8 minute read
Wilderness Medicine Suspension Trauma


Suspension Trauma
By Alexis Corcoran, MD, on behalf of the SAEM Wilderness Medicine Interest Group
“Climb if you will, but remember that courage and strength are nought without prudence…do nothing in haste; look well to each step, and from the beginning think what may be the end.” —Edward Whymper
Background
Suspension trauma, also called harness hang syndrome or orthostatic intolerance, results from hanging in a motionless vertical position suspended by a harness for a prolonged period. Any hobby or occupation that requires the use of a harness could potentially result in suspension trauma, so rock climbers, ice climbers, spelunkers, hunters in elevated stands, parachutists, other avid adventurists, electricians, and construction/high rise workers are at risk of life-threatening or fatal suspension sequelae. A large fall leading to extremity fracture(s), a head injury from falling debris, or any other medical problem or mechanism that leads to impaired awareness, decreased consciousness, or impaired mobility can lead to hanging suspended vertically and immobile in the harness. Suspension trauma is a true emergency, as it can cause death in as little as 10 minutes, though, if it occurs, death typically takes place between 15 and 40 minutes. This article will review current literature surrounding suspension trauma, rescue, and management.
Harness Introduction
Harnesses connect outdoor enthusiasts or high-rise workers to an anchor point with a rope as they ascend or descend a wall or structure. Different types of harnesses are used for different activities, as each call for different features, styles, and capacities to hold gear. Climbing harnesses focus their support on the waist and legs, while high rise/construction harnesses focus their support on the waist, legs, shoulders, and chest. The following two figures highlight the main features and differences between these two categories of harnesses, while Table 1 identifies more distinguishing features between harness types.
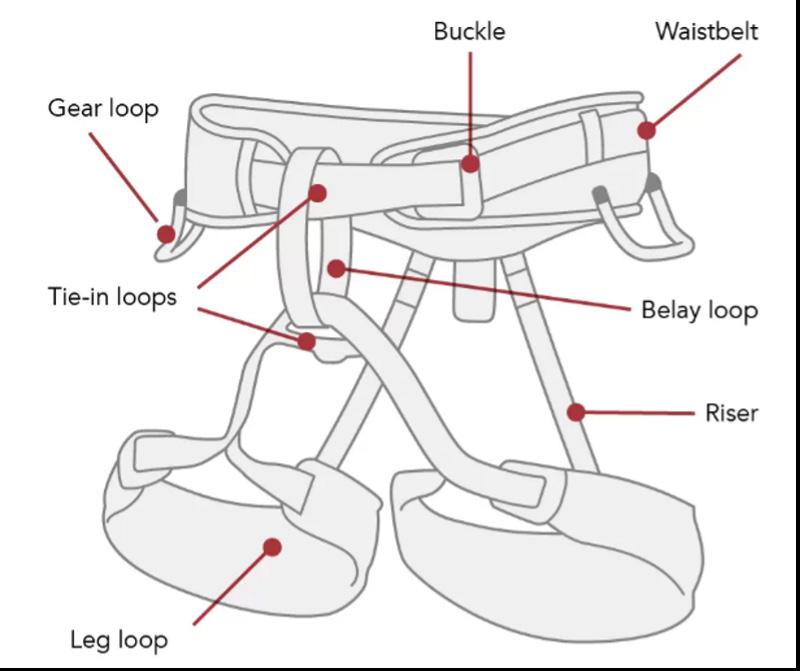
Figure 1: Basic Climbing Harness Features
• The waistbelt is the wide opening at the top that tightens above the waist. Padding depends on harness type. • Leg loops can, but don’t always, adjust around each leg for comfort. These keep the person upright during a fall and help disperse weight when hanging. Padding depends on harness type. • The belay loop attaches to the carabiner and belay device for the belayer. • Tie-in-points (aka hard points) are a redundant system where a rope runs through for the climber. This is the point of connection for fall arrest. • Elastic risers adjust the distance between the waistbelt and leg loops.
Pathophysiology
There is debate of the pathophysiology of harness hang syndrome; however, the most accepted mechanism is a failure of the passive venous pump system. In normal physiologic states, blood pooling dependently is forced back towards the heart with flexion/ movement of the lower extremities and one-way valves within the venous system. When someone is hanging motionless in a harness, their femoral veins may have decreased flow due to external pressure from the harness
as well as decreased lower extremity movement which may be secondary to the position of the harness, fatigue, hypothermia, injury, or unconsciousness. The degree of risk of suspension trauma is increased with blood loss and prior cardiovascular disease.
The combination of decreased flow from external pressure and decreased flow from lack of movement can lead to a decreased effective circulating volume (by up to 20%) mimicking hypovolemic shock. Some people have been observed to lose consciousness within minutes of being suspended, potentially secondary to this decreased effective circulating volume of blood and reduction in cerebral perfusion thereafter. Presyncopal signs and symptoms in this case may include dizziness, pallor, shortness of breath, blurred vision, nausea, diaphoresis, numbness of the legs, decreasing blood pressure, and increasing heart rate. Without suspension in a harness, syncope will usually resolve the underlying pathophysiology of orthostatic hypotension as the body will become horizontal and the blood will return to the heart and subsequently to the brain. However, when people are suspended in a harness, they are unable to turn horizontally which leaves this compensatory mechanism useless.
During rescue from suspension, there is some danger of post-rescue death as the person is turned horizontal from vertical, although the literature has conflicting hypotheses behind the mechanism. In some studies, there are reports of “reflow syndrome,” which results from systemic release of toxin buildup in the hypoxic lower extremities. These toxins can lead to acute kidney injury, cardiac arrythmias, and disseminated intravascular coagulation much like rhabdomyolysis. In other studies, there are reports of the heart’s inability to tolerate the abruptly increased blood flow, leading to a clinical picture much like high output cardiac failure. While these complications are severe and life-threatening, it seems as though many guidelines for rescue follow studies such as Thomassen et al. (2015), and Lee and Porter (2007) who report there is no evidence of reflow syndrome in suspension trauma and the safest rescue technique is quickly turning the person horizontally given the risks of maintaining the vertical position. Various

• The dorsal large D ring is the point of connection for the fall of arrest. • The chest buckle adjusts the size of the harness to the wearer. • The friction torso buckle adjusts the length of the harness, but if installed improperly by the worker there is risk of falling out of the harness. • The right and left D rings are used for positioning of applications when the worker needs their hands to be free. • Leg straps are like those on climbing harnesses.
“When someone is hanging motionless in a harness, their femoral veins may have decreased flow due to external pressure from the harness as well as decreased lower
Figure 3: Foothold deployment.
WILDERNESS MEDICINE
continued from Page 39
rescue techniques are detailed in the following section.
Rescue Techniques and Postrescue Management
Under 29 CFR 1926.502 (d) (Fall Protection Systems Criteria and Practices), Occupational Safety and Health Administration (OSHA) in the United States requires that employers provide for “prompt rescue of employees in the event of a fall or shall assure that employees are able to rescue themselves.” OSHA and National Standards Institute of the United States recommend contact to the suspended person within four to six minutes and prompt rescue to follow.
The suspended person should initially attempt self-rescue, but if this fails, they should “pump” their legs frequently to activate the muscles and reduce the risk of venous pooling until rescue. If possible, the harness should come equipped with deployable footholds that can be used to alleviate pressure, delay symptoms, and provide support for shifting position frequently and for muscle pumping. A cordelette (large sling) or etrier (webbing/ladder) can be attached inside small storage packs to the sides of a body harness to easily be deployed as shown in Figure 3. The suspended person should ideally try to position themselves as horizontally as possible. This can be done with use of footholds, placing feet on the structure/ wall near them, or attempting a sitting position in the harness.
For rescue, bystanders or rescue teams can use pulley systems, brake-tube systems, winch systems, controlled descent devices, and/or rope ladders. Special care should be taken to control profuse bleeding prior to or during rescue to maintain as much circulating volume as possible.
After rescue, OSHA guidelines currently advise to place person in a sitting position with their knees close to their chest in a “W” position. They do not recommend placing person horizontally if possible. However, multiple reviews, including by the Health and Safety Executive in the U.K. in 2009 and Mortimer (2011) recommend that all post-suspension patients be immediately placed in a fully horizontal position for recovery and treatment to restore circulation to vital organs. Many of these reviews argue that the potential risk of reperfusion injury or reflow syndrome is much lower than that of continued effective hypovolemia and hypoxia. In conclusion, rescuers should be aware of the risks of maintaining a more vertical position during rescue and the risks of immediate horizontal positioning, and they should be prepared to manage the potential sequelae of whichever rescue position they choose.
SPORT/GYM CLIMBING HARNESS TRAD (TRADITIONAL) CLIMBING HARNESS
• lightweight • streamlined • light or no padding • multiple gear loops • supports the upper legs and waist • heavier than sport • padded waist belts and leg loops • multiple gear loops • supports the upper legs and waist


BIG WALL CLIMBING HARNESS
• copious padding • larger and stronger gear loops • full strength loop in back for attaching a haul line • supports the upper legs and waist • lightweight • less padding (reduced moisture absorption and freezing) • ample gear loops • dedicated ice clipper slots • supports the upper legs and waist • minimal to no padding • supports the upper legs, waist, shoulders, and chest
ICE/ALPINE HARNESS FULL BODY HARNESS

Suspension trauma is a potential serious complication in outdoor recreation and certain occupations. Further understanding of its physiology and treatment may improve management of this specific condition.
ABOUT THE AUTHOR
Alexis Corcoran is a fourthyear medical student at Albert Einstein College of Medicine who will be applying into emergency medicine with the Class of 2022. While in medical school, she organized multiple emergency simulations, trained with wilderness survival and medical experts in Colorado and Utah, and formed a team of 50 volunteers who produced and distributed over 9,700 face shields and surgical masks for COVID-19 PPE
Resources:
• Suspension Syndrome: Hanging by a Thread (and a Rope) • Does the horizontal position increase risk of rescue death following suspension trauma? • Suspension trauma • Self-Rescue: The Best Fall Protection Equipment for It • Harness fitting part 1: number & type of adjusters • Best climbing harness review • Harness Safety • Preventing Suspension Trauma, fact sheet 5. • Ask a Pro: What is suspension trauma (AKA harness hang syndrome)? • Will your safety harness kill you? • Suspension Trauma/Orthostatic Intolerance: Safety and Health
Information Bulletin • Harness Suspension: review and evaluation of existing information • Risks and management of prolonged suspension in an Alpine harness








