

EXECUTIVE SUMMARY 1 Table of Contents Acknowledgments ................................................................................................................................2 Acronyms 3 ExecutiveSummary.....................................................................................................................4 Introduction..................................................................................................................................6 Background..................................................................................................................................7 Methodology 12 ModernizingEligibilitySystemsandProcesses 12 Summary 14 Problem Statement ............................................................................................................................ 15 Policy Recommendations 17 IncreasingHealthCareAccessibility......................................................................................22 Summary 23 Problem Statement 24 Policy Recommendations 26 EffectivelyLeveragingManagedCareOrganizations.........................................................31 Summary .............................................................................................................................................. 32 Problem Statement 33 Policy Recommendations.................................................................................................................. 34 AddressingFederalImmigrationPolicy 38 Summary 39 Problem Statement 40 Policy Recommendations.................................................................................................................. 45 Conclusion 49 Appendices 51 Appendix A: Special Populations Outreach Resources 52 Appendix B: Contending with Fiscal Constraints ......................................................................... 53 Appendix C: Arizona Managed Care Organizations Contract Excerpts 57 Appendix D: Arizona Alternative Payment Models 62 Appendix E: Participant Biographies .............................................................................................. 63 Appendix F: Endnotes 65
Acknowledgments
This report was prepared by Master in Public Affairs and Master in Public Policy students at Princeton University’s Woodrow Wilson School of Public and International Affairs. This report incorporates information gathered through students’ independent research, inperson interviews conducted between October 26 and November 1, 2019, and invaluable guidance from course instructors Heather Howard and Dan Meuse. The report fulfills the Woodrow Wilson School’s degree requirements for an immersive policy workshop and associated policy proposal.
We are especially grateful to our partners in the Nevada Department of Health and Human Services, Division of Health Care Financing and Policy that enabled us to conduct research and make recommendations on this important topic, particularly to Administrator Suzanne Bierman. We also wish to extend our gratitude to the many policymakers, health professionals, and subject matter experts who shared their perspectives with us throughout the course of this project. We hope that this report will contribute to ongoing efforts to build on the success of Medicaid expansion in Nevada.
Tom Betlach, former Arizona Medicaid Director
Suzanne Bierman, Nevada Department of Health and Human Services, Division of Health Care Financing and Policy
Bobbette Bond, Culinary Health Fund
Nancy Bowen, Nevada Primary Care Association
Tiffanie Flemming, University Medical Center of Southern Nevada
Vick Gill, University Medical Center of Southern Nevada
Roxanna Gonzalez, Nevada Department of Health and Human Services, Department of Welfare and Social Supports
Kayla Hillegass, University Medical Center of Southern Nevada
Gabrielle Jones, Legal Aid of Southern Nevada
Michael Kagan, University of Nevada, Las Vegas Immigration Clinic
Heather Korbulic, Nevada Health Link
Steve Messinger, Nevada Primary Care Association
Catherine O’Mara, Nevada State Medical Association
Pam Norcia, University Medical Center of Southern Nevada
Senator Julia Ratti, Nevada State Senate
Dee Towner, University Medical Center of Southern Nevada
Marcia Turner, University Medical Center of Southern Nevada
Mike Willden, former Chief of Staff to Governor Brian Sandoval and Nevada Department of Health and Human Services Director
Angie Wilson, Washoe Tribal Health Center
Tracey Woods, Anthem
Gail Yedinack, University Medical Center of Southern Nevada
EXECUTIVE SUMMARY 2
Acronyms
ACA Patient Protection and Affordable Care Act
AHCCCS Arizona Health Care Cost Containment System
APM Alternative Payment Model
APRN Advanced Practice Registered Nurse
APTC Advance Premium Tax Credit
CBO Community-Based Organization
CHC Community Health Center
CHIP Children’s Health Insurance Program
CoC Continuum of Care
DHS U.S. Department of Homeland Security
DWSS Nevada Department of Welfare and Supportive Services
FFS Fee-for-Service
FSS Family Service Specialist
HMIS Homeless Management Information System
HPSA Health Professional Shortage Area
HSI Health Services Initiative
HUD U.S. Department of Housing and Urban Development
IHS Indian Health Service
INA Immigration and Nationality Act
LIHTC Low-Income Housing Tax Credit
LPR Lawful Permanent Resident
MBT Modified Business Tax
MCO Managed Care Organization
MMIS Medicaid Management Information System
MOU Memorandum of Understanding
NAICS North American Industry Classification System
REACH Resources for the Early Advancement of Child Health
RFP Request for Proposal
SDOH Social Determinants of Health
SIM State Innovation Model
SOW Statement of Work
TANF Temporary Assistance for Needy Families
TOP Targeted Outreach Partnerships
EXECUTIVE SUMMARY 3
EXECUTIVE SUMMARY
Nevada’s health care system has undergone a fundamental transformation in the five years since the expansion of Medicaid in 2014. In 2012, nearly 30 percent of Nevadans were uninsured almost 600,000 individuals. Less than a decade later the state has cut its uninsured rate in half and doubled the size of its Medicaid program. Despite this laudable progress, challenges persist: the state has the highest uninsured rate of any Medicaid expansion state and an estimated 400,000 Nevadans remain without insurance, including nearly 150,000 that are presumed Medicaid eligible but unenrolled.1
This report’s short- and long-term recommendations aim to increase enrollment in Medicaid among the population of Nevadans who are eligible but uninsured Improving Medicaid coverage rates would provide additional benefits for individuals throughout the state, leverage increased federal funding, and strengthen the health care safety net. Specifically, the report focuses on four domains with identified opportunities for policy changes that would increase Medicaid enrollment or better retain people already in the program. These domains and associated policy recommendations are listed in Table 1 below.

EXECUTIVE SUMMARY 4
Table 1. Summary of Policy Recommendations Policy Area Short-Term Long-Term
✓ Increase the share of Medicaid applications filed online to expedite eligibility determinations
✓ Hire additional eligibility workers to increase onsite determination capacity
✓ Build IT capacity for realtime eligibility determinations
Modernizing Eligibility Systems & Processes
✓ Adopt a Medicaid state plan amendment to establish a full presumptive eligibility program
✓ Adopt a Medicaid state plan amendment to implement 12month continuous eligibility for children in Medicaid
✓ Suspend, rather than terminate, Medicaid coverage for enrollees who become incarcerated
✓ Support policies aiming to alleviate Nevada’s provider shortage to increase access for Medicaid enrollees
✓ Implement income attestation and verification practices that expedite Medicaid enrollment
✓ Streamline and automate Medicaid renewal to reduce program churn
Increasing Health Care Accessibility
✓ Seek partners, projects, and funding to better identify the Medicaid-eligible but uninsured population
✓ Leverage available funds and lowcost, best practice strategies to target and expand outreach
✓ Improve frontline processes for Tribal Medicaid claims
✓ Consider rebranding Medicaid
✓ Increase Medicaid reimbursement rates
✓ Incentivize rural students and rural service to pursue health profession careers
✓ Increase the quantity of residencies in Nevada
Effectively Leveraging Managed Care Organizations (MCOs)
✓ Ensure MCOs meet network adequacy and appointment standards
✓ Require MCOs to provide transportation
✓ Require MCOs to have justice and housing leads to coordinate transitions and support
✓ Streamline data sharing and matching between the state and MCOs
✓ Require MCOs to reinvest part of their profits into communities
✓ Implement alternative payment models
Addressing Federal Immigration Policy
✓ Develop a coordinated strategy for education and outreach on the public charge rule
✓ Waive 5-year bar for pregnant LPR women
✓ Disseminate information on CHCstargeting undocumented populations
✓ Use state dollars to expand Medicaid coverage to undocumented populations (youth)
EXECUTIVE SUMMARY 5
INTRODUCTION
The passage of the Patient Protection and Affordable Care Act (ACA) in 2010 represented the most significant health insurance transformation in a generation. As modified by the Supreme Court, the ACA gave states the opportunity to expand Medicaid public health insurance for low-income individuals and families to previously uninsured populations up to 138 percent of the federal poverty line, with most of the cost of expansion borne by the federal government. In 2014, Nevada used this opportunity to expand its Medicaid program, radically altering the state health insurance landscape. This has given hundreds of thousands of lowincome adults and children that previously had no coverage access to affordable health care for the first time. Medicaid has grown at a staggering pace over the past five years: Nevada’s program has nearly doubled in size and the statewide uninsured rate has been halved 2,3
Yet the rapid growth in the Medicaid program has been accompanied by commensurate challenges The capacity of existing program infrastructure is strained, the state faces a significant provider shortage that reduces access to health care even among the insured, and vulnerable groups such as immigrants and American Indians face additional obstacles to accessing coverage and care.
State efforts to address these challenges are stymied by a lack of resources and budgetary flexibility.
Despite the constraints, there are significant opportunities to increase health insurance coverage and care for lowincome individuals within the state. This report assesses the challenges and opportunities in the Nevada health care policy landscape to increase coverage and care for low-income Nevadans. In particular, the report examines policy implications for the state health care and insurance system across four domains:
(1) Modernizing eligibility systems and processes;
(2) Improving health care accessibility;
(3) Effectively leveraging Managed Care Organizations; and
(4) Addressing federal immigration policy.
The report begins with a high-level background on the state health care policy context, followed by discussion of each of the domains listed above. Within each of these sections, the report discusses the challenges facing the state and makes short- and long-term recommendations to increase Medicaid enrollment and health care access for lowincome Nevadans.
INTRODUCTION 6
BACKGROUND
Nevada’sdemographyshapesitspolicy andservicedeliverylandscape
Nevada is a dynamic state undergoing significant changes. The state is the fastest growing in the country, currently home to more than three million people, and growing at a rate of more than two percent annually.4,5 Nevada is geographically, demographically, and culturally diverse.
An estimated 28 percent of Nevada’s population is low-income.6 Much of Nevada’s population comes from outside the state: in 2016, an estimated 54 percent of residents were born in other states and nearly 20 percent of residents were born in other countries.7 At present, working-age adults (age 18-64) make up roughly two-thirds of the state population.8 Over the next decade, population growth among the elderly in Nevada is expected to vastly outpace population growth among children and adults, with rates of 25.3 percent, 2.4 percent, and -1.1 percent, respectively.9 This age and income distribution is likely to put more pressure on an already strained health care system in the years to come.
By population, the state is primarily urban: more than nine in ten residents live in the state’s three urban counties and 73 percent of the state’s population lives in Clark County alone 10 By geography, however, the state is primarily rural or frontier: rural and frontier populations are spread across 87 percent of the state’s
land mass.11 These dynamics pose a dual health care delivery challenge: it is difficult to ensure sufficient care in the vast and sparsely populated rural areas as well as in the densely populated southern region.
Medicaidexpansionhastransformedthe healthinsurancelandscapeinNevada
In December 2012, Governor Brian Sandoval announced his decision to expand Medicaid in Nevada, becoming the first Republican governor in the country to do so. Since the expansion began in 2014, more than 335,000 people have signed up for the program, nearly doubling the Medicaid population in the state.12 Expansion has also cut uninsured rates in half, from 20.7 percent to 11 percent.13,14 Additionally, Nevada’s 46 percent decline in uninsured rates among children between 2013 and 2016 was best in the nation.15 As illustrated in Figure 1, Medicaid enrollment increased sharply after expansion but has largely plateaued since 2017.16 As of August 2019, there are 631,562 Medicaid enrollees in Nevada (roughly 19 percent of the state population).17
It is unclear to what extent concerns about the future of the ACA particularly ongoing federal litigation in Texasv. UnitedStatesregarding the constitutionality of the law and the Trump administration’s efforts to repeal or undermine the ACA have influenced Nevada’s Medicaid enrollment trends. Nationally, census data shows that the uninsured rate including among children
BACKGROUND 7
recently increased for the first time since before the enactment of the ACA in the wake of federal actions such as the repeal of the ACA’s individual mandate penalty, cuts in advertising and enrollment assistance for the ACA marketplaces, the public charge rule, and the approval of Medicaid work requirements in certain states.18
Despiteprogress,thereremainsa significantuninsuredpopulation
Though Nevada has made great strides in coverage since Medicaid expansion, it still ranks low nationally on many health insurance indicators. The Guinn Center estimates that by the end of 2017, 400,000 Nevadans remained without health insurance.19 In 2018, Nevada ranked among the bottom five states for overall health insurance coverage (88.8 percent insured, 45th place) and kids’
health insurance coverage (92 percent insured, 46th place).20 Among states that chose to expand Medicaid, Nevada ranks lowest on health insurance coverage. 21,22 Data on Nevada’s uninsured population and subpopulation uninsured rates is included in Tables 1 and 2 below.
One of the significant puzzles underlying the high uninsured rate is that the Guinn Center estimates that more than half of Nevada’s uninsured are likely eligible for low-cost insurance through Medicaid, Nevada Check Up (the state’s version of the federal Children’s Health Insurance Program [CHIP]), or subsidized private coverage on the private health insurance marketplace through the Advance Premium Tax Credit (APTC).23 Ultimately the composition of Nevada’s Medicaideligible but unenrolled population remains unclear.
BACKGROUND 8
350,000 400,000 450,000 500,000 550,000 600,000 650,000 Jan 2014 Mar 2014 May 2014 Jul 2014 Sep 2014 Nov 2014 Jan 2015 Mar 2015 May 2015 Jul 2015 Sep 2015 Nov 2015 Jan 2016 Mar 2016 May 2016 Jul 2016 Sep 2016 Nov 2016 Jan 2017 Mar 2017 May 2017 Jul 2017 Sep 2017 Nov 2017 Jan 2018 Mar 2018 May 2018 Jul 2018 Sep 2018 Nov 2018 Jan 2019 Mar 2019 May 2019 Jul 2019 Total Medicaid and CHIP enrollment
Figure 1. Medicaid enrollment has slowed after initial significant growth
*In the 2019 Guinn Center report, the “other” category includes all racial identities other than white, black, Asian, American Indian, and Native Hawaiian/Pacific Islander.
*numbers do not total to 100%; each percentage is relative to an opposite population group (ex: 32% of Nevada’s uninsured are non-citizens, while 68% are citizens)
**if the uninsurance rate is estimated at 11 percent rather than 14 percent, undocumented immigrants would represent an estimated 30 percent of Nevada’s uninsured population.
BACKGROUND 9
Nevadan subpopulation Uninsured rate Overall state population 14% American Indian populations 19% Rural counties 12% Urban counties 14% Adults age 26-44 22.1% “Other” race* 27.6% Asian 11.3% Latinos 23.8% White, non-Latino 9.2%
Table 2 Uninsured rates for various target demographics, as estimated by the Guinn Center
Population As a percentage of Nevada’s uninsured population* Non-citizens 32.4% Latino 59% Clark County 77% Non-elderly adults 81% Adults age 26-34 21.8% Adults age 35-44 19.6% Undocumented immigrants, estimate 23.7%** Employed 62.9%
Table 3. Characteristics of Nevada’s uninsured population, as estimated by the Guinn Center
Healthcareaccess,notonlyinsurance, posesasignificantstatewidechallenge
Nevada is facing an access to care crisis. Eleven of the state’s seventeen counties are considered primary medical care health professional shortage areas (HPSAs): 67.3 percent of the state’s population lives in counties with insufficient access to medical care health professionals. In addition, 14 counties (housing 72 percent of the state population) are considered dental health professional shortage areas.24 Sixteen counties are considered mental health professional shortage areas, resulting in insufficient access to mental health care for 94.3 percent of the state’s population.25 In this environment, even with health insurance an individual may have to wait weeks or months to see a primary care provider or specialist. These are significant impediments to care and may disincentivize individuals from seeking health insurance at all.
Fiscalconstraintsposechallengetomajor reforminNevada
Throughout our conversations, stakeholders repeated concerns about the fiscal limits of potential health reforms. Nevada, unlike many other states, does not have an income tax as a primary source of revenue. The state is forced to rely on a combination of many smaller taxes to sustain the general fund and pay for public programs, especially in education and health care. These fiscal constraints influence the fiscal and political feasibility of solutions considered for this report.
These fiscal constraints are institutionalized in state law. Not only are certain types of taxes expressly prohibited
or limited in the state Constitution, but permitted types of tax increases require a two-thirds majority in both houses of the state legislature
Although outside the direct scope of this report, these fiscal constraints play a heavy role in defining the political and budgetary feasibility of our recommendations. Thus, Appendix B includes a more detailed discussion of these constraints, along with policy recommendations.
Healthcareissueshavepolitical
momentuminNevadaatpresent Medicaid expansion drastically altered the state’s health insurance landscape, and new opportunities are arising to build on this transformative progress. This past year, the health insurance landscape changed again when the state switched from a federally-supported state-based health insurance exchange to a fully statebased exchange, Nevada Health Link. This transition is expected to save the state more than $4 million in the first year of operation.26 It is also expected to facilitate better data collection and outreach efforts, as well as support Nevada-specific policy adaptations.27 This transition may open doors for improved Medicaid coverage rates and additional collaboration between Nevada Health Link and the Medicaid program
BACKGROUND 10
In addition, the 2019 legislative session included a number of health care reforms, including bills that:28
• Ended surprise emergency room medical bills;
• Codified protections for individuals with pre-existing conditions to not be denied health coverage;
• Increased transparency for pricing prescription drugs to treat asthma; and
• Created a Patient Protection Commission to identify areas for health care system improvements.
The Patient Protection Commission, in particular, represents a significant step toward more substantial health reforms in Nevada. The Commission will have 11 representatives from industry, academia,
and patient advocacy, and is charged with examining health care costs, quality, and equity across the state.29 This Commission provides an opportunity to improve health insurance coverage and access to quality health care. While the Commission does not have regulatory authority, it can propose up to three bills for the Nevada Legislature and is poised to play an important advisory role, especially since the Nevada Legislature will not meet again until 2021.30
These recent developments indicate the significant momentum and opportunities in Nevada’s health care policy landscape. There are avenues to act on the challenges outlined above and throughout this report, and an appetite within Nevada to do so.
BACKGROUND 11
METHODOLOGY
Policy recommendations in this report are divided into short- and long-term options across four domains:
(1) Modernizing eligibility systems and processes;
(2) Improving health care accessibility;
(3) Effectively leveraging Managed Care Organizations;
(4) Addressing federal immigration policy

Short-term options represent immediate and achievable opportunities for policy action with significant added value that
help build on the successes of Medicaid expansion.
Long-term options represent more ambitious, yet viable, opportunities which face larger financial and/or political obstacles to their implementation. Readers can find detailed descriptions of each policy option and their respective constraints outlined in relevant sections of this report Finally, Appendix B includes long-term policy options focused on contending with Nevada’s fiscal constraints.
METHODOLOGY 12
SUMMARY
Nevada has had to quickly adapt to accommodate the rapid growth in the Medicaid program since the 2014 expansion. While these efforts have resulted in more than 300,000 newly insured individuals, there are still opportunities for advancement to modernize the eligibility and renewal systems and processes that support Medicaid in Nevada. Specifically, this report puts forward recommendations that blend building capacity for in-person eligibility, bolstering information technology (IT) systems to automate eligibility and renewal, and changing policies to make it easier to get and keep eligible persons on Medicaid.
Short-Term
(1) Increase the share of Medicaid applications filed online;
(2) Increase the supply of eligibility workers;
(3) Adopt Medicaid state plan amendments to:
a. Establish a full presumptive eligibility program
b. Implement 12-month continuous eligibility for children in Medicaid; and
(4) Suspend, rather than terminate, Medicaid coverage for enrollees who become incarcerated
Long-Term
(1) Build IT capacity for real-time eligibility determinations;
(2) Implement income attestation and verification practices that expedite Medicaid enrollment; and
(3) Automate Medicaid redetermination
Modernizing Eligibility Systems and Processes 14
PROBLEM STATEMENT
Nevada’s Medicaid eligibility policies are largely consumer-friendly and designed to promote enrollment and retention. Unlike some states in recent years, Nevada has not imposed artificial barriers that make it more difficult to maintain coverage. On the contrary, Nevada’s implementation of Medicaid expansion and recent establishment of a state-based marketplace demonstrate the state’s continued leadership in promoting health coverage.
However, in certain areas Nevada’s progress has not kept pace with other states. Three key areas stand out as potential opportunities for improvement: eligibility determination and renewal, presumptive eligibility, and onsite determinations.
Currentsystemsinhibitautomated processes
Nevada has significantly updated its online systems for Medicaid application and eligibility screening to facilitate the significant growth of the program since expansion began in 2014. While these systems have eased the burden of application and renewal for thousands of Nevadans, there is still room to improve the utilization of the online system and to work toward automated real-time eligibility determinations and renewals. Technology, rather than willpower, likely impedes progress on these fronts: existing information technology (IT) infrastructure presents significant challenges to automating processes and is in need of modernization.
Nevada currently exceeds the national average for Medicaid eligibility determinations made in seven days or fewer for Modified Adjusted Gross Income (MAGI) applicants (i.e., those eligible for the program on the basis of income) 62 percent versus 57 percent nationally. However, less than 25 percent of determinations were completed in realtime defined by the ACA as determinations made in 24 hours or less compared with 40 percent nationally and between 50 and 75 percent in Arizona, Colorado, and New Mexico.31 Furthermore, Nevada is one of only five states that does not conduct automated renewals.32,33
Ultimately, making determination and renewal processes as smooth as possible can ensure people have an easily accessible entry point into Medicaid and that they are able to maintain coverage long-term
Demandhasoutpacedthesupplyof onsiteeligibilitydeterminations
The rapid expansion of Medicaid-eligible residents in Nevada combined with the pace of population growth has placed significant demand on the Department of Welfare and Supportive Services’ (DWSS) onsite eligibility determination capabilities. Currently, DWSS employs 35 individuals with the ability to perform onsite determinations at 132 different sites throughout Nevada.34 These individuals are either Family Service Specialists (FSS) or Supervisors who are assigned to the Targeted Outreach Partnerships (TOP) team in DWSS. Despite
Modernizing Eligibility Systems and Processes 15
this extensive coverage, there are still 53 sites that have requested but not received an eligibility worker as of December 2019
Presumptiveeligibilityhaslimitedreach
Presumptive eligibility is a critical tool that allows health care providers treating an uninsured patient to screen them for Medicaid eligibility. If they deem the patient eligible, the provider can then enroll the patient in temporary Medicaid coverage and receive Medicaid payment for services provided, even before the patient’s full Medicaid application is processed.
In Nevada, presumptive eligibility is currently limited to hospitals. Unlike many states, Nevada does not have its own presumptive eligibility program.35 The current system in Nevada exists due to a provision of the ACA that made presumptive eligibility available to all hospitals regardless of whether the state had a formal presumptive eligibility program at the time.36 Nevada has a Medicaid state plan amendment implementing this provision, as all states were required to do under the ACA.37
In addition to being limited to hospitals, this ACA provision is also limited to Medicaid beneficiaries.38 Nevada operates CHIP as a separate program (Nevada Check Up) from Medicaid, which results in the current situation where children covered by Nevada Check Up are not eligible for presumptive eligibility.
In contrast, states that have their own presumptive eligibility programs can choose for the program to have a significantly broader reach. These states are able to establish their own definitions
of what constitutes a “qualified entity” for presumptive eligibility, allowing them to expand the definition to more than only hospitals 39 For example, some states use this ability to expand presumptive eligibility to non-hospital providers such as Community Health Centers (CHCs) and Tribal health centers.
Similarly, states with separate CHIP programs that have their own presumptive eligibility programs can expand presumptive eligibility to children covered by CHIP.40
In theory, there should be less need for presumptive eligibility programs today than in the past, given the increased speed of Medicaid application processing and determinations. As discussed in this report, however, Nevada has not yet achieved a high rate of real-time Medicaid determinations compared to other states, giving presumptive eligibility an important role to play.
Finally, the current limitations of presumptive eligibility in Nevada also limit its potential as an outreach tool. States that certify other community-based providers and organizations beyond hospitals as “qualified entities” are able to take advantage of the fact that these groups may engage with Medicaideligible but uninsured people who do not frequently interact with the traditional health care system. Nevada’s lack of a formal presumptive eligibility program prevents it from taking advantage of this opportunity to reach the uninsured where they are and connect them to Medicaid or Nevada Check Up coverage.
Modernizing Eligibility Systems and Processes 16
Eligibilitypoliciesleavebehindcertain populations
Nevada currently offers 12-month continuous eligibility for children enrolled in Nevada Check Up, but not for children enrolled in Medicaid. This lack of policy alignment treats continuous coverage for children differently on the basis of which program they are enrolled in
Additionally, as of 2019 Nevada is one of only a handful of states that opts to terminate rather than suspend coverage
for individuals entering jail or prison.41 This poses challenges to returning citizens when they leave jail or prison and must reapply for Medicaid instead of having their coverage automatically reinstated. Given the high prevalence of mental and behavioral health disorders among incarcerated and formerly incarcerated individuals in Nevada, this population should be a priority for Medicaid enrollment. However, this population can be difficult to reach.
POLICY RECOMMENDATIONS
SHORT-TERM
IncreasetheshareofMedicaid applicationsfiledonlinetoexpedite eligibilitydeterminations
Nevada has made significant strides in updating its customer-facing online applications. It features many of the national best practices in online application interfaces, including a mobilecompatible application and accounts through which individuals can upload verification documentation as well as the ability to stop, start, revise, and renew their application. However, as of January 2019 only 30 to 40 percent of Nevada Medicaid applications for non-disabled groups (i.e., children, pregnant women, parents, and expansion adults) were filed online 42 This is more than ten points below the national average, as well as behind nearby states such as Arizona (72 percent), New Mexico (65 percent), and Colorado (62 percent).43 The Kaiser Family Foundation found that, on average, states
with higher rates of online applications filed also had a shorter processing time for eligibility determinations.44 Online applications are a critical arena for efforts to reduce time between application and enrollment.
During interviews, DWSS staff reported anecdotal evidence that individuals may prefer the paper application. However, continued reliance on paper applications will inhibit efforts to streamline and hasten eligibility determinations. Where possible, DWSS employees should encourage individuals to use online applications or work with the individual to jointly fill out the online application. DWSS should issue similar guidance to partner organizations assisting with Medicaid enrollment such as community-based organizations (CBOs) and CHCs. Increasing the share of online applications through Access Nevada DWSS’ online benefits application and management portal will enable Medicaid enrollees to manage their benefits longterm. It will also enable the state to
Modernizing Eligibility Systems and Processes 17
aggregate information that can enable automated systems for eligibility determination and renewal. This theme is discussed in greater depth later in this chapter.
Increasethesupplyofeligibilityworkers
The 35 DWSS employees that perform onsite determinations are stretched thin, making immediate efficiency increases difficult. While seven employees are permanently stationed in high demand locations, the remaining 28 rotate to different sites around the state on a set schedule.45
The most feasible option for expanding capabilities, then, is to hire additional eligibility workers. This option would allow for DWSS to supply eligibility workers to the 53 sites that have unmet need. This option may be difficult to pursue given the fiscal constraints Nevada faces. These constraints are detailed in Appendix B.
AdoptaMedicaidstateplanamendment toestablishafullpresumptiveeligibility program
As discussed previously, Nevada does not have its own presumptive eligibility program. This currently limits Medicaid presumptive eligibility to hospitals. By officially implementing presumptive eligibility, Nevada could capitalize on this policy’s potential to reach a broader range of uninsured Nevadans and to connect them to Medicaid coverage.
EligibilityGroups: Offerpresumptive eligibilityforchildreninNevadaCheckUp andchildrenandpregnantwomenin Medicaid,alongwithadultsandparents servedbytheIndianHealthServiceand Tribalhealthcenters
When establishing a presumptive eligibility program, Nevada will need to specify the eligibility groups to which it would apply. Prior to the ACA, presumptive eligibility was only an option for children and pregnant women, but the ACA added the options of offering presumptive eligibility to parents and childless adults.46
Currently, 20 states offer Medicaid presumptive eligibility for children and 30 states offer it for pregnant women.47 Of the 36 states with separate CHIP programs, 11 of them offer presumptive eligibility for CHIP.48 A smaller number of states offers presumptive eligibility for childless adults and parents in Medicaid, with six states including adults and nine states including parents.49
Extending presumptive eligibility to children in Nevada Check Up and children and pregnant women in Medicaid would align Nevada’s presumptive eligibility program with neighboring Colorado, New Mexico, and California all of which cover children, pregnant women, and CHIP children.50
In addition, Nevada should also consider offering presumptive eligibility for adults and parents in Medicaid. These groups are less-commonly covered by presumptive eligibility, but a broader approach could help connect Medicaideligible adults to coverage.
Regardless of whether Nevada elects to offer presumptive eligibility for adults and parents more broadly, Nevada may consider adopting New Mexico’s policy of offering it specifically for adults and
Modernizing Eligibility Systems and Processes 18
parents served by the Indian Health Service and Tribal health centers.51
QualifiedEntities: Establishabroadlist thatincludesCommunityHealthCenters, Tribalhealthcenters,andotherMedicaid andNevadaCheckUpprovidersin additiontohospitals
One major benefit of establishing a presumptive eligibility program for Nevada will be the ability to expand the range of “qualified entities” for presumptive eligibility beyond hospitals.52
To ensure that the presumptive eligibility program reaches its potential to expand enrollment outreach and meet community needs, Nevada officials should cast a wide net and carefully consider input from community-based organizations when determining which types of organizations can qualify for presumptive eligibility.
We strongly recommend offering presumptive eligibility in CHCs and Tribal health centers, but the full list can and should be broader than this. Other options for consideration include schools, correctional facilities, and Head Start programs.53
Adoptastateplanamendmentto implement12-monthcontinuouseligibility forchildreninMedicaid
Nevada currently has 12-month continuous eligibility for children on Nevada Check Up, but not for children on Medicaid.54 Twelve-month continuous eligibility is an important policy that ensures that a Medicaid-enrolled child can remain enrolled for the entire year even if their family undergoes a change in eligibility during that year.
As of January 2019, 24 states including nearby Colorado and New Mexico offer 12-month continuous eligibility for children in Medicaid.55 The concerning national decline in children’s enrollment in Medicaid and CHIP in recent months underscores the importance of maintaining policies that support enrollment retention and stable coverage for children.56
Implementing this recommendation would align Nevada’s Medicaid program with current policy in Nevada Check Up and help to promote stable enrollment for children.
Suspend,ratherthanterminate,Medicaid coverageforenrolleeswhobecome incarcerated
Until 2020, Nevada has had a policy of terminating the Medicaid coverage of individuals who become incarcerated. Nevada has been an outlier in this respect; most states merely suspend Medicaid coverage for incarcerated individuals. As of fiscal year 2019, 42 states opt to suspend rather than terminate Medicaid coverage for enrollees who enter jails, and 43 states do so for enrollees who enter prisons.57
According to our conversations with DWSS, Nevada has already been working on this policy change and plans to finalize implementation in early 2020. This policy change will make it easier to reinstate Medicaid coverage for individuals upon release from jails or prisons, improving rates of insurance coverage while also easing reentry into society for formerly incarcerated individuals.
Modernizing Eligibility Systems and Processes 19
LONG-TERM
BuildITcapacityforreal-timeeligibility determinations
As discussed above, less than 25 percent of Medicaid eligibility determinations in Nevada are completed in real-time (i.e., in less than 24 hours); this falls well below the national average. Capacity to conduct real-time eligibility determinations is contingent upon electronic data systems that can automatically query state and federal databases to verify eligibility criteria such as citizenship and/or immigration status, residency, income, social security number, and household composition. The state has built a strong foundation to conduct real-time determinations by establishing access to electronic data sources available to verify each of these factors, including but not limited to:58,59
• State Wage Information Collection Agency;
• State New Hire Database;
• Social Security Administration;
• Unemployment Insurance;
• National Vital Statistics System;
• U.S. Citizenship and Immigration Services Systematic Alien Verification for Entitlements Program; and
• Federal Data Services Hub.
DWSS reports that each of these verification processes happen separately with limited automation or system integration.60 To automate these processes would require significant IT systems upgrades, representing additional investment. While an IT overhaul can be costly, the Centers for Medicare and Medicaid Services (CMS)
will match state investment in Medicaid eligibility and enrollment systems up to 90 percent for development and design and up to 75 percent for maintenance and operations.61
Furthermore, over the long-term, investing in these systems would reduce the worker capacity currently required for eligibility determinations and increase agency efficiency.
Implementincomeattestationand verificationpracticesthatexpedite Medicaidenrollment
Currently, Nevada makes a Medicaid eligibility determination only after verifying income and other eligibility factors.62 Instead, Nevada can alter their processes to accept self-attested income and verify income after making the eligibility determination via electronic data systems (e.g., the Federal Data Services Hub, DWSS benefits data, state unemployment insurance data) a best practice to increase real-time eligibility determinations. Under this protocol the state could still maintain its Reasonable Compatibility Standard of requesting documentation if there is a discrepancy of more than $225 between self-attested income and electronic databases. However, the vast majority of applicants could receive an eligibility determination and be enrolled in Medicaid based on self-attested income without having the lag between application, determination, and enrollment.
Currently, 14 states have some form of reliance on income self-attestation, 11
Modernizing Eligibility Systems and Processes 20
with and four without post-verification procedures.63 Oregon, Oklahoma, Colorado, and Washington have all reported no increase in eligibility determination errors since changing their systems to rely on self-attested income based on state audits. Oklahoma estimates only two percent of applicants were terminated from the program after verification processes found incomes were too high compared with self-attested income.64,65
However, relying on self-attestation with post-verification requires a seamless feedback loop between the Medicaid Management Information System (MMIS) and Medicaid eligibility determination databases to allow someone to be enrolled and then undergo verification processes. Nevada’s current IT systems do not have this capacity and would need to be updated to implement a selfattestation standard.
AutomateMedicaidredeterminationto reduceprogramchurn
Nevada has implemented many Medicaid redetermination best practices such as initiating redetermination during case worker check-ins to ensure continuous eligibility, pre-populated renewal forms, telephone renewals, and 12-month continuous eligibility for Nevada Check Up enrollees. However, the state is one of only five (as of January 2019) that does not perform any automated Medicaid renewals.66 The existence of the aforementioned best practices provides a substantial launching pad for this best practice within Nevada, and lessons can be learned from other state automated determination processes (see Box 1).67,68
Like other recommendations in this section, implementing automated renewal practices will require IT systems that can automatically flag applications coming up for renewal, batch them, and query relevant data systems for updated eligibility information. This capacity would have to be built and would likely require additional IT infrastructure investment.
Box 1. Automated Renewal Case Studies
Arizona.Arizona’s online application portal automatically verifies eligibility information 45 to 60 days prior to a beneficiary’s renewal date. If the individual continues to meet eligibility requirements: (1) the portal shows the information that was used to complete the renewal; (2) states that the beneficiary was found to remain eligible; and (3) asks the beneficiary to contact the Department of Economic Security if any of the listed information has changed. Beneficiaries are automatically renewed even if they do not submit updated information.
Washington.In Washington state, 60 days before a Medicaid client’s renewal date Washington’s application portal automatically sends a batch of applications to the Federal Data Services Hub to verify identity, citizenship, and income in line with Medicaid eligibility requirements. If the information meets eligibility criteria, the state sends a letter informing the client of their Medicaid renewal. If they are deemed ineligible, the state informs individuals of their redetermination status and offers the opportunity to upload new documentation to the online portal to prove eligibility. Nearly 85 percent of cases are automatically renewed with no further documentation required.
Modernizing Eligibility Systems and Processes 21
SUMMARY
Nevada has an access to care crisis. First, the widely reported provider shortage affects all Nevadans and may disincentivize individuals from signing up for health insurance. Second, Medicaid outreach is in need of data that clearly identifies Nevada’s Medicaideligible but uninsured populations, which would enable the state to improve perceived access to Medicaid among these demographics. Adopting outreach best practices may also improve perceived access to care. While increasing access to care is a long-term undertaking, there are also interventions the state can begin working toward in the shortterm. In particular, this report recommends:
Short-Term
(1) Seek partners, projects, and funding through which to better identify the Medicaideligible but uninsured populations;
(2) Survey individuals exiting Medicaid to understand their motivations for exiting the program;
(3) Leverage well-known personalities and low-cost channels to improve the impact of existing outreach budgets;
(4) Leverage CHIP Health Services Initiatives (HSI) funding for outreach;
(5) Add a Community Health Center directory to the “Welcome to Medicaid” pamphlet;
(6) Improve frontline processes for Tribal Medicaid claims; and
(7) Support state solutions to expand the provider pool and the capacity of current providers
Long-Term
(1) Consider rebranding Medicaid;
(2) Increase Medicaid reimbursement rates;
(3) Incentivize rural students and rural service to pursue health profession careers; and
(4) Increase the quantity of residencies in Nevada
Increasing Health Care Accessibility 23
PROBLEM STATEMENT
Providershortageevidentacrossmost healthprofessionsandareasinNevada
Interviewees across Nevada flagged the state’s health care provider shortage as a key factor impacting the Medicaid population. The state’s Medicaid expansion led to an impressively sharp increase in Medicaid enrollment, but that increase was not accompanied by a commensurate expansion in access. In fact, Medicaid expansion may have exacerbated the existing provider shortage problem in Nevada, which was already worsening due to the state’s rapid population growth.
When comparing the number of medical professionals per 100,000 people in Nevada to the national average, Nevada’s numbers are significantly lower. This is true even after consistent growth in the number of providers over the last decade. For example, between 2008 and 2018, the number of licensed physicians increased by approximately 30 percent (1,387).69 Because of rapid growth in the state, the number of licensed physicians per 100,000 population only increased 17 percent during that time (176 to 206).70 Figure 2 highlights analysis conducted by the Nevada Health Workforce Research Center at the University of Nevada, Reno.71
Of note, the lowest provider to population ratios in Nevada are in rural counties. While Nevada as a whole has seen its health care workforce grow, albeit not quickly enough, rural and frontier Nevada has seen a decreasein key health professions workforce positions. For
example, in the last decade, rural and frontier counties have lost:
• 13 licensed physicians (5% decline);
• 3 psychiatrists (50% decline); and
• 11 psychologists (52% decline).72
Rural and frontier counties have seen growth in health professions workforce positions such as:
• Licensed Registered Nurses (+111, 8.5%);
• Licensed Advanced Practice Nurses (+39, 92.8%); and
• Licensed Physician Assistants (+21, 40.4%).73
Nevada’sMedicaidpopulationisamong thehardesthitbytheprovidershortage
The severe provider shortage means that there are not enough appointments available for the number of Nevadans that need them. As a result, many Nevadans struggle to secure a primary care or specialist visit. According to interviewees, Medicaid enrollees struggle more than average Nevadans to secure an appointment because not all providers accept Medicaid
Increasing Health Care Accessibility 24
Providers who do accept Medicaid often deprioritize Medicaid patients due to low Medicaid reimbursement rates relative to Medicare and private insurance Furthermore, Medicaid recipients may be more likely to miss appointments due to inflexible work schedules, travel difficulties, or lack of education on and experience with primary and specialist care. In response, some providers develop workarounds to continue to serve Medicaid patients (e.g., schedule all Medicaid appointments on one day to reduce impact of no-shows), but such
workarounds fail to significantly expand access for Medicaid enrollees
Interviewees reported that enrollees’ first appointment with a primary care provider was not the only hurdle. Even when providers attempt to assist a Medicaid recipient with scheduling referral visits to specialists, providers struggle to secure an appointment for their Medicaid patients. The wait times offered when asking on behalf of a Medicaid patient are longer than those offered when calling on behalf of a privately insured patient.
Furthermore, interviewees flagged that the perceived lack of access to care may discourage individuals from enrolling in Medicaid. The perception, and perhaps reality, that even with Medicaid individuals will not be able to see a doctor reduces the perceived value of Medicaid enrollment.
NegativeperceptionsofMedicaidmay discourageenrollment
Throughout interviews, some state health care professionals indicated perception issues that may prevent Nevadans from enrolling in Medicaid. First and foremost, some perceive Medicaid to have a negative stigma within Nevada and nationwide. Unfortunately, eligible individuals may decline to enroll in Medicaid and other government entitlements for fear of judgment from neighbors or coworkers. National-level surveys show that the lowest-income Americans suffer the most from the negative stigma, which creates a selfdefeating cycle in which those who need help the most refuse to accept it, further deteriorating their economic conditions.74 Interviewees emphasized Nevada’s










Increasing Health Care Accessibility 25
102 106 112 308 402 513 522 782 946 1075 2480 139 221 728 2170 438 978 269 320 3696 5134 54 290 302 565 725 1084 0 2000 4000 6000 Opticians Dietician and Nutritionists Surgical Technologists Occupational Therapists Pharmacists Radiologic Technologists Speech Language Pathologists Physical Therapists Paramedics Clinical/Medical Lab… Social Workers Psychiatrists Licensed Clinical Social… Psychologists Mental Health & Substance… Dental Assistants Dental Hygenists APRNs Certified Registered Nurse… Licensed Practical Nurses Registered Nurses Physician Assistants Physicians in Primary Care Physicians in General Practice Physicians in Surgical… Physicians in Other Specialties Physicians in Medical… Other Mental & Behavioral Oral Nursing Physicians and Physician Assistants
100,000
Figure 2. Additional Providers Needed to Meet the National Average for Providers per
libertarian influence, particularly as it relates to a culture of independence and individual hard work. These cultural views may ultimately obstruct Medicaid enrollment.
Lackofknowledgeaboutthe
characteristicsofNevada’sMedicaideligiblebutuninsuredpopulationimpede outreachefforts
A recent report by the Guinn Center highlighted key characteristics of Nevada’s uninsured population, but relatively little about the characteristics of the subpopulation that may be eligible for Medicaid.75 However, it may be reasonable to extrapolate characteristics of Nevada’s Medicaid-eligible but uninsured population based on the Guinn Center’s information about Nevada’s uninsured population. For example, many Medicaid-eligible but uninsured individuals likely live in urban areas given that Clark, Carson, and Washoe counties host 90.5 percent of the state’s population and 91.6 percent of the state’s uninsured. Further, Nevada’s significant Latino population likely hosts a disproportionate share of Medicaid-eligible but uninsured individuals Latino individuals represent just 36 percent of Nevada’s population but 59 percent of its uninsured population. Medicaid-eligible individuals within this population may be difficult reach due to language barriers, fear of Medicaid enrollment’s repercussions for undocumented family members, and generally younger age. Young adults are traditionally difficult to reach, and Latino Nevadans’ median age is 27.8 relative to the state median age of 37.7.
In addition to data about Nevada’s Medicaid-eligible but uninsured
population, decisionmakers expressed interest in data concerning the relative success of existing outreach efforts and outcomes for Nevadans who lose coverage in the transition into or out of Medicaid. These data gaps the characteristics of the potentially Medicaideligible but uninsured population and an evaluation of current outreach efforts may compound existing access issues and impede efficient outreach efforts.
POLICY RECOMMENDATIONS SHORT-TERM
Seekpartners,projects,andfunding throughwhichtobetteridentifythe Medicaid-eligiblebutuninsured population
Immediately following Medicaid expansion, Nevada’s enrollment and coverage rates spiked. Now that these rates have plateaued, the Medicaid Office may seek to prioritize efforts to identify the remaining Medicaid-eligible but uninsured populations, as well as outreach strategies that can most effectively reach these populations. More data will help state officials coordinate targeted and efficient outreach efforts based on a refined understanding of who needs to be targeted and whether or not this population is currently reached by Medicaid outreach.
Short-term steps that may facilitate this data collection include collaborating with Nevada Health Link to leverage the data recently acquired through Nevada’s
Increasing Health Care Accessibility 26
transition to a state-based marketplace. The state could also seek technical assistance from academic researchers or state-focused NGOs to identify and/or model characteristics of Nevada’s Medicaid-eligible but uninsured population.
SurveyindividualsexitingMedicaidto understandtheirmotivationsforexiting theprogram
Recent national data indicates a troubling decline in Medicaid enrollment. From December 2017 to July 2019, net Medicaid and CHIP enrollment dropped by 1.1 million among children and 750,000 among adults 76 Although Nevada’s 0.9 percent decline in Medicaid enrollment over this period was less than the national average decline of 2.6 percent, the state should closely monitor its enrollment trends going forward 77 A survey sent to individuals as or after they exit Medicaid may help the state to understand what motivates individuals who drop Medicaid coverage and to craft policy solutions that address this problem. This recommendation may also further clarify the motivations of the Medicaideligible but uninsured population.
Leveragewell-knownpersonalitiesand low-costchannelstoimprovetheimpact ofexistingoutreachbudgets
Medicaid’s slowing growth since expansion presents an opportunity for the state to re-calibrate its outreach efforts. The state and its partners currently employ a number of the “best practice” outreach strategies identified in the literature. These include outreach efforts at hospitals, clinics, and detention centers; mobile-enabled enrollment technology; and a Medicaid enrollment van that travels
through Las Vegas and some rural communities. To build on these best practices, the literature suggests implementing these strategies as among the most efficient ways to improve Medicaid enrollment:78
• Advertise through broad market mediums like radio, television, and newspapers;
• Leverage Managed Care Organizations as a marketing and outreach partner;
• Recruit the governor and other senior state figures to appear on advertisements, as their personal commitment would show that Medicaid is an executive-level priority;
• Leverage other well-known personalities such as the Las Vegas Golden Knights and Aces in advertisements to generate mass appeal;
• Set up educational booths at community gatherings such as state fairs, job fairs, and local sporting events;
• Conduct outreach at local businesses, job placement sites, grocery stores, schools, community centers, places of worship, and other locations that families frequently attend; and
• Use mobile technology as an outreach and enrollment tool, especially given many low-income individuals’ only access to the internet is through their mobile device.
In addition, the state may seek targeted outreach strategies for populations that make up a high proportion of Nevada’s Medicaid-eligible but uninsured population. Until additional data on the characteristics of this population can be
Increasing Health Care Accessibility 27
collected to guide outreach efforts, it is reasonable to assume that outreach should be targeted toward Nevada’s urban, Latino, American Indian, and young adult populations. Appendix A features a list of resources and best practices for outreach targeted at these subpopulations. These recommendations can be implemented in the near future to maximize the impact of ongoing and future outreach efforts.
LeverageCHIPHSIfundingforoutreach
Despite the importance of Medicaid enrollment outreach, a persistent challenge is the relative lack of dedicated funding for such outreach. One potential source of funding for future enrollment outreach efforts is the Children’s Health Insurance Program Health Services Initiatives (CHIP HSI), which is available to support state initiatives focused on improving health outcomes for lowincome children. For example, until 2019 Nevada had a CHIP HSI to provide “behavioral health and early intervention services to children in targeted, high-risk, public schools,” called the Resources for the Early Advancement of Child Health (REACH) program.79 States can receive federal funding for HSIs at the CHIP matching rate, which in Nevada is 86.25 percent for fiscal year 2020.80 However, such funding must fall under the 10 percent cap on administrative costs in CHIP (i.e., the state’s administrative costs and HSI spending combined must be less than 10 percent of CHIP spending).81
To the extent that Nevada Check Up currently has room under the 10 percent cap, Nevada should take advantage of HSIs to leverage federal and state CHIP funding to support targeted outreach
efforts to connect low-income children to Nevada Check Up or Medicaid coverage.
AddaCommunityHealthCenterdirectory tothe“WelcometoMedicaid”pamphlet toincreaseperceivedaccess
All CHCs accept Medicaid. Because many private providers in Nevada do not regularly accept Medicaid, it is important to ensure that Medicaid enrollees are aware of the location, hours, and services provided by their nearest CHC. However, because Nevada CHCs lack consistent branding, many Medicaid-eligible individuals may fail to recognize and utilize their nearest CHC. As such, Nevada should consider adding a directory of CHCs to the “Welcome to Medicaid” packet currently distributed by DWSS and MCOs. CHCs should be marketed as “community health centers that accept Medicaid” to avoid any potential stigma around federally supported health care. CHC information in the welcome packet should include: a state map of CHC locations; each location’s address and contact information; a list of basic services provided by CHCs; and a footnote that explains that additional providers may provide Medicaid and should be called directly. This directory requires minimal additional financing or staffing; it is wellsuited for short-term implementation.
ImprovefrontlineprocessesforTribal Medicaidclaims
Tribal communities face a number of unique obstacles, exemptions, and regulations when they seek Medicaid coverage. American Indian patients enrolled in Medicaid who are referred from an Indian Health Services (IHS) facility to non-IHS care should be covered as would an MCO beneficiary who had been
Increasing Health Care Accessibility 28
referred by their primary care provider to a specialist.82 However, the unique circumstances of American Indian Medicaid patients are sometimes misunderstood or not recognized by frontline MCO staff, who may deny payment when American Indians seek referred specialist care. MCOs can address this stumbling block by including all Tribal providers within their directory of approved providers and/or by improving education among the frontline workers that handle insurance claims from American Indian Medicaid enrollees.
Supportstatesolutionstoexpandthe providerpoolandthecapacityofcurrent providers
Poor access to care for Medicaid recipients due to the provider shortage hinders efforts to increase Medicaid enrollment among eligible populations. Enrolling may seem pointless for those who view efforts to seek care even with coverage as a hopeless endeavor. The state should support and advocate for solutions to the provider shortage due to the disparate impact of the shortage on Medicaid patients. Nevada will not be able to completely fix its provider shortage in the next few years. It will take time to graduate new residents and ruralfocused students. However, there are near-term solutions that the state can embrace and advocate for now: near-term solutions can immediately reduce the negative impacts of the provider shortage. Possible policy solutions for the state to increase capacity and supply include:
Pilotingtext-messagereminderswith providerstolowerno-showrate
Interviewees shared that using textmessage reminders about appointments
helped reduce no-show rates among lowincome patients at one health center in the state. Nevada should consider a partnership with providers to pilot a similar program. Such a pilot could help nudge recipients to more appointments, improving health and increasing provider confidence in Medicaid recipients’ likelihood of attending an appointment. The pilot program would not require significant funding and would have immediate impact, making it a simple and politically viable policy.
Reassessingscopeofpracticelimitations
Nevada is much closer to the national average for the number of physician assistants per 100,000 population than for most other health care professions. Expanding the legal scope for such a position would be an immediate step towards solving the provider shortage. Such expansions would allow current Nevada health professionals to do more and would help recruit health professionals from other states. For example, when Nevada allowed Advanced Practice Registered Nurses (APRNs) to operate their own practices without a physician, the number of APRNs doubled in four years (760 to 1,595).83 The state’s extreme provider shortage may place enough pressure on politicians to pursue this policy change despite likely opposition from the state’s current provider groups.
Reviewinglicensingrequirementsand processes
Interviewees shared that Nevada’s licensing requirements are among the most restrictive in the country. Loosening such requirements may widen the pool of Nevada health professionals (e.g.,
Increasing Health Care Accessibility 29
facilitating the licensing of foreign-born and/or foreign-trained doctors), as well as help recruit providers from other states. The primary obstacle to this policy may be provider opposition, but the nearimmediate nature of this solution may make it politically viable.
LONG-TERM
ConsiderrebrandingNevadaMedicaid
Over 30 states refer to their Medicaid program by an alternative name. The majority of them use state mascots or other easily identifiable names that evoke state pride. DenaliCare (Alaska), HuskyHealth (Connecticut), SoonerCare (Oklahoma), and TennCare (Tennessee) are a few examples. Nevada’s Medicaid program could rename itself SilverCare, NevadaCare, or any other name that elicits state pride. Renaming the Medicaid program could help build its brand with Nevadans as a Nevada-specific rather than federal program, which may influence how eligible individuals feel when deciding whether to sign up.
IncreaseMedicaidreimbursementratesto increasethenumberofproviders acceptingMedicaidpatients
The larger the discrepancy between commercial and Medicaid reimbursement rates, the more the provider shortage impacts Medicaid recipients disproportionately. An increase in rates would help ensure equitable access to providers across the state. However, fiscal constraints may impede progress on this policy change.
Incentivizeruralstudentsandruralservice topursuehealthprofessioncareers
For most health professions, the provider shortage is worst in rural areas of Nevada.84 To increase the number of medical professionals willing to serve in such communities, the state should incentivize rural students to apply to medical schools in the state. Rural medical students serve in rural areas after graduation at higher rates than non-rural students.85 Additionally, the state should consider scholarship programs that require a certain number of years of service in rural Nevada after graduation; even students who leave Nevada for residency would need to return to serve their promised years. The fiscal climate of Nevada would likely delay the passing of such initiatives even if passed, this solution would take years to show impact due to the long timeline of medical education.
Increasethequantityofresidenciesin Nevada
Multiple interviewees emphasized that more than 50 percent of doctors stay in the area where they complete their residencies; thus, increasing the number of doctors who complete their residency in the state will increase the number who ultimately stay in Nevada. Nevada has already made strides in this regard, but additional residencies particularly at facilities that benefit underserved populations such as Tribal health centers and urban and rural CHCs should remain a key priority for the state. Identifying funding for residencies will be a challenge in Nevada’s fiscal climate. This policy would address the provider shortage over a longer time horizon due to the timeline of medical education.
Increasing Health Care Accessibility 30

SUMMARY
Nevada is undergoing a process of stakeholder engagement in advance of a future reprocurement for their Managed Care Organizations (MCOs) the entities that serve as the insurers for nearly three-quarters of Medicaid recipients in the state. This presents a substantial opportunity for the state to articulate its priorities and leverage MCOs to utilize managed care to a greater degree to support the health and wellbeing of Medicaid enrollees, particularly the most vulnerable subgroups such as formerly incarcerated or homeless individuals. This report recommends including a mix of shortand long-term priorities in the upcoming MCO Request for Proposals (RFP):
Short-Term
(1) Reduce appointment “no-show” rates; and
(2) Designate justice system and housing services coordinators
Long-Term
(1) Support community reinvestment efforts;
(2) Streamline data-sharing between the state and MCOs; and
(3) Explore Alternative Payment Models
Effectively Leveraging Managed Care Organizations 32
PROBLEM STATEMENT
MCOs have a responsibility to ensure health care access and quality of care for their enrollees. In Nevada, three national MCOs UnitedHealth Group, Anthem, and Centene provide care coordination for Medicaid enrollees in Clark and Washoe counties, where 88 percent of Nevada’s population resides.86 Effective and efficient management of these contracts is important both to patient outcomes and the reputation of the Medicaid program.
In order to guarantee enrollee access to essential services, the state requires MCOs to meet robust network adequacy standards. Given the provider shortage, there are questions surrounding whether MCOs are meeting those standards. While the state conducts regular network adequacy validation, this is an area for constant vigilance.87 Interviews with stakeholders in the state revealed that some providers are not accepting Medicaid patients or have unreasonably long wait times.
In general, MCOs are equipped to play an important role in addressing social determinants of health (SDOH), but often do not go beyond their required services. In our interviews, stakeholders suggested that MCOs in Nevada have pulled back their SDOH investments in recent years. To some extent, MCOs have little incentive to bear the upfront costs of these investments if they are not guaranteed to reap the benefits, given the churn between managed care plans.
MCOs are also in a position to improve care coordination for enrollees that churn
in and out of the program. Many of Medicaid’s highest-cost users are patients with complex care needs that cycle through hospitals, homeless shelters, and jails 88 Improved health care coordination for this population could produce significant cost-savings for the state. MCOs have the flexibility and resources to best coordinate care for these enrollees. Yet, MCOs in Nevada have not yet implemented creative strategies used in other states for supportive housing and justice system transitions at significant scale. For example, stakeholder interviews revealed that MCOs are doing little to coordinate their activities with local partners even though they are serving the same population.
To better coordinate care for enrollees, the state and MCOs should streamline data-sharing. While the MCOs share a series of quarterly reports, as required by the MCO agreement, stakeholder interviews suggest that enrollee contact information should be more continuously updated, checked for accuracy, and shared with the state
In addition, the state and MCOs should collaborate to better match enrollee data with databases of homeless and justiceinvolved individuals. In order to better manage their care, MCOs need to know when enrollees are experiencing housing crises or transitioning through the justice system. For example, Nevada currently terminates Medicaid eligibility for incarcerated individuals. Plans need to know when their enrollees are incarcerated and released, in order to
Effectively Leveraging Managed Care Organizations 33
reinstate them in Medicaid and maintain continuous access to care.
Finally, Nevada MCOs should embrace alternative payment strategies (APMs) more fully. Currently, MCOs are simply administering based on fee-for-service (FFS) rates. Implementing innovative payment strategies would be more likely to drive improved health outcomes and cost-savings.
POLICY RECOMMENDATIONS
The state is currently undergoing a process of stakeholder engagement in advance of a future re-procurement for their MCOs. The procurement process is an important opportunity to signal priorities for performance improvement. The statement of work (SOW) included in the RFP should be a roadmap for the state’s managed care expectations, assessment of proposals, and future contract requirements 89 It is important that the SOW establish clear performance priority areas and create meaningful incentives and consequences for performance.
The state should highlight its priorities in the SOW, along with measurable objectives and a timeline for revisiting plan performance to these objectives. The state should consider asking plans to present progress made toward these objectives six months after the start date of the new contracts, though some recommendations highlighted here may take longer to implement.
Box 2. Arizona MCO Contract: Transportation
TheContractorshallensurethat populationswithongoingmedical needs,includingbutnotlimitedto dialysis,radiationandchemotherapy, havecoordinated,reliable,medically necessarytransportationtoensure membersarriveon-timeforregularly scheduledappointments.
TheContractorshallestablish processestomonitorandreducethe appointment“no-show”rateby providerandservicetype.
Arizona’s MCO contract language (excerpts included in Boxes 2–4 and Appendix D) can serve as a model for updates to the Nevada SOW. Arizona’s state Medicaid program is operated by Arizona Health Care Cost Containment System (AHCCCS). AHCCS contracts with two of the three national MCOs that participate in Nevada: UnitedHealth Group and Centene. In Arizona, 84 percent of Medicaid enrollees are enrolled in managed care, compared to 69 percent in Nevada.90 Arizona has been a leader in implementing alternative payment strategies, streamlining justice system transitions, and providing housing supports to Medicaid enrollees, and offers important lessons for Nevada
SHORT-TERM
Reduceappointment“no-show”rates MCOs should be made responsible for reducing the appointment “no-show” rate amongst their enrollees, including providing transportation when appointments are far away and there is
Effectively Leveraging Managed Care Organizations 34
Box 3. Arizona MCO Contract: Justice System Transitions
JusticeSystemLiaison:whoislocated inArizona,isthesinglepointof contactforcommunicationwiththe justicesystem;istheinteragency liaisonwiththeArizonaDepartment ofCorrections(ADOC),CountyJails, Sherriff’sOffice,CorrectionalHealth Services,ArizonaDepartmentof JuvenileCorrections(ADJC),Arizona OfficeoftheCourts(AOC)and ProbationDepartments;andis responsibleforJusticeSystemreachininitiatives.
Box 4. Arizona MCO Contract: Housing-Related Supports
TheContractorshallalsoensurethata staffperson(s)isdesignatedasthe expert(s)onhousingandeducation resourceswithintheContractor’sservice area.Ingeneral,thisindividualmustbe availabletoassistmemberswithupto dateinformationdesignedtoaid membersinmakinginformeddecisions abouttheirindependentlivinggoals.
little reliable public transportation available. The state should require that MCOs monitor and ensure that enrollees attend their appointments and establish processes to reduce appointment “noshows.”
Designatejusticesystemandhousing servicescoordinators
The state should require each MCO plan have a designated justice lead who acts as the project manager for transitions for justice-involved enrollees. For example, Arizona’s MCO contract requires each
plan to have a justice liaison responsible for collaborating with all relevant stakeholders in their geographic service area. The justice liaison is responsible for justice system reach-in, designing protocols to re-enroll individuals coming out of jail and prison, and connecting enrollees to physical and behavioral health services upon re-entry 91
In interviews, Arizona Medicaid officials pointed to the contractually required justice lead as critical to the success of their justice system transitions initiative. Arizona Medicaid also has quarterly criminal justice transition meetings with the justice liaisons from each plan.
Similarly, each MCO plan should have a designated housing lead who acts as the project manager responsible for coordinating with housing providers in the service area. The housing lead should be an expert on the provision of housing supports in the region and should refer Medicaid enrollees for housing-related supports and coordinate with housing providers.
LONG-TERM
Supportcommunityreinvestmentefforts
The state should require that MCOs reinvest a percentage of their profits into the community. For example, Arizona’s MCO contract requires that plans commit six percent of their profit to community reinvestment. Most Arizona MCOs have used these community reinvestment funds for SDOH activities, although this is not explicitly required 92
Effectively Leveraging Managed Care Organizations 35
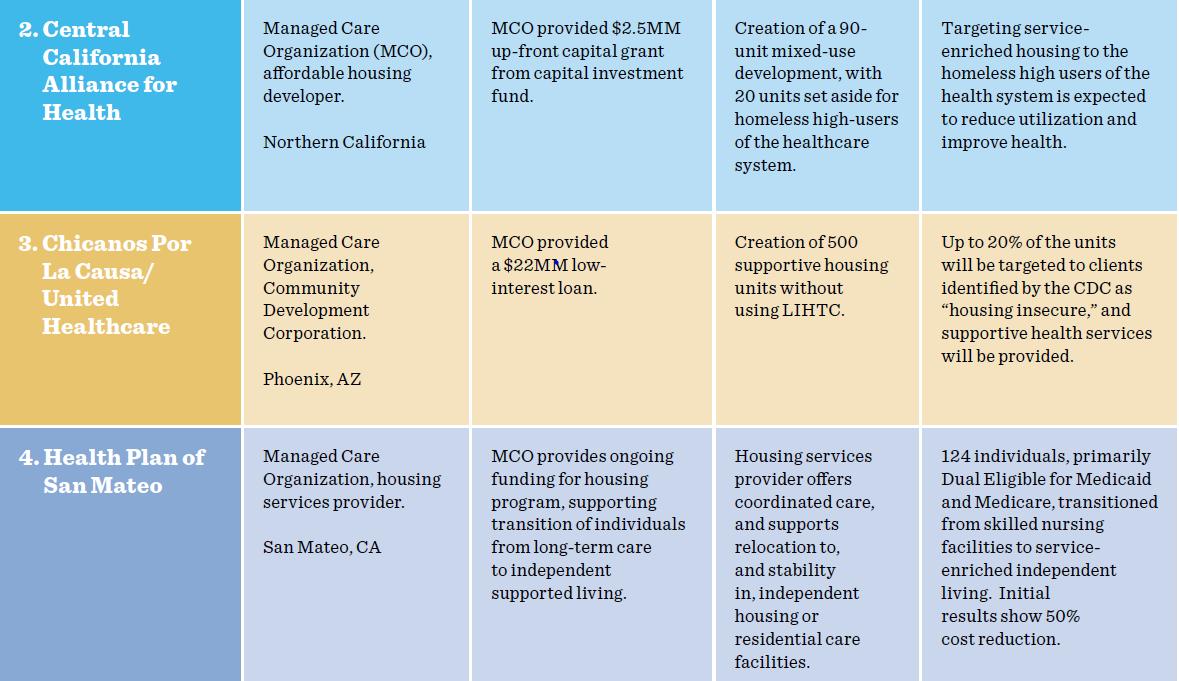
Nevada should encourage community reinvestment dollars be used to develop innovative partnerships with community development organizations and housing providers. For example, UnitedHealthcare partnered with a community development organization in Phoenix, AZ to buy an apartment complex, creating 500 supportive housing units for their enrollees 94
Streamlinedata-sharingbetweenthe stateandMCOs
The state should consider streamlining data-sharing between the Medicaid program and MCOs. Currently, MCOs report to the state on a quarterly basis. These reports likely need to be more frequent to capture the most current enrollee contact information. For example, in Arizona MCOs have direct access to the state system to update enrollee contract information
continuously. Arizona officials made this decision because MCOs typically have more updated contact information for enrollees than does the state, due to their care coordination activities.
In addition, the state should work with counties and MCOs to improve their data-matching capabilities with databases of homeless and justiceinvolved individuals. This should be the responsibility of the plans’ justice and housing leads and will require creating data-sharing agreements and Memoranda of Understanding (MOUs) with state and county-level public agencies. Data matching with these databases is critical to coordinate care for enrollees experiencing incarceration and housing crises.
Data sharing should be as close to realtime as possible. For example, Arizona
Effectively Leveraging Managed Care Organizations 36
Table 4. Innovative MCO Partnership Models93
MCOs get a list of enrollees that are experiencing justice transitions on their daily roster. They are notified 30 days before enrollees are released from jail or prison, which gives them time to put care coordination plans in place.
Twenty-three states have electronic, automated data exchange processes between corrections and Medicaid agencies.95 This allows for the reinstatement of Medicaid enrollment for incarcerated individuals upon release. Notably, all of the states with data exchange processes in place suspend rather than terminate Medicaid eligibility when an enrollee is incarcerated. As noted in our Modernizing Eligibility Systems and Processes recommendations, Nevada is currently planning to adopt this approach in fiscal year 2020, which will allow Medicaid to be more quickly and easily reinstated upon reentry.
Several states, including Michigan, Massachusetts, Connecticut, and certain counties in California match Medicaid data with homelessness data on a quarterly basis 96 Arizona is currently considering this strategy as well. These states match Medicaid enrollee data with Homeless Management Information Systems (HMIS). HMIS are databases that each regional Continuum of Care (CoC) are required to maintain by the U.S. Department of Housing and Urban Development (HUD).
In interviews with MCOs in California, MCOs emphasized that quarterly data
matching with HMIS was crucial to their supportive housing strategy. Data matching allowed them to prioritize the highest-need enrollees for scarce supportive housing units.
ExploreAlternativePaymentModels
The state should consider implementing APMs to incentivize MCOs to invest in the state priorities outlined above. We recommend that the state look closely at Arizona’s Alternative Payment Model Initiative (included in Appendix D), as a model 97
In 2016, Arizona received a State Innovation Model (SIM) grant to focus on three areas of care coordination: individuals served by the American Indian Health Plan, individuals transitioning out of incarceration, and behavioral and physical health integration for individuals with complex health conditions. With these priorities in mind, Arizona required their MCOs reach 50 percent value-based payments by 2019 98
Under the APM Initiative, contractors may receive funds above capitation rates for implementing APM arrangements and select quality measures identified by the state. The performance-based payments made by MCOs to providers are reimbursed by AHCCCS through a lump sum payment at the completion of the contract year. Incentive payments may not exceed five percent of the approved capitation payments 99
Effectively Leveraging Managed Care Organizations 37
100

SUMMARY
Twenty percent of all Nevadans more than half a million individuals were born outside the United States. Understanding the unique health coverage challenges facing immigrant communities is critical to comprehend uninsurance in the state. Federal immigration policies, including the public charge rule, have created a chilling effect across immigrant communities and families. While the state cannot directly change federal immigration policies, it can adopt policies and outreach efforts to help immigrant communities feel safe to sign up for health insurance. In particular, this report recommends:
Short-Term
(1) Waive the five-year waiting period for Medicaid eligibility for qualified non-citizen pregnant women;
(2) Develop a coordinated education and outreach strategy on the public charge rule, including forming a working group and producing statewide guidance on the impact of the rule;
(3) Compile a directory of Community Health Center locations to be shared with the undocumented immigrant community; and
(4) Incorporate a ‘public charge’ option in Medicaid leavers survey
Long-Term
(1) Build in safeguards for immigrants in automatic Medicaid determination procedures; and
(2) Allocate state-only funds to extend Medicaid coverage to undocumented immigrants.
Addressing Federal Immigration Policy 39
PROBLEM STATEMENT
Federallawinhibitsimmigrants’accessto healthinsurance
One in five Nevadans were born outside of the United States, with more than half a million immigrants calling the Silver State home in 2017.101 Nevada had the sixthhighest share of foreign-born residents in the country that year.102 The state’s immigrants primarily hail from Mexico (39.5 percent) and the Philippines (14.3 percent), and more than half (46.8 percent) are non-citizens.103 Due to the size of this population, every stakeholder we spoke to emphasized the significant and specific barriers that immigrant communities face with regard to accessing affordable health care.
One of the principal barriers is eligibility restrictions for public health benefits under federal law. To be eligible for coverage through most forms of Medicaid or CHIP (Nevada Check Up), an immigrant must be a “qualified non-citizen” a designation that includes Lawful Permanent Residents (LPRs) and other subgroups and meet their state’s income and residency rules.104 In addition, the Trump administration’s recent policies, in particular changes to the public charge rule, have led to some immigrants’ reluctance to access such benefits. The shifting policy landscape exacerbates existing fear and misinformation among immigrant communities who are already wary of receiving federal benefits or sharing any personal information with government entities. Quantifying the chilling effect of federal immigration policies in Nevada is difficult; however, this chilling effect has been examined in
national research and our interviews in Nevada supported its existence as a significant factor.
Nevada’s high share of mixed-status families further complicates matters, as barriers to health access have widespread effects across households. In 2016, 16 percent of the state’s population (about 457,200 Nevadans) were U.S.-born Americans with at least one immigrant parent. More than half of those individuals lived with at least one undocumented family member between 2010 and 2014. During the same period, more than one in seven children in the state were U.S. citizens living with at least one undocumented family member (95,973 children in total).105 Therefore, any immigrant-specific barriers to accessing health care in Nevada, like those detailed below, have ripple effects within families and across whole communities in the state.
Lawfullyresiding,non-citizenpregnant womenstillfacebarrierstoMedicaid access
Even after attaining qualified non-citizen status, immigrants must wait five years to access Medicaid or CHIP benefits. However, federal law allows states to waive the waiting period for children and pregnant women. In 2017, former Governor Brian Sandoval signed Senate Bill 325 to waive this waiting period for children 18 years and younger.106
Nevada joins 33 other states with similar exemptions.107 The Nevada Division of Public and Behavioral Health anticipated that 7,484 children would become eligible for coverage under Medicaid and Nevada Check Up during each fiscal year 2017-
Addressing Federal Immigration Policy 40
2018 and 2018-2019 as a result of SB 325.108 The Nevada Legislature, however, has not pursued similar legislation to waive the five-year waiting period for qualified non-citizen pregnant women, creating an opportunity for action in the 2021 session.

Thepublicchargerulehascreateda chillingeffectonMedicaidandCHIP enrollment
On August 14, 2019, the Department of Homeland Security (DHS) published a new rule expanding the public charge ground of inadmissibility in the Immigration and Nationality Act (INA). The policy would bar more immigrants from becoming LPRs
because of their potential future use of public benefits. In particular, under the rule, non-U.S. nationals would be inadmissible to enter the country and thus ineligible to obtain LPR status if they are “more likely than not at any time in the future to receive one or more public benefits...for more than 12 months within any 36-month period.”109 Most forms of Medicaid would count as ‘public benefits’ under the rule. This change represents a dramatic break from previous policy, under which the federal government had specified that it would not consider use of Medicaid, CHIP, or other non-cash programs in public charge determinations.110
Addressing Federal Immigration Policy 41
Figure 3. Medicaid/CHIP Coverage for Lawfully Residing Immigrant Children and Pregnant Women, January 2019111
Days before the rule was set to be implemented on October 15, 2019, the U.S. District Courts for the Southern District of New York, Northern District of California, Eastern District of Washington, Northern District of Illinois, and District of Maryland ordered that DHS cannot implement and enforce the new rule anywhere in the United States until the relevant legal challenges were resolved. However, in December 2019, the U.S. Court of Appeals for the Ninth Circuit lifted the preliminary injunctions from the courts in Washington and California; a few days later, the U.S. Court of Appeals for the Fourth Circuit lifted the injunction from the court in Maryland In January 2020, the Supreme Court lifted the nationwide preliminary injunction from the court in New York.112 As a result, DHS is now free to move forward with implementing the public charge rule in all states except Illinois while the legal challenges work their way through the courts.
Even prior to the rule’s implementation, most stakeholders we spoke with confirmed that the rule is leading to decreases in participation in Medicaid among immigrant families and their primarily U.S.-born children for several reasons
Those who are directly impacted by the policy may have disenrolled in anticipation of the rule taking effect or because they did not know that courts had halted its implementation. The rule will affect people seeking to become LPRs, or green card holders, and those seeking to immigrate to the U.S. It also will affect certain individuals looking to extend or adjust their non-immigrant status while in
the country.113 In 2016, 11,555 Nevadans obtained LPR status, many of whom were already present in the U.S.114 LPR status comes with stronger protection from deportation and is a key step toward citizenship for immigrants seeking naturalization. Thus, many individuals seeking to become LPRs may prematurely leave Medicaid out of an abundance of caution. Other individuals may have disenrolled prematurely because they already believed that the rule had gone into effect and did not know about the preliminary injunctions that initially halted its implementation before being lifted.
Some Nevadans may not understand who the rule impacts, disenrolling themselves or their children in confusion. In a significant narrowing from the proposed rule, the final rule only affects applicants for admission or adjustment of status (not their family members). Thus, it should not have negative immigration consequences for the vast majority of LPRs, naturalized citizens, or members of the families of those seeking admission or status adjustment. Additionally, applicants for admission to the country are unlikely to have received public benefits in this country in the recent past, and those hoping for status adjustment will have been ineligible for most of the relevant benefits.115 Nevertheless, previous experience and recent research indicate that the rule will cause people to forsake Medicaid enrollment or to disenroll themselves and their children from programs like Medicaid. This occurs because they do not understand the rule’s impact and fear that their or their children’s enrollment could jeopardize their or their family members’ immigration status.116 Stakeholders in Nevada
Addressing Federal Immigration Policy 42
confirmed that many immigrants incorrectly believe that the rule may have negative implications for them or their children.
The rule increased fear broadly across immigrant families about using public programs for themselves and their children, regardless of whether they are directly affected by the changes.
Hundreds of thousands of Nevadans live in mixed immigration status families that may include lawfully present immigrants, undocumented immigrants, and/or citizens. According to those interacting with Nevada’s immigrant communities, the public charge rule is having a strong chilling effect, making many people in immigrant households both citizens and noncitizens fearful of receiving any public benefits. In other words, people are disenrolling from or not applying for benefits for themselves and other family members because of fear that benefit receipt will have negative immigration consequences.
If the public charge rule remains in effect for the long-term, automatic Medicaid determination procedures will pose an additional challenge for Nevada. One advantage of the ACA has been to streamline eligibility procedures. Some states have taken that further, adopting programs such as express-lane eligibility and broad presumptive eligibility programs. Such initiatives might raise additional concerns under the public charge rule because they might have the unintended consequence of subjecting immigrants to a Medicaid application or screening without their knowledge. In Nevada, this might be an issue on the new Nevada Health Link if individuals applying
for subsidized marketplace coverage appear Medicaid eligible and are automatically referred for a Medicaid determination without their knowledge.
Undocumentedimmigrantshavelimited coverageoptions
Undocumented immigrants face the most significant barriers to health care access of any foreign-born subgroup. Under federal law, this population cannot access Medicaid, CHIP, or subsidies through Nevada Health Link, and can rarely access employer-sponsored insurance.117 Undocumented immigrants must therefore resort to purchasing private insurance or seeking care at Community Health Centers (CHCs) or emergency rooms. However, stakeholders reported that many immigrants are unaware of CHCs in their area, and thus travel longer distances than necessary to access care.
Estimates of the size of Nevada’s undocumented population range from 129,000 to 210,000 individuals. While it is a point of debate within the state,118,119 according to estimates in a recent Guinn Center report, undocumented immigrants represent nearly one-quarter (23.7 percent) of Nevada’s uninsured population.120
There are few avenues available to expand Medicaid coverage to undocumented Nevadans. The first option is for the Nevada Legislature to pass a bill authorizing the use of state-only funds to extend Medicaid benefits to this population, as California has done. A much loftier goal requires action from Congress to pass federal immigration reform and grant legal status to some portion of the undocumented population,
Addressing Federal Immigration Policy 43
allowing them to enroll in Medicaid and CHIP and access marketplace subsidies. Given the current gridlock in Washington, this outcome remains unlikely in the nearterm.
Addressing Federal Immigration Policy 44
POLICY RECOMMENDATIONS
SHORT-TERM
Waivethefive-yearwaitingperiodfor Medicaideligibilityforqualifiednoncitizenpregnantwoman
The Nevada State Legislature should pass a bill allowing qualified non-citizen pregnant women to access Medicaid without a five-year waiting period. Most of the stakeholders we spoke to agreed that this proposal is politically feasible, given the Legislature’s and former Governor Sandoval’s willingness to pass a similar bill in 2017 that waived the waiting period for children under 19 years of age. Twentyfive states have already waived the waiting period for lawfully present pregnant women, including six states in the West: California, Colorado, Nebraska, New Mexico, Washington, and Wyoming.121
The Legislature should make this policy a priority for the 2021 legislative session. There is political will among stakeholders and legislators to pursue this type of legislation in the upcoming session. This policy would improve birth and maternal health outcomes. Given the severe racial disparities in maternal mortality rates, it would also promote health equity, building on Governor Sisolak’s recent creation of a Maternal Mortality Review Committee.122 This proposal builds upon reforms already enacted for immigrant children and would follow the precedent set by a number of states in the region. While precise estimates of the number of persons impacted have not been published, clearly advancing the health
and wellbeing of this important population would be a step toward more comprehensive coverage in Nevada.
There are fiscal implications for this proposal for context, the 2017 legislation for immigrant children had an estimated cost of $39 million over a period of two fiscal years but significant public health benefits 123,124 Moreover, expanding Medicaid eligibility for this population could reduce the fiscal burden of uncompensated care and reliance on emergency care.
Developacoordinatededucationand outreachstrategyonthepubliccharge rule
As noted, chilling effects on Medicaid and Nevada Check Up participation likely extend beyond individuals who could be directly affected by the public charge rule’s changes. Outreach and education efforts to immigrant communities and their families, aimed at reducing fears and confusion stemming from the rule, can minimize this effect. Those working with immigrant communities in Nevada noted that educational efforts were often successful in spurring reenrollment in public benefits for those who had previously disenrolled due to the public charge rule. This strategy should include two primary components:
OrganizeaNevadapublicchargeworking group
Nevada should organize a working group to develop a clear and unified message about the public charge rule. Its goal
Addressing Federal Immigration Policy 45
should be to mitigate the rule’s chilling effect on access and to help immigrant Nevadans make informed decisions about their health and immigration status. It should explain the current state of the rule, who is affected, and that Nevadans not affected by the rule should not stop using public benefits unnecessarily. The working group should consist of public and private organizations with expertise in immigration policy and public benefits, as well as those with strong connections to the immigrant community who are seen has trusted messengers. Potential members could include:
• Nevada Office for New Americans;
• Nevada Department of Health and Human Services Division of Health Care Financing and Policy and Division of Welfare and Supportive Service;
• Make the Road Nevada;
• Legal Aid of Southern Nevada;
• UNLV Immigration Law Clinic;
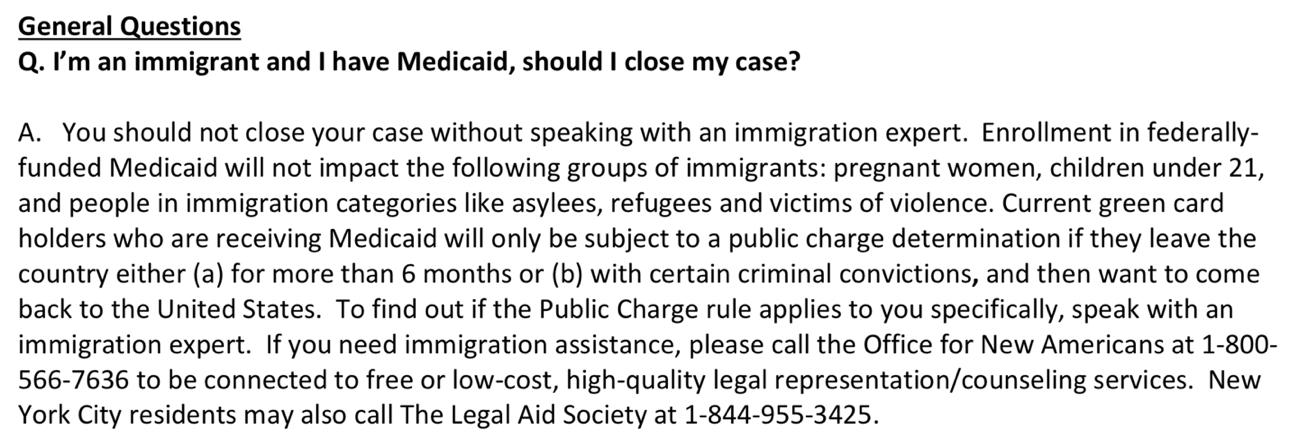
• Nevada Immigrant Coalition;
• Catholic Charities;
• UNITE HERE; and
• Nevada Primary Care Association
To ensure the success of the working group, the state will need to designate a lead entity that will take primary responsibility for convening the group and implementing its recommendations. Given the fear government engenders in some immigrant communities, the state will have to carefully consider which groups to lead this effort and disseminate information to overcome the existing fear and misinformation in the immigrant community surrounding the public charge rule.
CreateapublicchargeFAQ
The aforementioned working group should create a co-branded document addressing frequently asked questions (FAQs) about the public charge rule, and specifically its implications for Medicaid and Nevada Check Up. The working group could model the document after FAQs and talking points from other state and localities. The below example from NY State of Health, the state’s health insurance marketplace, clarifies who might be impacted by the rule. It also provides information about how to get legal help for those confused about whether the new rule might apply to them (see Figure 4).
Addressing Federal Immigration Policy 46
Figure 4. New York State of Health Public Charge FAQ Example125,126
The primary audience for the FAQ document would be the immigrant community in Nevada potentially impacted by the rule, whether directly or indirectly. Therefore, the document should be translated into multiple languages and disseminated through stakeholders and channels that have credibility among these communities. A secondary audience includes individuals who interact with the immigrant clients and may be asked questions about the public charge rule, including frontline social service workers.
Several Nevada stakeholders have already produced educational materials on the public charge rule, which can feed into the proposed master document. This is a lowcost proposal with minimal design, translation, and printing expenses.
CompileadirectoryofCommunityHealth Centerlocationstosharewiththe undocumentedimmigrantcommunity
Given federal laws and limited health insurance options for undocumented immigrants, CHCs play an important role in access to care for undocumented immigrants in Nevada. The state should leverage the creation of a CHC directory for new Medicaid enrollees (as recommended in the Increasing Health Care Accessibility section of this report). The state should ensure this document is translated into multiple languages and distributed to stakeholders with ties to the immigrant community, including the working group mentioned above, to ensure effective dissemination of the information to relevant populations.
Incorporatea‘publiccharge’optioninthe Medicaidleaverssurvey
As suggested in the Increasing Health Care Accessibility section, Nevada should conduct a survey of individuals who drop Medicaid coverage to better understand why individuals are leaving Medicaid. Having a public charge option question on this survey could help to quantify the rule’s impact on disenrollment. Responses to question might also influence which educational messages the state features on its outreach materials. This would provide much-needed data on the effect of the public charge rule on Medicaid disenrollment.
LONG-TERM
Buildinsafeguardsforimmigrantsin automaticdeterminationproceduresfor Medicaid
Now that the nationwide injunctions have been lifted and DHS will be implementing the public charge rule, Nevada should implement safeguards for any automatic Medicaid determination procedures. These initiatives risk the unintended consequence of subjecting an immigrant client to a Medicaid application or screening without their knowledge. For example, Nevada Health Link could add an additional step to its enrollment process, which would require an applicant’s affirmation before referring them for an automatic Medicaid determination on the basis of potential income eligibility. Alternatively, the Department of Welfare and Social Supports could ensure that IT systems divert any non-citizen applying for Medicaid to a manual, rather than automated, determination process.
Addressing Federal Immigration Policy 47
While this proposal may slow the process of Medicaid enrollment for noncitizens, it also avoids inadvertently jeopardizing individuals’ immigration status under the public charge rule. Further, adding a confirmation should be a relatively minor adjustment to the Nevada Health Link and Access Nevada websites.
Allocatestate-onlyfundstoextend Medicaidcoveragetoundocumented immigrants
The Nevada State Legislature should consider legislation allowing the state budget to extend Nevada Medicaid benefits to low-income undocumented immigrants, likely starting with youth. This type of public investment is the only way that Nevada can systematically provide health insurance coverage to the undocumented population.
This action would follow the precedent set by six states that use state funds to cover income-eligible children regardless of immigration status.127 California has the most generous policy: the state legislature voted in 2016 to extend Medi-Cal (the state Medicaid program) benefits to lowincome undocumented youth ages 18 or
younger using state-only funds. The state went further in 2019, extending these benefits to the 19-25 age group starting in 2020, which will benefit an estimated 138,000 individuals.128
This policy would decrease the uninsured rate in Nevada while reducing the undocumented population’s reliance on emergency services. Nevada can look to processes undertaken by California and other states, especially as they relate to a cost-benefit analysis of implementation.
Nevada’s tight fiscal position, discussed Appendix B, is a significant obstacle to this proposal. The funds used to cover undocumented individuals would not be eligible for a federal Medicaid match and the state would be liable for 100 percent of the cost of services for this population. This would be a substantial investment for the state and would require a concerted effort to build political will in the Nevada Legislature.
Addressing Federal Immigration Policy 48
CONCLUSION
Nevada has made enormous progress in recent years in expanding health care coverage and access for Nevadans. As a result of Nevada’s decision to expand Medicaid under the ACA, hundreds of thousands of Nevadans gained Medicaid coverage, while the state’s uninsured rate was cut almost in half. More recently, Nevada’s establishment of a state-based marketplace and the Patient Protection Commission demonstrate state leaders’ continued commitment to improving health care for Nevadans.
Yet as this report has highlighted, Nevada still faces numerous challenges in increasing its Medicaid enrollment and in overcoming systemic barriers to health care access and coverage. However, each of these challenges is accompanied by opportunities for policy change both big and small to improve access to care for all Nevadans.
First, though Nevada’s Medicaid eligibility systems have been stretched by recent program growth, real opportunities exist to streamline processes and modernize systems to facilitate Medicaid enrollment Long-term, the state will need to enhance its information technology (IT) capacity to do real-time determinations and automated renewals, but in the meantime can implement a more expansive presumptive eligibility program, expand continuous eligibility for children on Medicaid, and suspend (rather than terminate) coverage for individuals who are incarcerated to retain enrollment.
Nevada’s provider shortage limits all Nevadans’ access to necessary health services, but its effects are intensified among the Medicaid-eligible population because fewer available providers regularly see Medicaid patients. To alleviate and ultimately end the provider shortage, the state must consider both short- and long-term policy changes. Over the long term, the state should look to increase the quantity of medical residencies and build additional medical professional education pipelines. In the short-term, the state should leverage lowcost opportunities and best practices to improve outreach; increase awareness of Community Health Centers; and reassess scope of practice and licensing limitations.
The state has a significant opportunity to increase quality of care and investment in social determinants of health for Medicaid enrollees in its upcoming re-procurement of Managed Care Organizations
Specifically, the state should seek immediate impact through provisions to increase supports for transportation, housing, and reentry from incarceration
Over the long-term, the state should seek improved data sharing and matching capabilities, community reinvestment initiatives, and alternative payment models.
Given that a fifth of Nevada’s population is foreign-born, understanding the unique challenges and perceptions of the immigrant community is critical to creating effective policy solutions. Federal policy
CONCLUSION 49
constrains what the state can do on largescale systematic changes, but the state can coordinate outreach with trusted organizations and individuals in immigrant communities, increase awareness of CHCs to ensure immigrant communities can access care, and amend state policy to waive the five-year bar for lawfully present qualified immigrant pregnant women to access Medicaid. In the long-run, assuming a significant portion of the uninsured population is undocumented, the state could use state-only dollars to fund Medicaid coverage for undocumented immigrants a significant fiscal undertaking for the state without federal matching funds.
Finally, the challenges outlined throughout the report are compounded by a fiscal environment that cannot support large expansions of the health care system. While there are changes that can be made on the margins, these changes still present significant political challenges and may not generate enough

revenue to fix many of the systematic issues facing Nevada’s health care system.
In the face of these challenges, Nevada has worked tirelessly to reduce the state’s uninsured rate and to make health care accessible for all Nevadans. To reach and cover the remaining uninsured will be a significant challenge, but the state has already demonstrated the necessary creativity and dedication to ensure all Nevadans have access to quality health care and coverage.
CONCLUSION 50

Appendix A: Special Populations Outreach Resources
This appendix serves as a library of available resources and best practices for targeted outreach to communities that may be represented among Nevada’s Medicaid-eligible but uninsured population. It is not exhaustive.
General:
• “Special populations”: CMS page focused on outreach and education for traditionally hard-to-reach populations. Features webinar slides, ready-made flyers, and additional resources.129
o Highlight: webinar slides with effective and ineffective strategies for a variety of Nevada-relevant special populations130
• Outreach and Enrollment Strategies for Reaching the Medicaid Eligible but Uninsured Population: Kaiser Family Foundation overview131
Hispanic/Latino populations:
• CMS PowerPoint on outreach to Latino communities132
• InsureKidsNow PowerPoint on outreach to Latino communities133
• Ciudado De Salud: Spanish-language version of CMS’s Healthcare.gov webpage. Links to Nevada Health Link, features Spanish language resources for individuals seeking health insurance.134
o Highlight: Application guidance that lists what information and documents will be needed to complete enrollment and why it is necessary135
Rural communities:
• CMS Rural Health Strategy: report on how CMS seeks to support coverage in rural communities (including resources for states or strategy ideas for states)136
• Reaching Rural Communities: InsureKidsNow list of strategies and outreach materials for rural communities137
American Indian communities:
• InsureKidsNow Booklet: best practices for engaging with American Indian communities around Medicaid138
• CMS Library of resources and materials139
o Highlight: this booklet that provides basic messaging and contact information for all Tribal facilities in Nevada140
• Arizona state example: clear guidance for providers that interact with American Indian patients; Nevada may benefit from similar materials that could then be shared with providers, to encourage health care access among American Indian patients141
Appendices 52
Appendix B: Contending with Fiscal Constraints
SUMMARY
Nevada, unlike many other states, does not have an income tax as a primary source of revenue. The state is forced to rely on a combination of many smaller taxes to sustain the general fund and pay for public programs, especially in education and health care. These fiscal constraints influence the feasibility of solutions considered for this report. This section considers modifications to existing taxes that could bring in additional funding for public programs like Medicaid. Most of the recommendations made were mentioned or touched upon in our meetings. All recommendations in this section are long-term; it will take time to build the political will to raise revenues, no matter how crucial for expanding health coverage and care in Nevada. Specifically, this section recommends (presented in order of most to least politically feasible):
Long-Term
(1) Increase the marijuana excise retail tax by five percentage points;
(2) Increase the insurance premium tax rate to four percent;
(3) Increase Commerce Tax revenues with a flat rate increase between 0.05 and 0.1 percent;
(4) Eliminate the two-tiered nature of the Modified Business Tax by setting a uniform rate of two percent; and
(5) Reform the property tax
PROBLEM STATEMENT
Without new revenue sources, improvements in health care outcomes will be limited. Throughout our conversations, stakeholders repeated concerns about the fiscal and ensuing political limits of potential health reforms. With current levels of funding, particularly in the State General Fund, there is a ceiling to how much the state can truly improve health care access. Many of the longer-term and more ambitious policy options provided in this report will demand some increase in revenues and an expansion of resources.
There are two primary institutional constraints that limit the probability of increased funding for continued capacity building. First, constitutionally permitted legislative measures that aim “to create, generate, or increase any public revenues in any form” must pass with a two-thirds majority in both houses of the state legislature.142 Second, some taxes in the Constitution are either outright unallowed (e.g., the income tax) or are limited (e.g., the property tax cannot exceed $5.00 out of every $100).143,144
Recently implemented wholesale and retail marijuana excise taxes contributed $69,872,630 to the total $6,871,824,265 revenue over the course of the 2017-2018 fiscal year.145 Nearly two-thirds of the marijuana tax revenues came from the 10 percent retail excise tax. These funds originally went to the state rainy-day fund, but now contribute to the Distributive School Account.146 The 15 percent
Appendices 53
wholesale excise tax revenues also contribute to school funds as well as pay for the implementation of the taxation.147 Neither of these contribute to the health care systems that will address consequences of marijuana use on lung health in the years to come.
Another tax, the insurance premium tax, remains at 3.5 percent. Tax revenues have also grown from $240,559,705 in FY 20122013 to $381,540,406 in FY 2017-2018 after the Legislature and Governor Sandoval capped the amount of tax credit applicable by each insurer to $5,000,000 in 2013.148
The Commerce Tax, passed and signed in 2015, raised $201,926,513 in FY 20172018, contributing entirely to the State General Fund.149 The tax rate varies by North American Industry Classification System (NAICS) code. 150
In the 2019 legislative session, a simple majority in the Legislature delayed the scheduled July decrease of the Modified Business Tax (MBT) rate, currently set at 1.475 percent.151 However, opposing legislators filed a lawsuit on the constitutionality of this change in the summer of 2019.152 The hearing for this lawsuit is set for April 2020.
Finally, the property tax formula maintains unique-to-Nevada features that depress potential sources of revenue for county governments, which fund county-owned health care facilities like the University Medical Center of Southern Nevada. The tax has a maximum rate of $3.64 per $100 of taxable value. The tax features 1.5 percent depreciation factor on the assessed value of property (evaluated at
replacement cost), which does not reset at the point of resale. The tax also features a cap on the increase of the tax liability of residential property at three percent. For non-residential property, the cap is either a 10-year rolling average percentage change in the assessed value of the property or twice the increase of CPI, as long as it is not more than eight percent.153
POLICY RECOMMENDATIONS
Due to the higher legislative threshold required of revenue increases, all of the proposals should be understood as longterm policy options due to the political will necessary to enact them. Of these, the final two proposed policy options a change in the MBT and reforming the value assessment formula of the property tax are likely the most difficult to achieve. Recommendations are arranged from least to most ambitious. All recommendations aim to loosen the fiscal constraints on Nevada’s efforts to expand access to care.
LONG-TERM
Increasethemarijuanaexciseretailtaxby fivepercentagepointstofundhealthcare
An increase in the marijuana retail tax represents a viable approach to expand funding for health access. The rate in Nevada remains below those of comparative states (e.g., Colorado, California).154 Therefore, raising it from 10 to 15 percent will not cause Nevada to lose tax competitiveness, and will likely raise over $10 million. This increase also presents an opportunity to address the likely negative heath externalities155 of legalizing marijuana use. This may be the
Appendices 54
most politically feasible of the fiscal policy options presented here.
Increasetheinsurancepremiumtaxrate tofourpercent
Given the continued growth of revenues from the insurance premium tax, the Legislature could consider increasing the rate from 3.5 percent to four percent to further boost State General Fund revenues. The revenues will depend on how the quantity of premiums provided respond to the tax rate change. Still, the tax change should generate tens of millions of dollars in additional revenue.
Alternatively, revenues from the insurance premium tax could increase if the Legislature decides to decrease the cap of the maximum tax credit amount from $5 million to $4.5 million or $4 million. Further research should be conducted to estimate the precise revenue increases possible through these changes.
IncreaseCommerceTaxrevenueswitha flatrateincreasebetween0.05and0.1 percent
Another option to increase General Fund revenues is to increase the commerce tax. With rates for this tax already well below one percent across industries, a flat increase between 0.05 and 0.1 percent across all industries would generate considerable revenues.
Eliminatethetwo-tierednatureofthe ModifiedBusinessTaxbysettinga uniformrateoftwopercent
To increase funds for the State General Fund, the Legislature could both prevent the sunsetting of the rate decrease of the MBT and bring all businesses subject to the MBT to two percent the rate currently
set only for financial institutions. This change would follow longstanding, widely held policy principles of tax equity. The change would significantly increase revenues, which were predicted to be about $319 million by a Tax Foundation report in 2015, when the MBT rate still stood at 1.17 percent.156
Complementary or alternative reforms of the MBT include:
• Decreasing or eliminating the quarterly tax exemption of $85,000 in wages to broaden the tax base; and/or
• Establishing a graduated tax based with different rates for different brackets (i.e., an MBT rate of 0.5 percent for wages up to $85,000, one percent for $85,001 to $200,000, two percent $200,000 and above).
Given the recent lawsuit, however, attempted changes in the rate may spur particularly strong political opposition to potential reforms.
Reformthepropertytaxthroughamultistepprocess
The property tax does not provide funds to the General Fund but will provide some funds for organizations like University Medical Center of Southern Nevada and other publicly funded health providers Property tax reform, however, will likely remain critical to stabilizing the education system. Should the state enact property tax reform along the lines outlined below, fiscal space may open for the state, enabling further improvement of access to affordable health care.
Appendices 55
The state legislature should consider a number of reforms for the property tax’s depreciation rate:
a) Resetting the depreciation rate at the point of sale; and/or
b) Enacting a scheduled decrease of the depreciation rate over time until it reaches zero percent; or
c) Entirely eliminating the depreciation rate.
The state could enact options (a) and (b) jointly, but once the depreciation factor reaches zero percent either at the end of the scheduled decrease of option (b) or through option (c), option (a) ceases to be consequential.
The legislature could also consider changing the formulas for the caps on tax liability increases. Specifically, it could
consider shortening the window of time over which the percentage of the change in assessed property values for nonresidential properties is averaged from 10 to five years. If it were to do so, it should also multiply the increase of the previous year’s CPI by four instead of two.
The property tax does not require a constitutional amendment to address the most concerning features. However, the fact that legislators pursued an amendment to address the property tax indicated that it may be easier to amend the constitution than to establish the necessary revenues to provide or stabilize essential public goods through legislation. Lowering the threshold necessary to raise the necessary state revenues to a threefifths majority may be worthy of consideration.
Appendices 56
Appendix C: Arizona Managed Care Organizations Contract Excerpts
Excerpts from Arizona Health Care Cost Containment System (AHCCCS) MCO Contract Amendment, Section D: Program Requirements (available at: https://www.azahcccs.gov/Resources/Downloads/ContractAmendments/ACC/YH190 001_ACC_AMD7.pdf)
Transportation:
32. APPOINTMENT STANDARDS
The Contractor shall actively monitor and track provider compliance with appointment availability standards as required in ACOM Policy 417 [42 CFR 438.206(c)(1)]. The Contractor shall ensure that providers offer a range of appointment availability, per appointment timeliness standards, for intakes, initial services, and ongoing services based upon the clinical need of the member. The exclusive use of same-day only appointment scheduling and/or open access is prohibited within the Contractor’s network. The Contractor is required to conduct regular reviews of the availability of providers and report this information as specified in Section F, Attachment F3, Contractor Chart of Deliverables.
The Contractor shall ensure that populations with ongoing medical needs, including but not limited to dialysis, radiation and chemotherapy, have coordinated, reliable, medically necessary transportation to ensure members arrive on-time for regularly scheduled appointments and are picked up upon completion of the entire scheduled treatment.
For wait time in the office, the Contractor shall actively monitor and ensure that a member's waiting time for a scheduled appointment at the provider’s office is no more than 45 minutes, except when the provider is unavailable due to an emergency.
If the Contractor’s network is unable to provide medically necessary services required under Contract, the Contractor shall ensure timely and adequate coverage of these services through an out of network provider until a network provider is contracted. The Contractor shall ensure coordination with respect to authorization and payment issues in these circumstances [42 CFR 457.1230(a), 42 CFR 438.206(b)(4) and (5)].
For medically necessary non-emergent transportation, the Contractor shall schedule transportation so that the member arrives on time for the appointment, but no sooner than one hour before the appointment; nor have to wait more than one hour after the conclusion of the treatment for transportation home; nor be picked up prior to the completion of treatment. The Contractor must develop and implement a quarterly performance auditing protocol to evaluate compliance with the standards above for all subcontracted transportation vendors/brokers and require corrective action if standards are not met.
The Contractor must use the results of appointment standards monitoring to assure adequate appointment availability in order to reduce unnecessary emergency department utilization. The Contractor is also encouraged to contract with or employ the services of non-emergency facilities to address member non-emergency care issues occurring after regular office hours or on weekends.
Appendices 57
The Contractor shall establish processes to monitor and reduce the appointment “no-show” rate by provider and service type. As best practices are identified, AHCCCS may require implementation by the Contractor. The Contractor shall have written policies and procedures about educating its provider network regarding appointment time requirements. The Contractor must develop a corrective action plan when appointment standards are not met. In addition, the Contractor must develop a corrective action plan in conjunction with the provider when appropriate [42 CFR 457.1230(a), 42 CFR 438.206(c)(1)(iv)-(vi)]. Appointment standards shall be included in the Contractor’s Provider Manual. The Contractor is encouraged to include the standards in the provider subcontracts. (ContractAmendment, pg165-166)
Justice System Transitions:
Key Staff Positions:
Justice System Liaison: who is located in Arizona, is the single point of contact for communication with the justice system; is the interagency liaison with the Arizona Department of Corrections (ADOC), County Jails, Sherriff’s Office, Correctional Health Services, Arizona Department of Juvenile Corrections (ADJC), Arizona Office of the Courts (AOC) and Probation Departments; and is responsible for Justice System reach-in initiatives. (ContractAmendment,pg113).
Collaboration with System Stakeholders: The Contractor shall work in partnership with the RBHA and all AHCCCS Complete Care Contractors in its Geographic Service Area(s) to meet, agree upon, and reduce to writing, joint collaborative protocols with each County, District, or Regional Office of:
1. Administrative Office of the Courts,
2. Juvenile Probation and Adult Probation,
3. Arizona Department of Corrections and Arizona Department of Juvenile Corrections, and
4. The Veteran’s Administration.
The Contractor shall address in each collaborative protocol, at a minimum, the following:
1. Procedures for each entity to coordinate the delivery of covered services to members served by both entities,
2. Mechanisms for resolving problems,
3. Information sharing,
4. Resources each entity commits for the care and support of members mutually served,
5. Procedures to identify and address joint training needs, and
6. Where applicable, procedures to have providers co-located at juvenile detention centers or other agency locations as directed by AHCCCS.
In the collaborative protocols with the Administrative Office of the Courts, Juvenile Probation and Adult Probation, the Contractor shall adopt strategies to optimize the use of services in connection with Mental Health Courts and Drug Courts.
The Contractor shall work in partnership with the RBHA and all AHCCCS Complete Care Contractors in its Geographic Service Area(s) to meet, agree upon and reduce to writing joint collaborative protocols with local law enforcement and first responders, which, at a minimum, shall address:
1. Continuity of covered services during a crisis,
2. Information about the use and availability of Contractor’s crisis response services,
3. Jail diversion and safety,
4. Strengthening relationships between first responders and providers when support or assistance is needed in working with or engaging members, and
Appendices 58
5. Procedures to identify and address joint training needs.
In addition to the above, the Contractor shall work in partnership with the RBHA and all AHCCCS Complete Care Contractors in its Geographic Service Area(s) to meet, agree upon, and reduce to writing Memorandums of Understanding (MOUs) specific to the following correctional entities:
1. Arizona Administrative Office of the Courts for Juvenile and Adult Probation,
2. The Arizona Department of Corrections for Juvenile and Adults, and
3. The county jails.
At a minimum, the MOUs shall include the following Contractor care coordination requirements:
1. Partner with the justice system to communicate timely data necessary for coordination of care in conformance with all applicable administrative orders, 42 CFR Part 2, and Health Insurance Portability and Accountability Act (HIPAA) requirements that permit the sharing of written, verbal and electronic information,
2. Establish and maintain coordination of care processes as outlined in AMPM Policy 541 and AMPM Policy 1020, and
3. Utilize data sharing agreements and administrative orders that permit the sharing of written, verbal and electronic information at the time of admission into the facility and at the time of discharge.
To the extent permitted by State and federal laws regarding privacy and confidentiality, the data may be shared without the permission of the member if the medications are used to treat substance use disorders and data may consist of:
1. Individual’s Name (FN, MI, LN),
2. DOB,
3. AHCCCS ID,
4. Social Security Number,
5. Gender,
6. Court Ordered Treatment (COT) status,
7. Public Fiduciary/Guardianship status,
8. Assigned Behavioral Health Provider Agency,
9. Assigned Behavioral Health Provider’s Phone Number,
10. Name of AHCCCS Complete Care Contractor
11. Primary Care Provider’s Name,
12. Primary Care Provider’s Phone Number,
13. Diagnoses (Medical and Psychiatric), and
14. Medications.
The Contractor shall:
1. Offer customized training that is designed to strengthen staff’s ability to effectively work with individuals in the correctional facility,
2. Share information that assists the clinical team in developing treatment plans that incorporate community release conditions, as appropriate, and
3. Develop policies and procedures that identify specific time frames to have the team (i.e. Correctional Facility, the Contractor, Provider and Jail Coordinator) convene to discuss services and resources needed for the individual to safely transition into the community upon release.
The Contractor shall submit all written protocols and MOUs as specified in Section F, Attachment F3, Contractor Chart of Deliverables and review and update on an annual basis as needed.
Appendices 59
Justice System Reach-in Care Coordination System: To facilitate the transition of members transitioning out of jails and prisons into communities, AHCCCS is engaged in a data exchange process that allows AHCCCS to suspend eligibility upon incarceration, rather than terminate coverage. Upon the member’s release, the member’s AHCCCS eligibility is un-suspended allowing for immediate care coordination activities. To support this initiative the Contractor is required to participate in criminal justice system “reach-in” care coordination efforts.
The Contractor shall conduct reach-in care coordination for members who have been incarcerated in the adult correctional system for 30 days or longer, and have an anticipated release date. Reach-in care coordination activities shall begin upon knowledge of a member’s anticipated release date. The Contractor shall collaborate with criminal justice partners (e.g. Jails, Sherriff’s Office, Correctional Health Services, Arizona Department of Corrections, including Community Supervision, Probation, Courts), to identify justice-involved members in the adult criminal justice system with physical and/or behavioral health chronic and/or complex care needs prior to member’s release. In addition to members identified as having a chronic and/or complex care need, the Contractor shall conduct reach-in care coordination for members in the adult correctional system who have a substance use disorder and/or meet medical necessity criteria to receive Medical Assisted Treatment (MAT).
The Contractor shall report the Reach-In Plan to AHCCCS, as described below, in the annual Medical Management Plan and report outcome summaries in the Medical Management Evaluation, as specified in Section F, Attachment F3, Contractor Chart of Deliverables. The Contractor shall monitor progress throughout the year and submit quarterly reporting to AHCCCS, as specified in Section F, Attachment F3, Contractor Chart of Deliverables, of the number of members involved in reach-in activities. In addition, AHCCCS may run performance metrics such as emergency room utilization, inpatient utilization, reduction in recidivism and other access to care measures for the population to monitor care coordination activities and effectiveness. Administrative and Contractor care coordination requirements are outlined in AMPM Policy 1020.
The Contractor shall notify AHCCCS upon becoming aware that a member may be an inmate of a public institution when the member’s enrollment has not been suspended, and will receive a file from AHCCCS as specified in Section D, Paragraph 51, Capitation Adjustment.
In addition to the care coordination requirements, Contractors shall also utilize the renewal date information provided by AHCCCS to identify incarcerated members that may have missed their eligibility redetermination date while incarcerated causing a discontinuance of benefits and provide assistance with reapplication for AHCCCS Medical Assistance upon release.
(ContractAmendment,pg144-147)
Housing-Related Supports:
Pg 104-105
Supported Housing: The Contractor is responsible for the provision of Title XIX/XXI wrap-around services to assist members with identifying independent living goals and providing members information about local resources which may help the member to obtain, and maintain, housing in an independent community setting (e.g. rehabilitation and support services). The Contractor is also required to maintain ongoing communication with the RBHA(s) for Contractor/RBHA shared members who are in need of, who qualify for, and who are currently receiving Non-Title XIX/XXI supported housing services (rent/utility subsidies and relocation services) in order to ensure adequate coordination of care for these members. The Contractor shall have policies in place outlining coordination of care processes for these members, including procedures for collaboration with the RBHA. The Contractor shall identify members with housing needs and develop a monitoring process to support transition or post-transition activities including, but not limited to, requests and referrals, transition wait times, transition barriers and special needs, rent amount, monthly income amounts,
Appendices 60
location of housing options chosen, and counties chosen for transition. The Contractor shall attend the quarterly AHCCCS Housing Meeting and submit a Housing Report as specified in Section F, Attachment F3, Contractor Chart of Deliverables. The report shall include information regarding members who have been identified as having an affordable housing need, through the Contractor’s established process/system for members to request and be referred to affordable housing resources, including those members referred to the RBHA for Non-Title XIX/XXI supported housing services (rent/utility subsidies and relocation services) and at a minimum shall include:
1. Member Name referred,
2. AHCCCS ID,
3. Date of Person’s Request,
4. Date of Housing Referral to Housing Provider,
5. Date Housing Provider made direct contact with Referred Person or designated representative (voice message/email/regular mail do not qualify),
6. Outcome of Housing Referral,
7. Date Housed, and
8. New Address.
The Contractor shall also ensure that a staff person(s) is designated as the expert(s) on housing and education resources within the Contractor’s service area. In general, this individual must be available to assist members with up to date information designed to aid members in making informed decisions about their independent living goals. See also Section D, Paragraph 15, Staff Requirements. (Contract Amendment,pg104-105)
Additional Required Staff:
Housing and Education staff designated as the subject matter expert(s) on the provision of housing and education issues and resources to members within the Contractor’s service area. (ContractAmendment, pg116)
Homeless Management Information System: AHCCCS is considering a relationship with the Continuum of Care (CoC) to gain access to the Homeless Management Information Systems (HMIS) in order to identify AHCCCS members who are homeless. AHCCCS would then share this information with Contractors to provide early intervention and medically necessary services. As part of this effort, AHCCCS will work with Contractors to identify opportunities and requirements for Contractors and related housing network providers. (ContractAmendment,pg234)
Appendices 61
Appendix D: Arizona Alternative Payment Models
Excerpts from Arizona Health Care Cost Containment System (AHCCCS) Alternative Payment Model Strategy (available at: https://www.azahcccs.gov/shared/Downloads/ACOM/PolicyFiles/300/307.pdf)
Appendices 62
Appendix E: Participant Biographies
Rich André is from Queens, New York and graduated from Amherst College in 2009. Prior to graduate school, he spent several years advocating for and implementing inclusive immigration policies, first at the New York City Mayor’s Office of Immigrant Affairs and then in communities across the country with New American Economy. At Princeton, Rich is studying domestic policy with a focus on racial and economic justice.
Emily Apple is originally from Brooklyn, New York and graduated from the City University of New York - Hunter College with a B.A. in Political Science. She previously worked on issues of economic security and mobility in the New York City Mayor’s Office focusing on policies and programs in the areas of workforce development, education, and youth development. Emily has continued this work at Princeton, focusing her studies on domestic social welfare policy.
Maia Cotelo is originally from Uruguay, but grew up in Mississippi. She graduated in 2016 from the University of Mississippi with a B.A. in international studies, economics, and mathematics. Prior to Princeton, Maia worked for two years at The Advisory Board Company/Education Advisory Board in Washington D.C., conducting short-term research projects on behalf of K-12 and higher education institutions. She is studying domestic policy while at Princeton, with a focus on poverty reduction and education policy.
Francisco Díez-Buzo grew up in upstate New York and the suburbs of St. Paul, Minnesota before attending Yale University. He then moved to Cape Town, South Africa, studying the political economic development of Mozambican anti-poverty measures. He then returned to the U.S. and worked as an organizer and strategist across several political campaigns before becoming a Content Researcher at TED Talks. At Princeton, he focuses on the political economy of inequality.
Artin Haghshenas is from New Jersey and graduated from Rutgers University in 2015. Prior to her time at Princeton, Artin spent three years as an Advisor to U.S. Senator Bob Menendez. Artin studies domestic policy while at Princeton, with a focus on health policy.
Thomas Huelskoetter grew up in Alabama and Virginia and graduated from Kenyon College in 2012 Prior to Princeton, he spent five years as a health policy analyst at the Center for American Progress in Washington, D C , where he focused primarily on research and advocacy related to the ACA, Medicaid, and prescription drug prices. At Princeton, he is studying domestic policy with a focus on health policy.
Appendices 63
Eric McCrery is from Old Hickory, Tennessee and is a graduate of the United States Naval Academy. Prior to Princeton, Eric served as a Marine Corps infantry officer, deploying to Afghanistan and Europe. He is studying domestic policy while at Princeton, and plans to return to Tennessee to work on economic development after graduation.
Eric Parolin grew up in New Hampshire and graduated from Boston College in 2013 with a B.A. in both mathematics and economics. Prior to Princeton, Eric worked in financial stability policy at the Federal Reserve Board of Governors and U.S. Department of the Treasury, and most recently worked in the U.S. Senate Finance Committee in tax policy. At Princeton, Eric is focusing on inequality and rural public policy.
Ashley Semanskee is originally from Edmonds, Washington. She graduated from Stanford University in 2015. Prior to graduate school, she worked in San Francisco at Kaiser Family Foundation (KFF), studying health reform and private insurance markets. At Princeton, she is studying economics and health policy.
Alisa Tiwari is originally from Washington, D.C., and graduated from Princeton University in 2014. She then spent two years working on criminal justice reform at the U.S. Department of Justice, primarily civil rights investigations into police departments and prisons. As a graduate student, she focuses on issues of race and inequality and is pursuing a J.D. at Yale Law School.
Alex Wheatley was born in Kansas. She received her B.A. in biology from Princeton in 2016 and has remained at Princeton as a Scholar in the Nation's Service (SINSI Program), completing two years of federal fellowship work between her first and second year of MPA coursework. She's primarily interested in public health and development.
Appendices 64
Appendix F: Endnotes
1 “Nevada’s Uninsured Population” (Kenny C Guinn Center for Policy Priorities, 2019), https://guinncenter.org/publications/policyreports/guinn-center-nevadas-uninsured-population-2019/.
2 Current estimates of Nevada’s uninsured population vary, with multiple sources estimating a 2018 uninsurance rate of 11% and the most recent Guinn Center estimating a 2017 uninsurance rate of 14%.
3 Louise Norris, “Nevada and the ACA’s Medicaid Expansion,” Healthinsurance.Org, November 30, 2018, https://www.healthinsurance.org/nevada-medicaid/; Douglas Conway, “Health Insurance Coverage by Type of Coverage and State: 2018,” American Community Survey Briefs (U.S. Census Bureau, November 2019), https://www.census.gov/content/dam/Census/library/publications/2019/acs/acsbr18-03.pdf; “Health Insurance Coverage of the Total Population: 2018,” Kaiser Family Foundation: State Health Facts, n.d., https://www.kff.org/other/state-indicator/totalpopulation/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D.
4 US Census Bureau, “Nevada and Idaho Are the Nation’s Fastest-Growing States,” The United States Census Bureau, accessed January 2, 2020, https://www.census.gov/newsroom/press-releases/2018/estimates-national-state.html."
5 Associated Press, “Nevada passes 3M population mark with push from Californians,” November 24, 2019, https://apnews.com/32430f171f4d4457903cb047a2b22811.
6 “Medicaid in Nevada” (Kaiser Family Foundation, October 2019), http://files.kff.org/attachment/fact-sheet-medicaid-state-NV.
7 Tabor Griswold, John Packham, Laima Etchegoyhen, Victoria Young, et al., “Nevada Rural and Frontier Health Data Book” (University of Nevada, Reno School of Medicine, Office of Statewide Initiatives, January 2019), https://med.unr.edu/statewide/reports/data-book-2019.
8 Griswold, Packham, Etchegoyhen, Young, et al.
9 Griswold, Packham, Etchegoyhen, Young, et al.
10 Griswold, Packham, Etchegoyhen, Young, et al.
11 Tabor Griswold, John Packham, Laima Etchegoyhen, Tory Jorgensen, et al., “Nevada Rural and Frontier Health Data Book” (University of Nevada, Reno School of Medicine, Nevada State Office of Rural Health, January 2017), https://med.unr.edu/Documents/med/statewide/reports/2017%20Nevada%20Rural%20and%20Frontier%20Health%20Data%20Book_ADA.pdf
12 Norris, “Nevada and the ACA’s Medicaid Expansion.”
13 Current estimates of Nevada’s uninsured population vary, with multiple sources estimating a 2018 uninsurance rate of 11% and the most recent Guinn Center estimating a 2017 uninsurance rate of 14%.
14 Norris, “Nevada and the ACA’s Medicaid Expansion”; Conway, “Health Insurance Coverage by Type of Coverage and State: 2018”; “Health Insurance Coverage of the Total Population: 2018.”
15 Larry Matheis, “Commentary: Nevada Medicaid Expansion Has Been a Roaring Success,” Las Vegas Review-Journal, July 28, 2018, https://www.reviewjournal.com/opinion/commentary-nevada-medicaid-expansion-has-been-a-roaring-success/.
16 “Health Insurance Coverage of the Total Population: 2018.”
17 Norris, “Nevada and the ACA’s Medicaid Expansion”; Conway, “Health Insurance Coverage by Type of Coverage and State: 2018.”
18 Rachana Pradhan, “Number of uninsured Americans rises for the first time since Obamacare,” Politico, September 10, 2019, https://www.politico.com/story/2019/09/10/health-insurance-rate-1719381.
19 “Nevada’s Uninsured Population.”
20 “Healthcare Report Card: Achieving Healthcare for All,” Nevada Medical Center, 2019, https://nvmedicalcenter.org/nevada-healthcarestatistics/healthcare-access/.
21 “Healthcare Report Card: Achieving Healthcare for All,” Nevada Medical Center.
22 “Nevada’s Uninsured Population.”
23 Ibid.
24 Griswold, Packham, Etchegoyhen, Young, et al., “Nevada Rural and Frontier Health Data Book.”
25 Griswold, Packham, Etchegoyhen, Young, et al.
26 Geoff Dornan, “Open Enrollment for Affordable Care Act Health Insurance Beggins Nov 1 in Nevada,” The Record-Courier, October 20, 2019, https://www.recordcourier.com/news/local/open-enrollment-for-affordable-care-act-health-insurance-begins-nov-1-in-nevada/.
27 Dornan.
28 “Governor Sisolak Expands Access to Affordable Health Care, Keeps Promises to Educators, and Grows Economic Opportunities for Working Nevadans During First Legislative Session,” Nevada Governor Steve Sisolak, June 4, 2019.
29 Helen Kalla, “Governor Sisolak Signs Bill Creating Patient Protection Commission,” Nevada Governor Steve Sisolak, June 7, 2019, http://gov.nv.gov/News/Press/2019/Governor_Sisolak_Signs_Bill_Creating_Patient_Protection_Commission/.
30 Nevada Senate Bill 544, effective June 7, 2019, https://www.leg.state.nv.us/App/NELIS/REL/80th2019/Bill/7053/Overview.
31 Tricia Brooks, Lauren Roygardner, and Samantha Artiga, “Medicaid and CHIP Eligibility, Enrollment, and Cost Sharing Policies, as of January 2019: Findings from a 50-State Survey” (Kaiser Family Foundation, March 2019), http://files.kff.org/attachment/Report-Medicaid-and-CHIPEligibility-Enrollment-Renewal-and-Cost-Sharing-Policies-as-of-January-2019.
32 Brooks, Roygardner, and Artiga.
33 “Medicaid MAGI and CHIP Application Processing Time Report” (Washington, D.C.: U.S. Centers for Medicare and Medicaid Services, November 7, 2019), https://www.medicaid.gov/state-overviews/downloads/magi-and-chip-application-processing-time/magi-application-timereport-2019.pdf.
34 Email correspondence with Division of Welfare and Supportive Services, December 12, 2019.
35 Kaiser Family Foundation, “Presumptive Eligibility in Medicaid and CHIP,” https://www.kff.org/health-reform/state-indicator/presumptiveeligibility-in-medicaid-chip/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D.
Appendices 65
36 Centers for Medicare & Medicaid Services, “Medicaid and CHIP FAQs: Implementing Hospital Presumptive Eligibility Programs,” https://www.medicaid.gov/state-resource-center/faq-medicaid-and-chip-affordable-care-act-implementation/downloads/faqs-by-topichospital-pe-01-23-14.pdf
37 Centers for Medicare & Medicaid Services, “Nevada State Plan Amendment 14-0001,” https://www.medicaid.gov/State-resourcecenter/Medicaid-State-Plan-Amendments/Downloads/NV/NV-14-0001.pdf
38 Centers for Medicare & Medicaid Services, “Medicaid and CHIP FAQs: Implementing Hospital Presumptive Eligibility Programs,” https://www.medicaid.gov/state-resource-center/faq-medicaid-and-chip-affordable-care-act-implementation/downloads/faqs-by-topichospital-pe-01-23-14.pdf
39 Tricia Brooks, “Hospital Presumptive Eligibility,” Health Affairs, January 2014, https://www.healthaffairs.org/do/10.1377/hpb20140109.508614/full/
40 Centers for Medicare & Medicaid Services, “Medicaid and CHIP FAQs: Implementing Hospital Presumptive Eligibility Programs,” https://www.medicaid.gov/state-resource-center/faq-medicaid-and-chip-affordable-care-act-implementation/downloads/faqs-by-topichospital-pe-01-23-14.pdf.
41 Kaiser Family Foundation, “States Reporting Corrections-Related Medicaid Enrollment Policies In Place for Prisons or Jails,” https://www.kff.org/medicaid/state-indicator/states-reporting-corrections-related-medicaid-enrollment-policies-in-place-for-prisons-orjails/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D
42 Brooks, Roygardner, and Artiga, “Medicaid and CHIP Eligibility, Enrollment, and Cost Sharing Policies, as of January 2019: Findings from a 50State Survey.”
43 Brooks, Roygardner, and Artiga.
44 Samantha Artiga and Maria Diaz, “How Quickly Are States Connecting Applicants to Medicaid and CHIP Coverage?,” Kaiser Family Foundation (blog), January 11, 2019, https://www.kff.org/medicaid/issue-brief/how-quickly-are-states-connecting-applicants-to-medicaid-and-chipcoverage/.
45 Email correspondence with Division of Welfare and Supportive Services, December 12, 2019.
46 Tricia Brooks, “Hospital Presumptive Eligibility.”
47 Kaiser Family Foundation, “Presumptive Eligibility in Medicaid and CHIP,” https://www.kff.org/health-reform/state-indicator/presumptiveeligibility-in-medicaid-chip/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D
48 Ibid.
49 Ibid.
50 Ibid.
51 Ibid.
52 Tricia Brooks, “Hospital Presumptive Eligibility.”
53 Ibidd.
54 Centers for Medicare & Medicaid Services, “Continuous Eligibility for Medicaid and CHIP Coverage,” https://www.medicaid.gov/medicaid/outreach-and-enrollment/continuous-eligibility/index.html.
55 Brooks et al, “Medicaid and CHIP Eligibility, Enrollment, and Cost Sharing Policies as of January 2019: Findings from a 50-State Survey,” http://files.kff.org/attachment/Report-Medicaid-and-CHIP-Eligibility-Enrollment-Renewal-and-Cost-Sharing-Policies-as-of-January-2019
56 Tricia Brooks, Edwin Park, and Lauren Roygardner, “Medicaid and CHIP Enrollment Decline Suggests the Child Uninsured Rate May Rise Again,” Georgetown University Health Policy Institute – Center for Children and Families, May 2019, https://ccf.georgetown.edu/2019/05/28/medicaid-and-chip-enrollment-decline/
57 Kaiser Family Foundation, “States Reporting Corrections-Related Medicaid Enrollment Policies In Place for Prisons or Jails,” https://www.kff.org/medicaid/state-indicator/states-reporting-corrections-related-medicaid-enrollment-policies-in-place-for-prisons-orjails/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D
58 “Nevada MAGI-Based Eligibility Verification Plan” (U.S. Centers for Medicare and Medicaid Services, n.d.), https://www.medicaid.gov/medicaid/program-information/eligibility-verification-policies/downloads/nevada-verification-plan-templatefinal.pdf.
59 Email correspondence with Division of Welfare and Supportive Services, December 12, 2019.
60 Email correspondence with Division of Welfare and Supportive Services, December 12, 2019.
61 “Fact Sheet: Mechanized Claims Processing and Information Retrieval Systems (90/10) Final Rule (CMS 2392-F)” (U.S. Centers for Medicare and Medicaid Services, December 3, 2015), https://www.medicaid.gov/medicaid-chip-program-information/by-topics/data-andsystems/downloads/medicaid-90-10-final-rule-fact-sheet.pdf.
62 “Nevada MAGI-Based Eligibility Verification Plan.”
63 “Medicaid/CHIP Eligibility Verification Plans,” accessed December 14, 2019, https://www.medicaid.gov/medicaid/eligibility/verificationplans/index.html.
64 “Simplified, Real-Time Verification Issue Brief,” Medicaid and CHIP Learning Collaboratives (U.S. Centers for Medicare and Medicaid Services, April 2013), https://www.medicaid.gov/state-resource-center/mac-learning-collaboratives/downloads/realtimebrief.pdf.
65 Jane Wishner et al., “Medicaid Real-Time Eligibility Determinations and Automated Renewals: Lessons for Medi-Cal from Colorado and Washington” (Washington, D.C.: Urban Institute, August 2018), https://www.urban.org/sites/default/files/publication/98904/medicaid_realtime_eligibility_determinations_and_automated_renewals_2.pdf.
66 Brooks, Roygardner, and Artiga, “Medicaid and CHIP Eligibility, Enrollment, and Cost Sharing Policies, as of January 2019: Findings from a 50State Survey.”
67 Wishner et al., “Medicaid Real-Time Eligibility Determinations and Automated Renewals: Lessons for Medi-Cal from Colorado and Washington.”
68 Emily Zylla et al., “Assessment and Synthesis of Selected Medicaid Eligibility, Enrollment, and Renewal Processes and Systems in Six States” (Minneapolis, MN: State Health Access Data Assistance Center (SHADAC) at the University of Minnesota, School of Public Health, Division of Health Policy and Management, October 19, 2018), https://www.macpac.gov/wp-content/uploads/2018/11/Assessment-and-Synthesis-ofSelected-Medicaid-Eligibility-Enrollment-and-Renewal-Processes-and-Systems-in-Six-States.pdf.
Appendices 66
69 Griswold, Tabor and John Packham and Victoria Young, “Health Workforce in Nevada: A Chartbook,” Nevada Health Workforce Research Center, August 2019, page 2. https://med.unr.edu/Documents/med/statewide/reports/HWIN%20Chartbook%20August%202019(0).pdf
70 Ibid.
71 Ibid, page 21.
72 Griswold, Packham and Young, “Health Workforce in Nevada: A Chartbook.”
73 Ibid.
74 Heidi Allen et al., “The Role of Stigma in Access to Health Care for the Poor,” The Milbank Quarterly 92, no. 2 (2014): 289–318.
75Guinn Center, “Nevada’s Uninsured Population.”
76 Kaiser Family Foundation, “Analysis of Recent Declines in Medicaid and CHIP Enrollment,” November 25, 2019, https://www.kff.org/medicaid/fact-sheet/analysis-of-recent-declines-in-medicaid-and-chip-enrollment/.
77 Kaiser Family Foundation, “Analysis of Recent Declines in Medicaid and CHIP Enrollment.”
78 “Special Populations,” CMS Health Insurance Marketplace: Outreach and Education, n.d., https://marketplace.cms.gov/outreach-andeducation/special-populations.html; Ruth Parker, Victor Wu, and Kavita Patel, “Successfully Engaging Hard-to-Reach Populations in Health Insurance: A Focus on Outreach, Sign Up and Retention, and Use,” Roundtable on Health Literacy; Collaborative on Health Literacy and Access, Health Care Coverage, and Care (Institute of Medicine, 2015), http://nationalacademies.org/hmd/~/media/Files/Activity%20Files/PublicHealth/HealthLiteracy/Commissioned%20Papers%20Updated%202017/Parker%20et%20al%202015%20Engaging%20hardtoreach%20populations.pdf; Samantha Artiga, Robin Rudowitz, and Jennifer Tolbert, “Outreach and Enrollment Strategies for Reaching the Medicaid Eligible Bu Uninsured Population,” Kaiser Family Foundation, March 2, 2016, https://www.kff.org/medicaid/issue-brief/outreach-and-enrollment-strategies-for-reaching-the-medicaid-eligible-butuninsured-population/.
79 “CHIP Health Services Initiatives: What They Are and How States Use Them” (Medicaid and CHIP Payment and Access Commission, July 2019), https://www.macpac.gov/wp-content/uploads/2019/07/CHIP-Health-Services-Initiatives.pdf.
80 “Enhanced Federal Medical Assistance Percentage (FMAP) for CHIP: FY2020,” Kaiser Family Foundation, n.d., https://www.kff.org/other/state-indicator/enhanced-federal-matching-ratechip/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D.
81 “CHIP Health Services Initiatives: What They Are and How States Use Them.”
82 Vikki Wachino, “Indian Provisions in the Final Medicaid and Children’s Health Insurance Program Managed Care Regulations” (Center for Medicaid and CHIP Services, December 14, 2016), https://www.medicaid.gov/federal-policy-guidance/downloads/cib121416.pdf; “Question: May Indian Health Programs Function as Primary Care Providers (PCP) for American Indians and Alaskan Natives (AI/AN)?,” Nevada Department of Health and Human Services, Division of Health Care Financing and Policy, n.d., http://dhcfp.nv.gov/Pgms/CPT/IHPfaq/.
83 Corbin, April, “Nurse practitioners are one part of solution to NV’s doctor shortage,” Nevada Current, July 26,2019, https://www.nevadacurrent.com/2019/07/26/nurse-practitioners-are-one-part-of-solution-to-nvs-doctor-shortage/
84 Griswold, Packham and Young, “Health Workforce in Nevada: A Chartbook.”
85 Griswold, Packham and Young, “A Comparison of Urban and Rural Medical Student’s Academic Performance and Rural Retention in Nevada –UME Graduates 2005-2014,” Nevada Health Workforce Research Center, June 2019, page 1.
86 “U.S. Census Bureau QuickFacts: Washoe County, Nevada; Clark County, Nevada; Nevada.” (Census Bureau QuickFacts, n.d.), www.census.gov/quickfacts/fact/table/washoecountynevada,clarkcountynevada,NV/LND110210.
87 Health Services Advisory Group, “State Fiscal Year 2017–2018 External Quality Review Technical Report” (Division of Health Care Financing and Policy, Nevada Medicaid Managed Care, November 2018), http://dhcfp.nv.gov/uploadedFiles/dhcfpnvgov/content/Resources/AdminSupport/Reports/NV2017-18_EQR_TR_F1.pdf.
88 Jeffrey Brenner et al., “Health Care Hotspotting in the United States.” (The Abdul Latif Jameel Poverty Action Lab (J-PAL), 2017), https://www.povertyactionlab.org/evaluation/health-care-hotspotting-united-states.
89 Bailit Health Purchasing, LLC, “Value-Based Purchasing for Managed Care Procurements: A Toolkit for State Medicaid Agencie” (State Health & Value Strategies, n.d.), https://www.shvs.org/wp-content/uploads/2018/01/SHVS_Medicaid-Toolkit_Final.pdf.
90 “State Health Facts: Total Medicaid MCO Enrollment” (Kaiser Family Foundation, 2017), https://www.kff.org/other/state-indicator/totalmedicaid-mco-enrollment/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D.
91 “Support for Individuals Transitioning out of the Criminal Justice System” (Arizona Health Care Cost Containment System (AHCCCS), n.d.), https://www.azahcccs.gov/AHCCCS/Initiatives/CareCoordination/justiceinitiatives.html.
92 Jami Snyder, “AHCCS Targeted Investments Program Sustainability Plan” (Arizona Health Care Cost Containment System (AHCCCS), March 29, 2019), https://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Waivers/1115/downloads/az/Health-Care-CostContainment-System/az-hccc-target-stability-plan-20190812.pdf.
93 Mercy Housing and The Low Income Investment Fund, “Innovative Models In Health And Housing” (The California Endowment and the Kresge Foundation, August 2017), https://www.liifund.org/wp-content/uploads/2017/08/Health-and-Housing-LIIF-Mercy-Report-2017.pdf.
94 Mercy Housing and The Low Income Investment Fund.
95 “States Reporting Corrections-Related Medicaid Enrollment Policies In Place for Prisons or Jails” (Kaiser Family Foundation, 2019), https://www.kff.org/medicaid/state-indicator/states-reporting-corrections-related-medicaid-enrollment-policies-in-place-for-prisons-orjails/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Corrections%20and%20Medicaid%20Agencies%20Have%20Electronic,%20Auto mated%20Data%20Exchange%20Processes%20to%20Facilitate%20Suspension%2FReinstatement%20of%20Enrollment%22,%22sort%22:%22as c%22%7D.
96 “Using Data to Identify Housing Needs and Target Resources” (Medicaid Innovation Accelerator Program, November 7, 2018), https://www.medicaid.gov/state-resource-center/innovation-accelerator-program/iap-downloads/program-areas/nds-using-datatranscript.pdf.
97 “Alternative Payment Model Initiative - Strategies and Performance-Based Payments Incentive” (Arizona Health Care Cost Containment System (AHCCCS), 2019), https://www.azahcccs.gov/shared/Downloads/ACOM/PolicyFiles/300/307.pdf.
98 “Arizona State Health Care Innovation Plan” (Arizona Health Care Cost Containment System (AHCCCS), July 5, 2016), https://www.azahcccs.gov/AHCCCS/Downloads/StateInovation/SIMArizonaStateHealthCareInnovationPlan.pdf.
Appendices 67
99 “Contract Amendment,” CONTRACT/RFP NO. YH19-0001 (Arizona Health Care Cost Containment System (AHCCCS), 2019), https://www.azahcccs.gov/Resources/Downloads/ContractAmendments/ACC/YH190001_ACC_AMD7.pdf.
100 Mercy Housing and The Low Income Investment Fund, “Innovative Models In Health And Housing.”
101 New American Economy, “Immigrants and the Economy in Nevada,” https://www.newamericaneconomy.org/locations/nevada/ (last accessed December 2019).
102 Ibid.
103 American Immigration Council, “Immigrants in Nevada,” October 6, 2017, https://www.americanimmigrationcouncil.org/research/immigrants-in-nevada.\
104 Healthcare.gov, “Coverage for lawfully present immigrants,” https://www.healthcare.gov/immigrants/lawfully-present-immigrants/ (last accessed December 2019). The term “qualified non-citizen” includes: Lawful Permanent Residents (LPR/Green Card Holder); asylees; refugees; Cuban/Haitian entrants; paroled into the U.S. for at least one year; conditional entrant granted before 1980; battered non-citizens, spouses, children, or parents; victims of trafficking and his or her spouse, child, sibling, or parent or individuals with a pending application for a victim of trafficking visa; granted withholding of deportation; and a member of a federally recognized Indian tribe or American Indian born in Canada.
105 American Immigration Council, “Immigrants in Nevada.”
106 Nevada Senate, “Senate Bill 325,” https://www.leg.state.nv.us/App/NELIS/REL/79th2017/Bill/5311/Overview
107 Centers for Medicare & Medicaid Services, “Medicaid and CHIP Coverage of Lawfully Residing Children & Pregnant Women,” https://www.medicaid.gov/medicaid/outreach-and-enrollment/lawfully-residing/index.html (last accessed December 2019).
108 Nevada Division of Public and Behavioral Health, “Medicaid Eligibility for non-citizen Children Lawfully Residing in the United States Less than Five Years,” http://dpbh.nv.gov/uploadedFiles/dpbhnvgov/content/Programs/MIP/Images/SB325info.pdf.
109 U.S. Citizenship & Immigration Services, “Final Rule on Public Charge Ground of Inadmissibility,” https://www.uscis.gov/legal-resources/finalrule-public-charge-ground-inadmissibility (last accessed December 2019).
110 Ben Harrington, “DHS Final Rule on Public Charge: Overview and Considerations for Congress,” Congressional Research Service, August 16, 2019, https://fas.org/sgp/crs/homesec/LSB10341.pdf
111 Brooks, Roygardner, and Artiga, “Medicaid and CHIP Eligibility, Enrollment, and Cost Sharing Policies, as of January 2019: Findings from a 50State Survey.”
112 Wendy E. Parmet, “Supreme Court Allows Public Charge Rule To Take Effect While Appeals Continue,” Health Affairs Blog, February 3, 2020, https://www.healthaffairs.org/do/10.1377/hblog20200131.845894/full/
113 Some immigrants, including refugees and asylees and other humanitarian immigrants, remain exempt from public charge determinations under law. Public charge policies do not apply to LPRs seeking to obtain citizenship.
114 Department of Homeland Security, “2016 Yearbook of Immigration Statistics: Table 4. Persons Obtaining Lawful Permanent Resident Status By State Or Territory Of Residence: Fiscal Years 2014 To 2016,” https://www.dhs.gov/immigration-statistics/yearbook/2016/table4
115 Jeanne Batalova, Michael Fix, and Mark Greenberg, “Millions Will Feel Chilling Effects of U.S. Public-Charge Rule That Is Also Likely to Reshape Legal Immigration,” Migration Policy Institute, August 2019, https://www.migrationpolicy.org/news/chilling-effects-us-public-chargerule-commentary.
116 Kaiser Family Foundation, “Changes to “Public Charge” Inadmissibility Rule: Implications for Health and Health Coverage,” August 12, 2019, kff.org/disparities-policy/fact-sheet/public-charge-policies-for-immigrants-implications-for-health-coverage.
117 Samantha Artiga and Maria Diaz, “Health Coverage and Care of Undocumented Immigrants,” Kaiser Family Foundation, July 15, 2019, https://www.kff.org/disparities-policy/issue-brief/health-coverage-and-care-of-undocumented-immigrants/
118 Migration Policy Institute, “Profile of the Unauthorized Population: Nevada,” https://www.migrationpolicy.org/data/unauthorizedimmigrant-population/state/NV (last accessed December 2019).
119 Guinn Center, “Nevada’s Uninsured Population.”
120 Ibid.
121 Centers for Medicare & Medicaid Services, “Medicaid and CHIP Coverage of Lawfully Residing Children & Pregnant Women,” https://www.medicaid.gov/medicaid/outreach-and-enrollment/lawfully-residing/index.html (last accessed December 2019).
122 Michael Lyle, “Sisolak signs legislation to create Maternal Mortality Review Committee,” Nevada Current, May 3, 2019, https://www.nevadacurrent.com/blog/sisolak-signs-legislation-to-create-maternal-mortality-review-committee/.
123 Nevada Senate, “Senate Bill 325 Fiscal Note, Division of Health Care Financing and Policy,” March 25, 2017, https://www.leg.state.nv.us/Session/79th2017/FiscalNotes/7844.pdf
124 Nevada Senate, “Senate Bill 325 Fiscal Note, Division of Welfare and Supportive Services,” March 25, 2017, https://www.leg.state.nv.us/Session/79th2017/FiscalNotes/7845.pdf
125 New York State of Health, “Medicaid and Public Charge - Q&As for Assistors,” http://www.chcanys.org/clientuploads/__2019/HCS/NYSOH_Public_Charge_Assistor_QAs_Final_081619_.pdf (last accessed December 2019).
126 Other useful public charge resources from other states, localities and community and legal organizations include: Protecting Immigrant Families Toolkit for State and Local Government Officials (provides key messages, model fact sheets and guidance); Know Your Rights and Does Public Charge Apply to Me? (consumer-friendly at-a-glance materials); LA County FAQs (FAQs for all immigrants but needs to be updated postinjunction); Public Charge Screening Tool (resource pulled together by NY Legal Aid and other partners to walk through public charge applicability); and Immigrant Legal Resource Center Public Charge Outreach Toolkit (community communication resources, including a model presentation and presenter’s script). For more comprehensive resources, see SHVS materials, including: SHVS webinar slides (provides overview on public charge final rule and implications and SHVS FAQs (addresses common questions on the public charge final rule, including effective date with the preliminary injunction and pending litigation).
127 The District of Columbia, Illinois, Massachusetts, New York, Oregon and Washington use state funds to cover income-eligible children regardless of immigration status. In addition, some states use state funds to cover adult immigrants, but the coverage is often limited to targeted groups.
128 Sammy Caiola, “Young Undocumented Californians Cheer Promise Of Health Benefits,” National Public Radio, July 11, 2019, https://www.npr.org/sections/health-shots/2019/07/11/739536305/young-undocumented-californians-cheer-promise-of-health-benefits
Appendices 68
129 Centers for Medicare & Medicaid Services, “Outreach & education: Special populations,” https://marketplace.cms.gov/outreach-andeducation/special-populations.html (last accessed January 2020).
130 Centers for Medicare & Medicaid Services, “Enrolling Young Adults and Other Hard-to-Reach Populations,” https://marketplace.cms.gov/outreach-and-education/balancing-the-risk-pool.pdf
131 Samantha Artiga, Robin Rudowitz, and Jennifer Tolbert, “Outreach and Enrollment Strategies for Reaching the Medicaid Eligible but Uninsured Population,” Kaiser Family Foundation, March 2, 2016, https://www.kff.org/medicaid/issue-brief/outreach-and-enrollmentstrategies-for-reaching-the-medicaid-eligible-but-uninsured-population/
132 Centers for Medicare & Medicaid Services, “Marketplace Outreach: Best Practices for Outreach to Latino Communities,” https://marketplace.cms.gov/technical-assistance-resources/outreach-latino-communities.pdf
133 Insure Kids Now, “Increasing Medicaid and CHIP Enrollment in Hispanic Communities,” https://www.insurekidsnow.gov/downloads/webinars-videos/webinar-slides/2016-09-14-webinarslides.pdf
134 Centers for Medicare & Medicaid Services, “CiudadoDeSalud.gov,” https://www.cuidadodesalud.gov/es/
135 Centers for Medicare & Medicaid Services, “Prepárese para solicitar o reinscribirse en su Cobertura de Seguro Médico del Mercado,” https://www.cuidadodesalud.gov/downloads/es/apply-for-or-renew-coverage.pdf
136 Centers for Medicare & Medicaid Services, “CMS Rural Health Strategy,” https://www.cms.gov/About-CMS/AgencyInformation/OMH/Downloads/Rural-Strategy-2018.pdf
137 Insure Kids Now, “Reaching Rural Communities,” https://www.insurekidsnow.gov/initiatives/rural-communities/index.html (last accessed December 2019).
138 Leslie Foster, Michael Cavanaugh, and Theresa Feeley-Summerl, “How Can My Organization Connect American Indian and Alaska Native Children to Health Coverage? A Guide to Fundamentals and Promising Practices,” Insure Kids Now, Fall 2019, https://www.insurekidsnow.gov/downloads/library/misc/outreach-and-enrollment-fundamentals-ai-an.pdf
139 Centers for Medicare & Medicaid Services, “American Indian/Alaska Native: Outreach & Education Resources,” https://www.cms.gov/Outreach-and-Education/American-Indian-Alaska-Native/AIAN/Outreach-and-Education/index (last accessed December 2019).
140 Centers for Medicare & Medicaid Services, “Serving American Indians and Alaska Natives in Arizona, Nevada, and Utah,” August 2019, https://www.cms.gov/Outreach-and-Education/American-Indian-Alaska-Native/AIAN/Outreach-and-Education/pdf/brochure_OE-booklet9.pdf
141 Arizona Health Care Cost Containment System, “American Indian Health Provider Resources,” https://www.azahcccs.gov/AmericanIndians/Providers/ (last accessed December 2019).
142 “THE CONSTITUTION OF THE STATE OF NEVADA,” accessed December 15, 2019, https://www.leg.state.nv.us/const/nvconst.html.
143 “Property Taxes in Nevada,” Guinn Center For Policy Priorities, accessed December 15, 2019, https://guinncenter.org/photo-essay/propertytaxes/.
144 “THE CONSTITUTION OF THE STATE OF NEVADA.”
145 “Annual-Report-FY18.Pdf,” accessed December 13, 2019, https://tax.nv.gov/uploadedFiles/taxnvgov/Content/TaxLibrary/Annual-ReportFY18.pdf.
146 “SB545,” accessed December 13, 2019, https://www.leg.state.nv.us/Session/80th2019/Reports/history.cfm?ID=1204.
147 “Taxes,” accessed December 13, 2019, http://marijuana.nv.gov/Businesses/Taxes/.
148 “Annual-Report-FY18.Pdf.”
149 “Annual-Report-FY18.Pdf.”
150 “NRS: CHAPTER 363C - COMMERCE TAX,” accessed December 14, 2019, https://www.leg.state.nv.us/NRS/NRS-363C.html#NRS363CSec310.
151 “Annual-Report-FY18.Pdf.”
152 Geoff Dornan, “Nevada Republican Business Tax Lawsuit on Hold,” accessed December 15, 2019, https://www.nnbusinessview.com/news/nevada-republican-business-tax-lawsuit-on-hold/.
153 Liz Malm et al., “SIMPLIFYING NEVADA’S TAXES: A FRAMEWORK FOR THE FUTURE,” n.d., 83.
154 Janelle Cammenga, “How High Are Recreational Marijuana Taxes in Your State? | 2019,” Tax Foundation (blog), April 24, 2019, https://taxfoundation.org/2019-recreational-marijuana-taxes/.
155 “Marijuana and Lung Health,” American Lung Association, accessed December 14, 2019, https://www.lung.org/stop-smoking/smokingfacts/marijuana-and-lung-health.html.
156 Malm et al., “SIMPLIFYING NEVADA’S TAXES: A FRAMEWORK FOR THE FUTURE.”
Appendices 69
