider how people living with low vision experience the world,”
Hobson says.
“The information sessions have allowed us to present the impacts of vision loss in a tangible and human way and put a patient-centric lens on the experience.”
In his practice, Papatheodorou says the team is now acutely aware of the role that patient support organisations play.
“Even if time in the test room is limited, we want to make sure we’re discussing the potential benefits for the patient and how it may improve their daily life, even at the earlier stages of vision loss,” he says.
After a year of collaboration, Specsavers and Vision Australia have been encouraged by the pilot. Many lessons have been learned about the referral process, and valuable knowledge has been shared between Specsavers optometrists and the patient support service.
“This important work with Specsavers is helping to ensure no Australian goes through the experience of living with low vision without being connected with the support and services that can improve their quality of life,” adds Hobson.
Insight’s new website keeps you updated on the latest industry news and information. With a world-class responsive design, Insight is now accessible seamlessly on any device, 24/7.
Sign-up FREE to our eNewsletters and industry reports delivered weekly straight to your inbox.
Opti-Soothe Preservative-free Eyelid Wipes are textured wipes for daily eyelid hygiene, infused with: Tea Tree Oil, Hyaluronic Acid, Chamomile, Aloe Vera & Green Tea Extract.
• Preservative-free
• 30 sterile textured wipes
• Unique gentle formulation
FATHER INSPIRATION FOR DISPENSING CAREER
DISPENSER DETAILS
Name: Jo Hershman
Position: Manager & wholesale business owner
(Rialto Eyewear)
Location: Cammeray
Optometrist, NSW
Years in industry: 35
1. What initially attracted you to a career
My father, Neil Hershman, ran a successful group of optometrists in the UK and from an early age, I would accompany him to help out. Later, when I started working alongside him, it gave me the opportunity to travel and work across the UK. The diversity of practice locations taught me valuable lessons about product selections for different demographics.
2. What are your main career highlights?
Firstly, I was fortunate to learn from the respected Professor Mo Jalie, a lecturer at City & Islington’s facilities. Secondly, I have had the opportunity to apply my education and experience to create Rialto Eyewear, my wholesale frame business with exclusive agency for Laibach & York, TC Charton and Rialto.
3. What are your strengths as an optical dispenser?
My attention to detail ensures eyewear fits both the prescription and the client’s needs. Staying up to date on the latest optical products,
definitely gives me an edge in making informed recommendations. Working both in retail and wholesale, I can contribute positively at different levels and it’s exciting to see my brands represented in optometry practices throughout the country.
4. What advice would you give yourself at the beginning of your career?
One of my biggest regrets is not establishing Rialto Eyewear sooner. I should have followed in my father’s footsteps when I first came to Australia.
5. What are the opportunities and challenges facing optical dispensing?
With the abundance of choices available to consumers today, practices must differentiate their services and provide excellent customer experiences to foster loyalty. The internet has created a vast marketplace for consumers. Offering exclusive products and delivering outstanding customer service are key strategies to compete effectively.
6. How do you ensure your skills and knowledge stay current?
I subscribe to optical magazines and forums, not just in Australia but worldwide. This keeps me informed on new products and the latest trends which usually emerge in Europe before reaching Australia. I also prioritise attending trade shows and maintaining regular communication with sales representatives, whether you buy from them or not. This insight is crucial in formulating our product mix at Rialto Eyewear too.
7. Why did you become a member of ODA?
It’s great to have an association with its members at the core. It serves as a source of information, and a facilitator of ongoing education.
8. What would you say to others thinking of joining ODA?
I encourage you to join the ODA. It provides a wealth of information, and the webinars alone are worth the membership fee.
Images:
Jo Hershman.
ABOVE: Jo Hershman’s passion for optics comes from her father, Neil, who ran a successful optometry group in the UK.
ABOVE: Attention to detail is one of Jo Hershman's strengths as an optical dispenser.
LOW VISION PATIENTS AND THE MOMENTS THAT MATTER
Simply spending a few minutes at the end of a consultation to discuss options with a low vision patient can be a life-altering interaction, writes Vision Australia's NABILL JACOB.
Eyecare professionals recognise modern medicine and new technologies have enormous benefits for patients with visual problems, but it’s important to remember many who lose their sight need help beyond what can be achieved with science and optics alone.
“MAINTAINING INDEPENDENT LIVING IS ARGUABLY THE MOST IMPORTANT SUPPORT, WE AS CLINICIANS, SHOULD PRESERVE.”
Unless you have had personal experience with sight loss – whether it’s progressive disease or an immediate loss –it is hard to imagine the life-altering impact. In most cases, the adaption needed is detrimental to the quality of that person’s life. All patients react differently; some may not yet be ready to accept it and the subsequent loss of independence.
Things like general mobility and navigation, digital communication, employment, socialising, shopping and medication management.
In addition, many studies have indicated the significant risk of falls or other injuries, exclusion and depression as vision decreases. Safety often threatens a person’s ability to remain in their own home. Maintaining independent living is arguably the most important support, we as clinicians, should preserve. The loss of something as simple as being able to read can be devastating.
WHAT DISPENSERS CAN DO
Anecdotally, approximately 60% of low vision patients still wear glasses to help. Of
all the eye professions, optical dispensers probably spend the most time with a patient assisting with optical needs in an arguably more relaxed and less clinical environment. Optical enhancement of their vision will be minimal in most cases, but this is where increasing the scope of your role may be beneficial.
Being able to explain a low vision condition and options, other than optical ones, can benefit the patient greatly. Making yourself aware of the specialised services Vision Australia provides to can be life-changing too.
As part of the eyecare team the optical dispenser is crucial. We know sometimes the optometrist may have already referred or discussed low vision services but hearing the same message twice can reinforce the message. Of course, sometimes things slips through the cracks and the optical dispenser can be the last line of defence.
HELPING A VISION IMPAIRED PATIENT
The great news is that life doesn’t stop after vision loss. By assessing a patient’s sight, namely their functional vision, Vision Australia can determine the best pathway. This may be maximising any remaining vision with more specialised optical aids, vision substitution e.g. use of senses such as hearing and/or touch, as well as looking at adapting that person’s physical environment.
Vision Australia can tailor strategies, services, aids and the latest technology, to achieve a patient’s personal goals and aspirations.
Regardless of remaining vision, or the stage of life whether it be a newborn or older Australian, Vision Australia can provide a one-stop-shop of services:
• Low vision orthoptist functional vision assessment, advice, optical aid options and prescription
• In-home ass essment and modification by occupational therapists to promote safe and improved living spaces
• Mobility training to develop the confidence and skill to safely navigate the environs. This may include using a white cane with or without a Seeing Eye Dog
• Technology consultants can recommend a range of adaptive technology options
based on individual requirements
• Support to prepare for, gain and stay in meaningful employment
• Facilitate understanding and access to the NDIS or My Aged Care funding streams
• Vision Australia radio and audio library introduction, with access to thousands of publications in multiple languages
• Age-appropriate social support groups
• In hous e direct access to retail aids, equipment and technology with expert retail staff to assist.
And yes, optical dispensers can refer, with a few things to note and some key criteria:
• The patient needs to be diagnosed with a permanent, non-correctable or progressive eye condition
• If you have any concerns that vision impairment is putting a patient at risk
• When a patient needs support adjusting to vision loss
• When vision loss starts to impact the quality of daily life
• Refer sooner rather than later when visual acuity and/or visual fields may be significantly impacted (e.g. < 6/12)
• The gradual introduction of the Oculo e-referral platform is ensuring a seamless referral option
Vision Australia has 150-plus years of providing services and programs to the blind and low vision community in Australia. This is done in various ways including telehealth and outreach services across and/or through their 30 offices nationally. The message is simple: easy and timely referral to Vision Australia can be life-changing and even life-saving for a newly diagnosed or long-suffering vision impaired patient.
Even if a patient isn’t ready, planting a seed of hope that expert and compassionate help is available for them live the life they choose is important.
A few minutes spent during your consultation can make all the difference.
RIGHT: A low vision patient using an aid to check prices at the supermarket.
ABOUT THE AUTHOR: Nabill Jacob is an orthoptist and the clinical relationship manager at Vision Australia. Image: Vision Australia.
NABILL JACOB
Image: Nabill Jacob.
LOOKING BACK AS WE FOCUS ON THE FUTURE
Professor KATHRYN ROSE reflects on a half-century in the orthoptics industry, and the many advances that have been made, particularly in education and research.
“I CAN’T QUITE BELIEVE WE ARE WHERE WE ARE AND WHERE WE WILL BE AS A PROFESSION IN THE NOT TOO DISTANT FUTURE.“
With retirement in March 2024 I can reflect on a 50-year career as an orthoptist, educator and researcher, and the tremendous changes in orthoptics that have occurred over that time.
I was in the last cohort trained at Sydney Eye Hospital, in a course that was focused purely on traditional orthoptics.
I spent the years after graduation working as a sole orthoptist in western Sydney, where few orthoptists worked at the time, and at Bankstown and Prince of Wales hospitals, which introduced me to working collaboratively with ophthalmologists.
Importantly, I became the community orthoptist in Liverpool.
Working with community nurses in school screening brought me face-to-face with the unmet need for eyecare in the area and ignited my passion for ensuring children had every opportunity to develop good vision and the best eyesight for their education. Adding ophthalmics to my skillset led to an offer in the late 1970s from Cumberland College of Health Sciences (CCHS) School of Orthoptics in NSW to introduce teaching in this area in the then-Diploma course.
I found teaching very rewarding and continued to work part-time at CCHS while working in private practice until the mid-1980s. By this time the scope of the orthoptics course had expanded to include a number of ancillary ophthalmic skills, which most orthoptists today would be surprised were not the norm prior to the 1980s.
That expanded role for orthoptists and the inclusion of core science and social science subjects was leading towards the first Bachelor of Orthoptics.
However, I had taken a side-step. In order to progress as an academic I needed further qualifications. A Graduate Diploma in Neuroscience and PhD in Visual Neuroscience from John Curtin School of Medical Research at the Australian National University provided me with an understanding of the importance of research and its potential to drive knowledge and change practice.
It was during this time that I became interested in the emerging epidemic of myopia in East Asia, eventually leading me to epidemiological research and a research
actively with research groups in South-East Asia and China.
The landscape of orthoptic education was very different when I returned in 2000 to what was now the School of Applied Vision Science, University of Sydney.
It was recognised that to elevate orthoptics’ profile and professional standing in the clinical and scientific communities, it was crucial to increase research output and foster more advanced research qualifications within the field.
The next five years made slow headway, but as involvement in major epidemiological studies grew, such as the Blue Mountains Eye studies and the Sydney Childhood Eye studies such as the Sydney Myopia Study, opportunities for high-quality PhD projects also grew, while research started to become embedded in every aspect of the course.
The transition to the University of Technology Sydney (UTS) in 2015 was crucial for the establishment of the high-quality UTS Master of Orthoptics.
Working in a collaborative environment with other allied health professionals, we were finally able to develop all of the key features of orthoptic education at UTS today.
Using blended learning modes of education allowed students to maximise the value of their face-to-face time with lecturers and to use case-based peer learning in small groups.
Housed in purpose-built facilities, we were able to conduct dedicated clinical laboratory teaching, led by practitioner teachers who brought their up-to-date
allowed the development of an intensive, highly scaffolded and educationally robust course of education.
The course content is guided by a supportive Orthoptic Industry Advisory Board, enhanced by collaboration with the major players in the ophthalmic industry and staffed by highly educated and dedicated lecturers and researchers, most of whom are home-grown PhDs.
This has enabled UTS Orthoptics to consider the future of orthoptic practice and, in particular, areas where there is opportunity for learning to perform in an advanced scope of orthoptic practice, and how this level of expertise is best achieved.
The next stage of orthoptic education I leave to others as I exit left, but occasionally I look back to all that has changed and grown in my time in the profession and can’t quite believe we are where we are and where we will be as a profession in the not too distant future.
ABOUT THE AUTHOR: Professor Kathryn Rose has played an integral role in developing the profession through the education of future orthoptists as lecturer at the University of Sydney for many years and as the head of discipline at University of Technology Sydney (UTS) from 2014 to 2024. She is also a leading international researcher on the development of vision and refractive errors in children and adolescents.
ORTHOPTICS AUSTRALIA is the national peak body representing orthoptists in Australia. OA’s Vision is to support orthoptists to provide excellence and equity in eye health care. Visit: orthoptics.org.au
Image: Orthoptics Australia.
Education and the teaching of orthoptics has changed greatly over the past 50 years.
Image: Kathryn Rose.
KEEPING ON TOP OF YOUR BUSINESS DIRECTORY LISTINGS
Unknown to many practitioners, Google, Microsoft, and Apple have created business directory listings for them without their input or permission. CARL JONES outlines compliance issues and practice growth opportunities.
“THESE LISTINGS SERVE AS THE FIRST AND OFTEN ONLY IMPRESSION A POTENTIAL NEW PATIENT GETS OF A PRACTICE OR INDIVIDUAL PRACTITIONER.”
Australian healthcare professionals generally understand the need to adhere to Australian Health Practitioner Regulation Agency (Ahpra) Guidelines, The National Law, and the Competition and Consumer Act when advertising their services. Many practitioners are unaware of the rules in relation to local business directory listings. The Ahpra Guidelines define local business directory listings as advertising rather than social media.
But many face an ‘unclaimed listings’ dilemma.
Unknown to many practices and practitioners, Google, Microsoft, and Apple have created business directory listings for them without their input or permission. These unclaimed directory listings often contain incorrect information. They serve as the first and often only impression a potential new patient gets of a practice or individual practitioner because they appear at the top of the Google results page above websites. If the first impression is not favourable, people will tend not to proceed to your website and instead consider other practitioners.
THE CHALLENGE OF CONTROL
Practitioners cannot delete a listing created for them nor will platforms delete an unwanted listing. The platforms are in a race, each trying to be the largest business directory. Control and maintenance of these listings is therefore a problem forced onto the practitioner.
Listings are created from data found by Google on websites and crowdsourced by user suggestions. Google may find outdated information from anywhere on the web, and anyone may ‘suggest an edit’ to Google. Google may edit your listing information so that it doesn’t accurately represent what you do or what your qualifications are. Google will edit a listing, even if it has been claimed by you, and generally won’t notify you of the changes until you log into your account. That edited information is live to the public until you revert it. Constant vigilance is required. Many professional associations in Australia have asked Google to disable reviews for practitioners. Google has not yet made changes in France, which is usually the first jurisdiction to win such concessions.
A Google My Business account is the way practice owners can claim ownership of their business profile.
Frustratingly, reviews are a central feature of listings and here to stay.
THE SOLUTION: ACTIVE MANAGEMENT
Ahpra requires healthcare providers to Check > Correct > Comply when advertising a regulated health service. Practitioners need to manage the listings themselves or via a management provider.
Here are some steps to effectively manage your local directory listings:
1. Start by creating an account and claiming your listings on the following platforms: - Google Business Profile
- Microsoft Bing Places for Business - Apple Business Connect
2. Ensure that the data accurately represents you or your practice. If visibility to high purchase intent customers is important to you, consider the search engine optimisation guidelines set out by each platform or consult your management provider.
3. Frequently check your listings for data updates. Respond to all Google reviews with an acknowledgment that does not imply that the information in the review is a testimonial.
Flag all inappropriate reviews with Google and follow-up with their customer service team if the review is not removed after flagging.
Compliance with the Guidelines requires practitioners to check their local business listings and correct them as required to
comply with Section 30 of the Health Practitioner Regulation National Law. Compliance should always be met. This requires healthcare providers to have a real-time monitoring and audit process in place and to promptly correct non-complying content that is visible to patients. If it is impractical to frequently monitor your listings, consider outsourcing the management of them. This is possible by inviting a manager to your listings via the settings tab of each listing. You continue to own the listings, and the manager can be replaced or removed by you at any time.
THE SHIFT TOWARDS AI
In 2025, powered by AI, these platforms will aim to deliver a simple, perfectly correct answer to a user. The AI needs quality data to give a correct answer. Google regards the information contained in their own business listings as superior to information published on websites. Information on your listings, even reviews, which are often ill-thought-out, will soon significantly influence how the public perceives you and your practice. Active management of online directory listings is a necessity for practitioners. A proactive approach helps to maintain professional standards, enhances the patient experience and assists practice growth. The time to act is now.
ABOUT THE AUTHOR: Carl Jones is a product specialist at localmanager.com.au.
Image: Vladimka
Image: Primacy Group.
SOAPBOX
COMBATING ‘FRAGILITY’ OF OPHTHALMIC META-ANALYSES
Translational Research (PROTON) is led by Associate Professor Rupesh Agrawal, from the National Healthcare Group Eye Institute (NHGEI), Singapore. PROTON is committed to advancing research and innovation in ocular inflammatory and infectious diseases. As part of our efforts, we have performed more than 10 systematic reviews and meta-analyses, providing valuable insights into these complex conditions and contributing to the development of more effective treatments and interventions.
Our group recently read up on an article by Nanji et al., which discussed the statistical fragility of meta-analyses in the ophthalmology field.1 His paper found that unfortunately, the statistical significance of various papers often hinged on the outcome of a handful of patients. Associated with this, Nanji’s group recommended the usage of the Fragility Index (FI) parameter – an easily interpretable measure of statistical robustness of any published systematic review and meta-analysis.2 So, what are the implications for the everyday eyecare professional?
First, we need to define meta-analyses. These are a form of systematic review that synthesise data from multiple previous studies addressing the same research question, thereby increasing the overall sample size and improving the
statistical power and generalisability of They are a valuable tool in evidence-based practice, often used by clinicians to inform decision-making and develop review articles. The process of conducting a meta-analysis involves several rigorous steps, including the systematic selection of relevant studies, development of strict inclusion and exclusion criteria, data extraction, and advanced statistical analyses to combine the results across studies, among other methodological considerations. Clinical practice is inherently shaped by academic literature, the best available evidence, and the strength of its recommendations.4 The summative nature of existing evidence portrayed by meta-analyses make it the strongest candidate for informing clinical practice worldwide.5 To put this into perspective, the meta-analysis published in 2014 by Tham et al, titled ‘Global Prevalence of Glaucoma and Projections of Glaucoma Burden through 2040: A Systematic Review and Meta-Analysis’ is among the most highly cited papers in the field of ophthalmology ever published.6 According to Google Scholar at the time of writing, this meta-analysis has been cited a whopping 7,083 times, placing it within the top 1% of most highly cited ophthalmology articles of all time.7 It has gone on to influence public policy, including Optometry Australia’s Clinical Practice Guide on Glaucoma.8
However, the meta-analyses which are most influenced by the usage of the Fragility Index (FI) statistic are those which evaluate differences between the clinical outcomes of two interventions. This is because the downstream impact is the favoured practice of one approach over the other, and misleading statistical outcomes could starkly affect patient care across the field. Some examples of such meta-analyses include these by Tai et al and Quiroz-Reyes et al.9,10
In response to Nanji’s group, we added on by outlining a series of recommendations for the ophthalmology community with regards to future meta-analyses publications.11 These include:
• Incorporation of Fragility Index (FI) in the reporting and publication of all meta-analyses, with guidelines governing
a standard minimum FI before publication can proceed
• Greater community focus on the quality of meta-analyses over the quantity
• Provision of deeper contextual interpretations of findings to draw relevance between statistical significances and clinical practice
• Enhancement of peer review processes on meta-analyses, including the usage of appraisal tools
• More strategic funding and resource allocation towards training junior researchers on advanced statistical methods and meta-analyses proficiency
• Exploration of innovative approaches to meta-analyses, including large language models (LLMs) and other artificial intelligence (AI) technologies
• Enhancement of search strategies and increased availability of Cochrane Courses to reduce publication bias
• Improvement in the declaration of statistical methods and more thorough guidelines on their usage to maintain statistical rigour within the field Translationally, clinicians likely won’t be able to observe any improvements in the reliability of meta-analyses. However, as the pinnacle of statistical rigour in the academic world, meta-analyses have great influence in the scientific advancement of the field as a whole.12 While our patients may look the same as yesterday, inaccurate clinical practice guidelines may take decades, or even the next century, to manifest. It is paramount that we work towards a goal of reliable scientific literature as a community to ensure we tread along the right path, shoulder-to-shoulder.
ABOUT THE AUTHOR
Name: Mattias Wei Ren Kon
Qualifications: Currently an undergraduate reading my Bachelor’s Affiliations: Yong Loo Lin School of Medicine, National University of Singapore Location: Singapore Years in industry: 1
NOTE: Dr William Rojas-Carabali and A/Prof Rupesh Agrawal co-authored this article. References are available upon request and will appear in the online version of this article.
THE SUMMATIVE NATURE OF EXISTING EVIDENCE PORTRAYED BY META-ANALYSES MAKE IT THE STRONGEST CANDIDATE FOR INFORMING CLINICAL PRACTICE WORLDWIDE.
Image: Mattias Wei Ren Kon.
EVENTS CALENDAR
DECEMBER
2024
INTERNATIONAL SOCIETY OF OCULAR ONCOLOGY
Goa, India
3 – 7 December isoo2024.com
FEBRUARY 2025
MIDO EYEWEAR SHOW
Milan, Italy
8 – 10 February mido.com
ANZGS CONGRESS
Perth, Australia
14 – 16 February anzgsconference.com
VISION EXPO EAST
Florida, US
19 – 22 February east.visionexpo.com
MARCH 2025
100% OPTICAL
London, UK
1 – 3 March 100percentoptical.com
ODA INTERNATIONAL CONFERENCE
Sydney, Australia
7 – 8 March odamembers.com.au
APRIL
2025
ASIA-PACIFIC ACADEMY OF OPHTHALMOLOGY CONGRESS
New Delhi, India 3 – 6 April 2025.apaophth.org
MAY
2025
ARVO 2025 Utah, US 4 – 8 May arvo.org/annual-meeting
JUNE
2025
ODMAFAIR25
Sydney, Australia 27 – 29 June odma.com.au
JULY
2025
AUSCRS 2025
Darwin, Australia 16 – 19 July auscrs.org.au/2025-conference
Image: Min Jing/shutterstock.com.
Image: Vision Expo.
Image: Prime Creative Media.
heading to Darwin in July.
ICC Sydney will host ODMAFair25, Optometry NSW/ACT’s Super Sunday, and ACBO Connect 2025 under the same roof.
America’s flagship optical trade event Vision Expo East is taking place in Florida in February.
CHANGING LIVES THROUGH BETTER SIGHT
SPECSAVERS STORIES: DAVID TCHUNG
HOW DID YOU COME TO WORK AT SPECSAVERS?
I started my journey as an optical assistant while studying for my optometry degree. I wanted to get some hands-on practical experience in the optics field to complement my study. Having a pleasant first eye exam at Specsavers, I was eager to learn from professionals within the network.
WHAT WAS YOUR FIRST ROLE WITHIN THE BUSINESS?
Being an optical assistant involved pre-testing patients before they see the optometrist. I was super excited by the opportunity to put my optometry learnings into practice; seeing a wide array of ocular pathology and liaising with the optometrist on things I wasn’t quite sure of. It benefited both of us as we had the opportunity to briefly discuss rare cases and plan ahead before consulting with patients. Other responsibilities as an optical assistant included arriving customers, three-way handover with the optometry team and the patient, and guiding patients with their frame and lens choices based on their lifestyle needs. There was a huge amount of technical knowledge involved as an optical assistant but I’m grateful for the experience – it continues to benefit me after four years as an optometrist.
WHAT GROWTH OPPORTUNITIES HAVE PRESENTED THEMSELVES?
Upon graduating as an optometrist at the end of 2019, I relocated to Gippsland and started my full-time optometry role at Specsavers Sale. Occasionally, I’ve provided cover at the Traralgon and Warragul stores, allowing me to cover a range of patient demographics and
Specsavers
SO LET’S TALK!
In a few short years, Specsavers has achieved market leadership in Australia and New Zealand with more people choosing to have their eyes tested and buy their prescription eyewear from Specsavers than any other optometrist. To learn more about these roles, or to put your hand up for other roles as they emerge, please contact us today:
interesting cases as well as experiencing different styles store processes and cultures.
WHAT ARE YOUR TOP CAREER HIGHLIGHTS SINCE JOINING SPECSAVERS?
After three-plus years of practising in Gippsland, I came across a rare opportunity of joining the Specsavers Mobile Optometry Team (MOT). Having a strong interest in clinical optometry coupled with my experience of working across multiple Specsavers stores, I thought this was the perfect opportunity for my career development. It allows me to provide crucial eyecare to communities in need while allowing me to explore this wonderful country. Another big milestone was the opportunity to join the Pathway Program while being based on the Sunshine Coast. On top of that, I also have the pleasure of being the primary mentor of two excellent graduate optometrists and being directly involved in their early career development.
WHAT EXCITES YOU MOST ABOUT TURNING UP FOR WORK EACH DAY?
A bit cliché, but it is the simple things we do on a daily basis that often have the biggest impact on the lives of others. This may be as simple as prescribing glasses so patients can see and do what they enjoy most, such as reading a newspaper. It may be reassuring them that despite their flashes/floaters, it’s a normal process that happens and nothing of concern was seen today and advising them of symptoms to look out for with close reviews. A bit of reassurance and peace of mind can go a long way in making a big difference to the wellbeing and happiness of our patients.
ALL SPECSAVERS STORES NOW WITH OCT
Optometrist Joint Venture Partnership Opportunity – New Store, Swan Hill, VIC Specsavers has an exciting opportunity for an Optometrist looking to take the next step in their career and join the brand as a Joint Venture Partner at our brand-new store in Swan Hill, Victoria. Swan Hill is a vibrant city in Victoria’s northwest that blends regional charm with urban convenience. Situated along the picturesque Murray River, the city boasts stunning riverfront views, fresh produce, and a warm climate. With an array of outdoor recreational activities, cultural attractions, and a welcoming community – Swan Hill has something to offer everyone!
Optometrist Joint Venture Partnership Opportunity – New Store, Hamilton, VIC Specsavers are on the lookout for expressions of interest from Optometrists looking to take the next step in their career and join the brand as a Joint Venture Partner at our brand-new store in Hamilton, Victoria. Successful applicants will receive Specsavers’ award-winning support in building up their business, including team recruitment support and end-to-end financing on new stores. Specsavers Hamilton will be a new site offering the latest store features including optical test rooms, pre-test rooms, dispensing desks, state-of-the-art equipment including OCT, and the latest Specsavers fit out with digital displays and illuminated shelving.
Optometrist Opportunity – $170,000 package on offer! Specsavers Burnie, TAS
Working for Specsavers Burnie offers an exciting opportunity to enhance your knowledge and experience in optometry. In this new role, you’ll gain regular exposure to a diverse range of pathology cases, increasing your clinical skills. The strong relationships between Burnie’s optometrists and local ophthalmologists and eye hospitals foster a collaborative environment, ensuring you learn from experts in the field. With cutting-edge technology—including OCT free for every patient and career development opportunities, including Pathway to Partnership, you’ll be part of a team dedicated to providing exceptional eye care. Join us at Specsavers Burnie and make a meaningful impact!
Optometrist opportunity – Specsavers Gisborne, NZ
Join our Specsavers team as a full-time optometrist in Gisborne, one of New Zealand’s sunniest regions. We are seeking a skilled Optometrist to contribute to our vibrant community, renowned for its rich culture and stunning beaches. Enjoy a rewarding career in a supportive environment. Apply today!
Graduate Opportunities
Specsavers are still looking for final year students to join the Specsavers Graduate Program for 2025! With strong career development paths for optometrists, great graduate packages and a diverse range of patients in locations all across Australia and New Zealand, Specsavers remain the market leader within the Optical industry. If you like the idea of building your career and working in a patient-focused environment, then reach out to the graduate team at anz.graduateoptometry@specsavers.com
Marei von Brackel has been appointed as the new
expertise “perfectly aligns with our company’s goals and vision”, HOYA stated. “Joining us with the aim of enhancing our sales department and contributing to the continued growth and success of HOYA Lens insights that will greatly benefit both our team and