Related Procedural Documents: MMSOP34 Disposal of Waste Pharmaceutical used within Community Health Services
Review Date: 25/10/2021
It is the responsibility of users to ensure that you are using the most up to date document template – i.e. obtained via the intranet.
In developing/reviewing this policy Provide Community has had regard to the principles of the NHS Constitution.
Version Control Sheet
Version Date
Author Status
Comment
V1 Sept 2008 Director of Corporate Development and Governance for NHS Mid Essex New Approved
V2 July 2012 Infection Prevention Nurse Lead Review again in 6 months This policy was reviewed in line with transition to CECS CIC
The author has requested a 6 month review date because of new health care waste guidelines version 2 (2012) and the implications for teams working in the community
V2.1 December 12 Infection Prevention Nurse Lead Approved for a further 3 months Awaiting National Guidance
V2.2 May ‘13 Infection Prevention Nurse Lead Approved for a further 3 months Awaiting National Guidance – no change.
V2.3 August 2013 Infection Prevention Nurse Lead Approved for a further 6 months Awaiting National Guidance – no change
V2.4 September 2013 Steph Schuster Quality & Safety Administrator No change to review date Updated in line with organisation name change and restructure
V2.5 Nov 2013 Infection Prevention Lead Nurse Review of Policy Awaiting National Guidance – no change
V3 Nov 2014 Infection Prevention Lead Nurse Review of Policy Clarification of guidance for waste in patients’ own homes and new
contact details for NHS Property Services
V4 September 2016 Head of Infection Prevention Approved Review system & add audit tool and clinical waste collection from home patients.
V5 October 2018 Specialist Infection Prevention nurse Policy review/ new template
1. Purpose
This Healthcare Waste Policy replaces its predecessor The Waste Management Policy. It ensures that Provide meets its legal obligations taking into consideration the requirements of waste, health & safety, and carriage (transport) regulations.
Healthcare waste refers to waste produced by healthcare activities. For the purpose of this document the policy applies to domestic waste , sharps waste, infectious and offensive waste produced in Provide premises by Provide staff in patients’ homes and by primary care and by primary care contractors in healthcare premises and in patients’ homes.
This policy adopts the methodology for identifying and classifying infectious and offensive waste that complies with health & safety, transport and waste regulations. It includes a revised colour-coded waste segregation and packaging system following national guidance. It makes use of European Waste Catalogue (EWC) codes, replacing the abandoned clinical waste classification groups A – E.
This policy complies with Care Quality Commission Outcome 10 ‘safety and suitability of premises’ and decrees that ‘people receive care in, work in or visit safe surroundings that promote their wellbeing’.
2. Aim
This policy provides the framework for the management of Healthcare waste in Provide. It aims to secure the health and safety of employees, primary care contractors, visitors and clients, and help to protect the environment.
3. Legal Framework
There are three separate legal areas that govern waste generated on health care premises:
• Environment and Waste
• Transport
• Health and Safety
The following legislation applies to waste generation in health care premises:
• Control of Pollution (Amendment) Act 1989
• The Environmental Protection Act 1990 (Section 33 and 34)
• Environmental Protection (Duty of Care) Regulations (England, Scotland and Wales) 1991
• The Carriage of Dangerous Goods and Use of Transportable Pressure Equipment Regulations 2009 SI 1348
• Schedule 3 of the Control of Substances Hazards to Health Regulations (COSHH) 2002
• Health and Safety at Work Act 1974
• The Health and Safety (Consultation with Employees) Regulations 1996
• The Hazardous Waste (England and Wales) Regulations 2005
• The Hazardous Waste (Amendments) Regulations 2009
• Waste electrical and electronic equipment directive 2002/96/EC
• Batteries and accumulators and waste batteries and accumulators directive 2006/66/EC
• The management of H&S at work regulations 1999
• The Safe management of Healthcare waste: HTM 07-01 (2013):DH
The above legislation is detailed in (Appendix 1)
Premises Registration
All premises that produce over 500 kg of all types of hazardous waste per year, including electrical, medicinal, infectious, offensive etc., must be registered with the Environment Agency.
NHS Property Services is responsible for ensuring that all premises (including bedded areas, hospitals, health centres and clinics) are registered with the Environment Agency where applicable. As a community provider, PROVIDE delivers services from these properties.
The registration number for each site can be obtained from the Waste Contracts monitoring officer for NHS Property Services.
Provide has several sites with different contractors: The clinical waste contract for the community clinics is overseen by NHS Property Services but responsibility for the safe practice sits with the ‘waste producer’ - Provide.
The services are subcontracted out to a private waste company by NHS Property Services:
SCRL is responsible for: Witham Health Centre; Springfield Green Clinic; Moulsham Lodge Clinic; Central Clinic; Burnham Clinic; SWF Clinic; Halstead hospital; Technikon house; Spinks Lane , Parkside Maldon Clinic and Moulsham Grange. Provide staff retain their own responsibility for waste under duty of care.
St Peters Hospital, St Michael’s and Braintree Community Hospital sites are managed as part of the Mid Essex Hospital Trust contract, but Provide staff retain their own responsibility for waste under duty of care.
Carbon Footprint
Waste is a high priority as it has a significant carbon footprint. To effectively manage healthcare waste, this healthcare policy identifies who is responsible for waste and provides clears processes to manage waste streams.
4. Roles and
Responsibilities
Under the Duty of Care all staff must ensure that all waste is disposed of correctly. Healthcare waste must be segregated immediately by the person generating the waste into appropriate colour-coded storage or waste disposal bags or containers as being compliant with current national legislation and local policies.
Healthcare waste must be labelled, stored and transported and disposed of in accordance with current legislation and local policies.
All employees must ensure that they safeguard the health and safety of themselves and others by adhering to this policy.
It is strongly recommended that any person coming into contact with clinical waste or sharps should be vaccinated against Hepatitis B.
Please refer to Optima Occupational Health Services for further advice: 0345 643 4368.
NHS Property Services
Responsible for:
• Coordinating and managing all healthcare waste and other waste management activities
• Procuring waste disposal contracts
• Monitoring contracts
• Organising waste training (see Appendix 3) in conjunction with the clinical waste contractor
• Performance monitoring waste audits, as part of contractual agreement with Provide, requesting an annual waste audit, to include analyzing results and providing appropriate action plans.
The purpose of the audits are to document evidence of effective segregation, waste acceptance criteria and to demonstrate that Provide is compliant with Waste Regulations and compliant with Duty of Care to ensure that the waste disposal contracts are effective in providing the needs of Provide and its sub- contractors.
Provide Chief Executive
Ultimately responsible for ensuring that clinical waste is managed in compliance with relevant Health and Safety, Transport, Procurement and Hazardous Waste legislation.
The ward, clinic, department, managers
Responsible for ensuring all waste in their area is safely and correctly handled and disposed of. All managers must also ensure that all Consignment Notes are checked and filed. The Consignment Note must be kept for three years from the date of issue.
Line managers
Responsible for ensuring that staff receive training on waste management on commencement of employment and receive regular updates as part of the mandatory training refresher programme.
The employee
Generating the waste is responsible for its disposal into the correct container and the safe sealing and marking of the waste container. The employee must highlight any problems with waste management to their line manager as soon as possible. The employee must highlight to their manager where they still need to attend refresher training. The employee should segregate and dispose of waste in the appropriate waste stream.
The waste contractors
Responsible for the collection, treatment and the disposal of clinical waste. They are also responsible for informing the NHS Property Services where there are issues of Provide non-compliance with Hazardous Waste Regulations, other relevant environmental legislation and other requirements to which the organisation subscribes.
The Infection Prevention team and clinical staff
Responsible for:
• Advising on healthcare waste
• Participating in clinical waste audits
• Raising awareness through infection prevention training and routine premise visits
• Training Provide staff on clinical waste management and legislation
5. Waste Classification
Domestic waste
Domestic waste is defined as non-offensive, non-hazardous waste that can go into a domestic/household black bag. Domestic waste should not contain any infectious materials, sharps or medicinal products.
The disposal of offensive healthcare waste by a healthcare professional into domestic waste bag constitutes an offence under duty of care. The only exception is healthcare workers practising in the community setting (i.e. patient’s own home) where limited provision is made for the placement of offensive waste items into domestic waste: refer to DH (2013) The Safe Management of Healthcare Waste, Department of Health.
Waste regulation requires the classification of waste on the basis of hazardous characteristics and point of production. This document introduces the new methodology for identifying and classifying infectious waste according to the European Waste Catalogue. Only waste generated from healthcare practice by a healthcare practitioner is considered as infectious waste.
Clinical Waste
The following outlines the new methodology for identifying and classifying waste and the inclusion of European Waste Catalogue (EWC) Codes.
Clinical Waste and hazardous waste
Clinical waste is defined as:
• Any waste which consists wholly or partly of human or animal tissue, blood or other body fluids, excretions, drugs or other pharmaceutical products, swabs or dressings, syringes , needles or other sharp instruments, being waste which unless rendered safe may prove hazardous to any person coming into contact with it
• Any other waste arising from medical, nursing, dental, veterinary, pharmaceutical or similar practice, investigation, treatment, care, teaching or research, or the collection of blood for transfusion, being waste which may cause infection to any person coming into contact with it
• Any waste produced by healthcare activities, including waste produced in the community from healthcare sources (i.e. not electrical or domestic)
• Clinical waste can be divided into 3 groups:
o Any healthcare waste which poses a risk of infection
o Certain healthcare wastes which pose a chemical hazard
o Medicines and medicinally –contaminated waste containing a pharmaceutically –active agent.
Infectious Waste
Infectious waste is any waste containing viable micro-organisms or their toxins which are known or reliably believed to cause disease in man or animals.
Infectious waste must be divided into Category A and Category B infectious waste.
Category A
An infectious substance which is transported in a form that, when exposure to it occurs, is capable of causing permanent disability, life threatening or fatal disease to humans or animals e.g. waste contaminated with pathogens presenting the most severe risk of infection e.g. Ebola virus (Appendix 4). This waste must be treated i.e. by autoclaving onsite prior to removal to a disposal facility
Category A waste is unlikely to be produced from healthcare premises within the UK apart from Laboratory waste.
Category B
An infectious substance which does not meet the criteria for inclusion in category A. This waste does not need to be treated i.e. by autoclaving on-site prior to removal to a disposal facility. Most infectious clinical waste generated within the community/primary care environment is within Category B waste.
Offensive Waste
Offensive waste is waste that:
• may cause offence due to the presence of body fluids
• is not known or suspected to possess any hazardous properties
• is not identified by the producer as needing disinfection, or any other treatment, to reduce the number of microorganisms present
Examples of offensive waste include the following if they are contaminated with a body fluid: continence pads, nappies, sanitary waste and other items which pose a minimal risk of infection such as empty catheter bags, plasters, protective clothing. Minimum treatment/disposal for offensive waste is landfill in a suitable licensed facility.
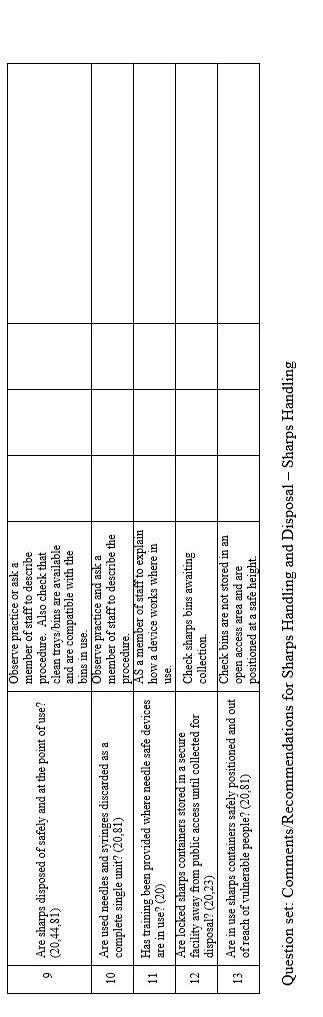
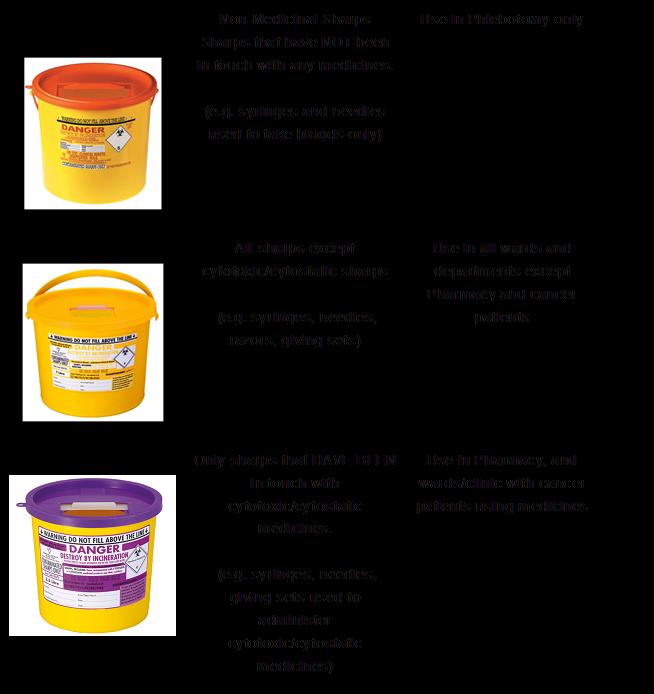
Sharps Waste
Sharps are items that could cause cuts or puncture wounds, including needles, scalpel and other blades, razors, knives, infusion sets etc, that have the potential to cause infection.
Care must be taken when assembling sharps containers to ensure the lid is securely in place. Sharps containers must be sealed labeled and replaced when contents reach the marked black line on the bin. If the sharps container is seldom used, it should be replaced after a maximum of 3 months regardless of the filled capacity. Therefore the sharps container must be signed and dated on assembly in order to identify when 3 months have expired. Sharps containers must always be kept at waist height on a level surface (or in a wall bracket) in a clinical area to prevent injury to children.
All sharps contaminated with cytotoxic/cytostatic medicines must be placed in purple lidded sharps bins, (Appendix 9). Please note that BCG is classed as a cytotoxic/cytostatic.
Liquid Waste
Any liquid clinical waste being placed within the clinical waste stream e.g. suction fluids or urine must be solidified with an appropriate gelling agent to prevent leakage, spillage and overflow and therefore reduce the risk of cross contamination. Wherever possible, pre-gelled suction liners must be used.
Pharmaceutical Waste
Please refer to MM34: Disposal of Pharmaceutical Waste within Community Health Services policy. Any unused medicines from members of the public should normally be returned to a pharmacy where a contract is in place to dispose of such medicines. The immediate container of the medicines should be placed in the appropriate bin, with outer containers being disposed of through other routes (caution with labels giving patient’s name).
Medicines used in the course of healthcare treatment, e.g. injections, should be disposed of in the appropriate sharps container.
6. Segregation of Waste
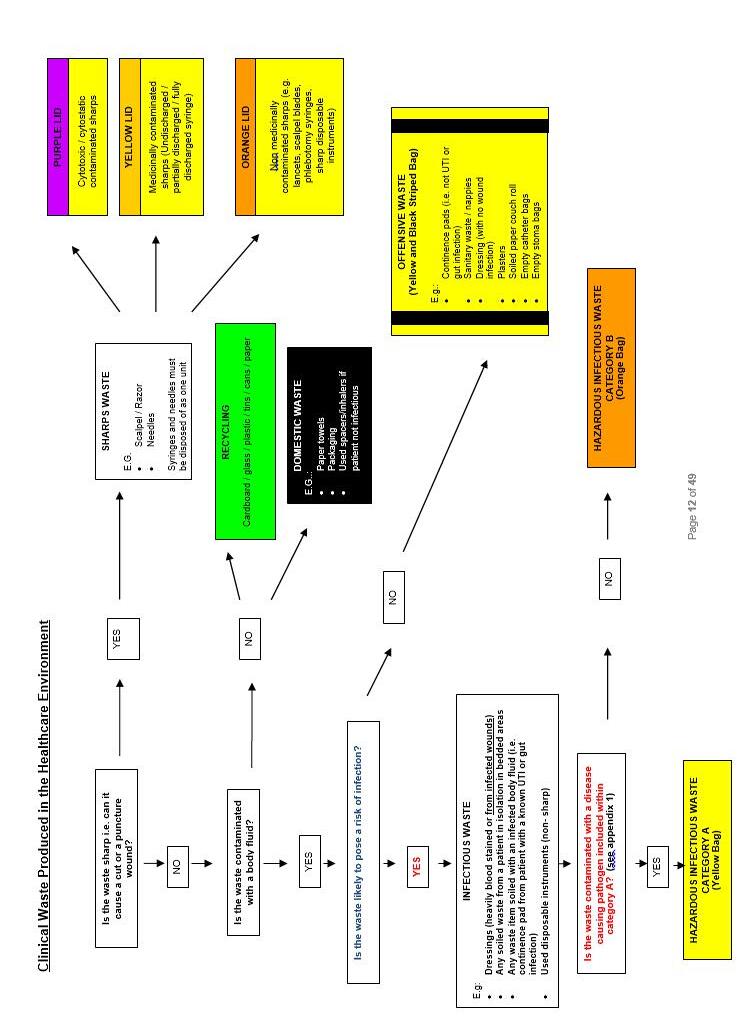
An assessment for chemical and clinical waste hazards must first be carried out. If not contaminated with a chemical or clinical waste hazard, then the following risk assessment must be followed.
The following flow-charts apply to clinical waste produced in the Healthcare Environment (4.2.1a)
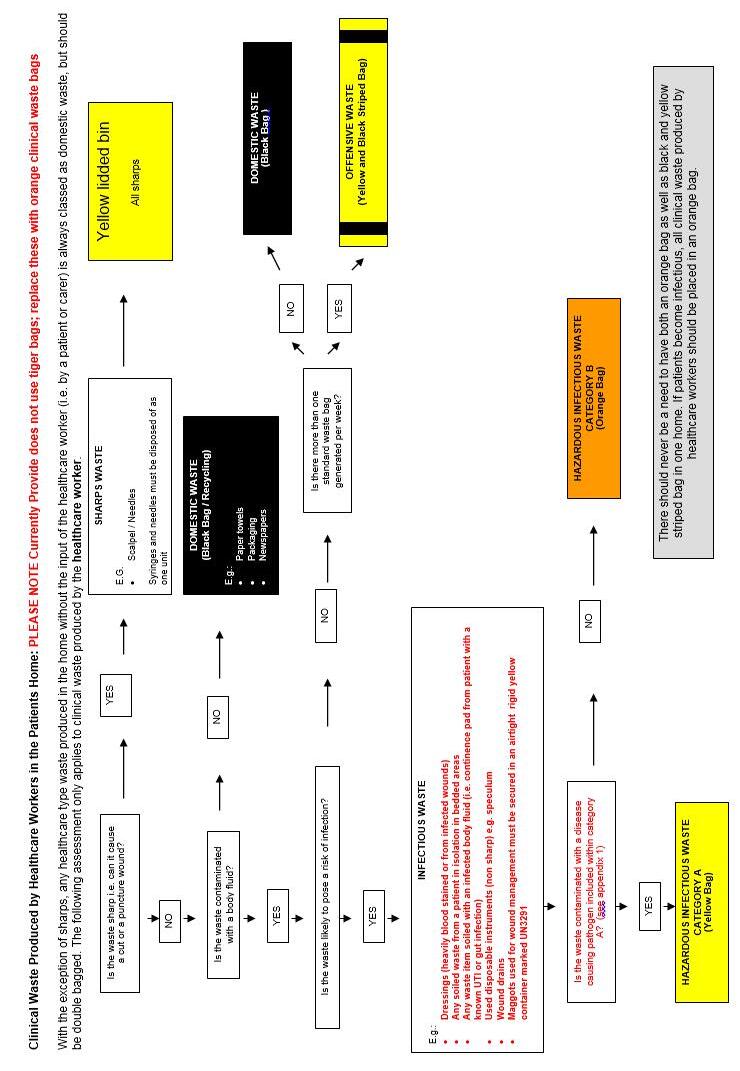
PLEASE NOTE – PROVIDE SERVICES DO NOT CURRENTLY USE TIGER BAGS in any of its facilities.
Healthcare Waste (Clinical Waste) Produced by a Healthcare Worker Outside of the Healthcare Environment i.e. in the patient’s own home
Such waste will be produced by community nurses, podiatrists, dental staff and phlebotomists carrying out domiciliary visits. Where a healthcare worker (HCW) generates the waste, it is deemed as belonging to them and not the patient or householder.
To accurately assess whether the waste generated is infectious, a risk assessment should be performed.
The risk assessment template is on SystmOne template and must be completed for all patients’ at the initial assessment.
This should be based on the professional assessment, clinical signs and symptoms, and any prior knowledge of the patient. For example if a wound assessment indicates that the wound is infected, all associated contaminated dressings should be classified as infectious waste and packaged for appropriate treatment and disposal. This requires a licensed clinical waste contractor to collect the waste. It must be placed into a clinical waste bag (orange). It can be stored in a safe place in the patient’s home, if consent is given. Please see examples of infectious waste below:
• Infected wound exudate material is present in the waste generated
• Chest drains, evacuations drains, IV polymeric devices, drains generating large quantities of waste which would not normally be in the household waste
If a large amount of waste is being generated (i.e. standard sized black refuse bag/ per week) the waste must be placed in a Clinical waste bag (orange) and removed by a licensed clinical waste contractor (Please complete Appendix 11 Clinical Waste home form)
Patients with MRSA:
Where a patient in the community has been diagnosed with MRSA and is being cared for by a healthcare worker (HCW), the waste generated is not necessarily infectious. In assessing the risk of infection from waste produced by a patient with MRSA, the following should be considered: (see examples of waste management 1& 2 below).
• Orange waste bags are indicated only when infectious material is present in the waste generated (i.e. infected wound exudate)
• Has patient been prescribed antibiotics for the infected wound/site?
If the patient is known to be colonised with MRSA, the MRSA status does not affect the assessment of the waste If the assessment identifies that the waste is not infectious it can be placed in the domestic refuse e.g. small dressings and plasters, incontinence products etc. This type of waste must be wrapped in a plastic bag (which is not orange) and placed in the household waste in a solid dustbin/wheelie bin with lid to avoid any pest problems and odours associated with split bags
Provide staff needing to dispose of infectious and offensive waste, i.e. it is not appropriate to dispose of in the domestic waste (see above), should follow the process below:
1) The HCW can safely transport very small quantities of infectious waste / clinical waste from the home environment back to base only if there is a registered waste collection at the base and that he/she has a secure, leak proof rigid container that complies with packaging instruction P621 and UN approval. A maximum of 20kg of waste can be transported in a vehicle by a HCW, without completing a transport document. The HCW must ensure that it is kept in a rigid container in the boot of the vehicle to ensure the waste is secure and hidden to prevent any spillage or theft.
2) Sharps generated by the HCW in a client’s home, can be transported in the vehicle of the HCW in a sharps container. If the HCW is travelling on public transport, on foot or bike, sharps waste produced by the HCW can only be transported back to base in a community sized (0.6 litre) UN approved sharps bin. All sharps bins must be securely locked (where necessary using the temporary closure mechanism).
3) For all patients requiring a clinical waste contract, staff must contact Provide: Facilities & Estates who will set up a community waste contract on your behalf to collect clinical waste from the patient’s home. Please use (Form: O11IP Clinical waste form), following the link on SystmOne using the waste assessment template.
Provide staff and the primary care contractor must comply with ‘Duty of Care’ including the requirement for document completion and transfer. In summary, the producer bears full responsibility for the waste, its storage and packaging, arranging for its collection and preparing the required documentation.
Examples of waste generated by the HCW in a patient’s home:
Stoma/catheter bags
If a healthcare worker is involved in the care of a stoma site, the waste from a stoma patient can be disposed of in the black bag waste stream, unless more than a standard size bag is generated a week. In this case it should be placed in orange clinical waste bag and collected by a registered waste contractor.
If the person develops any type of gastrointestinal infection or the site becomes infected, all of the waste must be disposed of as infectious waste into the orange bag waste stream. It must be collected by a registered waste contractor.
Maggots
All maggots used for wound management must be secured in an airtight rigid yellow container and marked as UN 3291 and disposed of as per supplier’s instruction.
Disposable instruments
Metal disposable instruments must be put into an orange-lidded community sharps bin.
Plastic disposable instruments
Pose no risk of sharps injury and can therefore be disposed of in the same way as any other clinical or domestic waste in the patient’s home.
Lancets
For blood sugar measurements / insulin syringe & needle. During a home visit these can be disposed of in a yellow lidded sharps bin.
Clinical Waste Produced in Schools and Special Schools
Waste contaminated with body fluids e.g. nappies, incontinence pads etc need to be packaged and disposed of as per procedures and local Council policy. It is the responsibility of school welfare to arrange disposal by local Council collections.
Sharps used by immunisation practitioners for immunisation sessions Immunisation practitioners have a duty to ensure that sharps are disposed of correctly following an immunisation session.
Empty sharps bins (UN 3291 yellow lid) should be taken to the School together with all other materials (vaccines, swabs, alcohol hand gels, plasters etc.) by the immunisation practitioners.
Sharps bins must be no more than ¾ full (up to the black line on the container), and then locked, signed and dated for disposal.
The immunisation practitioners are responsible for transporting used sharps waste back to central bases for waste collection. All staff must sign to say they understand the procedure for transporting hazardous goods. All staff must keep a copy of the Transport Document (Appendix 5) in their cars at all times. All used sharps containers are transported in a securely lidded leak proof container that complies with packaging instruction P621 and UN approval which is contained within the boot of their car. It is the responsibility of the nurse to ensure that the sharps bins are stored safely and preferably disposed of at the end of each session.
BCG vaccinations are classed as cytotoxic/cytostatic and should be disposed of in purple lidded sharps bins.
Clinical waste produced by the patient only in their own home
Waste from domestic minor first aid and self-care e.g. soiled sanitary products and plasters are not normally considered to be infectious. Where the householder is self-injecting with no HCW involved, the GP should prescribe a sharps bin for the patient. The appropriate coloured sharps bin should be prescribed by the GP. The patient or carer should be trained in how to use the sharps bin when it is prescribed to ensure that they understand how to safely assemble, store and correctly seal it, and where appropriate label it.
Once the sharps bin is three quarters full (up to the marked black line on the sharps box), the householder should seal the sharps bin and return it to a pharmacy or GP surgery for disposal. If the patient is housebound and a carer cannot return the sharps bin, Provide will organise a home collection. However, if a member of the public arrives at any Provide healthcare premises with sharps waste, this should be accepted and the person told how to obtain approved sharps bin via their GP and return it to a pharmacy next time. If brought into the healthcare premises in an unsafe condition, the member of staff receiving the receptacle must, render it safe by putting it in a rigid container and locking it away until a large enough sharps bin can be obtained and the items sealed within it for disposal. The whole unit must be placed into the sharps bin and the receptacle handled as little as possible.
7. Transport
Transportation of Healthcare Waste – On Provide Premises
All staff that handle Healthcare waste (clinical waste) must be fully trained in the correct procedures on how to handle it.
The containers used for the transportation and outside storage of Healthcare waste (clinical waste) within hospital sites, e.g. healthcare sites in Provide, practices, pharmacies and dentists who choose to be within Provide contracts, health centres and clinics will be constructed so that:
• Surfaces of the container are smooth and impermeable
• They do not harbour insects
• Can be easily cleaned and drained and do not encourage waste to lodge externally
• The waste may be easily loaded, secured and unloaded
The containers/secured wheelie bins must be disinfected following leakages and spills, and at regular intervals, at least once every six months.
Clinical waste must not under any circumstances be transported with any other type of waste.
Personal Protective Clothing
The following protective clothing must be available for porters transporting large volumes of waste:
• Suitable heavy duty, reinforced, needle-proof gloves
• Safety shoes or industrial Wellington boots to protect the feet against the risk of containers being accidentally dropped. The soles of such shoes or boots should be non-slip and need to provide protection against the spillage or sharps These will be provided by the relevant contractor for staff that come in contact with clinical waste. i.e. porters
• An industrial apron or leg protectors if container handling creates a risk of bodily contact.
The waste management contractor is required to deal with spillages of liquids and sharps in a safe manner.
Immunisation
Staff handling healthcare waste should be offered appropriate immunisation, including hepatitis A, B and tetanus.
Transportation of Clinical Waste – Off Provide Premises
A licensed waste contractor collects the Clinical waste (health care waste) on a regular basis from all sites. The collections are carried out from most sites once a week and from larger sites more often. The waste is then transported to a disposal site. Clinical waste is usually collected at intervals agreed with the producer, e.g. on monthly or six weekly basis, although more frequently if the need arises. Waste should not normally be secured (i.e. lid firmly closed and sealed) for collection until the container is twothirds full or at specified legal time limit, e.g. cytotoxic six monthly intervals.
Transport of packaged goods
Hospitals and clinics are responsible for requiring dangerous goods to be transported offsite. These become the ‘consignor’ and it is their duty to comply with the transport legislation in ‘legislation and healthcare waste’. The carriage regulations require:
• Classification and identification
• Packaging
• Marking
• Labelling
• documentation
Packing provision for healthcare waste:
Category B (3291)* Clinical waste: Rigid packaging or wheeled bins
Packing instructions
Rigid, leak proof packaging. All packaging including UN- approved packaging must be fit for purpose and capable of safely containing the goods (leak-proof) when in transport, whether carrying liquids or solids.
Transport of Clinical waste
Most clinical waste will be transported as UN 3291 and it is subject to the packing requirements P621. Whilst in transport, clinical waste must be carried in a rigid outer packaging unless transported in bulk. Community nurses collecting clinical waste in their vehicles should ensure they use rigid, secure and leak-proof receptacles in which bags are placed.
Soiled surgical instruments
Where healthcare organisations transport instruments by road to centralized sterile services they are exempt from the terms of ADR, (European agreement concerning the international carriage of dangerous goods by road) as long as the instruments are:
• Packed in packaging designed and constructed in such a way that, under normal conditions of carriage, they cannot break, be punctured or leak their contents, and the packaging is designed to meet the construction requirements detailed in the Safe Management of Healthcare Waste (2013, DH).
• NHS Property Services: Contracts monitoring Officer, monitors the waste contractor to ensure that they are compliant with all current legislation. This should occur on at least an annual basis, e.g. practically follow the waste contractor and ensure that the waste is collected and transported correctly to the waste treatment facility. This is part of the Duty of Care of the organisation.
Contract meetings to monitor performance will be held annually and usually also on a quarterly basis (see contract). This responsibility is with NHS Property Services. Provide as part of their contractual arrangements will audit their services annually.
In order to comply with legislation certain documentation must be completed and accompany the waste on its journey from collection to waste treatment facility. A waste
transfer note is required for non-hazardous waste and a consignment note is required for hazardous waste.
The HCW producing the waste can transport the clinical waste from the home environment back to base where there is a registered waste collection (see 4.2.2). A maximum of 20kg of waste can be transported in a vehicle by a HCW. The waste must be transported in a secure, leak proof rigid container that complies with packaging instruction P621 and UN approval. The HCW must ensure that it is kept in a rigid container in the boot of the vehicle to ensure the waste is secure and hidden to prevent any spillage or theft. The Transport Document must be easily accessible in the vehicle should it need to be seen by the Emergency Services in the event of an accident or incident.
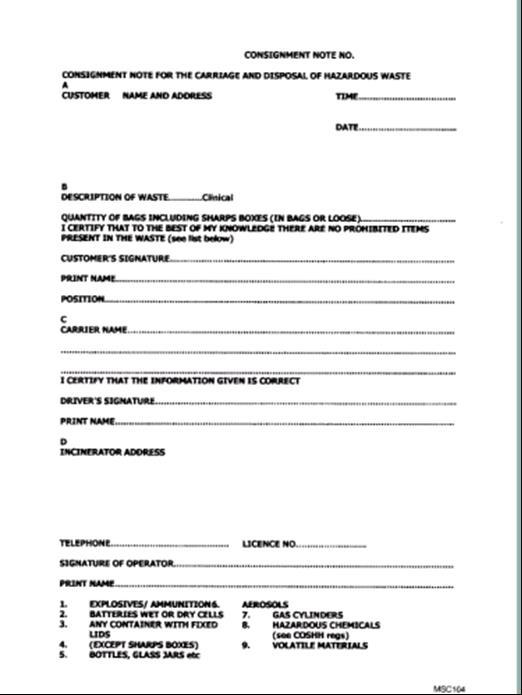
Consignment Note
A Waste Consignment Note must be completed for each clinical waste collection at clinic sites. An example of a consignment note can be found in (Appendix 7). A copy is left on site after each collection. This must be filed in a separate file, and readily accessible to anyone who needs to inspect it (e.g. Waste Contracts Manager, Infection prevention team, and Environment Agency etc.). On a regular basis a copy is sent from the waste contractor to the site that produced the clinical waste. The Manager or responsible person must marry up the two copies, and check to ensure the information is correct and that the waste disposal company has signed it to show that the waste has been disposed of. If there are any inconsistencies between the two copies, the contracts monitoring officer should be contacted. The waste disposal company must also send consignee returns to the producer periodically (normally quarterly) which must be checked against consignment notes.
All Consignment Notes must be kept for three years from the date of issue
Each type of waste should carry a code to comply with the List of Wastes (England) Regulation (List of Legal Definitions) 2005. These are shown in (Appendix 8).
8. Storage and Labelling
Storage
All bins in clinical areas should be lidded and foot or sensor operated and must be rigid sided, to reduce the risk of infection. All new bins purchased should be of a hands free type, for further information contact the Infection Prevention Team, Medicines Management Team or the Estates & Facilities Team.
The external storage areas should be large enough to ensure that different types of waste can be stored separately i.e. domestic, offensive, infectious and sharps. This could be in separate cages, trunks or wheelie bins.
The collection containers and areas will be kept secure from unauthorized persons and entry by animals and free from infestation by rodents and insects. The containers must be kept locked at all times, and wheeled containers must be kept secure. Keys will be kept by a person designated by the manager and the contractor removing the clinical waste. Where possible a combination lock with pre-agreed combination provided by Estates & Facilities Team should be used.
Provide must provide a spillage kit to deal with clinical waste spillages. Clinical staff are required to deal with spills of blood or other body fluids in a safe manner.
Regular cleaning of the containers and areas must be carried out using General Purpose Detergent and hot water, at least once every six months (or after a spillage). Managers are responsible for ensuring that they are cleaned. For further information contact the contracts monitoring officer for NHS Property Services.
Should there be insufficient capacity in the containers on a regular basis, appropriate measures must be taken e.g. arrange extra collections via the waste contractor/ service provider or purchase an extra container via the Estates & Facilities
Under no circumstances must clinical waste be left in corridors or in a place that is not secured.
Storage areas must be:
• Well-lit and ventilated
• Sited away from food preparation and general storage areas, and from routes used by the public
• Where possible, enclosed and secure
• Sited on a well-drained, impervious hard-standing
• Readily accessible but only to authorised people
• Kept locked and secure when not in use
• Provided with wash-down facilities for waste are desirable
• Provided with washing facilities for employees
• Provided with separate, clearly labelled areas for waste destined for different treatment /disposal options
• Provided with access to first aid facilities
Labelling
All sharps bins must be signed and dated by the individual member of staff on assembly, and when locked before disposal.
9. Management of Clinical Waste in the Community Setting (Category B)
Assessing whether waste poses a risk of infection
Healthcare staff working in the community are responsible for waste produced as a result of their activities. This means everyone who manages waste or has a responsibility for waste is required to fully comply with their duty of care. The community healthcare worker must first access and classify the waste correctly.
Healthcare workers in the community working in patients’ homes will need to assess the waste. To accurately assess whether the waste generated is infectious, a risk assessment should be performed. This should be based on the professional assessment, clinical signs, symptoms and any prior knowledge of the patient. Please refer to initial waste assessment template on SystmOne.
These general categories should be used to subcategorise the waste:
• Infectious-waste from any known or suspected infection, and from any other cases where a risk of infection has been identified
• Contaminated with body fluids more suited to the offensive classification (that is, lower risk wastes).
Risk assessment approach to waste segregation based on likelihood of infection being present
Contaminant Proposed general classification
Urine, faeces, vomit and sputum
Blood, pus and wound exudates
Offensive (where risk assessment had indicated that no infection is present, and no other risk of infection exist)
Examples Exception to this rule
Urine bags, incontinence pads, single-use bowls, nappies, PPE
Gastrointestinal and other infections that are readily transmissible in the community setting (e.g. verocytotoxin-producing Escherichia coli (VTEC), campylobacter, salmonella, chickenpox/shingles)¹
Hepatitis B and C, HIV –only if blood is present¹
Infectious unless assessment indicates no infection present. If no infection, and no other risk of infection, then offensive
Dressings from wounds, wound drains, delivery packs
Blood transfusion items
Dressings contaminated with blood/wound exudates assessed not to be infectious.
Maternity sanitary waste where screening or knowledge has confirmed that no infection is present and no other risk of infection exists
Notes:
All Category A and B species, and therefore downstream waste items, will be deemed infectious/hazardous under waste regulations irrespective of the contaminant matrix.
1. Potential hazards from the use of cytotoxic and cytostatic medicines may also be relevant in some instances and with some drugs. This would also prevent the waste being considered offensive
Non-infectious waste
• Contaminated dressings from a wound assessment by the healthcare worker as non-infectious can be treated as non-hazardous and should be disposed of in the domestic waste as long as the quantity of waste does not exceed the normal amount of waste generated by the household (i.e. if it exceeds more than 1 large black refuse sack per week-then it is not classed as offensive waste) If large volumes are being produced ,these waste items should be placed into orange
clinical waste bags and be disposed of by the licenced, contracted clinical waste operator.
• Non-infectious waste: examples of these types of waste include dressings, bed pads, bandages and protective items (i.e. gloves & aprons) contaminated with bodily fluids –where the assessment process leads the HCW to believe the waste does not pose a risk of infection risk.
• The domestic waste option can only be used with the householders permission and the offensive waste item must be double-bagged (using a sandwich type bag or bin liner) before placing in the householder’s domestic waste bin.
When to set up a clinical waste contract
• If waste is a larger quantity than normally produced by the household (defined as equivalent to 1 large refuse sack size per week).
• Or if the waste is deemed to be INFECTIOUS waste (i.e. the patient has a known wound infection)
Examples of potential waste issues relating to community integrated care teams
• A patient colonised with MRSA –the waste generated in the patient’s home is treated as offensive waste (normal household waste).
• An infected wound, patient has a known infection as is been treated with antibiotics( Orange clinical waste –set up clinical waste contract )
• Maggots (Larval therapy) –should be disposed of either in a rigid Yellow-lidded container or double-bagged yellow and treated as infectious waste (Orange clinical waste –set up clinical waste contract)
• Storage of Clinical Waste in patient’s home: The householder must consent to storing the waste (not accessible by children or animals) until collected by a licenced, contracted clinical waste contractor.
10.Training
Clear information, instruction and training on categorising waste will be provided for staff in areas where clinical waste arises. Managers will be responsible for ensuring that staff receive the job specific training.
Training will be included within the Induction Training, followed by update training. Each provider will be responsible for the arranging of the induction and mandatory training, in addition to maintaining the relevant records. The provider will also give sufficient information, instruction and training as is necessary to ensure the health and safety of employees carrying out procedures involving clinical waste. This provision will also apply to those persons not in direct employment, such as agency staff. However, responsibility for training rests with their employer (Appendix 3).
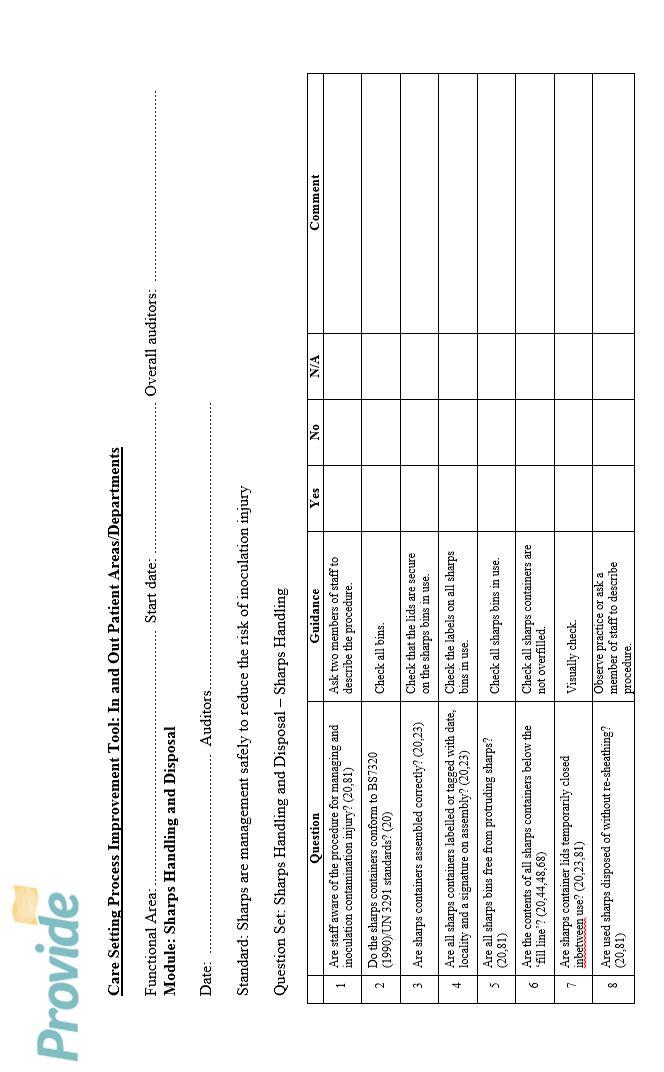
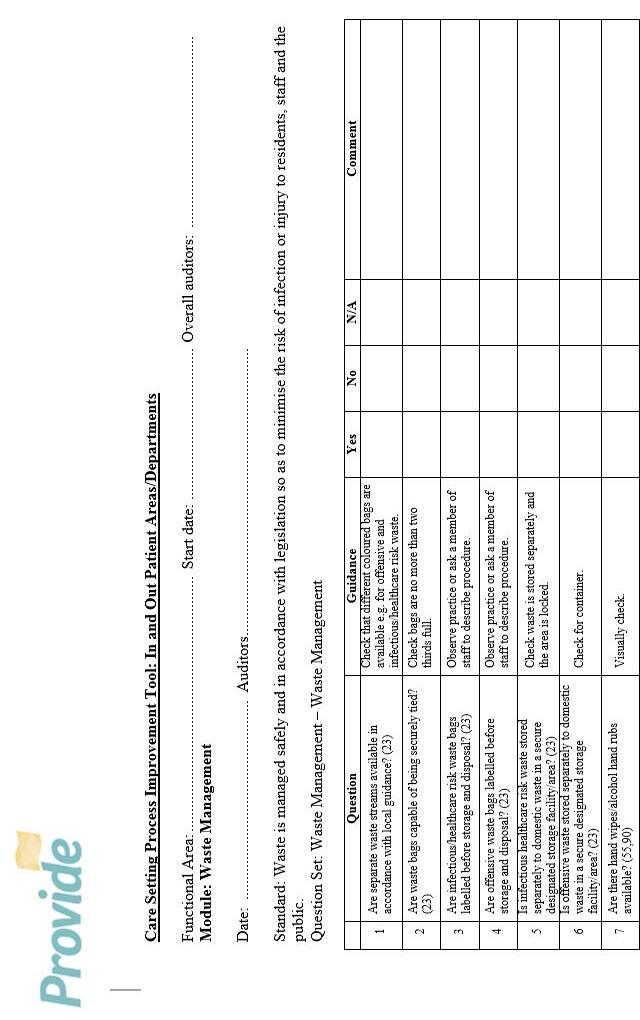
11.Waste Audit
Waste audits are an essential tool in assessing the composition of a waste stream for the purpose of compliance with Provide Duty of Care and for monitoring waste segregation. The audit results can be used to develop and influence waste management policies and procedures and identify appropriate recycling options. Annual audits provide a snapshot of waste management practices.
Pre-acceptance audits are now a legal requirement and are carried out by all sites. These audits monitor the effectiveness of waste segregation, training and training to demonstrate compliance and where required to take action to remedy non-compliance.
Feedback will be given to staff and management on outcomes of audits by the auditor and respective managers will be responsible for any follow-up action needed.
Scope of audits
• Provide will carry out an annual audit at larger sites and contractor sites will be carried out by an external auditor
• Monthly audit programme high impact intervention /observational audit tool audits compliance with sharps policy
• Waste management template on SystmOne for all community staff working in patients’ homes
12.Contingencies
NHS Property Services is responsible for ensuring that as part of the contract with the Transport Company and Disposal Company they must have contingency plans built in. This would mean that the responsibility for any transport or disposal problems would revert back to the respective companies.
13.References
The Carriage of Dangerous Goods and Use of Transportable Pressure Equipment Regulations 2009 SI 1348
The Controlled Waste Regulations 1992
The Environmental Protection Act 1990 (c.43)
Environmental Protection (Duty of Care) Regulations 1991
The Hazardous Waste (England and Wales) Regulations 2005
The Hazardous Waste (England and Wales) Amendments Regulations 2016
Environment and sustainability, Health Technical Memorandum 07-01: Safe Management of Healthcare Waste 2006
Schedule 3 of the Control of Substances Hazards to Health Regulations (COSHH) 2002
Health and Safety at Work Act 1974
The Health and Safety (Consultation with Employees) Regulations 1996
The List of Wastes (England) Regulations 2005
Royal College of Nursing (2014). The management of waste from Health, Social and Personal Care . RCN. London.
Safe Management of Health Care Waste, RCN guidance, November 2007
Safe management of healthcare waste: 2013 .DH
Infection; Prevention and Control of healthcare-associated infections in primary and community care92012); NICE clinical guideline 139. www.nice.org.uk/cg139
The Health and Social Care Act 2008: Code of Practice on the Prevention and Control of infections and related guidance. DH
The Management of Health & Safety at Work Regulations 2006 (2006 amendment and 1999 regulations)
Waste Electrical and Electronic Equipment Directive 2002/96/EC
The Waste Electrical and Electronic Equipment Directive (WEEE Directive) was introduced in January 2007.
The WEEE Directive aims to reduce the amount of electrical and electronic equipment being produced and to encourage everyone to reuse, recycle and recover it.
The WEEE Directive also aims to improve the environmental performance of businesses that manufacture, supply, use, recycle and recover electrical and electronic equipment.
If you are an importer, rebranded or manufacturerof new electrical or electronic equipment, then it's likely that you'll need to comply with the UK's WEEE Regulations, which in part implement the WEEE Directive. If you do need to comply, then you must register on a producer compliance scheme.
You may also have obligations under the WEEE Regulations if you are a business with electrical or electronic equipment to dispose of, or if you sell electrical or electronic equipment.
Our role is to provide information and advice on complying with the WEEE Regulations to producers of Electrical or Electronic Equipment (EEE) and the waste management industry.
Batteries and Accumulators and Waste Batteries and Accumulators Directive (2006/66/EC)
Establishes a legal framework and schemes for collecting, treating and recycling portable, industrial and vehicle batteries. Applies to all types of batteries except when used for military and space equipment
The Management of Health & Safety at Work Regulations 2006 (2006 amendment and 1999 regulations)
The Management of Health and Safety at Work Regulations 2006 places a duty on employers to assess and manage risks to their employees and others arising from work activities.
Employers must also make arrangements to ensure the health and safety of the workplace, including making arrangements for emergencies, adequate information and training for employees and for health surveillance where appropriate.
Employees must work safely in accordance with their training and instructions given to them. Employees must also notify the employer or the person responsible for health and safety of any serious or immediate danger to health and safety or any shortcoming in health and safety arrangements.
Appendix 1: Legal and Statutory Requirements
Section 34 of the Environmental Protection Duty of Care (EPA) Act 1991
The main responsibilities of the waste producer are:
• Describe the waste fully and accurately.
• Complete and sign a waste transfer note (or consignment note for hazardous waste) prior to waste being transferred to another party.
• Pack waste securely (where appropriate) in line with the Carriage Regulations
• Store waste safely on site.
• Register as a waste carrier (if required) and make all reasonable checks on waste carriers.
• Select an appropriate treatment or disposal method.
• Ensure waste falls within the terms of the waste contractor’s waste management licence or permit.
Section
45 of the Environmental Protection
The section states:
(EPA) Act 1991
‘It is the duty of each waste collection authority to arrange for the collection of household waste in its area. It also states that the authority may make a reasonable charge for the collection of certain types of household waste to reflect the higher disposal costs and separate collection arrangements that have to be made. These include clinical waste from a domestic property.’
Waste management licenses and permits are required for the storage, treatment and disposal of many different types of waste. Generally, a license is not required for the storage of waste on the site where it was produced, as this is covered by a waste management license exemption.
Health and Safety Legislation Act 1974
All risks associated with health care waste must be assessed, including those risks that may affect members of the public as well as staff. Procedures and policies must be in place to ensure effective management of the risks. These need to be part of the organisations’ overall health and safety management procedures and policies.
Employers are responsible for complying with health and safety legislation. Self-employed staff are treated as employees under health and safety legislation, legal duties with the respect to Health and Safety at Work legislation cannot be passed on by means of a contract.
The Control of Substances Hazardous to Health Regulations (COSHH) 2002
Employers must, among other things:
• Assess the risks to employees and others from health care waste.
• Make arrangements for reviewing the assessment as and when necessary, but at no less than two yearly intervals – and sooner if there is any reason to suggest the risk assessment is no longer valid.
• Aim to eliminate or prevent these risks, and if this is not possible to adequately control the risks.
• Provide suitable and sufficient information, instruction and training for employees about the risks.
• Provide health surveillance and immunisation where appropriate.
The Management of Health and Safety at Work Regulations 2006
Employers must among other things:
• Make a suitable and sufficient assessment of the risks to employees and others. If they have five or more employees, they must record the significant findings of the assessment.
• Take particular account in their assessment of risks to new and expectant mothers and their unborn and breast-feeding children.
• Take particular account in their assessment of risks to young people.
• Make arrangements for the effective planning, organisation, and control.
• Monitor and review any precautions
• Provide health surveillance where appropriate
• Have access to competent health and safety advice.
• Provide information for employees.
• Co-operate with other employers who may share the workplace.
The Carriage of Dangerous Goods and Use of Transportable Pressure Equipment Regulations (‘The Carriage Regulations’) 2009
The carriage of Dangerous Goods (those materials with an identifiable hazard) is subject to regulatory control. The Carriage Regulations are intended to reduce, to reasonable levels, the risk of harm or damage to people, property and the environment posed by the carriage of dangerous goods.
It is recommended that a Dangerous Goods Safety Advisor (DGSA) is appointed or advice sought from a qualified DGSA for carriage, related packaging, loading, filling or unloading of dangerous goods. It is the duty of the DGSA to monitor and advise on dangerous goods carriage compliance and ensure relevant incidents/accidents are properly investigated and reported. The DGSA must also prepare an annual report on dangerous good activities.
Waste Electrical and Electronic Equipment (WEEE) Directive 2006
Another piece of legislation that affects Healthcare Waste is the Waste Electrical and Electronic Equipment (WEEE) Regulations.
The HazardousWaste(England andWales) Regulations 2005 andAmendments 2016 and the List of Wastes (England) Regulations 2005
Hazardous Waste is the term used to describe waste with hazardous waste properties in line with the European Hazardous Waste Directive. Both of these regulations define and regulate the segregation and movement of hazardous waste in England and Wales from the point of production to the final point of disposal or recovery. These Regulations, among other things, require produces of hazardous waste to notify the regulatory authority.
The Hazardous Waste (England and Wales) Amendments Regulations 2009 regard registering with the Environment Agency if more than 500kg of hazardous waste produced in a 12 month period. For guidance on the registration process, contact the Estates & Facilities Department.
Appendix 2: Waste Colour Coding
Waste Receptacle Description
Yellow with purple stripe
Yellow purple lid
Infectious waste contaminated with cytotoxic and /or cytostatic medicinal products
Sharps contaminated with cytotoxic and /or cytostatic medicinal products
Example Contents
Dressings / tubing from cytotoxic and/or cytostatic treatment
Sharps used to administer cytotoxic products.
Yellow/orange
waste
Infectious waste,
category A – yellow
category B – orange
see section 4
Non- medicinally contaminated sharps
Orange top
Medicinally contaminated sharps
Yellow top
amalgam waste
Soiled dressings from infected wounds and other items contaminated with infectious body fluids
Sharps from phlebotomy minor surgery instruments scalpel blades, razor blades
Ampoules, vaccine syringes and needles
Local anaesthetic syringes and needles
Amalgam
Dental
CONTAINER
Human hygiene waste and Non-infectious disposable equipment, bedding plaster casts, etc.
(Provide is currently not using tiger bags, but putting offensive waste into orange clinical waste bags ) Black bag
Blue
Red
1100 litre green wheelie bin Cardboard
1100 litre blue wheelie bin
ONLY use blue lidded sealed units for patient returned medicines
(include solids, liquids and aerosols)
ONLY use purple lidded containers for cytotoxic and cytostatic medicines
Pharmacy Waste
Pharmacy Waste
Appendix 3: Training
Training needs vary depending on the job and on the individual. All staff involved in handling clinical waste need training, information and instruction in:
• The risks associated with clinical waste, its segregation, handling, storage and collection;
• Personal hygiene;
• Any procedures which apply to their particular type of work;
• Procedures for dealing with spillages and accidents;
• Emergency procedures;
• The appropriate use of protective clothing.
Training for staff that collects, transfer, transport or handle quantities of clinical waste needs to cover:
• Checking that storage containers are sealed effectively before handling;
• Ensuring that the origin of the waste is marked on the container;
• Handling sacks/containers correctly;
• Using handles to move rigid containers;
• Checking that the seal on any used sharps container is unbroken when movement is complete;
• Special problems relating to sharps disposal;
• Procedures in case of accidental spillage and how to report an incident;
• Safe and appropriate cleaning and disinfection procedures.
• Risk assessments for infectious waste in patients’ homes
• Template on SystmOne
Appendix 4: The ADR 2005 Category A Pathogen List
INDICATIVE EXAMPLES OF INFECTIOUS SUBSTANCES INCLUDED IN CATEGORY A
IN ANY FORM UNLESS OTHERWISE INDICATED (ADR 2005. Section 2.6.3.2.2.1 (a))
(Provided in compliance with the Carriage of Dangerous Goods and Use of Transportable Pressure Equipment Regulations 2009 (as amended))
The person in charge of this vehicle is a Community Healthcare Practitioner, acting for Provide, who travels extensively in the area providing home treatment for patients.
Articles and substances carried on the vehicle are outputs from patient treatments. They are listed in The Carriage of Dangerous Goods and Use of Transportable Pressure Receptacles Regulations 2004 and identified for transport purposes as:
UN3291 Clinical Waste, Unspecified, N.O.S. (health care risk waste), 6.2 II being conveyed to a Trust site for end-disposal.
UN3291, Clinical Waste, Unspecified, N.O.S. (pathogen infected medical instruments), 6.2, II being conveyed to a Sterilisation Centre for cleaning and further use.
UN3373 Diagnostic Specimens - being conveyed to a laboratory for analysis.
Volumes carried will be variable day to day but are not expected to exceed 20 kilograms in aggregate and, therefore, they qualify for the relaxation of the Dangerous Goods Carriage Regulations under the ‘Excepted Quantity’ provisions.
It is certified by the Trust that packaging’s used for containment of these articles and substances meet the technical standards listed in the Regulations:
In the event of incident involving this vehicle, an Emergency Services representative is requested to advise Provide by contacting: 07623 507 914 (or out of hours the relevant Provide out of hours contact on 07623 507 914). MEHT – Waste Contract Manager: 01245 514017
Note for Emergency Services Personnel – WRITTEN EMERGENCY INFORMATION FOR UN3291 IS ON REVERSE
EMERGENCY INFORMATION FOR:
UN3291, CLINICAL WASTE, UNSPECIFIED, N.O.S. 6.2, II
Extinguishing media – Fine Waste Spray
Personal Protection – Liquid-tight chemical protective clothing conforming to BS8228, in combination with self-contained open circuit positive pressure compressed air breathing.
Appendix 6:
Appendix
7: Site Waste Audit Tool
Appendix 8: Example Consignment Note (for clinic sites)
Appendix 9: List of Legal Waste Definitions
(List of Wastes (England) Regulation 2005)
N.B. THIS APPENDIX IS ONLY APPLICABLE TO WASTE PRODUCTS ON PROVIDE ESSEX COMMUNITY SERVICES SITES
18 01 06* Sharps, contaminated with medicines, infectious
Used syringes with needles attached, broken glass ampoules, needles, scalpels and other blades, infusion sets (the sharps part) contaminated with medicines should be placed in a yellow lidded sharps container.
N.B. If the above is contaminated with Cytotoxic or Cytostatic products they must be placed into separate sharps container with purple lid and disposed of as Hazardous waste 18 01 08*.
18 01 03* Infectious
Waste whose collection and disposal is subject to special requirements in order to prevent infection. The NHS has divided this into two sub-categories:
1. Minimum treatment/disposal required is incineration in a suitable licensed or permitted facility. This will be placed into Yellow bags. This is highly unlikely to be generated in the community.
2. Minimum treatment/disposal is to be rendered safe in a suitable licensed or permitted facility. This will be placed into an Orange bag and will be the infectious waste generated by Provide.
18 01 04 Offensive Waste (No known source of infection)
Waste whose collection and disposal are not subject to special requirements in order to prevent infection. Minimum treatment/disposal required is deep landfill in a suitable licensed or permitted facility. This will be placed into orange clinical waste bags (as we currently do not use Tiger bags). This will normally be generated in the community setting (Care Home / Residential Home) and consist of dressings, disposable clothing, incontinence pads, feminine hygiene and renal.
18 01 10* Amalgam waste from dental care
Amalgam must not be released into the foul drains and separators must be fitted to all dental facilities to prevent this occurring. These units collect the amalgam and are removed as a sealed unit for recycling with amalgam collected from day to day operations.
These must be stored in containers provided by contractor prior to disposal.
Appendix 10: List of Cytotoxic and Cytostatic Drugs
Currently there is no official list of cytotoxic & cytotoxic medicines in England & Wales, but the Environment Agency has suggested that the following list, prepared in America, is a useful starting position. Please note that the names of the medicines are American, so they may not be totally familiar in England & Wales
Yes, if you have insurance to drive your car for work. You must also carry a Transport Document as per Appendix 5.
If a client in their own home has MRSA which waste stream should I put their waste?
If a patient is colonised but not receiving treatment for an infection then the status of the patient does not affect the waste stream –therefore normal household waste.
If the patient is colonised and receiving treatment – then yes –waste assessment is necessary - please use waste risk assessment template on SystmOne
If the patient is MRSA positive, receiving treatment and microorganism is present in the waste stream – then yes, class as infectious waste. A clinical waste contract will require to be set up.
In a school situation, where should a nappy be disposed of if a child is known to have HIV?
They should be treated the same as any other nappy waste in accordance with the school policy.
Does the Community Health Care Worker have to supply the client with waste disposal bags for disposal from their home?
If you are required to set up contract with licenced, contracted clinical waste contractor –yes they will supply the bags for infectious waste.
When a Community Health Care Worker changes a stoma bag and/or a catheter in the clients home, which waste stream should they be disposed of?
If less than 1 bag normal household waste –if more than 1 bag –offensive waste stream –orange clinical waste bag and licensed contracted clinical waste contractor will need to collect
When a Community Health Care Worker changes an incontinence pad in the clients’ home, which waste stream should they be disposed of?
The incontinence pad should be double-bagged and placed in the domestic waste.
In a client’s home where do I put blue plastic forceps from a dressing for disposal?
As this does not present any risk of sharps injury it can be disposed of in the same way as any other clinical waste in the clients’ home: domestic waste.
Appendix 12: Clinical Waste Collection Form
This form should be completed by a health care professional
This form is to ensure we are undertaking our duty of care, to ensure health care waste is classified correctly when collected from patients’ homes by our services.
I confirm the waste described is an accurate description of the needs of the patient, to ensure waste is disposed of correctly in accordance with the waste ‘duty of care’
Healthcare Professional Signature: ..............................................................................Date:
Thank you.
This information will be shared with our collection contractor by Provide Facilities & Estates team securely destroyed when services are no longer required. Please email form to: provide.estates@nhs.net
Name of project/policy/strategy (hereafter referred to as “initiative”):
IPPOL12 –Healthcare waste policy – Sharps, Infectious and Offensive Waste arising from Healthcare Activities
Provide a brief summary (bullet points) of the aims of the initiative and main activities:
Project/Policy Manager: Specialist Infection Prevention Nurse Date: Oct 2018
This stage establishes whether a proposed initiative will have an impact from an equality perspective on any particular group of people or community – i.e. on the grounds of race (incl. religion/faith), gender (incl. sexual orientation), age, disability, or whether it is “equality neutral” (i.e. have no effect either positive or negative). In the case of gender, consider whether men and women are affected differently.
Q1. Who will benefit from this initiative? Is there likely to be a positive impact on specific groups/communities (whether or not they are the intended beneficiaries), and if so, how? Or is it clear at this stage that it will be equality “neutral”? i.e. will have no particular effect on any group.
Neutral
Q2. Is there likely to be an adverse impact on one or more minority/under-represented or community groups as a result of this initiative? If so, who may be affected and why? Or is it clear at this stage that it will be equality “neutral”?
Neutral
Q3. Is the impact of the initiative – whether positive or negative - significant enough to warrant a more detailed assessment (Stage 2 – see guidance)? If not, will there be monitoring and review to assess the impact over a period time? Briefly (bullet points) give reasons for your answer and any steps you are taking to address particular issues, including any consultation with staff or external groups/agencies.
Neutral
Guidelines: Things to consider
• Equality impact assessments at Provide take account of relevant equality legislation and include age, (i.e. young and old,); race and ethnicity, gender, disability, religion and faith, and sexual orientation.
• The initiative may have a positive, negative or neutral impact, i.e. have no particular effect on the group/community.
• Where a negative (i.e. adverse) impact is identified, it may be appropriate to make a more detailed EIA (see Stage 2), or, as important, take early action to redress this – e.g. by abandoning or modifying the initiative. NB: If the initiative contravenes equality legislation, it must be abandoned or modified.
• Where an initiative has a positive impact on groups/community relations, the EIA should make this explicit, to enable the outcomes to be monitored over its lifespan.
• Where there is a positive impact on particular groups does this mean there could be an adverse impact on others, and if so can this be justified? - e.g. are there other existing or planned initiatives which redress this?
• It may not be possible to provide detailed answers to some of these questions at the start of the initiative. The EIA may identify a lack of relevant data, and that data-gathering is a specific action required to inform the initiative as it develops, and also to form part of a continuing evaluation and review process.
• It is envisaged that it will be relatively rare for full impact assessments to be carried out at Provide. Usually, where there are particular problems identified in the screening stage, it is envisaged that the approach will be amended at this stage, and/or setting up a monitoring/evaluation system to review a policy’s impact over time.
EQUALITY IMPACT ASSESSMENT TEMPLATE: Stage 2:
(To be used where the ‘screening phase has identified a substantial problem/concern)
This stage examines the initiative in more detail in order to obtain further information where required about its potential adverse or positive impact from an equality perspective. It will help inform whether any action needs to be taken and may form part of a continuing assessment framework as the initiative develops.
Q1. What data/information is there on the target beneficiary groups/communities? Are any of these groups under- or over-represented? Do they have access to the same resources? What are your sources of data and are there any gaps?
N/A
Q2. Is there a potential for this initiative to have a positive impact, such as tackling discrimination, promoting equality of opportunity and good community relations? If yes, how? Which are the main groups it will have an impact on?
N/A
Q3. Will the initiative have an adverse impact on any particular group or community/community relations? If yes, in what way? Will the impact be different for different groups – e.g. men and women?
N/A
Q4. Has there been consultation/is consultation planned with stakeholders/ beneficiaries/ staff who will be affected by the initiative? Summarise (bullet points) any important issues arising from the consultation.
N/A
Q5. Given your answers to the previous questions, how will your plans be revised to reduce/eliminate negative impact or enhance positive impact? Are there specific factors which need to be taken into account?
N/A
Q6. How will the initiative continue to be monitored and evaluated, including its impact on particular groups/ improving community relations? Where appropriate, identify any additional data that will be required.
N/A
Guidelines: Things to consider
• An initiative may have a positive impact on some sectors of the community but leave others excluded or feeling they are excluded. Consideration should be given to how this can be tackled or minimised.
• It is important to ensure that relevant groups/communities are identified who should be consulted. This may require taking positive action to engage with those groups who are traditionally less likely to respond to consultations, and could form a specific part of the initiative.
• The consultation process should form a meaningful part of the initiative as it develops, and help inform any future action.
• If the EIA shows an adverse impact, is this because it contravenes any equality legislation? If so, the initiative must be modified or abandoned. There may be another way to meet the objective(s) of the initiative.
Further information:
Useful Websites www.equalityhumanrights.com Website for new Equality agency www.employers-forum.co.uk – Employers forum on disability www.disabilitynow.org.uk – online disability related newspaper www.efa.org.uk – Employers forum on age