EYE INJECTION PATIENT Inside a proposed incentive scheme for ophthalmologists treating macular disease
RED LIGHT THERAPY –A GUIDE FOR CLINICIANS
Four Australasian myopia authorities share insights on this emerging treatment
Why a new diffractive IOL design has this WA surgeon reconsidering his approach
Are you an Optical Dispenser looking for more? At Specsavers, we are dedicated to helping you expand your retail and optometry skills. Take advantage of ongoing training and development opportunities to further your career.
Feel like growing your Optical Dispensing Career? spectrum-anz.com/ careers-at-specsavers
UP TO $150 EYE INJECTION INCENTIVE PER BULK BILLED PATIENT, UNDER PROPOSED SCHEME
More details of a proposed $11 million-a-year ‘Neovascular AMD treatment incentive program’ that would financially encourage more ophthalmologists to bulk bill for intravitreal injections have been released, in an initiative ophthalmology bodies support.
Under Macular Disease Foundation Australia (MDFA)’s proposed scheme, all ophthalmologists who bulk bill eye injections for age pensioners with neovascular age-related macular disease (nAMD) would be eligible to receive an incentive payment from the Federal Government.
Under the program, which MDFA began advocating for in March 2025, the treating ophthalmologist would receive $100 per eye injection service per patient with a pension card.
If the patient needs injections in both eyes and this is performed on
the same day in the same service episode, the reimbursement is estimated to be $50 for the second eye. The total reimbursement for the ophthalmologist would then be $150 under this proposal.
The initiative has been modelled on the incentive payment schemes eligible GPs receive when they bulk
bill patients. According to Medicare data for 2023, 67% of people having eye injections were not bulk billed.
In contrast, 77% of people seeing their GP in the same year were bulk billed.
MDFA CEO Dr Kathy Chapman said the organisation welcomed both major parties’ recent commitments
NEW OPTOMETRY WORKFORCE STUDY UNDER WAY
Optometry Australia (OA) says it’s clear optometrists on the ground in many areas of the country are experiencing the impacts of looming workforce oversupply, as the body announced an updated workforce projections study due early 2025.
As the number of registered optometrists passed 7,000 in 2024, OA notes new optometry graduates are also “facing challenges in securing employment”.
It has made another formal submission to the Federal Government’s Occupation Shortage List (OSL) program, which reports an optometry shortage in all states and territories, except Queensland where a regional shortage is reported.
In addition, OA CEO Ms Skye Cappuccio said employment and
locum options were “very limited in most areas, and we have seen salaries stagnate and reduce”.
“Workforce oversupply is problematic for the profession and, ultimately, the community. This is why we have been advocating against the introduction of any new schools of optometry,” she said.
“At the same time, we know that there remains concerning level of unmet eye health needs across the country.
“There is opportunity to utilise our highly skilled optometry workforce in ways that can meet more of the unmet eyecare needs across our communities. This offers benefits for the profession and the community. It demands that we act today to ensure a positive future for tomorrow’s profession. This is a key focus for OA
and demands a collaborative effort from the profession.”
Optometry workforce supply is a complicated issue, with different perspectives.
Specsavers released a 2023 report stating a significant shortfall of more than 1,100 full time equivalent (FTE) optometrists by 2042, an undersupply of more than 1.5 million clinical optometry hours, or approximately a 12% shortage, compared to the total hours of eyecare expected in demand by then. This is despite projections optometry numbers will increase 57% from 5,266 FTE in 2022 to 8,261 by 2042.
Since 2010, four new optometry schools have emerged. The University
continued page 8
to further strengthening bulk billing incentives in general practice, which will see greater numbers of people saving money when visiting their GP.
“As people with neovascular AMD require frequent and ongoing eye injections, sometimes up to monthly, it is vital the government extends bulk billing to older Australians who require sight-saving injections,” she said.
People receiving eye injections for nAMD require, on average, six treatments per year, usually for the rest of their lives.
“However, access to public or bulk billed eye injection services is a postcode lottery as services are severely limited. The majority of people therefore have to seek treatment from private ophthalmologists,” Dr Chapman told Insight
glaring gap in its eye health system – the country has been functioning without a specially-trained paediatric ophthalmologist. Find out how Australasian ophthalmologists are lending their Pacific neighbour a hand.
page 63
IN THIS ISSUE
FEATURES
14
Our CEO recently spoke to us about the danger of nostalgia in business. The “this is how we’ve always done things” mindset that kills progress.
One of the privileges of trade media is the chance to bring attention to the more fringe topics and emerging innovations perched at the shores of the Australian
A new multifocal intraocular lens (IOL), an entirely new spectacle lens product category, and fascinating projects in the myopia space feature among new developments in this edition that will challenge how eyecare practitioners go about their clinical business. April is our annual myopia edition, and we’ve worked hard to go beyond the conventional to paint a picture of the future care model.
Workplace reform
Why KPIs, workforce oversupply and appointment times are atop the priority list for Optometry Australia.
39 New lens category
A look at why the demands of young presbyopes are not being met in today's optical market.
Take, for example, the topic on everyone’s lips right now, light-based myopia control therapy.
55 Record-setting affair
Momentum behind Optical Dispensers Australia continues after major conference success in Sydney.
Australian company Eyerising International has the country’s only approved treatment of this kind, repeated low level red-light (RLRL) therapy. And in a CPD article, some of Australasia’s biggest myopia authorities delve into the latest safety and efficacy data, while providing insights into how their own patients have performed. One of the authors, Melbourne’s Dr Philip Cheng, is even establishing a high myopia clinic –the first I’ve heard of – where RLRL will likely feature. RLRL forms part of another CPD article from QUT’s Dr Emily Woodman-Pieterse and Dr Rohan Hughes who explore the validity of other myopia control modalities like blue light optic nerve head stimulation, violet light glasses, and even classroom lighting.
As more safety and efficacy data emerges for long-term use of light therapies, will they replace current interventions, or act more as an adjunct?
Another interesting thing I learned this month was the use of ‘plano’ defocus myopia spectacles in non-myopes. This came in a conversation with NSW optometrist Dr Susan Ang as she detailed the experience of her eight-year-old son who, despite being +1.00 D, is wearing them as a preventative measure. This is based on a poster fellow Sydney optometrist Mr Oliver Woo presented at the 2024 International Myopia Conference.
Elsewhere, we explore the advent of a new lens category, spearheaded from HOYA. It focuses on the “early presbyope” – a potentially lucrative market for independents struggling to bridge the gap from single vision to progressive wear in patients.
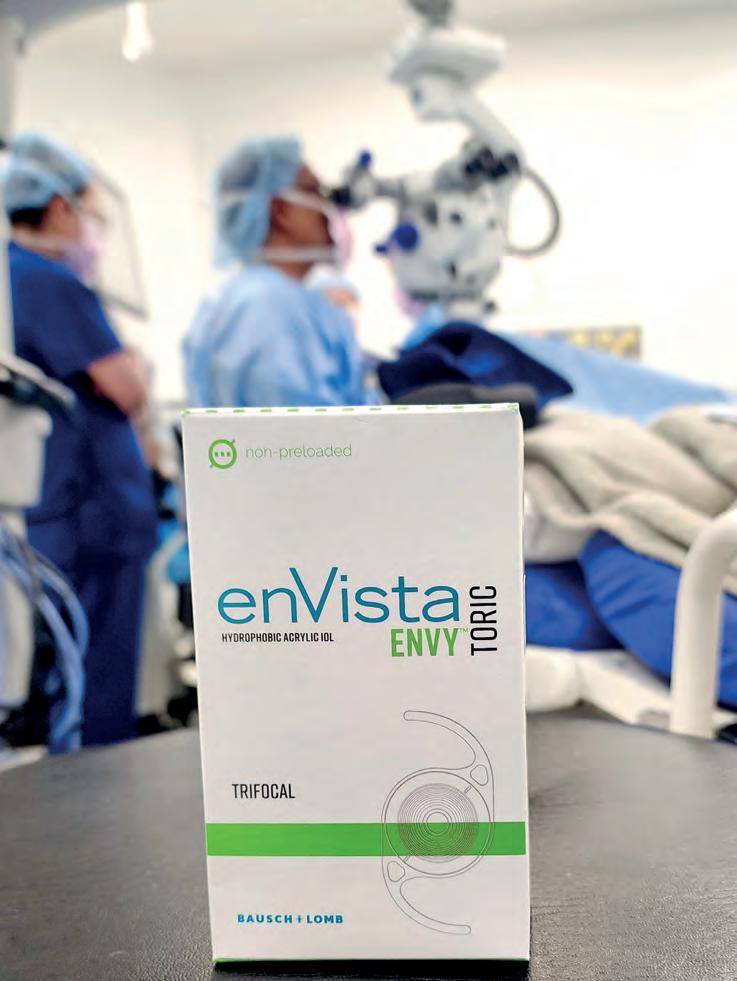
And for our ophthalmology readers cautious of diffractive trifocal IOLs, there are some good early signs from a new Bausch + Lomb lens that left Perth’s Dr Rob Paul pleasantly surprised.
Sometimes the smallest detail can alter your reality, and when you’re done with this edition, we have one request: continue to scrutinise the status quo.
MYLES HUME Editor
Just as Insight went to print, Ms KATRINA RONNE has been appointed CEO of the Australian Society of Ophthalmologists (ASO). She has served as the body's general manager of policy and strategy for much of the past decade, and has become the first female CEO in its 43-year history. "Time and again, [Katrina] has been responsible for developing policy and submissions to effectively communicate the ASO’s position on critical issues affecting Australian ophthalmologists and their patients,” outgoing CEO Mr
UPFRONT STAT
WEIRD
A routine cataract surgery in the UK turned into a bizarre discovery when doctors found a mass of contact lenses lodged under a woman’s right upper eyelid. According to the Royal Examiner, what initially appeared to be a single lens turned out to be a cluster of 17 lenses fused together by mucus. Upon further inspection, another 10 lenses were uncovered.
WONDERFUL
The Australian Society of Ophthalmologists has introduced its first vision-impaired board director, Mr Mark Grey from Tasmania. He was among three new appointees. President Dr Peter Sumich said each had strengths and expertise that would extend the “great work that has already been achieved or is under way”.
WACKY
Scientists have developed a teleoperated surgical robot that can perform complex eye procedures when mounted on a patient’s head, by passively compensating for natural head and eye movements. The approach enabled precise subretinal injections in an ex vivo eye sample mounted on a human volunteer, with higher success rates than previously reported with manual methods.
Kerry Gallagher AM said. IN OTHER NEWS, ophthalmologists can now prescribe the first and only bispecific antibody for macular oedema through the Pharmaceutical Benefits Scheme (PBS). From 1 March 2025, Vabysmo (faricimab), available as a 120 mg/mL solution vial, was listed for Australians with macular oedema secondary to retinal vein occlusion (RVO), where a blockage in a retinal vein leads to fluid build-up in the macula. The therapy can be administered at intervals of up to 16 weeks. The COMINO and BALATON Phase 3 studies showed Vabysmo delivered sustained visual
acuity gains comparable to aflibercept 2mg. FINALLY, EssilorLuxottica plans to produce 10 million units by the end of next year of its Ray-Ban Meta smart glasses as it looks to boost production capacity. That would be a significant jump on the more than two million units sold since their launch in September 2023. CEO Mr Francesco Milleri said the group was thinking about new releases with new features and new brands. “We look at this product like a shared platform ready to embark on third-party brands and new functions, also in the form of subscription services.”
The language of leadership
If you lead or manage people in your practice, 70% of your development in this area comes through experience, 20% is through social learning and 10% theory. Page 62.
WHAT'S ON
THIS MONTH APAO CONGRESS
3 – 6 April
The Asia-Pacific Academy of Ophthalmology Congress is taking place in New Delhi, India, with 18 invited speakers from Australia. 2025.apaophth.org/
Published by:
Complete calendar page 64 insightnews.com.au
NEXT MONTH OPTOMETRY VIRTUALLY CONNECTED
17 May
Optometry Australia’s one-day online event is returning, with up to 40 hours of CPD available. ovc.optometry.org.au
“Whilst there is currently no precedent for specialists to be bulk billed for delivering services, this unique problem demands a unique and unprecedented solution.”
MDFA said it had widespread support for its proposed practice incentive, the aim of which is to increase bulk billing rates “to support the most financially vulnerable Australians to keep having their sight-saving eye injections”.
RANZCO said it was supportive of MDFA’s work to support patients. Meanwhile, the Australian Society of Ophthalmologists said any incentive to increase bulk billing rates for nAMD treatment would be encouraged.
“The most applicable areas would be public hospital side clinics and remote practice,” ASO president Dr Peter Sumich said.
“Practice incentive payments to general practices usually come with many strings attached”, such as eligibility requirements, registrations, and ongoing compliance and audit, so he saw some challenges with a widespread roll-out in the private setting.
Half give up treatment after five years
According to MDFA, the total annual economic cost of vision loss in Australia is estimated to be $16.6 billion, or $29,000 per person with vision loss aged over 40. By targeting the most financially vulnerable people who need sight-saving treatment and encouraging more bulk billing, the organisation believes the incentive program would cost the government an
estimated $11.1 million a year.
Ultimately, it would save taxpayers $140 million annually in disability, aged care and other related health system costs. New research the organisation conducted with the University of New South Wales has revealed the median total cost for people living with macular disease who also receive eye injections is 12% ($3,621) of the annual government pension payment.
Close to 1,500 Australians with macular disease – Australia’s leading cause of blindness – completed MDFA’s survey, which also found that for almost one in 10 Australians who receive eye injections, the cost of living with their condition is more than $6,000 every year.
This is around 20% of the annual government pension payment.
These costs, which include eye specialist appointments, eye injection treatments and vision aids, were leaving pensioners with less money in their bank accounts for rent, bills, food and other essential life expenses, MDFA said.
If people with certain macular diseases cannot afford to receive eye injection treatments, they will lose their vision. As such, treatment persistence is said to be a significant problem, with approximately 50% of people discontinuing treatment within five years of starting eye injections. The main reason is cost burden.
MDFA’s research also showed the median total annual cost for people living in regional and remote areas is more than $400 higher per person compared with people in major cities ($2,658 vs $2,254).
“MORE THAN 72,000 PEOPLE HAVING EYE INJECTIONS HAVE NO CHOICE BUT TO PAY EXPENSIVE OUTOF-POCKET COSTS TO RECEIVE THEIR TREATMENT TO KEEP THEIR SIGHT.”
The highest cost was more than $1,700 more per year for people living remotely compared with people living in a metropolitan area ($8,911 vs $7,127).
Considering that most ophthalmologists work in metropolitan areas, access to treatment is reported to be a major challenge for people in regional and remote areas.
Dr Chapman said the findings highlighted a critical problem given MDFA research consistently identified cost and access as the two main reasons people delayed or stopped treatment.
“Eye injections are primarily delivered in private ophthalmology clinics in Australia, with only around 20% of them offering bulk billing, meaning that more than 72,000 people having eye injections have no choice but to pay expensive out-of-pocket costs to receive their treatment to keep their sight,” she said.
“Our research underscores the immense financial pressure that these high costs would have on people living with macular disease who rely on their pension payments to get by.
"Even when the country is not in a cost-of-living crisis, accessing affordable or bulk-billed treatment is an insurmountable problem for too many low-income earners, pensioners, and self-funded retirees.”
There are an estimated 1.9 million people in Australia with some form of macular disease. In 2023, more than 108,000 people with a treatable macular disease, including nAMD, diabetic macular oedema, and retinal vein occlusion, received an eye injection treatment.
SALARIES HAVE STAGNATED AND REDUCED, OA SAYS
continued from page 3
of Western Australia has the newest course, launched in 2021, with all 40 students in the inaugural 2024 graduate cohort securing work, and 90% staying on to work in WA.
OA’s own workforce supply study, to be completed soon, will provide an understanding of short- and medium-term supply and demand, drawing on known data and trend analysis.
“It will also consider the supply-need balance, looking at areas of identified unmet eyecare needs and opportunities for these to be addressed.”
In its submission to the OSL, OA said it had raised concerns about a significant
imbalance between optometry workforce supply and demand, while acknowledging the complex reality of workforce maldistribution.
“We note many available roles are filled through internal recruitment rather than public job postings, and the positions that are advertised often remain open for long periods due to geographic location challenges rather than a true shortage of optometrists,” OA stated.
The number of optometrists in Australia has grown to 7,150. Image: Inside Creative House/ Shutterstock.com.
“Furthermore, we comment that the data tells a clear story: with an increase in the number of optometry schools in recent years, the number of registered optometrists in Australia has increased significantly, with a steady rise from 5,399 in 2017 to 6,977 in 2023.”
That number is now 7,150, official data shows.
OA stated the optometry workforce per capita is now higher than many comparable countries, with particularly high concentrations in metropolitan and larger regional areas.
“Concern regarding a looming oversupply is being felt across the profession, with new evidence of concerning workplace conditions and reports from members indicating increasing job competition, fewer permanent full-time opportunities, and a stagnation or decline in salaries,” the organisation said.
“This is particularly evident for early-career optometrists, who are struggling to secure stable employment pathways.”
DR KATHY CHAPMAN MDFA
Image: MDFA.
EYE RESEARCH PROJECTS SECURE $8M IN 2025 NHMRC
Four eye research projects have secured more than $8 million in funding in the 2025 National Health and Medical Research Council (NHMRC) Investigator Grants scheme, with two of those featuring in the top tier with more than $3 million allocated each.
Professor Robyn Guymer, Professor Marcello Rosa, Associate Professor Lisa Zhuoting Zhu and Dr Alexis Britten-Jones – all based at Melbourne institutions – will receive the grants for their eye-related studies.
With the Federal Government providing $422 million for 229 “high-performing researchers” in this year’s round, the ophthalmic projects collectively account for $8.34 million.
Prof Guymer, deputy director and head of macular research at the Centre for Eye Research Australia (CERA), and Monash University’s Prof Rosa will each receive $3,014,025 for their work, the second-equal highest grant split across 32 projects.
Prof Guymer will use her funding to explore causes and cures in age-related macular degeneration (AMD), with a major focus on early intervention.
“This research aims to identify new
causative pathways leading to AMD as well as conduct two novel early interventions trials to prevent vision loss,” she said.
“This research will provide evidence for more feasible ways to conduct early intervention studies. ”
Prof Rosa, who heads up the Rosa Laboratory within the Monash Biomedicine Discovery Institute, will use her funding for a project entitled: ‘Pathways to vision following lesions of the primary visual cortex’.
She will explore how visual information can be channelled to non-damaged parts of the brain, in search of ways to restore vision following damage to an area called the primary visual cortex (V1).
“Vision depends not only on the eyes, but also on many brain areas. Without the latter the visual information cannot be decoded, and the person becomes blind even if the eyes are spared,” her application stated.
“For example, when V1 is damaged by stroke or trauma, a type of profound blindness ensues, for which there is no treatment.”
CERA had a second NHMRC recipient in A/ Prof Zhuoting Zhu will use $1,623,700 for a retinal-based test for cardiovascular disease
(CVD). With the eyes offering a window into vascular health, her research aims to exploit an AI model based on eye images “to provide precise and personalised management of CVD, ultimately reducing the risk of death and disability from this life-threatening condition”.
Meanwhile, Dr Alexis Britten-Jones, a clinician-researcher within the University of Melbourne’s Department of Optometry and Vision Sciences, will use her $688,405 grant to “advance ocular genomics to propel breakthrough treatments for blindness”. She will focus on inherited retinal diseases (IRD).
Among the 2025 grant recipients were A/ Prof Lisa Zhuoting Zhu (top left), Dr Alexis Britten-Jones (bottom left) and Prof Robyn Guymer (right). Images: CERA.
IN BRIEF
CATARACT IMPACT
A fresh study out of the UK has detailed the carbon footprint of single-use cataract surgical items versus reusable equivalents. The collaboration between University Hospital of Wales and Oxford’s Centre for Sustainable Healthcare evaluated the carbon impact in two ways: by “streamlining” the use of single-use packs, and transitioning from single-use items to reusable equivalents in cataract surgery. By streamlining they were able to achieve a carbon saving of 935 kgCO2e/year. Meanwhile, switching to reusables created a 309 kgCO2e/year saving. But a net carbon saving was achieved from 19 or more re-uses of the reusable items compared to single-use equivalents. Tellingly, they found “single-use items had a 27 times greater carbon footprint than reusable equivalents (322 kgCO2 vs. 12 kgCO2e respectively)”.
MEDICARE CHANGES
Several Medicare changes came into effect on 1 March 2025. They include changes to comprehensive consultations where items 10912 and 10913 combine into one, while 10913 and the previous ‘same practice’ restrictions have been removed. With visual fields, a third computerised perimetry test in a 12-month period where indicated by the presence of glaucoma with a high risk of clinically significant progression has been introduced. For optometrists conducting domiciliary visits, items 10931 to 10933 were replaced with a single item number, 10931. The scheduled fee is $43.75 and the co-claiming restrictions on domiciliary visits is now removed, enabling the billing of a short consultation (10916 or 10918) and computerised perimetry (10940 or 10941) at domiciliary visits. Also, contact lenses items 10921, 10922, 10923 and 10925 are combined into one item number, 10921, and the explanatory notes reworded to remove the requirement to deliver the lens. Other changes also came into effect for foreign body removal and residual vision (10942).
ESSILORLUX FINANCIALS
HEALTHSCOPE AND AHSA RESOLUTION REACHED
The Australian Health Service Alliance (AHSA) has reached an in-principle agreement with Healthscope, ensuring members of AHSA’s not-for-profit funds can continue to access care at Healthscope hospitals without additional out-of-pocket expenses.
Late in 2024 Healthscope, which lists 44 ophthalmologists working within its 38 hospitals, announced plans to charge members of several health funds a “hospital facility fee” of $50 for same-day services and $100 for overnight services, including those involving ophthalmology procedures.
After a backlash from the health funds involved, the situation escalated with Healthscope saying it would exercise its termination rights and provided 90 days’ notice as required under the contracts.
The Australian Medical Association stepped in, urging Healthscope, Bupa and AHSA to immediately resolve their respective funding disputes for the sake of patients.
In a media release, AHSA CEO Mr Andrew Sando said: “Our priority has always been to provide funds’ members access to high-quality, affordable private healthcare.
“This outcome safeguards their best interests while also supporting the continued delivery of safe, high-quality care.
“We know this has been a concerning time for many, however this agreement ensures uninterrupted access to private hospital care,” said Sando.
With this new agreement in place, AHSA’s 2.5 million members can access the full range of services available at Healthscope’s facilities, knowing they will not incur additional hospital charges, the release said.
“Over the past 12 months, we have strengthened our partnerships by signing new agreements with a number of leading private hospital operators across the country.”
“I look forward to continuing our partnership with Healthscope, and all private hospital providers, to ensure the best possible care for Australians and their families,” said Sando.
A STEP CLOSER TO ‘ADVANCED PRACTICE RECOGNITION’
Asia-Pacific saw the biggest growth in Q4 as EssilorLuxottica reported a 9.4% rise in global operating profit to €4.4 billion (AU$7.3 billion) in 2024. That was on the back of a 9.2% rise in revenue in the fourth quarter, bringing the total revenue for the year to €26.5 billion (AU$43.8 billion). In Asia-Pacific, which includes OPSM, Laubman & Pank and the Professional Services business in Australia, that revenue rose 14.1% to €864 million (AU$1.43 billion) in the fourth quarter, and 7% over the full year, at €3.2 billion (AU$5.29 billion). “We celebrate another year of remarkable achievements, ” said Mr Francesco Milleri, chairman and CEO, and Mr Paul du Saillant, deputy CEO.
Optometry Australia (OA) has completed the pilot phase for its Advanced Practice Recognition (APR) Program and is preparing to launch its course application process.
OA introduced the program in July 2024 as an initiative to support optometrists to achieve formal credentials for their advanced expertise in specific clinical areas, starting with glaucoma management.
At the time it said the program was a “win-win for optometrists, healthcare partners, and the community”.
It would play a “pivotal role in addressing gaps in advanced eyecare, improving access for patients, and streamlining co-management pathways with ophthalmologists and other professionals”.
The pilot brought together optometrists carefully recruited to represent a range of locations, career stages and
IN OPTOMETRY
practice types, to test and refine the APR framework.
“Their feedback and experiences have been invaluable, allowing us to fine-tune the program for its official launch, and we are very grateful for their support,” OA said.
“Incorporating insights from the pilot and working closely with the governance committee and other stakeholders to understand its outcomes, we are currently preparing to open applications for the first public intake round of the APR program.”
CEO Ms Skye Cappuccio said: “We recognised the incredible skills and qualifications of practitioners within the optometry workforce and saw a unique opportunity to support those work in advanced ways."
Applications will launch in the coming months, with a cap of 20 participants.
National Capital Private Hospital in Canberra is among the 38 hospitals affected. Image: Healthscope.
The program has begun with glaucoma expertise. Image: rh2010/stock. adobe.com.
DO AUTOMATED INSULIN DELIVERY SYSTEMS WORSEN DR?
Amid concerns that automated insulin delivery (AID) systems can worsen diabetic retinopathy, an Australasian study has demonstrated most people with type 1 diabetes can achieve stable or i mproved disease in the short term.
A continuous glucose monitor (pictured) is a crucial part of the AID system. Image: Halfpoint/Shutterstock. com.
The University of Otago-led study set out to investigate the impact AID systems – a relatively new technology allowing rapid improvements in glucose control – after concerns it may lead to early worsening of diabetic retinopathy, or progression during the first year.
Professor Ben Wheeler and Dr Francesc March led the work, which also involved Dr Mary Abraham from Western Australia’s The Kids Research Institute and Perth Children’s Hospital.
“We looked at the short-term effects of diabetic retinopathy in people aged 13 and older with type 1 diabetes after using automated insulin delivery systems for more than six months,” Dr March said.
“We included 165 people and we demonstrated that most participants, 79%, saw improvements or no change in their diabetic retinopathy, with younger age being a protective factor.”
AID systems help to keep blood glucose levels within a target range.
Dr March and his team conducted a retrospective, four centre observational study. Improvements in grading were seen in 32/165 (19%) of participants, 99/165 (60%) were considered stable, and 34/165 (21%) worsened.
The researchers said the study “helps to demonstrate the general safety of AID, as the vast majority of participants showed improvement, stability, or minimal worsening of diabetic retinopathy (to no more than minimal/mild disease) in the months following AID initiation”. The benefits of improving glycemia “far outweigh the risk” of short-term diabetic retinopathy deterioration. This is because it is rare and can be successfully managed.
SURGEONS IN PUBLIC SECTOR SEEING MORE COMPLEX CATARACT CASES
The largest study of contemporary phacoemulsification cataract surgery outcomes in Australia has highlighted concerns that surgeons in a public setting are increasingly seeing more complex cases from lower-socioeconomic patients.
And the researchers believe government policymakers and hospital administrators need to consider this when creating health policy to fund existing services and increasing service provision in the future.
The major review of cataract surgery from 5,018 consecutive cases at Sydney’s Westmead Hospital between May 2017 and August 2020, found just under half of the patients treated were “more complex cases with a higher burden of co-existing ocular pathology”.
At 48.9%, “this is one of the highest rates reported when compared to equivalent Western nations: significantly more than the UK Royal College of Ophthalmologists National Ophthalmic Database (36.9%), the Swedish National Cataract Registry (33%) or the American Academy’s Intelligent Research in Sight registry (35.4%)”.
The researchers, Dr Muhammad A Khan, Dr Brendon W H Lee, Dr Lauren Sartor, and Dr Chameen Samarawickrama, said the shift highlighted the “heterogenicity of cataract surgery cohorts based on location”.
It’s the largest study to date on contemporary phacoemulsification cataract surgery outcomes in Australia. Image: Dusko/stock.adobe.com.
“Our institution services approximately 1.2 million Australians, with a high referral rate from lower socioeconomic areas where patients tend to have multiple comorbidities, present late in the disease process, and have significant pathology at presentation.
“This is compounded by the significantly longer median waiting time for cataract surgery at our institution’s health district compared with national waiting times (330 days vs 98 days in 2019, respectively), which have further been exacerbated secondary to COVID-19 lockdowns, restrictions in elective surgery, the resultant backlog of cases.”
The researchers set out review the Australian and New Zealand cataract literature to provide a benchmark of outcomes from the region.
ASO WELCOMES NEW YEAR WITH INCOMING BOARD APPOINTMENTS
Mark Grey (left), Dr Tricia Drew and Dr Rahul Chakrabarti have been appointed to the board of directors at the ASO. Image: ASO.
The Australian Society of Ophthalmologists (ASO) has begun the new year with three incoming appointments to its board of directors.
Victorian ophthalmologists Dr Rahul Chakrabarti and Dr Tricia Drew will join Mr Mark Grey from Tasmania in a move to “further strengthen and develop the ASO’s
advocacy and efficiency”, the ASO said. Grey’s appointment is also historical, as the first vision-impaired representative to be appointed to the ASO board.
ASO president Dr Peter Sumich said each of the incoming directors had strengths and areas of expertise that would extend the “great work that had already been achieved or is underway at the ASO”.
“We have been in a period of peacekeeping for some time but are seeing this shift as various issues across Australian healthcare are reaching a crisis point,” he said.
“With advocacy playing an essential role as we tackle the new year and the challenges that undoubtedly lie ahead, the ASO is pleased to announce these appointments and share that our voice — the voice of Australian ophthalmologists and their patients — is growing stronger.”
Start your career with the local experts in eyecare
At EyeQ, we offer support to maximise your potential
Whether you’re a recent graduate or experienced optometrist, aspiring optical dispenser or have a few years in the optical industry, at EyeQ, we believe in providing our people with the best personalised support to maximise their potential.
Opportunities exist right across Australia both in metro and regional locations.
Start your career in a well-established practice with state of the art equipment, modern fitouts and a great team of people around you to support you through your journey.
Is a redesign of the optometry workplace needed?
KPIs, workforce oversupply and appointment times are atop the priority list for Optometry Australia, as a study it commissioned calls for urgent reform so optometrists can look forward to a stronger, more sustainable future.
In February, two pieces of news, just two days apart, provided some sobering insights into the working lives of optometrists in Australia.
The first was released on 12 February from the Australian Health Practitioner Regulation Agency (Ahpra). The regulator had fresh data showing that although the majority of optometrists want to stay in their profession, more than one in 10 were unsure about their future or have plans to leave the workforce, some within a year.
Although the study didn’t have specific reasons for optometry, the second announcement on 14 February provided some clues.
It was from an Optometry Australia (OA)-backed survey into the professional lives of 505 optometrists across Australia. That study itself found 7% of respondents were considering leaving the profession within the next year.
Concerns with workforce oversupply, the “squeezing in” of follow up appointments and “moral distress” caused by KPIs and other pressures were some of the big issues highlighted in the report, entitled: ‘Working conditions of employed optometrists: A workforce survey’.
Led by Flinders University’s Professor Nicola Anstice, initial findings from the report reveal that despite optometrists consistently delivering high-quality, evidence-based patient care, “significant workplace reform is urgently needed”.
"The Flinders University workforce survey confirmed reports from members about workplace standards and systems," OA CEO Ms Skye Cappuccio tells Insight
"It makes clear that many optometrists experience high job demands and insufficient job resources, leading to strain, dissatisfaction and moral distress. It appears there is not one individual element of workplace conditions causing this, but multiple, including work overload, fear of job loss, lack of autonomy and financially driven KPIs. There is a clear need to re-design workplace systems to ensure optometrists can practice with clinical autonomy and realise rewarding and sustainable careers."
Time allocation for appointments is a central issue in the report.
While the median appointment time for initial consultations was 30 minutes, and 20 minutes for follow up, it found 4% of optometrists were “not allocated any time for follow up appointments”, with these patients “squeezed in between other patients”.
The data contrasts with the situation several years ago in 2006, when
Horton et al. reported average consultation times for a first patient visit of 45 minutes, 15 minutes for a subsequent patient visit, and 60 minutes for a contact lens consultation.
“While most optometrists (57%) reported they see 60 patients or less per week (approximately 12 patients per day), 11% reported having >90 eye examinations booked per week,” the report stated. “Most optometrists noted that there was no specific time allocated for administrative tasks with a median administrative (clinical support time) allowance of 0 minutes per week.”
The survey notes some macro trends influencing optometry workforce conditions during the past 15 years.
They include the four new optometry programs, increased net migration to Australia, and reduction of Medicare subsidised comprehensive eye examinations from two-yearly to three-yearly.
Plus, a 2019 survey on the mental health and wellbeing of practising optometrists, led by Professor Sharon Bentley from QUT at the time, found approximately one in three experienced moderate to severe psychological distress, depression and anxiety.
The most common work-related issues identified were workload, retail pressures and career dissatisfaction.
More recently, an analysis of publicly available registration data found a significant number of early career optometrists are leaving the profession.
In the Flinders workforce survey, 23% of optometrists agreed or strongly agreed they had satisfactory career options and professional growth, 25% were satisfied with their current income, and 34% felt professionally isolated.
An ‘additional comments’ section showed concerns such as job losses due to the increasing number of optometry graduates, the pressure of financially driven key performance indicators (KPIs), lack of clinical autonomy, and work overload.
Salary stagnation was another concern. While not stated in the report, an Insight analysis of the latest Australian Taxation Office data shows the average taxable income of optometrists was $102,773 in 2021-22 – around $4,000 (3.7%) less than the year before.
One survey respondent said that, over time, they've worked hard to stay current, learning to interpret and apply new technologies in clinical practice, which has expanded their scope of responsibilities. Despite this, they
Optometry Australia says there is new evidence of concerning workplace conditions.
haven't been "appropriately compensated for these advancements, unlike other professions".
"In fact, my income has decreased, partly due to the oversupply of optometrists, leaving me in a position where I am effectively doing more for less."
Meanwhile, KPIs were highlighted as an example contributing to “optometrists experiencing significant moral distress”.
According to the report, this occurs when a healthcare professional knows the correct course of action but is unable to pursue this due to institutional or organisational constraints.
As an example, an optometrist highlighted a case where regional management directed them to turn away red eyes or similar appointments.
The optometrist said they explained this was against an optometrist’s duty of care, if they have time to see them.
"Optometrists feel they have limited autonomy and insufficient job control, are unable to develop themselves professionally, and are not provided with appropriate renumeration nor constructive feedback that is aligned with their role as a primary eye health care provider," the report noted.
"Most optometrists report that the only feedback they receive is on their ability to meet financially driven KPIs and many find this causes significant role conflict as a health care professional."
OPTOMETRY AUSTRALIA UPDATES POSITION STATEMENT
In response to these preliminary findings, on 14 February 2025, OA released an updated Position Statement on Workplace Conditions for Clinical Optometrists.
workplace standards and systems. We continue to call for prompt and meaningful action in this space."
Flinders University has been commencing the second phase of its study by hosting additional focus group discussions to explore how job demands and resources influence job satisfaction in optometry and to identify factors that foster positive working environments.
It has also shared the results and updated position statement with Ahpra and several of the nation’s largest optometry employers, asking for their support for immediate change.
"Encouragingly many of these stakeholders have been open to discussing
“While we celebrate the essential contributions optometrists make to the lives of their patients, the goal of this workforce survey is to unite the industry, tackle the challenges, and create a stronger, more sustainable future for all optometrists,” OA said.
Financial KPIs were highlighted as a pressure impacting workplace conditions.
Image: Svitlana Hulko/Shutterstock.
Myopia – sink or swim?
Myopia is surging around the world, with more younger patients at the head of the large wave now breaking against Australia’s ophthalmic sector. Insight assistant editor ROB MITCHELL looks at what the nation’s eyecare professionals are doing to push back the tide.
In 2020, as Australia and the rest of the world faced the global crisis of COVID-19 and its many consequences, another equally devastating health condition was building quietly but rapidly from what some described as an “emerging health issue” into what is now considered an epidemic.
The numbers and predictions are confronting.
The Child Myopia Working Group, a collaboration of leading optometrists and ophthalmologists from Australia and New Zealand established in 2018, estimated a current prevalence of 36% for the region. By 2050, this is forecast to rise to 55%.
Further, Australia is expected to have 4.1 million high myopes and New Zealand over 600,000 high myopes by that time, unless myopia management is implemented by everyone. This pales in comparison to the 2020 numbers that sat at around 1.1 million and 200,000 high myopes, respectively.
Given those numbers, it is probably no surprise that myopia is tipped to become the leading cause of avoidable blindness around the world, and younger children are increasingly at the crest of that dark, rising swell.
A recent study in the British Journal of Ophthalmology (BJO) found that short-sightedness had tripled in children between 1990 and 2023, with the rise “particularly notable” after the COVID pandemic, as nervous families struggled to break free of the perceived safety of isolation and indoor activity.
That meant vulnerable young eyes were more focused on small screens, rather than the vital eye exercise obtained in outdoor play and interaction.
That BJO research is backed up Down Under, where the Australian College of Optometry (ACO) says myopia is affecting more Australian children than ever before, and they are presenting at increasingly younger ages.
“In less than 20 years, the typical onset age has fallen from 11 years of age to 8 years – a shift that has significant implications for long-term vision and overall eye health,” the ACO says.
Those issues with younger eyes are growing into significant problems for the economy.
Australia’s Brien Holden Vision Institute, quoting a study in the scientific journal Ophthalmology, said impairment caused by uncorrected myopia cost the global economy an estimated US$244 billion in lost productivity in 2015, a figure supported by the BJO’s own reporting.
That means when an eyecare professional has a young patient in front of them, they are not only considering how to remedy that child’s faltering
“I tell the parents, you don't see very many surfers who are short-sighted; you don't see kids doing outdoor sports who are short-sighted.”
Dr Trent Sandercoe Norwest Eye Clinic
vision, they are also weighing treatments that will impact on not only their academic performance but also that person’s contribution to the community
But just as the Australasian Child Myopia Working Group was set up to meet that building swell, other professionals and organisations are also reacting to help their colleagues and young patients swim rather than sink.
PLENTY OF TOOLS IN THE TOOL BELT
Myopia may have surged around the world but so have the tools and resources to combat that rise.
Myopia Profile began nine years ago as a single piece of paper put together by Brisbane optometrist Dr Kate Gifford, a collection of notes from her lectures about the eye disease.
Now it is one of the world’s premier sources of support and assistance for eyecare professionals, practices and parents. Its emailing list runs into the tens of thousands and last year there were 26 million interactions with its web-based platforms.
That’s jumped 700% in the past couple of years, matching the rise of myopia and the angst that follows in its wake, says Ms Jeanne Saw, manager of professional affairs and relationships.
She says eyecare professionals will find plenty of educational content on MyopiaProfile.com and in its Knowledge Centre section, including articles, and clinical and science summaries. Parents too can find valuable, evidence-based information.
“We have developed our ‘Made Simple’ courses to address the growing need for quick and simple breakdowns of key myopia topics for busy
Image: Trent Sandercoe.
The global tsunami that is myopia is having an impact on Australian shores as well.
practitioners. So there's myopia management, orthok made simple, atropine made simple courses for example,” says Saw.
“They are topics that you really need, to become confident in prescribing for myopia management.”
Like so many others, Myopia Profile has had to adapt to not only the tsunami of cases in Australia and around the world but also the increasingly younger patients carried along with it.
“A lot of the time when a really young child comes in and they're myopic, optometrists can feel quite overwhelmed by that, because of the eye health concerns but also because it begs the question of co-management with ophthalmologists,” says Saw.
“Do we need to get an ophthalmologist involved? What are the things that we should look out for when a young child comes in with myopia, because there's also things that you have to consider, like syndromic myopia as well.”
Professionals need to consider the parents too.
Which is why Myopia Profile has also developed mykidsvision.org, a public-facing website driven specifically by questions from nervous, worried parents.
“We found that a lot of parents were starting to become more cognisant of myopia and wanting to ensure the eye health of their children as they grow up,” she says.
Those questions tend to revolve around the symptoms of myopia, when parents should bring their child in for an eye test, and treatments.
Parents are also keen to know more about how much time children should spend outdoors to help halt the progression of the eye disease, and also about screen time.
Saw says this information “empowers” the parents and helps make potentially awkward conversations about behavioural change a little easier.
“The best way to approach it would probably be to start with questions like, How old are your children? How much time do they spend on their devices? Have they had an eye test yet? How much time do they spend outdoors?
“Those are all very important questions to ask, even if it's just the adult in the consult room and not the child or their children – asking questions definitely starts the conversation.”
And encouraging children to spend more time outdoors and less on small
screens are among the easiest of interventions, she says.
“Even if there is a low risk of myopia, it's a good idea to provide that advice to both parents and patients, because not only does it give the best chance of a child not becoming myopic, but there are other benefits to it as well.”
Raising awareness is vital for professionals too.
“A lot of times, some optometrists think that atropine is the best intervention to use,” says Saw, “but of course, you also need an optical, single-vision lens to correct the vision.
“So for me, optical treatments provide correction of myopia, but also control of myopia, and I think that's a really important point for practitioners.”
Like Myopia Profile, the Australian College of Optometry (ACO) has also had to adapt and put together new resources to help the ophthalmic sector come to grips with myopia and its increasingly younger cohort.
That includes its 2025 Advanced Certificate in Children’s Vision (ACCV) course, which equips optometrists with “the skills to confidently diagnose and manage many paediatric conditions”, including myopia.
Ms Catherine Tay, clinical education co-ordinator of the course, says it has been designed with working professionals in mind and combines evidence-based learning with practical experience.
“Keeping up with the latest research and techniques is becoming increasingly essential in modern practice, particularly when managing the diverse and complex needs of young patients,” she says.
The ACO is also offering a new short course - Myopia Management in Clinical Practice – five weeks of intensive online study, scheduled to launch in early October 2025.
It is designed with clinical optometrists in mind, with a practical evidence-based perspective, but it also delves into emerging research and technology. The course comprises four modules covering topics ranging from emmetropization, risk factors for myopia progression and pathological considerations, to effective communication, treatment strategies and treatment alteration.
RAISING AWARENESS OF A RISING PROBLEM
Dr Joe Paul, head of professional services at Specsavers, would love to see an eye test considered as routine for a child as a visit to the dentist.
Dr Trent Sandercoe works with one of the many young patients ophthalmologists are increasingly seeing in their practices.
Image:
Trent Sandercoe.
“We found that a lot of parents were starting to become more cognisant of myopia and wanting to ensure the eye health of their children as they grow up.”
Jeanne
Saw Myopia Profile
“There's still a lack of understanding among people in Australia, of the importance of having an eye check for young kids,” he says. “We're not there yet as optometrists, but it should be part of just regular health checks.”
In the meantime, in part because of the rise of myopia but also to bridge that gap and build awareness of eye health, Specsavers often sends its optometrists out into the community.
“A number of our optometrists do school screenings to help diagnose myopia,” he says.
“They are talking to local communities and using those links to make sure that we're spreading awareness outside of the test room, doing everything we can to encourage good visual habits and outdoor time.”
He says the numbers inside the test room are proof that the global concerns about myopia are justified and such initiatives are needed.
A Specsavers 2022 retrospective review of more than three million de-identified patient records aged 18 and under showed child myopia detection rates had increased to 28.8% in Australia and remained as high as
29.8% in New Zealand. This review also found that the age at which patients were being diagnosed with myopia was decreasing.
In the UK, he notes studies have found similar results and show that the typical onset of myopia occurs in children aged between six and nine, and its progression is most rapid under 10 years of age.
“Now, more than a third of our kids in some of our stores are myopic, and it's getting bigger.
“In 2016 the average kid was -1.00 D when we first picked them up; it's close to -2.00 D in their worst eye now.”
In the face of such challenging numbers, Specsavers is also building knowledge and awareness of myopia within its practices.
“A few years back we started developing some kits and guides for all our stores to borrow, and we work very closely with suppliers and other groups to develop educational content and meeting webinars.
“It's been part of our grad program as well.”
The content covers myopia diagnosis and management, but also how to approach younger patients and their parents.
“It is around comfort and confidence,” says Dr Paul. “The optometrists learn the general skills they need in university to be confident, but they don’t get a lot of exposure to young kids in clinic in university.
“We have some tips and tricks, ways to quickly build confidence and help them feel comfortable doing the job they all know how to do.”
That’s important because he feels optometrists need to talk about therapies as well as lifestyle change.
“Perhaps years ago, optometrists wouldn't have been comfortable suggesting behavioural changes, but I think times have changed.
“We've got good evidence now,” he says. “There are studies coming out that show that time outdoors can in fact help prevent progression.
“We've known about near-work for a long time, and we know screens are
Image: Jeanne Saw.
not what we should be spending a lot of time on. So it's about having that conversation with the parents, informing them of the risks and, wherever possible, just working with parents or with the kids.”
Sydney independent optometrist Dr Susan Ang says a notable trend among her colleagues is the number of pre-myopes they’re now picking up.
A common example is a four-year old with 6/6 vision, who should ideally be around +1.50 D. To become emmetropic, they would need to maintain this “hyperopic reserve” until eight years old.
“If you’re a +0.50 and you're six years old, you're already considered a myope, a pre-myope.”
Her own eight-year-old son sits at +1.00 D, but after he shifted a diopter in six months despite “carefully engineering him”, she placed him in a pair of plano Stellest myopia control lenses as a preventative measure while reading and in the classroom.
“But it's hard to get a parent to spend $900 to $1000 to try to prevent their kids from becoming myopic when they see perfectly clear. I have that benefit of being able to easily access these products and scan him every three months and seeing where it goes.”
Having more sensitive tools for axial length measurement has been a key factor in picking up kids earlier.
Eyecare professionals need to be mindful of that, even if a young patient appears to have good vision. The key is to test, to test early and to try to obtain some idea of the child’s axial length.
“We know that if they're more than 23.07mm at six years old, then they're at risk of myopia,” she says. “But even asking parents to have no handheld technology till four years old has been a challenge.”
PARENTS MORE AWARE OF MYOPIA
Dr Trent Sandercoe says the ophthalmic sector is working quickly to adapt to the rise of myopia, the earlier onset of the condition, and the new
therapies to combat it. “In the past, we just went ‘you’re myopic’, gave you a pair of glasses and sent you on your way,” says the paediatric and general ophthalmologist working out of Western Sydney.
But that has changed considerably with a greater understanding of what's going on with myopia and the greater number of young patients bursting through the doors of practices around the country.
Dr Sandercoe says that’s because parents are more aware of it and keen to get their children checked and then treated, and more children are being picked up in various screening programs, especially in New South Wales.
“Those predisposed are presenting earlier, and we're getting kids that may not necessarily have been myopic in the past but are now presenting with it,” he says.
“So there’s definitely more than what I saw when I first started my ophthalmology training.”
He finds most of his young patients, and particularly those aged over nine, reasonably easy to deal with.
The key, says Dr Sandercoe, is to get a good subjective refraction for those aged over nine or cycloplegic refraction for those under nine in that first consultation.
That can be a challenge but is especially important if the child has ADHD, developmental delay or is on the autistic spectrum. But it is vital to get a good baseline.
“Number two is getting a good axial length, because it's what’s driving what's going on.”
On top that he likes to look at the keratometry to make sure he’s not missing something like keratoconus.
“And then I always make sure there's no red flags.”
He believes very young children presenting with high myopia need to see an ophthalmologist or paediatrician to make sure they don’t have an underlying issue, like Sticklers syndrome or retinal dystrophy.
If there is a hint of myopia, parents can be “very motivated” to go down the pathway of treatment.
“My approach is, I'll see them every six months,” says Dr Sandercoe. “And I want to demonstrate that there's axial length growth. And if there is then you start treating it, and that needs to be in my threshold, somewhere between 0.2 and 0.3 millimetres in a year.”
Six months is also a good amount of time to see if any treatment is working.
Often, with children so early in their potential myopia journey, that treatment involves a healthy dose of common sense.
“The strategies tend to involve simple things like walking to and from school,” he says.
“That gets you 20-30 minutes of daylight exposure.
“There’s getting a weekend outdoor sport, which is doing many things at once – you are increasing their socialisation, they're getting exercise and they're getting outdoor daylight exposure.
“I tell the parents, you don't see very many surfers who are short-sighted; you don't see kids doing outdoor sports who are short-sighted.”
Other treatments can include atropine drops, but not all children are happy to take them, even at a low dose.
“I'm a big fan of the peripheral defocusing lenses, because they're doing something when the child is doing nothing else is, and they don't require much compliance to get you wearing glasses.”
Dr Sandercoe is not such a big fan of the orthok that others advocate, “because I've seen what happens when people get nasty infections with them”.
But all of the eyecare professionals readily agree on one thing: In the face of this epidemic, doing nothing is not an option.
As Dr Paul puts it: “The outcome if we don't do anything to change this is a huge expense to the medical system and a lot more potentially avoidable blindness of people in Australia.”
A staff member from Specsavers’ Port Lincoln, South Australia, store tests a young child during a school screening for myopia.
Image: Mikaela Frick Photography.
This medicinal product is subject to additional monitoring in Australia. This will allow quick identification of new safety information. Healthcare professionals are asked to report any suspected adverse events at https://www.tga.gov.au/reporting-problems.
Shifting the myopia mindset
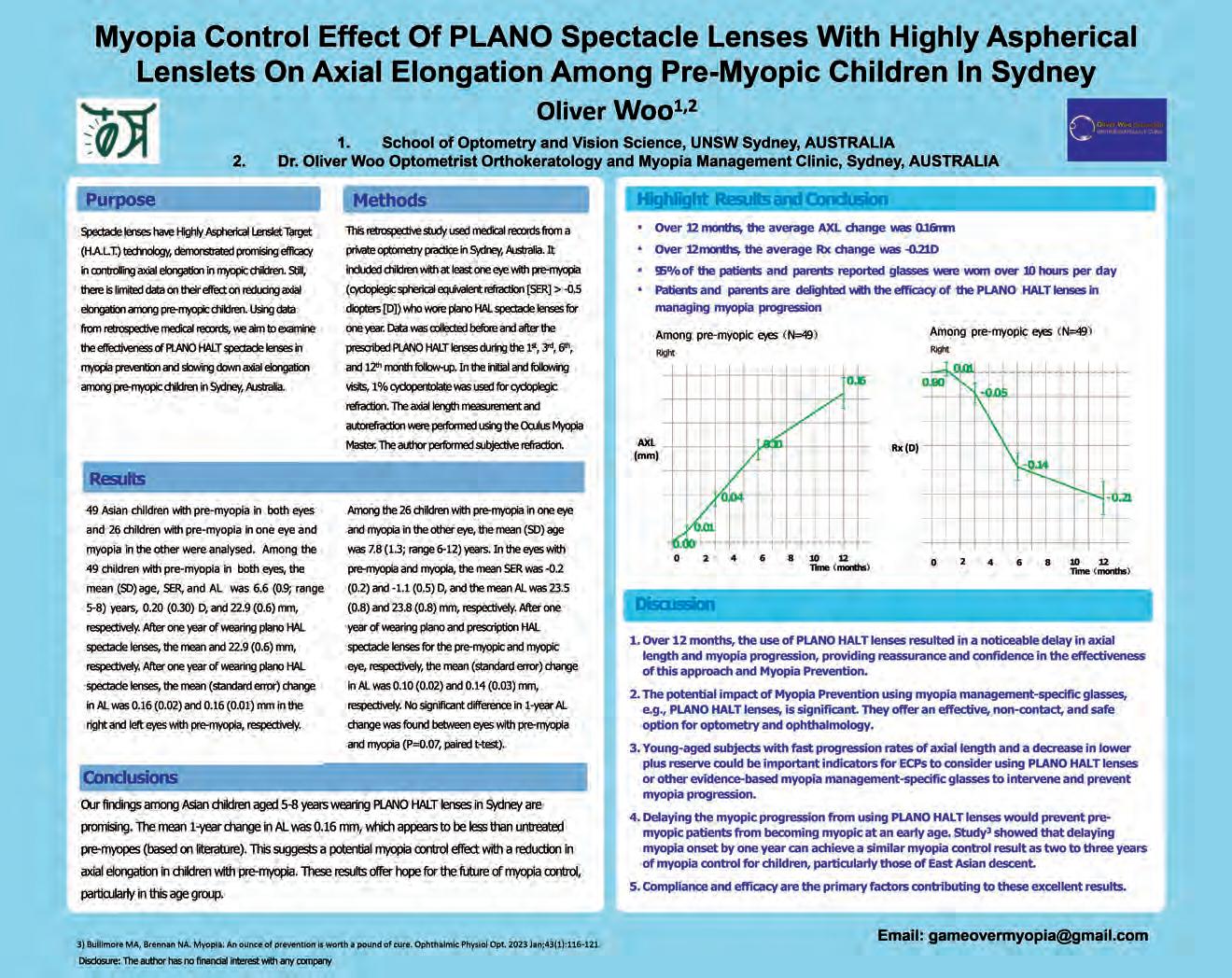
Sydney optometrist Dr OLIVER WOO explains why colleagues need to be on the look out for pre-myopes and how prescribing plano defocus spectacle lenses have become a preventative tool in his practice.
China (Figure 1), and have over 100 pre-myope patients using plano Stellest in practice – most who are incredibly happy and satisfied.
My plano Stellest prescribing criteria:
• ≥3 consultations over six to nine months with biometry measured each visit.
• Cycloplegic refraction in the first visit is a must.
• Axial elongation >0.20mm and or refractive shift ≥0.50D in six months.
• Low hyperopic reserve relative to age norms.
• Family history of early-onset myopia.
Case: Hyperopic reserve and axial length changed significantly in six months
• Six-year-old Asian male Baseline (2022): Axial length: 23.40 mm (OD – right eye), 23.46 mm (OS –left eyeº. Rx: +0.75 -0.25 X 3, +0.75 -0.25 X 176, unaided 6/6 visual acuity. : Axial growth surged (+0.27 mm OD, +0.29 mm OS). cussed the progression and lowering hyperopic reserve with parents. Plano Stellest was prescribed with a myopia management specific frame. : Growth slowed to 0.18 mm (OD) and 0.19 mm (OS) with plano Stellest. Rx: Plano -0.75 X3 (OD) and Plano -0.75 X 176 (OS)
We witnessed a significant axial slowdown of 0.27mm/six months vs. .18mm/30 months* OD and 0.29mm/six months vs. 0.19mm/30 months* OS, and the refractive changes for both eyes were much slower than before plano Stellest. With this approach, it’s great to demonstrate to parents the line has flattened with only a 0.12 mm change in their son’s eyeball length in the last 12
Myopia management is not only about slowing progression in axial length and refractive error in confirmed myopes. We can even do it before it comes. By delaying each 1.00 D of progression, we reduce myopia maculopathy risk by 67%* and a 0.25 D reduction in myopia (equivalent to about 0.1 mm) yields close to a 10% reduction in risk.* We need to strive to detect and identify potential pre-myopes earlier from regular and comprehensive exams,
Figure 1: Dr Oliver Woo’s retrospective study used medical records from his Sydney practice involving 85 children with pre-myopia in one or both eyes. Among Asian children aged five to eight years wearing plano Stellest lenses, mean one-year change in axial length was 0.16 mm, which appears to be less than untreated pre-myopes (based on literature).
Images: Oliver Woo.
Dr Oliver Woo, Sydney optometrist.
Reveal the unexpected
Discover LuxOR® REVALIA™
Alcon’s microscope for anterior and posterior procedures, delivering superior visualisation through proprietary ILLUMIN-i technology:1-4
33% Greater Depth of Field*4
6x larger, more stable, red reflex†2,4,5
Alcon Biometer and Phaco Integration1,6,7
*Compared to conventional focused illumination microscopes. Assuming 200 mm working distance, LuxOR Revalia adds 65 mm to the focal length, resulting in 33% increase vs. a conventional 200mm microscope. †Compared to ZEISS* Lumera* T, Lumera* 700, and LEICA* M-820 microscopes. *Trademarks are the property of their respective owners.
References: 1. LuxOR Revalia User Manual. 2. Cionni RJ, Pei R, Dimalanta R, et al. Evaluating red reflex and surgeon preference between nearly-collimated and focused beam microscope illumination systems. Transl Vis Sci Technol. 2015;4(4):7. 3. Alcon data on file, 2014. 4. Schwiegerling J & Dimalanta R. Depth of focus measurements of ophthalmic surgical microscopes. Poster presented at: The Association for Research in Vision and Ophthalmology; May 1-5, 2016; Seattle, WA. 5. Alcon drawing number 955-7210-004, 2014, Scientific Support Document, Communication for Alcon LuxOR Red Reflex and Depth of Focus Calculations. 6. Centurion Vision system User Manual. 7. Verion Digital Marker M User Manual.
There’s a lot to think about when faced with a progressing myope. Is their script up to date? Is the treatment arresting axial length growth? And, most importantly, how can you be sure the retina hasn’t been compromised out in the periphery?
Sydney optometrist Dr Susan Ang could be considered an early adopter in myopia management, but it wasn’t necessarily pursued out of interest.
It was 2004, and her Eyestore practice, an independent located in the western Sydney suburb of Bankstown, had a big focus on paediatric eyecare and a patient-base that was around 95% Asian descent.
With myopes streaming into her consulting room, she needed to offer more than single vision spectacles; the emerging evidence demanded it. So starting out with orthokeratology (orthok), bifocal and multifocal ophthalmic lenses, she got to work expanding her treatment repertoire over the years to include atropine and more precise interventions like specially designed soft lenses and myopia-specific spectacle lenses.
But by 2019, there was a nagging feeling her approach wasn’t complete.
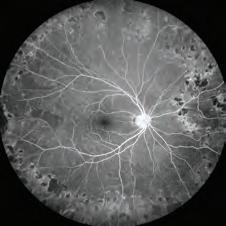
The International Myopia Institute (IMI) was putting out white papers documenting best practice. A biometer for axial length was necessary, but so was an ultra-widefield retinal imaging device if she to was pick up pathologic myopia or other related complications.
“We wanted to go up a notch, just to ensure we were following the IMI papers, obtaining a strong baseline and giving the best level of care to our children,” says Dr Ang, who has certification with the International Academy of Children’s Myopia Management and is an Orthokeratology Society of Oceania member in fellowship training.
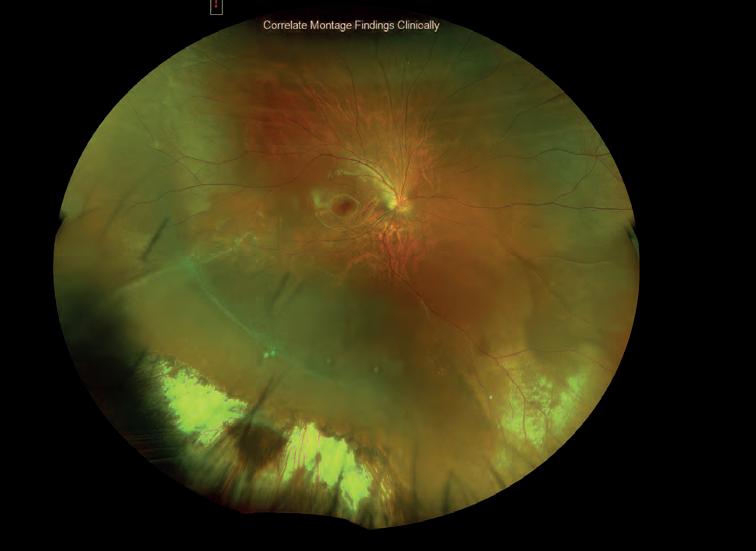
“As soon as we installed the Optos Daytona, we began noticing how many retinal holes and tears we were missing, because we usually waited for a symptom or a sign to appear.”
The Daytona is the most common Optos technology found in the optometry setting and in Australia has become a feature of independents looking to step up and differentiate their service. It produces a 200° single-capture retinal image (optomap) – up to 82% of the retina – in less than half a second while offering other functionality like autofluorescence.
For Dr Ang, whose practice sees a high volume of progressing myopes weekly, it’s allowing her to pick up peripheral retinal pathology she couldn’t see otherwise through fundoscopy or biomicroscopy, or to document lesions that would have been recorded with written notes.
“It also removes any doubt or question marks over whether something might have been missed by the optometrist on the day, which is vital from a medico liability point of view, especially when we’re treating so many children – a picture tells 1,000 words,” she says.
“Now we’ve spotted a child as young as 10 with a retinal hole and 14 is the youngest I’ve seen with an asymptomatic tear, so we see great value of using optomap imaging as a screening tool.”
In such cases, they are promptly referred to the vitreoretinal surgeon across the road, Dr Thomas Pham, where several options are on the table like prophylactic barrier laser treatment. He also uses an Optos system, making data sharing seamless.
Every patient starting myopia treatment in Dr Ang’s practice has an optomap taken to obtain a baseline. Others who are -4.00 D or more –
regardless of their condition or age – are also recommended, as well as those presenting with flashes and/or floaters.
She’s scanned children as young as three on the device, gaining an insight into the child’s retinal health that would have been extremely difficult otherwise.
In cases of high myopia – a refractive error of at least -6.00D or an axial length of 26.5mm or more – it’s allowed her to check for signs of myopic maculopathy that can impact people in their most productive years.
But Optos technology has also challenged many long-held beliefs.
“We always think that you've got to have very long eyeballs to get a tear or a hole – and I think the Optos has prompted us to not follow that misnomer as strictly. 'It’s not rare, unless it's in your chair', kind of thing. It’s shown us they can happen to anybody.”
When describing the value of Optos imaging to her practice, Dr Ang uses words like “failsafe”, “armour guard”, “clinical confidence”. It’s an indisputable, time-stamped record of the patient’s retinal health. It’s vital in a condition like myopia that can progress rapidly, and when other optometrists work under you autonomously.
Plus, with a certain number of scans per week, she’s pretty sure the return on investment (ROI), in monetary terms, has probably been met.
But it’s something she hasn’t thought about much; it’s the hard-to-measure stuff – like loyalty, word-of-mouth-referrals and the patient’s ongoing contribution to society – that reminds her it was an investment worth making.
GETTING MYOPES INVESTED IN THEIR PLAN
Two cases spring to mind for Victorian optometrist Mr Jason Teh when asked when an optomap image has influenced his myopia clinic.
The first, a -3.00 D 14-year-old who visited his In2Eyes practice in Surrey Hills, in Melbourne’s east, had several retinal holes in the extreme periphery.
It was a surprise finding, and after some monitoring he was referred for prophylactic barrier laser treatment.
He recalls another case of a young child who came in earlier than expected for an orthok review due to blurred vision they thought was related to the treatment.
“It turned out to be a retinal detachment. Unfortunately, he had to be referred straightaway to undergo major surgery, a scleral buckle.
“If you've got a full-blown retinal detachment, any quick view into the retina will show you that. But with the Optos, it's nice to be able to see the before and after photos, to see if there were any early signs. In this case, unfortunately, there weren't any, so it was probably a very acute event.”
Teh picks up lacquer cracks that appear in extremely long eyes, as well as chorioretinal atrophy.
“But that’s very rare. I think I've seen that once in 20 years, so it's
Image: Jason Teh.
“It allows you to also see chorioretinal changes, which are rare, but the autofluorescence function is quite helpful for assessing the impact of the myopia at different retinal layers.”
main uses are for peripheral degeneration and detecting early retinal detachment for myopic patients. But it images the optic nerve as well, allowing you to see the myopic presence, or any nerve peripapillary atrophy that you can track over time.”
In his practice, his protocol is to monitor young myopic patients every six months, with optomap scans obtained annually.
At the first visit, a montage of scans (central, up, down, left and right), is captured for a baseline. It’s a vital moment to educate patients on myopia, using a 3D eye model the Optos system generates.
He demonstrates how, when the eye elongates, it creates strain on the delicate retinal tissues. It gets the patient invested in their care, to take treatment compliance seriously, and creates an air of professionalism for the optometrist.
Another key feature of the Optos Daytona is fundus autofluorescence, which has proved its worth in extreme cases like myopic maculopathy.
“Depending on what you're looking for, what structure you're looking at, the hyperfluorescence will show up as metabolic stress in the RPE, for example, or it might suggest your RPE is undergoing atrophy.
IT’S THE GOODWILL THAT COUNTS
Heading back to Sydney, businessman Mr Paul Lee operates three boutique-style practices under The Eye Piece banner. Since 2020, he has been keen to make Optos ultra-widefield imaging standard in the patient journey, realising it was imperative to remain at the “forefront of independent practice”.
The Eye Piece.
“And from a business perspective, I thought it could attract and bring in more patients, but the optometry team has seen huge clinical benefits with it too," he says.
“The way you take the photo, the way it's displayed and how the information is relayed helps to elevate the experience too.”
Lee’s optometrists, Ms Patricia Tsong and Ms Adeline Wong, say retinal imaging has become more common in optometry, so it’s becoming easier to encourage most patients to take it up and pay the additional fee.
An Optos Daytona is installed at Lee’s Sydney CBD and Balmain locations. The third practice, in Wahroonga, is surrounded by schools and sees the majority of their myopia patients – but it hasn’t quite got the floor space, so patients are sent to the other locations when a retinal scan is necessary.
In Wong’s experience, she’s typically picking up retinal pathology in high myopes in their 60-70s, and while OCT detects most of myopic maculopathy, optomap imaging has made her job easier to visualise and record peripheral lesions.
For Tsong, she recently picked up a temporal retinal hole in a 16-year-old borderline high myope.
Naturally, patients like this are thankful and relieved. It galvanises the patient-practitioner bond, which is a bonus in progressing myopes early in their eye health journey.
“When we pick something up, the patients are so grateful,” Lee says. “Often Patricia and Adeline get chocolates and flowers as a thank you for preventing something more sinister happening to their vision, so it's a great outcome for everyone.”
Across town, Dr Ang has had the same experience in her Sydney store. The investment has been more than been justified in monetary terms, but she’s equally happy with the good will it has generated.
“Sometimes you can't measure impact financially, because when you’ve picked something up and referred that patient, you’ve got them for life,” she says.
“And they’ll start sending their friends and their family along to you too.”
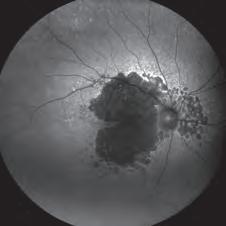
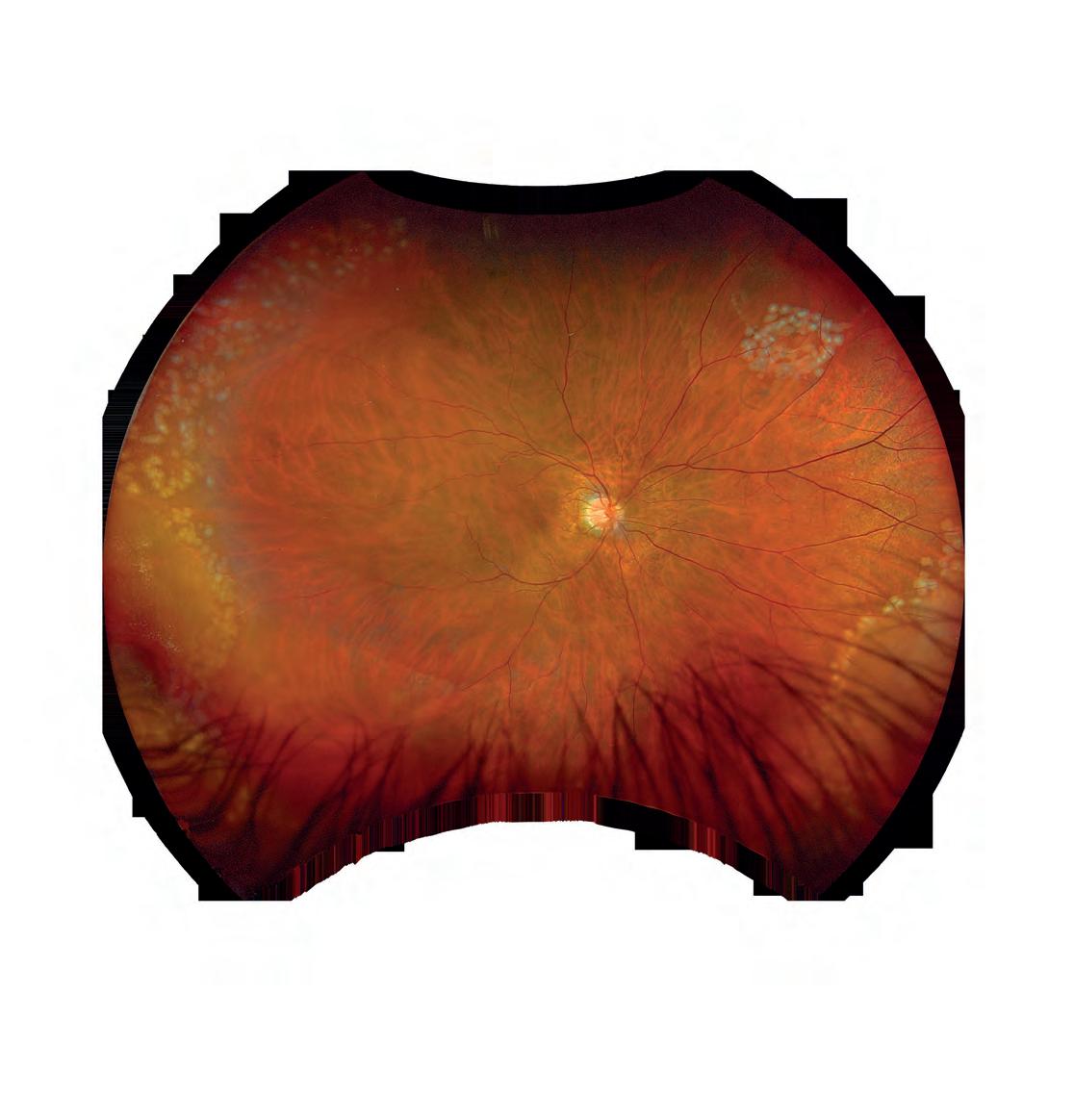
OPPOSITE: A myopic orthok patient, under Jason Teh's care, with a retinal detachment that ultimately required a scleral bucked (pictured).
ABOVE: A left eye inferotemporal hole Dr Susan Ang (far right) diagnosed in a 12-year-old boy with a -4.00 D prescription on orthok treatment.
Introducing Optos imaging in two The Eye Piece practices, Sydney, has elevated the patient experience.
Image: Susan Ang.
Image: Susan Ang.
Spreading the word
CooperVision’s MiSight 1 day is a key product helping slow the progression of myopia in children. As optometry increasingly embraces myopia management as the standard of care, the emphasis is shifting to ensuring the largest possible proportion undertake treatment with the most suitable product for the individual.
Optometrist and contact lens practitioner Ms Jessica Chi, the owner of Eyetech Optometrists in Melbourne, has been offering MiSight 1 day for a number of years. Within her myopia toolkit, she regards the soft contact lens as one of the small number of treatments with a strong, long-term evidence base.
The lens was subjected to a large, seven-year, multi-centre study involving a mix of ethnicities and looking not only at safety and efficacy, but also the reaction of children and parents to soft lens wear.
This is essential in a condition like myopia, given the importance of achieving the best possible result over a decade or more of treatment.
Few, if any, of the current crop of myopia control interventions are backed by a study of this length. As such, it’s the first and only FDA-approved product proven to slow myopia progression in children aged eight to 12 at the initiation of treatment. On average, age-appropriate children wearing MiSight 1 day progressed less than -1.00 D over six years.
As an optical treatment, Chi appreciates how MiSight 1 day provides the dual benefit of myopia control and vision correction. Being a soft contact lens it is also ideal for the active lives of kids.
And because soft lenses are unlikely to be removed or worn incorrectly during the day (like spectacles can be), the necessary full-time “dose” of myopic defocus is more certain of being delivered. In the case of MiSight 1 day, this is a minimum of 10 hours per day, six days per week, CooperVision reports.
For Chi, who’s also the Victorian president of the Cornea and Contact Lens Society of Australia (CCLSA), familiarity has built a fondness for the product.
“Knowing that it’s a proven, and importantly, safe treatment over a long period gives me the necessary confidence to recommend it to parents of children who would benefit,” she says.
With the expansion of the power range from to -10.00 D in 2022, one question is whether the special optical design still delivers sufficient myopic defocus to the unusually prolate retinas often seen in high myopia?
A recent study published in Ophthalmic and Physiological Optics, demonstrated the lens’ ability to deliver consistent retinal defocus in such eyes.
ABOVE: On average, age-appropriate children wearing MiSight 1 day progressed less than -1.00 D over six years.
The work, led by associate scientist Dr Dawn Meyer of Indiana University School of Optometry, found the MiSight 1 day design demonstrated significant optical defocus across varying view distances and retinal regions.
That gives Chi even more confidence to use the lens in her practice and recommend it to parents and often very young patients.
“Many parents put all trust in the practitioner, and as the practitioner, it is our responsibility to be up to date with the latest clinical evidence,” she says. “However, some parents want a bit more, and feel more confident reading into the science.
“It’s up to us to instil that confidence in parents, and I wouldn’t say that I was confident in it if I didn’t have the evidence.”
That science is supported by Chi’s patients.
“Feedback is almost unanimously good,” she says. “It’s simple and easy to use, they can see well, and then there’s confidence that we can control their myopia.
“The only complaint is, in the beginning, it can be a little bit tricky to get on and off, but that’s no different to any other contact lens. Occasionally, some patients experience some dryness, however it’s that’s usually alleviated by lubricant eye drops.”
She says that, using the MiSight 1 day soft contact lens, there has been no progression in the “vast majority” of her patients, and “the ones who have had progression, they’ve progressed at a much slower rate”.
Often, for those who have shown progression, the right questions can reveal why.
“I’ve had one child who was well controlled, and then at one review demonstrated progression. I discovered that was because he was waking up early and reading before his parents put the contacts in for him. It is important with all myopia control techniques to continue to ask the right questions. It is easy to blame the product being ineffective, however, much of the time it can be due to non-compliance.”
Contact lenses may not be for everyone, she says.
CooperVision has come up with a product suitable for close to 100% of
children, and patients as young as five have been shown to confidently apply and remove MiSight 1 day on their own.
“But there are some kids and families very resistant to contact lenses and no matter how hard you try, there’s some people that just have an extreme fear of anything near their eyes,” she adds.
“However, I never view this as a no, simply as a ‘not yet’.”
Chi believes optometrists can overcome this by portraying confidence in the product.
“If you demonstrate confidence in the treatment, then you won’t give the parents the confidence to want to use it. Parents are often very nervous about prescribing contacts for their children at a young age.
“But I find that the kids are actually the easiest and the most compliant,
because they’re used to following instruction, and they usually have not yet developed a rebellious nature.”
Mr Joe Tanner, the head of professional affairs at CooperVision, acknowledges that conversations with parents about myopia, the potential impact on their child, and the recommendation for contact lenses for young children can sometimes be challenging.
“Explaining the need to slow myopia’s progression is not at first a good-news discussion,” he says. “But once the need to act is communicated, the discussion should become a positive one whereby the parent and child feel they are taking control of the condition with the expert support of their optometrist.
“One of the common questions that practitioners get from parents, and I certainly remember being asked this a lot when I was in practice, is, will it get worse?
“And of course, now our answer is, it probably will get worse. But there are things we can do about it, very effective things.”
In the case of MiSight 1 day the positive discussion is informed by many years of research. It’s also supported by plenty of feedback to CooperVision, from practitioners like Chi.
“You’ve got a thoroughly proven treatment with a lot of long-term evidence behind it,” says Tanner.
“Now it’s just about getting myopia management to as many children who need it, and there’s still a lot of children who would benefit from wearing soft lenses to achieve this.
He encourages eyecare professionals to take up that challenge.
“With MiSight 1 day, we are only asking that the child undertake a trial so they and their parent gain a proper understanding of the practical benefits of contact lens wear. That ‘try before you buy’ aspect is another real advantage of this form of treatment."
Australia’s first plant-based optical lenses. ECO6 is the first lens material crafted entirely from plant-derived resources, revolutionizing traditional optical lens manufacturing.
By replacing petrochemicals with biomass plant-based materials, ECO6 is designed to significantly lower greenhouse gas emissions compared to conventional petroleum-based products. crlabs.au/range/eco6
Green looks good on you!
Image: Eyetech Optometrists.
Optometrist Jess Chi works with a young patient at her clinic.
Upgrade and take control
He’s only just had the upgrade installed but already this optometry practice owner is seeing the need for others to take up the software and play their part in pushing back against the building wave of myopia.
Mr Gavin Boneham is excited.
The owner and principal optometrist at Boneham Optometrist Eyecare Plus in Sydney is also president of the Orthokeratology Society of Oceania.
As part of that he has long had a focus on myopia control and how the use of orthokeratology (orthok), among other treatments, can slow its progression.
And now he has an upgraded piece of kit to help him in that endeavour.
Two days before talking with Insight, Boneham received the new Myopia Management software upgrade for his REVO 80 OCT scanner. And he’s still buzzing about what this will mean for his patients and practice, and its potential, once he puts the technology to work in his myopia clinic.
He was already impressed with the REVO device – made by Polish manufacturer Optopol and distributed in Australia by OptiMed – and the support he gets with it.
“I’ve had a REVO for a few years now and it allows me to do an axial length measurement for myopia control. I can look at the retina, I can do OCT imaging of the retina, and they’re always updating their software.”
A device with many functions means more value for money and space in the testing room.
Those functions include up to 130,000 A-scan/sec scanning speeds and OCT-A. There’s a full-colour fundus camera and the ability to combine simultaneous OCT and fundus images.
There’s also optional ‘modules’, such as T-OCT for corneal curvature maps, and B-OCT for biometry in myopia management and intraocular lens calculation, capturing axial length, central cornea thickness, anterior chamber depth, lens thickness, pupil size, choroidal thickness, and white to white.
But what has Boneham particularly excited about the Myopia Management software is its ability to turn his REVO OCT into a powerful myopia management and monitoring device.
OptiMed says the upgrade allows for biometric and topography monitoring. It
also enables “trend analysis over population norms”.
That means access to data from three key population databases: Nicer European, a scale representative of younger European children; Tidman, a model based on a wider European age-range; and Sanz Diez, based on research carried out in China, with its higher prevalence of myopia.
That is combined with the device’s measurement of the axial length and its already extensive scans of the anterior and posterior boundary of the cornea, the anterior and posterior boundary of the lens, as well as the posterior boundary of the retina.
When that data is compared with inputs about the patient’s family history and environmental conditions, including how much time they spend outdoors and on small screens, this helps to deliver a clearer idea of where that patient falls compared with others of similar age and ethnicity.
REVO OCT also provides the user with the ability to measure choroidal thickness and populate this data into the myopia management module.
The ability to measure this metric is something standard biometers can’t not perform, but with REVO being an OCT it already has the capabilities to measure every layer of the retina and the ability to enter this data into the programme is becoming increasingly important for those monitoring this patient database.
More information is coming out on its relevance and being able to correlate and measure this metric as part of the module sets REVO aside as unique and adds even more value to this device being at the forefront of this new wave of myopia management.
Analysis using the artificial intelligence within the software gives the practitioner a clearer picture of that person’s myopia risk, what is likely to happen if changes are not made, and then information about the efficacy of any treatments prescribed.
Despite only recently accessing the module, Boneham is already confident that his patients, especially the parents of potentially myopic children, are going to be just as impressed as he is.
“So you can show the parents – OK, your kid is at this stage; if he or she keeps going this way, they’re going to end up here. So we’ve got to be a bit aggressive, or not, depending on the information.
“It’s also us saying, here’s the best, the latest myopia module and analysis program. So we’ve got your kid, you can rest assured that your child is getting the best care with our practice.”
Using the upgrade during follow-up appointments can quickly track if treatments are working or need adjusting.
Boneham says that gives him the confidence to “hit it hard”, and means patient and parent are more likely to listen and act, even if that means lifestyle changes, such as more time outdoors and less time on small screens.
But it’s not just the patient who benefits. Boneham can see numerous advantages for the practice as well.
He says the module is easy to use for anyone considered “computer-savvy”.
“I can do it; it passed the Grandpa test.”
It fits nicely into the practice workflow and actually speeds up the process with patients.
“The software does all of this straight away, I don’t have to do it manually,” he says. “It will probably save about five minutes for each patient.”
Boneham is an early adopter of the module and the technology.
But he doesn’t see it as a luxury or a nice-to-have. As much as it might help one independent practice differentiate itself from others, he believes the tsunami of myopia around the world means this equipment should be commonplace in optometry practices around Australia.
“The World Optometry Council has said everyone has to practise myopia management – that’s the standard of care now.
“Every practice should be doing it. And if you want to do it, you want to do it well, with an OCT and an axial length measurement.
“And this shows the parent as well, I’m paying all this money but we’re getting this result.”
Image: Gavin Boneham.
Principal optometrist Gavin Boneham gets to grips with the new software that has made his REVO 80 OCT scanner a myopia management and monitoring device.
Light therapy in myopia
Light therapy is a rapidly expanding field in myopia intervention, with multiple promising options on the horizon. QUT’s DR EMILY WOODMAN-PIETERSE and DR ROHAN HUGHES expect they will become adjunctive therapies to complement current interventions. But what do optometrists need to know now?
LABOUT THE AUTHORS:
LEARNING OBJECTIVES:
At the completion of this article, the reader should be able to improve their knowledge of emerging myopia control interventions, including:
• Understand the mechanisms behind light therapy's effects on axial eye growth.
• Evaluate the effectiveness of repeated red light therapy (RRL) in slowing myopia progression.
• Advise patients on balancing increased outdoor activity with sun safety practices to prevent myopia.
• Understand the potential of various light therapies as emerging interventions for myopia management.
ight therapy is delivered by a device that emits a controlled light dose, commonly applied in the treatment of dermatological conditions and mood and sleep disorders. Following the discovery that outdoor light exposure can influence refractive error development and eye growth,1 interest in light therapy as a potential intervention for myopia control has surged.
Epidemiological evidence suggests that the lowest incidence and prevalence of myopia in childhood are associated with the greatest amount of outdoor activity.1
Although the characteristics of the outdoor environment responsible for this protective effect are unclear, the higher intensity and/or the broader spectral distribution of sunlight are the most likely culprit and are absent in indoor environments. 2
While recommending that young, at-risk patients spend more time outdoors is a safe, simple and affordable solution with additional health benefits, this may not be practical in all locations and climates, and as such, light-based interventions – such as repeated red light therapy, violet/ultraviolet (UV) light therapy, blue spot stimulation and enhanced indoor lighting designs – have emerged as potential treatments to complement existing myopia control interventions. 3
Animal studies suggest that chromatic cues within light can modulate axial eye growth and refractive error development, driven by the eye’s inherent longitudinal chromatic aberration. 4In some animal models, those reared under short (blue and violet) wavelengths developed less myopia than those raised under long (red) wavelengths, consistent with eye growth changes predicted by longitudinal chromatic aberration (Figure 1).
However, some primate studies have been contradictory, with longer wavelengths found to slow eye growth. These findings have inspired the use of light therapy to limit myopia development and progression in children using a variety of wavelengths. 3
OUTDOOR TIME
While the ideal timing and intensity of outdoor light is still being determined, evidence suggests children at high risk of myopia should be encouraged by their eyecare provider to aim for two to three hours per day (or 14-21 hours per week) outdoors to reduce their odds of developing myopia. 5
Randomised controlled trials conduced in Chinese and Taiwanese schools, in which children were allocated additional outdoor time (such as additional
1. Longitudinal chromatic aberration within the eye as a mechanism for increasing (long wavelength) or decreasing (short wavelength) axial eye growth.
daily sessions of outdoor activity, enforced outdoor play during recess, and incentivised outdoor activities on weekends for students and their families) have found significantly lower myopia incidence, axial eye growth and myopic refractive shifts in non-myopic children.1, 3 However, the benefits for children who are already myopic are smaller and clinically insignificant.1
SUN SAFETY
While the aim of myopia control is to reduce the long-term risk of pathological myopia development and vision impairment, practitioners should be aware that the potentially sight- and life-threating complications of excessive UV radiation exposure should be of equal concern. Although diseases associated with excessive UV exposure to the skin and eyes do not typically manifest until adulthood, the damage is sustained primarily in childhood when the melanocytes in juvenile skin are more susceptible to DNA damage.6 Myopia control messaging must also emphasise the importance of sun safety measures, with research suggesting that even when wearing sunglasses, hats, or seeking shade outdoors, light levels are still above the threshold illuminance for myopia prevention.7
FIGURE
Dr Emily C. Woodman-Pieterse Centre for Vision and Eye Research, Queensland University of Technology
Queensland University of Technology
FIGURE 2. Potential mechanisms for reduced axial eye growth using red light. Mitochondria absorb energy from red light, which increases cellular energy output. This may reduce scleral remodelling and eye growth directly through stimulation of collagen and fibroblasts which strengthen the sclera, or indirectly through improved choroidal blood flow and oxygenation which reduces scleral hypoxia.
CLASSROOM LIGHTING
Since two-to-three hours a day outdoors may not be possible for all, improvement of indoor lighting, particularly in classrooms, may be a viable alternative for large-scale implementation. Select primary schools in China have participated in classroom-based lighting intervention studies, where either illuminance levels8 or spectral composition of light sources9 have been altered to more closely resemble outdoor environments.
Traditionally lit classrooms in China have an average luminance of 74 lux, but in schools that redesigned their lighting to ensure a minimum desktop illuminance of 300 lux, the incidence of new myopia fell from 10% to 4% over 12 months.8 Similarly, in schools that introduced artificially synthesised light sources to mimic the spectrum of daylight, myopia incidence decreased by 5% in seven to nine year-old children over three years. While these interventions have produced small but significant reductions in cases of new myopia, they have failed to slow progression in children with established myopia. As with outdoor light programs, practitioners may find that children at high risk for myopia onset gain the most benefit from modified indoor lighting.
REPEATED RED LIGHT THERAPY
Repeated red-light (RRL) therapy has gained significant interest in recent years, with the greatest volume of clinical trial data and most promising evidence supporting myopia control efficacy of the light therapy options. 3
While numerous RRL therapy devices have been used overseas, only one has been approved by the Therapeutic Goods Administration for use in Australia: the ‘Myopia Management Device’ (Eyerising International). This is a home-based, desktop device that delivers red light via a semiconductor laser with a peak wavelength of
650nm and illuminance levels of approximately 1600 lux through the pupil. Treatment is administered twice daily for three minutes each session (a minimum of four hours between sessions), five days a week. Systematic reviews and meta-analyses have concluded that RRL therapy may be effective in slowing eye growth and myopia progression, 3,10 with treatment effects detected from four weeks to 24-months after commencement. However, only one study to date followed participants for longer than 12 months.11 Given that myopia typically progresses for many years in childhood before
which may be causing retinal toxicity or altering chorioretinal metabolism.12 There have been no serious device-related adverse events reported in the clinical trials conducted, however, a case has been reported of a 12-year-old girl who sustained outer retinal damage, similar in appearance to laser-induced maculopathy, after five months of RRL therapy (once treatment was terminated, the patient partially recovered over a period of three months).13
To enable widespread adoption of RRL therapy as a safe and effective option for myopia control, future clinical trials will require comprehensive assessments of retinal structure and function beyond visual acuity measurements and macular OCT, such as multifocal electroretinography and high-resolution imaging of photoreceptors and other retinal cells.
Recently, the Chinese government has changed the regulation of RRL devices which will have implications for future study of its effectiveness and safety, and may impact the adoption of RRL treatments.14
BLUE LIGHT ONH STIMULATION
Blue light (peak wavelength ~480 nm) has been found to activate the melanopsin photopigment located within the human eye, likely in a similar manner to sunlight. Melanopsin is contained within the cell bodies, axons and dendrites of the intrinsically photosensitive retinal ganglion cells (ipRGCs), a small subset of retinal ganglion cells that are thought to be responsible for the light-mediated mechanisms that regulate eye growth and myopia development (Figure 3). 2
The axons of the ipRGCs converge at the optic disc and form the optic nerve, so that the highest
“LIGHT THERAPY IS A RAPIDLY EXPANDING FIELD IN MYOPIA INTERVENTION, WITH MULTIPLE PROMISING TREATMENT OPTIONS ON THE HORIZON”
stabilising in late adolescence/early adulthood, studies of longer duration are required to support widespread adoption of RRL therapy. Additionally, it appears there is moderate rebound on cessation, although not enough to completely eliminate all benefit gained from the 12-month treatment period.11 If the treatment effects are not sustainable, the clinical utility of this treatment is limited.
HOW DOES RED LIGHT THERAPY WORK?
There are multiple theories as to how RRL therapy thickens the choroid and slows eye growth. The prevailing theory is that red light of a specific wavelength (~650 nm) may increase cellular energy production and nitric oxide release that either increases choroidal blood flow and oxygenation and reduces scleral hypoxia, or stimulates the production of scleral collagen and fibroblasts, both of which are thought to strengthen the sclera and reduce axial eye growth (Figure 2).
There has been some suggestion that the choroid may be thickening in response to the high energy levels emitted from these instruments,
density of melanopsin exists within the region of the optic nerve head. Optic nerve head stimulation with a small, circular patch of blue light allows for maximum ipRGC stimulation that, in turn, stimulates retinal amacrine cells to release dopamine and slow eye growth, while avoiding rod and cone pathway activation within the retina that may inhibit dopamine release.15 An additional benefit of this targeted light therapy delivered to the optic nerve head is that the absence of rods and cones means the light stimulus is virtually undetected by the wearer during the treatment.
A digital application – MyopiaX (Dopavision GmbH) and associated hardware have been developed, delivered via a standard smartphone inserted into a virtual reality (VR) headset, which allows simultaneous bilateral blind spot stimulation while the wearer plays a video game controlled using a Bluetooth gaming controller.15 There are several interactive, age-appropriate games available via the MyopiaX app designed to engage the child and stabilise their gaze during the treatment (~10-minutes per session, twice per day), allowing
for reliable blind spot stimulation.
A randomised, controlled, multicentre clinical trial of the MyopiaX in Europe has recently concluded, in which children were assigned to use the MyopiaX app while axial eye length, choroidal thickness, refractive error, and safety measures were monitored over a 12-month period and compared to children wearing myopia control spectacles (ClinicalTrials. gov ID: NCT04967287). While the longer-term clinical trial data on efficacy and safety is yet to be published and established, short-term studies have demonstrated that blue spot stimulation can improve contrast sensitivity, increase electrical retinal activity, thicken the choroid and shorten axial eye length, which suggests that longer-term use may have the potential to slow myopic eye growth.15
CYAN LIGHT
Based on the knowledge that some intrinsic properties of sunlight influences refractive error development, some studies have investigated whether exposure to cyan light (peak wavelength ~500 nm), which falls within the spectral sensitivity of melanopsin, could reduce myopic eye growth via the melanopsin-ipRGC signalling pathway (Figure 3).16,17 The effect of short-term use of low-powered LEDs emitting cyan light, via both commercially available (Re-timer Pty Ltd)16 and experimental frame designs,17 have been investigated in children and adults. Both studies showed that cyan light had the potential to cause significant choroidal thickening, either through exposure to 30-minutes of light therapy each morning for one week16 or one single two-hour session of exposure, which was also accompanied by axial eye shortening.17
Given that these short-term ocular changes have been shown to serve as a biomarker for longer-term slowed eye growth, it has been speculated that similar devices could be used for myopia intervention following further research and development. While the Re-timer device is commercially available for the treatment of sleep and circadian rhythm disturbances such as jet lag, insomnia and seasonal affective disorder; it should not be used for the purpose of
REFERENCES
1. Dhakal R, Shah R, Huntjens B, Verkicharla PK, Lawrenson JG. Time spent outdoors as an intervention for myopia prevention and control in children: an overview of systematic reviews. Ophthalmic Physiol Opt. 2022; 42 (3): 545-58.
2. Muralidharan AR, Lança C, Biswas S, Barathi VA, Wan Yu Shermaine L, Seang-Mei S, et al. Light and myopia: from epidemiological studies to neurobiological mechanisms. Ther Adv Ophthalmol. 2021; 13: 25158414211059246.
3. Chang DJ, P LS, Jeong J, Saw SM, Sevdalis N, Najjar RP. Light Therapy for Myopia Prevention and Control: A Systematic Review on Effectiveness, Safety, and Implementation. Transl Vis Sci Technol. 2024;13 (8): 31.
4. Troilo D, Smith EL, 3rd, Nickla DL, Ashby R, Tkatchenko AV, Ostrin LA, et al. IMI - Report on Experimental Models of Emmetropization and Myopia. Invest Ophthalmol Vis Sci. 2019; 60 (3): M31-m88.
5. Ho CL, Wu WF, Liou YM. Dose-Response Relationship of Outdoor Exposure and Myopia Indicators: A Systematic Review and Meta-Analysis of Various Research Methods. Int J Environ Res Public Health. 2019; 16 (14).
6. Sharma S, Rose L, Schulz A, Sharma DP, Zeldovich A, Azzi C, et al. Myopia intervention and ultraviolet radiation related eye diseases: A narrative literature review. Taiwan J Ophthalmol. 2024; 14 (2): 151-8.
7. L anca C, Teo A, Vivagandan A, Htoon HM, Najjar RP, Spiegel DP, et al. The Effects of Different Outdoor Environments, Sunglasses and Hats on Light Levels: Implications for Myopia Prevention. Transl Vis Sci Technol. 2019; 8 (4): 7.
FIGURE 3. Light-dopamine theory as a potential mechanism for reducing axial eye growth through increased outdoor light, cyan light therapy, or blue light ONH stimulation. The melanopsin on the membranes of the intrinsically photosensitive retinal ganglion cells (ipRGCs) stimulates the dopaminergic amacrine cells within the retina to release dopamine, which increases choroidal thickness and decreases axial eye growth.
myopia control unless evidence of efficacy in large scale clinical trials becomes available.
VIOLET LIGHT
Violet light (360-400 nm) is abundant in daylight and outdoor environments, but almost entirely absent indoors. Windows, car windshields, and ordinary spectacle lenses and contact lenses block violet light, and fluorescent, incandescent, and LED sources irradiate no violet light. This prompted a Japanese research group to investigate whether violet light can slow progression in primary school aged children who were already myopic.18 Children wore custom-built, 3D-printed frames that emitted violet light for three hours each day between 11:00am and 2:00pm, over a three-month period, after which significant reduction in eye growth and refraction progression was reported in some of the age-groups tested.
Compared to red light therapy, very few studies have investigated violet/UV light on myopia prevention and control, sample sizes have been relatively small, and the evidence available shows
8. Hua WJ, Jin JX, Wu XY, Yang JW, Jiang X, Gao GP, et al. Elevated light levels in schools have a protective effect on myopia. Ophthalmic Physiol Opt. 2015; 35 (3): 252-62.
9. Cai HM, Li MY, Cao Y, Wu YL, Liang M, Chen YS, et al. Effect of artificial natural light on the development of myopia among primary school-age children in China: a three-year longitudinal study. Int J Ophthalmol. 2024; 17 (5): 924-31.
10. Tang J, Liao Y, Yan N, Dereje SB, Wang J, Luo Y, et al. Efficacy of Repeated Low-Level Red-Light Therapy for Slowing the Progression of Childhood Myopia: A Systematic Review and Meta-analysis. Am J Ophthalmol. 2023; 252: 153-63.
11. Xiong R, Zhu Z, Jiang Y, Kong X, Zhang J, Wang W, et al. Sustained and rebound effect of repeated low-level red-light therapy on myopia control: A 2-year post-trial follow-up study. Clin Exp Ophthalmol. 2022; 50 (9): 1013-24.
12. Ostrin LA, Schill AW. Red light instruments for myopia exceed safety limits. Ophthalmic Physiol Opt. 2024; 44 (2): 241-8.
13. Liu H, Yang Y, Guo J, Peng J, Zhao P. Retinal Damage After Repeated Low-level Red-Light Laser Exposure. JAMA Ophthalmol. 2023; 141 (7): 693-5.
14. Wang YX, Wang N, Wong TY. Red Light Therapy for Myopia—Current Regulatory Changes in China. JAMA Ophthalmol. Published online January 23, 2025. doi:10.1001/ jamaophthalmol.2024.5977
15. Amorim-de-Sousa A, Chakraborty R, Collins MJ, Fernandes P, González-Méijome J, Hannibal J, et al. Blue light stimulation of the blind spot in human: from melanopsin to clinically relevant biomarkers of myopia. Bioelectron Med. 2024; 10 (1): 26.
much more modest treatment effects. 3 Although no adverse events have been reported in these violet light clinical trials, the longer-term risks of excessive UV light exposure are well known, and require consideration with respect to these devices.
CONCLUSION
Light therapy is a rapidly expanding field in myopia intervention, with multiple promising treatment options on the horizon, such as RRL therapy, blue light optic nerve head stimulation, and violet light glasses. It is expected that, in coming years, as more safety and efficacy data become available for long-term use of these devices, they will become popular adjunctive therapies to complement currently available myopia control treatments. In the meantime, outdoor time recommendations should be included in all management discussions in established or emerging myopic children. Equally as important, practitioners must emphasise that increased sunlight exposure must be accompanied by sun safety strategies, such as sunglasses and hats, and seeking shade outdoors.
16. Read SA, Pieterse EC, Alonso-Caneiro D, Bormann R, Hong S, Lo CH, et al. Daily morning light therapy is associated with an increase in choroidal thickness in healthy young adults. Sci Rep. 2018; 8 (1): 8200.
17. Chakraborty R, Baranton K, Pic E, Didone J, Kim W, Lam K, et al. Axial length reduction and choroidal thickening with short-term exposure to cyan light in human subjects. Ophthalmic Physiol Opt. 2024; 44 (7): 1414-32.
18. Torii H, Mori K, Okano T, Kondo S, Yang HY, Yotsukura E, et al. Short-Term Exposure to Violet Light Emitted from Eyeglass Frames in Myopic Children: A Randomized Pilot Clinical Trial. J Clin Med. 2022; 11 (20).
NOTE: Insight readers can scan the QR code or visit insightnews.com.au/cpd/ to access a link to this article to include in their own CPD log book.
Feeling proud to have been accredited as a Great Place to Work® in Australia and New Zealand for the past five years and named one of Australia’s Best Workplaces for two years running. In 2024, we were recognised as one of the Best Workplaces in the World! Find your best at Specsavers?
spectrum-anz.com/ careers-at-specsavers
ABOUT THE AUTHORS:
Repeated low-level red-light therapy: a guide for clinicians
Doctor of Optometry, CertOcTher, FACO, General manager city clinics, Australian College of Optometry, Melbourne
Over the past year, repeated low-level red-light therapy has been commercially available in Australia and New Zealand for the slowing of myopia progression. But how effective is it, and how should optometrists begin incorporating it into their practices? Four leading Australasian myopia authorities share insights on this emerging treatment.
MBOptom MPH GradCertUniversityTeaching, Manager paediatric and rehabilitative services, Australian College of Optometry, Melbourne
LEARNING OBJECTIVES:
At the completion of this article, the reader should be able to discuss RLRL with their myopia patients, including:
• Understand the efficacy of RLRL in clinical studies, particularly for high myopia.
• Explore the underlying mechanisms behind RLRL’s effect and its role in axial shortening.
• Report on the efficacy of RLRL in an Australian multiethnic population.
• Understand how to identify appropriate patients for RLRL.
• Assess and monitor patients on RLRL to ensure ongoing efficacy and safety.
yopia is an increasingly global issue, projected to affect one in two people worldwide by 2050.1 Through a combination of genetic and environmental risk factors, such as increased screen time and less time spent outdoors, the growing epidemic of myopia requires effective myopia control treatments to slow progression in childhood, ideally before it progresses to high myopia with its accompanied sight-threatening risks. Indeed, every diopter counts, as even a 1.00 D increase has been shown to increase the later risk of myopic maculopathy by 67%. 2
THE RISE OF RED-LIGHT THERAPY
One of the newest myopia control interventions to be introduced is repeated low-level red-light (RLRL) therapy. This involves young patients using a home-use device that emits visible red light at 650nm through a low-level laser. The therapy requires two sessions per day, each lasting three minutes, five days a week, with a mandatory four-hour interval between sessions. The device tracks each time it is used and is connected to an online portal where parents and clinicians can log on to access real-time compliance monitoring.
The first randomised controlled trial of RLRL was published in 2021, demonstrating a 69.4% efficacy in slowing myopic progression in terms of axial length and 76.6% efficacy in terms of spherical equivalence. The efficacy was even higher at 87.7% for children who were more than 75% compliant, which is similar to completing treatment seven to eight times per week. 3 Since then, numerous studies and systematic reviews have demonstrated strong efficacy of this non-invasive intervention.
Key studies have highlighted the effectiveness of RLRL, with a two-year follow-up study to the landmark trial showing a 75% reduction in myopic progression over two years.4 Another study comparing RLRL to the well-established 0.01% atropine found that RLRL was significantly more effective in slowing myopic progression over 12 months. 5
Additionally, studies on RLRL in highly myopic populations – often overlooked in myopia research – have shown promising results. Two studies of patients of -4.00 D and -6.00 D or higher found that RLRL achieved over 100% efficacy in slowing
myopia and even caused axial shortening.6,7 Notably, while RLRL can be used effectively as a standalone treatment, it can also be combined with all other therapies except atropine, and has shown considerable effect in slowing myopia progression when combined with orthokeratology. 8,9
SAFETY OF RLRL
A recent systematic review evaluating the safety of RLRL reported a side effect rate of 0.088 per 100 patient-years, far lower than other myopia control treatments like atropine or orthokeratology, with the main side effect noted being a temporary afterimage.10 Only one case report of an adverse event was noted from the literature, with a complete recovery of the patient noted on later follow-up.11,12 Although the exact mechanism of RLRL has yet to be elucidated, a common significant finding across numerous studies of RLRL is that it causes significant choroidal thickening, as well as an increase in retinal and choroidal blood flow. 3,13 Studies have also shown that this choroidal thickening correlates to the degree of clinical efficacy and may be related to alleviating scleral
BELOW: The first international studies of the Eyerising device are now yielding results outside of China, from countries like Australia, Japan and Spain.
1. Line graph showing the adjusted mean changes (95% CI) in axial length from baseline to 12 months in an Australian school-aged population.
AXIAL ‘SHORTENING’
A distinctive feature of RLRL, compared to other myopia control treatments, is its ability not only to slow the axial elongation of the eye associated with myopia but also to promote significant axial shortening (greater than 0.05 mm per year) in some patients14,15 This phenomenon was observed in 21.9% of participants in the landmark trial at 12 months, and in 26.5% of participants in a separate real-world study of 434 myopic children aged between three to 17.14,15 In addition, for the RLRL group that exhibited AL shortening, choroidal thickness thickening could only explain 28.3% of AL shortening.14 This suggests that the observed AL shortening may be related to true scleral remodeling, rather than an apparent shortening due to choroidal thickening, highlighting the potential for RLRL to directly influence structural changes in the eye.
INTERNATIONAL UPTAKE
While RLRL research thus far has been largely published from China, the only RLRL device to have attained international regulatory approval to date is the Eyerising device. Excitingly, the first international studies of this device are now yielding results from countries like Japan, Australia and Spain. Commercial interest is also growing, with the Eyerising device now available in several regions (Europe, Australia, New Zealand, UK, Malaysia, Vietnam and Turkey). In Australia and New Zealand, patients are approaching the completion of up to two years of RLRL treatment.
Below, four early adopters and users of RLRL in Australia and New Zealand discuss their experiences and insights into this new treatment modality, and where they see RLRL positioned into myopia management in future.
Assessing efficacy of RLRL in an Australian population
Nellie Deen and Zeinab Fakih are paediatric optometrists at the Australian College of Optometry in Melbourne, Australia, where they serve as general manager of city clinics and manager of paediatric
2. Line graph showing the adjusted mean changes (95% CI) in spherical equivalence refraction from baseline to 12 months in an Australian school-aged population.
services, respectively. Together, they led a pioneering 12-month study on RLRL in Australia, which investigated its efficacy in school-aged Australian children and concluded in December 2024. This study was the first to examine RLRL in a non-Chinese population and followed the same inclusion and exclusion criteria as the landmark trial in China, allowing for direct comparison.
Our trial recruited 34 multi-ethnic children aged eight to 13, who were randomly assigned to either use the Eyerising device or single-vision spectacles. Over 12 months, the RLRL group showed significantly less myopic progression,
also good at an average of 60.0%, and generally they found the Eyerising device easy to tolerate. Going forwards, we are excited to be soon presenting and publishing this work. Furthermore, following the conclusion of the clinical trial, ACO Eye Health has since incorporated RLRL into its myopia clinic framework. As a public health provider, ACO Eye Health will offer RLRL at a reduced cost for eligible patients. The clinic will also continue to monitor and follow up the trial’s participants, particularly those continuing to use RLRL, for additional learnings as to RLRL’s continued efficacy and safety.
“A DISTINCTIVE FEATURE OF RLRL, COMPARED TO OTHER MYOPIA CONTROL TREATMENTS, IS ITS ABILITY NOT ONLY TO SLOW THE AXIAL ELONGATION OF THE EYE ASSOCIATED WITH MYOPIA BUT ALSO TO PROMOTE SIGNIFICANT AXIAL SHORTENING (GREATER THAN 0.05MM PER YEAR) IN SOME PATIENTS.”
with mean axial shortening at one, three, six and 12 months, and a 12-month progression of -0.03 mm compared to controls at 0.12 mm. Spherical equivalence progression was also considerably less in the RLRL group, with 0.09 D of improvement, while the control group experienced a progression of -0.21 D. No adverse events or structural changes on OCT were reported, supporting the safety profile of RLRL in this population. Patient compliance was
Patient Identification
Philip Cheng is a distinguished myopia control optometrist based in Melbourne, and is the founder and director of Eyecare Concepts | The Myopia Clinic Melbourne, dedicated to innovative myopia management strategies. With vast experience across a full spectrum of myopia control methods, including orthokeratology and atropine, he has recently introduced RLRL into his clinic as a novel approach.
FIGURES 3A AND 3B. Line graphs showing the adjusted mean changes (95% CI) in axial length and spherical equivalence refraction from baseline to 12 months in a highly myopic population.
FIGURE
FIGURE
For my initial RLRL patients, I have focused on high myopia, a subgroup where I have a large patient base, and for whom I am developing a specialised clinic. High myopia, defined as -6.00 D or more, affects 4% of the global population,1 with projections of 9.8% by 2050 and up to 20% in parts of Southeast Asia.
It significantly increases the risks of complications such as glaucoma, retinal detachment and myopic maculopathy, which can lead to irreversible visual loss. Even a 1.00 D increase in myopia has been demonstrated to increase the risk of myopic maculopathy by 67%, 2 therefore addressing progression in high myopes is critical.
Evidence for the efficacy of myopia control interventions in high myopia is limited, as these patients are often excluded from studies. A 2024 systematic review identified only 12 studies, with efficacy ranging from 50-60%.16 Treatments like orthokeratology are off-label for myopia above -6.00 D and often challenging to fit. Myopia management spectacle lenses, available up to -10.00 D, also have limitations, with thick lenses in high myopia cases that can be cosmetically unappealing.
In contrast, RLRL has demonstrated strong clinical efficacy in treating high myopia, with two studies showing exceptional results in slowing or even halting myopic progression.6,7 Both studies showed mean axial shortening in RLRL patients of 0.06 mm and -0.11 mm, respectively, and a higher percentage of patients (50-60%) experiencing axial shortening compared to in normal myopia (20-30%). A further advantage of RLRL is that it can be administrated as an adjunctive treatment for patients using optical interventions such as orthokeratology, soft contact lenses and peripheral defocus spectacle lenses, with combination therapy often proving more effective than monotherapy.
Given these developments, I am prescribing RLRL for my highly myopic patients, as well as those who are rapidly progressing towards high myopia or continuing to demonstrate progression using mainstay myopia control treatments.
Examples of these patients include those who are progressing on even moderate-to-high doses of atropine well above 0.05%, and patients already treated with combined optical interventions with atropine. As RLRL is believed to involve a different mechanism to slow myopic progression, it is a promising new approach for treating these challenging patients.
Real world patient experiences of RLRL
Jagrut Lallu is a New Zealand-based optometrist and partner at Rose Optometry, as well as a clinical senior lecturer at Deakin School of Optometry. He has been active in myopia management for several years, acting as IMI ambassador for New Zealand and World College of Optometry Asia Pacific
ambassador for myopia. He was one of the first clinicians to start using RLRL in New Zealand, with now over 60 patients on the therapy and 20 that have been using it for over a year.
Generally, I have found RLRL to be well-tolerated by my patients and I have seen some fantastic results including axial shortening and sustained choroidal thickening.
In particular, I have found ideal results in patients who were progressing despite utilising myopia management options and as an adjunctive therapy for many of my patients on orthokeratology.
FIGURE 4. Line graph showing the adjusted mean changes (95% CI) in axial length from baseline to 12 months comparing orthokeratology alone to combination therapy of RLRL and orthokeratology in patients with annual axial length (AL) elongation of ≥0.50 mm despite undergoing orthokeratology.
Through the addition of RLRL, these patients have seen virtually no myopic progression and need not wear glasses during the day, which they have responded very positively to. This ‘glasses-off’ finding is similarly reported in two published studies of combination use of RLRL and orthokeratology, where in patients who had been using orthokeratology for 12 months with continued myopic progression, the addition of RLRL resulted in -0.10 mm and -0.02 mm axial shortening over the following 12-month period respectively. 8,9
FIGURE 5. Case study of the axial length progression of an eight-year-old patient in New Zealand on combination RLRL and orthokeratology.
In one case, I had been seeing an eight-year-old myopic boy on orthokeratology whose refraction had been controlled, but whose axial length was continuing to progress. In November of 2023, I therefore added on RLRL.
Since then, I have noticed slight reduction and later stabilisation of the axial length over the past year, with the child also exhibiting a 98% compliance to the treatment.
Speaking to the safety of RLRL, none of my patients have yet experienced any side effects. I am an advocate of regular follow-up and monitoring including OCT (which Eyerising International also recommends), finding it useful both from an efficacy perspective to see results from as early as the first month, and from a safety perspective for continued reassurance.
THE WAY FORWARD
Overall, RLRL represents a promising innovation in myopia control, with increasing international evidence supporting its efficacy and safety and steadily growing clinical uptake. Clinicians interested in trying out RLRL can be reassured of its maintained efficacy in international users, and
when looking for their first patients, may find greater success in difficult-to-treat patients, such as the highly myopic or treatment-resistant patients, where RLRL can be used either as a standalone or combination therapy.
There is also continued research ongoing into all facets of RLRL, including its long-term efficacy over three years or more, and a better understanding of its underlying mechanism and retinal effect. In the future, it is anticipated this will strengthen the position of RLRL as a key player in myopia management.
NOTE: References will appear in the online version of this article and are available upon request.
PanOptix®
• >3 million implants worldwide†§3 • 99% patient satisfaction4 Vivity® • >1 million implants worldwide†‡3 • The first and only extended depth of focus IOL with X-WAVE Technology#5-8
† Based on worldwide sales of AcrySof® and Clareon® IOLs.
‡ Based on worldwide IOL unit sales, 2023.
§ Based on Clareon® PanOptix® and AcrySof® PanOptix® sales 2023.
* Trademarks are the property of their respective owners.
# Based on in vitro examinations of glistenings, surface haze and SSNGs; as compared to Clareon CNA0T0, TECNIS* ZCB00, TECNIS* OptiBlue, Eternity* W-60 and enVista* MX60; n=30 per group; p<0.001.
References: 1. Alcon data on file, 2023; [REF-22137]. 2. Market Scope 2023 IOL Market Report; [REF-23630]. 3. Alcon data on file, 2024; [REF-24102] (available on request). 4. Modi et al. Visual and Patient-Reported Outcomes of a Diffractive Trifocal Intraocular Lens Compared with Those of a Monofocal Intraocular Lens. 2020 Sep 28;S0161-6420(20)30677-1. 5. Clareon Vivity Directions for Use; [REF-20979]. 6. Alcon data on file. US Patent 9968440 B2. 15 May 2018; [REF-03130]. 7. Alcon data on file, 2017. TDOC-0055576; [REF-09755]. 8. Bala C et al. Multi-country clinical outcomes of a new nondiffractive presbyopia-correcting intraocular lens. J Cataract Refract Surg 2022;48(2):136–143; [REF-17338].
HOYA has developed a lens design specifically for patients experiencing the first symptoms of presbyopia, spurring a whole new category that will allow independents to better serve the late-30s to mid-40s age bracket.
Often in life, it’s the grey areas that cause the most trouble. With no clear-cut choices, one can settle for a sub-optimal outcome. Some will rue the decision, while others will accept their situation and move on.
Welcome to the world of the early presbyope, an emerging and burgeoning patient demographic in their late 30s to mid-40s who, according to one lens manufacturer, have largely found themselves stuck without a vision correction solution that adequately meets their needs.
By 2030, millennials (Generation Y) will be the largest consumer demographic. As digital natives, they have grown alongside technological advancements, shaping a deep integration with digital devices. Now, as the oldest millennials enter their early 40s, their visual needs are shifting significantly.
It’s an issue lens manufacturer HOYA has been thinking long and hard about: how can the industry better cater for the current millennial crop when initial presbyopic symptoms set in?
In response, the company has created what it describes as a new lens category – and a potentially lucrative one that bridges an important gap in the lens market today.
Its new VisuPro All Day and VisuPro Flex advanced focus spectacle lenses are coming to Australia and New Zealand in early April 2025.
“The needs of young presbyopes are not being met in the market today,
“It means independents can offer an advanced lens design but it's pitched at a price point that's much lower than an entry-level progressive lens.”
Ulli Hentschel HOYA Lens Australia
and this is a category designed to bridge that gap, to ensure they’re able to access an advanced lens design specially designed for them,” says HOYA Lens Australia’s training and development manager Mr Ulli Hentschel.
The experience of the early presbyope sits in contrast to that of the fully-fledged presbyope, perhaps someone over 50, who has a raft of progressive lens, contact lens, or refractive surgical options. There’s even an eye drop approved in some countries.
For the early presbyope, the choices aren’t as obvious. With most people now spending an average of eight to 10 hours a day on screens, it may start with new vision challenges such as eye strain, blurred vision, and headaches during close work. It can be insidious, with many not realising the gradual decline in near vision and putting up with it for years.
Eventually, it becomes a source of daily discomfort affecting quality of life.
But once patients come to this realisation, barriers exist. As Hentschel points out, apprehension may creep in about the cost of jumping into progressive lenses, adaption concerns or the perception it’s a sign of aging.
Either way, he says early presbyopes often face a decision that leaves the patient and practitioner dissatisfied. That is, staying in single vision lenses, opting for entry level progressives, or even other options like anti-fatigue glasses.
There’s also the non-spectacle wearer, such as emmetropes, contact lens users, and post-refractive surgery patients, who now require near vision support for the first time. Other than readers, what can they reach for?
VisuPro All Day and VisuPro Flex have been designed with these two patient profiles in mind. And, importantly, they will be offered at a price point that sits between single vision lenses and an entry point progressive.
HOYA’s own research involving 7,043 people found 53% of existing spectacle wearers between 36 to 44 years have increasing problems seeing clearly in the near distance and when using digital devices.
“One of the big challenges in the presbyope market today is the significant jump in cost from single vision to progressive lenses,” Hentschel says.
“Even though they have been wearing glasses for a while and are familiar
Images: HOYA Lens Australia.
As the oldest millennials enter their early 40s, their visual needs are shifting, HOYA says.
with the costs involved there can be a tendency for them to choose a more basic progressive lens to make price less of an issue.”
In the same study referenced above, 60% of non-spectacle wearers in the 36 to 44 age bracket have near vision issues with handheld technology.
“This is the other category of people to consider. They have never required glasses at all, or perhaps they’re post-LASIK or have worn contact lenses, but they start realising their arms aren’t long enough to read their phone, or they struggle with the menu in a dimly lit restaurant,” Hentschel says.
“It's the first time they’re ever considering a pair of glasses, so talking about a pair of progressive lenses can be a shock to the system, especially when these patients would benefit most from a premium design to give them the most natural vision.”
These are some of the challenges HOYA’s VisuPro All Day and VisuPro Flex are trying to resolve.
“It means independents can offer an advanced lens design but it's pitched at a price point that's much lower than an entry-level progressive lens.”
And over a long-term horizon, the new lens design can ease the early presbyope into a progressive design when the time is right.
DISTINCT PATIENT PROFILES
When the optical engineers at HOYA were developing VisuPro All Day and VisuPro Flex, it was clear two distinct designs would be needed for the existing spectacle wearer and non-spectacle wearer, respectively.
VisuPro All Day, according to Hentschel, is for the classic myope who has required glasses for distance previously but is noticing a mild near vision deficit.
“We needed to create a lens that can work for them, because they are going to be wearing them all the time,” he says.
“It still gives priority to clear, uninterrupted distance vision, while providing an additional, low add in the near zone that supports their needs up close.”
With VisuPro Flex, the design has been varied with the understanding that patients wearing this lens – typically an emmetrope with early presbyopia –won’t be wearing their glasses all the time.
That could include activities like driving, or maybe they’re someone who wears plano sunglasses outside.
“This lens is more tailored to the near zone. It provides wider fields of view at near [compared with VisuPro All Day] and a lesser field view in the distance, but in saying that, these wearers can wear their glasses all day if they wish,” Hentschel says.
HOYA’s Binocular Harmonization Technology (BHT) underpins the design. It considers the prescription for the right and left eyes to “calculate and harmonise the prescription in the lenses for effortless focusing, stability and enhanced depth of vision for all wearers”.
Plus, Focus Max Optimization provides additional vision support at close
distance, which the company says allows sharper and more comfortable focus during near distance activities and digital usage. It can also help reduce eye strain or visual fatigue when working with digital devices – a benefit that over two-thirds of young presbyopic patients HOYA surveyed were highly interested in.
One question independent optometrists using HOYA lenses might have is how VisuPro differs from occupational and anti-fatigue lenses?
Hentschel says occupational lenses, such as HOYA’s iD Workstyle 3 product line, are geared towards more mature presbyopes who struggle at their workstations due to the narrow field in their existing progressives. They might require +2.00 D or more, and demand a wider field of view in the near and intermediate, switching back to their progressives once they leave the office.
But VisuPro is more tailored to those with a lower add demand, while still offering a distance power in the lens. Wearers can use them all day – a key difference.
In anti-fatigue lenses, these are configured around the wearer’s distance vision, with a small “boost” in the near zone at the bottom of the lens. Hentschel says these weren’t intended for presbyopes, but for people in their 20s and early 30s struggling with digital eye strain – headaches and sore and dry eyes temporarily – due to a high volume of near work.
“So they’re not actually presbyopic,” he says.
“The new category we’ve created can be thought of as a natural progression, taking those patients wearing anti-fatigue lenses five to 10 years ago – who are now in their mid-30s and early 40s and having issues with the first signs of presbyopia. VisuPro could be the next option that gives them that low add, near vision support.”
VisuPro All Day and VisuPro Flex will become available to Australian independents in early April 2025. HOYA coatings, including its premium Hi-Vision Meiryo Diamond technology, Sensity light adaption and polarisation are all optional extras that can be added to the lens.
Learning modules on the HOYA Learning Centre platform, and additional education will be provided in person when company representatives visit practices.
By bringing the lens into their practice, Hentschel says independents can demonstrate a more personalised service to a patient cohort who haven’t had their needs met adequately.
“Of course, it’s another way for independents to differentiate, but a key point is that it opens the door for practices to say to this age demographic that this is a product specially designed for you,” he says.
“This demographic is the next wave of presbyopes, there’s a huge volume on the cusp. They're all in the workforce now and so there’s a huge opportunity for both the practice and the patient to get a lens solution they’re extremely satisfied with.”
VisuPro All Day and VisuPro Flex have been designed with two patient profiles in mind.
The golden touch
ZEISS has developed its first premium-tier coating, setting new standards in cleanability, durability and clarity along with a new aesthetic ‘hue’.
How can I stand out and create that personal touch? It’s one of the big challenges of running an independent optometry practice in 2025, and a question many spectacle wearers have themselves. Today, practices have access to a host of instrumentation, frame collections and lens designs that can give their business an edge while ensuring the patient walks out the door with a lasting impression.
Within that, many are discovering new opportunities with lens coatings that are meeting new demands for anti-reflection, smudge resistance and durability, while incorporating elements for aesthetic appeal.
ZEISS DuraVision Gold UV lenses, a new coating available to the Australian market from 1 April 2025, has been designed to address these requirements.
For the first time, it extends the company’s lens coating portfolio to the premium tier, offering “greater cleanability, durability and clarity” than its existing DuraVision coatings.
To boot, it features a subtle golden reflex hue “for a luxurious look”. For practices it represents new upselling opportunities and ways to confidently help patients personalise their appearance, by matching the lenses with certain frame designs and skin complexions.
To understand the features and benefits patients prioritise in their lenses, and inform its new coating design, ZEISS conducted a consumer study with 19,800 participants across 18 countries.
Maintaining clear vision at all times came out on top, while smudge resistance and a lens that is easy and quick to clean were other important factors. Some expressed that if they must wear spectacles, they want them to enhance their individual look.
“It is of utmost importance for independents to be able to offer a premium coating today that will meet the expectations of their consumers,” says Ms Elmarie Pretorius, professional services manager for ZEISS Vision Care Australia & New Zealand.
“ZEISS DuraVision Gold UV allows ZEISS customers to offer a unique coating that offers exceptional clarity, durability and are easy to clean but also customise their look and style. It meets consumers’ expectations, delivering solutions that combine clear vision with bold, stylish design.”
Introducing ZEISS CleanGuard, a new technology, has helped elevate ZEISS DuraVision Gold UV as its new flagship coating.
This advanced surface chemistry features a modified molecular structure “that significantly increases contact angles of water drops and oil-like
“ZEISS
DuraVision Gold UV allows ZEISS customers to offer a unique coating that offers exceptional clarity, durability and are easy to clean but also customise their look and style.”
Elmarie Pretorius ZEISS Vision Care
The new coating features a subtle golden reflex hue “for a luxurious look”.
substances”. Compared to previous ZEISS coatings, this makes lenses up to three times faster to clean, adding a convenience factor for wearers. Additionally, a patented anti-static layer repels dust and dirt. It means smears and smudges can be removed much faster and easier. It’s an improvement that 90% of consumers have also noticed and appreciated, ZEISS says.
Pretorius says R&D labs across many countries, including ZEISS’ South Australia facility, have played a part in the development and testing of CleanGuard technology and the ZEISS DuraVision Gold UV coating itself. Durability has been a big part of the testing phase, with ZEISS DuraVision Gold UV lenses coming with big improvements in this area.
They are designed to stay scratch-free for longer thanks to multiple densely packed metal oxide layers combined with an extra hard coat to ensure high-level scratch resistance.
This gives ZEISS DuraVision Gold UV a notable score of 16 for the Bayer industry standard test for scratch resistance. To put this in perspective, a Bayer ratio above 10 is considered very high, the company says.
SHINING IN LOW LIGHTING
While a golden residual reflectance on the lens surface can add a tasteful touch to the lens (more on this later), it also offers a better visual experience.
To demonstrate this, ZEISS refers to a scenario: Imagine an evening stroll or enjoying a drink in a bar with subdued lighting. In this and other low-light conditions, eye sensitivity shifts towards shorter wavelengths into the blue light spectrum – and for the human eye, seeing clearly gets harder.
Now, in such circumstances, the company says patients choosing ZEISS DuraVision Gold UV may perceive noticeably enhanced vision performance.
The reason is that compared to lenses with blueish or greenish coatings –such as ZEISS’ DuraVision Platinum UV or DuraVision Chrome UV – ZEISS DuraVision Gold UV shows less reflectance in the specific light spectrum between 380-500 nanometers.
By reducing reflections on the lens surface, ZEISS DuraVision Gold UV offers higher transmission and hence clearer vision – especially when it gets dark.
Images: ZEISS.
With this in mind, who are the ideal candidates for the coating?
Pretorius says ZEISS DuraVision Gold UV can be recommended to any patient from single vision to progressive wearers. Those struggling in low light conditions would especially benefit “as the darker the environment the clearer the lens”.
“ZEISS DuraVision Gold UV shows up to six times lower blue light reflections. As a consequence, lenses appear less yellow and much clearer in see-through,” she says.
“The up to 90% lower yellowness compared to blueish ZEISS DuraVision coatings becomes explicitly visible in modern artificial LED lighting when looking at a white wall or bright monitor screens.”
A SIGN OF SOPHISTICATION
When consumers look for timeless, sophisticated eyewear, gold is a colour they often reach for.
With ZEISS DuraVision Gold UV, ZEISS has been able to incorporate an appetite for this colour into the lenses themselves.
Pretorius says the golden residual reflectance on the surface of lenses can significantly enhance their aesthetic appeal and complement various elements.
For example, she says they can beautifully complement frames in shades of gold, brown, and even black.
“The subtle golden reflection can also enhance certain complexions, including various skin tones and hair colours,” she adds.
“The golden reflectance can work well with specific sun prescription tints. And when using ZEISS PhotoFusion X lenses, the golden anti-reflective coating becomes more pronounced when the lenses are activated by sunlight. This feature can improve the aesthetic appeal as the lenses adapt to different lighting conditions.”
ZEISS DuraVision portfolio – tailored solutions to meet consumer needs:
• ZEISS DuraVision Gold UV – a premium tier coating incorporating ne w ZEISS CleanGuard technology, offering exceptionally clear vision with better cleanability, upgraded scratch resistance and a subtle golden reflex hue for a luxurious look. Enhanced lens clarity in low-light conditions, and diminished lens yellowness through the lens are other features.
• ZE I SS DuraVision Platinum UV – a top tier coating featuring a light blue hue with the lowest reflection in daylight conditions
• ZEI SS DuraVision Chrome UV – an entry tier coating featuring a light green hue
• ZEI SS BlueProtect UV – special usage for blue light protection.
for Dry Eye relief
A new technology has elevated ZEISS DuraVision Gold UV into ZEISS' flagship coating.
iCare EIDON presents a more colour-balanced retinal image with greater richness allowing for improved discriminative power and diagnostic accuracy, providing a precise documentation of retinal structures.1
1 Fantaguzzi, F., Servillo, A., Sacconi, R. et al. Comparison of peripheral extension, acquisition time, and image chromaticity of Optos, Clarus, and EIDON systems. Graefes Arch Clin Exp Ophthalmol 261, 1289–1297 (2023). https://doi.org/10.1007/s00417-022-05923-z
Enviable results
Perth ophthalmologist A/Prof ROB PAUL explains why the latest diffractive intraocular lens design from Bausch + Lomb has him reconsidering his approach when patients come seeking spectacle independence.
At a time when all the buzz in cataract surgery is centred on so-called extended depth of focus (EDOF) intraocular lenses (IOLs), Western Australian ophthalmologist A/Prof Rob Paul has made a lens with a diffractive anterior surface his new go-to in presbyopia correction.
While the ability to see from near to far has been the major drawcard of diffractive designs, the not-fully-resolved issue of glare, haloes and starbursts – as EDOFs improve – has seen some recent favouritism towards the latter category.
But the new enVista Envy hydrophobic acrylic IOL from Bausch + Lomb has A/Prof Paul rethinking the way he goes about cataract refractive surgery. The “full range of vision” lens just became available to Australian surgeons, with A/Prof Paul having implanted 12 at the time of writing – the most of any surgeon in Australia.
He’s always treated new multifocal IOLs (although B+L doesn’t refer to enVista Envy this way) with caution. But was surprised to see patients with this IOL read small print, along with 6/6 to 6/9 distance vision and little to no visual disturbances one day post-operatively. The results have also been backed up in one-month follow-ups.
“It would definitely be my first choice lens for anyone wanting presbyopia correction at this point in time,” he says.
“Often ophthalmologists in the general sphere want a lens that's not going to cause any issues for them later down the line – and that's where this lens comes to the fore.”
Based on the enVista platform, B+L has made improvements in the optical design in developing the enVista Envy.
The “enviable” dysphotopsia tolerance is a major selling point. Fourto-six-month data out of the US involving more than 300 people found 88% had little to no bothersomeness with glare, 80% with haloes and 91% with starbursts. The numbers were even better in a Canadian study: 96%, 88% and 94%, respectively. 1,2
For a competing trifocal in a separate study, those numbers were 72-73%.
In terms of the range of vision, the lens offers 4.00 D of continuous vision, 4 with the US studying showing 79% of patients achieved N4 (near), 91% 6/7.5 (intermediate) and 85% 6/6 (distance) – all in bilateral photopic conditions.1
The Canada study demonstrated the near-vision benefits, with 91% reporting little to no difficulty reading a mobile screen and 95% when reading a computer screen. 2
“As the technology has evolved, my general feeling is most Australian patients, whilst they want spectacle independence, maintaining distance vision is very important, as well as minimising anything like glare and haloes – we want it all,” A/Prof Paul says.
“This is where a lens like this appeals, because it gives the full range of vision and it's got a very high tolerance to dysphotopsia – it surprised me.”
Some crucial design has enabled this, and A/Prof Paul has been impressed with the results in patients implanted bilaterally with enVista
Envy. Others have received an off-label mix of enVista Envy in one eye, with an EDOF implanted in the dominant eye.
“I performed my own glare and haloes test on patients with a pinpoint source of light, and we actually saw greater starbursts in the EDOF design – there was no dysphotopsia symptoms that we could see with the enVista Envy one month post-op.
“I am waiting for more data to see if bilaterally implanted patients are getting any significant glare and haloes, and if it continues as I predict, I'll routinely implant it bilaterally.”
A/Prof Paul says a common fear preventing some ophthalmologists from fully embracing diffractive designs is the residual refractive
The lens features propriety technology called ActivSync designed to reduce light scattering.
Image:
Dr Rob Paul.
Perth’s Dr Rob Paul has had early access to Bausch + Lomb’s new enVista Envy IOL.
Image: Bausch + Lomb.
NEW DEPTHS IN ASTIGMATISM CORRECTION
Another drawcard for Australian surgeons – who have a particularly high toric implantation rate 6 with estimates ranging from 30% to more than 50% – is the new features to address corneal astigmatism.
B+L has introduced Low-Cyl technology, helping surgeons broaden the treatable astigmatism range to as low as 0.9 D at the IOL plane.7 It’s the first and only full range of vision toric platform that can offer this, according to the company.
It’s important considering 74% of cataract patients have less than 1.25 D of corneal astigmatism. 8
At the other end of the spectrum, the maximum available cylinder on enVista Envy is -5.75 D at the IOL plane, and it’s reported to be the only toric platform that treats in half-step cylinders (up to 3.50 D at IOL plane).
“In my experience, and the studies have shown, anything above 0.7 D is worth treating with a toric IOL, and most of my enVista Envy patients have had some sort of toric correction. It leads to less aberrations, better distance vision, and certainly ensures the lens is better tolerated overall,” says A/Prof Paul.
He adds that a longstanding benefit of the enVista platform is its rotational stability and toric alignment, with 110-degrees of capsular bag contact, and 300% more radial compression force than traditional hydrophobic IOLs.10
All up, 94.4% of eyes had less than five-degrees of rotation, which B+L says equates to proven rotational stability through 180 days post operatively. 8
The rotational stability is aided by fenestrated holes in the enVista Envy Toric, simplifying lens manipulation during surgery, allowing both clockwise and counterclockwise positioning in the capsular bag.11
“I’ve also found it leads to less optic stress on the capsular bag,” A/Prof Paul adds.
O ne of the big reasons A/Prof Paul has used the enVista platform
“In my experience, and the studies have shown, anything above 0.7 D is worth treating with a toric IOL, and most of my enVista Envy patients have had some sort of toric correction. It leads to less aberrations, better distance vision, and certainly ensures the lens is better tolerated overal.”
error causing a wax-like distance vision. But he hasn’t seen that with enVista Envy.
“When you get better reading, you expect a reduction in distance vision, but I’m not seeing that. In addition to being 6/6 to 6/9 for distance vision, my patients have been N5 to N6 for up close, monocular,” he says.
“But the shocking finding for me has been the minimal glare and haloes, and after speaking to the company I’ve understood why; it’s due to their proprietary technology which is akin to graduated steps on the diffractive rings, lessening the amount of light scattering.”
This propriety technology is part of a new optical design that B+L calls ActivSync. It is designed to enhance image contrast when patients require it most, evenly distributing light in photopic (well-lit) conditions and prioritising distance in mesopic (low light) conditions. 5
“When you look at the defocus curve it’s a very flat line, from about zero to -3.00 D, so it doesn't deviate much like multifocal lenses might,” Dr Paul says.
“That’s part of the reason why the vision is quite good for distance. And with the ActivSync optics, this leads to an even energy distribution of light. So in dimmer conditions, when the pupil is greater than 4 mm, it prioritises distance.
“That's one of the special features of this lens, it’s why the distance vision is still quite good, even in the low contrast conditions.” 1-3, 5
traditionally is its glistening-free material, the only IOL of its kind with this FDA indication.
Now, enVista Envy features glistening-free material with improved scratch resistance and 25 times the hardness of traditional hydrophobic IOLs.12
At the same time, one aspect B+L has been keen to improve is the unfolding time of the enVista, which it has achieved in recent years with a change to the material.
It’s something A/Prof Paul can attest to.
“I’ve noticed the change in the fabric of the actual lens – and have had no problems with the unfolding time,” he says.
B+L’s SureEdge design is also an appealing feature, helping the surgeon against posterior capsular opacification.14, 15
“The fact it’s a hydrophobic IOL is another huge benefit for me because a lot of the other lenses out there that I would deem competitors are hydrophilic that have the potential to opacify over time,” he says.
“All in all, I’ve been pleasantly surprised, especially in the way it has performed offering excellent near vision results while few, if any, dysphotopsia symptoms in the cases I’ve performed so far.”
NOTE: References are available upon request and will appear in the o nline version of this article.
The enVista Envy Toric means surgeons can broaden the treatable astigmatism range to as low as 0.9 D.
Image: Dr Rob Paul.
Is your vision becoming blurry up close?
Bring your world into focus with VisuPro: advanced focus spectacle lenses
VisuPro advanced focus lenses are specifically tailored to the unique visual needs of patients in their late 30s up to mid 40s experiencing first presbyopic symptoms. It provides them with a rejuvenated vision experience, sharp vision and comfortable focus across all distances all day long.
To learn more about VisuPro spectacle lenses, contact your HOYA Sales Consultant or free call 1800 500 971.
LEI initiative for greater access
People living in the east of Perth’s vast metropolitan area have little or no access to public eyecare services, resulting in dire consequences for some. Lions Eye Institute is hoping to fix this with an intriguing initiative.
Ms Gaela Hilditch’s battle with glaucoma began with a squash ball – the one that hit her in the eye.
That was more than 50 years ago, but the journey from there to now, as she recovers from eye surgery in her West Australia home, is sadly indicative of the long slog many people go through to have their eye issues recognised and fixed.
It’s a problem that WA’s Lions Eye Institute (LEI) is hoping to solve with a new glaucoma collaborative care initiative that gives patients faster, better access to eye care and preserves or improves their sight.
Hilditch’s problems didn’t seem too bad in the immediate aftermath of her scrape with the squash ball, but she then started having problems with her vision.
Opticians in her home country, Britain, were unable to detect any issues and simply prescribed eye drops.
Fast-forward 25 years to Perth, where ophthalmologist Professor Bill Morgan established that she had trauma-induced glaucoma.
Incredibly, Hilditch says that she’s one of the lucky ones.
Her surgery was covered by private health insurance and the 74-year-old is now on the road to recovery and improved vision.
That’s not possible for everyone in Perth, particularly people who are outside the central Perth area and quite some distance from the only public eyecare facility at Royal Perth Hospital. Added to this, most glaucoma sufferers are over 60.
Hilditch is involved in a Consumer Engagement Committee, in which people shared sometimes desperate stories of inequities in access to eyecare and glaucoma treatment in WA.
“They’re older, they’ve got disabilities, they are very vulnerable,” Hilditch says. “They’ve got to go all the way into Perth. They can’t find a park, and they can’t necessarily even drive, because they are partially blind.
“Some of them are waiting a whole year to be seen and, in the meantime, they’ve lost even more vision.
LEI is hoping to address many of these issues in its initiative.
It has teamed up with the University of Western Australia and Royal Perth Hospital (RPH) to bring top-quality glaucoma services combined with optometry services to sufferers in parts of the city with limited access to public and private eyecare.
Morgan, a professor of ophthalmology at the university and a consultant ophthalmologist at LEI and RPH, has seen how this poor access to timely services over many years has played out unhappily for patients.
“The biggest challenge has been the increasing division between, if you like, private eyecare provision and the public clinic provision,” he says.
“The metropolitan area is essentially divided, with the western area of
“The
appointment times were much faster, the number of people waiting for an appointment plummeted, the cost of providing the service was significantly less and patient satisfaction was much higher – it was a case of win, win, win.”
the city facing the ocean having good access to services and then once
“People in the eastern parts of the city have really limited access to eyecare, particularly if they can’t afford private eyecare or are deterred
He says the collaboration will help to address these long-standing
The initiative has earned a $276,000 grant from the WA state government as part of its $4 million program of support for innovative projects to address health priorities.
“When we applied for the grant, which was about May or June of 2023, there were already large numbers of glaucoma patients who were ‘over boundary’, meaning they had gone past the recommended four- or six-month appointment time, and they hadn’t been seen,” Prof Morgan says.
To help fix this, students from the university’s Doctor of Optometry program – which opened in 2021 – will be part of the solution at the LEI clinic at Midland, in Perth’s eastern corridor.
Supervised by a senior lecturer experienced in glaucoma, they will process various scans and tests, with an initial focus on those patients who have been waiting the longest for their next appointments or who appear to have fallen out of focus.
“The senior lecturer and students will make a decision on the patients and prepare a report saying this patient’s got this type of glaucoma, consistent with the information they received, and it’s either stable or may have progressed, and then we recommend ‘X’ follow up,
Prof Bill Morgan Lions Eye Institute
Image: Frances Andrijich/LEI.
Professor Bill Morgan examines a patient.
Image: Frances Andrijich/LEI.
including at the Midland clinic,” Prof Morgan says.
The team will co-ordinate with RPH to provide more specialist follow-up treatment and ophthalmology services for those patients who need it. Patients return to Midland if their condition is stable and follow-up tests are needed.
“It’s a triaging process, if you like, filtering patients who genuinely require ophthalmology input and assessment, instead of trying to channel them all through a narrow funnel into Royal Perth Hospital, which struggles to cope with the volume.”
The state grant will help to cover the extra administrative support needed at Midland and RPH, and the extra time invested by the supervising senior lecturer and students involved. It will also help cover the role of a senior registrar, who will vet the work and ensure the right clinical decisions are being made.
The hope is that the collaboration, set to start in the next couple of months, will reduce the burden on the stretched health system and ease the journey for glaucoma sufferers.
But the optometry students will also benefit, Prof Morgan says.
“We will be supporting the optometry program while at the same time helping to improve eyecare services in Perth and introducing students into that demographic where the need is greatest.”
If the collaboration is successful and the funding continues, the plan is to move the focus from glaucoma to other eye conditions like macular degeneration and paediatric myopia.
VF2000 NEOPORTABLE VISUAL FIELD ANALYZER
The New Standard in Visual Field Testing
V irtual Reality Visual Field device - incorporates complete Visual Field analysis.
Detailed progression analysis and the most versatile & efficient vision screening technology. Latest technology provides the same reliability and reports as the “gold standard”.
Prof Morgan is confident the success will be the same as the C-Eye-C program in New South Wales,
“It’s an idea that originally came from England and was taken up by Professor Andrew White at
“Westmead, a western suburb of Sydney, is like a corollary to the eastern suburbs in Perth and the same problems of large numbers of over-boundary patients was occurring at Westmead Hospital.
“Professor White established the C-Eye-C program, with university optometry academics and hospital staff collaborating to create a new service. Patients with glaucoma who were thought to be relatively stable at Westmead Hospital had their follow-up visit at the C-Eye-C facility, taking pressure
“They found that the appointment times were much faster, the number of people waiting for an appointment plummeted, the cost of providing the service was significantly less and patient satisfaction was much higher, because they didn’t wait so long in the clinic to be seen when they were assessed.
Supplied complete with a Tablet PC –BlueTooth interface with the VF2000 NEO.
Compact/Space-saving/Portable - can be used anywhere, no need for a darkened room.
Active eye tracking –enhances reliability.
Full and Fast Thresholds VF Testing plus Neuro, Kinetic, Ptosis and Esterman tests FDT Testing
Stereopsis Visual Acuity and Contrast Sensitivity
Colour Testing (Ishihara, D15 and Advanced Colour Tests) Eye Mobility and Strabismus
It was 25 years after Gaela Hilditch was hit by a ball in the eye that she was diagnosed with trauma-induced glaucoma.
Image: Gaela Hilditch.
Meet Kirsty Banfield
B.Sci(Optom)
According to Kirsty Banfield, our optometrist partner at George & Matilda Eyecare for Mt Martha Optical, “every pair of eyes is a puzzle”. That explains why, even after 40 years, she still loves her profession. “I like people… I now see kids of patients who used to be kids. I like the allied health aspect of our industry and how there have been changes and progression in technology, helping improve the prevention of eye disease”.
Kirsty always had the ambition to own a business and in 1998, she grabbed the opportunity to buy Mt Martha Optical, in the Mornington Peninsula in Melbourne, building it into a successful practice known for its outstanding level of patient care.
“We have seen growth in our practice since we joined G&M. This has been due to their marketing focus, investment in new equipment and staff who support us everyday.”
Kirsty first met Chris Beer, George & Matilda’s founder and CEO, during a business trip. Over the next couple of years with a delay during COVID, Mt Martha Optical joined G&M and was successfully onboarded in December 2020. “I felt the timing was right and the fit was right. Our ideals are the same. G&M is about being patient first and this aligns with my values. I also wanted to plan my retirement well in advance, and I knew that with G&M, my staff would be looked after, today and in the future”.
Seeking sweet relief – Identifying and managing dry eye in patients with diabetes
Diabetes increases the risk of dry eye disease (DED), impacting vision and quality of life. MEGAN ZABELL explores the key mechanisms behind diabetes-associated DED, evidence-based management strategies and the pivotal role of the optometrist.
Secondary dry eye – what is it? Secondary dry eye is simply dry eye that has developed as a consequence or complication of an underlying condition.1 This can include iatrogenic dry eye, which is dry eye induced by medication or a medical or surgical procedure. Examples of medications or procedures identified as a risk factor of dry eye include: hormone replacement therapy, refractive surgery, antihistamines, and antidepressant medications.2
Systemic health can also impact the risk of having dry eye disease (DED) – diabetes mellitus is one of the leading systemic risk factors for dry eye disease.3
The interaction between diabetes mellitus and DED is quite a complicated one. Diabetes affects almost one in 10 adults aged 20-79 worldwide,4 causing elevated blood glucose due to insufficient insulin production (Type 1) or insufficient insulin sensitivity (Type 2).
There are a number of key features of diabetes mellitus which contribute towards elevated risk of DED.3 Some of the features of diabetes mellitus that can contribute to this risk include chronic hyperglycaemia, diabetic peripheral neuropathy, decreased insulin levels, microvasculopathy and systemic hyperosmotic disturbances; these can lead to lacrimal unit dysfunction, tear film dysfunction and abnormal tear dynamics, ultimately contributing to DED.3
Management of diabetes mellitus is commonly centred around diet and exercise, glucose monitoring, insulin supplementation and the use of non-insulin antidiabetic medications like metformin. However, evidence suggests that the use of metformin may, itself, increase the risk of diabetes-associated DED. In a study looking at
LEARNING OBJECTIVES:
At the completion of this article, the reader should be able to improve their management of dry eye disease, including:
• Define secondary dry eye and its relationship to systemic conditions like diabetes.
• Recommend appropriate lubricants and treatment strategies based on tear film deficiencies.
• Integrate a preservative-free, multi-dose solution into dry eye management plans for improved patient outcomes.
patients with and without diabetes and the various risk factors for dry eye it was found that among the patients with diabetes, 82.6% of patients with dry eyes (n = 46) were metformin users, compared to only 54% of the group without dry eye (n = 74). This is a statistically significant difference between the groups (p<0.001), indicating that metformin use is a risk factor for DED, above and beyond the pre-existing risk of having diabetes.5 While it is difficult to specify the prevalence of diabetes-related DED (D-DED), a meta-analysis of four case-control studies found that the risk of DED was 30% higher in patients with diabetes as compared to control (patients without diabetes).6
Both DED and diabetes represent a threat to a sufferer’s quality of life (QoL). Patients with Type 2 Diabetes (T2D) have been identified as having inadequate health-related QoL in the following areas: physical function, social functioning, mental health, emotional health, vitality and body pain.7
Similarly, DED markedly undermines patients’ QoL in areas including: physical function, activities of daily living, workplace productivity, social functioning and mental health.8 DED has also been associated with increased self-assessed depression score,9 and patients with DED commonly report anxiety symptoms (37.2%) and disorders (11.4%).10 It has also been demonstrated in the literature that symptoms of DED are associated with reduced QoL in both Type 1 Diabetes (T1D) and T2D, irrespective of whether the patient has diabetic retinopathy.8
There are a number of structural changes that occur to the tear film in diabetes. Peripheral neuropathy and hyperglycaemia have been identified as the leading cause of some of these structural
FIGURE 1. The complex interaction between diabetes and DED.3
changes.11 Most components of the tear film and ocular structures that are vital to the tear film can be affected by changes that occur during diabetes:
Aqueous changes
• Hyperglycaemia can lead to microvascular damage to the lacrimal gland, and diabetic peripheral neuropathy is associated with impairment of lacrimal innervation, which both contribute to diminished tear production (corneal sensitivity and diminished reflex tearing).11
Mucin changes
• Corneal hypoesthesia can cause decreased mucin production by goblet cells, which leads to reduced tear film stability.11
Lipid changes
• Decreased corneal sensitivity, which reduces the blink rate, leads to the destabilisation of the lipid layer of the tear film and results in increased excess evaporation. Insulin is essential for the desired sebaceous gland activity and is known to induce glandular cell proliferation and lipid secretion. Hyperglycaemia has been shown to contribute to lipolysis in adipocytes. Hyperglycaemia could lead to morphologic changes and a gradual loss of meibomian gland epithelial cells.11
Meibomian gland changes
• Patients with diabetes have been observed to have higher meibomian gland scores, lower meibomian gland expressibility and lid margin abnormalities.12
Epithelial changes
• Diabetes mellitus can cause alterations in the corneal epithelial basal cells and basement membrane, leading to corneal epitheliopathy and adhesion disorders. Loss of corneal nerves in diabetes mellitus leads to reduced neurotrophic support, resulting in accelerated loss and reduced proliferation of epithelial cells. Diabetes mellitus also causes the production of the abnormal basal lamina and inadequate adhesion of epithelial cells to an
abnormal basement membrane.11
In the case of patients with diabetes, early diagnosis and effective treatment of DED are essential to avoid the risk of complications.3 Making a diagnosis of DED and forming a management plan can be done as in cases of DED not related to diabetes, one useful resource is the Tear Film and Ocular Surface Society (TFOS) Dry Eye Workshop II Report (DEWSII).13,14 There is also synchrony in the management strategies applied for both diabetes and DED. Several important elements of diabetes management also support optimal management strategies of DED15,16 – for example, adequate glycaemic control which reduces the risk of microvascular complication in diabetes17 also improves corneal nerve health.15
Adequate systemic hydration is important for patients with diabetes, who may be at greater risk of dehydration,18 and ensuring adequate systemic hydration also supports proper tear production for DED.15 Similarly for patients with diabetes, weight loss improves glycaemic control, reducing the need for glucose-lowering medications19 – a higher body mass index (BMI) has also been linked with metaplasia and goblet cell loss in DED.15 A further important element that links diabetes management and DED management is aiming to maintain optimal insulin levels – while insulin deficiency is a defining feature of diabetes mellitus, adequate insulin mediates healthy epithelial cell metabolism crucial for ocular surface health.15
The management for DED secondary to diabetes follows the same principles as laid out by the four-step management algorithm in TFOS DEWSII,14 with the incorporation of some of the concepts mentioned in the preceding paragraph. After triaging dry eye symptoms and establishing that the tear film exhibits a loss of homeostasis indicative of DED, the dry eye can then be subtyped into aqueous-deficient dry eye (if the mucoaqueous layer of the tear film in insufficient), evaporative dry eye (if the lipid
layer of the tear film is insufficient causing increased evaporation rates), or a mixed type of dry eye that exhibits signs of both subtypes.13 As identified, patients with DED and diabetes may have either (or both) layers of the tear film affected, so the tear film should be carefully assessed when designing a DED management strategy.
If a DED sufferer has insufficiencies in both the lipid and mucoaqueous layers of their tear film, a sensible management strategy would be, among other therapies if needed, recommending an ocular lubricant that supplements both layers of the tear film to avoid the potential burden that needing to use multiple drops could cause. As identified by TFOS DEWSII it is recommended to use a lipid-containing tear supplement in the case of the DED having an evaporative component,14 something that is supported by clinical evidence.20 In a six-month multicentre, double-masked randomised controlled trial it was found that both lipid-based and non-lipid based tear supplements improved mild-moderate cases of DED, yet the evaporative cases benefited preferentially from lipid-based supplementation.20
A Phase 4, multicentre, open label interventional study investigating the effects of a combination lipid and aqueous lubricating eye drop on symptoms of DED for patients who had evaporative, aqueous deficient, or mixed subtypes of dry eye found that the propylene glycol-hydroxypropyl guar nanoemulsion that is Systane COMPLETE provided immediate and sustained relief of DED symptoms across all subtypes of dry eye.21
Patients with diabetes who attend for eye tests require thorough examination due to the potential ocular complications. One that can’t be neglected among these potential ocular side effects is dry eye – dry eye secondary to diabetes can affect either or both layers of the tear film. Management recommendations for dry eye secondary to diabetes is equivalent to other dry eyes – one consideration for a tear film that has either or both layers affected could be Systane COMPLETE Lubricant Eye Drops, which has been shown to address the symptoms of evaporative, aqueous deficient, and mixed dry eye for up to eight hours.21 It is available in a multi-dose preservative-free bottle that can be kept for up to three months after opening.
NOTE: References available upon request and will appear in the online version of this article. The author is a paid employee of Alcon.
FIGURE 2. TFOS DEWSII Recommended Diagnostic Approach for Dry Eye.13
A new era in slit lamp tonometry
The world’s first slit lamp mounted rebound tonometer
A highly accurate and reliable technique
Enhanced patient comfort and ease of use
Also available: IC100 and IC200 handheld tonometers.
Experience the world’s first slit lamp mounted rebound tonometer.
Looking globally, acting locally
The 2025 ODA conference offered plenty of advice from international speakers that attendees can use in their own practices. Insight was there to take in the world view and the growth of local optical dispensing.
History was on the minds of many during the 2025 Optical Dispensers Australia (ODA) International Conference in Sydney.
As the event kicked off, Cyclone Alfred, the biggest storm to hit Queensland and northern New South Wales in decades, was making landfall and prevented about 20 people from making the trip south to the InterContinental Sydney on 7-8 March.
But the show went on, and did so in record-setting fashion, according to ODA CEO Ms April Petrusma’s introduction during the first day and the event gala later that evening.
She told those gathered that, in its third year, ODA was delivering the biggest event ever to celebrate optical dispensing in Australia, with more than 300 people at its gala.
They were also celebrating a record number of graduates, with 239 having completed the Australasian College of Optical Dispensing (ACOD) Certificate IV in Optical Dispensing course in 2024, and another 45 in New Zealand.
That and the louder voice of ODA were huge successes for not only the industry but also the organisation, she said.
“We are three years old now,” she said, “and the feedback received . . . is that we’ve really made some waves.”
Those waves had been felt beyond Australian shores.
As well as advocating for optical dispensers, organising conferences, webinars, lens lab tours, and hands-on workshops, ODA had facilitated important outreach work. In July 2024, Petrusma and 12 eyecare professionals “provided vision screening, eye education and free glasses to isolated communities in the Fiji Islands”.
“We screened more than 1,300 people and dispensed more than 400 pairs of glasses,” she said, highlighting a silent auction to raise funds for its next volunteer project.
“As an optical dispenser you play a crucial role in shaping the visual outcomes of every single person that you serve."
Post-event, Petrusma told Insight “the level of engagement from across the industry and success of the conference highlights ODA's important role in driving progress within our field”.
“In an unregulated profession, it was extremely encouraging to see a full room
of delegates, all there to learn and nurture their own professional development.”
She said the two-day program provided an “invaluable opportunity” to connect with global industry leaders, whilst learning about the latest technologies and advancements in optical dispensing.
DISPENSERS WILL NEVER HAVE ‘CRISIS OF CONSCIENCE’
History was also top of mind for the gala event’s keynote speaker, George & Matilda Eyecare founder, CEO and managing director Mr Chris Beer.
He told the graduates that they would never have a day in their working profession when they would experience a “crisis of conscience and feel like you don’t have a purpose”.
“It’s about making a real difference in people’s lives with every pair of glasses that you fit. It’s a privilege to do what we do every day.”
But much had changed in the 40 years since he had started in the industry as an optical dispenser and mechanic.
And more was to come.
“The one thing I can tell everyone in this room today is that the changes over the last 40 years that I’ve seen will seem like a mere blink of an eye compared with what’s coming now,” he said.
“We are living in the most exciting, transformative period of human history. Embrace it, jump on board and come along for the ride.”
He left the audience with a couple of thoughts: “Always say ‘yes’ to every opportunity that presents itself – you are always better off being a generalist than a specialist; and always give back more than you take.”
ADVICE FROM AROUND THE GLOBE
If Beer was keen to promote a diversity of skills and knowledge, there was plenty on offer from the international speakers at the two-day event, with experts from Germany, Fiji, Scotland, and France, as well as around Australasia.
And due to the cyclone and the absence of one of the Queensland speakers, Petrusma organised an expert panel for a Q&A session, thought to be an Australian first. Panelists represented all major lens suppliers in Australia, giving the audience a rare opportunity to ask questions and learn from all the major suppliers in one place.
The main education program kicked off with an update on myopia.
Professor Padmaja Sankaridurg, the head of global myopia management at ZEISS Vision Care, told those attending that the most recent research suggested eyecare professionals were likely to get a lot busier in the coming years.
Images: Prime Creative Media.
Scottish dispensing optician Fiona Anderson has everyone’s attention during her presentation on how to deal with children and their entourages.
ODA CEO April Petrusma addresses the audience during the gala evening.
ODA EXCELLENCE AWARDS WINNERS
Rookie of the Year Award:
Rhian Hobbs, Wills Street Eyecare in Bendigo, Victoria.
CEO’s Member Dedication Award: Keren Peet, 20/20 Sight and Style Optometrists in Mornington, Victoria.
Outstanding Practice Owner Award: Barry Telfer, Angelo Street Optical in South Perth, Western Australia.
Role Model and Leadership Award: Rayleen Tamblyn, ACOD and Specsavers in Erina, New South Wales.
Community Champion Award: Lyn Simeon, Teachers Health Centre in Parramatta, New South Wales.
ODA National Medal for Optical Dispensing Excellence: Dominique Jorgensen, The University of Western Australia Optometry and Vision Science School, Western Australia.
ABOVE: Dominique Jorgensen (right) won the ODA National Medal for Optical Dispensing Excellence. She is with ODA CEO April Petrusma, and Todd Spencer of CR Labs.
The prevalence of myopia in adults currently was much less than that in children, she said. But that was likely to change significantly in the next two decades, with today’s large number of myopic children becoming myopic adults and prevalence in children likely to rise, with recent evidence indicating that in China alone, prevalence in those aged 0-19 was tipped to hit 60% by 2030.
That was why there was a growing focus on stopping young children from becoming myopes in the first place, with China setting a number of targets and health authorities in the US looking to declare myopia as a disease, to allow more options and support from policy-makers and other related bodies.
Prof Sankaridurg said the burden of myopia had become “quite substantial” and would only increase in future.
She said recent work had focused on young and pre-myopic children. Whilst research had promoted outdoor activity, recent pilot trials also considered the positives of reducing near work .
Additionally, studies had also shown that atropine could have a greater effect than outdoor time but that there was “bounce” in the myopia when that ended. More recent efforts include use of myopia control spectacles, which appear to show promise and might be a sound strategy in young children.
In those that are already myopic, many treatments are available and include spectacles, soft lenses, orthok, atropine and red-light therapy, but she urged all to consider strategies when the patient was young and pre-myopic – “that’s the age when we can get more bang for our buck”.
Passion, flair and design were the focuses for Ms Claire Ferreira.
The eyewear frame designer for global luxury brands Face á Face, WOOW and Alium, and co-artistic director at the Design Eyewear Group, took the audience through the design process.
The French designer said the creative workload was driven by the show calendar and a year-long process of design, development and hand-made manufacturing to bring a frame to the market.
Face á Face takes design inspiration from art – “keeping our eyes and mind wide open, even on our days off”; Paris – “a way to express our creative position”; Createur – shape and sculpture, “building models based on ideas”; the Signature – “the art of detail”; and, of course, colour.
It was about spontaneity and innovation.
“If you have a blank sheet of paper thinking I have to design something great, nothing will come. But then if you start to look around, to have fun, share, draw, relax and catch the spontaneity to generate ideas, that’s the secret. You have to unplug to be able to plug in again.”
Mr Ulli Hentschel, optical dispenser and HOYA Lens Australia’s national training and development manager, said there were great opportunities for practices that embraced the Gen X and Y generations.
He said those born between 1980 and 1994 were already Australia’s largest population group and were set to be its biggest consumer cohort by 2030.
Many of them were in their late-30s to early-40s and starting to show symptoms of presbyopia, including eye fatigue, eye strain, and headaches.
They were a “tidal wave about to come into your stores”.
People of this generation had embraced the “Experience Economy,” he said; they valued travel, work-life balance and self-improvement.
“Vision care is increasingly viewed as part of a holistic approach to health, with wellbeing being especially important.”
But there was a lack of solutions for young presbyopes resistant to progressive lenses because of price, design and positioning.
That’s why HOYA had created the VisuPro lens, available from April 2025, which was targeted as a “bridge” from single vision to progressive lens where the pricing can be significantly higher.
In an entertaining presentation during which attendees were sent to the four corners of the room as Doves, Owls, Peacocks or Eagles, Ms Virgilia Readett discussed how optical dispensers could use behavioural profiling in their practices.
The optical dispenser and senior ACOD trainer and assessor said that identifying the different birds among customers could encourage productive conversations, help with successful sales, and reduce trouble spots with clients.
It was all about D.O.P.E.
People were either Doves, who liked to listen rather than talk and put welfare first; Owls, who were logical, analytical and sought structure and predictability; Peacocks, who were charismatic, animated, sought popularity and liked to talk rather than listen; or Eagles – confident, ambitious people who liked a challenge, power and authority, and put results before feelings.
Each had different traits and recognising and understanding these in customers – and team members – could make a practice more efficient and successful. It could also encourage referrals.
Scottish paediatric dispensing optician Ms Fiona Anderson had plenty of good ideas to help eyecare professionals deal with the ‘blur’ that can be active
The record-breaking class of 2024. Graduates from the Australasian College of Optical Dispensing (ACOD) Cert IV in Optical Dispensing course at the ODA Gala.
young patients. She said they could be a real challenge – “they move about and wriggle” – but their entourage – “mum, dad, gran, big sister, sometimes the dog” –could be just as challenging.
She offered some advice, including:
• Remember that a child’s anatomy and their head is a different ratio to that of the parents.
• Children can’t always explain and you may have to pick up on cues and body language.
• Give the child your full attention. Encourage them to give their opinion or point of view. Listen to them and respond appropriately. And don’t expect too much –their attention span will be shorter than yours.
• You have to like children, which can be quite difficult sometimes. “They are like animals and can sense if you don’t like them.”
Make your practice as welcoming as possible for children.
• Adopt the shoe shop mentality – measure first and then bring what fits. “If you let children choose shoes they will pick the most inappropriate ones.”
Anderson said parents were often upset to find their child needed glasses, so “the more information you can give the parents at the beginning, the less shock it will be later if there are changes in future, including prescription changes”.
Did you know that Pantone’s official Colour of 2025 is Mocha Mousse?
That was one of the insights from Ms Shiva Taghvaei, optical dispenser and senior commercial manager at Safilo Australia, during her presentation on using data and psychology to decode frames.
She said that Safilo, as part of its extensive design process for any new frames, worked with leading forecasting agencies like Pantone to get a better picture of trends in fashion and colour.
The company also leveraged its five Global Design Hubs – Padua, Milan, New York, Hong Kong, and Portland – bringing together 150 designers who create over 3,000 new models annually, blending global creativity with local expertise. The company also used advanced data analytics to track consumer behaviour.
Optical dispensers could also use data, she said, in combination with their own observations and insights, to help drive sales in their practices.
“Know the brands, know your customer, understand their lifestyle, age group and preferences; link them to the right brand story.”
Research showed that 51% of customers chose their frames based on information from sales staff (30% for sunglasses), and 40% from the in-store displays (60%).
Just 20% made a decision based on what was in the shop window (26% for sunglasses).
The four key things driving choice were professional recommendations, fashion and personal identity, pricing and value, and social influencers and celebrity endorsements.”
George & Matilda CEO Chris Beer presents the keynote to the ODA Gala.
SLOWING DOWN TO GO FASTER
DISPENSER DETAILS
Name: Alison Middleton
Position: Optical manager and dispenser
Location: Optical by National Pharmacies, Adelaide
Years in industry: 22
1. What inspired you to pursue an optical dispensing career, and how has your perspective changed over time?
My early career was in sunglasses retailing. It naturally led me to a role as a sunglass department manager in an optical business. I was eager to combine my passion for fashion with a new challenge. I was initially captivated by how optical dispensers not only made fashion and styling decisions with customers but also engaged in deep lifestyle and technical conversations. Watching them perform the “magic” of precise measurements was fascinating– I wanted to learn more. Over time, I’ve come to appreciate how rewarding the work is, not only because of the blend of artistry and precision but because of the profound impact we have on people’s daily lives. The experience has broadened my perspective, and now, it feels more like a calling than a career.
2. What are the most influential moments and people that led you to this point?
One influential person was a learning and development leader, who taught me the magic of blending styling and fashion with deep lifestyle and dispensing conversations. He then taught me how to pass these beautiful skills on. Another inspired me to volunteer, helping provide eyecare and glasses to under-served communities in Australia and overseas. I’ll never forget revisiting a school for at-risk youth I volunteered at a year earlier. The outgoing young woman in front of me was a totally different person to the shy young girl struggling to stay engaged in school when we dispensed her first set of glasses. It was an amazing transformation to witness.
3. What’s something you know now that you wished you understood at the start of your career?
For the love of all things good, ask for help far more often! Slow down to go faster, and you’re never going to learn it all. Every day there will still be some odd conundrum that you’ve never dealt with
before. It’s truly OK to not have all the answers and seek support.
4. Can you share a moment when you made a significant impact on a patient’s life?
There are so many moments, but one stands out. A young man, about 16, came to have his eyes tested. He was shy and surprised to learn he was myopic. I styled him in a great frame that I knew looked fantastic, but he really wasn’t convinced. When he came to collect his glasses, I got him to look at the leaves on the trees outside first, which was fun because he had that full “oh wow, trees have leaves” experience, and then I got him to check himself out in the mirror and he realised how good he looked in glasses. He came to us a shy awkward teen and walked out a confident young man. That’s the kind of difference I love making.
5. What innovations in eyewear or technology are you most excited about, and why?
What I find super fun is the variety of tints, mirrors, flash coatings, photochromic colours and anti-reflective coatings now available, meaning we can design truly unique eyewear solutions that are incredibly individual, functional and stylish.
6. What skills or qualities do you believe are most important for an optical dispenser to thrive in today’s market?
Communication and relationship building. This enables us to ask the right questions, so we can
design great solutions and troubleshoot the problems that will arise from time-to-time. We also need to value our technical skills and maintain a learner’s mindset to keep us fresh and learning.
7. How do you ensure your skills and knowledge stay current in such a fast moving industry?
One of my favourite ways has been working with the Australasian College of Optical Dispensing (ACOD) and optometry students in my store. The students keep me hitting the books after asking another super technical question. Over the years, I’ve taken on every opportunity, such as project training, regional management and business coaching, which means my career has been broad and I understand aspects of optical retailing from a granular technical level and a higher-level business point of view.
8. Why did you become a member of ODA, and what value do you see in the organisation?
I became a member because I saw how ODA values the art, talent and skills of optical dispensing and is working to raise the profile of well trained and educated optical dispensers both within the industry and outside of it. I wanted a resource where I can easily access community and ongoing education while promoting all the different facets of what we do.
Alison Middleton believes communication and relationship building are the vital skills for optical dispensers
FINDING CONFIDENCE WITH LENS COATINGS
Lens coatings might seem like a minor detail, but they play a crucial role in the performance and clarity of glasses. Often underestimated, JUSTIN CHIANG explains why they shouldn’t be.
L“AS OUR UNDERSTANDING OF LIGHT AND OPTICS DEEPENS, WE CAN EXPECT EVEN MORE SOPHISTICATED COATINGS WITH ENHANCED VISUAL PERFORMANCE AND PROTECTION.”
et’s start with multicoats. As the name suggests, it comprises multiple layers of different materials, each with a specific function. These layers can manipulate light in various ways, such as reflecting certain wavelengths or enhancing transmission. Multicoats enhance lens properties like light transmission, reflection, and durability. Although multicoats are much more complicated and used in many industries for many purposes, in the optical industry, "multicoat" often refers to anti-reflective (AR) coatings, although these are just one type.
HOW AR COATINGS WORK
Reflections occur when light hits a surface and bounces back. AR coatings use a "thin film" to manipulate light interference. There are two types of interference:
• C onstructive interference – this occurs when materials with similar refractive indices are layered together. In this phenomenon, the crests and troughs of light waves align, amplifying each other, which is exemplified in mirror coatings.
• D estructive interference – this is when two wavelengths with the same amplitude are exactly half a wavelength out of sync. The crest of one wave will match up with the trough of another wave, and the two will cancel each other out.
THE IMPORTANCE OF AR COATINGS
BELOW: An antireflective coating is made up of a stack of ultra-thin, alternating layers that work to eliminate reflections and allowing more light to pass through.
An anti-reflective coating is made up of a stack of ultra-thin layers, some highly refractive and some low refractive index materials. These alternating layers create the desired destructive interference, eliminating reflections and allowing more light to pass through to the eye.
Why are AR coatings necessary? When light encounters a lens, a portion of it reflects off both the front and back surfaces. This reflection reduces the amount of light that ultimately reaches our eyes. This reduction can range from 7.7% to as much as 17%, especially in high index material, and that's before considering the light lost due to the lens material and its thickness. Furthermore, this reflection leads to a phenomenon known as 'ghosting' or 'halos'. Ghosting manifests as a faint, secondary image slightly offset from the primary one, while halos appear as bright circles or rings surrounding light sources. Therefore, AR coatings are essential to maximise light transmission and minimise these visual distractions. Beyond the visual enhancements, multicoats act as a crucial barrier between the lens and environment. Since lens materials and hardcoats are organic, the inorganic multicoat layer serves to block moisture and chemicals, preventing them from deteriorating the lens material. For example, a tinted lens with only a hardcoat will show colour fading and changes much faster than one with a multicoat. Although some wearers may dislike the multicoat bloom colour on sunglasses, some manufacturers do offer a front vacuum deposition coating without bloom, along with a back surface anti-reflective coating.
THE BENEFITS FOR WEARERS
While the light lost due to reflection might seem minimal under normal lighting, it becomes critical in low-light conditions, such as night driving. Individuals over 65 require significantly more light than 18-year-olds, making AR coatings essential for them. Modern AR coatings typically have a reflectance of around 0.8%, but advanced coatings can reduce this to as low as 0.19%. This reduction ensures less than 1% of light is reflected from the lens surface, allowing 99% to reach the eye.
Consequently, wearer comfort is improved, visual clarity is enhanced, colour contrast is increased, and eye strain is reduced. Moreover, the aesthetic of the glasses is improved, giving the lenses a nearly invisible appearance.
THE MANUFACTURING PROCESS
The coating design can affect the durability, such as scratch resistance. Despite variations in coating formulas among lens manufacturers, their production necessitates a clean, dust-free environment. Consequently, environmental control is as crucial to coating quality as the coating design itself. Factors such as double-door entry systems within the factory, cleanroom access protocols, dust-free room maintenance, and precise temperature and humidity regulation can lead to drastically different results, even when using identical equipment and formulas. This also explains why certain manufacturers produce better coatings than others.
CARING FOR MULTICOATED LENSES
Despite their benefits, AR coatings can experience issues such as scratching, peeling, and cracking. These often arise from improper care or exposure to extreme conditions. It’s essential to clean them properly and avoid exposing them to high heat. It is the duty of optical industry professionals to educate customers to enhance and optimise the coating's benefits.
Lens coating technology continues to evolve, with advancements in materials and processes. As our understanding of light and optics deepens, we can expect even more sophisticated coatings with enhanced visual performance and protection.
ABOUT THE AUTHOR: Justin Chiang is the general manager at Tokai Optical Australia. He’s a trained optical dispenser with more than 20 years’ industry experience working for corporate and independent groups.
JUSTIN CHIANG
Images: Justin Chiang.
SUPPORTING TIMOR LESTE’S FIRST ORTHOPTIST
Ms JO LYNCH explains how a chance conversation led to an ongoing partnership with the National Eye Centre in Dili, Timor Leste, and support for the country’s first, and so far only, orthoptist.
JO LYNCH
“LIDIA’S JOURNEY REPRESENTS A CRUCIAL STEP TOWARD STRENGTHENING ORTHOPTIC CARE IN TIMOR LESTE. HER TRAINING AND ACCESS TO EQUIPMENT WILL DIRECTLY IMPROVE EYECARE SERVICES FOR CHILDREN AND ADULTS ALIKE.”
Timor Leste, one of Australia’s closest neighbours, is also one of the poorest nations in the region. After gaining independence in 2002, it had to rebuild its health system from scratch. With a population of 1.35 million, access to quality eyecare remains limited, and the need for skilled professionals is critical.
At the 2019 RANZCO Conference, I met three Timorese ophthalmology registrars while waiting in line for lunch. Their accounts of working in eye health in East Timor with limited resources struck a chord. We exchanged contact details, and I pondered the stark contrast between their work environment and my own.
Years later, an orthoptic colleague from Eye Surgery Associates in Melbourne, Ms Cec Whitford, informed me they had a fully functional but no longer needed JedMed A-Scanner.
I reached out to the Timorese ophthalmology registrars, who confirmed they could use it but lacked funds for purchase or shipping. This led to a broader conversation about their challenges. They had two non-functional iCares, only one broken set of loupes for five surgeons, and one basic A-Scanner. Determined to help, I worked with Cec
We also gathered additional supplies, including a USB blower, rechargeable headlamps, and thermal paper rolls.
More generous members of the eyecare community soon joined the effort. Designs For Vision provided a new iCare and 600 probes at a discounted price. Mr Jason Hogan from Hogies Australia donated two high-quality sets of loupes.
In August 2023, I travelled to Dili, Timor Leste, to personally deliver the equipment. At the National Eye Centre (NEC) I met the staff, demonstrated the JedMed A-Scanner, and repaired their broken iCares.
Most importantly, I met Ms Lidia Amaral, Timor Leste’s first and only orthoptist.
She plays a critical role in assessing paediatric patients in a small room decorated with a Winnie-the-Pooh mural. Spending time with her, I saw first-hand how the lack of clinical equipment limited the care she could provide.
practitioners. The NEC is supported by the Fred Hollows Foundation, the Australian Government, and the Timor Leste Ministry of Health.
Her passion for learning and improving her skills to better serve her patients was inspiring.
I felt sure I could help bridge the gap between Lidia’s challenges and the resources readily available to Australian orthoptists. Back in Melbourne, I worked on assembling a full set of orthoptic tests with support from Designs for Vision, Adelaide Orthoptics, and Kids Eye Gear.
I arranged for Dr Manoj Kumar Sharma, then head of the NEC, to collect these at RANZCO in Perth.
Beyond providing equipment, I wanted to support Lidia’s desire for more clinical experience. I set about organising a clinical observership for her at the Royal Children’s Hospital (RCH) in Melbourne.
With help from Dr Anu Matthew, Dr Sandra Staffieri, and Ms Cathy Lewis, we secured a two-week placement and arranged a training visa. In November 2024, I returned to Dili and accompanied Lidia to Melbourne.
During her placement, Lidia gained hands-on experience in various clinics, including congenital cataract, retinoblastoma, congenital glaucoma, and ocular motility.
This training, coupled with new testing equipment, significantly enhanced
Other initiatives, like the East Timor Eye Project (ETEP), provide clinical training and equipment. I was inspired by these efforts and the impact individuals can have.
Lidia’s journey represents a crucial step toward strengthening orthoptic care in Timor Leste. Her training and access to equipment will directly improve eyecare services for children and adults alike.
If anyone in the eye care community would like to support ongoing orthoptic training for Lidia or the NEC’s optometrist, Mr Gil Costa, the NEC would be incredibly grateful. Please reach out to execofficer@orthoptics.org.au for more information.
ABOUT THE AUTHOR: Jo Lynch is an orthoptist at Eye Surgery Associates in Melbourne and has also worked at the Royal Children’s Hospital. Her main interest is in ocular electrophysiology, working with Associate Professor Heather Mack, also glaucoma and paediatrics. She is the current chair of the Victorian Branch of Orthoptics Australia.
ORTHOPTICS AUSTRALIA is the national peak body representing orthoptists in Australia. OA’s Vision is to support orthoptists to provide excellence and equity in eye health care. Visit: orthoptics.org.au
Images: Jo Lynch.
Lidia Amaral, Timor Leste’s first orthoptist
FRONTLINE LEADERSHIP IN HEALTHCARE
Many people become ‘accidental managers’, but with the right training, guidance and experience, they can become effective leaders in their clinics. Some key behaviours will also ensure they get the most out of their team, writes ALAN STEVENSON.
I’ll own up. I’ve been a bit cute with the title. What I’ll actually be discussing is your role as a manager in whatever company or industry you’re in now or possibly in future.
Being a student around leadership and high performing teams, I’ve discovered the core of being a ‘great’ leader can be distilled down to a handful of skills.
“A GOOD COACH USES PROBLEMS AS A CHANCE TO LISTEN, ASK QUESTIONS, RAISE AWARENESS AROUND ‘BLIND SPOTS,’ AND CHALLENGE THINKING AND DEEPLY HELD BELIEFS.”
Before we go on, it’s important we understand what it means to be skilful. The Cambridge Dictionary defines ‘skill’ as “an ability to do an activity or job well, especially because you have practised it”. This is important; leadership is something that requires ongoing practise.
Let’s start with how one becomes responsible for a group of people.
An October 2023 study by the UK Charted Management Institute (CMI) and YouGov found 82% entering management positions have not had proper training.
According to the research, these “accidental managers” are often promoted for the wrong reasons, with nearly half surveyed (46%) believing colleagues won promotions based on internal relationships and profile, rather than their ability and performance.
Is training the answer? Well, maybe. There is a popular training model, 70:20:10. The key takeaway from this model is that courses, workshops and e-learning will only provide 10% of development. The remaining 20% is through social learning and 70% experiential – getting your hands dirty.
BELOW: Ten desirable traits Google found in its managers.
All too often we enrol people into a training course with the expectation they will emerge an expert. Very seldom does this
happen and we are missing around 90% of the opportunity.
We sometimes spend too much time discussing the difference between management and leadership. Often leadership is promoted as being superior to management. I don’t subscribe to that.
A distinction I particularly align with is from John P. Kotter, Konosuke Matsushita Professor of Leadership, Emeritus at Harvard Business School, who argues they are “two distinctive and complementary systems of action”.
“Each has its own function and characteristic activities. Both are necessary for success in an increasingly complex and volatile business environment,” he says. So, are you a manager or a leader? The answer is both. There are functions you perform that require management skills while leadership skills enhance the overall performance of your team.
What might this blend of management and leadership look like?
Back in the early 2000s, Google, having gone through a period of rapid growth and expansion, posed the question: ‘Do managers matter?’. It experimented with various structures without real success.
In 2009, Project Oxygen was launched, a multi-year research initiative. Later that year, the “people analytics” teams at the company produced what might be called the ‘Eight Habits of Highly Effective Google Managers’. More were eventually added, making a total of 10 (Figure 1).
You can see that Google doesn't distinguish between what might be classified as
‘management’ or ‘leadership’. Note #1 – Is a good coach. Like the coach of a sports team, a good coach uses problems as a chance to listen (research shows the more a manager listens, the better people think they are at giving feedback), ask questions, raise awareness around ‘blind spots,’ and challenge thinking and deeply held beliefs.
I’ve been studying leadership and high performing teams since around 2008, about the time Project Oxygen was initiated.
Fast forward 16 years, and I would now like to focus on five leadership capabilities that my experience and studies of ‘good’ leaders demonstrate consistently.
From the Harvard Business Publishing Corporate Learning ‘Five crucial capabilities for today’s frontline leaders’, it states:
1. Develops others – by coaching and delivering ongoing feedback that energises employees instead of draining them.
2. Leads teams that deliver – by using strong interpersonal skills to build team cohesion, focusing on what matters, and providing meaningful work.
3. Leads authentically – by demonstrating behaviours aligned with one’s principles and values, as well as earning the trust of others through empathy, self-awareness, and the ability to admit mistakes.
4. Communicates for influence and impact – by strengthening communication skills required both in person and across distances, dealing effectively with conflict, and managing difficult conversations.
5. Champions inclusion – by helping all team members feel a sense of belonging, curbing biases, and celebrating diversity.
These five leadership capabilities correlate well against the results of Google’s Project Oxygen.
Going into your clinic today, be curious about:
• How would I rate my skill level against these five capabilities?
• How would my team rate me against them?
• What am I doing to support the development of someone that I feel might be ready for promotion?
ABOUT THE AUTHOR: Alan Stevenson is the principal consultant at Barclayss with more than 40 years of experience working in operational and safety support roles with people from different cultures and countries creating safe and productive workplaces. He also presented at the 2024 RANZCO Practice Managers Conference.
ALAN STEVENSON
SOAPBOX TRAINING PNG’S FIRST PAEDIATRIC OPHTHALMOLOGIST
BY DR CESAR CARRILLO
Even in Australia’s developed eye health system, paediatric ophthalmologists are in short supply. In fact, RANZCO describes an “impending critical shortage” brought about by a confluence of factors.
But in Papua New Guinea (PNG) the situation is much more desperate. The country has never had a trained paediatric ophthalmologist. That’s about to change though, with support from Sight For All and a team of paediatric sub-specialists across Australasia.
Childhood blindness is second only to cataract as the leading cause of blindness in low-and-middle income countries. PNG has a population of 10.3 million and over 40,000 people are reported to be blind in both eyes.
The estimated prevalence of blindness in PNG is 5.6%, although this is more prevalent in the highlands, particularly affecting women with a blindness rate of 11.1% and men with a rate of 6.6%.
The current childhood blindness situation in PNG is not widely known due a lack of studies. Information from the PNG Prevention of Blindness Committee (PBL) estimates there are approximately 6 million children in PNG and that the blindness prevalence would be approximately 4%. However, some extrapolated data from 2015- 2017 suggests that it might be as high as 7.4% for children living with vision impairment or blindness.
It’s well known blind and visually impaired children are afflicted for a lifetime, causing a significant economic burden on the family and community. Blindness affects the
child’s psychomotor and emotional development, education, opportunities for employment and earning potential, thereby increasing poverty.
For many years Sight For All has been in consultation with ophthalmic colleagues in PNG, particularly in terms of addressing childhood blindness. There is a need for training of ophthalmic sub-specialty training in PNG and Sight For All became a member of the PNG Prevention of Blindness Committee in 2023, to support sub-specialty training in the country.
Through the support from the Australian and New Zealand Eye Foundation (ANZEF), Santos and Karma foundation, Sight For All is establishing the first paediatric ophthalmology clinic at Port Moresby General Hospital and conducting the first paediatric ophthalmology fellowship in PNG.
The PNG paediatric ophthalmology in-country fellowship project is designed to provide guidance and instruction to the PNG Fellow to treat children within the Port Moresby General Hospital. One female ophthalmologist, Dr Maggie Mangot, was selected for the fellowship and she will gain competency in specialised surgical techniques and clinical skills through a comprehensive teaching curriculum, guidance within a clinical setting and direction during hands on surgical tuition. To support the teaching of Dr Mangot and enable the most effective diagnosis and treatment of children’s eye conditions in PNG, specific ophthalmic infrastructure is required. A specialty children’s eye clinic was established in October 2024 by Dr Kim Tan, Sight For All’s Australian paediatric ophthalmology lead visionary, as well as the organisation’s CEO, Mrs Judy Hatswell, at Port Moresby General Hospital where Dr Mangot is diagnosing and treating children. Specific clinical equipment and surgical instruments have been donated to allow the creation of this paediatric eye clinic. The project is being implemented over two years. Sight For All is sending one fully trained Australian or New Zealand paediatric ophthalmologist for a week every second month to spend time in the clinic and theatre conducting comprehensive hands-on training. Each visit has a specific theme for which the fellow will need to prepare tutorials
research activities and will be required to maintain a clinical and surgical logbook to monitor progress.
Australian and New Zealand ophthalmologists can make a significant contribution to fighting avoidable blindness in PNG by contributing to Sight For All’s paediatric ophthalmology fellowship in Port Moresby. The project calls on the high level of knowledge and skills of the voluntary visiting specialists. The sustainability of the program combined with the very efficient use of resources means the project will have a profound local impact for a modest financial input. The ‘in country’ training means that the fellows will be taught in their own environment and with an appropriate spectrum of PNG patients with relevant local issues. The ripple effects of the program will be far-reaching and sustainable for many years to come.
ABOUT THE AUTHOR
Name: Dr Cesar Carrillo
Qualifications: MD, MHID
Affiliations: International development manager, Sight For All; Ophthalmology
Department Royal Adelaide Hospital, Clinical
Associate Lecturer ,The University of Adelaide
Location: Adelaide, South Australia
Years in industry: 23
THE ‘IN COUNTRY’ TRAINING MEANS THAT THE FELLOWS WILL BE TAUGHT IN THEIR OWN ENVIRONMENT AND WITH AN APPROPRIATE SPECTRUM OF PNG PATIENTS WITH RELEVANT LOCAL ISSUES.
ABOVE: PNG’s first paediatric ophthalmologist in fellowship training, Dr Maggie Mangot.
Images:
Sight For All.
EVENTS CALENDAR
APRIL 2025
ASIA-PACIFIC ACADEMY OF OPHTHALMOLOGY CONGRESS
New Delhi, India 3 – 6 April 2025.apaophth.org
GOLD COAST INTERACTIVE
Gold Coast, Australia 13 – 14 April interactive.optometry.org.au
MAY 2025
ARVO 2025
Utah, US 4 – 8 May arvo.org/annual-meeting
OPTOMETRY VIRTUALLY CONNECTED
Online, Australia 17 May ovc.optometry.org.au
JUNE 2025
INTERNATIONAL ORTHOPTIC CONGRESS
Brisbane, Australia
27 – 29 June ioc2025.com.au
ODMAFAIR25
Sydney, Australia
27 – 29 June odma.com.au
To list an event in our calendar email: myles.hume@primecreative.com.au
SEPTEMBER 2025
SILMO PARIS
ASIA-PACIFIC STRABISMUS AND PAEDIATRIC OPHTHALMOLOGY SOCIETY CONGRESS
Brisbane, Australia 29 June – 1 July apspos.org/apspos-congress-2025
JULY 2025
AUSCRS 2025
Darwin, Australia 16 – 19 July auscrs.org.au/2025-conference
Paris, France 26 – 29 September silmoparis.com/en
NOVEMBER 2025
RANZCO CONGRESS
Melbourne, Australia 14 – 17 November ranzco2025.com
AUSCRS 2025 is heading to Darwin, where cataract and refractive surgeons can take
latest technology and techniques.
Melbourne is hosting the 2025 RANZCO Congress in November.
The Optometry Australia-run online event, Optometry Virtually Connected, will have up to 40 CPD hours available.
SPECSAVERS STORIES: MONICA HOANG
HOW DID YOU COME TO WORK AT SPECSAVERS?
CHANGING LIVES THROUGH BETTER SIGHT AND HEARING
I was studying in my second year at Flinders University and the advertisement for an optical assistant at Specsavers Norwood Place was announced on the optometry student forums. It felt like my first adult job, and I didn’t know what to expect. I just knew Specsavers was one of the major optical companies and I love how the network supports self-development and learning.
WHAT WAS YOUR FIRST ROLE IN THE BUSINESS?
I started as a retail assistant, being involved in every step of the patient journey outside of the eye test itself. Daily tasks would include booking appointments, welcoming customers to their appointments, operating clinical devices such as fundus cameras, OCT and visual fields, frame styling, dispensing glasses, teaching customers how to use contact lenses, fitting and adjusting glasses and troubleshooting patient concerns. I also got to work with the most fun and amazing team. The optometrists in store also became great mentors and were always happy to answer optometry-related questions as I neared the end of my degree. Because of this experience, I bonded easily with the retail team, and you would sometimes find me out front helping.
WHAT GROWTH OPPORTUNITIES HAVE PRESENTED THEMSELVES?
After three years, that’s when the mobile optometrist role was mentioned to me. I didn’t know it existed, but it was perfect for me because I could experience various stores while staying with Specsavers. Now, I travel to Specsavers stores across Australia that need cover. I have recently completed my Pathway Program, which has given me the leadership skills I’ll need to one day run my own Specsavers store. I’m also loving acting as a mentor to one of our newly appointed graduates in the Wyalla store.
WHAT ARE YOUR TOP CAREER HIGHLIGHTS SINCE JOINING SPECSAVERS?
I am grateful to have experienced many roles in this company. As an optical dispenser, I learned how to provide good customer service and improved my communication skills and confidence. As a graduate optometrist, I had mentors that gave me guidance and space to develop my skills and become the type of optometrist and person I wanted to be. At Specsavers Hollywood, I performed eye tests in Vietnamese for the local Vietnamese patients who spoke limited English. This was so rewarding – they were so excited and grateful. Now, as a mobile optometrist, I have never loved my job more. I travel to cities and towns I would have never otherwise. I am making a difference by making optometry accessible in regional areas. It’s made me feel more competent; I may not be there for reviews, so I need to be confident and thorough in my triage and treatment plans so the patient is properly cared for even when I have left.
WHAT EXCITES YOU MOST ABOUT TURNING UP FOR WORK EACH DAY?
I eventually started my graduate optometry program at Specsavers Hollywood, which was close to my home and where I had my first ever eye test. My employer/mentor was also the optometrist that performed my first eye examination and treated my amblyopia as a child. After finishing my graduate program, I continued to work at the same store and began mentoring optometry students, as well as helping at one of the graduate induction events.
Specsavers YOUR CAREER, NO LIMITS
Optometrist Partnership Opportunity in Karratha with potential to earn up to $250,000
Specsavers Karratha is offering an exciting opportunity for an experienced Optometrist to join the brand as a Partner, with the potential to earn up to $250k. Karratha is a seaside gem capturing the essence of coastal charm and natural beauty. Specsavers Karratha will be a new site offering the latest store features including optical test rooms, pre-test rooms, dispensing desks, and state-of-the-art equipment including OCT. The store will also showcase the latest Specsavers design, with digital displays and illuminated shelving. Successful applicants will receive Specsavers’ award-winning support in building up their business, including team recruitment support and end-to-end financing on new stores.
Optometrist opportunity – Specsavers Taupo, NZ
Join our vibrant Specsavers Taupō store as an optometrist! Enjoy a balanced lifestyle with stunning lake views, outdoor adventures, and a family-friendly atmosphere. Taupō offers affordable living, great schools, and ample work opportunities in tourism and healthcare. Experience a fulfilling career in one of New Zealand’s most beautiful spots!
SO LET’S TALK!
In a few short years, Specsavers has achieved market leadership in Australia and New Zealand with more people choosing to have their eyes tested and buy their prescription eyewear from Specsavers than any other optometrist.
To learn more about these roles, or to put your hand up for other roles as they emerge, please contact us today:
Joint Venture Partnership opportunities enquiries: Carly Parkinson on +61 (0) 478 201 057 or E carly.parkinson@specsavers.com
Locum employment enquiries: ANZ.locumteam@specsavers.com
Graduate employment enquiries: apac.graduateteam@specsavers.com Years within the business: 9
I love that each day is different and not predictable. I can come to work knowing I have the tools to make a difference to someone’s vision, eye health and quality of life.
Specsavers Emerald offering up to $190,000 package
Specsavers Emerald are currently on the lookout for an Optometrist to join their team. The hub of the Central QLD Highlands – Emerald has all the amenities of a big city, with a laid back, community feel. Our Emerald store prides itself on their wonderful team, who work closely together to provide excellent customer service. Work with market leading equipment including OCT free for every patient. Enjoy excellent opportunities for further career development and progression. An extremely attractive salary package is on offer of up to $190k.
Graduate Opportunities
The Specsavers ‘Early Bird Package’ which offers our highest sign on bonus yet is now live! For select opportunities across ANZ, final year optometry students will be eligible for either a $30,000 or $20,000 sign on bonus when they sign an employment contract before June 30 2025. At Specsavers you will have access to cutting edge technology and be part of the driving force bringing Optometry into the forefront of the healthcare industry. If you’re a final year student or recently graduated, please contact anz.graduateoptometry@specsavers.com for more information.
People on the move
BRITISH OPHTHALMOLOGIST MAKES MOVE DOWN UNDER
Experienced UK ophthalmologist Dr Jeremy Diamond has moved to Australia and joined Vision Eye Institute Boronia. He offers care for a range of eye conditions and surgical procedures and has performed over 15,000 cataract and glaucoma surgeries and led the glaucoma department at the prestigious Bristol Eye Hospital for 20 years. Additionally, Dr Diamond has authored more than 50 research papers and textbook chapters, achieved a PhD and received eleven research grants.
EXPERIENCED BUSINESS FIGURE MAKES VISION EYE INSTITUTE RETURN
Mr Antonio Monteiro, previously a member of Vision Eye Institute’s finance team, has returned in 2025 as the company's general manager for Victoria. He oversees the state’s consulting practices and has commercial oversight of Vision Hospital Group day surgeries in Victoria. During his time away from VEI, he held senior positions at Healthscope as its commercial manager (data & analytics) and at St Vincent’s Health Australia as its strategy consultant.
RED LIGHT MYOPIA DEVICE MANUFACTURER WELCOMES OPTOMETRIST
Optometrist Mr Daniel Bishay has recently joined Eyerising International as its professional affairs manager. With a background in orthoptics, optometry and clinical education as a Deakin casual academic, Bishay is excited to now be providing clinical and educational expertise to support eyecare professionals in their adoption and implementation of the company's repeated low-level red-light therapy.
AHPRA’S NEW CEO A STANDOUT AMONG STRONG CANDIDATE LIST
The Australian Health Practitioner Regulation Agency (Ahpra) has appointed Mr Justin Untersteiner as CEO. Untersteiner, joining in April 2025, brings more than 20 years’ experience in regulation and compliance, most recently as chief operating officer at the Australian Financial Complaints Authority. Ahpra board chair Ms Gill Callister said Untersteiner was an impressive leader who stood out in a field of domestic and international candidates.
1001 OPTICAL APPOINTS EXPERIENCED FIGURE AS NEW GENERAL MANAGER
Mr Dylan Oblein has been promoted to general manager of 1001 Optical, an independent family-owned business with 15 boutique practices across Australia. After joining the company in September 2023, he previously held regional manager and national sales manager roles. He has almost 20 years of optometry industry experience, holding roles at Luxottica, Specsavers, George & Matilda and Eyecare Plus.
COOPERVISION ANNOUNCES PROMOTION TO BOLSTER MYOPIA STRATEGY
Ms Jennifer Lambert, who has spent the past four years as senior director, global myopia management, has been appointed to the new role of vice president, myopia management & cornea care at CooperVision. Lambert’s role is part of a move by the company to transform its myopia category and combat the global epidemic. It has elevated the myopia management group within its global commercial structure and plans to add other managerial roles specific to customer engagement and new product market development.